User login
USPSTF gives breastfeeding support a ‘B’ grade
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
Anticipate monoclonals in first-line therapy for multiple myeloma
NEW YORK – Monoclonal antibodies may soon have more of a role in the front-line treatment setting for multiple myeloma and as part of precollection/transplant regimens–or “so-called in vivo purges,” according to Tomer M. Mark, MD, of the department of clinical medicine at the Cornell University, New York.
They could also be used both in the preclinical setting for smoldering multiple myeloma, and for maintenance following transplant, which makes sense given that they are, for the most part, not myelosuppressive and have “very tolerable toxicities,” he said.
Myeloma is “sort of catching up to lymphoma in terms of antibody use and development. ... Approval trials are underway,” Dr. Mark said at Imedex: Lymphoma & Myeloma, an international congress on hematologic malignancies.
The successes of the phase III trials CASTOR and POLLUX in patients with relapsed and refractory multiple myeloma have paved the way for trials to examine daratumumab in first-line combination therapy.
In POLLUX, progression-free survival, time to progression, and overall response rate were superior with daratumumab in combination with lenalidomide/dexamethasone, as compared with lenalidomide/dexamethasone alone, in relapsed or refractory multiple myeloma patients. In CASTOR, daratumumab in combination with bortezomib and dexamethasone was superior to bortezomib and dexamethasone alone in a similar patient population. Of note, the effect was attenuated in those with multiple prior lines of treatment, which is, perhaps, an argument for moving monoclonal antibodies closer to the start of therapy, he said.
Daratumumab (Darzalex), which targets CD38, is currently indicated for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent or who are double refractory to a proteasome inhibitor and an immunomodulatory agent.
Similarly, elotuzumab (Empliciti), an immunostimulatory monoclonal antibody targeting a cell-surface receptor with both direct activation of natural killer cells and the capacity to trigger antibody-dependent, cell-mediated cytotoxicity of myeloma cells, is indicated in combination with lenalidomide/dexamethasone in patients who have received one to three therapies. Elotuzumab was shown in one trial to be associated with progression-free survival of 68% at 1 and 41% at 2 years when used with lenalidomide/dexamethasone. Patients receiving elotuzumab had a relative reduction of 30% in the risk of disease progression or death as compared with the control group.
In an ongoing trial with initial results reported at the 2015 American Society of Hematology annual meeting, elotuzumab with bortezomib/dexamethasone was associated with a more modest improvement in median progression-free survival, which was 9.9 months with triple therapy and 6.8 months with bortezomib/dexamethasone alone.
Both drugs have shown activity as single agents. In a phase I study, elotuzumab was associated with disease stability in 26% of patients, Dr. Mark said. Daratumumab, used as monotherapy in a study of relapsed or relapsed/refractory multiple myeloma patients, was associated with good overall response and progression-free survival, and “quite amazing” overall survival of 65%.
Other monoclonal antibodies in development include isatuximab (anti-CD38), lorvotuzumab mertansine (anti-CD56), and indatuximab ravtansine (anti-CD128), Dr. Mark said.
Dr. Mark reported receiving research funding from Celgene and Amgen, serving on speakers bureaus for Celgene, Millennium, Amgen, and Bristol-Myers Squibb, and serving on an advisory committee for Celgene and Millennium.
NEW YORK – Monoclonal antibodies may soon have more of a role in the front-line treatment setting for multiple myeloma and as part of precollection/transplant regimens–or “so-called in vivo purges,” according to Tomer M. Mark, MD, of the department of clinical medicine at the Cornell University, New York.
They could also be used both in the preclinical setting for smoldering multiple myeloma, and for maintenance following transplant, which makes sense given that they are, for the most part, not myelosuppressive and have “very tolerable toxicities,” he said.
Myeloma is “sort of catching up to lymphoma in terms of antibody use and development. ... Approval trials are underway,” Dr. Mark said at Imedex: Lymphoma & Myeloma, an international congress on hematologic malignancies.
The successes of the phase III trials CASTOR and POLLUX in patients with relapsed and refractory multiple myeloma have paved the way for trials to examine daratumumab in first-line combination therapy.
In POLLUX, progression-free survival, time to progression, and overall response rate were superior with daratumumab in combination with lenalidomide/dexamethasone, as compared with lenalidomide/dexamethasone alone, in relapsed or refractory multiple myeloma patients. In CASTOR, daratumumab in combination with bortezomib and dexamethasone was superior to bortezomib and dexamethasone alone in a similar patient population. Of note, the effect was attenuated in those with multiple prior lines of treatment, which is, perhaps, an argument for moving monoclonal antibodies closer to the start of therapy, he said.
Daratumumab (Darzalex), which targets CD38, is currently indicated for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent or who are double refractory to a proteasome inhibitor and an immunomodulatory agent.
Similarly, elotuzumab (Empliciti), an immunostimulatory monoclonal antibody targeting a cell-surface receptor with both direct activation of natural killer cells and the capacity to trigger antibody-dependent, cell-mediated cytotoxicity of myeloma cells, is indicated in combination with lenalidomide/dexamethasone in patients who have received one to three therapies. Elotuzumab was shown in one trial to be associated with progression-free survival of 68% at 1 and 41% at 2 years when used with lenalidomide/dexamethasone. Patients receiving elotuzumab had a relative reduction of 30% in the risk of disease progression or death as compared with the control group.
In an ongoing trial with initial results reported at the 2015 American Society of Hematology annual meeting, elotuzumab with bortezomib/dexamethasone was associated with a more modest improvement in median progression-free survival, which was 9.9 months with triple therapy and 6.8 months with bortezomib/dexamethasone alone.
Both drugs have shown activity as single agents. In a phase I study, elotuzumab was associated with disease stability in 26% of patients, Dr. Mark said. Daratumumab, used as monotherapy in a study of relapsed or relapsed/refractory multiple myeloma patients, was associated with good overall response and progression-free survival, and “quite amazing” overall survival of 65%.
Other monoclonal antibodies in development include isatuximab (anti-CD38), lorvotuzumab mertansine (anti-CD56), and indatuximab ravtansine (anti-CD128), Dr. Mark said.
Dr. Mark reported receiving research funding from Celgene and Amgen, serving on speakers bureaus for Celgene, Millennium, Amgen, and Bristol-Myers Squibb, and serving on an advisory committee for Celgene and Millennium.
NEW YORK – Monoclonal antibodies may soon have more of a role in the front-line treatment setting for multiple myeloma and as part of precollection/transplant regimens–or “so-called in vivo purges,” according to Tomer M. Mark, MD, of the department of clinical medicine at the Cornell University, New York.
They could also be used both in the preclinical setting for smoldering multiple myeloma, and for maintenance following transplant, which makes sense given that they are, for the most part, not myelosuppressive and have “very tolerable toxicities,” he said.
Myeloma is “sort of catching up to lymphoma in terms of antibody use and development. ... Approval trials are underway,” Dr. Mark said at Imedex: Lymphoma & Myeloma, an international congress on hematologic malignancies.
The successes of the phase III trials CASTOR and POLLUX in patients with relapsed and refractory multiple myeloma have paved the way for trials to examine daratumumab in first-line combination therapy.
In POLLUX, progression-free survival, time to progression, and overall response rate were superior with daratumumab in combination with lenalidomide/dexamethasone, as compared with lenalidomide/dexamethasone alone, in relapsed or refractory multiple myeloma patients. In CASTOR, daratumumab in combination with bortezomib and dexamethasone was superior to bortezomib and dexamethasone alone in a similar patient population. Of note, the effect was attenuated in those with multiple prior lines of treatment, which is, perhaps, an argument for moving monoclonal antibodies closer to the start of therapy, he said.
Daratumumab (Darzalex), which targets CD38, is currently indicated for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent or who are double refractory to a proteasome inhibitor and an immunomodulatory agent.
Similarly, elotuzumab (Empliciti), an immunostimulatory monoclonal antibody targeting a cell-surface receptor with both direct activation of natural killer cells and the capacity to trigger antibody-dependent, cell-mediated cytotoxicity of myeloma cells, is indicated in combination with lenalidomide/dexamethasone in patients who have received one to three therapies. Elotuzumab was shown in one trial to be associated with progression-free survival of 68% at 1 and 41% at 2 years when used with lenalidomide/dexamethasone. Patients receiving elotuzumab had a relative reduction of 30% in the risk of disease progression or death as compared with the control group.
In an ongoing trial with initial results reported at the 2015 American Society of Hematology annual meeting, elotuzumab with bortezomib/dexamethasone was associated with a more modest improvement in median progression-free survival, which was 9.9 months with triple therapy and 6.8 months with bortezomib/dexamethasone alone.
Both drugs have shown activity as single agents. In a phase I study, elotuzumab was associated with disease stability in 26% of patients, Dr. Mark said. Daratumumab, used as monotherapy in a study of relapsed or relapsed/refractory multiple myeloma patients, was associated with good overall response and progression-free survival, and “quite amazing” overall survival of 65%.
Other monoclonal antibodies in development include isatuximab (anti-CD38), lorvotuzumab mertansine (anti-CD56), and indatuximab ravtansine (anti-CD128), Dr. Mark said.
