User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
CV admissions on the rise in Americans with cancer
Although cardiovascular disease (CVD) is known to often strike the mortal blow in patients with cancer, a national analysis puts in stark relief the burden of CV-related hospitalizations in this vulnerable population.
, whereas admissions fell 10.9% among those without cancer.
Admissions increased steadily across all cancer types, except prostate cancer, with heart failure being the most common reason for admission.
“Hospital admissions is really important because we know that the size of this group is increasing, given that they live longer and many of the treatments that we offer cause cardiovascular disease or increase the risk of having cardiovascular events. So, from a health care planning perspective, I think it’s really important to see what the burden is likely to be in the next few years,” senior author Mamas Mamas, MD, Keele University, England, told this news organization.
For physicians and the wider population, he said, the findings underscore the need to shift the conversation from saying that patients with cancer are at increased CVD risk to asking how to mitigate this risk. “Because I would say that this increase in cardiovascular admissions, that’s a failure from a preventative perspective.”
The study was published in the European Heart Journal: Quality of Care & Clinical Outcomes.
Individual cancer types
The researchers, led by Ofer Kobo, MD, also with Keele University, used the National Inpatient Sample to identify 42.5 million weighted cases of CV admissions for acute myocardial infarction (AMI), pulmonary embolism, ischemic stroke, heart failure, atrial fibrillation (AFib) or atrial flutter, and intracranial hemorrhage from January 2004 to December 2017. Of these, 1.9 million had a record of cancer.
Patients with cancer were older; had a higher prevalence of valvular disease, anemia, and coagulopathy; and had a lower prevalence of hypertension, diabetes mellitus, and obesity than did patients without cancer.
The most common cancer type was hematologic cancers (26.1%), followed by lung (18.7%), gastrointestinal (12.4%), prostate (11.6%), breast (6.7%), and other in 24.4%.
The admission rate increased across all six admission causes – between 7% for AMI and ischemic stroke and 46% for AFib.
Heart failure was the chief reason for admission among all patients. Annual rates per 100,000 U.S. population increased in patients with cancer (from 13.6 to 16.6; P for trend = .02) and declined in those without (from 352.2 to 349.8; P for trend < .001).
“In the past, patients would be started on medications, and perhaps the importance of monitoring [left ventricular] LV function wasn’t as widely known, whereas now we’re much more aggressive in looking at it and much more aggressive at trying to prevent it,” Dr. Mamas said. “But even with this greater identification and attempting to modify regimens, we’re still getting quite substantial increases in heart failure admissions in this population. And what really surprised me is that it wasn’t just in the breast cancer population, but it was nearly across the board.”
He noted that patients are at highest risk from CV events within the first 2 years of cancer diagnosis. “So that’s really the time where you’ve got to be really aggressive in looking and working up their cardiovascular profile.”
Patients with hematologic cancers (9.7-13.5), lung (7.4-8.9), and gastrointestinal cancer (4.6-6.3) had the highest crude admission rates of CV hospitalizations per 100,000 U.S. population.
The CV admission rate went up from 2.5 to 3.7 per 100,000 U.S. population for breast cancer, and in prostate cancer, the rate dropped from 5.8 to 4.8 per 100,000 U.S. population.
Of note, patients with hematologic cancers also had the highest rate of heart failure hospitalization across all cancer types, which, coupled with their increasing admission rates, likely reflects their exposure to a “constellation of cardiotoxic therapies” as well as pathologic processes related to the cancers themselves, the authors suggest.
In-hospital mortality rates were higher among patients with cancer than those without, ranging from 5% for patients with breast cancer to 9.6% for patients with lung cancer versus 4.2% for those without cancer.
Among patients with cancer, the odds ratio for mortality was highest in those admitted with AFib (4.43), followed by pulmonary embolism (2.36), AMI (2.31), ischemic stroke (2.29), and heart failure (2.24).
In line with prior work and general population trends, in-hospital deaths in primary CV admissions trended lower among patients with cancer over the study period.
Mitigating risk
Commenting on the study, Joerg Herrmann, MD, director of the cardio-oncology clinic at Mayo Clinic, Rochester, Minn., said that the data are “extremely important” because they reflect admissions during a new era of cancer therapy. “Targeted therapies all came out about the turn of the millennium, so we’re not really looking at cancer patients treated with only old and ancient strategies.”
This may be one reason for the increased admissions, but because the study lacked information on specific cancer treatments and the date of cancer diagnosis, it’s not possible to tease out whether the uptick is related to cardiotoxicity or because the oncology outcomes have improved so much that this is a growing population, he said.
One clear implication, however, is that whoever is working on the hospital service will see more patients with a cancer diagnosis, Dr. Herrmann observed.
“Though some may have tried to maybe not get involved with this topic as much, it really calls for some broader scope to get familiar with this very entity,” he said. “And that plays out, in particular, in those patients with a diagnosis of active cancer.”
Dr. Herrmann and colleagues previously reported that patients with active leukemia or lymphoma who were hospitalized with acute coronary syndrome were less likely to receive guideline-directed therapies, even at the Mayo Clinic.
Similarly, a 2020 report by Dr. Mamas and colleagues found that patients with a variety of active cancers derived similar benefit from primary percutaneous coronary intervention for ST-segment–elevation MI as those without cancer but received the treatment less commonly.
Although there’s a greater appreciation that patients with cancer benefit equally from aggressive treatment, much more can be done to mitigate CV risk, Dr. Mamas noted. Valuable coronary information captured by MRI and CT done as part of the cancer investigation is often overlooked. For example, “we know that breast calcification and vascular calcification in the breast are very strong predictors of cardiovascular outcomes and yet people aren’t using this information.”
There are numerous shared risk factors in the development of cancer and coronary artery disease, and patients with cancer often have much worse CV risk profiles but aren’t routinely risk stratified from a CV perspective, he said.
Dr. Mamas said that his team is also studying whether CVD risk prediction tools like the Framingham Risk Score, which were derived from noncancer populations, work as well in patients with cancer. “Often, when you look at the performance of these tools in populations that weren’t covered, they’re much worse.”
“A lot of cancer survivors worry about the recurrence of their cancer and will religiously go and have repeated scans, religiously check themselves, and have all these investigations but don’t think about the actual risk that is greater for them, which is cardiovascular risk,” he said.
The authors report no study funding or relevant financial relationships.
A version of this article first appeared on Medscape.com.
Although cardiovascular disease (CVD) is known to often strike the mortal blow in patients with cancer, a national analysis puts in stark relief the burden of CV-related hospitalizations in this vulnerable population.
, whereas admissions fell 10.9% among those without cancer.
Admissions increased steadily across all cancer types, except prostate cancer, with heart failure being the most common reason for admission.
“Hospital admissions is really important because we know that the size of this group is increasing, given that they live longer and many of the treatments that we offer cause cardiovascular disease or increase the risk of having cardiovascular events. So, from a health care planning perspective, I think it’s really important to see what the burden is likely to be in the next few years,” senior author Mamas Mamas, MD, Keele University, England, told this news organization.
For physicians and the wider population, he said, the findings underscore the need to shift the conversation from saying that patients with cancer are at increased CVD risk to asking how to mitigate this risk. “Because I would say that this increase in cardiovascular admissions, that’s a failure from a preventative perspective.”
The study was published in the European Heart Journal: Quality of Care & Clinical Outcomes.
Individual cancer types
The researchers, led by Ofer Kobo, MD, also with Keele University, used the National Inpatient Sample to identify 42.5 million weighted cases of CV admissions for acute myocardial infarction (AMI), pulmonary embolism, ischemic stroke, heart failure, atrial fibrillation (AFib) or atrial flutter, and intracranial hemorrhage from January 2004 to December 2017. Of these, 1.9 million had a record of cancer.
Patients with cancer were older; had a higher prevalence of valvular disease, anemia, and coagulopathy; and had a lower prevalence of hypertension, diabetes mellitus, and obesity than did patients without cancer.
The most common cancer type was hematologic cancers (26.1%), followed by lung (18.7%), gastrointestinal (12.4%), prostate (11.6%), breast (6.7%), and other in 24.4%.
The admission rate increased across all six admission causes – between 7% for AMI and ischemic stroke and 46% for AFib.
Heart failure was the chief reason for admission among all patients. Annual rates per 100,000 U.S. population increased in patients with cancer (from 13.6 to 16.6; P for trend = .02) and declined in those without (from 352.2 to 349.8; P for trend < .001).
“In the past, patients would be started on medications, and perhaps the importance of monitoring [left ventricular] LV function wasn’t as widely known, whereas now we’re much more aggressive in looking at it and much more aggressive at trying to prevent it,” Dr. Mamas said. “But even with this greater identification and attempting to modify regimens, we’re still getting quite substantial increases in heart failure admissions in this population. And what really surprised me is that it wasn’t just in the breast cancer population, but it was nearly across the board.”
He noted that patients are at highest risk from CV events within the first 2 years of cancer diagnosis. “So that’s really the time where you’ve got to be really aggressive in looking and working up their cardiovascular profile.”
