User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Early-onset CRC associated with longer survival
Individuals diagnosed with primary colorectal cancer (CRC) at less than 50 years of age have better survival outcomes than individuals diagnosed at 51-55 years, based on data from more than 750,000 patients.
This finding emphasizes the importance of early CRC detection in younger individuals, reported lead author En Cheng, MD, PhD, of Yale University, New Haven, Conn., and colleagues.
“Early-onset CRC (i.e., CRC diagnosed at age less than 50 years) has been characterized by unique clinical, genetic, and epigenetic characteristics, and thus it may be associated with different survival from CRC diagnosed among individuals older than 50 years,” the investigators wrote in JAMA Network Open. Previous studies comparing survival times across age groups have yielded inconsistent results.
To gain a better understanding, the investigator conducted a retrospective study using data from the National Cancer Database. Excluding patients with primary CRC who had concomitant diagnosis, history of other malignant tumors, noninvasive adenocarcinoma, or missing data, the final dataset included 769,871 patients. Early-onset CRC was defined by age less than 50 years, whereas later-onset CRC was defined by ages 51-55 years.
“Individuals diagnosed at age 50 years were excluded to minimize an apparent screening detection bias at age 50 years in our population, given that these individuals disproportionately presented with earlier stages,” the investigators wrote.
Initial comparisons across groups revealed several significant differences. Individuals in the early-onset group were more often women (47.3% vs. 43.8%; P < .001), members of races in the “other” category (6.9% vs. 5.9%; P < .001), and Medicaid patients (12.3% vs. 10.3%; P < .001). They were also more likely to be diagnosed with stage IV cancer (27.8% vs 24.1%; P < .001) and have rectal tumors (29.3% vs. 28.7%; P = .004).
In the unadjusted Kaplan-Meier analysis, patients with early-onset CRC had a lower 10-year survival rate (53.6%; 95% CI, 53.2%-54.0% vs. 54.3%; 95% CI, 53.8%-54.8%; P < .001). The fully adjusted model revealed significantly higher survival for early-onset patients, compared with later-onset patients (adjusted hazard ratio, 0.95; 95% CI, 0.93-0.96; P < .001) . This disparity deepened when adjusting only for stage (HR, 0.89; 95% CI, 0.88-0.90; P < .001).
Survival was longest among patients 35-39 years (aHR, 0.88; 95% CI, 0.84-0.92; P < .001), compared with those aged 51-55, and among early-onset individuals with stage I disease (a HR, 0.87; 95% CI, 0.81-0.93; P < .001) or stage II disease (a HR, 0.86; 95% CI, 0.82-0.90; P < .001), compared with those having the same stages of later-onset CRC. No survival advantage was observed among patients diagnosed at age 25 or younger or those with stage III or IV disease.
“Interestingly, hereditary nonpolyposis colorectal cancer, owing to underlying mismatch repair deficiency, is associated with superior survival and is often diagnosed in individuals from ages 35-45 years,” the investigators noted. “In contrast, adenomatous polyposis coli syndrome is more common in individuals who are diagnosed with CRC at age younger than 20 years (10%), compared with those diagnosed at later ages (0.1%), and adenomatous polyposis coli syndrome is not associated with a survival advantage. These high penetrance syndromes could partly account for the relative heterogeneity in survival across ages among individuals with early-onset CRC.”
Cautious about interpretation
Dr. Cheng and colleagues concluded their publication with a disclaimer: “Our finding of a survival advantage associated with early-onset CRC among younger individuals should be interpreted cautiously, given that the advantage had a small magnitude and was heterogeneous by age and stage,” they wrote. “Further study is needed to understand the underlying heterogeneity of survival by age and stage among individuals with early-onset CRC.”
Kirbi L. Yelorda, MD, of Stanford (Calif.) University, and colleagues, had a similar interpretation.
“These results offer support for effectiveness of treatment in patients diagnosed with CRC at younger ages; however, they must be interpreted within the context of epidemiological and biological factors,” Dr. Yelorda and colleagues wrote in an accompanying editorial.
The findings also suggest that the recent reduction in recommended screening age by the U.S. Preventive Services Task Force – from 50 years to 45 years – is warranted, they added, but screening younger patients remains unnecessary.
“While these results do not suggest that screening should start for patients younger than 45 years, they do support the benefit of early detection in young patients,” Dr. Yelorda and colleagues wrote, noting a “fairly low incidence rate” among individuals younger than 45, which is insufficient to justify the risk-to-benefit ratio and increased costs associated with expanded screening.
Important but not surprising
It’s “not surprising” that early-onset patients typically have better survival than later-onset patients, according to Joseph C. Anderson, MD, associate professor at White River Junction Veterans Affairs Medical Center, Hartford, Vt.; Geisel School of Medicine at Dartmouth, Hanover, N.H.; and the University of Connecticut, Farmington.
“They’re younger, have less comorbidities, and can tolerate chemotherapy,” Dr. Anderson said in an interview. “It’s not surprising that people do poorly with later stages. Younger people are no exception.”
Dr. Anderson, who previously coauthored an editorial weighing the pros and cons of earlier screening, noted that earlier screening is needed because of the rising incidence of late-stage diagnoses among younger patients, which, as the study found, are associated with worse outcomes.
Beyond adherence to screening recommendations, Dr. Anderson urged clinicians to be aggressive when doing a workup of CRC symptoms in younger patients, among whom delayed diagnoses are more common.
“We can’t just say it’s something more benign, like hemorrhoids, like we used to,” Dr. Anderson said. “Somebody who’s 30 years old and having rectal bleeding needs to be evaluated promptly – there can’t be a delay.”
The study was supported by the National Institutes of Health and Stand Up To Cancer (grant administered by the American Association for Cancer Research). The investigators disclosed relationships with Evergrande Group, Janssen, Revolution Medicines, and others. One editorialist reported serving as a member of the USPSTF when the guideline for colorectal cancer was developed, and being a coauthor on the guideline. No other disclosures were reported among editorialists. Dr. Anderson reported no relevant conflicts of interest.
Individuals diagnosed with primary colorectal cancer (CRC) at less than 50 years of age have better survival outcomes than individuals diagnosed at 51-55 years, based on data from more than 750,000 patients.
This finding emphasizes the importance of early CRC detection in younger individuals, reported lead author En Cheng, MD, PhD, of Yale University, New Haven, Conn., and colleagues.
“Early-onset CRC (i.e., CRC diagnosed at age less than 50 years) has been characterized by unique clinical, genetic, and epigenetic characteristics, and thus it may be associated with different survival from CRC diagnosed among individuals older than 50 years,” the investigators wrote in JAMA Network Open. Previous studies comparing survival times across age groups have yielded inconsistent results.
To gain a better understanding, the investigator conducted a retrospective study using data from the National Cancer Database. Excluding patients with primary CRC who had concomitant diagnosis, history of other malignant tumors, noninvasive adenocarcinoma, or missing data, the final dataset included 769,871 patients. Early-onset CRC was defined by age less than 50 years, whereas later-onset CRC was defined by ages 51-55 years.
“Individuals diagnosed at age 50 years were excluded to minimize an apparent screening detection bias at age 50 years in our population, given that these individuals disproportionately presented with earlier stages,” the investigators wrote.
Initial comparisons across groups revealed several significant differences. Individuals in the early-onset group were more often women (47.3% vs. 43.8%; P < .001), members of races in the “other” category (6.9% vs. 5.9%; P < .001), and Medicaid patients (12.3% vs. 10.3%; P < .001). They were also more likely to be diagnosed with stage IV cancer (27.8% vs 24.1%; P < .001) and have rectal tumors (29.3% vs. 28.7%; P = .004).
In the unadjusted Kaplan-Meier analysis, patients with early-onset CRC had a lower 10-year survival rate (53.6%; 95% CI, 53.2%-54.0% vs. 54.3%; 95% CI, 53.8%-54.8%; P < .001). The fully adjusted model revealed significantly higher survival for early-onset patients, compared with later-onset patients (adjusted hazard ratio, 0.95; 95% CI, 0.93-0.96; P < .001) . This disparity deepened when adjusting only for stage (HR, 0.89; 95% CI, 0.88-0.90; P < .001).
Survival was longest among patients 35-39 years (aHR, 0.88; 95% CI, 0.84-0.92; P < .001), compared with those aged 51-55, and among early-onset individuals with stage I disease (a HR, 0.87; 95% CI, 0.81-0.93; P < .001) or stage II disease (a HR, 0.86; 95% CI, 0.82-0.90; P < .001), compared with those having the same stages of later-onset CRC. No survival advantage was observed among patients diagnosed at age 25 or younger or those with stage III or IV disease.
“Interestingly, hereditary nonpolyposis colorectal cancer, owing to underlying mismatch repair deficiency, is associated with superior survival and is often diagnosed in individuals from ages 35-45 years,” the investigators noted. “In contrast, adenomatous polyposis coli syndrome is more common in individuals who are diagnosed with CRC at age younger than 20 years (10%), compared with those diagnosed at later ages (0.1%), and adenomatous polyposis coli syndrome is not associated with a survival advantage. These high penetrance syndromes could partly account for the relative heterogeneity in survival across ages among individuals with early-onset CRC.”
Cautious about interpretation
Dr. Cheng and colleagues concluded their publication with a disclaimer: “Our finding of a survival advantage associated with early-onset CRC among younger individuals should be interpreted cautiously, given that the advantage had a small magnitude and was heterogeneous by age and stage,” they wrote. “Further study is needed to understand the underlying heterogeneity of survival by age and stage among individuals with early-onset CRC.”
Kirbi L. Yelorda, MD, of Stanford (Calif.) University, and colleagues, had a similar interpretation.
“These results offer support for effectiveness of treatment in patients diagnosed with CRC at younger ages; however, they must be interpreted within the context of epidemiological and biological factors,” Dr. Yelorda and colleagues wrote in an accompanying editorial.
The findings also suggest that the recent reduction in recommended screening age by the U.S. Preventive Services Task Force – from 50 years to 45 years – is warranted, they added, but screening younger patients remains unnecessary.
“While these results do not suggest that screening should start for patients younger than 45 years, they do support the benefit of early detection in young patients,” Dr. Yelorda and colleagues wrote, noting a “fairly low incidence rate” among individuals younger than 45, which is insufficient to justify the risk-to-benefit ratio and increased costs associated with expanded screening.
Important but not surprising
It’s “not surprising” that early-onset patients typically have better survival than later-onset patients, according to Joseph C. Anderson, MD, associate professor at White River Junction Veterans Affairs Medical Center, Hartford, Vt.; Geisel School of Medicine at Dartmouth, Hanover, N.H.; and the University of Connecticut, Farmington.
“They’re younger, have less comorbidities, and can tolerate chemotherapy,” Dr. Anderson said in an interview. “It’s not surprising that people do poorly with later stages. Younger people are no exception.”
Dr. Anderson, who previously coauthored an editorial weighing the pros and cons of earlier screening, noted that earlier screening is needed because of the rising incidence of late-stage diagnoses among younger patients, which, as the study found, are associated with worse outcomes.
Beyond adherence to screening recommendations, Dr. Anderson urged clinicians to be aggressive when doing a workup of CRC symptoms in younger patients, among whom delayed diagnoses are more common.
“We can’t just say it’s something more benign, like hemorrhoids, like we used to,” Dr. Anderson said. “Somebody who’s 30 years old and having rectal bleeding needs to be evaluated promptly – there can’t be a delay.”
The study was supported by the National Institutes of Health and Stand Up To Cancer (grant administered by the American Association for Cancer Research). The investigators disclosed relationships with Evergrande Group, Janssen, Revolution Medicines, and others. One editorialist reported serving as a member of the USPSTF when the guideline for colorectal cancer was developed, and being a coauthor on the guideline. No other disclosures were reported among editorialists. Dr. Anderson reported no relevant conflicts of interest.
Individuals diagnosed with primary colorectal cancer (CRC) at less than 50 years of age have better survival outcomes than individuals diagnosed at 51-55 years, based on data from more than 750,000 patients.
This finding emphasizes the importance of early CRC detection in younger individuals, reported lead author En Cheng, MD, PhD, of Yale University, New Haven, Conn., and colleagues.
“Early-onset CRC (i.e., CRC diagnosed at age less than 50 years) has been characterized by unique clinical, genetic, and epigenetic characteristics, and thus it may be associated with different survival from CRC diagnosed among individuals older than 50 years,” the investigators wrote in JAMA Network Open. Previous studies comparing survival times across age groups have yielded inconsistent results.
To gain a better understanding, the investigator conducted a retrospective study using data from the National Cancer Database. Excluding patients with primary CRC who had concomitant diagnosis, history of other malignant tumors, noninvasive adenocarcinoma, or missing data, the final dataset included 769,871 patients. Early-onset CRC was defined by age less than 50 years, whereas later-onset CRC was defined by ages 51-55 years.
“Individuals diagnosed at age 50 years were excluded to minimize an apparent screening detection bias at age 50 years in our population, given that these individuals disproportionately presented with earlier stages,” the investigators wrote.
Initial comparisons across groups revealed several significant differences. Individuals in the early-onset group were more often women (47.3% vs. 43.8%; P < .001), members of races in the “other” category (6.9% vs. 5.9%; P < .001), and Medicaid patients (12.3% vs. 10.3%; P < .001). They were also more likely to be diagnosed with stage IV cancer (27.8% vs 24.1%; P < .001) and have rectal tumors (29.3% vs. 28.7%; P = .004).
In the unadjusted Kaplan-Meier analysis, patients with early-onset CRC had a lower 10-year survival rate (53.6%; 95% CI, 53.2%-54.0% vs. 54.3%; 95% CI, 53.8%-54.8%; P < .001). The fully adjusted model revealed significantly higher survival for early-onset patients, compared with later-onset patients (adjusted hazard ratio, 0.95; 95% CI, 0.93-0.96; P < .001) . This disparity deepened when adjusting only for stage (HR, 0.89; 95% CI, 0.88-0.90; P < .001).
Survival was longest among patients 35-39 years (aHR, 0.88; 95% CI, 0.84-0.92; P < .001), compared with those aged 51-55, and among early-onset individuals with stage I disease (a HR, 0.87; 95% CI, 0.81-0.93; P < .001) or stage II disease (a HR, 0.86; 95% CI, 0.82-0.90; P < .001), compared with those having the same stages of later-onset CRC. No survival advantage was observed among patients diagnosed at age 25 or younger or those with stage III or IV disease.
“Interestingly, hereditary nonpolyposis colorectal cancer, owing to underlying mismatch repair deficiency, is associated with superior survival and is often diagnosed in individuals from ages 35-45 years,” the investigators noted. “In contrast, adenomatous polyposis coli syndrome is more common in individuals who are diagnosed with CRC at age younger than 20 years (10%), compared with those diagnosed at later ages (0.1%), and adenomatous polyposis coli syndrome is not associated with a survival advantage. These high penetrance syndromes could partly account for the relative heterogeneity in survival across ages among individuals with early-onset CRC.”
Cautious about interpretation
Dr. Cheng and colleagues concluded their publication with a disclaimer: “Our finding of a survival advantage associated with early-onset CRC among younger individuals should be interpreted cautiously, given that the advantage had a small magnitude and was heterogeneous by age and stage,” they wrote. “Further study is needed to understand the underlying heterogeneity of survival by age and stage among individuals with early-onset CRC.”
Kirbi L. Yelorda, MD, of Stanford (Calif.) University, and colleagues, had a similar interpretation.
“These results offer support for effectiveness of treatment in patients diagnosed with CRC at younger ages; however, they must be interpreted within the context of epidemiological and biological factors,” Dr. Yelorda and colleagues wrote in an accompanying editorial.
The findings also suggest that the recent reduction in recommended screening age by the U.S. Preventive Services Task Force – from 50 years to 45 years – is warranted, they added, but screening younger patients remains unnecessary.
“While these results do not suggest that screening should start for patients younger than 45 years, they do support the benefit of early detection in young patients,” Dr. Yelorda and colleagues wrote, noting a “fairly low incidence rate” among individuals younger than 45, which is insufficient to justify the risk-to-benefit ratio and increased costs associated with expanded screening.
Important but not surprising
It’s “not surprising” that early-onset patients typically have better survival than later-onset patients, according to Joseph C. Anderson, MD, associate professor at White River Junction Veterans Affairs Medical Center, Hartford, Vt.; Geisel School of Medicine at Dartmouth, Hanover, N.H.; and the University of Connecticut, Farmington.
