User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Radiologist fatigue affects breast imaging interpretation
, based on data from more than 97,000 screening mammograms.
Psychology literature has shown the impact of fatigue on performance in a range of settings, and previous studies have shown that radiologists’ performances are more accurate earlier in their shifts compared to later-shift performance, write Michael H. Bernstein, PhD, and colleagues at Brown University, Providence, R.I., in a study published online Jan. 11 in Radiology.
The effect of time of day on performance may be greater for more detailed imaging modalities that are more “cognitively taxing,” and the effect may be greater in less-experienced radiologists, but the impact of time and experience on overall patient recall and false-positive rates has not been well-studied, the researchers said.
In the retrospective review, the researchers identified 97,671 screening mammograms read by 18 radiologists at one of 12 community sites between Jan. 2018 and Dec. 2019. The researchers analyzed the results by type of image, either standard digital mammography (DM) or the more complex digital breast tomosynthesis (DBT). The researchers separated radiologists into two groups: those with at least 5 post-training years of experience and those with less than 5 post-training years of experience. A total of nine radiologists fell into each category.
Overall, the recall rates were significantly different and higher for DM versus DBT (10.2% vs. 9.0%; P = .006). The false-positive (FP) rate also differed significantly and was higher for DM versus DBT (9.8% vs. 8.6%; P = .004).
The odds of recall increased by 11.5% with each hour of reading time for radiologists with less than 5 post-training years of experience for both DBT (odds ratio, 1.12) and DM (OR, 1.09). For the more experienced radiologists, the odds of recall increased by 1.6% for each hour of reading time for DBT but decreased by 0.1% for DM, with no significant difference.
Similarly, the odds of an FP result increased by 12.1% for DBT and 9% for DM per hour of reading time for radiologists with less experience. For more experienced radiologists, the odds of an FP increased by 1.6% for DBT but decreased by 1.1% for DM per hour of reading time.
Cancer detection (defined as true-positive, or TP) was not higher for DM across time, the researchers note. However, “DBT achieved a higher TP rate than DM regardless of the time of day; this shows that for DBT to maintain a constant and superior TP rate relative to DM, radiologists’ FP rates had to go up as the day went on,” they write. “That is, although DBT achieves a superior TP rate, more junior radiologists appeared to compensate for their fatigue later in the day when using DBT by recalling a broader range of mammograms, more of which were FP findings.”
The researchers caution that their findings were limited by several factors, including the study’s retrospective design and the lack of randomization of the imaging technology, patients, and time of day, which prohibit conclusions regarding causality. Other limitations included the consideration of time of day without the ability to use hours since the start of a clinical shift and the use of a 5-year mark to indicate experience without accounting for work volume.
However, the stronger impact of a time-of-day effect for more junior radiologists agrees with findings from other studies, the researchers add. More empirical research is needed, and the researchers propose a longitudinal study of how time of day affects radiologists as they gain experience, as well as experimental studies to test strategies for mitigating the time-of-day effect observed in the current study.
Scheduled breaks may reduce impact of fatigue
“Digital breast tomosynthesis is increasingly used in clinical practice and takes significantly longer to interpret compared with digital mammography,” said corresponding author Ana P. Lourenco, MD, in an interview. “Radiologists interpret hundreds of images for each screening digital breast tomosynthesis exam, compared with four images for each screening digital mammogram exam; this may certainly contribute to radiologist fatigue.”
“I found it interesting that there was a difference based on years of experience of the radiologist, but I was not surprised that recall rate increased later in the day, as some of us had anecdotally noted this in our clinical practice,” Dr. Lourenco said. In fact, the idea to conduct the study was prompted by a conversation with her statistician colleagues “about how I subjectively felt like my own recall rate increased at the end of the day.”
Ways to counteract the impact of fatigue could include intermittent breaks to refocus attention, said Dr. Lourenco. “Potential barriers would include imaging volumes and attending to patients in the breast imaging center,” she said. “If we can show that decreasing fatigue improves mammography performance metrics, then this may encourage practices to support such interventions.”
However, “more research that includes a larger number of radiologists, wider range of imaging interpretation experience, perhaps even experimental studies comparing metrics for radiologists reading with scheduled breaks versus without such breaks would be of interest,” Dr. Lourenco said.
Fatigue in health care goes beyond radiology
“Due primarily to staffing shortages and increased volume and complexity of patients, burnout and fatigue of all medical personnel, not just physicians, have become hallmarks of modern health care delivery in the United States, and this has been exacerbated by COVID-19 and other societal factors,” said Jeffrey C. Weinreb, MD, professor of radiology and biomedical imaging at Yale University, New Haven, Conn., in an interview.
Previous studies have documented the fact that radiologists are among the specialists most affected by burnout and fatigue, and it has an impact on their performance, Dr. Weinreb said. The current study is important because it tries to pinpoint the key variables that are responsible for fatigue, so resources can be directed to effect change, he said.
Dr. Weinreb said he was not particularly surprised by the study findings. “Diagnostic mammography is a high-volume repetitive enterprise, so it would have been surprising if radiologist experience and time of day had no effect on performance and recall rate,” he said. “As most radiologists will attest based on personal experience, human beings get tired and lose some level of cognition over the course of a long, intense workday,” he added.
“I am a bit surprised that less experienced radiologists were more likely to recommend additional imaging at a higher rate when interpreting DBT but not for DM and only later in the day,” Dr. Weinreb noted. “The authors suggest that this could be due to the increased number of images that are viewed with DBT and the different ways experienced and less experienced radiologists process the information. However, there could be other explanations, such as differences in volumes or differences in ages.”
“Reducing the study volumes per radiologist is one obvious solution to reducing fatigue, but it will not be practical in many practices,” said Dr. Weinreb. “The important work of interpreting diagnostic mammograms needs to continue and grow. Without an increase in radiologist mammographers in the labor pool, this is not going to happen any time soon.”
Instead, “more immediate obvious solutions to radiologist fatigue in clinical practice include more frequent breaks during the workday, which would include walking around and not looking at a computer or cell phone screen, fewer images per study, report templates, streamlined workflow, more variety in daily work, and AI assistance for interpretation and reporting,” said Dr. Weinreb. Using nonradiologists when possible to relieve some of the burden could be considered, “but this is a complex and politically charged issue,” he noted.
Radiology is a well-compensated specialty, but further increasing compensation would help to mitigate burnout, said Dr. Weinreb. However, “perhaps even more important is making certain that the efforts of individual radiologists are appreciated and recognized,” he said.
As for additional research needs, “mammographers are not the only radiologists experiencing fatigue, but the most critical contributing factors for other types of imaging exams and subspecialities may not be identical,” Dr. Weinreb emphasized. “Data for other radiologists, similar to that provided by this study for diagnostic mammography, could be useful.
“An additional area of research could address the issue of individual radiologist circadian rhythms,” said Dr. Weinreb. “Perhaps we could rigorously determine whom amongst us is a ‘morning person’ versus one who performs equally well or better later in the day and use this information for radiologist scheduling,” he said. “Finally, once we know the key factors affecting performance for each type of exam and subspecialty, studies of possible incremental and combined benefits of various interventions would be needed.”
The study received no outside funding. The researchers and Dr. Weinreb have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, based on data from more than 97,000 screening mammograms.
Psychology literature has shown the impact of fatigue on performance in a range of settings, and previous studies have shown that radiologists’ performances are more accurate earlier in their shifts compared to later-shift performance, write Michael H. Bernstein, PhD, and colleagues at Brown University, Providence, R.I., in a study published online Jan. 11 in Radiology.
