User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
First possible case of deer-to-human COVID transmission identified
according a new preprint study that hasn’t yet been peer-reviewed.
Typically, humans spread the virus to deer, and then deer spread it to other deer. But new evidence suggests that the virus could spill over from deer into humans. The researchers identified a COVID-19 case in someone from Ontario who had recently been in contact with deer.
“This particular case, while raising a red flag, doesn’t seem to be hugely alarming,” Finlay Maguire, PhD, one of the study authors and an epidemiologist at Dalhousie University, told CBC News.
“While we haven’t seen [transmission from deer to humans] happen directly, we sampled from the human case around the same time we sampled from the deer, and we sampled from around the same location,” he said. “There is also a plausible link by which it could have happened, in that the individual involved is known to have had considerable contact with deer.”
Dr. Maguire and colleagues have been monitoring the spread of the coronavirus among animals. They analyzed nasal swabs and lymph node samples taken from hundreds of deer that were killed by hunters in fall 2021 in southwestern and eastern Ontario. Among 298 sampled deer, 17 tested positive -- all from southwestern Ontario.
During the analysis, they found a “highly divergent” coronavirus lineage, which means a cluster of samples with many mutations. Around the same time, they found a genetically similar version in a person from the same region.
The study points to the need for better surveillance of the coronavirus, Dr. Maguire told CBC News, including in humans, animals, plants, and the broader environment. Researchers aren’t quite sure how deer contract the virus from humans, but it could happen through contaminated water, direct contact, food, farming, or other animals such as mink.
The coronavirus lineage identified in the study is different from what’s circulating among humans now, and it’s not related to the Delta or Omicron variants. The closest genetic relative came from samples taken from humans and mink in Michigan in 2020, which means the divergent lineage mutated and evolved over time.
“It’s reassuring that we found no evidence of further transmission, during a time when we were doing a lot of sampling and a lot of sequencing,” Samira Mubareka, MD, one of the study authors and a virologist at Sunnybrook Health Sciences Centre, told CBC News.
“If we continue to do this surveillance, we’ll get a much better sense of what the actual risk is,” she said.
So far, the coronavirus has been found in wild white-tailed deer in the northeastern United States and central Canadian provinces.
Other known cases of transmission from animals to humans have been identified in farmed mink and potentially hamsters, the news outlet reported. But for the most part, humans transmit the virus to animals and are most likely to catch the virus from other people.
At the same time, the Public Health Agency of Canada has issued guidance for hunters, trappers, and those who handle wild deer. People should wear gloves, goggles, and a mask when they could be exposed to respiratory tissues and fluids, especially indoors.
Coronaviruses are killed by normal cooking temperatures, the agency said, and there has been no evidence that cooked venison can spread the virus.
A version of this article first appeared on WebMD.com.
according a new preprint study that hasn’t yet been peer-reviewed.
Typically, humans spread the virus to deer, and then deer spread it to other deer. But new evidence suggests that the virus could spill over from deer into humans. The researchers identified a COVID-19 case in someone from Ontario who had recently been in contact with deer.
“This particular case, while raising a red flag, doesn’t seem to be hugely alarming,” Finlay Maguire, PhD, one of the study authors and an epidemiologist at Dalhousie University, told CBC News.
“While we haven’t seen [transmission from deer to humans] happen directly, we sampled from the human case around the same time we sampled from the deer, and we sampled from around the same location,” he said. “There is also a plausible link by which it could have happened, in that the individual involved is known to have had considerable contact with deer.”
Dr. Maguire and colleagues have been monitoring the spread of the coronavirus among animals. They analyzed nasal swabs and lymph node samples taken from hundreds of deer that were killed by hunters in fall 2021 in southwestern and eastern Ontario. Among 298 sampled deer, 17 tested positive -- all from southwestern Ontario.
During the analysis, they found a “highly divergent” coronavirus lineage, which means a cluster of samples with many mutations. Around the same time, they found a genetically similar version in a person from the same region.
The study points to the need for better surveillance of the coronavirus, Dr. Maguire told CBC News, including in humans, animals, plants, and the broader environment. Researchers aren’t quite sure how deer contract the virus from humans, but it could happen through contaminated water, direct contact, food, farming, or other animals such as mink.
The coronavirus lineage identified in the study is different from what’s circulating among humans now, and it’s not related to the Delta or Omicron variants. The closest genetic relative came from samples taken from humans and mink in Michigan in 2020, which means the divergent lineage mutated and evolved over time.
“It’s reassuring that we found no evidence of further transmission, during a time when we were doing a lot of sampling and a lot of sequencing,” Samira Mubareka, MD, one of the study authors and a virologist at Sunnybrook Health Sciences Centre, told CBC News.
“If we continue to do this surveillance, we’ll get a much better sense of what the actual risk is,” she said.
So far, the coronavirus has been found in wild white-tailed deer in the northeastern United States and central Canadian provinces.
Other known cases of transmission from animals to humans have been identified in farmed mink and potentially hamsters, the news outlet reported. But for the most part, humans transmit the virus to animals and are most likely to catch the virus from other people.
At the same time, the Public Health Agency of Canada has issued guidance for hunters, trappers, and those who handle wild deer. People should wear gloves, goggles, and a mask when they could be exposed to respiratory tissues and fluids, especially indoors.
Coronaviruses are killed by normal cooking temperatures, the agency said, and there has been no evidence that cooked venison can spread the virus.
A version of this article first appeared on WebMD.com.
according a new preprint study that hasn’t yet been peer-reviewed.
Typically, humans spread the virus to deer, and then deer spread it to other deer. But new evidence suggests that the virus could spill over from deer into humans. The researchers identified a COVID-19 case in someone from Ontario who had recently been in contact with deer.
“This particular case, while raising a red flag, doesn’t seem to be hugely alarming,” Finlay Maguire, PhD, one of the study authors and an epidemiologist at Dalhousie University, told CBC News.
“While we haven’t seen [transmission from deer to humans] happen directly, we sampled from the human case around the same time we sampled from the deer, and we sampled from around the same location,” he said. “There is also a plausible link by which it could have happened, in that the individual involved is known to have had considerable contact with deer.”
Dr. Maguire and colleagues have been monitoring the spread of the coronavirus among animals. They analyzed nasal swabs and lymph node samples taken from hundreds of deer that were killed by hunters in fall 2021 in southwestern and eastern Ontario. Among 298 sampled deer, 17 tested positive -- all from southwestern Ontario.
During the analysis, they found a “highly divergent” coronavirus lineage, which means a cluster of samples with many mutations. Around the same time, they found a genetically similar version in a person from the same region.
The study points to the need for better surveillance of the coronavirus, Dr. Maguire told CBC News, including in humans, animals, plants, and the broader environment. Researchers aren’t quite sure how deer contract the virus from humans, but it could happen through contaminated water, direct contact, food, farming, or other animals such as mink.
The coronavirus lineage identified in the study is different from what’s circulating among humans now, and it’s not related to the Delta or Omicron variants. The closest genetic relative came from samples taken from humans and mink in Michigan in 2020, which means the divergent lineage mutated and evolved over time.
“It’s reassuring that we found no evidence of further transmission, during a time when we were doing a lot of sampling and a lot of sequencing,” Samira Mubareka, MD, one of the study authors and a virologist at Sunnybrook Health Sciences Centre, told CBC News.
“If we continue to do this surveillance, we’ll get a much better sense of what the actual risk is,” she said.
So far, the coronavirus has been found in wild white-tailed deer in the northeastern United States and central Canadian provinces.
Other known cases of transmission from animals to humans have been identified in farmed mink and potentially hamsters, the news outlet reported. But for the most part, humans transmit the virus to animals and are most likely to catch the virus from other people.
At the same time, the Public Health Agency of Canada has issued guidance for hunters, trappers, and those who handle wild deer. People should wear gloves, goggles, and a mask when they could be exposed to respiratory tissues and fluids, especially indoors.
Coronaviruses are killed by normal cooking temperatures, the agency said, and there has been no evidence that cooked venison can spread the virus.
A version of this article first appeared on WebMD.com.
EMA recommends PreHevbri hepatitis B vaccine for approval
The European Medicines Agency’s (EMA’s) human medicines committee has recommended approval of a hepatitis B vaccine for adults.
The agency’s Committee for Medicinal Products for Human Use (CHMP) granted a positive opinion for PreHevbri on Feb. 24 for active immunization against hepatitis B virus (HBV) infection. PreHevbri (PreHevBrio in the United States and Sci-B-Vac in Israel) received approval from the Food and Drug Administration on Nov. 30, 2021. The vaccine is produced by VBI Vaccines (Delaware) Inc., based in Cambridge, Mass.
The World Health Organization estimates that more than 290 million people globally are infected with HBV. HBV is the leading cause of liver disease, and an estimated 900,000 people die every year from complications from chronic HBV infection, according to a VBI Vaccine press release. A 2019 report from the European Centre for Disease Prevention and Control found that adults in the European Union aged 35-44 had the highest rates of acute infections with HBV, and people aged 25-34 had the highest rate of chronic HBV infections. Vaccination programs are key interventions in preventing transmission of the virus, the report noted.