“They’re younger, have less comorbidities, and can tolerate chemotherapy,” Dr. Anderson said in an interview. “It’s not surprising that people do poorly with later stages. Younger people are no exception.”
Dr. Anderson, who previously coauthored an editorial weighing the pros and cons of earlier screening, noted that earlier screening is needed because of the rising incidence of late-stage diagnoses among younger patients, which, as the study found, are associated with worse outcomes.
Beyond adherence to screening recommendations, Dr. Anderson urged clinicians to be aggressive when doing a workup of CRC symptoms in younger patients, among whom delayed diagnoses are more common.
“We can’t just say it’s something more benign, like hemorrhoids, like we used to,” Dr. Anderson said. “Somebody who’s 30 years old and having rectal bleeding needs to be evaluated promptly – there can’t be a delay.”
The study was supported by the National Institutes of Health and Stand Up To Cancer (grant administered by the American Association for Cancer Research). The investigators disclosed relationships with Evergrande Group, Janssen, Revolution Medicines, and others. One editorialist reported serving as a member of the USPSTF when the guideline for colorectal cancer was developed, and being a coauthor on the guideline. No other disclosures were reported among editorialists. Dr. Anderson reported no relevant conflicts of interest.
FROM JAMA NETWORK OPEN
Ponatinib/blinatumomab start strong against Ph+ALL
For adults with Philadelphia chromosome–positive acute lymphoblastic leukemia (Ph+ALL), frontline therapy with the chemotherapy-free combination of ponatinib (Iclusig) and blinatumomab (Blincyto) shows promise as an alternative to early hematopoietic stem cell transplantation (HSCT), investigators in a single-arm phase 2 study reported.
In an interim analysis of the combination in patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase chronic myeloid leukemia (CML), 20 patients who received it as frontline therapy had a rate of complete responses (CR) or complete responses with partial recovery of blood counts (CRp) of 100% and a complete molecular remission (CMR) rate of 85%, reported Nicholas Short, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This translated into an estimated 2-year overall survival of 93%, with no patients undergoing transplant in first remission, and none having relapse at last follow-up,” he said in an oral abstract presented during the European Hematology Association annual congress.
Among patients with relapsed/refractory Ph+ALL, the CR/CRp rate was 89%, the CMR rate was 88%, and the estimated 2-year overall survival rate was 53%, he said.
Transplants on hold
“The big selling point is the ability to avoid stem cell transplant, which is not always the first thing you do in Ph-positive ALL, but it’s always on your mind,” said Gwen Nichols, MD, chief medical officer of the Leukemia and Lymphoma Society, who was not involved in the study.
“It looks, albeit with very limited follow-up, that patients haven’t relapsed yet such that transplant would be necessary. Anything we can do to avoid people having long-term complications that go along with an allogeneic transplant is a step in the right direction,” she said in an interview.
One combination, three cohorts
Ph+ALL comprises about 25% of all adult ALL. The standard of care in newly diagnosed patients is chemotherapy plus a tyrosine kinase inhibitor (TKI) targeted against the BCR-ABL transcript.
Ponatinib is a pan-BCR-ABL TKI that has been shown to have activity against ALL with T315I mutations, which are present in about 75% of the cases of relapsed disease, Dr. Short said.
Blinatumomab is a bi-specific T-cell engager (BiTe) that has been shown to be effective as monotherapy against relapsed/refractory Ph+ALL as monotherapy and in combination with dasatinib.
Dr. Short and colleagues enrolled patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase CML. Patients in the frontline cohort could have received one or two prior lines of chemotherapy with or without a TKI.
The patients all had Eastern Cooperative Oncology Group performance status of 0-2, and adequate liver function.
Patients with clinically significant cardiovascular disease or central nervous system disease pathology were excluded, except that patients with CNS leukemia could be enrolled.
The induction phase consisted of 30 mg ponatinib daily plus blinatumomab standard dosing on a 4-week-on, 2-week-off schedule. Patients in CMR, defined for frontline patients as undetectable BCR-ABL transcripts by polymerase chain reaction, then received up to four consolidation cycles of the regimen with ponatinib at a 15-mg dose, followed by 5 years of ponatinib 15-mg maintenance. All patients also received CNS prophylaxis with 12 cycles of intrathecal chemotherapy with alternating administration of methotrexate and cytarabine.
Of the 35 patients treated to date with the combination, 20 with Ph+ALL received it as frontline therapy and 10 received it for relapsed/refractory disease; 5 patients with CML in lymphoid blast phase also were treated.
High CMR, CR rates
As noted before, the CMR rate, the primary endpoint among patients with newly diagnosed Ph+ALL, was 85%, with a CR/CRp rate of 100%. Six of the patients in the frontline group and one in the salvage therapy group had CRs but were positive for minimal residual disease (MRD) at study outset.
The CR/CRp rate for the entire cohort of 28 patients (excluding those with a CR at start) was 96%, with only 1 patient who had relapsed/refractory disease not having a CR. This patient had received ponatinib in a prior salvage regimen.
The CMR rate among the entire cohort was 79%, with 85% of patients in the frontline ALL cohort having a CMR, 88% in the relapsed/refractory cohort, and 40% in the CML cohort. There were no early deaths among any patients.
“After one cycle of ponatinib plus blinatumomab, 84% of frontline patients had achieved at least a major molecular response, and 58% had achieved a CMR. Among those with relapsed/refractory Ph+ALL, 75% achieved CMR after one cycle of therapy,” Dr. Short said.
Of the 20 frontline patients in CR, one patient experienced visual changes and possible stroke that were considered possibly related to the study medication. This patient was taken off study. During a later maintenance regimen this patient developed a non-ST elevation myocardial infarction and died from postprocedural bleeding and hypovolemic shock following a cardiac catheterization procedure.
The remainder of patients in the frontline cohort had ongoing responses without the need for HSCT at last follow-up. There were no relapses, with a median duration of CR of 6 months,
Among the 10 with relapsed/refractory Ph+ALL, one did not have a response, and the remaining 9 had CR/CRps.
Of the latter groups, four went on to allogeneic HSCT and three were still alive; one patient who underwent a transplant experienced a relapse and died. One additional patient was alive with relapsed disease with T315I and E255V mutations at the time of relapse, one patient in CR who went off study due to insurance issues died from an unknown cause, and the three remaining patients had ongoing responses without transplant.
Among the five patients with CML in lymphoid blast phase, two had relapses, but both are still alive and currently in remission, and three have ongoing responses without transplant.
After a median follow-up of 12 months the 1-year event-free survival (EFS) rate for the entire 35-patient group was 76%, and the 2-year EFS was 70%.
The 1-year overall survival rate was 93%, and the 2-year OS rate was 80%.
Among patients in the frontline group, the 1-year and 2-year EFS and OS rates were all 93%.
For the relapsed/refractory cohort, the estimated 2-year EFS was 41% and OS was 53%. For the CML cohort, the 2-year EFS was 60%, with all patients still alive at last follow-up.
There were no grade 4 adverse events on study. Grade 3 adverse events considered at least possibly related to study treatment were elevated lipase, fever/febrile neutropenia, increased alanine aminotransferase, cerebrovascular ischemia, hypertension, pancreatitis, deep vein thrombosis, and encephalopathy. There were no cases of grade 3 cytokine release syndrome or tremor.
The study was sponsored by MD Anderson Cancer Center with collaboration from the National Cancer Institute, Amgen, and Takeda. Dr. Short has disclosed relationships with Amgen and Takeda. Dr. Nichols reported having no conflicts of interest.
For adults with Philadelphia chromosome–positive acute lymphoblastic leukemia (Ph+ALL), frontline therapy with the chemotherapy-free combination of ponatinib (Iclusig) and blinatumomab (Blincyto) shows promise as an alternative to early hematopoietic stem cell transplantation (HSCT), investigators in a single-arm phase 2 study reported.
In an interim analysis of the combination in patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase chronic myeloid leukemia (CML), 20 patients who received it as frontline therapy had a rate of complete responses (CR) or complete responses with partial recovery of blood counts (CRp) of 100% and a complete molecular remission (CMR) rate of 85%, reported Nicholas Short, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This translated into an estimated 2-year overall survival of 93%, with no patients undergoing transplant in first remission, and none having relapse at last follow-up,” he said in an oral abstract presented during the European Hematology Association annual congress.
Among patients with relapsed/refractory Ph+ALL, the CR/CRp rate was 89%, the CMR rate was 88%, and the estimated 2-year overall survival rate was 53%, he said.
Transplants on hold
“The big selling point is the ability to avoid stem cell transplant, which is not always the first thing you do in Ph-positive ALL, but it’s always on your mind,” said Gwen Nichols, MD, chief medical officer of the Leukemia and Lymphoma Society, who was not involved in the study.
“It looks, albeit with very limited follow-up, that patients haven’t relapsed yet such that transplant would be necessary. Anything we can do to avoid people having long-term complications that go along with an allogeneic transplant is a step in the right direction,” she said in an interview.
One combination, three cohorts
Ph+ALL comprises about 25% of all adult ALL. The standard of care in newly diagnosed patients is chemotherapy plus a tyrosine kinase inhibitor (TKI) targeted against the BCR-ABL transcript.
Ponatinib is a pan-BCR-ABL TKI that has been shown to have activity against ALL with T315I mutations, which are present in about 75% of the cases of relapsed disease, Dr. Short said.
Blinatumomab is a bi-specific T-cell engager (BiTe) that has been shown to be effective as monotherapy against relapsed/refractory Ph+ALL as monotherapy and in combination with dasatinib.
Dr. Short and colleagues enrolled patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase CML. Patients in the frontline cohort could have received one or two prior lines of chemotherapy with or without a TKI.
The patients all had Eastern Cooperative Oncology Group performance status of 0-2, and adequate liver function.
Patients with clinically significant cardiovascular disease or central nervous system disease pathology were excluded, except that patients with CNS leukemia could be enrolled.
The induction phase consisted of 30 mg ponatinib daily plus blinatumomab standard dosing on a 4-week-on, 2-week-off schedule. Patients in CMR, defined for frontline patients as undetectable BCR-ABL transcripts by polymerase chain reaction, then received up to four consolidation cycles of the regimen with ponatinib at a 15-mg dose, followed by 5 years of ponatinib 15-mg maintenance. All patients also received CNS prophylaxis with 12 cycles of intrathecal chemotherapy with alternating administration of methotrexate and cytarabine.
Of the 35 patients treated to date with the combination, 20 with Ph+ALL received it as frontline therapy and 10 received it for relapsed/refractory disease; 5 patients with CML in lymphoid blast phase also were treated.
High CMR, CR rates
As noted before, the CMR rate, the primary endpoint among patients with newly diagnosed Ph+ALL, was 85%, with a CR/CRp rate of 100%. Six of the patients in the frontline group and one in the salvage therapy group had CRs but were positive for minimal residual disease (MRD) at study outset.
The CR/CRp rate for the entire cohort of 28 patients (excluding those with a CR at start) was 96%, with only 1 patient who had relapsed/refractory disease not having a CR. This patient had received ponatinib in a prior salvage regimen.
The CMR rate among the entire cohort was 79%, with 85% of patients in the frontline ALL cohort having a CMR, 88% in the relapsed/refractory cohort, and 40% in the CML cohort. There were no early deaths among any patients.
“After one cycle of ponatinib plus blinatumomab, 84% of frontline patients had achieved at least a major molecular response, and 58% had achieved a CMR. Among those with relapsed/refractory Ph+ALL, 75% achieved CMR after one cycle of therapy,” Dr. Short said.
Of the 20 frontline patients in CR, one patient experienced visual changes and possible stroke that were considered possibly related to the study medication. This patient was taken off study. During a later maintenance regimen this patient developed a non-ST elevation myocardial infarction and died from postprocedural bleeding and hypovolemic shock following a cardiac catheterization procedure.
The remainder of patients in the frontline cohort had ongoing responses without the need for HSCT at last follow-up. There were no relapses, with a median duration of CR of 6 months,
Among the 10 with relapsed/refractory Ph+ALL, one did not have a response, and the remaining 9 had CR/CRps.
Of the latter groups, four went on to allogeneic HSCT and three were still alive; one patient who underwent a transplant experienced a relapse and died. One additional patient was alive with relapsed disease with T315I and E255V mutations at the time of relapse, one patient in CR who went off study due to insurance issues died from an unknown cause, and the three remaining patients had ongoing responses without transplant.
Among the five patients with CML in lymphoid blast phase, two had relapses, but both are still alive and currently in remission, and three have ongoing responses without transplant.
After a median follow-up of 12 months the 1-year event-free survival (EFS) rate for the entire 35-patient group was 76%, and the 2-year EFS was 70%.
The 1-year overall survival rate was 93%, and the 2-year OS rate was 80%.
Among patients in the frontline group, the 1-year and 2-year EFS and OS rates were all 93%.
For the relapsed/refractory cohort, the estimated 2-year EFS was 41% and OS was 53%. For the CML cohort, the 2-year EFS was 60%, with all patients still alive at last follow-up.
There were no grade 4 adverse events on study. Grade 3 adverse events considered at least possibly related to study treatment were elevated lipase, fever/febrile neutropenia, increased alanine aminotransferase, cerebrovascular ischemia, hypertension, pancreatitis, deep vein thrombosis, and encephalopathy. There were no cases of grade 3 cytokine release syndrome or tremor.
The study was sponsored by MD Anderson Cancer Center with collaboration from the National Cancer Institute, Amgen, and Takeda. Dr. Short has disclosed relationships with Amgen and Takeda. Dr. Nichols reported having no conflicts of interest.
For adults with Philadelphia chromosome–positive acute lymphoblastic leukemia (Ph+ALL), frontline therapy with the chemotherapy-free combination of ponatinib (Iclusig) and blinatumomab (Blincyto) shows promise as an alternative to early hematopoietic stem cell transplantation (HSCT), investigators in a single-arm phase 2 study reported.
In an interim analysis of the combination in patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase chronic myeloid leukemia (CML), 20 patients who received it as frontline therapy had a rate of complete responses (CR) or complete responses with partial recovery of blood counts (CRp) of 100% and a complete molecular remission (CMR) rate of 85%, reported Nicholas Short, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This translated into an estimated 2-year overall survival of 93%, with no patients undergoing transplant in first remission, and none having relapse at last follow-up,” he said in an oral abstract presented during the European Hematology Association annual congress.
Among patients with relapsed/refractory Ph+ALL, the CR/CRp rate was 89%, the CMR rate was 88%, and the estimated 2-year overall survival rate was 53%, he said.
Transplants on hold
“The big selling point is the ability to avoid stem cell transplant, which is not always the first thing you do in Ph-positive ALL, but it’s always on your mind,” said Gwen Nichols, MD, chief medical officer of the Leukemia and Lymphoma Society, who was not involved in the study.
“It looks, albeit with very limited follow-up, that patients haven’t relapsed yet such that transplant would be necessary. Anything we can do to avoid people having long-term complications that go along with an allogeneic transplant is a step in the right direction,” she said in an interview.
One combination, three cohorts
Ph+ALL comprises about 25% of all adult ALL. The standard of care in newly diagnosed patients is chemotherapy plus a tyrosine kinase inhibitor (TKI) targeted against the BCR-ABL transcript.
Ponatinib is a pan-BCR-ABL TKI that has been shown to have activity against ALL with T315I mutations, which are present in about 75% of the cases of relapsed disease, Dr. Short said.
Blinatumomab is a bi-specific T-cell engager (BiTe) that has been shown to be effective as monotherapy against relapsed/refractory Ph+ALL as monotherapy and in combination with dasatinib.
Dr. Short and colleagues enrolled patients with newly diagnosed or relapsed/refractory Ph+ALL or lymphoid accelerated or blast phase CML. Patients in the frontline cohort could have received one or two prior lines of chemotherapy with or without a TKI.
The patients all had Eastern Cooperative Oncology Group performance status of 0-2, and adequate liver function.
Patients with clinically significant cardiovascular disease or central nervous system disease pathology were excluded, except that patients with CNS leukemia could be enrolled.
The induction phase consisted of 30 mg ponatinib daily plus blinatumomab standard dosing on a 4-week-on, 2-week-off schedule. Patients in CMR, defined for frontline patients as undetectable BCR-ABL transcripts by polymerase chain reaction, then received up to four consolidation cycles of the regimen with ponatinib at a 15-mg dose, followed by 5 years of ponatinib 15-mg maintenance. All patients also received CNS prophylaxis with 12 cycles of intrathecal chemotherapy with alternating administration of methotrexate and cytarabine.
