User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Coronavirus can spread to heart, brain days after infection
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
Children and COVID: Nearly 200,000 new cases reported in 1 week
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
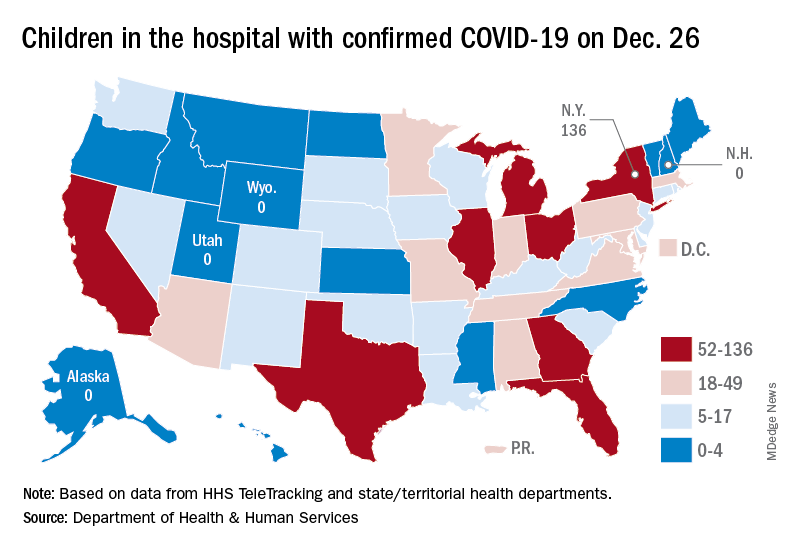
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
Most cancer patients with breakthrough COVID-19 infection experience severe outcomes
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF ONCOLOGY
CVS, Walmart plan bigger in-store clinics: Will primary care practices suffer?
Jordan Grumet, MD, an internist in Northbrook, Ill., left his private practice about 2 years ago, partly because of competition from local retail clinics.
“We were always fighting the pharmacy clinics,” he said. “My generation of doctors was brought up to think we should have a one-stop shop. That was the idea behind being a primary care doctor. So it was very destructive to know your patients were going to another provider.”
Local retail clinics and urgent care centers were also co-opting many of the minor acute care visits that help primary care practices survive. “The number of visits for flu shots and simple medical problems drops,” said Dr. Grumet, who is now an end-of-life-care consultant and also works in hospices. “That can put downward economic pressure on primary care practices.”
Competition for primary care practices is ready to heat up even more, and the environment may soon become even more threatening for primary care doctors. Over the last year, the two largest pharmacy chains – CVS and Walgreens – announced their intentions to build larger retail clinics that will offer many aspects of traditional primary care. Walmart will also be doing the same.
How many geographical areas will be affected is unknown. However,
“There will be more competition, no question,” said George Abraham, MD, MPH, president of the American College of Physicians.
Andrew Bazemore, MD, MPH, senior vice president of research and policy for the American Board of Family Medicine, agreed. “Seeing retail clinics finally embrace the promise of coordination and comprehensiveness in primary care is a promising step. It’s good to see CVS, Walmart, and Walgreens embracing the notion that they have to do more than just urgent care. On the flip side, it’s a source of competition for longstanding primary care clinics.”
Jeff Kagan, MD, an internist in Newington, Conn., noted that during the pandemic the booming demand for primary care has reduced competition from alternative care settings.
“But if this was not pandemic times, it would be very different. There are more urgent care walk-in clinics that do some primary care, and they are pulling away patients.”
New alternative care settings
The number of retail health centers has leveled off at around 2,000 clinics, about the same as in 2016. But CVS, which has around half that total, is now adding HealthHUB facilities, which offer nonemergency care. CVS had 800 of these quasi-primary care clinics in the first quarter of 2021 and planned to have 1,000 by the end of 2021, according to Managed Healthcare Executive.
Walgreens closed 150 of its retail clinics while partnering with VillageMD to develop 600 VillageMD clinics that are larger than its current in-store offices. The chain plans to build these clinics adjacent to Walgreens stores in 30 markets over the next 4 years. Currently, Walgreens has more than 50 VillageMD clinics, mostly in Sunbelt states.
Walmart opened the first of its new expanded-service clinics in 2019. Now it has clinics in Georgia, Arkansas, Texas, and Florida. These Walmart Health locations offer urgent care, primary care, labs, x-ray, and mental health therapy, as well as dental, optical, and hearing services.
The number of urgent care centers (UCCs), meanwhile, has mushroomed during the last decade. With the addition of 400-500 centers every year since 2014, there were 9,279 UCCs in the United States as of June 2019, according to the Urgent Care Association.
These UCCs usually have on-staff physicians. In contrast, most retail clinics are staffed by nurse practitioners. Another big difference is that in retail clinics, two-thirds of the patients – many of them young and healthy – have no regular primary care clinician; only a third of UCC patients don’t have a personal physician.
Because of these rootless patients, competition from retail clinics “is no big deal” to some primary care practices, said Ateev Mehrotra, MD, a Harvard Medical School professor in Boston who has studied alternative care settings. On the other hand, he asked, why do so few UCC patients have a regular physician? That raises the question of how many of these patients would go to a primary care office if there were no retail clinics or UCCs.
Economic pressure on practices
Dr. Grumet’s point about retail clinics and UCCs depriving his practice of easy, lucrative visits is widely echoed among his peers. The fee-for-service payment system based on Medicare rates exacerbates the problem. As Dr. Abraham pointed out, when primary care doctors see a higher percentage of patients with complicated problems, the doctors don’t get compensated fairly for those visits.
Minor acute care, Dr. Abraham noted, is “easier work for the same pay. When I review 100 pages of records for someone who was hospitalized and figure out their 10 different problems and 20 medications, I get paid virtually the same as if I treated a diabetic with a common cold or a foot laceration. The complexity of thought is not factored completely into the reimbursement. And we use the easier visits to offset the more complex ones.”
What happened to continuity of care?
The fragmentation of care between primary care practices and alternative care settings also “diminishes the primary care function,” Dr. Bazemore said.
“Primary care is supposed to be first contact, covering most of what a patient needs – comprehensive, coordinated, and continuous,” he observed. “When you fragment and separate an urgent care function from the rest, so it’s not done in the context of that first contact, you weaken the primary care component without enhancing its function.”
Observers doubt the advent of larger retail clinics that provide more services is likely to solve this problem. In Dr. Mehrotra’s view, CVS’ HealthHUBs “are all about supporting primary care. But are they really? Who are the patients supposed to come back to? This is a critical point: When you ask patients who’s in charge of their care, what are they going to say?”
Retail clinics and urgent care centers have a similar issue, Dr. Grumet said. “If you see patients in the office, and they have problems late at night, they can call you. There’s a continuity of care you don’t get in alternative care settings. The real goal in those places is to get patients in, assess them, and get them out. Which is fine – for minor things. But for someone who needs more comprehensive care, it’s not so good.”
This is why the ACP advised against the provision of chronic care in alternative care settings, said Dr. Abraham. “The problem with retail clinics is they’ve expanded into chronic care management in one or more episodes that require care, but not true continuity of care. When you go to a primary care physician’s office, we discuss more than just acute problems or chronic health issues; we talk about wellness, lifestyle, preventive services, vaccines, and your family. Relationship-building occurs, which transcends more than care interaction. In a setting where you get your care and you leave, longitudinal, holistic care doesn’t build.”
Dr. Kagan put it more succinctly: “Sometimes urgent care walk-in clinics get in over their head [with chronic care]. They like the guy who has high blood pressure and comes in once or twice a year for a prescription refill. But they’re not involved with the guy who has much more trouble.”
None of the urgent care doctors he knows of are taking long-term responsibility for their patients, Dr. Kagan added. “They don’t schedule follow-ups. They’ll see a patient for something, then say: ‘If you’re not better, come back and see me in a couple of weeks.’ ”
Two flavors of urgent care
Dr. Kagan has seen another type of doctor-patient relationship since he sold his practice to Hartford HealthCare 2 years ago. Hartford HealthCare owns 50% of an urgent care group called GoHealth.
“If our Hartford HealthCare patients can’t get into the office, we encourage them to go to a GoHealth facility,” he noted. “It’s not competition; it’s like one of our colleagues. We use the same EMR, so I can see everything that happens. I can even send someone who needs an x-ray to a GoHealth Center just for that.”
Moreover, GoHealth provides only urgent care. “So if it’s one of my patients, they refer them back to me for follow-up. And if somebody wanders in there without a primary care physician, they’ll hook them up with a Hartford HealthCare clinician.”
Dr. Bazemore has had a similar experience. He practices 1 day a week in his residency clinic in Fairfax, Va., which is owned by the Inova Health System. Inova created an adjoining urgent care facility that is open 7 days a week and uses the same EMR as Dr. Bazemore’s clinic.
This is the kind of relationship that Dr. Abraham would like to see between alternative care settings and traditional primary care practices: complementary rather than competitive. However, he questions the motives of hospital systems that own urgent care centers.
“Health care systems are starting these urgent care centers because they want to cash in on the same market,” he said. “I’m not convinced that their goal is to feed their primary care doctors. That is a potential advantage, but they also feed their specialists and try to blend procedures and other lucrative aspects of care into their system.”
What pharmacy chains are up to
Pharmacy chains have their own ulterior motives, Dr. Abraham noted. They built retail clinics for the same reason they sell drugs: to increase sales of consumer goods in their stores. Dr. Bazemore added that retail clinics also aim “to achieve a certain patient volume and incentivize what’s purchased in the pharmacy.”
Exacerbating the situation, CVS now owns Aetna, one of the biggest health insurers. Dr. Kagan believed that CVS’ new emphasis on HealthHUBs may be related to that. “CVS seems to be closing drugstores and opening up more primary care places, and now that they own Aetna, they’re trying to make Aetna patients go to CVS when they have a problem,” he said. Aetna patients are now required to fill their prescriptions at CVS.
Walmart has said it plans to open expanded-service clinics in locales that don’t have sufficient primary care, especially rural areas. The experts we consulted agree that Walmart won’t stop there if its new model is successful. In fact, Dr. Bazemore noted, competition from the new generation of in-store clinics is likely to be in areas where there are plenty of primary care doctors.
“For economic reasons, you’re going to see more of these clinics fill spaces where there’s already a sufficiency [of primary care] – starting with wealthy suburban areas,” Dr. Bazemore said. “Where you have a Walmart, Walgreens, or CVS, you tend to find more purchasers. I don’t know that it’s necessarily the answer to our access problems.”
What should primary care doctors do?
The obvious response of primary care practices to competition from retail clinics and urgent care centers that are open 7 days a week, 12 hours a day, is to expand their hours. In addition, they can introduce same-day scheduling or reserve a block of time every day for walk-in patients.
That’s the approach that Dr. Grumet took in his private practice. “When my patients called me, I tried to deal with it right away. So it was baffling that some of them went to retail clinics.”
Actually, it’s not so baffling, Dr. Abraham said, when you consider that retail clinics are part of a one-stop-shopping experience that will become even more all-encompassing in stores that add quasi-primary care clinics. “You can pick up the consumables you need, you can pick up prescriptions, and you can see your physician without having to make multiple stops. It’s a great idea for pharmacies.”
How about telemedicine? A lot of acute care similar to that provided in alternative care settings can be offered during virtual visits, noted Dr. Bazemore. However, the pharmacy chains have been providing telemedicine for years, using third-party services. And while the convenience of virtual visits appeals to some patients, that’s no guarantee they won’t go to retail clinics.
Reaching out to patients with reminders about the need for checkups and preventive visits, either by phone or through a patient portal, is another technique that practices can use to retain patients. A recent Press Ganey poll showed that people value this kind of communication. But it hardly seems sufficient to hold off the competitive assault of pharmacy chains.
A flaw in the pharmacies’ strategy, however, could eventually come back to bite them: Because the new, larger clinics don’t provide comprehensive care, people will eventually have to turn to traditional primary care – if it’s still around.
“Here’s the problem,” Dr. Grumet explained. “If you’re going to do [in-store primary care], you have to take ownership of the patient and manage everything. You have to be a full-fledged primary care practice with on-call hours and ER coverage. Otherwise, you’re taking bits and pieces – probably low-hanging fruit – to make money, and taking those away from the primary care practice. Which means you’re taking them from the people who should be doing the job.”
A version of this article first appeared on Medscape.com.
Jordan Grumet, MD, an internist in Northbrook, Ill., left his private practice about 2 years ago, partly because of competition from local retail clinics.
“We were always fighting the pharmacy clinics,” he said. “My generation of doctors was brought up to think we should have a one-stop shop. That was the idea behind being a primary care doctor. So it was very destructive to know your patients were going to another provider.”
