User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Uptake uncertain for potent new LDL-lowerer inclisiran
As inclisiran, a first-in-class LDL-cholesterol lowering drug, enters the U.S. market following Food and Drug Administration approval in December 2021, several issues muddy how popular inclisiran will be in actual practice. That’s despite stellar phase 3 trial evidence for safety, tolerability, and a potent lipid-lowering effect.
The active ingredient of inclisiran (Leqvio) is a small interfering RNA (siRNA) molecule that shuts down production of the PCSK9 (proprotein convertase subtilisin/kexin type 9) protein, an enzyme that’s made and functions primarily in the liver and degrades cellular receptors for LDL cholesterol. Inhibiting PCSK9 production means LDL-cholesterol receptors accumulate and boost the ability of liver cells to pull more LDL cholesterol out of blood.
PCSK9 inhibition is the most potent LDL-cholesterol lowering method now available, and it works well in patients who have maxed out LDL reduction by diet and statin treatment. The siRNA of inclisiran is tweaked to target the molecule to the surface of liver cells following subcutaneous injection. Other modifications of the siRNA give it stability that allows twice-a-year dosing, although patients receive a third injection during their first year to hasten a maximum treatment effect.
Inclisiran’s FDA approval relied on results from three pivotal trials that together enrolled 3,660 patients with either atherosclerotic cardiovascular disease (ASCVD), ASCVD risk equivalents, or heterozygous familial hypercholesterolemia (HeFH), and LDL-cholesterol levels of at least 70 mg/dL in those with established ASCVD, or at least 100 mg/dL in other patients. (HeFH and ASCVD are the drug’s approved indications.) Pooled data from the three trials showed that inclisiran was safe and well tolerated during 18 months and produced an average LDL-cholesterol reduction after 510 days (1.4 years) of about 51% compared to baseline after correction for placebo effects (J Am Coll Cardiol. 2021 Mar 9;77 [9]:1182-93).
These data showed inclisiran was about as safe and effective for reducing LDL-cholesterol as agents from another class of PCSK9 inhibitors that rely on injected antibodies to inactivate PCSK9. Two agents from this class, alirocumab (Praluent) and evolocumab (Repatha), both came on the U.S. market in 2015. Although their performance in routine practice during the ensuing 6-plus years has been as safe and effective as what they showed in their respective registration trials, they have faced a rocky uptake road that’s been primarily hindered by the hefty price tag that both drugs carry.
Prior-authorization blues
When they first came out, evolocumab and alirocumab were burdened by annual drug costs of roughly $14,000, a fact that led to widespread prior-authorization and copay barriers set up by U.S. insurers. Although these barriers gradually lessened over time, in part aided by a substantial price cut for both drugs that led to annual drug costs more in the range of $6,000/year, they remain relatively pricey and are still not easy to start in patients because of prior-authorization requirements, said clinicians.
Recent penetration of the older PCSK9 inhibitors into eligible U.S. patients “is only about 1%-2%, based on the latest data,” said Michael H. Davidson, MD, a lipid specialist and director of Preventive Cardiology at the University of Chicago.
“We have these great, effective drugs, but they haven’t really made an impact over the past 5 years,” because of very limited uptake, a situation Dr. Davidson called “very disappointing,” during an interview.
Given this recent history, inclisiran, another expensive PCSK9 inhibitor, may face similar coverage pushback as it hits the U.S. market with a retail price, announced by its manufacturer Novartis, of $3,250/dose. This means that patients who start the drug and receive their initial dose, a second dose after 3 months, and then additional doses every 6 months, rack up a drug cost of close to $10,000 the first year on the drug and $6,500 each subsequent year.
This treatment schedule highlights the major logistical difference that distinguishes inclisiran from the antibody-based PCSK9 inhibitors, which are given by repeated subcutaneous injection every 2 or 4 weeks, usually with patients self-injecting the drugs at home. The less-frequent dosing schedule for inclisiran prompted the drug’s developers to schedule injections by a clinician in an office setting in the pivotal trials, which led to labeling for inclisiran that specifies administration only by a health care professional.
The ‘buy-and-bill’ coverage model
This difference in drug administration between inclisiran and the antibody-based PCSK9 inhibitors set up Novartis to promote insurance reimbursement for inclisiran using a “buy-and-bill” paradigm that was first developed for oncology drugs and which may provide a loophole around the prior-authorization roadblocks that hindered early uptake of the antibody-based PCSK9 inhibitors.
It’s also an approach that has made U.S. clinicians unsure how it will play out in practice. Infrequent inclisiran dosing may also boost patient compliance.
“Adherence is the greatest challenge in preventive cardiology, and thus inclisiran has the potential to be a game changer,” commented Christie M. Ballantyne, MD, professor and chief of cardiology at Baylor College of Medicine, Houston.
“Will it be easier for physicians to write a prescription and for patients to get the medication without a demanding and frustrating prior-authorization process?” he wondered during an interview. “I’m waiting to see how this unfolds, especially in systems where pharmacy is not fully integrated with the outpatient setting. In some ways, this is as big of an experiment as was development of the drug,” Dr. Ballantyne said.
Although the prior-authorization hoops for evolocumab and alirocumab have become easier to jump through, “most physicians don’t have the resources to handle it and don’t bother,” noted Dr. Davidson, and he’s concerned that infrastructure challenges will also hamper the buy-and-bill strategy for inclisiran.
He also expressed skepticism that the prior-authorization barrier will disappear. “Payers don’t want to open a large population to a very expensive drug without some gatekeeping,” he said, while acknowledging that in late January 2022 he did not yet have personal experience administering inclisiran or navigating its insurance reimbursement.
Boosting patient compliance
Dr. Davidson agreed that the prospect for enhanced patient compliance with inclisiran was intriguing and had already drawn the interest of some of his patients.
“There is a lot of appeal” to a treatment that’s only given once every 6 months, he said. “Compliance is a major issue, and this is less work for patients.”
“The biggest possible attraction of inclisiran is that it is given twice a year, but whether this plays out as anticipated in the real world need to be seen,” cautioned Vijay Nambi, MD, a cardiologist at the Michael E. DeBakey VA Hospital, Houston, and at Baylor College of Medicine who has written about inclisiran. He noted that while two doses a year is “on paper very attractive,” this scheme opens the door to missed or delayed appointments because of vacations, other patient travel, or events like a pandemic.
“The biggest pro for inclisiran is the dosing schedule,” said Chandni Bardolia, PharmD, a drug information specialist at Tabula Rasa Healthcare, Moorestown, N.J., who has analyzed and written about inclisiran and other lipid-lowering medications. “Twice yearly dosing following initiation will be a huge benefit to improve adherence and reduce the number of injections.”
However, inclisiran’s attractive dosing schedule as well as its safety and potent efficacy do not tell the whole story, she highlighted in an interview.
Inclisiran’s clinical evidence still cooking
“I see inclisiran as a last-line drug, mainly because the current alternatives have more safety and efficacy data,” Dr. Bardolia said.
Inclisiran’s “cost and the fact that there are other agents with clinical outcome data already available [alirocumab and evolocumab] means inclisiran is not a first-line agent after statins,” agreed Dr. Nambi.
The FDA based its inclisiran approval entirely on the drug’s demonstrated safety and LDL-lowering efficacy. The cardiovascular outcomes trial for inclisiran, ORION-4, with about 15,000 enrolled patients, started in 2018 and remains in progress with full results expected in 2026.
The lack of clinical outcomes data for inclisiran is a major limitation, said Neil J. Stone, MD, a cardiologist and professor at Northwestern University, Chicago, and vice chair of the panel that wrote the most recent cholesterol guideline for the American College of Cardiology and American Heart Association.
“My greatest concern is the lack of outcome trial data. That’s very important,” Dr. Stone said in an interview.
But others minimize this limitation given the overwhelming evidence that links lower levels of LDL-cholesterol to reduced clinical events.
Most clinicians “support lower LDL as a surrogate” for reduced clinical events, “just like blood pressure and hemoglobin A1c,” noted Dr. Davidson, although he conceded that a “substantial minority wants to wait to see inclisiran’s outcome benefits.”
It’s all about price
While opinions are mixed on the need for clinical outcomes data, experts are more uniform in seeing drug prices that run to several thousands per year as the main uptake issue.
“We need to look at the cost-efficacy with inclisiran, and we need benefit data to determine this,” said Dr. Stone.
“Outcomes data are central to characterizing value. I imagine that costs will impact adoption and dissemination” of inclisiran, commented Paul L. Hess, MD, a cardiologist at the Rocky Mountain Regional VA Medical Center, Denver.
Patient interest in less frequent dosing will be important for driving use, but “ultimately cost will be the most important driving factor,” for inclisiran uptake, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado School of Medicine, Aurora.
Dr. Davidson has ties to New Amsterdam Pharma and Amgen, which markets evolocumab (Repatha). Dr. Ballantyne is a consultant to numerous companies, including Amgen and Regeneron, which market alirocumab (Praluent). Dr. Nambi has been a site investigator for studies sponsored by Amgen, and by Merck, which markets the LDL-cholesterol drug ezetimibe (Zetia) and is developing an oral PCSK9 inhibitor (he said that the views he expressed are his own and don’t represent that of the department of Veterans Affairs or Baylor.) Dr. Bardolia had no disclosures beyond her employment at Tabula Rasa Healthcare. Dr. Stone, Dr. Hess, and Dr. Eckel had no relevant disclosures.
As inclisiran, a first-in-class LDL-cholesterol lowering drug, enters the U.S. market following Food and Drug Administration approval in December 2021, several issues muddy how popular inclisiran will be in actual practice. That’s despite stellar phase 3 trial evidence for safety, tolerability, and a potent lipid-lowering effect.
The active ingredient of inclisiran (Leqvio) is a small interfering RNA (siRNA) molecule that shuts down production of the PCSK9 (proprotein convertase subtilisin/kexin type 9) protein, an enzyme that’s made and functions primarily in the liver and degrades cellular receptors for LDL cholesterol. Inhibiting PCSK9 production means LDL-cholesterol receptors accumulate and boost the ability of liver cells to pull more LDL cholesterol out of blood.
PCSK9 inhibition is the most potent LDL-cholesterol lowering method now available, and it works well in patients who have maxed out LDL reduction by diet and statin treatment. The siRNA of inclisiran is tweaked to target the molecule to the surface of liver cells following subcutaneous injection. Other modifications of the siRNA give it stability that allows twice-a-year dosing, although patients receive a third injection during their first year to hasten a maximum treatment effect.
Inclisiran’s FDA approval relied on results from three pivotal trials that together enrolled 3,660 patients with either atherosclerotic cardiovascular disease (ASCVD), ASCVD risk equivalents, or heterozygous familial hypercholesterolemia (HeFH), and LDL-cholesterol levels of at least 70 mg/dL in those with established ASCVD, or at least 100 mg/dL in other patients. (HeFH and ASCVD are the drug’s approved indications.) Pooled data from the three trials showed that inclisiran was safe and well tolerated during 18 months and produced an average LDL-cholesterol reduction after 510 days (1.4 years) of about 51% compared to baseline after correction for placebo effects (J Am Coll Cardiol. 2021 Mar 9;77 [9]:1182-93).
These data showed inclisiran was about as safe and effective for reducing LDL-cholesterol as agents from another class of PCSK9 inhibitors that rely on injected antibodies to inactivate PCSK9. Two agents from this class, alirocumab (Praluent) and evolocumab (Repatha), both came on the U.S. market in 2015. Although their performance in routine practice during the ensuing 6-plus years has been as safe and effective as what they showed in their respective registration trials, they have faced a rocky uptake road that’s been primarily hindered by the hefty price tag that both drugs carry.
Prior-authorization blues
When they first came out, evolocumab and alirocumab were burdened by annual drug costs of roughly $14,000, a fact that led to widespread prior-authorization and copay barriers set up by U.S. insurers. Although these barriers gradually lessened over time, in part aided by a substantial price cut for both drugs that led to annual drug costs more in the range of $6,000/year, they remain relatively pricey and are still not easy to start in patients because of prior-authorization requirements, said clinicians.
Recent penetration of the older PCSK9 inhibitors into eligible U.S. patients “is only about 1%-2%, based on the latest data,” said Michael H. Davidson, MD, a lipid specialist and director of Preventive Cardiology at the University of Chicago.
“We have these great, effective drugs, but they haven’t really made an impact over the past 5 years,” because of very limited uptake, a situation Dr. Davidson called “very disappointing,” during an interview.
Given this recent history, inclisiran, another expensive PCSK9 inhibitor, may face similar coverage pushback as it hits the U.S. market with a retail price, announced by its manufacturer Novartis, of $3,250/dose. This means that patients who start the drug and receive their initial dose, a second dose after 3 months, and then additional doses every 6 months, rack up a drug cost of close to $10,000 the first year on the drug and $6,500 each subsequent year.
This treatment schedule highlights the major logistical difference that distinguishes inclisiran from the antibody-based PCSK9 inhibitors, which are given by repeated subcutaneous injection every 2 or 4 weeks, usually with patients self-injecting the drugs at home. The less-frequent dosing schedule for inclisiran prompted the drug’s developers to schedule injections by a clinician in an office setting in the pivotal trials, which led to labeling for inclisiran that specifies administration only by a health care professional.
The ‘buy-and-bill’ coverage model
This difference in drug administration between inclisiran and the antibody-based PCSK9 inhibitors set up Novartis to promote insurance reimbursement for inclisiran using a “buy-and-bill” paradigm that was first developed for oncology drugs and which may provide a loophole around the prior-authorization roadblocks that hindered early uptake of the antibody-based PCSK9 inhibitors.
It’s also an approach that has made U.S. clinicians unsure how it will play out in practice. Infrequent inclisiran dosing may also boost patient compliance.
“Adherence is the greatest challenge in preventive cardiology, and thus inclisiran has the potential to be a game changer,” commented Christie M. Ballantyne, MD, professor and chief of cardiology at Baylor College of Medicine, Houston.
“Will it be easier for physicians to write a prescription and for patients to get the medication without a demanding and frustrating prior-authorization process?” he wondered during an interview. “I’m waiting to see how this unfolds, especially in systems where pharmacy is not fully integrated with the outpatient setting. In some ways, this is as big of an experiment as was development of the drug,” Dr. Ballantyne said.
Although the prior-authorization hoops for evolocumab and alirocumab have become easier to jump through, “most physicians don’t have the resources to handle it and don’t bother,” noted Dr. Davidson, and he’s concerned that infrastructure challenges will also hamper the buy-and-bill strategy for inclisiran.
He also expressed skepticism that the prior-authorization barrier will disappear. “Payers don’t want to open a large population to a very expensive drug without some gatekeeping,” he said, while acknowledging that in late January 2022 he did not yet have personal experience administering inclisiran or navigating its insurance reimbursement.
Boosting patient compliance
Dr. Davidson agreed that the prospect for enhanced patient compliance with inclisiran was intriguing and had already drawn the interest of some of his patients.
“There is a lot of appeal” to a treatment that’s only given once every 6 months, he said. “Compliance is a major issue, and this is less work for patients.”
“The biggest possible attraction of inclisiran is that it is given twice a year, but whether this plays out as anticipated in the real world need to be seen,” cautioned Vijay Nambi, MD, a cardiologist at the Michael E. DeBakey VA Hospital, Houston, and at Baylor College of Medicine who has written about inclisiran. He noted that while two doses a year is “on paper very attractive,” this scheme opens the door to missed or delayed appointments because of vacations, other patient travel, or events like a pandemic.
“The biggest pro for inclisiran is the dosing schedule,” said Chandni Bardolia, PharmD, a drug information specialist at Tabula Rasa Healthcare, Moorestown, N.J., who has analyzed and written about inclisiran and other lipid-lowering medications. “Twice yearly dosing following initiation will be a huge benefit to improve adherence and reduce the number of injections.”
However, inclisiran’s attractive dosing schedule as well as its safety and potent efficacy do not tell the whole story, she highlighted in an interview.
Inclisiran’s clinical evidence still cooking
“I see inclisiran as a last-line drug, mainly because the current alternatives have more safety and efficacy data,” Dr. Bardolia said.
Inclisiran’s “cost and the fact that there are other agents with clinical outcome data already available [alirocumab and evolocumab] means inclisiran is not a first-line agent after statins,” agreed Dr. Nambi.
The FDA based its inclisiran approval entirely on the drug’s demonstrated safety and LDL-lowering efficacy. The cardiovascular outcomes trial for inclisiran, ORION-4, with about 15,000 enrolled patients, started in 2018 and remains in progress with full results expected in 2026.
The lack of clinical outcomes data for inclisiran is a major limitation, said Neil J. Stone, MD, a cardiologist and professor at Northwestern University, Chicago, and vice chair of the panel that wrote the most recent cholesterol guideline for the American College of Cardiology and American Heart Association.
“My greatest concern is the lack of outcome trial data. That’s very important,” Dr. Stone said in an interview.
But others minimize this limitation given the overwhelming evidence that links lower levels of LDL-cholesterol to reduced clinical events.
Most clinicians “support lower LDL as a surrogate” for reduced clinical events, “just like blood pressure and hemoglobin A1c,” noted Dr. Davidson, although he conceded that a “substantial minority wants to wait to see inclisiran’s outcome benefits.”
It’s all about price
While opinions are mixed on the need for clinical outcomes data, experts are more uniform in seeing drug prices that run to several thousands per year as the main uptake issue.
“We need to look at the cost-efficacy with inclisiran, and we need benefit data to determine this,” said Dr. Stone.
“Outcomes data are central to characterizing value. I imagine that costs will impact adoption and dissemination” of inclisiran, commented Paul L. Hess, MD, a cardiologist at the Rocky Mountain Regional VA Medical Center, Denver.