The effect of time of day on performance may be greater for more detailed imaging modalities that are more “cognitively taxing,” and the effect may be greater in less-experienced radiologists, but the impact of time and experience on overall patient recall and false-positive rates has not been well-studied, the researchers said.
In the retrospective review, the researchers identified 97,671 screening mammograms read by 18 radiologists at one of 12 community sites between Jan. 2018 and Dec. 2019. The researchers analyzed the results by type of image, either standard digital mammography (DM) or the more complex digital breast tomosynthesis (DBT). The researchers separated radiologists into two groups: those with at least 5 post-training years of experience and those with less than 5 post-training years of experience. A total of nine radiologists fell into each category.
Overall, the recall rates were significantly different and higher for DM versus DBT (10.2% vs. 9.0%; P = .006). The false-positive (FP) rate also differed significantly and was higher for DM versus DBT (9.8% vs. 8.6%; P = .004).
The odds of recall increased by 11.5% with each hour of reading time for radiologists with less than 5 post-training years of experience for both DBT (odds ratio, 1.12) and DM (OR, 1.09). For the more experienced radiologists, the odds of recall increased by 1.6% for each hour of reading time for DBT but decreased by 0.1% for DM, with no significant difference.
Similarly, the odds of an FP result increased by 12.1% for DBT and 9% for DM per hour of reading time for radiologists with less experience. For more experienced radiologists, the odds of an FP increased by 1.6% for DBT but decreased by 1.1% for DM per hour of reading time.
Cancer detection (defined as true-positive, or TP) was not higher for DM across time, the researchers note. However, “DBT achieved a higher TP rate than DM regardless of the time of day; this shows that for DBT to maintain a constant and superior TP rate relative to DM, radiologists’ FP rates had to go up as the day went on,” they write. “That is, although DBT achieves a superior TP rate, more junior radiologists appeared to compensate for their fatigue later in the day when using DBT by recalling a broader range of mammograms, more of which were FP findings.”
The researchers caution that their findings were limited by several factors, including the study’s retrospective design and the lack of randomization of the imaging technology, patients, and time of day, which prohibit conclusions regarding causality. Other limitations included the consideration of time of day without the ability to use hours since the start of a clinical shift and the use of a 5-year mark to indicate experience without accounting for work volume.
However, the stronger impact of a time-of-day effect for more junior radiologists agrees with findings from other studies, the researchers add. More empirical research is needed, and the researchers propose a longitudinal study of how time of day affects radiologists as they gain experience, as well as experimental studies to test strategies for mitigating the time-of-day effect observed in the current study.
Scheduled breaks may reduce impact of fatigue
“Digital breast tomosynthesis is increasingly used in clinical practice and takes significantly longer to interpret compared with digital mammography,” said corresponding author Ana P. Lourenco, MD, in an interview. “Radiologists interpret hundreds of images for each screening digital breast tomosynthesis exam, compared with four images for each screening digital mammogram exam; this may certainly contribute to radiologist fatigue.”
“I found it interesting that there was a difference based on years of experience of the radiologist, but I was not surprised that recall rate increased later in the day, as some of us had anecdotally noted this in our clinical practice,” Dr. Lourenco said. In fact, the idea to conduct the study was prompted by a conversation with her statistician colleagues “about how I subjectively felt like my own recall rate increased at the end of the day.”
Ways to counteract the impact of fatigue could include intermittent breaks to refocus attention, said Dr. Lourenco. “Potential barriers would include imaging volumes and attending to patients in the breast imaging center,” she said. “If we can show that decreasing fatigue improves mammography performance metrics, then this may encourage practices to support such interventions.”
However, “more research that includes a larger number of radiologists, wider range of imaging interpretation experience, perhaps even experimental studies comparing metrics for radiologists reading with scheduled breaks versus without such breaks would be of interest,” Dr. Lourenco said.
Fatigue in health care goes beyond radiology
“Due primarily to staffing shortages and increased volume and complexity of patients, burnout and fatigue of all medical personnel, not just physicians, have become hallmarks of modern health care delivery in the United States, and this has been exacerbated by COVID-19 and other societal factors,” said Jeffrey C. Weinreb, MD, professor of radiology and biomedical imaging at Yale University, New Haven, Conn., in an interview.
Previous studies have documented the fact that radiologists are among the specialists most affected by burnout and fatigue, and it has an impact on their performance, Dr. Weinreb said. The current study is important because it tries to pinpoint the key variables that are responsible for fatigue, so resources can be directed to effect change, he said.
Dr. Weinreb said he was not particularly surprised by the study findings. “Diagnostic mammography is a high-volume repetitive enterprise, so it would have been surprising if radiologist experience and time of day had no effect on performance and recall rate,” he said. “As most radiologists will attest based on personal experience, human beings get tired and lose some level of cognition over the course of a long, intense workday,” he added.
“I am a bit surprised that less experienced radiologists were more likely to recommend additional imaging at a higher rate when interpreting DBT but not for DM and only later in the day,” Dr. Weinreb noted. “The authors suggest that this could be due to the increased number of images that are viewed with DBT and the different ways experienced and less experienced radiologists process the information. However, there could be other explanations, such as differences in volumes or differences in ages.”
“Reducing the study volumes per radiologist is one obvious solution to reducing fatigue, but it will not be practical in many practices,” said Dr. Weinreb. “The important work of interpreting diagnostic mammograms needs to continue and grow. Without an increase in radiologist mammographers in the labor pool, this is not going to happen any time soon.”
Instead, “more immediate obvious solutions to radiologist fatigue in clinical practice include more frequent breaks during the workday, which would include walking around and not looking at a computer or cell phone screen, fewer images per study, report templates, streamlined workflow, more variety in daily work, and AI assistance for interpretation and reporting,” said Dr. Weinreb. Using nonradiologists when possible to relieve some of the burden could be considered, “but this is a complex and politically charged issue,” he noted.
Radiology is a well-compensated specialty, but further increasing compensation would help to mitigate burnout, said Dr. Weinreb. However, “perhaps even more important is making certain that the efforts of individual radiologists are appreciated and recognized,” he said.
As for additional research needs, “mammographers are not the only radiologists experiencing fatigue, but the most critical contributing factors for other types of imaging exams and subspecialities may not be identical,” Dr. Weinreb emphasized. “Data for other radiologists, similar to that provided by this study for diagnostic mammography, could be useful.
“An additional area of research could address the issue of individual radiologist circadian rhythms,” said Dr. Weinreb. “Perhaps we could rigorously determine whom amongst us is a ‘morning person’ versus one who performs equally well or better later in the day and use this information for radiologist scheduling,” he said. “Finally, once we know the key factors affecting performance for each type of exam and subspecialty, studies of possible incremental and combined benefits of various interventions would be needed.”
The study received no outside funding. The researchers and Dr. Weinreb have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, based on data from more than 97,000 screening mammograms.
Psychology literature has shown the impact of fatigue on performance in a range of settings, and previous studies have shown that radiologists’ performances are more accurate earlier in their shifts compared to later-shift performance, write Michael H. Bernstein, PhD, and colleagues at Brown University, Providence, R.I., in a study published online Jan. 11 in Radiology.
The effect of time of day on performance may be greater for more detailed imaging modalities that are more “cognitively taxing,” and the effect may be greater in less-experienced radiologists, but the impact of time and experience on overall patient recall and false-positive rates has not been well-studied, the researchers said.