Local retail clinics and urgent care centers were also co-opting many of the minor acute care visits that help primary care practices survive. “The number of visits for flu shots and simple medical problems drops,” said Dr. Grumet, who is now an end-of-life-care consultant and also works in hospices. “That can put downward economic pressure on primary care practices.”
Competition for primary care practices is ready to heat up even more, and the environment may soon become even more threatening for primary care doctors. Over the last year, the two largest pharmacy chains – CVS and Walgreens – announced their intentions to build larger retail clinics that will offer many aspects of traditional primary care. Walmart will also be doing the same.
How many geographical areas will be affected is unknown. However,
“There will be more competition, no question,” said George Abraham, MD, MPH, president of the American College of Physicians.
Andrew Bazemore, MD, MPH, senior vice president of research and policy for the American Board of Family Medicine, agreed. “Seeing retail clinics finally embrace the promise of coordination and comprehensiveness in primary care is a promising step. It’s good to see CVS, Walmart, and Walgreens embracing the notion that they have to do more than just urgent care. On the flip side, it’s a source of competition for longstanding primary care clinics.”
Jeff Kagan, MD, an internist in Newington, Conn., noted that during the pandemic the booming demand for primary care has reduced competition from alternative care settings.
“But if this was not pandemic times, it would be very different. There are more urgent care walk-in clinics that do some primary care, and they are pulling away patients.”
New alternative care settings
The number of retail health centers has leveled off at around 2,000 clinics, about the same as in 2016. But CVS, which has around half that total, is now adding HealthHUB facilities, which offer nonemergency care. CVS had 800 of these quasi-primary care clinics in the first quarter of 2021 and planned to have 1,000 by the end of 2021, according to Managed Healthcare Executive.
Walgreens closed 150 of its retail clinics while partnering with VillageMD to develop 600 VillageMD clinics that are larger than its current in-store offices. The chain plans to build these clinics adjacent to Walgreens stores in 30 markets over the next 4 years. Currently, Walgreens has more than 50 VillageMD clinics, mostly in Sunbelt states.
Walmart opened the first of its new expanded-service clinics in 2019. Now it has clinics in Georgia, Arkansas, Texas, and Florida. These Walmart Health locations offer urgent care, primary care, labs, x-ray, and mental health therapy, as well as dental, optical, and hearing services.
The number of urgent care centers (UCCs), meanwhile, has mushroomed during the last decade. With the addition of 400-500 centers every year since 2014, there were 9,279 UCCs in the United States as of June 2019, according to the Urgent Care Association.
These UCCs usually have on-staff physicians. In contrast, most retail clinics are staffed by nurse practitioners. Another big difference is that in retail clinics, two-thirds of the patients – many of them young and healthy – have no regular primary care clinician; only a third of UCC patients don’t have a personal physician.
Because of these rootless patients, competition from retail clinics “is no big deal” to some primary care practices, said Ateev Mehrotra, MD, a Harvard Medical School professor in Boston who has studied alternative care settings. On the other hand, he asked, why do so few UCC patients have a regular physician? That raises the question of how many of these patients would go to a primary care office if there were no retail clinics or UCCs.
Economic pressure on practices
Dr. Grumet’s point about retail clinics and UCCs depriving his practice of easy, lucrative visits is widely echoed among his peers. The fee-for-service payment system based on Medicare rates exacerbates the problem. As Dr. Abraham pointed out, when primary care doctors see a higher percentage of patients with complicated problems, the doctors don’t get compensated fairly for those visits.
Minor acute care, Dr. Abraham noted, is “easier work for the same pay. When I review 100 pages of records for someone who was hospitalized and figure out their 10 different problems and 20 medications, I get paid virtually the same as if I treated a diabetic with a common cold or a foot laceration. The complexity of thought is not factored completely into the reimbursement. And we use the easier visits to offset the more complex ones.”
What happened to continuity of care?
The fragmentation of care between primary care practices and alternative care settings also “diminishes the primary care function,” Dr. Bazemore said.
“Primary care is supposed to be first contact, covering most of what a patient needs – comprehensive, coordinated, and continuous,” he observed. “When you fragment and separate an urgent care function from the rest, so it’s not done in the context of that first contact, you weaken the primary care component without enhancing its function.”
Observers doubt the advent of larger retail clinics that provide more services is likely to solve this problem. In Dr. Mehrotra’s view, CVS’ HealthHUBs “are all about supporting primary care. But are they really? Who are the patients supposed to come back to? This is a critical point: When you ask patients who’s in charge of their care, what are they going to say?”
Retail clinics and urgent care centers have a similar issue, Dr. Grumet said. “If you see patients in the office, and they have problems late at night, they can call you. There’s a continuity of care you don’t get in alternative care settings. The real goal in those places is to get patients in, assess them, and get them out. Which is fine – for minor things. But for someone who needs more comprehensive care, it’s not so good.”
This is why the ACP advised against the provision of chronic care in alternative care settings, said Dr. Abraham. “The problem with retail clinics is they’ve expanded into chronic care management in one or more episodes that require care, but not true continuity of care. When you go to a primary care physician’s office, we discuss more than just acute problems or chronic health issues; we talk about wellness, lifestyle, preventive services, vaccines, and your family. Relationship-building occurs, which transcends more than care interaction. In a setting where you get your care and you leave, longitudinal, holistic care doesn’t build.”
Dr. Kagan put it more succinctly: “Sometimes urgent care walk-in clinics get in over their head [with chronic care]. They like the guy who has high blood pressure and comes in once or twice a year for a prescription refill. But they’re not involved with the guy who has much more trouble.”
None of the urgent care doctors he knows of are taking long-term responsibility for their patients, Dr. Kagan added. “They don’t schedule follow-ups. They’ll see a patient for something, then say: ‘If you’re not better, come back and see me in a couple of weeks.’ ”
Two flavors of urgent care
Dr. Kagan has seen another type of doctor-patient relationship since he sold his practice to Hartford HealthCare 2 years ago. Hartford HealthCare owns 50% of an urgent care group called GoHealth.
“If our Hartford HealthCare patients can’t get into the office, we encourage them to go to a GoHealth facility,” he noted. “It’s not competition; it’s like one of our colleagues. We use the same EMR, so I can see everything that happens. I can even send someone who needs an x-ray to a GoHealth Center just for that.”
Moreover, GoHealth provides only urgent care. “So if it’s one of my patients, they refer them back to me for follow-up. And if somebody wanders in there without a primary care physician, they’ll hook them up with a Hartford HealthCare clinician.”
Dr. Bazemore has had a similar experience. He practices 1 day a week in his residency clinic in Fairfax, Va., which is owned by the Inova Health System. Inova created an adjoining urgent care facility that is open 7 days a week and uses the same EMR as Dr. Bazemore’s clinic.
This is the kind of relationship that Dr. Abraham would like to see between alternative care settings and traditional primary care practices: complementary rather than competitive. However, he questions the motives of hospital systems that own urgent care centers.
“Health care systems are starting these urgent care centers because they want to cash in on the same market,” he said. “I’m not convinced that their goal is to feed their primary care doctors. That is a potential advantage, but they also feed their specialists and try to blend procedures and other lucrative aspects of care into their system.”
What pharmacy chains are up to
Pharmacy chains have their own ulterior motives, Dr. Abraham noted. They built retail clinics for the same reason they sell drugs: to increase sales of consumer goods in their stores. Dr. Bazemore added that retail clinics also aim “to achieve a certain patient volume and incentivize what’s purchased in the pharmacy.”
Exacerbating the situation, CVS now owns Aetna, one of the biggest health insurers. Dr. Kagan believed that CVS’ new emphasis on HealthHUBs may be related to that. “CVS seems to be closing drugstores and opening up more primary care places, and now that they own Aetna, they’re trying to make Aetna patients go to CVS when they have a problem,” he said. Aetna patients are now required to fill their prescriptions at CVS.
Walmart has said it plans to open expanded-service clinics in locales that don’t have sufficient primary care, especially rural areas. The experts we consulted agree that Walmart won’t stop there if its new model is successful. In fact, Dr. Bazemore noted, competition from the new generation of in-store clinics is likely to be in areas where there are plenty of primary care doctors.
“For economic reasons, you’re going to see more of these clinics fill spaces where there’s already a sufficiency [of primary care] – starting with wealthy suburban areas,” Dr. Bazemore said. “Where you have a Walmart, Walgreens, or CVS, you tend to find more purchasers. I don’t know that it’s necessarily the answer to our access problems.”
What should primary care doctors do?
The obvious response of primary care practices to competition from retail clinics and urgent care centers that are open 7 days a week, 12 hours a day, is to expand their hours. In addition, they can introduce same-day scheduling or reserve a block of time every day for walk-in patients.
That’s the approach that Dr. Grumet took in his private practice. “When my patients called me, I tried to deal with it right away. So it was baffling that some of them went to retail clinics.”
Actually, it’s not so baffling, Dr. Abraham said, when you consider that retail clinics are part of a one-stop-shopping experience that will become even more all-encompassing in stores that add quasi-primary care clinics. “You can pick up the consumables you need, you can pick up prescriptions, and you can see your physician without having to make multiple stops. It’s a great idea for pharmacies.”
How about telemedicine? A lot of acute care similar to that provided in alternative care settings can be offered during virtual visits, noted Dr. Bazemore. However, the pharmacy chains have been providing telemedicine for years, using third-party services. And while the convenience of virtual visits appeals to some patients, that’s no guarantee they won’t go to retail clinics.
Reaching out to patients with reminders about the need for checkups and preventive visits, either by phone or through a patient portal, is another technique that practices can use to retain patients. A recent Press Ganey poll showed that people value this kind of communication. But it hardly seems sufficient to hold off the competitive assault of pharmacy chains.
A flaw in the pharmacies’ strategy, however, could eventually come back to bite them: Because the new, larger clinics don’t provide comprehensive care, people will eventually have to turn to traditional primary care – if it’s still around.
“Here’s the problem,” Dr. Grumet explained. “If you’re going to do [in-store primary care], you have to take ownership of the patient and manage everything. You have to be a full-fledged primary care practice with on-call hours and ER coverage. Otherwise, you’re taking bits and pieces – probably low-hanging fruit – to make money, and taking those away from the primary care practice. Which means you’re taking them from the people who should be doing the job.”
A version of this article first appeared on Medscape.com.
Jordan Grumet, MD, an internist in Northbrook, Ill., left his private practice about 2 years ago, partly because of competition from local retail clinics.
“We were always fighting the pharmacy clinics,” he said. “My generation of doctors was brought up to think we should have a one-stop shop. That was the idea behind being a primary care doctor. So it was very destructive to know your patients were going to another provider.”
Local retail clinics and urgent care centers were also co-opting many of the minor acute care visits that help primary care practices survive. “The number of visits for flu shots and simple medical problems drops,” said Dr. Grumet, who is now an end-of-life-care consultant and also works in hospices. “That can put downward economic pressure on primary care practices.”
Competition for primary care practices is ready to heat up even more, and the environment may soon become even more threatening for primary care doctors. Over the last year, the two largest pharmacy chains – CVS and Walgreens – announced their intentions to build larger retail clinics that will offer many aspects of traditional primary care. Walmart will also be doing the same.
How many geographical areas will be affected is unknown. However,
“There will be more competition, no question,” said George Abraham, MD, MPH, president of the American College of Physicians.
Andrew Bazemore, MD, MPH, senior vice president of research and policy for the American Board of Family Medicine, agreed. “Seeing retail clinics finally embrace the promise of coordination and comprehensiveness in primary care is a promising step. It’s good to see CVS, Walmart, and Walgreens embracing the notion that they have to do more than just urgent care. On the flip side, it’s a source of competition for longstanding primary care clinics.”
Jeff Kagan, MD, an internist in Newington, Conn., noted that during the pandemic the booming demand for primary care has reduced competition from alternative care settings.
“But if this was not pandemic times, it would be very different. There are more urgent care walk-in clinics that do some primary care, and they are pulling away patients.”
New alternative care settings
The number of retail health centers has leveled off at around 2,000 clinics, about the same as in 2016. But CVS, which has around half that total, is now adding HealthHUB facilities, which offer nonemergency care. CVS had 800 of these quasi-primary care clinics in the first quarter of 2021 and planned to have 1,000 by the end of 2021, according to Managed Healthcare Executive.
Walgreens closed 150 of its retail clinics while partnering with VillageMD to develop 600 VillageMD clinics that are larger than its current in-store offices. The chain plans to build these clinics adjacent to Walgreens stores in 30 markets over the next 4 years. Currently, Walgreens has more than 50 VillageMD clinics, mostly in Sunbelt states.
Walmart opened the first of its new expanded-service clinics in 2019. Now it has clinics in Georgia, Arkansas, Texas, and Florida. These Walmart Health locations offer urgent care, primary care, labs, x-ray, and mental health therapy, as well as dental, optical, and hearing services.