PreHevbri is a hepatitis B vaccine composed of three surface antigens of the hepatitis B virus. The vaccine is administered via injection in three doses on a 0-, 1-, and 6-month schedule and is indicated for use in adults aged 18 years and older.
The CHMP recommendation was based on data from a safety and immunogenicity study, which included 1,607 participants aged 18 and older, and a lot-to-lot study, which included 2,838 adults aged 18-45, according the VBI vaccine press release.
The recommendation will now be reviewed by the European Commission. If approved, PreHevbri will be the only three-antigen HBV vaccine for adults approved in the European Union.
A version of this article first appeared on Medscape.com.
The European Medicines Agency’s (EMA’s) human medicines committee has recommended approval of a hepatitis B vaccine for adults.
The agency’s Committee for Medicinal Products for Human Use (CHMP) granted a positive opinion for PreHevbri on Feb. 24 for active immunization against hepatitis B virus (HBV) infection. PreHevbri (PreHevBrio in the United States and Sci-B-Vac in Israel) received approval from the Food and Drug Administration on Nov. 30, 2021. The vaccine is produced by VBI Vaccines (Delaware) Inc., based in Cambridge, Mass.
The World Health Organization estimates that more than 290 million people globally are infected with HBV. HBV is the leading cause of liver disease, and an estimated 900,000 people die every year from complications from chronic HBV infection, according to a VBI Vaccine press release. A 2019 report from the European Centre for Disease Prevention and Control found that adults in the European Union aged 35-44 had the highest rates of acute infections with HBV, and people aged 25-34 had the highest rate of chronic HBV infections. Vaccination programs are key interventions in preventing transmission of the virus, the report noted.
PreHevbri is a hepatitis B vaccine composed of three surface antigens of the hepatitis B virus. The vaccine is administered via injection in three doses on a 0-, 1-, and 6-month schedule and is indicated for use in adults aged 18 years and older.
The CHMP recommendation was based on data from a safety and immunogenicity study, which included 1,607 participants aged 18 and older, and a lot-to-lot study, which included 2,838 adults aged 18-45, according the VBI vaccine press release.
The recommendation will now be reviewed by the European Commission. If approved, PreHevbri will be the only three-antigen HBV vaccine for adults approved in the European Union.
A version of this article first appeared on Medscape.com.
The European Medicines Agency’s (EMA’s) human medicines committee has recommended approval of a hepatitis B vaccine for adults.
The agency’s Committee for Medicinal Products for Human Use (CHMP) granted a positive opinion for PreHevbri on Feb. 24 for active immunization against hepatitis B virus (HBV) infection. PreHevbri (PreHevBrio in the United States and Sci-B-Vac in Israel) received approval from the Food and Drug Administration on Nov. 30, 2021. The vaccine is produced by VBI Vaccines (Delaware) Inc., based in Cambridge, Mass.
The World Health Organization estimates that more than 290 million people globally are infected with HBV. HBV is the leading cause of liver disease, and an estimated 900,000 people die every year from complications from chronic HBV infection, according to a VBI Vaccine press release. A 2019 report from the European Centre for Disease Prevention and Control found that adults in the European Union aged 35-44 had the highest rates of acute infections with HBV, and people aged 25-34 had the highest rate of chronic HBV infections. Vaccination programs are key interventions in preventing transmission of the virus, the report noted.
PreHevbri is a hepatitis B vaccine composed of three surface antigens of the hepatitis B virus. The vaccine is administered via injection in three doses on a 0-, 1-, and 6-month schedule and is indicated for use in adults aged 18 years and older.
The CHMP recommendation was based on data from a safety and immunogenicity study, which included 1,607 participants aged 18 and older, and a lot-to-lot study, which included 2,838 adults aged 18-45, according the VBI vaccine press release.
The recommendation will now be reviewed by the European Commission. If approved, PreHevbri will be the only three-antigen HBV vaccine for adults approved in the European Union.
A version of this article first appeared on Medscape.com.
Evidence mounts for paramagnetic rim lesions in diagnosing MS
WEST PALM BEACH, FLA. – , new research suggests.
Results from two studies add to the mounting evidence underscoring the importance of the imaging features, researchers noted. “Our data suggest that the presence and number of iron rim lesions hold a prognostic value for long-term disability in MS, especially the presence of four or more rim lesions,” said Amjad I. AlTokhis, School of Medicine, University of Nottingham, United Kingdom, and Division of Clinical Neuroscience, Nottingham University Hospitals NHS Trust, who was the lead author of both studies.
Importantly, the effect of the rim lesions on disability was greater than that of established prognostic biomarkers of T2 white matter lesion count and volume, she noted.
“This could support the use of iron rim lesions as an imaging biomarker for disease severity and worse prognosis,” said Dr. AlTokhis. “These findings also support that iron rim lesions might be clinically useful not only diagnostically but also for disease progression and predicting future disability in MS,” she added.
The findings were presented at the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS) Forum 2022.
Sign of aggressive disease?
Dozens of studies have linked rim lesions, which are also known as iron rim lesions because of their composition of iron-laden macrophages/microglia, to more severe disease course in MS, as well as to having potential as an important imaging biomarker for diagnosis. However, studies have often been limited to smaller longitudinal cohorts.
In the first study, Dr. AlTokhis and colleagues enrolled 91 patients with MS (56 women) between 2008 and 2013 for whom 7 Tesla (7T) MRI was available with SWI-filtered phase sequencing.
At baseline, among 42 patients with clinically isolated syndrome, 50% had one or more of the rim lesions. The corresponding rates were 38% among 34 patients with relapsing-remitting MS, 38% among 18 patients with primary-progressive MS, and as high as 71% among 17 patients with secondary-progressive MS (P < .05 vs. primary progressive MS and clinically isolated syndrome).
At a median follow-up of 9 years, 18 of the patients with clinically isolated syndrome and relapsing-remitting MS progressed to secondary progressive MS; and among them, 56% had at least one rim lesion.
Of 24 who did not progress to secondary progressive MS, only 33% had at least one rim lesion.
The median baseline level of disease severity in the entire cohort, as measured by Age-Related Multiple Sclerosis Score (ARMSS), was 5.4. However, the median score among patients with rim lesions was higher, compared with those without the lesions (ARMSS, 6.7 vs. 5.0).
After the median 9-year follow-up, disease severity remained higher among those with versus those without the lesions (ARMSS, 7.3 vs. 6.3).
Patients with rim lesions had more white matter lesions overall; and a further analysis surprisingly showed that the number of rim lesions was indeed associated with long-term disability (P = .005).
“Detecting four or more iron rim lesions could be a sign of more aggressive disease and disability – thus, possibly useful in earlier treatment and a potential target for therapies,” Dr. AlTokhis said.
“Also, for clinical practicality, [the number of] iron rim lesions had the most direct effect on disability compared to white matter lesion count and volume, supporting its role as an independent prognostic imaging biomarker,” she added.
Dr. AlTokhis noted that “detecting and counting rim lesions is much easier than assessing all white matter lesions, adding to the clinical utility of this sign.”
Diagnostic value
The second study, presented at the meeting by coinvestigator Brian Renner, MD, Department of Neurology at Cedars Sinai, Los Angeles, reported on the significance of the rim lesions in MS diagnosis. It included 95 patients who had presented for new evaluation on suspicion of MS at 10 centers in the North American Imaging in MS Cooperative (NAIMS).
Of these participants, 44 (46%) were positively diagnosed according to McDonald 2017 criteria (MC2017) for MS, while 37 (39%) were given an alternative diagnosis to MS. Fourteen were considered at risk for MS with diagnoses of clinically isolating syndrome or radiologically isolating syndrome.
Overall, among the 44 with an MS diagnosis, 34 had one or more rim lesions; among the 51 who did not meet an MS diagnosis, only six had one or more of the rim lesions. One or more rim lesions were further observed in three patients with radiologically isolating syndrome and one patient with clinically isolating syndrome.
Among those with one or more of the rim lesions, a diagnosis of MS with MC2017 MS criteria was identified with a high sensitivity of 80%, high specificity of 88%, accuracy of 84%, and an AUC of 81%.
“We’ve shown that paramagnetic rim lesions are highly specific for MS, and the sensitivity of rim lesions for MS is higher than previously reported, despite similar techniques in rating, processing, and evaluation – which was likely related to the nature of the cohort,” Dr. Renner said.
Promising data
During the NAIMS symposium, Christopher C. Hemond, MD, assistant professor or neurology at the University of Massachusetts Medical School, Worcester, noted to meeting attendees that the rim lesions were seen across the entire course of the MS disease spectrum, spanning from radiologically isolating syndrome to secondary progressive MS.
“We know paramagnetic rim lesions are visible at all disease stages. They are uniquely larger and more destructive than their rimless peers and are associated with stronger disease severity,” said Dr. Hemond, who was not involved with the research.
“There is promising data at this point suggesting that [the rim lesions] may represent a biomarker predictive of future disability accumulation,” he added.
Dr. Hemond noted that, unlike in Dr. Renner’s study, the bulk of previous studies have indicated that rim lesions “are associated with a high specificity but only modest sensitivity, in the mid-50% range, for the diagnosis of MS in comparison to some conditions that mimic MS.”