Patients with hematologic cancers (9.7-13.5), lung (7.4-8.9), and gastrointestinal cancer (4.6-6.3) had the highest crude admission rates of CV hospitalizations per 100,000 U.S. population.
The CV admission rate went up from 2.5 to 3.7 per 100,000 U.S. population for breast cancer, and in prostate cancer, the rate dropped from 5.8 to 4.8 per 100,000 U.S. population.
Of note, patients with hematologic cancers also had the highest rate of heart failure hospitalization across all cancer types, which, coupled with their increasing admission rates, likely reflects their exposure to a “constellation of cardiotoxic therapies” as well as pathologic processes related to the cancers themselves, the authors suggest.
In-hospital mortality rates were higher among patients with cancer than those without, ranging from 5% for patients with breast cancer to 9.6% for patients with lung cancer versus 4.2% for those without cancer.
Among patients with cancer, the odds ratio for mortality was highest in those admitted with AFib (4.43), followed by pulmonary embolism (2.36), AMI (2.31), ischemic stroke (2.29), and heart failure (2.24).
In line with prior work and general population trends, in-hospital deaths in primary CV admissions trended lower among patients with cancer over the study period.
Mitigating risk
Commenting on the study, Joerg Herrmann, MD, director of the cardio-oncology clinic at Mayo Clinic, Rochester, Minn., said that the data are “extremely important” because they reflect admissions during a new era of cancer therapy. “Targeted therapies all came out about the turn of the millennium, so we’re not really looking at cancer patients treated with only old and ancient strategies.”
This may be one reason for the increased admissions, but because the study lacked information on specific cancer treatments and the date of cancer diagnosis, it’s not possible to tease out whether the uptick is related to cardiotoxicity or because the oncology outcomes have improved so much that this is a growing population, he said.
One clear implication, however, is that whoever is working on the hospital service will see more patients with a cancer diagnosis, Dr. Herrmann observed.
“Though some may have tried to maybe not get involved with this topic as much, it really calls for some broader scope to get familiar with this very entity,” he said. “And that plays out, in particular, in those patients with a diagnosis of active cancer.”
Dr. Herrmann and colleagues previously reported that patients with active leukemia or lymphoma who were hospitalized with acute coronary syndrome were less likely to receive guideline-directed therapies, even at the Mayo Clinic.
Similarly, a 2020 report by Dr. Mamas and colleagues found that patients with a variety of active cancers derived similar benefit from primary percutaneous coronary intervention for ST-segment–elevation MI as those without cancer but received the treatment less commonly.
Although there’s a greater appreciation that patients with cancer benefit equally from aggressive treatment, much more can be done to mitigate CV risk, Dr. Mamas noted. Valuable coronary information captured by MRI and CT done as part of the cancer investigation is often overlooked. For example, “we know that breast calcification and vascular calcification in the breast are very strong predictors of cardiovascular outcomes and yet people aren’t using this information.”
There are numerous shared risk factors in the development of cancer and coronary artery disease, and patients with cancer often have much worse CV risk profiles but aren’t routinely risk stratified from a CV perspective, he said.
Dr. Mamas said that his team is also studying whether CVD risk prediction tools like the Framingham Risk Score, which were derived from noncancer populations, work as well in patients with cancer. “Often, when you look at the performance of these tools in populations that weren’t covered, they’re much worse.”
“A lot of cancer survivors worry about the recurrence of their cancer and will religiously go and have repeated scans, religiously check themselves, and have all these investigations but don’t think about the actual risk that is greater for them, which is cardiovascular risk,” he said.
The authors report no study funding or relevant financial relationships.
A version of this article first appeared on Medscape.com.
Although cardiovascular disease (CVD) is known to often strike the mortal blow in patients with cancer, a national analysis puts in stark relief the burden of CV-related hospitalizations in this vulnerable population.
, whereas admissions fell 10.9% among those without cancer.
Admissions increased steadily across all cancer types, except prostate cancer, with heart failure being the most common reason for admission.
“Hospital admissions is really important because we know that the size of this group is increasing, given that they live longer and many of the treatments that we offer cause cardiovascular disease or increase the risk of having cardiovascular events. So, from a health care planning perspective, I think it’s really important to see what the burden is likely to be in the next few years,” senior author Mamas Mamas, MD, Keele University, England, told this news organization.
For physicians and the wider population, he said, the findings underscore the need to shift the conversation from saying that patients with cancer are at increased CVD risk to asking how to mitigate this risk. “Because I would say that this increase in cardiovascular admissions, that’s a failure from a preventative perspective.”
The study was published in the European Heart Journal: Quality of Care & Clinical Outcomes.
Individual cancer types
The researchers, led by Ofer Kobo, MD, also with Keele University, used the National Inpatient Sample to identify 42.5 million weighted cases of CV admissions for acute myocardial infarction (AMI), pulmonary embolism, ischemic stroke, heart failure, atrial fibrillation (AFib) or atrial flutter, and intracranial hemorrhage from January 2004 to December 2017. Of these, 1.9 million had a record of cancer.
Patients with cancer were older; had a higher prevalence of valvular disease, anemia, and coagulopathy; and had a lower prevalence of hypertension, diabetes mellitus, and obesity than did patients without cancer.
The most common cancer type was hematologic cancers (26.1%), followed by lung (18.7%), gastrointestinal (12.4%), prostate (11.6%), breast (6.7%), and other in 24.4%.
The admission rate increased across all six admission causes – between 7% for AMI and ischemic stroke and 46% for AFib.
Heart failure was the chief reason for admission among all patients. Annual rates per 100,000 U.S. population increased in patients with cancer (from 13.6 to 16.6; P for trend = .02) and declined in those without (from 352.2 to 349.8; P for trend < .001).
“In the past, patients would be started on medications, and perhaps the importance of monitoring [left ventricular] LV function wasn’t as widely known, whereas now we’re much more aggressive in looking at it and much more aggressive at trying to prevent it,” Dr. Mamas said. “But even with this greater identification and attempting to modify regimens, we’re still getting quite substantial increases in heart failure admissions in this population. And what really surprised me is that it wasn’t just in the breast cancer population, but it was nearly across the board.”
He noted that patients are at highest risk from CV events within the first 2 years of cancer diagnosis. “So that’s really the time where you’ve got to be really aggressive in looking and working up their cardiovascular profile.”
Patients with hematologic cancers (9.7-13.5), lung (7.4-8.9), and gastrointestinal cancer (4.6-6.3) had the highest crude admission rates of CV hospitalizations per 100,000 U.S. population.
The CV admission rate went up from 2.5 to 3.7 per 100,000 U.S. population for breast cancer, and in prostate cancer, the rate dropped from 5.8 to 4.8 per 100,000 U.S. population.
Of note, patients with hematologic cancers also had the highest rate of heart failure hospitalization across all cancer types, which, coupled with their increasing admission rates, likely reflects their exposure to a “constellation of cardiotoxic therapies” as well as pathologic processes related to the cancers themselves, the authors suggest.
In-hospital mortality rates were higher among patients with cancer than those without, ranging from 5% for patients with breast cancer to 9.6% for patients with lung cancer versus 4.2% for those without cancer.
Among patients with cancer, the odds ratio for mortality was highest in those admitted with AFib (4.43), followed by pulmonary embolism (2.36), AMI (2.31), ischemic stroke (2.29), and heart failure (2.24).
In line with prior work and general population trends, in-hospital deaths in primary CV admissions trended lower among patients with cancer over the study period.
Mitigating risk
Commenting on the study, Joerg Herrmann, MD, director of the cardio-oncology clinic at Mayo Clinic, Rochester, Minn., said that the data are “extremely important” because they reflect admissions during a new era of cancer therapy. “Targeted therapies all came out about the turn of the millennium, so we’re not really looking at cancer patients treated with only old and ancient strategies.”
This may be one reason for the increased admissions, but because the study lacked information on specific cancer treatments and the date of cancer diagnosis, it’s not possible to tease out whether the uptick is related to cardiotoxicity or because the oncology outcomes have improved so much that this is a growing population, he said.
One clear implication, however, is that whoever is working on the hospital service will see more patients with a cancer diagnosis, Dr. Herrmann observed.
“Though some may have tried to maybe not get involved with this topic as much, it really calls for some broader scope to get familiar with this very entity,” he said. “And that plays out, in particular, in those patients with a diagnosis of active cancer.”
Dr. Herrmann and colleagues previously reported that patients with active leukemia or lymphoma who were hospitalized with acute coronary syndrome were less likely to receive guideline-directed therapies, even at the Mayo Clinic.
Similarly, a 2020 report by Dr. Mamas and colleagues found that patients with a variety of active cancers derived similar benefit from primary percutaneous coronary intervention for ST-segment–elevation MI as those without cancer but received the treatment less commonly.
Although there’s a greater appreciation that patients with cancer benefit equally from aggressive treatment, much more can be done to mitigate CV risk, Dr. Mamas noted. Valuable coronary information captured by MRI and CT done as part of the cancer investigation is often overlooked. For example, “we know that breast calcification and vascular calcification in the breast are very strong predictors of cardiovascular outcomes and yet people aren’t using this information.”
