User login
Early and Accurate Identification of Parkinson Disease Among US Veterans (FULL)
Parkinson disease (PD) affects about 680,000 in the US, including > 110,000 veterans (Caroline Tanner, MD, PhD, unpublished data).1 In the next 10 years, this number is expected to double, in part because of the aging of the US population.1 Although the classic diagnostic criteria emphasize motor symptoms that include tremor, gait disturbance, and paucity of movement, there is increasing recognition that disease pathology begins decades before the development of motor impairment.2
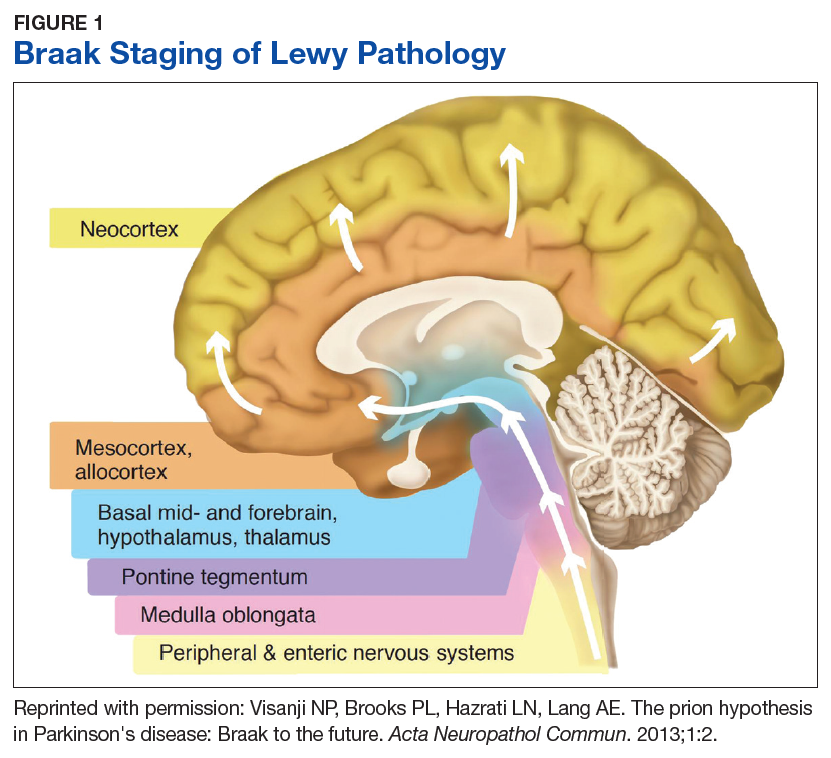
Pathologic studies confirm that by the onset of motor symptoms, at least 30% of nigrostriatal neurons are lost or dysfunctional.3-5 Similarly, the Braak staging hypothesis posits initial deposition of Lewy bodies in the olfactory bulb and the dorsal motor nucleus of the vagus nerve, followed by prion-like spread through the brain stem into the midbrain/substantia nigra, and finally into the cortex (Figure 1).6
The decades-long prodromal or preclinical phase represents a unique opportunity for early identification of those at highest risk for developing the motor symptoms of Parkinson disease.7 Accurate identification, ideally before the onset of manifest motor disability, would not only improve prognostic counseling of veterans and families, but also could allow for early enrollment into trials of potentially disease-modifying therapeutic agents. Thus, early and accurate identification of PD is an important goal of the care of veterans with potential PD.
Prodromal Symptoms
Prodromal PD, as defined by the International Parkinson Disease and Movement Disorders Society (MDS), focuses on nonmotor symptoms that herald the onset of manifest motor PD.8 The most commonly assessed nonmotor features include olfaction, constipation, sleep disturbance, and mood disorders.
Olfaction is impaired in > 90% of patients with motor PD at the time of diagnosis; by contrast, the prevalence of hyposmia in the general population ranges from 20% to 50%, with higher rates in older adults and in smokers.9-11 Thus, olfaction appears to be a relatively sensitive, though nonspecific, prodromal feature. Importantly, subjective report of hyposmia is poorly reliable, so a number of different tests have been developed for objective assessment of olfactory dysfunction.12 The 12-item Brief Smell Identification Test (B-SIT), derived from the longer University of Pennsylvania Smell Identification Test, is a “scratch-and-sniff” forced multiple choice test that can be self-administered by cooperative patients.13,14 The B-SIT has been validated in multiple ethnic and cultural groups and shows high discrimination between PD subjects and controls.13,15 Of note, olfactory impairment appears to be associated with risk of cognitive decline in PD, further emphasizing the need for accurate assessment to guide prognosis.16
Like hyposmia, constipation can be noted long before the diagnosis of manifest motor PD.17 After adjustment for lifestyle factors, constipated individuals have up to 4.5-fold increased odds of developing PD, and those with constipation suffer worsened disease outcomes and health-related quality of life.17-20 Some groups have demonstrated alterations in gut microbiota of those with prodromal PD, which suggests local inflammatory processes and intestinal permeability may contribute to protein misfolding and disease development.21,22 This also raises the intriguing possibility that dietary alterations may be neuroprotective or neurorestorative, although this has yet to be tested in humans.23,24
Like constipation, mood changes can precede the appearance of manifest motor PD.25,26 Case control studies suggest a higher risk of developing PD among individuals who were previously diagnosed with depression or anxiety, particularly in the 1 to 2 years prior to PD diagnosis.27-29 Both apathy and anxiety are associated with striatal dopamine dysfunction, particularly in the right caudate nucleus, which suggests that mood changes are directly related to disease pathology.30,31
Of the prodromal features, rapid eye movement sleep behavior disorder (RBD) is associated with the highest risk of conversion to motor PD.8 Up to 80% of older men with socalled idiopathic RBD develop a parkinsonian syndrome within 20 years; risk is divided about equally between idiopathic PD and dementia with Lewy bodies (DLB).32 Collateral history from a bed-partner is usually sufficient to make the diagnosis, although, this is often confounded by the prevalence of nightmares in those with posttraumatic stress disorder in the veteran population.32 Thus, in suspected cases, obtaining a polysomnogram can aid in distinguishing between idiopathic PC and DLB.33 Given the specificity of RBD as a marker of synuclein deposition and the high risk of progression to a degenerative syndrome, accurate diagnosis and counseling is imperative.
Each of the prodromal nonmotor features of PD are at best moderately sensitive or specific in isolation, but in concert, they can be used to develop a Parkinson risk score. For instance, the MDS prodromal criteria combine individual likelihood ratios into Bayesian analysis to determine a combined probability of PD, which can be further stratified to probable or possible prodromal PD (probability > 80%, > 50%, respectively).8 These criteria have been applied to several independent cohorts and demonstrate high sensitivity and specificity, especially over time.34,35 Applicability in a veteran population has yet to be determined.
Use of Imaging in Diagnosis
Although clinical diagnostic criteria and prodromal features can improve diagnostic accuracy, it can be extremely challenging to distinguish idiopathic PD from nondegenerative parkinsonism or atypical syndromes (see below). Compared with the gold standard of pathologic assessment, the clinical diagnostic accuracy for PD ranges from 73% for nonexperts to 80% for fellowship-trained movement disorders specialists.36 Thus, objective biomarkers are sought to improve diagnostic accuracy both for clinical care as well as for research purposes, such as enrollment into clinical trials.
Multiple potential imaging biomarkers for preclinical PD can aid in early diagnosis and help differentiate PD from related but distinct disorders. While beyond the scope of this review, these techniques have recently been reviewed.7 Of these, the most widely available and accurate is dopamine transporter (DAT) imaging, which uses a radioiodinated ligand that binds to DAT on striatal dopaminergic terminals; binding is detected through single photon emission computed tomography (SPECT) scanning. Thus, a SPECT DaTscan (GE Healthcare Bio-Sciences, Little Chalfont, England) directly assesses the integrity of the presynaptic nigrostriatal system and is well correlated with severity of motor and nonmotor parkinsonism.37,38
In individuals with suspected prodromal PD, abnormal DaTscans are associated with faster progression to manifest motor PD.39 However, it should be noted that a number of medications, several of which are commonly utilized in the veteran population, can affect the outcome of a DaTscan.40 Some of these medications only mildly affect the outcome, so the physician interpreting the scan should be made aware of their use, while others need to be held for days to weeks so as not to invalidate the DaTscan. DaTscan also do not differentiate between PD and atypical degenerative parkinsonisms such as multiple system atrophy (MSA), DLB, progressive supranuclear palsy (PSP), or corticobasal syndrome (CBS). Nevertheless, these scans can be used to distinguish degenerative parkinsonisms from other conditions that can be difficult to distinguish clinically from PD, including essential tremor, normal pressure hydrocephalus, vascular parkinsonism, or druginduced parkinsonism (DIP).
DIP usually is caused by blockade of postsynaptic dopamine receptors by antipsychotic medications, which are prescribed to as many as 1 in 4 older veterans; antiemetic agents such as metoclopramide are also potential offenders if used chronically.41 The risk of DIP appears to be associated with the D2 binding affinity of the drug. Thus, of the newer atypical antipsychotics, clozapine and quetiapine appear to have the lowest risk, while ziprasidone and aripiprazole have the highest binding affinity and therefore the highest risk.42 In many patients, parkinsonism persists even after discontinuation of the offending agent, suggesting that in at least a subset of patients, DIP may be an “unmasking” of latent PD rather than a true adverse effect of the medication. The prodromal features discussed above can be used to distinguish isolated DIP from unmasked latent PD.43 In a study we conducted in veterans at the Michael J. Crescenz VA Medical Center in Philadelphia, Pennsylvania, hyposmia in particular was shown to be highly predictive of an underlying dopaminergic deficit with an odds ratio of 63.44
Other important considerations in the differential diagnosis of PD are the atypical degenerative parkinsonian syndromes, formerly called Parkinson plus syndromes. These may be further divided into the synucleinopathies (MSA, DLB) or the tauopathies (PSP, CBS), depending on the predominant amyloidogenic protein. Early in the disease, the atypical syndromes and idiopathic PD may be clinically indistinguishable, although the atypical syndromes tend to progress more rapidly and often have a less robust response to levodopa.
Radiologic and fluid biomarkers for the atypical syndromes are under active investigation; at present the most accessible study is magnetic resonance imaging (MRI), which may show characteristic features such as degeneration of the pontocerebellar fibers in MSA or midbrain atrophy in PSP.45,46 By contrast, standard MRI sequences in idiopathic PD are usually normal, although high-resolution (7 tesla) imaging can reveal loss of neuromelanin in the substantia nigra.47 MRI also can be useful in the workup of suspected normal pressure hydrocephalus or vascular parkinsonism, which would show disproportionate ventriculomegaly with transependymal flow, or white matter lesions in the basal ganglia, respectively.
Data-Based Identification of Preclinical PD
The integration of clinical motor or prodromal features with biomarker data has led to the development of several large-scale clinical and administrative databases to identify PD. The Parkinson Progression Markers Initiative initially enrolled only de novo clinically identified people with PD, but it expanded to include a prodromal cohort who are being assessed for rates of conversion to PD.48 Similarly, metabolic imaging can be combined with prodromal symptoms, such as hyposmia or RBD, to predict risk for phenoconversion into manifest motor PD.49
The PREDICT-PD study synthesizes mood symptoms, RBD, smell testing, genotyping, and keyboard-tapping tasks to divide individuals into high-, middle-, and low-risk groups; interim analysis at 3 years of follow-up (N = 842) demonstrated a hazard ratio of 4.39 (95% CI, 1.03-18.68) for the diagnosis of PD in the highrisk group compared with the low-risk group.50 Lastly, administrative claims data for prodromal features, such as constipation, RBD, and mood symptoms, is highly predictive of eventual PD diagnosis.51 VA databases accessed through the Corporate Data Warehouse are complementary sources of information to nonveteranspecific Medicare databases; to our knowledge there has not yet been a comprehensive search of VA databases to identify veterans with preclinical PD.
Risk Factors Associated With Military Service
A number of potential environmental risk factors may increase the risk of developing Parkinson disease for veterans. Perhaps the most commonly recognized is pesticide exposure, particularly given the presumptive service connections established by the VA for Parkinson disease and exposure to Agent Orange or contaminated water at Camp Lejeune.52,53 Both dioxin, the toxic ingredient in Agent Orange, and the solvents trichloroethylene and perchloroethylene, found in the water supply at Camp Lejeune, interfere with mitochondrial function leading to oxidative stress and apoptosis of nigrostriatal neurons.54,55 Other potential exposures, which are not necessarily limited to the veteran population, include rotenone, a phytochemical used to kill fish in reservoirs, and paraquat, an herbicide that may directly promote synuclein aggregation.56,57 Veterans who have reported exposure to these or other environmental chemicals in civilian life should be carefully assessed for the presence of motor PD or prodromal features.
Traumatic brain injury (TBI) also may be a risk factor for PD, which may be particularly relevant for veterans who had served in Iraq or Afghanistan. Retrospective claims data suggest a strong association between PD and recent TBI in the 5 to 10 years prior to motor PD diagnosis.58,59 A recent assessment of combat veterans with TBI found that even mild TBI was associated with a 56% increased risk of PD, while moderate-to-severe TBI was associated with an 83% higher risk of PD.60 The pathologic mechanism for this link is unclear, but post-TBI inflammatory processes may lead to the formation of reactive oxygen species and/or glutamatergic excitotoxicity, thus leading to secondary injury in the nigrostriatal pathway.61 As with prodromal symptoms, the risk of PD related to environmental risk factors may be synergistic; repetitive TBI may be more damaging than a single injury, and a combination of TBI and pesticide exposure markedly increases PD risk beyond the risk of TBI or the risk of pesticides alone.62 Recently, parkinsonism, including Parkinson disease, was recognized as a service connected condition for veterans with a servicerelated moderate or severe TBI.63
Conclusion
Because of the substantial impact on quality of life and disability-adjusted life years, early and accurate identification and management of veterans at risk for PD is an important priority area for the VA. The 10-year cost of PD-related benefits through the VA was estimated at $3.5 billion in fiscal year 2010, and that number is likely to rise in coming years, due to the aging population as well as synergistic effects of independent risk factors described above.64 In response, the VA has created a network of specialty care sites, known as Parkinson Disease Research, Education, and Clinical Centers (PADRECCs) located in Philadelphia, Pennsylvania; Richmond, Virginia; Houston, Texas; West Los Angeles and San Francisco, California; and Seattle, Washington/ Portland, Oregon (www.parkinsons.va.gov).
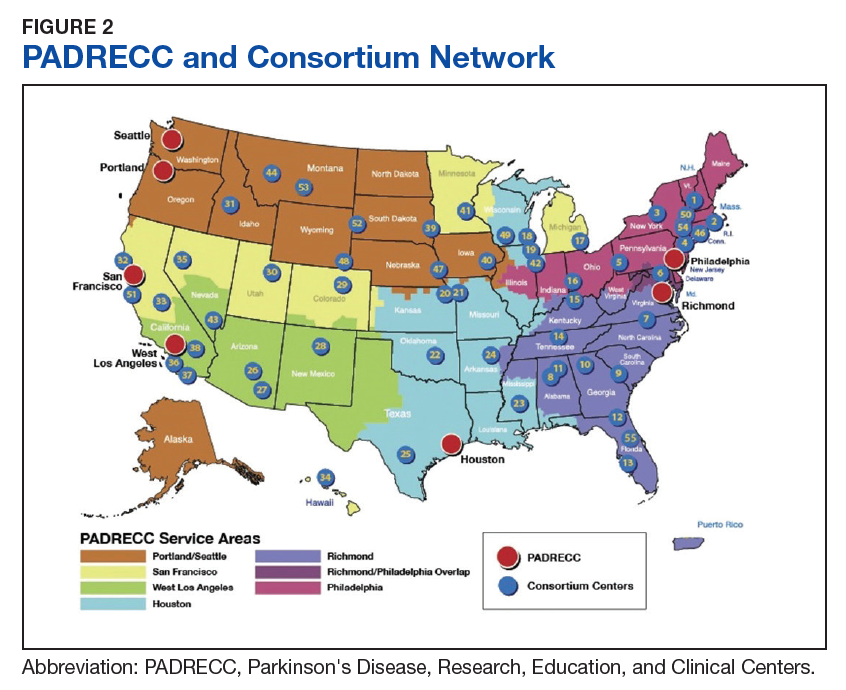
The PADRECCs are supplemented by a National VA PD Consortium network of VA physicians trained in PD management (Figure 2). Studies, including one investigating care of veterans with PD, have demonstrated that involvement of specialty care services early in the course of PD leads to improved patient outcomes.65,66 In addition to patient-facing resources such as support groups and specialized physical/occupational/speech therapy, PADRECCs and the consortium sites are national leaders in PD education and clinical trials and provide high-quality, multidisciplinary care for veterans with PD.67 Thus, veterans with significant risk factors or prodromal symptoms of PD should be referred into the PADRECC/Consortium network in order to maximize their quality of care and quality of life.
1. Marras C, Beck JC, Bower JH, et al; Parkinson’s Foundation P4 Group. Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 2018;4:21.
2. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591-1601.
3. Fearnley JM, Lees AJ. Ageing and Parkinson’s disease: substantia nigra regional selectivity. Brain. 1991;114(pt 5):2283-2301.
4. Greffard S, Verny M, Bonnet A-M, et al. Motor score of the Unified Parkinson Disease Rating Scale as a good predictor of Lewy body-associated neuronal loss in the substantia nigra. Arch Neurol. 2006;63(4):584-588.
5. Hilker R, Schweitzer K, Coburger S, et al. Nonlinear progression of Parkinson disease as determined by serial positron emission tomographic imaging of striatal fluorodopa F 18 activity. Arch Neurol. 2005;62(3):378-382.
6. Braak H, Del Tredici K, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
7. Mantri S, Morley JF, Siderowf AD. The importance of preclinical diagnostics in Parkinson disease. Parkinsonism Relat Disord. 2018;pii:S1353-8020(18)30396-1. [Epub ahead of print]
8. Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2015;30(12):1600-1611.
9. Haehner A, Boesveldt S, Berendse HW, et al. Prevalence of smell loss in Parkinson’s disease – a multicenter study. Parkinsonism Relat Disord. 2009;15(7):490-494.
10. Mullol J, Alobid I, Mariño-Sánchez F, et al. Furthering the understanding of olfaction, prevalence of loss of smell and risk factors: a population-based survey (OLFACAT study). BMJ Open. 2012;2(6).pii:e001256.
11. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, Rosenberg L. Smell identification ability: changes with age. Science. 1984;226(4681):1441-1443.
12. Doty RL. Olfactory dysfunction in Parkinson disease. Nat Rev Neurol. 2012;8(6):329-339.
13. Double KL, Rowe DB, Hayes M, et al. Identifying the pattern of olfactory deficits in Parkinson disease using the brief smell identification test. Arch Neurol. 2003;60(4):545-549.
14. Doty RL, Shaman P, Dann M. Development of the University of Pennsylvania Smell Identification Test: a standardized microencapsulated test of olfactory function. Physiol Behav. 1984;32(3):489-502.
15. Morley JF, Cohen A, Silveira-Moriyama L, et al. Optimizing olfactory testing for the diagnosis of Parkinson’s disease: item analysis of the University of Pennsylvania smell identification test. NPJ Parkinsons Dis. 2018;4:2.
16. Fullard ME, Tran B, Xie SX, et al. Olfactory impairment predicts cognitive decline in early Parkinson’s disease. Parkinsonism Relat Disord. 2016;25:45-51.
17. Savica R, Carlin JM, Grossardt BR, et al. Medical records documentation of constipation preceding Parkinson disease: a case-control study. Neurology. 2009;73(21):1752-1758.
18. Abbott RD, Petrovitch H, White LR, et al. Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology. 2001;57(3):456-462.
19. Stocchi F, Torti M. Constipation in Parkinson’s disease. Int Rev Neurobiol. 2017;134:811-826.
20. Yu QJ, Yu SY, Zuo LJ, et al. Parkinson disease with constipation: clinical features and relevant factors. Sci Rep. 2018;8(1):567.
21. Hill-Burns EM, Debelius JW, Morton JT, et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov Disord. 2017;32(5):739-749.
22. Mulak A, Bonaz B. Brain-gut-microbiota axis in Parkinson’s disease. World J Gastroenterol. 2015;21(37): 10609-10620.
23. Shah SP, Duda JE. Dietary modifications in Parkinson’s disease: a neuroprotective intervention? Med Hypotheses. 2015;85(6):1002-1005.
24. Perez-Pardo P, de Jong EM, Broersen LM, et al. Promising effects of neurorestorative diets on motor, cognitive, and gastrointestinal dysfunction after symptom development in a mouse model of Parkinson’s disease. Front Aging Neurosci. 2017;9:57.
25. Fang F, Xu Q, Park Y, et al. Depression and the subsequent risk of Parkinson’s disease in the NIH-AARP Diet and Health Study. Mov Disord. 2010;25(9):1157-1162.
26. Leentjens AFG, Van den Akker M, Metsemakers JFM, Lousberg R, Verhey FRJ. Higher incidence of depression preceding the onset of Parkinson’s disease: a register study. Mov Disord. 2003;18(4):414-418.
27. Alonso A, Rodriguez LAG, Logroscino G, Hernán MA. Use of antidepressants and the risk of Parkinson’s disease: a prospective study. J Neurol Neurosurg Psychiatry. 2009;80(6):671-674.
28. Weisskopf MG, Chen H, Schwarzschild MA, Kawachi I, Ascherio A. Prospective study of phobic anxiety and risk of Parkinson’s disease. Mov Disord. 2003;18(6):646-651.
29. Darweesh SK, Verlinden VJ, Stricker BH, Hofman A, Koudstaal PJ, Ikram MA. Trajectories of prediagnostic functioning in Parkinson’s disease. Brain. 2017;140(2):429-441.
30. Santangelo G, Vitale C, Picillo M, et al. Apathy and striatal dopamine transporter levels in de-novo, untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2015;21(5):489-493.
31. Erro R, Pappatà S, Amboni M, et al. Anxiety is associated with striatal dopamine transporter availability in newly diagnosed untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2012;18(9):1034-1038.
32. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013;14(8):
744-748.
33. Melendez J, Hesselbacher S, Sharafkhaneh A, Hirshkowitz M. Assessment of REM sleep behavior disorder in veterans with posttraumatic stress disorder. Chest. 2011;140(4):967A.
34. Pilotto A, Heinzel S, Suenkel U, et al. Application of the movement disorder society prodromal Parkinson’s disease research criteria in 2 independent prospective cohorts. Mov Disord. 2017;32(7):1025-1034.
35. Fereshtehnejad S-M, Montplaisir JY, Pelletier A, Gagnon J-F, Berg D, Postuma RB. Validation of the MDS research criteria for prodromal Parkinson’s disease: Longitudinal assessment in a REM sleep behavior disorder (RBD) cohort. Mov Disord. 2017;32(6):865-873.
36. Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G. Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology. 2016;86(6):566-576.
37. Moccia M, Pappatà S, Picillo M, et al. Dopamine transporter availability in motor subtypes of de novo drug-naïve Parkinson’s disease. J Neurol. 2014;261(11):2112-2118.
38. Siepel FJ, Brønnick KS, Booij J, et al. Cognitive executive impairment and dopaminergic deficits in de novo Parkinson’s disease. Mov Disord. 2014;29(14):1802-1808.
39. Iranzo A, Valldeoriola F, Lomeña F, et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study. Lancet Neurol. 2011;10(9):797-805.
40. Booij J, Kemp P. Dopamine transporter imaging with [(123)I]FP-CIT SPECT: potential effects of drugs. Eur J Nucl Med Mol Imaging. 2008;35(2):424-438.
41. Gellad WF, Aspinall SL, Handler SM, et al. Use of antipsychotics among older residents in VA nursing homes. Med Care. 2012;50(11):954-960.
42. Mauri MC, Paletta S, Maffini M, et al. Clinical pharmacology of atypical antipsychotics: an update. EXCLI J. 2014;13:1163-1191.
43. Morley JF, Duda JE. Use of hyposmia and other non-motor symptoms to distinguish between drug-induced parkinsonism and Parkinson’s disease. J Parkinsons Dis. 2014;4(2):169-173.
44. Morley JF, Cheng G, Dubroff JG, Wood S, Wilkinson JR, Duda JE. Olfactory impairment predicts underlying dopaminergic deficit in presumed drug-induced parkinsonism. Mov Disord Clin Pract. 2017;4(4):603-606.
45. Whitwell JL, Höglinger GU, Antonini A, et al; Movement Disorder Society-endorsed PSP Study Group. Radiological biomarkers for diagnosis in PSP: where are we and where do we need to be? Mov Disord. 2017;32(7):955-971.
46. Laurens B, Constantinescu R, Freeman R, et al. Fluid biomarkers in multiple system atrophy: A review of the MSA Biomarker Initiative. Neurobiol Dis. 2015;80:29-41.
47. Barber TR, Klein JC, Mackay CE, Hu MTM. Neuroimaging in pre-motor Parkinson’s disease. NeuroImage Clin. 2017;15:215-227.
48. Parkinson Progression Marker Initiative. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol. 2011;95(4):629-635.
49. Meles SK, Vadasz D, Renken RJ, et al. FDG PET, dopamine transporter SPECT, and olfaction: combining biomarkers in REM sleep behavior disorder. Mov Disord. 2017;32(10):1482-1486.
50. Noyce AJ, R’Bibo L, Peress L, et al. PREDICT‐PD: an online approach to prospectively identify risk indicators of Parkinson’s disease. Mov Disord. 2017 Feb; 32(2): 219–226.
51. Searles Nielsen S, Warden MN, Camacho-Soto A, Willis AW, Wright BA, Racette BA. A predictive model to identify Parkinson disease from administrative claims data. Neurology. 2017;89(14):1448-1456.
52. Institute of Medicine. Veterans and Agent Orange: Update 2012. National Academies Press: Washington, DC; 2013.
53. Department of Veterans Affairs. Diseases associated with exposure to Contaminants in the Water Supply at Camp Lejeune. Final rule. Fed Regist. 2017;82(9):4173-4185.
54. Goldman SM, Quinlan PJ, Ross GW, et al. Solvent exposures and Parkinson disease risk in twins. Ann Neurol. 2012;71(6):776-784.
55. Liu M, Shin EJ, Dang DK, et al. Trichloroethylene and Parkinson’s disease: risk assessment. Mol Neurobiol. 2018;55(7):6201-6214.
56. Betarbet R, Sherer TB, MacKenzie G, Garcia-Osuna M, Panov AV, Greenamyre JT. Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci. 2000;3(12):1301-1306.
57. Manning-Bog AB, McCormack AL, Li J, Uversky VN, Fink AL, Monte DAD. The herbicide paraquat causes up-regulation and aggregation of alpha-synuclein in mice: paraquat and alpha-synuclein. J Biol Chem. 2002;277(3):1641-1644.
58. Camacho-Soto A, Warden MN, Searles Nielsen S, et al. Traumatic brain injury in the prodromal period of Parkinson’s disease: a large epidemiological study using medicare data. Ann Neurol. 2017;82(5):744-754.
59. Gardner RC, Burke JF, Nettiksimmons J, Goldman S, Tanner CM, Yaffe K. Traumatic brain injury in later life increases risk for Parkinson disease. Ann Neurol. 2015;77(6):987-995.
