User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Donafenib shows potential as first-line treatment of advanced hepatocellular carcinoma
“An improvement in the pharmacotherapy of advanced HCC remains a clinical need,” wrote Feng Bi, MD, of Sichuan University, in Chengdu, China, and colleagues.
Liver cancer is one of the most common cancers worldwide, with HCC representing 90% of liver malignancies. HCC most commonly occurs in people with liver disease, particularly in those with chronic hepatitis B and C and although rare, HCC is the ninth leading cause of cancer deaths in the United States. Most patients are diagnosed at the advanced stage with a median survival of 6-8 months. Sorafenib, the standard first-line therapy for advanced HCC, has demonstrated the median OS of 10.7 to 14.7 months. No other monotherapy has shown a significant improvement in OS, compared with sorafenib. Donafenib has shown favorable efficacy and safety in phase 1 studies.
This phase 2-3 trial evaluated the efficacy and safety of first-line donafenib, compared with sorafenib, in 668 Chinese patients with advanced HCC. Patients were randomly assigned to receive twice-daily oral donafenib 0.2 g or sorafenib 0.4 g until intolerable toxicity or disease progression. The primary end point was OS, tested for noninferiority and superiority.
Compared with sorafenib, donafenib significantly prolonged OS, 10.3 and 12.1 months, respectively, (hazard ratio, 95% confidence interval, 0.699-0.988; 0.83; P = .0245), and the superiority criteria for OS were met. Donafenib also presented improved safety and tolerability. Common drug-related adverse events, such as hand-foot skin reactions and diarrhea, and drug-related grade 3 or higher adverse events, occurred in fewer patients receiving donafenib than sorafenib, (38% vs. 50%; P = .0018). The authors noted that this lower frequency in adverse events with donafenib “contributed to improved patient adherence and decreased levels of drug interruption and discontinuation.”
Donafenib is a novel, oral, small-molecule, multikinase inhibitor that suppresses tumor cell proliferation and angiogenesis by inhibiting vascular endothelial growth factor receptors and platelet-derived growth factor receptors, and Raf kinases. It is a derivative of sorafenib and in June 2021, it was approved in China as a treatment for unresectable hepatocellular carcinoma for patients who have not received systemic treatment. It is not yet available in the United States.
“This pivotal head-to-head comparison study is the first to demonstrate noninferiority and superiority of a monotherapy, donafenib, with statistically significant extension in OS over sorafenib for first-line treatment of advanced HCC,” the authors wrote. “Compared with international trials, patients in this study presented with more severe baseline disease states, further emphasizing the positive response observed with donafenib.”
Another study, published in the same issue of the Journal of Clinical Oncology, compared tremelimumab and durvalumab as monotherapies and in combination for patients with unresectable HCC, found that use a single priming dose of tremelimumab combined with durvalumab showed the best benefit-risk profile.
“An improvement in the pharmacotherapy of advanced HCC remains a clinical need,” wrote Feng Bi, MD, of Sichuan University, in Chengdu, China, and colleagues.
Liver cancer is one of the most common cancers worldwide, with HCC representing 90% of liver malignancies. HCC most commonly occurs in people with liver disease, particularly in those with chronic hepatitis B and C and although rare, HCC is the ninth leading cause of cancer deaths in the United States. Most patients are diagnosed at the advanced stage with a median survival of 6-8 months. Sorafenib, the standard first-line therapy for advanced HCC, has demonstrated the median OS of 10.7 to 14.7 months. No other monotherapy has shown a significant improvement in OS, compared with sorafenib. Donafenib has shown favorable efficacy and safety in phase 1 studies.
This phase 2-3 trial evaluated the efficacy and safety of first-line donafenib, compared with sorafenib, in 668 Chinese patients with advanced HCC. Patients were randomly assigned to receive twice-daily oral donafenib 0.2 g or sorafenib 0.4 g until intolerable toxicity or disease progression. The primary end point was OS, tested for noninferiority and superiority.
Compared with sorafenib, donafenib significantly prolonged OS, 10.3 and 12.1 months, respectively, (hazard ratio, 95% confidence interval, 0.699-0.988; 0.83; P = .0245), and the superiority criteria for OS were met. Donafenib also presented improved safety and tolerability. Common drug-related adverse events, such as hand-foot skin reactions and diarrhea, and drug-related grade 3 or higher adverse events, occurred in fewer patients receiving donafenib than sorafenib, (38% vs. 50%; P = .0018). The authors noted that this lower frequency in adverse events with donafenib “contributed to improved patient adherence and decreased levels of drug interruption and discontinuation.”
Donafenib is a novel, oral, small-molecule, multikinase inhibitor that suppresses tumor cell proliferation and angiogenesis by inhibiting vascular endothelial growth factor receptors and platelet-derived growth factor receptors, and Raf kinases. It is a derivative of sorafenib and in June 2021, it was approved in China as a treatment for unresectable hepatocellular carcinoma for patients who have not received systemic treatment. It is not yet available in the United States.
“This pivotal head-to-head comparison study is the first to demonstrate noninferiority and superiority of a monotherapy, donafenib, with statistically significant extension in OS over sorafenib for first-line treatment of advanced HCC,” the authors wrote. “Compared with international trials, patients in this study presented with more severe baseline disease states, further emphasizing the positive response observed with donafenib.”
Another study, published in the same issue of the Journal of Clinical Oncology, compared tremelimumab and durvalumab as monotherapies and in combination for patients with unresectable HCC, found that use a single priming dose of tremelimumab combined with durvalumab showed the best benefit-risk profile.
“An improvement in the pharmacotherapy of advanced HCC remains a clinical need,” wrote Feng Bi, MD, of Sichuan University, in Chengdu, China, and colleagues.
Liver cancer is one of the most common cancers worldwide, with HCC representing 90% of liver malignancies. HCC most commonly occurs in people with liver disease, particularly in those with chronic hepatitis B and C and although rare, HCC is the ninth leading cause of cancer deaths in the United States. Most patients are diagnosed at the advanced stage with a median survival of 6-8 months. Sorafenib, the standard first-line therapy for advanced HCC, has demonstrated the median OS of 10.7 to 14.7 months. No other monotherapy has shown a significant improvement in OS, compared with sorafenib. Donafenib has shown favorable efficacy and safety in phase 1 studies.
This phase 2-3 trial evaluated the efficacy and safety of first-line donafenib, compared with sorafenib, in 668 Chinese patients with advanced HCC. Patients were randomly assigned to receive twice-daily oral donafenib 0.2 g or sorafenib 0.4 g until intolerable toxicity or disease progression. The primary end point was OS, tested for noninferiority and superiority.
Compared with sorafenib, donafenib significantly prolonged OS, 10.3 and 12.1 months, respectively, (hazard ratio, 95% confidence interval, 0.699-0.988; 0.83; P = .0245), and the superiority criteria for OS were met. Donafenib also presented improved safety and tolerability. Common drug-related adverse events, such as hand-foot skin reactions and diarrhea, and drug-related grade 3 or higher adverse events, occurred in fewer patients receiving donafenib than sorafenib, (38% vs. 50%; P = .0018). The authors noted that this lower frequency in adverse events with donafenib “contributed to improved patient adherence and decreased levels of drug interruption and discontinuation.”
Donafenib is a novel, oral, small-molecule, multikinase inhibitor that suppresses tumor cell proliferation and angiogenesis by inhibiting vascular endothelial growth factor receptors and platelet-derived growth factor receptors, and Raf kinases. It is a derivative of sorafenib and in June 2021, it was approved in China as a treatment for unresectable hepatocellular carcinoma for patients who have not received systemic treatment. It is not yet available in the United States.
“This pivotal head-to-head comparison study is the first to demonstrate noninferiority and superiority of a monotherapy, donafenib, with statistically significant extension in OS over sorafenib for first-line treatment of advanced HCC,” the authors wrote. “Compared with international trials, patients in this study presented with more severe baseline disease states, further emphasizing the positive response observed with donafenib.”
Another study, published in the same issue of the Journal of Clinical Oncology, compared tremelimumab and durvalumab as monotherapies and in combination for patients with unresectable HCC, found that use a single priming dose of tremelimumab combined with durvalumab showed the best benefit-risk profile.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
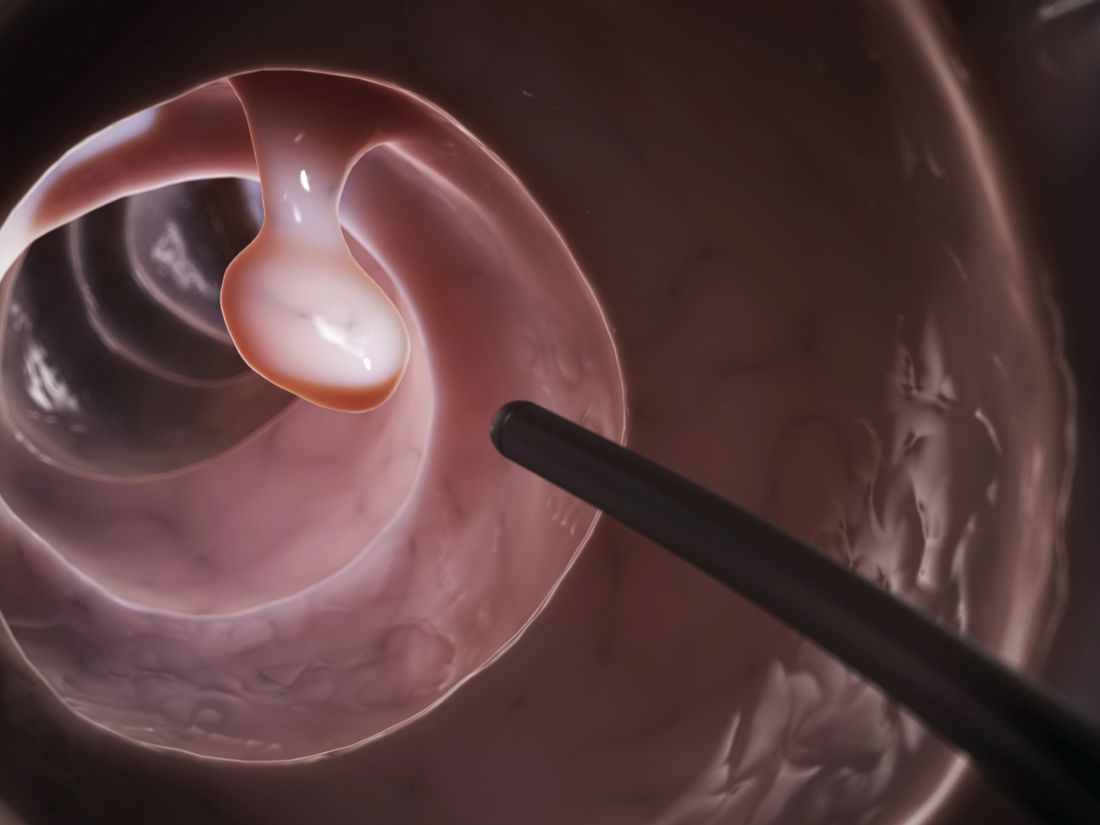
Few poorly prepped colonoscopies repeated within 1 year
Approximately one-third of colonoscopies with inadequate bowel preparation were repeated within 1 year despite current guidelines, according to data from a new study of more than 260,000 procedures.
Previous studies have shown that poor bowel prep, which occurs in approximately 25% of colonoscopies, can lead to lesion miss rates of as much as 42%-48%, Audrey H. Calderwood, MD, an associate professor of medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues wrote. However, factors affecting recommendations for repeat colonoscopies following poor bowel prep have not been examined.