Dr. Mark reported receiving research funding from Celgene and Amgen, serving on speakers bureaus for Celgene, Millennium, Amgen, and Bristol-Myers Squibb, and serving on an advisory committee for Celgene and Millennium.
EXPERT ANALYSIS FROM IMEDEX: LYMPHOMA & MYELOMA
TOPCAT, a third time around
Shakespeare, in Romeo and Juliet, refers to the proverb, “A cat has nine lives. For three he plays, for three he strays, and for the last he stays.”
TOPCAT is back again, having randomized its first patient with heart failure with preserved ejection fraction (HFpEF) almost 10 years ago for its treatment with spironolactone (SPIRO), a mineralocorticoid receptor antagonist.

The first report of the results of TOPCAT in 2014 indicated that there was no benefit associate with SPIRO therapy tested in the 3,445 patients randomized in 244 sites around the world (N Engl J Med. 2014 Apr 10;370[15]:1383-92). A subsequent analysis of data carried out in 2015 reported a striking regional difference in the outcome of patients randomized in the 1,767 patients in the Americas, compared with the 1,678 randomized in Russia and Georgia (Circulation. 2015 Jan 6;131[1]:34-42). In the Americas, there was an 18% decrease in the primary event of death and heart failure rehospitalization (3.6% in the SPIRO vs. 4.9% in the placebo; hazard ratio, 0.82; P = .026). There was essentially no difference in the groups randomized in Russia and Georgia, which had a 1.6% placebo event rate.
And now in 2016, at the recent meeting of the Heart Failure Society of America, we were informed that there was no detectable level of blood canrenone, a metabolite of SPIRO, in 30% of the 66 randomized patients in Russia and Georgia, compared with 3% of the patients randomized in the Americas (Cardiology News. Oct 2016. p 8). These data tend to confirm that the patients randomized in Russia and Georgia were either undertreated or not treated. In fact, after examination of the baseline characteristics of the two groups it is possible that many of the patients may not have had heart failure at all.
So what are we left with? One thing that is clear is that the management of TOPCAT was flawed and constitutes an example of how not to run an international clinical trial. Can we make any conclusion about the benefit of SPIRO? TOPCAT initially was powered for over 3,515 patients and 630 events in order to achieve a 85% benefit. The current analysis has now narrowed the population down to 1,787 patients with 522 events with an 18% decrease (P = .02) in the primary end point. During the mean follow-up of 3.3 years there was a placebo mortality of 4.9%, which is impressive in the setting of concomitant beta-blocker and renin angiotensin-converting enzyme inhibitor therapy. The only significant adverse observation was a threefold occurrence in hyperkalemia (potassium greater than 5.5 mmols/L) in the 25.2% in the Americas group treated with SPIRO, compared with the Russian-Georgian patients
Unfortunately the answer is not entirely clear. We all know who HFpEF patients are when they walk into the clinic but identifying them for a clinical trial has been difficult if not impossible. As for me, I will choose to treat their hypertension aggressively (not an easy task) and prevent or suppress their arrhythmias. In that project I will use beta-blockers and SPIRO to prevent their next heart failure episode and hope for the best.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Shakespeare, in Romeo and Juliet, refers to the proverb, “A cat has nine lives. For three he plays, for three he strays, and for the last he stays.”
TOPCAT is back again, having randomized its first patient with heart failure with preserved ejection fraction (HFpEF) almost 10 years ago for its treatment with spironolactone (SPIRO), a mineralocorticoid receptor antagonist.
The first report of the results of TOPCAT in 2014 indicated that there was no benefit associate with SPIRO therapy tested in the 3,445 patients randomized in 244 sites around the world (N Engl J Med. 2014 Apr 10;370[15]:1383-92). A subsequent analysis of data carried out in 2015 reported a striking regional difference in the outcome of patients randomized in the 1,767 patients in the Americas, compared with the 1,678 randomized in Russia and Georgia (Circulation. 2015 Jan 6;131[1]:34-42). In the Americas, there was an 18% decrease in the primary event of death and heart failure rehospitalization (3.6% in the SPIRO vs. 4.9% in the placebo; hazard ratio, 0.82; P = .026). There was essentially no difference in the groups randomized in Russia and Georgia, which had a 1.6% placebo event rate.
And now in 2016, at the recent meeting of the Heart Failure Society of America, we were informed that there was no detectable level of blood canrenone, a metabolite of SPIRO, in 30% of the 66 randomized patients in Russia and Georgia, compared with 3% of the patients randomized in the Americas (Cardiology News. Oct 2016. p 8). These data tend to confirm that the patients randomized in Russia and Georgia were either undertreated or not treated. In fact, after examination of the baseline characteristics of the two groups it is possible that many of the patients may not have had heart failure at all.
So what are we left with? One thing that is clear is that the management of TOPCAT was flawed and constitutes an example of how not to run an international clinical trial. Can we make any conclusion about the benefit of SPIRO? TOPCAT initially was powered for over 3,515 patients and 630 events in order to achieve a 85% benefit. The current analysis has now narrowed the population down to 1,787 patients with 522 events with an 18% decrease (P = .02) in the primary end point. During the mean follow-up of 3.3 years there was a placebo mortality of 4.9%, which is impressive in the setting of concomitant beta-blocker and renin angiotensin-converting enzyme inhibitor therapy. The only significant adverse observation was a threefold occurrence in hyperkalemia (potassium greater than 5.5 mmols/L) in the 25.2% in the Americas group treated with SPIRO, compared with the Russian-Georgian patients
Unfortunately the answer is not entirely clear. We all know who HFpEF patients are when they walk into the clinic but identifying them for a clinical trial has been difficult if not impossible. As for me, I will choose to treat their hypertension aggressively (not an easy task) and prevent or suppress their arrhythmias. In that project I will use beta-blockers and SPIRO to prevent their next heart failure episode and hope for the best.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Shakespeare, in Romeo and Juliet, refers to the proverb, “A cat has nine lives. For three he plays, for three he strays, and for the last he stays.”
TOPCAT is back again, having randomized its first patient with heart failure with preserved ejection fraction (HFpEF) almost 10 years ago for its treatment with spironolactone (SPIRO), a mineralocorticoid receptor antagonist.
The first report of the results of TOPCAT in 2014 indicated that there was no benefit associate with SPIRO therapy tested in the 3,445 patients randomized in 244 sites around the world (N Engl J Med. 2014 Apr 10;370[15]:1383-92). A subsequent analysis of data carried out in 2015 reported a striking regional difference in the outcome of patients randomized in the 1,767 patients in the Americas, compared with the 1,678 randomized in Russia and Georgia (Circulation. 2015 Jan 6;131[1]:34-42). In the Americas, there was an 18% decrease in the primary event of death and heart failure rehospitalization (3.6% in the SPIRO vs. 4.9% in the placebo; hazard ratio, 0.82; P = .026). There was essentially no difference in the groups randomized in Russia and Georgia, which had a 1.6% placebo event rate.
And now in 2016, at the recent meeting of the Heart Failure Society of America, we were informed that there was no detectable level of blood canrenone, a metabolite of SPIRO, in 30% of the 66 randomized patients in Russia and Georgia, compared with 3% of the patients randomized in the Americas (Cardiology News. Oct 2016. p 8). These data tend to confirm that the patients randomized in Russia and Georgia were either undertreated or not treated. In fact, after examination of the baseline characteristics of the two groups it is possible that many of the patients may not have had heart failure at all.
So what are we left with? One thing that is clear is that the management of TOPCAT was flawed and constitutes an example of how not to run an international clinical trial. Can we make any conclusion about the benefit of SPIRO? TOPCAT initially was powered for over 3,515 patients and 630 events in order to achieve a 85% benefit. The current analysis has now narrowed the population down to 1,787 patients with 522 events with an 18% decrease (P = .02) in the primary end point. During the mean follow-up of 3.3 years there was a placebo mortality of 4.9%, which is impressive in the setting of concomitant beta-blocker and renin angiotensin-converting enzyme inhibitor therapy. The only significant adverse observation was a threefold occurrence in hyperkalemia (potassium greater than 5.5 mmols/L) in the 25.2% in the Americas group treated with SPIRO, compared with the Russian-Georgian patients
Unfortunately the answer is not entirely clear. We all know who HFpEF patients are when they walk into the clinic but identifying them for a clinical trial has been difficult if not impossible. As for me, I will choose to treat their hypertension aggressively (not an easy task) and prevent or suppress their arrhythmias. In that project I will use beta-blockers and SPIRO to prevent their next heart failure episode and hope for the best.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Plecanatide safe, effective for chronic constipation
LAS VEGAS – Two new studies suggest that the peptide plecanatide is safe and effective in the treatment of chronic idiopathic constipation. The drug had a low rate of diarrhea, about 7.1%.
The research, presented in two posters at the annual meeting of the American College of Gastroenterology, includes a pooled efficacy and safety analysis from two previous phase III clinical trials, as well as an open-label extension study.
Though there is no way to be sure in the absence of head-to-head studies, plecanatide could have a better tolerability profile than the existing constipation drugs like lubiprostone (Amitiza) and linaclotide (Linzess).

The drug is a derivative of uroguanylin, a peptide found in the gastrointestinal tract. Like the native peptide, plecanatide stimulates digestive fluid movement in the proximal small intestine, which in turn encourages regular bowel function. “I think because it is so much closer to the innate uroguanylin molecule, it will have better tolerability,” said Dr. Rao in an interview.