In the retrospective review, the researchers identified 97,671 screening mammograms read by 18 radiologists at one of 12 community sites between Jan. 2018 and Dec. 2019. The researchers analyzed the results by type of image, either standard digital mammography (DM) or the more complex digital breast tomosynthesis (DBT). The researchers separated radiologists into two groups: those with at least 5 post-training years of experience and those with less than 5 post-training years of experience. A total of nine radiologists fell into each category.
Overall, the recall rates were significantly different and higher for DM versus DBT (10.2% vs. 9.0%; P = .006). The false-positive (FP) rate also differed significantly and was higher for DM versus DBT (9.8% vs. 8.6%; P = .004).
The odds of recall increased by 11.5% with each hour of reading time for radiologists with less than 5 post-training years of experience for both DBT (odds ratio, 1.12) and DM (OR, 1.09). For the more experienced radiologists, the odds of recall increased by 1.6% for each hour of reading time for DBT but decreased by 0.1% for DM, with no significant difference.
Similarly, the odds of an FP result increased by 12.1% for DBT and 9% for DM per hour of reading time for radiologists with less experience. For more experienced radiologists, the odds of an FP increased by 1.6% for DBT but decreased by 1.1% for DM per hour of reading time.
Cancer detection (defined as true-positive, or TP) was not higher for DM across time, the researchers note. However, “DBT achieved a higher TP rate than DM regardless of the time of day; this shows that for DBT to maintain a constant and superior TP rate relative to DM, radiologists’ FP rates had to go up as the day went on,” they write. “That is, although DBT achieves a superior TP rate, more junior radiologists appeared to compensate for their fatigue later in the day when using DBT by recalling a broader range of mammograms, more of which were FP findings.”
The researchers caution that their findings were limited by several factors, including the study’s retrospective design and the lack of randomization of the imaging technology, patients, and time of day, which prohibit conclusions regarding causality. Other limitations included the consideration of time of day without the ability to use hours since the start of a clinical shift and the use of a 5-year mark to indicate experience without accounting for work volume.
However, the stronger impact of a time-of-day effect for more junior radiologists agrees with findings from other studies, the researchers add. More empirical research is needed, and the researchers propose a longitudinal study of how time of day affects radiologists as they gain experience, as well as experimental studies to test strategies for mitigating the time-of-day effect observed in the current study.
Scheduled breaks may reduce impact of fatigue
“Digital breast tomosynthesis is increasingly used in clinical practice and takes significantly longer to interpret compared with digital mammography,” said corresponding author Ana P. Lourenco, MD, in an interview. “Radiologists interpret hundreds of images for each screening digital breast tomosynthesis exam, compared with four images for each screening digital mammogram exam; this may certainly contribute to radiologist fatigue.”
“I found it interesting that there was a difference based on years of experience of the radiologist, but I was not surprised that recall rate increased later in the day, as some of us had anecdotally noted this in our clinical practice,” Dr. Lourenco said. In fact, the idea to conduct the study was prompted by a conversation with her statistician colleagues “about how I subjectively felt like my own recall rate increased at the end of the day.”
Ways to counteract the impact of fatigue could include intermittent breaks to refocus attention, said Dr. Lourenco. “Potential barriers would include imaging volumes and attending to patients in the breast imaging center,” she said. “If we can show that decreasing fatigue improves mammography performance metrics, then this may encourage practices to support such interventions.”
However, “more research that includes a larger number of radiologists, wider range of imaging interpretation experience, perhaps even experimental studies comparing metrics for radiologists reading with scheduled breaks versus without such breaks would be of interest,” Dr. Lourenco said.
Fatigue in health care goes beyond radiology
“Due primarily to staffing shortages and increased volume and complexity of patients, burnout and fatigue of all medical personnel, not just physicians, have become hallmarks of modern health care delivery in the United States, and this has been exacerbated by COVID-19 and other societal factors,” said Jeffrey C. Weinreb, MD, professor of radiology and biomedical imaging at Yale University, New Haven, Conn., in an interview.
Previous studies have documented the fact that radiologists are among the specialists most affected by burnout and fatigue, and it has an impact on their performance, Dr. Weinreb said. The current study is important because it tries to pinpoint the key variables that are responsible for fatigue, so resources can be directed to effect change, he said.
Dr. Weinreb said he was not particularly surprised by the study findings. “Diagnostic mammography is a high-volume repetitive enterprise, so it would have been surprising if radiologist experience and time of day had no effect on performance and recall rate,” he said. “As most radiologists will attest based on personal experience, human beings get tired and lose some level of cognition over the course of a long, intense workday,” he added.
“I am a bit surprised that less experienced radiologists were more likely to recommend additional imaging at a higher rate when interpreting DBT but not for DM and only later in the day,” Dr. Weinreb noted. “The authors suggest that this could be due to the increased number of images that are viewed with DBT and the different ways experienced and less experienced radiologists process the information. However, there could be other explanations, such as differences in volumes or differences in ages.”
“Reducing the study volumes per radiologist is one obvious solution to reducing fatigue, but it will not be practical in many practices,” said Dr. Weinreb. “The important work of interpreting diagnostic mammograms needs to continue and grow. Without an increase in radiologist mammographers in the labor pool, this is not going to happen any time soon.”
Instead, “more immediate obvious solutions to radiologist fatigue in clinical practice include more frequent breaks during the workday, which would include walking around and not looking at a computer or cell phone screen, fewer images per study, report templates, streamlined workflow, more variety in daily work, and AI assistance for interpretation and reporting,” said Dr. Weinreb. Using nonradiologists when possible to relieve some of the burden could be considered, “but this is a complex and politically charged issue,” he noted.
Radiology is a well-compensated specialty, but further increasing compensation would help to mitigate burnout, said Dr. Weinreb. However, “perhaps even more important is making certain that the efforts of individual radiologists are appreciated and recognized,” he said.
As for additional research needs, “mammographers are not the only radiologists experiencing fatigue, but the most critical contributing factors for other types of imaging exams and subspecialities may not be identical,” Dr. Weinreb emphasized. “Data for other radiologists, similar to that provided by this study for diagnostic mammography, could be useful.
“An additional area of research could address the issue of individual radiologist circadian rhythms,” said Dr. Weinreb. “Perhaps we could rigorously determine whom amongst us is a ‘morning person’ versus one who performs equally well or better later in the day and use this information for radiologist scheduling,” he said. “Finally, once we know the key factors affecting performance for each type of exam and subspecialty, studies of possible incremental and combined benefits of various interventions would be needed.”
The study received no outside funding. The researchers and Dr. Weinreb have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
OTC cannabidiol products tied to improved pain, sleep, anxiety
Interim findings from Advancing CBD Education and Science, a 100% virtual, open label, randomized, controlled trial, show study participants experienced various degrees of “clinically meaningful” improvements in sleep quality, anxiety, and pain.
“ACES is the largest clinical trial ever conducted on commercially available CBD products and provides first-of-its-kind real world evidence into what conditions users may experience benefit from CBD usage, whether these benefits are clinically meaningful, what attributes of CBD products may impact health outcomes, and what side effects may occur,” study coinvestigator Jessica Saleska, PhD, MPH, director of research at Radicle Science, the company that conducted the study, told this news organization.
Scant evidence
Despite the growing market size of commercially available CBD products “there is still scant data on the effectiveness of over-the-counter cannabinoid products due to the cost, speed, and scale limitations of the current approach to scientific research,” Jeff Chen, MD, MBA, cofounder and CEO of Radicle Science, told this news organization.
One of the study’s goals, said Ethan Russo, MD, a neurologist, founder/CEO of CReDO Science, and scientific adviser for Radicle, is to help consumers make informed decisions before purchasing and using commercially available oral CBD products.