In the study, published in Gastrointestinal Endoscopy, the researchers conducted a cross-sectional retrospective analysis of 260,314 colonoscopies reported to the GI Quality Improvement Consortium (GIQuIC) from 2011 to 2018. The review included adults aged 50-75 years in whom bowel preparation was deemed inadequate. The GIQuIC database defines adequate bowel preparation as “sufficient to accurately detect polyps greater than 5 mm in size,” the researchers noted. The procedures in this study were performed at 672 sites by 4,001 endoscopists, and the primary outcome was a recommendation for a repeat colonoscopy within 1 year.
In 31.9% of the procedures, the recommended follow-up interval for repeat colonoscopy was within 1 year, and there were no significant differences according to indication for the procedures (32.3% of screening and 31.2% of surveillance). Of these, 54.9% of patients received a follow-up interval of 1 year and 24.7% a follow-up interval within 3 months. Only 2.4% were advised they required no follow-up procedure.
The researchers found that patients with more severe disease had a higher likelihood of receiving a recommendation for follow-up colonoscopy within 1 year – 84% with adenocarcinoma, 51.8% with advanced lesions, and 23.2% with one to two small adenomas.
In the multivariate analysis, there were specific patient factors significantly associated with 1-year follow-up recommendations. The researchers found patients aged 70-75 years were less likely than younger patients (adjusted odds ratio, 0.96; 95% confidence interval, 0.93-0.98) to receive a 1-year follow-up recommendation; men were more likely than women (aOR, 1.04; 95% CI, 1.02-1.06) to receive a 1-year follow-up recommendation; and patients with adenocarcinoma findings more likely to receive a 1-year follow-up recommendation compared to those with no adenocarcinoma (aOR, 10.43; 95% CI, 7.77-13.98). In addition, they found patients residing in the Northeast and those whose procedure was performed by an endoscopist with an adenoma detection rate of at least25% were more likely to receive recommendations for a repeat colonoscopy within 1 year.
“The recommendation for repeat screening or surveillance colonoscopy within 1 year when the index colonoscopy has an inadequate bowel preparation is currently a quality measure in gastroenterology,” the researchers noted. “Although our study period started in 2011, when we looked at the time period of 2014 to 2018, which is after publication of guidelines of when to repeat colonoscopy after inadequate bowel preparation, there were still low rates of guideline-concordant recommendations.”
These overall low rates, which are consistent with other studies, may be due uncertainty on the part of the endoscopist in determining inadequate bowel prep based on evolving guidelines, the researchers noted. However, the higher frequency of recommendations for repeat procedures within 1 year for patients with advanced disease suggests that endoscopists are taking pathology into account.
The study findings were limited by several factors, including the lack of standardized assessment of bowel prep quality, variation in descriptions of bowel cleanliness, and lack of information on the primary factor in follow-up recommendations. However, the results were strengthened by the large sample size, the inclusion of multiple sites and providers, and the low volume of timely repeat procedures, which has clinical implications in terms of missed lesions, “including potential interval CRC [colorectal cancer],” the researchers said.
Get the word out on describing preps and planning follow-ups
The current study is important because it highlights that, even when endoscopists have a reasonable understanding on how to set follow-up intervals for polyp follow-up, what to do with a patient who comes in poorly prepped is more of a problem, Kim L. Isaacs, MD, of the University of North Carolina at Chapel Hill, said in an interview.
Dr Isaacs said she was not surprised by the study findings. “There are all gradations of inadequate preps that limit visualization in different ways, and there are many ways of recording this on procedure reports. The findings in the current study emphasize several points. The first is that the recommendation of following up an inadequate or poor prep in a year needs to be widely disseminated. The second is that there needs to be more education on standardization on how preps are described. In some poor preps, much of the colon can be seen, and clinicians can identify polyps 5-6 mm, so a 1-year follow-up may not be needed.” This type of research is challenging if the data are not standardized, she added.
Dr. Isaacs agreed with the authors’ description of repeat colonoscopies after poor bowel prep as a quality improvement area given the variability in following current recommendations, which leads into next steps for research.
“Understanding reasons for the recommendations that endoscopists made for follow-up would be the next step in this type of research,” Dr Isaacs noted. “After that, studies on the impact of an educational intervention, followed by repeating the initial assessment.”
The study received no outside funding. The researchers had no financial conflicts to disclose; however, lead author Dr. Calderwood disclosed support from the National Cancer Institute, the Dartmouth-Hitchcock Cancer Research Fellows Program, the Dartmouth-Hitchcock Norris Cotton Cancer Center, and the Dartmouth Clinical and Translational Science Institute. Dr Isaacs had no financial conflicts to disclose but has previously served on the editorial board of GI & Hepatology News.
Approximately one-third of colonoscopies with inadequate bowel preparation were repeated within 1 year despite current guidelines, according to data from a new study of more than 260,000 procedures.
Previous studies have shown that poor bowel prep, which occurs in approximately 25% of colonoscopies, can lead to lesion miss rates of as much as 42%-48%, Audrey H. Calderwood, MD, an associate professor of medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues wrote. However, factors affecting recommendations for repeat colonoscopies following poor bowel prep have not been examined.
In the study, published in Gastrointestinal Endoscopy, the researchers conducted a cross-sectional retrospective analysis of 260,314 colonoscopies reported to the GI Quality Improvement Consortium (GIQuIC) from 2011 to 2018. The review included adults aged 50-75 years in whom bowel preparation was deemed inadequate. The GIQuIC database defines adequate bowel preparation as “sufficient to accurately detect polyps greater than 5 mm in size,” the researchers noted. The procedures in this study were performed at 672 sites by 4,001 endoscopists, and the primary outcome was a recommendation for a repeat colonoscopy within 1 year.
In 31.9% of the procedures, the recommended follow-up interval for repeat colonoscopy was within 1 year, and there were no significant differences according to indication for the procedures (32.3% of screening and 31.2% of surveillance). Of these, 54.9% of patients received a follow-up interval of 1 year and 24.7% a follow-up interval within 3 months. Only 2.4% were advised they required no follow-up procedure.
The researchers found that patients with more severe disease had a higher likelihood of receiving a recommendation for follow-up colonoscopy within 1 year – 84% with adenocarcinoma, 51.8% with advanced lesions, and 23.2% with one to two small adenomas.
In the multivariate analysis, there were specific patient factors significantly associated with 1-year follow-up recommendations. The researchers found patients aged 70-75 years were less likely than younger patients (adjusted odds ratio, 0.96; 95% confidence interval, 0.93-0.98) to receive a 1-year follow-up recommendation; men were more likely than women (aOR, 1.04; 95% CI, 1.02-1.06) to receive a 1-year follow-up recommendation; and patients with adenocarcinoma findings more likely to receive a 1-year follow-up recommendation compared to those with no adenocarcinoma (aOR, 10.43; 95% CI, 7.77-13.98). In addition, they found patients residing in the Northeast and those whose procedure was performed by an endoscopist with an adenoma detection rate of at least25% were more likely to receive recommendations for a repeat colonoscopy within 1 year.
“The recommendation for repeat screening or surveillance colonoscopy within 1 year when the index colonoscopy has an inadequate bowel preparation is currently a quality measure in gastroenterology,” the researchers noted. “Although our study period started in 2011, when we looked at the time period of 2014 to 2018, which is after publication of guidelines of when to repeat colonoscopy after inadequate bowel preparation, there were still low rates of guideline-concordant recommendations.”
These overall low rates, which are consistent with other studies, may be due uncertainty on the part of the endoscopist in determining inadequate bowel prep based on evolving guidelines, the researchers noted. However, the higher frequency of recommendations for repeat procedures within 1 year for patients with advanced disease suggests that endoscopists are taking pathology into account.
The study findings were limited by several factors, including the lack of standardized assessment of bowel prep quality, variation in descriptions of bowel cleanliness, and lack of information on the primary factor in follow-up recommendations. However, the results were strengthened by the large sample size, the inclusion of multiple sites and providers, and the low volume of timely repeat procedures, which has clinical implications in terms of missed lesions, “including potential interval CRC [colorectal cancer],” the researchers said.
Get the word out on describing preps and planning follow-ups
The current study is important because it highlights that, even when endoscopists have a reasonable understanding on how to set follow-up intervals for polyp follow-up, what to do with a patient who comes in poorly prepped is more of a problem, Kim L. Isaacs, MD, of the University of North Carolina at Chapel Hill, said in an interview.
Dr Isaacs said she was not surprised by the study findings. “There are all gradations of inadequate preps that limit visualization in different ways, and there are many ways of recording this on procedure reports. The findings in the current study emphasize several points. The first is that the recommendation of following up an inadequate or poor prep in a year needs to be widely disseminated. The second is that there needs to be more education on standardization on how preps are described. In some poor preps, much of the colon can be seen, and clinicians can identify polyps 5-6 mm, so a 1-year follow-up may not be needed.” This type of research is challenging if the data are not standardized, she added.
Dr. Isaacs agreed with the authors’ description of repeat colonoscopies after poor bowel prep as a quality improvement area given the variability in following current recommendations, which leads into next steps for research.
“Understanding reasons for the recommendations that endoscopists made for follow-up would be the next step in this type of research,” Dr Isaacs noted. “After that, studies on the impact of an educational intervention, followed by repeating the initial assessment.”
The study received no outside funding. The researchers had no financial conflicts to disclose; however, lead author Dr. Calderwood disclosed support from the National Cancer Institute, the Dartmouth-Hitchcock Cancer Research Fellows Program, the Dartmouth-Hitchcock Norris Cotton Cancer Center, and the Dartmouth Clinical and Translational Science Institute. Dr Isaacs had no financial conflicts to disclose but has previously served on the editorial board of GI & Hepatology News.
Approximately one-third of colonoscopies with inadequate bowel preparation were repeated within 1 year despite current guidelines, according to data from a new study of more than 260,000 procedures.
Previous studies have shown that poor bowel prep, which occurs in approximately 25% of colonoscopies, can lead to lesion miss rates of as much as 42%-48%, Audrey H. Calderwood, MD, an associate professor of medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues wrote. However, factors affecting recommendations for repeat colonoscopies following poor bowel prep have not been examined.
In the study, published in Gastrointestinal Endoscopy, the researchers conducted a cross-sectional retrospective analysis of 260,314 colonoscopies reported to the GI Quality Improvement Consortium (GIQuIC) from 2011 to 2018. The review included adults aged 50-75 years in whom bowel preparation was deemed inadequate. The GIQuIC database defines adequate bowel preparation as “sufficient to accurately detect polyps greater than 5 mm in size,” the researchers noted. The procedures in this study were performed at 672 sites by 4,001 endoscopists, and the primary outcome was a recommendation for a repeat colonoscopy within 1 year.
In 31.9% of the procedures, the recommended follow-up interval for repeat colonoscopy was within 1 year, and there were no significant differences according to indication for the procedures (32.3% of screening and 31.2% of surveillance). Of these, 54.9% of patients received a follow-up interval of 1 year and 24.7% a follow-up interval within 3 months. Only 2.4% were advised they required no follow-up procedure.
The researchers found that patients with more severe disease had a higher likelihood of receiving a recommendation for follow-up colonoscopy within 1 year – 84% with adenocarcinoma, 51.8% with advanced lesions, and 23.2% with one to two small adenomas.
In the multivariate analysis, there were specific patient factors significantly associated with 1-year follow-up recommendations. The researchers found patients aged 70-75 years were less likely than younger patients (adjusted odds ratio, 0.96; 95% confidence interval, 0.93-0.98) to receive a 1-year follow-up recommendation; men were more likely than women (aOR, 1.04; 95% CI, 1.02-1.06) to receive a 1-year follow-up recommendation; and patients with adenocarcinoma findings more likely to receive a 1-year follow-up recommendation compared to those with no adenocarcinoma (aOR, 10.43; 95% CI, 7.77-13.98). In addition, they found patients residing in the Northeast and those whose procedure was performed by an endoscopist with an adenoma detection rate of at least25% were more likely to receive recommendations for a repeat colonoscopy within 1 year.