The open-label study followed 2,370 patients who received 3-mg or 6-mg doses of plecanatide once daily for up to 72 weeks. The most common adverse events were diarrhea (7.1%) and urinary tract infection (2.2%), and these were the only adverse events that occurred at a frequency above 2%.
About 5% of patients discontinued due to adverse events, 3.1% because of diarrhea. Patients were also asked to score their satisfaction with the drug and their willingness to continue on it, and the median values to those answers corresponded to quite satisfied and quite likely to continue.
The other study was a pooled analysis of two previously presented double-blind, placebo-controlled phase III trials of plecanatide. These studies included 2,791 patients with chronic idiopathic constipation who were treated over the course of 12 weeks, with 3- and 6-mg doses. Both groups showed significant improvements in the rate of durable overall complete spontaneous bowel movements: 20.5% in the 3-mg group and 19.8% in the 6-mg group, compared with 11.5% in the placebo group (P less than .001 for both comparisons).
Patients experienced improvements as early as the first week of treatment (31.6% in the 3-mg group versus 16.1% in placebo, P less than .001), and improvements were maintained through the end of the treatment period. There were also significant improvements in secondary endpoints, including stool consistency, straining, and bloating.
Adverse events occurred in 30.6% of subjects taking the 3-mg dose and 31.1% of those taking 6 mg, compared with 28.7% in the placebo group. As with the long-term study, the most common adverse event was diarrhea (4.6% in 3 mg and 5.1% in 6 mg, compared with 1.3% in placebo). Of those in the 3-mg group, 4.1% discontinued, as did 4.5% in the 6-mg group, and 2.2% in the placebo group.
“I think these are very exciting results. They clearly show a benefit of plecanatide in patients with chronic constipation. These are really methodologically rigorous, large clinical trials that should provide doctors and patients with confidence that the drug will provide benefits,” commented William D. Chey, MD, a professor of medicine at the University of Michigan, Ann Arbor.
Plecanatide is also being developed for irritable bowel syndrome with constipation, and has finished recruitment for two phase III clinical trials, which Synergy expects to report on later this year.
Dr. Rao is a member of an advisory committee for Forest Laboratories, Hollister, In Control Medical, Ironwood, Sucampo, and Vibrant. Dr. Chey is a consultant for Ironwood and Synergy.
AGA Resource
AGA offers information for your patients about constipation at http://www.gastro.org/patient-care/conditions-diseases/constipation.
LAS VEGAS – Two new studies suggest that the peptide plecanatide is safe and effective in the treatment of chronic idiopathic constipation. The drug had a low rate of diarrhea, about 7.1%.
The research, presented in two posters at the annual meeting of the American College of Gastroenterology, includes a pooled efficacy and safety analysis from two previous phase III clinical trials, as well as an open-label extension study.
Though there is no way to be sure in the absence of head-to-head studies, plecanatide could have a better tolerability profile than the existing constipation drugs like lubiprostone (Amitiza) and linaclotide (Linzess).
The drug is a derivative of uroguanylin, a peptide found in the gastrointestinal tract. Like the native peptide, plecanatide stimulates digestive fluid movement in the proximal small intestine, which in turn encourages regular bowel function. “I think because it is so much closer to the innate uroguanylin molecule, it will have better tolerability,” said Dr. Rao in an interview.
The open-label study followed 2,370 patients who received 3-mg or 6-mg doses of plecanatide once daily for up to 72 weeks. The most common adverse events were diarrhea (7.1%) and urinary tract infection (2.2%), and these were the only adverse events that occurred at a frequency above 2%.
About 5% of patients discontinued due to adverse events, 3.1% because of diarrhea. Patients were also asked to score their satisfaction with the drug and their willingness to continue on it, and the median values to those answers corresponded to quite satisfied and quite likely to continue.
The other study was a pooled analysis of two previously presented double-blind, placebo-controlled phase III trials of plecanatide. These studies included 2,791 patients with chronic idiopathic constipation who were treated over the course of 12 weeks, with 3- and 6-mg doses. Both groups showed significant improvements in the rate of durable overall complete spontaneous bowel movements: 20.5% in the 3-mg group and 19.8% in the 6-mg group, compared with 11.5% in the placebo group (P less than .001 for both comparisons).
Patients experienced improvements as early as the first week of treatment (31.6% in the 3-mg group versus 16.1% in placebo, P less than .001), and improvements were maintained through the end of the treatment period. There were also significant improvements in secondary endpoints, including stool consistency, straining, and bloating.
Adverse events occurred in 30.6% of subjects taking the 3-mg dose and 31.1% of those taking 6 mg, compared with 28.7% in the placebo group. As with the long-term study, the most common adverse event was diarrhea (4.6% in 3 mg and 5.1% in 6 mg, compared with 1.3% in placebo). Of those in the 3-mg group, 4.1% discontinued, as did 4.5% in the 6-mg group, and 2.2% in the placebo group.
“I think these are very exciting results. They clearly show a benefit of plecanatide in patients with chronic constipation. These are really methodologically rigorous, large clinical trials that should provide doctors and patients with confidence that the drug will provide benefits,” commented William D. Chey, MD, a professor of medicine at the University of Michigan, Ann Arbor.
Plecanatide is also being developed for irritable bowel syndrome with constipation, and has finished recruitment for two phase III clinical trials, which Synergy expects to report on later this year.
Dr. Rao is a member of an advisory committee for Forest Laboratories, Hollister, In Control Medical, Ironwood, Sucampo, and Vibrant. Dr. Chey is a consultant for Ironwood and Synergy.
AGA Resource
AGA offers information for your patients about constipation at http://www.gastro.org/patient-care/conditions-diseases/constipation.
LAS VEGAS – Two new studies suggest that the peptide plecanatide is safe and effective in the treatment of chronic idiopathic constipation. The drug had a low rate of diarrhea, about 7.1%.
The research, presented in two posters at the annual meeting of the American College of Gastroenterology, includes a pooled efficacy and safety analysis from two previous phase III clinical trials, as well as an open-label extension study.
Though there is no way to be sure in the absence of head-to-head studies, plecanatide could have a better tolerability profile than the existing constipation drugs like lubiprostone (Amitiza) and linaclotide (Linzess).
The drug is a derivative of uroguanylin, a peptide found in the gastrointestinal tract. Like the native peptide, plecanatide stimulates digestive fluid movement in the proximal small intestine, which in turn encourages regular bowel function. “I think because it is so much closer to the innate uroguanylin molecule, it will have better tolerability,” said Dr. Rao in an interview.
The open-label study followed 2,370 patients who received 3-mg or 6-mg doses of plecanatide once daily for up to 72 weeks. The most common adverse events were diarrhea (7.1%) and urinary tract infection (2.2%), and these were the only adverse events that occurred at a frequency above 2%.
About 5% of patients discontinued due to adverse events, 3.1% because of diarrhea. Patients were also asked to score their satisfaction with the drug and their willingness to continue on it, and the median values to those answers corresponded to quite satisfied and quite likely to continue.
The other study was a pooled analysis of two previously presented double-blind, placebo-controlled phase III trials of plecanatide. These studies included 2,791 patients with chronic idiopathic constipation who were treated over the course of 12 weeks, with 3- and 6-mg doses. Both groups showed significant improvements in the rate of durable overall complete spontaneous bowel movements: 20.5% in the 3-mg group and 19.8% in the 6-mg group, compared with 11.5% in the placebo group (P less than .001 for both comparisons).
Patients experienced improvements as early as the first week of treatment (31.6% in the 3-mg group versus 16.1% in placebo, P less than .001), and improvements were maintained through the end of the treatment period. There were also significant improvements in secondary endpoints, including stool consistency, straining, and bloating.
Adverse events occurred in 30.6% of subjects taking the 3-mg dose and 31.1% of those taking 6 mg, compared with 28.7% in the placebo group. As with the long-term study, the most common adverse event was diarrhea (4.6% in 3 mg and 5.1% in 6 mg, compared with 1.3% in placebo). Of those in the 3-mg group, 4.1% discontinued, as did 4.5% in the 6-mg group, and 2.2% in the placebo group.
“I think these are very exciting results. They clearly show a benefit of plecanatide in patients with chronic constipation. These are really methodologically rigorous, large clinical trials that should provide doctors and patients with confidence that the drug will provide benefits,” commented William D. Chey, MD, a professor of medicine at the University of Michigan, Ann Arbor.
Plecanatide is also being developed for irritable bowel syndrome with constipation, and has finished recruitment for two phase III clinical trials, which Synergy expects to report on later this year.
Dr. Rao is a member of an advisory committee for Forest Laboratories, Hollister, In Control Medical, Ironwood, Sucampo, and Vibrant. Dr. Chey is a consultant for Ironwood and Synergy.
AGA Resource
AGA offers information for your patients about constipation at http://www.gastro.org/patient-care/conditions-diseases/constipation.
AT ACG 2016
Key clinical point: Plecanatide is safe and effective in the treatment of idiopathic chronic constipation.
Major finding: A long-term study and an analysis of two phase III clinical trials show the drug is effective at reducing constipation and has low rates of adverse events and discontinuation.