60. Gardner RC, Byers AL, Barnes DE, Li Y, Boscardin J, Yaffe K. Mild TBI and risk of Parkinson disease: a Chronic Effects of Neurotrauma Consortium Study. Neurology. 2018;90(20):e1771-e1779.
61. Cruz-Haces M, Tang J, Acosta G, Fernandez J, Shi R. Pathological correlations between traumatic brain injury and chronic neurodegenerative diseases. Transl Neurodegener. 2017;6:20.
62. Lee PC, Bordelon Y, Bronstein J, Ritz B. Traumatic brain injury, paraquat exposure, and their relationship to Parkinson disease. Neurology. 2012;79(20):2061-2066.
63. Disabilities that are proximately due to, or aggravated by, service-connected disease or injury. 38 CFR §3.310.
64. Diseases Associated With Exposure to Certain Herbicide Agents (Hairy Cell Leukemia and Other Chronic B-Cell Leukemias, Parkinson’s Disease and Ischemic Heart Disease). Federal Regist. 2010;75(173):53202-53216. To be codified at 38 CFR §3.
65. Cheng EM, Swarztrauber K, Siderowf AD, et al. Association of specialist involvement and quality of care for Parkinson’s disease. Mov Disord. 2007;22(4):515-522.
66. Qamar MA, Harington G, Trump S, Johnson J, Roberts F, Frost E. Multidisciplinary care in Parkinson’s disease. Int Rev Neurobiol. 2017;132:511-523.
67. Pogoda TK, Cramer IE, Meterko M, et al. Patient and organizational factors related to education and support use by veterans with Parkinson’s disease. Mov Disord. 2009;24(13):1916-1924.
Parkinson disease (PD) affects about 680,000 in the US, including > 110,000 veterans (Caroline Tanner, MD, PhD, unpublished data).1 In the next 10 years, this number is expected to double, in part because of the aging of the US population.1 Although the classic diagnostic criteria emphasize motor symptoms that include tremor, gait disturbance, and paucity of movement, there is increasing recognition that disease pathology begins decades before the development of motor impairment.2
Pathologic studies confirm that by the onset of motor symptoms, at least 30% of nigrostriatal neurons are lost or dysfunctional.3-5 Similarly, the Braak staging hypothesis posits initial deposition of Lewy bodies in the olfactory bulb and the dorsal motor nucleus of the vagus nerve, followed by prion-like spread through the brain stem into the midbrain/substantia nigra, and finally into the cortex (Figure 1).6
The decades-long prodromal or preclinical phase represents a unique opportunity for early identification of those at highest risk for developing the motor symptoms of Parkinson disease.7 Accurate identification, ideally before the onset of manifest motor disability, would not only improve prognostic counseling of veterans and families, but also could allow for early enrollment into trials of potentially disease-modifying therapeutic agents. Thus, early and accurate identification of PD is an important goal of the care of veterans with potential PD.
Prodromal Symptoms
Prodromal PD, as defined by the International Parkinson Disease and Movement Disorders Society (MDS), focuses on nonmotor symptoms that herald the onset of manifest motor PD.8 The most commonly assessed nonmotor features include olfaction, constipation, sleep disturbance, and mood disorders.
Olfaction is impaired in > 90% of patients with motor PD at the time of diagnosis; by contrast, the prevalence of hyposmia in the general population ranges from 20% to 50%, with higher rates in older adults and in smokers.9-11 Thus, olfaction appears to be a relatively sensitive, though nonspecific, prodromal feature. Importantly, subjective report of hyposmia is poorly reliable, so a number of different tests have been developed for objective assessment of olfactory dysfunction.12 The 12-item Brief Smell Identification Test (B-SIT), derived from the longer University of Pennsylvania Smell Identification Test, is a “scratch-and-sniff” forced multiple choice test that can be self-administered by cooperative patients.13,14 The B-SIT has been validated in multiple ethnic and cultural groups and shows high discrimination between PD subjects and controls.13,15 Of note, olfactory impairment appears to be associated with risk of cognitive decline in PD, further emphasizing the need for accurate assessment to guide prognosis.16
Like hyposmia, constipation can be noted long before the diagnosis of manifest motor PD.17 After adjustment for lifestyle factors, constipated individuals have up to 4.5-fold increased odds of developing PD, and those with constipation suffer worsened disease outcomes and health-related quality of life.17-20 Some groups have demonstrated alterations in gut microbiota of those with prodromal PD, which suggests local inflammatory processes and intestinal permeability may contribute to protein misfolding and disease development.21,22 This also raises the intriguing possibility that dietary alterations may be neuroprotective or neurorestorative, although this has yet to be tested in humans.23,24
Like constipation, mood changes can precede the appearance of manifest motor PD.25,26 Case control studies suggest a higher risk of developing PD among individuals who were previously diagnosed with depression or anxiety, particularly in the 1 to 2 years prior to PD diagnosis.27-29 Both apathy and anxiety are associated with striatal dopamine dysfunction, particularly in the right caudate nucleus, which suggests that mood changes are directly related to disease pathology.30,31
Of the prodromal features, rapid eye movement sleep behavior disorder (RBD) is associated with the highest risk of conversion to motor PD.8 Up to 80% of older men with socalled idiopathic RBD develop a parkinsonian syndrome within 20 years; risk is divided about equally between idiopathic PD and dementia with Lewy bodies (DLB).32 Collateral history from a bed-partner is usually sufficient to make the diagnosis, although, this is often confounded by the prevalence of nightmares in those with posttraumatic stress disorder in the veteran population.32 Thus, in suspected cases, obtaining a polysomnogram can aid in distinguishing between idiopathic PC and DLB.33 Given the specificity of RBD as a marker of synuclein deposition and the high risk of progression to a degenerative syndrome, accurate diagnosis and counseling is imperative.
Each of the prodromal nonmotor features of PD are at best moderately sensitive or specific in isolation, but in concert, they can be used to develop a Parkinson risk score. For instance, the MDS prodromal criteria combine individual likelihood ratios into Bayesian analysis to determine a combined probability of PD, which can be further stratified to probable or possible prodromal PD (probability > 80%, > 50%, respectively).8 These criteria have been applied to several independent cohorts and demonstrate high sensitivity and specificity, especially over time.34,35 Applicability in a veteran population has yet to be determined.
Use of Imaging in Diagnosis
Although clinical diagnostic criteria and prodromal features can improve diagnostic accuracy, it can be extremely challenging to distinguish idiopathic PD from nondegenerative parkinsonism or atypical syndromes (see below). Compared with the gold standard of pathologic assessment, the clinical diagnostic accuracy for PD ranges from 73% for nonexperts to 80% for fellowship-trained movement disorders specialists.36 Thus, objective biomarkers are sought to improve diagnostic accuracy both for clinical care as well as for research purposes, such as enrollment into clinical trials.
Multiple potential imaging biomarkers for preclinical PD can aid in early diagnosis and help differentiate PD from related but distinct disorders. While beyond the scope of this review, these techniques have recently been reviewed.7 Of these, the most widely available and accurate is dopamine transporter (DAT) imaging, which uses a radioiodinated ligand that binds to DAT on striatal dopaminergic terminals; binding is detected through single photon emission computed tomography (SPECT) scanning. Thus, a SPECT DaTscan (GE Healthcare Bio-Sciences, Little Chalfont, England) directly assesses the integrity of the presynaptic nigrostriatal system and is well correlated with severity of motor and nonmotor parkinsonism.37,38
In individuals with suspected prodromal PD, abnormal DaTscans are associated with faster progression to manifest motor PD.39 However, it should be noted that a number of medications, several of which are commonly utilized in the veteran population, can affect the outcome of a DaTscan.40 Some of these medications only mildly affect the outcome, so the physician interpreting the scan should be made aware of their use, while others need to be held for days to weeks so as not to invalidate the DaTscan. DaTscan also do not differentiate between PD and atypical degenerative parkinsonisms such as multiple system atrophy (MSA), DLB, progressive supranuclear palsy (PSP), or corticobasal syndrome (CBS). Nevertheless, these scans can be used to distinguish degenerative parkinsonisms from other conditions that can be difficult to distinguish clinically from PD, including essential tremor, normal pressure hydrocephalus, vascular parkinsonism, or druginduced parkinsonism (DIP).
DIP usually is caused by blockade of postsynaptic dopamine receptors by antipsychotic medications, which are prescribed to as many as 1 in 4 older veterans; antiemetic agents such as metoclopramide are also potential offenders if used chronically.41 The risk of DIP appears to be associated with the D2 binding affinity of the drug. Thus, of the newer atypical antipsychotics, clozapine and quetiapine appear to have the lowest risk, while ziprasidone and aripiprazole have the highest binding affinity and therefore the highest risk.42 In many patients, parkinsonism persists even after discontinuation of the offending agent, suggesting that in at least a subset of patients, DIP may be an “unmasking” of latent PD rather than a true adverse effect of the medication. The prodromal features discussed above can be used to distinguish isolated DIP from unmasked latent PD.43 In a study we conducted in veterans at the Michael J. Crescenz VA Medical Center in Philadelphia, Pennsylvania, hyposmia in particular was shown to be highly predictive of an underlying dopaminergic deficit with an odds ratio of 63.44
Other important considerations in the differential diagnosis of PD are the atypical degenerative parkinsonian syndromes, formerly called Parkinson plus syndromes. These may be further divided into the synucleinopathies (MSA, DLB) or the tauopathies (PSP, CBS), depending on the predominant amyloidogenic protein. Early in the disease, the atypical syndromes and idiopathic PD may be clinically indistinguishable, although the atypical syndromes tend to progress more rapidly and often have a less robust response to levodopa.
Radiologic and fluid biomarkers for the atypical syndromes are under active investigation; at present the most accessible study is magnetic resonance imaging (MRI), which may show characteristic features such as degeneration of the pontocerebellar fibers in MSA or midbrain atrophy in PSP.45,46 By contrast, standard MRI sequences in idiopathic PD are usually normal, although high-resolution (7 tesla) imaging can reveal loss of neuromelanin in the substantia nigra.47 MRI also can be useful in the workup of suspected normal pressure hydrocephalus or vascular parkinsonism, which would show disproportionate ventriculomegaly with transependymal flow, or white matter lesions in the basal ganglia, respectively.
Data-Based Identification of Preclinical PD
The integration of clinical motor or prodromal features with biomarker data has led to the development of several large-scale clinical and administrative databases to identify PD. The Parkinson Progression Markers Initiative initially enrolled only de novo clinically identified people with PD, but it expanded to include a prodromal cohort who are being assessed for rates of conversion to PD.48 Similarly, metabolic imaging can be combined with prodromal symptoms, such as hyposmia or RBD, to predict risk for phenoconversion into manifest motor PD.49
The PREDICT-PD study synthesizes mood symptoms, RBD, smell testing, genotyping, and keyboard-tapping tasks to divide individuals into high-, middle-, and low-risk groups; interim analysis at 3 years of follow-up (N = 842) demonstrated a hazard ratio of 4.39 (95% CI, 1.03-18.68) for the diagnosis of PD in the highrisk group compared with the low-risk group.50 Lastly, administrative claims data for prodromal features, such as constipation, RBD, and mood symptoms, is highly predictive of eventual PD diagnosis.51 VA databases accessed through the Corporate Data Warehouse are complementary sources of information to nonveteranspecific Medicare databases; to our knowledge there has not yet been a comprehensive search of VA databases to identify veterans with preclinical PD.
Risk Factors Associated With Military Service
A number of potential environmental risk factors may increase the risk of developing Parkinson disease for veterans. Perhaps the most commonly recognized is pesticide exposure, particularly given the presumptive service connections established by the VA for Parkinson disease and exposure to Agent Orange or contaminated water at Camp Lejeune.52,53 Both dioxin, the toxic ingredient in Agent Orange, and the solvents trichloroethylene and perchloroethylene, found in the water supply at Camp Lejeune, interfere with mitochondrial function leading to oxidative stress and apoptosis of nigrostriatal neurons.54,55 Other potential exposures, which are not necessarily limited to the veteran population, include rotenone, a phytochemical used to kill fish in reservoirs, and paraquat, an herbicide that may directly promote synuclein aggregation.56,57 Veterans who have reported exposure to these or other environmental chemicals in civilian life should be carefully assessed for the presence of motor PD or prodromal features.
Traumatic brain injury (TBI) also may be a risk factor for PD, which may be particularly relevant for veterans who had served in Iraq or Afghanistan. Retrospective claims data suggest a strong association between PD and recent TBI in the 5 to 10 years prior to motor PD diagnosis.58,59 A recent assessment of combat veterans with TBI found that even mild TBI was associated with a 56% increased risk of PD, while moderate-to-severe TBI was associated with an 83% higher risk of PD.60 The pathologic mechanism for this link is unclear, but post-TBI inflammatory processes may lead to the formation of reactive oxygen species and/or glutamatergic excitotoxicity, thus leading to secondary injury in the nigrostriatal pathway.61 As with prodromal symptoms, the risk of PD related to environmental risk factors may be synergistic; repetitive TBI may be more damaging than a single injury, and a combination of TBI and pesticide exposure markedly increases PD risk beyond the risk of TBI or the risk of pesticides alone.62 Recently, parkinsonism, including Parkinson disease, was recognized as a service connected condition for veterans with a servicerelated moderate or severe TBI.63
Conclusion
Because of the substantial impact on quality of life and disability-adjusted life years, early and accurate identification and management of veterans at risk for PD is an important priority area for the VA. The 10-year cost of PD-related benefits through the VA was estimated at $3.5 billion in fiscal year 2010, and that number is likely to rise in coming years, due to the aging population as well as synergistic effects of independent risk factors described above.64 In response, the VA has created a network of specialty care sites, known as Parkinson Disease Research, Education, and Clinical Centers (PADRECCs) located in Philadelphia, Pennsylvania; Richmond, Virginia; Houston, Texas; West Los Angeles and San Francisco, California; and Seattle, Washington/ Portland, Oregon (www.parkinsons.va.gov).
The PADRECCs are supplemented by a National VA PD Consortium network of VA physicians trained in PD management (Figure 2). Studies, including one investigating care of veterans with PD, have demonstrated that involvement of specialty care services early in the course of PD leads to improved patient outcomes.65,66 In addition to patient-facing resources such as support groups and specialized physical/occupational/speech therapy, PADRECCs and the consortium sites are national leaders in PD education and clinical trials and provide high-quality, multidisciplinary care for veterans with PD.67 Thus, veterans with significant risk factors or prodromal symptoms of PD should be referred into the PADRECC/Consortium network in order to maximize their quality of care and quality of life.
Parkinson disease (PD) affects about 680,000 in the US, including > 110,000 veterans (Caroline Tanner, MD, PhD, unpublished data).1 In the next 10 years, this number is expected to double, in part because of the aging of the US population.1 Although the classic diagnostic criteria emphasize motor symptoms that include tremor, gait disturbance, and paucity of movement, there is increasing recognition that disease pathology begins decades before the development of motor impairment.2
Pathologic studies confirm that by the onset of motor symptoms, at least 30% of nigrostriatal neurons are lost or dysfunctional.3-5 Similarly, the Braak staging hypothesis posits initial deposition of Lewy bodies in the olfactory bulb and the dorsal motor nucleus of the vagus nerve, followed by prion-like spread through the brain stem into the midbrain/substantia nigra, and finally into the cortex (Figure 1).6
The decades-long prodromal or preclinical phase represents a unique opportunity for early identification of those at highest risk for developing the motor symptoms of Parkinson disease.7 Accurate identification, ideally before the onset of manifest motor disability, would not only improve prognostic counseling of veterans and families, but also could allow for early enrollment into trials of potentially disease-modifying therapeutic agents. Thus, early and accurate identification of PD is an important goal of the care of veterans with potential PD.
Prodromal Symptoms
Prodromal PD, as defined by the International Parkinson Disease and Movement Disorders Society (MDS), focuses on nonmotor symptoms that herald the onset of manifest motor PD.8 The most commonly assessed nonmotor features include olfaction, constipation, sleep disturbance, and mood disorders.
Olfaction is impaired in > 90% of patients with motor PD at the time of diagnosis; by contrast, the prevalence of hyposmia in the general population ranges from 20% to 50%, with higher rates in older adults and in smokers.9-11 Thus, olfaction appears to be a relatively sensitive, though nonspecific, prodromal feature. Importantly, subjective report of hyposmia is poorly reliable, so a number of different tests have been developed for objective assessment of olfactory dysfunction.12 The 12-item Brief Smell Identification Test (B-SIT), derived from the longer University of Pennsylvania Smell Identification Test, is a “scratch-and-sniff” forced multiple choice test that can be self-administered by cooperative patients.13,14 The B-SIT has been validated in multiple ethnic and cultural groups and shows high discrimination between PD subjects and controls.13,15 Of note, olfactory impairment appears to be associated with risk of cognitive decline in PD, further emphasizing the need for accurate assessment to guide prognosis.16
Like hyposmia, constipation can be noted long before the diagnosis of manifest motor PD.17 After adjustment for lifestyle factors, constipated individuals have up to 4.5-fold increased odds of developing PD, and those with constipation suffer worsened disease outcomes and health-related quality of life.17-20 Some groups have demonstrated alterations in gut microbiota of those with prodromal PD, which suggests local inflammatory processes and intestinal permeability may contribute to protein misfolding and disease development.21,22 This also raises the intriguing possibility that dietary alterations may be neuroprotective or neurorestorative, although this has yet to be tested in humans.23,24
Like constipation, mood changes can precede the appearance of manifest motor PD.25,26 Case control studies suggest a higher risk of developing PD among individuals who were previously diagnosed with depression or anxiety, particularly in the 1 to 2 years prior to PD diagnosis.27-29 Both apathy and anxiety are associated with striatal dopamine dysfunction, particularly in the right caudate nucleus, which suggests that mood changes are directly related to disease pathology.30,31
Of the prodromal features, rapid eye movement sleep behavior disorder (RBD) is associated with the highest risk of conversion to motor PD.8 Up to 80% of older men with socalled idiopathic RBD develop a parkinsonian syndrome within 20 years; risk is divided about equally between idiopathic PD and dementia with Lewy bodies (DLB).32 Collateral history from a bed-partner is usually sufficient to make the diagnosis, although, this is often confounded by the prevalence of nightmares in those with posttraumatic stress disorder in the veteran population.32 Thus, in suspected cases, obtaining a polysomnogram can aid in distinguishing between idiopathic PC and DLB.33 Given the specificity of RBD as a marker of synuclein deposition and the high risk of progression to a degenerative syndrome, accurate diagnosis and counseling is imperative.
Each of the prodromal nonmotor features of PD are at best moderately sensitive or specific in isolation, but in concert, they can be used to develop a Parkinson risk score. For instance, the MDS prodromal criteria combine individual likelihood ratios into Bayesian analysis to determine a combined probability of PD, which can be further stratified to probable or possible prodromal PD (probability > 80%, > 50%, respectively).8 These criteria have been applied to several independent cohorts and demonstrate high sensitivity and specificity, especially over time.34,35 Applicability in a veteran population has yet to be determined.
Use of Imaging in Diagnosis
Although clinical diagnostic criteria and prodromal features can improve diagnostic accuracy, it can be extremely challenging to distinguish idiopathic PD from nondegenerative parkinsonism or atypical syndromes (see below). Compared with the gold standard of pathologic assessment, the clinical diagnostic accuracy for PD ranges from 73% for nonexperts to 80% for fellowship-trained movement disorders specialists.36 Thus, objective biomarkers are sought to improve diagnostic accuracy both for clinical care as well as for research purposes, such as enrollment into clinical trials.
Multiple potential imaging biomarkers for preclinical PD can aid in early diagnosis and help differentiate PD from related but distinct disorders. While beyond the scope of this review, these techniques have recently been reviewed.7 Of these, the most widely available and accurate is dopamine transporter (DAT) imaging, which uses a radioiodinated ligand that binds to DAT on striatal dopaminergic terminals; binding is detected through single photon emission computed tomography (SPECT) scanning. Thus, a SPECT DaTscan (GE Healthcare Bio-Sciences, Little Chalfont, England) directly assesses the integrity of the presynaptic nigrostriatal system and is well correlated with severity of motor and nonmotor parkinsonism.37,38
In individuals with suspected prodromal PD, abnormal DaTscans are associated with faster progression to manifest motor PD.39 However, it should be noted that a number of medications, several of which are commonly utilized in the veteran population, can affect the outcome of a DaTscan.40 Some of these medications only mildly affect the outcome, so the physician interpreting the scan should be made aware of their use, while others need to be held for days to weeks so as not to invalidate the DaTscan. DaTscan also do not differentiate between PD and atypical degenerative parkinsonisms such as multiple system atrophy (MSA), DLB, progressive supranuclear palsy (PSP), or corticobasal syndrome (CBS). Nevertheless, these scans can be used to distinguish degenerative parkinsonisms from other conditions that can be difficult to distinguish clinically from PD, including essential tremor, normal pressure hydrocephalus, vascular parkinsonism, or druginduced parkinsonism (DIP).
DIP usually is caused by blockade of postsynaptic dopamine receptors by antipsychotic medications, which are prescribed to as many as 1 in 4 older veterans; antiemetic agents such as metoclopramide are also potential offenders if used chronically.41 The risk of DIP appears to be associated with the D2 binding affinity of the drug. Thus, of the newer atypical antipsychotics, clozapine and quetiapine appear to have the lowest risk, while ziprasidone and aripiprazole have the highest binding affinity and therefore the highest risk.42 In many patients, parkinsonism persists even after discontinuation of the offending agent, suggesting that in at least a subset of patients, DIP may be an “unmasking” of latent PD rather than a true adverse effect of the medication. The prodromal features discussed above can be used to distinguish isolated DIP from unmasked latent PD.43 In a study we conducted in veterans at the Michael J. Crescenz VA Medical Center in Philadelphia, Pennsylvania, hyposmia in particular was shown to be highly predictive of an underlying dopaminergic deficit with an odds ratio of 63.44
Other important considerations in the differential diagnosis of PD are the atypical degenerative parkinsonian syndromes, formerly called Parkinson plus syndromes. These may be further divided into the synucleinopathies (MSA, DLB) or the tauopathies (PSP, CBS), depending on the predominant amyloidogenic protein. Early in the disease, the atypical syndromes and idiopathic PD may be clinically indistinguishable, although the atypical syndromes tend to progress more rapidly and often have a less robust response to levodopa.
Radiologic and fluid biomarkers for the atypical syndromes are under active investigation; at present the most accessible study is magnetic resonance imaging (MRI), which may show characteristic features such as degeneration of the pontocerebellar fibers in MSA or midbrain atrophy in PSP.45,46 By contrast, standard MRI sequences in idiopathic PD are usually normal, although high-resolution (7 tesla) imaging can reveal loss of neuromelanin in the substantia nigra.47 MRI also can be useful in the workup of suspected normal pressure hydrocephalus or vascular parkinsonism, which would show disproportionate ventriculomegaly with transependymal flow, or white matter lesions in the basal ganglia, respectively.
Data-Based Identification of Preclinical PD
The integration of clinical motor or prodromal features with biomarker data has led to the development of several large-scale clinical and administrative databases to identify PD. The Parkinson Progression Markers Initiative initially enrolled only de novo clinically identified people with PD, but it expanded to include a prodromal cohort who are being assessed for rates of conversion to PD.48 Similarly, metabolic imaging can be combined with prodromal symptoms, such as hyposmia or RBD, to predict risk for phenoconversion into manifest motor PD.49
The PREDICT-PD study synthesizes mood symptoms, RBD, smell testing, genotyping, and keyboard-tapping tasks to divide individuals into high-, middle-, and low-risk groups; interim analysis at 3 years of follow-up (N = 842) demonstrated a hazard ratio of 4.39 (95% CI, 1.03-18.68) for the diagnosis of PD in the highrisk group compared with the low-risk group.50 Lastly, administrative claims data for prodromal features, such as constipation, RBD, and mood symptoms, is highly predictive of eventual PD diagnosis.51 VA databases accessed through the Corporate Data Warehouse are complementary sources of information to nonveteranspecific Medicare databases; to our knowledge there has not yet been a comprehensive search of VA databases to identify veterans with preclinical PD.
Risk Factors Associated With Military Service
A number of potential environmental risk factors may increase the risk of developing Parkinson disease for veterans. Perhaps the most commonly recognized is pesticide exposure, particularly given the presumptive service connections established by the VA for Parkinson disease and exposure to Agent Orange or contaminated water at Camp Lejeune.52,53 Both dioxin, the toxic ingredient in Agent Orange, and the solvents trichloroethylene and perchloroethylene, found in the water supply at Camp Lejeune, interfere with mitochondrial function leading to oxidative stress and apoptosis of nigrostriatal neurons.54,55 Other potential exposures, which are not necessarily limited to the veteran population, include rotenone, a phytochemical used to kill fish in reservoirs, and paraquat, an herbicide that may directly promote synuclein aggregation.56,57 Veterans who have reported exposure to these or other environmental chemicals in civilian life should be carefully assessed for the presence of motor PD or prodromal features.
Traumatic brain injury (TBI) also may be a risk factor for PD, which may be particularly relevant for veterans who had served in Iraq or Afghanistan. Retrospective claims data suggest a strong association between PD and recent TBI in the 5 to 10 years prior to motor PD diagnosis.58,59 A recent assessment of combat veterans with TBI found that even mild TBI was associated with a 56% increased risk of PD, while moderate-to-severe TBI was associated with an 83% higher risk of PD.60 The pathologic mechanism for this link is unclear, but post-TBI inflammatory processes may lead to the formation of reactive oxygen species and/or glutamatergic excitotoxicity, thus leading to secondary injury in the nigrostriatal pathway.61 As with prodromal symptoms, the risk of PD related to environmental risk factors may be synergistic; repetitive TBI may be more damaging than a single injury, and a combination of TBI and pesticide exposure markedly increases PD risk beyond the risk of TBI or the risk of pesticides alone.62 Recently, parkinsonism, including Parkinson disease, was recognized as a service connected condition for veterans with a servicerelated moderate or severe TBI.63
Conclusion
Because of the substantial impact on quality of life and disability-adjusted life years, early and accurate identification and management of veterans at risk for PD is an important priority area for the VA. The 10-year cost of PD-related benefits through the VA was estimated at $3.5 billion in fiscal year 2010, and that number is likely to rise in coming years, due to the aging population as well as synergistic effects of independent risk factors described above.64 In response, the VA has created a network of specialty care sites, known as Parkinson Disease Research, Education, and Clinical Centers (PADRECCs) located in Philadelphia, Pennsylvania; Richmond, Virginia; Houston, Texas; West Los Angeles and San Francisco, California; and Seattle, Washington/ Portland, Oregon (www.parkinsons.va.gov).
The PADRECCs are supplemented by a National VA PD Consortium network of VA physicians trained in PD management (Figure 2). Studies, including one investigating care of veterans with PD, have demonstrated that involvement of specialty care services early in the course of PD leads to improved patient outcomes.65,66 In addition to patient-facing resources such as support groups and specialized physical/occupational/speech therapy, PADRECCs and the consortium sites are national leaders in PD education and clinical trials and provide high-quality, multidisciplinary care for veterans with PD.67 Thus, veterans with significant risk factors or prodromal symptoms of PD should be referred into the PADRECC/Consortium network in order to maximize their quality of care and quality of life.
1. Marras C, Beck JC, Bower JH, et al; Parkinson’s Foundation P4 Group. Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 2018;4:21.
2. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591-1601.