There are numerous shared risk factors in the development of cancer and coronary artery disease, and patients with cancer often have much worse CV risk profiles but aren’t routinely risk stratified from a CV perspective, he said.
Dr. Mamas said that his team is also studying whether CVD risk prediction tools like the Framingham Risk Score, which were derived from noncancer populations, work as well in patients with cancer. “Often, when you look at the performance of these tools in populations that weren’t covered, they’re much worse.”
“A lot of cancer survivors worry about the recurrence of their cancer and will religiously go and have repeated scans, religiously check themselves, and have all these investigations but don’t think about the actual risk that is greater for them, which is cardiovascular risk,” he said.
The authors report no study funding or relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM European Heart Journal: Quality of Care & Clinical Outcomes
Consensus Statement Supporting the Presence of Onsite Radiation Oncology Departments at VHA Medical Centers
Radiation therapy, along with surgery and systemic therapy, is a primary therapeutic modality for cancer management. At least half of cancer patients receive radiation as part of their treatment regimen.1 Multiple studies demonstrate that radiotherapy is underutilized worldwide.2 One reason for underutilization of radiotherapy globally is poor access to this treatment modality. Factors that contribute to poor access include long wait times for consultation, delays in treatment initiation, distance to a treatment facility, and poor coordination of care.
Taskforce Findings
The presence of onsite radiation oncology and its impact on utilization of radiotherapy is poorly studied. The Veterans Health Administration (VHA) Palliative Radiotherapy Taskforce recently conducted a survey to determine the barriers to referral and timeliness of treatment for palliative radiotherapy within the VHA.3 Key findings of this study comparing centers with onsite radiation departments with centers without onsite radiation departments include:
a. Radiation consults are more likely to be completed within 1 week of consult request at centers with onsite radiation therapy (68% vs 31%, respectively; P = .01).
b. Centers with onsite radiation therapy more frequently deliver emergent treatment within 24 hours for patients with spinal cord compression, an emergency condition in which prompt radiation can prevent or minimize long-term neurologic disability (94% vs 70%, respectively; P = .01).
c. Referring practitioners with onsite radiation departments are less likely to report difficulty contacting a radiation oncologist as a barrier to referral for palliative radiotherapy (0% vs 20%, respectively; P = .006).
d. Referring practitioners with onsite radiotherapy report patient travel as a barrier to referral for palliative radiotherapy less frequently (28% vs 71%, respectively; P < .001).
e. Practitioners with onsite radiation oncology departments are more likely to have multidisciplinary tumor boards (31% vs 3%, respectively; P = .01) and are more likely to be influenced by radiation oncology recommendations at tumor boards (69% vs 44%, respectively; P = .02).
Based on the findings of this study, the VHA Palliative Radiotherapy Taskforce has prepared this consensus statement regarding the importance of onsite radiation oncology departments at VHA medical centers. More information regarding our 5 key findings and their implications for patient care are as follows:
Timeliness of Radiation Oncology Consultation
Delays in radiation oncology consultation, which can also delay treatment initiation, are associated with poor satisfaction among both patients and referring clinicians.4 Wait times have been identified as a barrier to utilization of radiotherapy by both patients and clinicians.5,6 Furthermore, delays in initiation of definitive therapy have been associated with worse outcomes, including worse overall survival.7,8 Our survey study demonstrates that consults for palliative radiotherapy are occurring in a more timely manner at centers with onsite radiation departments. Radiation oncology consults are more frequently completed within 1 week at centers with onsite radiation oncology departments compared with centers without onsite radiation oncology departments (68% vs 31%, P = .01). This trend would likely be seen for nonpalliative, definitive cases as well. The presence of radiation oncology departments onsite at VHA medical centers is an important component of timely care for veterans to optimize outcomes of cancer treatment.
Timely Delivery of Radiotherapy for Oncologic Emergencies
There are a few scenarios in which emergent radiation treatment, within 24 hours, is indicated. These include malignant spinal cord compression, uncal herniation from brain metastasis, superior vena cava syndrome, and tumor hemorrhage.9 Studies on management of metastatic spinal cord compression demonstrate that delays in treatment are associated with reduced ambulation10 as well as loss of sphincter function and incontinence.11
Our study demonstrates that VHA medical centers with onsite radiotherapy more frequently deliver radiotherapy within 24 hours for patients with metastatic spinal cord compression. This timely delivery of treatment is critical to optimizing functional status and quality of life in patients requiring treatment for oncologic emergencies. Revisiting treatment pathways for such situations at regular intervals is crucial given that residents and staff may rotate and be unfamiliar with emergency protocols.
Communication With Radiation Oncologists
Several studies have demonstrated that the inability to contact a radiation oncologist and poor communication result in decreased referrals for palliative radiotherapy.12,13 Our study demonstrates that onsite radiation oncology is associated with improved ability to contact a radiation oncologist. About 20% of clinicians at facilities without onsite radiation oncology reported difficulty contacting a radiation oncologist, compared with 0% at facilities with onsite radiation departments (P = .006).
It is possible that increased radiation oncology presence at VHA medical centers, through attenuation of barriers related to contacting a radiation oncologist and improved communication, would lead to increased use of radiotherapy. Increased communication between referring clinicians and radiation oncologists also can help with education of those clinicians making the referral. Since knowledge gaps have been identified in multiple studies as a barrier to referral for radiotherapy, such communication and increased education on the role of radiotherapy could increase use.12-14
Patient Travel
Patient ability to travel was the most commonly reported barrier (81%) to referral for palliative radiotherapy in our study. Travel time and transportation difficulties have been established in multiple studies as barriers to radiotherapy for both definitive and palliative management.15-18 Travel for radiotherapy was much less frequently reported as a barrier among respondents with onsite radiation oncology departments compared with those without onsite radiation departments (28% vs 71%, respectively; P < .001).
It is therefore possible that expansion of VHA radiation oncology services, allowing for provision of onsite radiotherapy at more VHA facilities, would reduce travel burden. Increasing travel accommodations for patients and provision of patient lodging on hospital campuses, which is already offered at some VHA medical centers (ie, Fisher House Foundation), could also help attenuate this barrier.
Multidisciplinary Tumor Boards
Our study demonstrates that centers with onsite radiation departments more frequently hold multidisciplinary tumor boards compared with centers without radiation departments (31% vs 3%, respectively; P = .01). Multidisciplinary tumor boards allow subspecialties to meet regularly to communicate about patient care and can help mitigate barriers related to communication and education of the referring health care practitioners.
As cases are discussed in multidisciplinary tumor boards, health care practitioners have the opportunity to make recommendations and provide education on potential benefits and/or downsides of treatments offered by their respective specialties. Several studies have demonstrated that cases discussed at multidisciplinary tumor boards are more likely to be referred for radiation therapy.19-21 Furthermore, multidisciplinary tumor boards have been associated with improved treatment outcomes.22
Conclusions
In this consensus statement the VHA Palliative Radiotherapy Taskforce recommends the optimization of use of radiotherapy within the VHA. Radiation oncology services should be maintained where present in the VHA, with consideration for expansion of services to additional facilities. Telehealth should be used to expedite consults and treatment. Hypofractionation should be used, when appropriate, to ease travel burden. Options for transportation services and onsite housing, or hospitalization, should be understood by practitioners and offered to patients to mitigate barriers related to travel.