Commenting on the findings, Dr. Hemond noted the results from Dr. Renner’s ongoing study “are critical in building confidence in the translational use of this biomarker to assist in ruling in a diagnosis of MS,” while Dr. AlTokis’ study “adds to and is consistent with the growing literature of pathological associations of paramagnetic rim lesions in MS.”
Dr. Hemond added that the NAIMS cooperative plans to publish guidance in the area in the coming months.
“Although paramagnetic rim lesions have strong pathological associations in MS, it remains unclear if the presence of these lesions should change MS clinical management at the present time,” he said.
During the NAIMS session, Francesca Bagnato, MD, PhD, Vanderbilt University Medical Center, Nashville, Tenn., noted the growing importance of the role of rim lesions in clinical research. “It is clear that these paramagnetic rim lesions are going to be the new biomarker for the next generation of clinical trials,” she said.
Dr. Renner’s study received funding from the Race to Erase MS Foundation. Dr. AlTokhis, Dr. Renner, and Dr. Hemond have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WEST PALM BEACH, FLA. – , new research suggests.
Results from two studies add to the mounting evidence underscoring the importance of the imaging features, researchers noted. “Our data suggest that the presence and number of iron rim lesions hold a prognostic value for long-term disability in MS, especially the presence of four or more rim lesions,” said Amjad I. AlTokhis, School of Medicine, University of Nottingham, United Kingdom, and Division of Clinical Neuroscience, Nottingham University Hospitals NHS Trust, who was the lead author of both studies.
Importantly, the effect of the rim lesions on disability was greater than that of established prognostic biomarkers of T2 white matter lesion count and volume, she noted.
“This could support the use of iron rim lesions as an imaging biomarker for disease severity and worse prognosis,” said Dr. AlTokhis. “These findings also support that iron rim lesions might be clinically useful not only diagnostically but also for disease progression and predicting future disability in MS,” she added.
The findings were presented at the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS) Forum 2022.
Sign of aggressive disease?
Dozens of studies have linked rim lesions, which are also known as iron rim lesions because of their composition of iron-laden macrophages/microglia, to more severe disease course in MS, as well as to having potential as an important imaging biomarker for diagnosis. However, studies have often been limited to smaller longitudinal cohorts.
In the first study, Dr. AlTokhis and colleagues enrolled 91 patients with MS (56 women) between 2008 and 2013 for whom 7 Tesla (7T) MRI was available with SWI-filtered phase sequencing.
At baseline, among 42 patients with clinically isolated syndrome, 50% had one or more of the rim lesions. The corresponding rates were 38% among 34 patients with relapsing-remitting MS, 38% among 18 patients with primary-progressive MS, and as high as 71% among 17 patients with secondary-progressive MS (P < .05 vs. primary progressive MS and clinically isolated syndrome).
At a median follow-up of 9 years, 18 of the patients with clinically isolated syndrome and relapsing-remitting MS progressed to secondary progressive MS; and among them, 56% had at least one rim lesion.
Of 24 who did not progress to secondary progressive MS, only 33% had at least one rim lesion.
The median baseline level of disease severity in the entire cohort, as measured by Age-Related Multiple Sclerosis Score (ARMSS), was 5.4. However, the median score among patients with rim lesions was higher, compared with those without the lesions (ARMSS, 6.7 vs. 5.0).
After the median 9-year follow-up, disease severity remained higher among those with versus those without the lesions (ARMSS, 7.3 vs. 6.3).
Patients with rim lesions had more white matter lesions overall; and a further analysis surprisingly showed that the number of rim lesions was indeed associated with long-term disability (P = .005).
“Detecting four or more iron rim lesions could be a sign of more aggressive disease and disability – thus, possibly useful in earlier treatment and a potential target for therapies,” Dr. AlTokhis said.
“Also, for clinical practicality, [the number of] iron rim lesions had the most direct effect on disability compared to white matter lesion count and volume, supporting its role as an independent prognostic imaging biomarker,” she added.
Dr. AlTokhis noted that “detecting and counting rim lesions is much easier than assessing all white matter lesions, adding to the clinical utility of this sign.”
Diagnostic value
The second study, presented at the meeting by coinvestigator Brian Renner, MD, Department of Neurology at Cedars Sinai, Los Angeles, reported on the significance of the rim lesions in MS diagnosis. It included 95 patients who had presented for new evaluation on suspicion of MS at 10 centers in the North American Imaging in MS Cooperative (NAIMS).
Of these participants, 44 (46%) were positively diagnosed according to McDonald 2017 criteria (MC2017) for MS, while 37 (39%) were given an alternative diagnosis to MS. Fourteen were considered at risk for MS with diagnoses of clinically isolating syndrome or radiologically isolating syndrome.
Overall, among the 44 with an MS diagnosis, 34 had one or more rim lesions; among the 51 who did not meet an MS diagnosis, only six had one or more of the rim lesions. One or more rim lesions were further observed in three patients with radiologically isolating syndrome and one patient with clinically isolating syndrome.
Among those with one or more of the rim lesions, a diagnosis of MS with MC2017 MS criteria was identified with a high sensitivity of 80%, high specificity of 88%, accuracy of 84%, and an AUC of 81%.
“We’ve shown that paramagnetic rim lesions are highly specific for MS, and the sensitivity of rim lesions for MS is higher than previously reported, despite similar techniques in rating, processing, and evaluation – which was likely related to the nature of the cohort,” Dr. Renner said.
Promising data
During the NAIMS symposium, Christopher C. Hemond, MD, assistant professor or neurology at the University of Massachusetts Medical School, Worcester, noted to meeting attendees that the rim lesions were seen across the entire course of the MS disease spectrum, spanning from radiologically isolating syndrome to secondary progressive MS.
“We know paramagnetic rim lesions are visible at all disease stages. They are uniquely larger and more destructive than their rimless peers and are associated with stronger disease severity,” said Dr. Hemond, who was not involved with the research.
“There is promising data at this point suggesting that [the rim lesions] may represent a biomarker predictive of future disability accumulation,” he added.
Dr. Hemond noted that, unlike in Dr. Renner’s study, the bulk of previous studies have indicated that rim lesions “are associated with a high specificity but only modest sensitivity, in the mid-50% range, for the diagnosis of MS in comparison to some conditions that mimic MS.”
Commenting on the findings, Dr. Hemond noted the results from Dr. Renner’s ongoing study “are critical in building confidence in the translational use of this biomarker to assist in ruling in a diagnosis of MS,” while Dr. AlTokis’ study “adds to and is consistent with the growing literature of pathological associations of paramagnetic rim lesions in MS.”
Dr. Hemond added that the NAIMS cooperative plans to publish guidance in the area in the coming months.
“Although paramagnetic rim lesions have strong pathological associations in MS, it remains unclear if the presence of these lesions should change MS clinical management at the present time,” he said.
During the NAIMS session, Francesca Bagnato, MD, PhD, Vanderbilt University Medical Center, Nashville, Tenn., noted the growing importance of the role of rim lesions in clinical research. “It is clear that these paramagnetic rim lesions are going to be the new biomarker for the next generation of clinical trials,” she said.
Dr. Renner’s study received funding from the Race to Erase MS Foundation. Dr. AlTokhis, Dr. Renner, and Dr. Hemond have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WEST PALM BEACH, FLA. – , new research suggests.
Results from two studies add to the mounting evidence underscoring the importance of the imaging features, researchers noted. “Our data suggest that the presence and number of iron rim lesions hold a prognostic value for long-term disability in MS, especially the presence of four or more rim lesions,” said Amjad I. AlTokhis, School of Medicine, University of Nottingham, United Kingdom, and Division of Clinical Neuroscience, Nottingham University Hospitals NHS Trust, who was the lead author of both studies.
Importantly, the effect of the rim lesions on disability was greater than that of established prognostic biomarkers of T2 white matter lesion count and volume, she noted.
“This could support the use of iron rim lesions as an imaging biomarker for disease severity and worse prognosis,” said Dr. AlTokhis. “These findings also support that iron rim lesions might be clinically useful not only diagnostically but also for disease progression and predicting future disability in MS,” she added.
The findings were presented at the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS) Forum 2022.
Sign of aggressive disease?
Dozens of studies have linked rim lesions, which are also known as iron rim lesions because of their composition of iron-laden macrophages/microglia, to more severe disease course in MS, as well as to having potential as an important imaging biomarker for diagnosis. However, studies have often been limited to smaller longitudinal cohorts.
In the first study, Dr. AlTokhis and colleagues enrolled 91 patients with MS (56 women) between 2008 and 2013 for whom 7 Tesla (7T) MRI was available with SWI-filtered phase sequencing.
At baseline, among 42 patients with clinically isolated syndrome, 50% had one or more of the rim lesions. The corresponding rates were 38% among 34 patients with relapsing-remitting MS, 38% among 18 patients with primary-progressive MS, and as high as 71% among 17 patients with secondary-progressive MS (P < .05 vs. primary progressive MS and clinically isolated syndrome).