3. Fearnley JM, Lees AJ. Ageing and Parkinson’s disease: substantia nigra regional selectivity. Brain. 1991;114(pt 5):2283-2301.
4. Greffard S, Verny M, Bonnet A-M, et al. Motor score of the Unified Parkinson Disease Rating Scale as a good predictor of Lewy body-associated neuronal loss in the substantia nigra. Arch Neurol. 2006;63(4):584-588.
5. Hilker R, Schweitzer K, Coburger S, et al. Nonlinear progression of Parkinson disease as determined by serial positron emission tomographic imaging of striatal fluorodopa F 18 activity. Arch Neurol. 2005;62(3):378-382.
6. Braak H, Del Tredici K, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
7. Mantri S, Morley JF, Siderowf AD. The importance of preclinical diagnostics in Parkinson disease. Parkinsonism Relat Disord. 2018;pii:S1353-8020(18)30396-1. [Epub ahead of print]
8. Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2015;30(12):1600-1611.
9. Haehner A, Boesveldt S, Berendse HW, et al. Prevalence of smell loss in Parkinson’s disease – a multicenter study. Parkinsonism Relat Disord. 2009;15(7):490-494.
10. Mullol J, Alobid I, Mariño-Sánchez F, et al. Furthering the understanding of olfaction, prevalence of loss of smell and risk factors: a population-based survey (OLFACAT study). BMJ Open. 2012;2(6).pii:e001256.
11. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, Rosenberg L. Smell identification ability: changes with age. Science. 1984;226(4681):1441-1443.
12. Doty RL. Olfactory dysfunction in Parkinson disease. Nat Rev Neurol. 2012;8(6):329-339.
13. Double KL, Rowe DB, Hayes M, et al. Identifying the pattern of olfactory deficits in Parkinson disease using the brief smell identification test. Arch Neurol. 2003;60(4):545-549.
14. Doty RL, Shaman P, Dann M. Development of the University of Pennsylvania Smell Identification Test: a standardized microencapsulated test of olfactory function. Physiol Behav. 1984;32(3):489-502.
15. Morley JF, Cohen A, Silveira-Moriyama L, et al. Optimizing olfactory testing for the diagnosis of Parkinson’s disease: item analysis of the University of Pennsylvania smell identification test. NPJ Parkinsons Dis. 2018;4:2.
16. Fullard ME, Tran B, Xie SX, et al. Olfactory impairment predicts cognitive decline in early Parkinson’s disease. Parkinsonism Relat Disord. 2016;25:45-51.
17. Savica R, Carlin JM, Grossardt BR, et al. Medical records documentation of constipation preceding Parkinson disease: a case-control study. Neurology. 2009;73(21):1752-1758.
18. Abbott RD, Petrovitch H, White LR, et al. Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology. 2001;57(3):456-462.
19. Stocchi F, Torti M. Constipation in Parkinson’s disease. Int Rev Neurobiol. 2017;134:811-826.
20. Yu QJ, Yu SY, Zuo LJ, et al. Parkinson disease with constipation: clinical features and relevant factors. Sci Rep. 2018;8(1):567.
21. Hill-Burns EM, Debelius JW, Morton JT, et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov Disord. 2017;32(5):739-749.
22. Mulak A, Bonaz B. Brain-gut-microbiota axis in Parkinson’s disease. World J Gastroenterol. 2015;21(37): 10609-10620.
23. Shah SP, Duda JE. Dietary modifications in Parkinson’s disease: a neuroprotective intervention? Med Hypotheses. 2015;85(6):1002-1005.
24. Perez-Pardo P, de Jong EM, Broersen LM, et al. Promising effects of neurorestorative diets on motor, cognitive, and gastrointestinal dysfunction after symptom development in a mouse model of Parkinson’s disease. Front Aging Neurosci. 2017;9:57.
25. Fang F, Xu Q, Park Y, et al. Depression and the subsequent risk of Parkinson’s disease in the NIH-AARP Diet and Health Study. Mov Disord. 2010;25(9):1157-1162.
26. Leentjens AFG, Van den Akker M, Metsemakers JFM, Lousberg R, Verhey FRJ. Higher incidence of depression preceding the onset of Parkinson’s disease: a register study. Mov Disord. 2003;18(4):414-418.
27. Alonso A, Rodriguez LAG, Logroscino G, Hernán MA. Use of antidepressants and the risk of Parkinson’s disease: a prospective study. J Neurol Neurosurg Psychiatry. 2009;80(6):671-674.
28. Weisskopf MG, Chen H, Schwarzschild MA, Kawachi I, Ascherio A. Prospective study of phobic anxiety and risk of Parkinson’s disease. Mov Disord. 2003;18(6):646-651.
29. Darweesh SK, Verlinden VJ, Stricker BH, Hofman A, Koudstaal PJ, Ikram MA. Trajectories of prediagnostic functioning in Parkinson’s disease. Brain. 2017;140(2):429-441.
30. Santangelo G, Vitale C, Picillo M, et al. Apathy and striatal dopamine transporter levels in de-novo, untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2015;21(5):489-493.
31. Erro R, Pappatà S, Amboni M, et al. Anxiety is associated with striatal dopamine transporter availability in newly diagnosed untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2012;18(9):1034-1038.
32. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013;14(8):
744-748.
33. Melendez J, Hesselbacher S, Sharafkhaneh A, Hirshkowitz M. Assessment of REM sleep behavior disorder in veterans with posttraumatic stress disorder. Chest. 2011;140(4):967A.
34. Pilotto A, Heinzel S, Suenkel U, et al. Application of the movement disorder society prodromal Parkinson’s disease research criteria in 2 independent prospective cohorts. Mov Disord. 2017;32(7):1025-1034.
35. Fereshtehnejad S-M, Montplaisir JY, Pelletier A, Gagnon J-F, Berg D, Postuma RB. Validation of the MDS research criteria for prodromal Parkinson’s disease: Longitudinal assessment in a REM sleep behavior disorder (RBD) cohort. Mov Disord. 2017;32(6):865-873.
36. Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G. Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology. 2016;86(6):566-576.
37. Moccia M, Pappatà S, Picillo M, et al. Dopamine transporter availability in motor subtypes of de novo drug-naïve Parkinson’s disease. J Neurol. 2014;261(11):2112-2118.
38. Siepel FJ, Brønnick KS, Booij J, et al. Cognitive executive impairment and dopaminergic deficits in de novo Parkinson’s disease. Mov Disord. 2014;29(14):1802-1808.
39. Iranzo A, Valldeoriola F, Lomeña F, et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study. Lancet Neurol. 2011;10(9):797-805.
40. Booij J, Kemp P. Dopamine transporter imaging with [(123)I]FP-CIT SPECT: potential effects of drugs. Eur J Nucl Med Mol Imaging. 2008;35(2):424-438.
41. Gellad WF, Aspinall SL, Handler SM, et al. Use of antipsychotics among older residents in VA nursing homes. Med Care. 2012;50(11):954-960.
42. Mauri MC, Paletta S, Maffini M, et al. Clinical pharmacology of atypical antipsychotics: an update. EXCLI J. 2014;13:1163-1191.
43. Morley JF, Duda JE. Use of hyposmia and other non-motor symptoms to distinguish between drug-induced parkinsonism and Parkinson’s disease. J Parkinsons Dis. 2014;4(2):169-173.
44. Morley JF, Cheng G, Dubroff JG, Wood S, Wilkinson JR, Duda JE. Olfactory impairment predicts underlying dopaminergic deficit in presumed drug-induced parkinsonism. Mov Disord Clin Pract. 2017;4(4):603-606.
45. Whitwell JL, Höglinger GU, Antonini A, et al; Movement Disorder Society-endorsed PSP Study Group. Radiological biomarkers for diagnosis in PSP: where are we and where do we need to be? Mov Disord. 2017;32(7):955-971.
46. Laurens B, Constantinescu R, Freeman R, et al. Fluid biomarkers in multiple system atrophy: A review of the MSA Biomarker Initiative. Neurobiol Dis. 2015;80:29-41.
47. Barber TR, Klein JC, Mackay CE, Hu MTM. Neuroimaging in pre-motor Parkinson’s disease. NeuroImage Clin. 2017;15:215-227.
48. Parkinson Progression Marker Initiative. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol. 2011;95(4):629-635.
49. Meles SK, Vadasz D, Renken RJ, et al. FDG PET, dopamine transporter SPECT, and olfaction: combining biomarkers in REM sleep behavior disorder. Mov Disord. 2017;32(10):1482-1486.
50. Noyce AJ, R’Bibo L, Peress L, et al. PREDICT‐PD: an online approach to prospectively identify risk indicators of Parkinson’s disease. Mov Disord. 2017 Feb; 32(2): 219–226.
51. Searles Nielsen S, Warden MN, Camacho-Soto A, Willis AW, Wright BA, Racette BA. A predictive model to identify Parkinson disease from administrative claims data. Neurology. 2017;89(14):1448-1456.
52. Institute of Medicine. Veterans and Agent Orange: Update 2012. National Academies Press: Washington, DC; 2013.
53. Department of Veterans Affairs. Diseases associated with exposure to Contaminants in the Water Supply at Camp Lejeune. Final rule. Fed Regist. 2017;82(9):4173-4185.
54. Goldman SM, Quinlan PJ, Ross GW, et al. Solvent exposures and Parkinson disease risk in twins. Ann Neurol. 2012;71(6):776-784.
55. Liu M, Shin EJ, Dang DK, et al. Trichloroethylene and Parkinson’s disease: risk assessment. Mol Neurobiol. 2018;55(7):6201-6214.
56. Betarbet R, Sherer TB, MacKenzie G, Garcia-Osuna M, Panov AV, Greenamyre JT. Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci. 2000;3(12):1301-1306.
57. Manning-Bog AB, McCormack AL, Li J, Uversky VN, Fink AL, Monte DAD. The herbicide paraquat causes up-regulation and aggregation of alpha-synuclein in mice: paraquat and alpha-synuclein. J Biol Chem. 2002;277(3):1641-1644.
58. Camacho-Soto A, Warden MN, Searles Nielsen S, et al. Traumatic brain injury in the prodromal period of Parkinson’s disease: a large epidemiological study using medicare data. Ann Neurol. 2017;82(5):744-754.
59. Gardner RC, Burke JF, Nettiksimmons J, Goldman S, Tanner CM, Yaffe K. Traumatic brain injury in later life increases risk for Parkinson disease. Ann Neurol. 2015;77(6):987-995.
60. Gardner RC, Byers AL, Barnes DE, Li Y, Boscardin J, Yaffe K. Mild TBI and risk of Parkinson disease: a Chronic Effects of Neurotrauma Consortium Study. Neurology. 2018;90(20):e1771-e1779.
61. Cruz-Haces M, Tang J, Acosta G, Fernandez J, Shi R. Pathological correlations between traumatic brain injury and chronic neurodegenerative diseases. Transl Neurodegener. 2017;6:20.
62. Lee PC, Bordelon Y, Bronstein J, Ritz B. Traumatic brain injury, paraquat exposure, and their relationship to Parkinson disease. Neurology. 2012;79(20):2061-2066.
63. Disabilities that are proximately due to, or aggravated by, service-connected disease or injury. 38 CFR §3.310.
64. Diseases Associated With Exposure to Certain Herbicide Agents (Hairy Cell Leukemia and Other Chronic B-Cell Leukemias, Parkinson’s Disease and Ischemic Heart Disease). Federal Regist. 2010;75(173):53202-53216. To be codified at 38 CFR §3.
65. Cheng EM, Swarztrauber K, Siderowf AD, et al. Association of specialist involvement and quality of care for Parkinson’s disease. Mov Disord. 2007;22(4):515-522.
66. Qamar MA, Harington G, Trump S, Johnson J, Roberts F, Frost E. Multidisciplinary care in Parkinson’s disease. Int Rev Neurobiol. 2017;132:511-523.
67. Pogoda TK, Cramer IE, Meterko M, et al. Patient and organizational factors related to education and support use by veterans with Parkinson’s disease. Mov Disord. 2009;24(13):1916-1924.
1. Marras C, Beck JC, Bower JH, et al; Parkinson’s Foundation P4 Group. Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 2018;4:21.
2. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591-1601.
3. Fearnley JM, Lees AJ. Ageing and Parkinson’s disease: substantia nigra regional selectivity. Brain. 1991;114(pt 5):2283-2301.
4. Greffard S, Verny M, Bonnet A-M, et al. Motor score of the Unified Parkinson Disease Rating Scale as a good predictor of Lewy body-associated neuronal loss in the substantia nigra. Arch Neurol. 2006;63(4):584-588.
5. Hilker R, Schweitzer K, Coburger S, et al. Nonlinear progression of Parkinson disease as determined by serial positron emission tomographic imaging of striatal fluorodopa F 18 activity. Arch Neurol. 2005;62(3):378-382.
6. Braak H, Del Tredici K, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
7. Mantri S, Morley JF, Siderowf AD. The importance of preclinical diagnostics in Parkinson disease. Parkinsonism Relat Disord. 2018;pii:S1353-8020(18)30396-1. [Epub ahead of print]
8. Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2015;30(12):1600-1611.
9. Haehner A, Boesveldt S, Berendse HW, et al. Prevalence of smell loss in Parkinson’s disease – a multicenter study. Parkinsonism Relat Disord. 2009;15(7):490-494.
10. Mullol J, Alobid I, Mariño-Sánchez F, et al. Furthering the understanding of olfaction, prevalence of loss of smell and risk factors: a population-based survey (OLFACAT study). BMJ Open. 2012;2(6).pii:e001256.
11. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, Rosenberg L. Smell identification ability: changes with age. Science. 1984;226(4681):1441-1443.
12. Doty RL. Olfactory dysfunction in Parkinson disease. Nat Rev Neurol. 2012;8(6):329-339.
13. Double KL, Rowe DB, Hayes M, et al. Identifying the pattern of olfactory deficits in Parkinson disease using the brief smell identification test. Arch Neurol. 2003;60(4):545-549.
14. Doty RL, Shaman P, Dann M. Development of the University of Pennsylvania Smell Identification Test: a standardized microencapsulated test of olfactory function. Physiol Behav. 1984;32(3):489-502.
15. Morley JF, Cohen A, Silveira-Moriyama L, et al. Optimizing olfactory testing for the diagnosis of Parkinson’s disease: item analysis of the University of Pennsylvania smell identification test. NPJ Parkinsons Dis. 2018;4:2.
16. Fullard ME, Tran B, Xie SX, et al. Olfactory impairment predicts cognitive decline in early Parkinson’s disease. Parkinsonism Relat Disord. 2016;25:45-51.
17. Savica R, Carlin JM, Grossardt BR, et al. Medical records documentation of constipation preceding Parkinson disease: a case-control study. Neurology. 2009;73(21):1752-1758.
18. Abbott RD, Petrovitch H, White LR, et al. Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology. 2001;57(3):456-462.
19. Stocchi F, Torti M. Constipation in Parkinson’s disease. Int Rev Neurobiol. 2017;134:811-826.
20. Yu QJ, Yu SY, Zuo LJ, et al. Parkinson disease with constipation: clinical features and relevant factors. Sci Rep. 2018;8(1):567.
21. Hill-Burns EM, Debelius JW, Morton JT, et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov Disord. 2017;32(5):739-749.
22. Mulak A, Bonaz B. Brain-gut-microbiota axis in Parkinson’s disease. World J Gastroenterol. 2015;21(37): 10609-10620.
23. Shah SP, Duda JE. Dietary modifications in Parkinson’s disease: a neuroprotective intervention? Med Hypotheses. 2015;85(6):1002-1005.
24. Perez-Pardo P, de Jong EM, Broersen LM, et al. Promising effects of neurorestorative diets on motor, cognitive, and gastrointestinal dysfunction after symptom development in a mouse model of Parkinson’s disease. Front Aging Neurosci. 2017;9:57.
25. Fang F, Xu Q, Park Y, et al. Depression and the subsequent risk of Parkinson’s disease in the NIH-AARP Diet and Health Study. Mov Disord. 2010;25(9):1157-1162.
26. Leentjens AFG, Van den Akker M, Metsemakers JFM, Lousberg R, Verhey FRJ. Higher incidence of depression preceding the onset of Parkinson’s disease: a register study. Mov Disord. 2003;18(4):414-418.
27. Alonso A, Rodriguez LAG, Logroscino G, Hernán MA. Use of antidepressants and the risk of Parkinson’s disease: a prospective study. J Neurol Neurosurg Psychiatry. 2009;80(6):671-674.
28. Weisskopf MG, Chen H, Schwarzschild MA, Kawachi I, Ascherio A. Prospective study of phobic anxiety and risk of Parkinson’s disease. Mov Disord. 2003;18(6):646-651.
29. Darweesh SK, Verlinden VJ, Stricker BH, Hofman A, Koudstaal PJ, Ikram MA. Trajectories of prediagnostic functioning in Parkinson’s disease. Brain. 2017;140(2):429-441.
30. Santangelo G, Vitale C, Picillo M, et al. Apathy and striatal dopamine transporter levels in de-novo, untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2015;21(5):489-493.
31. Erro R, Pappatà S, Amboni M, et al. Anxiety is associated with striatal dopamine transporter availability in newly diagnosed untreated Parkinson’s disease patients. Parkinsonism Relat Disord. 2012;18(9):1034-1038.
32. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013;14(8):
744-748.
33. Melendez J, Hesselbacher S, Sharafkhaneh A, Hirshkowitz M. Assessment of REM sleep behavior disorder in veterans with posttraumatic stress disorder. Chest. 2011;140(4):967A.
34. Pilotto A, Heinzel S, Suenkel U, et al. Application of the movement disorder society prodromal Parkinson’s disease research criteria in 2 independent prospective cohorts. Mov Disord. 2017;32(7):1025-1034.
35. Fereshtehnejad S-M, Montplaisir JY, Pelletier A, Gagnon J-F, Berg D, Postuma RB. Validation of the MDS research criteria for prodromal Parkinson’s disease: Longitudinal assessment in a REM sleep behavior disorder (RBD) cohort. Mov Disord. 2017;32(6):865-873.
36. Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G. Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology. 2016;86(6):566-576.
37. Moccia M, Pappatà S, Picillo M, et al. Dopamine transporter availability in motor subtypes of de novo drug-naïve Parkinson’s disease. J Neurol. 2014;261(11):2112-2118.
38. Siepel FJ, Brønnick KS, Booij J, et al. Cognitive executive impairment and dopaminergic deficits in de novo Parkinson’s disease. Mov Disord. 2014;29(14):1802-1808.
39. Iranzo A, Valldeoriola F, Lomeña F, et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study. Lancet Neurol. 2011;10(9):797-805.
40. Booij J, Kemp P. Dopamine transporter imaging with [(123)I]FP-CIT SPECT: potential effects of drugs. Eur J Nucl Med Mol Imaging. 2008;35(2):424-438.
41. Gellad WF, Aspinall SL, Handler SM, et al. Use of antipsychotics among older residents in VA nursing homes. Med Care. 2012;50(11):954-960.
42. Mauri MC, Paletta S, Maffini M, et al. Clinical pharmacology of atypical antipsychotics: an update. EXCLI J. 2014;13:1163-1191.
43. Morley JF, Duda JE. Use of hyposmia and other non-motor symptoms to distinguish between drug-induced parkinsonism and Parkinson’s disease. J Parkinsons Dis. 2014;4(2):169-173.
44. Morley JF, Cheng G, Dubroff JG, Wood S, Wilkinson JR, Duda JE. Olfactory impairment predicts underlying dopaminergic deficit in presumed drug-induced parkinsonism. Mov Disord Clin Pract. 2017;4(4):603-606.
45. Whitwell JL, Höglinger GU, Antonini A, et al; Movement Disorder Society-endorsed PSP Study Group. Radiological biomarkers for diagnosis in PSP: where are we and where do we need to be? Mov Disord. 2017;32(7):955-971.
46. Laurens B, Constantinescu R, Freeman R, et al. Fluid biomarkers in multiple system atrophy: A review of the MSA Biomarker Initiative. Neurobiol Dis. 2015;80:29-41.
47. Barber TR, Klein JC, Mackay CE, Hu MTM. Neuroimaging in pre-motor Parkinson’s disease. NeuroImage Clin. 2017;15:215-227.
48. Parkinson Progression Marker Initiative. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol. 2011;95(4):629-635.
49. Meles SK, Vadasz D, Renken RJ, et al. FDG PET, dopamine transporter SPECT, and olfaction: combining biomarkers in REM sleep behavior disorder. Mov Disord. 2017;32(10):1482-1486.
50. Noyce AJ, R’Bibo L, Peress L, et al. PREDICT‐PD: an online approach to prospectively identify risk indicators of Parkinson’s disease. Mov Disord. 2017 Feb; 32(2): 219–226.
51. Searles Nielsen S, Warden MN, Camacho-Soto A, Willis AW, Wright BA, Racette BA. A predictive model to identify Parkinson disease from administrative claims data. Neurology. 2017;89(14):1448-1456.
52. Institute of Medicine. Veterans and Agent Orange: Update 2012. National Academies Press: Washington, DC; 2013.
53. Department of Veterans Affairs. Diseases associated with exposure to Contaminants in the Water Supply at Camp Lejeune. Final rule. Fed Regist. 2017;82(9):4173-4185.
54. Goldman SM, Quinlan PJ, Ross GW, et al. Solvent exposures and Parkinson disease risk in twins. Ann Neurol. 2012;71(6):776-784.
55. Liu M, Shin EJ, Dang DK, et al. Trichloroethylene and Parkinson’s disease: risk assessment. Mol Neurobiol. 2018;55(7):6201-6214.
56. Betarbet R, Sherer TB, MacKenzie G, Garcia-Osuna M, Panov AV, Greenamyre JT. Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci. 2000;3(12):1301-1306.
57. Manning-Bog AB, McCormack AL, Li J, Uversky VN, Fink AL, Monte DAD. The herbicide paraquat causes up-regulation and aggregation of alpha-synuclein in mice: paraquat and alpha-synuclein. J Biol Chem. 2002;277(3):1641-1644.
58. Camacho-Soto A, Warden MN, Searles Nielsen S, et al. Traumatic brain injury in the prodromal period of Parkinson’s disease: a large epidemiological study using medicare data. Ann Neurol. 2017;82(5):744-754.
59. Gardner RC, Burke JF, Nettiksimmons J, Goldman S, Tanner CM, Yaffe K. Traumatic brain injury in later life increases risk for Parkinson disease. Ann Neurol. 2015;77(6):987-995.
60. Gardner RC, Byers AL, Barnes DE, Li Y, Boscardin J, Yaffe K. Mild TBI and risk of Parkinson disease: a Chronic Effects of Neurotrauma Consortium Study. Neurology. 2018;90(20):e1771-e1779.
61. Cruz-Haces M, Tang J, Acosta G, Fernandez J, Shi R. Pathological correlations between traumatic brain injury and chronic neurodegenerative diseases. Transl Neurodegener. 2017;6:20.
62. Lee PC, Bordelon Y, Bronstein J, Ritz B. Traumatic brain injury, paraquat exposure, and their relationship to Parkinson disease. Neurology. 2012;79(20):2061-2066.
63. Disabilities that are proximately due to, or aggravated by, service-connected disease or injury. 38 CFR §3.310.
64. Diseases Associated With Exposure to Certain Herbicide Agents (Hairy Cell Leukemia and Other Chronic B-Cell Leukemias, Parkinson’s Disease and Ischemic Heart Disease). Federal Regist. 2010;75(173):53202-53216. To be codified at 38 CFR §3.
65. Cheng EM, Swarztrauber K, Siderowf AD, et al. Association of specialist involvement and quality of care for Parkinson’s disease. Mov Disord. 2007;22(4):515-522.
66. Qamar MA, Harington G, Trump S, Johnson J, Roberts F, Frost E. Multidisciplinary care in Parkinson’s disease. Int Rev Neurobiol. 2017;132:511-523.
67. Pogoda TK, Cramer IE, Meterko M, et al. Patient and organizational factors related to education and support use by veterans with Parkinson’s disease. Mov Disord. 2009;24(13):1916-1924.
Hemolytic Uremic Syndrome With Severe Neurologic Complications in an Adult (FULL)
The case of a female presenting with Shiga toxin-producing Escherichia coli and hemolytic uremic syndrome highlights a severe neurologic complication that canbe associated with these conditions.
Hemolytic uremic syndrome (HUS) is a rare illness that can be acquired through the consumption of food products contaminated with strains of Shiga toxin-producing Escherichia coli (E coli; STEC).1 Between 6% and 15% of individuals infected with STEC develop HUS, with children affected more frequently than adults.2,3 This strain of E coli releases Shiga toxin into the systemic circulation, which causes a thrombotic microangiopathy resulting in the characteristic HUS triad of symptoms: acute renal insufficiency, thrombocytopenia, and hemolytic anemia.4-6
Although neurologic features are common in HUS, they have not been extensively studied, particularly in adults. We report a case of STEC 0157:H7 subtype HUS in an adult with severe neurologic complications. This case highlights the neurological sequelae in an adult with typical STEC-HUS. The use of treatment modalities, such as plasmapheresis and eculizumab, and their use in adult typical STEC-HUS also is explored.
Case
A 53-year-old white woman with no pertinent past medical history presented to the Bay Pines Veterans Affairs Healthcare System Emergency Department with a 2-day history of abdominal pain, vomiting, nausea, diarrhea, and bright bloody stools. She returned from a cruise to the Bahamas 3 days prior, where she ate local foods, including salads. She reported no fever, shortness of breath, chest pain, headache, and cognitive difficulties. She presented with a normal mental status and neurologic exam. Apart from leukocytosis and elevated glucose level, her laboratory results at initial presentation were normal, (Table). A stool sample showed occult blood with white blood cell counts (WBCs) but was negative for Clostridium difficile. She was started on ciprofloxacin 400 mg and metronidazole 500 mg on the day of admission.
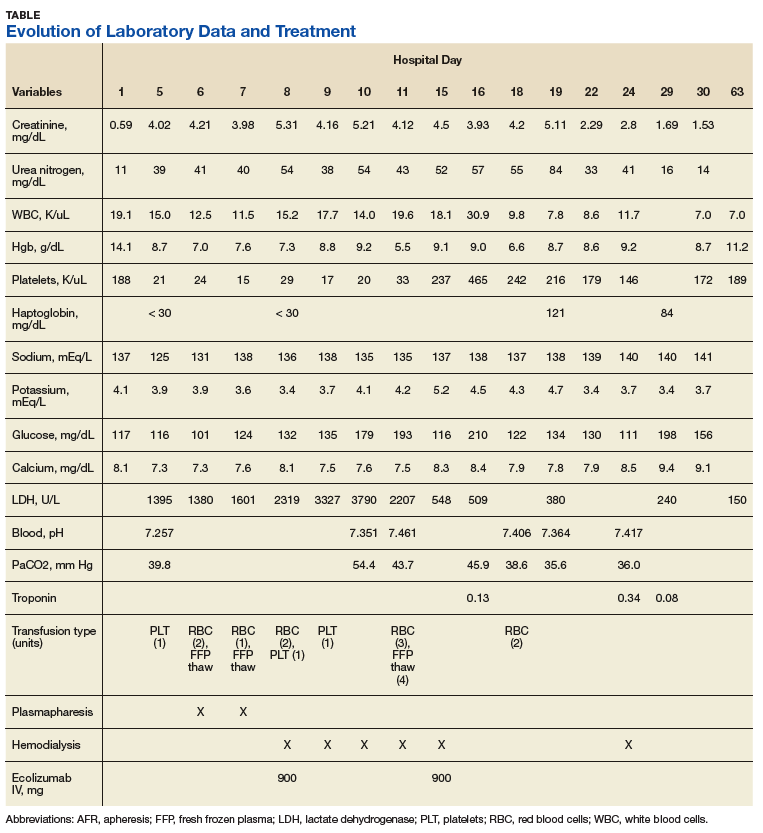
Hematuria was found on hospital day 2. On hospital day 4, the patient exhibited word finding difficulties. Blood studies revealed anemia, thrombocytopenia, leukocytosis, and increasing blood urea nitrogen (BUN) and creatinine. A computed tomography scan of the head was normal. Laboratory analysis showed schistocytes in the peripheral blood smear.