Of the 35 patients treated to date with the combination, 20 with Ph+ALL received it as frontline therapy and 10 received it for relapsed/refractory disease; 5 patients with CML in lymphoid blast phase also were treated.
High CMR, CR rates
As noted before, the CMR rate, the primary endpoint among patients with newly diagnosed Ph+ALL, was 85%, with a CR/CRp rate of 100%. Six of the patients in the frontline group and one in the salvage therapy group had CRs but were positive for minimal residual disease (MRD) at study outset.
The CR/CRp rate for the entire cohort of 28 patients (excluding those with a CR at start) was 96%, with only 1 patient who had relapsed/refractory disease not having a CR. This patient had received ponatinib in a prior salvage regimen.
The CMR rate among the entire cohort was 79%, with 85% of patients in the frontline ALL cohort having a CMR, 88% in the relapsed/refractory cohort, and 40% in the CML cohort. There were no early deaths among any patients.
“After one cycle of ponatinib plus blinatumomab, 84% of frontline patients had achieved at least a major molecular response, and 58% had achieved a CMR. Among those with relapsed/refractory Ph+ALL, 75% achieved CMR after one cycle of therapy,” Dr. Short said.
Of the 20 frontline patients in CR, one patient experienced visual changes and possible stroke that were considered possibly related to the study medication. This patient was taken off study. During a later maintenance regimen this patient developed a non-ST elevation myocardial infarction and died from postprocedural bleeding and hypovolemic shock following a cardiac catheterization procedure.
The remainder of patients in the frontline cohort had ongoing responses without the need for HSCT at last follow-up. There were no relapses, with a median duration of CR of 6 months,
Among the 10 with relapsed/refractory Ph+ALL, one did not have a response, and the remaining 9 had CR/CRps.
Of the latter groups, four went on to allogeneic HSCT and three were still alive; one patient who underwent a transplant experienced a relapse and died. One additional patient was alive with relapsed disease with T315I and E255V mutations at the time of relapse, one patient in CR who went off study due to insurance issues died from an unknown cause, and the three remaining patients had ongoing responses without transplant.
Among the five patients with CML in lymphoid blast phase, two had relapses, but both are still alive and currently in remission, and three have ongoing responses without transplant.
After a median follow-up of 12 months the 1-year event-free survival (EFS) rate for the entire 35-patient group was 76%, and the 2-year EFS was 70%.
The 1-year overall survival rate was 93%, and the 2-year OS rate was 80%.
Among patients in the frontline group, the 1-year and 2-year EFS and OS rates were all 93%.
For the relapsed/refractory cohort, the estimated 2-year EFS was 41% and OS was 53%. For the CML cohort, the 2-year EFS was 60%, with all patients still alive at last follow-up.
There were no grade 4 adverse events on study. Grade 3 adverse events considered at least possibly related to study treatment were elevated lipase, fever/febrile neutropenia, increased alanine aminotransferase, cerebrovascular ischemia, hypertension, pancreatitis, deep vein thrombosis, and encephalopathy. There were no cases of grade 3 cytokine release syndrome or tremor.
The study was sponsored by MD Anderson Cancer Center with collaboration from the National Cancer Institute, Amgen, and Takeda. Dr. Short has disclosed relationships with Amgen and Takeda. Dr. Nichols reported having no conflicts of interest.
FROM EHA 2021
Novel molecule prolongs half-life of bleeding disorder treatments
A novel therapeutic approach using aptamers – short single strands of DNA or RNA designed to selectively bind to a target – shows promise for treating von Willebrand Disease (VWD), and other congenital bleed disorders such as hemophilia A, investigators say.
In a proof-of-concept study using healthy volunteers, the experimental anti–von Willebrand factor (VWF) molecule BT200 appeared to decrease clearance of VWF and resulted in a twofold increase in endogenous levels of VWF and factor VIII at low doses.
BT200 is currently being explored in a phase 2 trial in patients with hemophilia A and VWD type 2B, Katarina Kovacevic, MPharm, from the Medical University of Vienna, reported at the European Hematology Association annual congress.
“We expect to see a half-life increase of 2 to 4 times of factor VIII products, which will allow us to have a longer time between treatments,” she said in an oral abstract presentation (Abstract S302).
Lab-made nucleotide strings
Aptamers are sometimes call “chemical antibodies” because of their high affinity and high specificity for extracellular targets, Dr. Kovacevic said. Unlike conventional humanized or human-derived antibodies, however, they are nonimmunogenic and are less costly to manufacture.
In a previous study from her center, a different anti-VWF aptamer labeled ARC1779 increased plasma levels of VWF, factor VIII, and platelet counts in patients with VWD type 2B.
However, the drug was inconvenient to use, requiring 72-hour infusions, she noted.
In a study published in Feb. 4, 2021 in Scientific Reports, Dr. Kovacevic and colleagues reported that BT200 blocks VWF and platelet function in patients with ischemic strokes, even in the presence of high levels of VWF in patients with left carotid artery atherosclerotic strokes.
The ability of the molecule to block VWF platelet binding may explain how the anti-VWF agent actually results in higher circulating levels of VWF, which also carries factor VIII, said Veronica H. Flood, MD, a VWD specialist at Children’s Hospital of Wisconsin and associate professor at the Medical College of Wisconsin in Milwaukee.
“It might inhibit clearance of the von Willebrand factor, so it’s almost like this was an incidental side effect,” she said in an interview. “Incidentally, this happens to also give you higher levels of the von Willebrand factor and the factor VIII, and with a longer half-life than anything we currently have, so it’s a super-creative strategy,” she said.
Dr. Flood was not involved in the study.
Long half-life
BT200 is a third-generation peglyated anti-VWF aptamer that has been shown in preclinical studies to have a long half-life in nonhuman primates. It inhibits the A1 domain of VWF to prevent it from binding to platelet glycoprotein 1b (GP1b).
In the randomized, double-blind, placebo-controlled trial reported at the EHA congress, 88 healthy volunteers received single doses of BT200 ranging from 0.l8 mg to 48 mg by subcutaneous injection or intravenous infusion, 8 received multiple doses, 8 were evaluated for possible interactions with desmopressin, and 8 were evaluated for bioavailability of the aptamer.
The investigators observed a dose-related increase in BT200 concentrations, with a mean plasma terminal elimination half life of between 118 and 284 hours (about 5-12 days). There was also a dose-dependent increase in bioavailability of the agents, reaching 90% at the highest dose level.
The ability of BT200 to inhibit the A1 domains of VWF also was dose dependent, with the largest effect seen with doses of 12 mg and higher. The molecule decreased VWF activity and ristocetin-induced platelet aggregation, and prolonged collagen adenosine diphosphate closure time.
At the highest doses, BT200 caused complete inhibition of VWF (P < .001), and volunteers developed clinical signs of mild mucosal bleeding.
But the aptamer also increased in a dose-dependent fashion VWF antigen levels and factor VIII clotting activity more than fourfold (P <.001).
“This resulted in increased thrombogenicity as measured by thrombin generation and enhanced clotting. In the absence of an increase in VWF propeptide levels, this effect is considered due to decreased clearance of VWF,” the investigators wrote in the study abstract.
They noted that they saw a clinically meaningful twofold increase in both VWF and factor VIII at doses lower than 6 mg.
‘Super-exciting strategy’
“This trial identified a novel mechanism of action for BT200: It decreases the clearance of VWF/FVIII, which can be exploited for congenital bleeding disorders. This built a solid foundation for an ongoing basket trial in patients with von Willebrand disease or hemophilia A, which already confirms the expected effect sizes,” Dr. Kovacevic and colleagues wrote.
“I will be interested to see what the clinical side effects are, because there may be some off-target effects, but in reality it is a super-exciting strategy, and there is really a dire need for longer half-life products for these patients,” Dr. Flood said.
The study was sponsored by Band Therapeutics, a division of Guardian Therapeutics. Dr. Kovacevic and Dr. Flood reported having no conflicts of interest to disclose.
A novel therapeutic approach using aptamers – short single strands of DNA or RNA designed to selectively bind to a target – shows promise for treating von Willebrand Disease (VWD), and other congenital bleed disorders such as hemophilia A, investigators say.
In a proof-of-concept study using healthy volunteers, the experimental anti–von Willebrand factor (VWF) molecule BT200 appeared to decrease clearance of VWF and resulted in a twofold increase in endogenous levels of VWF and factor VIII at low doses.
BT200 is currently being explored in a phase 2 trial in patients with hemophilia A and VWD type 2B, Katarina Kovacevic, MPharm, from the Medical University of Vienna, reported at the European Hematology Association annual congress.
“We expect to see a half-life increase of 2 to 4 times of factor VIII products, which will allow us to have a longer time between treatments,” she said in an oral abstract presentation (Abstract S302).
Lab-made nucleotide strings
Aptamers are sometimes call “chemical antibodies” because of their high affinity and high specificity for extracellular targets, Dr. Kovacevic said. Unlike conventional humanized or human-derived antibodies, however, they are nonimmunogenic and are less costly to manufacture.
In a previous study from her center, a different anti-VWF aptamer labeled ARC1779 increased plasma levels of VWF, factor VIII, and platelet counts in patients with VWD type 2B.
However, the drug was inconvenient to use, requiring 72-hour infusions, she noted.
In a study published in Feb. 4, 2021 in Scientific Reports, Dr. Kovacevic and colleagues reported that BT200 blocks VWF and platelet function in patients with ischemic strokes, even in the presence of high levels of VWF in patients with left carotid artery atherosclerotic strokes.
The ability of the molecule to block VWF platelet binding may explain how the anti-VWF agent actually results in higher circulating levels of VWF, which also carries factor VIII, said Veronica H. Flood, MD, a VWD specialist at Children’s Hospital of Wisconsin and associate professor at the Medical College of Wisconsin in Milwaukee.
“It might inhibit clearance of the von Willebrand factor, so it’s almost like this was an incidental side effect,” she said in an interview. “Incidentally, this happens to also give you higher levels of the von Willebrand factor and the factor VIII, and with a longer half-life than anything we currently have, so it’s a super-creative strategy,” she said.
Dr. Flood was not involved in the study.
Long half-life
BT200 is a third-generation peglyated anti-VWF aptamer that has been shown in preclinical studies to have a long half-life in nonhuman primates. It inhibits the A1 domain of VWF to prevent it from binding to platelet glycoprotein 1b (GP1b).
In the randomized, double-blind, placebo-controlled trial reported at the EHA congress, 88 healthy volunteers received single doses of BT200 ranging from 0.l8 mg to 48 mg by subcutaneous injection or intravenous infusion, 8 received multiple doses, 8 were evaluated for possible interactions with desmopressin, and 8 were evaluated for bioavailability of the aptamer.
The investigators observed a dose-related increase in BT200 concentrations, with a mean plasma terminal elimination half life of between 118 and 284 hours (about 5-12 days). There was also a dose-dependent increase in bioavailability of the agents, reaching 90% at the highest dose level.
The ability of BT200 to inhibit the A1 domains of VWF also was dose dependent, with the largest effect seen with doses of 12 mg and higher. The molecule decreased VWF activity and ristocetin-induced platelet aggregation, and prolonged collagen adenosine diphosphate closure time.
At the highest doses, BT200 caused complete inhibition of VWF (P < .001), and volunteers developed clinical signs of mild mucosal bleeding.
But the aptamer also increased in a dose-dependent fashion VWF antigen levels and factor VIII clotting activity more than fourfold (P <.001).
“This resulted in increased thrombogenicity as measured by thrombin generation and enhanced clotting. In the absence of an increase in VWF propeptide levels, this effect is considered due to decreased clearance of VWF,” the investigators wrote in the study abstract.
They noted that they saw a clinically meaningful twofold increase in both VWF and factor VIII at doses lower than 6 mg.
‘Super-exciting strategy’
“This trial identified a novel mechanism of action for BT200: It decreases the clearance of VWF/FVIII, which can be exploited for congenital bleeding disorders. This built a solid foundation for an ongoing basket trial in patients with von Willebrand disease or hemophilia A, which already confirms the expected effect sizes,” Dr. Kovacevic and colleagues wrote.
“I will be interested to see what the clinical side effects are, because there may be some off-target effects, but in reality it is a super-exciting strategy, and there is really a dire need for longer half-life products for these patients,” Dr. Flood said.
The study was sponsored by Band Therapeutics, a division of Guardian Therapeutics. Dr. Kovacevic and Dr. Flood reported having no conflicts of interest to disclose.
A novel therapeutic approach using aptamers – short single strands of DNA or RNA designed to selectively bind to a target – shows promise for treating von Willebrand Disease (VWD), and other congenital bleed disorders such as hemophilia A, investigators say.
In a proof-of-concept study using healthy volunteers, the experimental anti–von Willebrand factor (VWF) molecule BT200 appeared to decrease clearance of VWF and resulted in a twofold increase in endogenous levels of VWF and factor VIII at low doses.
BT200 is currently being explored in a phase 2 trial in patients with hemophilia A and VWD type 2B, Katarina Kovacevic, MPharm, from the Medical University of Vienna, reported at the European Hematology Association annual congress.
“We expect to see a half-life increase of 2 to 4 times of factor VIII products, which will allow us to have a longer time between treatments,” she said in an oral abstract presentation (Abstract S302).
Lab-made nucleotide strings
Aptamers are sometimes call “chemical antibodies” because of their high affinity and high specificity for extracellular targets, Dr. Kovacevic said. Unlike conventional humanized or human-derived antibodies, however, they are nonimmunogenic and are less costly to manufacture.
In a previous study from her center, a different anti-VWF aptamer labeled ARC1779 increased plasma levels of VWF, factor VIII, and platelet counts in patients with VWD type 2B.
However, the drug was inconvenient to use, requiring 72-hour infusions, she noted.
In a study published in Feb. 4, 2021 in Scientific Reports, Dr. Kovacevic and colleagues reported that BT200 blocks VWF and platelet function in patients with ischemic strokes, even in the presence of high levels of VWF in patients with left carotid artery atherosclerotic strokes.
The ability of the molecule to block VWF platelet binding may explain how the anti-VWF agent actually results in higher circulating levels of VWF, which also carries factor VIII, said Veronica H. Flood, MD, a VWD specialist at Children’s Hospital of Wisconsin and associate professor at the Medical College of Wisconsin in Milwaukee.
“It might inhibit clearance of the von Willebrand factor, so it’s almost like this was an incidental side effect,” she said in an interview. “Incidentally, this happens to also give you higher levels of the von Willebrand factor and the factor VIII, and with a longer half-life than anything we currently have, so it’s a super-creative strategy,” she said.
Dr. Flood was not involved in the study.
Long half-life
BT200 is a third-generation peglyated anti-VWF aptamer that has been shown in preclinical studies to have a long half-life in nonhuman primates. It inhibits the A1 domain of VWF to prevent it from binding to platelet glycoprotein 1b (GP1b).
In the randomized, double-blind, placebo-controlled trial reported at the EHA congress, 88 healthy volunteers received single doses of BT200 ranging from 0.l8 mg to 48 mg by subcutaneous injection or intravenous infusion, 8 received multiple doses, 8 were evaluated for possible interactions with desmopressin, and 8 were evaluated for bioavailability of the aptamer.
The investigators observed a dose-related increase in BT200 concentrations, with a mean plasma terminal elimination half life of between 118 and 284 hours (about 5-12 days). There was also a dose-dependent increase in bioavailability of the agents, reaching 90% at the highest dose level.
The ability of BT200 to inhibit the A1 domains of VWF also was dose dependent, with the largest effect seen with doses of 12 mg and higher. The molecule decreased VWF activity and ristocetin-induced platelet aggregation, and prolonged collagen adenosine diphosphate closure time.
At the highest doses, BT200 caused complete inhibition of VWF (P < .001), and volunteers developed clinical signs of mild mucosal bleeding.
But the aptamer also increased in a dose-dependent fashion VWF antigen levels and factor VIII clotting activity more than fourfold (P <.001).
“This resulted in increased thrombogenicity as measured by thrombin generation and enhanced clotting. In the absence of an increase in VWF propeptide levels, this effect is considered due to decreased clearance of VWF,” the investigators wrote in the study abstract.
They noted that they saw a clinically meaningful twofold increase in both VWF and factor VIII at doses lower than 6 mg.