Patient interest in less frequent dosing will be important for driving use, but “ultimately cost will be the most important driving factor,” for inclisiran uptake, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado School of Medicine, Aurora.
Dr. Davidson has ties to New Amsterdam Pharma and Amgen, which markets evolocumab (Repatha). Dr. Ballantyne is a consultant to numerous companies, including Amgen and Regeneron, which market alirocumab (Praluent). Dr. Nambi has been a site investigator for studies sponsored by Amgen, and by Merck, which markets the LDL-cholesterol drug ezetimibe (Zetia) and is developing an oral PCSK9 inhibitor (he said that the views he expressed are his own and don’t represent that of the department of Veterans Affairs or Baylor.) Dr. Bardolia had no disclosures beyond her employment at Tabula Rasa Healthcare. Dr. Stone, Dr. Hess, and Dr. Eckel had no relevant disclosures.
As inclisiran, a first-in-class LDL-cholesterol lowering drug, enters the U.S. market following Food and Drug Administration approval in December 2021, several issues muddy how popular inclisiran will be in actual practice. That’s despite stellar phase 3 trial evidence for safety, tolerability, and a potent lipid-lowering effect.
The active ingredient of inclisiran (Leqvio) is a small interfering RNA (siRNA) molecule that shuts down production of the PCSK9 (proprotein convertase subtilisin/kexin type 9) protein, an enzyme that’s made and functions primarily in the liver and degrades cellular receptors for LDL cholesterol. Inhibiting PCSK9 production means LDL-cholesterol receptors accumulate and boost the ability of liver cells to pull more LDL cholesterol out of blood.
PCSK9 inhibition is the most potent LDL-cholesterol lowering method now available, and it works well in patients who have maxed out LDL reduction by diet and statin treatment. The siRNA of inclisiran is tweaked to target the molecule to the surface of liver cells following subcutaneous injection. Other modifications of the siRNA give it stability that allows twice-a-year dosing, although patients receive a third injection during their first year to hasten a maximum treatment effect.
Inclisiran’s FDA approval relied on results from three pivotal trials that together enrolled 3,660 patients with either atherosclerotic cardiovascular disease (ASCVD), ASCVD risk equivalents, or heterozygous familial hypercholesterolemia (HeFH), and LDL-cholesterol levels of at least 70 mg/dL in those with established ASCVD, or at least 100 mg/dL in other patients. (HeFH and ASCVD are the drug’s approved indications.) Pooled data from the three trials showed that inclisiran was safe and well tolerated during 18 months and produced an average LDL-cholesterol reduction after 510 days (1.4 years) of about 51% compared to baseline after correction for placebo effects (J Am Coll Cardiol. 2021 Mar 9;77 [9]:1182-93).
These data showed inclisiran was about as safe and effective for reducing LDL-cholesterol as agents from another class of PCSK9 inhibitors that rely on injected antibodies to inactivate PCSK9. Two agents from this class, alirocumab (Praluent) and evolocumab (Repatha), both came on the U.S. market in 2015. Although their performance in routine practice during the ensuing 6-plus years has been as safe and effective as what they showed in their respective registration trials, they have faced a rocky uptake road that’s been primarily hindered by the hefty price tag that both drugs carry.
Prior-authorization blues
When they first came out, evolocumab and alirocumab were burdened by annual drug costs of roughly $14,000, a fact that led to widespread prior-authorization and copay barriers set up by U.S. insurers. Although these barriers gradually lessened over time, in part aided by a substantial price cut for both drugs that led to annual drug costs more in the range of $6,000/year, they remain relatively pricey and are still not easy to start in patients because of prior-authorization requirements, said clinicians.
Recent penetration of the older PCSK9 inhibitors into eligible U.S. patients “is only about 1%-2%, based on the latest data,” said Michael H. Davidson, MD, a lipid specialist and director of Preventive Cardiology at the University of Chicago.
“We have these great, effective drugs, but they haven’t really made an impact over the past 5 years,” because of very limited uptake, a situation Dr. Davidson called “very disappointing,” during an interview.
Given this recent history, inclisiran, another expensive PCSK9 inhibitor, may face similar coverage pushback as it hits the U.S. market with a retail price, announced by its manufacturer Novartis, of $3,250/dose. This means that patients who start the drug and receive their initial dose, a second dose after 3 months, and then additional doses every 6 months, rack up a drug cost of close to $10,000 the first year on the drug and $6,500 each subsequent year.
This treatment schedule highlights the major logistical difference that distinguishes inclisiran from the antibody-based PCSK9 inhibitors, which are given by repeated subcutaneous injection every 2 or 4 weeks, usually with patients self-injecting the drugs at home. The less-frequent dosing schedule for inclisiran prompted the drug’s developers to schedule injections by a clinician in an office setting in the pivotal trials, which led to labeling for inclisiran that specifies administration only by a health care professional.
The ‘buy-and-bill’ coverage model
This difference in drug administration between inclisiran and the antibody-based PCSK9 inhibitors set up Novartis to promote insurance reimbursement for inclisiran using a “buy-and-bill” paradigm that was first developed for oncology drugs and which may provide a loophole around the prior-authorization roadblocks that hindered early uptake of the antibody-based PCSK9 inhibitors.
It’s also an approach that has made U.S. clinicians unsure how it will play out in practice. Infrequent inclisiran dosing may also boost patient compliance.
“Adherence is the greatest challenge in preventive cardiology, and thus inclisiran has the potential to be a game changer,” commented Christie M. Ballantyne, MD, professor and chief of cardiology at Baylor College of Medicine, Houston.
“Will it be easier for physicians to write a prescription and for patients to get the medication without a demanding and frustrating prior-authorization process?” he wondered during an interview. “I’m waiting to see how this unfolds, especially in systems where pharmacy is not fully integrated with the outpatient setting. In some ways, this is as big of an experiment as was development of the drug,” Dr. Ballantyne said.
Although the prior-authorization hoops for evolocumab and alirocumab have become easier to jump through, “most physicians don’t have the resources to handle it and don’t bother,” noted Dr. Davidson, and he’s concerned that infrastructure challenges will also hamper the buy-and-bill strategy for inclisiran.
He also expressed skepticism that the prior-authorization barrier will disappear. “Payers don’t want to open a large population to a very expensive drug without some gatekeeping,” he said, while acknowledging that in late January 2022 he did not yet have personal experience administering inclisiran or navigating its insurance reimbursement.
Boosting patient compliance
Dr. Davidson agreed that the prospect for enhanced patient compliance with inclisiran was intriguing and had already drawn the interest of some of his patients.
“There is a lot of appeal” to a treatment that’s only given once every 6 months, he said. “Compliance is a major issue, and this is less work for patients.”
“The biggest possible attraction of inclisiran is that it is given twice a year, but whether this plays out as anticipated in the real world need to be seen,” cautioned Vijay Nambi, MD, a cardiologist at the Michael E. DeBakey VA Hospital, Houston, and at Baylor College of Medicine who has written about inclisiran. He noted that while two doses a year is “on paper very attractive,” this scheme opens the door to missed or delayed appointments because of vacations, other patient travel, or events like a pandemic.
“The biggest pro for inclisiran is the dosing schedule,” said Chandni Bardolia, PharmD, a drug information specialist at Tabula Rasa Healthcare, Moorestown, N.J., who has analyzed and written about inclisiran and other lipid-lowering medications. “Twice yearly dosing following initiation will be a huge benefit to improve adherence and reduce the number of injections.”
However, inclisiran’s attractive dosing schedule as well as its safety and potent efficacy do not tell the whole story, she highlighted in an interview.
Inclisiran’s clinical evidence still cooking
“I see inclisiran as a last-line drug, mainly because the current alternatives have more safety and efficacy data,” Dr. Bardolia said.
Inclisiran’s “cost and the fact that there are other agents with clinical outcome data already available [alirocumab and evolocumab] means inclisiran is not a first-line agent after statins,” agreed Dr. Nambi.
The FDA based its inclisiran approval entirely on the drug’s demonstrated safety and LDL-lowering efficacy. The cardiovascular outcomes trial for inclisiran, ORION-4, with about 15,000 enrolled patients, started in 2018 and remains in progress with full results expected in 2026.
The lack of clinical outcomes data for inclisiran is a major limitation, said Neil J. Stone, MD, a cardiologist and professor at Northwestern University, Chicago, and vice chair of the panel that wrote the most recent cholesterol guideline for the American College of Cardiology and American Heart Association.
“My greatest concern is the lack of outcome trial data. That’s very important,” Dr. Stone said in an interview.
But others minimize this limitation given the overwhelming evidence that links lower levels of LDL-cholesterol to reduced clinical events.
Most clinicians “support lower LDL as a surrogate” for reduced clinical events, “just like blood pressure and hemoglobin A1c,” noted Dr. Davidson, although he conceded that a “substantial minority wants to wait to see inclisiran’s outcome benefits.”
It’s all about price
While opinions are mixed on the need for clinical outcomes data, experts are more uniform in seeing drug prices that run to several thousands per year as the main uptake issue.
“We need to look at the cost-efficacy with inclisiran, and we need benefit data to determine this,” said Dr. Stone.
“Outcomes data are central to characterizing value. I imagine that costs will impact adoption and dissemination” of inclisiran, commented Paul L. Hess, MD, a cardiologist at the Rocky Mountain Regional VA Medical Center, Denver.
Patient interest in less frequent dosing will be important for driving use, but “ultimately cost will be the most important driving factor,” for inclisiran uptake, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado School of Medicine, Aurora.
Dr. Davidson has ties to New Amsterdam Pharma and Amgen, which markets evolocumab (Repatha). Dr. Ballantyne is a consultant to numerous companies, including Amgen and Regeneron, which market alirocumab (Praluent). Dr. Nambi has been a site investigator for studies sponsored by Amgen, and by Merck, which markets the LDL-cholesterol drug ezetimibe (Zetia) and is developing an oral PCSK9 inhibitor (he said that the views he expressed are his own and don’t represent that of the department of Veterans Affairs or Baylor.) Dr. Bardolia had no disclosures beyond her employment at Tabula Rasa Healthcare. Dr. Stone, Dr. Hess, and Dr. Eckel had no relevant disclosures.
Presence of autoantibodies most predictive of long COVID in study
Other significant early predictors of prolonged COVID symptoms – which the researchers called postacute sequelae – were having type 2 diabetes, SARS-CoV-2 RNAemia, and Epstein-Barr virus (EBV) viremia, Yapeng Su, PhD, of the Institute for Systems Biology (ISB) in Seattle, and colleagues wrote in Cell.
Having EBV viremia suggested that latent EBV has been reactivated, the authors noted.

“The most important postacute sequelae [that is conditions that are consequences of a disease] of COVID is the presence of autoantibodies,” James R. Heath, PhD, president of ISB and a bioengineering professor at the University of Washington, Seattle, said in an interview. “It’s about two times more important than the others.”
Dr. Heath and coauthors said early detection of this and other variables could prompt earlier aggressive treatment in patients susceptible to long COVID and ward off lingering symptoms.
“These predictive measures of long COVID can also help to better inform patients of their possible disease course,” study coauthor Daniel G. Chen, an undergraduate researcher at ISB, said in an interview. “We were also able to partially resolve the immunological underpinnings of some postacute sequelae of COVID in a way that suggested potential therapies, and the timing of those therapies.”

For example, he continued, the use of antivirals very early in the infectious course may mitigate the later development of long COVID. “This will, of course, have to be explored in an appropriately designed clinical trial.
“We also identified biomarkers of certain types of long COVID, such as neurological sequelae. Those biomarkers can help define the condition, which is a first step towards developing treatments.”
Study findings
With COVID patients monitored for 2 or 3 months, the study findings of the international “multiomic profiling” analysis include:
- Subclinical patient autoantibodies that reduce anti–SARS-CoV-2 antibodies suggest there is immune dysregulation during COVID-19 infection.
- Reactivation of latent other viruses during initial infection may be contributing to long COVID.
- Gastrointestinal postacute sequelae of COVID presents with a unique postacute expansion of cytotoxic T cells.
- SARS-CoV-2–specific and cytomegalovirus-specific CD8+ T cells displayed unique dynamics during recovery from infection.
According to the authors, as many as 69% of COVID-19 patients suffer from long COVID – a range of new, recurrent, or ongoing problems 4 or more weeks following initial SARS-CoV-2 infection. These may include memory loss, gastrointestinal distress, fatigue, anosmia, and shortness of breath.
Long COVID has been associated with acute disease severity, and is suspected to be related to autoimmune factors and unresolved viral fragments, according to the paper.
Research methods
The international study did a deep and detailed dive into multiple molecular markers of long COVID. It enrolled 209 COVID-19 patients with varying degrees of disease severity and matched them to 457 healthy controls. The researchers’ goal was to identify discrete and quantifiable long COVID factors and guide possible preemptive treatment.
Patients were assessed at three time points: at initial diagnosis, during the acute disease phase about a week later, and again 2 to 3 months post onset of symptoms after recovery from the acute phase of COVID. At the third assessment, some patients had lingering symptoms such as fatigue (52% ), cough (25%), and loss of taste or sense of smell (18%).
Blood draws were analyzed for autoantibodies and SARS-CoV-2–specific antibodies, global plasma proteomic and metabolomic profiles, and single-cell multiomic characterizations of peripheral blood mononuclear cells.
Each blood draw was paired with nasal-swab and plasma measurements of SARS-CoV-2 viral load and the data sets were integrated with electronic health records and self-reported patient symptoms to guide the interpretation of the molecular signatures of long COVID.
Author conclusions
The authors found an association between T2 hyperinflammation and long COVID–anticipating autoantibodies. This association further implies that hyperinflammation-controlling therapies in the acute stage of COVID may influence whether a patient experiences long COVID. “However, the detailed timing and context of these therapies matter, and, thus, future well-controlled studies will be needed to test these and other therapeutic implications,” Dr. Su and colleagues wrote.
Moreover, the negative correlations between anti–SARS-CoV-2 IgG and certain autoantibodies may suggest that patients with elevated autoantibody levels are more susceptible to breakthrough infections, the authors said.
“Many patients with high autoantibodies simultaneously have low protective antibodies that neutralize SARS-CoV-2, and that’s going to make them more susceptible to breakthrough infections,” Mr. Chen explained.*
“Detectability of most [long COVID-19 factors] at COVID diagnosis emphasizes the importance of early disease measurements for understanding emergent chronic conditions and suggests [long COVID] treatment strategies,” they wrote.
According to Mr. Chen, there are clear similarities in underlying immunobiology between patients with COVID autoantibodies and patients with systemic lupus erythematosus.
“These findings are also helping us frame our thinking around other chronic autoimmune conditions, such as postacute Lyme syndrome, for example,” said Dr. Heath.
The bottom line, said Mr. Chen, is that measuring early long COVID indicators may result in preventive treatments. “An example is the cortisol deficiency we see in certain long COVID patients. There are known treatments such as cortisol replacement therapy that should be explored for this group.”
Outside expert’s take on findings
Commenting on the study, Sherry Hsiang-Yi Chou, MD, who was not involved in the research, called the study a very important first step in understanding the path of this complex phenomenon and perhaps other conditions with long-term side effects.

“The researchers have done huge amount of innovative scientific work. They’ve shown the DNA signature of how our bodies respond to this disease,” said Dr. Chou, who is chief of the division of neurocritical care at Northwestern Medicine in Chicago.
“This type of research will help us scientifically understand and differentiate the various syndromes within long COVID. It will help identify who’s at risk for different aspects of this syndrome and lead to following them for longer periods in clinical trials,” she added.
The authors acknowledged that lengthier studies in larger cohorts were needed to see which patients will develop long-term chronic postacute sequelae of COVID.
This research was supported by the Wilke Family Foundation, the Parker Institute for Cancer Immunotherapy, Merck, and the Biomedical Advanced Research and Development Authority. Other support came from the National Institutes of Health, the Bill and Melinda Gates Foundation, Saint John’s Cancer Center, Fred Hutchinson Cancer Research Center, and the European Union’s Horizon 2020 research and innovation program. Dr. Heath is a cofounder of Pact Pharma. He and several coauthors disclosed various ties to multiple private-sector companies. Mr. Chen and Dr. Chou had no competing interests.
*Correction, 1/28: An earlier version of this story misidentified Daniel G. Chen, an undergraduate researcher at ISB.
Other significant early predictors of prolonged COVID symptoms – which the researchers called postacute sequelae – were having type 2 diabetes, SARS-CoV-2 RNAemia, and Epstein-Barr virus (EBV) viremia, Yapeng Su, PhD, of the Institute for Systems Biology (ISB) in Seattle, and colleagues wrote in Cell.
Having EBV viremia suggested that latent EBV has been reactivated, the authors noted.
“The most important postacute sequelae [that is conditions that are consequences of a disease] of COVID is the presence of autoantibodies,” James R. Heath, PhD, president of ISB and a bioengineering professor at the University of Washington, Seattle, said in an interview. “It’s about two times more important than the others.”
Dr. Heath and coauthors said early detection of this and other variables could prompt earlier aggressive treatment in patients susceptible to long COVID and ward off lingering symptoms.
“These predictive measures of long COVID can also help to better inform patients of their possible disease course,” study coauthor Daniel G. Chen, an undergraduate researcher at ISB, said in an interview. “We were also able to partially resolve the immunological underpinnings of some postacute sequelae of COVID in a way that suggested potential therapies, and the timing of those therapies.”
For example, he continued, the use of antivirals very early in the infectious course may mitigate the later development of long COVID. “This will, of course, have to be explored in an appropriately designed clinical trial.
“We also identified biomarkers of certain types of long COVID, such as neurological sequelae. Those biomarkers can help define the condition, which is a first step towards developing treatments.”
Study findings
With COVID patients monitored for 2 or 3 months, the study findings of the international “multiomic profiling” analysis include:
- Subclinical patient autoantibodies that reduce anti–SARS-CoV-2 antibodies suggest there is immune dysregulation during COVID-19 infection.