The patient’s cognitive functioning deteriorated on hospital day 5. She was not oriented to time or place. Her laboratory results showed complement level C3 at 70 mg/dL (ref: 83-193 mg/dL) complement C4 at 12 mg/dL (ref: 15-57mg/dL). The patient exhibited oliguria and hyponatremia, as well as both metabolic and respiratory acidosis; dialysis was then initiated. Results from the stool sample that was collected on hospital day 1 were received and tested positive for Shiga toxin.
At this point, the patient’s presentation of hemolytic anemia and thrombocytopenia in the setting of acute bloody diarrheal illness with known Shiga toxin, schistocytes on blood smear, and lack of pertinent medical history for other causes of this presentation made STEC-HUS the leading differential diagnosis. Plasmapheresis was ordered and performed on hospital day 6 and 7. Shiga toxin was no longer detected in the stool and antibiotics were stopped on hospital day 7.
The patient’s progressive deterioration in mental status continued on hospital day 8. She was not oriented to time or place, unable to perform simple calculations, and could not spell the word “hand” backwards. Physicians observed repetitive jerking motions of the upper extremities that were worse on the left side. An electroencephalogram (EEG) revealed right hemispheric sharp waves that were thought to be epileptiform (Figure 1). The patient began taking levetiracetam 1500 mg IV with 750 mg bid maintenance for seizure control. Plasmapheresis was discontinued due to her continued neurologic deterioration on this therapy. Consequently, eculizumab 900 mg IV was given along with the Neisseria meningitidis (N meningitidis) vaccine and a 19-day course of azithromycin 250 mg po as prophylaxis for encapsulated bacteria.
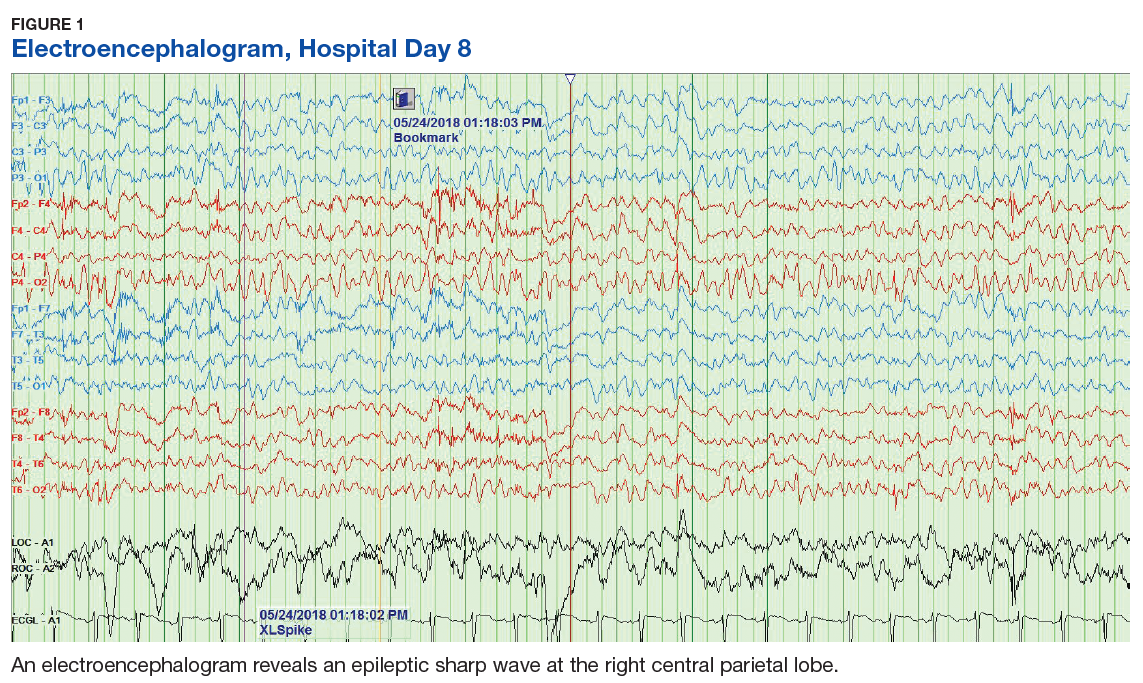
The patient continued to seize on hospital days 10 through 13. Oculocephalic maneuvers showed a tendency to keep her eyes deviated to the right. Her pupils continued to react to light. A repeat EEG showed diffuse slowing (5-6 Hz) with no epileptic activity seen (Figure 2). A second dose of eculizumab 900 mg IV was administered on hospital day 15. The patient experienced cardiac arrest on hospital day 16 and was successfully resuscitated. On hospital day 25 (10 days after receiving her second dose of eculizumab), the patient was able to speak and follow simple commands but exhibited difficulty concentrating and poor impulse control.
The patient was alert and oriented to person, place, time, and situation on hospital day 28 (6 days after the third and final dose of eculizumab). A neurologic exam was significant only for a slight intention tremor. She was continued on levetiracetam with a plan to be maintained on the medication for the next 6 months for seizure control. She was discharged on hospital day 30.
Twenty-eight days postdischarge (57 days postadmission), the patient showed marked recovery. She had returned to her previous employment as a business administrator on a part-time basis and exhibited no deficiencies in executive functioning or handling activities of daily living. Although she had been very active prior to this illness, she now experienced decreased physical and mental endurance; however, this gradually improved with physical therapy. She planned on returning to work on a full-time basis when she had regained her stamina. She also noticed difficulties in retaining short term memory since her discharge but believed that these symptoms were remitting. On examination her mental status and neurologic exam was significant for inability to continue serial 7s, left sided 4/5 muscle strength in quadriceps and thumb to 5th metacarpal adduction, bilateral 1+ reflexes in muscle groups tested (triceps, biceps, brachioradialis, patellar, and Achilles), loss of dull pinprick sensation bilaterally at web of hands, deficit in tandem gait while looking away, and slight intention tremor on finger to nose testing bilaterally (with left hand tremor more pronounced than right). Her complete blood count was normal. Her recovery continues to be monitored in an outpatient setting.
Discussion
HUS is characterized by 3 core clinical features: microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury.4 Schistocytes are seen on peripheral blood smear and occur due to the passage of red blood cells over the microvascular thrombi induced by the disease. HUS can be classified as typical, atypical, or occurring with a coexisting disease. Typical HUS is associated with STEC 0157:H7 subtype, a bacterium known to be acquired through contaminated food and via human-to-human transmission.6-8 In the case of typical STEC 0157:H7, the bacterium releases a verotoxin that damages the vascular endothelium, thereby leading to activation of the coagulation cascade and eventually the formation of thrombi.4 It has been hypothesized that the Shiga toxin also activates the alternative complement pathway directly, which could contribute to thrombosis.9 This would explain the findings of low complement levels in our patient. Atypical HUS is primarily attributable to mutations in the alternative complement pathway. Causes for the third type of HUS can include Streptococcus pneumoniae, HIV, drug toxicity, and alterations in the metabolism of cobalamin C.
Epidemiologically, 15.3% of children aged < 5 years develop typical HUS after exposure to STEC compared with 1.2% of adults aged 18 to 59 years. The median age of patients who developed HUS from STEC exposure was 4 years compared with 16 years for those who did not develop HUS.2
Neurologic manifestations increase mortality for HUS patients.10 These have been described in the pediatric population as alteration in consciousness (85%), seizures (71%), pyramidal syndrome (52%), and extrapyramidal syndrome with hypertonia (42%).11 Brain imaging in children has demonstrated hemorrhagic lesions involving the pons, basal ganglia, and occipital cortex.11 Blood flow to areas such as the cerebellum, brainstem, and orbitofrontal area can be compromised.10 Adult patients with HUS can present without lesions on cranial magnetic resonance imaging (MRI), but instead with transient symmetric vasogenic edema of the central brain stem.12 Unfortunately in this case, MRI was not performed because it was thought to provide limited aid in diagnosis and to avoid unnecessary testing for the acutely ill patient.
The underlying pathophysiology of neurologic manifestations in patients may be due to a metabolic disturbance, toxin-mediated damage of the vascular endothelium, or toxin-induced cytokine release resulting in death of neural cells and subsequent neuroinflammation. However, the most likely mechanism is parenchymal ischemic changes related to microangiopathy.11,13 Pediatric patients often experience seizures and altered mental status, and their EEGs display delta waves.13 This patient’s diffuse slowing on her second EEG and altered mental status suggests that the neuropathologic mechanisms for typical HUS in adults may be similar to those in children.
HUS Treatment
The treatment and management of adults with typical STEC-HUS is evolving. The patient was first suspected to have an infectious colitis and empiric antibiotics were initiated. Some studies suggest that antibiotic administration may worsen the course of HUS in children as it may lead to release and subsequent absorption of Shiga toxin in the intestine.9,14 However, there is little evidence to suggest harm or efficacy of administration in adults. It is unclear what role antibiotic administration played in the recovery time of HUS given the co-administration of other treatments such as eculizumab and plasmapheresis, but it does appear to have helped with the initial E coli infection.
Plasmapheresis was subsequently administered, due to its documented benefit in the treatment of HUS.15 However, it should be noted that even though plasmapheresis is currently used in patients with CNS involvement, it remains unproven with conflicting information on its efficacy.3,16 The mechanism of action is unclear, but it has been hypothesized that plasmapheresis prevents microangiopathy caused by microthrombi.3,16 For this reason, eculizumab is becoming the mainstay for treatment of STEC-HUS with neurologic complications given the lack of well researched alternative treatments. In this case study, the use of plasmapheresis did not result in clinical improvement, and was abandoned after 2 days of treatment.
Eculizumab is a humanized, recombinant monoclonal IgG antibody that is a terminal complement inhibitor of the alternative complement system at the final step to cleave C5.17 The Shiga toxin may directly activate the complement system via the alternative pathway, which can result in uncontrolled platelet and white blood cell activation and depletion, endothelial cell damage, and hemolysis. The galvanized complement system leads to a series of cascading events that contribute to organ damage and death.9 Eculizumab is FDA approved for use in atypical HUS.18 It also can be used off-label to treat typical-HUS in adults with neurologic complications.
Eculizumab interferes with the immune response against encapsulated bacteria because it inhibits the alternative complement pathway. Thus, vaccination against N meningitides is recommended 2 weeks prior to the administration of eculizumab. However, in situations where the risks of delaying eculizumab for 2 weeks are greater than the risk of developing an N meningitides infection, eculizumab may be given without delay.18 Given the rapid deterioration of our patient’s condition, the vaccine and eculizumab were given together with prophylactic azithromycin. Although penicillin is the standard for prophylaxis in this situation, the patient’s penicillin allergy led to the use of azithromycin 250 mg po once a day. Literature also suggests azithromycin reduces the carriage duration of E coli-induced colitis.19 As such, it is possible that some improvement in the patient’s condition could be attributed to the elimination of the pathogen and toxin.
Conclusion
Three doses of eculizumab were administered at weekly intervals, with the first dose on hospital day 8 and the final dose on hospital day 22. Prior to the first dose, the patient displayed significant decline in mental status with EEG findings of right hemisphere epileptogenic discharges. After her third dose, she was found to have a drastically improved mental status exam and a normal EEG. One week later, she was discharged home. At the time of her 1-month follow-up, she was independent in all activities of daily living and had returned to part-time work. Apart from subtle cognitive changes, the remainder of her neurologic exam was normal.
There is evidence that supports the efficacy of eculizumab in children with HUS with neurologic symptoms on dialysis.20 However, its use in adults is not well established.21 This patient required dialysis and had neurologic symptoms similar to pediatric patients described in the literature, and responded similarly to the eculizumab. The rationale for the use of eculizumab in STEC-HUS also is evidenced by in vitro demonstrations of complement activation in STEC-HUS.22-25 This case report adds to the literature supporting the use of eculizumab in adult patients with typical HUS with neurological complications. Further research is necessary to develop guidelines in the treatment of adult STEC-HUS with regards to neurologic complications.
Acknowledgments
The authors would like to thank Pete DiStaso, REEGT for his work on obtaining the electroencephalograms and Anthony Rinaldi, PsyD; Julie Cessnapalas, PsyD; and Syed Faizan Sagheer for proof-reading the article.
1. Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet. 2005;365(9464):1073-1086.
2. Gould LH, Demma L, Jones TF, et al. Hemolytic uremic syndrome and death in persons with Escherichia coli O157:H7 infection, foodborne diseases active surveillance network sites, 2000-2006. Clin Infect Dis. 2009;49(10):1480-1485.
3. Boyce TG, Swerdlow DL, Griffin PM. Escherichia coli O157:H7 and the hemolytic-uremic syndrome. N Engl J Med. 1995;333(6):364-368.
4. Rondeau E, Peraldi MN. Escherichia coli and the hemolytic-uremic syndrome. N Engl J Med. 1996;335(9):660-662.
5. Te Loo DM, van Hinsbergh VW, van den Heuvel LP, Monnens LA. Detection of verocytotoxin bound to circulating polymorphonuclear leukocytes of patients with hemolytic uremic syndrome. J Am Soc Nephrol. 2001;12(4):800-806.
6. Tran SL, Jenkins C, Livrelli V, Schüller S. Shiga toxin 2 translocation across intestinal epithelium is linked to virulence of Shiga toxin-producing Escherichia coli in humans. Microbiology. 2018;164(4):509-516.
7. Jokiranta TS. HUS and atypical HUS. Blood. 2017;129(21):2847-2856.
8. Ferens WA, Hovde CJ. Escherichia coli O157:H7: animal reservoir and sources of human infection. Foodborne Pathog Dis. 2011;8(4):465-487.
9. Percheron L, Gramada R, Tellier S, et al. Eculizumab treatment in severe pediatric STEC-HUS: a multicenter retrospective study. Pediatr Nephrol. 2018;33(8):1385-1394.
10. Hosaka T, Nakamagoe K, Tamaoka A. Hemolytic uremic syndrome-associated encephalopathy successfully treated with corticosteroids. Intern Med. 2017;56(21):2937-2941.
11. Nathanson S, Kwon T, Elmaleh M, et al. Acute neurological involvement in diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2010;5(7):1218-1228.
12. Wengenroth M, Hoeltje J, Repenthin J, et al. Central nervous system involvement in adults with epidemic hemolytic uremic syndrome. AJNR Am J Neuroradiol. 2013;34(5):1016-1021, S1.
13. Eriksson KJ, Boyd SG, Tasker RC. Acute neurology and neurophysiology of haemolytic-uraemic syndrome. Arch Dis Child. 2001;84(5):434-435.
14. Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342(26):1930-1936.
15. Nguyen TC, Kiss JE, Goldman JR, Carcillo JA. The role of plasmapheresis in critical illness. Crit Care Clin. 2012;28(3):453-468, vii.
16. Loos S, Ahlenstiel T, Kranz B, et al. An outbreak of Shiga toxin-producing Escherichia coli O104:H4 hemolytic uremic syndrome in Germany: presentation and short-term outcome in children. Clin Infect Dis. 2012;55(6):753-759.
17. Hossain MA, Cheema A, Kalathil S, et al. Atypical hemolytic uremic syndrome: Laboratory characteristics, complement-amplifying conditions, renal biopsy, and genetic mutations. Saudi J Kidney Dis Transpl. 2018;29(2):276-283.
18. Soliris (eculizumab) [package insert]. Cheshire, CT: Alexion Pharmaceuticals, Inc; 2011.
19. Keenswijk W, Raes A, Vande Walle J. Is eculizumab efficacious in Shigatoxin-associated hemolytic uremic syndrome? A narrative review of current evidence. Eur J Pediatr. 2018;177(3):311-318.
20. Lapeyraque AL, Malina M, Fremeaux-Bacchi V, et al. Eculizumab in severe Shiga-toxin-associated HUS. N Engl J Med. 2011;364(26):2561-2563.
21. Pape L, Hartmann H, Bange FC, Suerbaum S, Bueltmann E, Ahlenstiel-Grunow T. Eculizumab in typical hemolytic uremic syndrome (HUS) with neurological involvement. Medicine (Baltimore). 2015;94(24):e1000.
22. Kim Y, Miller K, Michael AF. Breakdown products of C3 and factor B in hemolytic-uremic syndrome. J Lab Clin Med. 1977;89(4):845-850.
23. Monnens L, Molenaar J, Lambert PH, Proesmans W, van Munster P. The complement system in hemolytic-uremic syndrome in childhood. Clin Nephrol. 1980;13(4):168-171.
24. Thurman JM, Marians R, Emlen W, et al. Alternative pathway of complement in children with diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2009;4(12):1920-1924.
25. Ståhl AL, Sartz L, Karpman D. Complement activation on platelet-leukocyte complexes and microparticles in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome. Blood. 2011;117(20):5503-5513.
The case of a female presenting with Shiga toxin-producing Escherichia coli and hemolytic uremic syndrome highlights a severe neurologic complication that canbe associated with these conditions.
The case of a female presenting with Shiga toxin-producing Escherichia coli and hemolytic uremic syndrome highlights a severe neurologic complication that canbe associated with these conditions.
Hemolytic uremic syndrome (HUS) is a rare illness that can be acquired through the consumption of food products contaminated with strains of Shiga toxin-producing Escherichia coli (E coli; STEC).1 Between 6% and 15% of individuals infected with STEC develop HUS, with children affected more frequently than adults.2,3 This strain of E coli releases Shiga toxin into the systemic circulation, which causes a thrombotic microangiopathy resulting in the characteristic HUS triad of symptoms: acute renal insufficiency, thrombocytopenia, and hemolytic anemia.4-6
Although neurologic features are common in HUS, they have not been extensively studied, particularly in adults. We report a case of STEC 0157:H7 subtype HUS in an adult with severe neurologic complications. This case highlights the neurological sequelae in an adult with typical STEC-HUS. The use of treatment modalities, such as plasmapheresis and eculizumab, and their use in adult typical STEC-HUS also is explored.
Case
A 53-year-old white woman with no pertinent past medical history presented to the Bay Pines Veterans Affairs Healthcare System Emergency Department with a 2-day history of abdominal pain, vomiting, nausea, diarrhea, and bright bloody stools. She returned from a cruise to the Bahamas 3 days prior, where she ate local foods, including salads. She reported no fever, shortness of breath, chest pain, headache, and cognitive difficulties. She presented with a normal mental status and neurologic exam. Apart from leukocytosis and elevated glucose level, her laboratory results at initial presentation were normal, (Table). A stool sample showed occult blood with white blood cell counts (WBCs) but was negative for Clostridium difficile. She was started on ciprofloxacin 400 mg and metronidazole 500 mg on the day of admission.
Hematuria was found on hospital day 2. On hospital day 4, the patient exhibited word finding difficulties. Blood studies revealed anemia, thrombocytopenia, leukocytosis, and increasing blood urea nitrogen (BUN) and creatinine. A computed tomography scan of the head was normal. Laboratory analysis showed schistocytes in the peripheral blood smear.
The patient’s cognitive functioning deteriorated on hospital day 5. She was not oriented to time or place. Her laboratory results showed complement level C3 at 70 mg/dL (ref: 83-193 mg/dL) complement C4 at 12 mg/dL (ref: 15-57mg/dL). The patient exhibited oliguria and hyponatremia, as well as both metabolic and respiratory acidosis; dialysis was then initiated. Results from the stool sample that was collected on hospital day 1 were received and tested positive for Shiga toxin.
At this point, the patient’s presentation of hemolytic anemia and thrombocytopenia in the setting of acute bloody diarrheal illness with known Shiga toxin, schistocytes on blood smear, and lack of pertinent medical history for other causes of this presentation made STEC-HUS the leading differential diagnosis. Plasmapheresis was ordered and performed on hospital day 6 and 7. Shiga toxin was no longer detected in the stool and antibiotics were stopped on hospital day 7.
The patient’s progressive deterioration in mental status continued on hospital day 8. She was not oriented to time or place, unable to perform simple calculations, and could not spell the word “hand” backwards. Physicians observed repetitive jerking motions of the upper extremities that were worse on the left side. An electroencephalogram (EEG) revealed right hemispheric sharp waves that were thought to be epileptiform (Figure 1). The patient began taking levetiracetam 1500 mg IV with 750 mg bid maintenance for seizure control. Plasmapheresis was discontinued due to her continued neurologic deterioration on this therapy. Consequently, eculizumab 900 mg IV was given along with the Neisseria meningitidis (N meningitidis) vaccine and a 19-day course of azithromycin 250 mg po as prophylaxis for encapsulated bacteria.
The patient continued to seize on hospital days 10 through 13. Oculocephalic maneuvers showed a tendency to keep her eyes deviated to the right. Her pupils continued to react to light. A repeat EEG showed diffuse slowing (5-6 Hz) with no epileptic activity seen (Figure 2). A second dose of eculizumab 900 mg IV was administered on hospital day 15. The patient experienced cardiac arrest on hospital day 16 and was successfully resuscitated. On hospital day 25 (10 days after receiving her second dose of eculizumab), the patient was able to speak and follow simple commands but exhibited difficulty concentrating and poor impulse control.
The patient was alert and oriented to person, place, time, and situation on hospital day 28 (6 days after the third and final dose of eculizumab). A neurologic exam was significant only for a slight intention tremor. She was continued on levetiracetam with a plan to be maintained on the medication for the next 6 months for seizure control. She was discharged on hospital day 30.
Twenty-eight days postdischarge (57 days postadmission), the patient showed marked recovery. She had returned to her previous employment as a business administrator on a part-time basis and exhibited no deficiencies in executive functioning or handling activities of daily living. Although she had been very active prior to this illness, she now experienced decreased physical and mental endurance; however, this gradually improved with physical therapy. She planned on returning to work on a full-time basis when she had regained her stamina. She also noticed difficulties in retaining short term memory since her discharge but believed that these symptoms were remitting. On examination her mental status and neurologic exam was significant for inability to continue serial 7s, left sided 4/5 muscle strength in quadriceps and thumb to 5th metacarpal adduction, bilateral 1+ reflexes in muscle groups tested (triceps, biceps, brachioradialis, patellar, and Achilles), loss of dull pinprick sensation bilaterally at web of hands, deficit in tandem gait while looking away, and slight intention tremor on finger to nose testing bilaterally (with left hand tremor more pronounced than right). Her complete blood count was normal. Her recovery continues to be monitored in an outpatient setting.
Discussion
HUS is characterized by 3 core clinical features: microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury.4 Schistocytes are seen on peripheral blood smear and occur due to the passage of red blood cells over the microvascular thrombi induced by the disease. HUS can be classified as typical, atypical, or occurring with a coexisting disease. Typical HUS is associated with STEC 0157:H7 subtype, a bacterium known to be acquired through contaminated food and via human-to-human transmission.6-8 In the case of typical STEC 0157:H7, the bacterium releases a verotoxin that damages the vascular endothelium, thereby leading to activation of the coagulation cascade and eventually the formation of thrombi.4 It has been hypothesized that the Shiga toxin also activates the alternative complement pathway directly, which could contribute to thrombosis.9 This would explain the findings of low complement levels in our patient. Atypical HUS is primarily attributable to mutations in the alternative complement pathway. Causes for the third type of HUS can include Streptococcus pneumoniae, HIV, drug toxicity, and alterations in the metabolism of cobalamin C.
Epidemiologically, 15.3% of children aged < 5 years develop typical HUS after exposure to STEC compared with 1.2% of adults aged 18 to 59 years. The median age of patients who developed HUS from STEC exposure was 4 years compared with 16 years for those who did not develop HUS.2
Neurologic manifestations increase mortality for HUS patients.10 These have been described in the pediatric population as alteration in consciousness (85%), seizures (71%), pyramidal syndrome (52%), and extrapyramidal syndrome with hypertonia (42%).11 Brain imaging in children has demonstrated hemorrhagic lesions involving the pons, basal ganglia, and occipital cortex.11 Blood flow to areas such as the cerebellum, brainstem, and orbitofrontal area can be compromised.10 Adult patients with HUS can present without lesions on cranial magnetic resonance imaging (MRI), but instead with transient symmetric vasogenic edema of the central brain stem.12 Unfortunately in this case, MRI was not performed because it was thought to provide limited aid in diagnosis and to avoid unnecessary testing for the acutely ill patient.
The underlying pathophysiology of neurologic manifestations in patients may be due to a metabolic disturbance, toxin-mediated damage of the vascular endothelium, or toxin-induced cytokine release resulting in death of neural cells and subsequent neuroinflammation. However, the most likely mechanism is parenchymal ischemic changes related to microangiopathy.11,13 Pediatric patients often experience seizures and altered mental status, and their EEGs display delta waves.13 This patient’s diffuse slowing on her second EEG and altered mental status suggests that the neuropathologic mechanisms for typical HUS in adults may be similar to those in children.
HUS Treatment
The treatment and management of adults with typical STEC-HUS is evolving. The patient was first suspected to have an infectious colitis and empiric antibiotics were initiated. Some studies suggest that antibiotic administration may worsen the course of HUS in children as it may lead to release and subsequent absorption of Shiga toxin in the intestine.9,14 However, there is little evidence to suggest harm or efficacy of administration in adults. It is unclear what role antibiotic administration played in the recovery time of HUS given the co-administration of other treatments such as eculizumab and plasmapheresis, but it does appear to have helped with the initial E coli infection.
Plasmapheresis was subsequently administered, due to its documented benefit in the treatment of HUS.15 However, it should be noted that even though plasmapheresis is currently used in patients with CNS involvement, it remains unproven with conflicting information on its efficacy.3,16 The mechanism of action is unclear, but it has been hypothesized that plasmapheresis prevents microangiopathy caused by microthrombi.3,16 For this reason, eculizumab is becoming the mainstay for treatment of STEC-HUS with neurologic complications given the lack of well researched alternative treatments. In this case study, the use of plasmapheresis did not result in clinical improvement, and was abandoned after 2 days of treatment.
Eculizumab is a humanized, recombinant monoclonal IgG antibody that is a terminal complement inhibitor of the alternative complement system at the final step to cleave C5.17 The Shiga toxin may directly activate the complement system via the alternative pathway, which can result in uncontrolled platelet and white blood cell activation and depletion, endothelial cell damage, and hemolysis. The galvanized complement system leads to a series of cascading events that contribute to organ damage and death.9 Eculizumab is FDA approved for use in atypical HUS.18 It also can be used off-label to treat typical-HUS in adults with neurologic complications.