The number of urgent care centers (UCCs), meanwhile, has mushroomed during the last decade. With the addition of 400-500 centers every year since 2014, there were 9,279 UCCs in the United States as of June 2019, according to the Urgent Care Association.
These UCCs usually have on-staff physicians. In contrast, most retail clinics are staffed by nurse practitioners. Another big difference is that in retail clinics, two-thirds of the patients – many of them young and healthy – have no regular primary care clinician; only a third of UCC patients don’t have a personal physician.
Because of these rootless patients, competition from retail clinics “is no big deal” to some primary care practices, said Ateev Mehrotra, MD, a Harvard Medical School professor in Boston who has studied alternative care settings. On the other hand, he asked, why do so few UCC patients have a regular physician? That raises the question of how many of these patients would go to a primary care office if there were no retail clinics or UCCs.
Economic pressure on practices
Dr. Grumet’s point about retail clinics and UCCs depriving his practice of easy, lucrative visits is widely echoed among his peers. The fee-for-service payment system based on Medicare rates exacerbates the problem. As Dr. Abraham pointed out, when primary care doctors see a higher percentage of patients with complicated problems, the doctors don’t get compensated fairly for those visits.
Minor acute care, Dr. Abraham noted, is “easier work for the same pay. When I review 100 pages of records for someone who was hospitalized and figure out their 10 different problems and 20 medications, I get paid virtually the same as if I treated a diabetic with a common cold or a foot laceration. The complexity of thought is not factored completely into the reimbursement. And we use the easier visits to offset the more complex ones.”
What happened to continuity of care?
The fragmentation of care between primary care practices and alternative care settings also “diminishes the primary care function,” Dr. Bazemore said.
“Primary care is supposed to be first contact, covering most of what a patient needs – comprehensive, coordinated, and continuous,” he observed. “When you fragment and separate an urgent care function from the rest, so it’s not done in the context of that first contact, you weaken the primary care component without enhancing its function.”
Observers doubt the advent of larger retail clinics that provide more services is likely to solve this problem. In Dr. Mehrotra’s view, CVS’ HealthHUBs “are all about supporting primary care. But are they really? Who are the patients supposed to come back to? This is a critical point: When you ask patients who’s in charge of their care, what are they going to say?”
Retail clinics and urgent care centers have a similar issue, Dr. Grumet said. “If you see patients in the office, and they have problems late at night, they can call you. There’s a continuity of care you don’t get in alternative care settings. The real goal in those places is to get patients in, assess them, and get them out. Which is fine – for minor things. But for someone who needs more comprehensive care, it’s not so good.”
This is why the ACP advised against the provision of chronic care in alternative care settings, said Dr. Abraham. “The problem with retail clinics is they’ve expanded into chronic care management in one or more episodes that require care, but not true continuity of care. When you go to a primary care physician’s office, we discuss more than just acute problems or chronic health issues; we talk about wellness, lifestyle, preventive services, vaccines, and your family. Relationship-building occurs, which transcends more than care interaction. In a setting where you get your care and you leave, longitudinal, holistic care doesn’t build.”
Dr. Kagan put it more succinctly: “Sometimes urgent care walk-in clinics get in over their head [with chronic care]. They like the guy who has high blood pressure and comes in once or twice a year for a prescription refill. But they’re not involved with the guy who has much more trouble.”
None of the urgent care doctors he knows of are taking long-term responsibility for their patients, Dr. Kagan added. “They don’t schedule follow-ups. They’ll see a patient for something, then say: ‘If you’re not better, come back and see me in a couple of weeks.’ ”
Two flavors of urgent care
Dr. Kagan has seen another type of doctor-patient relationship since he sold his practice to Hartford HealthCare 2 years ago. Hartford HealthCare owns 50% of an urgent care group called GoHealth.
“If our Hartford HealthCare patients can’t get into the office, we encourage them to go to a GoHealth facility,” he noted. “It’s not competition; it’s like one of our colleagues. We use the same EMR, so I can see everything that happens. I can even send someone who needs an x-ray to a GoHealth Center just for that.”
Moreover, GoHealth provides only urgent care. “So if it’s one of my patients, they refer them back to me for follow-up. And if somebody wanders in there without a primary care physician, they’ll hook them up with a Hartford HealthCare clinician.”
Dr. Bazemore has had a similar experience. He practices 1 day a week in his residency clinic in Fairfax, Va., which is owned by the Inova Health System. Inova created an adjoining urgent care facility that is open 7 days a week and uses the same EMR as Dr. Bazemore’s clinic.
This is the kind of relationship that Dr. Abraham would like to see between alternative care settings and traditional primary care practices: complementary rather than competitive. However, he questions the motives of hospital systems that own urgent care centers.
“Health care systems are starting these urgent care centers because they want to cash in on the same market,” he said. “I’m not convinced that their goal is to feed their primary care doctors. That is a potential advantage, but they also feed their specialists and try to blend procedures and other lucrative aspects of care into their system.”
What pharmacy chains are up to
Pharmacy chains have their own ulterior motives, Dr. Abraham noted. They built retail clinics for the same reason they sell drugs: to increase sales of consumer goods in their stores. Dr. Bazemore added that retail clinics also aim “to achieve a certain patient volume and incentivize what’s purchased in the pharmacy.”
Exacerbating the situation, CVS now owns Aetna, one of the biggest health insurers. Dr. Kagan believed that CVS’ new emphasis on HealthHUBs may be related to that. “CVS seems to be closing drugstores and opening up more primary care places, and now that they own Aetna, they’re trying to make Aetna patients go to CVS when they have a problem,” he said. Aetna patients are now required to fill their prescriptions at CVS.
Walmart has said it plans to open expanded-service clinics in locales that don’t have sufficient primary care, especially rural areas. The experts we consulted agree that Walmart won’t stop there if its new model is successful. In fact, Dr. Bazemore noted, competition from the new generation of in-store clinics is likely to be in areas where there are plenty of primary care doctors.
“For economic reasons, you’re going to see more of these clinics fill spaces where there’s already a sufficiency [of primary care] – starting with wealthy suburban areas,” Dr. Bazemore said. “Where you have a Walmart, Walgreens, or CVS, you tend to find more purchasers. I don’t know that it’s necessarily the answer to our access problems.”
What should primary care doctors do?
The obvious response of primary care practices to competition from retail clinics and urgent care centers that are open 7 days a week, 12 hours a day, is to expand their hours. In addition, they can introduce same-day scheduling or reserve a block of time every day for walk-in patients.
That’s the approach that Dr. Grumet took in his private practice. “When my patients called me, I tried to deal with it right away. So it was baffling that some of them went to retail clinics.”
Actually, it’s not so baffling, Dr. Abraham said, when you consider that retail clinics are part of a one-stop-shopping experience that will become even more all-encompassing in stores that add quasi-primary care clinics. “You can pick up the consumables you need, you can pick up prescriptions, and you can see your physician without having to make multiple stops. It’s a great idea for pharmacies.”
How about telemedicine? A lot of acute care similar to that provided in alternative care settings can be offered during virtual visits, noted Dr. Bazemore. However, the pharmacy chains have been providing telemedicine for years, using third-party services. And while the convenience of virtual visits appeals to some patients, that’s no guarantee they won’t go to retail clinics.
Reaching out to patients with reminders about the need for checkups and preventive visits, either by phone or through a patient portal, is another technique that practices can use to retain patients. A recent Press Ganey poll showed that people value this kind of communication. But it hardly seems sufficient to hold off the competitive assault of pharmacy chains.
A flaw in the pharmacies’ strategy, however, could eventually come back to bite them: Because the new, larger clinics don’t provide comprehensive care, people will eventually have to turn to traditional primary care – if it’s still around.
“Here’s the problem,” Dr. Grumet explained. “If you’re going to do [in-store primary care], you have to take ownership of the patient and manage everything. You have to be a full-fledged primary care practice with on-call hours and ER coverage. Otherwise, you’re taking bits and pieces – probably low-hanging fruit – to make money, and taking those away from the primary care practice. Which means you’re taking them from the people who should be doing the job.”
A version of this article first appeared on Medscape.com.
COVID-19–associated ocular mucormycosis outbreak case study reveals high-risk group for deadly complication
Earlier this year, hospitals in India were dealing not only with the coronavirus pandemic but also with a surge in a potentially lethal fungal infection in patients previously treated for COVID-19. Mucormycosis, also known as black fungus, is typically a rare infection, but India had recorded more than 45,000 cases as of July 2021.
Now, a recent report suggests that patients with COVID-19–associated rhino-orbital cerebral mucormycosis (CAM) may have a higher mortality rate than previously estimated. The study was published Dec. 9 in JAMA Ophthalmology.
“The mortality indicators we observed, such as assisted ventilation and presence of severe orbital manifestations, can help physicians triage patients for emergency procedures, such as functional endoscopic sinus surgery (FESS), and administer systemic antifungal agents when in short supply,” the study authors wrote.
Mucormycosis usually infects immunocompromised patients. Previous research has found that poorly controlled diabetes – an epidemic in India – and use of high-dose systemic corticosteroids are two main risk factors for developing CAM. Even before COVID-19, India had a high incidence of mucormycosis compared to other countries, but cases exist around the world. In fact, on Dec. 17, the Centers for Disease Control and Prevention reported 10 isolated cases of COVID-19–associated mucormycosis identified in Arkansas hospitals between July and September 2021.
The disease can cause blurred vision, black lesions on the nose or inside of the mouth, and facial swelling. In rhino-orbital cerebral mucormycosis, extensive infection can necessitate orbital exenteration surgery, a disfiguring procedure that typically involves removal of the entire contents of the bony eye socket, as well as removal of the sinuses. Estimates for the mortality rate for this disease range from 14% to nearly 80%.
To better understand the cumulative morality rates for CAM and to identify additional risk factors, researchers reviewed the medical records of patients diagnosed and treated for CAM at a tertiary care multispecialty government hospital in Maharashtra, a state in the west-central region of India. The analysis included patients who died after admission or who had at minimum 30 days of documented follow-up. All diagnoses occurred between March 1 and May 30, 2021. All patients underwent comprehensive ophthalmic exams and routine blood workups.
Seventy-three patients were included in the study, with the average age of 53.5 years; 66% of the patients were male, and 74% of all patients had diabetes. Of the 47 individuals with available COVID-19 vaccination information, 89% had not had either shot of the vaccine, and 11% had the first dose. No patients in the cohort had received both doses of the vaccine; 87% of the patients were previously hospitalized for COVID-19, with 43 needing supplemental oxygen, 14 receiving noninvasive ventilation and ventilator support (NIV), and three requiring mechanical ventilation.
Patients developed CAM a median of 28 days after being discharged from the hospital for COVID-19 treatment; 26 patients died, 18 patients underwent FESS, and five underwent orbital exenteration. While 36% of patients died overall, the researchers found the cumulative probability of death from CAM rose from 26% at day 7 to 53% at day 21. They also found that the patients who died had more severe COVID-19, indicated by more days spent on supplemental oxygen (P = .003) and increased need for NIV or mechanical ventilation (P = .02) compared to patients who survived CAM. Those who died also had poorer visual acuity, with 35% of the group having no light perception during examination compared to 6% of surviving CAM patients (P = .02).
These findings are largely “confirmatory to what we previously knew, which is that [CAM] is a very bad disease with high morbidity and high mortality,” Ilan Schwartz, MD, PHD, an infectious disease physician at the University of Alberta, Edmonton, who researches emerging fungal infections, said in an interview. He was not involved with the research.
While larger studies looking at similar questions have been published, the new report has longer patient follow-up and is “better positioned to be able to estimate the mortality rate,” Dr. Schwartz noted. Even with 30 days of follow-up, “patients can have ongoing problems for many months, and so it’s possible that the true mortality rate is even higher, once you get beyond that period,” he added.
But Santosh G. Honavar, MD, the director of medical services at the Centre for Sight Eye Hospital in Hyderabad, India, also unaffiliated with the study, noted that the subset of patients included in the latest report may have had much more severe infection – and subsequently higher mortality rates – than a more generalized study in a broader patient population.
For example, a study by Mrittika Sen, PhD, Dr. Honavar, and their coauthors, published in the Indian Journal of Ophthalmology earlier this year, found a mortality rate of 14% when they examined the records of more than 2,800 patients across 102 treatment centers.
Taking that into account, “we believe that the actual mortality may be somewhere between the 14% reported by Sen et al. from the large Indian series and the 53% that we report at 3 weeks,” the JAMA Ophthalmology authors wrote.
Dr. Honavar also noted that the new report of severe infection outcomes identifies subgroups at higher risk of death due to CAM: those with severe COVID-19 infection or orbital disease. These groups “would need higher surveillance for mucormycosis, thus enabling early diagnosis and prompt initiation of amphotericin B upon diagnosis of mucormycosis,” he said in an interview. “These measures can possibly minimize the risk of death.”