Data source: Open-label extension trial and randomized, placebo-controlled, clinical trials.
Disclosures: Dr. Rao is a member of an advisory committee for Forest Laboratories, Hollister, In Control Medical, Ironwood, Sucampo, and Vibrant. Dr. Chey is a consultant for Ironwood.
Protein May Predict Risk for Chemotherapy-Induced Peripheral Neuropathy
A promising biomarker strategy may help identify patients at risk for severe paclitaxel-induced neuropathy. Although weekly paclitaxel is more effective than a 3-weekly regimen, the treatment comes at the price of more severe sensory peripheral neuropathy (PN). As yet, treatment for chemotherapy-induced peripheral neuropathy (CIPN) is only symptomatic, say researchers from University of Singapore and National University Cancer Institute, Singapore.
Related: Is Chemotherapy a Good Choice for Neuroendocrine Tumors?
Their previous research, however, suggested that a protein called NDRG1 might be useful in predicting paclitaxel-induced PN. NDRG1 is a protein “ubiquitously” expressed in human tissues and tumors, the researchers note, particularly in peripheral nerve tissue. The protein also has been implicated in degrading myelin in Charcot-Marie-Tooth disease, a hereditary motor and sensory neuropathy.
Related: ASCO's Chemotherapy Administration Safety Standards
To expand on their earlier research, the researchers conducted another study in 111 patients with early stage breast cancer. Of those patients, 41% had human epidermal growth factor receptor (HER)-2 positive breast cancer and received adjuvant trastuzumab along with paclitaxel. Over a median of 12 weeks, 77 patients (69%) developed all-grade PN; in 17, the neuropathy was severe enough to mandate reducing or delaying doses or stopping paclitaxel. Peripheral neuropathy occurred before cycle 6 in 48%. Not surprisingly, patients with diabetes had more severe neuropathy (44% vs 11%). The researchers found no differences in neuropathy among various age groups or races; however, they also noted that most of the patients were Chinese.
Related: Palliative Chemotherapy May Be Harmful
The mean NDRG1 score of patients without severe neuropathy was 7.7, compared with 5.4 for patients with severe neuropathy. Fifty-four patients had an NDRGI score of < 7; of those, 13 (24%) developed severe neuropathy compared with only 4 of 57 (7%) of patients with a score above 7.
The researchers are performing a larger prospective study to explore the mechanisms of NDRG1 regulation to support their findings.
Source:
Sundar R, Jeyasekharan AD, Pang B, et al. PLoS ONE. 2016;11(10):e0164319.
doi:10.1371/journal.pone.0164319.
A promising biomarker strategy may help identify patients at risk for severe paclitaxel-induced neuropathy. Although weekly paclitaxel is more effective than a 3-weekly regimen, the treatment comes at the price of more severe sensory peripheral neuropathy (PN). As yet, treatment for chemotherapy-induced peripheral neuropathy (CIPN) is only symptomatic, say researchers from University of Singapore and National University Cancer Institute, Singapore.
Related: Is Chemotherapy a Good Choice for Neuroendocrine Tumors?
Their previous research, however, suggested that a protein called NDRG1 might be useful in predicting paclitaxel-induced PN. NDRG1 is a protein “ubiquitously” expressed in human tissues and tumors, the researchers note, particularly in peripheral nerve tissue. The protein also has been implicated in degrading myelin in Charcot-Marie-Tooth disease, a hereditary motor and sensory neuropathy.
Related: ASCO's Chemotherapy Administration Safety Standards
To expand on their earlier research, the researchers conducted another study in 111 patients with early stage breast cancer. Of those patients, 41% had human epidermal growth factor receptor (HER)-2 positive breast cancer and received adjuvant trastuzumab along with paclitaxel. Over a median of 12 weeks, 77 patients (69%) developed all-grade PN; in 17, the neuropathy was severe enough to mandate reducing or delaying doses or stopping paclitaxel. Peripheral neuropathy occurred before cycle 6 in 48%. Not surprisingly, patients with diabetes had more severe neuropathy (44% vs 11%). The researchers found no differences in neuropathy among various age groups or races; however, they also noted that most of the patients were Chinese.
Related: Palliative Chemotherapy May Be Harmful
The mean NDRG1 score of patients without severe neuropathy was 7.7, compared with 5.4 for patients with severe neuropathy. Fifty-four patients had an NDRGI score of < 7; of those, 13 (24%) developed severe neuropathy compared with only 4 of 57 (7%) of patients with a score above 7.
The researchers are performing a larger prospective study to explore the mechanisms of NDRG1 regulation to support their findings.
Source:
Sundar R, Jeyasekharan AD, Pang B, et al. PLoS ONE. 2016;11(10):e0164319.
doi:10.1371/journal.pone.0164319.
A promising biomarker strategy may help identify patients at risk for severe paclitaxel-induced neuropathy. Although weekly paclitaxel is more effective than a 3-weekly regimen, the treatment comes at the price of more severe sensory peripheral neuropathy (PN). As yet, treatment for chemotherapy-induced peripheral neuropathy (CIPN) is only symptomatic, say researchers from University of Singapore and National University Cancer Institute, Singapore.
Related: Is Chemotherapy a Good Choice for Neuroendocrine Tumors?
Their previous research, however, suggested that a protein called NDRG1 might be useful in predicting paclitaxel-induced PN. NDRG1 is a protein “ubiquitously” expressed in human tissues and tumors, the researchers note, particularly in peripheral nerve tissue. The protein also has been implicated in degrading myelin in Charcot-Marie-Tooth disease, a hereditary motor and sensory neuropathy.
Related: ASCO's Chemotherapy Administration Safety Standards
To expand on their earlier research, the researchers conducted another study in 111 patients with early stage breast cancer. Of those patients, 41% had human epidermal growth factor receptor (HER)-2 positive breast cancer and received adjuvant trastuzumab along with paclitaxel. Over a median of 12 weeks, 77 patients (69%) developed all-grade PN; in 17, the neuropathy was severe enough to mandate reducing or delaying doses or stopping paclitaxel. Peripheral neuropathy occurred before cycle 6 in 48%. Not surprisingly, patients with diabetes had more severe neuropathy (44% vs 11%). The researchers found no differences in neuropathy among various age groups or races; however, they also noted that most of the patients were Chinese.
Related: Palliative Chemotherapy May Be Harmful
The mean NDRG1 score of patients without severe neuropathy was 7.7, compared with 5.4 for patients with severe neuropathy. Fifty-four patients had an NDRGI score of < 7; of those, 13 (24%) developed severe neuropathy compared with only 4 of 57 (7%) of patients with a score above 7.
The researchers are performing a larger prospective study to explore the mechanisms of NDRG1 regulation to support their findings.
Source:
Sundar R, Jeyasekharan AD, Pang B, et al. PLoS ONE. 2016;11(10):e0164319.
doi:10.1371/journal.pone.0164319.
MACRA final rule exempts many more doctors
Physicians who do not have a large Medicare population or who do not bill much to Medicare Part B will get a bit more breathing room to avoid having to participate in MACRA’s Quality Payment Program.
In a final rule posted Oct. 14 that sets out how the Medicare Access and CHIP Reauthorization Act (MACRA) will work, the Centers for Medicare & Medicaid Services increased the threshold for inclusion in the new value-based payment program from the initial proposal of physicians who bill Medicare more than $10,000 per year or treat more than 100 Medicare patients per year to those who bill more than $30,000 per year or provide care to more than 100 Medicare patients per year.
However, agency officials noted that it is committed to helping these small and solo practices become active participants in the Quality Payment Program.

“We heard these concerns and are taking additional steps to aid small practices, including reducing the time and cost to participate, excluding more small practices, increasing the availability of Advanced APMs [Alternative Payment Models] to small practices, allowing practices to begin participation at their own pace, changing one of the qualifications for participation in Advanced APMs to be practice-based as an alternative to total cost–based, and conducting significant technical support and outreach to small practices using $20 million a year over the next 5 years.”
CMS officials estimate that the new threshold will exclude an estimated 380,000 physicians and health care providers, up from about 225,000 under the initially proposed threshold.
Mr. Slavitt added that with these changes, “we estimate that small [practice] physicians will have the same level of participation as that of other practice sizes.”
The flexibility of participation was first announced Sept. 8, in a blog post outlining four options for participation in the Quality Payment Program:
• Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
• Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
• Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
• Option 4: For those who qualify, participate in an Advanced Alternative Payment Model beginning next year.
That said, under the final rule, those who fail to do the bare minimum and report no data in 2017 will face a 4% pay cut in 2019.
“We are pleased CMS listened to the AGA’s concerns regarding the complexity of MACRA, its implementation, and its impact on small practices, among other issues,” said Timothy C. Wang, MD, AGAF, AGA Institute President, Columbia University, New York. “We believe that designation of 2017 as a transition year will allow GI’s the opportunity to understand the new value-based reimbursement system, and AGA stands ready to guide the GI community to survive and thrive in the new environment.”
“I am sure [the pay cuts are] going to impact some providers,” John Feore, director at Avalere Health, said in an interview. “But with the options, you can report on a very small number of measures, one for each of the categories, for a continuous 90-day period, and you will be sort of held harmless [and able] to transition over time into the program.”