- Reactivation of latent other viruses during initial infection may be contributing to long COVID.
- Gastrointestinal postacute sequelae of COVID presents with a unique postacute expansion of cytotoxic T cells.
- SARS-CoV-2–specific and cytomegalovirus-specific CD8+ T cells displayed unique dynamics during recovery from infection.
According to the authors, as many as 69% of COVID-19 patients suffer from long COVID – a range of new, recurrent, or ongoing problems 4 or more weeks following initial SARS-CoV-2 infection. These may include memory loss, gastrointestinal distress, fatigue, anosmia, and shortness of breath.
Long COVID has been associated with acute disease severity, and is suspected to be related to autoimmune factors and unresolved viral fragments, according to the paper.
Research methods
The international study did a deep and detailed dive into multiple molecular markers of long COVID. It enrolled 209 COVID-19 patients with varying degrees of disease severity and matched them to 457 healthy controls. The researchers’ goal was to identify discrete and quantifiable long COVID factors and guide possible preemptive treatment.
Patients were assessed at three time points: at initial diagnosis, during the acute disease phase about a week later, and again 2 to 3 months post onset of symptoms after recovery from the acute phase of COVID. At the third assessment, some patients had lingering symptoms such as fatigue (52% ), cough (25%), and loss of taste or sense of smell (18%).
Blood draws were analyzed for autoantibodies and SARS-CoV-2–specific antibodies, global plasma proteomic and metabolomic profiles, and single-cell multiomic characterizations of peripheral blood mononuclear cells.
Each blood draw was paired with nasal-swab and plasma measurements of SARS-CoV-2 viral load and the data sets were integrated with electronic health records and self-reported patient symptoms to guide the interpretation of the molecular signatures of long COVID.
Author conclusions
The authors found an association between T2 hyperinflammation and long COVID–anticipating autoantibodies. This association further implies that hyperinflammation-controlling therapies in the acute stage of COVID may influence whether a patient experiences long COVID. “However, the detailed timing and context of these therapies matter, and, thus, future well-controlled studies will be needed to test these and other therapeutic implications,” Dr. Su and colleagues wrote.
Moreover, the negative correlations between anti–SARS-CoV-2 IgG and certain autoantibodies may suggest that patients with elevated autoantibody levels are more susceptible to breakthrough infections, the authors said.
“Many patients with high autoantibodies simultaneously have low protective antibodies that neutralize SARS-CoV-2, and that’s going to make them more susceptible to breakthrough infections,” Mr. Chen explained.*
“Detectability of most [long COVID-19 factors] at COVID diagnosis emphasizes the importance of early disease measurements for understanding emergent chronic conditions and suggests [long COVID] treatment strategies,” they wrote.
According to Mr. Chen, there are clear similarities in underlying immunobiology between patients with COVID autoantibodies and patients with systemic lupus erythematosus.
“These findings are also helping us frame our thinking around other chronic autoimmune conditions, such as postacute Lyme syndrome, for example,” said Dr. Heath.
The bottom line, said Mr. Chen, is that measuring early long COVID indicators may result in preventive treatments. “An example is the cortisol deficiency we see in certain long COVID patients. There are known treatments such as cortisol replacement therapy that should be explored for this group.”
Outside expert’s take on findings
Commenting on the study, Sherry Hsiang-Yi Chou, MD, who was not involved in the research, called the study a very important first step in understanding the path of this complex phenomenon and perhaps other conditions with long-term side effects.
“The researchers have done huge amount of innovative scientific work. They’ve shown the DNA signature of how our bodies respond to this disease,” said Dr. Chou, who is chief of the division of neurocritical care at Northwestern Medicine in Chicago.
“This type of research will help us scientifically understand and differentiate the various syndromes within long COVID. It will help identify who’s at risk for different aspects of this syndrome and lead to following them for longer periods in clinical trials,” she added.
The authors acknowledged that lengthier studies in larger cohorts were needed to see which patients will develop long-term chronic postacute sequelae of COVID.
This research was supported by the Wilke Family Foundation, the Parker Institute for Cancer Immunotherapy, Merck, and the Biomedical Advanced Research and Development Authority. Other support came from the National Institutes of Health, the Bill and Melinda Gates Foundation, Saint John’s Cancer Center, Fred Hutchinson Cancer Research Center, and the European Union’s Horizon 2020 research and innovation program. Dr. Heath is a cofounder of Pact Pharma. He and several coauthors disclosed various ties to multiple private-sector companies. Mr. Chen and Dr. Chou had no competing interests.
*Correction, 1/28: An earlier version of this story misidentified Daniel G. Chen, an undergraduate researcher at ISB.
Other significant early predictors of prolonged COVID symptoms – which the researchers called postacute sequelae – were having type 2 diabetes, SARS-CoV-2 RNAemia, and Epstein-Barr virus (EBV) viremia, Yapeng Su, PhD, of the Institute for Systems Biology (ISB) in Seattle, and colleagues wrote in Cell.
Having EBV viremia suggested that latent EBV has been reactivated, the authors noted.
“The most important postacute sequelae [that is conditions that are consequences of a disease] of COVID is the presence of autoantibodies,” James R. Heath, PhD, president of ISB and a bioengineering professor at the University of Washington, Seattle, said in an interview. “It’s about two times more important than the others.”
Dr. Heath and coauthors said early detection of this and other variables could prompt earlier aggressive treatment in patients susceptible to long COVID and ward off lingering symptoms.
“These predictive measures of long COVID can also help to better inform patients of their possible disease course,” study coauthor Daniel G. Chen, an undergraduate researcher at ISB, said in an interview. “We were also able to partially resolve the immunological underpinnings of some postacute sequelae of COVID in a way that suggested potential therapies, and the timing of those therapies.”
For example, he continued, the use of antivirals very early in the infectious course may mitigate the later development of long COVID. “This will, of course, have to be explored in an appropriately designed clinical trial.
“We also identified biomarkers of certain types of long COVID, such as neurological sequelae. Those biomarkers can help define the condition, which is a first step towards developing treatments.”
Study findings
With COVID patients monitored for 2 or 3 months, the study findings of the international “multiomic profiling” analysis include:
- Subclinical patient autoantibodies that reduce anti–SARS-CoV-2 antibodies suggest there is immune dysregulation during COVID-19 infection.
- Reactivation of latent other viruses during initial infection may be contributing to long COVID.
- Gastrointestinal postacute sequelae of COVID presents with a unique postacute expansion of cytotoxic T cells.
- SARS-CoV-2–specific and cytomegalovirus-specific CD8+ T cells displayed unique dynamics during recovery from infection.
According to the authors, as many as 69% of COVID-19 patients suffer from long COVID – a range of new, recurrent, or ongoing problems 4 or more weeks following initial SARS-CoV-2 infection. These may include memory loss, gastrointestinal distress, fatigue, anosmia, and shortness of breath.
Long COVID has been associated with acute disease severity, and is suspected to be related to autoimmune factors and unresolved viral fragments, according to the paper.
Research methods
The international study did a deep and detailed dive into multiple molecular markers of long COVID. It enrolled 209 COVID-19 patients with varying degrees of disease severity and matched them to 457 healthy controls. The researchers’ goal was to identify discrete and quantifiable long COVID factors and guide possible preemptive treatment.
Patients were assessed at three time points: at initial diagnosis, during the acute disease phase about a week later, and again 2 to 3 months post onset of symptoms after recovery from the acute phase of COVID. At the third assessment, some patients had lingering symptoms such as fatigue (52% ), cough (25%), and loss of taste or sense of smell (18%).
Blood draws were analyzed for autoantibodies and SARS-CoV-2–specific antibodies, global plasma proteomic and metabolomic profiles, and single-cell multiomic characterizations of peripheral blood mononuclear cells.
Each blood draw was paired with nasal-swab and plasma measurements of SARS-CoV-2 viral load and the data sets were integrated with electronic health records and self-reported patient symptoms to guide the interpretation of the molecular signatures of long COVID.
Author conclusions
The authors found an association between T2 hyperinflammation and long COVID–anticipating autoantibodies. This association further implies that hyperinflammation-controlling therapies in the acute stage of COVID may influence whether a patient experiences long COVID. “However, the detailed timing and context of these therapies matter, and, thus, future well-controlled studies will be needed to test these and other therapeutic implications,” Dr. Su and colleagues wrote.
Moreover, the negative correlations between anti–SARS-CoV-2 IgG and certain autoantibodies may suggest that patients with elevated autoantibody levels are more susceptible to breakthrough infections, the authors said.
“Many patients with high autoantibodies simultaneously have low protective antibodies that neutralize SARS-CoV-2, and that’s going to make them more susceptible to breakthrough infections,” Mr. Chen explained.*
“Detectability of most [long COVID-19 factors] at COVID diagnosis emphasizes the importance of early disease measurements for understanding emergent chronic conditions and suggests [long COVID] treatment strategies,” they wrote.
According to Mr. Chen, there are clear similarities in underlying immunobiology between patients with COVID autoantibodies and patients with systemic lupus erythematosus.
“These findings are also helping us frame our thinking around other chronic autoimmune conditions, such as postacute Lyme syndrome, for example,” said Dr. Heath.
The bottom line, said Mr. Chen, is that measuring early long COVID indicators may result in preventive treatments. “An example is the cortisol deficiency we see in certain long COVID patients. There are known treatments such as cortisol replacement therapy that should be explored for this group.”
Outside expert’s take on findings
Commenting on the study, Sherry Hsiang-Yi Chou, MD, who was not involved in the research, called the study a very important first step in understanding the path of this complex phenomenon and perhaps other conditions with long-term side effects.
“The researchers have done huge amount of innovative scientific work. They’ve shown the DNA signature of how our bodies respond to this disease,” said Dr. Chou, who is chief of the division of neurocritical care at Northwestern Medicine in Chicago.
“This type of research will help us scientifically understand and differentiate the various syndromes within long COVID. It will help identify who’s at risk for different aspects of this syndrome and lead to following them for longer periods in clinical trials,” she added.
The authors acknowledged that lengthier studies in larger cohorts were needed to see which patients will develop long-term chronic postacute sequelae of COVID.
This research was supported by the Wilke Family Foundation, the Parker Institute for Cancer Immunotherapy, Merck, and the Biomedical Advanced Research and Development Authority. Other support came from the National Institutes of Health, the Bill and Melinda Gates Foundation, Saint John’s Cancer Center, Fred Hutchinson Cancer Research Center, and the European Union’s Horizon 2020 research and innovation program. Dr. Heath is a cofounder of Pact Pharma. He and several coauthors disclosed various ties to multiple private-sector companies. Mr. Chen and Dr. Chou had no competing interests.
*Correction, 1/28: An earlier version of this story misidentified Daniel G. Chen, an undergraduate researcher at ISB.
FROM CELL
USPSTF says evidence still lacking for AFib screening in asymptomatic patients
The guidance is similar to the task force’s 2018 statement on screening for AFib with electrocardiography in asymptomatic adults 65 years or older, but lowers the inclusion age to adults 50 years or older.
“This 2021 evidence review included searching for evidence on additional screening methods such as automated blood pressure cuffs, pulse oximeters, and consumer devices such as smartwatches and smartphone apps. However, even with this expanded scope, the USPSTF did not find evidence to recommend for or against screening for AF,” the task force states.
The prevalence of increases in age from less than 0.2% in adults younger than 55 years to about 10% in those 85 years or older, the group says. The prevalence is higher in men than in women, but it is uncertain if it differs by race and ethnicity.
Although AFib substantially increases the risk for stroke, the stroke risk associated with subclinical AFib, particularly that of shorter duration lasting less than 24 hours or of lower burden, as might be detected by some screening approaches, is “uncertain,” the task force adds.
The updated recommendations were published online in JAMA, along with a separate evidence report and editorial.
The task force reviewed 26 studies in 113,784 patients, including 12 new to the update.
Studies showed that systematic screening detected significantly more AFib than no screening or pulse palpation (absolute difference, 1.0%-4.8% over up to 12 months). In two of the trials, however, only 10.7% and 44.5% of participants actually received the screening test.
The review included three randomized trials of screening vs. no screening that reported on health outcomes, but only one, STROKESTOP, was powered for health outcomes. It found a significantly lower risk for the primary composite endpoint of ischemic or hemorrhagic stroke, system embolism, bleeding leading to hospitalization, and all-cause mortality with twice-daily intermittent single-lead ECG monitoring for 14 days, compared with no screening. However, there were no significant differences in any of the individual outcomes of the composite endpoint.
“Additionally, and probably the most important thing to appreciate for the STROKESTOP study is that it has several limitations,” task force member Gbenga Ogedegbe, MD, MPH, of New York University told this news organization. The intervention was not masked, and outcomes weren’t centrally adjudicated.
Further, “about 11% of patients in the trial had a history of transient ischemic attack (TIA), stroke, or embolism and the population that we’re looking at within the task force are people without symptoms or history of stroke or ischemic attack,” he said. “That’s the fundamental difference here. So those limitations make it difficult to say that STROKESTOP actually has benefit.”
Notably absent from the review was the recent LOOP study, which found no significant benefit on outcomes with continuous monitoring with an implantable loop recorder (ILR) over usual care in older adults.
While it “offers some context for this issue,” it was not eligible for inclusion because 25% of the population had a prior history of stroke, TIA, or embolism and “because this screening approach may not be feasible for primary care settings,” lead author of the Evidence Report Leila Kahwati, MD, MPH, from RTI International’s Social and Health Organizational Research and Evaluation Program and the University of North Carolina at Chapel Hill, explained in an email.
Treatment with warfarin (mean, 1.5 years) was associated with a lower risk for ischemic stroke (relative risk, 0.32) and all-cause mortality (relative risk, 0.68), while direct oral anticoagulants were associated with a lower incidence of stroke (adjusted odds ratio range, 0.32-0.44). Patients had an increased risk for major bleeding with both warfarin (pooled relative risk, 1.8) and direct-acting oral anticoagulants (odds ratio, 1.38-2.21), but confidence intervals did not exclude a null effect.
The USPSTF found no trials that reported on the benefits of anticoagulation therapy in screen-detected patients.
In an accompanying editorial Philip Greenland, MD, points out that the task force’s conclusion differs from the 2020 European Society of Cardiology AFib guideline, which endorses opportunistic screening for AFib by pulse palpation or ECG rhythm strip in patients 65 years or older (class I recommendation) and advises that clinicians consider systematic ECG screening to detect AFib in people 75 years or older, or those at high risk for stroke (class IIa).
To possibly resolve whether screening for AFib in asymptomatic patients is justified, “future trials may need to consider enrolling only higher risk patients and identifying those with AF of longer duration,” said Dr. Greenland, JAMA editor and professor of preventive medicine and medicine at Northwestern University, Chicago.
“One important point raised by the LOOP trial is whether there is a threshold for AF duration that is most strongly associated with stroke risk and therefore most likely to benefit from anticoagulation,” he writes. Indeed, the LOOP authors themselves questioned whether the trial’s short AFib duration of 6 minutes may have led to many low-risk patients being diagnosed and treated.
“Additionally, trials need to recognize the need for longer monitoring periods (preferably continuous), and perhaps novel wearables will allow long-term monitoring, with accurate interpretation of the ECG and long-term adherence,” Dr. Greenland said.
In a related editorial in JAMA Internal Medicine, John Mandrola, MD, Baptist Health Louisville, Ky., and Andrew Foy, MD, Pennsylvania State University, Hershey, point out that continuous ILR monitoring in the LOOP trial found threefold more AFib and led to 2.7-fold higher rates of oral anticoagulation use, compared with standard care. Yet, there was no statistically significant difference in stroke reduction, and the 20% relative reduction in thromboembolic complications in the screened group was offset by a 26% relative increase in major bleeding.
“Perhaps the most remarkable aspect of the AF screening trials is that as the tools for screening improve, from a single 12-lead ECG to 14-day recordings and then the always-on ILR, more AF is detected and more [oral anticoagulant] is used, yet there is little demonstrable improvement in outcomes,” Dr. Mandrola and Dr. Foy write.
The editorialists also point to the potential for rhythm monitoring to lead to misdiagnosis and downstream cascades of care. “If you assume a 2% AF prevalence, even a device with 98% specificity will misdiagnose approximately 2000 individuals for every million screened.”
Dr. Mandrola told this news organization that the “greatest value” of these reports on AF screening and the critical appraisal of them is as an exercise in thinking about the limits of screening for disease. As James Maxwell Glover Wilson and Gunner Jungner wrote in their 1968 textbook, “Principles and Practice of Screening for Disease”: “in theory, screening is an admirable method of combating disease … [but] in practice, there are snags.”
“It would be good for the public to understand these snags…because they also apply to cancer, coronary calcium testing, and vascular screening as well,” Dr. Mandrola said.
Asked whether it’s possible to put the genie back in the bottle now that every other patient in clinic may have an ECG on their wrist, Dr. Ogedegbe said, “if a patient has no history of stroke or TIA and is 50 years or older, really, monitoring with these devices for AFib, there’s no evidence for or against doing that. Ultimately, the clinician has got to use their clinical judgment in talking to these patients.”
A related editorial in JAMA Cardiology suggests that, to be effective, the movement toward consumer-based screening must first show that such an approach improves outcomes and must deal with the paradox that those at highest risk for AFib and AFib-related stroke may be the least likely to own these technologies unless supported by the healthcare system.
“In addition, appropriate care pathways for confirming the diagnosis and, if necessary, initiating appropriate treatment in individuals with positive findings will need to be established,” Rod Passman, MD, Northwestern University, and Ben Freedman, MBBS, PhD, University of Sydney, Australia, say. “It will also be critical to ensure that device costs and variable technological literacy do not create barriers to making screening accessible to all those at risk.”