Eculizumab interferes with the immune response against encapsulated bacteria because it inhibits the alternative complement pathway. Thus, vaccination against N meningitides is recommended 2 weeks prior to the administration of eculizumab. However, in situations where the risks of delaying eculizumab for 2 weeks are greater than the risk of developing an N meningitides infection, eculizumab may be given without delay.18 Given the rapid deterioration of our patient’s condition, the vaccine and eculizumab were given together with prophylactic azithromycin. Although penicillin is the standard for prophylaxis in this situation, the patient’s penicillin allergy led to the use of azithromycin 250 mg po once a day. Literature also suggests azithromycin reduces the carriage duration of E coli-induced colitis.19 As such, it is possible that some improvement in the patient’s condition could be attributed to the elimination of the pathogen and toxin.
Conclusion
Three doses of eculizumab were administered at weekly intervals, with the first dose on hospital day 8 and the final dose on hospital day 22. Prior to the first dose, the patient displayed significant decline in mental status with EEG findings of right hemisphere epileptogenic discharges. After her third dose, she was found to have a drastically improved mental status exam and a normal EEG. One week later, she was discharged home. At the time of her 1-month follow-up, she was independent in all activities of daily living and had returned to part-time work. Apart from subtle cognitive changes, the remainder of her neurologic exam was normal.
There is evidence that supports the efficacy of eculizumab in children with HUS with neurologic symptoms on dialysis.20 However, its use in adults is not well established.21 This patient required dialysis and had neurologic symptoms similar to pediatric patients described in the literature, and responded similarly to the eculizumab. The rationale for the use of eculizumab in STEC-HUS also is evidenced by in vitro demonstrations of complement activation in STEC-HUS.22-25 This case report adds to the literature supporting the use of eculizumab in adult patients with typical HUS with neurological complications. Further research is necessary to develop guidelines in the treatment of adult STEC-HUS with regards to neurologic complications.
Acknowledgments
The authors would like to thank Pete DiStaso, REEGT for his work on obtaining the electroencephalograms and Anthony Rinaldi, PsyD; Julie Cessnapalas, PsyD; and Syed Faizan Sagheer for proof-reading the article.
Hemolytic uremic syndrome (HUS) is a rare illness that can be acquired through the consumption of food products contaminated with strains of Shiga toxin-producing Escherichia coli (E coli; STEC).1 Between 6% and 15% of individuals infected with STEC develop HUS, with children affected more frequently than adults.2,3 This strain of E coli releases Shiga toxin into the systemic circulation, which causes a thrombotic microangiopathy resulting in the characteristic HUS triad of symptoms: acute renal insufficiency, thrombocytopenia, and hemolytic anemia.4-6
Although neurologic features are common in HUS, they have not been extensively studied, particularly in adults. We report a case of STEC 0157:H7 subtype HUS in an adult with severe neurologic complications. This case highlights the neurological sequelae in an adult with typical STEC-HUS. The use of treatment modalities, such as plasmapheresis and eculizumab, and their use in adult typical STEC-HUS also is explored.
Case
A 53-year-old white woman with no pertinent past medical history presented to the Bay Pines Veterans Affairs Healthcare System Emergency Department with a 2-day history of abdominal pain, vomiting, nausea, diarrhea, and bright bloody stools. She returned from a cruise to the Bahamas 3 days prior, where she ate local foods, including salads. She reported no fever, shortness of breath, chest pain, headache, and cognitive difficulties. She presented with a normal mental status and neurologic exam. Apart from leukocytosis and elevated glucose level, her laboratory results at initial presentation were normal, (Table). A stool sample showed occult blood with white blood cell counts (WBCs) but was negative for Clostridium difficile. She was started on ciprofloxacin 400 mg and metronidazole 500 mg on the day of admission.
Hematuria was found on hospital day 2. On hospital day 4, the patient exhibited word finding difficulties. Blood studies revealed anemia, thrombocytopenia, leukocytosis, and increasing blood urea nitrogen (BUN) and creatinine. A computed tomography scan of the head was normal. Laboratory analysis showed schistocytes in the peripheral blood smear.
The patient’s cognitive functioning deteriorated on hospital day 5. She was not oriented to time or place. Her laboratory results showed complement level C3 at 70 mg/dL (ref: 83-193 mg/dL) complement C4 at 12 mg/dL (ref: 15-57mg/dL). The patient exhibited oliguria and hyponatremia, as well as both metabolic and respiratory acidosis; dialysis was then initiated. Results from the stool sample that was collected on hospital day 1 were received and tested positive for Shiga toxin.
At this point, the patient’s presentation of hemolytic anemia and thrombocytopenia in the setting of acute bloody diarrheal illness with known Shiga toxin, schistocytes on blood smear, and lack of pertinent medical history for other causes of this presentation made STEC-HUS the leading differential diagnosis. Plasmapheresis was ordered and performed on hospital day 6 and 7. Shiga toxin was no longer detected in the stool and antibiotics were stopped on hospital day 7.
The patient’s progressive deterioration in mental status continued on hospital day 8. She was not oriented to time or place, unable to perform simple calculations, and could not spell the word “hand” backwards. Physicians observed repetitive jerking motions of the upper extremities that were worse on the left side. An electroencephalogram (EEG) revealed right hemispheric sharp waves that were thought to be epileptiform (Figure 1). The patient began taking levetiracetam 1500 mg IV with 750 mg bid maintenance for seizure control. Plasmapheresis was discontinued due to her continued neurologic deterioration on this therapy. Consequently, eculizumab 900 mg IV was given along with the Neisseria meningitidis (N meningitidis) vaccine and a 19-day course of azithromycin 250 mg po as prophylaxis for encapsulated bacteria.
The patient continued to seize on hospital days 10 through 13. Oculocephalic maneuvers showed a tendency to keep her eyes deviated to the right. Her pupils continued to react to light. A repeat EEG showed diffuse slowing (5-6 Hz) with no epileptic activity seen (Figure 2). A second dose of eculizumab 900 mg IV was administered on hospital day 15. The patient experienced cardiac arrest on hospital day 16 and was successfully resuscitated. On hospital day 25 (10 days after receiving her second dose of eculizumab), the patient was able to speak and follow simple commands but exhibited difficulty concentrating and poor impulse control.
The patient was alert and oriented to person, place, time, and situation on hospital day 28 (6 days after the third and final dose of eculizumab). A neurologic exam was significant only for a slight intention tremor. She was continued on levetiracetam with a plan to be maintained on the medication for the next 6 months for seizure control. She was discharged on hospital day 30.
Twenty-eight days postdischarge (57 days postadmission), the patient showed marked recovery. She had returned to her previous employment as a business administrator on a part-time basis and exhibited no deficiencies in executive functioning or handling activities of daily living. Although she had been very active prior to this illness, she now experienced decreased physical and mental endurance; however, this gradually improved with physical therapy. She planned on returning to work on a full-time basis when she had regained her stamina. She also noticed difficulties in retaining short term memory since her discharge but believed that these symptoms were remitting. On examination her mental status and neurologic exam was significant for inability to continue serial 7s, left sided 4/5 muscle strength in quadriceps and thumb to 5th metacarpal adduction, bilateral 1+ reflexes in muscle groups tested (triceps, biceps, brachioradialis, patellar, and Achilles), loss of dull pinprick sensation bilaterally at web of hands, deficit in tandem gait while looking away, and slight intention tremor on finger to nose testing bilaterally (with left hand tremor more pronounced than right). Her complete blood count was normal. Her recovery continues to be monitored in an outpatient setting.
Discussion
HUS is characterized by 3 core clinical features: microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury.4 Schistocytes are seen on peripheral blood smear and occur due to the passage of red blood cells over the microvascular thrombi induced by the disease. HUS can be classified as typical, atypical, or occurring with a coexisting disease. Typical HUS is associated with STEC 0157:H7 subtype, a bacterium known to be acquired through contaminated food and via human-to-human transmission.6-8 In the case of typical STEC 0157:H7, the bacterium releases a verotoxin that damages the vascular endothelium, thereby leading to activation of the coagulation cascade and eventually the formation of thrombi.4 It has been hypothesized that the Shiga toxin also activates the alternative complement pathway directly, which could contribute to thrombosis.9 This would explain the findings of low complement levels in our patient. Atypical HUS is primarily attributable to mutations in the alternative complement pathway. Causes for the third type of HUS can include Streptococcus pneumoniae, HIV, drug toxicity, and alterations in the metabolism of cobalamin C.
Epidemiologically, 15.3% of children aged < 5 years develop typical HUS after exposure to STEC compared with 1.2% of adults aged 18 to 59 years. The median age of patients who developed HUS from STEC exposure was 4 years compared with 16 years for those who did not develop HUS.2
Neurologic manifestations increase mortality for HUS patients.10 These have been described in the pediatric population as alteration in consciousness (85%), seizures (71%), pyramidal syndrome (52%), and extrapyramidal syndrome with hypertonia (42%).11 Brain imaging in children has demonstrated hemorrhagic lesions involving the pons, basal ganglia, and occipital cortex.11 Blood flow to areas such as the cerebellum, brainstem, and orbitofrontal area can be compromised.10 Adult patients with HUS can present without lesions on cranial magnetic resonance imaging (MRI), but instead with transient symmetric vasogenic edema of the central brain stem.12 Unfortunately in this case, MRI was not performed because it was thought to provide limited aid in diagnosis and to avoid unnecessary testing for the acutely ill patient.
The underlying pathophysiology of neurologic manifestations in patients may be due to a metabolic disturbance, toxin-mediated damage of the vascular endothelium, or toxin-induced cytokine release resulting in death of neural cells and subsequent neuroinflammation. However, the most likely mechanism is parenchymal ischemic changes related to microangiopathy.11,13 Pediatric patients often experience seizures and altered mental status, and their EEGs display delta waves.13 This patient’s diffuse slowing on her second EEG and altered mental status suggests that the neuropathologic mechanisms for typical HUS in adults may be similar to those in children.
HUS Treatment
The treatment and management of adults with typical STEC-HUS is evolving. The patient was first suspected to have an infectious colitis and empiric antibiotics were initiated. Some studies suggest that antibiotic administration may worsen the course of HUS in children as it may lead to release and subsequent absorption of Shiga toxin in the intestine.9,14 However, there is little evidence to suggest harm or efficacy of administration in adults. It is unclear what role antibiotic administration played in the recovery time of HUS given the co-administration of other treatments such as eculizumab and plasmapheresis, but it does appear to have helped with the initial E coli infection.
Plasmapheresis was subsequently administered, due to its documented benefit in the treatment of HUS.15 However, it should be noted that even though plasmapheresis is currently used in patients with CNS involvement, it remains unproven with conflicting information on its efficacy.3,16 The mechanism of action is unclear, but it has been hypothesized that plasmapheresis prevents microangiopathy caused by microthrombi.3,16 For this reason, eculizumab is becoming the mainstay for treatment of STEC-HUS with neurologic complications given the lack of well researched alternative treatments. In this case study, the use of plasmapheresis did not result in clinical improvement, and was abandoned after 2 days of treatment.
Eculizumab is a humanized, recombinant monoclonal IgG antibody that is a terminal complement inhibitor of the alternative complement system at the final step to cleave C5.17 The Shiga toxin may directly activate the complement system via the alternative pathway, which can result in uncontrolled platelet and white blood cell activation and depletion, endothelial cell damage, and hemolysis. The galvanized complement system leads to a series of cascading events that contribute to organ damage and death.9 Eculizumab is FDA approved for use in atypical HUS.18 It also can be used off-label to treat typical-HUS in adults with neurologic complications.
Eculizumab interferes with the immune response against encapsulated bacteria because it inhibits the alternative complement pathway. Thus, vaccination against N meningitides is recommended 2 weeks prior to the administration of eculizumab. However, in situations where the risks of delaying eculizumab for 2 weeks are greater than the risk of developing an N meningitides infection, eculizumab may be given without delay.18 Given the rapid deterioration of our patient’s condition, the vaccine and eculizumab were given together with prophylactic azithromycin. Although penicillin is the standard for prophylaxis in this situation, the patient’s penicillin allergy led to the use of azithromycin 250 mg po once a day. Literature also suggests azithromycin reduces the carriage duration of E coli-induced colitis.19 As such, it is possible that some improvement in the patient’s condition could be attributed to the elimination of the pathogen and toxin.
Conclusion
Three doses of eculizumab were administered at weekly intervals, with the first dose on hospital day 8 and the final dose on hospital day 22. Prior to the first dose, the patient displayed significant decline in mental status with EEG findings of right hemisphere epileptogenic discharges. After her third dose, she was found to have a drastically improved mental status exam and a normal EEG. One week later, she was discharged home. At the time of her 1-month follow-up, she was independent in all activities of daily living and had returned to part-time work. Apart from subtle cognitive changes, the remainder of her neurologic exam was normal.
There is evidence that supports the efficacy of eculizumab in children with HUS with neurologic symptoms on dialysis.20 However, its use in adults is not well established.21 This patient required dialysis and had neurologic symptoms similar to pediatric patients described in the literature, and responded similarly to the eculizumab. The rationale for the use of eculizumab in STEC-HUS also is evidenced by in vitro demonstrations of complement activation in STEC-HUS.22-25 This case report adds to the literature supporting the use of eculizumab in adult patients with typical HUS with neurological complications. Further research is necessary to develop guidelines in the treatment of adult STEC-HUS with regards to neurologic complications.
Acknowledgments
The authors would like to thank Pete DiStaso, REEGT for his work on obtaining the electroencephalograms and Anthony Rinaldi, PsyD; Julie Cessnapalas, PsyD; and Syed Faizan Sagheer for proof-reading the article.
1. Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet. 2005;365(9464):1073-1086.
2. Gould LH, Demma L, Jones TF, et al. Hemolytic uremic syndrome and death in persons with Escherichia coli O157:H7 infection, foodborne diseases active surveillance network sites, 2000-2006. Clin Infect Dis. 2009;49(10):1480-1485.
3. Boyce TG, Swerdlow DL, Griffin PM. Escherichia coli O157:H7 and the hemolytic-uremic syndrome. N Engl J Med. 1995;333(6):364-368.
4. Rondeau E, Peraldi MN. Escherichia coli and the hemolytic-uremic syndrome. N Engl J Med. 1996;335(9):660-662.
5. Te Loo DM, van Hinsbergh VW, van den Heuvel LP, Monnens LA. Detection of verocytotoxin bound to circulating polymorphonuclear leukocytes of patients with hemolytic uremic syndrome. J Am Soc Nephrol. 2001;12(4):800-806.
6. Tran SL, Jenkins C, Livrelli V, Schüller S. Shiga toxin 2 translocation across intestinal epithelium is linked to virulence of Shiga toxin-producing Escherichia coli in humans. Microbiology. 2018;164(4):509-516.
7. Jokiranta TS. HUS and atypical HUS. Blood. 2017;129(21):2847-2856.
8. Ferens WA, Hovde CJ. Escherichia coli O157:H7: animal reservoir and sources of human infection. Foodborne Pathog Dis. 2011;8(4):465-487.
9. Percheron L, Gramada R, Tellier S, et al. Eculizumab treatment in severe pediatric STEC-HUS: a multicenter retrospective study. Pediatr Nephrol. 2018;33(8):1385-1394.
10. Hosaka T, Nakamagoe K, Tamaoka A. Hemolytic uremic syndrome-associated encephalopathy successfully treated with corticosteroids. Intern Med. 2017;56(21):2937-2941.
11. Nathanson S, Kwon T, Elmaleh M, et al. Acute neurological involvement in diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2010;5(7):1218-1228.
12. Wengenroth M, Hoeltje J, Repenthin J, et al. Central nervous system involvement in adults with epidemic hemolytic uremic syndrome. AJNR Am J Neuroradiol. 2013;34(5):1016-1021, S1.
13. Eriksson KJ, Boyd SG, Tasker RC. Acute neurology and neurophysiology of haemolytic-uraemic syndrome. Arch Dis Child. 2001;84(5):434-435.
14. Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342(26):1930-1936.
15. Nguyen TC, Kiss JE, Goldman JR, Carcillo JA. The role of plasmapheresis in critical illness. Crit Care Clin. 2012;28(3):453-468, vii.
16. Loos S, Ahlenstiel T, Kranz B, et al. An outbreak of Shiga toxin-producing Escherichia coli O104:H4 hemolytic uremic syndrome in Germany: presentation and short-term outcome in children. Clin Infect Dis. 2012;55(6):753-759.
17. Hossain MA, Cheema A, Kalathil S, et al. Atypical hemolytic uremic syndrome: Laboratory characteristics, complement-amplifying conditions, renal biopsy, and genetic mutations. Saudi J Kidney Dis Transpl. 2018;29(2):276-283.
18. Soliris (eculizumab) [package insert]. Cheshire, CT: Alexion Pharmaceuticals, Inc; 2011.
19. Keenswijk W, Raes A, Vande Walle J. Is eculizumab efficacious in Shigatoxin-associated hemolytic uremic syndrome? A narrative review of current evidence. Eur J Pediatr. 2018;177(3):311-318.
20. Lapeyraque AL, Malina M, Fremeaux-Bacchi V, et al. Eculizumab in severe Shiga-toxin-associated HUS. N Engl J Med. 2011;364(26):2561-2563.
21. Pape L, Hartmann H, Bange FC, Suerbaum S, Bueltmann E, Ahlenstiel-Grunow T. Eculizumab in typical hemolytic uremic syndrome (HUS) with neurological involvement. Medicine (Baltimore). 2015;94(24):e1000.
22. Kim Y, Miller K, Michael AF. Breakdown products of C3 and factor B in hemolytic-uremic syndrome. J Lab Clin Med. 1977;89(4):845-850.
23. Monnens L, Molenaar J, Lambert PH, Proesmans W, van Munster P. The complement system in hemolytic-uremic syndrome in childhood. Clin Nephrol. 1980;13(4):168-171.
24. Thurman JM, Marians R, Emlen W, et al. Alternative pathway of complement in children with diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2009;4(12):1920-1924.
25. Ståhl AL, Sartz L, Karpman D. Complement activation on platelet-leukocyte complexes and microparticles in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome. Blood. 2011;117(20):5503-5513.
1. Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet. 2005;365(9464):1073-1086.
2. Gould LH, Demma L, Jones TF, et al. Hemolytic uremic syndrome and death in persons with Escherichia coli O157:H7 infection, foodborne diseases active surveillance network sites, 2000-2006. Clin Infect Dis. 2009;49(10):1480-1485.
3. Boyce TG, Swerdlow DL, Griffin PM. Escherichia coli O157:H7 and the hemolytic-uremic syndrome. N Engl J Med. 1995;333(6):364-368.
4. Rondeau E, Peraldi MN. Escherichia coli and the hemolytic-uremic syndrome. N Engl J Med. 1996;335(9):660-662.
5. Te Loo DM, van Hinsbergh VW, van den Heuvel LP, Monnens LA. Detection of verocytotoxin bound to circulating polymorphonuclear leukocytes of patients with hemolytic uremic syndrome. J Am Soc Nephrol. 2001;12(4):800-806.
6. Tran SL, Jenkins C, Livrelli V, Schüller S. Shiga toxin 2 translocation across intestinal epithelium is linked to virulence of Shiga toxin-producing Escherichia coli in humans. Microbiology. 2018;164(4):509-516.
7. Jokiranta TS. HUS and atypical HUS. Blood. 2017;129(21):2847-2856.
8. Ferens WA, Hovde CJ. Escherichia coli O157:H7: animal reservoir and sources of human infection. Foodborne Pathog Dis. 2011;8(4):465-487.
9. Percheron L, Gramada R, Tellier S, et al. Eculizumab treatment in severe pediatric STEC-HUS: a multicenter retrospective study. Pediatr Nephrol. 2018;33(8):1385-1394.
10. Hosaka T, Nakamagoe K, Tamaoka A. Hemolytic uremic syndrome-associated encephalopathy successfully treated with corticosteroids. Intern Med. 2017;56(21):2937-2941.
11. Nathanson S, Kwon T, Elmaleh M, et al. Acute neurological involvement in diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2010;5(7):1218-1228.
12. Wengenroth M, Hoeltje J, Repenthin J, et al. Central nervous system involvement in adults with epidemic hemolytic uremic syndrome. AJNR Am J Neuroradiol. 2013;34(5):1016-1021, S1.
13. Eriksson KJ, Boyd SG, Tasker RC. Acute neurology and neurophysiology of haemolytic-uraemic syndrome. Arch Dis Child. 2001;84(5):434-435.
14. Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342(26):1930-1936.
15. Nguyen TC, Kiss JE, Goldman JR, Carcillo JA. The role of plasmapheresis in critical illness. Crit Care Clin. 2012;28(3):453-468, vii.
16. Loos S, Ahlenstiel T, Kranz B, et al. An outbreak of Shiga toxin-producing Escherichia coli O104:H4 hemolytic uremic syndrome in Germany: presentation and short-term outcome in children. Clin Infect Dis. 2012;55(6):753-759.
17. Hossain MA, Cheema A, Kalathil S, et al. Atypical hemolytic uremic syndrome: Laboratory characteristics, complement-amplifying conditions, renal biopsy, and genetic mutations. Saudi J Kidney Dis Transpl. 2018;29(2):276-283.
18. Soliris (eculizumab) [package insert]. Cheshire, CT: Alexion Pharmaceuticals, Inc; 2011.
19. Keenswijk W, Raes A, Vande Walle J. Is eculizumab efficacious in Shigatoxin-associated hemolytic uremic syndrome? A narrative review of current evidence. Eur J Pediatr. 2018;177(3):311-318.
20. Lapeyraque AL, Malina M, Fremeaux-Bacchi V, et al. Eculizumab in severe Shiga-toxin-associated HUS. N Engl J Med. 2011;364(26):2561-2563.
21. Pape L, Hartmann H, Bange FC, Suerbaum S, Bueltmann E, Ahlenstiel-Grunow T. Eculizumab in typical hemolytic uremic syndrome (HUS) with neurological involvement. Medicine (Baltimore). 2015;94(24):e1000.
22. Kim Y, Miller K, Michael AF. Breakdown products of C3 and factor B in hemolytic-uremic syndrome. J Lab Clin Med. 1977;89(4):845-850.
23. Monnens L, Molenaar J, Lambert PH, Proesmans W, van Munster P. The complement system in hemolytic-uremic syndrome in childhood. Clin Nephrol. 1980;13(4):168-171.
24. Thurman JM, Marians R, Emlen W, et al. Alternative pathway of complement in children with diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2009;4(12):1920-1924.
25. Ståhl AL, Sartz L, Karpman D. Complement activation on platelet-leukocyte complexes and microparticles in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome. Blood. 2011;117(20):5503-5513.
Starting to assess the toll
This morning, Megan A. Adams (a GI & Hepatology News Associate Editor and a Michigan faculty member) and I held an hour-long video conference with all of our Michigan GI fellows. Our four third-year fellows talked about their job search and employment plans for July. Three will join academic centers (UNC, University of Wisconsin, Henry Ford) and one will enter private practice (Atlanta Gastroenterology). I was glad to hear that all had been reassured that their positions were secure despite the COVID-19 impact. As I speak with colleagues across the country, all (whether health system physicians, academic faculty, or community gastroenterologists) are experiencing the financial, emotional, and operational effects of this pandemic. This is an experience that will define our professional careers.

As one of three chief clinical officers at Michigan Medicine, I am part of a four-person team that leads the faculty medical group and the ambulatory portion of our health system. Each of our segments (ambulatory, adult hospital, children’s hospital, and medical school) have targets for sustained cost reductions that total $400 million and Michigan Medicine (as published in the news) plans to reduce our workforce (nonfaculty) by 1,400. We have a hiring freeze, leaders are taking salary reductions, and we have instituted other painful, cost-saving measures. The physician leaders we hired just 12 months ago to oversee a new faculty group structure were thrust into a firestorm. Department chairs, division chiefs, nursing and administrative leaders all are having to make heart-wrenching cost-cutting decisions. Together, we have to make individual reductions in force or retain decisions about people we work with daily. This emotional toll will never truly heal for anyone involved.
There will be little time to recover. We are scrambling to reopen safely, with a planned process. We have a backlog of 12,000 surgeries and 8,000 endoscopy procedures that have been deferred. Eight-hundred children are behind in their well-child medical care, frightened patients are sitting home with critical aortic stenosis, dangerous hypertension, growing cancers, and other urgent medical needs. Private practices are facing the same issues, financial pressures, and emotional toll.
Anna Quindlen once said, “Grief is a whisper in the world, but a clamor within.” Recognize the toll this is taking and don’t be alone with your grief.
John I. Allen, MD, MBA, AGAF
Editor in Chief
This morning, Megan A. Adams (a GI & Hepatology News Associate Editor and a Michigan faculty member) and I held an hour-long video conference with all of our Michigan GI fellows. Our four third-year fellows talked about their job search and employment plans for July. Three will join academic centers (UNC, University of Wisconsin, Henry Ford) and one will enter private practice (Atlanta Gastroenterology). I was glad to hear that all had been reassured that their positions were secure despite the COVID-19 impact. As I speak with colleagues across the country, all (whether health system physicians, academic faculty, or community gastroenterologists) are experiencing the financial, emotional, and operational effects of this pandemic. This is an experience that will define our professional careers.
As one of three chief clinical officers at Michigan Medicine, I am part of a four-person team that leads the faculty medical group and the ambulatory portion of our health system. Each of our segments (ambulatory, adult hospital, children’s hospital, and medical school) have targets for sustained cost reductions that total $400 million and Michigan Medicine (as published in the news) plans to reduce our workforce (nonfaculty) by 1,400. We have a hiring freeze, leaders are taking salary reductions, and we have instituted other painful, cost-saving measures. The physician leaders we hired just 12 months ago to oversee a new faculty group structure were thrust into a firestorm. Department chairs, division chiefs, nursing and administrative leaders all are having to make heart-wrenching cost-cutting decisions. Together, we have to make individual reductions in force or retain decisions about people we work with daily. This emotional toll will never truly heal for anyone involved.
There will be little time to recover. We are scrambling to reopen safely, with a planned process. We have a backlog of 12,000 surgeries and 8,000 endoscopy procedures that have been deferred. Eight-hundred children are behind in their well-child medical care, frightened patients are sitting home with critical aortic stenosis, dangerous hypertension, growing cancers, and other urgent medical needs. Private practices are facing the same issues, financial pressures, and emotional toll.
Anna Quindlen once said, “Grief is a whisper in the world, but a clamor within.” Recognize the toll this is taking and don’t be alone with your grief.
John I. Allen, MD, MBA, AGAF
Editor in Chief
This morning, Megan A. Adams (a GI & Hepatology News Associate Editor and a Michigan faculty member) and I held an hour-long video conference with all of our Michigan GI fellows. Our four third-year fellows talked about their job search and employment plans for July. Three will join academic centers (UNC, University of Wisconsin, Henry Ford) and one will enter private practice (Atlanta Gastroenterology). I was glad to hear that all had been reassured that their positions were secure despite the COVID-19 impact. As I speak with colleagues across the country, all (whether health system physicians, academic faculty, or community gastroenterologists) are experiencing the financial, emotional, and operational effects of this pandemic. This is an experience that will define our professional careers.
As one of three chief clinical officers at Michigan Medicine, I am part of a four-person team that leads the faculty medical group and the ambulatory portion of our health system. Each of our segments (ambulatory, adult hospital, children’s hospital, and medical school) have targets for sustained cost reductions that total $400 million and Michigan Medicine (as published in the news) plans to reduce our workforce (nonfaculty) by 1,400. We have a hiring freeze, leaders are taking salary reductions, and we have instituted other painful, cost-saving measures. The physician leaders we hired just 12 months ago to oversee a new faculty group structure were thrust into a firestorm. Department chairs, division chiefs, nursing and administrative leaders all are having to make heart-wrenching cost-cutting decisions. Together, we have to make individual reductions in force or retain decisions about people we work with daily. This emotional toll will never truly heal for anyone involved.