‘Super-exciting strategy’
“This trial identified a novel mechanism of action for BT200: It decreases the clearance of VWF/FVIII, which can be exploited for congenital bleeding disorders. This built a solid foundation for an ongoing basket trial in patients with von Willebrand disease or hemophilia A, which already confirms the expected effect sizes,” Dr. Kovacevic and colleagues wrote.
“I will be interested to see what the clinical side effects are, because there may be some off-target effects, but in reality it is a super-exciting strategy, and there is really a dire need for longer half-life products for these patients,” Dr. Flood said.
The study was sponsored by Band Therapeutics, a division of Guardian Therapeutics. Dr. Kovacevic and Dr. Flood reported having no conflicts of interest to disclose.
FROM EHA 2021
Rapid update to ASCO breast cancer guidelines after OlympiA data
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
Reduced-intensity transplant benefits older patients with AML
Among older patients with acute myeloid leukemia (AML), survival is significantly better when they undergo reduced-intensity conditioning (RIC) before receiving an allogeneic hematopoietic cell transplant (HCT) at first remission. This improvement in survival is seen regardless of key factors such as genotype and the status of minimal residual disease (MRD) after initial chemotherapy, results from two large randomized trials show.
“Two consecutive trials of more than 1,500 older AML patients above 60 years of age demonstrate a consistent benefit for RIC transplant in first remission,” said first author Nigel Russell, MD, of Guy’s Hospital, London, and Nottingham University, England. “This benefit is seen independent of their post-course 1 MRD status,” he added.
Dr. Russell presented the new data at the European Hematology Association (EHA) 2021 Annual Meeting.
Commenting on the study, Charles Craddock, MD, said in an interview that the results “confirm the growing importance of RIC transplantation as a central treatment management strategy in high-risk AML and in this population high risk patients over 60.”
“[These findings] reinforce the evolving treatment paradigm that, in fit adults over 60 with AML, hematopoietic cell transplantation should be considered an essential component of their management plan,” said Dr. Craddock, academic director of the Center for Clinical Haematology, Queen Elizabeth Hospital, Birmingham, England.
Patients with AML who are older than 60 years can achieve complete remission with intensive chemotherapy alone; however, relapse is common, and only about 20% survive for 5 years, Dr. Russell explained.
HCT significantly improves survival outcomes, and the development of RIC has made transplantation accessible to high-risk patients by making the procedure more tolerable with lower toxicity in comparison with conventional conditioning regimens.
However, there is ongoing debate over the prognostic effect of key factors in pretransplant conditioning that may be predictive of the risk for post-transplant relapse – in particular, the presence of MRD after the first course of conditioning, he explained.
To more closely investigate those factors and the rate of survival of older patients with AML who undergo RIC transplant, Dr. Russell and his colleagues evaluated results from the National Cancer Research Institute’s (NCRI) AML16 trial, which was conducted from 2006 to 2012, and interim results from the NCRI AML18 trial, which started in 2015 and is ongoing.
Both trials employed double induction of daunorubicin and clofarabine or, in the AML16 trial, AraC ± gemtuzumab, and in the AML18 trial, daunorubicin and AraC (DA) + gemtuzumab.
In AML18, patients who were MRD positive after course 1 were randomly assigned to undergo either an intensification randomization after either FLAG-Ida or DA+cladribine or DA alone.
In AML16, of 983 patients in first complete response, 144 (15%) subsequently underwent RIC transplant. The median follow-up for survival from complete response was 45 months.
In the AML18 trial, of 847 patients, 648 patients achieved complete response. Among them, 201 (31%) underwent transplant. The median follow-up of survival was 45 months.
The results of both trials showed greater benefit with RIC transplant versus chemotherapy alone.
In the AML16 trial, among patients aged 60 to 70 who received RIC, survival at 5 years was significantly improved compared with chemotherapy alone (37% vs. 19%; hazard ratio, 0.65; 95% confidence interval, 0.52-0.82; P < .001).
In AML16, the higher survival benefit in comparison with chemotherapy alone was observed in the RIC group across subgroups of risk level, as stratified according to in the multivariate Wheatley risk group score. Subgroup stratification was based on age, cytogenics, and other factors (HR, 0.66; 95% CI, 0.53-0.83; P < .001).
Importantly, the survival benefits were significantly greater with RIC transplant regardless of MRD-negative or MRD-positive status after course 1 (HR, 0.68; 95% CI, 0.54-0.85; P < .001).
Allograft transplant was also more favorable regardless of FLT3 ITD or NPM1 mutation status (P for heterogeneity by genetic subgroups, 0.61).
In AML16, no groups were found to have benefited more with RIC. Consequently, the criteria for transplant in AML18 trial were based on patients’ health status and donor availability.
An interim analysis of the ongoing AML 18 trial further underscored an overall benefit of RIC transplant. Rates of 3-year survival from remission were 48% with RIC transplant, versus 37.4% with chemotherapy alone (P = .027). The benefit was independent of MRD status after conditioning course 1, similar to the AML16 results (HR, 0.71; 95% CI, 0.54-0.95; P = .02).
Although the rate of transplantation in the AML18 trial was higher among patients who were MRD positive in comparison with those who were MRD negative (36% vs. 24.8%), the rates of post-transplant survival were not significantly different between those who were MRD positive and those who were MRD negative after course 1 (51.1% vs. 46.6% at 3 years; P = .84).
The authors evaluated the effects of a second conditioning course on transplant outcomes among patients who did not initially achieve an MRD-negative complete remission.
They found that 60% of patients did convert from MRD-positive to MRD-negative status after course 2. Among those patients, the survival versus chemotherapy alone was substantially higher (HR, 0.32; 95% CI, 0.11-0.92) compared to those who remained MRD-negative (HR 0.74; 95% CI, 0.32-1.72).
However, the authors note that, owing to a lack of heterogeneity, the results don’t necessarily mean that the patients who remained MRD positive did not also benefit from transplant.
“There was a significant benefit for transplant in those who converted to MRD negativity,” Dr. Russell said.
“With a hazard ratio of .32, this was far superior to those who remained MRD-positive post course 2,” he said.
“These results show that MRD status after course 1 is important information in terms of response to therapy and can alter your treatment strategy if you’re considering a transplant as an option for these patients,” Dr. Russell told this news organization.
In further commenting, Dr. Craddock said the research highlights the importance of randomized trials with regard to whether patients who are MRD-positive before transplant will benefit from an additional course of therapy to reduce the MRD load.
“Most get two courses, but the question is, if they are still MRD positive, should they get a third course, and if so, what should that look like?” he said.
“There are currently no randomized controlled trials to address that ongoing question, and they need to be done,” he added.
Dr. Russell has relationships with Pfizer, Astellas, and Jazz Pharma. Dr. Craddock has a relationship with Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
Among older patients with acute myeloid leukemia (AML), survival is significantly better when they undergo reduced-intensity conditioning (RIC) before receiving an allogeneic hematopoietic cell transplant (HCT) at first remission. This improvement in survival is seen regardless of key factors such as genotype and the status of minimal residual disease (MRD) after initial chemotherapy, results from two large randomized trials show.
“Two consecutive trials of more than 1,500 older AML patients above 60 years of age demonstrate a consistent benefit for RIC transplant in first remission,” said first author Nigel Russell, MD, of Guy’s Hospital, London, and Nottingham University, England. “This benefit is seen independent of their post-course 1 MRD status,” he added.
Dr. Russell presented the new data at the European Hematology Association (EHA) 2021 Annual Meeting.
Commenting on the study, Charles Craddock, MD, said in an interview that the results “confirm the growing importance of RIC transplantation as a central treatment management strategy in high-risk AML and in this population high risk patients over 60.”
“[These findings] reinforce the evolving treatment paradigm that, in fit adults over 60 with AML, hematopoietic cell transplantation should be considered an essential component of their management plan,” said Dr. Craddock, academic director of the Center for Clinical Haematology, Queen Elizabeth Hospital, Birmingham, England.
Patients with AML who are older than 60 years can achieve complete remission with intensive chemotherapy alone; however, relapse is common, and only about 20% survive for 5 years, Dr. Russell explained.
HCT significantly improves survival outcomes, and the development of RIC has made transplantation accessible to high-risk patients by making the procedure more tolerable with lower toxicity in comparison with conventional conditioning regimens.
However, there is ongoing debate over the prognostic effect of key factors in pretransplant conditioning that may be predictive of the risk for post-transplant relapse – in particular, the presence of MRD after the first course of conditioning, he explained.
To more closely investigate those factors and the rate of survival of older patients with AML who undergo RIC transplant, Dr. Russell and his colleagues evaluated results from the National Cancer Research Institute’s (NCRI) AML16 trial, which was conducted from 2006 to 2012, and interim results from the NCRI AML18 trial, which started in 2015 and is ongoing.
Both trials employed double induction of daunorubicin and clofarabine or, in the AML16 trial, AraC ± gemtuzumab, and in the AML18 trial, daunorubicin and AraC (DA) + gemtuzumab.
In AML18, patients who were MRD positive after course 1 were randomly assigned to undergo either an intensification randomization after either FLAG-Ida or DA+cladribine or DA alone.
In AML16, of 983 patients in first complete response, 144 (15%) subsequently underwent RIC transplant. The median follow-up for survival from complete response was 45 months.
In the AML18 trial, of 847 patients, 648 patients achieved complete response. Among them, 201 (31%) underwent transplant. The median follow-up of survival was 45 months.
The results of both trials showed greater benefit with RIC transplant versus chemotherapy alone.
In the AML16 trial, among patients aged 60 to 70 who received RIC, survival at 5 years was significantly improved compared with chemotherapy alone (37% vs. 19%; hazard ratio, 0.65; 95% confidence interval, 0.52-0.82; P < .001).
In AML16, the higher survival benefit in comparison with chemotherapy alone was observed in the RIC group across subgroups of risk level, as stratified according to in the multivariate Wheatley risk group score. Subgroup stratification was based on age, cytogenics, and other factors (HR, 0.66; 95% CI, 0.53-0.83; P < .001).
Importantly, the survival benefits were significantly greater with RIC transplant regardless of MRD-negative or MRD-positive status after course 1 (HR, 0.68; 95% CI, 0.54-0.85; P < .001).
Allograft transplant was also more favorable regardless of FLT3 ITD or NPM1 mutation status (P for heterogeneity by genetic subgroups, 0.61).
In AML16, no groups were found to have benefited more with RIC. Consequently, the criteria for transplant in AML18 trial were based on patients’ health status and donor availability.
An interim analysis of the ongoing AML 18 trial further underscored an overall benefit of RIC transplant. Rates of 3-year survival from remission were 48% with RIC transplant, versus 37.4% with chemotherapy alone (P = .027). The benefit was independent of MRD status after conditioning course 1, similar to the AML16 results (HR, 0.71; 95% CI, 0.54-0.95; P = .02).
Although the rate of transplantation in the AML18 trial was higher among patients who were MRD positive in comparison with those who were MRD negative (36% vs. 24.8%), the rates of post-transplant survival were not significantly different between those who were MRD positive and those who were MRD negative after course 1 (51.1% vs. 46.6% at 3 years; P = .84).
The authors evaluated the effects of a second conditioning course on transplant outcomes among patients who did not initially achieve an MRD-negative complete remission.
They found that 60% of patients did convert from MRD-positive to MRD-negative status after course 2. Among those patients, the survival versus chemotherapy alone was substantially higher (HR, 0.32; 95% CI, 0.11-0.92) compared to those who remained MRD-negative (HR 0.74; 95% CI, 0.32-1.72).
However, the authors note that, owing to a lack of heterogeneity, the results don’t necessarily mean that the patients who remained MRD positive did not also benefit from transplant.
“There was a significant benefit for transplant in those who converted to MRD negativity,” Dr. Russell said.
“With a hazard ratio of .32, this was far superior to those who remained MRD-positive post course 2,” he said.
“These results show that MRD status after course 1 is important information in terms of response to therapy and can alter your treatment strategy if you’re considering a transplant as an option for these patients,” Dr. Russell told this news organization.
In further commenting, Dr. Craddock said the research highlights the importance of randomized trials with regard to whether patients who are MRD-positive before transplant will benefit from an additional course of therapy to reduce the MRD load.
“Most get two courses, but the question is, if they are still MRD positive, should they get a third course, and if so, what should that look like?” he said.
“There are currently no randomized controlled trials to address that ongoing question, and they need to be done,” he added.
Dr. Russell has relationships with Pfizer, Astellas, and Jazz Pharma. Dr. Craddock has a relationship with Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
Among older patients with acute myeloid leukemia (AML), survival is significantly better when they undergo reduced-intensity conditioning (RIC) before receiving an allogeneic hematopoietic cell transplant (HCT) at first remission. This improvement in survival is seen regardless of key factors such as genotype and the status of minimal residual disease (MRD) after initial chemotherapy, results from two large randomized trials show.
“Two consecutive trials of more than 1,500 older AML patients above 60 years of age demonstrate a consistent benefit for RIC transplant in first remission,” said first author Nigel Russell, MD, of Guy’s Hospital, London, and Nottingham University, England. “This benefit is seen independent of their post-course 1 MRD status,” he added.
Dr. Russell presented the new data at the European Hematology Association (EHA) 2021 Annual Meeting.
Commenting on the study, Charles Craddock, MD, said in an interview that the results “confirm the growing importance of RIC transplantation as a central treatment management strategy in high-risk AML and in this population high risk patients over 60.”
“[These findings] reinforce the evolving treatment paradigm that, in fit adults over 60 with AML, hematopoietic cell transplantation should be considered an essential component of their management plan,” said Dr. Craddock, academic director of the Center for Clinical Haematology, Queen Elizabeth Hospital, Birmingham, England.
Patients with AML who are older than 60 years can achieve complete remission with intensive chemotherapy alone; however, relapse is common, and only about 20% survive for 5 years, Dr. Russell explained.
HCT significantly improves survival outcomes, and the development of RIC has made transplantation accessible to high-risk patients by making the procedure more tolerable with lower toxicity in comparison with conventional conditioning regimens.
However, there is ongoing debate over the prognostic effect of key factors in pretransplant conditioning that may be predictive of the risk for post-transplant relapse – in particular, the presence of MRD after the first course of conditioning, he explained.
To more closely investigate those factors and the rate of survival of older patients with AML who undergo RIC transplant, Dr. Russell and his colleagues evaluated results from the National Cancer Research Institute’s (NCRI) AML16 trial, which was conducted from 2006 to 2012, and interim results from the NCRI AML18 trial, which started in 2015 and is ongoing.
Both trials employed double induction of daunorubicin and clofarabine or, in the AML16 trial, AraC ± gemtuzumab, and in the AML18 trial, daunorubicin and AraC (DA) + gemtuzumab.
In AML18, patients who were MRD positive after course 1 were randomly assigned to undergo either an intensification randomization after either FLAG-Ida or DA+cladribine or DA alone.
In AML16, of 983 patients in first complete response, 144 (15%) subsequently underwent RIC transplant. The median follow-up for survival from complete response was 45 months.
In the AML18 trial, of 847 patients, 648 patients achieved complete response. Among them, 201 (31%) underwent transplant. The median follow-up of survival was 45 months.
The results of both trials showed greater benefit with RIC transplant versus chemotherapy alone.
In the AML16 trial, among patients aged 60 to 70 who received RIC, survival at 5 years was significantly improved compared with chemotherapy alone (37% vs. 19%; hazard ratio, 0.65; 95% confidence interval, 0.52-0.82; P < .001).
In AML16, the higher survival benefit in comparison with chemotherapy alone was observed in the RIC group across subgroups of risk level, as stratified according to in the multivariate Wheatley risk group score. Subgroup stratification was based on age, cytogenics, and other factors (HR, 0.66; 95% CI, 0.53-0.83; P < .001).
Importantly, the survival benefits were significantly greater with RIC transplant regardless of MRD-negative or MRD-positive status after course 1 (HR, 0.68; 95% CI, 0.54-0.85; P < .001).
Allograft transplant was also more favorable regardless of FLT3 ITD or NPM1 mutation status (P for heterogeneity by genetic subgroups, 0.61).
In AML16, no groups were found to have benefited more with RIC. Consequently, the criteria for transplant in AML18 trial were based on patients’ health status and donor availability.
An interim analysis of the ongoing AML 18 trial further underscored an overall benefit of RIC transplant. Rates of 3-year survival from remission were 48% with RIC transplant, versus 37.4% with chemotherapy alone (P = .027). The benefit was independent of MRD status after conditioning course 1, similar to the AML16 results (HR, 0.71; 95% CI, 0.54-0.95; P = .02).