Finally, in a related editorial in JAMA Network Open Matthew Kalscheur, MD, and Zachary D. Goldberger, MD, both from the University of Wisconsin-Madison, say the potential benefits of early AFib detection should extend beyond stroke prevention.
“Patients identified with AF likely would benefit from targeted management of modifiable risk factors that contribute to AF, including obesity, hypertension, alcohol use, sleep apnea, smoking, and diabetes,” they write.
All members of the USPSTF receive travel reimbursement and an honorarium for participating in USPSTF meetings. Dr. Ogedegbe has a study included in the Evidence-based Practice Center report for this topic. Dr. Kahwati reported no relevant financial conflicts of interest. Dr. Greenland reported receiving research grants from the National Institutes of Health and from the American Heart Association. Dr. Mandrola is a regular contributor to this news organization. Dr. Foy, Dr. Kalscheur, and Dr. Goldberger reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The guidance is similar to the task force’s 2018 statement on screening for AFib with electrocardiography in asymptomatic adults 65 years or older, but lowers the inclusion age to adults 50 years or older.
“This 2021 evidence review included searching for evidence on additional screening methods such as automated blood pressure cuffs, pulse oximeters, and consumer devices such as smartwatches and smartphone apps. However, even with this expanded scope, the USPSTF did not find evidence to recommend for or against screening for AF,” the task force states.
The prevalence of increases in age from less than 0.2% in adults younger than 55 years to about 10% in those 85 years or older, the group says. The prevalence is higher in men than in women, but it is uncertain if it differs by race and ethnicity.
Although AFib substantially increases the risk for stroke, the stroke risk associated with subclinical AFib, particularly that of shorter duration lasting less than 24 hours or of lower burden, as might be detected by some screening approaches, is “uncertain,” the task force adds.
The updated recommendations were published online in JAMA, along with a separate evidence report and editorial.
The task force reviewed 26 studies in 113,784 patients, including 12 new to the update.
Studies showed that systematic screening detected significantly more AFib than no screening or pulse palpation (absolute difference, 1.0%-4.8% over up to 12 months). In two of the trials, however, only 10.7% and 44.5% of participants actually received the screening test.
The review included three randomized trials of screening vs. no screening that reported on health outcomes, but only one, STROKESTOP, was powered for health outcomes. It found a significantly lower risk for the primary composite endpoint of ischemic or hemorrhagic stroke, system embolism, bleeding leading to hospitalization, and all-cause mortality with twice-daily intermittent single-lead ECG monitoring for 14 days, compared with no screening. However, there were no significant differences in any of the individual outcomes of the composite endpoint.
“Additionally, and probably the most important thing to appreciate for the STROKESTOP study is that it has several limitations,” task force member Gbenga Ogedegbe, MD, MPH, of New York University told this news organization. The intervention was not masked, and outcomes weren’t centrally adjudicated.
Further, “about 11% of patients in the trial had a history of transient ischemic attack (TIA), stroke, or embolism and the population that we’re looking at within the task force are people without symptoms or history of stroke or ischemic attack,” he said. “That’s the fundamental difference here. So those limitations make it difficult to say that STROKESTOP actually has benefit.”
Notably absent from the review was the recent LOOP study, which found no significant benefit on outcomes with continuous monitoring with an implantable loop recorder (ILR) over usual care in older adults.
While it “offers some context for this issue,” it was not eligible for inclusion because 25% of the population had a prior history of stroke, TIA, or embolism and “because this screening approach may not be feasible for primary care settings,” lead author of the Evidence Report Leila Kahwati, MD, MPH, from RTI International’s Social and Health Organizational Research and Evaluation Program and the University of North Carolina at Chapel Hill, explained in an email.
Treatment with warfarin (mean, 1.5 years) was associated with a lower risk for ischemic stroke (relative risk, 0.32) and all-cause mortality (relative risk, 0.68), while direct oral anticoagulants were associated with a lower incidence of stroke (adjusted odds ratio range, 0.32-0.44). Patients had an increased risk for major bleeding with both warfarin (pooled relative risk, 1.8) and direct-acting oral anticoagulants (odds ratio, 1.38-2.21), but confidence intervals did not exclude a null effect.
The USPSTF found no trials that reported on the benefits of anticoagulation therapy in screen-detected patients.
In an accompanying editorial Philip Greenland, MD, points out that the task force’s conclusion differs from the 2020 European Society of Cardiology AFib guideline, which endorses opportunistic screening for AFib by pulse palpation or ECG rhythm strip in patients 65 years or older (class I recommendation) and advises that clinicians consider systematic ECG screening to detect AFib in people 75 years or older, or those at high risk for stroke (class IIa).
To possibly resolve whether screening for AFib in asymptomatic patients is justified, “future trials may need to consider enrolling only higher risk patients and identifying those with AF of longer duration,” said Dr. Greenland, JAMA editor and professor of preventive medicine and medicine at Northwestern University, Chicago.
“One important point raised by the LOOP trial is whether there is a threshold for AF duration that is most strongly associated with stroke risk and therefore most likely to benefit from anticoagulation,” he writes. Indeed, the LOOP authors themselves questioned whether the trial’s short AFib duration of 6 minutes may have led to many low-risk patients being diagnosed and treated.
“Additionally, trials need to recognize the need for longer monitoring periods (preferably continuous), and perhaps novel wearables will allow long-term monitoring, with accurate interpretation of the ECG and long-term adherence,” Dr. Greenland said.
In a related editorial in JAMA Internal Medicine, John Mandrola, MD, Baptist Health Louisville, Ky., and Andrew Foy, MD, Pennsylvania State University, Hershey, point out that continuous ILR monitoring in the LOOP trial found threefold more AFib and led to 2.7-fold higher rates of oral anticoagulation use, compared with standard care. Yet, there was no statistically significant difference in stroke reduction, and the 20% relative reduction in thromboembolic complications in the screened group was offset by a 26% relative increase in major bleeding.
“Perhaps the most remarkable aspect of the AF screening trials is that as the tools for screening improve, from a single 12-lead ECG to 14-day recordings and then the always-on ILR, more AF is detected and more [oral anticoagulant] is used, yet there is little demonstrable improvement in outcomes,” Dr. Mandrola and Dr. Foy write.
The editorialists also point to the potential for rhythm monitoring to lead to misdiagnosis and downstream cascades of care. “If you assume a 2% AF prevalence, even a device with 98% specificity will misdiagnose approximately 2000 individuals for every million screened.”
Dr. Mandrola told this news organization that the “greatest value” of these reports on AF screening and the critical appraisal of them is as an exercise in thinking about the limits of screening for disease. As James Maxwell Glover Wilson and Gunner Jungner wrote in their 1968 textbook, “Principles and Practice of Screening for Disease”: “in theory, screening is an admirable method of combating disease … [but] in practice, there are snags.”
“It would be good for the public to understand these snags…because they also apply to cancer, coronary calcium testing, and vascular screening as well,” Dr. Mandrola said.
Asked whether it’s possible to put the genie back in the bottle now that every other patient in clinic may have an ECG on their wrist, Dr. Ogedegbe said, “if a patient has no history of stroke or TIA and is 50 years or older, really, monitoring with these devices for AFib, there’s no evidence for or against doing that. Ultimately, the clinician has got to use their clinical judgment in talking to these patients.”
A related editorial in JAMA Cardiology suggests that, to be effective, the movement toward consumer-based screening must first show that such an approach improves outcomes and must deal with the paradox that those at highest risk for AFib and AFib-related stroke may be the least likely to own these technologies unless supported by the healthcare system.
“In addition, appropriate care pathways for confirming the diagnosis and, if necessary, initiating appropriate treatment in individuals with positive findings will need to be established,” Rod Passman, MD, Northwestern University, and Ben Freedman, MBBS, PhD, University of Sydney, Australia, say. “It will also be critical to ensure that device costs and variable technological literacy do not create barriers to making screening accessible to all those at risk.”
Finally, in a related editorial in JAMA Network Open Matthew Kalscheur, MD, and Zachary D. Goldberger, MD, both from the University of Wisconsin-Madison, say the potential benefits of early AFib detection should extend beyond stroke prevention.
“Patients identified with AF likely would benefit from targeted management of modifiable risk factors that contribute to AF, including obesity, hypertension, alcohol use, sleep apnea, smoking, and diabetes,” they write.
All members of the USPSTF receive travel reimbursement and an honorarium for participating in USPSTF meetings. Dr. Ogedegbe has a study included in the Evidence-based Practice Center report for this topic. Dr. Kahwati reported no relevant financial conflicts of interest. Dr. Greenland reported receiving research grants from the National Institutes of Health and from the American Heart Association. Dr. Mandrola is a regular contributor to this news organization. Dr. Foy, Dr. Kalscheur, and Dr. Goldberger reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The guidance is similar to the task force’s 2018 statement on screening for AFib with electrocardiography in asymptomatic adults 65 years or older, but lowers the inclusion age to adults 50 years or older.
“This 2021 evidence review included searching for evidence on additional screening methods such as automated blood pressure cuffs, pulse oximeters, and consumer devices such as smartwatches and smartphone apps. However, even with this expanded scope, the USPSTF did not find evidence to recommend for or against screening for AF,” the task force states.
The prevalence of increases in age from less than 0.2% in adults younger than 55 years to about 10% in those 85 years or older, the group says. The prevalence is higher in men than in women, but it is uncertain if it differs by race and ethnicity.
Although AFib substantially increases the risk for stroke, the stroke risk associated with subclinical AFib, particularly that of shorter duration lasting less than 24 hours or of lower burden, as might be detected by some screening approaches, is “uncertain,” the task force adds.
The updated recommendations were published online in JAMA, along with a separate evidence report and editorial.
The task force reviewed 26 studies in 113,784 patients, including 12 new to the update.
Studies showed that systematic screening detected significantly more AFib than no screening or pulse palpation (absolute difference, 1.0%-4.8% over up to 12 months). In two of the trials, however, only 10.7% and 44.5% of participants actually received the screening test.
The review included three randomized trials of screening vs. no screening that reported on health outcomes, but only one, STROKESTOP, was powered for health outcomes. It found a significantly lower risk for the primary composite endpoint of ischemic or hemorrhagic stroke, system embolism, bleeding leading to hospitalization, and all-cause mortality with twice-daily intermittent single-lead ECG monitoring for 14 days, compared with no screening. However, there were no significant differences in any of the individual outcomes of the composite endpoint.
“Additionally, and probably the most important thing to appreciate for the STROKESTOP study is that it has several limitations,” task force member Gbenga Ogedegbe, MD, MPH, of New York University told this news organization. The intervention was not masked, and outcomes weren’t centrally adjudicated.
Further, “about 11% of patients in the trial had a history of transient ischemic attack (TIA), stroke, or embolism and the population that we’re looking at within the task force are people without symptoms or history of stroke or ischemic attack,” he said. “That’s the fundamental difference here. So those limitations make it difficult to say that STROKESTOP actually has benefit.”
Notably absent from the review was the recent LOOP study, which found no significant benefit on outcomes with continuous monitoring with an implantable loop recorder (ILR) over usual care in older adults.
While it “offers some context for this issue,” it was not eligible for inclusion because 25% of the population had a prior history of stroke, TIA, or embolism and “because this screening approach may not be feasible for primary care settings,” lead author of the Evidence Report Leila Kahwati, MD, MPH, from RTI International’s Social and Health Organizational Research and Evaluation Program and the University of North Carolina at Chapel Hill, explained in an email.
Treatment with warfarin (mean, 1.5 years) was associated with a lower risk for ischemic stroke (relative risk, 0.32) and all-cause mortality (relative risk, 0.68), while direct oral anticoagulants were associated with a lower incidence of stroke (adjusted odds ratio range, 0.32-0.44). Patients had an increased risk for major bleeding with both warfarin (pooled relative risk, 1.8) and direct-acting oral anticoagulants (odds ratio, 1.38-2.21), but confidence intervals did not exclude a null effect.
The USPSTF found no trials that reported on the benefits of anticoagulation therapy in screen-detected patients.
In an accompanying editorial Philip Greenland, MD, points out that the task force’s conclusion differs from the 2020 European Society of Cardiology AFib guideline, which endorses opportunistic screening for AFib by pulse palpation or ECG rhythm strip in patients 65 years or older (class I recommendation) and advises that clinicians consider systematic ECG screening to detect AFib in people 75 years or older, or those at high risk for stroke (class IIa).
To possibly resolve whether screening for AFib in asymptomatic patients is justified, “future trials may need to consider enrolling only higher risk patients and identifying those with AF of longer duration,” said Dr. Greenland, JAMA editor and professor of preventive medicine and medicine at Northwestern University, Chicago.
“One important point raised by the LOOP trial is whether there is a threshold for AF duration that is most strongly associated with stroke risk and therefore most likely to benefit from anticoagulation,” he writes. Indeed, the LOOP authors themselves questioned whether the trial’s short AFib duration of 6 minutes may have led to many low-risk patients being diagnosed and treated.
“Additionally, trials need to recognize the need for longer monitoring periods (preferably continuous), and perhaps novel wearables will allow long-term monitoring, with accurate interpretation of the ECG and long-term adherence,” Dr. Greenland said.
In a related editorial in JAMA Internal Medicine, John Mandrola, MD, Baptist Health Louisville, Ky., and Andrew Foy, MD, Pennsylvania State University, Hershey, point out that continuous ILR monitoring in the LOOP trial found threefold more AFib and led to 2.7-fold higher rates of oral anticoagulation use, compared with standard care. Yet, there was no statistically significant difference in stroke reduction, and the 20% relative reduction in thromboembolic complications in the screened group was offset by a 26% relative increase in major bleeding.
“Perhaps the most remarkable aspect of the AF screening trials is that as the tools for screening improve, from a single 12-lead ECG to 14-day recordings and then the always-on ILR, more AF is detected and more [oral anticoagulant] is used, yet there is little demonstrable improvement in outcomes,” Dr. Mandrola and Dr. Foy write.
The editorialists also point to the potential for rhythm monitoring to lead to misdiagnosis and downstream cascades of care. “If you assume a 2% AF prevalence, even a device with 98% specificity will misdiagnose approximately 2000 individuals for every million screened.”
Dr. Mandrola told this news organization that the “greatest value” of these reports on AF screening and the critical appraisal of them is as an exercise in thinking about the limits of screening for disease. As James Maxwell Glover Wilson and Gunner Jungner wrote in their 1968 textbook, “Principles and Practice of Screening for Disease”: “in theory, screening is an admirable method of combating disease … [but] in practice, there are snags.”
“It would be good for the public to understand these snags…because they also apply to cancer, coronary calcium testing, and vascular screening as well,” Dr. Mandrola said.
Asked whether it’s possible to put the genie back in the bottle now that every other patient in clinic may have an ECG on their wrist, Dr. Ogedegbe said, “if a patient has no history of stroke or TIA and is 50 years or older, really, monitoring with these devices for AFib, there’s no evidence for or against doing that. Ultimately, the clinician has got to use their clinical judgment in talking to these patients.”
A related editorial in JAMA Cardiology suggests that, to be effective, the movement toward consumer-based screening must first show that such an approach improves outcomes and must deal with the paradox that those at highest risk for AFib and AFib-related stroke may be the least likely to own these technologies unless supported by the healthcare system.
“In addition, appropriate care pathways for confirming the diagnosis and, if necessary, initiating appropriate treatment in individuals with positive findings will need to be established,” Rod Passman, MD, Northwestern University, and Ben Freedman, MBBS, PhD, University of Sydney, Australia, say. “It will also be critical to ensure that device costs and variable technological literacy do not create barriers to making screening accessible to all those at risk.”
Finally, in a related editorial in JAMA Network Open Matthew Kalscheur, MD, and Zachary D. Goldberger, MD, both from the University of Wisconsin-Madison, say the potential benefits of early AFib detection should extend beyond stroke prevention.
“Patients identified with AF likely would benefit from targeted management of modifiable risk factors that contribute to AF, including obesity, hypertension, alcohol use, sleep apnea, smoking, and diabetes,” they write.
All members of the USPSTF receive travel reimbursement and an honorarium for participating in USPSTF meetings. Dr. Ogedegbe has a study included in the Evidence-based Practice Center report for this topic. Dr. Kahwati reported no relevant financial conflicts of interest. Dr. Greenland reported receiving research grants from the National Institutes of Health and from the American Heart Association. Dr. Mandrola is a regular contributor to this news organization. Dr. Foy, Dr. Kalscheur, and Dr. Goldberger reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
One in five female oncologists considering leaving academia, survey finds
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Ketamine an ‘intriguing new therapy’ for alcoholism
Three weekly infusions of the dissociative anesthetic ketamine coupled with mindfulness-based relapse prevention therapy may help adults with alcohol use disorder (AUD) maintain abstinence, new research suggests.
Preliminary results from a phase 2, double-blind, placebo-controlled trial show ketamine was well tolerated and, compared with placebo, associated with more days of abstinence from alcohol at 6 months.
The results suggest ketamine plus psychological therapy may be a “new, relatively brief treatment that has long lasting effects in AUD,” Celia Morgan, PhD, professor of psychopharmacology, University of Exeter, United Kingdom, told this news organization.
The study was published online Jan. 11 in the American Journal of Psychiatry.
Target depression
Depressive symptoms are common in patients under treatment for AUD and increase relapse risk.
“Ketamine may support alcohol abstinence by temporarily alleviating depressive symptoms during the high-risk relapse period in the weeks after detoxification,” the investigators note.
Ketamine may also provide a “temporary boost to synaptogenesis and neurogenesis, which may allow psychological therapies and new strategies for managing addiction to embed more readily,” they add.
To test these theories, the researchers recruited 96 adults (mean age, 44 years, 35 women) with severe AUD to participate in the trial.
All participants had to abstain from alcohol for at least 24 hours before the trial started and have a reading of 0.0 on a breath alcohol test at the baseline visit.