Ongoing research on CAM cases will continue to inform knowledge and treatment of the disease, but there are still unanswered questions. “We still have a fairly unsatisfactory understanding of exactly why this [CAM] epidemic occurred and why it was so bad,” Dr. Schwartz noted. And while mucormycosis cases have seemed to drop off since the surge earlier this year, “I don’t think we’re out of the woods,” he added. “There’s a lot more awareness in India and around the world about this disease now, but we’re still quite vulnerable to seeing it again.”
Dr. Honavar is the editor-in-chief of the Indian Journal of Ophthalmology. Dr. Schwartz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Earlier this year, hospitals in India were dealing not only with the coronavirus pandemic but also with a surge in a potentially lethal fungal infection in patients previously treated for COVID-19. Mucormycosis, also known as black fungus, is typically a rare infection, but India had recorded more than 45,000 cases as of July 2021.
Now, a recent report suggests that patients with COVID-19–associated rhino-orbital cerebral mucormycosis (CAM) may have a higher mortality rate than previously estimated. The study was published Dec. 9 in JAMA Ophthalmology.
“The mortality indicators we observed, such as assisted ventilation and presence of severe orbital manifestations, can help physicians triage patients for emergency procedures, such as functional endoscopic sinus surgery (FESS), and administer systemic antifungal agents when in short supply,” the study authors wrote.
Mucormycosis usually infects immunocompromised patients. Previous research has found that poorly controlled diabetes – an epidemic in India – and use of high-dose systemic corticosteroids are two main risk factors for developing CAM. Even before COVID-19, India had a high incidence of mucormycosis compared to other countries, but cases exist around the world. In fact, on Dec. 17, the Centers for Disease Control and Prevention reported 10 isolated cases of COVID-19–associated mucormycosis identified in Arkansas hospitals between July and September 2021.
The disease can cause blurred vision, black lesions on the nose or inside of the mouth, and facial swelling. In rhino-orbital cerebral mucormycosis, extensive infection can necessitate orbital exenteration surgery, a disfiguring procedure that typically involves removal of the entire contents of the bony eye socket, as well as removal of the sinuses. Estimates for the mortality rate for this disease range from 14% to nearly 80%.
To better understand the cumulative morality rates for CAM and to identify additional risk factors, researchers reviewed the medical records of patients diagnosed and treated for CAM at a tertiary care multispecialty government hospital in Maharashtra, a state in the west-central region of India. The analysis included patients who died after admission or who had at minimum 30 days of documented follow-up. All diagnoses occurred between March 1 and May 30, 2021. All patients underwent comprehensive ophthalmic exams and routine blood workups.
Seventy-three patients were included in the study, with the average age of 53.5 years; 66% of the patients were male, and 74% of all patients had diabetes. Of the 47 individuals with available COVID-19 vaccination information, 89% had not had either shot of the vaccine, and 11% had the first dose. No patients in the cohort had received both doses of the vaccine; 87% of the patients were previously hospitalized for COVID-19, with 43 needing supplemental oxygen, 14 receiving noninvasive ventilation and ventilator support (NIV), and three requiring mechanical ventilation.
Patients developed CAM a median of 28 days after being discharged from the hospital for COVID-19 treatment; 26 patients died, 18 patients underwent FESS, and five underwent orbital exenteration. While 36% of patients died overall, the researchers found the cumulative probability of death from CAM rose from 26% at day 7 to 53% at day 21. They also found that the patients who died had more severe COVID-19, indicated by more days spent on supplemental oxygen (P = .003) and increased need for NIV or mechanical ventilation (P = .02) compared to patients who survived CAM. Those who died also had poorer visual acuity, with 35% of the group having no light perception during examination compared to 6% of surviving CAM patients (P = .02).
These findings are largely “confirmatory to what we previously knew, which is that [CAM] is a very bad disease with high morbidity and high mortality,” Ilan Schwartz, MD, PHD, an infectious disease physician at the University of Alberta, Edmonton, who researches emerging fungal infections, said in an interview. He was not involved with the research.
While larger studies looking at similar questions have been published, the new report has longer patient follow-up and is “better positioned to be able to estimate the mortality rate,” Dr. Schwartz noted. Even with 30 days of follow-up, “patients can have ongoing problems for many months, and so it’s possible that the true mortality rate is even higher, once you get beyond that period,” he added.
But Santosh G. Honavar, MD, the director of medical services at the Centre for Sight Eye Hospital in Hyderabad, India, also unaffiliated with the study, noted that the subset of patients included in the latest report may have had much more severe infection – and subsequently higher mortality rates – than a more generalized study in a broader patient population.
For example, a study by Mrittika Sen, PhD, Dr. Honavar, and their coauthors, published in the Indian Journal of Ophthalmology earlier this year, found a mortality rate of 14% when they examined the records of more than 2,800 patients across 102 treatment centers.
Taking that into account, “we believe that the actual mortality may be somewhere between the 14% reported by Sen et al. from the large Indian series and the 53% that we report at 3 weeks,” the JAMA Ophthalmology authors wrote.
Dr. Honavar also noted that the new report of severe infection outcomes identifies subgroups at higher risk of death due to CAM: those with severe COVID-19 infection or orbital disease. These groups “would need higher surveillance for mucormycosis, thus enabling early diagnosis and prompt initiation of amphotericin B upon diagnosis of mucormycosis,” he said in an interview. “These measures can possibly minimize the risk of death.”
Ongoing research on CAM cases will continue to inform knowledge and treatment of the disease, but there are still unanswered questions. “We still have a fairly unsatisfactory understanding of exactly why this [CAM] epidemic occurred and why it was so bad,” Dr. Schwartz noted. And while mucormycosis cases have seemed to drop off since the surge earlier this year, “I don’t think we’re out of the woods,” he added. “There’s a lot more awareness in India and around the world about this disease now, but we’re still quite vulnerable to seeing it again.”
Dr. Honavar is the editor-in-chief of the Indian Journal of Ophthalmology. Dr. Schwartz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Earlier this year, hospitals in India were dealing not only with the coronavirus pandemic but also with a surge in a potentially lethal fungal infection in patients previously treated for COVID-19. Mucormycosis, also known as black fungus, is typically a rare infection, but India had recorded more than 45,000 cases as of July 2021.
Now, a recent report suggests that patients with COVID-19–associated rhino-orbital cerebral mucormycosis (CAM) may have a higher mortality rate than previously estimated. The study was published Dec. 9 in JAMA Ophthalmology.
“The mortality indicators we observed, such as assisted ventilation and presence of severe orbital manifestations, can help physicians triage patients for emergency procedures, such as functional endoscopic sinus surgery (FESS), and administer systemic antifungal agents when in short supply,” the study authors wrote.
Mucormycosis usually infects immunocompromised patients. Previous research has found that poorly controlled diabetes – an epidemic in India – and use of high-dose systemic corticosteroids are two main risk factors for developing CAM. Even before COVID-19, India had a high incidence of mucormycosis compared to other countries, but cases exist around the world. In fact, on Dec. 17, the Centers for Disease Control and Prevention reported 10 isolated cases of COVID-19–associated mucormycosis identified in Arkansas hospitals between July and September 2021.
The disease can cause blurred vision, black lesions on the nose or inside of the mouth, and facial swelling. In rhino-orbital cerebral mucormycosis, extensive infection can necessitate orbital exenteration surgery, a disfiguring procedure that typically involves removal of the entire contents of the bony eye socket, as well as removal of the sinuses. Estimates for the mortality rate for this disease range from 14% to nearly 80%.
To better understand the cumulative morality rates for CAM and to identify additional risk factors, researchers reviewed the medical records of patients diagnosed and treated for CAM at a tertiary care multispecialty government hospital in Maharashtra, a state in the west-central region of India. The analysis included patients who died after admission or who had at minimum 30 days of documented follow-up. All diagnoses occurred between March 1 and May 30, 2021. All patients underwent comprehensive ophthalmic exams and routine blood workups.
Seventy-three patients were included in the study, with the average age of 53.5 years; 66% of the patients were male, and 74% of all patients had diabetes. Of the 47 individuals with available COVID-19 vaccination information, 89% had not had either shot of the vaccine, and 11% had the first dose. No patients in the cohort had received both doses of the vaccine; 87% of the patients were previously hospitalized for COVID-19, with 43 needing supplemental oxygen, 14 receiving noninvasive ventilation and ventilator support (NIV), and three requiring mechanical ventilation.
Patients developed CAM a median of 28 days after being discharged from the hospital for COVID-19 treatment; 26 patients died, 18 patients underwent FESS, and five underwent orbital exenteration. While 36% of patients died overall, the researchers found the cumulative probability of death from CAM rose from 26% at day 7 to 53% at day 21. They also found that the patients who died had more severe COVID-19, indicated by more days spent on supplemental oxygen (P = .003) and increased need for NIV or mechanical ventilation (P = .02) compared to patients who survived CAM. Those who died also had poorer visual acuity, with 35% of the group having no light perception during examination compared to 6% of surviving CAM patients (P = .02).
These findings are largely “confirmatory to what we previously knew, which is that [CAM] is a very bad disease with high morbidity and high mortality,” Ilan Schwartz, MD, PHD, an infectious disease physician at the University of Alberta, Edmonton, who researches emerging fungal infections, said in an interview. He was not involved with the research.
While larger studies looking at similar questions have been published, the new report has longer patient follow-up and is “better positioned to be able to estimate the mortality rate,” Dr. Schwartz noted. Even with 30 days of follow-up, “patients can have ongoing problems for many months, and so it’s possible that the true mortality rate is even higher, once you get beyond that period,” he added.
But Santosh G. Honavar, MD, the director of medical services at the Centre for Sight Eye Hospital in Hyderabad, India, also unaffiliated with the study, noted that the subset of patients included in the latest report may have had much more severe infection – and subsequently higher mortality rates – than a more generalized study in a broader patient population.
For example, a study by Mrittika Sen, PhD, Dr. Honavar, and their coauthors, published in the Indian Journal of Ophthalmology earlier this year, found a mortality rate of 14% when they examined the records of more than 2,800 patients across 102 treatment centers.
Taking that into account, “we believe that the actual mortality may be somewhere between the 14% reported by Sen et al. from the large Indian series and the 53% that we report at 3 weeks,” the JAMA Ophthalmology authors wrote.
Dr. Honavar also noted that the new report of severe infection outcomes identifies subgroups at higher risk of death due to CAM: those with severe COVID-19 infection or orbital disease. These groups “would need higher surveillance for mucormycosis, thus enabling early diagnosis and prompt initiation of amphotericin B upon diagnosis of mucormycosis,” he said in an interview. “These measures can possibly minimize the risk of death.”
Ongoing research on CAM cases will continue to inform knowledge and treatment of the disease, but there are still unanswered questions. “We still have a fairly unsatisfactory understanding of exactly why this [CAM] epidemic occurred and why it was so bad,” Dr. Schwartz noted. And while mucormycosis cases have seemed to drop off since the surge earlier this year, “I don’t think we’re out of the woods,” he added. “There’s a lot more awareness in India and around the world about this disease now, but we’re still quite vulnerable to seeing it again.”
Dr. Honavar is the editor-in-chief of the Indian Journal of Ophthalmology. Dr. Schwartz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA OPHTHALMOLOGY
COVID-19 vaccinations in people with HIV reflect general rates despite higher mortality risk, study says
Around the world, people with HIV show variations in COVID-19 vaccination rates similar to those seen in the general population, raising concerns because of their increased risk for morbidity and mortality from COVID-19 infection.
“To our knowledge, this analysis presents the first and largest investigation of vaccination rates among people with HIV,” reported the authors in research published in the Journal of Infectious Diseases.
The findings reflect data on nearly 7,000 people with HIV participating in the REPRIEVE clinical trial. As of July, COVID-19 vaccination rates ranged from a high of 71% in higher income regions to just 18% in sub-Saharan Africa and bottomed out at 0% in Haiti.
“This disparity in COVID-19 vaccination rates among people with HIV across income regions may increase morbidity from COVID-19 in the most vulnerable HIV populations,” the authors noted.
In general, people with HIV have been shown in recent research to have as much as 29% higher odds of morality from COVID-19 than the general population, and a 20% higher odds of hospitalization, hence their need for vaccination is especially pressing.
To understand the vaccination rates, the authors looked at data from the ongoing REPRIEVE trial, designed to investigate primary cardiovascular prevention worldwide among people with HIV. The trial includes data on COVID-19 vaccination status, providing a unique opportunity to capture those rates.