Physician organizations were supportive of the final rule, particularly regarding how it addresses the concerns of small/solo practices.
CMS officials “took a significant step last month to address AMA concerns about the original proposal,” American Medical Association President Andrew W. Gurman, MD, said in a statement. “The final rule includes additional steps to help small and rural practices by raising the low-volume threshold exemption, and practices of all sizes will benefit from reduced MIPS reporting requirements. Our initial review indicates that CMS has been responsive to many concerns raised by the AMA.”
CMS officials said that the agency is looking into creating an accountable care organization (ACO) “Track 1 Plus” model that would qualify as an APM. Currently, ACOs that are in Track 1 share savings but do not assume risk. The agency said that the Track 1 Plus model would have organizations assuming some nominal level of risk that would be smaller, compared with those in the Medicare Shared Savings Program (MSSP) Track 2 and Track 3, as well as those that qualify as Next Generation ACOs. CMS plans to have the ACO Track 1 Plus Model ready for the 2018 reporting year.
Physicians who do not have a large Medicare population or who do not bill much to Medicare Part B will get a bit more breathing room to avoid having to participate in MACRA’s Quality Payment Program.
In a final rule posted Oct. 14 that sets out how the Medicare Access and CHIP Reauthorization Act (MACRA) will work, the Centers for Medicare & Medicaid Services increased the threshold for inclusion in the new value-based payment program from the initial proposal of physicians who bill Medicare more than $10,000 per year or treat more than 100 Medicare patients per year to those who bill more than $30,000 per year or provide care to more than 100 Medicare patients per year.
However, agency officials noted that it is committed to helping these small and solo practices become active participants in the Quality Payment Program.
“We heard these concerns and are taking additional steps to aid small practices, including reducing the time and cost to participate, excluding more small practices, increasing the availability of Advanced APMs [Alternative Payment Models] to small practices, allowing practices to begin participation at their own pace, changing one of the qualifications for participation in Advanced APMs to be practice-based as an alternative to total cost–based, and conducting significant technical support and outreach to small practices using $20 million a year over the next 5 years.”
CMS officials estimate that the new threshold will exclude an estimated 380,000 physicians and health care providers, up from about 225,000 under the initially proposed threshold.
Mr. Slavitt added that with these changes, “we estimate that small [practice] physicians will have the same level of participation as that of other practice sizes.”
The flexibility of participation was first announced Sept. 8, in a blog post outlining four options for participation in the Quality Payment Program:
• Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
• Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
• Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
• Option 4: For those who qualify, participate in an Advanced Alternative Payment Model beginning next year.
That said, under the final rule, those who fail to do the bare minimum and report no data in 2017 will face a 4% pay cut in 2019.
“We are pleased CMS listened to the AGA’s concerns regarding the complexity of MACRA, its implementation, and its impact on small practices, among other issues,” said Timothy C. Wang, MD, AGAF, AGA Institute President, Columbia University, New York. “We believe that designation of 2017 as a transition year will allow GI’s the opportunity to understand the new value-based reimbursement system, and AGA stands ready to guide the GI community to survive and thrive in the new environment.”
“I am sure [the pay cuts are] going to impact some providers,” John Feore, director at Avalere Health, said in an interview. “But with the options, you can report on a very small number of measures, one for each of the categories, for a continuous 90-day period, and you will be sort of held harmless [and able] to transition over time into the program.”
Physician organizations were supportive of the final rule, particularly regarding how it addresses the concerns of small/solo practices.
CMS officials “took a significant step last month to address AMA concerns about the original proposal,” American Medical Association President Andrew W. Gurman, MD, said in a statement. “The final rule includes additional steps to help small and rural practices by raising the low-volume threshold exemption, and practices of all sizes will benefit from reduced MIPS reporting requirements. Our initial review indicates that CMS has been responsive to many concerns raised by the AMA.”
CMS officials said that the agency is looking into creating an accountable care organization (ACO) “Track 1 Plus” model that would qualify as an APM. Currently, ACOs that are in Track 1 share savings but do not assume risk. The agency said that the Track 1 Plus model would have organizations assuming some nominal level of risk that would be smaller, compared with those in the Medicare Shared Savings Program (MSSP) Track 2 and Track 3, as well as those that qualify as Next Generation ACOs. CMS plans to have the ACO Track 1 Plus Model ready for the 2018 reporting year.
Physicians who do not have a large Medicare population or who do not bill much to Medicare Part B will get a bit more breathing room to avoid having to participate in MACRA’s Quality Payment Program.
In a final rule posted Oct. 14 that sets out how the Medicare Access and CHIP Reauthorization Act (MACRA) will work, the Centers for Medicare & Medicaid Services increased the threshold for inclusion in the new value-based payment program from the initial proposal of physicians who bill Medicare more than $10,000 per year or treat more than 100 Medicare patients per year to those who bill more than $30,000 per year or provide care to more than 100 Medicare patients per year.
However, agency officials noted that it is committed to helping these small and solo practices become active participants in the Quality Payment Program.
“We heard these concerns and are taking additional steps to aid small practices, including reducing the time and cost to participate, excluding more small practices, increasing the availability of Advanced APMs [Alternative Payment Models] to small practices, allowing practices to begin participation at their own pace, changing one of the qualifications for participation in Advanced APMs to be practice-based as an alternative to total cost–based, and conducting significant technical support and outreach to small practices using $20 million a year over the next 5 years.”
CMS officials estimate that the new threshold will exclude an estimated 380,000 physicians and health care providers, up from about 225,000 under the initially proposed threshold.
Mr. Slavitt added that with these changes, “we estimate that small [practice] physicians will have the same level of participation as that of other practice sizes.”
The flexibility of participation was first announced Sept. 8, in a blog post outlining four options for participation in the Quality Payment Program:
• Option 1: Test the quality payment program in 2017 by submitting data without facing any negative payment adjustments. This will give physicians the year to make sure their processes are in place and ready for broader participation in 2018 and beyond.
• Option 2: Delay the start of the performance period and participate for just part of 2017. Depending on how long a physician delays reporting quality information back to CMS, they could still qualify for a smaller bonus payment.
• Option 3: Participate for the entire calendar year as called for by the law and be eligible for the full participation bonuses.
• Option 4: For those who qualify, participate in an Advanced Alternative Payment Model beginning next year.
That said, under the final rule, those who fail to do the bare minimum and report no data in 2017 will face a 4% pay cut in 2019.
“We are pleased CMS listened to the AGA’s concerns regarding the complexity of MACRA, its implementation, and its impact on small practices, among other issues,” said Timothy C. Wang, MD, AGAF, AGA Institute President, Columbia University, New York. “We believe that designation of 2017 as a transition year will allow GI’s the opportunity to understand the new value-based reimbursement system, and AGA stands ready to guide the GI community to survive and thrive in the new environment.”
“I am sure [the pay cuts are] going to impact some providers,” John Feore, director at Avalere Health, said in an interview. “But with the options, you can report on a very small number of measures, one for each of the categories, for a continuous 90-day period, and you will be sort of held harmless [and able] to transition over time into the program.”
Physician organizations were supportive of the final rule, particularly regarding how it addresses the concerns of small/solo practices.
CMS officials “took a significant step last month to address AMA concerns about the original proposal,” American Medical Association President Andrew W. Gurman, MD, said in a statement. “The final rule includes additional steps to help small and rural practices by raising the low-volume threshold exemption, and practices of all sizes will benefit from reduced MIPS reporting requirements. Our initial review indicates that CMS has been responsive to many concerns raised by the AMA.”
CMS officials said that the agency is looking into creating an accountable care organization (ACO) “Track 1 Plus” model that would qualify as an APM. Currently, ACOs that are in Track 1 share savings but do not assume risk. The agency said that the Track 1 Plus model would have organizations assuming some nominal level of risk that would be smaller, compared with those in the Medicare Shared Savings Program (MSSP) Track 2 and Track 3, as well as those that qualify as Next Generation ACOs. CMS plans to have the ACO Track 1 Plus Model ready for the 2018 reporting year.
High-status occupation spells worse response to antidepressant therapy
VIENNA – Depressed patients with a high-status job appear to be significantly less responsive to antidepressant therapy than other workers, Joseph Zohar, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
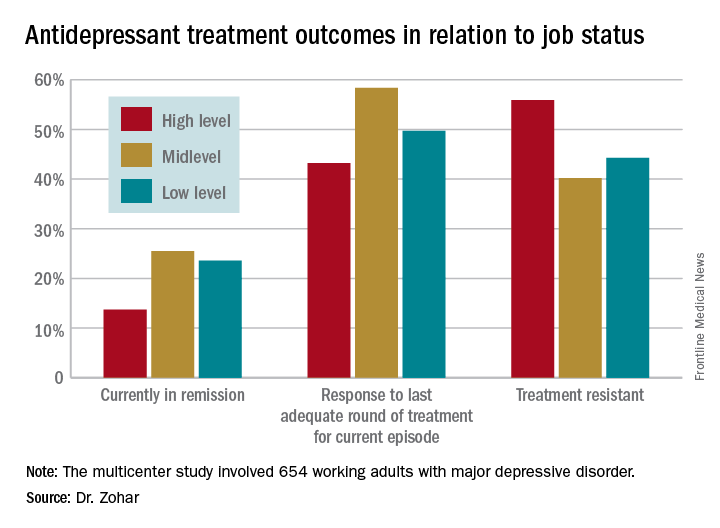
He presented a multicenter study of 654 Austrian, Israeli, Belgian, and Italian working adults with major depressive disorder. Those categorized as having a high occupational level were significantly less likely to have responded to the most recent trial of antidepressant medication for their current episode. They also had a significantly higher rate of treatment-resistant depression as defined by nonresponse to at least two previous adequate treatment trials, compared with the patients with mid- or low-level occupations.

