User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Fracking sites tied to increased heart failure hospitalizations
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
‘Worrisome’ rates of suicidal thoughts and behaviors in children with epilepsy
new research suggests. In a study of more than 100 youth with the disorder, more than 40% had depression, 30% had anxiety, and about 1 in 10 exhibited signs of suicidal thoughts and behaviors.
These rates “are really worrisome” and highlight the need to screen all children and young adults with epilepsy for psychiatric disorders, said study author Tatiana Falcone, MD, assistant professor of neurology and child and adolescent psychiatry at the Cleveland Clinic.
“It’s very important to screen for suicidality and for depression and anxiety, even when patients aren’t reporting symptoms,” said Dr. Falcone.
Previous research shows children with epilepsy will attend the emergency room with symptoms such as headache or stomachache “when the main reason for the visit was the kid was suicidal,” Dr. Falcone said. “Unless you ask the specific question: ‘Are you having thoughts about hurting yourself?’ this will go unreported,” she added.
The findings were presented at the American Epilepsy Society’s 74th Annual Meeting, which was held online this year because of the COVID-19 pandemic.
Red flag
Not much is known about suicidality in children and youth with epilepsy except that depression and anxiety – the most common psychiatric comorbidities in this population – appear to contribute to suicidal thoughts.
Dr. Falcone said that she and her colleagues often see children and adolescents with epilepsy in their clinic who have attempted suicide. In recent years, the clinicians have increased efforts to try to identify them before they carry out a successful suicide attempt, said lead investigator Anjali Dagar, MD, clinical research psychiatry fellow at Cleveland Clinic.
The study included 119 patients aged 10-24 years (mean age, 15.8 years; 54.6% female). All attended an epilepsy clinic or underwent testing in the pediatric epilepsy monitoring unit at the Cleveland Clinic and did not have a psychiatric diagnosis.
Epilepsy severity ranged among study participants. About half were drug resistant and were at the center for surgical evaluation and the others were newly diagnosed.
Participants filled out questionnaires to self-report psychiatric conditions. The validated screening tools included the Center for Epidemiological Studies Depression Scale for Children (CES-DC), the Screen for Child Anxiety Related Emotional Disorders (SCARED), and the Ask Suicide–Screening Questions (ASQ).
A score of 15 or higher on the CES-DC indicates a risk for depression. On the SCARED test, a score higher than 32 indicates anxiety. Recent research has shown that anxiety is a main risk factor “in moving people from contemplating suicide to actually carrying it out,” Dr. Falcone said.
The ASQ includes four questions about suicidal thoughts and whether respondents have tried to hurt themselves. Dr. Dagar noted that a positive response to any of these questions should raise a red flag.
Very high rates
Results showed that almost one-third (30.2%) of the participants scored positive for anxiety on SCARED and 41.2% scored positive for depression on the CSE-DC. These are “very high” rates, Dr. Falcone said. For comparison, the rate of reported anxiety is less than 10% in school surveys.
In addition, the Centers for Disease Control and Prevention reports about 3% of 2- to 17-year-olds in the general population have depression. Even compared with other chronic illnesses (including diabetes, heart disease, and cancer), children with epilepsy have a higher rate of depression, said Dr. Falcone.
More than 1 in 10 (10.9%) participants in the study exhibited signs of suicidality, as shown by having at least one positive response on the ASQ. “That’s a lot,” and much higher than the estimated rate in the general teen population, Dr. Falcone noted.
She noted that “these are just general kids with epilepsy” who had not been previously diagnosed with a psychiatric disorder.
“Depression, anxiety, and suicidality are very frequent comorbidities in patients with epilepsy; and even if a patient is not reporting any symptoms, we should be asking these questions to help them,” she said.
Study participants who had at least one positive response on the ASQ had a mean score of 32.1 on the SCARED, compared with a mean score of 18.3 for those who did not have a positive response on the ASQ (P = .003).
“We wanted to see if there was a direct association in our sample between anxiety and suicidal thoughts, and we found [that] yes there was,” Dr. Falcone said. There was also an association with depression. More than 26% of participants who scored 16 or higher on the CES-DC indicated at least one positive response on the ASQ. This is significantly higher than those who scored 15 or below on the CES-DC (P < .0001).
Bidirectional relationship
The findings suggest that either depression or anxiety may contribute to suicidal thoughts or behaviors, Dr. Dagar said. “It’s like two hands. It could be anxiety leading to suicidality, or it could be depression, or it could be both.”
Dr. Falcone noted that children with epilepsy who aren’t sure when they’ll get their next seizure, or who are bullied at school for being different, may be especially prone to anxiety or depression.
There’s a bit of a “chicken-and-egg” relationship between depression and epilepsy, a disorder affecting electrical signals in the brain, she said. Previous research has shown that a “bidirectional relationship” is involved.
“Even in patients with depression who are not diagnosed with epilepsy, the incidence of epilepsy is 3% higher just because you have depression,” Dr. Falcone said.
Suicidal youth tend to attempt suicide more than once. Dr. Falcone and colleagues are trying to intervene “at different levels,” be that in the hospital or as an outpatient, to prevent this from happening. “We want to find out what different things we can do to engage them and improve the probability they don’t reattempt,” she said.
All children and youth with epilepsy should be screened for anxiety, depression, and suicidal thoughts and behaviors. From age 10 years, children with epilepsy should be screened at least once a year, but those with a psychiatric disorder should be screened more often, Dr. Falcone added. The investigators note their findings need to be confirmed in larger, more diverse studies.
Importance of screening
Michael Privitera, MD, director of the Epilepsy Center and professor of neurology at the University of Cincinnati Gardner Neuroscience Institute, said the findings reinforce that, as with adults, depression and anxiety are common in children with epilepsy.
“Neurologists should take advantage of the many psychiatric screening tools available to identify these problems in their pediatric and adult patients,” Dr. Privitera said. Even more importantly, screening may help identify those who may be at highest risk of suicide.
The study was funded by the Health Resources Services Administration. The investigators and Dr. Privitera have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests. In a study of more than 100 youth with the disorder, more than 40% had depression, 30% had anxiety, and about 1 in 10 exhibited signs of suicidal thoughts and behaviors.
These rates “are really worrisome” and highlight the need to screen all children and young adults with epilepsy for psychiatric disorders, said study author Tatiana Falcone, MD, assistant professor of neurology and child and adolescent psychiatry at the Cleveland Clinic.
“It’s very important to screen for suicidality and for depression and anxiety, even when patients aren’t reporting symptoms,” said Dr. Falcone.
Previous research shows children with epilepsy will attend the emergency room with symptoms such as headache or stomachache “when the main reason for the visit was the kid was suicidal,” Dr. Falcone said. “Unless you ask the specific question: ‘Are you having thoughts about hurting yourself?’ this will go unreported,” she added.
The findings were presented at the American Epilepsy Society’s 74th Annual Meeting, which was held online this year because of the COVID-19 pandemic.
Red flag
Not much is known about suicidality in children and youth with epilepsy except that depression and anxiety – the most common psychiatric comorbidities in this population – appear to contribute to suicidal thoughts.
Dr. Falcone said that she and her colleagues often see children and adolescents with epilepsy in their clinic who have attempted suicide. In recent years, the clinicians have increased efforts to try to identify them before they carry out a successful suicide attempt, said lead investigator Anjali Dagar, MD, clinical research psychiatry fellow at Cleveland Clinic.
The study included 119 patients aged 10-24 years (mean age, 15.8 years; 54.6% female). All attended an epilepsy clinic or underwent testing in the pediatric epilepsy monitoring unit at the Cleveland Clinic and did not have a psychiatric diagnosis.
Epilepsy severity ranged among study participants. About half were drug resistant and were at the center for surgical evaluation and the others were newly diagnosed.
Participants filled out questionnaires to self-report psychiatric conditions. The validated screening tools included the Center for Epidemiological Studies Depression Scale for Children (CES-DC), the Screen for Child Anxiety Related Emotional Disorders (SCARED), and the Ask Suicide–Screening Questions (ASQ).
A score of 15 or higher on the CES-DC indicates a risk for depression. On the SCARED test, a score higher than 32 indicates anxiety. Recent research has shown that anxiety is a main risk factor “in moving people from contemplating suicide to actually carrying it out,” Dr. Falcone said.
The ASQ includes four questions about suicidal thoughts and whether respondents have tried to hurt themselves. Dr. Dagar noted that a positive response to any of these questions should raise a red flag.
Very high rates
Results showed that almost one-third (30.2%) of the participants scored positive for anxiety on SCARED and 41.2% scored positive for depression on the CSE-DC. These are “very high” rates, Dr. Falcone said. For comparison, the rate of reported anxiety is less than 10% in school surveys.
In addition, the Centers for Disease Control and Prevention reports about 3% of 2- to 17-year-olds in the general population have depression. Even compared with other chronic illnesses (including diabetes, heart disease, and cancer), children with epilepsy have a higher rate of depression, said Dr. Falcone.
More than 1 in 10 (10.9%) participants in the study exhibited signs of suicidality, as shown by having at least one positive response on the ASQ. “That’s a lot,” and much higher than the estimated rate in the general teen population, Dr. Falcone noted.
She noted that “these are just general kids with epilepsy” who had not been previously diagnosed with a psychiatric disorder.
“Depression, anxiety, and suicidality are very frequent comorbidities in patients with epilepsy; and even if a patient is not reporting any symptoms, we should be asking these questions to help them,” she said.
Study participants who had at least one positive response on the ASQ had a mean score of 32.1 on the SCARED, compared with a mean score of 18.3 for those who did not have a positive response on the ASQ (P = .003).
“We wanted to see if there was a direct association in our sample between anxiety and suicidal thoughts, and we found [that] yes there was,” Dr. Falcone said. There was also an association with depression. More than 26% of participants who scored 16 or higher on the CES-DC indicated at least one positive response on the ASQ. This is significantly higher than those who scored 15 or below on the CES-DC (P < .0001).
Bidirectional relationship
The findings suggest that either depression or anxiety may contribute to suicidal thoughts or behaviors, Dr. Dagar said. “It’s like two hands. It could be anxiety leading to suicidality, or it could be depression, or it could be both.”
Dr. Falcone noted that children with epilepsy who aren’t sure when they’ll get their next seizure, or who are bullied at school for being different, may be especially prone to anxiety or depression.
There’s a bit of a “chicken-and-egg” relationship between depression and epilepsy, a disorder affecting electrical signals in the brain, she said. Previous research has shown that a “bidirectional relationship” is involved.
“Even in patients with depression who are not diagnosed with epilepsy, the incidence of epilepsy is 3% higher just because you have depression,” Dr. Falcone said.
Suicidal youth tend to attempt suicide more than once. Dr. Falcone and colleagues are trying to intervene “at different levels,” be that in the hospital or as an outpatient, to prevent this from happening. “We want to find out what different things we can do to engage them and improve the probability they don’t reattempt,” she said.
All children and youth with epilepsy should be screened for anxiety, depression, and suicidal thoughts and behaviors. From age 10 years, children with epilepsy should be screened at least once a year, but those with a psychiatric disorder should be screened more often, Dr. Falcone added. The investigators note their findings need to be confirmed in larger, more diverse studies.
Importance of screening
Michael Privitera, MD, director of the Epilepsy Center and professor of neurology at the University of Cincinnati Gardner Neuroscience Institute, said the findings reinforce that, as with adults, depression and anxiety are common in children with epilepsy.
“Neurologists should take advantage of the many psychiatric screening tools available to identify these problems in their pediatric and adult patients,” Dr. Privitera said. Even more importantly, screening may help identify those who may be at highest risk of suicide.
The study was funded by the Health Resources Services Administration. The investigators and Dr. Privitera have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests. In a study of more than 100 youth with the disorder, more than 40% had depression, 30% had anxiety, and about 1 in 10 exhibited signs of suicidal thoughts and behaviors.
These rates “are really worrisome” and highlight the need to screen all children and young adults with epilepsy for psychiatric disorders, said study author Tatiana Falcone, MD, assistant professor of neurology and child and adolescent psychiatry at the Cleveland Clinic.
“It’s very important to screen for suicidality and for depression and anxiety, even when patients aren’t reporting symptoms,” said Dr. Falcone.
Previous research shows children with epilepsy will attend the emergency room with symptoms such as headache or stomachache “when the main reason for the visit was the kid was suicidal,” Dr. Falcone said. “Unless you ask the specific question: ‘Are you having thoughts about hurting yourself?’ this will go unreported,” she added.