Participants were randomly allocated to one of four groups:
1. three weekly ketamine infusions of 0.8 mg/kg IV over 40 minutes plus psychological therapy
2. three saline infusions plus psychological therapy
3. three ketamine infusions plus alcohol education
4. three saline infusions plus alcohol education
The primary outcome was self-reported percentage of days abstinent, as well as confirmed alcohol relapse at 6-month follow-up.
(mean difference, 10.1%; 95% confidence interval, 1.1-19.0), “although confidence intervals were wide, consistent with a proof-of-concept study,” the authors note.
The greatest reduction in total days off alcohol occurred in the ketamine plus relapse-prevention therapy group compared with the saline plus alcohol education group (mean difference, 15.9%; 95% CI, 3.8-28.1).
There was no significant difference in relapse rate between the ketamine and placebo groups. No serious adverse effects were reported in any participant.
Growing evidence
These findings support some other studies that have also suggested a benefit of ketamine in AUD.
As reported by this news organization, one recent study found a single infusion of ketamine combined with counseling may help alcohol-dependent patients curb their drinking.
A separate study showed that a single dose of ketamine plus therapy that focused on reactivating drinking-related “maladaptive reward memories” reduced drinking urges and alcohol intake more than just ketamine or a placebo infusion alone.
“That ketamine can reduce both alcohol use and depression in AUD is encouraging therapeutically,” the researchers write.
“While a clear link between depression and AUD is acknowledged, alcohol and mental health services still struggle to meet the needs of dual-diagnosis patients, so ketamine may represent a solution to this long-standing comorbidity,” they add.
Dr. Morgan said in an interview that adjunctive ketamine with relapse-prevention therapy is “currently being delivered in Awakn Clinics in the U.K. and Norway, but we need to conduct the phase 3 trial in order to make the treatment more widely accessible.”
An ‘Intriguing new therapy’
Reached for comment, Timothy Brennan, MD, MPH, chief of clinical services, Addiction Institute of Mount Sinai, New York, said ketamine “continues to be an intriguing new therapy for a variety of mental health conditions.”
“Unfortunately, the study did not show any difference in rates of relapse to alcohol, though an improvement in days of abstinence is certainly noteworthy,” Dr. Brennan said in an interview.
“Because this was just a proof-of-concept study and did not compare ketamine to any FDA-approved pharmacotherapy for alcohol, it remains too early to recommend ketamine infusions to those suffering from alcohol use disorder,” he cautioned.
The study was supported by the Medical Research Council. Dr. Morgan has received royalties for KARE (Ketamine for Reduction of Alcoholic Relapse) therapy license distribution. KARE therapy is licensed from University of Exeter to Awakn Life Sciences. Dr. Morgan has received research funding from Awakn Life Sciences and has served as a consultant for Janssen Pharmaceuticals. Other coauthors have disclosed relationships with industry; the full list can be found with the original article. Dr. Brennan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Three weekly infusions of the dissociative anesthetic ketamine coupled with mindfulness-based relapse prevention therapy may help adults with alcohol use disorder (AUD) maintain abstinence, new research suggests.
Preliminary results from a phase 2, double-blind, placebo-controlled trial show ketamine was well tolerated and, compared with placebo, associated with more days of abstinence from alcohol at 6 months.
The results suggest ketamine plus psychological therapy may be a “new, relatively brief treatment that has long lasting effects in AUD,” Celia Morgan, PhD, professor of psychopharmacology, University of Exeter, United Kingdom, told this news organization.
The study was published online Jan. 11 in the American Journal of Psychiatry.
Target depression
Depressive symptoms are common in patients under treatment for AUD and increase relapse risk.
“Ketamine may support alcohol abstinence by temporarily alleviating depressive symptoms during the high-risk relapse period in the weeks after detoxification,” the investigators note.
Ketamine may also provide a “temporary boost to synaptogenesis and neurogenesis, which may allow psychological therapies and new strategies for managing addiction to embed more readily,” they add.
To test these theories, the researchers recruited 96 adults (mean age, 44 years, 35 women) with severe AUD to participate in the trial.
All participants had to abstain from alcohol for at least 24 hours before the trial started and have a reading of 0.0 on a breath alcohol test at the baseline visit.
Participants were randomly allocated to one of four groups:
1. three weekly ketamine infusions of 0.8 mg/kg IV over 40 minutes plus psychological therapy
2. three saline infusions plus psychological therapy
3. three ketamine infusions plus alcohol education
4. three saline infusions plus alcohol education
The primary outcome was self-reported percentage of days abstinent, as well as confirmed alcohol relapse at 6-month follow-up.
(mean difference, 10.1%; 95% confidence interval, 1.1-19.0), “although confidence intervals were wide, consistent with a proof-of-concept study,” the authors note.
The greatest reduction in total days off alcohol occurred in the ketamine plus relapse-prevention therapy group compared with the saline plus alcohol education group (mean difference, 15.9%; 95% CI, 3.8-28.1).
There was no significant difference in relapse rate between the ketamine and placebo groups. No serious adverse effects were reported in any participant.
Growing evidence
These findings support some other studies that have also suggested a benefit of ketamine in AUD.
As reported by this news organization, one recent study found a single infusion of ketamine combined with counseling may help alcohol-dependent patients curb their drinking.
A separate study showed that a single dose of ketamine plus therapy that focused on reactivating drinking-related “maladaptive reward memories” reduced drinking urges and alcohol intake more than just ketamine or a placebo infusion alone.
“That ketamine can reduce both alcohol use and depression in AUD is encouraging therapeutically,” the researchers write.
“While a clear link between depression and AUD is acknowledged, alcohol and mental health services still struggle to meet the needs of dual-diagnosis patients, so ketamine may represent a solution to this long-standing comorbidity,” they add.
Dr. Morgan said in an interview that adjunctive ketamine with relapse-prevention therapy is “currently being delivered in Awakn Clinics in the U.K. and Norway, but we need to conduct the phase 3 trial in order to make the treatment more widely accessible.”
An ‘Intriguing new therapy’
Reached for comment, Timothy Brennan, MD, MPH, chief of clinical services, Addiction Institute of Mount Sinai, New York, said ketamine “continues to be an intriguing new therapy for a variety of mental health conditions.”
“Unfortunately, the study did not show any difference in rates of relapse to alcohol, though an improvement in days of abstinence is certainly noteworthy,” Dr. Brennan said in an interview.
“Because this was just a proof-of-concept study and did not compare ketamine to any FDA-approved pharmacotherapy for alcohol, it remains too early to recommend ketamine infusions to those suffering from alcohol use disorder,” he cautioned.
The study was supported by the Medical Research Council. Dr. Morgan has received royalties for KARE (Ketamine for Reduction of Alcoholic Relapse) therapy license distribution. KARE therapy is licensed from University of Exeter to Awakn Life Sciences. Dr. Morgan has received research funding from Awakn Life Sciences and has served as a consultant for Janssen Pharmaceuticals. Other coauthors have disclosed relationships with industry; the full list can be found with the original article. Dr. Brennan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Three weekly infusions of the dissociative anesthetic ketamine coupled with mindfulness-based relapse prevention therapy may help adults with alcohol use disorder (AUD) maintain abstinence, new research suggests.
Preliminary results from a phase 2, double-blind, placebo-controlled trial show ketamine was well tolerated and, compared with placebo, associated with more days of abstinence from alcohol at 6 months.
The results suggest ketamine plus psychological therapy may be a “new, relatively brief treatment that has long lasting effects in AUD,” Celia Morgan, PhD, professor of psychopharmacology, University of Exeter, United Kingdom, told this news organization.
The study was published online Jan. 11 in the American Journal of Psychiatry.
Target depression
Depressive symptoms are common in patients under treatment for AUD and increase relapse risk.
“Ketamine may support alcohol abstinence by temporarily alleviating depressive symptoms during the high-risk relapse period in the weeks after detoxification,” the investigators note.
Ketamine may also provide a “temporary boost to synaptogenesis and neurogenesis, which may allow psychological therapies and new strategies for managing addiction to embed more readily,” they add.
To test these theories, the researchers recruited 96 adults (mean age, 44 years, 35 women) with severe AUD to participate in the trial.
All participants had to abstain from alcohol for at least 24 hours before the trial started and have a reading of 0.0 on a breath alcohol test at the baseline visit.
Participants were randomly allocated to one of four groups:
1. three weekly ketamine infusions of 0.8 mg/kg IV over 40 minutes plus psychological therapy
2. three saline infusions plus psychological therapy
3. three ketamine infusions plus alcohol education
4. three saline infusions plus alcohol education
The primary outcome was self-reported percentage of days abstinent, as well as confirmed alcohol relapse at 6-month follow-up.
(mean difference, 10.1%; 95% confidence interval, 1.1-19.0), “although confidence intervals were wide, consistent with a proof-of-concept study,” the authors note.
The greatest reduction in total days off alcohol occurred in the ketamine plus relapse-prevention therapy group compared with the saline plus alcohol education group (mean difference, 15.9%; 95% CI, 3.8-28.1).
There was no significant difference in relapse rate between the ketamine and placebo groups. No serious adverse effects were reported in any participant.
Growing evidence
These findings support some other studies that have also suggested a benefit of ketamine in AUD.
As reported by this news organization, one recent study found a single infusion of ketamine combined with counseling may help alcohol-dependent patients curb their drinking.
A separate study showed that a single dose of ketamine plus therapy that focused on reactivating drinking-related “maladaptive reward memories” reduced drinking urges and alcohol intake more than just ketamine or a placebo infusion alone.
“That ketamine can reduce both alcohol use and depression in AUD is encouraging therapeutically,” the researchers write.
“While a clear link between depression and AUD is acknowledged, alcohol and mental health services still struggle to meet the needs of dual-diagnosis patients, so ketamine may represent a solution to this long-standing comorbidity,” they add.
Dr. Morgan said in an interview that adjunctive ketamine with relapse-prevention therapy is “currently being delivered in Awakn Clinics in the U.K. and Norway, but we need to conduct the phase 3 trial in order to make the treatment more widely accessible.”
An ‘Intriguing new therapy’
Reached for comment, Timothy Brennan, MD, MPH, chief of clinical services, Addiction Institute of Mount Sinai, New York, said ketamine “continues to be an intriguing new therapy for a variety of mental health conditions.”
“Unfortunately, the study did not show any difference in rates of relapse to alcohol, though an improvement in days of abstinence is certainly noteworthy,” Dr. Brennan said in an interview.
“Because this was just a proof-of-concept study and did not compare ketamine to any FDA-approved pharmacotherapy for alcohol, it remains too early to recommend ketamine infusions to those suffering from alcohol use disorder,” he cautioned.
The study was supported by the Medical Research Council. Dr. Morgan has received royalties for KARE (Ketamine for Reduction of Alcoholic Relapse) therapy license distribution. KARE therapy is licensed from University of Exeter to Awakn Life Sciences. Dr. Morgan has received research funding from Awakn Life Sciences and has served as a consultant for Janssen Pharmaceuticals. Other coauthors have disclosed relationships with industry; the full list can be found with the original article. Dr. Brennan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Decades of research fail to resolve disparities in gastrointestinal cancer care
Men and White people receive better treatment for gastroesophageal cancer than women, Blacks, and Latinos despite years of studies highlighting disparities in care, researchers say.
The problem is complex because it stems from both biological and socioeconomic factors, but some signs of improvement are beginning to show, said Nathaniel R. Evans III, MD, a professor of surgery at Thomas Jefferson University in Philadelphia.
“Repeatedly, we see that, although we know how patients should be treated, there are oftentimes subsets of patients who don’t receive that same level of care,” said Dr. Evans in a general session talk at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
Black patients with esophageal cancer are 38% more likely to die from the condition than White patients, he said, citing a 2013 study (Ann Surg Oncol. 2013 doi: 10.1245/s10434-012-2807-3). For Latino patients, mortality is 20% higher than for White patients.
The difference can mostly be explained by the rate of esophagectomy, which is 52% lower for Black patients and 29% lower for Latino patients, compared with White patients, the study found.
Besides race and gender, insurance status also influences who gets surgery, Dr. Evans said, citing data from the National Cancer Database. Black patients are less likely to get surgery and more likely to die at all stages and histologies, he said. They wait longer for treatment and are more likely to receive no treatment at all.
Women also suffer from disparities, said Anna Dorothea Wagner, MD, head of the gastrointestinal cancer clinic at Lausanne University Hospital in Lausanne (Switzerland), who spoke at the symposium with Dr Evans.
Seventy-five percent of men with esophageal and gastric adenocarcinoma get curative treatments, compared with only 60% of women, Dr. Wagner said, citing a 2020 study on which she is an author. Women are more likely to get palliative care. As a result, only 30% of women survive the condition for 5 years or more compared to 34% of men, she said. “At the moment we don’t know whether this is due to either patient preferences or cognitive or bias of physicians.”
Disparities in treatment outcomes because of biological differences
For women, some disparities also arise out of clear biological differences, Dr. Wagner said. Sex hormone signaling affects cancer susceptibility, and sex-biased gene expression signatures have been detected in multiple cancer types.
Women with poorly differentiated and signet-cell pathology are less likely to survive their cancer than men with the same histology, she said.
Many studies have shown that chemotherapy is more toxic to women than men without being more efficacious, she added. This suggests that the optimal doses might be different for women and men.
Responding to a question from the audience, Dr. Wagner said more research is needed on transgender patients to understand how these factors affect them.
Dr. Evans attributed the racial and ethnic disparities to some combination of differential histology, stage at diagnosis, access to care, socioeconomics, and inherent bias.
“The problem is not new,” Dr. Evans said. He described studies that found disparities in the 1970s. “But the good news is that things do seem to be getting better.”
Between 2000 and 2011, the number of esophagectomies being performed at high-volume hospitals increased, he said. The overall mortality after esophagectomy has consequently decreased over this time, and the gap in this rate between White and Black people has closed, he said. “Specialization and centralization clearly improve outcomes for certain surgical procedures.”
To address the problem everyone should acknowledge the disparities, particularly in the access to surgery. “I think one of the best tools we have to try to address the disparity is education, both for patients and providers,” Dr. Evans said.
Care teams must become more diverse and culturally competent to combat longstanding distrust and improve communication, he said.
In December, ASCO announced an “action plan” to address equity, diversity and inclusion in cancer care. The organization promised to improve clinical trial eligibility, and train researchers about inherent bias in order to make the trials more representative of the cancer population.
It vowed to increase participation of underrepresented groups in its professional development programs and leadership roles, and educate its members about equity. And, it resolved to provide resources to providers so they could advocate for better quality of care, especially in rural and disadvantaged settings.
Dr. Wagner disclosed relationships with Alligator Bioscience, BMS, Dragonfly Therapeutics, Lilly, Merck KGaA, MSD Oncology, Servier/Pfizer, and Abbvie. Dr. Evans disclosed relationships with Bristol Myers Squibb Foundation and Intuitive Surgical.
This article was updated 1/28/22.
Men and White people receive better treatment for gastroesophageal cancer than women, Blacks, and Latinos despite years of studies highlighting disparities in care, researchers say.
The problem is complex because it stems from both biological and socioeconomic factors, but some signs of improvement are beginning to show, said Nathaniel R. Evans III, MD, a professor of surgery at Thomas Jefferson University in Philadelphia.
“Repeatedly, we see that, although we know how patients should be treated, there are oftentimes subsets of patients who don’t receive that same level of care,” said Dr. Evans in a general session talk at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
Black patients with esophageal cancer are 38% more likely to die from the condition than White patients, he said, citing a 2013 study (Ann Surg Oncol. 2013 doi: 10.1245/s10434-012-2807-3). For Latino patients, mortality is 20% higher than for White patients.
The difference can mostly be explained by the rate of esophagectomy, which is 52% lower for Black patients and 29% lower for Latino patients, compared with White patients, the study found.
Besides race and gender, insurance status also influences who gets surgery, Dr. Evans said, citing data from the National Cancer Database. Black patients are less likely to get surgery and more likely to die at all stages and histologies, he said. They wait longer for treatment and are more likely to receive no treatment at all.
Women also suffer from disparities, said Anna Dorothea Wagner, MD, head of the gastrointestinal cancer clinic at Lausanne University Hospital in Lausanne (Switzerland), who spoke at the symposium with Dr Evans.
Seventy-five percent of men with esophageal and gastric adenocarcinoma get curative treatments, compared with only 60% of women, Dr. Wagner said, citing a 2020 study on which she is an author. Women are more likely to get palliative care. As a result, only 30% of women survive the condition for 5 years or more compared to 34% of men, she said. “At the moment we don’t know whether this is due to either patient preferences or cognitive or bias of physicians.”
Disparities in treatment outcomes because of biological differences
For women, some disparities also arise out of clear biological differences, Dr. Wagner said. Sex hormone signaling affects cancer susceptibility, and sex-biased gene expression signatures have been detected in multiple cancer types.
Women with poorly differentiated and signet-cell pathology are less likely to survive their cancer than men with the same histology, she said.
Many studies have shown that chemotherapy is more toxic to women than men without being more efficacious, she added. This suggests that the optimal doses might be different for women and men.
Responding to a question from the audience, Dr. Wagner said more research is needed on transgender patients to understand how these factors affect them.
Dr. Evans attributed the racial and ethnic disparities to some combination of differential histology, stage at diagnosis, access to care, socioeconomics, and inherent bias.
“The problem is not new,” Dr. Evans said. He described studies that found disparities in the 1970s. “But the good news is that things do seem to be getting better.”
Between 2000 and 2011, the number of esophagectomies being performed at high-volume hospitals increased, he said. The overall mortality after esophagectomy has consequently decreased over this time, and the gap in this rate between White and Black people has closed, he said. “Specialization and centralization clearly improve outcomes for certain surgical procedures.”