“These results show that the need for precise prescribing is not only related to the symptoms and genetics but also to occupational level. One might need to prescribe different medication for the same disorder and need to take into account the occupational level in order to reach optimum effect,” he continued.
He and his coinvestigators categorized occupational level according to Hollingshead’s Occupational Scale, a tool widely used by sociologists. Occupational level is a different concept from socioeconomic status. It incorporates prestige, entry qualifications, job responsibilities, and skill requirements – as well as earnings. Examples of high occupational level jobs in this construct include physicians, engineers, architects, scientists, lawyers, CEOs, and professors.
Fifty-one percent of the study participants were classified as having high-status occupations, with the rest evenly divided between mid- and low-level occupations. Only 43.2% of patients in the high-level group had responded to their last treatment episode based upon clinical judgment and a Hamilton Depression Rating Scale score of 17 or less, compared with 58.4% of patients with mid- and 49.7% with low-level jobs.
At this point the explanation for the observed relationship between occupation level and antidepressant treatment response remains speculative. This is the first large study of its kind, and the results require confirmation. If the findings hold up, the results could have important implications for employers, who might want to discourage patients with high-status jobs and a history of treatment-resistant depression from particularly high work stress environments in order to reduce depression-related disability in the workplace, according to the psychiatrist.
Potential explanations for the findings include the possibility that depressed patients in high-level occupations are more likely to have poor illness acceptance, be less adherent to prescribed medications, or possess certain personality, cognitive, or behavioral differences that predispose to poor treatment outcome.
The study was funded by the ECNP’s Expert Platform on Mental Health – Focus on Depression. Dr. Zohar reported having no relevant financial conflicts.
VIENNA – Depressed patients with a high-status job appear to be significantly less responsive to antidepressant therapy than other workers, Joseph Zohar, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
He presented a multicenter study of 654 Austrian, Israeli, Belgian, and Italian working adults with major depressive disorder. Those categorized as having a high occupational level were significantly less likely to have responded to the most recent trial of antidepressant medication for their current episode. They also had a significantly higher rate of treatment-resistant depression as defined by nonresponse to at least two previous adequate treatment trials, compared with the patients with mid- or low-level occupations.
“These results show that the need for precise prescribing is not only related to the symptoms and genetics but also to occupational level. One might need to prescribe different medication for the same disorder and need to take into account the occupational level in order to reach optimum effect,” he continued.
He and his coinvestigators categorized occupational level according to Hollingshead’s Occupational Scale, a tool widely used by sociologists. Occupational level is a different concept from socioeconomic status. It incorporates prestige, entry qualifications, job responsibilities, and skill requirements – as well as earnings. Examples of high occupational level jobs in this construct include physicians, engineers, architects, scientists, lawyers, CEOs, and professors.
Fifty-one percent of the study participants were classified as having high-status occupations, with the rest evenly divided between mid- and low-level occupations. Only 43.2% of patients in the high-level group had responded to their last treatment episode based upon clinical judgment and a Hamilton Depression Rating Scale score of 17 or less, compared with 58.4% of patients with mid- and 49.7% with low-level jobs.
At this point the explanation for the observed relationship between occupation level and antidepressant treatment response remains speculative. This is the first large study of its kind, and the results require confirmation. If the findings hold up, the results could have important implications for employers, who might want to discourage patients with high-status jobs and a history of treatment-resistant depression from particularly high work stress environments in order to reduce depression-related disability in the workplace, according to the psychiatrist.
Potential explanations for the findings include the possibility that depressed patients in high-level occupations are more likely to have poor illness acceptance, be less adherent to prescribed medications, or possess certain personality, cognitive, or behavioral differences that predispose to poor treatment outcome.
The study was funded by the ECNP’s Expert Platform on Mental Health – Focus on Depression. Dr. Zohar reported having no relevant financial conflicts.
VIENNA – Depressed patients with a high-status job appear to be significantly less responsive to antidepressant therapy than other workers, Joseph Zohar, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
He presented a multicenter study of 654 Austrian, Israeli, Belgian, and Italian working adults with major depressive disorder. Those categorized as having a high occupational level were significantly less likely to have responded to the most recent trial of antidepressant medication for their current episode. They also had a significantly higher rate of treatment-resistant depression as defined by nonresponse to at least two previous adequate treatment trials, compared with the patients with mid- or low-level occupations.
“These results show that the need for precise prescribing is not only related to the symptoms and genetics but also to occupational level. One might need to prescribe different medication for the same disorder and need to take into account the occupational level in order to reach optimum effect,” he continued.
He and his coinvestigators categorized occupational level according to Hollingshead’s Occupational Scale, a tool widely used by sociologists. Occupational level is a different concept from socioeconomic status. It incorporates prestige, entry qualifications, job responsibilities, and skill requirements – as well as earnings. Examples of high occupational level jobs in this construct include physicians, engineers, architects, scientists, lawyers, CEOs, and professors.
Fifty-one percent of the study participants were classified as having high-status occupations, with the rest evenly divided between mid- and low-level occupations. Only 43.2% of patients in the high-level group had responded to their last treatment episode based upon clinical judgment and a Hamilton Depression Rating Scale score of 17 or less, compared with 58.4% of patients with mid- and 49.7% with low-level jobs.
At this point the explanation for the observed relationship between occupation level and antidepressant treatment response remains speculative. This is the first large study of its kind, and the results require confirmation. If the findings hold up, the results could have important implications for employers, who might want to discourage patients with high-status jobs and a history of treatment-resistant depression from particularly high work stress environments in order to reduce depression-related disability in the workplace, according to the psychiatrist.
Potential explanations for the findings include the possibility that depressed patients in high-level occupations are more likely to have poor illness acceptance, be less adherent to prescribed medications, or possess certain personality, cognitive, or behavioral differences that predispose to poor treatment outcome.
The study was funded by the ECNP’s Expert Platform on Mental Health – Focus on Depression. Dr. Zohar reported having no relevant financial conflicts.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Fifty-six percent of patients with high-status occupations who were treated for major depression were classified as treatment resistant, compared with 40% of patients with midlevel occupations and 44% with low-level occupations.
Data source: A study of 654 working adults with major depression in four countries.
Disclosures: The study was funded by the Expert Platform on Mental Health Focus on Depression. The presenter reported having no relevant financial conflicts.

Few non-ICU patients receive palliative care consults
LOS ANGELES – A significant percentage of patients who meet criteria for palliative care consultations do not receive a consult during their hospital stay, results from a single-center retrospective analysis showed.
“Physicians need to recognize the palliative care needs of patients with chronic illnesses other than malignancy before they get admitted to the ICU, especially when these patients are admitted repeatedly for the same problem [and] have a significant decline in functional status with a large symptom burden,” Mohleen Kang, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There is a potential missed opportunity for these conversations to occur with the patients and their family prior to their decompensation and crisis.”

Twenty-nine percent (132) of the patients studied met an indication for a palliative care consult (PCC), with only 35 (27%) of such patients having received a PCC. Patients with metastatic cancer were significantly more likely to have received a PCC, compared with non-cancer patients (64% vs. 21%, respectively; P less than .001), while patients with New York Heart Association Class III or IV congestive heart failure were less likely to receive a PCC, compared with those who did not have congestive heart failure (5.6% vs. 29.8%; P = .014).
Criteria for PCC on admission include a life-limiting diagnosis and more than one admission in the past 3 months, decline in function, or complex care requirements. Criteria for PCC during hospitalization include life-limiting diagnosis and uncertainty about decisions, an ICU stay greater than 7 days, or lack of goals of care.
Dr. Kang, chief resident in the department of medicine at New Jersey Medical School, Newark, presented the results, which were of patients admitted to the department of medicine at University Hospital in Newark in 2015. Those admitted to the ICU within 24 hours of admission were excluded from the analysis, leaving 461 patient charts that were screened for PCC needs based on the consensus report from the Center to Advance Palliative Care.
The patients who met an indication for PCC had a mean age of 60 years and an average length of stay of 7 days. The percentages of these patients who were female, African American, and Hispanic were 45%, 40%, and 21%, respectively.
On multivariate analysis, patients who had a PCC within 72 hours of admission were eight times more likely to have a hospital length of stay less than 7 days (P = .019), while those who had a PCC within 48 hours of admission were 20 times more likely to have a hospital length of stay less than 7 days (P = .017). “So if we intervened early, we were able to decrease their length of stay to less than 7 days,” Dr. Kang said at the meeting.
She acknowledged certain limitations of the study, including its small sample size, retrospective design, and lack of follow-up. “This study also has a lot of confounding socioeconomic factors that do not make it applicable to every hospital across the country,” she said. “This is not a homogeneous patient population.”