The findings were presented at the American Epilepsy Society’s 74th Annual Meeting, which was held online this year because of the COVID-19 pandemic.
Red flag
Not much is known about suicidality in children and youth with epilepsy except that depression and anxiety – the most common psychiatric comorbidities in this population – appear to contribute to suicidal thoughts.
Dr. Falcone said that she and her colleagues often see children and adolescents with epilepsy in their clinic who have attempted suicide. In recent years, the clinicians have increased efforts to try to identify them before they carry out a successful suicide attempt, said lead investigator Anjali Dagar, MD, clinical research psychiatry fellow at Cleveland Clinic.
The study included 119 patients aged 10-24 years (mean age, 15.8 years; 54.6% female). All attended an epilepsy clinic or underwent testing in the pediatric epilepsy monitoring unit at the Cleveland Clinic and did not have a psychiatric diagnosis.
Epilepsy severity ranged among study participants. About half were drug resistant and were at the center for surgical evaluation and the others were newly diagnosed.
Participants filled out questionnaires to self-report psychiatric conditions. The validated screening tools included the Center for Epidemiological Studies Depression Scale for Children (CES-DC), the Screen for Child Anxiety Related Emotional Disorders (SCARED), and the Ask Suicide–Screening Questions (ASQ).
A score of 15 or higher on the CES-DC indicates a risk for depression. On the SCARED test, a score higher than 32 indicates anxiety. Recent research has shown that anxiety is a main risk factor “in moving people from contemplating suicide to actually carrying it out,” Dr. Falcone said.
The ASQ includes four questions about suicidal thoughts and whether respondents have tried to hurt themselves. Dr. Dagar noted that a positive response to any of these questions should raise a red flag.
Very high rates
Results showed that almost one-third (30.2%) of the participants scored positive for anxiety on SCARED and 41.2% scored positive for depression on the CSE-DC. These are “very high” rates, Dr. Falcone said. For comparison, the rate of reported anxiety is less than 10% in school surveys.
In addition, the Centers for Disease Control and Prevention reports about 3% of 2- to 17-year-olds in the general population have depression. Even compared with other chronic illnesses (including diabetes, heart disease, and cancer), children with epilepsy have a higher rate of depression, said Dr. Falcone.
More than 1 in 10 (10.9%) participants in the study exhibited signs of suicidality, as shown by having at least one positive response on the ASQ. “That’s a lot,” and much higher than the estimated rate in the general teen population, Dr. Falcone noted.
She noted that “these are just general kids with epilepsy” who had not been previously diagnosed with a psychiatric disorder.
“Depression, anxiety, and suicidality are very frequent comorbidities in patients with epilepsy; and even if a patient is not reporting any symptoms, we should be asking these questions to help them,” she said.
Study participants who had at least one positive response on the ASQ had a mean score of 32.1 on the SCARED, compared with a mean score of 18.3 for those who did not have a positive response on the ASQ (P = .003).
“We wanted to see if there was a direct association in our sample between anxiety and suicidal thoughts, and we found [that] yes there was,” Dr. Falcone said. There was also an association with depression. More than 26% of participants who scored 16 or higher on the CES-DC indicated at least one positive response on the ASQ. This is significantly higher than those who scored 15 or below on the CES-DC (P < .0001).
Bidirectional relationship
The findings suggest that either depression or anxiety may contribute to suicidal thoughts or behaviors, Dr. Dagar said. “It’s like two hands. It could be anxiety leading to suicidality, or it could be depression, or it could be both.”
Dr. Falcone noted that children with epilepsy who aren’t sure when they’ll get their next seizure, or who are bullied at school for being different, may be especially prone to anxiety or depression.
There’s a bit of a “chicken-and-egg” relationship between depression and epilepsy, a disorder affecting electrical signals in the brain, she said. Previous research has shown that a “bidirectional relationship” is involved.
“Even in patients with depression who are not diagnosed with epilepsy, the incidence of epilepsy is 3% higher just because you have depression,” Dr. Falcone said.
Suicidal youth tend to attempt suicide more than once. Dr. Falcone and colleagues are trying to intervene “at different levels,” be that in the hospital or as an outpatient, to prevent this from happening. “We want to find out what different things we can do to engage them and improve the probability they don’t reattempt,” she said.
All children and youth with epilepsy should be screened for anxiety, depression, and suicidal thoughts and behaviors. From age 10 years, children with epilepsy should be screened at least once a year, but those with a psychiatric disorder should be screened more often, Dr. Falcone added. The investigators note their findings need to be confirmed in larger, more diverse studies.
Importance of screening
Michael Privitera, MD, director of the Epilepsy Center and professor of neurology at the University of Cincinnati Gardner Neuroscience Institute, said the findings reinforce that, as with adults, depression and anxiety are common in children with epilepsy.
“Neurologists should take advantage of the many psychiatric screening tools available to identify these problems in their pediatric and adult patients,” Dr. Privitera said. Even more importantly, screening may help identify those who may be at highest risk of suicide.
The study was funded by the Health Resources Services Administration. The investigators and Dr. Privitera have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM AES 2020
Medical societies waive fees, weigh other options during pandemic
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
COVID-19’s toll on member facilities pushed the American Academy of Sleep Medicine (AASM) recently to take a sizable gamble.
AASM announced in September that it would waive facility fees at all 2,648 AASM-accredited sleep facilities for 2021.
At $1,800-$2,600 for each facility, that will mean lost revenue of between $4.8 million and $6.9 million, but it’s a risk the academy felt it had to take.
AASM President Kannan Ramar, MBBS, MD, said in an interview that they are betting on the future of the field.
An internal survey of members, he said, found that nearly half (46%) of the 551 respondents thought they might have to close by the end of the year.
In addition, 66% reported a lower patient volume in the past month, and 36% reported that their practice or facility had to apply for loans or other financial assistance because of COVID-19, AASM said in its press release.
“We are hoping that if we help our members through this, they will be there for our patients,” Dr. Ramar said.
Other medical societies also are weighing options, straddling the line between needing income to provide resources for members but being acutely aware of the financial toll the pandemic is taking, according to one sampling.
As previously reported, primary care practices are projected to lose more than $68,000 in revenue per full-time physician in 2020, after steep drops in office visits and the collection of fees from March to May, according to a study led by researchers in the Blavatnik Institute at Harvard Medical School, Boston.
Those losses were calculated without considering a potential second wave of COVID-19 this year, the authors noted.
‘We can survive this’
Although AASM waived fees for its member facilities, individual physician fees have not been reduced so far. But the group is looking for more ways to help lower the economic burden on members, Dr. Ramar said.
“I don’t think we’ve ever been in this situation in the 45 years of the academy. This is a once-in-a-lifetime event for challenges we’re going through,” he said. “The board and the leadership realized that, if we’re going to do something, this is the time to do it.”
In addition to waiving the fees, AASM and the AASM Foundation are offering relief funding to state and regional sleep societies and research award recipients through programs created in response to COVID-19.
Some societies said they are not making changes to their dues or fees, some are forgoing cost-of-living fee increases, and some are waiving registration fees for annual meetings.
The American College of Allergy, Asthma and Immunology (ACAAI) waived most members’ registration fees for its annual meeting in November. Typically, that fee would be $500-$800 per member, plus charges for some premium sessions, Michael Blaiss, MD, ACAAI executive medical director, said.
Dr. Blaiss said in an interview that the college thought offering its 6,000 members essentially 25 free hours of CME would benefit them more than waiving annual membership dues, which are about $425 for physicians in the United States.
If the pandemic stretches through 2021, Dr. Blaiss said, “We can survive this. I’m not worried about that at all.”
But he acknowledged the painful effect on medical societies.
“I don’t think any organization would tell you it’s not having an effect on their income,” he said. “I know it is for us and for virtually any medical organization. A high percentage of income comes from the annual meeting.”
Waiving dues has not been a high priority among members in communications so far, Blaiss said.
American Academy of Dermatology President Bruce H. Thiers, MD, said in an interview that there will be no cost-of-living increase for 2021 dues, and AAD members can request a reduction in dues, which will be considered on a case-by-case basis.
“We understand that many members will have to make tough financial decisions,” he said.
In addition, AAD, which has more than 20,000 members, is exploring payment options to help members spread out the cost of membership.
ACP extends membership
The American College of Physicians, whose membership cycle starts in July, did not reduce dues but extended membership at no cost for 3 months through September to its 163,000 members, Phil Masters, MD, ACP’s vice president of membership, said in an interview.
It also expanded its educational offerings related to the pandemic, including webinars on physician wellness and issues regarding telemedicine.
He said expanding educational resources rather than waiving dues was an intentional decision after much discussion because “we’re primarily a services resource organization.”
Membership data are still being calculated, but early indications are that membership is not increasing this year, after seeing annual growth of about 2%-2.5%, Dr. Masters said. He noted that income is down “by several percent.” Annual membership dues average about $500 for physicians who have been practicing for 10 years.
“We’re well positioned to tolerate the ups and downs,” he said, but he acknowledged that “there’s no question the financial impact has been devastating on some practices.”
Like some other associations, ACP decided to cancel this year’s annual meeting, which had been planned for April. The 2021 annual meeting will be conducted online from April 29 to May 1.
Smaller organizations that rely heavily on income from the annual meeting will be severely challenged the longer the pandemic continues, Dr. Masters said.
The decision is not as simple as whether to reduce or eliminate dues, he noted. Organizations will have to reexamine their missions and structure their fees and offerings according to the needs of members.
“It’s a balance in doing things for the community at large and balancing the need to be sensitive to financial implications,” Dr. Masters said.
This article first appeared on Medscape.com.
Prioritize COVID-19 vaccination in both types of diabetes, say docs
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The risk for increased COVID-19 severity in people with type 1 diabetes appears similar to that of type 2 diabetes, contrary to some official advice from the Centers for Disease Control and Prevention. The new finding indicates that people with both types should be priority for receiving a vaccine, investigators say.
The study is the first to prospectively evaluate both inpatients and outpatients and to examine COVID-19 severity factors in addition to death in people with type 1 and type 2 diabetes separately, and was published online Dec. 2 in Diabetes Care.
Among the patients, who were seen at Vanderbilt University Medical Center in Nashville, Tenn., between March and August of 2020, those with both type 1 and type 2 diabetes had between a three- and fourfold greater risk for COVID-19 hospitalization and greater illness severity compared with people without diabetes after adjustments for age, race, and a number of other risk factors.
This finding is important since as of Dec. 1, 2020, the CDC has classified the diabetes types differently in terms of underlying medical conditions that increase the risk for severe COVID-19.
Adults of any age with type 2 diabetes are considered “at increased risk of severe illness” from the virus that causes COVID-19 whereas the CDC says those with type 1 “might be at an increased risk.”
Lead author of the new paper Justin M. Gregory, MD, said in an interview: “I think this needs revision based on the current evidence. I think the data presented in our study and that of Barron et al. in Lancet Endocrinology 2020 indicate the need to place type 1 diabetes at parity with type 2 diabetes.
“These studies indicate both conditions carry an adjusted odds ratio of three to four when compared with people without diabetes for hospitalization, illness severity, and mortality,” he stressed.
Vaccines look promising for patients with diabetes
There were no phase 3 vaccine data available for the vaccine at the time that Dr. Gregory, of the Ian M. Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University, Nashville, Tenn., and colleagues were writing their manuscript in late summer, so the article does not mention this.
But now, Dr. Gregory said, “Based on the initial press releases from Pfizer and Moderna, I am now optimistic that these vaccines might mitigate the excess morbidity and mortality from COVID-19 experienced by patients with diabetes.
“I am eager to see what we learn on December 10 and 17 [the scheduled dates for the meetings of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee to review the Pfizer and Moderna vaccines, respectively].”
But with the winter pandemic surge in the meantime, “Our investigation suggests that as COVID-19 hospitalizations rise, patients with both type 1 and 2 diabetes will comprise a disproportionately higher number of those admissions and, once hospitalized, demonstrate a greater degree of illness severity,” he and his colleagues said.
“In light of these data, we call on our colleagues to emphasize the importance of social distancing measures and hand hygiene, with particular emphasis on patients with diabetes, including those in the most vulnerable communities whom our study affirms will face the most severe impact.”
After adjustments, excess severity risk similar for both diabetes types
The new study data came from electronic health records at Vanderbilt University Medical Center, comprising 137 primary care, urgent care, and hospital facilities where patients were tested for SARS-CoV-2 regardless of the reason for their visit.