Designed to eliminate all physical infrastructure, which minimizes costs and facilitates faster execution, ACES was conducted much like a phase 4 clinical trial, collating real-world data gathered over 4 weeks.
“The process that Radicle scientists [have] advanced is sort of a crowdsourcing approach to doing clinical science,” Dr. Russo said. “Hopefully, there is going to be a considerable amount of data generated that [will] affect people’s buying options.”
The study also aimed to evaluate product attributes, including composition, mode of use, dosage, dosage timing and frequency, and their correlation to degrees of outcomes.
Dr. Russo explained why product composition is an important factor, especially when dealing with CBD. “What happens with any given [CBD] preparation is going to be totally a function of other components, if any.
“For example, there’s this mistaken notion that cannabidiol is sedating; it is not. Pure cannabidiol is stimulating in low and moderate amounts. Where the confusion has arisen is that the early chemovars containing cannabidiol were also predominant in myrcene, the sedating terpene, [thereby] creating this misimpression that it is good for sleep,” he added.
However, CBD might also affect sleep by reducing anxiety that interferes with it. “What’s clear is that cannabidiol is an antianxiety agent, if you have a sufficient dose,” Dr. Russo said.
The 4-week study included 2,704 participants aged 21 years and older, self-reporting anxiety, chronic pain, or sleep disturbances as a primary reason for taking CBD. Study participants were randomly assigned to receive 1 of 13 commercially available oral CBD extracts.
Participants were allocated to 1 of 14 cohorts, comprising 13 treatment groups with 208 participants each who received a single CBD product, or a wait-list control group of 296 participants who received product at the study’s end.
The primary outcome focused on “clinically meaningful” changes, which were defined as “distinct and palpable improvements in quality of life through improvements in respective health outcomes.”
Secondary outcomes included changes in sleep, anxiety, and pain based on several validated indices, including the PROMIS (Patient-Reported Outcome Measurement Information System) Sleep Short Form; the PROMIS Anxiety Scale; the Patient Global Impression of Change; the Pain, Enjoyment, General Activity scale; and the General Anxiety Disorder–7 scale.
The interim study results are promising, with participants reporting, on average, a 71% improvement in well-being. Additionally, 63% reported clinically meaningful improvements in anxiety, and 61% in sleep quality. The CBD products provided smaller benefits in pain management, with less than half (47%) experiencing meaningful improvements.
In addition to improvement in sleep, pain, and anxiety, these data highlight how rapidly benefits occurred; most were realized during the first week of the study, with up to 61% of treatment group participants reporting a therapeutic effect within 1-4 hours of taking their assigned product.
Overcoming the placebo effect
Commenting on the research, Justin Strickland, PhD, an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, who was not involved in the research, said without knowing a lot about the pharmacology of the products being tested, early dramatic improvements in these measures, such as sleep impairment, are common.
“There are some data to suggest that there is an expectancy effect when we talk about the therapeutic benefit of cannabinoid products, (i.e., when someone has the expectation that they are going to experience a stronger effect) but this is true of any drug in an open label trial,” Dr. Strickland added.
Dr. Russo took the point a step further. “It’s getting near impossible to look at cannabinoid compounds, even with randomized, controlled trials because of the burgeoning placebo responses. When you couple it with the fact that consumers have the mistaken notion that cannabis-based drugs are miraculous, the expectations are so high that everyone thinks that they’re on the real stuff, even if it’s a placebo group.”
Still, both Dr. Strickland and Dr. Russo highlighted the fact that ACES mirrors real-world experience, which will they hope will inform the use of CBD and CBD-based preparations moving forward. By removing certain barriers like institutional bureaucracy or federal funding restrictions inherent to more traditional randomized controlled trial design, ACES might provide data that bridge the gap between efficacy and effectiveness.
ACES was funded by Radicle Science. Dr. Chen is cofounder and CEO of Radicle Science. Dr. Russo and Dr. Strickland disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Interim findings from Advancing CBD Education and Science, a 100% virtual, open label, randomized, controlled trial, show study participants experienced various degrees of “clinically meaningful” improvements in sleep quality, anxiety, and pain.
“ACES is the largest clinical trial ever conducted on commercially available CBD products and provides first-of-its-kind real world evidence into what conditions users may experience benefit from CBD usage, whether these benefits are clinically meaningful, what attributes of CBD products may impact health outcomes, and what side effects may occur,” study coinvestigator Jessica Saleska, PhD, MPH, director of research at Radicle Science, the company that conducted the study, told this news organization.
Scant evidence
Despite the growing market size of commercially available CBD products “there is still scant data on the effectiveness of over-the-counter cannabinoid products due to the cost, speed, and scale limitations of the current approach to scientific research,” Jeff Chen, MD, MBA, cofounder and CEO of Radicle Science, told this news organization.
One of the study’s goals, said Ethan Russo, MD, a neurologist, founder/CEO of CReDO Science, and scientific adviser for Radicle, is to help consumers make informed decisions before purchasing and using commercially available oral CBD products.
Designed to eliminate all physical infrastructure, which minimizes costs and facilitates faster execution, ACES was conducted much like a phase 4 clinical trial, collating real-world data gathered over 4 weeks.
“The process that Radicle scientists [have] advanced is sort of a crowdsourcing approach to doing clinical science,” Dr. Russo said. “Hopefully, there is going to be a considerable amount of data generated that [will] affect people’s buying options.”
The study also aimed to evaluate product attributes, including composition, mode of use, dosage, dosage timing and frequency, and their correlation to degrees of outcomes.
Dr. Russo explained why product composition is an important factor, especially when dealing with CBD. “What happens with any given [CBD] preparation is going to be totally a function of other components, if any.
“For example, there’s this mistaken notion that cannabidiol is sedating; it is not. Pure cannabidiol is stimulating in low and moderate amounts. Where the confusion has arisen is that the early chemovars containing cannabidiol were also predominant in myrcene, the sedating terpene, [thereby] creating this misimpression that it is good for sleep,” he added.
However, CBD might also affect sleep by reducing anxiety that interferes with it. “What’s clear is that cannabidiol is an antianxiety agent, if you have a sufficient dose,” Dr. Russo said.
The 4-week study included 2,704 participants aged 21 years and older, self-reporting anxiety, chronic pain, or sleep disturbances as a primary reason for taking CBD. Study participants were randomly assigned to receive 1 of 13 commercially available oral CBD extracts.
Participants were allocated to 1 of 14 cohorts, comprising 13 treatment groups with 208 participants each who received a single CBD product, or a wait-list control group of 296 participants who received product at the study’s end.
The primary outcome focused on “clinically meaningful” changes, which were defined as “distinct and palpable improvements in quality of life through improvements in respective health outcomes.”
Secondary outcomes included changes in sleep, anxiety, and pain based on several validated indices, including the PROMIS (Patient-Reported Outcome Measurement Information System) Sleep Short Form; the PROMIS Anxiety Scale; the Patient Global Impression of Change; the Pain, Enjoyment, General Activity scale; and the General Anxiety Disorder–7 scale.
The interim study results are promising, with participants reporting, on average, a 71% improvement in well-being. Additionally, 63% reported clinically meaningful improvements in anxiety, and 61% in sleep quality. The CBD products provided smaller benefits in pain management, with less than half (47%) experiencing meaningful improvements.
In addition to improvement in sleep, pain, and anxiety, these data highlight how rapidly benefits occurred; most were realized during the first week of the study, with up to 61% of treatment group participants reporting a therapeutic effect within 1-4 hours of taking their assigned product.