To address the problem everyone should acknowledge the disparities, particularly in the access to surgery. “I think one of the best tools we have to try to address the disparity is education, both for patients and providers,” Dr. Evans said.
Care teams must become more diverse and culturally competent to combat longstanding distrust and improve communication, he said.
In December, ASCO announced an “action plan” to address equity, diversity and inclusion in cancer care. The organization promised to improve clinical trial eligibility, and train researchers about inherent bias in order to make the trials more representative of the cancer population.
It vowed to increase participation of underrepresented groups in its professional development programs and leadership roles, and educate its members about equity. And, it resolved to provide resources to providers so they could advocate for better quality of care, especially in rural and disadvantaged settings.
Dr. Wagner disclosed relationships with Alligator Bioscience, BMS, Dragonfly Therapeutics, Lilly, Merck KGaA, MSD Oncology, Servier/Pfizer, and Abbvie. Dr. Evans disclosed relationships with Bristol Myers Squibb Foundation and Intuitive Surgical.
This article was updated 1/28/22.
Men and White people receive better treatment for gastroesophageal cancer than women, Blacks, and Latinos despite years of studies highlighting disparities in care, researchers say.
The problem is complex because it stems from both biological and socioeconomic factors, but some signs of improvement are beginning to show, said Nathaniel R. Evans III, MD, a professor of surgery at Thomas Jefferson University in Philadelphia.
“Repeatedly, we see that, although we know how patients should be treated, there are oftentimes subsets of patients who don’t receive that same level of care,” said Dr. Evans in a general session talk at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
Black patients with esophageal cancer are 38% more likely to die from the condition than White patients, he said, citing a 2013 study (Ann Surg Oncol. 2013 doi: 10.1245/s10434-012-2807-3). For Latino patients, mortality is 20% higher than for White patients.
The difference can mostly be explained by the rate of esophagectomy, which is 52% lower for Black patients and 29% lower for Latino patients, compared with White patients, the study found.
Besides race and gender, insurance status also influences who gets surgery, Dr. Evans said, citing data from the National Cancer Database. Black patients are less likely to get surgery and more likely to die at all stages and histologies, he said. They wait longer for treatment and are more likely to receive no treatment at all.
Women also suffer from disparities, said Anna Dorothea Wagner, MD, head of the gastrointestinal cancer clinic at Lausanne University Hospital in Lausanne (Switzerland), who spoke at the symposium with Dr Evans.
Seventy-five percent of men with esophageal and gastric adenocarcinoma get curative treatments, compared with only 60% of women, Dr. Wagner said, citing a 2020 study on which she is an author. Women are more likely to get palliative care. As a result, only 30% of women survive the condition for 5 years or more compared to 34% of men, she said. “At the moment we don’t know whether this is due to either patient preferences or cognitive or bias of physicians.”
Disparities in treatment outcomes because of biological differences
For women, some disparities also arise out of clear biological differences, Dr. Wagner said. Sex hormone signaling affects cancer susceptibility, and sex-biased gene expression signatures have been detected in multiple cancer types.
Women with poorly differentiated and signet-cell pathology are less likely to survive their cancer than men with the same histology, she said.
Many studies have shown that chemotherapy is more toxic to women than men without being more efficacious, she added. This suggests that the optimal doses might be different for women and men.
Responding to a question from the audience, Dr. Wagner said more research is needed on transgender patients to understand how these factors affect them.
Dr. Evans attributed the racial and ethnic disparities to some combination of differential histology, stage at diagnosis, access to care, socioeconomics, and inherent bias.
“The problem is not new,” Dr. Evans said. He described studies that found disparities in the 1970s. “But the good news is that things do seem to be getting better.”
Between 2000 and 2011, the number of esophagectomies being performed at high-volume hospitals increased, he said. The overall mortality after esophagectomy has consequently decreased over this time, and the gap in this rate between White and Black people has closed, he said. “Specialization and centralization clearly improve outcomes for certain surgical procedures.”
To address the problem everyone should acknowledge the disparities, particularly in the access to surgery. “I think one of the best tools we have to try to address the disparity is education, both for patients and providers,” Dr. Evans said.
Care teams must become more diverse and culturally competent to combat longstanding distrust and improve communication, he said.
In December, ASCO announced an “action plan” to address equity, diversity and inclusion in cancer care. The organization promised to improve clinical trial eligibility, and train researchers about inherent bias in order to make the trials more representative of the cancer population.
It vowed to increase participation of underrepresented groups in its professional development programs and leadership roles, and educate its members about equity. And, it resolved to provide resources to providers so they could advocate for better quality of care, especially in rural and disadvantaged settings.
Dr. Wagner disclosed relationships with Alligator Bioscience, BMS, Dragonfly Therapeutics, Lilly, Merck KGaA, MSD Oncology, Servier/Pfizer, and Abbvie. Dr. Evans disclosed relationships with Bristol Myers Squibb Foundation and Intuitive Surgical.
This article was updated 1/28/22.
FROM GI CANCERS SYMPOSIUM 2022
Can immunotherapy replace surgery for stomach cancer?
GERCOR NEONIPIGA was a phase 2 study with no comparator group and only 32 patients, but even so, after a 6-cycle course of nivolumab and ipilimumab, there was no sign of tumor in 17 of the 29 patients (59%) who had surgery specimens evaluable by pathology.
Indeed, two patients refused surgery after their preop endoscopic biopsies came back clear with no tumor cells. Surgery was called off in a third patient who developed metastases beforehand.
After a median of 12 months follow-up, there’s was no recurrence or progression in 30 patients (94%). The remaining two included the metastatic patient and one who died 3 days after surgery from cardiovascular complications.
If the findings pan out with additional research, the approach could be a boon for people who respond. “Avoiding surgery is a dream for these patients,” said lead investigator Thierry Andre, MD, a medical oncology professor at Sorbonne University, Paris, when he presented the findings at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
The trial “raises the question whether surgery can be delayed or avoided in some patients with localized” disease. Given the findings, “it seems possible not for all but probably for half, maybe more.” As in the two subjects who opted out of surgery, preop endoscopic biopsies could be used to identify complete responders with active surveillance afterwards, he said.
The study included 16 patients with gastric cancer and 16 with esophagogastric adenocarcinoma. They were mismatch repair deficient, which Dr. Andre said predicts response to immunotherapy.
At baseline, 22 had stage T3 disease and four had stage T2 disease, and stage was not evaluable by echo-endoscopy in 6. Nodal status was unknown, but the patients had no metastases at baseline.
They underwent six nivolumab 240-mg infusions and two ipilimumab 1–mg/kg infusions over 12 weeks, followed by R0 resections a median of 5 weeks after the last nivolumab injection.
Surgical specimens from 17 patients (59%) showed a complete pathological response to neoadjuvant immunotherapy (Becker tumor regression grade (TRG) 1a, ypT0N0). TRG was 1b – less than 10% residual tumor in tumor bed in four patients. TRG was 2 in two patients with 10%-50% of residual tumor remaining, and six had a TRG of 3 with more than half of the tumor remaining after immunotherapy.
Based on tumor response, 25 patients had nine additional nivolumab infusions after surgery with 480 mg infused monthly.
Dr. Andre explained that people want to avoid surgery because of the substantial morbidity that was shown in the study, plus 54% of patients had complications, including anastomotic leaks, pancreatitis, pneumonia, and other problems.
There were no new safety signals with neoadjuvant therapy; 25% of patients had grade 3 or 4 events.
The study was conducted in 10 centers in France. About three-quarters of the subjects were men and the median age was 65 years.
Bristol Meyers Squibb supplied the nivolumab and ipilimumab and partially funded the work. Many of the investigators had ties to the company, including Dr. Andre, who is a consultant for BMS and reported payments from the company.
GERCOR NEONIPIGA was a phase 2 study with no comparator group and only 32 patients, but even so, after a 6-cycle course of nivolumab and ipilimumab, there was no sign of tumor in 17 of the 29 patients (59%) who had surgery specimens evaluable by pathology.
Indeed, two patients refused surgery after their preop endoscopic biopsies came back clear with no tumor cells. Surgery was called off in a third patient who developed metastases beforehand.
After a median of 12 months follow-up, there’s was no recurrence or progression in 30 patients (94%). The remaining two included the metastatic patient and one who died 3 days after surgery from cardiovascular complications.
If the findings pan out with additional research, the approach could be a boon for people who respond. “Avoiding surgery is a dream for these patients,” said lead investigator Thierry Andre, MD, a medical oncology professor at Sorbonne University, Paris, when he presented the findings at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
The trial “raises the question whether surgery can be delayed or avoided in some patients with localized” disease. Given the findings, “it seems possible not for all but probably for half, maybe more.” As in the two subjects who opted out of surgery, preop endoscopic biopsies could be used to identify complete responders with active surveillance afterwards, he said.
The study included 16 patients with gastric cancer and 16 with esophagogastric adenocarcinoma. They were mismatch repair deficient, which Dr. Andre said predicts response to immunotherapy.
At baseline, 22 had stage T3 disease and four had stage T2 disease, and stage was not evaluable by echo-endoscopy in 6. Nodal status was unknown, but the patients had no metastases at baseline.
They underwent six nivolumab 240-mg infusions and two ipilimumab 1–mg/kg infusions over 12 weeks, followed by R0 resections a median of 5 weeks after the last nivolumab injection.
Surgical specimens from 17 patients (59%) showed a complete pathological response to neoadjuvant immunotherapy (Becker tumor regression grade (TRG) 1a, ypT0N0). TRG was 1b – less than 10% residual tumor in tumor bed in four patients. TRG was 2 in two patients with 10%-50% of residual tumor remaining, and six had a TRG of 3 with more than half of the tumor remaining after immunotherapy.
Based on tumor response, 25 patients had nine additional nivolumab infusions after surgery with 480 mg infused monthly.
Dr. Andre explained that people want to avoid surgery because of the substantial morbidity that was shown in the study, plus 54% of patients had complications, including anastomotic leaks, pancreatitis, pneumonia, and other problems.
There were no new safety signals with neoadjuvant therapy; 25% of patients had grade 3 or 4 events.
The study was conducted in 10 centers in France. About three-quarters of the subjects were men and the median age was 65 years.
Bristol Meyers Squibb supplied the nivolumab and ipilimumab and partially funded the work. Many of the investigators had ties to the company, including Dr. Andre, who is a consultant for BMS and reported payments from the company.
GERCOR NEONIPIGA was a phase 2 study with no comparator group and only 32 patients, but even so, after a 6-cycle course of nivolumab and ipilimumab, there was no sign of tumor in 17 of the 29 patients (59%) who had surgery specimens evaluable by pathology.
Indeed, two patients refused surgery after their preop endoscopic biopsies came back clear with no tumor cells. Surgery was called off in a third patient who developed metastases beforehand.
After a median of 12 months follow-up, there’s was no recurrence or progression in 30 patients (94%). The remaining two included the metastatic patient and one who died 3 days after surgery from cardiovascular complications.
If the findings pan out with additional research, the approach could be a boon for people who respond. “Avoiding surgery is a dream for these patients,” said lead investigator Thierry Andre, MD, a medical oncology professor at Sorbonne University, Paris, when he presented the findings at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium.
The trial “raises the question whether surgery can be delayed or avoided in some patients with localized” disease. Given the findings, “it seems possible not for all but probably for half, maybe more.” As in the two subjects who opted out of surgery, preop endoscopic biopsies could be used to identify complete responders with active surveillance afterwards, he said.
The study included 16 patients with gastric cancer and 16 with esophagogastric adenocarcinoma. They were mismatch repair deficient, which Dr. Andre said predicts response to immunotherapy.
At baseline, 22 had stage T3 disease and four had stage T2 disease, and stage was not evaluable by echo-endoscopy in 6. Nodal status was unknown, but the patients had no metastases at baseline.
They underwent six nivolumab 240-mg infusions and two ipilimumab 1–mg/kg infusions over 12 weeks, followed by R0 resections a median of 5 weeks after the last nivolumab injection.
Surgical specimens from 17 patients (59%) showed a complete pathological response to neoadjuvant immunotherapy (Becker tumor regression grade (TRG) 1a, ypT0N0). TRG was 1b – less than 10% residual tumor in tumor bed in four patients. TRG was 2 in two patients with 10%-50% of residual tumor remaining, and six had a TRG of 3 with more than half of the tumor remaining after immunotherapy.
Based on tumor response, 25 patients had nine additional nivolumab infusions after surgery with 480 mg infused monthly.
Dr. Andre explained that people want to avoid surgery because of the substantial morbidity that was shown in the study, plus 54% of patients had complications, including anastomotic leaks, pancreatitis, pneumonia, and other problems.
There were no new safety signals with neoadjuvant therapy; 25% of patients had grade 3 or 4 events.
The study was conducted in 10 centers in France. About three-quarters of the subjects were men and the median age was 65 years.
Bristol Meyers Squibb supplied the nivolumab and ipilimumab and partially funded the work. Many of the investigators had ties to the company, including Dr. Andre, who is a consultant for BMS and reported payments from the company.
FROM GI CANCERS SYMPOSIUM 2022
Allopurinol found safe in patients with concomitant gout, CKD
Allopurinol treatment is not associated with increased mortality in patients with gout and chronic kidney disease even at 5 years after starting treatment, a study has found.
Around one in five patients with gout also have chronic kidney disease, and previous research suggests that hyperuricemia is itself a contributor to renal disease, which is why there has been interest in the use of serum urate–lowering medication in patients with both conditions.
Since the publication of two earlier randomized controlled trials suggested a twofold increase in mortality among patients with renal disease who were treated with allopurinol in an attempt to slow progression, there has been wariness about the drug in patients with compromised renal function.
In a study published in Annals of Internal Medicine, Jie Wei, PhD, of Xiangya Hospital at Central South University in Changsha, China, and coauthors report the results of their retrospective, population-based study of 5,277 adults aged 40 and older with gout and moderate to severe chronic kidney disease who were initiated on allopurinol and 5,277 matched individuals not on allopurinol.
At 5 years after the patients started allopurinol, the study found that mortality was a statistically significant 15% lower (hazard ratio, 0.85; 95% confidence interval, 0.77-0.93) among those on allopurinol, compared with those not taking the drug. The rate was 4.9 deaths per 100 person-years among those on allopurinol, compared with 5.8 among those not taking it.
The researchers also created two simulated randomized clinical trials from the data for initiators of allopurinol, replicating each initiator twice. The first trial assigned patient replicates either to achieving a target serum urate level of less than 0.36 mmol/L within a year or not achieving it. The second assigned patient replicates to either an allopurinol dose-escalation group or no dose escalation.
For the target serum urate level study, 1,484 achieved the target, and this was associated with a 13% lower hazard ratio for mortality that just missed statistical significance (HR, 0.87; 95% confidence interval, 0.75-1.01).
In the dose-escalation study, there were 773 participants who increased their dose of allopurinol in the first year after initiation – from a median of 100 mg/day to a median final dose of 300 mg/day – and 2,923 who didn’t. Those who escalated their dose had a nonsignificant 12% lower risk of mortality (HR, 0.88; 95% CI, 0.73-1.07), compared with those who didn’t.
The authors suggest that this could be the result of confounding, as patients who achieved target serum urate levels may have been of better health generally than those who didn’t, which could also have contributed to lower mortality.
Coauthor of the study Yuqing Zhang, DSc, of Massachusetts General Hospital and Harvard Medical School, Boston, said there had previously been a theory that allopurinol could protect against progression of renal disease. However, the two randomized, controlled trials in patients with chronic kidney disease but not gout published in 2020 suggested that allopurinol was instead associated with a doubling of mortality in this group.
“This study really shows convincing evidence that among gout patients with renal disease, allopurinol does not increase mortality,” Dr. Zhang told this news organization. He suggested the reason that the earlier studies had found higher mortality among patients on allopurinol was because those patients did not have gout. Given that gout can increase mortality, treating it effectively with allopurinol may therefore reduce mortality even in patients with concurrent chronic kidney disease.
Commenting on the study, Angelo Gaffo, MD, from the Birmingham VA Medical Center and the division of rheumatology at the University of Alabama at Birmingham, said that, while there had been data suggesting increased mortality, the findings from this “very well-done” study were reassuring and even suggested a possible decrease in mortality associated with allopurinol.

“I wouldn’t scream it out loud because it needs confirmation, but it’s something also that we have a sense that could be true,” he said.
Dr. Gaffo noted that patients treated with allopurinol tended to be those with fewer comorbidities. “Patients who have a lot of comorbidities probably are less likely to have their dose of allopurinol started or increased because of some concerns that practitioners may have about putting them on another medicine or increasing the dose of that medicine,” he said.
He also stressed that the findings still need replication in other large database studies, given that a prospective, randomized clinical trial addressing such a question would be difficult to conduct.
The study was supported by the Project Program of National Clinical Research Center for Geriatric Disorders, the National Natural Science Foundation of China, and the U.S. National Institutes of Health. Two authors reported consulting fees from the pharmaceutical sector unrelated to the study. No other conflicts of interest were declared.
A version of this article first appeared on Medscape.com.
Allopurinol treatment is not associated with increased mortality in patients with gout and chronic kidney disease even at 5 years after starting treatment, a study has found.
Around one in five patients with gout also have chronic kidney disease, and previous research suggests that hyperuricemia is itself a contributor to renal disease, which is why there has been interest in the use of serum urate–lowering medication in patients with both conditions.
Since the publication of two earlier randomized controlled trials suggested a twofold increase in mortality among patients with renal disease who were treated with allopurinol in an attempt to slow progression, there has been wariness about the drug in patients with compromised renal function.
In a study published in Annals of Internal Medicine, Jie Wei, PhD, of Xiangya Hospital at Central South University in Changsha, China, and coauthors report the results of their retrospective, population-based study of 5,277 adults aged 40 and older with gout and moderate to severe chronic kidney disease who were initiated on allopurinol and 5,277 matched individuals not on allopurinol.