Between March 17 and August 7, 2020, 6,451 patients tested positive for COVID-19. Of those, 273 had type 2 diabetes and 40 had type 1 diabetes.
Children younger than 18 years accounted for 20% of those with type 1 diabetes and 9.4% of those without diabetes, but none of the type 2 group. The group with type 2 diabetes was considerably older than the type 1 diabetes and no-diabetes groups, 58 years versus 37 and 33 years, respectively.
Before adjustment for baseline characteristics that differed between groups, patients with type 1 diabetes appeared to have a risk for hospitalization and greater illness severity that was intermediate between the group with no diabetes and the group with type 2 diabetes, the researchers said.
But after adjustment for age, race, sex, hypertension, smoking, and body mass index, people with type 1 diabetes had odds ratios of 3.90 for hospitalization and 3.35 for greater illness severity, which was similar to risk in type 2 diabetes (3.36 and 3.42, respectively), compared to those without diabetes.
Deep dive explores COVID-19 severity risk factors in type 1 diabetes
The investigators then conducted a detailed chart review for 37 of the 40 patients with type 1 diabetes and phone surveys with 15 of them.
The majority (28) had not been hospitalized, and only one was hospitalized for diabetic ketoacidosis (DKA) within 14 days of positive SARS-CoV-2 testing.
This contrasts with a report from the T1D Exchange, in which nearly half of 33 patients with type 1 diabetes and COVID-19 had been hospitalized with DKA. The reason for the discrepancy may be that more severe patients would more likely be referred to the T1D Exchange Registry, Dr. Gregory and colleagues hypothesized.
Clinical factors associated with COVID-19 severity (P < .05) in their study included a prior hypertension diagnosis, higher hemoglobin A1c, at least one prior DKA admission in the past year, and not using a continuous glucose monitor (CGM).
Hospitalizations were twice as likely and illness severity nearly twice as great among those with type 1 diabetes who were Black versus White. Just 8% of those with private insurance were hospitalized, compared with 60% of those with public insurance and 67% with no insurance (P = .001).
“Whereas previous reports have indicated proportionally higher rates of hospitalizations from COVID-19 among Black patients and those with public insurance, this study is the first to show a similar finding in the population with type 1 diabetes,” Dr. Gregory and colleagues wrote.
Only 9% of patients using a CGM were hospitalized versus 47% who used blood glucose meters (P < .016). Similarly, hospitalizations occurred in 6% using an insulin pump versus 33% using multiple daily injections (P < .085).
“Our analysis cannot exclude the possibility that greater amounts of diabetes technology use are a surrogate for higher socioeconomic status,” they noted.
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, JDRF, and the Appleby Foundation. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FDA safety alert: Face masks with metal can burn during MRI
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
After a patient’s face was burned in the outline of a mask worn during a 3-Tesla MRI neck scan, the US Food and Drug Administration (FDA) cautioned that face masks containing metal can heat to unsafe temperatures during scanning.
Clinicians have known for years to ask patients to remove all metal jewelry and other objects prior to an MRI. The widespread wearing of face masks during the COVID-19 pandemic, however, adds one more consideration to the list.
The FDA’s December 7 safety communication applies to surgical and nonsurgical face masks and respirators.
The injury risk relates to rapid heating of metal components. Many face masks contain a nose wire or metal clip that helps the product conform to the face. Some masks contain metal nanoparticles, while others feature antimicrobial coatings with silver or copper. Each of these products should be avoided during MRI scanning. Also watch out for staples on headbands, the FDA warned.
If the metal content of a face mask is unknown, the FDA suggests providing the patient with a facial covering that is known not to contain any metal.
Robert E. Watson Jr, MD, PhD, chair of the American College of Radiology (ACR) Committee on MR Safety, agreed. He recommended that facilities “provide patients with masks known to be MRI-safe and not permit patient-owned masks in the MRI.”
Watson suggested this strategy at a time when face masks are required.
“COVID-19 safety protocols require that patients wear masks when being scanned, to decrease infection risk to MRI staff, decrease risk of contaminating the MRI scanner, and to protect themselves from infection,” he told Medscape Medical News. “Any conducting metal that enters the MRI machine is at risk of heating due to the radiofrequency fields inherent to image generation.”
Adverse events related to the metal components of a face mask should be reported to the FDA using the MedWatch voluntary reporting form. In addition, healthcare providers subject to the FDA user facility reporting requirements should follow procedures at their facilities to report such events.
This article first appeared on Medscape.com.
Air pollution linked to brain amyloid pathology
Higher levels of air pollution were associated with an increased risk for amyloid-beta pathology in a new study of older adults with cognitive impairment. “Many studies have now found a link between air pollution and clinical outcomes of dementia or cognitive decline,” said lead author Leonardo Iaccarino, PhD, Weill Institute for Neurosciences, University of California, San Francisco. “But this study is now showing a clear link between air pollution and a biomarker of Alzheimer’s disease: It shows a relationship between bad air quality and pathology in the brain.
“We believe that exposure to air pollution should be considered as one factor in the lifetime risk of developing Alzheimer’s disease,” he added. “We believe it is a significant determinant. Our results suggest that, if we can reduce occupational and residential exposure to air pollution, then this could help reduce the risk of Alzheimer’s disease.”
The study was published online Nov. 30 in JAMA Neurology.
A modifiable risk factor
Dr. Iaccarino explained that it is well known that air pollution is linked to poor health outcomes. “As well as cardiovascular and respiratory disease, there is also growing interest in the relationship between air pollution and brain health,” he said. “The link is becoming more and more convincing, with evidence from laboratory, animal, and human studies suggesting that individuals exposed to poor air quality have an increased risk of cognitive decline and dementia.”
In addition, this year, the Lancet Commission included air pollution in its updated list of modifiable risk factors for dementia.
For the current study, the researchers analyzed data from the Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) Study, which included more than 18,000 U.S. participants with cognitive impairment who received an amyloid positron-emission tomography scan between 2016 and 2018.
The investigators used data from the IDEAS study to assess the relationship between the air quality at the place of residence of each patient and the likelihood of a positive amyloid PET result. Public records from the U.S. Environmental Protection Agency were used to estimate air quality in individual ZIP-code areas during two periods – 2002-2003 (approximately 14 years before the amyloid PET scan) and 2015-2016 (approximately 1 year before the amyloid PET scan).
Results showed that those living in an area with increased air pollution, as determined using concentrations of predicted fine particulate matter (PM2.5), had a higher probability of a positive amyloid PET scan. This association was dose dependent and statistically significant after adjusting for demographic, lifestyle, and socioeconomic factors as well as medical comorbidities. The association was seen in both periods; the adjusted odds ratio was 1.10 in 2002-2003 and 1.15 in 2015-2016.
“This shows about a 10% increased probability of a positive amyloid test for individuals living in the worst polluted areas, compared with those in the least polluted areas,” Dr. Iaccarino explained.
Every unit increase in PM2.5 in 2002-2003 was associated with an increased probability of positive amyloid findings on PET of 0.5%. Every unit increase in PM2.5 in for the 2015-2016 period was associated with an increased probability of positive amyloid findings on PET of 0.8%.
“This was a very large cohort study, and we adjusted for multiple other factors, so these are pretty robust findings,” Dr. Iaccarino said.
Exposure to higher ozone concentrations was not associated with amyloid positivity on PET scans in either time window.
“These findings suggest that brain amyloid-beta accumulation could be one of the biological pathways in the increased incidence of dementia and cognitive decline associated with exposure to air pollution,” the researchers stated.
A public health concern
“Adverse effects of airborne toxic pollutants associated with amyloid-beta pathology should be considered in public health policy decisions and should inform individual lifetime risk of developing Alzheimer’s disease and dementia,” they concluded.
Dr. Iaccarino noted that, although governments need to take primary action in reducing air pollution, individuals can make some changes to reduce their exposure to poor-quality air.
“Such changes could include not going out or using masks when pollution levels are very high (as happened recently in California with the wildfires) and avoiding areas where the air quality is known to be bad. In addition, there are activities which increase indoor air pollution which can be changed, such as certain types of cooking, cigarette smoking, use of coal fires,” he commented.
“Based on our findings, it would be reasonable to take action on these things, especially for individuals at higher risk of cardiovascular and respiratory disease or Alzheimer’s,” he added.
On a more optimistic note, Dr. Iaccarino pointed out that air quality in the United States has improved significantly in recent years. Meaningful improvements were found between the two periods in this analysis study (2002-2016), “so we are going in the right direction.”
The IDEAS Study was funded by the Alzheimer’s Association, the American College of Radiology, Avid Radiopharmaceuticals, GE Healthcare, and Life Molecular Imaging. Dr. Iaccarino has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Higher levels of air pollution were associated with an increased risk for amyloid-beta pathology in a new study of older adults with cognitive impairment. “Many studies have now found a link between air pollution and clinical outcomes of dementia or cognitive decline,” said lead author Leonardo Iaccarino, PhD, Weill Institute for Neurosciences, University of California, San Francisco. “But this study is now showing a clear link between air pollution and a biomarker of Alzheimer’s disease: It shows a relationship between bad air quality and pathology in the brain.
“We believe that exposure to air pollution should be considered as one factor in the lifetime risk of developing Alzheimer’s disease,” he added. “We believe it is a significant determinant. Our results suggest that, if we can reduce occupational and residential exposure to air pollution, then this could help reduce the risk of Alzheimer’s disease.”
The study was published online Nov. 30 in JAMA Neurology.
A modifiable risk factor
Dr. Iaccarino explained that it is well known that air pollution is linked to poor health outcomes. “As well as cardiovascular and respiratory disease, there is also growing interest in the relationship between air pollution and brain health,” he said. “The link is becoming more and more convincing, with evidence from laboratory, animal, and human studies suggesting that individuals exposed to poor air quality have an increased risk of cognitive decline and dementia.”
In addition, this year, the Lancet Commission included air pollution in its updated list of modifiable risk factors for dementia.
For the current study, the researchers analyzed data from the Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) Study, which included more than 18,000 U.S. participants with cognitive impairment who received an amyloid positron-emission tomography scan between 2016 and 2018.
The investigators used data from the IDEAS study to assess the relationship between the air quality at the place of residence of each patient and the likelihood of a positive amyloid PET result. Public records from the U.S. Environmental Protection Agency were used to estimate air quality in individual ZIP-code areas during two periods – 2002-2003 (approximately 14 years before the amyloid PET scan) and 2015-2016 (approximately 1 year before the amyloid PET scan).
Results showed that those living in an area with increased air pollution, as determined using concentrations of predicted fine particulate matter (PM2.5), had a higher probability of a positive amyloid PET scan. This association was dose dependent and statistically significant after adjusting for demographic, lifestyle, and socioeconomic factors as well as medical comorbidities. The association was seen in both periods; the adjusted odds ratio was 1.10 in 2002-2003 and 1.15 in 2015-2016.
“This shows about a 10% increased probability of a positive amyloid test for individuals living in the worst polluted areas, compared with those in the least polluted areas,” Dr. Iaccarino explained.
Every unit increase in PM2.5 in 2002-2003 was associated with an increased probability of positive amyloid findings on PET of 0.5%. Every unit increase in PM2.5 in for the 2015-2016 period was associated with an increased probability of positive amyloid findings on PET of 0.8%.
“This was a very large cohort study, and we adjusted for multiple other factors, so these are pretty robust findings,” Dr. Iaccarino said.
Exposure to higher ozone concentrations was not associated with amyloid positivity on PET scans in either time window.
“These findings suggest that brain amyloid-beta accumulation could be one of the biological pathways in the increased incidence of dementia and cognitive decline associated with exposure to air pollution,” the researchers stated.
A public health concern
“Adverse effects of airborne toxic pollutants associated with amyloid-beta pathology should be considered in public health policy decisions and should inform individual lifetime risk of developing Alzheimer’s disease and dementia,” they concluded.
Dr. Iaccarino noted that, although governments need to take primary action in reducing air pollution, individuals can make some changes to reduce their exposure to poor-quality air.
“Such changes could include not going out or using masks when pollution levels are very high (as happened recently in California with the wildfires) and avoiding areas where the air quality is known to be bad. In addition, there are activities which increase indoor air pollution which can be changed, such as certain types of cooking, cigarette smoking, use of coal fires,” he commented.
“Based on our findings, it would be reasonable to take action on these things, especially for individuals at higher risk of cardiovascular and respiratory disease or Alzheimer’s,” he added.