Although the rate of transplantation in the AML18 trial was higher among patients who were MRD positive in comparison with those who were MRD negative (36% vs. 24.8%), the rates of post-transplant survival were not significantly different between those who were MRD positive and those who were MRD negative after course 1 (51.1% vs. 46.6% at 3 years; P = .84).
The authors evaluated the effects of a second conditioning course on transplant outcomes among patients who did not initially achieve an MRD-negative complete remission.
They found that 60% of patients did convert from MRD-positive to MRD-negative status after course 2. Among those patients, the survival versus chemotherapy alone was substantially higher (HR, 0.32; 95% CI, 0.11-0.92) compared to those who remained MRD-negative (HR 0.74; 95% CI, 0.32-1.72).
However, the authors note that, owing to a lack of heterogeneity, the results don’t necessarily mean that the patients who remained MRD positive did not also benefit from transplant.
“There was a significant benefit for transplant in those who converted to MRD negativity,” Dr. Russell said.
“With a hazard ratio of .32, this was far superior to those who remained MRD-positive post course 2,” he said.
“These results show that MRD status after course 1 is important information in terms of response to therapy and can alter your treatment strategy if you’re considering a transplant as an option for these patients,” Dr. Russell told this news organization.
In further commenting, Dr. Craddock said the research highlights the importance of randomized trials with regard to whether patients who are MRD-positive before transplant will benefit from an additional course of therapy to reduce the MRD load.
“Most get two courses, but the question is, if they are still MRD positive, should they get a third course, and if so, what should that look like?” he said.
“There are currently no randomized controlled trials to address that ongoing question, and they need to be done,” he added.
Dr. Russell has relationships with Pfizer, Astellas, and Jazz Pharma. Dr. Craddock has a relationship with Bristol-Myers Squibb.
A version of this article first appeared on Medscape.com.
DCIS: Biosignature helps guide postlumpectomy decisions
A biosignature tool helps women avoid unnecessary radiotherapy after undergoing lumpectomy for ductal carcinoma in situ (DCIS) – and also identifies women who need more intense treatment.
The DCISionRT test (PreludeDx) and its response subtype (Rst) biosignature provide personalized risk assessment, explains Frank Vicini, MD, a radiation oncologist at GenesisCare and a member of NRG Oncology, Pontiac, Mich.
He presented data on the test at a poster at the recent American Society of Clinical Oncology Annual Meeting.
They can also identify patients who would likely benefit from radiotherapy, Dr. Vicini reported.
The tool shows promise for identifying those whose cancer is likely to recur despite undergoing postlumpectomy radiotherapy – women who might benefit from intensified or alternate treatment approaches, he added.
The latter finding is particularly provocative because it suggests that the biosignatures “may appropriately identify patients with very radioresistant ductal carcinoma in situ,” Benjamin D. Smith, MD, commented during a poster discussion session at the meeting.
“I think these findings merit validation in translational research models,” said Dr. Smith, a radiation oncologist and professor of radiation oncology and health services research at the University of Texas MD Anderson Cancer Center, Houston.
DCISionRT, Rst, and risk
DCISionRT combines molecular biology innovations with risk-based scores to assess risk for recurrence, which is classified as either low or elevated, according to the test developer, PreludeDx.
Dr. Vicini and colleagues used the test to classify tissue samples from 485 women who were part of previous DCISionRT validation cohorts in Sweden, Australia, and the United States. The patients underwent breast cancer surgery (BCS) with or without radiotherapy between 1996 and 2011.
The Rst biosignature was used to further categorize those in the elevated-risk group as having a good response subtype (good Rst) or a poor response subtype (poor Rst) after BCS plus radiotherapy.
Radiotherapy was associated with significantly reduced recurrence rates among women with elevated risk and a good Rst (the hazard ratios for ipsilateral breast tumor recurrence [IBTR] and invasive breast cancer [IBC] were 0.18 and 0.15, respectively).
No radiotherapy benefit was seen among those with elevated risk and poor Rst.
The investigators also reported that, among patients with a poor Rst, 10-year IBTR and IBC rates were 25% and 16%, respectively, regardless of whether they received radiotherapy. These rates were much higher than the rates among women with good Rst (6.6% and 4.5%; hazard ratio, 3.6 and 4.4, respectively).
No significant difference was seen in 10-year IBTR and IBC rates among patients in the low-risk group, with or without radiotherapy.
Traditional clinicopathologic risk factors, including age younger than 50 years, grade 3 disease, and tumor size greater than 2.5 cm, did not identify poor versus good response subtypes in this cohort, and on multivariable analysis, neither of these factors nor endocrine therapy was significantly associated with IBTR or IBC.
Prospective validation needed
In his discussion, Dr. Smith said that the study provides “important data” that further validate the DCISionRT platform alone for assessing risk among women with DCIS who undergo BCS. But it is the Rst biosignature, which allows clinicians to “predict radioresistance of residual malignant chromogens following lumpectomy plus radiation therapy,” that really stands out, he added.
From the data presented, “it is reasonable to conclude that patients with a poor Rst score treated with lumpectomy and radiation had a much higher risk of in-breast tumor recurrence than one might predict or anticipate based on existing published randomized clinical trial data,” he said.
“In my opinion, it is very important to prospectively validate this finding with other cohorts,” he said. “Moving forward, I think there may come a time where there may be interest in studying radiosensitizing agents for poor-Rst ductal carcinoma in situ that are resistant to standard doses of radiation, and it may be that we consider the Rst as a factor moving forward in selecting patients for BCT versus mastectomy.”
However, because 75% of patients at elevated risk with poor Rst who undergo lumpectomy and radiotherapy do not experience recurrence in the decade following their treatment, it would be “inappropriate and misguided” to start recommending mastectomy for patients at DCISionRT elevated risk who have poor Rst, he said.
The study was funded by PreludeDx. Dr. Vicini reported employment with 21st Century Oncology and financial relationships with ImpediMed, Prelude Therapeutics, and Concure Oncology. Dr. Smith, through his employer, has an equity interest in Oncora Medical through a partnership agreement. He also has an uncompensated relationship with the American Society for Radiation Oncology.
A version of this article first appeared on Medscape.com.
A biosignature tool helps women avoid unnecessary radiotherapy after undergoing lumpectomy for ductal carcinoma in situ (DCIS) – and also identifies women who need more intense treatment.
The DCISionRT test (PreludeDx) and its response subtype (Rst) biosignature provide personalized risk assessment, explains Frank Vicini, MD, a radiation oncologist at GenesisCare and a member of NRG Oncology, Pontiac, Mich.
He presented data on the test at a poster at the recent American Society of Clinical Oncology Annual Meeting.
They can also identify patients who would likely benefit from radiotherapy, Dr. Vicini reported.
The tool shows promise for identifying those whose cancer is likely to recur despite undergoing postlumpectomy radiotherapy – women who might benefit from intensified or alternate treatment approaches, he added.
The latter finding is particularly provocative because it suggests that the biosignatures “may appropriately identify patients with very radioresistant ductal carcinoma in situ,” Benjamin D. Smith, MD, commented during a poster discussion session at the meeting.
“I think these findings merit validation in translational research models,” said Dr. Smith, a radiation oncologist and professor of radiation oncology and health services research at the University of Texas MD Anderson Cancer Center, Houston.
DCISionRT, Rst, and risk
DCISionRT combines molecular biology innovations with risk-based scores to assess risk for recurrence, which is classified as either low or elevated, according to the test developer, PreludeDx.
Dr. Vicini and colleagues used the test to classify tissue samples from 485 women who were part of previous DCISionRT validation cohorts in Sweden, Australia, and the United States. The patients underwent breast cancer surgery (BCS) with or without radiotherapy between 1996 and 2011.
The Rst biosignature was used to further categorize those in the elevated-risk group as having a good response subtype (good Rst) or a poor response subtype (poor Rst) after BCS plus radiotherapy.
Radiotherapy was associated with significantly reduced recurrence rates among women with elevated risk and a good Rst (the hazard ratios for ipsilateral breast tumor recurrence [IBTR] and invasive breast cancer [IBC] were 0.18 and 0.15, respectively).
No radiotherapy benefit was seen among those with elevated risk and poor Rst.
The investigators also reported that, among patients with a poor Rst, 10-year IBTR and IBC rates were 25% and 16%, respectively, regardless of whether they received radiotherapy. These rates were much higher than the rates among women with good Rst (6.6% and 4.5%; hazard ratio, 3.6 and 4.4, respectively).
No significant difference was seen in 10-year IBTR and IBC rates among patients in the low-risk group, with or without radiotherapy.
Traditional clinicopathologic risk factors, including age younger than 50 years, grade 3 disease, and tumor size greater than 2.5 cm, did not identify poor versus good response subtypes in this cohort, and on multivariable analysis, neither of these factors nor endocrine therapy was significantly associated with IBTR or IBC.
Prospective validation needed
In his discussion, Dr. Smith said that the study provides “important data” that further validate the DCISionRT platform alone for assessing risk among women with DCIS who undergo BCS. But it is the Rst biosignature, which allows clinicians to “predict radioresistance of residual malignant chromogens following lumpectomy plus radiation therapy,” that really stands out, he added.
From the data presented, “it is reasonable to conclude that patients with a poor Rst score treated with lumpectomy and radiation had a much higher risk of in-breast tumor recurrence than one might predict or anticipate based on existing published randomized clinical trial data,” he said.
“In my opinion, it is very important to prospectively validate this finding with other cohorts,” he said. “Moving forward, I think there may come a time where there may be interest in studying radiosensitizing agents for poor-Rst ductal carcinoma in situ that are resistant to standard doses of radiation, and it may be that we consider the Rst as a factor moving forward in selecting patients for BCT versus mastectomy.”
However, because 75% of patients at elevated risk with poor Rst who undergo lumpectomy and radiotherapy do not experience recurrence in the decade following their treatment, it would be “inappropriate and misguided” to start recommending mastectomy for patients at DCISionRT elevated risk who have poor Rst, he said.
The study was funded by PreludeDx. Dr. Vicini reported employment with 21st Century Oncology and financial relationships with ImpediMed, Prelude Therapeutics, and Concure Oncology. Dr. Smith, through his employer, has an equity interest in Oncora Medical through a partnership agreement. He also has an uncompensated relationship with the American Society for Radiation Oncology.
A version of this article first appeared on Medscape.com.
A biosignature tool helps women avoid unnecessary radiotherapy after undergoing lumpectomy for ductal carcinoma in situ (DCIS) – and also identifies women who need more intense treatment.
The DCISionRT test (PreludeDx) and its response subtype (Rst) biosignature provide personalized risk assessment, explains Frank Vicini, MD, a radiation oncologist at GenesisCare and a member of NRG Oncology, Pontiac, Mich.
He presented data on the test at a poster at the recent American Society of Clinical Oncology Annual Meeting.
They can also identify patients who would likely benefit from radiotherapy, Dr. Vicini reported.
The tool shows promise for identifying those whose cancer is likely to recur despite undergoing postlumpectomy radiotherapy – women who might benefit from intensified or alternate treatment approaches, he added.
The latter finding is particularly provocative because it suggests that the biosignatures “may appropriately identify patients with very radioresistant ductal carcinoma in situ,” Benjamin D. Smith, MD, commented during a poster discussion session at the meeting.
“I think these findings merit validation in translational research models,” said Dr. Smith, a radiation oncologist and professor of radiation oncology and health services research at the University of Texas MD Anderson Cancer Center, Houston.
DCISionRT, Rst, and risk
DCISionRT combines molecular biology innovations with risk-based scores to assess risk for recurrence, which is classified as either low or elevated, according to the test developer, PreludeDx.
Dr. Vicini and colleagues used the test to classify tissue samples from 485 women who were part of previous DCISionRT validation cohorts in Sweden, Australia, and the United States. The patients underwent breast cancer surgery (BCS) with or without radiotherapy between 1996 and 2011.
The Rst biosignature was used to further categorize those in the elevated-risk group as having a good response subtype (good Rst) or a poor response subtype (poor Rst) after BCS plus radiotherapy.
Radiotherapy was associated with significantly reduced recurrence rates among women with elevated risk and a good Rst (the hazard ratios for ipsilateral breast tumor recurrence [IBTR] and invasive breast cancer [IBC] were 0.18 and 0.15, respectively).
No radiotherapy benefit was seen among those with elevated risk and poor Rst.
The investigators also reported that, among patients with a poor Rst, 10-year IBTR and IBC rates were 25% and 16%, respectively, regardless of whether they received radiotherapy. These rates were much higher than the rates among women with good Rst (6.6% and 4.5%; hazard ratio, 3.6 and 4.4, respectively).
No significant difference was seen in 10-year IBTR and IBC rates among patients in the low-risk group, with or without radiotherapy.
Traditional clinicopathologic risk factors, including age younger than 50 years, grade 3 disease, and tumor size greater than 2.5 cm, did not identify poor versus good response subtypes in this cohort, and on multivariable analysis, neither of these factors nor endocrine therapy was significantly associated with IBTR or IBC.
Prospective validation needed
In his discussion, Dr. Smith said that the study provides “important data” that further validate the DCISionRT platform alone for assessing risk among women with DCIS who undergo BCS. But it is the Rst biosignature, which allows clinicians to “predict radioresistance of residual malignant chromogens following lumpectomy plus radiation therapy,” that really stands out, he added.
From the data presented, “it is reasonable to conclude that patients with a poor Rst score treated with lumpectomy and radiation had a much higher risk of in-breast tumor recurrence than one might predict or anticipate based on existing published randomized clinical trial data,” he said.
“In my opinion, it is very important to prospectively validate this finding with other cohorts,” he said. “Moving forward, I think there may come a time where there may be interest in studying radiosensitizing agents for poor-Rst ductal carcinoma in situ that are resistant to standard doses of radiation, and it may be that we consider the Rst as a factor moving forward in selecting patients for BCT versus mastectomy.”
However, because 75% of patients at elevated risk with poor Rst who undergo lumpectomy and radiotherapy do not experience recurrence in the decade following their treatment, it would be “inappropriate and misguided” to start recommending mastectomy for patients at DCISionRT elevated risk who have poor Rst, he said.
The study was funded by PreludeDx. Dr. Vicini reported employment with 21st Century Oncology and financial relationships with ImpediMed, Prelude Therapeutics, and Concure Oncology. Dr. Smith, through his employer, has an equity interest in Oncora Medical through a partnership agreement. He also has an uncompensated relationship with the American Society for Radiation Oncology.
A version of this article first appeared on Medscape.com.
Americans’ sun protection practices fall short of intentions
commissioned by the American Academy of Dermatology.
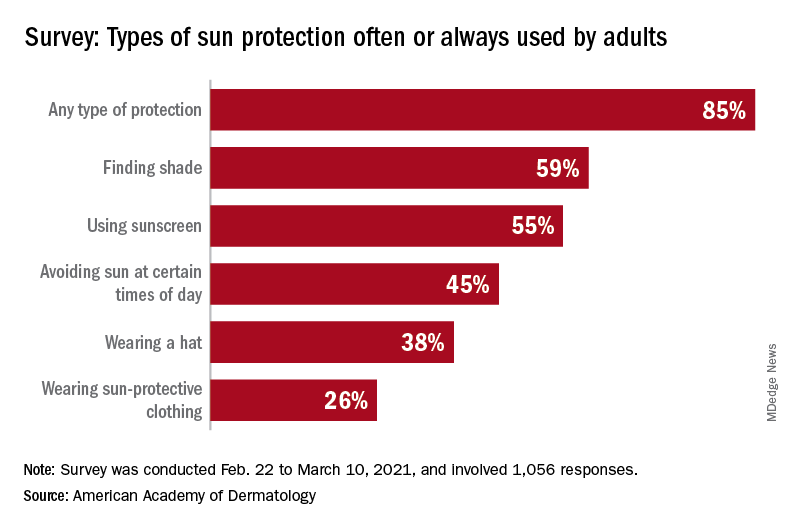
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
commissioned by the American Academy of Dermatology.
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
commissioned by the American Academy of Dermatology.
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
Freezing breast cancer to death avoids surgery: Why not further along?
In the United States, cryoablation or freezing tissue to death is a primary treatment option for a variety of cancers, including those originating in or spread to the bone, cervix, eye, kidney, liver, lung, pancreas, prostate, and skin.
Cryoablation for prostate cancer, one of the most common cancers in men, was first approved in the 1990s.