1. Barton MB, Jacob S, Shafiq J, et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiother Oncol. 2014;112(1):140-144. doi:10.1016/j.radonc.2014.03.024
2. Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol. 2015;16(10):1153-1186. doi:10.1016/S1470-2045(15)00222-3
3. Gutt R, Malhotra S, Hagan MP, et al. Palliative radiotherapy within the Veterans Health Administration: barriers to referral and timeliness of treatment. JCO Oncol Pract. 2021;17(12):e1913-e1922. doi:10.1200/OP.20.00981
4. Agazaryan N, Chow P, Lamb J, et al. The timeliness initiative: continuous process improvement for prompt initiation of radiation therapy treatment. Adv Radiat Oncol. 2020;5(5):1014-1021. Published 2020 Mar 10. doi:10.1016/j.adro.2020.01.007
5. Gillan C, Briggs K, Goytisolo Pazos A, et al. Barriers to accessing radiation therapy in Canada: a systematic review. Radiat Oncol. 2012;7:167. Published 2012 Oct 12. doi:10.1186/1748-717X-7-167
6. Hanna TP, Richardson H, Peng Y, Kong W, Zhang-Salomons J, Mackillop WJ. A population-based study of factors affecting the use of radiotherapy for endometrial cancer. Clin Oncol (R Coll Radiol). 2012;24(8):e113-e124. doi:10.1016/j.clon.2012.01.007
7. Ho AS, Kim S, Tighiouart M, et al. Quantitative survival impact of composite treatment delays in head and neck cancer. Cancer. 2018;124(15):3154-3162. doi:10.1002/cncr.31533
8. Cone EB, Marchese M, Paciotti M, et al. Assessment of time-to-treatment initiation and survival in a cohort of patients with common cancers. JAMA Netw Open. 2020;3(12):e2030072. Published 2020 Dec 1. doi:10.1001/jamanetworkopen.2020.30072
9. Mitera G, Swaminath A, Wong S, et al. Radiotherapy for oncologic emergencies on weekends: examining reasons for treatment and patterns of practice at a Canadian cancer centre. Curr Oncol. 2009;16(4):55-60. doi:10.3747/co.v16i4.352
10. Laufer I, Zuckerman SL, Bird JE, et al. Predicting neurologic recovery after surgery in patients with deficits secondary to MESCC: systematic review. Spine (Phila Pa 1976). 2016;41 (Suppl 20):S224-S230. doi:10.1097/BRS.0000000000001827
11. Husband DJ. Malignant spinal cord compression: prospective study of delays in referral and treatment. BMJ. 1998;317(7150):18-21. doi:10.1136/bmj.317.7150.18
12. Samant RS, Fitzgibbon E, Meng J, Graham ID. Family physicians’ perspectives regarding palliative radiotherapy. Radiother Oncol. 2006;78(1):101-106. doi:10.1016/j.radonc.2005.11.008
13. McCloskey SA, Tao ML, Rose CM, Fink A, Amadeo AM. National survey of perspectives of palliative radiation therapy: role, barriers, and needs. Cancer J. 2007;13(2):130-137. doi:10.1097/PPO.0b013e31804675d4
14. Chierchini S, Ingrosso G, Saldi S, Stracci F, Aristei C. Physician and patient barriers to radiotherapy service access: treatment referral implications. Cancer Manag Res. 2019;11:8829-8833. Published 2019 Oct 7. doi:10.2147/CMAR.S168941
15. Longacre CF, Neprash HT, Shippee ND, Tuttle TM, Virnig BA. Travel, treatment choice, and survival among breast cancer patients: a population-based analysis. Womens Health Rep (New Rochelle). 2021;2(1):1-10. Published 2021 Jan 11. doi:10.1089/whr.2020.0094
16. Yang DD, Muralidhar V, Mahal BA, et al. Travel distance as a barrier to receipt of adjuvant radiation therapy after radical Prostatectomy. Am J Clin Oncol. 2018;41(10):953-959. doi:10.1097/COC.0000000000000410
17. Sundaresan P, King M, Stockler M, Costa D, Milross C. Barriers to radiotherapy utilization: Consumer perceptions of issues influencing radiotherapy-related decisions. Asia Pac J Clin Oncol. 2017;13(5):e489-e496. doi:10.1111/ajco.12579
18. Ambroggi M, Biasini C, Del Giovane C, Fornari F, Cavanna L. Distance as a barrier to cancer diagnosis and treatment: review of the literature. Oncologist. 2015;20(12):1378-1385. doi:10.1634/theoncologist.2015-0110
19. Bydder S, Nowak A, Marion K, Phillips M, Atun R. The impact of case discussion at a multidisciplinary team meeting on the treatment and survival of patients with inoperable non-small cell lung cancer. Intern Med J. 2009;39(12):838-841. doi:10.1111/j.1445-5994.2009.02019.x
20. Brännström F, Bjerregaard JK, Winbladh A, et al. Multidisciplinary team conferences promote treatment according to guidelines in rectal cancer. Acta Oncol. 2015;54(4):447-453. doi:10.3109/0284186X.2014.952387
21. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat Rev. 2016;42:56-72. doi:10.1016/j.ctrv.2015.11.007
22. Freytag M, Herrlinger U, Hauser S, et al. Higher number of multidisciplinary tumor board meetings per case leads to improved clinical outcome. BMC Cancer. 2020;20(1):355. Published 2020 Apr 28. doi:10.1186/s12885-020-06809-1
Radiation therapy, along with surgery and systemic therapy, is a primary therapeutic modality for cancer management. At least half of cancer patients receive radiation as part of their treatment regimen.1 Multiple studies demonstrate that radiotherapy is underutilized worldwide.2 One reason for underutilization of radiotherapy globally is poor access to this treatment modality. Factors that contribute to poor access include long wait times for consultation, delays in treatment initiation, distance to a treatment facility, and poor coordination of care.
Taskforce Findings
The presence of onsite radiation oncology and its impact on utilization of radiotherapy is poorly studied. The Veterans Health Administration (VHA) Palliative Radiotherapy Taskforce recently conducted a survey to determine the barriers to referral and timeliness of treatment for palliative radiotherapy within the VHA.3 Key findings of this study comparing centers with onsite radiation departments with centers without onsite radiation departments include:
a. Radiation consults are more likely to be completed within 1 week of consult request at centers with onsite radiation therapy (68% vs 31%, respectively; P = .01).
b. Centers with onsite radiation therapy more frequently deliver emergent treatment within 24 hours for patients with spinal cord compression, an emergency condition in which prompt radiation can prevent or minimize long-term neurologic disability (94% vs 70%, respectively; P = .01).
c. Referring practitioners with onsite radiation departments are less likely to report difficulty contacting a radiation oncologist as a barrier to referral for palliative radiotherapy (0% vs 20%, respectively; P = .006).
d. Referring practitioners with onsite radiotherapy report patient travel as a barrier to referral for palliative radiotherapy less frequently (28% vs 71%, respectively; P < .001).
e. Practitioners with onsite radiation oncology departments are more likely to have multidisciplinary tumor boards (31% vs 3%, respectively; P = .01) and are more likely to be influenced by radiation oncology recommendations at tumor boards (69% vs 44%, respectively; P = .02).
Based on the findings of this study, the VHA Palliative Radiotherapy Taskforce has prepared this consensus statement regarding the importance of onsite radiation oncology departments at VHA medical centers. More information regarding our 5 key findings and their implications for patient care are as follows:
Timeliness of Radiation Oncology Consultation
Delays in radiation oncology consultation, which can also delay treatment initiation, are associated with poor satisfaction among both patients and referring clinicians.4 Wait times have been identified as a barrier to utilization of radiotherapy by both patients and clinicians.5,6 Furthermore, delays in initiation of definitive therapy have been associated with worse outcomes, including worse overall survival.7,8 Our survey study demonstrates that consults for palliative radiotherapy are occurring in a more timely manner at centers with onsite radiation departments. Radiation oncology consults are more frequently completed within 1 week at centers with onsite radiation oncology departments compared with centers without onsite radiation oncology departments (68% vs 31%, P = .01). This trend would likely be seen for nonpalliative, definitive cases as well. The presence of radiation oncology departments onsite at VHA medical centers is an important component of timely care for veterans to optimize outcomes of cancer treatment.
Timely Delivery of Radiotherapy for Oncologic Emergencies
There are a few scenarios in which emergent radiation treatment, within 24 hours, is indicated. These include malignant spinal cord compression, uncal herniation from brain metastasis, superior vena cava syndrome, and tumor hemorrhage.9 Studies on management of metastatic spinal cord compression demonstrate that delays in treatment are associated with reduced ambulation10 as well as loss of sphincter function and incontinence.11
Our study demonstrates that VHA medical centers with onsite radiotherapy more frequently deliver radiotherapy within 24 hours for patients with metastatic spinal cord compression. This timely delivery of treatment is critical to optimizing functional status and quality of life in patients requiring treatment for oncologic emergencies. Revisiting treatment pathways for such situations at regular intervals is crucial given that residents and staff may rotate and be unfamiliar with emergency protocols.
Communication With Radiation Oncologists
Several studies have demonstrated that the inability to contact a radiation oncologist and poor communication result in decreased referrals for palliative radiotherapy.12,13 Our study demonstrates that onsite radiation oncology is associated with improved ability to contact a radiation oncologist. About 20% of clinicians at facilities without onsite radiation oncology reported difficulty contacting a radiation oncologist, compared with 0% at facilities with onsite radiation departments (P = .006).
It is possible that increased radiation oncology presence at VHA medical centers, through attenuation of barriers related to contacting a radiation oncologist and improved communication, would lead to increased use of radiotherapy. Increased communication between referring clinicians and radiation oncologists also can help with education of those clinicians making the referral. Since knowledge gaps have been identified in multiple studies as a barrier to referral for radiotherapy, such communication and increased education on the role of radiotherapy could increase use.12-14
Patient Travel
Patient ability to travel was the most commonly reported barrier (81%) to referral for palliative radiotherapy in our study. Travel time and transportation difficulties have been established in multiple studies as barriers to radiotherapy for both definitive and palliative management.15-18 Travel for radiotherapy was much less frequently reported as a barrier among respondents with onsite radiation oncology departments compared with those without onsite radiation departments (28% vs 71%, respectively; P < .001).
It is therefore possible that expansion of VHA radiation oncology services, allowing for provision of onsite radiotherapy at more VHA facilities, would reduce travel burden. Increasing travel accommodations for patients and provision of patient lodging on hospital campuses, which is already offered at some VHA medical centers (ie, Fisher House Foundation), could also help attenuate this barrier.