The study’s principal investigator was Anne Sutherland, MD, medical intensive care unit director at University Hospital. Dr. Kang reported having no financial disclosures.
LOS ANGELES – A significant percentage of patients who meet criteria for palliative care consultations do not receive a consult during their hospital stay, results from a single-center retrospective analysis showed.
“Physicians need to recognize the palliative care needs of patients with chronic illnesses other than malignancy before they get admitted to the ICU, especially when these patients are admitted repeatedly for the same problem [and] have a significant decline in functional status with a large symptom burden,” Mohleen Kang, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There is a potential missed opportunity for these conversations to occur with the patients and their family prior to their decompensation and crisis.”
Twenty-nine percent (132) of the patients studied met an indication for a palliative care consult (PCC), with only 35 (27%) of such patients having received a PCC. Patients with metastatic cancer were significantly more likely to have received a PCC, compared with non-cancer patients (64% vs. 21%, respectively; P less than .001), while patients with New York Heart Association Class III or IV congestive heart failure were less likely to receive a PCC, compared with those who did not have congestive heart failure (5.6% vs. 29.8%; P = .014).
Criteria for PCC on admission include a life-limiting diagnosis and more than one admission in the past 3 months, decline in function, or complex care requirements. Criteria for PCC during hospitalization include life-limiting diagnosis and uncertainty about decisions, an ICU stay greater than 7 days, or lack of goals of care.
Dr. Kang, chief resident in the department of medicine at New Jersey Medical School, Newark, presented the results, which were of patients admitted to the department of medicine at University Hospital in Newark in 2015. Those admitted to the ICU within 24 hours of admission were excluded from the analysis, leaving 461 patient charts that were screened for PCC needs based on the consensus report from the Center to Advance Palliative Care.
The patients who met an indication for PCC had a mean age of 60 years and an average length of stay of 7 days. The percentages of these patients who were female, African American, and Hispanic were 45%, 40%, and 21%, respectively.
On multivariate analysis, patients who had a PCC within 72 hours of admission were eight times more likely to have a hospital length of stay less than 7 days (P = .019), while those who had a PCC within 48 hours of admission were 20 times more likely to have a hospital length of stay less than 7 days (P = .017). “So if we intervened early, we were able to decrease their length of stay to less than 7 days,” Dr. Kang said at the meeting.
She acknowledged certain limitations of the study, including its small sample size, retrospective design, and lack of follow-up. “This study also has a lot of confounding socioeconomic factors that do not make it applicable to every hospital across the country,” she said. “This is not a homogeneous patient population.”
The study’s principal investigator was Anne Sutherland, MD, medical intensive care unit director at University Hospital. Dr. Kang reported having no financial disclosures.
LOS ANGELES – A significant percentage of patients who meet criteria for palliative care consultations do not receive a consult during their hospital stay, results from a single-center retrospective analysis showed.
“Physicians need to recognize the palliative care needs of patients with chronic illnesses other than malignancy before they get admitted to the ICU, especially when these patients are admitted repeatedly for the same problem [and] have a significant decline in functional status with a large symptom burden,” Mohleen Kang, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “There is a potential missed opportunity for these conversations to occur with the patients and their family prior to their decompensation and crisis.”
Twenty-nine percent (132) of the patients studied met an indication for a palliative care consult (PCC), with only 35 (27%) of such patients having received a PCC. Patients with metastatic cancer were significantly more likely to have received a PCC, compared with non-cancer patients (64% vs. 21%, respectively; P less than .001), while patients with New York Heart Association Class III or IV congestive heart failure were less likely to receive a PCC, compared with those who did not have congestive heart failure (5.6% vs. 29.8%; P = .014).
Criteria for PCC on admission include a life-limiting diagnosis and more than one admission in the past 3 months, decline in function, or complex care requirements. Criteria for PCC during hospitalization include life-limiting diagnosis and uncertainty about decisions, an ICU stay greater than 7 days, or lack of goals of care.
Dr. Kang, chief resident in the department of medicine at New Jersey Medical School, Newark, presented the results, which were of patients admitted to the department of medicine at University Hospital in Newark in 2015. Those admitted to the ICU within 24 hours of admission were excluded from the analysis, leaving 461 patient charts that were screened for PCC needs based on the consensus report from the Center to Advance Palliative Care.
The patients who met an indication for PCC had a mean age of 60 years and an average length of stay of 7 days. The percentages of these patients who were female, African American, and Hispanic were 45%, 40%, and 21%, respectively.
On multivariate analysis, patients who had a PCC within 72 hours of admission were eight times more likely to have a hospital length of stay less than 7 days (P = .019), while those who had a PCC within 48 hours of admission were 20 times more likely to have a hospital length of stay less than 7 days (P = .017). “So if we intervened early, we were able to decrease their length of stay to less than 7 days,” Dr. Kang said at the meeting.
She acknowledged certain limitations of the study, including its small sample size, retrospective design, and lack of follow-up. “This study also has a lot of confounding socioeconomic factors that do not make it applicable to every hospital across the country,” she said. “This is not a homogeneous patient population.”
The study’s principal investigator was Anne Sutherland, MD, medical intensive care unit director at University Hospital. Dr. Kang reported having no financial disclosures.
AT CHEST 2016
Key clinical point:
Major finding: Patients with metastatic cancer were significantly more likely to have received a PCC, compared with non-cancer patients (64% vs. 21%, respectively; P less than .001).
Data source: A retrospective study of 132 patients admitted to the department of medicine at University Hospital in Newark, N.J., in 2015.
Disclosures: Dr. Kang reported having no financial disclosures.
Fluid administration in sepsis did not increase need for dialysis
LOS ANGELES – Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Tex.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio, 0.915; 95% confidence interval, 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).

“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received greater than or equal to 30 mL/kg of fluid resuscitation, while 28% received greater than or equal to 20 mL/kg of intravenous fluid resuscitation. It turned out that staff in the emergency department - where most of the patients were treated in the critical first 6 hours - were concerned about fluid overload and throwing patients into respiratory, heart, or renal failure, Dr. Jahoor said. The team didn’t find a difference in mortality when patients received 30 mL/kg - just over 2 L in a 70-kg patient - versus 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27%, and 32%, respectively.
There also weren’t increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr. Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter. You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr. Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” he said.
The investigators had no relevant financial disclosures.
LOS ANGELES – Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Tex.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio, 0.915; 95% confidence interval, 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).
“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received greater than or equal to 30 mL/kg of fluid resuscitation, while 28% received greater than or equal to 20 mL/kg of intravenous fluid resuscitation. It turned out that staff in the emergency department - where most of the patients were treated in the critical first 6 hours - were concerned about fluid overload and throwing patients into respiratory, heart, or renal failure, Dr. Jahoor said. The team didn’t find a difference in mortality when patients received 30 mL/kg - just over 2 L in a 70-kg patient - versus 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27%, and 32%, respectively.
There also weren’t increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr. Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter. You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr. Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” he said.
The investigators had no relevant financial disclosures.
LOS ANGELES – Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Tex.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio, 0.915; 95% confidence interval, 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).
“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received greater than or equal to 30 mL/kg of fluid resuscitation, while 28% received greater than or equal to 20 mL/kg of intravenous fluid resuscitation. It turned out that staff in the emergency department - where most of the patients were treated in the critical first 6 hours - were concerned about fluid overload and throwing patients into respiratory, heart, or renal failure, Dr. Jahoor said. The team didn’t find a difference in mortality when patients received 30 mL/kg - just over 2 L in a 70-kg patient - versus 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27%, and 32%, respectively.
There also weren’t increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr. Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter. You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr. Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” he said.
The investigators had no relevant financial disclosures.
AT CHEST 2016
Key clinical point:
Major finding: For every 1 mL/kg of fluid administered, the likelihood of dialysis decreased by 8.5% (OR, 0.915; 95% CI, 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis.
Data source: A review of 164 septic patients.
Disclosures: The investigators had no relevant financial disclosures.
Data point to optimal window for endoscopy in sicker patients with peptic ulcer bleeding
The timing of endoscopy may make the difference between life and death in sicker patients with peptic ulcer bleeding, according to an analysis of more than 12,000 patients treated in Denmark.
Patients who were hemodynamically stable but had a higher level of comorbidity were about half as likely to die during their hospital stay if they underwent endoscopy within 12-36 hours of presentation as compared with sooner or later, results showed (Gastrointest Endosc. 2016 Sep 10. doi: 10.1016/j.gie.2016.08.049). And hemodynamically unstable patients had a roughly one-fourth reduction in the odds of death if they underwent the procedure within 6-24 hours.
“Although caution should be applied when interpreting these data, the current recommendation of endoscopy within 0-24 hours may not be optimal for all patients,” wrote the investigators, who were led by Stig B. Laursen, PhD, department of medical gastroenterology, Odense (Denmark) University Hospital.
“Our data may suggest that in patients with major comorbidities, the first few hours of hospital admission might be best used for optimising treatment of comorbidities, which may include correction of severe anaemia, reversal of anticoagulants, and investigation for possible infection that requires rapid treatment with antibiotics,” they elaborate. “Likewise, in patients with hemodynamic instability, endoscopy between 6 and 24 hours from time of admission to hospital allows time for optimal resuscitation and initiating treatment of comorbid diseases before endoscopy. However, these data should not lead to delayed endoscopy in patients with severe hemodynamic instability not responding to intensive resuscitation.”