The study specifically included 6,952 people with HIV aged 40-75 years and on stable antiretroviral therapy (ART), without known cardiovascular disease, and a low to moderate atherosclerotic cardiovascular disease (ASCVD) risk.
The diverse participants with HIV were from 12 countries, including 66% who were people of color, as well as 32% women. Countries represented include Brazil (n = 1,042), Botswana (n = 273), Canada (n = 123), Haiti (n = 136), India (n = 469), Peru (n = 142), South Africa (n = 527), Spain (n = 198), Thailand (n = 582), Uganda (n = 175), United States (n = 3,162), and Zimbabwe (n = 123).
With vaccination defined as having received at least one vaccine shot, the overall cumulative COVID-19 vaccination rate in the study was 55% through July 2021.
By region, the highest cumulative rates were in the high-income countries of the United States and Canada (71%), followed by Latin America and the Caribbean (59%) – all consistent with the general population in these areas
Lower cumulative vaccination rates were observed in South Asia (49%), Southeast/East Asia (41%), and sub-Saharan Africa (18%), also reflecting the regional vaccination rates.
The United States had the highest country-specific COVID-19 vaccination rate of 72%, followed by Peru (69%) and Brazil (63%). Countries with the lowest vaccination rates were South Africa (18%), Uganda (3%), and Haiti (0%).
Of note, South Africa and Botswana have the largest share of deaths from HIV/AIDS, and both had very low COVID-19 vaccination rates in general, compared with high-income countries.
Overall, factors linked to the likelihood of being vaccinated included residing in the high-income U.S./Canada Global Burden of Disease superregion, as well as being White, male, older, having a higher body mass index (BMI), a higher ASCVD risk score, and longer duration of ART.
Participants’ decisions regarding COVID-19 vaccination in the study were made individually and were not based on any study-related recommendations or requirements, the authors noted.
Vaccination rates were higher among men than women in most regions, with the exception of sub-Saharan Africa. Vaccination rates were higher among Whites than Blacks in the U.S./Canada high-income region, with a high proportion of participants from the United States.
“It was surprising to us – and unfortunate – that in the high-income superregion vaccination rates were higher among individuals who identified as White than those who identified as Black and among men,” senior author Steven K. Grinspoon, MD, said in an interview.
“Given data for higher morbidity from COVID-19 among people of color with HIV, this disparity is likely to have significant public health implications,” said Dr. Grinspoon, a professor of medicine at Harvard Medical School and chief of the metabolism unit at Massachusetts General Hospital, both in Boston.
Newer data from the REPRIEVE study through October has shown continued steady increases in the cumulative vaccination rates in all regions, Dr. Grinspoon noted, with the largest increases in the Southeast/East Asia, South Asia, and sub-Saharan Africa, whereas a leveling off of rates was observed in the high-income regions.
Overall, “it is encouraging that rates among people with HIV are similar to and, in many regions, higher than the general population,” Dr. Grinspoon said.
However, with the data showing a higher risk for COVID-19 death in people with HIV, “it is critical that people with HIV, representing a vulnerable and immunocompromised population, be vaccinated for COVID-19,” Dr. Grinspoon said.
Commenting on the study, Monica Gandhi, MD, MPH, director of the Gladstone Center for AIDS Research at the University of California, San Francisco, agreed that “it is encouraging that these rates are as high as the general population, showing that there is not excess hesitancy among those living with HIV.”
Unlike other immunocompromised groups, people with HIV were not necessarily prioritized for vaccination, since antiretroviral therapy can reconstitute the immune system, “so I am not surprised the [vaccination] rates aren’t higher,” Dr. Gandhi, who was not involved with the study, said in an interview.
Nevertheless, “it is important that those with risk factors for more severe disease, such as higher BMI and higher cardiovascular disease, are prioritized for COVID-19 vaccination, [as] these are important groups in which to increase rates,” she said.
“The take-home message is that we have to increase our rates of vaccination in this critically important population,” Dr. Gandhi emphasized. “Global vaccine equity is paramount given that the burden of HIV infections remains in sub-Saharan Africa.”
The study received support from the National Institutes of Health and funding from Kowa Pharmaceuticals and Gilead Sciences. The authors and Dr. Gandhi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Around the world, people with HIV show variations in COVID-19 vaccination rates similar to those seen in the general population, raising concerns because of their increased risk for morbidity and mortality from COVID-19 infection.
“To our knowledge, this analysis presents the first and largest investigation of vaccination rates among people with HIV,” reported the authors in research published in the Journal of Infectious Diseases.
The findings reflect data on nearly 7,000 people with HIV participating in the REPRIEVE clinical trial. As of July, COVID-19 vaccination rates ranged from a high of 71% in higher income regions to just 18% in sub-Saharan Africa and bottomed out at 0% in Haiti.
“This disparity in COVID-19 vaccination rates among people with HIV across income regions may increase morbidity from COVID-19 in the most vulnerable HIV populations,” the authors noted.
In general, people with HIV have been shown in recent research to have as much as 29% higher odds of morality from COVID-19 than the general population, and a 20% higher odds of hospitalization, hence their need for vaccination is especially pressing.
To understand the vaccination rates, the authors looked at data from the ongoing REPRIEVE trial, designed to investigate primary cardiovascular prevention worldwide among people with HIV. The trial includes data on COVID-19 vaccination status, providing a unique opportunity to capture those rates.
The study specifically included 6,952 people with HIV aged 40-75 years and on stable antiretroviral therapy (ART), without known cardiovascular disease, and a low to moderate atherosclerotic cardiovascular disease (ASCVD) risk.
The diverse participants with HIV were from 12 countries, including 66% who were people of color, as well as 32% women. Countries represented include Brazil (n = 1,042), Botswana (n = 273), Canada (n = 123), Haiti (n = 136), India (n = 469), Peru (n = 142), South Africa (n = 527), Spain (n = 198), Thailand (n = 582), Uganda (n = 175), United States (n = 3,162), and Zimbabwe (n = 123).
With vaccination defined as having received at least one vaccine shot, the overall cumulative COVID-19 vaccination rate in the study was 55% through July 2021.
By region, the highest cumulative rates were in the high-income countries of the United States and Canada (71%), followed by Latin America and the Caribbean (59%) – all consistent with the general population in these areas
Lower cumulative vaccination rates were observed in South Asia (49%), Southeast/East Asia (41%), and sub-Saharan Africa (18%), also reflecting the regional vaccination rates.
The United States had the highest country-specific COVID-19 vaccination rate of 72%, followed by Peru (69%) and Brazil (63%). Countries with the lowest vaccination rates were South Africa (18%), Uganda (3%), and Haiti (0%).
Of note, South Africa and Botswana have the largest share of deaths from HIV/AIDS, and both had very low COVID-19 vaccination rates in general, compared with high-income countries.
Overall, factors linked to the likelihood of being vaccinated included residing in the high-income U.S./Canada Global Burden of Disease superregion, as well as being White, male, older, having a higher body mass index (BMI), a higher ASCVD risk score, and longer duration of ART.
Participants’ decisions regarding COVID-19 vaccination in the study were made individually and were not based on any study-related recommendations or requirements, the authors noted.
Vaccination rates were higher among men than women in most regions, with the exception of sub-Saharan Africa. Vaccination rates were higher among Whites than Blacks in the U.S./Canada high-income region, with a high proportion of participants from the United States.
“It was surprising to us – and unfortunate – that in the high-income superregion vaccination rates were higher among individuals who identified as White than those who identified as Black and among men,” senior author Steven K. Grinspoon, MD, said in an interview.
“Given data for higher morbidity from COVID-19 among people of color with HIV, this disparity is likely to have significant public health implications,” said Dr. Grinspoon, a professor of medicine at Harvard Medical School and chief of the metabolism unit at Massachusetts General Hospital, both in Boston.
Newer data from the REPRIEVE study through October has shown continued steady increases in the cumulative vaccination rates in all regions, Dr. Grinspoon noted, with the largest increases in the Southeast/East Asia, South Asia, and sub-Saharan Africa, whereas a leveling off of rates was observed in the high-income regions.
Overall, “it is encouraging that rates among people with HIV are similar to and, in many regions, higher than the general population,” Dr. Grinspoon said.
However, with the data showing a higher risk for COVID-19 death in people with HIV, “it is critical that people with HIV, representing a vulnerable and immunocompromised population, be vaccinated for COVID-19,” Dr. Grinspoon said.
Commenting on the study, Monica Gandhi, MD, MPH, director of the Gladstone Center for AIDS Research at the University of California, San Francisco, agreed that “it is encouraging that these rates are as high as the general population, showing that there is not excess hesitancy among those living with HIV.”
Unlike other immunocompromised groups, people with HIV were not necessarily prioritized for vaccination, since antiretroviral therapy can reconstitute the immune system, “so I am not surprised the [vaccination] rates aren’t higher,” Dr. Gandhi, who was not involved with the study, said in an interview.
Nevertheless, “it is important that those with risk factors for more severe disease, such as higher BMI and higher cardiovascular disease, are prioritized for COVID-19 vaccination, [as] these are important groups in which to increase rates,” she said.
“The take-home message is that we have to increase our rates of vaccination in this critically important population,” Dr. Gandhi emphasized. “Global vaccine equity is paramount given that the burden of HIV infections remains in sub-Saharan Africa.”
The study received support from the National Institutes of Health and funding from Kowa Pharmaceuticals and Gilead Sciences. The authors and Dr. Gandhi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Around the world, people with HIV show variations in COVID-19 vaccination rates similar to those seen in the general population, raising concerns because of their increased risk for morbidity and mortality from COVID-19 infection.
“To our knowledge, this analysis presents the first and largest investigation of vaccination rates among people with HIV,” reported the authors in research published in the Journal of Infectious Diseases.
The findings reflect data on nearly 7,000 people with HIV participating in the REPRIEVE clinical trial. As of July, COVID-19 vaccination rates ranged from a high of 71% in higher income regions to just 18% in sub-Saharan Africa and bottomed out at 0% in Haiti.
“This disparity in COVID-19 vaccination rates among people with HIV across income regions may increase morbidity from COVID-19 in the most vulnerable HIV populations,” the authors noted.
In general, people with HIV have been shown in recent research to have as much as 29% higher odds of morality from COVID-19 than the general population, and a 20% higher odds of hospitalization, hence their need for vaccination is especially pressing.
To understand the vaccination rates, the authors looked at data from the ongoing REPRIEVE trial, designed to investigate primary cardiovascular prevention worldwide among people with HIV. The trial includes data on COVID-19 vaccination status, providing a unique opportunity to capture those rates.
The study specifically included 6,952 people with HIV aged 40-75 years and on stable antiretroviral therapy (ART), without known cardiovascular disease, and a low to moderate atherosclerotic cardiovascular disease (ASCVD) risk.
The diverse participants with HIV were from 12 countries, including 66% who were people of color, as well as 32% women. Countries represented include Brazil (n = 1,042), Botswana (n = 273), Canada (n = 123), Haiti (n = 136), India (n = 469), Peru (n = 142), South Africa (n = 527), Spain (n = 198), Thailand (n = 582), Uganda (n = 175), United States (n = 3,162), and Zimbabwe (n = 123).
With vaccination defined as having received at least one vaccine shot, the overall cumulative COVID-19 vaccination rate in the study was 55% through July 2021.
By region, the highest cumulative rates were in the high-income countries of the United States and Canada (71%), followed by Latin America and the Caribbean (59%) – all consistent with the general population in these areas
Lower cumulative vaccination rates were observed in South Asia (49%), Southeast/East Asia (41%), and sub-Saharan Africa (18%), also reflecting the regional vaccination rates.
The United States had the highest country-specific COVID-19 vaccination rate of 72%, followed by Peru (69%) and Brazil (63%). Countries with the lowest vaccination rates were South Africa (18%), Uganda (3%), and Haiti (0%).
Of note, South Africa and Botswana have the largest share of deaths from HIV/AIDS, and both had very low COVID-19 vaccination rates in general, compared with high-income countries.
Overall, factors linked to the likelihood of being vaccinated included residing in the high-income U.S./Canada Global Burden of Disease superregion, as well as being White, male, older, having a higher body mass index (BMI), a higher ASCVD risk score, and longer duration of ART.
Participants’ decisions regarding COVID-19 vaccination in the study were made individually and were not based on any study-related recommendations or requirements, the authors noted.
Vaccination rates were higher among men than women in most regions, with the exception of sub-Saharan Africa. Vaccination rates were higher among Whites than Blacks in the U.S./Canada high-income region, with a high proportion of participants from the United States.
“It was surprising to us – and unfortunate – that in the high-income superregion vaccination rates were higher among individuals who identified as White than those who identified as Black and among men,” senior author Steven K. Grinspoon, MD, said in an interview.