Multidisciplinary Tumor Boards
Our study demonstrates that centers with onsite radiation departments more frequently hold multidisciplinary tumor boards compared with centers without radiation departments (31% vs 3%, respectively; P = .01). Multidisciplinary tumor boards allow subspecialties to meet regularly to communicate about patient care and can help mitigate barriers related to communication and education of the referring health care practitioners.
As cases are discussed in multidisciplinary tumor boards, health care practitioners have the opportunity to make recommendations and provide education on potential benefits and/or downsides of treatments offered by their respective specialties. Several studies have demonstrated that cases discussed at multidisciplinary tumor boards are more likely to be referred for radiation therapy.19-21 Furthermore, multidisciplinary tumor boards have been associated with improved treatment outcomes.22
Conclusions
In this consensus statement the VHA Palliative Radiotherapy Taskforce recommends the optimization of use of radiotherapy within the VHA. Radiation oncology services should be maintained where present in the VHA, with consideration for expansion of services to additional facilities. Telehealth should be used to expedite consults and treatment. Hypofractionation should be used, when appropriate, to ease travel burden. Options for transportation services and onsite housing, or hospitalization, should be understood by practitioners and offered to patients to mitigate barriers related to travel.
Radiation therapy, along with surgery and systemic therapy, is a primary therapeutic modality for cancer management. At least half of cancer patients receive radiation as part of their treatment regimen.1 Multiple studies demonstrate that radiotherapy is underutilized worldwide.2 One reason for underutilization of radiotherapy globally is poor access to this treatment modality. Factors that contribute to poor access include long wait times for consultation, delays in treatment initiation, distance to a treatment facility, and poor coordination of care.
Taskforce Findings
The presence of onsite radiation oncology and its impact on utilization of radiotherapy is poorly studied. The Veterans Health Administration (VHA) Palliative Radiotherapy Taskforce recently conducted a survey to determine the barriers to referral and timeliness of treatment for palliative radiotherapy within the VHA.3 Key findings of this study comparing centers with onsite radiation departments with centers without onsite radiation departments include:
a. Radiation consults are more likely to be completed within 1 week of consult request at centers with onsite radiation therapy (68% vs 31%, respectively; P = .01).
b. Centers with onsite radiation therapy more frequently deliver emergent treatment within 24 hours for patients with spinal cord compression, an emergency condition in which prompt radiation can prevent or minimize long-term neurologic disability (94% vs 70%, respectively; P = .01).
c. Referring practitioners with onsite radiation departments are less likely to report difficulty contacting a radiation oncologist as a barrier to referral for palliative radiotherapy (0% vs 20%, respectively; P = .006).
d. Referring practitioners with onsite radiotherapy report patient travel as a barrier to referral for palliative radiotherapy less frequently (28% vs 71%, respectively; P < .001).
e. Practitioners with onsite radiation oncology departments are more likely to have multidisciplinary tumor boards (31% vs 3%, respectively; P = .01) and are more likely to be influenced by radiation oncology recommendations at tumor boards (69% vs 44%, respectively; P = .02).
Based on the findings of this study, the VHA Palliative Radiotherapy Taskforce has prepared this consensus statement regarding the importance of onsite radiation oncology departments at VHA medical centers. More information regarding our 5 key findings and their implications for patient care are as follows:
Timeliness of Radiation Oncology Consultation
Delays in radiation oncology consultation, which can also delay treatment initiation, are associated with poor satisfaction among both patients and referring clinicians.4 Wait times have been identified as a barrier to utilization of radiotherapy by both patients and clinicians.5,6 Furthermore, delays in initiation of definitive therapy have been associated with worse outcomes, including worse overall survival.7,8 Our survey study demonstrates that consults for palliative radiotherapy are occurring in a more timely manner at centers with onsite radiation departments. Radiation oncology consults are more frequently completed within 1 week at centers with onsite radiation oncology departments compared with centers without onsite radiation oncology departments (68% vs 31%, P = .01). This trend would likely be seen for nonpalliative, definitive cases as well. The presence of radiation oncology departments onsite at VHA medical centers is an important component of timely care for veterans to optimize outcomes of cancer treatment.
Timely Delivery of Radiotherapy for Oncologic Emergencies
There are a few scenarios in which emergent radiation treatment, within 24 hours, is indicated. These include malignant spinal cord compression, uncal herniation from brain metastasis, superior vena cava syndrome, and tumor hemorrhage.9 Studies on management of metastatic spinal cord compression demonstrate that delays in treatment are associated with reduced ambulation10 as well as loss of sphincter function and incontinence.11
Our study demonstrates that VHA medical centers with onsite radiotherapy more frequently deliver radiotherapy within 24 hours for patients with metastatic spinal cord compression. This timely delivery of treatment is critical to optimizing functional status and quality of life in patients requiring treatment for oncologic emergencies. Revisiting treatment pathways for such situations at regular intervals is crucial given that residents and staff may rotate and be unfamiliar with emergency protocols.
Communication With Radiation Oncologists
Several studies have demonstrated that the inability to contact a radiation oncologist and poor communication result in decreased referrals for palliative radiotherapy.12,13 Our study demonstrates that onsite radiation oncology is associated with improved ability to contact a radiation oncologist. About 20% of clinicians at facilities without onsite radiation oncology reported difficulty contacting a radiation oncologist, compared with 0% at facilities with onsite radiation departments (P = .006).
It is possible that increased radiation oncology presence at VHA medical centers, through attenuation of barriers related to contacting a radiation oncologist and improved communication, would lead to increased use of radiotherapy. Increased communication between referring clinicians and radiation oncologists also can help with education of those clinicians making the referral. Since knowledge gaps have been identified in multiple studies as a barrier to referral for radiotherapy, such communication and increased education on the role of radiotherapy could increase use.12-14
Patient Travel
Patient ability to travel was the most commonly reported barrier (81%) to referral for palliative radiotherapy in our study. Travel time and transportation difficulties have been established in multiple studies as barriers to radiotherapy for both definitive and palliative management.15-18 Travel for radiotherapy was much less frequently reported as a barrier among respondents with onsite radiation oncology departments compared with those without onsite radiation departments (28% vs 71%, respectively; P < .001).
It is therefore possible that expansion of VHA radiation oncology services, allowing for provision of onsite radiotherapy at more VHA facilities, would reduce travel burden. Increasing travel accommodations for patients and provision of patient lodging on hospital campuses, which is already offered at some VHA medical centers (ie, Fisher House Foundation), could also help attenuate this barrier.
Multidisciplinary Tumor Boards
Our study demonstrates that centers with onsite radiation departments more frequently hold multidisciplinary tumor boards compared with centers without radiation departments (31% vs 3%, respectively; P = .01). Multidisciplinary tumor boards allow subspecialties to meet regularly to communicate about patient care and can help mitigate barriers related to communication and education of the referring health care practitioners.
As cases are discussed in multidisciplinary tumor boards, health care practitioners have the opportunity to make recommendations and provide education on potential benefits and/or downsides of treatments offered by their respective specialties. Several studies have demonstrated that cases discussed at multidisciplinary tumor boards are more likely to be referred for radiation therapy.19-21 Furthermore, multidisciplinary tumor boards have been associated with improved treatment outcomes.22
Conclusions
In this consensus statement the VHA Palliative Radiotherapy Taskforce recommends the optimization of use of radiotherapy within the VHA. Radiation oncology services should be maintained where present in the VHA, with consideration for expansion of services to additional facilities. Telehealth should be used to expedite consults and treatment. Hypofractionation should be used, when appropriate, to ease travel burden. Options for transportation services and onsite housing, or hospitalization, should be understood by practitioners and offered to patients to mitigate barriers related to travel.