But unlike in Europe, this nonsurgical approach is not approved for breast cancer in the United States; it is one of the most common cancers in women.
So why is this approach still experimental for breast cancer?
“I don’t know,” answered cryoablation researcher Richard Fine, MD, of West Cancer Center in Germantown, Tenn., when asked by this news organization.
“It’s very interesting how slow the [Food and Drug Administration] is in approving devices for breast cancer [when compared with] other cancers,” he said.
New clinical data
Perhaps new clinical data will eventually lead to approval of this nonsurgical technique for use in low-risk breast cancer. However, the related trial had a controversial design that might discourage uptake by practitioners if it is approved, said an expert not involved in the study.
Nevertheless, the new data show that cryoablation can be an effective treatment for small, low-risk, early-stage breast cancers in older patients.
The findings come from ICE-3, a multicenter single-arm study of cryoablation in 194 such patients with mean follow-up of roughly 3 years.
It used liquid nitrogen-based cryoablation technology from IceCure Medical Ltd., an Israeli company and the study sponsor.
The results show that 2.06% (n = 4) of patients had a recurrence in the same breast, which is “basically the same” as lumpectomy, the surgical standard for this patient group, said Dr. Fine, the lead investigator on the trial.
These are interim data, Dr. Fine said at the American Society of Breast Surgeons annual meeting, held virtually.
The primary outcome is the 5-year recurrence rate, and this is the first-ever cryoablation trial that does not involve follow-up surgery, he said.
Cryoablation, which delivers a gas to a tumor via a thin needle-like probe that is guided by ultrasound, has multiple advantages over surgery, Dr. Fine said.
“The noninvasive procedure is fast, painless, and can be delivered under local anesthesia in a doctor’s office. Recovery time is minimal and cosmetic outcomes are excellent with little loss of breast tissue and no scarring,” he said in a meeting press statement.
The potential market for cryoablation in breast cancer is large, as it is intended for tumors ≤1.5 cm, which comprise approximately 60%-70% of stage 1 breast cancers that are hormone receptor–positive (HR+), and HER2-negative (HER2–), Dr. Fine said in an interview.
Cryoablation is part of a logical, de-escalation of breast cancer care, he added. “We have moved from radical mastectomy to modified mastectomy to lumpectomy – so the next step in that evolution is ablative technology, which is ‘nonsurgical.’ ”
There are other experimental ablative treatments for breast cancer including high-frequency ultrasound and laser, but cryoablation is the furthest along in development.
Cryoablation as a primary cancer treatment was first approved for coverage by the Centers for Medicare & Medicaid Services for localized prostate cancer in 1999.
But the concept extends back to 1845, when English physician James Arnott first used iced salt solutions (about –20 °C or – 4 °F) to induce tissue necrosis, reducing tumor size and ameliorating pain. Because the crude cryogen needed to be applied topically, the pioneering technique was limited to breast and cervical cancers because of their accessibility.
Not likely to show superiority
The new study’s population was composed of women aged 60 years or older (mean of 75 years) with unifocal invasive ductal cancers measuring ≤1.5 cm or less that were all low-grade, HR+, and HER2–, as noted.
The liquid nitrogen–based cryoablation consisted of a freeze-thaw-freeze cycle that totals 20-40 minutes, with freezing temperatures targeting the tumor area and turning it into an “ice ball.”
That ice ball eventually surrounds the tumor, creating a “lethal zone,” and thus a margin in which no cancer exists, akin to surgery, said Dr. Fine.
There were no significant device-related adverse events or complications reported, say the investigators. Most of the adverse events were minor and included bruising, localized edema, minor skin freeze burn, rash, minor bleeding from needle insertion, minor local hematoma, skin induration, minor infection, and pruritis.
Two of 15 patients who underwent sentinel lymph node biopsies had a positive sentinel node. At the discretion of their treating physician, 27 patients underwent adjuvant radiation, 1 patient received chemotherapy, and 148 began endocrine therapy. More than 95% of the patients and 98% of physicians reported satisfaction from the cosmetic results during follow-up visits.
Because not all patients underwent sentinel lymph node biopsy and adjuvant radiation, there is likely to be controversy about this approach, suggested Deanna J. Attai, MD, a breast surgeon at the University of California, Los Angeles, and past president of the American Society of Breast Surgeons, who was asked for comment.
“We have studies that [indicate that] these treatments don’t add significant benefit [in this patient population] but there still is this hesitation [to forgo them],” she told this news organization.
“The patients in this study were exceedingly low risk,” she emphasized.
“Is 5 years enough to assess recurrence rates? The answer is probably no. Recurrences or distant metastases are more likely to happen 10-20 years later.”
Thus, it will be difficult to show that cryoablation is superior to surgery, she said.
“You can show that cryoablation is not inferior to lumpectomy alone – which allows patients to avoid the operating room,” Dr. Attai summarized.
The surgical mindset and breast cancer
Dr. Attai, who was not involved in the current trial, was an investigator in an earlier single-arm cooperative group study of cryoablation for breast cancer, which had the rate of complete tumor ablation as the primary outcome. The study, known as the American College of Surgeons Oncology Group Z1072 trial, enrolled 99 patients, all of whom underwent ablation followed by surgery. The study reported results in 2014 but was very slow to develop, she observed.
“I did my first training in 2004 and I don’t think the study opened for several years after that. I think there’s been a lot of hesitation to change the mindset that every cancer needs to be removed surgically,” Dr. Attai stated.
“When you put breast cancer in the context of the other organs, we are lagging behind a bit [with cryoablation],” she added.
“I don’t want to go there but … the innovation for male diseases and procedures sometimes surpasses that of women’s diseases,” she said.
But she also defended her fellow practitioners. “There’s been tremendous changes in management over the 27 years I’ve been in practice,” she said, citing the movement from mastectomy to lumpectomy as one of multiple big changes.
The disparity between the development of cryoablation for breast and prostate cancer is a mystery when you contemplate the potential side effects, Dr. Fine observed. “There’s not a lot of vital structures inside the breast, so you don’t have risks that you have with the prostate, including urinary incontinence and impotence.”
As a next move, the American Society of Breast Surgeons is planning to establish a cryoablation registry and aims to enroll 50 sites and 500 patients who are aged 55-85 years; for those aged 65-70, radiation therapy will be required, said Dr. Fine.
Currently, cryoablation for breast cancer is allowed only in a clinical trial, so a registry would expand usage considerably, he said.
However, cryoablation, including from IceCure, has FDA clearance for ablating cancerous tissue in general (but not breast cancer specifically).
Dr. Attai hopes the field is ready for the nonsurgical approach.
“Halsted died in 1922 and the Halsted radical mastectomy really didn’t start to fall out of favor until the 1950s, 1960,” said Dr. Attai, referring to Dr William Halsted, who pioneered the procedure in the 1890s. “I would hope we are better at speeding up our progress. Changing the surgical mindset takes time,” she said.
Dr. Fine was an investigator in the ICE3 trial, which is funded by IceCure Medical. Dr. Attai has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the United States, cryoablation or freezing tissue to death is a primary treatment option for a variety of cancers, including those originating in or spread to the bone, cervix, eye, kidney, liver, lung, pancreas, prostate, and skin.
Cryoablation for prostate cancer, one of the most common cancers in men, was first approved in the 1990s.
But unlike in Europe, this nonsurgical approach is not approved for breast cancer in the United States; it is one of the most common cancers in women.
So why is this approach still experimental for breast cancer?
“I don’t know,” answered cryoablation researcher Richard Fine, MD, of West Cancer Center in Germantown, Tenn., when asked by this news organization.
“It’s very interesting how slow the [Food and Drug Administration] is in approving devices for breast cancer [when compared with] other cancers,” he said.
New clinical data
Perhaps new clinical data will eventually lead to approval of this nonsurgical technique for use in low-risk breast cancer. However, the related trial had a controversial design that might discourage uptake by practitioners if it is approved, said an expert not involved in the study.
Nevertheless, the new data show that cryoablation can be an effective treatment for small, low-risk, early-stage breast cancers in older patients.
The findings come from ICE-3, a multicenter single-arm study of cryoablation in 194 such patients with mean follow-up of roughly 3 years.
It used liquid nitrogen-based cryoablation technology from IceCure Medical Ltd., an Israeli company and the study sponsor.
The results show that 2.06% (n = 4) of patients had a recurrence in the same breast, which is “basically the same” as lumpectomy, the surgical standard for this patient group, said Dr. Fine, the lead investigator on the trial.
These are interim data, Dr. Fine said at the American Society of Breast Surgeons annual meeting, held virtually.
The primary outcome is the 5-year recurrence rate, and this is the first-ever cryoablation trial that does not involve follow-up surgery, he said.
Cryoablation, which delivers a gas to a tumor via a thin needle-like probe that is guided by ultrasound, has multiple advantages over surgery, Dr. Fine said.
“The noninvasive procedure is fast, painless, and can be delivered under local anesthesia in a doctor’s office. Recovery time is minimal and cosmetic outcomes are excellent with little loss of breast tissue and no scarring,” he said in a meeting press statement.
The potential market for cryoablation in breast cancer is large, as it is intended for tumors ≤1.5 cm, which comprise approximately 60%-70% of stage 1 breast cancers that are hormone receptor–positive (HR+), and HER2-negative (HER2–), Dr. Fine said in an interview.
Cryoablation is part of a logical, de-escalation of breast cancer care, he added. “We have moved from radical mastectomy to modified mastectomy to lumpectomy – so the next step in that evolution is ablative technology, which is ‘nonsurgical.’ ”
There are other experimental ablative treatments for breast cancer including high-frequency ultrasound and laser, but cryoablation is the furthest along in development.
Cryoablation as a primary cancer treatment was first approved for coverage by the Centers for Medicare & Medicaid Services for localized prostate cancer in 1999.
But the concept extends back to 1845, when English physician James Arnott first used iced salt solutions (about –20 °C or – 4 °F) to induce tissue necrosis, reducing tumor size and ameliorating pain. Because the crude cryogen needed to be applied topically, the pioneering technique was limited to breast and cervical cancers because of their accessibility.
Not likely to show superiority
The new study’s population was composed of women aged 60 years or older (mean of 75 years) with unifocal invasive ductal cancers measuring ≤1.5 cm or less that were all low-grade, HR+, and HER2–, as noted.
The liquid nitrogen–based cryoablation consisted of a freeze-thaw-freeze cycle that totals 20-40 minutes, with freezing temperatures targeting the tumor area and turning it into an “ice ball.”
That ice ball eventually surrounds the tumor, creating a “lethal zone,” and thus a margin in which no cancer exists, akin to surgery, said Dr. Fine.
There were no significant device-related adverse events or complications reported, say the investigators. Most of the adverse events were minor and included bruising, localized edema, minor skin freeze burn, rash, minor bleeding from needle insertion, minor local hematoma, skin induration, minor infection, and pruritis.
Two of 15 patients who underwent sentinel lymph node biopsies had a positive sentinel node. At the discretion of their treating physician, 27 patients underwent adjuvant radiation, 1 patient received chemotherapy, and 148 began endocrine therapy. More than 95% of the patients and 98% of physicians reported satisfaction from the cosmetic results during follow-up visits.
Because not all patients underwent sentinel lymph node biopsy and adjuvant radiation, there is likely to be controversy about this approach, suggested Deanna J. Attai, MD, a breast surgeon at the University of California, Los Angeles, and past president of the American Society of Breast Surgeons, who was asked for comment.
“We have studies that [indicate that] these treatments don’t add significant benefit [in this patient population] but there still is this hesitation [to forgo them],” she told this news organization.
“The patients in this study were exceedingly low risk,” she emphasized.
“Is 5 years enough to assess recurrence rates? The answer is probably no. Recurrences or distant metastases are more likely to happen 10-20 years later.”
Thus, it will be difficult to show that cryoablation is superior to surgery, she said.
“You can show that cryoablation is not inferior to lumpectomy alone – which allows patients to avoid the operating room,” Dr. Attai summarized.
The surgical mindset and breast cancer
Dr. Attai, who was not involved in the current trial, was an investigator in an earlier single-arm cooperative group study of cryoablation for breast cancer, which had the rate of complete tumor ablation as the primary outcome. The study, known as the American College of Surgeons Oncology Group Z1072 trial, enrolled 99 patients, all of whom underwent ablation followed by surgery. The study reported results in 2014 but was very slow to develop, she observed.
“I did my first training in 2004 and I don’t think the study opened for several years after that. I think there’s been a lot of hesitation to change the mindset that every cancer needs to be removed surgically,” Dr. Attai stated.
“When you put breast cancer in the context of the other organs, we are lagging behind a bit [with cryoablation],” she added.
“I don’t want to go there but … the innovation for male diseases and procedures sometimes surpasses that of women’s diseases,” she said.
But she also defended her fellow practitioners. “There’s been tremendous changes in management over the 27 years I’ve been in practice,” she said, citing the movement from mastectomy to lumpectomy as one of multiple big changes.
The disparity between the development of cryoablation for breast and prostate cancer is a mystery when you contemplate the potential side effects, Dr. Fine observed. “There’s not a lot of vital structures inside the breast, so you don’t have risks that you have with the prostate, including urinary incontinence and impotence.”
As a next move, the American Society of Breast Surgeons is planning to establish a cryoablation registry and aims to enroll 50 sites and 500 patients who are aged 55-85 years; for those aged 65-70, radiation therapy will be required, said Dr. Fine.
Currently, cryoablation for breast cancer is allowed only in a clinical trial, so a registry would expand usage considerably, he said.
However, cryoablation, including from IceCure, has FDA clearance for ablating cancerous tissue in general (but not breast cancer specifically).
Dr. Attai hopes the field is ready for the nonsurgical approach.
“Halsted died in 1922 and the Halsted radical mastectomy really didn’t start to fall out of favor until the 1950s, 1960,” said Dr. Attai, referring to Dr William Halsted, who pioneered the procedure in the 1890s. “I would hope we are better at speeding up our progress. Changing the surgical mindset takes time,” she said.
Dr. Fine was an investigator in the ICE3 trial, which is funded by IceCure Medical. Dr. Attai has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the United States, cryoablation or freezing tissue to death is a primary treatment option for a variety of cancers, including those originating in or spread to the bone, cervix, eye, kidney, liver, lung, pancreas, prostate, and skin.
Cryoablation for prostate cancer, one of the most common cancers in men, was first approved in the 1990s.
But unlike in Europe, this nonsurgical approach is not approved for breast cancer in the United States; it is one of the most common cancers in women.
So why is this approach still experimental for breast cancer?
“I don’t know,” answered cryoablation researcher Richard Fine, MD, of West Cancer Center in Germantown, Tenn., when asked by this news organization.
“It’s very interesting how slow the [Food and Drug Administration] is in approving devices for breast cancer [when compared with] other cancers,” he said.
New clinical data
Perhaps new clinical data will eventually lead to approval of this nonsurgical technique for use in low-risk breast cancer. However, the related trial had a controversial design that might discourage uptake by practitioners if it is approved, said an expert not involved in the study.
Nevertheless, the new data show that cryoablation can be an effective treatment for small, low-risk, early-stage breast cancers in older patients.
The findings come from ICE-3, a multicenter single-arm study of cryoablation in 194 such patients with mean follow-up of roughly 3 years.
It used liquid nitrogen-based cryoablation technology from IceCure Medical Ltd., an Israeli company and the study sponsor.
The results show that 2.06% (n = 4) of patients had a recurrence in the same breast, which is “basically the same” as lumpectomy, the surgical standard for this patient group, said Dr. Fine, the lead investigator on the trial.
These are interim data, Dr. Fine said at the American Society of Breast Surgeons annual meeting, held virtually.
The primary outcome is the 5-year recurrence rate, and this is the first-ever cryoablation trial that does not involve follow-up surgery, he said.
Cryoablation, which delivers a gas to a tumor via a thin needle-like probe that is guided by ultrasound, has multiple advantages over surgery, Dr. Fine said.
“The noninvasive procedure is fast, painless, and can be delivered under local anesthesia in a doctor’s office. Recovery time is minimal and cosmetic outcomes are excellent with little loss of breast tissue and no scarring,” he said in a meeting press statement.
The potential market for cryoablation in breast cancer is large, as it is intended for tumors ≤1.5 cm, which comprise approximately 60%-70% of stage 1 breast cancers that are hormone receptor–positive (HR+), and HER2-negative (HER2–), Dr. Fine said in an interview.