There will be little time to recover. We are scrambling to reopen safely, with a planned process. We have a backlog of 12,000 surgeries and 8,000 endoscopy procedures that have been deferred. Eight-hundred children are behind in their well-child medical care, frightened patients are sitting home with critical aortic stenosis, dangerous hypertension, growing cancers, and other urgent medical needs. Private practices are facing the same issues, financial pressures, and emotional toll.
Anna Quindlen once said, “Grief is a whisper in the world, but a clamor within.” Recognize the toll this is taking and don’t be alone with your grief.
John I. Allen, MD, MBA, AGAF
Editor in Chief
The Pediatric Hospital Medicine Core Competencies: 2020 Revision. Authors, Editors, and Reviewers
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
Gaps in Treatment Guidelines for Atopic Dermatitis
Treatment options for atopic dermatitis have evolved significantly in the past several years, but the current guidelines have yet to catch up.
Drs Steven Feldman and Lindsay Strowd, from Wake Forest School of Medicine, discuss gaps in the American Academy of Dermatology treatment guidelines for atopic dermatitis.
The current guidelines have not been updated to include medications approved for atopic dermatitis, including crisaborole, a steroid-sparing ointment used to treat mild to moderate disease in patients 3 months of age and older.
Another drug that has been approved since the 2014 guidelines is the biologic dupilumab, which is a monoclonal antibody that acts on the IL-4 receptor. The agent inhibits the binding of IL-4 receptors to the principal cytokines responsible for mediating the disease. Dupilumab is administered by injection and is approved for patients 6 years and older with moderate to severe disease.
The doctors also discuss therapies for atopic dermatitis currently in development, including topical and oral JAK inhibitors. They agree that the long-term benefit of topical JAK inhibitors may be limited, but that oral JAK inhibitors have the potential to be more effective than dupilumab and more acceptable to patients who do not like injections.
--
Steven R. Feldman, MD, PhD, Professor, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Steven R. Feldman, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AbbVie; Alvotech; Advance Medical; Almirall; Arena; Bristol-Myers Squibb; Caremark; Amgen; Celgene; Galderma Laboratories; Gerson Lehrman Group; Guidepoint Global; Helsinn; Janssen; Kikaku; Leo Pharma; Eli Lilly and Company; Merck; Mylan; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sienna; Sun Pharma; Suncare Research; Xenoport
Serve(d) as a speaker for: AbbVie; Amgen; Celgene; Janssen; Leo Pharma; Eli Lilly and Company; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sun Pharma
Receive(d) grant support from: AbbVie; Amgen; Celgene; Galderma Laboratories; Janssen; Eli Lilly and Company; Novartis; Pfizer; Regeneron; Sanofi
Receive(d) royalties from: Informa; UpToDate; Xlibris
Holds stock in: Causa Technologies; Medical Quality Enhancement Corporation
Serves as founder and chief technology officer for: Causa Technologies
Lindsay C. Strowd, MD, Associate Professor, Vice Chair, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Lindsay C. Strowd, MD, has disclosed no relevant financial relationships.
Treatment options for atopic dermatitis have evolved significantly in the past several years, but the current guidelines have yet to catch up.
Drs Steven Feldman and Lindsay Strowd, from Wake Forest School of Medicine, discuss gaps in the American Academy of Dermatology treatment guidelines for atopic dermatitis.
The current guidelines have not been updated to include medications approved for atopic dermatitis, including crisaborole, a steroid-sparing ointment used to treat mild to moderate disease in patients 3 months of age and older.
Another drug that has been approved since the 2014 guidelines is the biologic dupilumab, which is a monoclonal antibody that acts on the IL-4 receptor. The agent inhibits the binding of IL-4 receptors to the principal cytokines responsible for mediating the disease. Dupilumab is administered by injection and is approved for patients 6 years and older with moderate to severe disease.
The doctors also discuss therapies for atopic dermatitis currently in development, including topical and oral JAK inhibitors. They agree that the long-term benefit of topical JAK inhibitors may be limited, but that oral JAK inhibitors have the potential to be more effective than dupilumab and more acceptable to patients who do not like injections.
--
Steven R. Feldman, MD, PhD, Professor, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Steven R. Feldman, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AbbVie; Alvotech; Advance Medical; Almirall; Arena; Bristol-Myers Squibb; Caremark; Amgen; Celgene; Galderma Laboratories; Gerson Lehrman Group; Guidepoint Global; Helsinn; Janssen; Kikaku; Leo Pharma; Eli Lilly and Company; Merck; Mylan; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sienna; Sun Pharma; Suncare Research; Xenoport
Serve(d) as a speaker for: AbbVie; Amgen; Celgene; Janssen; Leo Pharma; Eli Lilly and Company; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sun Pharma
Receive(d) grant support from: AbbVie; Amgen; Celgene; Galderma Laboratories; Janssen; Eli Lilly and Company; Novartis; Pfizer; Regeneron; Sanofi
Receive(d) royalties from: Informa; UpToDate; Xlibris
Holds stock in: Causa Technologies; Medical Quality Enhancement Corporation
Serves as founder and chief technology officer for: Causa Technologies
Lindsay C. Strowd, MD, Associate Professor, Vice Chair, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Lindsay C. Strowd, MD, has disclosed no relevant financial relationships.
Treatment options for atopic dermatitis have evolved significantly in the past several years, but the current guidelines have yet to catch up.
Drs Steven Feldman and Lindsay Strowd, from Wake Forest School of Medicine, discuss gaps in the American Academy of Dermatology treatment guidelines for atopic dermatitis.
The current guidelines have not been updated to include medications approved for atopic dermatitis, including crisaborole, a steroid-sparing ointment used to treat mild to moderate disease in patients 3 months of age and older.
Another drug that has been approved since the 2014 guidelines is the biologic dupilumab, which is a monoclonal antibody that acts on the IL-4 receptor. The agent inhibits the binding of IL-4 receptors to the principal cytokines responsible for mediating the disease. Dupilumab is administered by injection and is approved for patients 6 years and older with moderate to severe disease.
The doctors also discuss therapies for atopic dermatitis currently in development, including topical and oral JAK inhibitors. They agree that the long-term benefit of topical JAK inhibitors may be limited, but that oral JAK inhibitors have the potential to be more effective than dupilumab and more acceptable to patients who do not like injections.
--
Steven R. Feldman, MD, PhD, Professor, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Steven R. Feldman, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AbbVie; Alvotech; Advance Medical; Almirall; Arena; Bristol-Myers Squibb; Caremark; Amgen; Celgene; Galderma Laboratories; Gerson Lehrman Group; Guidepoint Global; Helsinn; Janssen; Kikaku; Leo Pharma; Eli Lilly and Company; Merck; Mylan; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sienna; Sun Pharma; Suncare Research; Xenoport
Serve(d) as a speaker for: AbbVie; Amgen; Celgene; Janssen; Leo Pharma; Eli Lilly and Company; Novartis; Ortho Dermatology; Pfizer; Regeneron; Sanofi; Sun Pharma
Receive(d) grant support from: AbbVie; Amgen; Celgene; Galderma Laboratories; Janssen; Eli Lilly and Company; Novartis; Pfizer; Regeneron; Sanofi
Receive(d) royalties from: Informa; UpToDate; Xlibris
Holds stock in: Causa Technologies; Medical Quality Enhancement Corporation
Serves as founder and chief technology officer for: Causa Technologies
Lindsay C. Strowd, MD, Associate Professor, Vice Chair, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, North Carolina
Lindsay C. Strowd, MD, has disclosed no relevant financial relationships.
Pyrotinib bests lapatinib in HER2+ metastatic breast cancer
PFS was extended by nearly 6 months among patients who received pyrotinib, a novel pan-HER2 inhibitor, combined with capecitabine. Grade 3 diarrhea occurred in nearly 31% of patients receiving the pyrotinib-capecitabine combination, though none of the patients discontinued treatment due to this adverse event.
Binghe Xu, MD, PhD, of the National Cancer Center/Cancer Hospital at the Chinese Academy of Medical Sciences and Peking Union Medical College in Beijing, presented these results, from the phase 3 PHOEBE trial, as part of the American Society of Clinical Oncology virtual scientific program.
The value of pyrotinib
Although there are already many targeted therapies for HER2-positive metastatic breast cancer, accessibility can be an issue, with drugs such as pertuzumab and trastuzumab emtansine (T-DM1) not available in all regions of the world, according to Dr. Xu.
“Before we initiated this clinical trial, lapatinib plus capecitabine was the only second-line standard of care against HER2-positive metastatic breast cancer in China,” he said.
Based, in part, on results of the PHOEBE trial, the combination of pyrotinib and capecitabine was approved in China as a second-line standard of care for patients with HER2-positive metastatic breast cancer, according to Dr. Xu.
Pyrotinib has now demonstrated “clinical value” in two phase 3 clinical trials, but its value in relation to pertuzumab, T-DM1, tucatinib, trastuzumab deruxtecan, or neratinib is less clear, said Aleix Prat, MD, PhD, of Hospital Clinic of Barcelona.
“Also, in my opinion, the toxicity profile needs attention,” Dr. Prat said in a discussion of the PHOEBE results that was also part of the virtual ASCO meeting.
The 31% incidence of grade 3 diarrhea was “very similar,” he said, to what was seen in PHENIX, another phase 3 trial of pyrotinib plus capecitabine that was presented at the 2019 ASCO annual meeting (J Clin Oncol 37, 2019 suppl; abstr 1001).
“What is the current therapy landscape? In my opinion, today, the first line remains taxane, trastuzumab, and pertuzumab; the second line T-DM1; and the third line tucatinib, trastuzumab, and capecitabine, with other treatment strategies reserved for later lines,” Dr. Prat said.
Study details
PHOEBE included 267 patients with HER2-positive metastatic breast cancer. They had previously received trastuzumab and taxanes, and/or anthracyclines, with up to two prior lines of chemotherapy for metastatic disease.
The patients’ median age was 50 years, 79% had visceral metastases at screening, and about 26% had trastuzumab resistance, Dr. Xu said. Resistance was defined as relapse within 6 months after adjuvant treatment or progression within 3 months of treatment for metastatic disease.
A statistically significant and clinically meaningful improvement was seen in PFS, the primary endpoint of the study, Dr. Xu said.
Median PFS by blinded independent central review was 12.5 months for the pyrotinib-capecitabine combination, compared with 6.8 months for lapatinib-capecitabine (hazard ratio, 0.39; 95% confidence interval, 0.27-0.56; P < .0001).
The PFS benefit was consistently observed across all predefined subgroups, including by trastuzumab resistance.
In trastuzumab-resistant patients, the median PFS was 12.5 months for the pyrotinib combination and 6.9 months for the lapatinib combination (HR, 0.60; 95% CI, 0.29-1.21). In patients without trastuzumab resistance, the median PFS was 12.5 months and 5.6 months, respectively (HR, 0.33; 95% CI, 0.21-0.51).
Although overall survival (OS) data were not yet mature, there was a “strong trend” toward a benefit with pyrotinib, Dr. Xu said. The 12-month OS rate was 91.3% for the pyrotinib combination and 77.4% for lapatinib. The median OS was not reached in either arm at the time of analysis.
Treatment-related adverse events of grade 3 or greater occurred in 57.5% of the pyrotinib arm and 34.1% of the lapatinib arm.
Diarrhea was the most common grade 3 or greater treatment-related adverse event, occurring in 30.6% of patients in the pyrotinib arm and 8.3% of those in the lapatinib arm. No grade 4 or 5 diarrhea was seen.
Overall, diarrhea occurred in 94.8% of patients in the pyrotinib arm and 62.1% of those in the lapatinib arm. However, pyrotinib-associated diarrhea was generally of low severity, occurred early, had a short duration, was reversible, and did not lead to treatment termination, according to Dr. Xu.
This study was funded by Jiangsu Hengrui Medicine Co. Ltd. Dr. Xu reported additional disclosures related to AstraZeneca, Eisai, Pfizer, and Roche. Dr. Prat disclosed relationships with Amgen, Daiichi Sankyo, Lilly, MSD Oncology, and other companies.
SOURCE: Xu B et al. ASCO 2020, Abstract 1003
PFS was extended by nearly 6 months among patients who received pyrotinib, a novel pan-HER2 inhibitor, combined with capecitabine. Grade 3 diarrhea occurred in nearly 31% of patients receiving the pyrotinib-capecitabine combination, though none of the patients discontinued treatment due to this adverse event.
Binghe Xu, MD, PhD, of the National Cancer Center/Cancer Hospital at the Chinese Academy of Medical Sciences and Peking Union Medical College in Beijing, presented these results, from the phase 3 PHOEBE trial, as part of the American Society of Clinical Oncology virtual scientific program.
The value of pyrotinib
Although there are already many targeted therapies for HER2-positive metastatic breast cancer, accessibility can be an issue, with drugs such as pertuzumab and trastuzumab emtansine (T-DM1) not available in all regions of the world, according to Dr. Xu.
“Before we initiated this clinical trial, lapatinib plus capecitabine was the only second-line standard of care against HER2-positive metastatic breast cancer in China,” he said.
Based, in part, on results of the PHOEBE trial, the combination of pyrotinib and capecitabine was approved in China as a second-line standard of care for patients with HER2-positive metastatic breast cancer, according to Dr. Xu.
Pyrotinib has now demonstrated “clinical value” in two phase 3 clinical trials, but its value in relation to pertuzumab, T-DM1, tucatinib, trastuzumab deruxtecan, or neratinib is less clear, said Aleix Prat, MD, PhD, of Hospital Clinic of Barcelona.
“Also, in my opinion, the toxicity profile needs attention,” Dr. Prat said in a discussion of the PHOEBE results that was also part of the virtual ASCO meeting.
The 31% incidence of grade 3 diarrhea was “very similar,” he said, to what was seen in PHENIX, another phase 3 trial of pyrotinib plus capecitabine that was presented at the 2019 ASCO annual meeting (J Clin Oncol 37, 2019 suppl; abstr 1001).
“What is the current therapy landscape? In my opinion, today, the first line remains taxane, trastuzumab, and pertuzumab; the second line T-DM1; and the third line tucatinib, trastuzumab, and capecitabine, with other treatment strategies reserved for later lines,” Dr. Prat said.
Study details
PHOEBE included 267 patients with HER2-positive metastatic breast cancer. They had previously received trastuzumab and taxanes, and/or anthracyclines, with up to two prior lines of chemotherapy for metastatic disease.
The patients’ median age was 50 years, 79% had visceral metastases at screening, and about 26% had trastuzumab resistance, Dr. Xu said. Resistance was defined as relapse within 6 months after adjuvant treatment or progression within 3 months of treatment for metastatic disease.
A statistically significant and clinically meaningful improvement was seen in PFS, the primary endpoint of the study, Dr. Xu said.
Median PFS by blinded independent central review was 12.5 months for the pyrotinib-capecitabine combination, compared with 6.8 months for lapatinib-capecitabine (hazard ratio, 0.39; 95% confidence interval, 0.27-0.56; P < .0001).
The PFS benefit was consistently observed across all predefined subgroups, including by trastuzumab resistance.
In trastuzumab-resistant patients, the median PFS was 12.5 months for the pyrotinib combination and 6.9 months for the lapatinib combination (HR, 0.60; 95% CI, 0.29-1.21). In patients without trastuzumab resistance, the median PFS was 12.5 months and 5.6 months, respectively (HR, 0.33; 95% CI, 0.21-0.51).
Although overall survival (OS) data were not yet mature, there was a “strong trend” toward a benefit with pyrotinib, Dr. Xu said. The 12-month OS rate was 91.3% for the pyrotinib combination and 77.4% for lapatinib. The median OS was not reached in either arm at the time of analysis.
Treatment-related adverse events of grade 3 or greater occurred in 57.5% of the pyrotinib arm and 34.1% of the lapatinib arm.
Diarrhea was the most common grade 3 or greater treatment-related adverse event, occurring in 30.6% of patients in the pyrotinib arm and 8.3% of those in the lapatinib arm. No grade 4 or 5 diarrhea was seen.
Overall, diarrhea occurred in 94.8% of patients in the pyrotinib arm and 62.1% of those in the lapatinib arm. However, pyrotinib-associated diarrhea was generally of low severity, occurred early, had a short duration, was reversible, and did not lead to treatment termination, according to Dr. Xu.
This study was funded by Jiangsu Hengrui Medicine Co. Ltd. Dr. Xu reported additional disclosures related to AstraZeneca, Eisai, Pfizer, and Roche. Dr. Prat disclosed relationships with Amgen, Daiichi Sankyo, Lilly, MSD Oncology, and other companies.
SOURCE: Xu B et al. ASCO 2020, Abstract 1003
PFS was extended by nearly 6 months among patients who received pyrotinib, a novel pan-HER2 inhibitor, combined with capecitabine. Grade 3 diarrhea occurred in nearly 31% of patients receiving the pyrotinib-capecitabine combination, though none of the patients discontinued treatment due to this adverse event.
Binghe Xu, MD, PhD, of the National Cancer Center/Cancer Hospital at the Chinese Academy of Medical Sciences and Peking Union Medical College in Beijing, presented these results, from the phase 3 PHOEBE trial, as part of the American Society of Clinical Oncology virtual scientific program.
The value of pyrotinib
Although there are already many targeted therapies for HER2-positive metastatic breast cancer, accessibility can be an issue, with drugs such as pertuzumab and trastuzumab emtansine (T-DM1) not available in all regions of the world, according to Dr. Xu.
“Before we initiated this clinical trial, lapatinib plus capecitabine was the only second-line standard of care against HER2-positive metastatic breast cancer in China,” he said.
Based, in part, on results of the PHOEBE trial, the combination of pyrotinib and capecitabine was approved in China as a second-line standard of care for patients with HER2-positive metastatic breast cancer, according to Dr. Xu.
Pyrotinib has now demonstrated “clinical value” in two phase 3 clinical trials, but its value in relation to pertuzumab, T-DM1, tucatinib, trastuzumab deruxtecan, or neratinib is less clear, said Aleix Prat, MD, PhD, of Hospital Clinic of Barcelona.
“Also, in my opinion, the toxicity profile needs attention,” Dr. Prat said in a discussion of the PHOEBE results that was also part of the virtual ASCO meeting.
The 31% incidence of grade 3 diarrhea was “very similar,” he said, to what was seen in PHENIX, another phase 3 trial of pyrotinib plus capecitabine that was presented at the 2019 ASCO annual meeting (J Clin Oncol 37, 2019 suppl; abstr 1001).
“What is the current therapy landscape? In my opinion, today, the first line remains taxane, trastuzumab, and pertuzumab; the second line T-DM1; and the third line tucatinib, trastuzumab, and capecitabine, with other treatment strategies reserved for later lines,” Dr. Prat said.
Study details
PHOEBE included 267 patients with HER2-positive metastatic breast cancer. They had previously received trastuzumab and taxanes, and/or anthracyclines, with up to two prior lines of chemotherapy for metastatic disease.
The patients’ median age was 50 years, 79% had visceral metastases at screening, and about 26% had trastuzumab resistance, Dr. Xu said. Resistance was defined as relapse within 6 months after adjuvant treatment or progression within 3 months of treatment for metastatic disease.
A statistically significant and clinically meaningful improvement was seen in PFS, the primary endpoint of the study, Dr. Xu said.
Median PFS by blinded independent central review was 12.5 months for the pyrotinib-capecitabine combination, compared with 6.8 months for lapatinib-capecitabine (hazard ratio, 0.39; 95% confidence interval, 0.27-0.56; P < .0001).
The PFS benefit was consistently observed across all predefined subgroups, including by trastuzumab resistance.
In trastuzumab-resistant patients, the median PFS was 12.5 months for the pyrotinib combination and 6.9 months for the lapatinib combination (HR, 0.60; 95% CI, 0.29-1.21). In patients without trastuzumab resistance, the median PFS was 12.5 months and 5.6 months, respectively (HR, 0.33; 95% CI, 0.21-0.51).
Although overall survival (OS) data were not yet mature, there was a “strong trend” toward a benefit with pyrotinib, Dr. Xu said. The 12-month OS rate was 91.3% for the pyrotinib combination and 77.4% for lapatinib. The median OS was not reached in either arm at the time of analysis.
Treatment-related adverse events of grade 3 or greater occurred in 57.5% of the pyrotinib arm and 34.1% of the lapatinib arm.
Diarrhea was the most common grade 3 or greater treatment-related adverse event, occurring in 30.6% of patients in the pyrotinib arm and 8.3% of those in the lapatinib arm. No grade 4 or 5 diarrhea was seen.
Overall, diarrhea occurred in 94.8% of patients in the pyrotinib arm and 62.1% of those in the lapatinib arm. However, pyrotinib-associated diarrhea was generally of low severity, occurred early, had a short duration, was reversible, and did not lead to treatment termination, according to Dr. Xu.
This study was funded by Jiangsu Hengrui Medicine Co. Ltd. Dr. Xu reported additional disclosures related to AstraZeneca, Eisai, Pfizer, and Roche. Dr. Prat disclosed relationships with Amgen, Daiichi Sankyo, Lilly, MSD Oncology, and other companies.
SOURCE: Xu B et al. ASCO 2020, Abstract 1003
FROM ASCO 2020
New guidance to optimize antipsychotic treatment
A new consensus statement recommends monitoring antipsychotic blood levels, also known as therapeutic drug monitoring (TDM), to inform treatment decisions and optimize safety and efficacy.
The statement, jointly authored by experts from the American Society of Clinical Psychopharmacology (ASCP) and the Germany-based Therapeutic Drug Monitoring Task Force of the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie, recommends antipsychotic TDM, particularly for specific patient groups and for patients with suspected nonadherence.
“This [TDM] is a valuable and reliable instrument for personalizing treatment, which is an increasing focus today – individualizing and tailoring pharmacotherapy,” lead author Georgios Schoretsanitis, MD, PhD, department of psychiatry, The Zucker Hillside Hospital, Northwell Health, Glen Oaks, and Center for Psychiatric Neuroscience, Feinstein Institute for Medical Research, Manhasset, New York, said in an interview.
“I am particularly satisfied to say that this paper adds much knowledge and is a holistic approach, focusing not only on theoretical knowledge but also aiming to make the life of clinicians easier, providing more of an algorithm and decision-making instrument for clinical use in everyday clinical scenarios and problems related to antipsychotic treatment,” he added.
The study was published online May 19 in the Journal of Clinical Psychiatry.
Problem-solving tool
“The therapeutic reference range for antipsychotic levels in blood consists of a lower limit, below which therapeutic response is relatively unlikely, and an upper limit, above which ADRs [adverse drug reactions] … are more likely to occur,” the authors wrote.
TDM can determine whether a patient has a subtherapeutic antipsychotic blood concentration and may explain a lack of response or a supra-therapeutic concentration, which could be associated with adverse drug reactions.
“It is important for clinicians to realize that this type of monitoring is not equally indicated for all antipsychotics and not planned as a way of providing insight if there are no questions. In other words, it is a problem-solving tool for a problem, a complicated situation, or a challenging scenario you’re trying to solve,” Dr. Schoretsanitis said.
The authors divided their recommendations regarding routine TDM for antipsychotics into four categories, based on level of evidence:
Strongly recommended (Level 1)
- Clozapine
- Fluphenazine
- Haloperidol
- Olanzapine
- Perazine
- Perphenazine
Recommended (Level 2)
- Aripiprazole
- Chlorpromazine
- Flupentixol
- Paliperidone
- Quetiapine
- Risperidone
- Sertindole
- Ziprasidone
Useful (Level 3)
- Brexpiprazole
- Cariprazine
- Chlorprothixene
- Iloperidone
- Loxapine
- Lurasidone
- Melperone
- Pimozide
Potentially useful (Level 4)
- Asenapine
Proven benefits
“We tried to narrow down specific situations and scenarios in which TDM can be useful and, in fact, has proven benefits,” said Dr. Schoretsanitis.
Patients who have no clinical response, even within established dose ranges, who have a recurrence or relapse during maintenance treatment, or who have ADRs are candidates for TDM.
Patients receiving polypharmacy can benefit from TDM because some coprescribed medications can raise or lower antipsychotic blood levels via overlapping metabolic pathways.
Additional populations requiring TDM are elderly patients, pregnant/lactating women, patients with medical comorbidities such as renal or hepatic disease, children/adolescents, patients with intellectual disabilities, and forensic or court-mandated patients.
Dr. Schoretsanitis noted that switching between formulations – for example from an oral to a long-acting injectable antipsychotic (LAI) – can “easily be guided by regular use of TDM,” as can switching from a brand name drug to a generic.
Patients with acute inflammatory conditions, such as COVID-19, “are good candidates for TDM, even with drugs that were previously well-tolerated, because inflammation affects the way the body metabolizes drugs, leaving patients at high risk for developing toxicity,” he added.
“The most common scenario for using TDM in clinical practice is to measure adherence to antipsychotics, since TDM is one of the most reliable ways to assess adherence and thereby prevent relapse or recurrence of the disease,” said Dr. Schoretsanitis.
Long overdue
Sheldon Preskorn, MD, professor of psychiatry, University of Kansas, Wichita, and chief science officer for KUSM-W Clinical Trials Unit, said in an interview that drawing blood 24 hours after taking the drug can help determine the patient’s clearance of the drug.
“If the level is too low, either the patient is not taking the drug at all, or is taking too little, or is a rapid metabolizer, so the dose may have to be adjusted,” said Dr. Preskorn, who was not involved in developing the consensus statement.
This is also an opportunity to initiate a conversation with patients regarding adherence, explaining that a low blood level will not have a therapeutic effect, discussing whether the patient has been taking the medication as prescribed, and addressing reasons for nonadherence, said Dr. Preskorn.
“We want to make it clear that clinicians should treat the patient, not the blood level,” said Dr. Schoretsanitis.
“If a person is tolerating and responding to medications well, but we measure and see something unexpected, such as low levels, this doesn’t mean we need to adjust the dose merely because the levels are low,” he added.
“Timing is very important” when measuring blood levels. For example, if a patient’s blood is usually tested in the morning but then is tested in the afternoon, he or she may exhibit a lower blood level, which may be reflective of the timing of the test rather than drug response.
“,” said Dr. Preskorn.
Also commenting on the consensus statement, Jonathan Meyer, MD, clinical professor of psychiatry, University of California, San Diego, said it brings attention to some of the key issues associated with antipsychotic plasma monitoring and shows TDM is a valuable decision-making tool.
Dr. Meyer, who was not involved in developing the document, pointed out that it may be difficult to obtain levels on newer antipsychotics, which require specialized labs that are not widely available and sometimes take up to 2 weeks to get results.
In such cases, physicians will have to rely on their best clinical judgment to manage an inadequate response until TDM results are available.
No commercial organizations had any role in funding the statement. Dr. Schoretsanitis has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Meyer reports having received speaking or advising fees in the prior 12 months from Acadia Pharmaceuticals, Alkermes, Allergan (now AbbVie), Intra-Cellular Therapies, Janssen Pharmaceutica, Neurocrine, Otsuka America Inc., Sunovion Pharmaceuticals, and Teva Pharmaceutical Industries Ltd. Dr. Preskorn reports having been an investigator and/or a consultant to more than 140 pharmaceutical, biotechnology, diagnostic, and device companies and to the Food and Drug Administration and other federal agencies.