1. Barton MB, Jacob S, Shafiq J, et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiother Oncol. 2014;112(1):140-144. doi:10.1016/j.radonc.2014.03.024
2. Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol. 2015;16(10):1153-1186. doi:10.1016/S1470-2045(15)00222-3
3. Gutt R, Malhotra S, Hagan MP, et al. Palliative radiotherapy within the Veterans Health Administration: barriers to referral and timeliness of treatment. JCO Oncol Pract. 2021;17(12):e1913-e1922. doi:10.1200/OP.20.00981
4. Agazaryan N, Chow P, Lamb J, et al. The timeliness initiative: continuous process improvement for prompt initiation of radiation therapy treatment. Adv Radiat Oncol. 2020;5(5):1014-1021. Published 2020 Mar 10. doi:10.1016/j.adro.2020.01.007
5. Gillan C, Briggs K, Goytisolo Pazos A, et al. Barriers to accessing radiation therapy in Canada: a systematic review. Radiat Oncol. 2012;7:167. Published 2012 Oct 12. doi:10.1186/1748-717X-7-167
6. Hanna TP, Richardson H, Peng Y, Kong W, Zhang-Salomons J, Mackillop WJ. A population-based study of factors affecting the use of radiotherapy for endometrial cancer. Clin Oncol (R Coll Radiol). 2012;24(8):e113-e124. doi:10.1016/j.clon.2012.01.007
7. Ho AS, Kim S, Tighiouart M, et al. Quantitative survival impact of composite treatment delays in head and neck cancer. Cancer. 2018;124(15):3154-3162. doi:10.1002/cncr.31533
8. Cone EB, Marchese M, Paciotti M, et al. Assessment of time-to-treatment initiation and survival in a cohort of patients with common cancers. JAMA Netw Open. 2020;3(12):e2030072. Published 2020 Dec 1. doi:10.1001/jamanetworkopen.2020.30072
9. Mitera G, Swaminath A, Wong S, et al. Radiotherapy for oncologic emergencies on weekends: examining reasons for treatment and patterns of practice at a Canadian cancer centre. Curr Oncol. 2009;16(4):55-60. doi:10.3747/co.v16i4.352
10. Laufer I, Zuckerman SL, Bird JE, et al. Predicting neurologic recovery after surgery in patients with deficits secondary to MESCC: systematic review. Spine (Phila Pa 1976). 2016;41 (Suppl 20):S224-S230. doi:10.1097/BRS.0000000000001827
11. Husband DJ. Malignant spinal cord compression: prospective study of delays in referral and treatment. BMJ. 1998;317(7150):18-21. doi:10.1136/bmj.317.7150.18
12. Samant RS, Fitzgibbon E, Meng J, Graham ID. Family physicians’ perspectives regarding palliative radiotherapy. Radiother Oncol. 2006;78(1):101-106. doi:10.1016/j.radonc.2005.11.008
13. McCloskey SA, Tao ML, Rose CM, Fink A, Amadeo AM. National survey of perspectives of palliative radiation therapy: role, barriers, and needs. Cancer J. 2007;13(2):130-137. doi:10.1097/PPO.0b013e31804675d4
14. Chierchini S, Ingrosso G, Saldi S, Stracci F, Aristei C. Physician and patient barriers to radiotherapy service access: treatment referral implications. Cancer Manag Res. 2019;11:8829-8833. Published 2019 Oct 7. doi:10.2147/CMAR.S168941
15. Longacre CF, Neprash HT, Shippee ND, Tuttle TM, Virnig BA. Travel, treatment choice, and survival among breast cancer patients: a population-based analysis. Womens Health Rep (New Rochelle). 2021;2(1):1-10. Published 2021 Jan 11. doi:10.1089/whr.2020.0094
16. Yang DD, Muralidhar V, Mahal BA, et al. Travel distance as a barrier to receipt of adjuvant radiation therapy after radical Prostatectomy. Am J Clin Oncol. 2018;41(10):953-959. doi:10.1097/COC.0000000000000410
17. Sundaresan P, King M, Stockler M, Costa D, Milross C. Barriers to radiotherapy utilization: Consumer perceptions of issues influencing radiotherapy-related decisions. Asia Pac J Clin Oncol. 2017;13(5):e489-e496. doi:10.1111/ajco.12579
18. Ambroggi M, Biasini C, Del Giovane C, Fornari F, Cavanna L. Distance as a barrier to cancer diagnosis and treatment: review of the literature. Oncologist. 2015;20(12):1378-1385. doi:10.1634/theoncologist.2015-0110
19. Bydder S, Nowak A, Marion K, Phillips M, Atun R. The impact of case discussion at a multidisciplinary team meeting on the treatment and survival of patients with inoperable non-small cell lung cancer. Intern Med J. 2009;39(12):838-841. doi:10.1111/j.1445-5994.2009.02019.x
20. Brännström F, Bjerregaard JK, Winbladh A, et al. Multidisciplinary team conferences promote treatment according to guidelines in rectal cancer. Acta Oncol. 2015;54(4):447-453. doi:10.3109/0284186X.2014.952387
21. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat Rev. 2016;42:56-72. doi:10.1016/j.ctrv.2015.11.007
22. Freytag M, Herrlinger U, Hauser S, et al. Higher number of multidisciplinary tumor board meetings per case leads to improved clinical outcome. BMC Cancer. 2020;20(1):355. Published 2020 Apr 28. doi:10.1186/s12885-020-06809-1
1. Barton MB, Jacob S, Shafiq J, et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiother Oncol. 2014;112(1):140-144. doi:10.1016/j.radonc.2014.03.024
2. Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol. 2015;16(10):1153-1186. doi:10.1016/S1470-2045(15)00222-3
3. Gutt R, Malhotra S, Hagan MP, et al. Palliative radiotherapy within the Veterans Health Administration: barriers to referral and timeliness of treatment. JCO Oncol Pract. 2021;17(12):e1913-e1922. doi:10.1200/OP.20.00981
4. Agazaryan N, Chow P, Lamb J, et al. The timeliness initiative: continuous process improvement for prompt initiation of radiation therapy treatment. Adv Radiat Oncol. 2020;5(5):1014-1021. Published 2020 Mar 10. doi:10.1016/j.adro.2020.01.007
5. Gillan C, Briggs K, Goytisolo Pazos A, et al. Barriers to accessing radiation therapy in Canada: a systematic review. Radiat Oncol. 2012;7:167. Published 2012 Oct 12. doi:10.1186/1748-717X-7-167
6. Hanna TP, Richardson H, Peng Y, Kong W, Zhang-Salomons J, Mackillop WJ. A population-based study of factors affecting the use of radiotherapy for endometrial cancer. Clin Oncol (R Coll Radiol). 2012;24(8):e113-e124. doi:10.1016/j.clon.2012.01.007
7. Ho AS, Kim S, Tighiouart M, et al. Quantitative survival impact of composite treatment delays in head and neck cancer. Cancer. 2018;124(15):3154-3162. doi:10.1002/cncr.31533
8. Cone EB, Marchese M, Paciotti M, et al. Assessment of time-to-treatment initiation and survival in a cohort of patients with common cancers. JAMA Netw Open. 2020;3(12):e2030072. Published 2020 Dec 1. doi:10.1001/jamanetworkopen.2020.30072
9. Mitera G, Swaminath A, Wong S, et al. Radiotherapy for oncologic emergencies on weekends: examining reasons for treatment and patterns of practice at a Canadian cancer centre. Curr Oncol. 2009;16(4):55-60. doi:10.3747/co.v16i4.352
10. Laufer I, Zuckerman SL, Bird JE, et al. Predicting neurologic recovery after surgery in patients with deficits secondary to MESCC: systematic review. Spine (Phila Pa 1976). 2016;41 (Suppl 20):S224-S230. doi:10.1097/BRS.0000000000001827
11. Husband DJ. Malignant spinal cord compression: prospective study of delays in referral and treatment. BMJ. 1998;317(7150):18-21. doi:10.1136/bmj.317.7150.18
12. Samant RS, Fitzgibbon E, Meng J, Graham ID. Family physicians’ perspectives regarding palliative radiotherapy. Radiother Oncol. 2006;78(1):101-106. doi:10.1016/j.radonc.2005.11.008
13. McCloskey SA, Tao ML, Rose CM, Fink A, Amadeo AM. National survey of perspectives of palliative radiation therapy: role, barriers, and needs. Cancer J. 2007;13(2):130-137. doi:10.1097/PPO.0b013e31804675d4
14. Chierchini S, Ingrosso G, Saldi S, Stracci F, Aristei C. Physician and patient barriers to radiotherapy service access: treatment referral implications. Cancer Manag Res. 2019;11:8829-8833. Published 2019 Oct 7. doi:10.2147/CMAR.S168941
15. Longacre CF, Neprash HT, Shippee ND, Tuttle TM, Virnig BA. Travel, treatment choice, and survival among breast cancer patients: a population-based analysis. Womens Health Rep (New Rochelle). 2021;2(1):1-10. Published 2021 Jan 11. doi:10.1089/whr.2020.0094
16. Yang DD, Muralidhar V, Mahal BA, et al. Travel distance as a barrier to receipt of adjuvant radiation therapy after radical Prostatectomy. Am J Clin Oncol. 2018;41(10):953-959. doi:10.1097/COC.0000000000000410
17. Sundaresan P, King M, Stockler M, Costa D, Milross C. Barriers to radiotherapy utilization: Consumer perceptions of issues influencing radiotherapy-related decisions. Asia Pac J Clin Oncol. 2017;13(5):e489-e496. doi:10.1111/ajco.12579
18. Ambroggi M, Biasini C, Del Giovane C, Fornari F, Cavanna L. Distance as a barrier to cancer diagnosis and treatment: review of the literature. Oncologist. 2015;20(12):1378-1385. doi:10.1634/theoncologist.2015-0110