“The recommendation for repeat screening or surveillance colonoscopy within 1 year when the index colonoscopy has an inadequate bowel preparation is currently a quality measure in gastroenterology,” the researchers noted. “Although our study period started in 2011, when we looked at the time period of 2014 to 2018, which is after publication of guidelines of when to repeat colonoscopy after inadequate bowel preparation, there were still low rates of guideline-concordant recommendations.”
These overall low rates, which are consistent with other studies, may be due uncertainty on the part of the endoscopist in determining inadequate bowel prep based on evolving guidelines, the researchers noted. However, the higher frequency of recommendations for repeat procedures within 1 year for patients with advanced disease suggests that endoscopists are taking pathology into account.
The study findings were limited by several factors, including the lack of standardized assessment of bowel prep quality, variation in descriptions of bowel cleanliness, and lack of information on the primary factor in follow-up recommendations. However, the results were strengthened by the large sample size, the inclusion of multiple sites and providers, and the low volume of timely repeat procedures, which has clinical implications in terms of missed lesions, “including potential interval CRC [colorectal cancer],” the researchers said.
Get the word out on describing preps and planning follow-ups
The current study is important because it highlights that, even when endoscopists have a reasonable understanding on how to set follow-up intervals for polyp follow-up, what to do with a patient who comes in poorly prepped is more of a problem, Kim L. Isaacs, MD, of the University of North Carolina at Chapel Hill, said in an interview.
Dr Isaacs said she was not surprised by the study findings. “There are all gradations of inadequate preps that limit visualization in different ways, and there are many ways of recording this on procedure reports. The findings in the current study emphasize several points. The first is that the recommendation of following up an inadequate or poor prep in a year needs to be widely disseminated. The second is that there needs to be more education on standardization on how preps are described. In some poor preps, much of the colon can be seen, and clinicians can identify polyps 5-6 mm, so a 1-year follow-up may not be needed.” This type of research is challenging if the data are not standardized, she added.
Dr. Isaacs agreed with the authors’ description of repeat colonoscopies after poor bowel prep as a quality improvement area given the variability in following current recommendations, which leads into next steps for research.
“Understanding reasons for the recommendations that endoscopists made for follow-up would be the next step in this type of research,” Dr Isaacs noted. “After that, studies on the impact of an educational intervention, followed by repeating the initial assessment.”
The study received no outside funding. The researchers had no financial conflicts to disclose; however, lead author Dr. Calderwood disclosed support from the National Cancer Institute, the Dartmouth-Hitchcock Cancer Research Fellows Program, the Dartmouth-Hitchcock Norris Cotton Cancer Center, and the Dartmouth Clinical and Translational Science Institute. Dr Isaacs had no financial conflicts to disclose but has previously served on the editorial board of GI & Hepatology News.
FROM GASTROINTESTINAL ENDOSCOPY
Could your patient benefit? New trials in lung cancer
Untreated PD-L1 non–small cell lung cancer (NSCLC). comparing pembrolizumab to the investigational immunotherapies ociperlimab (an anti-TIGIT antibody) and tislelizumab (an anti-PD-1 checkpoint inhibitor). Participants will be treated until death or progression of disease, whichever comes first, up to approximately 39 months. The multinational study started recruiting June 8 and hopes to enroll 605 participants. U.S. trial centers are in Alabama, Alaska, California, Florida, Hawaii, Kentucky, Maine, and Virginia. Overall survival (OS) is a primary outcome, and quality of life (QoL) will be tracked. More details are avaiable at clinicaltrials.gov.
Newly diagnosed, locally advanced, unresectable NSCLC. Adult patients with newly diagnosed, histologically confirmed, locally advanced, stage III unresectable NSCL are being recruited for a phase 3 study comparing sequential combinations of concurrent chemoradiotherapy and the immunotherapies ociperlimab, tislelizumab, and durvalumab (Imfinzi). Participants will receive therapy until disease progression or up to 16 months from randomization, whichever occurs first. The trial began recruiting on June 17 at the Central Care Cancer Center, in Bolivar, Mo. OS and QoL over 16 months are secondary outcomes. More details are avaiable at clinicaltrials.gov.
Limited-stage small cell lung cancer. Patients with untreated small cell lung cancer and documented limited-stage disease (stages Tx, T1-T4, N0-3, M0; AJCC staging, eighth edition) can join a phase 2 study comparing the immunotherapies ociperlimab and tislelizumab plus concurrent chemoradiotherapy to concurrent chemoradiotherapy alone. The trial will last 30 months from the date of the study’s first recruitment. Investigators are aiming to recruit 120 people globally. U.S. sites are in Alaska, Hawaii, Kansas, Missouri, Pennsylvania, Texas, and Wisconsin. Progression-free survival is the primary outcome. OS over 30 months is a secondary outcome. QoL will not be tracked. More details are avaiable at clinicaltrials.gov.
Stage III unresectable NSCLC. Patients with stage III unresectable NSCLC with positive circulating tumor DNA are being recruited for a phase 3 study testing whether or not circulating cancer cells in the blood can be decreased by combining standard treatment durvalumab with platinum-doublet chemotherapy (carboplatin/pemetrexed or carboplatin/paclitaxel). Patients will receive durvalumab for 1 year, with or without four cycles of chemotherapy. The study opened on August 25 at Stanford University, in California. OS over 2 years is a secondary outcome. QoL will not be assessed. More details are avaiable at clinicaltrials.gov.
Untreated stage IV NSCLC. Patients with nonsquamous stage IV NSCLC not treated for metastatic disease are being recruited for a phase 2 study of the experimental immunotherapy SEA-CD40 in combination with pembrolizumab, pemetrexed, and carboplatin. Participants will be treated for approximately 2 years. Objective response rate is the primary outcome. OS over 4 years is a secondary outcome. QoL will not be assessed. The study opened on September 30 in Arkansas, California, Minnesota, Ohio, and Texas. More details are avaiable at clinicaltrials.gov.
Untreated metastatic NSCLC. Patients with metastatic squamous or nonsquamous NSCLC are sought for a phase 3 trial that will compare a new subcutaneous formulation of pembrolizumab with standard intravenous pembrolizumab, both given in combination with chemotherapy. Patients will be treated with immunotherapy for up to approximately 2 years until the occurrence of disease progression or intolerable adverse events or the participant/physician decides to stop. Drug pharmacokinetic performance is the primary outcome measure. OS over 5 years will be analyzed as a secondary outcome. QoL will not be assessed. The international trial has U.S. sites in Florida, Montana, Tennessee, Texas, and Virginia. More details are available at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Untreated PD-L1 non–small cell lung cancer (NSCLC). comparing pembrolizumab to the investigational immunotherapies ociperlimab (an anti-TIGIT antibody) and tislelizumab (an anti-PD-1 checkpoint inhibitor). Participants will be treated until death or progression of disease, whichever comes first, up to approximately 39 months. The multinational study started recruiting June 8 and hopes to enroll 605 participants. U.S. trial centers are in Alabama, Alaska, California, Florida, Hawaii, Kentucky, Maine, and Virginia. Overall survival (OS) is a primary outcome, and quality of life (QoL) will be tracked. More details are avaiable at clinicaltrials.gov.
Newly diagnosed, locally advanced, unresectable NSCLC. Adult patients with newly diagnosed, histologically confirmed, locally advanced, stage III unresectable NSCL are being recruited for a phase 3 study comparing sequential combinations of concurrent chemoradiotherapy and the immunotherapies ociperlimab, tislelizumab, and durvalumab (Imfinzi). Participants will receive therapy until disease progression or up to 16 months from randomization, whichever occurs first. The trial began recruiting on June 17 at the Central Care Cancer Center, in Bolivar, Mo. OS and QoL over 16 months are secondary outcomes. More details are avaiable at clinicaltrials.gov.
Limited-stage small cell lung cancer. Patients with untreated small cell lung cancer and documented limited-stage disease (stages Tx, T1-T4, N0-3, M0; AJCC staging, eighth edition) can join a phase 2 study comparing the immunotherapies ociperlimab and tislelizumab plus concurrent chemoradiotherapy to concurrent chemoradiotherapy alone. The trial will last 30 months from the date of the study’s first recruitment. Investigators are aiming to recruit 120 people globally. U.S. sites are in Alaska, Hawaii, Kansas, Missouri, Pennsylvania, Texas, and Wisconsin. Progression-free survival is the primary outcome. OS over 30 months is a secondary outcome. QoL will not be tracked. More details are avaiable at clinicaltrials.gov.
Stage III unresectable NSCLC. Patients with stage III unresectable NSCLC with positive circulating tumor DNA are being recruited for a phase 3 study testing whether or not circulating cancer cells in the blood can be decreased by combining standard treatment durvalumab with platinum-doublet chemotherapy (carboplatin/pemetrexed or carboplatin/paclitaxel). Patients will receive durvalumab for 1 year, with or without four cycles of chemotherapy. The study opened on August 25 at Stanford University, in California. OS over 2 years is a secondary outcome. QoL will not be assessed. More details are avaiable at clinicaltrials.gov.
Untreated stage IV NSCLC. Patients with nonsquamous stage IV NSCLC not treated for metastatic disease are being recruited for a phase 2 study of the experimental immunotherapy SEA-CD40 in combination with pembrolizumab, pemetrexed, and carboplatin. Participants will be treated for approximately 2 years. Objective response rate is the primary outcome. OS over 4 years is a secondary outcome. QoL will not be assessed. The study opened on September 30 in Arkansas, California, Minnesota, Ohio, and Texas. More details are avaiable at clinicaltrials.gov.
Untreated metastatic NSCLC. Patients with metastatic squamous or nonsquamous NSCLC are sought for a phase 3 trial that will compare a new subcutaneous formulation of pembrolizumab with standard intravenous pembrolizumab, both given in combination with chemotherapy. Patients will be treated with immunotherapy for up to approximately 2 years until the occurrence of disease progression or intolerable adverse events or the participant/physician decides to stop. Drug pharmacokinetic performance is the primary outcome measure. OS over 5 years will be analyzed as a secondary outcome. QoL will not be assessed. The international trial has U.S. sites in Florida, Montana, Tennessee, Texas, and Virginia. More details are available at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Untreated PD-L1 non–small cell lung cancer (NSCLC). comparing pembrolizumab to the investigational immunotherapies ociperlimab (an anti-TIGIT antibody) and tislelizumab (an anti-PD-1 checkpoint inhibitor). Participants will be treated until death or progression of disease, whichever comes first, up to approximately 39 months. The multinational study started recruiting June 8 and hopes to enroll 605 participants. U.S. trial centers are in Alabama, Alaska, California, Florida, Hawaii, Kentucky, Maine, and Virginia. Overall survival (OS) is a primary outcome, and quality of life (QoL) will be tracked. More details are avaiable at clinicaltrials.gov.
Newly diagnosed, locally advanced, unresectable NSCLC. Adult patients with newly diagnosed, histologically confirmed, locally advanced, stage III unresectable NSCL are being recruited for a phase 3 study comparing sequential combinations of concurrent chemoradiotherapy and the immunotherapies ociperlimab, tislelizumab, and durvalumab (Imfinzi). Participants will receive therapy until disease progression or up to 16 months from randomization, whichever occurs first. The trial began recruiting on June 17 at the Central Care Cancer Center, in Bolivar, Mo. OS and QoL over 16 months are secondary outcomes. More details are avaiable at clinicaltrials.gov.
Limited-stage small cell lung cancer. Patients with untreated small cell lung cancer and documented limited-stage disease (stages Tx, T1-T4, N0-3, M0; AJCC staging, eighth edition) can join a phase 2 study comparing the immunotherapies ociperlimab and tislelizumab plus concurrent chemoradiotherapy to concurrent chemoradiotherapy alone. The trial will last 30 months from the date of the study’s first recruitment. Investigators are aiming to recruit 120 people globally. U.S. sites are in Alaska, Hawaii, Kansas, Missouri, Pennsylvania, Texas, and Wisconsin. Progression-free survival is the primary outcome. OS over 30 months is a secondary outcome. QoL will not be tracked. More details are avaiable at clinicaltrials.gov.