On a more optimistic note, Dr. Iaccarino pointed out that air quality in the United States has improved significantly in recent years. Meaningful improvements were found between the two periods in this analysis study (2002-2016), “so we are going in the right direction.”
The IDEAS Study was funded by the Alzheimer’s Association, the American College of Radiology, Avid Radiopharmaceuticals, GE Healthcare, and Life Molecular Imaging. Dr. Iaccarino has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Higher levels of air pollution were associated with an increased risk for amyloid-beta pathology in a new study of older adults with cognitive impairment. “Many studies have now found a link between air pollution and clinical outcomes of dementia or cognitive decline,” said lead author Leonardo Iaccarino, PhD, Weill Institute for Neurosciences, University of California, San Francisco. “But this study is now showing a clear link between air pollution and a biomarker of Alzheimer’s disease: It shows a relationship between bad air quality and pathology in the brain.
“We believe that exposure to air pollution should be considered as one factor in the lifetime risk of developing Alzheimer’s disease,” he added. “We believe it is a significant determinant. Our results suggest that, if we can reduce occupational and residential exposure to air pollution, then this could help reduce the risk of Alzheimer’s disease.”
The study was published online Nov. 30 in JAMA Neurology.
A modifiable risk factor
Dr. Iaccarino explained that it is well known that air pollution is linked to poor health outcomes. “As well as cardiovascular and respiratory disease, there is also growing interest in the relationship between air pollution and brain health,” he said. “The link is becoming more and more convincing, with evidence from laboratory, animal, and human studies suggesting that individuals exposed to poor air quality have an increased risk of cognitive decline and dementia.”
In addition, this year, the Lancet Commission included air pollution in its updated list of modifiable risk factors for dementia.
For the current study, the researchers analyzed data from the Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) Study, which included more than 18,000 U.S. participants with cognitive impairment who received an amyloid positron-emission tomography scan between 2016 and 2018.
The investigators used data from the IDEAS study to assess the relationship between the air quality at the place of residence of each patient and the likelihood of a positive amyloid PET result. Public records from the U.S. Environmental Protection Agency were used to estimate air quality in individual ZIP-code areas during two periods – 2002-2003 (approximately 14 years before the amyloid PET scan) and 2015-2016 (approximately 1 year before the amyloid PET scan).
Results showed that those living in an area with increased air pollution, as determined using concentrations of predicted fine particulate matter (PM2.5), had a higher probability of a positive amyloid PET scan. This association was dose dependent and statistically significant after adjusting for demographic, lifestyle, and socioeconomic factors as well as medical comorbidities. The association was seen in both periods; the adjusted odds ratio was 1.10 in 2002-2003 and 1.15 in 2015-2016.
“This shows about a 10% increased probability of a positive amyloid test for individuals living in the worst polluted areas, compared with those in the least polluted areas,” Dr. Iaccarino explained.
Every unit increase in PM2.5 in 2002-2003 was associated with an increased probability of positive amyloid findings on PET of 0.5%. Every unit increase in PM2.5 in for the 2015-2016 period was associated with an increased probability of positive amyloid findings on PET of 0.8%.
“This was a very large cohort study, and we adjusted for multiple other factors, so these are pretty robust findings,” Dr. Iaccarino said.
Exposure to higher ozone concentrations was not associated with amyloid positivity on PET scans in either time window.
“These findings suggest that brain amyloid-beta accumulation could be one of the biological pathways in the increased incidence of dementia and cognitive decline associated with exposure to air pollution,” the researchers stated.
A public health concern
“Adverse effects of airborne toxic pollutants associated with amyloid-beta pathology should be considered in public health policy decisions and should inform individual lifetime risk of developing Alzheimer’s disease and dementia,” they concluded.
Dr. Iaccarino noted that, although governments need to take primary action in reducing air pollution, individuals can make some changes to reduce their exposure to poor-quality air.
“Such changes could include not going out or using masks when pollution levels are very high (as happened recently in California with the wildfires) and avoiding areas where the air quality is known to be bad. In addition, there are activities which increase indoor air pollution which can be changed, such as certain types of cooking, cigarette smoking, use of coal fires,” he commented.
“Based on our findings, it would be reasonable to take action on these things, especially for individuals at higher risk of cardiovascular and respiratory disease or Alzheimer’s,” he added.
On a more optimistic note, Dr. Iaccarino pointed out that air quality in the United States has improved significantly in recent years. Meaningful improvements were found between the two periods in this analysis study (2002-2016), “so we are going in the right direction.”
The IDEAS Study was funded by the Alzheimer’s Association, the American College of Radiology, Avid Radiopharmaceuticals, GE Healthcare, and Life Molecular Imaging. Dr. Iaccarino has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM JAMA NEUROLOGY
Joint guidelines favor antibody testing for certain Lyme disease manifestations
New clinical practice guidelines on Lyme disease place a strong emphasis on antibody testing to assess for rheumatologic and neurologic syndromes. “Diagnostically, we recommend testing via antibodies, and an index of antibodies in cerebrospinal fluid [CSF] versus serum. Importantly, we recommend against using polymerase chain reaction [PCR] in CSF,” Jeffrey A. Rumbaugh, MD, PhD, a coauthor of the guidelines and a member of the American Academy of Neurology, said in an interview.

The Infectious Diseases Society of America, AAN, and the American College of Rheumatology convened a multidisciplinary panel to develop the 43 recommendations, seeking input from 12 additional medical specialties, and patients. The panel conducted a systematic review of available evidence on preventing, diagnosing, and treating Lyme disease, using the Grading of Recommendations Assessment, Development and Evaluation model to evaluate clinical evidence and strength of recommendations. The guidelines were simultaneous published in Clinical Infectious Diseases, Neurology, Arthritis & Rheumatology, and Arthritis Care & Research.
This is the first time these organizations have collaborated on joint Lyme disease guidelines, which focus mainly on neurologic, cardiac, and rheumatologic manifestations.
“We are very excited to provide these updated guidelines to assist clinicians working in numerous medical specialties around the country, and even the world, as they care for patients suffering from Lyme disease,” Dr. Rumbaugh said.
When to use and not to use PCR
Guideline authors called for specific testing regimens depending on presentation of symptoms. Generally, they advised that individuals with a skin rash suggestive of early disease seek a clinical diagnosis instead of laboratory testing.

Recommendations on Lyme arthritis support previous IDSA guidelines published in 2006, Linda K. Bockenstedt, MD, professor of medicine at Yale University, New Haven, Conn., and a coauthor of the guidelines, said in an interview.
To evaluate for potential Lyme arthritis, clinicians should choose serum antibody testing over PCR or culture of blood or synovial fluid/tissue. However, if a doctor is assessing a seropositive patient for Lyme arthritis diagnosis but needs more information for treatment decisions, the authors recommended PCR applied to synovial fluid or tissue over Borrelia culture.
“Synovial fluid can be analyzed by PCR, but sensitivity is generally lower than serology,” Dr. Bockenstedt explained. Additionally, culture of joint fluid or synovial tissue for Lyme spirochetes has 0% sensitivity in multiple studies. “For these reasons, we recommend serum antibody testing over PCR of joint fluid or other methods for an initial diagnosis.”
Serum antibody testing over PCR or culture is also recommended for identifying Lyme neuroborreliosis in the peripheral nervous system (PNS) or CNS.
Despite the recent popularity of Lyme PCR testing in hospitals and labs, “with Lyme at least, antibodies are better in the CSF,” Dr. Rumbaugh said. Studies have shown that “most patients with even early neurologic Lyme disease are seropositive by conventional antibody testing at time of initial clinical presentation, and that intrathecal antibody production, as demonstrated by an elevated CSF:serum index, is highly specific for CNS involvement.”
If done correctly, antibody testing is both sensitive and specific for neurologic Lyme disease. “On the other hand, sensitivity of Lyme PCR performed on CSF has been only in the 5%-17% range in studies. Incidentally, Lyme PCR on blood is also not sensitive and therefore not recommended,” Dr. Rumbaugh said.
Guideline authors recommended testing in patients with the following conditions: acute neurologic disorders such as meningitis, painful radiculoneuritis, mononeuropathy multiplex; evidence of spinal cord or brain inflammation; and acute myocarditis/pericarditis of unknown cause in an appropriate epidemiologic setting.
They did not recommend testing in patients with typical amyotrophic lateral sclerosis; relapsing remitting multiple sclerosis; Parkinson’s disease, dementia, or cognitive decline; new-onset seizures; other neurologic syndromes or those lacking clinical or epidemiologic history that would support a diagnosis of Lyme disease; and patients with chronic cardiomyopathy of unknown cause.
The authors also called for judicious use of electrocardiogram to screen for Lyme carditis, recommending it only in patients signs or symptoms of this condition. However, patients at risk for or showing signs of severe cardiac complications of Lyme disease should be hospitalized and monitored via ECG.
Timelines for antibiotics
Most patients with Lyme disease should receive oral antibiotics, although duration times vary depending on the disease state. “We recommend that prophylactic antibiotic therapy be given to adults and children only within 72 hours of removal of an identified high-risk tick bite, but not for bites that are equivocal risk or low risk,” according to the guideline authors.
Specific antibiotic treatment regimens by condition are as follows: 10-14 days for early-stage disease, 14 days for Lyme carditis, 14-21 days for neurologic Lyme disease, and 28 days for late Lyme arthritis.
“Despite arthritis occurring late in the course of infection, treatment with a 28-day course of oral antibiotic is effective, although the rates of complete resolution of joint swelling can vary,” Dr. Bockenstedt said. Clinicians may consider a second 28-day course of oral antibiotics or a 2- to 4-week course of ceftriaxone in patients with persistent swelling, after an initial course of oral antibiotics.
Citing knowledge gaps, the authors made no recommendation on secondary antibiotic treatment for unresolved Lyme arthritis. Rheumatologists can play an important role in the care of this small subset of patients, Dr. Bockenstedt noted. “Studies of patients with ‘postantibiotic Lyme arthritis’ show that they can be treated successfully with intra-articular steroids, nonsteroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, biologic response modifiers, and even synovectomy with successful outcomes.” Some of these therapies also work in cases where first courses of oral and intravenous antibiotics are unsuccessful.
“Antibiotic therapy for longer than 8 weeks is not expected to provide additional benefit to patients with persistent arthritis if that treatment has included one course of IV therapy,” the authors clarified.
For patients with Lyme disease–associated meningitis, cranial neuropathy, radiculoneuropathy, or other PNS manifestations, the authors recommended intravenous ceftriaxone, cefotaxime, penicillin G, or oral doxycycline over other antimicrobials.
“For most neurologic presentations, oral doxycycline is just as effective as appropriate IV antibiotics,” Dr. Rumbaugh said. “The exception is the relatively rare situation where the patient is felt to have parenchymal involvement of brain or spinal cord, in which case the guidelines recommend IV antibiotics over oral antibiotics.” In the studies, there was no statistically significant difference between oral or intravenous regimens in response rate or risk of adverse effects.
Patients with nonspecific symptoms such as fatigue, pain, or cognitive impairment following treatment should not receive additional antibiotic therapy if there’s no evidence of treatment failure or infection. These two markers “would include objective signs of disease activity, such as arthritis, meningitis, or neuropathy,” the guideline authors wrote in comments accompanying the recommendation.
Clinicians caring for patients with symptomatic bradycardia caused by Lyme carditis should consider temporary pacing measures instead of a permanent pacemaker. For patients hospitalized with Lyme carditis, “we suggest initially using IV ceftriaxone over oral antibiotics until there is evidence of clinical improvement, then switching to oral antibiotics to complete treatment,” they advised. Outpatients with this condition should receive oral antibiotics instead of intravenous antibiotics.
Advice on antibodies testing ‘particularly cogent’
For individuals without expertise in these areas, the recommendations are clear and useful, Daniel E. Furst, MD, professor of medicine (emeritus) at the University of California, Los Angeles, adjunct professor at the University of Washington, Seattle, and research professor at the University of Florence (Italy), said in an interview.

“As a rheumatologist, I would have appreciated literature references for some of the recommendations but, nevertheless, find these useful. I applaud the care with which the evidence was gathered and the general formatting, which tried to review multiple possible scenarios surrounding Lyme arthritis,” said Dr. Furst, offering a third-party perspective.
The advice on using antibodies tests to make a diagnosis of Lyme arthritis “is particularly cogent and more useful than trying to culture these fastidious organisms,” he added.