At a median follow-up of 9 years, 18 of the patients with clinically isolated syndrome and relapsing-remitting MS progressed to secondary progressive MS; and among them, 56% had at least one rim lesion.
Of 24 who did not progress to secondary progressive MS, only 33% had at least one rim lesion.
The median baseline level of disease severity in the entire cohort, as measured by Age-Related Multiple Sclerosis Score (ARMSS), was 5.4. However, the median score among patients with rim lesions was higher, compared with those without the lesions (ARMSS, 6.7 vs. 5.0).
After the median 9-year follow-up, disease severity remained higher among those with versus those without the lesions (ARMSS, 7.3 vs. 6.3).
Patients with rim lesions had more white matter lesions overall; and a further analysis surprisingly showed that the number of rim lesions was indeed associated with long-term disability (P = .005).
“Detecting four or more iron rim lesions could be a sign of more aggressive disease and disability – thus, possibly useful in earlier treatment and a potential target for therapies,” Dr. AlTokhis said.
“Also, for clinical practicality, [the number of] iron rim lesions had the most direct effect on disability compared to white matter lesion count and volume, supporting its role as an independent prognostic imaging biomarker,” she added.
Dr. AlTokhis noted that “detecting and counting rim lesions is much easier than assessing all white matter lesions, adding to the clinical utility of this sign.”
Diagnostic value
The second study, presented at the meeting by coinvestigator Brian Renner, MD, Department of Neurology at Cedars Sinai, Los Angeles, reported on the significance of the rim lesions in MS diagnosis. It included 95 patients who had presented for new evaluation on suspicion of MS at 10 centers in the North American Imaging in MS Cooperative (NAIMS).
Of these participants, 44 (46%) were positively diagnosed according to McDonald 2017 criteria (MC2017) for MS, while 37 (39%) were given an alternative diagnosis to MS. Fourteen were considered at risk for MS with diagnoses of clinically isolating syndrome or radiologically isolating syndrome.
Overall, among the 44 with an MS diagnosis, 34 had one or more rim lesions; among the 51 who did not meet an MS diagnosis, only six had one or more of the rim lesions. One or more rim lesions were further observed in three patients with radiologically isolating syndrome and one patient with clinically isolating syndrome.
Among those with one or more of the rim lesions, a diagnosis of MS with MC2017 MS criteria was identified with a high sensitivity of 80%, high specificity of 88%, accuracy of 84%, and an AUC of 81%.
“We’ve shown that paramagnetic rim lesions are highly specific for MS, and the sensitivity of rim lesions for MS is higher than previously reported, despite similar techniques in rating, processing, and evaluation – which was likely related to the nature of the cohort,” Dr. Renner said.
Promising data
During the NAIMS symposium, Christopher C. Hemond, MD, assistant professor or neurology at the University of Massachusetts Medical School, Worcester, noted to meeting attendees that the rim lesions were seen across the entire course of the MS disease spectrum, spanning from radiologically isolating syndrome to secondary progressive MS.
“We know paramagnetic rim lesions are visible at all disease stages. They are uniquely larger and more destructive than their rimless peers and are associated with stronger disease severity,” said Dr. Hemond, who was not involved with the research.
“There is promising data at this point suggesting that [the rim lesions] may represent a biomarker predictive of future disability accumulation,” he added.
Dr. Hemond noted that, unlike in Dr. Renner’s study, the bulk of previous studies have indicated that rim lesions “are associated with a high specificity but only modest sensitivity, in the mid-50% range, for the diagnosis of MS in comparison to some conditions that mimic MS.”
Commenting on the findings, Dr. Hemond noted the results from Dr. Renner’s ongoing study “are critical in building confidence in the translational use of this biomarker to assist in ruling in a diagnosis of MS,” while Dr. AlTokis’ study “adds to and is consistent with the growing literature of pathological associations of paramagnetic rim lesions in MS.”
Dr. Hemond added that the NAIMS cooperative plans to publish guidance in the area in the coming months.
“Although paramagnetic rim lesions have strong pathological associations in MS, it remains unclear if the presence of these lesions should change MS clinical management at the present time,” he said.
During the NAIMS session, Francesca Bagnato, MD, PhD, Vanderbilt University Medical Center, Nashville, Tenn., noted the growing importance of the role of rim lesions in clinical research. “It is clear that these paramagnetic rim lesions are going to be the new biomarker for the next generation of clinical trials,” she said.
Dr. Renner’s study received funding from the Race to Erase MS Foundation. Dr. AlTokhis, Dr. Renner, and Dr. Hemond have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
REPORTING FROM ACTRIMS FORUM 2022
Should all women be routinely screened for lung cancer?
especially those with a history of breast cancer, according to a new study published in BJS Open.
The 2021 screening guidelines include adults aged between 50 and 80 years who have a 20–pack-year smoking history and currently smoke or have quit within the past 15 years, but the guidelines do not include nonsmokers or patients with a history of previous malignancies, such as breast cancer.
Led by Daniela Molena, MD, a thoracic surgeon and director of esophageal surgery at Memorial Sloan Kettering Cancer Center, New York, researchers conducted an analysis of 2,192 women with first-time lung cancer who underwent lung resections at Memorial Sloan Kettering between January 2000 and December 2017. The study’s objective was to determine stage at diagnosis, survival, and eligibility for lung cancer screening among patients with lung cancer who had a previous breast cancer diagnosis and those who did not have a history of breast cancer.
Only 331 (15.1%) patients were previously diagnosed with breast cancer, which was not statistically significant. “Overall, there were no statistically significant differences in genomic or oncogenic pathway alterations between the two groups, which suggests that lung cancer in patients who previously had breast cancer may not be affected at the genomic level by the previous breast cancer,” the authors wrote.
However, at 58.4%, more than half of patients in the study (1,281 patients) were prior smokers and only 33.3% met the USPSTF criteria for lung cancer screening, which the authors said was concerning.
“The most important finding of the study was that a high percentage of women with lung cancer, regardless of breast cancer history, did not meet the current USPSTF criteria for lung cancer screening. This is very important given the observation that nearly half of the women included in the study did not have a history of smoking. As such, the role of imaging for other causes, such as cancer surveillance, becomes especially important for early cancer diagnosis,” Dr. Molena and colleagues wrote. “To reduce late-stage cancer diagnoses, further assessment of guidelines for lung cancer screening for all women may be needed.”
Instead, for almost half of women in the study group with a history of breast cancer, the lung cancer was detected on a routine follow-up imaging scan.
USPSTF guidelines for lung cancer screening do not include previous malignancy as a high-risk feature requiring evaluation, which may explain why so few women in this study were screened for lung cancer, even though lung cancer is more common in breast cancer survivors than the general population. Approximately 10% of women who have had breast cancer will develop a second malignancy within 10 years and in most cases, it will be lung cancer. Plus, according to the National Cancer Institute, breast, lung, and colorectal cancers are the three most common cancers in women and account for approximately 50% of all new cancer diagnoses in women in 2020.
A 2018 analysis published in Frontiers in Oncology found that, of more than 6,000 women with secondary primary lung cancer after having had breast cancer, 42% had distant-stage disease at the time of diagnosis which, Dr. Molena and colleagues said, suggests an ongoing need to update screening recommendations.
“Given that lung cancer has a 5-year overall survival rate of less than 20% (highlighting the benefits of early-stage diagnosis), a better understanding of lung cancer in women with a history of breast cancer could have important implications for screening and surveillance,” the authors wrote.
Estrogen is known to play a role in the development of lung cancer by activating the epidermal growth factor receptor (EGFR). Previous research has shown an increased risk of lung cancer in patients with estrogen receptor–negative, progesterone receptor–negative, HER2-negative, or triple-negative breast cancer.
“Antiestrogen treatment has been demonstrated to decrease the incidence of lung cancer and has been associated with improved long-term survival in patients with lung cancer after breast cancer. Future studies should seek to identify high-risk populations on the basis of hormone receptor status and antiestrogen therapy use,” the authors wrote.
The authors noted a number of limitations to the study, including the single hospital as the sole source of data, plus, the analysis did not account for the length of time since patients quit smoking and a lung cancer diagnosis. Nor did it consider other risk factors, such as radiation, chemotherapy, or antiestrogen therapies.
The authors did not disclose any study-related conflicts of interests.
This article was updated 3/2/22.
especially those with a history of breast cancer, according to a new study published in BJS Open.
The 2021 screening guidelines include adults aged between 50 and 80 years who have a 20–pack-year smoking history and currently smoke or have quit within the past 15 years, but the guidelines do not include nonsmokers or patients with a history of previous malignancies, such as breast cancer.
Led by Daniela Molena, MD, a thoracic surgeon and director of esophageal surgery at Memorial Sloan Kettering Cancer Center, New York, researchers conducted an analysis of 2,192 women with first-time lung cancer who underwent lung resections at Memorial Sloan Kettering between January 2000 and December 2017. The study’s objective was to determine stage at diagnosis, survival, and eligibility for lung cancer screening among patients with lung cancer who had a previous breast cancer diagnosis and those who did not have a history of breast cancer.