A version of this article originally appeared on Medscape.com.
A new consensus statement recommends monitoring antipsychotic blood levels, also known as therapeutic drug monitoring (TDM), to inform treatment decisions and optimize safety and efficacy.
The statement, jointly authored by experts from the American Society of Clinical Psychopharmacology (ASCP) and the Germany-based Therapeutic Drug Monitoring Task Force of the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie, recommends antipsychotic TDM, particularly for specific patient groups and for patients with suspected nonadherence.
“This [TDM] is a valuable and reliable instrument for personalizing treatment, which is an increasing focus today – individualizing and tailoring pharmacotherapy,” lead author Georgios Schoretsanitis, MD, PhD, department of psychiatry, The Zucker Hillside Hospital, Northwell Health, Glen Oaks, and Center for Psychiatric Neuroscience, Feinstein Institute for Medical Research, Manhasset, New York, said in an interview.
“I am particularly satisfied to say that this paper adds much knowledge and is a holistic approach, focusing not only on theoretical knowledge but also aiming to make the life of clinicians easier, providing more of an algorithm and decision-making instrument for clinical use in everyday clinical scenarios and problems related to antipsychotic treatment,” he added.
The study was published online May 19 in the Journal of Clinical Psychiatry.
Problem-solving tool
“The therapeutic reference range for antipsychotic levels in blood consists of a lower limit, below which therapeutic response is relatively unlikely, and an upper limit, above which ADRs [adverse drug reactions] … are more likely to occur,” the authors wrote.
TDM can determine whether a patient has a subtherapeutic antipsychotic blood concentration and may explain a lack of response or a supra-therapeutic concentration, which could be associated with adverse drug reactions.
“It is important for clinicians to realize that this type of monitoring is not equally indicated for all antipsychotics and not planned as a way of providing insight if there are no questions. In other words, it is a problem-solving tool for a problem, a complicated situation, or a challenging scenario you’re trying to solve,” Dr. Schoretsanitis said.
The authors divided their recommendations regarding routine TDM for antipsychotics into four categories, based on level of evidence:
Strongly recommended (Level 1)
- Clozapine
- Fluphenazine
- Haloperidol
- Olanzapine
- Perazine
- Perphenazine
Recommended (Level 2)
- Aripiprazole
- Chlorpromazine
- Flupentixol
- Paliperidone
- Quetiapine
- Risperidone
- Sertindole
- Ziprasidone
Useful (Level 3)
- Brexpiprazole
- Cariprazine
- Chlorprothixene
- Iloperidone
- Loxapine
- Lurasidone
- Melperone
- Pimozide
Potentially useful (Level 4)
- Asenapine
Proven benefits
“We tried to narrow down specific situations and scenarios in which TDM can be useful and, in fact, has proven benefits,” said Dr. Schoretsanitis.
Patients who have no clinical response, even within established dose ranges, who have a recurrence or relapse during maintenance treatment, or who have ADRs are candidates for TDM.
Patients receiving polypharmacy can benefit from TDM because some coprescribed medications can raise or lower antipsychotic blood levels via overlapping metabolic pathways.
Additional populations requiring TDM are elderly patients, pregnant/lactating women, patients with medical comorbidities such as renal or hepatic disease, children/adolescents, patients with intellectual disabilities, and forensic or court-mandated patients.
Dr. Schoretsanitis noted that switching between formulations – for example from an oral to a long-acting injectable antipsychotic (LAI) – can “easily be guided by regular use of TDM,” as can switching from a brand name drug to a generic.
Patients with acute inflammatory conditions, such as COVID-19, “are good candidates for TDM, even with drugs that were previously well-tolerated, because inflammation affects the way the body metabolizes drugs, leaving patients at high risk for developing toxicity,” he added.
“The most common scenario for using TDM in clinical practice is to measure adherence to antipsychotics, since TDM is one of the most reliable ways to assess adherence and thereby prevent relapse or recurrence of the disease,” said Dr. Schoretsanitis.
Long overdue
Sheldon Preskorn, MD, professor of psychiatry, University of Kansas, Wichita, and chief science officer for KUSM-W Clinical Trials Unit, said in an interview that drawing blood 24 hours after taking the drug can help determine the patient’s clearance of the drug.
“If the level is too low, either the patient is not taking the drug at all, or is taking too little, or is a rapid metabolizer, so the dose may have to be adjusted,” said Dr. Preskorn, who was not involved in developing the consensus statement.
This is also an opportunity to initiate a conversation with patients regarding adherence, explaining that a low blood level will not have a therapeutic effect, discussing whether the patient has been taking the medication as prescribed, and addressing reasons for nonadherence, said Dr. Preskorn.
“We want to make it clear that clinicians should treat the patient, not the blood level,” said Dr. Schoretsanitis.
“If a person is tolerating and responding to medications well, but we measure and see something unexpected, such as low levels, this doesn’t mean we need to adjust the dose merely because the levels are low,” he added.
“Timing is very important” when measuring blood levels. For example, if a patient’s blood is usually tested in the morning but then is tested in the afternoon, he or she may exhibit a lower blood level, which may be reflective of the timing of the test rather than drug response.
“,” said Dr. Preskorn.
Also commenting on the consensus statement, Jonathan Meyer, MD, clinical professor of psychiatry, University of California, San Diego, said it brings attention to some of the key issues associated with antipsychotic plasma monitoring and shows TDM is a valuable decision-making tool.
Dr. Meyer, who was not involved in developing the document, pointed out that it may be difficult to obtain levels on newer antipsychotics, which require specialized labs that are not widely available and sometimes take up to 2 weeks to get results.
In such cases, physicians will have to rely on their best clinical judgment to manage an inadequate response until TDM results are available.
No commercial organizations had any role in funding the statement. Dr. Schoretsanitis has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Meyer reports having received speaking or advising fees in the prior 12 months from Acadia Pharmaceuticals, Alkermes, Allergan (now AbbVie), Intra-Cellular Therapies, Janssen Pharmaceutica, Neurocrine, Otsuka America Inc., Sunovion Pharmaceuticals, and Teva Pharmaceutical Industries Ltd. Dr. Preskorn reports having been an investigator and/or a consultant to more than 140 pharmaceutical, biotechnology, diagnostic, and device companies and to the Food and Drug Administration and other federal agencies.
A version of this article originally appeared on Medscape.com.
A new consensus statement recommends monitoring antipsychotic blood levels, also known as therapeutic drug monitoring (TDM), to inform treatment decisions and optimize safety and efficacy.
The statement, jointly authored by experts from the American Society of Clinical Psychopharmacology (ASCP) and the Germany-based Therapeutic Drug Monitoring Task Force of the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie, recommends antipsychotic TDM, particularly for specific patient groups and for patients with suspected nonadherence.
“This [TDM] is a valuable and reliable instrument for personalizing treatment, which is an increasing focus today – individualizing and tailoring pharmacotherapy,” lead author Georgios Schoretsanitis, MD, PhD, department of psychiatry, The Zucker Hillside Hospital, Northwell Health, Glen Oaks, and Center for Psychiatric Neuroscience, Feinstein Institute for Medical Research, Manhasset, New York, said in an interview.
“I am particularly satisfied to say that this paper adds much knowledge and is a holistic approach, focusing not only on theoretical knowledge but also aiming to make the life of clinicians easier, providing more of an algorithm and decision-making instrument for clinical use in everyday clinical scenarios and problems related to antipsychotic treatment,” he added.
The study was published online May 19 in the Journal of Clinical Psychiatry.
Problem-solving tool
“The therapeutic reference range for antipsychotic levels in blood consists of a lower limit, below which therapeutic response is relatively unlikely, and an upper limit, above which ADRs [adverse drug reactions] … are more likely to occur,” the authors wrote.
TDM can determine whether a patient has a subtherapeutic antipsychotic blood concentration and may explain a lack of response or a supra-therapeutic concentration, which could be associated with adverse drug reactions.
“It is important for clinicians to realize that this type of monitoring is not equally indicated for all antipsychotics and not planned as a way of providing insight if there are no questions. In other words, it is a problem-solving tool for a problem, a complicated situation, or a challenging scenario you’re trying to solve,” Dr. Schoretsanitis said.
The authors divided their recommendations regarding routine TDM for antipsychotics into four categories, based on level of evidence:
Strongly recommended (Level 1)
- Clozapine
- Fluphenazine
- Haloperidol
- Olanzapine
- Perazine
- Perphenazine
Recommended (Level 2)
- Aripiprazole
- Chlorpromazine
- Flupentixol
- Paliperidone
- Quetiapine
- Risperidone
- Sertindole
- Ziprasidone
Useful (Level 3)
- Brexpiprazole
- Cariprazine
- Chlorprothixene
- Iloperidone
- Loxapine
- Lurasidone
- Melperone
- Pimozide
Potentially useful (Level 4)
- Asenapine
Proven benefits
“We tried to narrow down specific situations and scenarios in which TDM can be useful and, in fact, has proven benefits,” said Dr. Schoretsanitis.
Patients who have no clinical response, even within established dose ranges, who have a recurrence or relapse during maintenance treatment, or who have ADRs are candidates for TDM.
Patients receiving polypharmacy can benefit from TDM because some coprescribed medications can raise or lower antipsychotic blood levels via overlapping metabolic pathways.
Additional populations requiring TDM are elderly patients, pregnant/lactating women, patients with medical comorbidities such as renal or hepatic disease, children/adolescents, patients with intellectual disabilities, and forensic or court-mandated patients.
Dr. Schoretsanitis noted that switching between formulations – for example from an oral to a long-acting injectable antipsychotic (LAI) – can “easily be guided by regular use of TDM,” as can switching from a brand name drug to a generic.
Patients with acute inflammatory conditions, such as COVID-19, “are good candidates for TDM, even with drugs that were previously well-tolerated, because inflammation affects the way the body metabolizes drugs, leaving patients at high risk for developing toxicity,” he added.
“The most common scenario for using TDM in clinical practice is to measure adherence to antipsychotics, since TDM is one of the most reliable ways to assess adherence and thereby prevent relapse or recurrence of the disease,” said Dr. Schoretsanitis.
Long overdue
Sheldon Preskorn, MD, professor of psychiatry, University of Kansas, Wichita, and chief science officer for KUSM-W Clinical Trials Unit, said in an interview that drawing blood 24 hours after taking the drug can help determine the patient’s clearance of the drug.
“If the level is too low, either the patient is not taking the drug at all, or is taking too little, or is a rapid metabolizer, so the dose may have to be adjusted,” said Dr. Preskorn, who was not involved in developing the consensus statement.
This is also an opportunity to initiate a conversation with patients regarding adherence, explaining that a low blood level will not have a therapeutic effect, discussing whether the patient has been taking the medication as prescribed, and addressing reasons for nonadherence, said Dr. Preskorn.
“We want to make it clear that clinicians should treat the patient, not the blood level,” said Dr. Schoretsanitis.
“If a person is tolerating and responding to medications well, but we measure and see something unexpected, such as low levels, this doesn’t mean we need to adjust the dose merely because the levels are low,” he added.
“Timing is very important” when measuring blood levels. For example, if a patient’s blood is usually tested in the morning but then is tested in the afternoon, he or she may exhibit a lower blood level, which may be reflective of the timing of the test rather than drug response.
“,” said Dr. Preskorn.
Also commenting on the consensus statement, Jonathan Meyer, MD, clinical professor of psychiatry, University of California, San Diego, said it brings attention to some of the key issues associated with antipsychotic plasma monitoring and shows TDM is a valuable decision-making tool.
Dr. Meyer, who was not involved in developing the document, pointed out that it may be difficult to obtain levels on newer antipsychotics, which require specialized labs that are not widely available and sometimes take up to 2 weeks to get results.
In such cases, physicians will have to rely on their best clinical judgment to manage an inadequate response until TDM results are available.
No commercial organizations had any role in funding the statement. Dr. Schoretsanitis has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Meyer reports having received speaking or advising fees in the prior 12 months from Acadia Pharmaceuticals, Alkermes, Allergan (now AbbVie), Intra-Cellular Therapies, Janssen Pharmaceutica, Neurocrine, Otsuka America Inc., Sunovion Pharmaceuticals, and Teva Pharmaceutical Industries Ltd. Dr. Preskorn reports having been an investigator and/or a consultant to more than 140 pharmaceutical, biotechnology, diagnostic, and device companies and to the Food and Drug Administration and other federal agencies.
A version of this article originally appeared on Medscape.com.
Expanding the role of PARP inhibitors in breast cancer
For patients with BRCA-like triple-negative breast cancer (TNBC), adding veliparib to cisplatin chemotherapy may extend survival, based on results from the phase 3 SWOG S1416 trial.
All patients with BRCA-like TNBC had a significant improvement in progression-free survival (PFS) when they received veliparib plus cisplatin. Previously untreated patients with BRCA-like TNBC had a significant improvement in overall survival (OS) as well.
The results are a “very positive step towards expanding the role of PARP inhibitors beyond germline BRCA in breast cancer,” reported lead author Priyanka Sharma, MD, of the University of Kansas Medical Center in Kansas City, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
According to Dr. Sharma, PARP inhibitors have demonstrated efficacy for certain patients with BRCA wild-type ovarian cancer, such as those with homologous recombination deficiency, which also occurs in approximately half of patients with BRCA wild-type TNBC. In TNBC, homologous recombination deficiency and other aberrations lead to a BRCA-like disease phenotype, which may respond to PARP inhibitors.
Dr. Sharma noted that previous attempts to use PARP inhibitors for BRCA wild-type TNBC have revealed obstacles, such as the inefficacy of PARP inhibitor monotherapy and dose-limiting myelosuppression when PARP inhibitors were added to chemotherapy. The issue of bone marrow toxicity may be mitigated by veliparib, which has minimal PARP-trapping activity, she explained.
“A phase 1 trial has demonstrated that adequate doses of cisplatin can be delivered safely in combination with the near-maximal single-agent dose of veliparib in patients with metastatic TNBC,” Dr. Sharma said.
She and her colleagues put this finding to the test in a phase 3 trial that enrolled 335 patients with metastatic and/or loco-regionally recurrent TNBC or BRCA-associated HER2-negative breast cancer. Patients could be previously untreated or have received one prior cytotoxic chemotherapy for metastatic disease.
Of the patients enrolled, 321 met eligibility criteria, 294 had germline BRCA testing, and 209 had BRCA-like assessment.
Patients were divided into the following groups: germline BRCA-associated disease (n = 37), BRCA-like disease (n = 99), non-BRCA-like disease (n = 110), and unclassified (n = 75).
In each group, patients were randomized in a 1:1 ratio to receive cisplatin (75 mg/m2 on day 1) plus veliparib (300 mg twice daily on days 1-14) every 3 weeks, or cisplatin with placebo. The primary endpoint was PFS.
Results
Among patients with BRCA-like disease, there was a significant improvement in PFS and a trend toward improved OS when veliparib was added to cisplatin. The median PFS was 5.9 months with veliparib and 4.2 months with placebo (P = .006). The median OS was 14.0 months and 12.1 months, respectively (P = .067).
Among patients with previously untreated BRCA-like disease, there were significant improvements in both PFS and OS.
The median PFS in this group was 6.1 months with veliparib and 4.2 months with placebo (P = .008). The 12-month PFS rates were 23% and 3%, respectively.
The median OS in this group was 17.8 months with veliparib and 10.3 months with placebo (P = .048). The 24-month OS rates were 43% and 20%, respectively.
There were no survival benefits with veliparib among patients with unclassified disease, non-BRCA-like disease, or BRCA-associated disease.
Dr. Sharma noted that the lack of significant improvement in the BRCA-associated group was likely due to the small sample size. “FDA approval of PARP inhibitors for treatment of germline BRCA-associated metastatic breast cancer during the course of this trial impacted accrual to this group,” she said.
Veliparib was associated with a higher rate of grade 3-4 hematologic toxicities, including neutropenia (46% vs. 19%), leukopenia (27% vs. 7%), anemia (23% vs. 7%), and thrombocytopenia (19% vs. 3%).
Dr. Sharma said results from this trial should prompt further research. “The combination of veliparib plus cisplatin warrants further evaluation in larger randomized trials for patients with BRCA-like phenotype TNBC,” she said.
Invited discussant Catherine M. Kelly, MB BCh, of Mater Misericordiae University Hospital in Dublin, called the trial “an ambitious study” that has created a “valuable tissue bank” for future translational research. She agreed that more work is necessary.
“Further research is needed to identify the optimal homologous recombination deficiency biomarkers critical in the early treatment-naive and in the advanced treatment-exposed disease settings,” Dr. Kelly said.
SWOG S1416 was funded by the National Institutes of Health and AbbVie. Dr. Sharma disclosed relationships with AstraZeneca, Merck, Novartis, and other companies. Dr. Kelly reported affiliations with Pfizer, Novartis, Roche, and MSD Oncology.
SOURCE: Sharma et al. ASCO 2020, Abstract 1001.
For patients with BRCA-like triple-negative breast cancer (TNBC), adding veliparib to cisplatin chemotherapy may extend survival, based on results from the phase 3 SWOG S1416 trial.
All patients with BRCA-like TNBC had a significant improvement in progression-free survival (PFS) when they received veliparib plus cisplatin. Previously untreated patients with BRCA-like TNBC had a significant improvement in overall survival (OS) as well.
The results are a “very positive step towards expanding the role of PARP inhibitors beyond germline BRCA in breast cancer,” reported lead author Priyanka Sharma, MD, of the University of Kansas Medical Center in Kansas City, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
According to Dr. Sharma, PARP inhibitors have demonstrated efficacy for certain patients with BRCA wild-type ovarian cancer, such as those with homologous recombination deficiency, which also occurs in approximately half of patients with BRCA wild-type TNBC. In TNBC, homologous recombination deficiency and other aberrations lead to a BRCA-like disease phenotype, which may respond to PARP inhibitors.
Dr. Sharma noted that previous attempts to use PARP inhibitors for BRCA wild-type TNBC have revealed obstacles, such as the inefficacy of PARP inhibitor monotherapy and dose-limiting myelosuppression when PARP inhibitors were added to chemotherapy. The issue of bone marrow toxicity may be mitigated by veliparib, which has minimal PARP-trapping activity, she explained.
“A phase 1 trial has demonstrated that adequate doses of cisplatin can be delivered safely in combination with the near-maximal single-agent dose of veliparib in patients with metastatic TNBC,” Dr. Sharma said.
She and her colleagues put this finding to the test in a phase 3 trial that enrolled 335 patients with metastatic and/or loco-regionally recurrent TNBC or BRCA-associated HER2-negative breast cancer. Patients could be previously untreated or have received one prior cytotoxic chemotherapy for metastatic disease.
Of the patients enrolled, 321 met eligibility criteria, 294 had germline BRCA testing, and 209 had BRCA-like assessment.
Patients were divided into the following groups: germline BRCA-associated disease (n = 37), BRCA-like disease (n = 99), non-BRCA-like disease (n = 110), and unclassified (n = 75).
In each group, patients were randomized in a 1:1 ratio to receive cisplatin (75 mg/m2 on day 1) plus veliparib (300 mg twice daily on days 1-14) every 3 weeks, or cisplatin with placebo. The primary endpoint was PFS.
Results
Among patients with BRCA-like disease, there was a significant improvement in PFS and a trend toward improved OS when veliparib was added to cisplatin. The median PFS was 5.9 months with veliparib and 4.2 months with placebo (P = .006). The median OS was 14.0 months and 12.1 months, respectively (P = .067).
Among patients with previously untreated BRCA-like disease, there were significant improvements in both PFS and OS.
The median PFS in this group was 6.1 months with veliparib and 4.2 months with placebo (P = .008). The 12-month PFS rates were 23% and 3%, respectively.
The median OS in this group was 17.8 months with veliparib and 10.3 months with placebo (P = .048). The 24-month OS rates were 43% and 20%, respectively.
There were no survival benefits with veliparib among patients with unclassified disease, non-BRCA-like disease, or BRCA-associated disease.
Dr. Sharma noted that the lack of significant improvement in the BRCA-associated group was likely due to the small sample size. “FDA approval of PARP inhibitors for treatment of germline BRCA-associated metastatic breast cancer during the course of this trial impacted accrual to this group,” she said.
Veliparib was associated with a higher rate of grade 3-4 hematologic toxicities, including neutropenia (46% vs. 19%), leukopenia (27% vs. 7%), anemia (23% vs. 7%), and thrombocytopenia (19% vs. 3%).
Dr. Sharma said results from this trial should prompt further research. “The combination of veliparib plus cisplatin warrants further evaluation in larger randomized trials for patients with BRCA-like phenotype TNBC,” she said.
Invited discussant Catherine M. Kelly, MB BCh, of Mater Misericordiae University Hospital in Dublin, called the trial “an ambitious study” that has created a “valuable tissue bank” for future translational research. She agreed that more work is necessary.
“Further research is needed to identify the optimal homologous recombination deficiency biomarkers critical in the early treatment-naive and in the advanced treatment-exposed disease settings,” Dr. Kelly said.
SWOG S1416 was funded by the National Institutes of Health and AbbVie. Dr. Sharma disclosed relationships with AstraZeneca, Merck, Novartis, and other companies. Dr. Kelly reported affiliations with Pfizer, Novartis, Roche, and MSD Oncology.
SOURCE: Sharma et al. ASCO 2020, Abstract 1001.
For patients with BRCA-like triple-negative breast cancer (TNBC), adding veliparib to cisplatin chemotherapy may extend survival, based on results from the phase 3 SWOG S1416 trial.
All patients with BRCA-like TNBC had a significant improvement in progression-free survival (PFS) when they received veliparib plus cisplatin. Previously untreated patients with BRCA-like TNBC had a significant improvement in overall survival (OS) as well.
The results are a “very positive step towards expanding the role of PARP inhibitors beyond germline BRCA in breast cancer,” reported lead author Priyanka Sharma, MD, of the University of Kansas Medical Center in Kansas City, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
According to Dr. Sharma, PARP inhibitors have demonstrated efficacy for certain patients with BRCA wild-type ovarian cancer, such as those with homologous recombination deficiency, which also occurs in approximately half of patients with BRCA wild-type TNBC. In TNBC, homologous recombination deficiency and other aberrations lead to a BRCA-like disease phenotype, which may respond to PARP inhibitors.
Dr. Sharma noted that previous attempts to use PARP inhibitors for BRCA wild-type TNBC have revealed obstacles, such as the inefficacy of PARP inhibitor monotherapy and dose-limiting myelosuppression when PARP inhibitors were added to chemotherapy. The issue of bone marrow toxicity may be mitigated by veliparib, which has minimal PARP-trapping activity, she explained.
“A phase 1 trial has demonstrated that adequate doses of cisplatin can be delivered safely in combination with the near-maximal single-agent dose of veliparib in patients with metastatic TNBC,” Dr. Sharma said.
She and her colleagues put this finding to the test in a phase 3 trial that enrolled 335 patients with metastatic and/or loco-regionally recurrent TNBC or BRCA-associated HER2-negative breast cancer. Patients could be previously untreated or have received one prior cytotoxic chemotherapy for metastatic disease.
Of the patients enrolled, 321 met eligibility criteria, 294 had germline BRCA testing, and 209 had BRCA-like assessment.
Patients were divided into the following groups: germline BRCA-associated disease (n = 37), BRCA-like disease (n = 99), non-BRCA-like disease (n = 110), and unclassified (n = 75).
In each group, patients were randomized in a 1:1 ratio to receive cisplatin (75 mg/m2 on day 1) plus veliparib (300 mg twice daily on days 1-14) every 3 weeks, or cisplatin with placebo. The primary endpoint was PFS.
Results
Among patients with BRCA-like disease, there was a significant improvement in PFS and a trend toward improved OS when veliparib was added to cisplatin. The median PFS was 5.9 months with veliparib and 4.2 months with placebo (P = .006). The median OS was 14.0 months and 12.1 months, respectively (P = .067).
Among patients with previously untreated BRCA-like disease, there were significant improvements in both PFS and OS.
The median PFS in this group was 6.1 months with veliparib and 4.2 months with placebo (P = .008). The 12-month PFS rates were 23% and 3%, respectively.
The median OS in this group was 17.8 months with veliparib and 10.3 months with placebo (P = .048). The 24-month OS rates were 43% and 20%, respectively.
There were no survival benefits with veliparib among patients with unclassified disease, non-BRCA-like disease, or BRCA-associated disease.
Dr. Sharma noted that the lack of significant improvement in the BRCA-associated group was likely due to the small sample size. “FDA approval of PARP inhibitors for treatment of germline BRCA-associated metastatic breast cancer during the course of this trial impacted accrual to this group,” she said.
Veliparib was associated with a higher rate of grade 3-4 hematologic toxicities, including neutropenia (46% vs. 19%), leukopenia (27% vs. 7%), anemia (23% vs. 7%), and thrombocytopenia (19% vs. 3%).
Dr. Sharma said results from this trial should prompt further research. “The combination of veliparib plus cisplatin warrants further evaluation in larger randomized trials for patients with BRCA-like phenotype TNBC,” she said.
Invited discussant Catherine M. Kelly, MB BCh, of Mater Misericordiae University Hospital in Dublin, called the trial “an ambitious study” that has created a “valuable tissue bank” for future translational research. She agreed that more work is necessary.
“Further research is needed to identify the optimal homologous recombination deficiency biomarkers critical in the early treatment-naive and in the advanced treatment-exposed disease settings,” Dr. Kelly said.
SWOG S1416 was funded by the National Institutes of Health and AbbVie. Dr. Sharma disclosed relationships with AstraZeneca, Merck, Novartis, and other companies. Dr. Kelly reported affiliations with Pfizer, Novartis, Roche, and MSD Oncology.
SOURCE: Sharma et al. ASCO 2020, Abstract 1001.
FROM ASCO 2020
Trastuzumab deruxtecan proves active in HER2-mutated NSCLC
, an investigator reported.
The overall response rate (ORR) exceeded 60% among these heavily pretreated patients, with an estimated median progression-free survival (PFS) of 14 months, according to Egbert F. Smit, MD, PhD, of the Netherlands Cancer Institute.
Interstitial lung disease is an identified risk associated with T-DXd treatment, though the events in the DESTINY-Lung01 trial have been low-grade and have not resulted in any deaths, Dr. Smit said when presenting results from the trial as part of the American Society of Clinical Oncology virtual scientific program.
“These data demonstrate the potential of T-DXd as a new treatment option for patients with HER2-mutated non–small-cell lung cancer,” Dr. Smit said.
‘A good targeted therapy’
The findings are a “nice early confirmation” of the initial results seen with T-DXd in an earlier, smaller, phase 1 population, said invited discussant Grace K. Dy, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y.
“Trastuzumab-DXd showed clinical outcomes that meet the standards of what we expect a good targeted therapy should have in terms of overall response rate and progression free survival,” Dr. Dy said.
She noted that the ORR in DESTINY-Lung01 exceeds a 23% ORR seen among NSCLC patients treated with dual HER2-targeted therapy – trastuzumab plus pertuzumab – in a basket trial (J Clin Oncol. 2018 Feb 20;36[6]:536-42). Moreover, the response and PFS data “far surpass” results seen to date with oral tyrosine kinase inhibitors, including pyrotinib, poziotinib, neratinib, and afatinib.