Stage III unresectable NSCLC. Patients with stage III unresectable NSCLC with positive circulating tumor DNA are being recruited for a phase 3 study testing whether or not circulating cancer cells in the blood can be decreased by combining standard treatment durvalumab with platinum-doublet chemotherapy (carboplatin/pemetrexed or carboplatin/paclitaxel). Patients will receive durvalumab for 1 year, with or without four cycles of chemotherapy. The study opened on August 25 at Stanford University, in California. OS over 2 years is a secondary outcome. QoL will not be assessed. More details are avaiable at clinicaltrials.gov.
Untreated stage IV NSCLC. Patients with nonsquamous stage IV NSCLC not treated for metastatic disease are being recruited for a phase 2 study of the experimental immunotherapy SEA-CD40 in combination with pembrolizumab, pemetrexed, and carboplatin. Participants will be treated for approximately 2 years. Objective response rate is the primary outcome. OS over 4 years is a secondary outcome. QoL will not be assessed. The study opened on September 30 in Arkansas, California, Minnesota, Ohio, and Texas. More details are avaiable at clinicaltrials.gov.
Untreated metastatic NSCLC. Patients with metastatic squamous or nonsquamous NSCLC are sought for a phase 3 trial that will compare a new subcutaneous formulation of pembrolizumab with standard intravenous pembrolizumab, both given in combination with chemotherapy. Patients will be treated with immunotherapy for up to approximately 2 years until the occurrence of disease progression or intolerable adverse events or the participant/physician decides to stop. Drug pharmacokinetic performance is the primary outcome measure. OS over 5 years will be analyzed as a secondary outcome. QoL will not be assessed. The international trial has U.S. sites in Florida, Montana, Tennessee, Texas, and Virginia. More details are available at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Gut bacteria may fuel prostate cancer treatment resistance
A mainstay of treatment for prostate cancer is to deprive it of androgens, the hormones that make it grow. The testes are the main source of these hormones, so treatment can consist of either surgical removal of these organs or use of drugs to block their hormone production.
Over time, some prostate cancers become resistant to these treatments and begin to expand again. As with many cancers that show these behaviors, finding exactly what makes them resistant can be tricky.
A culprit may be bacteria that live in the gut. Researchers found that in castrated mice and in people having androgen deprivation therapy, some of these gut bacteria start producing androgens that are easily taken into the bloodstream. According to these new findings,published in the journal Science, the androgens seem to support the growth of prostate cancer and its resistance to treatment.
Androgen deprivation treatment may also lead to more of these hormone-producing microbes in the gut, the results suggest. Fecal bacterial of people with treatment-resistant prostate cancer also showed a link to lower life expectancy.
Fecal transplants from mice with treatment-resistant prostate cancer could trigger resistance in animals with disease susceptible to these hormones. When these mice received fecal transplants from humans with resistant cancer, the effect was the same: a shift to treatment resistance.
But the converse also was true: Fecal transplants from mice or humans with hormone-susceptible cancer contributed to limiting tumor growth.
The findings may suggest new therapeutic targets: the microbes living in the gut. In mouse studies, the researchers found that when they wiped out these bacteria, the cancer was much slower to progress to treatment resistance. Authors of a commentary accompanying the study say there are other places to look for bacteria that might be making these hormones, too, including the urinary tract or even in the tumor itself.
A version of this article first appeared on WebMD.com.
A mainstay of treatment for prostate cancer is to deprive it of androgens, the hormones that make it grow. The testes are the main source of these hormones, so treatment can consist of either surgical removal of these organs or use of drugs to block their hormone production.
Over time, some prostate cancers become resistant to these treatments and begin to expand again. As with many cancers that show these behaviors, finding exactly what makes them resistant can be tricky.
A culprit may be bacteria that live in the gut. Researchers found that in castrated mice and in people having androgen deprivation therapy, some of these gut bacteria start producing androgens that are easily taken into the bloodstream. According to these new findings,published in the journal Science, the androgens seem to support the growth of prostate cancer and its resistance to treatment.
Androgen deprivation treatment may also lead to more of these hormone-producing microbes in the gut, the results suggest. Fecal bacterial of people with treatment-resistant prostate cancer also showed a link to lower life expectancy.
Fecal transplants from mice with treatment-resistant prostate cancer could trigger resistance in animals with disease susceptible to these hormones. When these mice received fecal transplants from humans with resistant cancer, the effect was the same: a shift to treatment resistance.
But the converse also was true: Fecal transplants from mice or humans with hormone-susceptible cancer contributed to limiting tumor growth.
The findings may suggest new therapeutic targets: the microbes living in the gut. In mouse studies, the researchers found that when they wiped out these bacteria, the cancer was much slower to progress to treatment resistance. Authors of a commentary accompanying the study say there are other places to look for bacteria that might be making these hormones, too, including the urinary tract or even in the tumor itself.
A version of this article first appeared on WebMD.com.
A mainstay of treatment for prostate cancer is to deprive it of androgens, the hormones that make it grow. The testes are the main source of these hormones, so treatment can consist of either surgical removal of these organs or use of drugs to block their hormone production.
Over time, some prostate cancers become resistant to these treatments and begin to expand again. As with many cancers that show these behaviors, finding exactly what makes them resistant can be tricky.
A culprit may be bacteria that live in the gut. Researchers found that in castrated mice and in people having androgen deprivation therapy, some of these gut bacteria start producing androgens that are easily taken into the bloodstream. According to these new findings,published in the journal Science, the androgens seem to support the growth of prostate cancer and its resistance to treatment.
Androgen deprivation treatment may also lead to more of these hormone-producing microbes in the gut, the results suggest. Fecal bacterial of people with treatment-resistant prostate cancer also showed a link to lower life expectancy.
Fecal transplants from mice with treatment-resistant prostate cancer could trigger resistance in animals with disease susceptible to these hormones. When these mice received fecal transplants from humans with resistant cancer, the effect was the same: a shift to treatment resistance.
But the converse also was true: Fecal transplants from mice or humans with hormone-susceptible cancer contributed to limiting tumor growth.
The findings may suggest new therapeutic targets: the microbes living in the gut. In mouse studies, the researchers found that when they wiped out these bacteria, the cancer was much slower to progress to treatment resistance. Authors of a commentary accompanying the study say there are other places to look for bacteria that might be making these hormones, too, including the urinary tract or even in the tumor itself.
A version of this article first appeared on WebMD.com.
No advantages to using ADM in implant-based breast reconstruction
A European study involving 155 women found that the use of acellular dermal matrix (ADM) did not lead to fewer reoperations, nor was it superior in terms of health-related quality of life or patient-reported cosmetic outcomes.
“We feel that women considering implant-based reconstructions for breast cancer should be informed about the lack of evidence supporting its advantage,” said lead author Fredrik Lohmander MD, department of breast and endocrine surgery, section of breast urgery, Karolinska University Hospital, Stockholm.
It is difficult to say generally whether ADM should be used in IBBR, he noted. “We can only conclude from our trial that there is no hard evidence that ADM is beneficial when performing breast reconstructions with implants,” he said in an interview. “In selected patients, ADM might be indicated.”
The study was conducted in Sweden and the United Kingdom. “Mostly because of high costs, ADM in implant-based breast reconstructions in Sweden is not frequently used,” Dr. Lohmander said. “It is slightly more common in the U.K., but much more common in the U.S.A.”
Although biological meshes have received regulatory approval by the U.S. Food and Drug Administration for reconstructive purposes, ADM has not been approved for use in breast reconstruction surgery, and its use in this setting is off label.
The study was published online October 1 in JAMA Network Open.
Any advantage to using mesh device?
Previous studies of ADMs suggested that the mesh device conferred several benefits, including superior cosmetic results, less need for tissue expanders, fewer elective reoperations, and less capsular contracture. The use of a mesh device also enlarges the subpectoral pocket, which allows for larger fixed-volume implants, the authors note.
However, these suggested advantages have not been universally accepted, and the authors note that there have been reports of associated harm, such as higher rates of infection and implant loss.
The new study included 135 women from five centers in Sweden and the United Kingdom. The patients had breast cancer and had planned to undergo mastectomy and immediate IBBR between 2014 and May 2017.
The primary endpoint was the number of repeat surgeries at 2 years.
At the 2-year follow-up, 31 patients (48%) in the ADM group had undergone at least one reoperation on the ipsilateral side, vs 35 (54%) in the control group (P = .54). Results were similar for the contralateral side: 34 (53%) vs 31 (48%).
Two patients in the ADM group and three patients in the control group underwent a risk-reducing mastectomy on the contralateral side. These five surgeries were included in the final analysis.
For nine patients (14%) in the ADM arm, the implant was removed. Four of the removals took place within 6 months after early surgical complications. In the control group, seven patients (11%) underwent implant removal; four were removed within 6 months, owing to early surgical complications.
The secondary endpoint was postoperative health-related quality of life, including perception of body image and satisfaction with cosmetic outcome. There were no significant differences between the two groups.
Some questions remain
Approached for comment on the study, Sameer A. Patel, MD, FACS, chief of plastic and reconstructive surgery at Fox Chase Cancer Center, Philadelphia, noted that the practice of using AMD for breast reconstruction is quite common in the United States, so these data are informative and add to the current understanding of the value of ADM in breast reconstruction. “The study hypothesized that the use of ADM would reduce the number of reoperations within the first 24 months, which it did not,” he said. “This is despite the fact that the ADM group had a significantly higher number of direct-to-implant reconstructions.”
Importantly, the study showed that patient-reported outcomes, as opposed to surgeon’s evaluation of outcomes, were also not different for the most part between the two groups, Dr. Patel pointed out. “The only exception of small favorable advantage in the ADM group was for fitting bras,” he said.
However, there were limitations to the study’s endpoint. “I would add that there are some purported advantages of using ADM, such as reduction in postoperative pain and reduction in length of hospital stay, which are not evaluated by this study,” Patel explained. “Also, I am not certain that they can conclude from this study that capsular contracture is not reduced, because it is not designed to evaluate that.”
But the biggest limitation is one that study authors point out in their discussion at the end of the article, he added. “The use of prepectoral reconstruction is rapidly replacing the dual plane reconstruction that this paper used in the ADM group,” Dr. Patel said. “The role of ADM in prepectoral reconstruction is somewhat different than in the dual plane reconstruction, and so these results may not necessarily be extrapolated to prepectoral reconstruction.”
The study was funded with grants from the Swedish Breast Cancer Association and Stockholm City Council. The trial was initiated by Karolinska University Hospital and Karolinska Institutet. Acelity (an Allergan company) supplied the study with acellular dermal matrix meshes. Dr. Lohmander and Dr. Patel have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A European study involving 155 women found that the use of acellular dermal matrix (ADM) did not lead to fewer reoperations, nor was it superior in terms of health-related quality of life or patient-reported cosmetic outcomes.
“We feel that women considering implant-based reconstructions for breast cancer should be informed about the lack of evidence supporting its advantage,” said lead author Fredrik Lohmander MD, department of breast and endocrine surgery, section of breast urgery, Karolinska University Hospital, Stockholm.
It is difficult to say generally whether ADM should be used in IBBR, he noted. “We can only conclude from our trial that there is no hard evidence that ADM is beneficial when performing breast reconstructions with implants,” he said in an interview. “In selected patients, ADM might be indicated.”
The study was conducted in Sweden and the United Kingdom. “Mostly because of high costs, ADM in implant-based breast reconstructions in Sweden is not frequently used,” Dr. Lohmander said. “It is slightly more common in the U.K., but much more common in the U.S.A.”