At 5 years after the patients started allopurinol, the study found that mortality was a statistically significant 15% lower (hazard ratio, 0.85; 95% confidence interval, 0.77-0.93) among those on allopurinol, compared with those not taking the drug. The rate was 4.9 deaths per 100 person-years among those on allopurinol, compared with 5.8 among those not taking it.
The researchers also created two simulated randomized clinical trials from the data for initiators of allopurinol, replicating each initiator twice. The first trial assigned patient replicates either to achieving a target serum urate level of less than 0.36 mmol/L within a year or not achieving it. The second assigned patient replicates to either an allopurinol dose-escalation group or no dose escalation.
For the target serum urate level study, 1,484 achieved the target, and this was associated with a 13% lower hazard ratio for mortality that just missed statistical significance (HR, 0.87; 95% confidence interval, 0.75-1.01).
In the dose-escalation study, there were 773 participants who increased their dose of allopurinol in the first year after initiation – from a median of 100 mg/day to a median final dose of 300 mg/day – and 2,923 who didn’t. Those who escalated their dose had a nonsignificant 12% lower risk of mortality (HR, 0.88; 95% CI, 0.73-1.07), compared with those who didn’t.
The authors suggest that this could be the result of confounding, as patients who achieved target serum urate levels may have been of better health generally than those who didn’t, which could also have contributed to lower mortality.
Coauthor of the study Yuqing Zhang, DSc, of Massachusetts General Hospital and Harvard Medical School, Boston, said there had previously been a theory that allopurinol could protect against progression of renal disease. However, the two randomized, controlled trials in patients with chronic kidney disease but not gout published in 2020 suggested that allopurinol was instead associated with a doubling of mortality in this group.
“This study really shows convincing evidence that among gout patients with renal disease, allopurinol does not increase mortality,” Dr. Zhang told this news organization. He suggested the reason that the earlier studies had found higher mortality among patients on allopurinol was because those patients did not have gout. Given that gout can increase mortality, treating it effectively with allopurinol may therefore reduce mortality even in patients with concurrent chronic kidney disease.
Commenting on the study, Angelo Gaffo, MD, from the Birmingham VA Medical Center and the division of rheumatology at the University of Alabama at Birmingham, said that, while there had been data suggesting increased mortality, the findings from this “very well-done” study were reassuring and even suggested a possible decrease in mortality associated with allopurinol.
“I wouldn’t scream it out loud because it needs confirmation, but it’s something also that we have a sense that could be true,” he said.
Dr. Gaffo noted that patients treated with allopurinol tended to be those with fewer comorbidities. “Patients who have a lot of comorbidities probably are less likely to have their dose of allopurinol started or increased because of some concerns that practitioners may have about putting them on another medicine or increasing the dose of that medicine,” he said.
He also stressed that the findings still need replication in other large database studies, given that a prospective, randomized clinical trial addressing such a question would be difficult to conduct.
The study was supported by the Project Program of National Clinical Research Center for Geriatric Disorders, the National Natural Science Foundation of China, and the U.S. National Institutes of Health. Two authors reported consulting fees from the pharmaceutical sector unrelated to the study. No other conflicts of interest were declared.
A version of this article first appeared on Medscape.com.
Allopurinol treatment is not associated with increased mortality in patients with gout and chronic kidney disease even at 5 years after starting treatment, a study has found.
Around one in five patients with gout also have chronic kidney disease, and previous research suggests that hyperuricemia is itself a contributor to renal disease, which is why there has been interest in the use of serum urate–lowering medication in patients with both conditions.
Since the publication of two earlier randomized controlled trials suggested a twofold increase in mortality among patients with renal disease who were treated with allopurinol in an attempt to slow progression, there has been wariness about the drug in patients with compromised renal function.
In a study published in Annals of Internal Medicine, Jie Wei, PhD, of Xiangya Hospital at Central South University in Changsha, China, and coauthors report the results of their retrospective, population-based study of 5,277 adults aged 40 and older with gout and moderate to severe chronic kidney disease who were initiated on allopurinol and 5,277 matched individuals not on allopurinol.
At 5 years after the patients started allopurinol, the study found that mortality was a statistically significant 15% lower (hazard ratio, 0.85; 95% confidence interval, 0.77-0.93) among those on allopurinol, compared with those not taking the drug. The rate was 4.9 deaths per 100 person-years among those on allopurinol, compared with 5.8 among those not taking it.
The researchers also created two simulated randomized clinical trials from the data for initiators of allopurinol, replicating each initiator twice. The first trial assigned patient replicates either to achieving a target serum urate level of less than 0.36 mmol/L within a year or not achieving it. The second assigned patient replicates to either an allopurinol dose-escalation group or no dose escalation.
For the target serum urate level study, 1,484 achieved the target, and this was associated with a 13% lower hazard ratio for mortality that just missed statistical significance (HR, 0.87; 95% confidence interval, 0.75-1.01).
In the dose-escalation study, there were 773 participants who increased their dose of allopurinol in the first year after initiation – from a median of 100 mg/day to a median final dose of 300 mg/day – and 2,923 who didn’t. Those who escalated their dose had a nonsignificant 12% lower risk of mortality (HR, 0.88; 95% CI, 0.73-1.07), compared with those who didn’t.
The authors suggest that this could be the result of confounding, as patients who achieved target serum urate levels may have been of better health generally than those who didn’t, which could also have contributed to lower mortality.
Coauthor of the study Yuqing Zhang, DSc, of Massachusetts General Hospital and Harvard Medical School, Boston, said there had previously been a theory that allopurinol could protect against progression of renal disease. However, the two randomized, controlled trials in patients with chronic kidney disease but not gout published in 2020 suggested that allopurinol was instead associated with a doubling of mortality in this group.
“This study really shows convincing evidence that among gout patients with renal disease, allopurinol does not increase mortality,” Dr. Zhang told this news organization. He suggested the reason that the earlier studies had found higher mortality among patients on allopurinol was because those patients did not have gout. Given that gout can increase mortality, treating it effectively with allopurinol may therefore reduce mortality even in patients with concurrent chronic kidney disease.
Commenting on the study, Angelo Gaffo, MD, from the Birmingham VA Medical Center and the division of rheumatology at the University of Alabama at Birmingham, said that, while there had been data suggesting increased mortality, the findings from this “very well-done” study were reassuring and even suggested a possible decrease in mortality associated with allopurinol.
“I wouldn’t scream it out loud because it needs confirmation, but it’s something also that we have a sense that could be true,” he said.
Dr. Gaffo noted that patients treated with allopurinol tended to be those with fewer comorbidities. “Patients who have a lot of comorbidities probably are less likely to have their dose of allopurinol started or increased because of some concerns that practitioners may have about putting them on another medicine or increasing the dose of that medicine,” he said.
He also stressed that the findings still need replication in other large database studies, given that a prospective, randomized clinical trial addressing such a question would be difficult to conduct.
The study was supported by the Project Program of National Clinical Research Center for Geriatric Disorders, the National Natural Science Foundation of China, and the U.S. National Institutes of Health. Two authors reported consulting fees from the pharmaceutical sector unrelated to the study. No other conflicts of interest were declared.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Children and COVID: United States passes 10 million total cases
Weekly COVID-19 cases in children topped 1 million for the first time as the cumulative count surpassed 10 million since the start of the pandemic, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. Those 10.6 million child cases represent 18.4% of all cases, and the latest 1.15 million represented 25.5% of all cases for the week.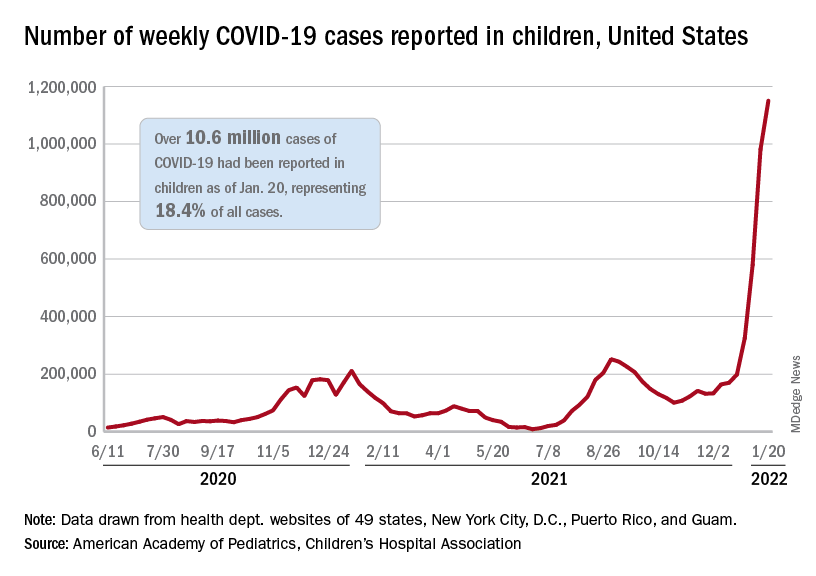
Regionally, the South had the most cases with over 380,000 for the week of Jan. 14-20, while the West was next with close to 350,000, followed by the Midwest and then the East. Among the states, the largest percent increases – on the order of 30% – came in New England (Massachusetts, Rhode Island, and Vermont), as well as Virginia and California, the AAP and CHA said.
Examining all those cases by vaccination status shows an obvious difference between the Omicron and Delta variants: The fully vaccinated have been hit much harder than before. For the week ending Dec. 25, 2021, the incidence of COVID-19 in children aged 12-17 years was 704 per 100,000 among those were unvaccinated and 384 per 100,000 in those who were fully vaccinated. During the Delta surge in the summer of 2021, the peak rates were 938 (unvaccinated) and 79 (vaccinated), the Centers for Disease Control and Prevention said.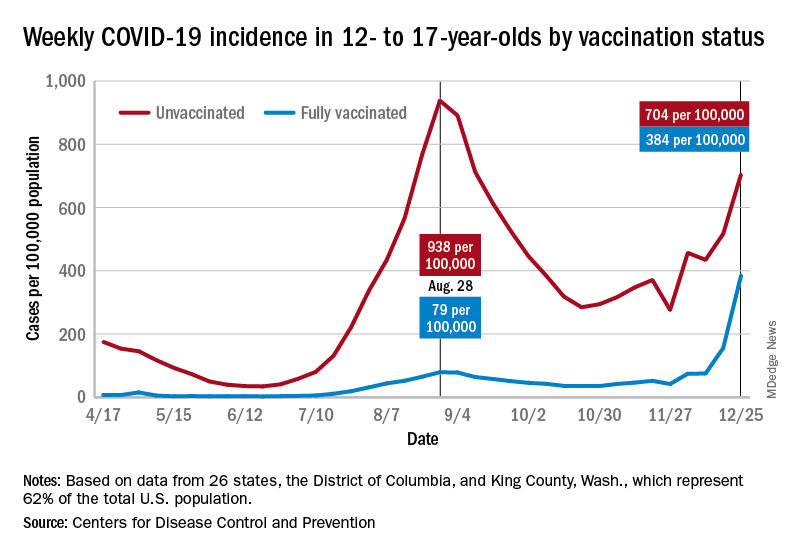
Hospitalizations are also at record levels, but two separate CDC databases seem to show a decline in child admissions over the last available week or so of data, which follows the trend among all ages. The peak among children aged 0-17 years came on Jan. 15, when the rate of new admissions reached 1.25 per 100,000, based on reporting to the CDC from 5,265 hospitals nationwide.
The second database, the COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), indicates that children aged 0-4 years had the highest admission rate, 14.5 per 100,000, for the week ending Jan. 8, compared with 5.5 per 100,000 for 12- to 17-year-olds and 2.3 per 100,000 for those aged 5-11 years. COVID-NET covers almost 100 counties in 10 states, along with 4 entire states, and represents about 10% of the U.S. population.
Vaccinations rose briefly in late December and into January to meet the Omicron surge, but the numbers for the latest week show a return to their earlier levels. In children aged 5-11 years, new vaccinations went from 381,000 for the week of Dec. 20-26 to 524,000 for Jan. 3-9, but fell to just 260,000 during Jan. 17-23. The response was a little later for those aged 12-17, with the big week coming Jan. 10-16, but there was still a 38% drop for Jan. 17-23, according to the CDC’s COVID Data Tracker.
Currently, 29.3% of all 5- to 11-year-olds have received at least one dose of the COVID vaccine, and an even 20.0% are fully vaccinated. For children aged 12-17, the corresponding figures are 65.8% and 55.1%, the CDC said.
Statewide vaccination rates vary from Vermont’s high of 61% for those aged 5-11 to 12% for Alabama, Louisiana, and Mississippi, while Hawaii has the highest rate for 12- to 17-year-olds at 92% and Wyoming has the lowest at 39%, the AAP reported.
Weekly COVID-19 cases in children topped 1 million for the first time as the cumulative count surpassed 10 million since the start of the pandemic, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. Those 10.6 million child cases represent 18.4% of all cases, and the latest 1.15 million represented 25.5% of all cases for the week.
Regionally, the South had the most cases with over 380,000 for the week of Jan. 14-20, while the West was next with close to 350,000, followed by the Midwest and then the East. Among the states, the largest percent increases – on the order of 30% – came in New England (Massachusetts, Rhode Island, and Vermont), as well as Virginia and California, the AAP and CHA said.
Examining all those cases by vaccination status shows an obvious difference between the Omicron and Delta variants: The fully vaccinated have been hit much harder than before. For the week ending Dec. 25, 2021, the incidence of COVID-19 in children aged 12-17 years was 704 per 100,000 among those were unvaccinated and 384 per 100,000 in those who were fully vaccinated. During the Delta surge in the summer of 2021, the peak rates were 938 (unvaccinated) and 79 (vaccinated), the Centers for Disease Control and Prevention said.
Hospitalizations are also at record levels, but two separate CDC databases seem to show a decline in child admissions over the last available week or so of data, which follows the trend among all ages. The peak among children aged 0-17 years came on Jan. 15, when the rate of new admissions reached 1.25 per 100,000, based on reporting to the CDC from 5,265 hospitals nationwide.
The second database, the COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), indicates that children aged 0-4 years had the highest admission rate, 14.5 per 100,000, for the week ending Jan. 8, compared with 5.5 per 100,000 for 12- to 17-year-olds and 2.3 per 100,000 for those aged 5-11 years. COVID-NET covers almost 100 counties in 10 states, along with 4 entire states, and represents about 10% of the U.S. population.
Vaccinations rose briefly in late December and into January to meet the Omicron surge, but the numbers for the latest week show a return to their earlier levels. In children aged 5-11 years, new vaccinations went from 381,000 for the week of Dec. 20-26 to 524,000 for Jan. 3-9, but fell to just 260,000 during Jan. 17-23. The response was a little later for those aged 12-17, with the big week coming Jan. 10-16, but there was still a 38% drop for Jan. 17-23, according to the CDC’s COVID Data Tracker.
Currently, 29.3% of all 5- to 11-year-olds have received at least one dose of the COVID vaccine, and an even 20.0% are fully vaccinated. For children aged 12-17, the corresponding figures are 65.8% and 55.1%, the CDC said.
Statewide vaccination rates vary from Vermont’s high of 61% for those aged 5-11 to 12% for Alabama, Louisiana, and Mississippi, while Hawaii has the highest rate for 12- to 17-year-olds at 92% and Wyoming has the lowest at 39%, the AAP reported.
Weekly COVID-19 cases in children topped 1 million for the first time as the cumulative count surpassed 10 million since the start of the pandemic, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. Those 10.6 million child cases represent 18.4% of all cases, and the latest 1.15 million represented 25.5% of all cases for the week.
Regionally, the South had the most cases with over 380,000 for the week of Jan. 14-20, while the West was next with close to 350,000, followed by the Midwest and then the East. Among the states, the largest percent increases – on the order of 30% – came in New England (Massachusetts, Rhode Island, and Vermont), as well as Virginia and California, the AAP and CHA said.
Examining all those cases by vaccination status shows an obvious difference between the Omicron and Delta variants: The fully vaccinated have been hit much harder than before. For the week ending Dec. 25, 2021, the incidence of COVID-19 in children aged 12-17 years was 704 per 100,000 among those were unvaccinated and 384 per 100,000 in those who were fully vaccinated. During the Delta surge in the summer of 2021, the peak rates were 938 (unvaccinated) and 79 (vaccinated), the Centers for Disease Control and Prevention said.
Hospitalizations are also at record levels, but two separate CDC databases seem to show a decline in child admissions over the last available week or so of data, which follows the trend among all ages. The peak among children aged 0-17 years came on Jan. 15, when the rate of new admissions reached 1.25 per 100,000, based on reporting to the CDC from 5,265 hospitals nationwide.
The second database, the COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), indicates that children aged 0-4 years had the highest admission rate, 14.5 per 100,000, for the week ending Jan. 8, compared with 5.5 per 100,000 for 12- to 17-year-olds and 2.3 per 100,000 for those aged 5-11 years. COVID-NET covers almost 100 counties in 10 states, along with 4 entire states, and represents about 10% of the U.S. population.
Vaccinations rose briefly in late December and into January to meet the Omicron surge, but the numbers for the latest week show a return to their earlier levels. In children aged 5-11 years, new vaccinations went from 381,000 for the week of Dec. 20-26 to 524,000 for Jan. 3-9, but fell to just 260,000 during Jan. 17-23. The response was a little later for those aged 12-17, with the big week coming Jan. 10-16, but there was still a 38% drop for Jan. 17-23, according to the CDC’s COVID Data Tracker.
Currently, 29.3% of all 5- to 11-year-olds have received at least one dose of the COVID vaccine, and an even 20.0% are fully vaccinated. For children aged 12-17, the corresponding figures are 65.8% and 55.1%, the CDC said.