The T-DXd results also look favorable in comparison to another antibody-drug conjugate, ado trastuzumab emtansine, Dr. Dy added, referencing another basket trial in which investigators reported an ORR of 44% and a median PFS of 5 months among 18 patients with advanced HER2-mutant lung adenocarcinomas (J Clin Oncol. 2018 Aug 20;36[24]:2532-7).
“Although T-DM1 [ado trastuzumab emtansine] demonstrated some degree of activity, its lower dosing, which was limited by the payload, lower drug-antibody ratio, and shorter half-life likely explain why results were better with T-DXd,” Dr. Dy said.
T-DXd was, in fact, designed to deliver an optimal antitumor effect, according to Dr. Smit.
The treatment incorporates a humanized anti-HER2 IgG1 monoclonal antibody that has the same amino acid sequence as trastuzumab. The antibody is attached via a cleavable, tumor-selective linker to a payload of deruxtecan, a topoisomerase I inhibitor.
The resulting antibody-drug conjugate has a high drug-to-antibody ratio, with 8 DXd molecules per monoclonal antibody, according to Dr. Smit.
Study details
The DESTINY-Lung01 trial included 42 patients with HER2-mutated NSCLC who received T-DXd at a dose of 6.4 mg/kg every 3 weeks. The patients’ median age was 63 years, and about 64% were female. Eastern Cooperative Oncology Group performance status was 0 in about one-quarter of the patients, and 1 in the remainder.
Patients had received up to six prior lines of treatment, including platinum-based chemotherapy in about 91%, a PD-1 or PD-L1 inhibitor in 55%, and docetaxel in 19%.
The confirmed ORR by independent central review was 61.9% (26/42). That included a single complete response (2.4%) and 25 partial responses (59.5%).
The duration of response was not reached (95% CI, 5.3 months to not estimable), and the median PFS was 14.0 months (95% CI, 6.4-14.0 months).
All patients experienced a treatment-related adverse event. Treatment-related events of grade 3 or greater were seen in 22 patients (52%). These mainly included decreased neutrophil count, anemia, nausea, vomiting, and fatigue.
There were five cases of interstitial lung disease, all of which were grade 2. In four cases, T-DXd was withdrawn. In one case, the drug was interrupted. All patients were treated with steroids.
“Two [patients] recovered, one recovered with sequelae, one was recovering, and one had not recovered by data cutoff,” Dr. Smit said.
DESTINY-Lung01 also includes a cohort of patients with HER2-expressing NSCLC not reported at the meeting. Enrollment in the HER2-mutated cohort that was reported has been expanded with another 50 patients to “better characterize the risk-benefit ratio,” Dr. Smit said.
The DESTINY-Lung01 study is sponsored by Daiichi Sankyo Inc. Dr. Smit reported relationships with Daiichi Sankyo and many other companies. Dr. Dy reported disclosures related to Amgen, AstraZeneca/Medimmune, GlaxoSmithKline, Takeda, and Tesaro.
SOURCE: Smit EF et al. ASCO 2020, Abstract 9504.
, an investigator reported.
The overall response rate (ORR) exceeded 60% among these heavily pretreated patients, with an estimated median progression-free survival (PFS) of 14 months, according to Egbert F. Smit, MD, PhD, of the Netherlands Cancer Institute.
Interstitial lung disease is an identified risk associated with T-DXd treatment, though the events in the DESTINY-Lung01 trial have been low-grade and have not resulted in any deaths, Dr. Smit said when presenting results from the trial as part of the American Society of Clinical Oncology virtual scientific program.
“These data demonstrate the potential of T-DXd as a new treatment option for patients with HER2-mutated non–small-cell lung cancer,” Dr. Smit said.
‘A good targeted therapy’
The findings are a “nice early confirmation” of the initial results seen with T-DXd in an earlier, smaller, phase 1 population, said invited discussant Grace K. Dy, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y.
“Trastuzumab-DXd showed clinical outcomes that meet the standards of what we expect a good targeted therapy should have in terms of overall response rate and progression free survival,” Dr. Dy said.
She noted that the ORR in DESTINY-Lung01 exceeds a 23% ORR seen among NSCLC patients treated with dual HER2-targeted therapy – trastuzumab plus pertuzumab – in a basket trial (J Clin Oncol. 2018 Feb 20;36[6]:536-42). Moreover, the response and PFS data “far surpass” results seen to date with oral tyrosine kinase inhibitors, including pyrotinib, poziotinib, neratinib, and afatinib.
The T-DXd results also look favorable in comparison to another antibody-drug conjugate, ado trastuzumab emtansine, Dr. Dy added, referencing another basket trial in which investigators reported an ORR of 44% and a median PFS of 5 months among 18 patients with advanced HER2-mutant lung adenocarcinomas (J Clin Oncol. 2018 Aug 20;36[24]:2532-7).
“Although T-DM1 [ado trastuzumab emtansine] demonstrated some degree of activity, its lower dosing, which was limited by the payload, lower drug-antibody ratio, and shorter half-life likely explain why results were better with T-DXd,” Dr. Dy said.
T-DXd was, in fact, designed to deliver an optimal antitumor effect, according to Dr. Smit.
The treatment incorporates a humanized anti-HER2 IgG1 monoclonal antibody that has the same amino acid sequence as trastuzumab. The antibody is attached via a cleavable, tumor-selective linker to a payload of deruxtecan, a topoisomerase I inhibitor.
The resulting antibody-drug conjugate has a high drug-to-antibody ratio, with 8 DXd molecules per monoclonal antibody, according to Dr. Smit.
Study details
The DESTINY-Lung01 trial included 42 patients with HER2-mutated NSCLC who received T-DXd at a dose of 6.4 mg/kg every 3 weeks. The patients’ median age was 63 years, and about 64% were female. Eastern Cooperative Oncology Group performance status was 0 in about one-quarter of the patients, and 1 in the remainder.
Patients had received up to six prior lines of treatment, including platinum-based chemotherapy in about 91%, a PD-1 or PD-L1 inhibitor in 55%, and docetaxel in 19%.
The confirmed ORR by independent central review was 61.9% (26/42). That included a single complete response (2.4%) and 25 partial responses (59.5%).
The duration of response was not reached (95% CI, 5.3 months to not estimable), and the median PFS was 14.0 months (95% CI, 6.4-14.0 months).
All patients experienced a treatment-related adverse event. Treatment-related events of grade 3 or greater were seen in 22 patients (52%). These mainly included decreased neutrophil count, anemia, nausea, vomiting, and fatigue.
There were five cases of interstitial lung disease, all of which were grade 2. In four cases, T-DXd was withdrawn. In one case, the drug was interrupted. All patients were treated with steroids.
“Two [patients] recovered, one recovered with sequelae, one was recovering, and one had not recovered by data cutoff,” Dr. Smit said.
DESTINY-Lung01 also includes a cohort of patients with HER2-expressing NSCLC not reported at the meeting. Enrollment in the HER2-mutated cohort that was reported has been expanded with another 50 patients to “better characterize the risk-benefit ratio,” Dr. Smit said.
The DESTINY-Lung01 study is sponsored by Daiichi Sankyo Inc. Dr. Smit reported relationships with Daiichi Sankyo and many other companies. Dr. Dy reported disclosures related to Amgen, AstraZeneca/Medimmune, GlaxoSmithKline, Takeda, and Tesaro.
SOURCE: Smit EF et al. ASCO 2020, Abstract 9504.
, an investigator reported.
The overall response rate (ORR) exceeded 60% among these heavily pretreated patients, with an estimated median progression-free survival (PFS) of 14 months, according to Egbert F. Smit, MD, PhD, of the Netherlands Cancer Institute.
Interstitial lung disease is an identified risk associated with T-DXd treatment, though the events in the DESTINY-Lung01 trial have been low-grade and have not resulted in any deaths, Dr. Smit said when presenting results from the trial as part of the American Society of Clinical Oncology virtual scientific program.
“These data demonstrate the potential of T-DXd as a new treatment option for patients with HER2-mutated non–small-cell lung cancer,” Dr. Smit said.
‘A good targeted therapy’
The findings are a “nice early confirmation” of the initial results seen with T-DXd in an earlier, smaller, phase 1 population, said invited discussant Grace K. Dy, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y.
“Trastuzumab-DXd showed clinical outcomes that meet the standards of what we expect a good targeted therapy should have in terms of overall response rate and progression free survival,” Dr. Dy said.
She noted that the ORR in DESTINY-Lung01 exceeds a 23% ORR seen among NSCLC patients treated with dual HER2-targeted therapy – trastuzumab plus pertuzumab – in a basket trial (J Clin Oncol. 2018 Feb 20;36[6]:536-42). Moreover, the response and PFS data “far surpass” results seen to date with oral tyrosine kinase inhibitors, including pyrotinib, poziotinib, neratinib, and afatinib.
The T-DXd results also look favorable in comparison to another antibody-drug conjugate, ado trastuzumab emtansine, Dr. Dy added, referencing another basket trial in which investigators reported an ORR of 44% and a median PFS of 5 months among 18 patients with advanced HER2-mutant lung adenocarcinomas (J Clin Oncol. 2018 Aug 20;36[24]:2532-7).
“Although T-DM1 [ado trastuzumab emtansine] demonstrated some degree of activity, its lower dosing, which was limited by the payload, lower drug-antibody ratio, and shorter half-life likely explain why results were better with T-DXd,” Dr. Dy said.
T-DXd was, in fact, designed to deliver an optimal antitumor effect, according to Dr. Smit.
The treatment incorporates a humanized anti-HER2 IgG1 monoclonal antibody that has the same amino acid sequence as trastuzumab. The antibody is attached via a cleavable, tumor-selective linker to a payload of deruxtecan, a topoisomerase I inhibitor.
The resulting antibody-drug conjugate has a high drug-to-antibody ratio, with 8 DXd molecules per monoclonal antibody, according to Dr. Smit.
Study details
The DESTINY-Lung01 trial included 42 patients with HER2-mutated NSCLC who received T-DXd at a dose of 6.4 mg/kg every 3 weeks. The patients’ median age was 63 years, and about 64% were female. Eastern Cooperative Oncology Group performance status was 0 in about one-quarter of the patients, and 1 in the remainder.
Patients had received up to six prior lines of treatment, including platinum-based chemotherapy in about 91%, a PD-1 or PD-L1 inhibitor in 55%, and docetaxel in 19%.
The confirmed ORR by independent central review was 61.9% (26/42). That included a single complete response (2.4%) and 25 partial responses (59.5%).
The duration of response was not reached (95% CI, 5.3 months to not estimable), and the median PFS was 14.0 months (95% CI, 6.4-14.0 months).
All patients experienced a treatment-related adverse event. Treatment-related events of grade 3 or greater were seen in 22 patients (52%). These mainly included decreased neutrophil count, anemia, nausea, vomiting, and fatigue.
There were five cases of interstitial lung disease, all of which were grade 2. In four cases, T-DXd was withdrawn. In one case, the drug was interrupted. All patients were treated with steroids.
“Two [patients] recovered, one recovered with sequelae, one was recovering, and one had not recovered by data cutoff,” Dr. Smit said.
DESTINY-Lung01 also includes a cohort of patients with HER2-expressing NSCLC not reported at the meeting. Enrollment in the HER2-mutated cohort that was reported has been expanded with another 50 patients to “better characterize the risk-benefit ratio,” Dr. Smit said.
The DESTINY-Lung01 study is sponsored by Daiichi Sankyo Inc. Dr. Smit reported relationships with Daiichi Sankyo and many other companies. Dr. Dy reported disclosures related to Amgen, AstraZeneca/Medimmune, GlaxoSmithKline, Takeda, and Tesaro.
SOURCE: Smit EF et al. ASCO 2020, Abstract 9504.
FROM ASCO 2020
ALTERNATE trial: No fulvestrant benefit in locally advanced ER+ HER2– breast cancer
Neither fulvestrant alone nor fulvestrant plus anastrozole improved the endocrine-sensitive disease rate (ESDR) versus anastrozole alone as neoadjuvant endocrine therapy in postmenopausal women with locally advanced estrogen receptor-positive HER2-negative (ER+ HER2–) breast cancer in the phase 3 ALTERNATE trial.
The ESDRs were 22.7% in 431 evaluable patients randomized to receive fulvestrant alone, 20.5% in 434 patients who received fulvestrant + anastrozole, and 18.6% in 434 who received anastrozole alone, Cynthia X. Ma, MD, PhD, reported as part of the American Society of Clinical Oncology virtual scientific program.
, said Dr. Ma, a professor at Washington University in St. Louis.
Study subjects had a median age of 64 years, clinical stage II/III ER+ HER2– breast cancer, and were randomized 1:1:1 between February 2014 and November 2018 to receive 6 months of treatment with 500 mg of intramuscular fulvestrant given every 4 weeks following a loading dose, fulvestrant plus a 1 mg daily oral does of anastrozole, or anastrozole alone prior to breast conserving surgery.
The groups were similar with respect to baseline characteristics, and more than 70% were eligible for breast conserving surgery prior to the start of neoadjuvant therapy, Dr. Ma noted, adding that the treatments were well tolerated.
Grade 3 or 4 adverse events were rare, and the percentage of patients experiencing arthralgia, myalgia, or hot flashes was low and similar across arms, she said.
“Neoadjuvant therapy downstages the tumor and improves the rate of breast conserving surgery,” Dr. Ma said, adding that pathologic tumor size, nodal status, Ki67 level, and ER status of resected tumors after neoadjuvant therapy have been shown to be independent prognostic factors for relapse-free survival.
A modified preoperative endocrine prognostic index (mPEPI) of 0 (defined as pT1-2 pN0 Ki67< 2.7%) or pathologic complete response (pCR) is associated with low risk of recurrence without adjuvant chemotherapy. ESDR, defined as the combined mPEPI 0 rates and pCR rates, was a co-primary endpoint of the ALTERNATE trial.
The rationale for studying fulvestrant with or without anastrozole in this setting came from the FALCON and S0226 trials showing superiority of those treatments versus anastrozole monotherapy as first-line endocrine therapy in the metastatic setting, Dr. Ma explained.
In the ALTERNATE trial, Ki67 was tested centrally on biopsies acquired prior to therapy, at weeks 4 and 12, and at surgery. Those with Ki67 greater than 10% at week 4 (20.7% of patients overall) or at week 12 (an additional 1.3% overall) were triaged to receive neoadjuvant chemotherapy; a similar number of patients in each group met these criteria, Dr. Ma said.
Further, patients with mPEPI score of 0 at surgery, were recommended to continue their assigned endocrine therapy without chemotherapy for 1.5 years followed by anastrozole for a total of 5 years of endocrine therapy. Those with mPEPI scores above zero, received chemotherapy and physician’s choice of endocrine therapy.
Follow-up is planned for 10 years. A second primary endpoint will be the breast cancer–free interval in the adjuvant setting.
Among the 936 patients with week 4 Ki67 of 10% or less who completed NET and surgery, the ESDRs were similar across the arms: 31.7% for fulvestrant alone, 26.3% with fulvestrant plus anastrozole, and 28.0% with anastrozole alone, Dr. Ma said.
Week 4 Ki67 reductions from baseline also were similar across the arms.
Nearly all patients with Ki67 of 10% or less at baseline continued to have Ki67 less than 10% at week 4, and about two-thirds of those with Ki67 over 10% at baseline had Ki67 less than 10% at week 4, she said, noting that these findings were also similar across treatment arms.
These first results from the ALTERNATE trial show that fewer than 2% of patients treated with 6 months of neoadjuvant endocrine therapy progressed, likely as a result of the Ki67 triaging strategy, Dr. Ma said.
“Neoadjuvant chemotherapy outcomes for patients with week 4 Ki67 over 10% will be reported later,” she said. “Genomic and biomarker correlates, as well as, importantly, relapse-free survivals are also awaited.”
An invited discussant, Antonio C. Wolff, MD, professor of oncology at Johns Hopkins University, Baltimore, said that while the co-primary endpoint of ESDR in the study was not met, the results provide “a few important messages.”
First, the study showed that low Ki67 at baseline largely stays low at 4 weeks. High Ki67 at baseline frequently became low at week 4, he said.
“Finally, we must congratulate Dr. Ma and colleagues on showing that research biopsies for integral biomarker testing can happen across the [National Clinical Trials Network] throughout the U.S., including most community sites,” he said, adding “that alone is a major accomplishment.”
Dr. Wolff also noted that the 5-year relapse-free survival data for patients who achieve mPEPI 0 at surgery are “awaited with great interest.”
The ALTERNATE trial is funded by the Alliance Foundation, NCI Biomarker, Imaging and Quality of Life Studies Funding Program, Breast Cancer Research Foundation, Genentech,and AstraZeneca. Dr. Ma reported consulting or advisory roles with a variety of pharmaceutical companies, and research funding from pharmaceutical companies to her institution. Dr. Wolff reported relationships (consulting or advisory roles and research funding) with Ionis, Biomarin, Celldex, and patents or royalties (issued or pending) associated with methylation in breast cancer.
SOURCE: Ma C et al. ASCO 2020: Abstract 504.
Neither fulvestrant alone nor fulvestrant plus anastrozole improved the endocrine-sensitive disease rate (ESDR) versus anastrozole alone as neoadjuvant endocrine therapy in postmenopausal women with locally advanced estrogen receptor-positive HER2-negative (ER+ HER2–) breast cancer in the phase 3 ALTERNATE trial.
The ESDRs were 22.7% in 431 evaluable patients randomized to receive fulvestrant alone, 20.5% in 434 patients who received fulvestrant + anastrozole, and 18.6% in 434 who received anastrozole alone, Cynthia X. Ma, MD, PhD, reported as part of the American Society of Clinical Oncology virtual scientific program.
, said Dr. Ma, a professor at Washington University in St. Louis.
Study subjects had a median age of 64 years, clinical stage II/III ER+ HER2– breast cancer, and were randomized 1:1:1 between February 2014 and November 2018 to receive 6 months of treatment with 500 mg of intramuscular fulvestrant given every 4 weeks following a loading dose, fulvestrant plus a 1 mg daily oral does of anastrozole, or anastrozole alone prior to breast conserving surgery.
The groups were similar with respect to baseline characteristics, and more than 70% were eligible for breast conserving surgery prior to the start of neoadjuvant therapy, Dr. Ma noted, adding that the treatments were well tolerated.
Grade 3 or 4 adverse events were rare, and the percentage of patients experiencing arthralgia, myalgia, or hot flashes was low and similar across arms, she said.
“Neoadjuvant therapy downstages the tumor and improves the rate of breast conserving surgery,” Dr. Ma said, adding that pathologic tumor size, nodal status, Ki67 level, and ER status of resected tumors after neoadjuvant therapy have been shown to be independent prognostic factors for relapse-free survival.
A modified preoperative endocrine prognostic index (mPEPI) of 0 (defined as pT1-2 pN0 Ki67< 2.7%) or pathologic complete response (pCR) is associated with low risk of recurrence without adjuvant chemotherapy. ESDR, defined as the combined mPEPI 0 rates and pCR rates, was a co-primary endpoint of the ALTERNATE trial.
The rationale for studying fulvestrant with or without anastrozole in this setting came from the FALCON and S0226 trials showing superiority of those treatments versus anastrozole monotherapy as first-line endocrine therapy in the metastatic setting, Dr. Ma explained.
In the ALTERNATE trial, Ki67 was tested centrally on biopsies acquired prior to therapy, at weeks 4 and 12, and at surgery. Those with Ki67 greater than 10% at week 4 (20.7% of patients overall) or at week 12 (an additional 1.3% overall) were triaged to receive neoadjuvant chemotherapy; a similar number of patients in each group met these criteria, Dr. Ma said.
Further, patients with mPEPI score of 0 at surgery, were recommended to continue their assigned endocrine therapy without chemotherapy for 1.5 years followed by anastrozole for a total of 5 years of endocrine therapy. Those with mPEPI scores above zero, received chemotherapy and physician’s choice of endocrine therapy.
Follow-up is planned for 10 years. A second primary endpoint will be the breast cancer–free interval in the adjuvant setting.
Among the 936 patients with week 4 Ki67 of 10% or less who completed NET and surgery, the ESDRs were similar across the arms: 31.7% for fulvestrant alone, 26.3% with fulvestrant plus anastrozole, and 28.0% with anastrozole alone, Dr. Ma said.
Week 4 Ki67 reductions from baseline also were similar across the arms.
Nearly all patients with Ki67 of 10% or less at baseline continued to have Ki67 less than 10% at week 4, and about two-thirds of those with Ki67 over 10% at baseline had Ki67 less than 10% at week 4, she said, noting that these findings were also similar across treatment arms.
These first results from the ALTERNATE trial show that fewer than 2% of patients treated with 6 months of neoadjuvant endocrine therapy progressed, likely as a result of the Ki67 triaging strategy, Dr. Ma said.
“Neoadjuvant chemotherapy outcomes for patients with week 4 Ki67 over 10% will be reported later,” she said. “Genomic and biomarker correlates, as well as, importantly, relapse-free survivals are also awaited.”
An invited discussant, Antonio C. Wolff, MD, professor of oncology at Johns Hopkins University, Baltimore, said that while the co-primary endpoint of ESDR in the study was not met, the results provide “a few important messages.”
First, the study showed that low Ki67 at baseline largely stays low at 4 weeks. High Ki67 at baseline frequently became low at week 4, he said.
“Finally, we must congratulate Dr. Ma and colleagues on showing that research biopsies for integral biomarker testing can happen across the [National Clinical Trials Network] throughout the U.S., including most community sites,” he said, adding “that alone is a major accomplishment.”
Dr. Wolff also noted that the 5-year relapse-free survival data for patients who achieve mPEPI 0 at surgery are “awaited with great interest.”
The ALTERNATE trial is funded by the Alliance Foundation, NCI Biomarker, Imaging and Quality of Life Studies Funding Program, Breast Cancer Research Foundation, Genentech,and AstraZeneca. Dr. Ma reported consulting or advisory roles with a variety of pharmaceutical companies, and research funding from pharmaceutical companies to her institution. Dr. Wolff reported relationships (consulting or advisory roles and research funding) with Ionis, Biomarin, Celldex, and patents or royalties (issued or pending) associated with methylation in breast cancer.
SOURCE: Ma C et al. ASCO 2020: Abstract 504.
Neither fulvestrant alone nor fulvestrant plus anastrozole improved the endocrine-sensitive disease rate (ESDR) versus anastrozole alone as neoadjuvant endocrine therapy in postmenopausal women with locally advanced estrogen receptor-positive HER2-negative (ER+ HER2–) breast cancer in the phase 3 ALTERNATE trial.
The ESDRs were 22.7% in 431 evaluable patients randomized to receive fulvestrant alone, 20.5% in 434 patients who received fulvestrant + anastrozole, and 18.6% in 434 who received anastrozole alone, Cynthia X. Ma, MD, PhD, reported as part of the American Society of Clinical Oncology virtual scientific program.
, said Dr. Ma, a professor at Washington University in St. Louis.
Study subjects had a median age of 64 years, clinical stage II/III ER+ HER2– breast cancer, and were randomized 1:1:1 between February 2014 and November 2018 to receive 6 months of treatment with 500 mg of intramuscular fulvestrant given every 4 weeks following a loading dose, fulvestrant plus a 1 mg daily oral does of anastrozole, or anastrozole alone prior to breast conserving surgery.
The groups were similar with respect to baseline characteristics, and more than 70% were eligible for breast conserving surgery prior to the start of neoadjuvant therapy, Dr. Ma noted, adding that the treatments were well tolerated.
Grade 3 or 4 adverse events were rare, and the percentage of patients experiencing arthralgia, myalgia, or hot flashes was low and similar across arms, she said.
“Neoadjuvant therapy downstages the tumor and improves the rate of breast conserving surgery,” Dr. Ma said, adding that pathologic tumor size, nodal status, Ki67 level, and ER status of resected tumors after neoadjuvant therapy have been shown to be independent prognostic factors for relapse-free survival.
A modified preoperative endocrine prognostic index (mPEPI) of 0 (defined as pT1-2 pN0 Ki67< 2.7%) or pathologic complete response (pCR) is associated with low risk of recurrence without adjuvant chemotherapy. ESDR, defined as the combined mPEPI 0 rates and pCR rates, was a co-primary endpoint of the ALTERNATE trial.
The rationale for studying fulvestrant with or without anastrozole in this setting came from the FALCON and S0226 trials showing superiority of those treatments versus anastrozole monotherapy as first-line endocrine therapy in the metastatic setting, Dr. Ma explained.
In the ALTERNATE trial, Ki67 was tested centrally on biopsies acquired prior to therapy, at weeks 4 and 12, and at surgery. Those with Ki67 greater than 10% at week 4 (20.7% of patients overall) or at week 12 (an additional 1.3% overall) were triaged to receive neoadjuvant chemotherapy; a similar number of patients in each group met these criteria, Dr. Ma said.
Further, patients with mPEPI score of 0 at surgery, were recommended to continue their assigned endocrine therapy without chemotherapy for 1.5 years followed by anastrozole for a total of 5 years of endocrine therapy. Those with mPEPI scores above zero, received chemotherapy and physician’s choice of endocrine therapy.
Follow-up is planned for 10 years. A second primary endpoint will be the breast cancer–free interval in the adjuvant setting.
Among the 936 patients with week 4 Ki67 of 10% or less who completed NET and surgery, the ESDRs were similar across the arms: 31.7% for fulvestrant alone, 26.3% with fulvestrant plus anastrozole, and 28.0% with anastrozole alone, Dr. Ma said.
Week 4 Ki67 reductions from baseline also were similar across the arms.
Nearly all patients with Ki67 of 10% or less at baseline continued to have Ki67 less than 10% at week 4, and about two-thirds of those with Ki67 over 10% at baseline had Ki67 less than 10% at week 4, she said, noting that these findings were also similar across treatment arms.
These first results from the ALTERNATE trial show that fewer than 2% of patients treated with 6 months of neoadjuvant endocrine therapy progressed, likely as a result of the Ki67 triaging strategy, Dr. Ma said.
“Neoadjuvant chemotherapy outcomes for patients with week 4 Ki67 over 10% will be reported later,” she said. “Genomic and biomarker correlates, as well as, importantly, relapse-free survivals are also awaited.”
An invited discussant, Antonio C. Wolff, MD, professor of oncology at Johns Hopkins University, Baltimore, said that while the co-primary endpoint of ESDR in the study was not met, the results provide “a few important messages.”
First, the study showed that low Ki67 at baseline largely stays low at 4 weeks. High Ki67 at baseline frequently became low at week 4, he said.
“Finally, we must congratulate Dr. Ma and colleagues on showing that research biopsies for integral biomarker testing can happen across the [National Clinical Trials Network] throughout the U.S., including most community sites,” he said, adding “that alone is a major accomplishment.”
Dr. Wolff also noted that the 5-year relapse-free survival data for patients who achieve mPEPI 0 at surgery are “awaited with great interest.”
The ALTERNATE trial is funded by the Alliance Foundation, NCI Biomarker, Imaging and Quality of Life Studies Funding Program, Breast Cancer Research Foundation, Genentech,and AstraZeneca. Dr. Ma reported consulting or advisory roles with a variety of pharmaceutical companies, and research funding from pharmaceutical companies to her institution. Dr. Wolff reported relationships (consulting or advisory roles and research funding) with Ionis, Biomarin, Celldex, and patents or royalties (issued or pending) associated with methylation in breast cancer.
SOURCE: Ma C et al. ASCO 2020: Abstract 504.
FROM ASCO 2020