The IDSA, AAN, and ACR provided support for the guideline. Dr. Bockenstedt reported receiving research funding from the National Institutes of Health and the Gordon and the Llura Gund Foundation and remuneration from L2 Diagnostics for investigator-initiated NIH-sponsored research. Dr. Rumbaugh had no conflicts of interest to disclose. Dr. Furst reported no conflicts of interest in commenting on these guidelines.
SOURCE: Rumbaugh JA et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1215.
New clinical practice guidelines on Lyme disease place a strong emphasis on antibody testing to assess for rheumatologic and neurologic syndromes. “Diagnostically, we recommend testing via antibodies, and an index of antibodies in cerebrospinal fluid [CSF] versus serum. Importantly, we recommend against using polymerase chain reaction [PCR] in CSF,” Jeffrey A. Rumbaugh, MD, PhD, a coauthor of the guidelines and a member of the American Academy of Neurology, said in an interview.
The Infectious Diseases Society of America, AAN, and the American College of Rheumatology convened a multidisciplinary panel to develop the 43 recommendations, seeking input from 12 additional medical specialties, and patients. The panel conducted a systematic review of available evidence on preventing, diagnosing, and treating Lyme disease, using the Grading of Recommendations Assessment, Development and Evaluation model to evaluate clinical evidence and strength of recommendations. The guidelines were simultaneous published in Clinical Infectious Diseases, Neurology, Arthritis & Rheumatology, and Arthritis Care & Research.
This is the first time these organizations have collaborated on joint Lyme disease guidelines, which focus mainly on neurologic, cardiac, and rheumatologic manifestations.
“We are very excited to provide these updated guidelines to assist clinicians working in numerous medical specialties around the country, and even the world, as they care for patients suffering from Lyme disease,” Dr. Rumbaugh said.
When to use and not to use PCR
Guideline authors called for specific testing regimens depending on presentation of symptoms. Generally, they advised that individuals with a skin rash suggestive of early disease seek a clinical diagnosis instead of laboratory testing.
Recommendations on Lyme arthritis support previous IDSA guidelines published in 2006, Linda K. Bockenstedt, MD, professor of medicine at Yale University, New Haven, Conn., and a coauthor of the guidelines, said in an interview.
To evaluate for potential Lyme arthritis, clinicians should choose serum antibody testing over PCR or culture of blood or synovial fluid/tissue. However, if a doctor is assessing a seropositive patient for Lyme arthritis diagnosis but needs more information for treatment decisions, the authors recommended PCR applied to synovial fluid or tissue over Borrelia culture.
“Synovial fluid can be analyzed by PCR, but sensitivity is generally lower than serology,” Dr. Bockenstedt explained. Additionally, culture of joint fluid or synovial tissue for Lyme spirochetes has 0% sensitivity in multiple studies. “For these reasons, we recommend serum antibody testing over PCR of joint fluid or other methods for an initial diagnosis.”
Serum antibody testing over PCR or culture is also recommended for identifying Lyme neuroborreliosis in the peripheral nervous system (PNS) or CNS.
Despite the recent popularity of Lyme PCR testing in hospitals and labs, “with Lyme at least, antibodies are better in the CSF,” Dr. Rumbaugh said. Studies have shown that “most patients with even early neurologic Lyme disease are seropositive by conventional antibody testing at time of initial clinical presentation, and that intrathecal antibody production, as demonstrated by an elevated CSF:serum index, is highly specific for CNS involvement.”
If done correctly, antibody testing is both sensitive and specific for neurologic Lyme disease. “On the other hand, sensitivity of Lyme PCR performed on CSF has been only in the 5%-17% range in studies. Incidentally, Lyme PCR on blood is also not sensitive and therefore not recommended,” Dr. Rumbaugh said.
Guideline authors recommended testing in patients with the following conditions: acute neurologic disorders such as meningitis, painful radiculoneuritis, mononeuropathy multiplex; evidence of spinal cord or brain inflammation; and acute myocarditis/pericarditis of unknown cause in an appropriate epidemiologic setting.
They did not recommend testing in patients with typical amyotrophic lateral sclerosis; relapsing remitting multiple sclerosis; Parkinson’s disease, dementia, or cognitive decline; new-onset seizures; other neurologic syndromes or those lacking clinical or epidemiologic history that would support a diagnosis of Lyme disease; and patients with chronic cardiomyopathy of unknown cause.
The authors also called for judicious use of electrocardiogram to screen for Lyme carditis, recommending it only in patients signs or symptoms of this condition. However, patients at risk for or showing signs of severe cardiac complications of Lyme disease should be hospitalized and monitored via ECG.
Timelines for antibiotics
Most patients with Lyme disease should receive oral antibiotics, although duration times vary depending on the disease state. “We recommend that prophylactic antibiotic therapy be given to adults and children only within 72 hours of removal of an identified high-risk tick bite, but not for bites that are equivocal risk or low risk,” according to the guideline authors.
Specific antibiotic treatment regimens by condition are as follows: 10-14 days for early-stage disease, 14 days for Lyme carditis, 14-21 days for neurologic Lyme disease, and 28 days for late Lyme arthritis.
“Despite arthritis occurring late in the course of infection, treatment with a 28-day course of oral antibiotic is effective, although the rates of complete resolution of joint swelling can vary,” Dr. Bockenstedt said. Clinicians may consider a second 28-day course of oral antibiotics or a 2- to 4-week course of ceftriaxone in patients with persistent swelling, after an initial course of oral antibiotics.
Citing knowledge gaps, the authors made no recommendation on secondary antibiotic treatment for unresolved Lyme arthritis. Rheumatologists can play an important role in the care of this small subset of patients, Dr. Bockenstedt noted. “Studies of patients with ‘postantibiotic Lyme arthritis’ show that they can be treated successfully with intra-articular steroids, nonsteroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, biologic response modifiers, and even synovectomy with successful outcomes.” Some of these therapies also work in cases where first courses of oral and intravenous antibiotics are unsuccessful.
“Antibiotic therapy for longer than 8 weeks is not expected to provide additional benefit to patients with persistent arthritis if that treatment has included one course of IV therapy,” the authors clarified.
For patients with Lyme disease–associated meningitis, cranial neuropathy, radiculoneuropathy, or other PNS manifestations, the authors recommended intravenous ceftriaxone, cefotaxime, penicillin G, or oral doxycycline over other antimicrobials.
“For most neurologic presentations, oral doxycycline is just as effective as appropriate IV antibiotics,” Dr. Rumbaugh said. “The exception is the relatively rare situation where the patient is felt to have parenchymal involvement of brain or spinal cord, in which case the guidelines recommend IV antibiotics over oral antibiotics.” In the studies, there was no statistically significant difference between oral or intravenous regimens in response rate or risk of adverse effects.
Patients with nonspecific symptoms such as fatigue, pain, or cognitive impairment following treatment should not receive additional antibiotic therapy if there’s no evidence of treatment failure or infection. These two markers “would include objective signs of disease activity, such as arthritis, meningitis, or neuropathy,” the guideline authors wrote in comments accompanying the recommendation.
Clinicians caring for patients with symptomatic bradycardia caused by Lyme carditis should consider temporary pacing measures instead of a permanent pacemaker. For patients hospitalized with Lyme carditis, “we suggest initially using IV ceftriaxone over oral antibiotics until there is evidence of clinical improvement, then switching to oral antibiotics to complete treatment,” they advised. Outpatients with this condition should receive oral antibiotics instead of intravenous antibiotics.
Advice on antibodies testing ‘particularly cogent’
For individuals without expertise in these areas, the recommendations are clear and useful, Daniel E. Furst, MD, professor of medicine (emeritus) at the University of California, Los Angeles, adjunct professor at the University of Washington, Seattle, and research professor at the University of Florence (Italy), said in an interview.
“As a rheumatologist, I would have appreciated literature references for some of the recommendations but, nevertheless, find these useful. I applaud the care with which the evidence was gathered and the general formatting, which tried to review multiple possible scenarios surrounding Lyme arthritis,” said Dr. Furst, offering a third-party perspective.
The advice on using antibodies tests to make a diagnosis of Lyme arthritis “is particularly cogent and more useful than trying to culture these fastidious organisms,” he added.
The IDSA, AAN, and ACR provided support for the guideline. Dr. Bockenstedt reported receiving research funding from the National Institutes of Health and the Gordon and the Llura Gund Foundation and remuneration from L2 Diagnostics for investigator-initiated NIH-sponsored research. Dr. Rumbaugh had no conflicts of interest to disclose. Dr. Furst reported no conflicts of interest in commenting on these guidelines.
SOURCE: Rumbaugh JA et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1215.
New clinical practice guidelines on Lyme disease place a strong emphasis on antibody testing to assess for rheumatologic and neurologic syndromes. “Diagnostically, we recommend testing via antibodies, and an index of antibodies in cerebrospinal fluid [CSF] versus serum. Importantly, we recommend against using polymerase chain reaction [PCR] in CSF,” Jeffrey A. Rumbaugh, MD, PhD, a coauthor of the guidelines and a member of the American Academy of Neurology, said in an interview.
The Infectious Diseases Society of America, AAN, and the American College of Rheumatology convened a multidisciplinary panel to develop the 43 recommendations, seeking input from 12 additional medical specialties, and patients. The panel conducted a systematic review of available evidence on preventing, diagnosing, and treating Lyme disease, using the Grading of Recommendations Assessment, Development and Evaluation model to evaluate clinical evidence and strength of recommendations. The guidelines were simultaneous published in Clinical Infectious Diseases, Neurology, Arthritis & Rheumatology, and Arthritis Care & Research.
This is the first time these organizations have collaborated on joint Lyme disease guidelines, which focus mainly on neurologic, cardiac, and rheumatologic manifestations.
“We are very excited to provide these updated guidelines to assist clinicians working in numerous medical specialties around the country, and even the world, as they care for patients suffering from Lyme disease,” Dr. Rumbaugh said.
When to use and not to use PCR
Guideline authors called for specific testing regimens depending on presentation of symptoms. Generally, they advised that individuals with a skin rash suggestive of early disease seek a clinical diagnosis instead of laboratory testing.
Recommendations on Lyme arthritis support previous IDSA guidelines published in 2006, Linda K. Bockenstedt, MD, professor of medicine at Yale University, New Haven, Conn., and a coauthor of the guidelines, said in an interview.
To evaluate for potential Lyme arthritis, clinicians should choose serum antibody testing over PCR or culture of blood or synovial fluid/tissue. However, if a doctor is assessing a seropositive patient for Lyme arthritis diagnosis but needs more information for treatment decisions, the authors recommended PCR applied to synovial fluid or tissue over Borrelia culture.
“Synovial fluid can be analyzed by PCR, but sensitivity is generally lower than serology,” Dr. Bockenstedt explained. Additionally, culture of joint fluid or synovial tissue for Lyme spirochetes has 0% sensitivity in multiple studies. “For these reasons, we recommend serum antibody testing over PCR of joint fluid or other methods for an initial diagnosis.”
Serum antibody testing over PCR or culture is also recommended for identifying Lyme neuroborreliosis in the peripheral nervous system (PNS) or CNS.
Despite the recent popularity of Lyme PCR testing in hospitals and labs, “with Lyme at least, antibodies are better in the CSF,” Dr. Rumbaugh said. Studies have shown that “most patients with even early neurologic Lyme disease are seropositive by conventional antibody testing at time of initial clinical presentation, and that intrathecal antibody production, as demonstrated by an elevated CSF:serum index, is highly specific for CNS involvement.”
If done correctly, antibody testing is both sensitive and specific for neurologic Lyme disease. “On the other hand, sensitivity of Lyme PCR performed on CSF has been only in the 5%-17% range in studies. Incidentally, Lyme PCR on blood is also not sensitive and therefore not recommended,” Dr. Rumbaugh said.
Guideline authors recommended testing in patients with the following conditions: acute neurologic disorders such as meningitis, painful radiculoneuritis, mononeuropathy multiplex; evidence of spinal cord or brain inflammation; and acute myocarditis/pericarditis of unknown cause in an appropriate epidemiologic setting.
They did not recommend testing in patients with typical amyotrophic lateral sclerosis; relapsing remitting multiple sclerosis; Parkinson’s disease, dementia, or cognitive decline; new-onset seizures; other neurologic syndromes or those lacking clinical or epidemiologic history that would support a diagnosis of Lyme disease; and patients with chronic cardiomyopathy of unknown cause.