Only 331 (15.1%) patients were previously diagnosed with breast cancer, which was not statistically significant. “Overall, there were no statistically significant differences in genomic or oncogenic pathway alterations between the two groups, which suggests that lung cancer in patients who previously had breast cancer may not be affected at the genomic level by the previous breast cancer,” the authors wrote.
However, at 58.4%, more than half of patients in the study (1,281 patients) were prior smokers and only 33.3% met the USPSTF criteria for lung cancer screening, which the authors said was concerning.
“The most important finding of the study was that a high percentage of women with lung cancer, regardless of breast cancer history, did not meet the current USPSTF criteria for lung cancer screening. This is very important given the observation that nearly half of the women included in the study did not have a history of smoking. As such, the role of imaging for other causes, such as cancer surveillance, becomes especially important for early cancer diagnosis,” Dr. Molena and colleagues wrote. “To reduce late-stage cancer diagnoses, further assessment of guidelines for lung cancer screening for all women may be needed.”
Instead, for almost half of women in the study group with a history of breast cancer, the lung cancer was detected on a routine follow-up imaging scan.
USPSTF guidelines for lung cancer screening do not include previous malignancy as a high-risk feature requiring evaluation, which may explain why so few women in this study were screened for lung cancer, even though lung cancer is more common in breast cancer survivors than the general population. Approximately 10% of women who have had breast cancer will develop a second malignancy within 10 years and in most cases, it will be lung cancer. Plus, according to the National Cancer Institute, breast, lung, and colorectal cancers are the three most common cancers in women and account for approximately 50% of all new cancer diagnoses in women in 2020.
A 2018 analysis published in Frontiers in Oncology found that, of more than 6,000 women with secondary primary lung cancer after having had breast cancer, 42% had distant-stage disease at the time of diagnosis which, Dr. Molena and colleagues said, suggests an ongoing need to update screening recommendations.
“Given that lung cancer has a 5-year overall survival rate of less than 20% (highlighting the benefits of early-stage diagnosis), a better understanding of lung cancer in women with a history of breast cancer could have important implications for screening and surveillance,” the authors wrote.
Estrogen is known to play a role in the development of lung cancer by activating the epidermal growth factor receptor (EGFR). Previous research has shown an increased risk of lung cancer in patients with estrogen receptor–negative, progesterone receptor–negative, HER2-negative, or triple-negative breast cancer.
“Antiestrogen treatment has been demonstrated to decrease the incidence of lung cancer and has been associated with improved long-term survival in patients with lung cancer after breast cancer. Future studies should seek to identify high-risk populations on the basis of hormone receptor status and antiestrogen therapy use,” the authors wrote.
The authors noted a number of limitations to the study, including the single hospital as the sole source of data, plus, the analysis did not account for the length of time since patients quit smoking and a lung cancer diagnosis. Nor did it consider other risk factors, such as radiation, chemotherapy, or antiestrogen therapies.
The authors did not disclose any study-related conflicts of interests.
This article was updated 3/2/22.
especially those with a history of breast cancer, according to a new study published in BJS Open.
The 2021 screening guidelines include adults aged between 50 and 80 years who have a 20–pack-year smoking history and currently smoke or have quit within the past 15 years, but the guidelines do not include nonsmokers or patients with a history of previous malignancies, such as breast cancer.
Led by Daniela Molena, MD, a thoracic surgeon and director of esophageal surgery at Memorial Sloan Kettering Cancer Center, New York, researchers conducted an analysis of 2,192 women with first-time lung cancer who underwent lung resections at Memorial Sloan Kettering between January 2000 and December 2017. The study’s objective was to determine stage at diagnosis, survival, and eligibility for lung cancer screening among patients with lung cancer who had a previous breast cancer diagnosis and those who did not have a history of breast cancer.
Only 331 (15.1%) patients were previously diagnosed with breast cancer, which was not statistically significant. “Overall, there were no statistically significant differences in genomic or oncogenic pathway alterations between the two groups, which suggests that lung cancer in patients who previously had breast cancer may not be affected at the genomic level by the previous breast cancer,” the authors wrote.
However, at 58.4%, more than half of patients in the study (1,281 patients) were prior smokers and only 33.3% met the USPSTF criteria for lung cancer screening, which the authors said was concerning.
“The most important finding of the study was that a high percentage of women with lung cancer, regardless of breast cancer history, did not meet the current USPSTF criteria for lung cancer screening. This is very important given the observation that nearly half of the women included in the study did not have a history of smoking. As such, the role of imaging for other causes, such as cancer surveillance, becomes especially important for early cancer diagnosis,” Dr. Molena and colleagues wrote. “To reduce late-stage cancer diagnoses, further assessment of guidelines for lung cancer screening for all women may be needed.”
Instead, for almost half of women in the study group with a history of breast cancer, the lung cancer was detected on a routine follow-up imaging scan.
USPSTF guidelines for lung cancer screening do not include previous malignancy as a high-risk feature requiring evaluation, which may explain why so few women in this study were screened for lung cancer, even though lung cancer is more common in breast cancer survivors than the general population. Approximately 10% of women who have had breast cancer will develop a second malignancy within 10 years and in most cases, it will be lung cancer. Plus, according to the National Cancer Institute, breast, lung, and colorectal cancers are the three most common cancers in women and account for approximately 50% of all new cancer diagnoses in women in 2020.
A 2018 analysis published in Frontiers in Oncology found that, of more than 6,000 women with secondary primary lung cancer after having had breast cancer, 42% had distant-stage disease at the time of diagnosis which, Dr. Molena and colleagues said, suggests an ongoing need to update screening recommendations.
“Given that lung cancer has a 5-year overall survival rate of less than 20% (highlighting the benefits of early-stage diagnosis), a better understanding of lung cancer in women with a history of breast cancer could have important implications for screening and surveillance,” the authors wrote.
Estrogen is known to play a role in the development of lung cancer by activating the epidermal growth factor receptor (EGFR). Previous research has shown an increased risk of lung cancer in patients with estrogen receptor–negative, progesterone receptor–negative, HER2-negative, or triple-negative breast cancer.
“Antiestrogen treatment has been demonstrated to decrease the incidence of lung cancer and has been associated with improved long-term survival in patients with lung cancer after breast cancer. Future studies should seek to identify high-risk populations on the basis of hormone receptor status and antiestrogen therapy use,” the authors wrote.
The authors noted a number of limitations to the study, including the single hospital as the sole source of data, plus, the analysis did not account for the length of time since patients quit smoking and a lung cancer diagnosis. Nor did it consider other risk factors, such as radiation, chemotherapy, or antiestrogen therapies.
The authors did not disclose any study-related conflicts of interests.
This article was updated 3/2/22.
FROM BJS OPEN
GI involvement may signal risk for MIS-C after COVID
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
Children and COVID: New cases down to pre-Omicron level
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.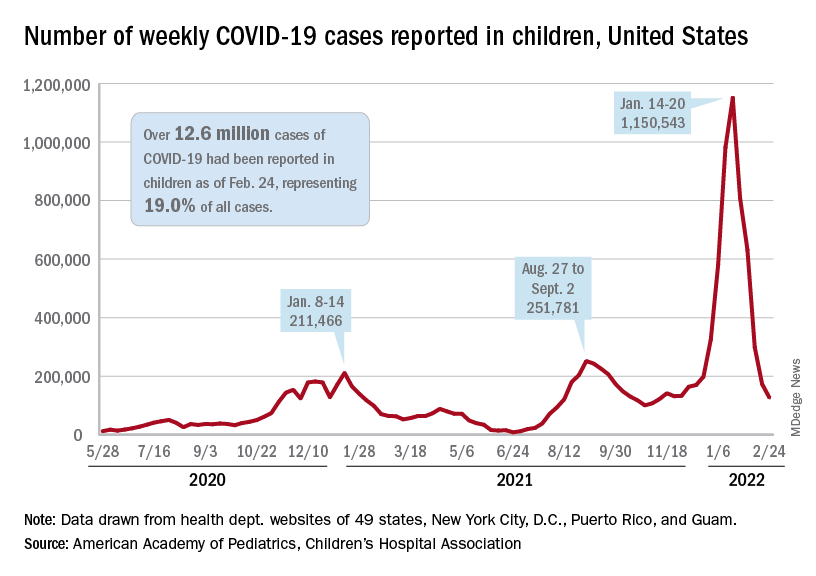
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.
FDA approves first drug for myelofibrosis with thrombocytopenia
Pacritinib (Vonjo, CTI BioPharma) is indicated for use in the treatment of adults with intermediate- or high-risk primary or secondary (post–polycythemia vera or post–essential thrombocythemia) myelofibrosis with a platelet count below 50 × 109/L.
Pacritinib is a novel oral kinase inhibitor with specificity for activity against Janus associated kinase 2 (JAK2) and IRAK1, without inhibiting JAK1. The recommended dosage is 200 mg orally twice daily.
In the United States, there are approximately 21,000 patients with myelofibrosis, notes the manufacturer. About one-third develop severe thrombocytopenia.
“Myelofibrosis with severe thrombocytopenia, defined as blood platelet counts below 50 × 109/L, has been shown to result in poor survival outcomes coupled with debilitating symptoms. Limited treatment options have rendered this disease as an area of urgent unmet medical need,” said John Mascarenhas, MD, associate professor, medicine, hematology, and medical oncology, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York.