19. Bydder S, Nowak A, Marion K, Phillips M, Atun R. The impact of case discussion at a multidisciplinary team meeting on the treatment and survival of patients with inoperable non-small cell lung cancer. Intern Med J. 2009;39(12):838-841. doi:10.1111/j.1445-5994.2009.02019.x
20. Brännström F, Bjerregaard JK, Winbladh A, et al. Multidisciplinary team conferences promote treatment according to guidelines in rectal cancer. Acta Oncol. 2015;54(4):447-453. doi:10.3109/0284186X.2014.952387
21. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat Rev. 2016;42:56-72. doi:10.1016/j.ctrv.2015.11.007
22. Freytag M, Herrlinger U, Hauser S, et al. Higher number of multidisciplinary tumor board meetings per case leads to improved clinical outcome. BMC Cancer. 2020;20(1):355. Published 2020 Apr 28. doi:10.1186/s12885-020-06809-1
Agent Orange Exposure, Transformation From MGUS to Multiple Myeloma, and Outcomes in Veterans
Multiple myeloma (MM) accounts for 1% to 2% of all cancers and slightly more than 17% of hematologic malignancies in the United States.1 MM is characterized by the neoplastic proliferation of immunoglobulin (Ig)-producing plasma cells with ≥ 10% clonal plasma cells in the bone marrow or biopsy-proven bony or soft tissue plasmacytoma, plus presence of related organ or tissue impairment or presence of a biomarker associated with near-inevitable progression to end-organ damage.2
Background
Up to 97% of patients with MM will have a monoclonal (M) protein produced and secreted by the malignant plasma cells, which can be detected by protein electrophoresis of the serum and an aliquot of urine from a 24-hour collection combined with immunofixation of the serum and urine. The M protein in MM usually consists of IgG 50% of the time and light chains 16% of the time. Patients who lack detectable M protein are considered to have nonsecretory myeloma. MM presents with end-organ damage, which includes hypercalcemia, renal dysfunction, anemia, or lytic bone lesions. Patients with MM frequently present with renal insufficiency due to cast nephropathy or light chain deposition disease.3
MM is thought to evolve from monoclonal gammopathy of uncertain significance (MGUS), an asymptomatic premalignant stage of clonal plasma cell proliferation with a risk of progression to active myeloma at 1% per year.4,5 Epidemiologic data suggest that people who develop MM have a genetic predisposition, but risk factors may develop or be acquired, such as age, immunosuppression, and environmental exposures. To better assess what causes transformation from MGUS to MM, it is important to identify agents that may cause this second hit.6
In November 1961, President John F. Kennedy authorized the start of Operation Ranch Hand, the US Air Force’s herbicide program during the Vietnam War. Twenty million gallons of various chemicals were sprayed in Vietnam, eastern Laos, and parts of Cambodia to defoliate rural land, depriving guerillas of their support base. Agent Orange (AO) was one of these chemicals; it is a mixed herbicide with traces of dioxin, a compound that has been associated with major health problems among exposed individuals.7 Several studies have evaluated exposure to AO and its potential harmful repercussions. Studies have assessed the link between AO and MGUS as well as AO to various leukemias, such as chronic lymphocytic leukemia.8,9 Other studies have shown the relationship between AO exposure and worse outcomes in persons with MM.10 To date, only a single abstract from a US Department of Veterans Affairs (VA) medical center has investigated the relationships between AO exposure and MGUS, MM, and the rate of transformation. The VA study of patients seen from 2005 to 2015 in Detroit, Michigan, found that AO exposure led to an increase in cumulative incidence rate of MGUS/MM, suggesting possible changes in disease biology and genetics.11
In this study, we aimed to determine the incidence of transformation of MGUS to MM in patients with and without exposure to AO. We then analyzed survival as a function of AO exposure, transformation, and clinical and sociodemographic variables. We also explored the impact of psychosocial variables and hematopoietic stem cell transplantation (HSCT), a standard of treatment for MM.
Methods
This retrospective cohort study assembled electronic health record (EHR) data from the Veterans Health Administration Corporate Data Warehouse (CDW). The VA Central Texas Veterans Healthcare System Institutional Review Board granted a waiver of consent for this record review. Eligible patients were Vietnam-era veterans who were in the military during the time that AO was used (1961-1971). Veterans were included if they were being cared for and received a diagnosis for MGUS or MM between October 1, 2009, and September 30, 2015 (all prevalent cases fiscal years 2010-2015). Cases were excluded if there was illogical death data or if age, race, ethnicity, body mass index (BMI), or prior-year diagnostic data were missing.
Measures
Patients were followed through April 2020. Presence of MGUS was defined by the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code 273.1. MM was identified by ICD-9 diagnosis codes 203.00, 203.01, and 203.02. The study index date was the earliest date of diagnosis of MGUS or MM in fiscal years 2010-2015. It was suspected that some patients with MM may have had a history of MGUS prior to this period. Therefore, for patients with MM, historical diagnosis of MGUS was extracted going back through the earliest data in the CDW (October 1999). Patients diagnosed with both MGUS and MM were considered transformation patients.
Other measures included age at index date, sex, race, ethnicity, VA priority status (a value 1 to 8 summarizing why the veteran qualified for VA care, such as military service-connected disability or very low income), and AO exposure authenticated per VA enrollment files and disability records. Service years were separated into 1961 to 1968 and 1969 to 1971 to match a change in the formulation of AO associated with decreased carcinogenic effect. Comorbidity data from the year prior to first MGUS/MM diagnosis in the observation period were extracted. Lifestyle factors associated with development of MGUS/MM were determined using the following codes: obesity per BMI calculation or diagnosis (ICD-9, 278.0), tobacco use per diagnosis (ICD-9, 305.1, V15.82), and survival from MGUS/MM diagnosis index date to date of death from any cause. Comorbidity was assessed using ICD-9 diagnosis codes to calculate the Charlson Comorbidity Index (CCI), which includes cardiovascular diseases, diabetes mellitus, liver and kidney diseases, cancers, and metastatic solid tumors. Cancers were omitted from our adapted CCI to avoid collinearity in the multivariable models. The theoretical maximum CCI score in this study was 25.12,13 Additional conditions known to be associated with variation in outcomes among veterans using the VA were indicated, including major depressive disorder, posttraumatic stress disorder (PTSD), alcohol use disorder (AUD), substance use disorder (SUD), and common chronic disease (hypertension, lipid disorders).14
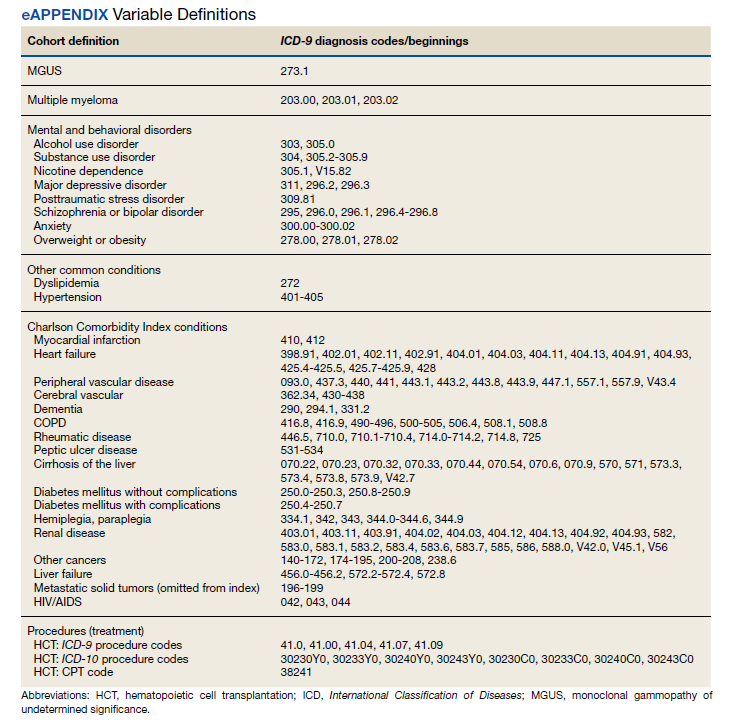
Treatment with autologous HSCT was defined by Current Procedural Terminology and ICD-9 Clinical Modification procedure codes for bone marrow and autologous HSCT occurring at any time in the CDW (eAppendix). Days elapsed from MM diagnosis to HSCT were calculated.
Statistical Analysis
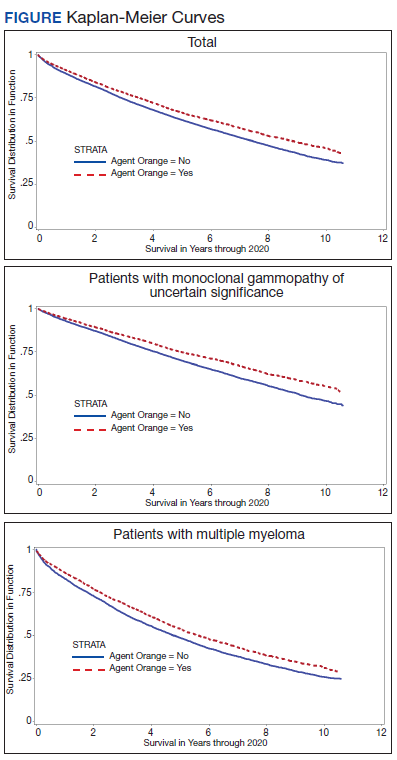
Sample characteristics were represented by frequencies and percentages for categorical variables and means and SDs (or medians and ranges where appropriate) for continuous variables. A χ2 test (or Fisher exact test when cell counts were low) assessed associations in bivariate comparisons. A 2-sample t test (or Wilcoxon rank sum test as appropriate) assessed differences in continuous variables between 2 groups. Kaplan-Meier curves depicted the unadjusted relationship of AO exposure to survival. Cox proportional hazards survival models examined an unadjusted model containing only the AO exposure indicator as a predictor and adjusted models were used for demographic and clinical factors for MGUS and patients with MM separately.