Overcoming the placebo effect
Commenting on the research, Justin Strickland, PhD, an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, who was not involved in the research, said without knowing a lot about the pharmacology of the products being tested, early dramatic improvements in these measures, such as sleep impairment, are common.
“There are some data to suggest that there is an expectancy effect when we talk about the therapeutic benefit of cannabinoid products, (i.e., when someone has the expectation that they are going to experience a stronger effect) but this is true of any drug in an open label trial,” Dr. Strickland added.
Dr. Russo took the point a step further. “It’s getting near impossible to look at cannabinoid compounds, even with randomized, controlled trials because of the burgeoning placebo responses. When you couple it with the fact that consumers have the mistaken notion that cannabis-based drugs are miraculous, the expectations are so high that everyone thinks that they’re on the real stuff, even if it’s a placebo group.”
Still, both Dr. Strickland and Dr. Russo highlighted the fact that ACES mirrors real-world experience, which will they hope will inform the use of CBD and CBD-based preparations moving forward. By removing certain barriers like institutional bureaucracy or federal funding restrictions inherent to more traditional randomized controlled trial design, ACES might provide data that bridge the gap between efficacy and effectiveness.
ACES was funded by Radicle Science. Dr. Chen is cofounder and CEO of Radicle Science. Dr. Russo and Dr. Strickland disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Interim findings from Advancing CBD Education and Science, a 100% virtual, open label, randomized, controlled trial, show study participants experienced various degrees of “clinically meaningful” improvements in sleep quality, anxiety, and pain.
“ACES is the largest clinical trial ever conducted on commercially available CBD products and provides first-of-its-kind real world evidence into what conditions users may experience benefit from CBD usage, whether these benefits are clinically meaningful, what attributes of CBD products may impact health outcomes, and what side effects may occur,” study coinvestigator Jessica Saleska, PhD, MPH, director of research at Radicle Science, the company that conducted the study, told this news organization.
Scant evidence
Despite the growing market size of commercially available CBD products “there is still scant data on the effectiveness of over-the-counter cannabinoid products due to the cost, speed, and scale limitations of the current approach to scientific research,” Jeff Chen, MD, MBA, cofounder and CEO of Radicle Science, told this news organization.
One of the study’s goals, said Ethan Russo, MD, a neurologist, founder/CEO of CReDO Science, and scientific adviser for Radicle, is to help consumers make informed decisions before purchasing and using commercially available oral CBD products.
Designed to eliminate all physical infrastructure, which minimizes costs and facilitates faster execution, ACES was conducted much like a phase 4 clinical trial, collating real-world data gathered over 4 weeks.
“The process that Radicle scientists [have] advanced is sort of a crowdsourcing approach to doing clinical science,” Dr. Russo said. “Hopefully, there is going to be a considerable amount of data generated that [will] affect people’s buying options.”
The study also aimed to evaluate product attributes, including composition, mode of use, dosage, dosage timing and frequency, and their correlation to degrees of outcomes.
Dr. Russo explained why product composition is an important factor, especially when dealing with CBD. “What happens with any given [CBD] preparation is going to be totally a function of other components, if any.
“For example, there’s this mistaken notion that cannabidiol is sedating; it is not. Pure cannabidiol is stimulating in low and moderate amounts. Where the confusion has arisen is that the early chemovars containing cannabidiol were also predominant in myrcene, the sedating terpene, [thereby] creating this misimpression that it is good for sleep,” he added.
However, CBD might also affect sleep by reducing anxiety that interferes with it. “What’s clear is that cannabidiol is an antianxiety agent, if you have a sufficient dose,” Dr. Russo said.
The 4-week study included 2,704 participants aged 21 years and older, self-reporting anxiety, chronic pain, or sleep disturbances as a primary reason for taking CBD. Study participants were randomly assigned to receive 1 of 13 commercially available oral CBD extracts.
Participants were allocated to 1 of 14 cohorts, comprising 13 treatment groups with 208 participants each who received a single CBD product, or a wait-list control group of 296 participants who received product at the study’s end.
The primary outcome focused on “clinically meaningful” changes, which were defined as “distinct and palpable improvements in quality of life through improvements in respective health outcomes.”
Secondary outcomes included changes in sleep, anxiety, and pain based on several validated indices, including the PROMIS (Patient-Reported Outcome Measurement Information System) Sleep Short Form; the PROMIS Anxiety Scale; the Patient Global Impression of Change; the Pain, Enjoyment, General Activity scale; and the General Anxiety Disorder–7 scale.
The interim study results are promising, with participants reporting, on average, a 71% improvement in well-being. Additionally, 63% reported clinically meaningful improvements in anxiety, and 61% in sleep quality. The CBD products provided smaller benefits in pain management, with less than half (47%) experiencing meaningful improvements.
In addition to improvement in sleep, pain, and anxiety, these data highlight how rapidly benefits occurred; most were realized during the first week of the study, with up to 61% of treatment group participants reporting a therapeutic effect within 1-4 hours of taking their assigned product.
Overcoming the placebo effect
Commenting on the research, Justin Strickland, PhD, an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, who was not involved in the research, said without knowing a lot about the pharmacology of the products being tested, early dramatic improvements in these measures, such as sleep impairment, are common.
“There are some data to suggest that there is an expectancy effect when we talk about the therapeutic benefit of cannabinoid products, (i.e., when someone has the expectation that they are going to experience a stronger effect) but this is true of any drug in an open label trial,” Dr. Strickland added.
Dr. Russo took the point a step further. “It’s getting near impossible to look at cannabinoid compounds, even with randomized, controlled trials because of the burgeoning placebo responses. When you couple it with the fact that consumers have the mistaken notion that cannabis-based drugs are miraculous, the expectations are so high that everyone thinks that they’re on the real stuff, even if it’s a placebo group.”
Still, both Dr. Strickland and Dr. Russo highlighted the fact that ACES mirrors real-world experience, which will they hope will inform the use of CBD and CBD-based preparations moving forward. By removing certain barriers like institutional bureaucracy or federal funding restrictions inherent to more traditional randomized controlled trial design, ACES might provide data that bridge the gap between efficacy and effectiveness.