“I am pleased to see that a new, efficacious, and safe treatment option is now available for these patients,” he said in a company press release.
Dr. Mascarenhas was the lead investigator of the phase 3 PERSIST-2 trial that was the basis for the approval. Results from the trial were published in 2018 in JAMA Oncology and reported in detail at the time by this news organization.
Authors of an accompanying editorial noted the trial was truncated after the FDA imposed a clinical hold on pacritinib in February 2016 after reports from an earlier trial, PERSIST-1, of patient deaths related to cardiac failure and arrest as well as intracranial hemorrhage. The clinical hold was lifted in January 2017 after the manufacturer provided the FDA with more mature data.
Despite the truncation, the PERSIST-2 trial provided sufficient data to obtain accelerated approval for the drug. The study compared pacritinib with best available therapy (BAT).
In the cohort of patients treated with pacritinib 200 mg twice daily, 29% of patients had a reduction in spleen volume of at least 35% compared with 3% of patients receiving BAT, which included ruxolitinib.
The company is now expected to demonstrate clinical benefit in a confirmatory trial and has the PACIFICA trial underway. Results are expected in mid-2025.
The most common adverse reactions (reported by ≥ 20% of patients) were diarrhea, thrombocytopenia, nausea, anemia, and peripheral edema. The most frequent serious adverse reactions (≥ 3%) were anemia, thrombocytopenia, pneumonia, cardiac failure, disease progression, pyrexia, and squamous cell carcinoma of the skin.
A version of this article first appeared on Medscape.com.
Pacritinib (Vonjo, CTI BioPharma) is indicated for use in the treatment of adults with intermediate- or high-risk primary or secondary (post–polycythemia vera or post–essential thrombocythemia) myelofibrosis with a platelet count below 50 × 109/L.
Pacritinib is a novel oral kinase inhibitor with specificity for activity against Janus associated kinase 2 (JAK2) and IRAK1, without inhibiting JAK1. The recommended dosage is 200 mg orally twice daily.
In the United States, there are approximately 21,000 patients with myelofibrosis, notes the manufacturer. About one-third develop severe thrombocytopenia.
“Myelofibrosis with severe thrombocytopenia, defined as blood platelet counts below 50 × 109/L, has been shown to result in poor survival outcomes coupled with debilitating symptoms. Limited treatment options have rendered this disease as an area of urgent unmet medical need,” said John Mascarenhas, MD, associate professor, medicine, hematology, and medical oncology, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York.
“I am pleased to see that a new, efficacious, and safe treatment option is now available for these patients,” he said in a company press release.
Dr. Mascarenhas was the lead investigator of the phase 3 PERSIST-2 trial that was the basis for the approval. Results from the trial were published in 2018 in JAMA Oncology and reported in detail at the time by this news organization.
Authors of an accompanying editorial noted the trial was truncated after the FDA imposed a clinical hold on pacritinib in February 2016 after reports from an earlier trial, PERSIST-1, of patient deaths related to cardiac failure and arrest as well as intracranial hemorrhage. The clinical hold was lifted in January 2017 after the manufacturer provided the FDA with more mature data.
Despite the truncation, the PERSIST-2 trial provided sufficient data to obtain accelerated approval for the drug. The study compared pacritinib with best available therapy (BAT).
In the cohort of patients treated with pacritinib 200 mg twice daily, 29% of patients had a reduction in spleen volume of at least 35% compared with 3% of patients receiving BAT, which included ruxolitinib.
The company is now expected to demonstrate clinical benefit in a confirmatory trial and has the PACIFICA trial underway. Results are expected in mid-2025.
The most common adverse reactions (reported by ≥ 20% of patients) were diarrhea, thrombocytopenia, nausea, anemia, and peripheral edema. The most frequent serious adverse reactions (≥ 3%) were anemia, thrombocytopenia, pneumonia, cardiac failure, disease progression, pyrexia, and squamous cell carcinoma of the skin.
A version of this article first appeared on Medscape.com.
Pacritinib (Vonjo, CTI BioPharma) is indicated for use in the treatment of adults with intermediate- or high-risk primary or secondary (post–polycythemia vera or post–essential thrombocythemia) myelofibrosis with a platelet count below 50 × 109/L.
Pacritinib is a novel oral kinase inhibitor with specificity for activity against Janus associated kinase 2 (JAK2) and IRAK1, without inhibiting JAK1. The recommended dosage is 200 mg orally twice daily.
In the United States, there are approximately 21,000 patients with myelofibrosis, notes the manufacturer. About one-third develop severe thrombocytopenia.
“Myelofibrosis with severe thrombocytopenia, defined as blood platelet counts below 50 × 109/L, has been shown to result in poor survival outcomes coupled with debilitating symptoms. Limited treatment options have rendered this disease as an area of urgent unmet medical need,” said John Mascarenhas, MD, associate professor, medicine, hematology, and medical oncology, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York.
“I am pleased to see that a new, efficacious, and safe treatment option is now available for these patients,” he said in a company press release.
Dr. Mascarenhas was the lead investigator of the phase 3 PERSIST-2 trial that was the basis for the approval. Results from the trial were published in 2018 in JAMA Oncology and reported in detail at the time by this news organization.
Authors of an accompanying editorial noted the trial was truncated after the FDA imposed a clinical hold on pacritinib in February 2016 after reports from an earlier trial, PERSIST-1, of patient deaths related to cardiac failure and arrest as well as intracranial hemorrhage. The clinical hold was lifted in January 2017 after the manufacturer provided the FDA with more mature data.
Despite the truncation, the PERSIST-2 trial provided sufficient data to obtain accelerated approval for the drug. The study compared pacritinib with best available therapy (BAT).
In the cohort of patients treated with pacritinib 200 mg twice daily, 29% of patients had a reduction in spleen volume of at least 35% compared with 3% of patients receiving BAT, which included ruxolitinib.
The company is now expected to demonstrate clinical benefit in a confirmatory trial and has the PACIFICA trial underway. Results are expected in mid-2025.
The most common adverse reactions (reported by ≥ 20% of patients) were diarrhea, thrombocytopenia, nausea, anemia, and peripheral edema. The most frequent serious adverse reactions (≥ 3%) were anemia, thrombocytopenia, pneumonia, cardiac failure, disease progression, pyrexia, and squamous cell carcinoma of the skin.
A version of this article first appeared on Medscape.com.
Elective surgery should be delayed 7 weeks after COVID-19 infection for unvaccinated patients, statement recommends
.
For patients fully vaccinated against COVID-19 with breakthrough infections, there is no consensus on how vaccination affects the time between COVID-19 infection and elective surgery. Clinicians should use their clinical judgment to schedule procedures, said Randall M. Clark, MD, president of the American Society of Anesthesiologists (ASA). “We need all physicians, anesthesiologists, surgeons, and others to base their decision to go ahead with elective surgery on the patient’s symptoms, their need for the procedure, and whether delays could cause other problems with their health,” he said in an interview.
Prior to these updated recommendations, which were published Feb. 22, the ASA and the APSF recommended a 4-week gap between COVID-19 diagnosis and elective surgery for asymptomatic or mild cases, regardless of a patient’s vaccination status.
Extending the wait time from 4 to 7 weeks was based on a multination study conducted in October 2020 following more than 140,000 surgical patients. Patients with previous COVID-19 infection had an increased risk for complications and death in elective surgery for up to 6 weeks following their diagnosis, compared with patients without COVID-19. Additional research in the United States found that patients with a preoperative COVID diagnosis were at higher risk for postoperative complications of respiratory failure for up to 4 weeks after diagnosis and postoperative pneumonia complications for up to 8 weeks after diagnosis.
Because these studies were conducted in unvaccinated populations or those with low vaccination rates, and preliminary data suggest vaccinated patients with breakthrough infections may have a lower risk for complications and death postinfection, “we felt that it was prudent to just make recommendations specific to unvaccinated patients,” Dr. Clark added.
Although this guidance is “very helpful” in that it summarizes the currently available research to give evidence-based recommendations, the 7-week wait time is a “very conservative estimate,” Brent Matthews, MD, surgeon-in-chief of the surgery care division of Atrium Health, Charlotte, N.C., told this news organization. At Atrium Health, surgery is scheduled at least 21 days after a patient’s COVID-19 diagnosis, regardless of their vaccination status, Dr. Matthews said.
The studies currently available were conducted earlier in the pandemic, when a different variant was prevalent, Dr. Matthews explained. The Omicron variant is currently the most prevalent COVID-19 variant and is less virulent than earlier strains of the virus. The joint statement does note that there is currently “no robust data” on patients infected with the Delta or Omicron variants of COVID-19, and that “the Omicron variant causes less severe disease and is more likely to reside in the oro- and nasopharynx without infiltration and damage to the lungs.”
Still, the new recommendations are a reminder to re-evaluate the potential complications from surgery for previously infected patients and to consider what comorbidities might make them more vulnerable, Dr. Matthews said. “The real power of the joint statement is to get people to ensure that they make an assessment of every patient that comes in front of them who has had a recent positive COVID test.”