Statewide vaccination rates vary from Vermont’s high of 61% for those aged 5-11 to 12% for Alabama, Louisiana, and Mississippi, while Hawaii has the highest rate for 12- to 17-year-olds at 92% and Wyoming has the lowest at 39%, the AAP reported.
COVID brain fog is a ‘true neurologic condition’
early research suggests. Investigators found abnormalities in cerebrospinal fluid (CSF) and other risk factors, including diabetes and hypertension, present in individuals with mild COVID-19 experiencing persistent cognitive problems, often referred to as “brain fog.”
“We’re seeing changes to the [CSF] in the brain of most people who report cognitive changes,” said Joanna Hellmuth, MD, assistant professor of neurology, Memory and Aging Center, University of California, San Francisco. “We’re just in the beginning stages, but I hope this study will provide some legitimacy to this being a true neurologic condition.”
The study was published online Jan. 18, 2022, in Annals of Clinical and Translational Neurology.
No guidance
There is currently no guidance on how to identify patients with COVID-related cognitive changes, said Dr. Hellmuth. “The term ‘brain fog’ is not based in science or medicine, but that’s the most common term we use to describe this.”
The analysis included adults with confirmed SARS-CoV-2 infection not requiring hospitalization who were enrolled in the Long-term Impact of Infection with Novel Coronavirus study.
Participants underwent a structured interview that covered COVID-19 illness, past medical history, preexisting cognitive risk factors, medications, and cognitive symptoms following onset of COVID-19. They also completed an in-person battery of cognitive tests.
The analysis included 22 participants with at least one new cognitive symptom who had cognitive post-acute sequelae of SARS-CoV-2 infection (PASC). Ten cognitive controls reported no new cognitive symptoms after acute infection.
Participants were a median age of 41 years, had a median of 16 years of education, and were assessed a median of 10.1 months from their first COVID-19 symptom. There were no group differences in terms of age, gender, years of education, or distribution of race/ethnicity (all P > .05).
Among those with cognitive PASC, 43% reported cognitive symptoms starting 1 or more months after the first COVID symptom. About 29% reported cognitive changes started 2 or more months after their first COVID symptom.
“The immune system could be altered in some way after the infection, and perhaps that’s what’s contributing to these delayed onset cognitive changes,” said Dr. Hellmuth.
Compared with controls, participants with cognitive PASC had more preexisting cognitive risk factors (a median of 2.5 vs. 0; P = .03). These included hypertension and diabetes, which increase the risk of stroke, mild cognitive impairment, vascular dementia, traumatic brain injury, (TBI), learning disabilities, anxiety, depression, stimulant use, and ADHD, which may make the brain more vulnerable to executive functioning problems.
Dr. Hellmuth noted that the study wasn’t powered to determine whether any individual risk factor was associated with risk of cognitive changes.
As there are no published neuropsychological testing criteria for cognitive PASC, the researchers applied the equivalent criteria for HIV-associated neurocognitive disorder (HAND), a similar, virally associated cognitive disorder. Only 59% of those with cognitive PASC met equivalent HAND criteria for objective cognitive impairment versus 70% of cognitive controls. This, the investigators noted, highlights “the challenges and incongruities of using subjective, versus objective cognitive assessments for diagnosis.”
Is self-report enough?
While there is currently “nothing objective doctors can hang their hats on to say ‘you do’ or ‘you don’t’ have cognitive changes related to COVID,” using the HAND criteria is “not particularly helpful,” said Dr. Hellmuth. “Comparing an individual to a population-based norm in this case is really nuanced, and we shouldn’t rely on this solely to determine whether they do, or don’t, have cognitive changes.”
Perhaps self-reports in this case are “enough” said Dr. Hellmuth. “People know their brains better than anyone else, better than any doctor will.”
A total of 13 in the cognitive PASC group and 4 in the control group consented to a lumbar puncture. Cognitive PASC participants were older than controls (median of 47 vs. 28 years; P = .03) with no other between-group differences.
Overall, 77% of participants with cognitive PASC had a CSF abnormality, compared with 0% of cognitive controls (P = .01). CSF abnormalities included elevated protein levels with no other explainable cause in 2 of the 13 subjects with PASC, which Dr. Hellmuth said is typically a marker of inflammation.
Researchers also noted abnormal oligoclonal banding, a collection of antibodies, in the blood or brain fluid. These were identified in 69% of participants with cognitive PASC, compared with 0% of cognitive controls (P = .03).
“When we find this pattern in both blood and brain, it suggests a systemic inflammatory disorder,” although “we have no idea what these antibodies are targeting,” said Dr. Hellmuth.
The study represents “the very beginning stages” of PASC becoming a medical diagnosis “where doctors know what to call it, how to treat it, and how to do blood and cerebrospinal fluid tests to diagnose it,” said Dr. Hellmuth.
She hopes PASC will receive medical legitimacy just as TBI has. In years past, a player was hit on the head or had their “bell rung,” simply returned to the field. “Now that we understand the science, we call it a mild TBI or concussion, and we have a very different medical approach to it.”
A limitation of the study was the small sample size, which may hinder the results’ validity. In addition, the study demographics may not reflect the broader population of those impacted by PASC.
‘A first substantial step’
Commenting on the research, William Schaffner, MD, professor, division of infectious diseases, Vanderbilt University Medical Center, Nashville, Tenn., said the new results represent “a first substantial step on the road to trying to find out what’s going on” with COVID patients dealing with cognitive issues.
Dr. Schaffner noted that elevated protein levels, identified in some study subjects, “is usually a consequence of previous inflammation” and is “a very interesting” finding. “In people who are otherwise normal, if you do a lumbar puncture, you don’t find elevated proteins.”
However, he noted the “diversity of results” from CSF examinations. “A single pattern does not leap out.”
What the researchers are observing “is not just a phenomenon of the mind or just something psychological,” said Dr. Schaffner. “Something physical is going on here.”
The study was funded by grants from the National Institute of Mental Health and the National Institute of Neurological Disorders and Stroke. Dr. Hellmuth received grant support from the National Institutes of Health/NIMH supporting this work and personal fees for medical-legal consultation outside of the submitted work. Dr. Schaffner has disclosed not relevant financial relationships.
A version of this article first appeared on Medscape.com.
early research suggests. Investigators found abnormalities in cerebrospinal fluid (CSF) and other risk factors, including diabetes and hypertension, present in individuals with mild COVID-19 experiencing persistent cognitive problems, often referred to as “brain fog.”
“We’re seeing changes to the [CSF] in the brain of most people who report cognitive changes,” said Joanna Hellmuth, MD, assistant professor of neurology, Memory and Aging Center, University of California, San Francisco. “We’re just in the beginning stages, but I hope this study will provide some legitimacy to this being a true neurologic condition.”
The study was published online Jan. 18, 2022, in Annals of Clinical and Translational Neurology.
No guidance
There is currently no guidance on how to identify patients with COVID-related cognitive changes, said Dr. Hellmuth. “The term ‘brain fog’ is not based in science or medicine, but that’s the most common term we use to describe this.”
The analysis included adults with confirmed SARS-CoV-2 infection not requiring hospitalization who were enrolled in the Long-term Impact of Infection with Novel Coronavirus study.
Participants underwent a structured interview that covered COVID-19 illness, past medical history, preexisting cognitive risk factors, medications, and cognitive symptoms following onset of COVID-19. They also completed an in-person battery of cognitive tests.
The analysis included 22 participants with at least one new cognitive symptom who had cognitive post-acute sequelae of SARS-CoV-2 infection (PASC). Ten cognitive controls reported no new cognitive symptoms after acute infection.
Participants were a median age of 41 years, had a median of 16 years of education, and were assessed a median of 10.1 months from their first COVID-19 symptom. There were no group differences in terms of age, gender, years of education, or distribution of race/ethnicity (all P > .05).
Among those with cognitive PASC, 43% reported cognitive symptoms starting 1 or more months after the first COVID symptom. About 29% reported cognitive changes started 2 or more months after their first COVID symptom.
“The immune system could be altered in some way after the infection, and perhaps that’s what’s contributing to these delayed onset cognitive changes,” said Dr. Hellmuth.
Compared with controls, participants with cognitive PASC had more preexisting cognitive risk factors (a median of 2.5 vs. 0; P = .03). These included hypertension and diabetes, which increase the risk of stroke, mild cognitive impairment, vascular dementia, traumatic brain injury, (TBI), learning disabilities, anxiety, depression, stimulant use, and ADHD, which may make the brain more vulnerable to executive functioning problems.
Dr. Hellmuth noted that the study wasn’t powered to determine whether any individual risk factor was associated with risk of cognitive changes.
As there are no published neuropsychological testing criteria for cognitive PASC, the researchers applied the equivalent criteria for HIV-associated neurocognitive disorder (HAND), a similar, virally associated cognitive disorder. Only 59% of those with cognitive PASC met equivalent HAND criteria for objective cognitive impairment versus 70% of cognitive controls. This, the investigators noted, highlights “the challenges and incongruities of using subjective, versus objective cognitive assessments for diagnosis.”
Is self-report enough?
While there is currently “nothing objective doctors can hang their hats on to say ‘you do’ or ‘you don’t’ have cognitive changes related to COVID,” using the HAND criteria is “not particularly helpful,” said Dr. Hellmuth. “Comparing an individual to a population-based norm in this case is really nuanced, and we shouldn’t rely on this solely to determine whether they do, or don’t, have cognitive changes.”
Perhaps self-reports in this case are “enough” said Dr. Hellmuth. “People know their brains better than anyone else, better than any doctor will.”
A total of 13 in the cognitive PASC group and 4 in the control group consented to a lumbar puncture. Cognitive PASC participants were older than controls (median of 47 vs. 28 years; P = .03) with no other between-group differences.
Overall, 77% of participants with cognitive PASC had a CSF abnormality, compared with 0% of cognitive controls (P = .01). CSF abnormalities included elevated protein levels with no other explainable cause in 2 of the 13 subjects with PASC, which Dr. Hellmuth said is typically a marker of inflammation.
Researchers also noted abnormal oligoclonal banding, a collection of antibodies, in the blood or brain fluid. These were identified in 69% of participants with cognitive PASC, compared with 0% of cognitive controls (P = .03).
“When we find this pattern in both blood and brain, it suggests a systemic inflammatory disorder,” although “we have no idea what these antibodies are targeting,” said Dr. Hellmuth.
The study represents “the very beginning stages” of PASC becoming a medical diagnosis “where doctors know what to call it, how to treat it, and how to do blood and cerebrospinal fluid tests to diagnose it,” said Dr. Hellmuth.
She hopes PASC will receive medical legitimacy just as TBI has. In years past, a player was hit on the head or had their “bell rung,” simply returned to the field. “Now that we understand the science, we call it a mild TBI or concussion, and we have a very different medical approach to it.”
A limitation of the study was the small sample size, which may hinder the results’ validity. In addition, the study demographics may not reflect the broader population of those impacted by PASC.
‘A first substantial step’
Commenting on the research, William Schaffner, MD, professor, division of infectious diseases, Vanderbilt University Medical Center, Nashville, Tenn., said the new results represent “a first substantial step on the road to trying to find out what’s going on” with COVID patients dealing with cognitive issues.
Dr. Schaffner noted that elevated protein levels, identified in some study subjects, “is usually a consequence of previous inflammation” and is “a very interesting” finding. “In people who are otherwise normal, if you do a lumbar puncture, you don’t find elevated proteins.”
However, he noted the “diversity of results” from CSF examinations. “A single pattern does not leap out.”
What the researchers are observing “is not just a phenomenon of the mind or just something psychological,” said Dr. Schaffner. “Something physical is going on here.”
The study was funded by grants from the National Institute of Mental Health and the National Institute of Neurological Disorders and Stroke. Dr. Hellmuth received grant support from the National Institutes of Health/NIMH supporting this work and personal fees for medical-legal consultation outside of the submitted work. Dr. Schaffner has disclosed not relevant financial relationships.
A version of this article first appeared on Medscape.com.
early research suggests. Investigators found abnormalities in cerebrospinal fluid (CSF) and other risk factors, including diabetes and hypertension, present in individuals with mild COVID-19 experiencing persistent cognitive problems, often referred to as “brain fog.”
“We’re seeing changes to the [CSF] in the brain of most people who report cognitive changes,” said Joanna Hellmuth, MD, assistant professor of neurology, Memory and Aging Center, University of California, San Francisco. “We’re just in the beginning stages, but I hope this study will provide some legitimacy to this being a true neurologic condition.”
The study was published online Jan. 18, 2022, in Annals of Clinical and Translational Neurology.
No guidance
There is currently no guidance on how to identify patients with COVID-related cognitive changes, said Dr. Hellmuth. “The term ‘brain fog’ is not based in science or medicine, but that’s the most common term we use to describe this.”
The analysis included adults with confirmed SARS-CoV-2 infection not requiring hospitalization who were enrolled in the Long-term Impact of Infection with Novel Coronavirus study.
Participants underwent a structured interview that covered COVID-19 illness, past medical history, preexisting cognitive risk factors, medications, and cognitive symptoms following onset of COVID-19. They also completed an in-person battery of cognitive tests.
The analysis included 22 participants with at least one new cognitive symptom who had cognitive post-acute sequelae of SARS-CoV-2 infection (PASC). Ten cognitive controls reported no new cognitive symptoms after acute infection.
Participants were a median age of 41 years, had a median of 16 years of education, and were assessed a median of 10.1 months from their first COVID-19 symptom. There were no group differences in terms of age, gender, years of education, or distribution of race/ethnicity (all P > .05).
Among those with cognitive PASC, 43% reported cognitive symptoms starting 1 or more months after the first COVID symptom. About 29% reported cognitive changes started 2 or more months after their first COVID symptom.
“The immune system could be altered in some way after the infection, and perhaps that’s what’s contributing to these delayed onset cognitive changes,” said Dr. Hellmuth.
Compared with controls, participants with cognitive PASC had more preexisting cognitive risk factors (a median of 2.5 vs. 0; P = .03). These included hypertension and diabetes, which increase the risk of stroke, mild cognitive impairment, vascular dementia, traumatic brain injury, (TBI), learning disabilities, anxiety, depression, stimulant use, and ADHD, which may make the brain more vulnerable to executive functioning problems.
Dr. Hellmuth noted that the study wasn’t powered to determine whether any individual risk factor was associated with risk of cognitive changes.
As there are no published neuropsychological testing criteria for cognitive PASC, the researchers applied the equivalent criteria for HIV-associated neurocognitive disorder (HAND), a similar, virally associated cognitive disorder. Only 59% of those with cognitive PASC met equivalent HAND criteria for objective cognitive impairment versus 70% of cognitive controls. This, the investigators noted, highlights “the challenges and incongruities of using subjective, versus objective cognitive assessments for diagnosis.”
Is self-report enough?
While there is currently “nothing objective doctors can hang their hats on to say ‘you do’ or ‘you don’t’ have cognitive changes related to COVID,” using the HAND criteria is “not particularly helpful,” said Dr. Hellmuth. “Comparing an individual to a population-based norm in this case is really nuanced, and we shouldn’t rely on this solely to determine whether they do, or don’t, have cognitive changes.”
Perhaps self-reports in this case are “enough” said Dr. Hellmuth. “People know their brains better than anyone else, better than any doctor will.”
A total of 13 in the cognitive PASC group and 4 in the control group consented to a lumbar puncture. Cognitive PASC participants were older than controls (median of 47 vs. 28 years; P = .03) with no other between-group differences.
Overall, 77% of participants with cognitive PASC had a CSF abnormality, compared with 0% of cognitive controls (P = .01). CSF abnormalities included elevated protein levels with no other explainable cause in 2 of the 13 subjects with PASC, which Dr. Hellmuth said is typically a marker of inflammation.
Researchers also noted abnormal oligoclonal banding, a collection of antibodies, in the blood or brain fluid. These were identified in 69% of participants with cognitive PASC, compared with 0% of cognitive controls (P = .03).
“When we find this pattern in both blood and brain, it suggests a systemic inflammatory disorder,” although “we have no idea what these antibodies are targeting,” said Dr. Hellmuth.
The study represents “the very beginning stages” of PASC becoming a medical diagnosis “where doctors know what to call it, how to treat it, and how to do blood and cerebrospinal fluid tests to diagnose it,” said Dr. Hellmuth.
She hopes PASC will receive medical legitimacy just as TBI has. In years past, a player was hit on the head or had their “bell rung,” simply returned to the field. “Now that we understand the science, we call it a mild TBI or concussion, and we have a very different medical approach to it.”
A limitation of the study was the small sample size, which may hinder the results’ validity. In addition, the study demographics may not reflect the broader population of those impacted by PASC.
‘A first substantial step’
Commenting on the research, William Schaffner, MD, professor, division of infectious diseases, Vanderbilt University Medical Center, Nashville, Tenn., said the new results represent “a first substantial step on the road to trying to find out what’s going on” with COVID patients dealing with cognitive issues.
Dr. Schaffner noted that elevated protein levels, identified in some study subjects, “is usually a consequence of previous inflammation” and is “a very interesting” finding. “In people who are otherwise normal, if you do a lumbar puncture, you don’t find elevated proteins.”
However, he noted the “diversity of results” from CSF examinations. “A single pattern does not leap out.”
What the researchers are observing “is not just a phenomenon of the mind or just something psychological,” said Dr. Schaffner. “Something physical is going on here.”
The study was funded by grants from the National Institute of Mental Health and the National Institute of Neurological Disorders and Stroke. Dr. Hellmuth received grant support from the National Institutes of Health/NIMH supporting this work and personal fees for medical-legal consultation outside of the submitted work. Dr. Schaffner has disclosed not relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF CLINICAL AND TRANSLATIONAL NEUROLOGY