ACES was funded by Radicle Science. Dr. Chen is cofounder and CEO of Radicle Science. Dr. Russo and Dr. Strickland disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physician burnout, depression compounded by COVID: Survey
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
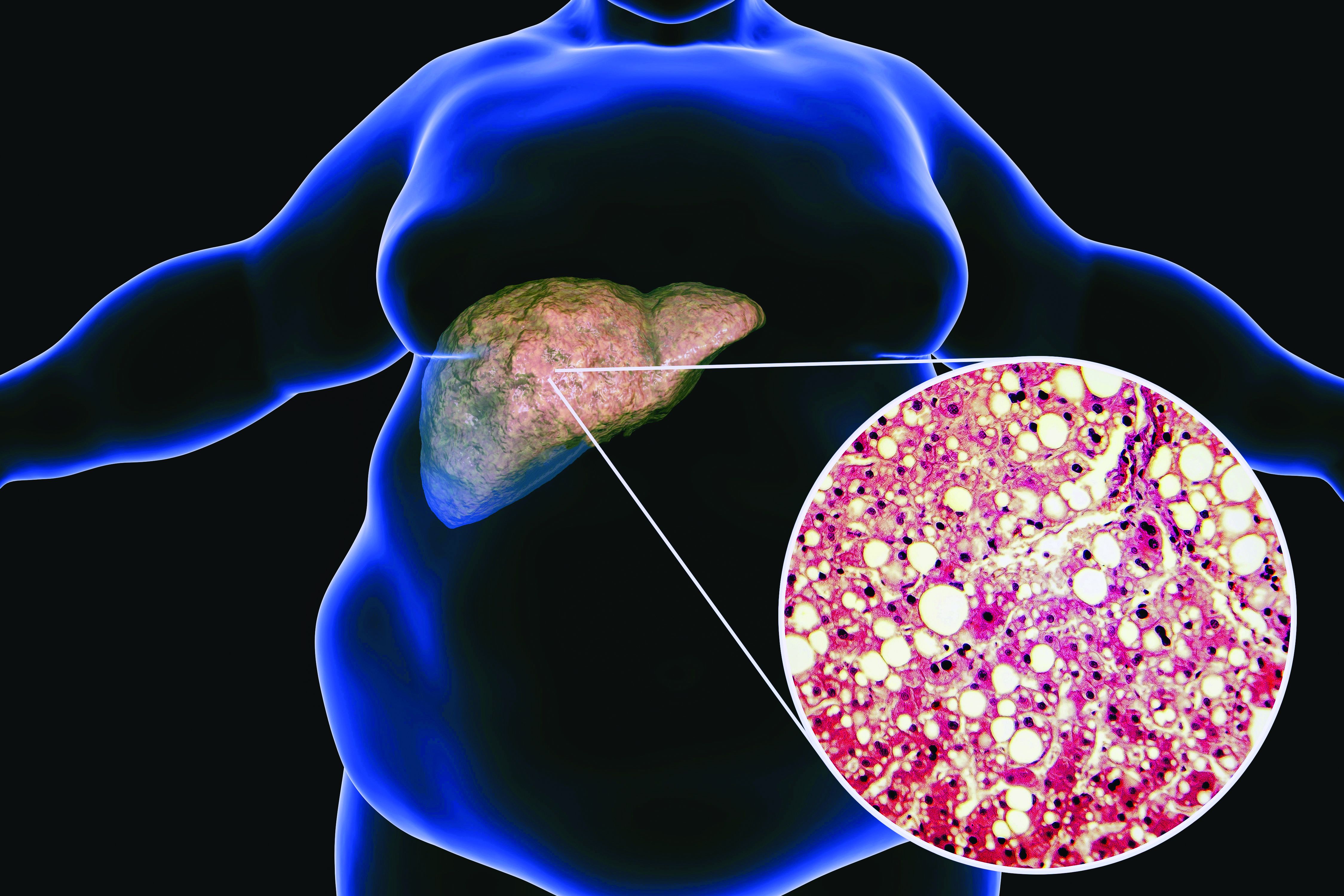
Long COVID associated with risk of metabolic liver disease
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
FROM OPEN FORUM INFECTIOUS DISEASES
Antimicrobial resistance linked to 1.2 million global deaths in 2019
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
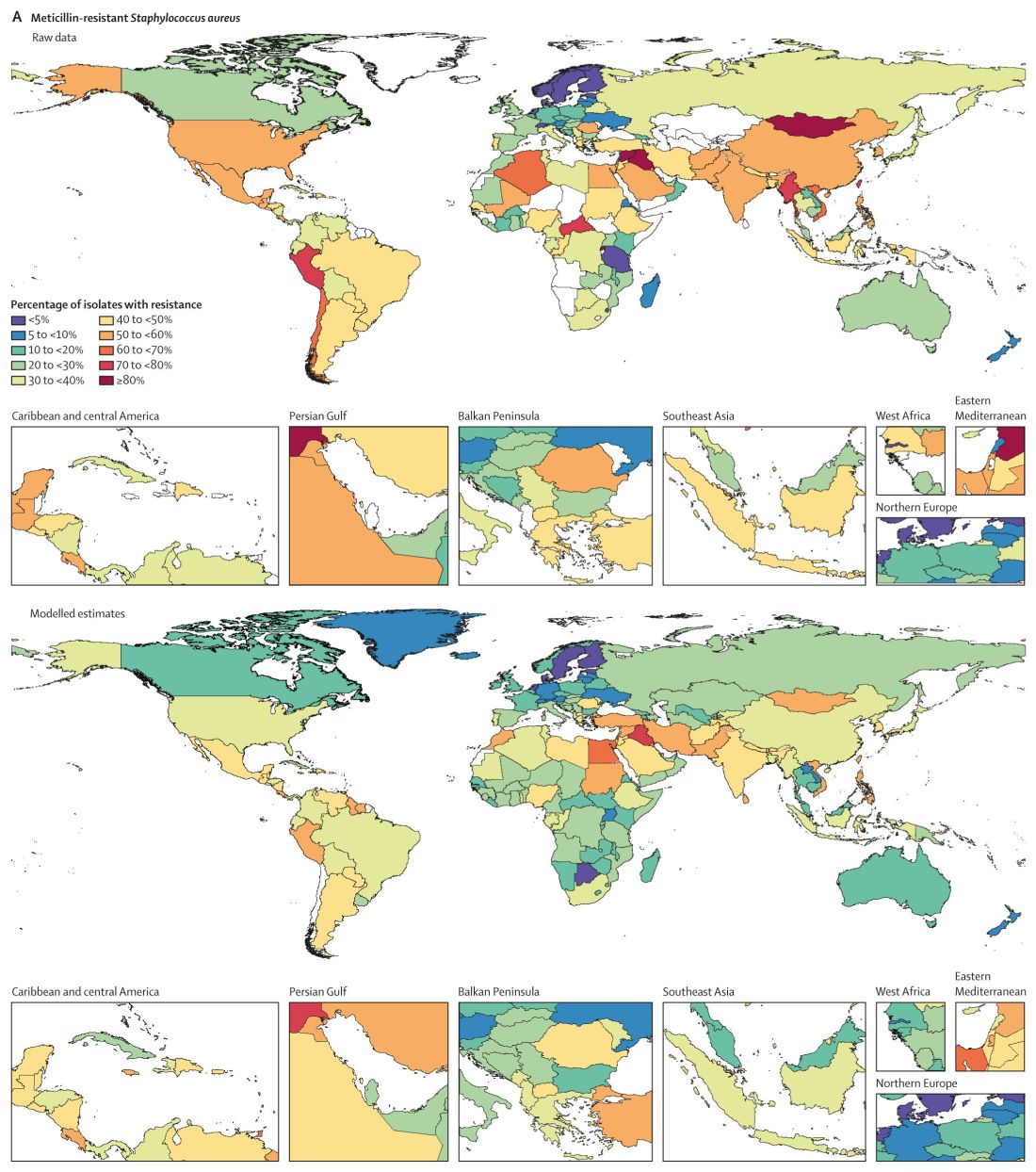
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
‘Incomprehensible’ CABG recommendation raises concerns
BUENOS AIRES – The Latin American Association of Cardiac and Endovascular Surgery (LACES) has demanded “urgent reconsideration” of the decision to downgrade the strength of the recommendation for revascularization or coronary artery bypass graft (CABG) surgery for multivessel disease in the new guideline on coronary artery revascularization, putting it in the same class as the recommendation for percutaneous coronary intervention, which has no apparent advantage over optimal medical therapy.
With the prevalence of stable ischemic heart disease in patients with multivessel disease, the contradiction between the evidence and the new recommendation “may affect the lives and survival of millions of patients worldwide and have a major socio-economic impact,” the association warned in a public letter.
In the 2011 guideline, CABG for patients with multivessel coronary artery disease was given a class I recommendation, which means that it is considered useful and effective and should be performed in the majority of patients in most circumstances. But the new, much weaker class IIb recommendation suggests that the benefit only marginally exceeds the risk and that it should be used selectively and only after careful consideration.