Cryoablation is part of a logical, de-escalation of breast cancer care, he added. “We have moved from radical mastectomy to modified mastectomy to lumpectomy – so the next step in that evolution is ablative technology, which is ‘nonsurgical.’ ”
There are other experimental ablative treatments for breast cancer including high-frequency ultrasound and laser, but cryoablation is the furthest along in development.
Cryoablation as a primary cancer treatment was first approved for coverage by the Centers for Medicare & Medicaid Services for localized prostate cancer in 1999.
But the concept extends back to 1845, when English physician James Arnott first used iced salt solutions (about –20 °C or – 4 °F) to induce tissue necrosis, reducing tumor size and ameliorating pain. Because the crude cryogen needed to be applied topically, the pioneering technique was limited to breast and cervical cancers because of their accessibility.
Not likely to show superiority
The new study’s population was composed of women aged 60 years or older (mean of 75 years) with unifocal invasive ductal cancers measuring ≤1.5 cm or less that were all low-grade, HR+, and HER2–, as noted.
The liquid nitrogen–based cryoablation consisted of a freeze-thaw-freeze cycle that totals 20-40 minutes, with freezing temperatures targeting the tumor area and turning it into an “ice ball.”
That ice ball eventually surrounds the tumor, creating a “lethal zone,” and thus a margin in which no cancer exists, akin to surgery, said Dr. Fine.
There were no significant device-related adverse events or complications reported, say the investigators. Most of the adverse events were minor and included bruising, localized edema, minor skin freeze burn, rash, minor bleeding from needle insertion, minor local hematoma, skin induration, minor infection, and pruritis.
Two of 15 patients who underwent sentinel lymph node biopsies had a positive sentinel node. At the discretion of their treating physician, 27 patients underwent adjuvant radiation, 1 patient received chemotherapy, and 148 began endocrine therapy. More than 95% of the patients and 98% of physicians reported satisfaction from the cosmetic results during follow-up visits.
Because not all patients underwent sentinel lymph node biopsy and adjuvant radiation, there is likely to be controversy about this approach, suggested Deanna J. Attai, MD, a breast surgeon at the University of California, Los Angeles, and past president of the American Society of Breast Surgeons, who was asked for comment.
“We have studies that [indicate that] these treatments don’t add significant benefit [in this patient population] but there still is this hesitation [to forgo them],” she told this news organization.
“The patients in this study were exceedingly low risk,” she emphasized.
“Is 5 years enough to assess recurrence rates? The answer is probably no. Recurrences or distant metastases are more likely to happen 10-20 years later.”
Thus, it will be difficult to show that cryoablation is superior to surgery, she said.
“You can show that cryoablation is not inferior to lumpectomy alone – which allows patients to avoid the operating room,” Dr. Attai summarized.
The surgical mindset and breast cancer
Dr. Attai, who was not involved in the current trial, was an investigator in an earlier single-arm cooperative group study of cryoablation for breast cancer, which had the rate of complete tumor ablation as the primary outcome. The study, known as the American College of Surgeons Oncology Group Z1072 trial, enrolled 99 patients, all of whom underwent ablation followed by surgery. The study reported results in 2014 but was very slow to develop, she observed.
“I did my first training in 2004 and I don’t think the study opened for several years after that. I think there’s been a lot of hesitation to change the mindset that every cancer needs to be removed surgically,” Dr. Attai stated.
“When you put breast cancer in the context of the other organs, we are lagging behind a bit [with cryoablation],” she added.
“I don’t want to go there but … the innovation for male diseases and procedures sometimes surpasses that of women’s diseases,” she said.
But she also defended her fellow practitioners. “There’s been tremendous changes in management over the 27 years I’ve been in practice,” she said, citing the movement from mastectomy to lumpectomy as one of multiple big changes.
The disparity between the development of cryoablation for breast and prostate cancer is a mystery when you contemplate the potential side effects, Dr. Fine observed. “There’s not a lot of vital structures inside the breast, so you don’t have risks that you have with the prostate, including urinary incontinence and impotence.”
As a next move, the American Society of Breast Surgeons is planning to establish a cryoablation registry and aims to enroll 50 sites and 500 patients who are aged 55-85 years; for those aged 65-70, radiation therapy will be required, said Dr. Fine.
Currently, cryoablation for breast cancer is allowed only in a clinical trial, so a registry would expand usage considerably, he said.
However, cryoablation, including from IceCure, has FDA clearance for ablating cancerous tissue in general (but not breast cancer specifically).
Dr. Attai hopes the field is ready for the nonsurgical approach.
“Halsted died in 1922 and the Halsted radical mastectomy really didn’t start to fall out of favor until the 1950s, 1960,” said Dr. Attai, referring to Dr William Halsted, who pioneered the procedure in the 1890s. “I would hope we are better at speeding up our progress. Changing the surgical mindset takes time,” she said.
Dr. Fine was an investigator in the ICE3 trial, which is funded by IceCure Medical. Dr. Attai has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Remarkable’ results for targeted therapy of rare CNS tumors
The results from three small studies of targeted therapy for rare brain tumors were “remarkable,” according to Jaishri Blakeley, MD, a neurology professor at Johns Hopkins Medicine, Baltimore, who discussed the studies after they were presented at the American Society of Clinical Oncology meeting.
Although most patients don’t have targetable mutations, molecular testing “is well worth the effort,” for those that do. “I think it’s fair to say that precision medicine” – well established in other tumor types – “is finally here in full force for neuro-oncology,” Dr. Blakeley said.
A promising start
Fifteen of 16 patients (94%) in one study had newly diagnosed and untreated papillary craniopharyngiomas (PCPs) that harbored BRAF V600E mutations, a common finding in PCPs, which have no effective medical treatment.
Tumors shrunk 68%-99% in 14 patients (93%) after treatment with the BRAF inhibitor vemurafenib plus the MEK inhibitor cobimetinib, which was included to stave off resistance to vemurafenib. The 24-month progression free survival was 93%.
The combination resulted in significant response in all patients who received at least one cycle of therapy, with a median 91% volume reduction. “Our study indicates that BRAF/MEK inhibitors could be a powerful tool in the treatment of previously untreated PCP, with the potential to avoid the morbidity associated with radiation and surgery,” concluded lead investigator and presenter Priscilla K. Brastianos, MD, associate professor of medicine at Mass General Cancer Center, Boston.
Thirty-three people in the second study had a mix of high and low grade gliomas or other CNS tumors positive for TRK gene fusions, a known oncogenic driver; the majority were children. They were treated with the TRK inhibitor larotrectinib after progressing on other systemic therapies.
The objective response rate was 30%, and the disease control rate was 73% at 24 weeks, with a median time to best response of 1.9 months. Tumors shrank in 82% of evaluable patients. Median progression-free survival was 18.3 months, and overall survival was not reached.
“These results support testing for TRK gene fusions for all patients with CNS tumors, especially if there is no known driver and especially in infants,” concluded lead investigator and presenter Sebastien Perreault, MD, a clinical assistant neurosciences professor at the University of Montreal.
The third study tested ALK inhibitors such as crizotinib in seven patients with adult-onset neuroblastoma, a rare and almost invariably fatal tumor known to be enriched for ALK mutations; the subjects were positive for them.
Their disease remained stable anywhere from 3.4 to 37.4 months. Median time to progression was 15.5 months, and median overall survival was 46.5 months.
ALK inhibitors “can be a well-tolerated options for treatment, improving time to progression. Development of resistance to one agent does not preclude use of other agents in the same drug class. ALK inhibitors should be considered when treating patients with this diagnosis,” said lead investigator and presenter Jessica Stiefel, MD, a pediatric hematology oncology fellow at Memorial Sloan Kettering Cancer Center, New York.
A ‘strong’ recommendation
The data “are great news” across the board. Targeted therapy applied to the right CNS tumor can have “dramatic” benefit for tumor control, Dr. Blakeley said.
But organizing molecular testing is not straightforward and requires strategies to balance “the use of precious resources, such as time money, and tissue,” with the potential benefit. Interpretation of testing results isn’t straightforward either, and is best handled by a molecular tumor board. Clinical pharmacists are also key to accessing expensive medications off label for CNS tumors.
Adverse events are also a consideration. Most of the subjects in the PCP study had grade 3/4 toxicity. Three patients in the ALK inhibitor study had to stop because of adverse events. Almost 40% on larotrectinib had grade 3 or 4 toxicity; nobody came off treatment, but a third had to skip doses.
Once an actionable mutation is identified, Dr. Blakeley’s “strong recommendation” is to enroll patients in a clinical trial that targets it, to take advantage the structure already in place to secure treatment, managed patients, and assess outcomes.
The National Cancer Institute’s MATCH trial is one of several options.
The BRAF/MEK inhibitor study was funded by Genentech and the National Institutes of Health. Dr. Brastianos had ties to numerous companies, including Pfizer, Lilly, and Merck. The TRK inhibitor study was funded by Bayer/Lilly. Dr. Perreault is a speaker and researcher for the company and has other ties. Dr. Blakeley is an adviser and/or researcher for a number of companies, including AbbVie, Astellas, BMS, and Exelixis. Dr. Stiefel didn’t have any disclosures, and didn’t report outside funding.
The results from three small studies of targeted therapy for rare brain tumors were “remarkable,” according to Jaishri Blakeley, MD, a neurology professor at Johns Hopkins Medicine, Baltimore, who discussed the studies after they were presented at the American Society of Clinical Oncology meeting.
Although most patients don’t have targetable mutations, molecular testing “is well worth the effort,” for those that do. “I think it’s fair to say that precision medicine” – well established in other tumor types – “is finally here in full force for neuro-oncology,” Dr. Blakeley said.
A promising start
Fifteen of 16 patients (94%) in one study had newly diagnosed and untreated papillary craniopharyngiomas (PCPs) that harbored BRAF V600E mutations, a common finding in PCPs, which have no effective medical treatment.
Tumors shrunk 68%-99% in 14 patients (93%) after treatment with the BRAF inhibitor vemurafenib plus the MEK inhibitor cobimetinib, which was included to stave off resistance to vemurafenib. The 24-month progression free survival was 93%.
The combination resulted in significant response in all patients who received at least one cycle of therapy, with a median 91% volume reduction. “Our study indicates that BRAF/MEK inhibitors could be a powerful tool in the treatment of previously untreated PCP, with the potential to avoid the morbidity associated with radiation and surgery,” concluded lead investigator and presenter Priscilla K. Brastianos, MD, associate professor of medicine at Mass General Cancer Center, Boston.
Thirty-three people in the second study had a mix of high and low grade gliomas or other CNS tumors positive for TRK gene fusions, a known oncogenic driver; the majority were children. They were treated with the TRK inhibitor larotrectinib after progressing on other systemic therapies.
The objective response rate was 30%, and the disease control rate was 73% at 24 weeks, with a median time to best response of 1.9 months. Tumors shrank in 82% of evaluable patients. Median progression-free survival was 18.3 months, and overall survival was not reached.
“These results support testing for TRK gene fusions for all patients with CNS tumors, especially if there is no known driver and especially in infants,” concluded lead investigator and presenter Sebastien Perreault, MD, a clinical assistant neurosciences professor at the University of Montreal.
The third study tested ALK inhibitors such as crizotinib in seven patients with adult-onset neuroblastoma, a rare and almost invariably fatal tumor known to be enriched for ALK mutations; the subjects were positive for them.
Their disease remained stable anywhere from 3.4 to 37.4 months. Median time to progression was 15.5 months, and median overall survival was 46.5 months.
ALK inhibitors “can be a well-tolerated options for treatment, improving time to progression. Development of resistance to one agent does not preclude use of other agents in the same drug class. ALK inhibitors should be considered when treating patients with this diagnosis,” said lead investigator and presenter Jessica Stiefel, MD, a pediatric hematology oncology fellow at Memorial Sloan Kettering Cancer Center, New York.
A ‘strong’ recommendation
The data “are great news” across the board. Targeted therapy applied to the right CNS tumor can have “dramatic” benefit for tumor control, Dr. Blakeley said.
But organizing molecular testing is not straightforward and requires strategies to balance “the use of precious resources, such as time money, and tissue,” with the potential benefit. Interpretation of testing results isn’t straightforward either, and is best handled by a molecular tumor board. Clinical pharmacists are also key to accessing expensive medications off label for CNS tumors.
Adverse events are also a consideration. Most of the subjects in the PCP study had grade 3/4 toxicity. Three patients in the ALK inhibitor study had to stop because of adverse events. Almost 40% on larotrectinib had grade 3 or 4 toxicity; nobody came off treatment, but a third had to skip doses.
Once an actionable mutation is identified, Dr. Blakeley’s “strong recommendation” is to enroll patients in a clinical trial that targets it, to take advantage the structure already in place to secure treatment, managed patients, and assess outcomes.
The National Cancer Institute’s MATCH trial is one of several options.
The BRAF/MEK inhibitor study was funded by Genentech and the National Institutes of Health. Dr. Brastianos had ties to numerous companies, including Pfizer, Lilly, and Merck. The TRK inhibitor study was funded by Bayer/Lilly. Dr. Perreault is a speaker and researcher for the company and has other ties. Dr. Blakeley is an adviser and/or researcher for a number of companies, including AbbVie, Astellas, BMS, and Exelixis. Dr. Stiefel didn’t have any disclosures, and didn’t report outside funding.
The results from three small studies of targeted therapy for rare brain tumors were “remarkable,” according to Jaishri Blakeley, MD, a neurology professor at Johns Hopkins Medicine, Baltimore, who discussed the studies after they were presented at the American Society of Clinical Oncology meeting.
Although most patients don’t have targetable mutations, molecular testing “is well worth the effort,” for those that do. “I think it’s fair to say that precision medicine” – well established in other tumor types – “is finally here in full force for neuro-oncology,” Dr. Blakeley said.
A promising start
Fifteen of 16 patients (94%) in one study had newly diagnosed and untreated papillary craniopharyngiomas (PCPs) that harbored BRAF V600E mutations, a common finding in PCPs, which have no effective medical treatment.
Tumors shrunk 68%-99% in 14 patients (93%) after treatment with the BRAF inhibitor vemurafenib plus the MEK inhibitor cobimetinib, which was included to stave off resistance to vemurafenib. The 24-month progression free survival was 93%.
The combination resulted in significant response in all patients who received at least one cycle of therapy, with a median 91% volume reduction. “Our study indicates that BRAF/MEK inhibitors could be a powerful tool in the treatment of previously untreated PCP, with the potential to avoid the morbidity associated with radiation and surgery,” concluded lead investigator and presenter Priscilla K. Brastianos, MD, associate professor of medicine at Mass General Cancer Center, Boston.
Thirty-three people in the second study had a mix of high and low grade gliomas or other CNS tumors positive for TRK gene fusions, a known oncogenic driver; the majority were children. They were treated with the TRK inhibitor larotrectinib after progressing on other systemic therapies.
The objective response rate was 30%, and the disease control rate was 73% at 24 weeks, with a median time to best response of 1.9 months. Tumors shrank in 82% of evaluable patients. Median progression-free survival was 18.3 months, and overall survival was not reached.
“These results support testing for TRK gene fusions for all patients with CNS tumors, especially if there is no known driver and especially in infants,” concluded lead investigator and presenter Sebastien Perreault, MD, a clinical assistant neurosciences professor at the University of Montreal.
The third study tested ALK inhibitors such as crizotinib in seven patients with adult-onset neuroblastoma, a rare and almost invariably fatal tumor known to be enriched for ALK mutations; the subjects were positive for them.
Their disease remained stable anywhere from 3.4 to 37.4 months. Median time to progression was 15.5 months, and median overall survival was 46.5 months.
ALK inhibitors “can be a well-tolerated options for treatment, improving time to progression. Development of resistance to one agent does not preclude use of other agents in the same drug class. ALK inhibitors should be considered when treating patients with this diagnosis,” said lead investigator and presenter Jessica Stiefel, MD, a pediatric hematology oncology fellow at Memorial Sloan Kettering Cancer Center, New York.
A ‘strong’ recommendation
The data “are great news” across the board. Targeted therapy applied to the right CNS tumor can have “dramatic” benefit for tumor control, Dr. Blakeley said.
But organizing molecular testing is not straightforward and requires strategies to balance “the use of precious resources, such as time money, and tissue,” with the potential benefit. Interpretation of testing results isn’t straightforward either, and is best handled by a molecular tumor board. Clinical pharmacists are also key to accessing expensive medications off label for CNS tumors.