“Given data for higher morbidity from COVID-19 among people of color with HIV, this disparity is likely to have significant public health implications,” said Dr. Grinspoon, a professor of medicine at Harvard Medical School and chief of the metabolism unit at Massachusetts General Hospital, both in Boston.
Newer data from the REPRIEVE study through October has shown continued steady increases in the cumulative vaccination rates in all regions, Dr. Grinspoon noted, with the largest increases in the Southeast/East Asia, South Asia, and sub-Saharan Africa, whereas a leveling off of rates was observed in the high-income regions.
Overall, “it is encouraging that rates among people with HIV are similar to and, in many regions, higher than the general population,” Dr. Grinspoon said.
However, with the data showing a higher risk for COVID-19 death in people with HIV, “it is critical that people with HIV, representing a vulnerable and immunocompromised population, be vaccinated for COVID-19,” Dr. Grinspoon said.
Commenting on the study, Monica Gandhi, MD, MPH, director of the Gladstone Center for AIDS Research at the University of California, San Francisco, agreed that “it is encouraging that these rates are as high as the general population, showing that there is not excess hesitancy among those living with HIV.”
Unlike other immunocompromised groups, people with HIV were not necessarily prioritized for vaccination, since antiretroviral therapy can reconstitute the immune system, “so I am not surprised the [vaccination] rates aren’t higher,” Dr. Gandhi, who was not involved with the study, said in an interview.
Nevertheless, “it is important that those with risk factors for more severe disease, such as higher BMI and higher cardiovascular disease, are prioritized for COVID-19 vaccination, [as] these are important groups in which to increase rates,” she said.
“The take-home message is that we have to increase our rates of vaccination in this critically important population,” Dr. Gandhi emphasized. “Global vaccine equity is paramount given that the burden of HIV infections remains in sub-Saharan Africa.”
The study received support from the National Institutes of Health and funding from Kowa Pharmaceuticals and Gilead Sciences. The authors and Dr. Gandhi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF INFECTIOUS DISEASES
COVID booster protection may wane in about 10 weeks, new data show
, according to new data from Britain.
U.K. health officials shared the data just before Christmas and noted that there haven’t been enough severe cases of the Omicron variant to calculate how well boosters protect against severe disease. But they believe the extra shots provide significant protection against hospitalization and death.
“It will be a few weeks before effectiveness against severe disease with Omicron can be estimated,” U.K. Health Security Agency officials wrote in the report. “However, based on experience with previous variants, this is likely to be substantially higher than the estimates against symptomatic disease.”
Since countries began reporting Omicron cases in November, multiple studies have suggested the variant is better at escaping antibodies from vaccination and previous infection, according to the New York Times. The U.K. report adds to that, noting that both the initial vaccine series and booster doses were less effective and faded faster against the Omicron variant than the Delta variant.
Among those who received two doses of the AstraZeneca vaccine, a booster of the Pfizer or Moderna vaccine was 60% effective at preventing symptomatic disease 2 to 4 weeks after the shot. But after 10 weeks, the Pfizer booster was 35% effective, and the Moderna booster was 45% effective. (The AstraZeneca vaccine is not authorized in the United States, but the Johnson & Johnson shot uses a similar technology, the New York Times reported.)
Among those who received three Pfizer doses, vaccine effectiveness was 70% about a week after the booster but dropped to 45% after 10 weeks. At the same time, those who received an initial two-dose series of the Pfizer vaccine and then a Moderna booster seemed to have 75% effectiveness up to 9 weeks.
The report was based on an analysis of 148,000 Delta cases and 68,000 Omicron cases in the United Kingdom through Dec. 20. So far, the U.K. health officials wrote, Omicron infections appear to be less severe and less likely to lead to hospitalization than Delta infections. At that time, 132 people with lab-confirmed Omicron had been admitted to hospitals, and 14 deaths had been reported among ages 52-96.
“This analysis is preliminary because of the small numbers of Omicron cases currently in hospital and the limited spread of Omicron into older age groups as yet,” the report said.
The reinfection rate has also increased for the Omicron variant, the report found. Among the 116,000 people who had an Omicron infection, about 11,000 -- or 9.5% -- were linked to a previously confirmed infection, which is likely an undercount of reinfections. In the data analyzed, 69 Omicron cases were a third episode of COVID-19 infection, and 290 cases occurred 60-89 days after a first infection.
A version of this article first appeared on WebMD.com.
, according to new data from Britain.
U.K. health officials shared the data just before Christmas and noted that there haven’t been enough severe cases of the Omicron variant to calculate how well boosters protect against severe disease. But they believe the extra shots provide significant protection against hospitalization and death.
“It will be a few weeks before effectiveness against severe disease with Omicron can be estimated,” U.K. Health Security Agency officials wrote in the report. “However, based on experience with previous variants, this is likely to be substantially higher than the estimates against symptomatic disease.”
Since countries began reporting Omicron cases in November, multiple studies have suggested the variant is better at escaping antibodies from vaccination and previous infection, according to the New York Times. The U.K. report adds to that, noting that both the initial vaccine series and booster doses were less effective and faded faster against the Omicron variant than the Delta variant.
Among those who received two doses of the AstraZeneca vaccine, a booster of the Pfizer or Moderna vaccine was 60% effective at preventing symptomatic disease 2 to 4 weeks after the shot. But after 10 weeks, the Pfizer booster was 35% effective, and the Moderna booster was 45% effective. (The AstraZeneca vaccine is not authorized in the United States, but the Johnson & Johnson shot uses a similar technology, the New York Times reported.)
Among those who received three Pfizer doses, vaccine effectiveness was 70% about a week after the booster but dropped to 45% after 10 weeks. At the same time, those who received an initial two-dose series of the Pfizer vaccine and then a Moderna booster seemed to have 75% effectiveness up to 9 weeks.
The report was based on an analysis of 148,000 Delta cases and 68,000 Omicron cases in the United Kingdom through Dec. 20. So far, the U.K. health officials wrote, Omicron infections appear to be less severe and less likely to lead to hospitalization than Delta infections. At that time, 132 people with lab-confirmed Omicron had been admitted to hospitals, and 14 deaths had been reported among ages 52-96.
“This analysis is preliminary because of the small numbers of Omicron cases currently in hospital and the limited spread of Omicron into older age groups as yet,” the report said.
The reinfection rate has also increased for the Omicron variant, the report found. Among the 116,000 people who had an Omicron infection, about 11,000 -- or 9.5% -- were linked to a previously confirmed infection, which is likely an undercount of reinfections. In the data analyzed, 69 Omicron cases were a third episode of COVID-19 infection, and 290 cases occurred 60-89 days after a first infection.
A version of this article first appeared on WebMD.com.
, according to new data from Britain.
U.K. health officials shared the data just before Christmas and noted that there haven’t been enough severe cases of the Omicron variant to calculate how well boosters protect against severe disease. But they believe the extra shots provide significant protection against hospitalization and death.
“It will be a few weeks before effectiveness against severe disease with Omicron can be estimated,” U.K. Health Security Agency officials wrote in the report. “However, based on experience with previous variants, this is likely to be substantially higher than the estimates against symptomatic disease.”
Since countries began reporting Omicron cases in November, multiple studies have suggested the variant is better at escaping antibodies from vaccination and previous infection, according to the New York Times. The U.K. report adds to that, noting that both the initial vaccine series and booster doses were less effective and faded faster against the Omicron variant than the Delta variant.
Among those who received two doses of the AstraZeneca vaccine, a booster of the Pfizer or Moderna vaccine was 60% effective at preventing symptomatic disease 2 to 4 weeks after the shot. But after 10 weeks, the Pfizer booster was 35% effective, and the Moderna booster was 45% effective. (The AstraZeneca vaccine is not authorized in the United States, but the Johnson & Johnson shot uses a similar technology, the New York Times reported.)
Among those who received three Pfizer doses, vaccine effectiveness was 70% about a week after the booster but dropped to 45% after 10 weeks. At the same time, those who received an initial two-dose series of the Pfizer vaccine and then a Moderna booster seemed to have 75% effectiveness up to 9 weeks.
The report was based on an analysis of 148,000 Delta cases and 68,000 Omicron cases in the United Kingdom through Dec. 20. So far, the U.K. health officials wrote, Omicron infections appear to be less severe and less likely to lead to hospitalization than Delta infections. At that time, 132 people with lab-confirmed Omicron had been admitted to hospitals, and 14 deaths had been reported among ages 52-96.
“This analysis is preliminary because of the small numbers of Omicron cases currently in hospital and the limited spread of Omicron into older age groups as yet,” the report said.
The reinfection rate has also increased for the Omicron variant, the report found. Among the 116,000 people who had an Omicron infection, about 11,000 -- or 9.5% -- were linked to a previously confirmed infection, which is likely an undercount of reinfections. In the data analyzed, 69 Omicron cases were a third episode of COVID-19 infection, and 290 cases occurred 60-89 days after a first infection.
A version of this article first appeared on WebMD.com.
Remdesivir may keep unvaccinated out of the hospital: Study
The antiviral remdesivir, an intravenous drug given mostly to seriously ill COVID-19 patients in hospitals, could keep unvaccinated people who become infected out of the hospital if given on an outpatient basis, a new study says.
Researchers studied 562 unvaccinated people from September 2020 to April 2021, according to the study published in the New England Journal of Medicine. The study determined the risk of hospitalization or death was 87% lower in study participants who were given remdesivir than participants who received a placebo.
All participants were at high risk of developing severe COVID-19 because of their age – they were over 60 – or because they had an underlying medical condition such as diabetes or obesity.
An important caveat: The findings are based on data collected before the Delta variant surged in the summer of 2021 or the Omicron variant surged late in the year, the Washington Post reported.
The new study says the drug could be helpful in keeping vaccinated as well as unvaccinated people out of the hospital – an important factor as the Omicron surge threatens to overwhelm health systems around the world.
Remdesivir could be a boon for COVID-19 patients in parts of the world that don’t have vaccines or for patients with immunocompromised systems.
“These data provide evidence that a 3-day course of remdesivir could play a critical role in helping COVID-19 patients stay out of the hospital,” Robert L. Gottlieb, MD, PhD, the therapeutic lead for COVID-19 research at Baylor Scott & White Health in Dallas, said in a news release from Gilead Pharmaceuticals. “While our hospitals are ready to assist patients in need, prevention and early intervention are preferable to reduce the risk of disease progression and allow patients not requiring oxygen to recover from home when appropriate.”
Remdesivir was the first antiviral for COVID-19 authorized by the Food and Drug Administration. It was given to then-President Donald Trump when he was hospitalized with COVID-19 in October 2020.
Gilead released the study findings in September.
A version of this article first appeared on WebMD.com.
The antiviral remdesivir, an intravenous drug given mostly to seriously ill COVID-19 patients in hospitals, could keep unvaccinated people who become infected out of the hospital if given on an outpatient basis, a new study says.
Researchers studied 562 unvaccinated people from September 2020 to April 2021, according to the study published in the New England Journal of Medicine. The study determined the risk of hospitalization or death was 87% lower in study participants who were given remdesivir than participants who received a placebo.
All participants were at high risk of developing severe COVID-19 because of their age – they were over 60 – or because they had an underlying medical condition such as diabetes or obesity.
An important caveat: The findings are based on data collected before the Delta variant surged in the summer of 2021 or the Omicron variant surged late in the year, the Washington Post reported.
The new study says the drug could be helpful in keeping vaccinated as well as unvaccinated people out of the hospital – an important factor as the Omicron surge threatens to overwhelm health systems around the world.
Remdesivir could be a boon for COVID-19 patients in parts of the world that don’t have vaccines or for patients with immunocompromised systems.
“These data provide evidence that a 3-day course of remdesivir could play a critical role in helping COVID-19 patients stay out of the hospital,” Robert L. Gottlieb, MD, PhD, the therapeutic lead for COVID-19 research at Baylor Scott & White Health in Dallas, said in a news release from Gilead Pharmaceuticals. “While our hospitals are ready to assist patients in need, prevention and early intervention are preferable to reduce the risk of disease progression and allow patients not requiring oxygen to recover from home when appropriate.”
Remdesivir was the first antiviral for COVID-19 authorized by the Food and Drug Administration. It was given to then-President Donald Trump when he was hospitalized with COVID-19 in October 2020.
Gilead released the study findings in September.
A version of this article first appeared on WebMD.com.
The antiviral remdesivir, an intravenous drug given mostly to seriously ill COVID-19 patients in hospitals, could keep unvaccinated people who become infected out of the hospital if given on an outpatient basis, a new study says.
Researchers studied 562 unvaccinated people from September 2020 to April 2021, according to the study published in the New England Journal of Medicine. The study determined the risk of hospitalization or death was 87% lower in study participants who were given remdesivir than participants who received a placebo.
All participants were at high risk of developing severe COVID-19 because of their age – they were over 60 – or because they had an underlying medical condition such as diabetes or obesity.