The authors also called for judicious use of electrocardiogram to screen for Lyme carditis, recommending it only in patients signs or symptoms of this condition. However, patients at risk for or showing signs of severe cardiac complications of Lyme disease should be hospitalized and monitored via ECG.
Timelines for antibiotics
Most patients with Lyme disease should receive oral antibiotics, although duration times vary depending on the disease state. “We recommend that prophylactic antibiotic therapy be given to adults and children only within 72 hours of removal of an identified high-risk tick bite, but not for bites that are equivocal risk or low risk,” according to the guideline authors.
Specific antibiotic treatment regimens by condition are as follows: 10-14 days for early-stage disease, 14 days for Lyme carditis, 14-21 days for neurologic Lyme disease, and 28 days for late Lyme arthritis.
“Despite arthritis occurring late in the course of infection, treatment with a 28-day course of oral antibiotic is effective, although the rates of complete resolution of joint swelling can vary,” Dr. Bockenstedt said. Clinicians may consider a second 28-day course of oral antibiotics or a 2- to 4-week course of ceftriaxone in patients with persistent swelling, after an initial course of oral antibiotics.
Citing knowledge gaps, the authors made no recommendation on secondary antibiotic treatment for unresolved Lyme arthritis. Rheumatologists can play an important role in the care of this small subset of patients, Dr. Bockenstedt noted. “Studies of patients with ‘postantibiotic Lyme arthritis’ show that they can be treated successfully with intra-articular steroids, nonsteroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, biologic response modifiers, and even synovectomy with successful outcomes.” Some of these therapies also work in cases where first courses of oral and intravenous antibiotics are unsuccessful.
“Antibiotic therapy for longer than 8 weeks is not expected to provide additional benefit to patients with persistent arthritis if that treatment has included one course of IV therapy,” the authors clarified.
For patients with Lyme disease–associated meningitis, cranial neuropathy, radiculoneuropathy, or other PNS manifestations, the authors recommended intravenous ceftriaxone, cefotaxime, penicillin G, or oral doxycycline over other antimicrobials.
“For most neurologic presentations, oral doxycycline is just as effective as appropriate IV antibiotics,” Dr. Rumbaugh said. “The exception is the relatively rare situation where the patient is felt to have parenchymal involvement of brain or spinal cord, in which case the guidelines recommend IV antibiotics over oral antibiotics.” In the studies, there was no statistically significant difference between oral or intravenous regimens in response rate or risk of adverse effects.
Patients with nonspecific symptoms such as fatigue, pain, or cognitive impairment following treatment should not receive additional antibiotic therapy if there’s no evidence of treatment failure or infection. These two markers “would include objective signs of disease activity, such as arthritis, meningitis, or neuropathy,” the guideline authors wrote in comments accompanying the recommendation.
Clinicians caring for patients with symptomatic bradycardia caused by Lyme carditis should consider temporary pacing measures instead of a permanent pacemaker. For patients hospitalized with Lyme carditis, “we suggest initially using IV ceftriaxone over oral antibiotics until there is evidence of clinical improvement, then switching to oral antibiotics to complete treatment,” they advised. Outpatients with this condition should receive oral antibiotics instead of intravenous antibiotics.
Advice on antibodies testing ‘particularly cogent’
For individuals without expertise in these areas, the recommendations are clear and useful, Daniel E. Furst, MD, professor of medicine (emeritus) at the University of California, Los Angeles, adjunct professor at the University of Washington, Seattle, and research professor at the University of Florence (Italy), said in an interview.
“As a rheumatologist, I would have appreciated literature references for some of the recommendations but, nevertheless, find these useful. I applaud the care with which the evidence was gathered and the general formatting, which tried to review multiple possible scenarios surrounding Lyme arthritis,” said Dr. Furst, offering a third-party perspective.
The advice on using antibodies tests to make a diagnosis of Lyme arthritis “is particularly cogent and more useful than trying to culture these fastidious organisms,” he added.
The IDSA, AAN, and ACR provided support for the guideline. Dr. Bockenstedt reported receiving research funding from the National Institutes of Health and the Gordon and the Llura Gund Foundation and remuneration from L2 Diagnostics for investigator-initiated NIH-sponsored research. Dr. Rumbaugh had no conflicts of interest to disclose. Dr. Furst reported no conflicts of interest in commenting on these guidelines.
SOURCE: Rumbaugh JA et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1215.
FROM CLINICAL INFECTIOUS DISEASES
COVID-19 and risk of clotting: ‘Be proactive about prevention’
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.

The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.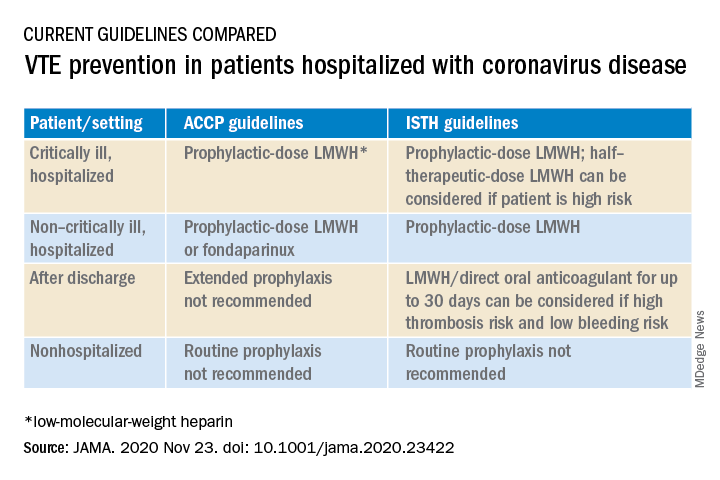
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
The risk of arterial and venous thrombosis in patients with COVID-19 has been a major issue throughout the pandemic, and how best to manage this risk is the subject of a new review article.
The article, by Gregory Dr. Piazza, MD, and David A. Morrow, MD, Brigham and Women’s Hospital, Boston, was published online in JAMA on Nov. 23.
“Basically we’re saying: ‘Be proactive about prevention,’” Dr. Piazza told this news organization.
There is growing recognition among those on the frontline that there is an increased risk of thrombosis in COVID-19 patients, Dr. Piazza said. The risk is highest in patients in the intensive care unit, but the risk is also increased in patients hospitalized with COVID-19, even those not in ICU.
“We don’t really know what the risk is in nonhospitalized COVID-19 patients, but we think it’s much lower than in those who are hospitalized,” he said. “We are waiting for data on the optimal way of managing this increased risk of thrombosis in COVID patients, but for the time being, we believe a systematic way of addressing this risk is best, with every patient hospitalized with COVID-19 receiving some type of thromboprophylaxis. This would mainly be with anticoagulation, but in patients in whom anticoagulation is contraindicated, then mechanical methods could be used, such as pneumatic compression boots or compression stockings.”
The authors report thrombotic complication rates of 2.6% in noncritically ill hospitalized patients with COVID-19 and 35.3% in critically ill patients from a recent U.S. registry study.
Autopsy findings of microthrombi in multiple organ systems, including the lungs, heart, and kidneys, suggest that thrombosis may contribute to multisystem organ dysfunction in severe COVID-19, they note. Although the pathophysiology is not fully defined, prothrombotic abnormalities have been identified in patients with COVID-19, including elevated levels of D-dimer, fibrinogen, and factor VIII, they add.
“There are several major questions about which COVID-19 patients to treat with thromboprophylaxis, how to treat them in term of levels of anticoagulation, and there are many ongoing clinical trials to try and answer these questions,” Dr. Piazza commented. “We need results from these randomized trials to provide a better compass for COVID-19 patients at risk of clotting.”
At present, clinicians can follow two different sets of guidelines on the issue, one from the American College of Chest Physicians and the other from the International Society on Thrombosis and Hemostasis, the authors note.
“The ACCP guidelines are very conservative and basically follow the evidence base for medical patients, while the ISTH guidelines are more aggressive and recommend increased levels of anticoagulation in both ICU and hospitalized non-ICU patients and also extend prophylaxis after discharge,” Dr. Piazza said.
“There is quite a difference between the two sets of guidelines, which can be a point of confusion,” he added.
Dr. Piazza notes that at his center every hospitalized COVID patient who does not have a contraindication to anticoagulation receives a standard prophylactic dose of a once-daily low-molecular-weight heparin (for example, enoxaparin 40 mg). A once-daily product is used to minimize infection risk to staff.
While all COVID patients in the ICU should automatically receive some anticoagulation, the optimal dose is an area of active investigation, he explained. “There were several early reports of ICU patients developing blood clots despite receiving standard thromboprophylaxis so perhaps we need to use higher doses. There are trials underway looking at this, and we would advise enrolling patients into these trials.”
If patients can’t be enrolled into trials, and clinicians feel higher anticoagulation levels are needed, Dr. Piazza advises following the ISTH guidance, which allows an intermediate dose of low-molecular-weight heparin (up to 1 mg/kg enoxaparin).
“Some experts are suggesting even higher doses may be needed in some ICU patients, such as the full therapeutic dose, but I worry about the risk of bleeding with such a strategy,” he said.
Dr. Piazza says they do not routinely give anticoagulation after discharge, but if this is desired then patients could be switched to an oral agent, and some of the direct-acting oral anticoagulants are approved for prophylactic use in medically ill patients.
Dr. Piazza points out that whether thromboprophylaxis should be used for nonhospitalized COVID patients who have risk factors for clotting such as a prior history of thrombosis or obesity is a pressing question, and he encourages clinicians to enroll these patients in clinical trials evaluating this issue, such as the PREVENT-HD trial.
“If they can’t enroll patents in a trial, then they have to make a decision whether the patient is high-enough risk to justify off-label use of anticoagulant. There is a case to be made for this, but there is no evidence for or against such action at present,” he noted.
At this time, neither the ISTH nor ACCP recommend measuring D-dimer to screen for venous thromboembolism or to determine intensity of prophylaxis or treatment, the authors note.
“Ongoing investigation will determine optimal preventive regimens in COVID-19 in the intensive care unit, at hospital discharge, and in nonhospitalized patients at high risk for thrombosis,” they conclude.
Dr. Piazza reported grants from Bayer, Bristol Myers Squibb, Boston Scientific, Janssen, and Portola, and personal fees from Agile, Amgen, Pfizer, and the Prairie Education and Research Cooperative outside the submitted work. Dr. Morrow reported grants from Abbott Laboratories, Amgen, Anthos Therapeutics, Esai, GlaxoSmithKline, Takeda, and The Medicines Company; grants and personal fees from AstraZeneca, Merck, Novartis, and Roche Diagnostics; and personal fees from Bayer Pharma and InCarda outside the submitted work.
A version of this article originally appeared on Medscape.com.
Oral steroids benefit patients with cluster headache
Adjunctive oral prednisone appears to significantly reduce cluster headache attacks, new research shows. Results of the multicenter, randomized, double-blind trial show that patients who received the steroid had 25% fewer attacks in the first week of therapy, compared with their counterparts who received placebo.
In addition, more than a third of patients in the prednisone group were pain free, and for almost half, headache frequency was reduced by at least 50% at day 7 of treatment.
These findings provide clear evidence that prednisone, in conjunction with the use of verapamil, is effective in cluster headache, said lead author Mark Obermann, MD, director, Center for Neurology, Asklepios Hospitals Seesen (Germany), and associate professor, University of Duisburg-Essen (Germany).
The key message, he added, is that all patients with cluster headache should receive prednisone at the start of an episode.
The study was published online Nov. 24 in the Lancet Neurology.
‘Suicide headaches’
Cluster headaches are intense unilateral attacks of facial and head pain. They last 15-180 minutes and predominantly affect men. They are accompanied by trigeminal autonomic symptoms and are extremely painful. “They’re referred to as ‘suicide headaches’ because the pain is so severe that patients often report they think about killing themselves to get rid of the pain,” said Dr. Obermann.
The cause is unclear, although there is some evidence that the hypothalamus is involved. The headaches sometimes follow a “strict circadian pattern,” said Dr. Obermann. He noted that the attacks might occur over a few weeks or months and then not return for months or even years.
An estimated 1 in 1,000 people experience cluster headache, but the condition is underrecognized, and research is scarce and poorly funded. Previous research does show that the calcium channel blocker verapamil, which is used to treat high blood pressure, is effective in cluster headache. However, it takes about 14 days to work and has to be slowly titrated because of cardiac side effects, said Dr. Obermann. For these reasons, international guidelines recommend initiating short-term preventive treatment with corticosteroids to suppress, or at least lessen, cluster headache attacks until long-term prevention is effective.