Adverse events are also a consideration. Most of the subjects in the PCP study had grade 3/4 toxicity. Three patients in the ALK inhibitor study had to stop because of adverse events. Almost 40% on larotrectinib had grade 3 or 4 toxicity; nobody came off treatment, but a third had to skip doses.
Once an actionable mutation is identified, Dr. Blakeley’s “strong recommendation” is to enroll patients in a clinical trial that targets it, to take advantage the structure already in place to secure treatment, managed patients, and assess outcomes.
The National Cancer Institute’s MATCH trial is one of several options.
The BRAF/MEK inhibitor study was funded by Genentech and the National Institutes of Health. Dr. Brastianos had ties to numerous companies, including Pfizer, Lilly, and Merck. The TRK inhibitor study was funded by Bayer/Lilly. Dr. Perreault is a speaker and researcher for the company and has other ties. Dr. Blakeley is an adviser and/or researcher for a number of companies, including AbbVie, Astellas, BMS, and Exelixis. Dr. Stiefel didn’t have any disclosures, and didn’t report outside funding.
FROM ASCO 2021
Experimental antibody-drug conjugate shown active against r/r DLBCL
Patients with relapsed or refractory B-cell non-Hodgkin lymphomas who are not candidates for hematopoietic stem cell transplant have a generally poor prognosis and few treatment options, but an experimental combination of the antibody-drug conjugate naratuximab with rituximab showed promising efficacy and acceptable safety in these patients in a phase 2 trial.
Among patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL) the combination was associated with a 44.7% overall response rate, including 31.6% complete responses, and two-thirds of patients had responses lasting more than 12 months, reported Moshe Yair Levy, MD, from Texas Oncology–Baylor Charles A Sammons Cancer Center in Dallas.
“This is, in my viewpoint, very exciting therapy,” he said in a question-and-answer session following his presentation of the data in a late-breaking abstract session during the European Hematology Association annual congress. (Abstract LB1903).
Naratuximab emtansine is an investigational antibody-drug conjugate (ADC) consisting of a humanized monoclonal antibody against CD37, a surface marker on B lymphocytes that is highly expressed in non-Hodgkin lymphoma (NHL), conjugated to a cytotoxic derivative of maitansine.
CD37 is also an internalizable cell-surface antigen, making it an attractive candidate for an ADC approach.
In a phase 1 trial, naratuximab monotherapy showed a good safety profile and a 22% overall response rate, Dr. Levy noted.
“What they found is that, if you coadminister this ADC with rituximab, you’re actually going to get more internalization of the CD37 monoclonal, therefore more payload delivered to your target cells,” he said.
He reported results of a multicenter, adaptive phase 2 study of the combination in patients with DLBCL and other relapsed/refractory NHL.
DLBCL and others
The trial was divided into two parts, with the first consisting of a safety run-in phase with expansion in patients with confirmed diagnoses of relapsed/refractory NHL, including DLBCL, follicular lymphoma, mantle cell lymphoma, and marginal zone lymphoma.
Patients with double- or triple-hit disease (with translocations in MYC plus either BCL2 and/or BCL6), bulky disease, or transformed lymphoma were eligible.
The second part consisted of two cohorts of patients with DLBCL treated with naratuximab and rituximab either weekly or every 3 weeks.
All patients in the study had received one to six prior lines of therapy, and had Eastern Cooperative Oncology Group performance status of 0-2. Patients with CNS lymphomas or prior anti-CD37 targeting therapy were excluded.
The safety population included 50 patients with DLBCL assigned to therapy every 3 weeks, 30 assigned to weekly therapy, and 20 patients with other NHL.
DLBCL efficacy
A total of 76 patients with DLBCL were evaluable for efficacy.
The ORR was 44% for patients in both the weekly and every 3 week cohorts, with 31.6% having complete responses.
Among 61 patients with nonbulky disease (longest diameter 7.5 cm or less), the ORR was 50.8%, and among 28 patients who had three or more prior lines of therapy the ORR was 46.4%, with 32.1% having a complete response.
Among responders followed for a median of 15 months, the median duration of response was not reached, and 66% had responses lasting beyond 12 months.
In the weekly dosing DLBCL cohort, 53.3% of patients discontinued treatment of both study drugs because of disease progression, as did 58% of those in the every 3 week cohort, and 30% of patients with other lymphomas. Only eight patients discontinued the combination because of treatment-emergent adverse events. Six patients had treatment-emergent adverse events leading to naratuximab dose reduction.
The most common grade 3 or 4 adverse events were neutropenia, leukopenia, lymphopenia and thrombocytopenias. Dr. Levy commented that the use of granulocyte colony-stimulating factor, which was not mandatory in the study, would likely have lowered the incidence of cytopenias.
There were 10 deaths during the study, 2 of which were considered to be treatment related, occurring in 1 patient each in the DLBCL dosing cohorts; 1 of the patients died from pneumonitis, and the other from left ventricular heart failure.
Other patients deaths were attributed to non–treatment-related cardiac arrest, acute renal failure, exacerbation of chronic heart failure, respiratory failure, multiorgan failure, lung infection, or colon adenocarcinoma.
Q 3 weeks suffices
In the question-and-answer session following the presentation, Kenny Lei, MD, from the Chinese University of Hong Kong asked Dr. Levy what the half-life of naratuximab is, and what was the investigator’s rationale for testing a weekly dosing schedule.
“I think the reason they checked the two different regimens, the Q week and the Q 3-week group, is that they noted that [naratuximab] was cleared relatively quickly, and they wanted to see whether or not, by giving Q weekly, when you get a continuous CD37 site occupancy if they would have a better outcome. But as you saw, in the groups there was really no clinically relevant difference in outcome,” Dr. Levy said.
Andrew Davies, MD, PhD, from the University of Southampton (England), asked whether the neutropenia seen in the study was related to myeloid expression of the target of from the off-target deconjugated payload.
“I don’t know that I necessarily have the answer to that,” Dr. Levy replied. “Remember there is the CD20 monoclonal rituximab which we know can cause neutropenia, as well as the CD37 and the target payload. I don’t know if we have enough information to attribute it to one specific component of the therapy,” he said.
The study was funded by Debiopharm International. Dr. Levy disclosed speaker activities for multiple companies, not including Debiopharm. Dr. Lei and Dr. Davies had no disclosures relevant to the study.
Patients with relapsed or refractory B-cell non-Hodgkin lymphomas who are not candidates for hematopoietic stem cell transplant have a generally poor prognosis and few treatment options, but an experimental combination of the antibody-drug conjugate naratuximab with rituximab showed promising efficacy and acceptable safety in these patients in a phase 2 trial.
Among patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL) the combination was associated with a 44.7% overall response rate, including 31.6% complete responses, and two-thirds of patients had responses lasting more than 12 months, reported Moshe Yair Levy, MD, from Texas Oncology–Baylor Charles A Sammons Cancer Center in Dallas.
“This is, in my viewpoint, very exciting therapy,” he said in a question-and-answer session following his presentation of the data in a late-breaking abstract session during the European Hematology Association annual congress. (Abstract LB1903).
Naratuximab emtansine is an investigational antibody-drug conjugate (ADC) consisting of a humanized monoclonal antibody against CD37, a surface marker on B lymphocytes that is highly expressed in non-Hodgkin lymphoma (NHL), conjugated to a cytotoxic derivative of maitansine.
CD37 is also an internalizable cell-surface antigen, making it an attractive candidate for an ADC approach.
In a phase 1 trial, naratuximab monotherapy showed a good safety profile and a 22% overall response rate, Dr. Levy noted.
“What they found is that, if you coadminister this ADC with rituximab, you’re actually going to get more internalization of the CD37 monoclonal, therefore more payload delivered to your target cells,” he said.
He reported results of a multicenter, adaptive phase 2 study of the combination in patients with DLBCL and other relapsed/refractory NHL.
DLBCL and others
The trial was divided into two parts, with the first consisting of a safety run-in phase with expansion in patients with confirmed diagnoses of relapsed/refractory NHL, including DLBCL, follicular lymphoma, mantle cell lymphoma, and marginal zone lymphoma.
Patients with double- or triple-hit disease (with translocations in MYC plus either BCL2 and/or BCL6), bulky disease, or transformed lymphoma were eligible.
The second part consisted of two cohorts of patients with DLBCL treated with naratuximab and rituximab either weekly or every 3 weeks.
All patients in the study had received one to six prior lines of therapy, and had Eastern Cooperative Oncology Group performance status of 0-2. Patients with CNS lymphomas or prior anti-CD37 targeting therapy were excluded.
The safety population included 50 patients with DLBCL assigned to therapy every 3 weeks, 30 assigned to weekly therapy, and 20 patients with other NHL.
DLBCL efficacy
A total of 76 patients with DLBCL were evaluable for efficacy.
The ORR was 44% for patients in both the weekly and every 3 week cohorts, with 31.6% having complete responses.
Among 61 patients with nonbulky disease (longest diameter 7.5 cm or less), the ORR was 50.8%, and among 28 patients who had three or more prior lines of therapy the ORR was 46.4%, with 32.1% having a complete response.
Among responders followed for a median of 15 months, the median duration of response was not reached, and 66% had responses lasting beyond 12 months.
In the weekly dosing DLBCL cohort, 53.3% of patients discontinued treatment of both study drugs because of disease progression, as did 58% of those in the every 3 week cohort, and 30% of patients with other lymphomas. Only eight patients discontinued the combination because of treatment-emergent adverse events. Six patients had treatment-emergent adverse events leading to naratuximab dose reduction.
The most common grade 3 or 4 adverse events were neutropenia, leukopenia, lymphopenia and thrombocytopenias. Dr. Levy commented that the use of granulocyte colony-stimulating factor, which was not mandatory in the study, would likely have lowered the incidence of cytopenias.
There were 10 deaths during the study, 2 of which were considered to be treatment related, occurring in 1 patient each in the DLBCL dosing cohorts; 1 of the patients died from pneumonitis, and the other from left ventricular heart failure.
Other patients deaths were attributed to non–treatment-related cardiac arrest, acute renal failure, exacerbation of chronic heart failure, respiratory failure, multiorgan failure, lung infection, or colon adenocarcinoma.
Q 3 weeks suffices
In the question-and-answer session following the presentation, Kenny Lei, MD, from the Chinese University of Hong Kong asked Dr. Levy what the half-life of naratuximab is, and what was the investigator’s rationale for testing a weekly dosing schedule.
“I think the reason they checked the two different regimens, the Q week and the Q 3-week group, is that they noted that [naratuximab] was cleared relatively quickly, and they wanted to see whether or not, by giving Q weekly, when you get a continuous CD37 site occupancy if they would have a better outcome. But as you saw, in the groups there was really no clinically relevant difference in outcome,” Dr. Levy said.
Andrew Davies, MD, PhD, from the University of Southampton (England), asked whether the neutropenia seen in the study was related to myeloid expression of the target of from the off-target deconjugated payload.
“I don’t know that I necessarily have the answer to that,” Dr. Levy replied. “Remember there is the CD20 monoclonal rituximab which we know can cause neutropenia, as well as the CD37 and the target payload. I don’t know if we have enough information to attribute it to one specific component of the therapy,” he said.
The study was funded by Debiopharm International. Dr. Levy disclosed speaker activities for multiple companies, not including Debiopharm. Dr. Lei and Dr. Davies had no disclosures relevant to the study.
Patients with relapsed or refractory B-cell non-Hodgkin lymphomas who are not candidates for hematopoietic stem cell transplant have a generally poor prognosis and few treatment options, but an experimental combination of the antibody-drug conjugate naratuximab with rituximab showed promising efficacy and acceptable safety in these patients in a phase 2 trial.
Among patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL) the combination was associated with a 44.7% overall response rate, including 31.6% complete responses, and two-thirds of patients had responses lasting more than 12 months, reported Moshe Yair Levy, MD, from Texas Oncology–Baylor Charles A Sammons Cancer Center in Dallas.
“This is, in my viewpoint, very exciting therapy,” he said in a question-and-answer session following his presentation of the data in a late-breaking abstract session during the European Hematology Association annual congress. (Abstract LB1903).
Naratuximab emtansine is an investigational antibody-drug conjugate (ADC) consisting of a humanized monoclonal antibody against CD37, a surface marker on B lymphocytes that is highly expressed in non-Hodgkin lymphoma (NHL), conjugated to a cytotoxic derivative of maitansine.
CD37 is also an internalizable cell-surface antigen, making it an attractive candidate for an ADC approach.
In a phase 1 trial, naratuximab monotherapy showed a good safety profile and a 22% overall response rate, Dr. Levy noted.
“What they found is that, if you coadminister this ADC with rituximab, you’re actually going to get more internalization of the CD37 monoclonal, therefore more payload delivered to your target cells,” he said.
He reported results of a multicenter, adaptive phase 2 study of the combination in patients with DLBCL and other relapsed/refractory NHL.
DLBCL and others
The trial was divided into two parts, with the first consisting of a safety run-in phase with expansion in patients with confirmed diagnoses of relapsed/refractory NHL, including DLBCL, follicular lymphoma, mantle cell lymphoma, and marginal zone lymphoma.
Patients with double- or triple-hit disease (with translocations in MYC plus either BCL2 and/or BCL6), bulky disease, or transformed lymphoma were eligible.
The second part consisted of two cohorts of patients with DLBCL treated with naratuximab and rituximab either weekly or every 3 weeks.
All patients in the study had received one to six prior lines of therapy, and had Eastern Cooperative Oncology Group performance status of 0-2. Patients with CNS lymphomas or prior anti-CD37 targeting therapy were excluded.
The safety population included 50 patients with DLBCL assigned to therapy every 3 weeks, 30 assigned to weekly therapy, and 20 patients with other NHL.
DLBCL efficacy
A total of 76 patients with DLBCL were evaluable for efficacy.
The ORR was 44% for patients in both the weekly and every 3 week cohorts, with 31.6% having complete responses.
Among 61 patients with nonbulky disease (longest diameter 7.5 cm or less), the ORR was 50.8%, and among 28 patients who had three or more prior lines of therapy the ORR was 46.4%, with 32.1% having a complete response.
Among responders followed for a median of 15 months, the median duration of response was not reached, and 66% had responses lasting beyond 12 months.
In the weekly dosing DLBCL cohort, 53.3% of patients discontinued treatment of both study drugs because of disease progression, as did 58% of those in the every 3 week cohort, and 30% of patients with other lymphomas. Only eight patients discontinued the combination because of treatment-emergent adverse events. Six patients had treatment-emergent adverse events leading to naratuximab dose reduction.
The most common grade 3 or 4 adverse events were neutropenia, leukopenia, lymphopenia and thrombocytopenias. Dr. Levy commented that the use of granulocyte colony-stimulating factor, which was not mandatory in the study, would likely have lowered the incidence of cytopenias.
There were 10 deaths during the study, 2 of which were considered to be treatment related, occurring in 1 patient each in the DLBCL dosing cohorts; 1 of the patients died from pneumonitis, and the other from left ventricular heart failure.
Other patients deaths were attributed to non–treatment-related cardiac arrest, acute renal failure, exacerbation of chronic heart failure, respiratory failure, multiorgan failure, lung infection, or colon adenocarcinoma.
Q 3 weeks suffices
In the question-and-answer session following the presentation, Kenny Lei, MD, from the Chinese University of Hong Kong asked Dr. Levy what the half-life of naratuximab is, and what was the investigator’s rationale for testing a weekly dosing schedule.
“I think the reason they checked the two different regimens, the Q week and the Q 3-week group, is that they noted that [naratuximab] was cleared relatively quickly, and they wanted to see whether or not, by giving Q weekly, when you get a continuous CD37 site occupancy if they would have a better outcome. But as you saw, in the groups there was really no clinically relevant difference in outcome,” Dr. Levy said.
Andrew Davies, MD, PhD, from the University of Southampton (England), asked whether the neutropenia seen in the study was related to myeloid expression of the target of from the off-target deconjugated payload.
“I don’t know that I necessarily have the answer to that,” Dr. Levy replied. “Remember there is the CD20 monoclonal rituximab which we know can cause neutropenia, as well as the CD37 and the target payload. I don’t know if we have enough information to attribute it to one specific component of the therapy,” he said.
The study was funded by Debiopharm International. Dr. Levy disclosed speaker activities for multiple companies, not including Debiopharm. Dr. Lei and Dr. Davies had no disclosures relevant to the study.
FROM EHA 2021