An important caveat: The findings are based on data collected before the Delta variant surged in the summer of 2021 or the Omicron variant surged late in the year, the Washington Post reported.
The new study says the drug could be helpful in keeping vaccinated as well as unvaccinated people out of the hospital – an important factor as the Omicron surge threatens to overwhelm health systems around the world.
Remdesivir could be a boon for COVID-19 patients in parts of the world that don’t have vaccines or for patients with immunocompromised systems.
“These data provide evidence that a 3-day course of remdesivir could play a critical role in helping COVID-19 patients stay out of the hospital,” Robert L. Gottlieb, MD, PhD, the therapeutic lead for COVID-19 research at Baylor Scott & White Health in Dallas, said in a news release from Gilead Pharmaceuticals. “While our hospitals are ready to assist patients in need, prevention and early intervention are preferable to reduce the risk of disease progression and allow patients not requiring oxygen to recover from home when appropriate.”
Remdesivir was the first antiviral for COVID-19 authorized by the Food and Drug Administration. It was given to then-President Donald Trump when he was hospitalized with COVID-19 in October 2020.
Gilead released the study findings in September.
A version of this article first appeared on WebMD.com.
ADA standards of care 2022: Screen more, personalize, use technology
The American Diabetes Association’s updated clinical recommendations for 2022 call for wider population screening, along with furthering the trends toward individualization of care use of diabetes technology.

The summary of changes from 2021 spans four pages. “Diabetes is a really dynamic field so there is a lot to update which is good. It means progress,” ADA chief science and medical officer Robert A. Gabbay, MD, PhD, told this news organization.
The ADA Standards of Medical Care in Diabetes – 2022 was published Dec. 20, 2021, online as a supplement to Diabetes Care.
Screening widened by age, in pregnancy, and for type 1 diabetes
One dramatic change is a drop in age to begin screening all people for prediabetes and diabetes from 45 years to 35 years, regardless of risk factors such as obesity.
“Sadly, there are increasing numbers of people with diabetes and developing diabetes younger,” Dr. Gabbay said.
In August 2021, the U.S. Preventive Services Task Force dropped its recommended age of diabetes screening from 40 to 35 years for people with overweight or obesity, but not universally, as ADA now has.
The ADA made its recommendation independently, Dr. Gabbay noted.
The recommendation for testing pregnant women early in gestation (<15 weeks) for preexisting diabetes was also expanded, from just those with risk factors to consideration of testing all women for undiagnosed diabetes at the time they’re planning pregnancy, and if not then, at the first prenatal visit. Screening for gestational diabetes is then performed at 24-28 weeks.
Again, this is caused by increasing diabetes onset at younger ages, Dr. Gabbay said. “We’re well aware that the number of women who have diabetes and don’t know it and become pregnant is significant and therefore screening early on is important.”
New guidance regarding autoantibody screening in adults suspected of having type 1 diabetes and genetic testing for those who don’t fit typical criteria for either of the two main types are based on the ADA/European Association for the Study of Diabetes joint consensus statement on type 1 diabetes in adults.
Individualization of care based on comorbidities, other factors
The concept of individualization of care in diabetes has been emphasized for several years now, but continues to be enhanced with new data and newly available management tools.
Regarding management of type 2 diabetes, several charts have been included to help guide decision-making.
One lists drug-specific and patient factors, including comorbidities, to consider when selecting glucose-lowering medications. A new table depicts a building with four “pillars,” for complication risk reduction, including management of blood pressure, lipids, and glucose, as well as use of agents with cardiovascular and kidney benefit.
“On the type 2 side, the choice of therapy is really guided by several factors. We lay them out in a nice diagram. ... A lot of useful information there compares classes of drugs in order to help clinicians make decisions on what would be the appropriate therapy for a given individual,” Dr. Gabbay said.
An algorithm for pharmacologic treatment includes considerations of weight, hypoglycemia, and cost. Tables are also provided listing average wholesale prices of insulins and noninsulin medications.
A section now entitled “Obesity and weight management for the prevention and treatment of type 2 diabetes” has added content regarding the importance of addressing obesity in diabetes, particularly in the context of the COVID-19 pandemic, and the addition of semaglutide as an approved obesity treatment.
“What we hope is that this engenders a shared decision-making process with the patient to identify what the goals are and then choose the appropriate therapy for those goals,” Dr. Gabbay said.
New information has also been added about management of nonalcoholic fatty liver disease. “I think that’s one of the unrecognized and unaddressed complications of diabetes that we’ll see in the future, particularly as new therapies come out,” Dr. Gabbay predicted.
The section on cardiovascular disease and risk management, endorsed for the fourth year in a row by the American College of Cardiology, includes several new recommendations, including diagnosis of hypertension at a single visit if blood pressure is 180/110 mm Hg or greater, and individualization of blood pressure targets.
Chronic kidney disease management has now been separated from other microvascular complications into a standalone section, with several new updates. Retinopathy, neuropathy, and foot care remain combined in one section.
Diabetes technology: Rapidly evolving, access an issue
The new technology section “doubles down on the time in [normal glucose] range (TIR) concept,” but also emphasizes the importance of time below range.
“When we see that, we need to make a therapeutic change. We were concerned that as there’s more and more information and numbers, users might not pick up on what’s important,” Dr. Gabbay noted.
The new standards also provides greater affirmation of the value of continuous glucose monitoring (CGM) for people with both type 1 and type 2 diabetes at any age, with individualized choice of devices.
Access to technology is a “big issue, and something the ADA has really been fighting for, particularly in terms of health disparities,” Dr. Gabbay said, noting that ADA has a new Health Equity Now platform, which includes a “bill of rights” calling for all patients with diabetes to have access to state-of-the-art technologies, including CGM.
Overall, he said, “I think the big picture is diabetes continues to evolve and advance. After careful review of the literature, the standards of care identifies at least four big areas where there are some changes that clinicians need to know about: screening, how to individualize treatment, considerations of comorbidities, and the important role that technology plays.”
Dr. Gabbay is an employee of the ADA.
A version of this article first appeared on Medscape.com.
The American Diabetes Association’s updated clinical recommendations for 2022 call for wider population screening, along with furthering the trends toward individualization of care use of diabetes technology.
The summary of changes from 2021 spans four pages. “Diabetes is a really dynamic field so there is a lot to update which is good. It means progress,” ADA chief science and medical officer Robert A. Gabbay, MD, PhD, told this news organization.
The ADA Standards of Medical Care in Diabetes – 2022 was published Dec. 20, 2021, online as a supplement to Diabetes Care.
Screening widened by age, in pregnancy, and for type 1 diabetes
One dramatic change is a drop in age to begin screening all people for prediabetes and diabetes from 45 years to 35 years, regardless of risk factors such as obesity.
“Sadly, there are increasing numbers of people with diabetes and developing diabetes younger,” Dr. Gabbay said.
In August 2021, the U.S. Preventive Services Task Force dropped its recommended age of diabetes screening from 40 to 35 years for people with overweight or obesity, but not universally, as ADA now has.
The ADA made its recommendation independently, Dr. Gabbay noted.
The recommendation for testing pregnant women early in gestation (<15 weeks) for preexisting diabetes was also expanded, from just those with risk factors to consideration of testing all women for undiagnosed diabetes at the time they’re planning pregnancy, and if not then, at the first prenatal visit. Screening for gestational diabetes is then performed at 24-28 weeks.
Again, this is caused by increasing diabetes onset at younger ages, Dr. Gabbay said. “We’re well aware that the number of women who have diabetes and don’t know it and become pregnant is significant and therefore screening early on is important.”
New guidance regarding autoantibody screening in adults suspected of having type 1 diabetes and genetic testing for those who don’t fit typical criteria for either of the two main types are based on the ADA/European Association for the Study of Diabetes joint consensus statement on type 1 diabetes in adults.
Individualization of care based on comorbidities, other factors
The concept of individualization of care in diabetes has been emphasized for several years now, but continues to be enhanced with new data and newly available management tools.
Regarding management of type 2 diabetes, several charts have been included to help guide decision-making.
One lists drug-specific and patient factors, including comorbidities, to consider when selecting glucose-lowering medications. A new table depicts a building with four “pillars,” for complication risk reduction, including management of blood pressure, lipids, and glucose, as well as use of agents with cardiovascular and kidney benefit.
“On the type 2 side, the choice of therapy is really guided by several factors. We lay them out in a nice diagram. ... A lot of useful information there compares classes of drugs in order to help clinicians make decisions on what would be the appropriate therapy for a given individual,” Dr. Gabbay said.
An algorithm for pharmacologic treatment includes considerations of weight, hypoglycemia, and cost. Tables are also provided listing average wholesale prices of insulins and noninsulin medications.
A section now entitled “Obesity and weight management for the prevention and treatment of type 2 diabetes” has added content regarding the importance of addressing obesity in diabetes, particularly in the context of the COVID-19 pandemic, and the addition of semaglutide as an approved obesity treatment.
“What we hope is that this engenders a shared decision-making process with the patient to identify what the goals are and then choose the appropriate therapy for those goals,” Dr. Gabbay said.
New information has also been added about management of nonalcoholic fatty liver disease. “I think that’s one of the unrecognized and unaddressed complications of diabetes that we’ll see in the future, particularly as new therapies come out,” Dr. Gabbay predicted.
The section on cardiovascular disease and risk management, endorsed for the fourth year in a row by the American College of Cardiology, includes several new recommendations, including diagnosis of hypertension at a single visit if blood pressure is 180/110 mm Hg or greater, and individualization of blood pressure targets.
Chronic kidney disease management has now been separated from other microvascular complications into a standalone section, with several new updates. Retinopathy, neuropathy, and foot care remain combined in one section.
Diabetes technology: Rapidly evolving, access an issue
The new technology section “doubles down on the time in [normal glucose] range (TIR) concept,” but also emphasizes the importance of time below range.
“When we see that, we need to make a therapeutic change. We were concerned that as there’s more and more information and numbers, users might not pick up on what’s important,” Dr. Gabbay noted.
The new standards also provides greater affirmation of the value of continuous glucose monitoring (CGM) for people with both type 1 and type 2 diabetes at any age, with individualized choice of devices.
Access to technology is a “big issue, and something the ADA has really been fighting for, particularly in terms of health disparities,” Dr. Gabbay said, noting that ADA has a new Health Equity Now platform, which includes a “bill of rights” calling for all patients with diabetes to have access to state-of-the-art technologies, including CGM.
Overall, he said, “I think the big picture is diabetes continues to evolve and advance. After careful review of the literature, the standards of care identifies at least four big areas where there are some changes that clinicians need to know about: screening, how to individualize treatment, considerations of comorbidities, and the important role that technology plays.”
Dr. Gabbay is an employee of the ADA.
A version of this article first appeared on Medscape.com.
The American Diabetes Association’s updated clinical recommendations for 2022 call for wider population screening, along with furthering the trends toward individualization of care use of diabetes technology.
The summary of changes from 2021 spans four pages. “Diabetes is a really dynamic field so there is a lot to update which is good. It means progress,” ADA chief science and medical officer Robert A. Gabbay, MD, PhD, told this news organization.
The ADA Standards of Medical Care in Diabetes – 2022 was published Dec. 20, 2021, online as a supplement to Diabetes Care.
Screening widened by age, in pregnancy, and for type 1 diabetes
One dramatic change is a drop in age to begin screening all people for prediabetes and diabetes from 45 years to 35 years, regardless of risk factors such as obesity.
“Sadly, there are increasing numbers of people with diabetes and developing diabetes younger,” Dr. Gabbay said.
In August 2021, the U.S. Preventive Services Task Force dropped its recommended age of diabetes screening from 40 to 35 years for people with overweight or obesity, but not universally, as ADA now has.
The ADA made its recommendation independently, Dr. Gabbay noted.
The recommendation for testing pregnant women early in gestation (<15 weeks) for preexisting diabetes was also expanded, from just those with risk factors to consideration of testing all women for undiagnosed diabetes at the time they’re planning pregnancy, and if not then, at the first prenatal visit. Screening for gestational diabetes is then performed at 24-28 weeks.
Again, this is caused by increasing diabetes onset at younger ages, Dr. Gabbay said. “We’re well aware that the number of women who have diabetes and don’t know it and become pregnant is significant and therefore screening early on is important.”
New guidance regarding autoantibody screening in adults suspected of having type 1 diabetes and genetic testing for those who don’t fit typical criteria for either of the two main types are based on the ADA/European Association for the Study of Diabetes joint consensus statement on type 1 diabetes in adults.
Individualization of care based on comorbidities, other factors
The concept of individualization of care in diabetes has been emphasized for several years now, but continues to be enhanced with new data and newly available management tools.
Regarding management of type 2 diabetes, several charts have been included to help guide decision-making.