Although biological meshes have received regulatory approval by the U.S. Food and Drug Administration for reconstructive purposes, ADM has not been approved for use in breast reconstruction surgery, and its use in this setting is off label.
The study was published online October 1 in JAMA Network Open.
Any advantage to using mesh device?
Previous studies of ADMs suggested that the mesh device conferred several benefits, including superior cosmetic results, less need for tissue expanders, fewer elective reoperations, and less capsular contracture. The use of a mesh device also enlarges the subpectoral pocket, which allows for larger fixed-volume implants, the authors note.
However, these suggested advantages have not been universally accepted, and the authors note that there have been reports of associated harm, such as higher rates of infection and implant loss.
The new study included 135 women from five centers in Sweden and the United Kingdom. The patients had breast cancer and had planned to undergo mastectomy and immediate IBBR between 2014 and May 2017.
The primary endpoint was the number of repeat surgeries at 2 years.
At the 2-year follow-up, 31 patients (48%) in the ADM group had undergone at least one reoperation on the ipsilateral side, vs 35 (54%) in the control group (P = .54). Results were similar for the contralateral side: 34 (53%) vs 31 (48%).
Two patients in the ADM group and three patients in the control group underwent a risk-reducing mastectomy on the contralateral side. These five surgeries were included in the final analysis.
For nine patients (14%) in the ADM arm, the implant was removed. Four of the removals took place within 6 months after early surgical complications. In the control group, seven patients (11%) underwent implant removal; four were removed within 6 months, owing to early surgical complications.
The secondary endpoint was postoperative health-related quality of life, including perception of body image and satisfaction with cosmetic outcome. There were no significant differences between the two groups.
Some questions remain
Approached for comment on the study, Sameer A. Patel, MD, FACS, chief of plastic and reconstructive surgery at Fox Chase Cancer Center, Philadelphia, noted that the practice of using AMD for breast reconstruction is quite common in the United States, so these data are informative and add to the current understanding of the value of ADM in breast reconstruction. “The study hypothesized that the use of ADM would reduce the number of reoperations within the first 24 months, which it did not,” he said. “This is despite the fact that the ADM group had a significantly higher number of direct-to-implant reconstructions.”
Importantly, the study showed that patient-reported outcomes, as opposed to surgeon’s evaluation of outcomes, were also not different for the most part between the two groups, Dr. Patel pointed out. “The only exception of small favorable advantage in the ADM group was for fitting bras,” he said.
However, there were limitations to the study’s endpoint. “I would add that there are some purported advantages of using ADM, such as reduction in postoperative pain and reduction in length of hospital stay, which are not evaluated by this study,” Patel explained. “Also, I am not certain that they can conclude from this study that capsular contracture is not reduced, because it is not designed to evaluate that.”
But the biggest limitation is one that study authors point out in their discussion at the end of the article, he added. “The use of prepectoral reconstruction is rapidly replacing the dual plane reconstruction that this paper used in the ADM group,” Dr. Patel said. “The role of ADM in prepectoral reconstruction is somewhat different than in the dual plane reconstruction, and so these results may not necessarily be extrapolated to prepectoral reconstruction.”
The study was funded with grants from the Swedish Breast Cancer Association and Stockholm City Council. The trial was initiated by Karolinska University Hospital and Karolinska Institutet. Acelity (an Allergan company) supplied the study with acellular dermal matrix meshes. Dr. Lohmander and Dr. Patel have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A European study involving 155 women found that the use of acellular dermal matrix (ADM) did not lead to fewer reoperations, nor was it superior in terms of health-related quality of life or patient-reported cosmetic outcomes.
“We feel that women considering implant-based reconstructions for breast cancer should be informed about the lack of evidence supporting its advantage,” said lead author Fredrik Lohmander MD, department of breast and endocrine surgery, section of breast urgery, Karolinska University Hospital, Stockholm.
It is difficult to say generally whether ADM should be used in IBBR, he noted. “We can only conclude from our trial that there is no hard evidence that ADM is beneficial when performing breast reconstructions with implants,” he said in an interview. “In selected patients, ADM might be indicated.”
The study was conducted in Sweden and the United Kingdom. “Mostly because of high costs, ADM in implant-based breast reconstructions in Sweden is not frequently used,” Dr. Lohmander said. “It is slightly more common in the U.K., but much more common in the U.S.A.”
Although biological meshes have received regulatory approval by the U.S. Food and Drug Administration for reconstructive purposes, ADM has not been approved for use in breast reconstruction surgery, and its use in this setting is off label.
The study was published online October 1 in JAMA Network Open.
Any advantage to using mesh device?
Previous studies of ADMs suggested that the mesh device conferred several benefits, including superior cosmetic results, less need for tissue expanders, fewer elective reoperations, and less capsular contracture. The use of a mesh device also enlarges the subpectoral pocket, which allows for larger fixed-volume implants, the authors note.
However, these suggested advantages have not been universally accepted, and the authors note that there have been reports of associated harm, such as higher rates of infection and implant loss.
The new study included 135 women from five centers in Sweden and the United Kingdom. The patients had breast cancer and had planned to undergo mastectomy and immediate IBBR between 2014 and May 2017.
The primary endpoint was the number of repeat surgeries at 2 years.
At the 2-year follow-up, 31 patients (48%) in the ADM group had undergone at least one reoperation on the ipsilateral side, vs 35 (54%) in the control group (P = .54). Results were similar for the contralateral side: 34 (53%) vs 31 (48%).
Two patients in the ADM group and three patients in the control group underwent a risk-reducing mastectomy on the contralateral side. These five surgeries were included in the final analysis.
For nine patients (14%) in the ADM arm, the implant was removed. Four of the removals took place within 6 months after early surgical complications. In the control group, seven patients (11%) underwent implant removal; four were removed within 6 months, owing to early surgical complications.
The secondary endpoint was postoperative health-related quality of life, including perception of body image and satisfaction with cosmetic outcome. There were no significant differences between the two groups.
Some questions remain
Approached for comment on the study, Sameer A. Patel, MD, FACS, chief of plastic and reconstructive surgery at Fox Chase Cancer Center, Philadelphia, noted that the practice of using AMD for breast reconstruction is quite common in the United States, so these data are informative and add to the current understanding of the value of ADM in breast reconstruction. “The study hypothesized that the use of ADM would reduce the number of reoperations within the first 24 months, which it did not,” he said. “This is despite the fact that the ADM group had a significantly higher number of direct-to-implant reconstructions.”
Importantly, the study showed that patient-reported outcomes, as opposed to surgeon’s evaluation of outcomes, were also not different for the most part between the two groups, Dr. Patel pointed out. “The only exception of small favorable advantage in the ADM group was for fitting bras,” he said.
However, there were limitations to the study’s endpoint. “I would add that there are some purported advantages of using ADM, such as reduction in postoperative pain and reduction in length of hospital stay, which are not evaluated by this study,” Patel explained. “Also, I am not certain that they can conclude from this study that capsular contracture is not reduced, because it is not designed to evaluate that.”
But the biggest limitation is one that study authors point out in their discussion at the end of the article, he added. “The use of prepectoral reconstruction is rapidly replacing the dual plane reconstruction that this paper used in the ADM group,” Dr. Patel said. “The role of ADM in prepectoral reconstruction is somewhat different than in the dual plane reconstruction, and so these results may not necessarily be extrapolated to prepectoral reconstruction.”
The study was funded with grants from the Swedish Breast Cancer Association and Stockholm City Council. The trial was initiated by Karolinska University Hospital and Karolinska Institutet. Acelity (an Allergan company) supplied the study with acellular dermal matrix meshes. Dr. Lohmander and Dr. Patel have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Watchful waiting sometimes best for asymptomatic basal cell carcinoma
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
FROM JAMA DERMATOLOGY
Community mourns nurse knocked over, killed in Times Square
in New York City. The Mass was promoted by the local consulate general of the Philippines.
Maria Ambrocio, 58, was visiting Times Square with a friend on October 1 when she was shoved to the ground by a man who reportedly snatched a cellphone and was running away. He later collided with a police officer before being arrested.
Ms. Ambrosio, of Bayonne, N.J., was taken to Bellevue Hospital in Manhattan with a traumatic brain injury. She was taken off life support a day later.
Jermaine Foster, 26, was charged with murder and robbery and is scheduled to appear in New York Criminal Court Thursday, according to court records.
Ms. Ambrocio, who had been a nurse for 25 years at Bayonne Medical Center in New Jersey, treated cancer patients, even during the height of the pandemic. The medical community at the hospital posted on social media, “Maria’s untimely death is a profound loss to us all, especially those whose lives she touched each day at Bayonne Medical Center.”
New York organizations expressed sympathy after the incident. Tom Harris, president of the Times Square Alliance, said in a statement shared with this news organization, “Our deepest condolences to the family of Maria Ambrocio. The killing of Maria Ambrocio near Times Square highlights one of our city’s greatest public safety challenges, the proliferation of people with untreated mental illness and drug addictions on our streets committing crimes without an effective strategy to address them. Our city needs to come together and solve these problems and those of us who work in these areas are willing and able to help. Let her death not be in vain.”
The New York Philippine consulate reported on its Facebook page that Ms. Ambrocio had just visited its office when the incident occurred. “We grieve with the rest of the Filipino Community over the death of our kababayan [countryman], Maria Ambrocio, a 58-year-old health frontliner from Bayonne, New Jersey....
“Maria’s passing was announced shortly after she was removed from life support a few hours ago. She had been on life support for the head trauma she sustained on Friday afternoon after she was knocked down by someone who was described as a mentally disturbed homeless man. Maria was walking with a kababayan near Times Square after visiting the Philippine consulate general when she was struck by the suspect, who was reportedly being chased after grabbing a mobile phone from someone.”
On the day she passed away, Bayonne Mayor Jimmy Davis shared an emotional message on Facebook: “I’m asking for all Bayonne people to say a prayer for Maria Ambrocio. Maria, an Oncology nurse at Bayonne Medical Center, was viciously attacked in an unprovoked assault by a deranged man in Times Square yesterday.
“Please keep Maria and her family in your thoughts through these difficult days.”
A version of this article first appeared on Medscape.com.
in New York City. The Mass was promoted by the local consulate general of the Philippines.
Maria Ambrocio, 58, was visiting Times Square with a friend on October 1 when she was shoved to the ground by a man who reportedly snatched a cellphone and was running away. He later collided with a police officer before being arrested.
Ms. Ambrosio, of Bayonne, N.J., was taken to Bellevue Hospital in Manhattan with a traumatic brain injury. She was taken off life support a day later.
Jermaine Foster, 26, was charged with murder and robbery and is scheduled to appear in New York Criminal Court Thursday, according to court records.
Ms. Ambrocio, who had been a nurse for 25 years at Bayonne Medical Center in New Jersey, treated cancer patients, even during the height of the pandemic. The medical community at the hospital posted on social media, “Maria’s untimely death is a profound loss to us all, especially those whose lives she touched each day at Bayonne Medical Center.”
New York organizations expressed sympathy after the incident. Tom Harris, president of the Times Square Alliance, said in a statement shared with this news organization, “Our deepest condolences to the family of Maria Ambrocio. The killing of Maria Ambrocio near Times Square highlights one of our city’s greatest public safety challenges, the proliferation of people with untreated mental illness and drug addictions on our streets committing crimes without an effective strategy to address them. Our city needs to come together and solve these problems and those of us who work in these areas are willing and able to help. Let her death not be in vain.”
The New York Philippine consulate reported on its Facebook page that Ms. Ambrocio had just visited its office when the incident occurred. “We grieve with the rest of the Filipino Community over the death of our kababayan [countryman], Maria Ambrocio, a 58-year-old health frontliner from Bayonne, New Jersey....
“Maria’s passing was announced shortly after she was removed from life support a few hours ago. She had been on life support for the head trauma she sustained on Friday afternoon after she was knocked down by someone who was described as a mentally disturbed homeless man. Maria was walking with a kababayan near Times Square after visiting the Philippine consulate general when she was struck by the suspect, who was reportedly being chased after grabbing a mobile phone from someone.”
On the day she passed away, Bayonne Mayor Jimmy Davis shared an emotional message on Facebook: “I’m asking for all Bayonne people to say a prayer for Maria Ambrocio. Maria, an Oncology nurse at Bayonne Medical Center, was viciously attacked in an unprovoked assault by a deranged man in Times Square yesterday.
“Please keep Maria and her family in your thoughts through these difficult days.”
A version of this article first appeared on Medscape.com.
in New York City. The Mass was promoted by the local consulate general of the Philippines.
Maria Ambrocio, 58, was visiting Times Square with a friend on October 1 when she was shoved to the ground by a man who reportedly snatched a cellphone and was running away. He later collided with a police officer before being arrested.
Ms. Ambrosio, of Bayonne, N.J., was taken to Bellevue Hospital in Manhattan with a traumatic brain injury. She was taken off life support a day later.
Jermaine Foster, 26, was charged with murder and robbery and is scheduled to appear in New York Criminal Court Thursday, according to court records.
Ms. Ambrocio, who had been a nurse for 25 years at Bayonne Medical Center in New Jersey, treated cancer patients, even during the height of the pandemic. The medical community at the hospital posted on social media, “Maria’s untimely death is a profound loss to us all, especially those whose lives she touched each day at Bayonne Medical Center.”
New York organizations expressed sympathy after the incident. Tom Harris, president of the Times Square Alliance, said in a statement shared with this news organization, “Our deepest condolences to the family of Maria Ambrocio. The killing of Maria Ambrocio near Times Square highlights one of our city’s greatest public safety challenges, the proliferation of people with untreated mental illness and drug addictions on our streets committing crimes without an effective strategy to address them. Our city needs to come together and solve these problems and those of us who work in these areas are willing and able to help. Let her death not be in vain.”
The New York Philippine consulate reported on its Facebook page that Ms. Ambrocio had just visited its office when the incident occurred. “We grieve with the rest of the Filipino Community over the death of our kababayan [countryman], Maria Ambrocio, a 58-year-old health frontliner from Bayonne, New Jersey....
“Maria’s passing was announced shortly after she was removed from life support a few hours ago. She had been on life support for the head trauma she sustained on Friday afternoon after she was knocked down by someone who was described as a mentally disturbed homeless man. Maria was walking with a kababayan near Times Square after visiting the Philippine consulate general when she was struck by the suspect, who was reportedly being chased after grabbing a mobile phone from someone.”
On the day she passed away, Bayonne Mayor Jimmy Davis shared an emotional message on Facebook: “I’m asking for all Bayonne people to say a prayer for Maria Ambrocio. Maria, an Oncology nurse at Bayonne Medical Center, was viciously attacked in an unprovoked assault by a deranged man in Times Square yesterday.
“Please keep Maria and her family in your thoughts through these difficult days.”
A version of this article first appeared on Medscape.com.
Benzene prompts recalls of spray antifungals and sunscreens

Bayer has voluntarily recalled batches of its Lotrimin and Tinactin products because of benzene detected in some samples, according to an Oct. 1 company announcement, available on the Food and Drug Administration website. “It is important to note that Bayer’s decision to voluntarily recall these products is a precautionary measure and that the levels detected are not expected to cause adverse health consequences in consumers,” the announcement said.
Benzene is classified as a human carcinogen present in the environment from both natural sources and human activity, and it has been shown to cause cancer with long-term exposure.
The products included in the recall – all in aerosol spray cans – are unexpired Lotrimin and Tinactin sprays with lot numbers starting with TN, CV, or NAA that were distributed to consumer venues between September 2018 and September 2021. The over-the-counter products are Lotrimin Anti-Fungal Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal Jock Itch (AFJI) Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal (AF) Athlete’s Foot Deodorant Powder Spray, Lotrimin AF Athlete’s Foot Liquid Spray, Lotrimin AF Athlete’s Foot Daily Prevention Deodorant Powder Spray, Tinactin Jock Itch (JI) Powder Spray, Tinactin Athlete’s Foot Deodorant Powder Spray, Tinactin Athlete’s Foot Powder Spray, and Tinactin Athlete’s Foot Liquid Spray.
Bayer has received no reports of adverse events related to the recall. The company also reported no concerns with its antifungal creams or other products.
In addition, Coppertone has issued a voluntary recall of specific lots of five spray sunscreen products because of the presence of benzene, according to a Sept. 30th company announcement, also posted on the FDA website. The recall includes Pure&Simple spray for babies, children, and adults; Coppertone Sport Mineral Spray; and Travel-sized Coppertone Sport spray. The specific lots were manufactured between January and June 2021, and are listed on the company announcement.
“Daily exposure to benzene at the levels detected in these affected Coppertone aerosol sunscreen spray products would not be expected to cause adverse health consequences based on generally accepted exposure modeling by numerous regulatory agencies,” according to the announcement. Coppertone has received no reports of adverse events related to the recall.
In the announcement, Coppertone advised consumers to discontinue use of the impacted products, dispose of the aerosol cans properly, and contact their physician or health care provider if they experience any problems related to the sunscreen sprays.
In May 2021, online pharmacy Valisure, which routinely tests their medications, petitioned the FDA to recall specific sunscreens after detecting high benzene levels in several brands and batches of sunscreen products. The FDA evaluated the petition, but the agency itself did not issue any recalls of sunscreens.
Clinicians are advised to report any adverse events to the FDA’s MedWatch Adverse Event Reporting program either online or by regular mail or fax using this form.
Bayer has voluntarily recalled batches of its Lotrimin and Tinactin products because of benzene detected in some samples, according to an Oct. 1 company announcement, available on the Food and Drug Administration website. “It is important to note that Bayer’s decision to voluntarily recall these products is a precautionary measure and that the levels detected are not expected to cause adverse health consequences in consumers,” the announcement said.
Benzene is classified as a human carcinogen present in the environment from both natural sources and human activity, and it has been shown to cause cancer with long-term exposure.
The products included in the recall – all in aerosol spray cans – are unexpired Lotrimin and Tinactin sprays with lot numbers starting with TN, CV, or NAA that were distributed to consumer venues between September 2018 and September 2021. The over-the-counter products are Lotrimin Anti-Fungal Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal Jock Itch (AFJI) Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal (AF) Athlete’s Foot Deodorant Powder Spray, Lotrimin AF Athlete’s Foot Liquid Spray, Lotrimin AF Athlete’s Foot Daily Prevention Deodorant Powder Spray, Tinactin Jock Itch (JI) Powder Spray, Tinactin Athlete’s Foot Deodorant Powder Spray, Tinactin Athlete’s Foot Powder Spray, and Tinactin Athlete’s Foot Liquid Spray.
Bayer has received no reports of adverse events related to the recall. The company also reported no concerns with its antifungal creams or other products.
In addition, Coppertone has issued a voluntary recall of specific lots of five spray sunscreen products because of the presence of benzene, according to a Sept. 30th company announcement, also posted on the FDA website. The recall includes Pure&Simple spray for babies, children, and adults; Coppertone Sport Mineral Spray; and Travel-sized Coppertone Sport spray. The specific lots were manufactured between January and June 2021, and are listed on the company announcement.
“Daily exposure to benzene at the levels detected in these affected Coppertone aerosol sunscreen spray products would not be expected to cause adverse health consequences based on generally accepted exposure modeling by numerous regulatory agencies,” according to the announcement. Coppertone has received no reports of adverse events related to the recall.
In the announcement, Coppertone advised consumers to discontinue use of the impacted products, dispose of the aerosol cans properly, and contact their physician or health care provider if they experience any problems related to the sunscreen sprays.
In May 2021, online pharmacy Valisure, which routinely tests their medications, petitioned the FDA to recall specific sunscreens after detecting high benzene levels in several brands and batches of sunscreen products. The FDA evaluated the petition, but the agency itself did not issue any recalls of sunscreens.
Clinicians are advised to report any adverse events to the FDA’s MedWatch Adverse Event Reporting program either online or by regular mail or fax using this form.
Bayer has voluntarily recalled batches of its Lotrimin and Tinactin products because of benzene detected in some samples, according to an Oct. 1 company announcement, available on the Food and Drug Administration website. “It is important to note that Bayer’s decision to voluntarily recall these products is a precautionary measure and that the levels detected are not expected to cause adverse health consequences in consumers,” the announcement said.
Benzene is classified as a human carcinogen present in the environment from both natural sources and human activity, and it has been shown to cause cancer with long-term exposure.
The products included in the recall – all in aerosol spray cans – are unexpired Lotrimin and Tinactin sprays with lot numbers starting with TN, CV, or NAA that were distributed to consumer venues between September 2018 and September 2021. The over-the-counter products are Lotrimin Anti-Fungal Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal Jock Itch (AFJI) Athlete’s Foot Powder Spray, Lotrimin Anti-Fungal (AF) Athlete’s Foot Deodorant Powder Spray, Lotrimin AF Athlete’s Foot Liquid Spray, Lotrimin AF Athlete’s Foot Daily Prevention Deodorant Powder Spray, Tinactin Jock Itch (JI) Powder Spray, Tinactin Athlete’s Foot Deodorant Powder Spray, Tinactin Athlete’s Foot Powder Spray, and Tinactin Athlete’s Foot Liquid Spray.
Bayer has received no reports of adverse events related to the recall. The company also reported no concerns with its antifungal creams or other products.
In addition, Coppertone has issued a voluntary recall of specific lots of five spray sunscreen products because of the presence of benzene, according to a Sept. 30th company announcement, also posted on the FDA website. The recall includes Pure&Simple spray for babies, children, and adults; Coppertone Sport Mineral Spray; and Travel-sized Coppertone Sport spray. The specific lots were manufactured between January and June 2021, and are listed on the company announcement.
“Daily exposure to benzene at the levels detected in these affected Coppertone aerosol sunscreen spray products would not be expected to cause adverse health consequences based on generally accepted exposure modeling by numerous regulatory agencies,” according to the announcement. Coppertone has received no reports of adverse events related to the recall.
In the announcement, Coppertone advised consumers to discontinue use of the impacted products, dispose of the aerosol cans properly, and contact their physician or health care provider if they experience any problems related to the sunscreen sprays.
In May 2021, online pharmacy Valisure, which routinely tests their medications, petitioned the FDA to recall specific sunscreens after detecting high benzene levels in several brands and batches of sunscreen products. The FDA evaluated the petition, but the agency itself did not issue any recalls of sunscreens.
Clinicians are advised to report any adverse events to the FDA’s MedWatch Adverse Event Reporting program either online or by regular mail or fax using this form.
‘Regionalized’ care tied to better survival in tough cancer
The Kaiser Permanente Northern California (KPNC) Gastric-Esophageal Cancer Program was established in 2016 to consolidate the care of patients with gastric cancer and increase physician specialization and standardization.
In a retrospective study, Kaiser Permanente investigators compared the outcomes of the 942 patients diagnosed before the regional gastric cancer team was established with the outcomes of the 487 patients treated after it was implemented. Overall, the transformation appears to enhance the delivery of care and improves clinical and oncologic outcomes.
For example, among 394 patients who received curative-intent surgery, overall survival at 2 years increased from 72.7% before the program to 85.5% afterward.
“The regionalized gastric cancer program combines the benefits of community-based care, which is local and convenient, with the expertise of a specialized cancer center,” said coauthor Lisa Herrinton, PhD, a research scientist at the Kaiser Permanente division of research, in a statement.
She added that, in their integrated care system, “it is easy for the different physicians that treat cancer patients – including surgical oncologists, medical oncologists, and radiation oncologists, among others – to come together and collaborate and tie their work flows together.”
The study was published in the Journal of Clinical Oncology.
Gastric cancer accounts for about 27,600 cases diagnosed annually in the United States, but the overall 5-year survival is still only 32%. About half of the cases are locoregional (stage I-III) and potentially eligible for curative-intent surgery and adjuvant therapy, the authors pointed out in the study.
As compared with North America, the incidence rate is five to six times higher in East Asia, but they have developed better surveillance for early detection and treatment is highly effective, as the increased incidence allows oncologists and surgeons to achieve greater specialization. Laparoscopic gastrectomy and extended (D2) lymph node dissection are more commonly performed in East Asia as compared with the United States, and surgical outcomes appear to be better in East Asia.
Regionalizing care
The rationale for regionalizing care was that increasing and concentrating the volume of cases to a specific location would make it more possible to introduce new surgical procedures as well as allow medical oncologists to uniformly introduce and standardize the use of the newest chemotherapy regimens.
Prior to regionalization, gastric cancer surgery was performed at 19 medical centers in the Kaiser system. Now, curative-intent laparoscopic gastrectomy with Roux-en-Y gastrojejunostomy or esophagojejunostomy and side-to-side jejunojejunostomy is subsequently performed at only two centers by five surgeons.
“The two centers were selected based on how skilled the surgeons were at performing advanced minimally invasive oncologic surgery,” said lead author Swee H. Teh, MD, surgical director, gastric cancer surgery, Kaiser Permanente Northern California. “We also looked at the center’s retrospective gastrectomy outcomes and the strength of the leadership that would be collaborating with the regional multidisciplinary team.”
Dr. Teh said in an interview that it was imperative that their regional gastric cancer centers have surgeons highly skilled in advanced minimally invasive gastrointestinal surgery. “This is a newer technique and not one of our more senior surgeons had been trained in [it],” he said. “With this change, some surgeons were now no longer performing gastric cancer surgery.”
Not only were the centers selected based on the surgical skills of the surgeons already there, but they also took into account the locations and geographical membership distribution. “We have found that our patients’ traveling distance to receive surgical care has not changed significantly,” Dr. Teh said.
Improved outcomes
The cohort included 1,429 eligible patients all stages of gastric cancer; one-third were treated after regionalization, 650 had stage I-III disease, and 394 underwent curative-intent surgery.
Overall survival at 2 years was 32.8% pre- and 37.3% post regionalization (P = .20) for all stages of cancer; stage I-III cases with or without surgery, 55.6% and 61.1%, respectively (P = .25); and among all surgery patients, 72.7% and 85.5%, respectively (P < .03).
Among patients who underwent surgery, the use of neoadjuvant chemotherapy increased from 35% to 66% (P < .0001), as did laparoscopic gastrectomy from 18% to 92% (P < .0001), and D2 lymphadenectomy from 2% to 80% (P < .0001). In addition, dissection of 15 or more lymph nodes also rose from 61% to 95% (P < .0001). Post regionalization, the resection margin was more often negative, and the resection less often involved other organs.
The median length of hospitalization declined from 7 to 3 days (P < .001) after regionalization but all-cause readmissions and reoperation at 30 and 90 days were similar in both cohorts. The risk of bowel obstruction was less frequent post regionalization (P = .01 at both 30 and 90 days), as was risk of infection (P = .03 at 30 days and P = .01 at 90 days).
The risk of one or more serious adverse events was also lower (P < .01), and 30-day mortality did not change (pre 0.7% and post 0.0%, P = .34).
Generalizability may not be feasible
But although this was successful for Kaiser, the authors note that a key limitation of the study is generalizability – and that regionalization may not be feasible in many U.S. settings.
“There needs to be a standardized workflow that all stakeholders agree upon,” Dr. Teh explained. “For example, in our gastric cancer staging pathway, all patients who are considered candidates for surgery have four staging tests: CT scan, PET scan and endoscopic ultrasound [EUS], and staging laparoscopy.”
Another important aspect is that in order to make sure the workflow is smooth and timely, all subspecialties responsible for the staging modalities need to create a “special access.” What this means, he continued, is for example, that the radiology department must ensure that these patients will have their CT scan and PET scans promptly. “Similarly, the GI department must provide quick access to EUS, and the surgery department must quickly provide a staging laparoscopy,” Dr. Teh said. “We have been extremely successful in achieving this goal.”
Dr. Teh also noted that a skilled patient navigator and a team where each member brings high-level expertise and experience to the table are also necessary. And innovative technology is also needed.
“We use artificial intelligence to identify all newly diagnosed cases of gastric [cancer], and within 24 hours of a patient’s diagnosis, a notification is sent to entire team about this new patient,” he added. “We also use AI to extract data to create a dashboard that will track each patient’s progress and outcomes, so that the results are accessible to every member of the team. The innovative technology has also helped us build a comprehensive survivorship program.”
They also noted in their study that European and Canadian systems, as well as the Department of Veterans Affairs, could probably implement components of this, including enhanced recovery after surgery.
The study had no specific funding. Dr. Teh and Dr. Herrinton have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Kaiser Permanente Northern California (KPNC) Gastric-Esophageal Cancer Program was established in 2016 to consolidate the care of patients with gastric cancer and increase physician specialization and standardization.
In a retrospective study, Kaiser Permanente investigators compared the outcomes of the 942 patients diagnosed before the regional gastric cancer team was established with the outcomes of the 487 patients treated after it was implemented. Overall, the transformation appears to enhance the delivery of care and improves clinical and oncologic outcomes.
For example, among 394 patients who received curative-intent surgery, overall survival at 2 years increased from 72.7% before the program to 85.5% afterward.
“The regionalized gastric cancer program combines the benefits of community-based care, which is local and convenient, with the expertise of a specialized cancer center,” said coauthor Lisa Herrinton, PhD, a research scientist at the Kaiser Permanente division of research, in a statement.
She added that, in their integrated care system, “it is easy for the different physicians that treat cancer patients – including surgical oncologists, medical oncologists, and radiation oncologists, among others – to come together and collaborate and tie their work flows together.”
The study was published in the Journal of Clinical Oncology.
Gastric cancer accounts for about 27,600 cases diagnosed annually in the United States, but the overall 5-year survival is still only 32%. About half of the cases are locoregional (stage I-III) and potentially eligible for curative-intent surgery and adjuvant therapy, the authors pointed out in the study.
As compared with North America, the incidence rate is five to six times higher in East Asia, but they have developed better surveillance for early detection and treatment is highly effective, as the increased incidence allows oncologists and surgeons to achieve greater specialization. Laparoscopic gastrectomy and extended (D2) lymph node dissection are more commonly performed in East Asia as compared with the United States, and surgical outcomes appear to be better in East Asia.
Regionalizing care
The rationale for regionalizing care was that increasing and concentrating the volume of cases to a specific location would make it more possible to introduce new surgical procedures as well as allow medical oncologists to uniformly introduce and standardize the use of the newest chemotherapy regimens.
Prior to regionalization, gastric cancer surgery was performed at 19 medical centers in the Kaiser system. Now, curative-intent laparoscopic gastrectomy with Roux-en-Y gastrojejunostomy or esophagojejunostomy and side-to-side jejunojejunostomy is subsequently performed at only two centers by five surgeons.
“The two centers were selected based on how skilled the surgeons were at performing advanced minimally invasive oncologic surgery,” said lead author Swee H. Teh, MD, surgical director, gastric cancer surgery, Kaiser Permanente Northern California. “We also looked at the center’s retrospective gastrectomy outcomes and the strength of the leadership that would be collaborating with the regional multidisciplinary team.”
Dr. Teh said in an interview that it was imperative that their regional gastric cancer centers have surgeons highly skilled in advanced minimally invasive gastrointestinal surgery. “This is a newer technique and not one of our more senior surgeons had been trained in [it],” he said. “With this change, some surgeons were now no longer performing gastric cancer surgery.”
Not only were the centers selected based on the surgical skills of the surgeons already there, but they also took into account the locations and geographical membership distribution. “We have found that our patients’ traveling distance to receive surgical care has not changed significantly,” Dr. Teh said.
Improved outcomes
The cohort included 1,429 eligible patients all stages of gastric cancer; one-third were treated after regionalization, 650 had stage I-III disease, and 394 underwent curative-intent surgery.
Overall survival at 2 years was 32.8% pre- and 37.3% post regionalization (P = .20) for all stages of cancer; stage I-III cases with or without surgery, 55.6% and 61.1%, respectively (P = .25); and among all surgery patients, 72.7% and 85.5%, respectively (P < .03).
Among patients who underwent surgery, the use of neoadjuvant chemotherapy increased from 35% to 66% (P < .0001), as did laparoscopic gastrectomy from 18% to 92% (P < .0001), and D2 lymphadenectomy from 2% to 80% (P < .0001). In addition, dissection of 15 or more lymph nodes also rose from 61% to 95% (P < .0001). Post regionalization, the resection margin was more often negative, and the resection less often involved other organs.
The median length of hospitalization declined from 7 to 3 days (P < .001) after regionalization but all-cause readmissions and reoperation at 30 and 90 days were similar in both cohorts. The risk of bowel obstruction was less frequent post regionalization (P = .01 at both 30 and 90 days), as was risk of infection (P = .03 at 30 days and P = .01 at 90 days).
The risk of one or more serious adverse events was also lower (P < .01), and 30-day mortality did not change (pre 0.7% and post 0.0%, P = .34).
Generalizability may not be feasible
But although this was successful for Kaiser, the authors note that a key limitation of the study is generalizability – and that regionalization may not be feasible in many U.S. settings.
“There needs to be a standardized workflow that all stakeholders agree upon,” Dr. Teh explained. “For example, in our gastric cancer staging pathway, all patients who are considered candidates for surgery have four staging tests: CT scan, PET scan and endoscopic ultrasound [EUS], and staging laparoscopy.”
Another important aspect is that in order to make sure the workflow is smooth and timely, all subspecialties responsible for the staging modalities need to create a “special access.” What this means, he continued, is for example, that the radiology department must ensure that these patients will have their CT scan and PET scans promptly. “Similarly, the GI department must provide quick access to EUS, and the surgery department must quickly provide a staging laparoscopy,” Dr. Teh said. “We have been extremely successful in achieving this goal.”
Dr. Teh also noted that a skilled patient navigator and a team where each member brings high-level expertise and experience to the table are also necessary. And innovative technology is also needed.
“We use artificial intelligence to identify all newly diagnosed cases of gastric [cancer], and within 24 hours of a patient’s diagnosis, a notification is sent to entire team about this new patient,” he added. “We also use AI to extract data to create a dashboard that will track each patient’s progress and outcomes, so that the results are accessible to every member of the team. The innovative technology has also helped us build a comprehensive survivorship program.”
They also noted in their study that European and Canadian systems, as well as the Department of Veterans Affairs, could probably implement components of this, including enhanced recovery after surgery.
The study had no specific funding. Dr. Teh and Dr. Herrinton have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Kaiser Permanente Northern California (KPNC) Gastric-Esophageal Cancer Program was established in 2016 to consolidate the care of patients with gastric cancer and increase physician specialization and standardization.
In a retrospective study, Kaiser Permanente investigators compared the outcomes of the 942 patients diagnosed before the regional gastric cancer team was established with the outcomes of the 487 patients treated after it was implemented. Overall, the transformation appears to enhance the delivery of care and improves clinical and oncologic outcomes.
For example, among 394 patients who received curative-intent surgery, overall survival at 2 years increased from 72.7% before the program to 85.5% afterward.
“The regionalized gastric cancer program combines the benefits of community-based care, which is local and convenient, with the expertise of a specialized cancer center,” said coauthor Lisa Herrinton, PhD, a research scientist at the Kaiser Permanente division of research, in a statement.
She added that, in their integrated care system, “it is easy for the different physicians that treat cancer patients – including surgical oncologists, medical oncologists, and radiation oncologists, among others – to come together and collaborate and tie their work flows together.”
The study was published in the Journal of Clinical Oncology.
Gastric cancer accounts for about 27,600 cases diagnosed annually in the United States, but the overall 5-year survival is still only 32%. About half of the cases are locoregional (stage I-III) and potentially eligible for curative-intent surgery and adjuvant therapy, the authors pointed out in the study.
As compared with North America, the incidence rate is five to six times higher in East Asia, but they have developed better surveillance for early detection and treatment is highly effective, as the increased incidence allows oncologists and surgeons to achieve greater specialization. Laparoscopic gastrectomy and extended (D2) lymph node dissection are more commonly performed in East Asia as compared with the United States, and surgical outcomes appear to be better in East Asia.
Regionalizing care
The rationale for regionalizing care was that increasing and concentrating the volume of cases to a specific location would make it more possible to introduce new surgical procedures as well as allow medical oncologists to uniformly introduce and standardize the use of the newest chemotherapy regimens.
Prior to regionalization, gastric cancer surgery was performed at 19 medical centers in the Kaiser system. Now, curative-intent laparoscopic gastrectomy with Roux-en-Y gastrojejunostomy or esophagojejunostomy and side-to-side jejunojejunostomy is subsequently performed at only two centers by five surgeons.
“The two centers were selected based on how skilled the surgeons were at performing advanced minimally invasive oncologic surgery,” said lead author Swee H. Teh, MD, surgical director, gastric cancer surgery, Kaiser Permanente Northern California. “We also looked at the center’s retrospective gastrectomy outcomes and the strength of the leadership that would be collaborating with the regional multidisciplinary team.”
Dr. Teh said in an interview that it was imperative that their regional gastric cancer centers have surgeons highly skilled in advanced minimally invasive gastrointestinal surgery. “This is a newer technique and not one of our more senior surgeons had been trained in [it],” he said. “With this change, some surgeons were now no longer performing gastric cancer surgery.”
Not only were the centers selected based on the surgical skills of the surgeons already there, but they also took into account the locations and geographical membership distribution. “We have found that our patients’ traveling distance to receive surgical care has not changed significantly,” Dr. Teh said.
Improved outcomes
The cohort included 1,429 eligible patients all stages of gastric cancer; one-third were treated after regionalization, 650 had stage I-III disease, and 394 underwent curative-intent surgery.
Overall survival at 2 years was 32.8% pre- and 37.3% post regionalization (P = .20) for all stages of cancer; stage I-III cases with or without surgery, 55.6% and 61.1%, respectively (P = .25); and among all surgery patients, 72.7% and 85.5%, respectively (P < .03).
Among patients who underwent surgery, the use of neoadjuvant chemotherapy increased from 35% to 66% (P < .0001), as did laparoscopic gastrectomy from 18% to 92% (P < .0001), and D2 lymphadenectomy from 2% to 80% (P < .0001). In addition, dissection of 15 or more lymph nodes also rose from 61% to 95% (P < .0001). Post regionalization, the resection margin was more often negative, and the resection less often involved other organs.
The median length of hospitalization declined from 7 to 3 days (P < .001) after regionalization but all-cause readmissions and reoperation at 30 and 90 days were similar in both cohorts. The risk of bowel obstruction was less frequent post regionalization (P = .01 at both 30 and 90 days), as was risk of infection (P = .03 at 30 days and P = .01 at 90 days).
The risk of one or more serious adverse events was also lower (P < .01), and 30-day mortality did not change (pre 0.7% and post 0.0%, P = .34).
Generalizability may not be feasible
But although this was successful for Kaiser, the authors note that a key limitation of the study is generalizability – and that regionalization may not be feasible in many U.S. settings.
“There needs to be a standardized workflow that all stakeholders agree upon,” Dr. Teh explained. “For example, in our gastric cancer staging pathway, all patients who are considered candidates for surgery have four staging tests: CT scan, PET scan and endoscopic ultrasound [EUS], and staging laparoscopy.”
Another important aspect is that in order to make sure the workflow is smooth and timely, all subspecialties responsible for the staging modalities need to create a “special access.” What this means, he continued, is for example, that the radiology department must ensure that these patients will have their CT scan and PET scans promptly. “Similarly, the GI department must provide quick access to EUS, and the surgery department must quickly provide a staging laparoscopy,” Dr. Teh said. “We have been extremely successful in achieving this goal.”
Dr. Teh also noted that a skilled patient navigator and a team where each member brings high-level expertise and experience to the table are also necessary. And innovative technology is also needed.
“We use artificial intelligence to identify all newly diagnosed cases of gastric [cancer], and within 24 hours of a patient’s diagnosis, a notification is sent to entire team about this new patient,” he added. “We also use AI to extract data to create a dashboard that will track each patient’s progress and outcomes, so that the results are accessible to every member of the team. The innovative technology has also helped us build a comprehensive survivorship program.”
They also noted in their study that European and Canadian systems, as well as the Department of Veterans Affairs, could probably implement components of this, including enhanced recovery after surgery.
The study had no specific funding. Dr. Teh and Dr. Herrinton have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Genes related to osteosarcoma survival identified
When they combined them into a risk score and added one additional factor – metastases at diagnosis – the model was an “excellent” predictor of 1-year survival, the team said (area under the curve, 0.947; 95% confidence interval, 0.832-0.972).
“The survival-associated” immune-related genes (IRGs) “examined in this study have potential for identifying prognosis in osteosarcoma and may be clinically useful as relevant clinical biomarkers and candidate targets for anticancer therapy,” said investigators led by Wangmi Liu, MD, of Zhejiang University in Hangzhou, China. The study was published in JAMA Network Open.
They explained that it’s often difficult to distinguish high- and low-risk patients at osteosarcoma diagnosis. To address the issue, they analyzed the genomic signatures of 84 patients in the Cancer Genome Atlas and their associated clinical information.
The team split their subjects evenly into high-risk and low-risk groups based on a score developed from their genetic signatures. A total of 26 patients in the high-risk group (61.9%) died over a median follow up of 4.1 years versus only 1 (2.4%) in the low-risk group.
The risk score also correlated positively with B-cell tumor infiltration, and negatively with infiltration of CD8 T cells and macrophages.
Overall, 16 genes were significantly up-regulated, and 187 genes were significantly down-regulated in the high-risk group, including three survival-associated IRGs: CCL2, CD79A, and FPR1.
The differentially expressed genes were most significantly associated with transmembrane signaling receptor activity and inflammatory response. The team noted that “it has been reported that inflammatory response plays a critical role in tumor initiation, promotion, malignant conversion, invasion, and metastases.”
Of the 14 survival-associated IRGs, 5 have been reported before in osteosarcoma. The other nine were deduced from computational analysis and may be potential treatment targets, including bone morphogenetic protein 8b (BMP8b). Another member of the BMP family, BMP9, has been shown to promote the proliferation of osteosarcoma cells, “which is similar to this study’s finding that BMP8b was a risk factor in osteosarcoma. Therefore, the role of BMP8b in osteosarcoma needs further research,” the team said.
“Because the database provides limited clinical information, other important factors, such as staging and grading, were not included in our analysis. Therefore, extrapolation based on the findings must be done very carefully,” they cautioned.
The work was supported by the National Natural Science Foundation of China and others. The investigators didn’t have any disclosures.
When they combined them into a risk score and added one additional factor – metastases at diagnosis – the model was an “excellent” predictor of 1-year survival, the team said (area under the curve, 0.947; 95% confidence interval, 0.832-0.972).
“The survival-associated” immune-related genes (IRGs) “examined in this study have potential for identifying prognosis in osteosarcoma and may be clinically useful as relevant clinical biomarkers and candidate targets for anticancer therapy,” said investigators led by Wangmi Liu, MD, of Zhejiang University in Hangzhou, China. The study was published in JAMA Network Open.
They explained that it’s often difficult to distinguish high- and low-risk patients at osteosarcoma diagnosis. To address the issue, they analyzed the genomic signatures of 84 patients in the Cancer Genome Atlas and their associated clinical information.
The team split their subjects evenly into high-risk and low-risk groups based on a score developed from their genetic signatures. A total of 26 patients in the high-risk group (61.9%) died over a median follow up of 4.1 years versus only 1 (2.4%) in the low-risk group.
The risk score also correlated positively with B-cell tumor infiltration, and negatively with infiltration of CD8 T cells and macrophages.
Overall, 16 genes were significantly up-regulated, and 187 genes were significantly down-regulated in the high-risk group, including three survival-associated IRGs: CCL2, CD79A, and FPR1.
The differentially expressed genes were most significantly associated with transmembrane signaling receptor activity and inflammatory response. The team noted that “it has been reported that inflammatory response plays a critical role in tumor initiation, promotion, malignant conversion, invasion, and metastases.”
Of the 14 survival-associated IRGs, 5 have been reported before in osteosarcoma. The other nine were deduced from computational analysis and may be potential treatment targets, including bone morphogenetic protein 8b (BMP8b). Another member of the BMP family, BMP9, has been shown to promote the proliferation of osteosarcoma cells, “which is similar to this study’s finding that BMP8b was a risk factor in osteosarcoma. Therefore, the role of BMP8b in osteosarcoma needs further research,” the team said.
“Because the database provides limited clinical information, other important factors, such as staging and grading, were not included in our analysis. Therefore, extrapolation based on the findings must be done very carefully,” they cautioned.
The work was supported by the National Natural Science Foundation of China and others. The investigators didn’t have any disclosures.
When they combined them into a risk score and added one additional factor – metastases at diagnosis – the model was an “excellent” predictor of 1-year survival, the team said (area under the curve, 0.947; 95% confidence interval, 0.832-0.972).
“The survival-associated” immune-related genes (IRGs) “examined in this study have potential for identifying prognosis in osteosarcoma and may be clinically useful as relevant clinical biomarkers and candidate targets for anticancer therapy,” said investigators led by Wangmi Liu, MD, of Zhejiang University in Hangzhou, China. The study was published in JAMA Network Open.
They explained that it’s often difficult to distinguish high- and low-risk patients at osteosarcoma diagnosis. To address the issue, they analyzed the genomic signatures of 84 patients in the Cancer Genome Atlas and their associated clinical information.
The team split their subjects evenly into high-risk and low-risk groups based on a score developed from their genetic signatures. A total of 26 patients in the high-risk group (61.9%) died over a median follow up of 4.1 years versus only 1 (2.4%) in the low-risk group.
The risk score also correlated positively with B-cell tumor infiltration, and negatively with infiltration of CD8 T cells and macrophages.
Overall, 16 genes were significantly up-regulated, and 187 genes were significantly down-regulated in the high-risk group, including three survival-associated IRGs: CCL2, CD79A, and FPR1.
The differentially expressed genes were most significantly associated with transmembrane signaling receptor activity and inflammatory response. The team noted that “it has been reported that inflammatory response plays a critical role in tumor initiation, promotion, malignant conversion, invasion, and metastases.”
Of the 14 survival-associated IRGs, 5 have been reported before in osteosarcoma. The other nine were deduced from computational analysis and may be potential treatment targets, including bone morphogenetic protein 8b (BMP8b). Another member of the BMP family, BMP9, has been shown to promote the proliferation of osteosarcoma cells, “which is similar to this study’s finding that BMP8b was a risk factor in osteosarcoma. Therefore, the role of BMP8b in osteosarcoma needs further research,” the team said.
“Because the database provides limited clinical information, other important factors, such as staging and grading, were not included in our analysis. Therefore, extrapolation based on the findings must be done very carefully,” they cautioned.
The work was supported by the National Natural Science Foundation of China and others. The investigators didn’t have any disclosures.
FROM JAMA NETWORK OPEN