A version of this article first appeared on Medscape.com.
.
For patients fully vaccinated against COVID-19 with breakthrough infections, there is no consensus on how vaccination affects the time between COVID-19 infection and elective surgery. Clinicians should use their clinical judgment to schedule procedures, said Randall M. Clark, MD, president of the American Society of Anesthesiologists (ASA). “We need all physicians, anesthesiologists, surgeons, and others to base their decision to go ahead with elective surgery on the patient’s symptoms, their need for the procedure, and whether delays could cause other problems with their health,” he said in an interview.
Prior to these updated recommendations, which were published Feb. 22, the ASA and the APSF recommended a 4-week gap between COVID-19 diagnosis and elective surgery for asymptomatic or mild cases, regardless of a patient’s vaccination status.
Extending the wait time from 4 to 7 weeks was based on a multination study conducted in October 2020 following more than 140,000 surgical patients. Patients with previous COVID-19 infection had an increased risk for complications and death in elective surgery for up to 6 weeks following their diagnosis, compared with patients without COVID-19. Additional research in the United States found that patients with a preoperative COVID diagnosis were at higher risk for postoperative complications of respiratory failure for up to 4 weeks after diagnosis and postoperative pneumonia complications for up to 8 weeks after diagnosis.
Because these studies were conducted in unvaccinated populations or those with low vaccination rates, and preliminary data suggest vaccinated patients with breakthrough infections may have a lower risk for complications and death postinfection, “we felt that it was prudent to just make recommendations specific to unvaccinated patients,” Dr. Clark added.
Although this guidance is “very helpful” in that it summarizes the currently available research to give evidence-based recommendations, the 7-week wait time is a “very conservative estimate,” Brent Matthews, MD, surgeon-in-chief of the surgery care division of Atrium Health, Charlotte, N.C., told this news organization. At Atrium Health, surgery is scheduled at least 21 days after a patient’s COVID-19 diagnosis, regardless of their vaccination status, Dr. Matthews said.
The studies currently available were conducted earlier in the pandemic, when a different variant was prevalent, Dr. Matthews explained. The Omicron variant is currently the most prevalent COVID-19 variant and is less virulent than earlier strains of the virus. The joint statement does note that there is currently “no robust data” on patients infected with the Delta or Omicron variants of COVID-19, and that “the Omicron variant causes less severe disease and is more likely to reside in the oro- and nasopharynx without infiltration and damage to the lungs.”
Still, the new recommendations are a reminder to re-evaluate the potential complications from surgery for previously infected patients and to consider what comorbidities might make them more vulnerable, Dr. Matthews said. “The real power of the joint statement is to get people to ensure that they make an assessment of every patient that comes in front of them who has had a recent positive COVID test.”
A version of this article first appeared on Medscape.com.
.
For patients fully vaccinated against COVID-19 with breakthrough infections, there is no consensus on how vaccination affects the time between COVID-19 infection and elective surgery. Clinicians should use their clinical judgment to schedule procedures, said Randall M. Clark, MD, president of the American Society of Anesthesiologists (ASA). “We need all physicians, anesthesiologists, surgeons, and others to base their decision to go ahead with elective surgery on the patient’s symptoms, their need for the procedure, and whether delays could cause other problems with their health,” he said in an interview.
Prior to these updated recommendations, which were published Feb. 22, the ASA and the APSF recommended a 4-week gap between COVID-19 diagnosis and elective surgery for asymptomatic or mild cases, regardless of a patient’s vaccination status.
Extending the wait time from 4 to 7 weeks was based on a multination study conducted in October 2020 following more than 140,000 surgical patients. Patients with previous COVID-19 infection had an increased risk for complications and death in elective surgery for up to 6 weeks following their diagnosis, compared with patients without COVID-19. Additional research in the United States found that patients with a preoperative COVID diagnosis were at higher risk for postoperative complications of respiratory failure for up to 4 weeks after diagnosis and postoperative pneumonia complications for up to 8 weeks after diagnosis.
Because these studies were conducted in unvaccinated populations or those with low vaccination rates, and preliminary data suggest vaccinated patients with breakthrough infections may have a lower risk for complications and death postinfection, “we felt that it was prudent to just make recommendations specific to unvaccinated patients,” Dr. Clark added.
Although this guidance is “very helpful” in that it summarizes the currently available research to give evidence-based recommendations, the 7-week wait time is a “very conservative estimate,” Brent Matthews, MD, surgeon-in-chief of the surgery care division of Atrium Health, Charlotte, N.C., told this news organization. At Atrium Health, surgery is scheduled at least 21 days after a patient’s COVID-19 diagnosis, regardless of their vaccination status, Dr. Matthews said.
The studies currently available were conducted earlier in the pandemic, when a different variant was prevalent, Dr. Matthews explained. The Omicron variant is currently the most prevalent COVID-19 variant and is less virulent than earlier strains of the virus. The joint statement does note that there is currently “no robust data” on patients infected with the Delta or Omicron variants of COVID-19, and that “the Omicron variant causes less severe disease and is more likely to reside in the oro- and nasopharynx without infiltration and damage to the lungs.”
Still, the new recommendations are a reminder to re-evaluate the potential complications from surgery for previously infected patients and to consider what comorbidities might make them more vulnerable, Dr. Matthews said. “The real power of the joint statement is to get people to ensure that they make an assessment of every patient that comes in front of them who has had a recent positive COVID test.”
A version of this article first appeared on Medscape.com.
Lung cancer drug price trends cause alarm, highlight need for reform
The findings underscore the need for price reform, according to the investigators, who analyzed prices for 17 brand-name medications used for treating metastatic non–small cell lung cancer (NSCLC).
Prices increased during the study period and correlated within each drug class, Aakash Desai, MBBS, and colleagues from the Mayo Clinic, Rochester, Minn., found.
“Because numerous new drugs have been approved for the treatment of NSCLC in recent years, we sought to specifically study the price competition among drugs used to treat this cancer subtype,” they explained, noting that for most drug classes price increases outpaced changes in the consumer price index for prescription medications and the inflation rate.
The findings were published Jan. 25, 2022, in JAMA Network Open.
Multiple brand-name medications across several drug classes, including four immune checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab, and durvalumab), five epidermal growth factor receptor inhibitors (gefitinib, afatinib, erlotinib, osimertinib, and dacomitinib), five anaplastic lymphoma kinase inhibitors (crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib), two BRAF inhibitors (dabrafenib, vemurafenib), and one MEK inhibitor (trametinib) were included in the analysis.
Median Pearson correlation coefficients approached 1.0 for all drug classes, indicating that prices increased despite within-class drug competition. Median values ranged from 0.898 for epidermal growth factor inhibitors to 0.999 for anaplastic lymphoma kinase inhibitors and BRAF and MEK inhibitors, the investigators found.
Median compounded annual growth rates (CAGRs) were 1.81% for immune checkpoint inhibitors, 2.56% for epidermal growth factor receptor inhibitors, 2.46% for anaplastic lymphoma kinase and ROS1 inhibitors, and 3.06% for BRAF and MEK inhibitors.
“With the exception of the immunotherapy class, the median cost CAGR outpaced the annual growth rate of the consumer price index for prescription drugs at 2.10% and, for all classes, the average yearly inflation rate of 1.75% during the same period,” they wrote.
Also of note, only one price decrease occurred among all therapeutic classes studied.
“This was observed for erlotinib between 2019 and 2020, and it corresponded with the introduction of a generic competitor to the market,” the authors said.
The findings are reminiscent of an earlier study that showed a 25% increase in the price of 24 patented injectable anticancer agents in the United States over a period of 8 years after launch.
“These increases in cost were not offset by supplemental U.S. Food and Drug Administration approvals, new competitors, or new off-label indications. Thus, price increases over time were not substantially reduced by market competition and increased at similar rates among drugs within the same class,” they wrote, adding that “although one might expect oncology drug prices to decrease over time after market entry, the list price of most anticancer agents increases paradoxically.”
The “lock-step price increases” observed without evidence of price competition in this analysis raise concerns about the affordability of promising oncology drugs, they said, concluding that “academic, industry, and government partnerships should be developed to address the high costs of prescription oncology drugs, which may soon be unaffordable for most patients if the trends discovered in the present study continue.”
Dr. Desai reported having no disclosures.
The findings underscore the need for price reform, according to the investigators, who analyzed prices for 17 brand-name medications used for treating metastatic non–small cell lung cancer (NSCLC).
Prices increased during the study period and correlated within each drug class, Aakash Desai, MBBS, and colleagues from the Mayo Clinic, Rochester, Minn., found.
“Because numerous new drugs have been approved for the treatment of NSCLC in recent years, we sought to specifically study the price competition among drugs used to treat this cancer subtype,” they explained, noting that for most drug classes price increases outpaced changes in the consumer price index for prescription medications and the inflation rate.
The findings were published Jan. 25, 2022, in JAMA Network Open.