One lists drug-specific and patient factors, including comorbidities, to consider when selecting glucose-lowering medications. A new table depicts a building with four “pillars,” for complication risk reduction, including management of blood pressure, lipids, and glucose, as well as use of agents with cardiovascular and kidney benefit.
“On the type 2 side, the choice of therapy is really guided by several factors. We lay them out in a nice diagram. ... A lot of useful information there compares classes of drugs in order to help clinicians make decisions on what would be the appropriate therapy for a given individual,” Dr. Gabbay said.
An algorithm for pharmacologic treatment includes considerations of weight, hypoglycemia, and cost. Tables are also provided listing average wholesale prices of insulins and noninsulin medications.
A section now entitled “Obesity and weight management for the prevention and treatment of type 2 diabetes” has added content regarding the importance of addressing obesity in diabetes, particularly in the context of the COVID-19 pandemic, and the addition of semaglutide as an approved obesity treatment.
“What we hope is that this engenders a shared decision-making process with the patient to identify what the goals are and then choose the appropriate therapy for those goals,” Dr. Gabbay said.
New information has also been added about management of nonalcoholic fatty liver disease. “I think that’s one of the unrecognized and unaddressed complications of diabetes that we’ll see in the future, particularly as new therapies come out,” Dr. Gabbay predicted.
The section on cardiovascular disease and risk management, endorsed for the fourth year in a row by the American College of Cardiology, includes several new recommendations, including diagnosis of hypertension at a single visit if blood pressure is 180/110 mm Hg or greater, and individualization of blood pressure targets.
Chronic kidney disease management has now been separated from other microvascular complications into a standalone section, with several new updates. Retinopathy, neuropathy, and foot care remain combined in one section.
Diabetes technology: Rapidly evolving, access an issue
The new technology section “doubles down on the time in [normal glucose] range (TIR) concept,” but also emphasizes the importance of time below range.
“When we see that, we need to make a therapeutic change. We were concerned that as there’s more and more information and numbers, users might not pick up on what’s important,” Dr. Gabbay noted.
The new standards also provides greater affirmation of the value of continuous glucose monitoring (CGM) for people with both type 1 and type 2 diabetes at any age, with individualized choice of devices.
Access to technology is a “big issue, and something the ADA has really been fighting for, particularly in terms of health disparities,” Dr. Gabbay said, noting that ADA has a new Health Equity Now platform, which includes a “bill of rights” calling for all patients with diabetes to have access to state-of-the-art technologies, including CGM.
Overall, he said, “I think the big picture is diabetes continues to evolve and advance. After careful review of the literature, the standards of care identifies at least four big areas where there are some changes that clinicians need to know about: screening, how to individualize treatment, considerations of comorbidities, and the important role that technology plays.”
Dr. Gabbay is an employee of the ADA.
A version of this article first appeared on Medscape.com.

Benefits of low-dose CT scanning for lung cancer screening explained
According to the Centers for Disease Control and Prevention, lung cancer is the third-most common cancer in the United States and the leading cause of cancer deaths in both men and women. Approximately, 150,000 Americans die every year from this disease.

In fact, it has been shown that low-dose CT scan screening can reduce lung cancer deaths by 20%-30% in high-risk populations.
In the United States, low-dose CT scan screening for lung cancer has largely become the norm. In July 2021, CHEST released new clinical guidelines. These guidelines cover 18 evidence-based recommendations as well as inclusion of further evidence regarding the benefits, risks, and use of CT screening.
In doing the risk assessment of low-dose CT scan as a method of lung cancer screening, meta-analyses were performed on evidence obtained through a literature search using PubMed, Embase, and the Cochrane Library. It was concluded that the benefits outweigh the risks as a method of lung cancer screening and can be utilized in reducing lung cancer deaths.
Low-dose CT scan screening was recommended for the following patients:
- Asymptomatic individuals aged 55-77 years with a history of smoking 30 or more pack-years. (This includes those who continue to smoke or who have quit in the previous 15 years. Annual screening is advised.)
- Asymptomatic individuals aged 55-80 years with a history of smoking 20-30 pack-years who either continue to smoke or have quit in the previous 15 years.
- For asymptomatic individuals who do not meet the above criteria but are predicted to benefit based on life-year gained calculations.
Don’t screen these patients
CT scan screening should not be performed on any person who does not meet any of the above three criteria.
Additionally, if a person has significant comorbidities that would limit their life expectancy, it is recommended not to do CT scan screening. Symptomatic patients should have appropriate diagnostic testing rather than screening.
Additional recommendations from the updated guidelines include developing appropriate counseling strategies as well as deciding what constitutes a positive test.
A positive test should be anything that warrants further evaluation rather than a return to annual screening. It was also advised that overtreatment strategies should be implemented. Additionally, smoking cessation treatment should be provided.
CHEST suggested undertaking a comprehensive approach involving multiple specialists including pulmonologists, radiologists, oncologists, etc. Strategies to ensure compliance with annual screening should also be devised, the guidelines say.
USPSTF’s updated guidelines
It should be noted that the U.S. Preventative Task Force released their own set of updated guidelines in March 2021. In these guidelines, the age at which lung cancer screening should be started was lowered from 55 years to 50 years.
Also, the USPSTF lowered the minimum required smoking history in order to be screened from 30 to 20 pack-years. Their purpose for doing this was to include more high-risk women as well as minorities.
With the changes, 14.5 million individuals living in the United States would be eligible for lung cancer screening by low-dose CT scan, an increase of 6.5 million people, compared with the previous guidelines.
While only small differences exist between the set of guidelines issued by CHEST and the ones issues by the USPSTF, lung cancer screening is still largely underutilized.
One of the barriers to screening may be patients’ lacking insurance coverage for it. As physicians, we need to advocate for these screening tools to be covered.
Other barriers include lack of patient knowledge regarding low-dose CT scans as a screening tool, patient time, and patient visits with their doctors being too short.
Key message
Part of the duties of physicians is to give our patients the best information. We can reduce lung cancer mortality in high risk patients by performing annual low-dose CT scans.
Whichever set of guidelines we chose to follow, we fail our patients if we don’t follow either set of them. The evidence is clear that a low-dose CT scan is a valuable screening tool to add to our practice of medicine.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
According to the Centers for Disease Control and Prevention, lung cancer is the third-most common cancer in the United States and the leading cause of cancer deaths in both men and women. Approximately, 150,000 Americans die every year from this disease.
In fact, it has been shown that low-dose CT scan screening can reduce lung cancer deaths by 20%-30% in high-risk populations.
In the United States, low-dose CT scan screening for lung cancer has largely become the norm. In July 2021, CHEST released new clinical guidelines. These guidelines cover 18 evidence-based recommendations as well as inclusion of further evidence regarding the benefits, risks, and use of CT screening.
In doing the risk assessment of low-dose CT scan as a method of lung cancer screening, meta-analyses were performed on evidence obtained through a literature search using PubMed, Embase, and the Cochrane Library. It was concluded that the benefits outweigh the risks as a method of lung cancer screening and can be utilized in reducing lung cancer deaths.
Low-dose CT scan screening was recommended for the following patients:
- Asymptomatic individuals aged 55-77 years with a history of smoking 30 or more pack-years. (This includes those who continue to smoke or who have quit in the previous 15 years. Annual screening is advised.)
- Asymptomatic individuals aged 55-80 years with a history of smoking 20-30 pack-years who either continue to smoke or have quit in the previous 15 years.
- For asymptomatic individuals who do not meet the above criteria but are predicted to benefit based on life-year gained calculations.
Don’t screen these patients
CT scan screening should not be performed on any person who does not meet any of the above three criteria.
Additionally, if a person has significant comorbidities that would limit their life expectancy, it is recommended not to do CT scan screening. Symptomatic patients should have appropriate diagnostic testing rather than screening.
Additional recommendations from the updated guidelines include developing appropriate counseling strategies as well as deciding what constitutes a positive test.
A positive test should be anything that warrants further evaluation rather than a return to annual screening. It was also advised that overtreatment strategies should be implemented. Additionally, smoking cessation treatment should be provided.
CHEST suggested undertaking a comprehensive approach involving multiple specialists including pulmonologists, radiologists, oncologists, etc. Strategies to ensure compliance with annual screening should also be devised, the guidelines say.
USPSTF’s updated guidelines
It should be noted that the U.S. Preventative Task Force released their own set of updated guidelines in March 2021. In these guidelines, the age at which lung cancer screening should be started was lowered from 55 years to 50 years.
Also, the USPSTF lowered the minimum required smoking history in order to be screened from 30 to 20 pack-years. Their purpose for doing this was to include more high-risk women as well as minorities.
With the changes, 14.5 million individuals living in the United States would be eligible for lung cancer screening by low-dose CT scan, an increase of 6.5 million people, compared with the previous guidelines.
While only small differences exist between the set of guidelines issued by CHEST and the ones issues by the USPSTF, lung cancer screening is still largely underutilized.
One of the barriers to screening may be patients’ lacking insurance coverage for it. As physicians, we need to advocate for these screening tools to be covered.
Other barriers include lack of patient knowledge regarding low-dose CT scans as a screening tool, patient time, and patient visits with their doctors being too short.
Key message
Part of the duties of physicians is to give our patients the best information. We can reduce lung cancer mortality in high risk patients by performing annual low-dose CT scans.
Whichever set of guidelines we chose to follow, we fail our patients if we don’t follow either set of them. The evidence is clear that a low-dose CT scan is a valuable screening tool to add to our practice of medicine.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
According to the Centers for Disease Control and Prevention, lung cancer is the third-most common cancer in the United States and the leading cause of cancer deaths in both men and women. Approximately, 150,000 Americans die every year from this disease.
In fact, it has been shown that low-dose CT scan screening can reduce lung cancer deaths by 20%-30% in high-risk populations.
In the United States, low-dose CT scan screening for lung cancer has largely become the norm. In July 2021, CHEST released new clinical guidelines. These guidelines cover 18 evidence-based recommendations as well as inclusion of further evidence regarding the benefits, risks, and use of CT screening.
In doing the risk assessment of low-dose CT scan as a method of lung cancer screening, meta-analyses were performed on evidence obtained through a literature search using PubMed, Embase, and the Cochrane Library. It was concluded that the benefits outweigh the risks as a method of lung cancer screening and can be utilized in reducing lung cancer deaths.
Low-dose CT scan screening was recommended for the following patients:
- Asymptomatic individuals aged 55-77 years with a history of smoking 30 or more pack-years. (This includes those who continue to smoke or who have quit in the previous 15 years. Annual screening is advised.)
- Asymptomatic individuals aged 55-80 years with a history of smoking 20-30 pack-years who either continue to smoke or have quit in the previous 15 years.
- For asymptomatic individuals who do not meet the above criteria but are predicted to benefit based on life-year gained calculations.
Don’t screen these patients
CT scan screening should not be performed on any person who does not meet any of the above three criteria.
Additionally, if a person has significant comorbidities that would limit their life expectancy, it is recommended not to do CT scan screening. Symptomatic patients should have appropriate diagnostic testing rather than screening.
Additional recommendations from the updated guidelines include developing appropriate counseling strategies as well as deciding what constitutes a positive test.
A positive test should be anything that warrants further evaluation rather than a return to annual screening. It was also advised that overtreatment strategies should be implemented. Additionally, smoking cessation treatment should be provided.
CHEST suggested undertaking a comprehensive approach involving multiple specialists including pulmonologists, radiologists, oncologists, etc. Strategies to ensure compliance with annual screening should also be devised, the guidelines say.
USPSTF’s updated guidelines
It should be noted that the U.S. Preventative Task Force released their own set of updated guidelines in March 2021. In these guidelines, the age at which lung cancer screening should be started was lowered from 55 years to 50 years.
Also, the USPSTF lowered the minimum required smoking history in order to be screened from 30 to 20 pack-years. Their purpose for doing this was to include more high-risk women as well as minorities.
With the changes, 14.5 million individuals living in the United States would be eligible for lung cancer screening by low-dose CT scan, an increase of 6.5 million people, compared with the previous guidelines.
While only small differences exist between the set of guidelines issued by CHEST and the ones issues by the USPSTF, lung cancer screening is still largely underutilized.
One of the barriers to screening may be patients’ lacking insurance coverage for it. As physicians, we need to advocate for these screening tools to be covered.
Other barriers include lack of patient knowledge regarding low-dose CT scans as a screening tool, patient time, and patient visits with their doctors being too short.
Key message
Part of the duties of physicians is to give our patients the best information. We can reduce lung cancer mortality in high risk patients by performing annual low-dose CT scans.
Whichever set of guidelines we chose to follow, we fail our patients if we don’t follow either set of them. The evidence is clear that a low-dose CT scan is a valuable screening tool to add to our practice of medicine.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.