“It is an incomprehensible rollercoaster drop in the recommendation level. We totally disagree. In the absence of evidence, a IIb level provides equal freedom to send a patient to surgery or not. And in patients who are not being sent to surgery, it could take years of survival before we can be sure that we are doing the right thing,” said LACES president Víctor Dayan, MD, PhD, from the cardiovascular center at the Hospital de Clínicas “Dr. Manuel Quintela”, which is part of the School of Medicine at the University of the Republic, Montevideo, Uruguay.
The change in the recommendation for this indication “reflects new evidence showing no advantage of coronary artery bypass grafting over medical therapy alone to improve survival in patients with three-vessel coronary disease with preserved left ventricular function and no left main disease,” according to the authors of the guideline, issued jointly by the American College of Cardiology (ACC), the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI). In particular, they cite the 2019 ISCHEMIA clinical study that failed to show that an early invasive strategy reduces major adverse cardiovascular events, compared with optimal medical therapy and a handful of meta-analyses.
However, ISCHEMIA did not discriminate between the two types of invasive strategy – CABG and percutaneous coronary intervention (PCI) – so cannot be considered as a basis to downgrade the CABG recommendation, Dr. Dayan explained.
“Furthermore, the authors neglected previous RCTs that have shown the survival benefit of CABG in these patients and decided to put PCI in the same [class of recommendation], although no RCT has been able to show any survival advantage of PCI compared to optimal medical treatment,” the LACES letter states.
Basis should be evidence, ‘not inferences’
Three large randomized clinical trials and a 1994 meta-analysis with individual patient data from seven studies firmly established that survival is better with CABG than with medical treatment, the letter continues. However, the guideline authors did not provide any additional randomized clinical trials that refute this evidence.
“Furthermore, the committee disregarded data from the Ten-Year Follow-up Survival of the Medicine, Angioplasty, or Surgery Study (MASS II) randomized control[led] trial, which showed a lower incidence of cardiac mortality (as part of its secondary outcomes) following CABG compared to optimal medical therapy and PCI,” the letter explains.
The guideline authors might have judged current optimal medical therapy to be better than what existed 10, 15, or 30 years ago, diluting the relative benefits of surgery, but the “recommendation in a guideline must act on evidence, not inferences. And there is no evidence to support this drop in recommendation class,” Dr. Dayan said.
Other experts have drawn attention to the fact that two surgical societies – the American Association for Thoracic Surgery (AAST) and the Society of Thoracic Surgeons (STS) – did not endorse the final document, despite having participated in its review, reported this news organization.
“This is a very disappointing update that will negatively affect the lives of many people,” tweeted Marc Pelletier, MD, head of cardiac surgery at University Hospitals, Case Western Reserve University, Cleveland.
Contradictions in the text that examines the evidence and the final recommendations, are “unclear” and “open to various interpretations, when they should be a pillar for decisionmaking,” said Javier Ferrari Ayarragaray, MD, president of the Argentine College of Cardiovascular Surgeons (CACCV) and vice president of LACES.
The new guidelines “show no additional randomized controlled trial to support this downgrade in the level of evidence,” according to a recent CACCV statement. “The inclusion, approval and endorsement of this type of [recommendation,] including [other] international surgical scientific societies, such as STS, AATS, EACTS, LACES[,] is necessary to obtain a better understanding and agreement on the current evidence.”
In a Dec. 17, 2021 response to LACES, Patrick O’Gara, MD, who was chair of the ACC/AHA Joint Committee on Clinical Practice Guidelines at the time, and his successor, Joshua Beckman, MD, explained that both organizations approved the guideline for publication and support its authors “in their interpretation of the published evidence and findings.”
The pair pointed out that the drafting committee members, who have extensive clinical judgment and experience, deliberated extensively on the issue and that the change from a class I to a class IIb recommendation was “carefully considered after a review of the entire available and relevant evidence.”
“When we bring together multiple organizations to review and summarize the evidence, we work collaboratively to interpret the extensive catalog of published and peer-reviewed literature and create clinical practice recommendations,” said Thomas Getchius, director of guideline strategy and operations at the AHA.
“The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed upon by the ACC, AHA, SCAI, and the full drafting committee,” Mr. Getchius said.
Dr. Dayan and Dr. Ferrari Ayarragaray have disclosed no relevant financial relationships. Mr. Getchius is an employee of the American Heart Association.
A version of this article first appeared on Medscape.com.
BUENOS AIRES – The Latin American Association of Cardiac and Endovascular Surgery (LACES) has demanded “urgent reconsideration” of the decision to downgrade the strength of the recommendation for revascularization or coronary artery bypass graft (CABG) surgery for multivessel disease in the new guideline on coronary artery revascularization, putting it in the same class as the recommendation for percutaneous coronary intervention, which has no apparent advantage over optimal medical therapy.
With the prevalence of stable ischemic heart disease in patients with multivessel disease, the contradiction between the evidence and the new recommendation “may affect the lives and survival of millions of patients worldwide and have a major socio-economic impact,” the association warned in a public letter.
In the 2011 guideline, CABG for patients with multivessel coronary artery disease was given a class I recommendation, which means that it is considered useful and effective and should be performed in the majority of patients in most circumstances. But the new, much weaker class IIb recommendation suggests that the benefit only marginally exceeds the risk and that it should be used selectively and only after careful consideration.
“It is an incomprehensible rollercoaster drop in the recommendation level. We totally disagree. In the absence of evidence, a IIb level provides equal freedom to send a patient to surgery or not. And in patients who are not being sent to surgery, it could take years of survival before we can be sure that we are doing the right thing,” said LACES president Víctor Dayan, MD, PhD, from the cardiovascular center at the Hospital de Clínicas “Dr. Manuel Quintela”, which is part of the School of Medicine at the University of the Republic, Montevideo, Uruguay.
The change in the recommendation for this indication “reflects new evidence showing no advantage of coronary artery bypass grafting over medical therapy alone to improve survival in patients with three-vessel coronary disease with preserved left ventricular function and no left main disease,” according to the authors of the guideline, issued jointly by the American College of Cardiology (ACC), the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI). In particular, they cite the 2019 ISCHEMIA clinical study that failed to show that an early invasive strategy reduces major adverse cardiovascular events, compared with optimal medical therapy and a handful of meta-analyses.
However, ISCHEMIA did not discriminate between the two types of invasive strategy – CABG and percutaneous coronary intervention (PCI) – so cannot be considered as a basis to downgrade the CABG recommendation, Dr. Dayan explained.
“Furthermore, the authors neglected previous RCTs that have shown the survival benefit of CABG in these patients and decided to put PCI in the same [class of recommendation], although no RCT has been able to show any survival advantage of PCI compared to optimal medical treatment,” the LACES letter states.
Basis should be evidence, ‘not inferences’
Three large randomized clinical trials and a 1994 meta-analysis with individual patient data from seven studies firmly established that survival is better with CABG than with medical treatment, the letter continues. However, the guideline authors did not provide any additional randomized clinical trials that refute this evidence.
“Furthermore, the committee disregarded data from the Ten-Year Follow-up Survival of the Medicine, Angioplasty, or Surgery Study (MASS II) randomized control[led] trial, which showed a lower incidence of cardiac mortality (as part of its secondary outcomes) following CABG compared to optimal medical therapy and PCI,” the letter explains.
The guideline authors might have judged current optimal medical therapy to be better than what existed 10, 15, or 30 years ago, diluting the relative benefits of surgery, but the “recommendation in a guideline must act on evidence, not inferences. And there is no evidence to support this drop in recommendation class,” Dr. Dayan said.