The investigators analyzed data from 12,601 consecutive patients with peptic ulcer bleeding admitted between January 2005 and September 2013 to Danish hospitals, where all patients had access to 24-hour endoscopy. Time to endoscopy was assessed from hospital admission, defined as arrival in the emergency department, or from symptom onset in patients who developed bleeding when already hospitalized.
For analyses, the patients were stratified by hemodynamic status (a marker for the severity of bleeding) and by American Society of Anesthesiologists score (a marker for the extent of comorbidity).
The timing of endoscopy did not significantly influence in-hospital or 30-day mortality in hemodynamically stable patients with an American Society of Anesthesiologists score of 1-2 as a whole, Dr. Laursen and his colleagues report. Subgroup analyses suggested a reduction of in-hospital mortality when it was done between 0 and 24 hours in those patients whose bleeding began outside the hospital (adjusted odds ratio, 0.48).
In contrast, analyses revealed a U-shaped association between timing and mortality for hemodynamically stable patients with an American Society of Anesthesiologists score of 3-5. For this group, in-hospital mortality was significantly lower when endoscopy was performed within 12-36 hours as compared with times outside this window (adjusted OR, 0.48), and 30-day mortality tended to be lower as well.
Similarly, timing appeared to influence outcome for hemodynamically unstable patients, having both systolic blood pressure below 100 mm Hg and heart rate above 100 beats/min. For this group, performance of endoscopy within 6-24 hours was associated with significantly lower in-hospital mortality (adjusted OR, 0.73) and also 30-day mortality (adjusted OR, 0.66). Patients’ American Society of Anesthesiologists score did not appear to play a role here.
The study’s findings may have been affected by unmeasured and unknown confounders, acknowledge the investigators, who declared that they have no competing interests related to the research.
“Although a well-powered randomized controlled trial represents the best way to account for these problems, randomizing patients with [peptic ulcer bleeding] to early versus late endoscopy will be very difficult, including from an ethical and methodological point of view,” they note.
The timing of endoscopy may make the difference between life and death in sicker patients with peptic ulcer bleeding, according to an analysis of more than 12,000 patients treated in Denmark.
Patients who were hemodynamically stable but had a higher level of comorbidity were about half as likely to die during their hospital stay if they underwent endoscopy within 12-36 hours of presentation as compared with sooner or later, results showed (Gastrointest Endosc. 2016 Sep 10. doi: 10.1016/j.gie.2016.08.049). And hemodynamically unstable patients had a roughly one-fourth reduction in the odds of death if they underwent the procedure within 6-24 hours.
“Although caution should be applied when interpreting these data, the current recommendation of endoscopy within 0-24 hours may not be optimal for all patients,” wrote the investigators, who were led by Stig B. Laursen, PhD, department of medical gastroenterology, Odense (Denmark) University Hospital.
“Our data may suggest that in patients with major comorbidities, the first few hours of hospital admission might be best used for optimising treatment of comorbidities, which may include correction of severe anaemia, reversal of anticoagulants, and investigation for possible infection that requires rapid treatment with antibiotics,” they elaborate. “Likewise, in patients with hemodynamic instability, endoscopy between 6 and 24 hours from time of admission to hospital allows time for optimal resuscitation and initiating treatment of comorbid diseases before endoscopy. However, these data should not lead to delayed endoscopy in patients with severe hemodynamic instability not responding to intensive resuscitation.”
The investigators analyzed data from 12,601 consecutive patients with peptic ulcer bleeding admitted between January 2005 and September 2013 to Danish hospitals, where all patients had access to 24-hour endoscopy. Time to endoscopy was assessed from hospital admission, defined as arrival in the emergency department, or from symptom onset in patients who developed bleeding when already hospitalized.
For analyses, the patients were stratified by hemodynamic status (a marker for the severity of bleeding) and by American Society of Anesthesiologists score (a marker for the extent of comorbidity).
The timing of endoscopy did not significantly influence in-hospital or 30-day mortality in hemodynamically stable patients with an American Society of Anesthesiologists score of 1-2 as a whole, Dr. Laursen and his colleagues report. Subgroup analyses suggested a reduction of in-hospital mortality when it was done between 0 and 24 hours in those patients whose bleeding began outside the hospital (adjusted odds ratio, 0.48).
In contrast, analyses revealed a U-shaped association between timing and mortality for hemodynamically stable patients with an American Society of Anesthesiologists score of 3-5. For this group, in-hospital mortality was significantly lower when endoscopy was performed within 12-36 hours as compared with times outside this window (adjusted OR, 0.48), and 30-day mortality tended to be lower as well.
Similarly, timing appeared to influence outcome for hemodynamically unstable patients, having both systolic blood pressure below 100 mm Hg and heart rate above 100 beats/min. For this group, performance of endoscopy within 6-24 hours was associated with significantly lower in-hospital mortality (adjusted OR, 0.73) and also 30-day mortality (adjusted OR, 0.66). Patients’ American Society of Anesthesiologists score did not appear to play a role here.
The study’s findings may have been affected by unmeasured and unknown confounders, acknowledge the investigators, who declared that they have no competing interests related to the research.
“Although a well-powered randomized controlled trial represents the best way to account for these problems, randomizing patients with [peptic ulcer bleeding] to early versus late endoscopy will be very difficult, including from an ethical and methodological point of view,” they note.
The timing of endoscopy may make the difference between life and death in sicker patients with peptic ulcer bleeding, according to an analysis of more than 12,000 patients treated in Denmark.
Patients who were hemodynamically stable but had a higher level of comorbidity were about half as likely to die during their hospital stay if they underwent endoscopy within 12-36 hours of presentation as compared with sooner or later, results showed (Gastrointest Endosc. 2016 Sep 10. doi: 10.1016/j.gie.2016.08.049). And hemodynamically unstable patients had a roughly one-fourth reduction in the odds of death if they underwent the procedure within 6-24 hours.
“Although caution should be applied when interpreting these data, the current recommendation of endoscopy within 0-24 hours may not be optimal for all patients,” wrote the investigators, who were led by Stig B. Laursen, PhD, department of medical gastroenterology, Odense (Denmark) University Hospital.
“Our data may suggest that in patients with major comorbidities, the first few hours of hospital admission might be best used for optimising treatment of comorbidities, which may include correction of severe anaemia, reversal of anticoagulants, and investigation for possible infection that requires rapid treatment with antibiotics,” they elaborate. “Likewise, in patients with hemodynamic instability, endoscopy between 6 and 24 hours from time of admission to hospital allows time for optimal resuscitation and initiating treatment of comorbid diseases before endoscopy. However, these data should not lead to delayed endoscopy in patients with severe hemodynamic instability not responding to intensive resuscitation.”
The investigators analyzed data from 12,601 consecutive patients with peptic ulcer bleeding admitted between January 2005 and September 2013 to Danish hospitals, where all patients had access to 24-hour endoscopy. Time to endoscopy was assessed from hospital admission, defined as arrival in the emergency department, or from symptom onset in patients who developed bleeding when already hospitalized.
For analyses, the patients were stratified by hemodynamic status (a marker for the severity of bleeding) and by American Society of Anesthesiologists score (a marker for the extent of comorbidity).
The timing of endoscopy did not significantly influence in-hospital or 30-day mortality in hemodynamically stable patients with an American Society of Anesthesiologists score of 1-2 as a whole, Dr. Laursen and his colleagues report. Subgroup analyses suggested a reduction of in-hospital mortality when it was done between 0 and 24 hours in those patients whose bleeding began outside the hospital (adjusted odds ratio, 0.48).
In contrast, analyses revealed a U-shaped association between timing and mortality for hemodynamically stable patients with an American Society of Anesthesiologists score of 3-5. For this group, in-hospital mortality was significantly lower when endoscopy was performed within 12-36 hours as compared with times outside this window (adjusted OR, 0.48), and 30-day mortality tended to be lower as well.
Similarly, timing appeared to influence outcome for hemodynamically unstable patients, having both systolic blood pressure below 100 mm Hg and heart rate above 100 beats/min. For this group, performance of endoscopy within 6-24 hours was associated with significantly lower in-hospital mortality (adjusted OR, 0.73) and also 30-day mortality (adjusted OR, 0.66). Patients’ American Society of Anesthesiologists score did not appear to play a role here.
The study’s findings may have been affected by unmeasured and unknown confounders, acknowledge the investigators, who declared that they have no competing interests related to the research.
“Although a well-powered randomized controlled trial represents the best way to account for these problems, randomizing patients with [peptic ulcer bleeding] to early versus late endoscopy will be very difficult, including from an ethical and methodological point of view,” they note.
Key clinical point:
Major finding: In-hospital mortality was lower when endoscopy was performed within 12-36 hours in hemodynamically stable patients with higher comorbidity (odds ratio, 0.48) and within 6-24 hours in hemodynamically unstable patients (OR, 0.73).
Data source: A nationwide cohort study of 12,601 consecutive patients admitted to Danish hospitals with peptic ulcer bleeding.
Disclosures: The investigators declare that they do not have any competing interests.