Multiple brand-name medications across several drug classes, including four immune checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab, and durvalumab), five epidermal growth factor receptor inhibitors (gefitinib, afatinib, erlotinib, osimertinib, and dacomitinib), five anaplastic lymphoma kinase inhibitors (crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib), two BRAF inhibitors (dabrafenib, vemurafenib), and one MEK inhibitor (trametinib) were included in the analysis.
Median Pearson correlation coefficients approached 1.0 for all drug classes, indicating that prices increased despite within-class drug competition. Median values ranged from 0.898 for epidermal growth factor inhibitors to 0.999 for anaplastic lymphoma kinase inhibitors and BRAF and MEK inhibitors, the investigators found.
Median compounded annual growth rates (CAGRs) were 1.81% for immune checkpoint inhibitors, 2.56% for epidermal growth factor receptor inhibitors, 2.46% for anaplastic lymphoma kinase and ROS1 inhibitors, and 3.06% for BRAF and MEK inhibitors.
“With the exception of the immunotherapy class, the median cost CAGR outpaced the annual growth rate of the consumer price index for prescription drugs at 2.10% and, for all classes, the average yearly inflation rate of 1.75% during the same period,” they wrote.
Also of note, only one price decrease occurred among all therapeutic classes studied.
“This was observed for erlotinib between 2019 and 2020, and it corresponded with the introduction of a generic competitor to the market,” the authors said.
The findings are reminiscent of an earlier study that showed a 25% increase in the price of 24 patented injectable anticancer agents in the United States over a period of 8 years after launch.
“These increases in cost were not offset by supplemental U.S. Food and Drug Administration approvals, new competitors, or new off-label indications. Thus, price increases over time were not substantially reduced by market competition and increased at similar rates among drugs within the same class,” they wrote, adding that “although one might expect oncology drug prices to decrease over time after market entry, the list price of most anticancer agents increases paradoxically.”
The “lock-step price increases” observed without evidence of price competition in this analysis raise concerns about the affordability of promising oncology drugs, they said, concluding that “academic, industry, and government partnerships should be developed to address the high costs of prescription oncology drugs, which may soon be unaffordable for most patients if the trends discovered in the present study continue.”
Dr. Desai reported having no disclosures.
The findings underscore the need for price reform, according to the investigators, who analyzed prices for 17 brand-name medications used for treating metastatic non–small cell lung cancer (NSCLC).
Prices increased during the study period and correlated within each drug class, Aakash Desai, MBBS, and colleagues from the Mayo Clinic, Rochester, Minn., found.
“Because numerous new drugs have been approved for the treatment of NSCLC in recent years, we sought to specifically study the price competition among drugs used to treat this cancer subtype,” they explained, noting that for most drug classes price increases outpaced changes in the consumer price index for prescription medications and the inflation rate.
The findings were published Jan. 25, 2022, in JAMA Network Open.
Multiple brand-name medications across several drug classes, including four immune checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab, and durvalumab), five epidermal growth factor receptor inhibitors (gefitinib, afatinib, erlotinib, osimertinib, and dacomitinib), five anaplastic lymphoma kinase inhibitors (crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib), two BRAF inhibitors (dabrafenib, vemurafenib), and one MEK inhibitor (trametinib) were included in the analysis.
Median Pearson correlation coefficients approached 1.0 for all drug classes, indicating that prices increased despite within-class drug competition. Median values ranged from 0.898 for epidermal growth factor inhibitors to 0.999 for anaplastic lymphoma kinase inhibitors and BRAF and MEK inhibitors, the investigators found.
Median compounded annual growth rates (CAGRs) were 1.81% for immune checkpoint inhibitors, 2.56% for epidermal growth factor receptor inhibitors, 2.46% for anaplastic lymphoma kinase and ROS1 inhibitors, and 3.06% for BRAF and MEK inhibitors.
“With the exception of the immunotherapy class, the median cost CAGR outpaced the annual growth rate of the consumer price index for prescription drugs at 2.10% and, for all classes, the average yearly inflation rate of 1.75% during the same period,” they wrote.
Also of note, only one price decrease occurred among all therapeutic classes studied.
“This was observed for erlotinib between 2019 and 2020, and it corresponded with the introduction of a generic competitor to the market,” the authors said.
The findings are reminiscent of an earlier study that showed a 25% increase in the price of 24 patented injectable anticancer agents in the United States over a period of 8 years after launch.
“These increases in cost were not offset by supplemental U.S. Food and Drug Administration approvals, new competitors, or new off-label indications. Thus, price increases over time were not substantially reduced by market competition and increased at similar rates among drugs within the same class,” they wrote, adding that “although one might expect oncology drug prices to decrease over time after market entry, the list price of most anticancer agents increases paradoxically.”
The “lock-step price increases” observed without evidence of price competition in this analysis raise concerns about the affordability of promising oncology drugs, they said, concluding that “academic, industry, and government partnerships should be developed to address the high costs of prescription oncology drugs, which may soon be unaffordable for most patients if the trends discovered in the present study continue.”
Dr. Desai reported having no disclosures.
FROM JAMA NETWORK OPEN
How Lp(a) can help improve ASCVD risk assessment
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).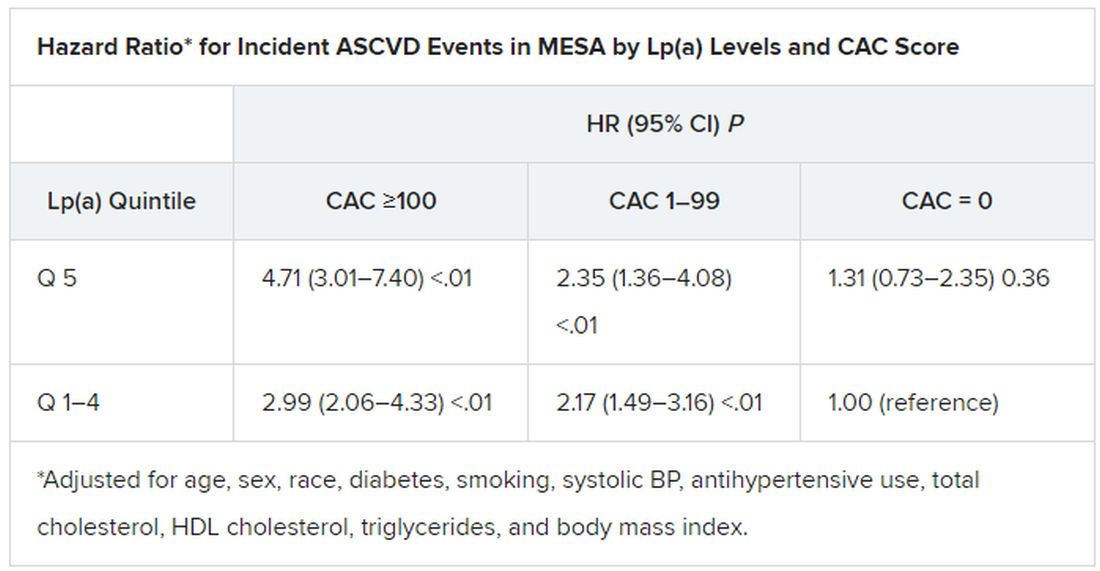
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).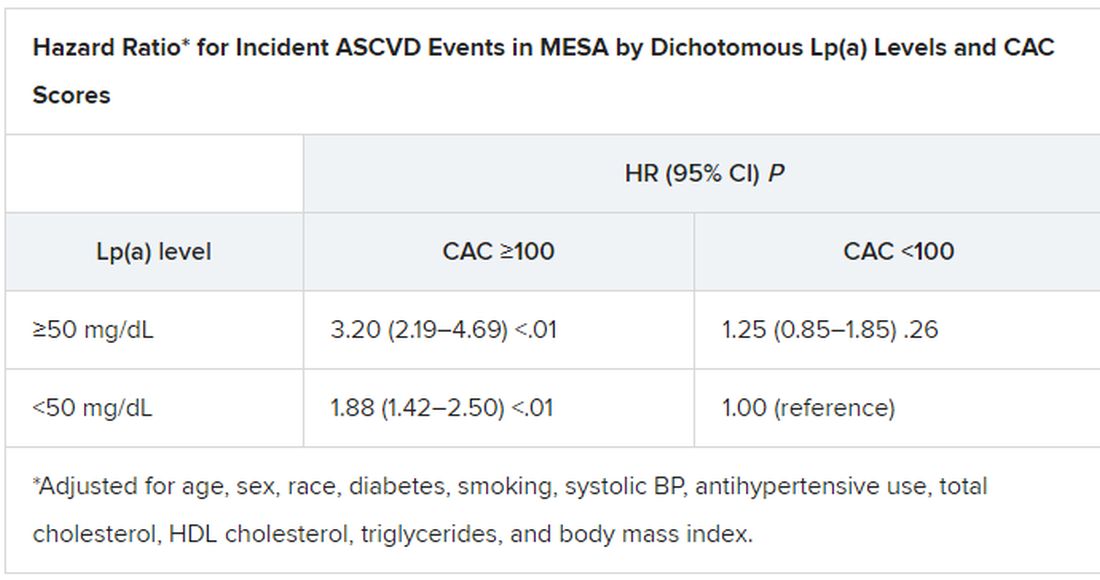
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY