User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Assessing Neutropenic Fever Management at Audie L. Murphy VA Medical Center (ALM VAMC)
BACKGROUND: Neutropenic fever poses a significant risk to cancer patients, with a major complication rate of 30% and mortality rate as high as 11%. Prompt evaluation with labs, imaging, and appropriate antibiotics are crucial to improving outcomes. In an attempt to reduce morbidity and mortality, the Infectious Disease Society of America (IDSA) and American Society of Clinical Oncology (ASCO) have set guidelines for the evaluation and treatment of neutropenic fever. The purpose of this project was to assess the management of neutropenic fever within our institution, and to identify potential areas for improvement in the care of these patients.
METHODS: We included patients seen at Audie L. Murphy VA Medical Center between September 1, 2018 and January 31, 2020 for neutropenic fever. We excluded patients without a diagnosis of malignancy and who had not received chemotherapy within the prior 4 weeks. We recorded the times of patient presentation, labs, imaging, and antibiotic administration. These were compared to the standards set forth by IDSA/ASCO. We also calculated average times to lab collection and to antibiotic administration. The proportion of patients who received unwarranted dose reductions of antibiotics also was assessed.
RESULTS: There were 35 unique encounters that met our inclusion criteria. All patients included in the study underwent all recommended diagnostic testing. 3 of 35 (8.6%) patients had CBC/CMP, 2 of 35 (5.7%) had urinalysis, 6 of 35 (17.1%) had blood cultures, and 3 of 35 (8.6%) had a chest x-ray (CXR) within the recommended 15 minutes from time of presentation. Only 3 of 35 (8.6%) patients received antibiotics within the recommended 1 hour from presentation. The average times to obtain CBC/CMP, urinalysis, blood cultures, CXR, and administration of antibiotics were 52.1 minutes, 162.4 minutes, 49.5 minutes, 96.1 minutes, and 308.4 minutes, respectively. 9 of 35 (25.7%) patients received unnecessary dose reductions of antibiotics.
CONCLUSIONS: Although patients received the appropriate evaluation according to IDSA/ASCO guidelines, the times to obtain appropriate diagnostic tests and administer recommend antibiotics were significantly prolonged. Establishing a standardized neutropenic fever protocol, prompt triaging, educational interventions, and identifying patients at risk for neutropenic fever may expedite care and improve outcomes for these high-risk patients.
BACKGROUND: Neutropenic fever poses a significant risk to cancer patients, with a major complication rate of 30% and mortality rate as high as 11%. Prompt evaluation with labs, imaging, and appropriate antibiotics are crucial to improving outcomes. In an attempt to reduce morbidity and mortality, the Infectious Disease Society of America (IDSA) and American Society of Clinical Oncology (ASCO) have set guidelines for the evaluation and treatment of neutropenic fever. The purpose of this project was to assess the management of neutropenic fever within our institution, and to identify potential areas for improvement in the care of these patients.
METHODS: We included patients seen at Audie L. Murphy VA Medical Center between September 1, 2018 and January 31, 2020 for neutropenic fever. We excluded patients without a diagnosis of malignancy and who had not received chemotherapy within the prior 4 weeks. We recorded the times of patient presentation, labs, imaging, and antibiotic administration. These were compared to the standards set forth by IDSA/ASCO. We also calculated average times to lab collection and to antibiotic administration. The proportion of patients who received unwarranted dose reductions of antibiotics also was assessed.
RESULTS: There were 35 unique encounters that met our inclusion criteria. All patients included in the study underwent all recommended diagnostic testing. 3 of 35 (8.6%) patients had CBC/CMP, 2 of 35 (5.7%) had urinalysis, 6 of 35 (17.1%) had blood cultures, and 3 of 35 (8.6%) had a chest x-ray (CXR) within the recommended 15 minutes from time of presentation. Only 3 of 35 (8.6%) patients received antibiotics within the recommended 1 hour from presentation. The average times to obtain CBC/CMP, urinalysis, blood cultures, CXR, and administration of antibiotics were 52.1 minutes, 162.4 minutes, 49.5 minutes, 96.1 minutes, and 308.4 minutes, respectively. 9 of 35 (25.7%) patients received unnecessary dose reductions of antibiotics.
CONCLUSIONS: Although patients received the appropriate evaluation according to IDSA/ASCO guidelines, the times to obtain appropriate diagnostic tests and administer recommend antibiotics were significantly prolonged. Establishing a standardized neutropenic fever protocol, prompt triaging, educational interventions, and identifying patients at risk for neutropenic fever may expedite care and improve outcomes for these high-risk patients.
BACKGROUND: Neutropenic fever poses a significant risk to cancer patients, with a major complication rate of 30% and mortality rate as high as 11%. Prompt evaluation with labs, imaging, and appropriate antibiotics are crucial to improving outcomes. In an attempt to reduce morbidity and mortality, the Infectious Disease Society of America (IDSA) and American Society of Clinical Oncology (ASCO) have set guidelines for the evaluation and treatment of neutropenic fever. The purpose of this project was to assess the management of neutropenic fever within our institution, and to identify potential areas for improvement in the care of these patients.
METHODS: We included patients seen at Audie L. Murphy VA Medical Center between September 1, 2018 and January 31, 2020 for neutropenic fever. We excluded patients without a diagnosis of malignancy and who had not received chemotherapy within the prior 4 weeks. We recorded the times of patient presentation, labs, imaging, and antibiotic administration. These were compared to the standards set forth by IDSA/ASCO. We also calculated average times to lab collection and to antibiotic administration. The proportion of patients who received unwarranted dose reductions of antibiotics also was assessed.
RESULTS: There were 35 unique encounters that met our inclusion criteria. All patients included in the study underwent all recommended diagnostic testing. 3 of 35 (8.6%) patients had CBC/CMP, 2 of 35 (5.7%) had urinalysis, 6 of 35 (17.1%) had blood cultures, and 3 of 35 (8.6%) had a chest x-ray (CXR) within the recommended 15 minutes from time of presentation. Only 3 of 35 (8.6%) patients received antibiotics within the recommended 1 hour from presentation. The average times to obtain CBC/CMP, urinalysis, blood cultures, CXR, and administration of antibiotics were 52.1 minutes, 162.4 minutes, 49.5 minutes, 96.1 minutes, and 308.4 minutes, respectively. 9 of 35 (25.7%) patients received unnecessary dose reductions of antibiotics.
CONCLUSIONS: Although patients received the appropriate evaluation according to IDSA/ASCO guidelines, the times to obtain appropriate diagnostic tests and administer recommend antibiotics were significantly prolonged. Establishing a standardized neutropenic fever protocol, prompt triaging, educational interventions, and identifying patients at risk for neutropenic fever may expedite care and improve outcomes for these high-risk patients.
Analysis of Oncology Telehealth Services in Veterans Health Administration
BACKGROUND: The purpose of this work is to assess the current utilization patterns of telehealth for oncology care and identify opportunities for increased utilization for underserved regions. In order to accurately and efficiently obtain this information a national data extraction and analysis was required to better understand the current needs. Approximately 33% of veterans are considered to live in rural America. A significant proportion of cancer patients must travel long distances to access cutting-edge VA cancer care. Some VAMCs provide academic subspecialized oncology care including next generation sequencing (NGS), genetic counseling, opportunities to enroll in clinical trials, and world-renowned clinical expert consultation. These services are not conveniently accessible for veterans therefore requiring a program which supports access to all.
METHODS: Baseline assessment measurements were identified to understand resource supply, demand, and telehealth utilization needs. Data were extracted from VA’s CDW and VSSCs Service Analysis Services cubes. 15 data measures from 8 data sources were pulled for 141 VAMCs spanning in time period from FY18 to March FY20.
Cluster Analysis, k-means clustering method, were used to classify VAMCs into distinct groups to identify facilities with the highest needs for oncology telehealth services. The evolutionary solving method was used to find the minimum sum of squared estimate of errors (SSE) allowing a more diversified approach in cluster assignment. Three cluster analysis were performed which include a combination of three variables specific to oncology staffing, telehealth usage, patient rurality, and community care consults (CCC).
RESULTS: Results show that 30 (21%) VAMCs are categorized as high need for TeleOncology. These facilities have low staff support, high CCC, and low telehealth usage. Of these, 11 (37%) VAMCs have high percent of rural patients. Eleven (8%) of all VAMCs are categorized as having high staff support, low CCC, and high telehealth usage; good hub site candidates for the National TeleOncology Program.
CONCLUSION: VA is expanding the National TeleOncology Program to offer oncology services to underserved VAMCs and Veterans across the United States. Results of this analysis are being applied to determine where to prioritize telehealth services for oncology care and which sites may serve as hubs.
BACKGROUND: The purpose of this work is to assess the current utilization patterns of telehealth for oncology care and identify opportunities for increased utilization for underserved regions. In order to accurately and efficiently obtain this information a national data extraction and analysis was required to better understand the current needs. Approximately 33% of veterans are considered to live in rural America. A significant proportion of cancer patients must travel long distances to access cutting-edge VA cancer care. Some VAMCs provide academic subspecialized oncology care including next generation sequencing (NGS), genetic counseling, opportunities to enroll in clinical trials, and world-renowned clinical expert consultation. These services are not conveniently accessible for veterans therefore requiring a program which supports access to all.
METHODS: Baseline assessment measurements were identified to understand resource supply, demand, and telehealth utilization needs. Data were extracted from VA’s CDW and VSSCs Service Analysis Services cubes. 15 data measures from 8 data sources were pulled for 141 VAMCs spanning in time period from FY18 to March FY20.
Cluster Analysis, k-means clustering method, were used to classify VAMCs into distinct groups to identify facilities with the highest needs for oncology telehealth services. The evolutionary solving method was used to find the minimum sum of squared estimate of errors (SSE) allowing a more diversified approach in cluster assignment. Three cluster analysis were performed which include a combination of three variables specific to oncology staffing, telehealth usage, patient rurality, and community care consults (CCC).
RESULTS: Results show that 30 (21%) VAMCs are categorized as high need for TeleOncology. These facilities have low staff support, high CCC, and low telehealth usage. Of these, 11 (37%) VAMCs have high percent of rural patients. Eleven (8%) of all VAMCs are categorized as having high staff support, low CCC, and high telehealth usage; good hub site candidates for the National TeleOncology Program.
CONCLUSION: VA is expanding the National TeleOncology Program to offer oncology services to underserved VAMCs and Veterans across the United States. Results of this analysis are being applied to determine where to prioritize telehealth services for oncology care and which sites may serve as hubs.
BACKGROUND: The purpose of this work is to assess the current utilization patterns of telehealth for oncology care and identify opportunities for increased utilization for underserved regions. In order to accurately and efficiently obtain this information a national data extraction and analysis was required to better understand the current needs. Approximately 33% of veterans are considered to live in rural America. A significant proportion of cancer patients must travel long distances to access cutting-edge VA cancer care. Some VAMCs provide academic subspecialized oncology care including next generation sequencing (NGS), genetic counseling, opportunities to enroll in clinical trials, and world-renowned clinical expert consultation. These services are not conveniently accessible for veterans therefore requiring a program which supports access to all.
METHODS: Baseline assessment measurements were identified to understand resource supply, demand, and telehealth utilization needs. Data were extracted from VA’s CDW and VSSCs Service Analysis Services cubes. 15 data measures from 8 data sources were pulled for 141 VAMCs spanning in time period from FY18 to March FY20.
Cluster Analysis, k-means clustering method, were used to classify VAMCs into distinct groups to identify facilities with the highest needs for oncology telehealth services. The evolutionary solving method was used to find the minimum sum of squared estimate of errors (SSE) allowing a more diversified approach in cluster assignment. Three cluster analysis were performed which include a combination of three variables specific to oncology staffing, telehealth usage, patient rurality, and community care consults (CCC).
RESULTS: Results show that 30 (21%) VAMCs are categorized as high need for TeleOncology. These facilities have low staff support, high CCC, and low telehealth usage. Of these, 11 (37%) VAMCs have high percent of rural patients. Eleven (8%) of all VAMCs are categorized as having high staff support, low CCC, and high telehealth usage; good hub site candidates for the National TeleOncology Program.
CONCLUSION: VA is expanding the National TeleOncology Program to offer oncology services to underserved VAMCs and Veterans across the United States. Results of this analysis are being applied to determine where to prioritize telehealth services for oncology care and which sites may serve as hubs.
A Single Center Experience of Immune Related Adverse Events From Immune Checkpoint Inhibitors and an Attempt to Identify Populations at High Risk
INTRODUCTION: American Society of Clinical Oncology (ASCO) has developed guidelines on the management of immune-related adverse events (irAEs) associated with immune checkpoint inhibitors (ICPIs). However, many irAEs are under-reported and the studies to investigate predictive factors are limited with variable results.
METHODS: A total of 66 patients who received ICPIs at Stratton VAMC Albany between January 2015 to December 2018 were studied. Computerized Patient Record System (CPRS) was used to do a retrospective chart review to identify irAEs and related parameters. IRB approval was obtained.
RESULTS: Sixty-three patients received PD-1 inhibitors (62 males). Our study included 39 patients with lung, 10 renal, 6 head and neck, 4 skin (melanoma), and 2 bladder cancers, and 1 metastatic cancer with unknown primary. Median age of patients with irAEs was 69.5 years versus 66.7 years for patients without irAEs. 23 (36.5%) patients experienced 28 irAEs. 45 patients received nivolumab, 18 (40%) of which had 21 irAEs. 17 got pembrolizumab and 5 (35.2%) had 7 irAEs. Majority of the irAEs were grade I (n=10, 35.7%) or grade II (n=11, 39.2%), while 6 (21.4%) grade III and only 1 (3.5%) grade IV irAE was observed. Median time to appearance of irAEs was 2 cycles. Immunotherapy was continued in 12, temporarily held in 7 and permanently discontinued only in 4 patients. No death was attributed to irAEs. Six patients developed diarrhea, 4 hepatitis, 6 skin rash, 5 thyroid issues and 3 pneumonitis. Rare irAEs included cardiac tamponade (grade IV), uveitis (grade II), central adrenal insufficiency and mild neutropenia in one patient each. 2 patients had pre-existing autoimmune conditions (rheumatoid arthritis and chronic dermatitis), both had transient flares though immunotherapy was continued. Of note, only 3 patients received PDL-1 inhibitors and 1 developed grade II polymyalgia rheumatica and hypothyroidism.
Using multivariate logistic regression, we found no significant association between irAEs and age, body mass index, derived neutrophil to lymphocyte ratio, chronic kidney disease or environmental/medical allergies.
CONCLUSIONS: ICPIs were generally well tolerated in our population, though prompt recognition of rare and severe irAEs is essential. Larger studies are needed to investigate the predictive risk factors for irAEs.
INTRODUCTION: American Society of Clinical Oncology (ASCO) has developed guidelines on the management of immune-related adverse events (irAEs) associated with immune checkpoint inhibitors (ICPIs). However, many irAEs are under-reported and the studies to investigate predictive factors are limited with variable results.
METHODS: A total of 66 patients who received ICPIs at Stratton VAMC Albany between January 2015 to December 2018 were studied. Computerized Patient Record System (CPRS) was used to do a retrospective chart review to identify irAEs and related parameters. IRB approval was obtained.
RESULTS: Sixty-three patients received PD-1 inhibitors (62 males). Our study included 39 patients with lung, 10 renal, 6 head and neck, 4 skin (melanoma), and 2 bladder cancers, and 1 metastatic cancer with unknown primary. Median age of patients with irAEs was 69.5 years versus 66.7 years for patients without irAEs. 23 (36.5%) patients experienced 28 irAEs. 45 patients received nivolumab, 18 (40%) of which had 21 irAEs. 17 got pembrolizumab and 5 (35.2%) had 7 irAEs. Majority of the irAEs were grade I (n=10, 35.7%) or grade II (n=11, 39.2%), while 6 (21.4%) grade III and only 1 (3.5%) grade IV irAE was observed. Median time to appearance of irAEs was 2 cycles. Immunotherapy was continued in 12, temporarily held in 7 and permanently discontinued only in 4 patients. No death was attributed to irAEs. Six patients developed diarrhea, 4 hepatitis, 6 skin rash, 5 thyroid issues and 3 pneumonitis. Rare irAEs included cardiac tamponade (grade IV), uveitis (grade II), central adrenal insufficiency and mild neutropenia in one patient each. 2 patients had pre-existing autoimmune conditions (rheumatoid arthritis and chronic dermatitis), both had transient flares though immunotherapy was continued. Of note, only 3 patients received PDL-1 inhibitors and 1 developed grade II polymyalgia rheumatica and hypothyroidism.
Using multivariate logistic regression, we found no significant association between irAEs and age, body mass index, derived neutrophil to lymphocyte ratio, chronic kidney disease or environmental/medical allergies.
CONCLUSIONS: ICPIs were generally well tolerated in our population, though prompt recognition of rare and severe irAEs is essential. Larger studies are needed to investigate the predictive risk factors for irAEs.
INTRODUCTION: American Society of Clinical Oncology (ASCO) has developed guidelines on the management of immune-related adverse events (irAEs) associated with immune checkpoint inhibitors (ICPIs). However, many irAEs are under-reported and the studies to investigate predictive factors are limited with variable results.
METHODS: A total of 66 patients who received ICPIs at Stratton VAMC Albany between January 2015 to December 2018 were studied. Computerized Patient Record System (CPRS) was used to do a retrospective chart review to identify irAEs and related parameters. IRB approval was obtained.
RESULTS: Sixty-three patients received PD-1 inhibitors (62 males). Our study included 39 patients with lung, 10 renal, 6 head and neck, 4 skin (melanoma), and 2 bladder cancers, and 1 metastatic cancer with unknown primary. Median age of patients with irAEs was 69.5 years versus 66.7 years for patients without irAEs. 23 (36.5%) patients experienced 28 irAEs. 45 patients received nivolumab, 18 (40%) of which had 21 irAEs. 17 got pembrolizumab and 5 (35.2%) had 7 irAEs. Majority of the irAEs were grade I (n=10, 35.7%) or grade II (n=11, 39.2%), while 6 (21.4%) grade III and only 1 (3.5%) grade IV irAE was observed. Median time to appearance of irAEs was 2 cycles. Immunotherapy was continued in 12, temporarily held in 7 and permanently discontinued only in 4 patients. No death was attributed to irAEs. Six patients developed diarrhea, 4 hepatitis, 6 skin rash, 5 thyroid issues and 3 pneumonitis. Rare irAEs included cardiac tamponade (grade IV), uveitis (grade II), central adrenal insufficiency and mild neutropenia in one patient each. 2 patients had pre-existing autoimmune conditions (rheumatoid arthritis and chronic dermatitis), both had transient flares though immunotherapy was continued. Of note, only 3 patients received PDL-1 inhibitors and 1 developed grade II polymyalgia rheumatica and hypothyroidism.
Using multivariate logistic regression, we found no significant association between irAEs and age, body mass index, derived neutrophil to lymphocyte ratio, chronic kidney disease or environmental/medical allergies.
CONCLUSIONS: ICPIs were generally well tolerated in our population, though prompt recognition of rare and severe irAEs is essential. Larger studies are needed to investigate the predictive risk factors for irAEs.
A Rare Case of Triple Positive Inflammatory Breast Cancer in An Elderly Male
BACKGROUND: An 84-year-old male presented with a rapidly growing left breast mass associated with warmth, erythema, and serous discharge from left nipple for 2.5 months. Physical exam revealed ‘peau d’orange’ appearance of skin and a 3×7 cm, firm, irregular, fixed mass in left breast. Core needle biopsy of left breast revealed invasive ductal carcinoma and a computed tomography scan of chest showed multiple small pulmonary nodules. Patient was diagnosed with inflammatory breast carcinoma (Stage IV, cT4d cN1 cM1), ER/ PR positive, HER-2 positive. BRCA testing was negative. After a normal MUGA scan, patient was started on weekly paclitaxel and trastuzumab. After 4 cycles patient developed diarrhea and elected to stop paclitaxel. After 10 cycles of trastuzumab, patient developed signs of heart failure and a MUGA showed depressed left ventricular ejection fraction (LVEF). Trastuzumab was held and patient was started on tamoxifen. Patient had progression of primary mass into a fungating lesion and evidence of new pulmonary metastatic disease on tamoxifen. The primary lesion was treated with palliative radiation and after a subsequent MUGA scan showed normalization of LVEF; trastuzumab was resumed. Patient had stable disease on trastuzumab and continued to follow with oncology.
DISCUSSION: Male breast cancer is < 1% of all breast cancer but incidence is rising in the US. Risk factors include family history, BRCA2 > BRCA1, obesity, cirrhosis, and radiation exposure. Inflammatory breast cancer (IBC) is a rapidly progressive malignancy with a clinicopathological diagnosis. There are paucity of data of IBC in men due to rarity of the disease. Many patients initially are misdiagnosed with mastitis, unresponsive to antibiotics. At diagnosis, most patients have a higher age compared with females (by 5-10 years), and advanced stage, though have a similar prognosis by stage. Prognostic factors and treatment principles are same as females with multimodal approach of chemotherapy, radiation therapy, and hormone therapy.
CONCLUSIONS: IBC in men is very rare and awareness of its risk factors and presentation can lead to early diagnosis and better survival. Urgent referral to oncology is needed if index of suspicion is high. Further research is needed for defining best treatment modalities in elderly males.”
BACKGROUND: An 84-year-old male presented with a rapidly growing left breast mass associated with warmth, erythema, and serous discharge from left nipple for 2.5 months. Physical exam revealed ‘peau d’orange’ appearance of skin and a 3×7 cm, firm, irregular, fixed mass in left breast. Core needle biopsy of left breast revealed invasive ductal carcinoma and a computed tomography scan of chest showed multiple small pulmonary nodules. Patient was diagnosed with inflammatory breast carcinoma (Stage IV, cT4d cN1 cM1), ER/ PR positive, HER-2 positive. BRCA testing was negative. After a normal MUGA scan, patient was started on weekly paclitaxel and trastuzumab. After 4 cycles patient developed diarrhea and elected to stop paclitaxel. After 10 cycles of trastuzumab, patient developed signs of heart failure and a MUGA showed depressed left ventricular ejection fraction (LVEF). Trastuzumab was held and patient was started on tamoxifen. Patient had progression of primary mass into a fungating lesion and evidence of new pulmonary metastatic disease on tamoxifen. The primary lesion was treated with palliative radiation and after a subsequent MUGA scan showed normalization of LVEF; trastuzumab was resumed. Patient had stable disease on trastuzumab and continued to follow with oncology.
DISCUSSION: Male breast cancer is < 1% of all breast cancer but incidence is rising in the US. Risk factors include family history, BRCA2 > BRCA1, obesity, cirrhosis, and radiation exposure. Inflammatory breast cancer (IBC) is a rapidly progressive malignancy with a clinicopathological diagnosis. There are paucity of data of IBC in men due to rarity of the disease. Many patients initially are misdiagnosed with mastitis, unresponsive to antibiotics. At diagnosis, most patients have a higher age compared with females (by 5-10 years), and advanced stage, though have a similar prognosis by stage. Prognostic factors and treatment principles are same as females with multimodal approach of chemotherapy, radiation therapy, and hormone therapy.
CONCLUSIONS: IBC in men is very rare and awareness of its risk factors and presentation can lead to early diagnosis and better survival. Urgent referral to oncology is needed if index of suspicion is high. Further research is needed for defining best treatment modalities in elderly males.”
BACKGROUND: An 84-year-old male presented with a rapidly growing left breast mass associated with warmth, erythema, and serous discharge from left nipple for 2.5 months. Physical exam revealed ‘peau d’orange’ appearance of skin and a 3×7 cm, firm, irregular, fixed mass in left breast. Core needle biopsy of left breast revealed invasive ductal carcinoma and a computed tomography scan of chest showed multiple small pulmonary nodules. Patient was diagnosed with inflammatory breast carcinoma (Stage IV, cT4d cN1 cM1), ER/ PR positive, HER-2 positive. BRCA testing was negative. After a normal MUGA scan, patient was started on weekly paclitaxel and trastuzumab. After 4 cycles patient developed diarrhea and elected to stop paclitaxel. After 10 cycles of trastuzumab, patient developed signs of heart failure and a MUGA showed depressed left ventricular ejection fraction (LVEF). Trastuzumab was held and patient was started on tamoxifen. Patient had progression of primary mass into a fungating lesion and evidence of new pulmonary metastatic disease on tamoxifen. The primary lesion was treated with palliative radiation and after a subsequent MUGA scan showed normalization of LVEF; trastuzumab was resumed. Patient had stable disease on trastuzumab and continued to follow with oncology.
DISCUSSION: Male breast cancer is < 1% of all breast cancer but incidence is rising in the US. Risk factors include family history, BRCA2 > BRCA1, obesity, cirrhosis, and radiation exposure. Inflammatory breast cancer (IBC) is a rapidly progressive malignancy with a clinicopathological diagnosis. There are paucity of data of IBC in men due to rarity of the disease. Many patients initially are misdiagnosed with mastitis, unresponsive to antibiotics. At diagnosis, most patients have a higher age compared with females (by 5-10 years), and advanced stage, though have a similar prognosis by stage. Prognostic factors and treatment principles are same as females with multimodal approach of chemotherapy, radiation therapy, and hormone therapy.
CONCLUSIONS: IBC in men is very rare and awareness of its risk factors and presentation can lead to early diagnosis and better survival. Urgent referral to oncology is needed if index of suspicion is high. Further research is needed for defining best treatment modalities in elderly males.”
A Multi-Center Retrospective Study Evaluating Palliative Antineoplastic Therapy Administered and Medication De-escalation in Veteran Cancer Patients Toward the End-of-life
BACKGROUND: Metastatic cancer patients near endof- life often continue to receive aggressive cancer treatments and are prescribed many chronic futile medications. The American Society of Clinical Oncology recommends avoiding use of chemotherapy towards end of life in solid tumor patients with poor performance due to potential risk of adverse events.
OBJECTIVES: The objective of this multi-site study was to evaluate the incidence of palliative antineoplastic therapy administration for patients with metastatic cancer as well as the number of patients who received non-essential medications at thirty and fourteen days prior to death.
METHODS: This was a retrospective, multicenter study conducted at 6 Veteran Affairs Medical Centers: Southern Arizona, Lexington, Robley Rex, John D Dingell, San Diego, and Richard L Roudebush. The electronic medical record system identified patients deceased between July 1, 2016 to June 30, 2018 with metastatic lung, colorectal, prostate, pancreatic cancer, or melanoma. Data were analyzed using descriptive analysis.
RESULTS: A total of 651 patients were included in the multicenter study, and the average age of veterans was 71 years with metastatic lung cancer being the most common malignancy at 55%. Within 30 days and 14 days of death, respectively, 24.6% and 13.2% had an antineoplastic agent. Within the last 30 days of life, 45% of patients received systemic chemotherapy, 38% received oral targeted agent, and 17% received immunotherapy. Within last 30 days of life, 50% received a first line treatment, 26.9% received a second line treatment, and 23.2% received ≥ third line of treatment. There was a large proportion of patients hospitalized (n=208) and/ or had ED visits (n=204) due to antineoplastic treatment and/or complications from malignancy. Within the last 30 days of death, 76.3% had ≥ 1 active chronic medication. Palliative care providers were the top recommenders for medication de-escalation.
CONCLUSION: The results of this multi-site retrospective study provides insight into the management of endof- life care for metastatic cancer patients across the VA health care system. Overall the results of this study demonstrate an opportunity for promoting detailed discussions with patients regarding palliative care earlier after diagnosis of metastatic cancer.
BACKGROUND: Metastatic cancer patients near endof- life often continue to receive aggressive cancer treatments and are prescribed many chronic futile medications. The American Society of Clinical Oncology recommends avoiding use of chemotherapy towards end of life in solid tumor patients with poor performance due to potential risk of adverse events.
OBJECTIVES: The objective of this multi-site study was to evaluate the incidence of palliative antineoplastic therapy administration for patients with metastatic cancer as well as the number of patients who received non-essential medications at thirty and fourteen days prior to death.
METHODS: This was a retrospective, multicenter study conducted at 6 Veteran Affairs Medical Centers: Southern Arizona, Lexington, Robley Rex, John D Dingell, San Diego, and Richard L Roudebush. The electronic medical record system identified patients deceased between July 1, 2016 to June 30, 2018 with metastatic lung, colorectal, prostate, pancreatic cancer, or melanoma. Data were analyzed using descriptive analysis.
RESULTS: A total of 651 patients were included in the multicenter study, and the average age of veterans was 71 years with metastatic lung cancer being the most common malignancy at 55%. Within 30 days and 14 days of death, respectively, 24.6% and 13.2% had an antineoplastic agent. Within the last 30 days of life, 45% of patients received systemic chemotherapy, 38% received oral targeted agent, and 17% received immunotherapy. Within last 30 days of life, 50% received a first line treatment, 26.9% received a second line treatment, and 23.2% received ≥ third line of treatment. There was a large proportion of patients hospitalized (n=208) and/ or had ED visits (n=204) due to antineoplastic treatment and/or complications from malignancy. Within the last 30 days of death, 76.3% had ≥ 1 active chronic medication. Palliative care providers were the top recommenders for medication de-escalation.
CONCLUSION: The results of this multi-site retrospective study provides insight into the management of endof- life care for metastatic cancer patients across the VA health care system. Overall the results of this study demonstrate an opportunity for promoting detailed discussions with patients regarding palliative care earlier after diagnosis of metastatic cancer.
BACKGROUND: Metastatic cancer patients near endof- life often continue to receive aggressive cancer treatments and are prescribed many chronic futile medications. The American Society of Clinical Oncology recommends avoiding use of chemotherapy towards end of life in solid tumor patients with poor performance due to potential risk of adverse events.
OBJECTIVES: The objective of this multi-site study was to evaluate the incidence of palliative antineoplastic therapy administration for patients with metastatic cancer as well as the number of patients who received non-essential medications at thirty and fourteen days prior to death.
METHODS: This was a retrospective, multicenter study conducted at 6 Veteran Affairs Medical Centers: Southern Arizona, Lexington, Robley Rex, John D Dingell, San Diego, and Richard L Roudebush. The electronic medical record system identified patients deceased between July 1, 2016 to June 30, 2018 with metastatic lung, colorectal, prostate, pancreatic cancer, or melanoma. Data were analyzed using descriptive analysis.
RESULTS: A total of 651 patients were included in the multicenter study, and the average age of veterans was 71 years with metastatic lung cancer being the most common malignancy at 55%. Within 30 days and 14 days of death, respectively, 24.6% and 13.2% had an antineoplastic agent. Within the last 30 days of life, 45% of patients received systemic chemotherapy, 38% received oral targeted agent, and 17% received immunotherapy. Within last 30 days of life, 50% received a first line treatment, 26.9% received a second line treatment, and 23.2% received ≥ third line of treatment. There was a large proportion of patients hospitalized (n=208) and/ or had ED visits (n=204) due to antineoplastic treatment and/or complications from malignancy. Within the last 30 days of death, 76.3% had ≥ 1 active chronic medication. Palliative care providers were the top recommenders for medication de-escalation.
CONCLUSION: The results of this multi-site retrospective study provides insight into the management of endof- life care for metastatic cancer patients across the VA health care system. Overall the results of this study demonstrate an opportunity for promoting detailed discussions with patients regarding palliative care earlier after diagnosis of metastatic cancer.
A Cognitive-Behavioral Stress Management Group for Men with Urologic Cancers: Pre- and Post-COVID
BACKGROUND: Urologic cancers and their treatments are associated with significant psychosocial challenges for veteran men, including sexual dysfunction, incontinence, fatigue, irritability, and depression. Although cancer support groups have been shown to be helpful for psychosocial distress, cognitive-behavioral stress management techniques have the capacity to directly address these challenges.
METHODS: A structured, open-enrollment, 6-session biweekly group was created in late 2017 as a cooperative effort between the urology department and comprehensive cancer center of a large VA medical center. Topics were selected based on their relevance to the population: (1) stress and the mind-body connection; (2) mindfulness; (3) sexual functioning and incontinence; (4) pain and sleep; (5) communicating with providers; and (6) managing anger and irritability. A clinical psychologist and/or psychology resident led the sessions, which include demonstration and practice of relaxation and mindfulness techniques, didactic presentations, and discussion. Medical providers received the group well and provides and a regular stream of referrals. Typical group size was between 2-6, and a total of 42 veterans have attended group sessions. The group was previously physically located in the urology clinic, reducing barriers and potentially stigma of access this type of service. After March 2020, the group transitioned to a weekly telephone- based group, continuing the same skills and topics, with good engagement and feedback from group members.
RESULTS: Group members have voiced increased confidence in managing their conditions and communicating with their providers, relief that they are not alone in their experience of potentially embarrassing side effects, and increased use of evidence-based stress management techniques.
CONCLUSION: Continuing this type of service during the COVID-19 pandemic has been important to help veteran manage the stress of postponed treatments (eg, radiation for prostate cancer), share information about hospital policies and procedures, and increase social connectedness with other similar patients.
BACKGROUND: Urologic cancers and their treatments are associated with significant psychosocial challenges for veteran men, including sexual dysfunction, incontinence, fatigue, irritability, and depression. Although cancer support groups have been shown to be helpful for psychosocial distress, cognitive-behavioral stress management techniques have the capacity to directly address these challenges.
METHODS: A structured, open-enrollment, 6-session biweekly group was created in late 2017 as a cooperative effort between the urology department and comprehensive cancer center of a large VA medical center. Topics were selected based on their relevance to the population: (1) stress and the mind-body connection; (2) mindfulness; (3) sexual functioning and incontinence; (4) pain and sleep; (5) communicating with providers; and (6) managing anger and irritability. A clinical psychologist and/or psychology resident led the sessions, which include demonstration and practice of relaxation and mindfulness techniques, didactic presentations, and discussion. Medical providers received the group well and provides and a regular stream of referrals. Typical group size was between 2-6, and a total of 42 veterans have attended group sessions. The group was previously physically located in the urology clinic, reducing barriers and potentially stigma of access this type of service. After March 2020, the group transitioned to a weekly telephone- based group, continuing the same skills and topics, with good engagement and feedback from group members.
RESULTS: Group members have voiced increased confidence in managing their conditions and communicating with their providers, relief that they are not alone in their experience of potentially embarrassing side effects, and increased use of evidence-based stress management techniques.
CONCLUSION: Continuing this type of service during the COVID-19 pandemic has been important to help veteran manage the stress of postponed treatments (eg, radiation for prostate cancer), share information about hospital policies and procedures, and increase social connectedness with other similar patients.
BACKGROUND: Urologic cancers and their treatments are associated with significant psychosocial challenges for veteran men, including sexual dysfunction, incontinence, fatigue, irritability, and depression. Although cancer support groups have been shown to be helpful for psychosocial distress, cognitive-behavioral stress management techniques have the capacity to directly address these challenges.
METHODS: A structured, open-enrollment, 6-session biweekly group was created in late 2017 as a cooperative effort between the urology department and comprehensive cancer center of a large VA medical center. Topics were selected based on their relevance to the population: (1) stress and the mind-body connection; (2) mindfulness; (3) sexual functioning and incontinence; (4) pain and sleep; (5) communicating with providers; and (6) managing anger and irritability. A clinical psychologist and/or psychology resident led the sessions, which include demonstration and practice of relaxation and mindfulness techniques, didactic presentations, and discussion. Medical providers received the group well and provides and a regular stream of referrals. Typical group size was between 2-6, and a total of 42 veterans have attended group sessions. The group was previously physically located in the urology clinic, reducing barriers and potentially stigma of access this type of service. After March 2020, the group transitioned to a weekly telephone- based group, continuing the same skills and topics, with good engagement and feedback from group members.
RESULTS: Group members have voiced increased confidence in managing their conditions and communicating with their providers, relief that they are not alone in their experience of potentially embarrassing side effects, and increased use of evidence-based stress management techniques.
CONCLUSION: Continuing this type of service during the COVID-19 pandemic has been important to help veteran manage the stress of postponed treatments (eg, radiation for prostate cancer), share information about hospital policies and procedures, and increase social connectedness with other similar patients.
A Case of Alectinib Cutaneous Toxicity and Results of a Desensitization Protocol
CASE REPORT: A male smoker aged 51 years with denovo metastatic NSCLC was treated with first-line chemoimmunotherapy. After 4 cycles, an EML4-ALK fusion was identified. At time of disease progression, alectinib 600mg BID was started after an 8-week washout period. Within 2 weeks, he developed a pruritic rash covering 90% of his BSA that required hospitalization and IV steroids. Biopsy confirmed a spongiotic and interface dermatitis with eosinophils consistent with a drug eruption. Rash was reported as an adverse event in the ALEX trial in 17% of patients treated with front-line alectinib but grade 3 rash was reported in only 1%.
A literature search demonstrated successful case reports of alectinib de-sensitization and thus a de-sensitization protocol was devised. Alectinib was started at 150mg daily and increased to 300mg BID over 2 weeks. His rash worsened resulting in a drug hold, treatment with oral prednisone, and a dose reduction to 300mg daily. The dose was increased to 300mg/450mg over 1 week when he developed painful mouth erosions. This resulted in a second dose hold and reduction to 300mg BID. After 2 weeks, alectinib was discontinued due to worsening rash with a plan to switch to an alternate ALK TKI, a strategy which has been successfully reported in the literature. Lorlatinib 100mg was recommended given phase 2 data demonstrating very low rates of rash (5% grade 1-2 and < 1% grade 3). While he did experience a facial rash within 2 weeks, a dose hold or reduction was not required. Nonetheless, lorlatinib was discontinued after 4 weeks due to other intolerable side effects and hypertriglyceridemia
DISCUSSION: Pembrolizumab has a terminal half-life of 22 days with steady state reached at 16 weeks with every 3-week dosing. It is therefore possible that prior exposure to pembrolizumab exacerbated the cutaneous toxicity of alectinib in this case. Multiple studies have shown that combining immunotherapy with alectinib leads to substantially more adverse events.
CONCLUSION: In patients with alectinib hypersensitivity, a de-sensitization protocol can be attempted. If hypersensitivity recurs, switching to an alternate ALK TKI is warranted. However, if immunotherapy has been previously administered without time for adequate washout, no TKI therapy may be tolerable.
CASE REPORT: A male smoker aged 51 years with denovo metastatic NSCLC was treated with first-line chemoimmunotherapy. After 4 cycles, an EML4-ALK fusion was identified. At time of disease progression, alectinib 600mg BID was started after an 8-week washout period. Within 2 weeks, he developed a pruritic rash covering 90% of his BSA that required hospitalization and IV steroids. Biopsy confirmed a spongiotic and interface dermatitis with eosinophils consistent with a drug eruption. Rash was reported as an adverse event in the ALEX trial in 17% of patients treated with front-line alectinib but grade 3 rash was reported in only 1%.
A literature search demonstrated successful case reports of alectinib de-sensitization and thus a de-sensitization protocol was devised. Alectinib was started at 150mg daily and increased to 300mg BID over 2 weeks. His rash worsened resulting in a drug hold, treatment with oral prednisone, and a dose reduction to 300mg daily. The dose was increased to 300mg/450mg over 1 week when he developed painful mouth erosions. This resulted in a second dose hold and reduction to 300mg BID. After 2 weeks, alectinib was discontinued due to worsening rash with a plan to switch to an alternate ALK TKI, a strategy which has been successfully reported in the literature. Lorlatinib 100mg was recommended given phase 2 data demonstrating very low rates of rash (5% grade 1-2 and < 1% grade 3). While he did experience a facial rash within 2 weeks, a dose hold or reduction was not required. Nonetheless, lorlatinib was discontinued after 4 weeks due to other intolerable side effects and hypertriglyceridemia
DISCUSSION: Pembrolizumab has a terminal half-life of 22 days with steady state reached at 16 weeks with every 3-week dosing. It is therefore possible that prior exposure to pembrolizumab exacerbated the cutaneous toxicity of alectinib in this case. Multiple studies have shown that combining immunotherapy with alectinib leads to substantially more adverse events.
CONCLUSION: In patients with alectinib hypersensitivity, a de-sensitization protocol can be attempted. If hypersensitivity recurs, switching to an alternate ALK TKI is warranted. However, if immunotherapy has been previously administered without time for adequate washout, no TKI therapy may be tolerable.
CASE REPORT: A male smoker aged 51 years with denovo metastatic NSCLC was treated with first-line chemoimmunotherapy. After 4 cycles, an EML4-ALK fusion was identified. At time of disease progression, alectinib 600mg BID was started after an 8-week washout period. Within 2 weeks, he developed a pruritic rash covering 90% of his BSA that required hospitalization and IV steroids. Biopsy confirmed a spongiotic and interface dermatitis with eosinophils consistent with a drug eruption. Rash was reported as an adverse event in the ALEX trial in 17% of patients treated with front-line alectinib but grade 3 rash was reported in only 1%.
A literature search demonstrated successful case reports of alectinib de-sensitization and thus a de-sensitization protocol was devised. Alectinib was started at 150mg daily and increased to 300mg BID over 2 weeks. His rash worsened resulting in a drug hold, treatment with oral prednisone, and a dose reduction to 300mg daily. The dose was increased to 300mg/450mg over 1 week when he developed painful mouth erosions. This resulted in a second dose hold and reduction to 300mg BID. After 2 weeks, alectinib was discontinued due to worsening rash with a plan to switch to an alternate ALK TKI, a strategy which has been successfully reported in the literature. Lorlatinib 100mg was recommended given phase 2 data demonstrating very low rates of rash (5% grade 1-2 and < 1% grade 3). While he did experience a facial rash within 2 weeks, a dose hold or reduction was not required. Nonetheless, lorlatinib was discontinued after 4 weeks due to other intolerable side effects and hypertriglyceridemia
DISCUSSION: Pembrolizumab has a terminal half-life of 22 days with steady state reached at 16 weeks with every 3-week dosing. It is therefore possible that prior exposure to pembrolizumab exacerbated the cutaneous toxicity of alectinib in this case. Multiple studies have shown that combining immunotherapy with alectinib leads to substantially more adverse events.
CONCLUSION: In patients with alectinib hypersensitivity, a de-sensitization protocol can be attempted. If hypersensitivity recurs, switching to an alternate ALK TKI is warranted. However, if immunotherapy has been previously administered without time for adequate washout, no TKI therapy may be tolerable.
Immunotherapy should not be withheld because of sex, age, or PS
The improvement in survival in many cancer types that is seen with immune checkpoint inhibitors (ICIs), when compared to control therapies, is not affected by the patient’s sex, age, or Eastern Cooperative Oncology Group (ECOG) performance status (PS), according to a new meta-analysis.
Therefore, treatment with these immunotherapies should not be withheld on the basis of these factors, the authors concluded.
Asked whether there have been such instances of withholding ICIs, lead author Yucai Wang, MD, PhD, Mayo Clinic, Rochester, Minnesota, told Medscape Medical News: “We did this study solely based on scientific questions we had and not because we were seeing any bias at the moment in the use of ICIs.
“And we saw that the survival benefits were very similar across all of the categories [we analyzed], with a survival benefit of about 20% from immunotherapy across the board, which is clinically meaningful,” he added.
The study was published online August 7 in JAMA Network Open.
“The comparable survival advantage between patients of different sex, age, and ECOG PS may encourage more patients to receive ICI treatment regardless of cancer types, lines of therapy, agents of immunotherapy, and intervention therapies,” the authors commented.
Wang noted that there have been conflicting reports in the literature suggesting that male patients may benefit more from immunotherapy than female patients and that older patients may benefit more from the same treatment than younger patients.
However, there are also suggestions in the literature that women experience a stronger immune response than men and that, with aging, the immune system generally undergoes immunosenescence.
In addition, the PS of oncology patients has been implicated in how well patients respond to immunotherapy.
Wang noted that the findings of past studies have contradicted each other.
Findings of the Meta-Analysis
The meta-analysis included 37 randomized clinical trials that involved a total of 23,760 patients with a variety of advanced cancers. “Most of the trials were phase 3 (n = 34) and conduced for subsequent lines of therapy (n = 22),” the authors explained.
The most common cancers treated with an ICI were non–small cell lung cancer and melanoma.
Pooled overall survival (OS) hazard ratios (HRs) were calculated on the basis of sex, age (younger than 65 years and 65 years and older), and an ECOG PS of 0 and 1 or higher.
Responses were stratified on the basis of cancer type, line of therapy, the ICI used, and the immunotherapy strategy used in the ICI arm.
Most of the drugs evaluated were PD-1 and PD-L1 inhibitors. The specific drugs assessed included ipilimumab, tremelimumab, nivolumab, pembrolizumab, atezolizumab, durvalumab, and avelumab.
A total of 32 trials that involved more than 20,000 patients reported HRs for death according to the patients’ sex. Thirty-four trials that involved more than 21,000 patients reported HRs for death according to patients’ age, and 30 trials that involved more than 19,000 patients reported HRs for death according to patients’ ECOG PS.
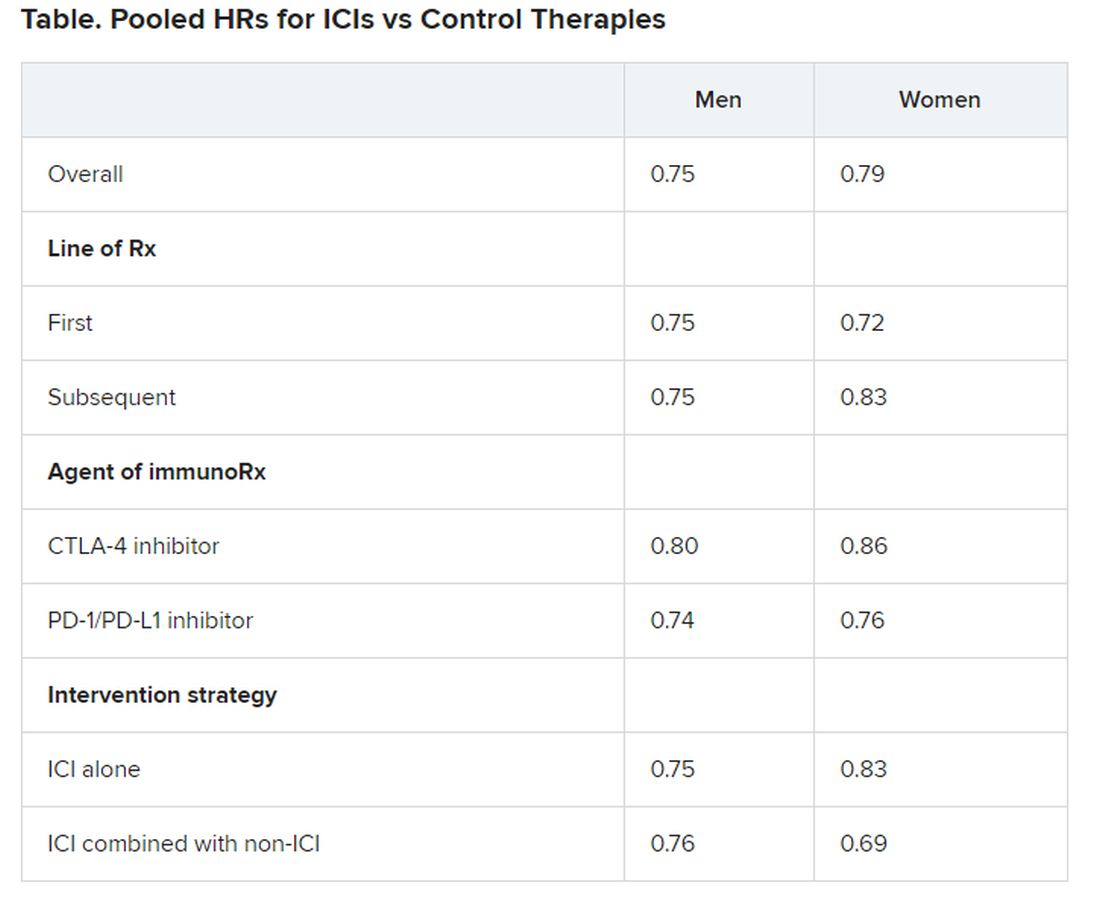
No significant differences in OS benefit were seen by cancer type, line of therapy, agent of immunotherapy, or intervention strategy, the investigators pointed out.
There were also no differences in survival benefit associated with immunotherapy vs control therapies for patients with an ECOG PS of 0 and an ECOG PS of 1 or greater. The OS benefit was 0.81 for those with an ECOG PS of 0 and 0.79 for those with an ECOG PS of 1 or greater.
Wang has disclosed no relevant financial relationships.
This article first appeared on Medscape.com .
The improvement in survival in many cancer types that is seen with immune checkpoint inhibitors (ICIs), when compared to control therapies, is not affected by the patient’s sex, age, or Eastern Cooperative Oncology Group (ECOG) performance status (PS), according to a new meta-analysis.
Therefore, treatment with these immunotherapies should not be withheld on the basis of these factors, the authors concluded.
Asked whether there have been such instances of withholding ICIs, lead author Yucai Wang, MD, PhD, Mayo Clinic, Rochester, Minnesota, told Medscape Medical News: “We did this study solely based on scientific questions we had and not because we were seeing any bias at the moment in the use of ICIs.
“And we saw that the survival benefits were very similar across all of the categories [we analyzed], with a survival benefit of about 20% from immunotherapy across the board, which is clinically meaningful,” he added.
The study was published online August 7 in JAMA Network Open.
“The comparable survival advantage between patients of different sex, age, and ECOG PS may encourage more patients to receive ICI treatment regardless of cancer types, lines of therapy, agents of immunotherapy, and intervention therapies,” the authors commented.
Wang noted that there have been conflicting reports in the literature suggesting that male patients may benefit more from immunotherapy than female patients and that older patients may benefit more from the same treatment than younger patients.
However, there are also suggestions in the literature that women experience a stronger immune response than men and that, with aging, the immune system generally undergoes immunosenescence.
In addition, the PS of oncology patients has been implicated in how well patients respond to immunotherapy.
Wang noted that the findings of past studies have contradicted each other.
Findings of the Meta-Analysis
The meta-analysis included 37 randomized clinical trials that involved a total of 23,760 patients with a variety of advanced cancers. “Most of the trials were phase 3 (n = 34) and conduced for subsequent lines of therapy (n = 22),” the authors explained.
The most common cancers treated with an ICI were non–small cell lung cancer and melanoma.
Pooled overall survival (OS) hazard ratios (HRs) were calculated on the basis of sex, age (younger than 65 years and 65 years and older), and an ECOG PS of 0 and 1 or higher.
Responses were stratified on the basis of cancer type, line of therapy, the ICI used, and the immunotherapy strategy used in the ICI arm.
Most of the drugs evaluated were PD-1 and PD-L1 inhibitors. The specific drugs assessed included ipilimumab, tremelimumab, nivolumab, pembrolizumab, atezolizumab, durvalumab, and avelumab.
A total of 32 trials that involved more than 20,000 patients reported HRs for death according to the patients’ sex. Thirty-four trials that involved more than 21,000 patients reported HRs for death according to patients’ age, and 30 trials that involved more than 19,000 patients reported HRs for death according to patients’ ECOG PS.
No significant differences in OS benefit were seen by cancer type, line of therapy, agent of immunotherapy, or intervention strategy, the investigators pointed out.
There were also no differences in survival benefit associated with immunotherapy vs control therapies for patients with an ECOG PS of 0 and an ECOG PS of 1 or greater. The OS benefit was 0.81 for those with an ECOG PS of 0 and 0.79 for those with an ECOG PS of 1 or greater.
Wang has disclosed no relevant financial relationships.
This article first appeared on Medscape.com .
The improvement in survival in many cancer types that is seen with immune checkpoint inhibitors (ICIs), when compared to control therapies, is not affected by the patient’s sex, age, or Eastern Cooperative Oncology Group (ECOG) performance status (PS), according to a new meta-analysis.
Therefore, treatment with these immunotherapies should not be withheld on the basis of these factors, the authors concluded.
Asked whether there have been such instances of withholding ICIs, lead author Yucai Wang, MD, PhD, Mayo Clinic, Rochester, Minnesota, told Medscape Medical News: “We did this study solely based on scientific questions we had and not because we were seeing any bias at the moment in the use of ICIs.
“And we saw that the survival benefits were very similar across all of the categories [we analyzed], with a survival benefit of about 20% from immunotherapy across the board, which is clinically meaningful,” he added.
The study was published online August 7 in JAMA Network Open.
“The comparable survival advantage between patients of different sex, age, and ECOG PS may encourage more patients to receive ICI treatment regardless of cancer types, lines of therapy, agents of immunotherapy, and intervention therapies,” the authors commented.
Wang noted that there have been conflicting reports in the literature suggesting that male patients may benefit more from immunotherapy than female patients and that older patients may benefit more from the same treatment than younger patients.
However, there are also suggestions in the literature that women experience a stronger immune response than men and that, with aging, the immune system generally undergoes immunosenescence.
In addition, the PS of oncology patients has been implicated in how well patients respond to immunotherapy.
Wang noted that the findings of past studies have contradicted each other.
Findings of the Meta-Analysis
The meta-analysis included 37 randomized clinical trials that involved a total of 23,760 patients with a variety of advanced cancers. “Most of the trials were phase 3 (n = 34) and conduced for subsequent lines of therapy (n = 22),” the authors explained.
The most common cancers treated with an ICI were non–small cell lung cancer and melanoma.
Pooled overall survival (OS) hazard ratios (HRs) were calculated on the basis of sex, age (younger than 65 years and 65 years and older), and an ECOG PS of 0 and 1 or higher.
Responses were stratified on the basis of cancer type, line of therapy, the ICI used, and the immunotherapy strategy used in the ICI arm.
Most of the drugs evaluated were PD-1 and PD-L1 inhibitors. The specific drugs assessed included ipilimumab, tremelimumab, nivolumab, pembrolizumab, atezolizumab, durvalumab, and avelumab.
A total of 32 trials that involved more than 20,000 patients reported HRs for death according to the patients’ sex. Thirty-four trials that involved more than 21,000 patients reported HRs for death according to patients’ age, and 30 trials that involved more than 19,000 patients reported HRs for death according to patients’ ECOG PS.
No significant differences in OS benefit were seen by cancer type, line of therapy, agent of immunotherapy, or intervention strategy, the investigators pointed out.
There were also no differences in survival benefit associated with immunotherapy vs control therapies for patients with an ECOG PS of 0 and an ECOG PS of 1 or greater. The OS benefit was 0.81 for those with an ECOG PS of 0 and 0.79 for those with an ECOG PS of 1 or greater.
Wang has disclosed no relevant financial relationships.
This article first appeared on Medscape.com .
Aspirin may accelerate cancer progression in older adults
Aspirin may accelerate the progression of advanced cancers and lead to an earlier death as a result, new data from the ASPREE study suggest.

The results showed that patients 65 years and older who started taking daily low-dose aspirin had a 19% higher chance of being diagnosed with metastatic cancer, a 22% higher chance of being diagnosed with a stage 4 tumor, and a 31% increased risk of death from stage 4 cancer, when compared with patients who took a placebo.
John J. McNeil, MBBS, PhD, of Monash University in Melbourne, Australia, and colleagues detailed these findings in the Journal of the National Cancer Institute.
“If confirmed, the clinical implications of these findings could be important for the use of aspirin in an older population,” the authors wrote.
When results of the ASPREE study were first reported in 2018, they “raised important concerns,” Ernest Hawk, MD, and Karen Colbert Maresso wrote in an editorial related to the current publication.
“Unlike ARRIVE, ASCEND, and nearly all prior primary prevention CVD [cardiovascular disease] trials of aspirin, ASPREE surprisingly demonstrated increased all-cause mortality in the aspirin group, which appeared to be driven largely by an increase in cancer-related deaths,” wrote the editorialists, who are both from the University of Texas MD Anderson Cancer Center in Houston.
Even though the ASPREE investigators have now taken a deeper dive into their data, the findings “neither explain nor alleviate the concerns raised by the initial ASPREE report,” the editorialists noted.
ASPREE design and results
ASPREE is a multicenter, double-blind trial of 19,114 older adults living in Australia (n = 16,703) or the United States (n = 2,411). Most patients were 70 years or older at baseline. However, the U.S. group also included patients 65 years and older who were racial/ethnic minorities (n = 564).
Patients were randomized to receive 100 mg of enteric-coated aspirin daily (n = 9,525) or matching placebo (n = 9,589) from March 2010 through December 2014.
At inclusion, all participants were free from cardiovascular disease, dementia, or physical disability. A previous history of cancer was not used to exclude participants, and 19.1% of patients had cancer at randomization. Most patients (89%) had not used aspirin regularly before entering the trial.
At a median follow-up of 4.7 years, there were 981 incident cancer events in the aspirin-treated group and 952 in the placebo-treated group, with an overall incident cancer rate of 10.1%.
Of the 1,933 patients with newly diagnosed cancer, 65.7% had a localized cancer, 18.8% had a new metastatic cancer, 5.8% had metastatic disease from an existing cancer, and 9.7% had a new hematologic or lymphatic cancer.
A quarter of cancer patients (n = 495) died as a result of their malignancy, with 52 dying from a cancer they already had at randomization.
Aspirin was not associated with the risk of first incident cancer diagnosis or incident localized cancer diagnosis. The hazard ratios were 1.04 for all incident cancers (95% confidence interval, 0.95-1.14) and 0.99 for incident localized cancers (95% CI, 0.89-1.11).
However, aspirin was associated with an increased risk of metastatic cancer and cancer presenting at stage 4. The HR for metastatic cancer was 1.19 (95% CI, 1.00-1.43), and the HR for newly diagnosed stage 4 cancer was 1.22 (95% CI, 1.02-1.45).
Furthermore, “an increased progression to death was observed amongst those randomized to aspirin, regardless of whether the initial cancer presentation had been localized or metastatic,” the investigators wrote.
The HRs for death were 1.35 for all cancers (95% CI, 1.13-1.61), 1.47 for localized cancers (95% CI, 1.07-2.02), and 1.30 for metastatic cancers (95% CI, 1.03-1.63).
“Deaths were particularly high among those on aspirin who were diagnosed with advanced solid cancers,” study author Andrew Chan, MD, of Massachusetts General Hospital in Boston, said in a press statement.
Indeed, HRs for death in patients with solid tumors presenting at stage 3 and 4 were a respective 2.11 (95% CI, 1.03-4.33) and 1.31 (95% CI, 1.04-1.64). This suggests a possible adverse effect of aspirin on the growth of cancers once they have already developed in older adults, Dr. Chan said.
Where does that leave aspirin for cancer prevention?
“Although these results suggest that we should be cautious about starting aspirin therapy in otherwise healthy older adults, this does not mean that individuals who are already taking aspirin – particularly if they began taking it at a younger age – should stop their aspirin regimen,” Dr. Chan said.
There are decades of data supporting the use of daily aspirin to prevent multiple cancer types, particularly colorectal cancer, in individuals under the age of 70 years. In a recent meta-analysis, for example, regular aspirin use was linked to a 27% reduced risk for colorectal cancer, a 33% reduced risk for squamous cell esophageal cancer, a 39% decreased risk for adenocarcinoma of the esophagus and gastric cardia, a 36% decreased risk for stomach cancer, a 38% decreased risk for hepatobiliary tract cancer, and a 22% decreased risk for pancreatic cancer.
While these figures are mostly based on observational and case-control studies, it “reaffirms the fact that, overall, when you look at all of the ages, that there is still a benefit of aspirin for cancer,” John Cuzick, PhD, of Queen Mary University of London (England), said in an interview.
In fact, the meta-analysis goes as far as suggesting that perhaps the dose of aspirin being used is too low, with the authors noting that there was a 35% risk reduction in colorectal cancer with a dose of 325 mg daily. That’s a new finding, Dr. Cuzick said.
He noted that the ASPREE study largely consists of patients 70 years of age or older, and the authors “draw some conclusions which we can’t ignore about potential safety.”
One of the safety concerns is the increased risk for gastrointestinal bleeding, which is why Dr. Cuzick and colleagues previously recommended caution in the use of aspirin to prevent cancer in elderly patients. The group published a study in 2015 that suggested a benefit of taking aspirin daily for 5-10 years in patients aged 50-65 years, but the risk/benefit ratio was unclear for patients 70 years and older.
The ASPREE data now add to those uncertainties and suggest “there may be some side effects that we do not understand,” Dr. Cuzick said.
“I’m still optimistic that aspirin is going to be important for cancer prevention, but probably focusing on ages 50-70,” he added. “[The ASPREE data] reinforce the caution that we have to take in terms of trying to understand what the side effects are and what’s going on at these older ages.”
Dr. Cuzick is currently leading the AsCaP Project, an international effort to better understand why aspirin might work in preventing some cancer types but not others. AsCaP is supported by Cancer Research UK and also includes Dr. Chan among the researchers attempting to find out which patients may benefit the most from aspirin and which may be at greater risk of adverse effects.
The ASPREE trial was funded by grants from the National Institute on Aging, the National Cancer Institute, the National Health and Medical Research Council of Australia, Monash University, and the Victorian Cancer Agency. Several ASPREE investigators disclosed financial relationships with Bayer Pharma. The editorialists had no conflicts of interest. Dr. Cuzick has been an advisory board member for Bayer in the past.
SOURCE: McNeil J et al. J Natl Cancer Inst. 2020 Aug 11. doi: 10.1093/jnci/djaa114.
Aspirin may accelerate the progression of advanced cancers and lead to an earlier death as a result, new data from the ASPREE study suggest.
The results showed that patients 65 years and older who started taking daily low-dose aspirin had a 19% higher chance of being diagnosed with metastatic cancer, a 22% higher chance of being diagnosed with a stage 4 tumor, and a 31% increased risk of death from stage 4 cancer, when compared with patients who took a placebo.
John J. McNeil, MBBS, PhD, of Monash University in Melbourne, Australia, and colleagues detailed these findings in the Journal of the National Cancer Institute.
“If confirmed, the clinical implications of these findings could be important for the use of aspirin in an older population,” the authors wrote.
When results of the ASPREE study were first reported in 2018, they “raised important concerns,” Ernest Hawk, MD, and Karen Colbert Maresso wrote in an editorial related to the current publication.
“Unlike ARRIVE, ASCEND, and nearly all prior primary prevention CVD [cardiovascular disease] trials of aspirin, ASPREE surprisingly demonstrated increased all-cause mortality in the aspirin group, which appeared to be driven largely by an increase in cancer-related deaths,” wrote the editorialists, who are both from the University of Texas MD Anderson Cancer Center in Houston.
Even though the ASPREE investigators have now taken a deeper dive into their data, the findings “neither explain nor alleviate the concerns raised by the initial ASPREE report,” the editorialists noted.
ASPREE design and results
ASPREE is a multicenter, double-blind trial of 19,114 older adults living in Australia (n = 16,703) or the United States (n = 2,411). Most patients were 70 years or older at baseline. However, the U.S. group also included patients 65 years and older who were racial/ethnic minorities (n = 564).
Patients were randomized to receive 100 mg of enteric-coated aspirin daily (n = 9,525) or matching placebo (n = 9,589) from March 2010 through December 2014.
At inclusion, all participants were free from cardiovascular disease, dementia, or physical disability. A previous history of cancer was not used to exclude participants, and 19.1% of patients had cancer at randomization. Most patients (89%) had not used aspirin regularly before entering the trial.
At a median follow-up of 4.7 years, there were 981 incident cancer events in the aspirin-treated group and 952 in the placebo-treated group, with an overall incident cancer rate of 10.1%.
Of the 1,933 patients with newly diagnosed cancer, 65.7% had a localized cancer, 18.8% had a new metastatic cancer, 5.8% had metastatic disease from an existing cancer, and 9.7% had a new hematologic or lymphatic cancer.
A quarter of cancer patients (n = 495) died as a result of their malignancy, with 52 dying from a cancer they already had at randomization.
Aspirin was not associated with the risk of first incident cancer diagnosis or incident localized cancer diagnosis. The hazard ratios were 1.04 for all incident cancers (95% confidence interval, 0.95-1.14) and 0.99 for incident localized cancers (95% CI, 0.89-1.11).
However, aspirin was associated with an increased risk of metastatic cancer and cancer presenting at stage 4. The HR for metastatic cancer was 1.19 (95% CI, 1.00-1.43), and the HR for newly diagnosed stage 4 cancer was 1.22 (95% CI, 1.02-1.45).
Furthermore, “an increased progression to death was observed amongst those randomized to aspirin, regardless of whether the initial cancer presentation had been localized or metastatic,” the investigators wrote.
The HRs for death were 1.35 for all cancers (95% CI, 1.13-1.61), 1.47 for localized cancers (95% CI, 1.07-2.02), and 1.30 for metastatic cancers (95% CI, 1.03-1.63).
“Deaths were particularly high among those on aspirin who were diagnosed with advanced solid cancers,” study author Andrew Chan, MD, of Massachusetts General Hospital in Boston, said in a press statement.
Indeed, HRs for death in patients with solid tumors presenting at stage 3 and 4 were a respective 2.11 (95% CI, 1.03-4.33) and 1.31 (95% CI, 1.04-1.64). This suggests a possible adverse effect of aspirin on the growth of cancers once they have already developed in older adults, Dr. Chan said.
Where does that leave aspirin for cancer prevention?
“Although these results suggest that we should be cautious about starting aspirin therapy in otherwise healthy older adults, this does not mean that individuals who are already taking aspirin – particularly if they began taking it at a younger age – should stop their aspirin regimen,” Dr. Chan said.
There are decades of data supporting the use of daily aspirin to prevent multiple cancer types, particularly colorectal cancer, in individuals under the age of 70 years. In a recent meta-analysis, for example, regular aspirin use was linked to a 27% reduced risk for colorectal cancer, a 33% reduced risk for squamous cell esophageal cancer, a 39% decreased risk for adenocarcinoma of the esophagus and gastric cardia, a 36% decreased risk for stomach cancer, a 38% decreased risk for hepatobiliary tract cancer, and a 22% decreased risk for pancreatic cancer.
While these figures are mostly based on observational and case-control studies, it “reaffirms the fact that, overall, when you look at all of the ages, that there is still a benefit of aspirin for cancer,” John Cuzick, PhD, of Queen Mary University of London (England), said in an interview.
In fact, the meta-analysis goes as far as suggesting that perhaps the dose of aspirin being used is too low, with the authors noting that there was a 35% risk reduction in colorectal cancer with a dose of 325 mg daily. That’s a new finding, Dr. Cuzick said.
He noted that the ASPREE study largely consists of patients 70 years of age or older, and the authors “draw some conclusions which we can’t ignore about potential safety.”
One of the safety concerns is the increased risk for gastrointestinal bleeding, which is why Dr. Cuzick and colleagues previously recommended caution in the use of aspirin to prevent cancer in elderly patients. The group published a study in 2015 that suggested a benefit of taking aspirin daily for 5-10 years in patients aged 50-65 years, but the risk/benefit ratio was unclear for patients 70 years and older.
The ASPREE data now add to those uncertainties and suggest “there may be some side effects that we do not understand,” Dr. Cuzick said.
“I’m still optimistic that aspirin is going to be important for cancer prevention, but probably focusing on ages 50-70,” he added. “[The ASPREE data] reinforce the caution that we have to take in terms of trying to understand what the side effects are and what’s going on at these older ages.”
Dr. Cuzick is currently leading the AsCaP Project, an international effort to better understand why aspirin might work in preventing some cancer types but not others. AsCaP is supported by Cancer Research UK and also includes Dr. Chan among the researchers attempting to find out which patients may benefit the most from aspirin and which may be at greater risk of adverse effects.
The ASPREE trial was funded by grants from the National Institute on Aging, the National Cancer Institute, the National Health and Medical Research Council of Australia, Monash University, and the Victorian Cancer Agency. Several ASPREE investigators disclosed financial relationships with Bayer Pharma. The editorialists had no conflicts of interest. Dr. Cuzick has been an advisory board member for Bayer in the past.
SOURCE: McNeil J et al. J Natl Cancer Inst. 2020 Aug 11. doi: 10.1093/jnci/djaa114.
Aspirin may accelerate the progression of advanced cancers and lead to an earlier death as a result, new data from the ASPREE study suggest.
The results showed that patients 65 years and older who started taking daily low-dose aspirin had a 19% higher chance of being diagnosed with metastatic cancer, a 22% higher chance of being diagnosed with a stage 4 tumor, and a 31% increased risk of death from stage 4 cancer, when compared with patients who took a placebo.
John J. McNeil, MBBS, PhD, of Monash University in Melbourne, Australia, and colleagues detailed these findings in the Journal of the National Cancer Institute.
“If confirmed, the clinical implications of these findings could be important for the use of aspirin in an older population,” the authors wrote.
When results of the ASPREE study were first reported in 2018, they “raised important concerns,” Ernest Hawk, MD, and Karen Colbert Maresso wrote in an editorial related to the current publication.
“Unlike ARRIVE, ASCEND, and nearly all prior primary prevention CVD [cardiovascular disease] trials of aspirin, ASPREE surprisingly demonstrated increased all-cause mortality in the aspirin group, which appeared to be driven largely by an increase in cancer-related deaths,” wrote the editorialists, who are both from the University of Texas MD Anderson Cancer Center in Houston.
Even though the ASPREE investigators have now taken a deeper dive into their data, the findings “neither explain nor alleviate the concerns raised by the initial ASPREE report,” the editorialists noted.
ASPREE design and results
ASPREE is a multicenter, double-blind trial of 19,114 older adults living in Australia (n = 16,703) or the United States (n = 2,411). Most patients were 70 years or older at baseline. However, the U.S. group also included patients 65 years and older who were racial/ethnic minorities (n = 564).
Patients were randomized to receive 100 mg of enteric-coated aspirin daily (n = 9,525) or matching placebo (n = 9,589) from March 2010 through December 2014.
At inclusion, all participants were free from cardiovascular disease, dementia, or physical disability. A previous history of cancer was not used to exclude participants, and 19.1% of patients had cancer at randomization. Most patients (89%) had not used aspirin regularly before entering the trial.
At a median follow-up of 4.7 years, there were 981 incident cancer events in the aspirin-treated group and 952 in the placebo-treated group, with an overall incident cancer rate of 10.1%.
Of the 1,933 patients with newly diagnosed cancer, 65.7% had a localized cancer, 18.8% had a new metastatic cancer, 5.8% had metastatic disease from an existing cancer, and 9.7% had a new hematologic or lymphatic cancer.
A quarter of cancer patients (n = 495) died as a result of their malignancy, with 52 dying from a cancer they already had at randomization.
Aspirin was not associated with the risk of first incident cancer diagnosis or incident localized cancer diagnosis. The hazard ratios were 1.04 for all incident cancers (95% confidence interval, 0.95-1.14) and 0.99 for incident localized cancers (95% CI, 0.89-1.11).
However, aspirin was associated with an increased risk of metastatic cancer and cancer presenting at stage 4. The HR for metastatic cancer was 1.19 (95% CI, 1.00-1.43), and the HR for newly diagnosed stage 4 cancer was 1.22 (95% CI, 1.02-1.45).
Furthermore, “an increased progression to death was observed amongst those randomized to aspirin, regardless of whether the initial cancer presentation had been localized or metastatic,” the investigators wrote.
The HRs for death were 1.35 for all cancers (95% CI, 1.13-1.61), 1.47 for localized cancers (95% CI, 1.07-2.02), and 1.30 for metastatic cancers (95% CI, 1.03-1.63).
“Deaths were particularly high among those on aspirin who were diagnosed with advanced solid cancers,” study author Andrew Chan, MD, of Massachusetts General Hospital in Boston, said in a press statement.
Indeed, HRs for death in patients with solid tumors presenting at stage 3 and 4 were a respective 2.11 (95% CI, 1.03-4.33) and 1.31 (95% CI, 1.04-1.64). This suggests a possible adverse effect of aspirin on the growth of cancers once they have already developed in older adults, Dr. Chan said.
Where does that leave aspirin for cancer prevention?
“Although these results suggest that we should be cautious about starting aspirin therapy in otherwise healthy older adults, this does not mean that individuals who are already taking aspirin – particularly if they began taking it at a younger age – should stop their aspirin regimen,” Dr. Chan said.
There are decades of data supporting the use of daily aspirin to prevent multiple cancer types, particularly colorectal cancer, in individuals under the age of 70 years. In a recent meta-analysis, for example, regular aspirin use was linked to a 27% reduced risk for colorectal cancer, a 33% reduced risk for squamous cell esophageal cancer, a 39% decreased risk for adenocarcinoma of the esophagus and gastric cardia, a 36% decreased risk for stomach cancer, a 38% decreased risk for hepatobiliary tract cancer, and a 22% decreased risk for pancreatic cancer.
While these figures are mostly based on observational and case-control studies, it “reaffirms the fact that, overall, when you look at all of the ages, that there is still a benefit of aspirin for cancer,” John Cuzick, PhD, of Queen Mary University of London (England), said in an interview.
In fact, the meta-analysis goes as far as suggesting that perhaps the dose of aspirin being used is too low, with the authors noting that there was a 35% risk reduction in colorectal cancer with a dose of 325 mg daily. That’s a new finding, Dr. Cuzick said.
He noted that the ASPREE study largely consists of patients 70 years of age or older, and the authors “draw some conclusions which we can’t ignore about potential safety.”
One of the safety concerns is the increased risk for gastrointestinal bleeding, which is why Dr. Cuzick and colleagues previously recommended caution in the use of aspirin to prevent cancer in elderly patients. The group published a study in 2015 that suggested a benefit of taking aspirin daily for 5-10 years in patients aged 50-65 years, but the risk/benefit ratio was unclear for patients 70 years and older.
The ASPREE data now add to those uncertainties and suggest “there may be some side effects that we do not understand,” Dr. Cuzick said.
“I’m still optimistic that aspirin is going to be important for cancer prevention, but probably focusing on ages 50-70,” he added. “[The ASPREE data] reinforce the caution that we have to take in terms of trying to understand what the side effects are and what’s going on at these older ages.”
Dr. Cuzick is currently leading the AsCaP Project, an international effort to better understand why aspirin might work in preventing some cancer types but not others. AsCaP is supported by Cancer Research UK and also includes Dr. Chan among the researchers attempting to find out which patients may benefit the most from aspirin and which may be at greater risk of adverse effects.
The ASPREE trial was funded by grants from the National Institute on Aging, the National Cancer Institute, the National Health and Medical Research Council of Australia, Monash University, and the Victorian Cancer Agency. Several ASPREE investigators disclosed financial relationships with Bayer Pharma. The editorialists had no conflicts of interest. Dr. Cuzick has been an advisory board member for Bayer in the past.
SOURCE: McNeil J et al. J Natl Cancer Inst. 2020 Aug 11. doi: 10.1093/jnci/djaa114.
FROM JOURNAL OF THE NATIONAL CANCER INSTITUTE
Tailored messaging needed to get cancer screening back on track
In late June, Lisa Richardson, MD, emerged from Atlanta, Georgia’s initial COVID-19 lockdown, and “got back out there” for some overdue doctor’s appointments, including a mammogram.
The mammogram was a particular priority for her, since she is director of the CDC’s Division of Cancer Prevention and Control. But she knows that cancer screening is going to be a much tougher sell for the average person going forward in the pandemic era.
“It really is a challenge trying to get people to feel comfortable coming back in to be screened,” she said. Richardson was speaking recently at the AACR virtual meeting: COVID-19 and Cancer, a virtual symposium on cancer prevention and early detection in the COVID-19 pandemic organized by the American Association for Cancer Research.
While health service shutdowns and stay-at-home orders forced the country’s initial precipitous decline in cancer screening, fear of contracting COVID-19 is a big part of what is preventing patients from returning.
“We’ve known even pre-pandemic that people were hesitant to do cancer screening and in some ways this has really given them an out to say, ‘Well, I’m going to hold off on that colonoscopy,’ ” Amy Leader, MD, from Thomas Jefferson University’s Kimmel Cancer Center in Philadelphia, Pennsylvania, said during the symposium.
Estimating the pandemic’s impact on cancer care
While the impact of the pandemic on cancer can only be estimated at the moment, the prospects are already daunting, said Richardson, speculating that the hard-won 26% drop in cancer mortality over the past two decades “may be put on hold or reversed” by COVID-19.
There could be as many as 10,000 excess deaths in the US from colorectal and breast cancer alone because of COVID-19 delays, predicted Norman E. Sharpless, director of the US National Cancer Institute in Bethesda, Maryland.
But even Sharpless acknowledges that his modeling gives a conservative estimate, “as it does not consider other cancer types, it does not account for the additional nonlethal morbidity from upstaging, and it assumes a moderate disruption in care that completely resolves after 6 months.”
With still no end to the pandemic in sight, the true scope of cancer screening and treatment disruptions will take a long time to assess, but several studies presented during the symposium revealed some early indications.
A national survey launched in mid-May, which involved 534 women either diagnosed with breast cancer or undergoing screening or diagnostic evaluation for it, found that delays in screening were reported by 31.7% of those with breast cancer, and 26.7% of those without. Additionally, 21% of those on active treatment for breast cancer reported treatment delays.
“It’s going to be really important to implement strategies to help patients return to care ... creating a culture and a feeling of safety among patients and communicating through the uncertainty that exists in the pandemic,” said study investigator Erica T. Warner, ScD MPH, from Massachusetts General Hospital, Boston.
Screening for prostate cancer (via prostate-specific antigen testing) also declined, though not as dramatically as that for breast cancer, noted Mara Epstein, ScD, from The Meyers Primary Care Institute, University of Massachusetts Medical School, Worcester. Her study at a large healthcare provider group compared rates of both screening and diagnostic mammographies, and also PSA testing, as well as breast and prostate biopsies in the first five months of 2020 vs the same months in 2019.
While a decrease from 2019 to 2020 was seen in all procedures over the entire study period, the greatest decline was seen in April for screening mammography (down 98%), and tomosynthesis (down 96%), as well as PSA testing (down 83%), she said.
More recent figures are hard to come by, but a recent weekly survey from the Primary Care Collaborative shows 46% of practices are offering preventive and chronic care management visits, but patients are not scheduling them, and 44% report that in-person visit volume is between 30%-50% below normal over the last 4 weeks.
Will COVID-19 exacerbate racial disparities in cancer?
Neither of the studies presented at the symposium analyzed cancer care disruptions by race, but there was concern among some panelists that cancer care disparities that existed before the pandemic will be magnified further.
“Over the next several months and into the next year there’s going to be some catch-up in screening and treatment, and one of my concerns is minority and underserved populations will not partake in that catch-up the way many middle-class Americans will,” said Otis Brawley, MD, from Johns Hopkins University, Baltimore, Maryland.
There is ample evidence that minority populations have been disproportionately hit by COVID-19, job losses, and lost health insurance, said the CDC’s Richardson, and all these factors could widen the cancer gap.
“It’s not a race thing, it’s a ‘what do you do thing,’ and an access to care thing, and what your socioeconomic status is,” Richardson said in an interview. “People who didn’t have sick leave before the pandemic still don’t have sick leave; if they didn’t have time to get their mammogram they still don’t have time.”
But she acknowledges that evidence is still lacking. Could some minority populations actually be less fearful of medical encounters because their work has already prevented them from sheltering in place? “It could go either way,” she said. “They might be less wary of venturing out into the clinic, but they also might reason that they’ve exposed themselves enough already at work and don’t want any additional exposure.”
In that regard, Richardson suggests population-specific messaging will be an important way of communicating with under-served populations to restart screening.
“We’re struggling at CDC with how to develop messages that resonate within different communities, because we’re missing the point of actually speaking to people within their culture and within the places that they live,” she said. “Just saying the same thing and putting a black face on it is not going to make a difference; you actually have to speak the language of the people you’re trying to reach — the same message in different packages.”
To that end, even before the pandemic, the CDC supported the development of Make It Your Own, a website that uses “evidence-based strategies” to assist healthcare organizations in customizing health information “by race, ethnicity, age, gender and location”, and target messages to “specific populations, cultural groups and languages”.
But Mass General’s Warner says she’s not sure she would argue for messages to be tailored by race, “at least not without evidence that values and priorities regarding returning to care differ between racial/ethnic groups.”
“Tailoring in the absence of data requires assumptions that may or may not be correct and ignores within-group heterogeneity,” Warner told Medscape Medical News. “However, I do believe that messaging about return to cancer screening and care should be multifaceted and use diverse imagery. This recognizes that some messages will resonate more or less with individuals based on their own characteristics, of which race may be one.”
Warner does believe in the power of tailored messaging though. “Part of the onus for healthcare institutions and providers is to make some decisions about who it is really important to bring back in soonest,” she said.
“Those are the ones we want to prioritize, as opposed to those who we want to get back into care but we don’t need to get them in right now,” Warner emphasized. “As they are balancing all the needs of their family and their community and their other needs, messaging that adds additional stress, worry, anxiety and shame is not what we want to do. So really we need to distinguish between these populations, identify the priorities, hit the hard message to people who really need it now, and encourage others to come back in as they can.”
Building trust
All the panelists agreed that building trust with the public will be key to getting cancer care back on track.
“I don’t think anyone trusts the healthcare community right now, but we already had this baseline distrust of healthcare among many minority communities, and now with COVID-19, the African American community in particular is seeing people go into the hospital and never come back,” said Richardson.
For Warner, the onus really falls on healthcare institutions. “We have to be proactive and not leave the burden of deciding when and how to return to care up to patients,” she said.
“What we need to focus on as much as possible is to get people to realize it is safe to come see the doctor,” said Johns Hopkins oncologist Brawley. “We have to make it safe for them to come see us, and then we have to convince them it is safe to come see us.”
Venturing out to her mammography appointment in early June, Richardson said she felt safe. “Everything was just the way it was supposed to be, everyone was masked, everyone was washing their hands,” she said.
Yet, by mid-June she had contracted COVID-19. “I don’t know where I got it,” she said. “No matter how careful you are, understand that if you’re in a total red spot, as I am, you can just get it.”
This article first appeared on Medscape.com.
In late June, Lisa Richardson, MD, emerged from Atlanta, Georgia’s initial COVID-19 lockdown, and “got back out there” for some overdue doctor’s appointments, including a mammogram.
The mammogram was a particular priority for her, since she is director of the CDC’s Division of Cancer Prevention and Control. But she knows that cancer screening is going to be a much tougher sell for the average person going forward in the pandemic era.
“It really is a challenge trying to get people to feel comfortable coming back in to be screened,” she said. Richardson was speaking recently at the AACR virtual meeting: COVID-19 and Cancer, a virtual symposium on cancer prevention and early detection in the COVID-19 pandemic organized by the American Association for Cancer Research.
While health service shutdowns and stay-at-home orders forced the country’s initial precipitous decline in cancer screening, fear of contracting COVID-19 is a big part of what is preventing patients from returning.
“We’ve known even pre-pandemic that people were hesitant to do cancer screening and in some ways this has really given them an out to say, ‘Well, I’m going to hold off on that colonoscopy,’ ” Amy Leader, MD, from Thomas Jefferson University’s Kimmel Cancer Center in Philadelphia, Pennsylvania, said during the symposium.
Estimating the pandemic’s impact on cancer care
While the impact of the pandemic on cancer can only be estimated at the moment, the prospects are already daunting, said Richardson, speculating that the hard-won 26% drop in cancer mortality over the past two decades “may be put on hold or reversed” by COVID-19.
There could be as many as 10,000 excess deaths in the US from colorectal and breast cancer alone because of COVID-19 delays, predicted Norman E. Sharpless, director of the US National Cancer Institute in Bethesda, Maryland.
But even Sharpless acknowledges that his modeling gives a conservative estimate, “as it does not consider other cancer types, it does not account for the additional nonlethal morbidity from upstaging, and it assumes a moderate disruption in care that completely resolves after 6 months.”
With still no end to the pandemic in sight, the true scope of cancer screening and treatment disruptions will take a long time to assess, but several studies presented during the symposium revealed some early indications.
A national survey launched in mid-May, which involved 534 women either diagnosed with breast cancer or undergoing screening or diagnostic evaluation for it, found that delays in screening were reported by 31.7% of those with breast cancer, and 26.7% of those without. Additionally, 21% of those on active treatment for breast cancer reported treatment delays.
“It’s going to be really important to implement strategies to help patients return to care ... creating a culture and a feeling of safety among patients and communicating through the uncertainty that exists in the pandemic,” said study investigator Erica T. Warner, ScD MPH, from Massachusetts General Hospital, Boston.
Screening for prostate cancer (via prostate-specific antigen testing) also declined, though not as dramatically as that for breast cancer, noted Mara Epstein, ScD, from The Meyers Primary Care Institute, University of Massachusetts Medical School, Worcester. Her study at a large healthcare provider group compared rates of both screening and diagnostic mammographies, and also PSA testing, as well as breast and prostate biopsies in the first five months of 2020 vs the same months in 2019.
While a decrease from 2019 to 2020 was seen in all procedures over the entire study period, the greatest decline was seen in April for screening mammography (down 98%), and tomosynthesis (down 96%), as well as PSA testing (down 83%), she said.
More recent figures are hard to come by, but a recent weekly survey from the Primary Care Collaborative shows 46% of practices are offering preventive and chronic care management visits, but patients are not scheduling them, and 44% report that in-person visit volume is between 30%-50% below normal over the last 4 weeks.
Will COVID-19 exacerbate racial disparities in cancer?
Neither of the studies presented at the symposium analyzed cancer care disruptions by race, but there was concern among some panelists that cancer care disparities that existed before the pandemic will be magnified further.
“Over the next several months and into the next year there’s going to be some catch-up in screening and treatment, and one of my concerns is minority and underserved populations will not partake in that catch-up the way many middle-class Americans will,” said Otis Brawley, MD, from Johns Hopkins University, Baltimore, Maryland.
There is ample evidence that minority populations have been disproportionately hit by COVID-19, job losses, and lost health insurance, said the CDC’s Richardson, and all these factors could widen the cancer gap.
“It’s not a race thing, it’s a ‘what do you do thing,’ and an access to care thing, and what your socioeconomic status is,” Richardson said in an interview. “People who didn’t have sick leave before the pandemic still don’t have sick leave; if they didn’t have time to get their mammogram they still don’t have time.”
But she acknowledges that evidence is still lacking. Could some minority populations actually be less fearful of medical encounters because their work has already prevented them from sheltering in place? “It could go either way,” she said. “They might be less wary of venturing out into the clinic, but they also might reason that they’ve exposed themselves enough already at work and don’t want any additional exposure.”
In that regard, Richardson suggests population-specific messaging will be an important way of communicating with under-served populations to restart screening.
“We’re struggling at CDC with how to develop messages that resonate within different communities, because we’re missing the point of actually speaking to people within their culture and within the places that they live,” she said. “Just saying the same thing and putting a black face on it is not going to make a difference; you actually have to speak the language of the people you’re trying to reach — the same message in different packages.”
To that end, even before the pandemic, the CDC supported the development of Make It Your Own, a website that uses “evidence-based strategies” to assist healthcare organizations in customizing health information “by race, ethnicity, age, gender and location”, and target messages to “specific populations, cultural groups and languages”.
But Mass General’s Warner says she’s not sure she would argue for messages to be tailored by race, “at least not without evidence that values and priorities regarding returning to care differ between racial/ethnic groups.”
“Tailoring in the absence of data requires assumptions that may or may not be correct and ignores within-group heterogeneity,” Warner told Medscape Medical News. “However, I do believe that messaging about return to cancer screening and care should be multifaceted and use diverse imagery. This recognizes that some messages will resonate more or less with individuals based on their own characteristics, of which race may be one.”
Warner does believe in the power of tailored messaging though. “Part of the onus for healthcare institutions and providers is to make some decisions about who it is really important to bring back in soonest,” she said.
“Those are the ones we want to prioritize, as opposed to those who we want to get back into care but we don’t need to get them in right now,” Warner emphasized. “As they are balancing all the needs of their family and their community and their other needs, messaging that adds additional stress, worry, anxiety and shame is not what we want to do. So really we need to distinguish between these populations, identify the priorities, hit the hard message to people who really need it now, and encourage others to come back in as they can.”
Building trust
All the panelists agreed that building trust with the public will be key to getting cancer care back on track.
“I don’t think anyone trusts the healthcare community right now, but we already had this baseline distrust of healthcare among many minority communities, and now with COVID-19, the African American community in particular is seeing people go into the hospital and never come back,” said Richardson.
For Warner, the onus really falls on healthcare institutions. “We have to be proactive and not leave the burden of deciding when and how to return to care up to patients,” she said.
“What we need to focus on as much as possible is to get people to realize it is safe to come see the doctor,” said Johns Hopkins oncologist Brawley. “We have to make it safe for them to come see us, and then we have to convince them it is safe to come see us.”
Venturing out to her mammography appointment in early June, Richardson said she felt safe. “Everything was just the way it was supposed to be, everyone was masked, everyone was washing their hands,” she said.
Yet, by mid-June she had contracted COVID-19. “I don’t know where I got it,” she said. “No matter how careful you are, understand that if you’re in a total red spot, as I am, you can just get it.”
This article first appeared on Medscape.com.
In late June, Lisa Richardson, MD, emerged from Atlanta, Georgia’s initial COVID-19 lockdown, and “got back out there” for some overdue doctor’s appointments, including a mammogram.
The mammogram was a particular priority for her, since she is director of the CDC’s Division of Cancer Prevention and Control. But she knows that cancer screening is going to be a much tougher sell for the average person going forward in the pandemic era.
“It really is a challenge trying to get people to feel comfortable coming back in to be screened,” she said. Richardson was speaking recently at the AACR virtual meeting: COVID-19 and Cancer, a virtual symposium on cancer prevention and early detection in the COVID-19 pandemic organized by the American Association for Cancer Research.
While health service shutdowns and stay-at-home orders forced the country’s initial precipitous decline in cancer screening, fear of contracting COVID-19 is a big part of what is preventing patients from returning.
“We’ve known even pre-pandemic that people were hesitant to do cancer screening and in some ways this has really given them an out to say, ‘Well, I’m going to hold off on that colonoscopy,’ ” Amy Leader, MD, from Thomas Jefferson University’s Kimmel Cancer Center in Philadelphia, Pennsylvania, said during the symposium.
Estimating the pandemic’s impact on cancer care
While the impact of the pandemic on cancer can only be estimated at the moment, the prospects are already daunting, said Richardson, speculating that the hard-won 26% drop in cancer mortality over the past two decades “may be put on hold or reversed” by COVID-19.
There could be as many as 10,000 excess deaths in the US from colorectal and breast cancer alone because of COVID-19 delays, predicted Norman E. Sharpless, director of the US National Cancer Institute in Bethesda, Maryland.
But even Sharpless acknowledges that his modeling gives a conservative estimate, “as it does not consider other cancer types, it does not account for the additional nonlethal morbidity from upstaging, and it assumes a moderate disruption in care that completely resolves after 6 months.”
With still no end to the pandemic in sight, the true scope of cancer screening and treatment disruptions will take a long time to assess, but several studies presented during the symposium revealed some early indications.
A national survey launched in mid-May, which involved 534 women either diagnosed with breast cancer or undergoing screening or diagnostic evaluation for it, found that delays in screening were reported by 31.7% of those with breast cancer, and 26.7% of those without. Additionally, 21% of those on active treatment for breast cancer reported treatment delays.
“It’s going to be really important to implement strategies to help patients return to care ... creating a culture and a feeling of safety among patients and communicating through the uncertainty that exists in the pandemic,” said study investigator Erica T. Warner, ScD MPH, from Massachusetts General Hospital, Boston.
Screening for prostate cancer (via prostate-specific antigen testing) also declined, though not as dramatically as that for breast cancer, noted Mara Epstein, ScD, from The Meyers Primary Care Institute, University of Massachusetts Medical School, Worcester. Her study at a large healthcare provider group compared rates of both screening and diagnostic mammographies, and also PSA testing, as well as breast and prostate biopsies in the first five months of 2020 vs the same months in 2019.
While a decrease from 2019 to 2020 was seen in all procedures over the entire study period, the greatest decline was seen in April for screening mammography (down 98%), and tomosynthesis (down 96%), as well as PSA testing (down 83%), she said.
More recent figures are hard to come by, but a recent weekly survey from the Primary Care Collaborative shows 46% of practices are offering preventive and chronic care management visits, but patients are not scheduling them, and 44% report that in-person visit volume is between 30%-50% below normal over the last 4 weeks.
Will COVID-19 exacerbate racial disparities in cancer?
Neither of the studies presented at the symposium analyzed cancer care disruptions by race, but there was concern among some panelists that cancer care disparities that existed before the pandemic will be magnified further.
“Over the next several months and into the next year there’s going to be some catch-up in screening and treatment, and one of my concerns is minority and underserved populations will not partake in that catch-up the way many middle-class Americans will,” said Otis Brawley, MD, from Johns Hopkins University, Baltimore, Maryland.
There is ample evidence that minority populations have been disproportionately hit by COVID-19, job losses, and lost health insurance, said the CDC’s Richardson, and all these factors could widen the cancer gap.
“It’s not a race thing, it’s a ‘what do you do thing,’ and an access to care thing, and what your socioeconomic status is,” Richardson said in an interview. “People who didn’t have sick leave before the pandemic still don’t have sick leave; if they didn’t have time to get their mammogram they still don’t have time.”
But she acknowledges that evidence is still lacking. Could some minority populations actually be less fearful of medical encounters because their work has already prevented them from sheltering in place? “It could go either way,” she said. “They might be less wary of venturing out into the clinic, but they also might reason that they’ve exposed themselves enough already at work and don’t want any additional exposure.”
In that regard, Richardson suggests population-specific messaging will be an important way of communicating with under-served populations to restart screening.
“We’re struggling at CDC with how to develop messages that resonate within different communities, because we’re missing the point of actually speaking to people within their culture and within the places that they live,” she said. “Just saying the same thing and putting a black face on it is not going to make a difference; you actually have to speak the language of the people you’re trying to reach — the same message in different packages.”
To that end, even before the pandemic, the CDC supported the development of Make It Your Own, a website that uses “evidence-based strategies” to assist healthcare organizations in customizing health information “by race, ethnicity, age, gender and location”, and target messages to “specific populations, cultural groups and languages”.
But Mass General’s Warner says she’s not sure she would argue for messages to be tailored by race, “at least not without evidence that values and priorities regarding returning to care differ between racial/ethnic groups.”
“Tailoring in the absence of data requires assumptions that may or may not be correct and ignores within-group heterogeneity,” Warner told Medscape Medical News. “However, I do believe that messaging about return to cancer screening and care should be multifaceted and use diverse imagery. This recognizes that some messages will resonate more or less with individuals based on their own characteristics, of which race may be one.”
Warner does believe in the power of tailored messaging though. “Part of the onus for healthcare institutions and providers is to make some decisions about who it is really important to bring back in soonest,” she said.
“Those are the ones we want to prioritize, as opposed to those who we want to get back into care but we don’t need to get them in right now,” Warner emphasized. “As they are balancing all the needs of their family and their community and their other needs, messaging that adds additional stress, worry, anxiety and shame is not what we want to do. So really we need to distinguish between these populations, identify the priorities, hit the hard message to people who really need it now, and encourage others to come back in as they can.”
Building trust
All the panelists agreed that building trust with the public will be key to getting cancer care back on track.
“I don’t think anyone trusts the healthcare community right now, but we already had this baseline distrust of healthcare among many minority communities, and now with COVID-19, the African American community in particular is seeing people go into the hospital and never come back,” said Richardson.
For Warner, the onus really falls on healthcare institutions. “We have to be proactive and not leave the burden of deciding when and how to return to care up to patients,” she said.
“What we need to focus on as much as possible is to get people to realize it is safe to come see the doctor,” said Johns Hopkins oncologist Brawley. “We have to make it safe for them to come see us, and then we have to convince them it is safe to come see us.”
Venturing out to her mammography appointment in early June, Richardson said she felt safe. “Everything was just the way it was supposed to be, everyone was masked, everyone was washing their hands,” she said.
Yet, by mid-June she had contracted COVID-19. “I don’t know where I got it,” she said. “No matter how careful you are, understand that if you’re in a total red spot, as I am, you can just get it.”
This article first appeared on Medscape.com.