Other experts have drawn attention to the fact that two surgical societies – the American Association for Thoracic Surgery (AAST) and the Society of Thoracic Surgeons (STS) – did not endorse the final document, despite having participated in its review, reported this news organization.
“This is a very disappointing update that will negatively affect the lives of many people,” tweeted Marc Pelletier, MD, head of cardiac surgery at University Hospitals, Case Western Reserve University, Cleveland.
Contradictions in the text that examines the evidence and the final recommendations, are “unclear” and “open to various interpretations, when they should be a pillar for decisionmaking,” said Javier Ferrari Ayarragaray, MD, president of the Argentine College of Cardiovascular Surgeons (CACCV) and vice president of LACES.
The new guidelines “show no additional randomized controlled trial to support this downgrade in the level of evidence,” according to a recent CACCV statement. “The inclusion, approval and endorsement of this type of [recommendation,] including [other] international surgical scientific societies, such as STS, AATS, EACTS, LACES[,] is necessary to obtain a better understanding and agreement on the current evidence.”
In a Dec. 17, 2021 response to LACES, Patrick O’Gara, MD, who was chair of the ACC/AHA Joint Committee on Clinical Practice Guidelines at the time, and his successor, Joshua Beckman, MD, explained that both organizations approved the guideline for publication and support its authors “in their interpretation of the published evidence and findings.”
The pair pointed out that the drafting committee members, who have extensive clinical judgment and experience, deliberated extensively on the issue and that the change from a class I to a class IIb recommendation was “carefully considered after a review of the entire available and relevant evidence.”
“When we bring together multiple organizations to review and summarize the evidence, we work collaboratively to interpret the extensive catalog of published and peer-reviewed literature and create clinical practice recommendations,” said Thomas Getchius, director of guideline strategy and operations at the AHA.
“The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed upon by the ACC, AHA, SCAI, and the full drafting committee,” Mr. Getchius said.
Dr. Dayan and Dr. Ferrari Ayarragaray have disclosed no relevant financial relationships. Mr. Getchius is an employee of the American Heart Association.
A version of this article first appeared on Medscape.com.
BUENOS AIRES – The Latin American Association of Cardiac and Endovascular Surgery (LACES) has demanded “urgent reconsideration” of the decision to downgrade the strength of the recommendation for revascularization or coronary artery bypass graft (CABG) surgery for multivessel disease in the new guideline on coronary artery revascularization, putting it in the same class as the recommendation for percutaneous coronary intervention, which has no apparent advantage over optimal medical therapy.
With the prevalence of stable ischemic heart disease in patients with multivessel disease, the contradiction between the evidence and the new recommendation “may affect the lives and survival of millions of patients worldwide and have a major socio-economic impact,” the association warned in a public letter.
In the 2011 guideline, CABG for patients with multivessel coronary artery disease was given a class I recommendation, which means that it is considered useful and effective and should be performed in the majority of patients in most circumstances. But the new, much weaker class IIb recommendation suggests that the benefit only marginally exceeds the risk and that it should be used selectively and only after careful consideration.
“It is an incomprehensible rollercoaster drop in the recommendation level. We totally disagree. In the absence of evidence, a IIb level provides equal freedom to send a patient to surgery or not. And in patients who are not being sent to surgery, it could take years of survival before we can be sure that we are doing the right thing,” said LACES president Víctor Dayan, MD, PhD, from the cardiovascular center at the Hospital de Clínicas “Dr. Manuel Quintela”, which is part of the School of Medicine at the University of the Republic, Montevideo, Uruguay.
The change in the recommendation for this indication “reflects new evidence showing no advantage of coronary artery bypass grafting over medical therapy alone to improve survival in patients with three-vessel coronary disease with preserved left ventricular function and no left main disease,” according to the authors of the guideline, issued jointly by the American College of Cardiology (ACC), the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI). In particular, they cite the 2019 ISCHEMIA clinical study that failed to show that an early invasive strategy reduces major adverse cardiovascular events, compared with optimal medical therapy and a handful of meta-analyses.
However, ISCHEMIA did not discriminate between the two types of invasive strategy – CABG and percutaneous coronary intervention (PCI) – so cannot be considered as a basis to downgrade the CABG recommendation, Dr. Dayan explained.
“Furthermore, the authors neglected previous RCTs that have shown the survival benefit of CABG in these patients and decided to put PCI in the same [class of recommendation], although no RCT has been able to show any survival advantage of PCI compared to optimal medical treatment,” the LACES letter states.
Basis should be evidence, ‘not inferences’
Three large randomized clinical trials and a 1994 meta-analysis with individual patient data from seven studies firmly established that survival is better with CABG than with medical treatment, the letter continues. However, the guideline authors did not provide any additional randomized clinical trials that refute this evidence.
“Furthermore, the committee disregarded data from the Ten-Year Follow-up Survival of the Medicine, Angioplasty, or Surgery Study (MASS II) randomized control[led] trial, which showed a lower incidence of cardiac mortality (as part of its secondary outcomes) following CABG compared to optimal medical therapy and PCI,” the letter explains.
The guideline authors might have judged current optimal medical therapy to be better than what existed 10, 15, or 30 years ago, diluting the relative benefits of surgery, but the “recommendation in a guideline must act on evidence, not inferences. And there is no evidence to support this drop in recommendation class,” Dr. Dayan said.
Other experts have drawn attention to the fact that two surgical societies – the American Association for Thoracic Surgery (AAST) and the Society of Thoracic Surgeons (STS) – did not endorse the final document, despite having participated in its review, reported this news organization.
“This is a very disappointing update that will negatively affect the lives of many people,” tweeted Marc Pelletier, MD, head of cardiac surgery at University Hospitals, Case Western Reserve University, Cleveland.
Contradictions in the text that examines the evidence and the final recommendations, are “unclear” and “open to various interpretations, when they should be a pillar for decisionmaking,” said Javier Ferrari Ayarragaray, MD, president of the Argentine College of Cardiovascular Surgeons (CACCV) and vice president of LACES.
The new guidelines “show no additional randomized controlled trial to support this downgrade in the level of evidence,” according to a recent CACCV statement. “The inclusion, approval and endorsement of this type of [recommendation,] including [other] international surgical scientific societies, such as STS, AATS, EACTS, LACES[,] is necessary to obtain a better understanding and agreement on the current evidence.”
In a Dec. 17, 2021 response to LACES, Patrick O’Gara, MD, who was chair of the ACC/AHA Joint Committee on Clinical Practice Guidelines at the time, and his successor, Joshua Beckman, MD, explained that both organizations approved the guideline for publication and support its authors “in their interpretation of the published evidence and findings.”
The pair pointed out that the drafting committee members, who have extensive clinical judgment and experience, deliberated extensively on the issue and that the change from a class I to a class IIb recommendation was “carefully considered after a review of the entire available and relevant evidence.”
“When we bring together multiple organizations to review and summarize the evidence, we work collaboratively to interpret the extensive catalog of published and peer-reviewed literature and create clinical practice recommendations,” said Thomas Getchius, director of guideline strategy and operations at the AHA.
“The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed upon by the ACC, AHA, SCAI, and the full drafting committee,” Mr. Getchius said.
Dr. Dayan and Dr. Ferrari Ayarragaray have disclosed no relevant financial relationships. Mr. Getchius is an employee of the American Heart Association.
A version of this article first appeared on Medscape.com.
Five things you should know about ‘free’ at-home COVID tests
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Novel biomarker found for Alzheimer’s disease
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
Two studies detail the dangers of COVID in pregnancy
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Breastfeeding linked to lower CVD risk in later life
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.