Although some clinicians treat cluster headaches with corticosteroids, others don’t because of a lack of evidence that shows they are effective. “There’s no evidence whatsoever on what the correct dose is or whether it helps at all. This is the gap we wanted to close,” said Dr. Obermann.
The study included 116 adult patients with cluster headache from 10 centers who were experiencing a cluster headache episode and were not taking prophylactic medication.
The trial only included patients who had an attack within 30 days of their current episode. The investigators included this restriction to reduce the possibility of spontaneous remission, which is “a big problem” in cluster headache trials, he said. To confirm that episodes were cluster headache attacks, patients were also required to have moderate to severe pain, indicated by a score of at least 5 on a numerical rating scale in which 0 indicates no pain and 10 indicates the worse imaginable pain.
Participants were allowed to use treatments for acute attack, but these therapies were limited to triptans, high-flow oxygen, intranasal lidocaine, ergotamine, and oral analgesics.
Debilitating pain
Patients were randomly assigned to receive oral prednisone (n = 53) or placebo (n = 56). The study groups were matched with respect to demographic and clinical characteristics. Prednisone was initiated at 100 mg/d for 5 days and was then tapered by 20 mg every 3 days in the active-treatment group. All patients also received oral verapamil at a starting dose of 40 mg three times per day. The dose was increased every 3 days by 40 mg to a maximum of 360 mg/d.
All participants received pantoprazole 20 mg to prevent the gastric side effects of prednisone. An attack was defined as a unilateral headache of moderate to severe intensity. The study lasted 28 days.
The study’s primary outcome was the mean number of cluster headache attacks during the first week of treatment with prednisone versus placebo.
The mean number of attacks during the first week of treatment was 7.1 in the prednisone group and 9.5 in the placebo group, for a difference of –2.4 attacks (95% confidence interval, –4.8 to –0.03; P = .002). “This might not sound like much,” but reducing the number of daily attacks from, say, eight to six “really makes a difference because the attacks are so painful,” said Dr. Obermann.
The prednisone group also came out on top for a number secondary outcomes. After the first 7 days, attacks ceased in 35% of the prednisone group versus 7% in the placebo group.
‘Clear evidence’ of efficacy
About 49% of patients who took prednisone reported a reduction of at least 50% in attack frequency at day 7. By comparison, 15% of patients who received placebo reported such a reduction. The number of cluster attacks at day 28 was less in the prednisone group than in the patients who received placebo.
With respect to treatment effect, the difference between prednisone and placebo gradually lessened over time “in parallel to the verapamil dose reaching its therapeutic effect,” the investigators noted. “Therefore, attack frequency reduction slowly converged between groups,” they added.
The study results provide “clear evidence” and should reassure clinicians that short-term prednisone early in a cluster headache attack is effective, said Dr. Obermann.
Adverse events, which included headache, palpitations, dizziness, and nausea, were as expected and were similar in the two groups. There were only two severe adverse events, both of which occurred in participants in the placebo group.
Dr. Obermann said the investigators were surprised that so many patients in the study were taking analgesics. “Analgesics don’t work in cluster headache; they just don’t work in this kind of pain.”
He noted that prednisone exposure of study patients spanned only 19 days and amounted to only 1,100 mg, which he believes is safe.
The prednisone dose used in the study is “what most clinicians use in clinical practice,” although there have been reports of success using 500 mg of IV prednisone over 5 days, said Dr. Obermann. He added that it would be “interesting to see if 50 mg would be just as good” as a starting dose.
Potential limitations of the study include the fact that the majority of participants were White, so the findings may not be generalizable to other populations.
Long-awaited results
In an accompanying editorial, Anne Ducros, MD, PhD, professor of neurology and director of the Headache Center, Montpellier (France) University Hospital, said the study provides “strong and long-awaited evidence supporting the use of oral steroids as a transitional treatment option.”
The trial “raises many topics for future research,” one of which is the long-term safety of prednisone for patients with cluster headache, said Dr. Ducros. She noted that use of high-dose steroids once or twice a year for 15 years or more “has the potential for severe systemic toxic effects,” such as corticosteroid-induced osteonecrosis of the femoral head.
Other questions about corticosteroid use for patients with cluster headache remain. These include understanding whether these agents provide better efficacy than occipital nerve injections and determining the optimal verapamil regimen, she noted.
In addition, the risk for oral steroid misuse needs to be studied, she said. She noted that drug misuse is common among patients with cluster headache.
Despite these questions, the results of this new study “provide an important step forward for patients with cluster headache, for whom safe and effective transitional therapies are much needed,” Dr. Ducros wrote.
Dr. Obermann has received fees from Sanofi, Biogen, Novartis, Teva Pharmaceuticals, and Eli Lilly and grants from Allergan and Heel Pharmaceuticals outside of this work. Dr. Ducros has received fees from Amgen, Novartis, Teva, and Eli Lilly; grants from the Programme Hospitalier de Recherche Clinique and from the Appel d’Offre Interne of Montpellier University Hospital; and nonfinancial support from SOS Oxygene.
A version of this article originally appeared on Medscape.com.
Adjunctive oral prednisone appears to significantly reduce cluster headache attacks, new research shows. Results of the multicenter, randomized, double-blind trial show that patients who received the steroid had 25% fewer attacks in the first week of therapy, compared with their counterparts who received placebo.
In addition, more than a third of patients in the prednisone group were pain free, and for almost half, headache frequency was reduced by at least 50% at day 7 of treatment.
These findings provide clear evidence that prednisone, in conjunction with the use of verapamil, is effective in cluster headache, said lead author Mark Obermann, MD, director, Center for Neurology, Asklepios Hospitals Seesen (Germany), and associate professor, University of Duisburg-Essen (Germany).
The key message, he added, is that all patients with cluster headache should receive prednisone at the start of an episode.
The study was published online Nov. 24 in the Lancet Neurology.
‘Suicide headaches’
Cluster headaches are intense unilateral attacks of facial and head pain. They last 15-180 minutes and predominantly affect men. They are accompanied by trigeminal autonomic symptoms and are extremely painful. “They’re referred to as ‘suicide headaches’ because the pain is so severe that patients often report they think about killing themselves to get rid of the pain,” said Dr. Obermann.
The cause is unclear, although there is some evidence that the hypothalamus is involved. The headaches sometimes follow a “strict circadian pattern,” said Dr. Obermann. He noted that the attacks might occur over a few weeks or months and then not return for months or even years.
An estimated 1 in 1,000 people experience cluster headache, but the condition is underrecognized, and research is scarce and poorly funded. Previous research does show that the calcium channel blocker verapamil, which is used to treat high blood pressure, is effective in cluster headache. However, it takes about 14 days to work and has to be slowly titrated because of cardiac side effects, said Dr. Obermann. For these reasons, international guidelines recommend initiating short-term preventive treatment with corticosteroids to suppress, or at least lessen, cluster headache attacks until long-term prevention is effective.
Although some clinicians treat cluster headaches with corticosteroids, others don’t because of a lack of evidence that shows they are effective. “There’s no evidence whatsoever on what the correct dose is or whether it helps at all. This is the gap we wanted to close,” said Dr. Obermann.
The study included 116 adult patients with cluster headache from 10 centers who were experiencing a cluster headache episode and were not taking prophylactic medication.
The trial only included patients who had an attack within 30 days of their current episode. The investigators included this restriction to reduce the possibility of spontaneous remission, which is “a big problem” in cluster headache trials, he said. To confirm that episodes were cluster headache attacks, patients were also required to have moderate to severe pain, indicated by a score of at least 5 on a numerical rating scale in which 0 indicates no pain and 10 indicates the worse imaginable pain.
Participants were allowed to use treatments for acute attack, but these therapies were limited to triptans, high-flow oxygen, intranasal lidocaine, ergotamine, and oral analgesics.
Debilitating pain
Patients were randomly assigned to receive oral prednisone (n = 53) or placebo (n = 56). The study groups were matched with respect to demographic and clinical characteristics. Prednisone was initiated at 100 mg/d for 5 days and was then tapered by 20 mg every 3 days in the active-treatment group. All patients also received oral verapamil at a starting dose of 40 mg three times per day. The dose was increased every 3 days by 40 mg to a maximum of 360 mg/d.
All participants received pantoprazole 20 mg to prevent the gastric side effects of prednisone. An attack was defined as a unilateral headache of moderate to severe intensity. The study lasted 28 days.
The study’s primary outcome was the mean number of cluster headache attacks during the first week of treatment with prednisone versus placebo.
The mean number of attacks during the first week of treatment was 7.1 in the prednisone group and 9.5 in the placebo group, for a difference of –2.4 attacks (95% confidence interval, –4.8 to –0.03; P = .002). “This might not sound like much,” but reducing the number of daily attacks from, say, eight to six “really makes a difference because the attacks are so painful,” said Dr. Obermann.
The prednisone group also came out on top for a number secondary outcomes. After the first 7 days, attacks ceased in 35% of the prednisone group versus 7% in the placebo group.
‘Clear evidence’ of efficacy
About 49% of patients who took prednisone reported a reduction of at least 50% in attack frequency at day 7. By comparison, 15% of patients who received placebo reported such a reduction. The number of cluster attacks at day 28 was less in the prednisone group than in the patients who received placebo.
With respect to treatment effect, the difference between prednisone and placebo gradually lessened over time “in parallel to the verapamil dose reaching its therapeutic effect,” the investigators noted. “Therefore, attack frequency reduction slowly converged between groups,” they added.
The study results provide “clear evidence” and should reassure clinicians that short-term prednisone early in a cluster headache attack is effective, said Dr. Obermann.
Adverse events, which included headache, palpitations, dizziness, and nausea, were as expected and were similar in the two groups. There were only two severe adverse events, both of which occurred in participants in the placebo group.
Dr. Obermann said the investigators were surprised that so many patients in the study were taking analgesics. “Analgesics don’t work in cluster headache; they just don’t work in this kind of pain.”
He noted that prednisone exposure of study patients spanned only 19 days and amounted to only 1,100 mg, which he believes is safe.
The prednisone dose used in the study is “what most clinicians use in clinical practice,” although there have been reports of success using 500 mg of IV prednisone over 5 days, said Dr. Obermann. He added that it would be “interesting to see if 50 mg would be just as good” as a starting dose.
Potential limitations of the study include the fact that the majority of participants were White, so the findings may not be generalizable to other populations.
Long-awaited results
In an accompanying editorial, Anne Ducros, MD, PhD, professor of neurology and director of the Headache Center, Montpellier (France) University Hospital, said the study provides “strong and long-awaited evidence supporting the use of oral steroids as a transitional treatment option.”
The trial “raises many topics for future research,” one of which is the long-term safety of prednisone for patients with cluster headache, said Dr. Ducros. She noted that use of high-dose steroids once or twice a year for 15 years or more “has the potential for severe systemic toxic effects,” such as corticosteroid-induced osteonecrosis of the femoral head.
Other questions about corticosteroid use for patients with cluster headache remain. These include understanding whether these agents provide better efficacy than occipital nerve injections and determining the optimal verapamil regimen, she noted.
In addition, the risk for oral steroid misuse needs to be studied, she said. She noted that drug misuse is common among patients with cluster headache.
Despite these questions, the results of this new study “provide an important step forward for patients with cluster headache, for whom safe and effective transitional therapies are much needed,” Dr. Ducros wrote.
Dr. Obermann has received fees from Sanofi, Biogen, Novartis, Teva Pharmaceuticals, and Eli Lilly and grants from Allergan and Heel Pharmaceuticals outside of this work. Dr. Ducros has received fees from Amgen, Novartis, Teva, and Eli Lilly; grants from the Programme Hospitalier de Recherche Clinique and from the Appel d’Offre Interne of Montpellier University Hospital; and nonfinancial support from SOS Oxygene.
A version of this article originally appeared on Medscape.com.
Adjunctive oral prednisone appears to significantly reduce cluster headache attacks, new research shows. Results of the multicenter, randomized, double-blind trial show that patients who received the steroid had 25% fewer attacks in the first week of therapy, compared with their counterparts who received placebo.
In addition, more than a third of patients in the prednisone group were pain free, and for almost half, headache frequency was reduced by at least 50% at day 7 of treatment.
These findings provide clear evidence that prednisone, in conjunction with the use of verapamil, is effective in cluster headache, said lead author Mark Obermann, MD, director, Center for Neurology, Asklepios Hospitals Seesen (Germany), and associate professor, University of Duisburg-Essen (Germany).
The key message, he added, is that all patients with cluster headache should receive prednisone at the start of an episode.
The study was published online Nov. 24 in the Lancet Neurology.
‘Suicide headaches’
Cluster headaches are intense unilateral attacks of facial and head pain. They last 15-180 minutes and predominantly affect men. They are accompanied by trigeminal autonomic symptoms and are extremely painful. “They’re referred to as ‘suicide headaches’ because the pain is so severe that patients often report they think about killing themselves to get rid of the pain,” said Dr. Obermann.
The cause is unclear, although there is some evidence that the hypothalamus is involved. The headaches sometimes follow a “strict circadian pattern,” said Dr. Obermann. He noted that the attacks might occur over a few weeks or months and then not return for months or even years.
An estimated 1 in 1,000 people experience cluster headache, but the condition is underrecognized, and research is scarce and poorly funded. Previous research does show that the calcium channel blocker verapamil, which is used to treat high blood pressure, is effective in cluster headache. However, it takes about 14 days to work and has to be slowly titrated because of cardiac side effects, said Dr. Obermann. For these reasons, international guidelines recommend initiating short-term preventive treatment with corticosteroids to suppress, or at least lessen, cluster headache attacks until long-term prevention is effective.
Although some clinicians treat cluster headaches with corticosteroids, others don’t because of a lack of evidence that shows they are effective. “There’s no evidence whatsoever on what the correct dose is or whether it helps at all. This is the gap we wanted to close,” said Dr. Obermann.
The study included 116 adult patients with cluster headache from 10 centers who were experiencing a cluster headache episode and were not taking prophylactic medication.
The trial only included patients who had an attack within 30 days of their current episode. The investigators included this restriction to reduce the possibility of spontaneous remission, which is “a big problem” in cluster headache trials, he said. To confirm that episodes were cluster headache attacks, patients were also required to have moderate to severe pain, indicated by a score of at least 5 on a numerical rating scale in which 0 indicates no pain and 10 indicates the worse imaginable pain.
Participants were allowed to use treatments for acute attack, but these therapies were limited to triptans, high-flow oxygen, intranasal lidocaine, ergotamine, and oral analgesics.
Debilitating pain
Patients were randomly assigned to receive oral prednisone (n = 53) or placebo (n = 56). The study groups were matched with respect to demographic and clinical characteristics. Prednisone was initiated at 100 mg/d for 5 days and was then tapered by 20 mg every 3 days in the active-treatment group. All patients also received oral verapamil at a starting dose of 40 mg three times per day. The dose was increased every 3 days by 40 mg to a maximum of 360 mg/d.
All participants received pantoprazole 20 mg to prevent the gastric side effects of prednisone. An attack was defined as a unilateral headache of moderate to severe intensity. The study lasted 28 days.
The study’s primary outcome was the mean number of cluster headache attacks during the first week of treatment with prednisone versus placebo.
The mean number of attacks during the first week of treatment was 7.1 in the prednisone group and 9.5 in the placebo group, for a difference of –2.4 attacks (95% confidence interval, –4.8 to –0.03; P = .002). “This might not sound like much,” but reducing the number of daily attacks from, say, eight to six “really makes a difference because the attacks are so painful,” said Dr. Obermann.
The prednisone group also came out on top for a number secondary outcomes. After the first 7 days, attacks ceased in 35% of the prednisone group versus 7% in the placebo group.
‘Clear evidence’ of efficacy
About 49% of patients who took prednisone reported a reduction of at least 50% in attack frequency at day 7. By comparison, 15% of patients who received placebo reported such a reduction. The number of cluster attacks at day 28 was less in the prednisone group than in the patients who received placebo.
With respect to treatment effect, the difference between prednisone and placebo gradually lessened over time “in parallel to the verapamil dose reaching its therapeutic effect,” the investigators noted. “Therefore, attack frequency reduction slowly converged between groups,” they added.
The study results provide “clear evidence” and should reassure clinicians that short-term prednisone early in a cluster headache attack is effective, said Dr. Obermann.
Adverse events, which included headache, palpitations, dizziness, and nausea, were as expected and were similar in the two groups. There were only two severe adverse events, both of which occurred in participants in the placebo group.
Dr. Obermann said the investigators were surprised that so many patients in the study were taking analgesics. “Analgesics don’t work in cluster headache; they just don’t work in this kind of pain.”
He noted that prednisone exposure of study patients spanned only 19 days and amounted to only 1,100 mg, which he believes is safe.
The prednisone dose used in the study is “what most clinicians use in clinical practice,” although there have been reports of success using 500 mg of IV prednisone over 5 days, said Dr. Obermann. He added that it would be “interesting to see if 50 mg would be just as good” as a starting dose.
Potential limitations of the study include the fact that the majority of participants were White, so the findings may not be generalizable to other populations.
Long-awaited results
In an accompanying editorial, Anne Ducros, MD, PhD, professor of neurology and director of the Headache Center, Montpellier (France) University Hospital, said the study provides “strong and long-awaited evidence supporting the use of oral steroids as a transitional treatment option.”
The trial “raises many topics for future research,” one of which is the long-term safety of prednisone for patients with cluster headache, said Dr. Ducros. She noted that use of high-dose steroids once or twice a year for 15 years or more “has the potential for severe systemic toxic effects,” such as corticosteroid-induced osteonecrosis of the femoral head.
Other questions about corticosteroid use for patients with cluster headache remain. These include understanding whether these agents provide better efficacy than occipital nerve injections and determining the optimal verapamil regimen, she noted.
In addition, the risk for oral steroid misuse needs to be studied, she said. She noted that drug misuse is common among patients with cluster headache.
Despite these questions, the results of this new study “provide an important step forward for patients with cluster headache, for whom safe and effective transitional therapies are much needed,” Dr. Ducros wrote.
Dr. Obermann has received fees from Sanofi, Biogen, Novartis, Teva Pharmaceuticals, and Eli Lilly and grants from Allergan and Heel Pharmaceuticals outside of this work. Dr. Ducros has received fees from Amgen, Novartis, Teva, and Eli Lilly; grants from the Programme Hospitalier de Recherche Clinique and from the Appel d’Offre Interne of Montpellier University Hospital; and nonfinancial support from SOS Oxygene.
A version of this article originally appeared on Medscape.com.
Lost time amid COVID-19
At the end of my second year of medical school was what I call “The Lost Month.”

Between the end of classes and USMLE-1 we had 30 days to study for an 800-question, 2-day test that covered the entirety of the first 2 years. If you failed it once, you had to retake it. If you failed it twice you were out of medical school.
It was understandably stressful and I felt like every minute counted. I stopped shaving for the month to free up a few extra minutes each day. I unplugged my TV and put it in a closet.
Every day was the same. I was up at 7:00, had corn flakes, walked to Creighton, and found an empty library room. I took 30 minutes off at lunch and dinner to get something from the student union to eat outside (the only chance I had to enjoy sunlight), then study again until 1:00-2:00 in the morning.
The whole month become a blur. Days of the week were meaningless, only the number left until boards. Saturday or Tuesday, my life was the same. I don’t remember many specifics.
That was “The Lost Month.”
Now, somewhere in the middle of my attendinghood, I’ve come to 2020 (and likely beyond) which is, “The Lost Year.”
The days of the week have a bit more meaning now, as I still go to my office for a few hours and am home on weekends. But the weeks and months blend together. I’m home most of the time, I busy myself with working, and I have meal breaks with my family. There are no vacations or parties or movies. Even the holidays aren’t that different from the weekends—there isn’t much else to do to pass the time. And the stress is still there (in the early 90s it was academic, today it’s financial).
At least now I still try to shave regularly.
Thirty years ago I passed the boards and moved on to where I am today. My fear of failing out of medical school never materialized.
Today I try to remain optimistic. Vaccines are coming. Our learning curve on treating COVID-19 is getting better. Hopefully, The Lost Year will gradually become a memory as life goes on and normalizes.
Like the The Lost Month, I have to view 2020 as bump in the road. If this is the worst crisis I and my loved ones have to go through, I can deal with that. I know we’re fortunate compared with others. I try to remember that every time I pass a Salvation Army kettle or canned food drive, and donate.
In 1990 I had a specific date when The Lost Month would be over, and it was coming up way too fast. In 2020 no such date exists, now or in the immediate future.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
At the end of my second year of medical school was what I call “The Lost Month.”
Between the end of classes and USMLE-1 we had 30 days to study for an 800-question, 2-day test that covered the entirety of the first 2 years. If you failed it once, you had to retake it. If you failed it twice you were out of medical school.
It was understandably stressful and I felt like every minute counted. I stopped shaving for the month to free up a few extra minutes each day. I unplugged my TV and put it in a closet.
Every day was the same. I was up at 7:00, had corn flakes, walked to Creighton, and found an empty library room. I took 30 minutes off at lunch and dinner to get something from the student union to eat outside (the only chance I had to enjoy sunlight), then study again until 1:00-2:00 in the morning.
The whole month become a blur. Days of the week were meaningless, only the number left until boards. Saturday or Tuesday, my life was the same. I don’t remember many specifics.
That was “The Lost Month.”
Now, somewhere in the middle of my attendinghood, I’ve come to 2020 (and likely beyond) which is, “The Lost Year.”
The days of the week have a bit more meaning now, as I still go to my office for a few hours and am home on weekends. But the weeks and months blend together. I’m home most of the time, I busy myself with working, and I have meal breaks with my family. There are no vacations or parties or movies. Even the holidays aren’t that different from the weekends—there isn’t much else to do to pass the time. And the stress is still there (in the early 90s it was academic, today it’s financial).
At least now I still try to shave regularly.
Thirty years ago I passed the boards and moved on to where I am today. My fear of failing out of medical school never materialized.
Today I try to remain optimistic. Vaccines are coming. Our learning curve on treating COVID-19 is getting better. Hopefully, The Lost Year will gradually become a memory as life goes on and normalizes.
Like the The Lost Month, I have to view 2020 as bump in the road. If this is the worst crisis I and my loved ones have to go through, I can deal with that. I know we’re fortunate compared with others. I try to remember that every time I pass a Salvation Army kettle or canned food drive, and donate.
In 1990 I had a specific date when The Lost Month would be over, and it was coming up way too fast. In 2020 no such date exists, now or in the immediate future.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
At the end of my second year of medical school was what I call “The Lost Month.”
Between the end of classes and USMLE-1 we had 30 days to study for an 800-question, 2-day test that covered the entirety of the first 2 years. If you failed it once, you had to retake it. If you failed it twice you were out of medical school.
It was understandably stressful and I felt like every minute counted. I stopped shaving for the month to free up a few extra minutes each day. I unplugged my TV and put it in a closet.
Every day was the same. I was up at 7:00, had corn flakes, walked to Creighton, and found an empty library room. I took 30 minutes off at lunch and dinner to get something from the student union to eat outside (the only chance I had to enjoy sunlight), then study again until 1:00-2:00 in the morning.
The whole month become a blur. Days of the week were meaningless, only the number left until boards. Saturday or Tuesday, my life was the same. I don’t remember many specifics.
That was “The Lost Month.”
Now, somewhere in the middle of my attendinghood, I’ve come to 2020 (and likely beyond) which is, “The Lost Year.”
The days of the week have a bit more meaning now, as I still go to my office for a few hours and am home on weekends. But the weeks and months blend together. I’m home most of the time, I busy myself with working, and I have meal breaks with my family. There are no vacations or parties or movies. Even the holidays aren’t that different from the weekends—there isn’t much else to do to pass the time. And the stress is still there (in the early 90s it was academic, today it’s financial).
At least now I still try to shave regularly.
Thirty years ago I passed the boards and moved on to where I am today. My fear of failing out of medical school never materialized.
Today I try to remain optimistic. Vaccines are coming. Our learning curve on treating COVID-19 is getting better. Hopefully, The Lost Year will gradually become a memory as life goes on and normalizes.
Like the The Lost Month, I have to view 2020 as bump in the road. If this is the worst crisis I and my loved ones have to go through, I can deal with that. I know we’re fortunate compared with others. I try to remember that every time I pass a Salvation Army kettle or canned food drive, and donate.
In 1990 I had a specific date when The Lost Month would be over, and it was coming up way too fast. In 2020 no such date exists, now or in the immediate future.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.