Predictors were age in decades, sex, Hispanic ethnicity, race, nicotine dependence, obesity, overweight, AUD, SUD, major depressive disorder, PTSD, and the adapted CCI. When modeling patients with MM, MGUS was added to the model to identify the transformation group. The interaction of AO with transformation was also analyzed for patients with MM. Results were reported as hazard ratios (HR) with their 95% CI.
Results
We identified 18,215 veterans diagnosed with either MGUS or MM during fiscal years 2010-2015 with 16,366 meeting inclusion criteria. Patients were excluded for missing data on exposure (n = 334), age (n = 12), race (n = 1058), ethnicity (n = 164), diagnosis (n = 47), treatment (n = 56), and BMI (n = 178). All were Vietnam War era veterans; 14 also served in other eras.
The cohort was 98.5% male (Table 1). Twenty-nine percent were Black veterans, 65% were White veterans, and 4% of individuals reported Hispanic ethnicity. Patients had a mean (SD) age of 66.7 (5.9) years (range, 52-96). Most patients were married (58%) or divorced/separated (27%). All were VA priority 1 to 5 (no 6, 7, or 8); 50% were priority 1 with 50% to 100% service-connected disability. Another 29% were eligible for VA care by reason of low income, 17% had 10% to 40% service-connected disability, and 4% were otherwise disabled.
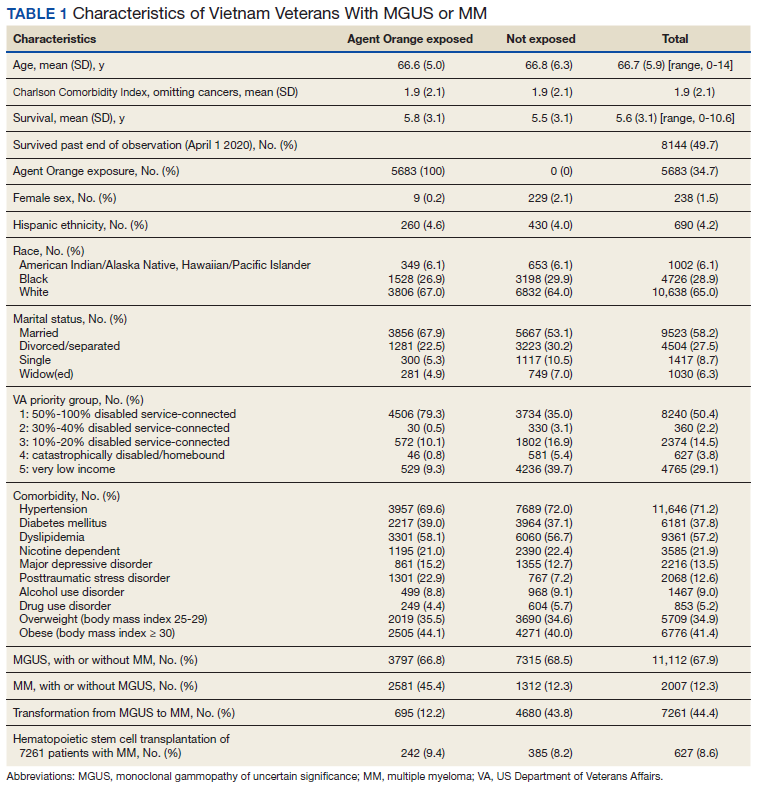
During fiscal years 2010 to 2015, 68% of our cohort had a diagnosis of MGUS (n = 11,112; 9105 had MGUS only), 44% had MM (n = 7261; 5254 had MM only), and 12% of these were transformation patients (n = 2007). AO exposure characterized 3102 MGUS-only patients (34%), 1886 MM-only patients (36%), and 695 transformation patients (35%) (χ2 = 4.92, P = .09). Among 5683 AO-exposed patients, 695 (12.2%) underwent MGUS-to-MM transformation. Among 10,683 nonexposed veterans, 1312 (12.3%) experienced transformation.
Comorbidity in the year leading up to the index MGUS/MM date determined using CCI was a mean (SD) of 1.9 (2.1) (range, 0-14). Among disorders not included in the CCI, 71% were diagnosed with hypertension, 57% with lipid disorders, 22% with nicotine dependence, 14% with major depressive disorder, 13% with PTSD, and 9% with AUD. Overweight (BMI 25 to < 30) and obesity (BMI ≥ 30) were common (35% and 41%, respectively). For 98% of patients, weight was measured within 90 days of their index MGUS/MM date. Most of the cohort (70%) were in Vietnam in 1961 to 1968.
HSCT was provided to 632 patients with MM (8.7%), including 441 patients who were treated after their index date and 219 patients treated before their index date. From fiscal years 2010 to 2015, the median (IQR) number of days from MM index date to HSCT receipt was 349 (243-650) days. Historical HSCT occurred a median (IQR) of 857 (353-1592) days before the index date, per data available back to October 1999; this median suggests long histories of MM in this cohort.
The unadjusted survival model found a very small inverse association of mortality with AO exposure in the total sample, meaning patients with documented AO exposure lived longer (HR, 0.85; 95% CI, 0.81-0.89; Table 2; Figure). Among 11,112 MGUS patients, AO was similarly associated with mortality (HR, 0.79; 95% CI, 0.74-0.84). The effect was also seen among 7269 patients with MM (HR, 0.86; 95% CI, 0.81-0.91).
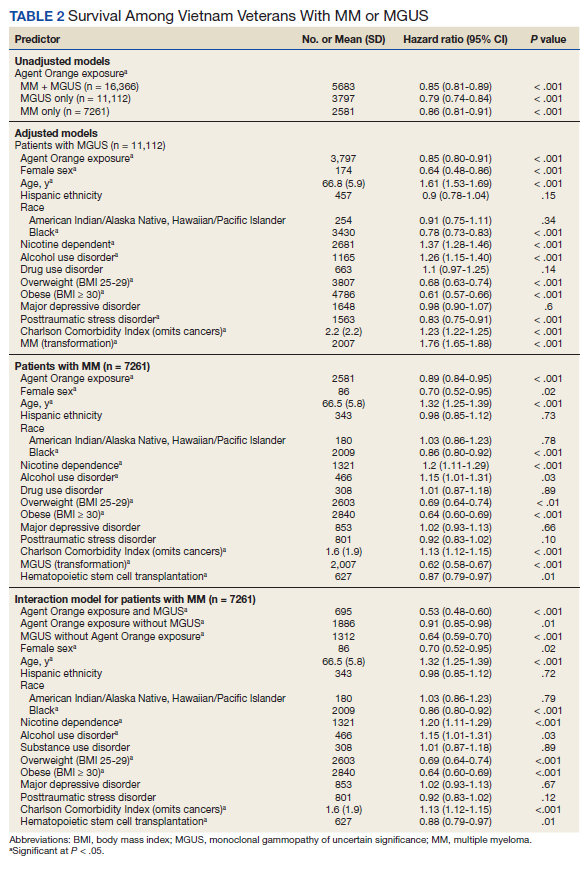
In the adjusted model of the total sample, the mortality hazard was greater for veterans who were older, with AUD and nicotine dependence, greater comorbidity per the CCI, diagnosis of MM, and transformation from MGUS to MM. Protective effects were noted for AO exposure, female sex, Black race, obesity, overweight, PTSD, and HSCT.
After adjusting for covariates, AO exposure was still associated with lower mortality among 11,112 patients with MGUS (HR, 0.85; 95% CI, 0.80-0.91). Risk factors were older age, nicotine dependence, AUD, the adapted CCI score (HR, 1.23 per point increase in the index; 95% CI, 1.22-1.25), and transformation to MM (HR, 1.76; 95% CI, 1.65-1.88). Additional protective factors were female sex, Black race, obesity, overweight, and PTSD.
After adjusting for covariates and limiting the analytic cohort to MM patients, the effect of AO exposure persisted (HR, 0.89; 95% CI, 0.84-0.95). Mortality risk factors were older age, nicotine dependence, AUD, and higher CCI score. Also protective were female sex, Black race, obesity, overweight, diagnosis of MGUS (transformation), and HSCT.
In the final model on patients with MM, the interaction term of AO exposure with transformation was significant. The combination of AO exposure with MGUS transformation had a greater protective effect than either AO exposure alone or MGUS without prior AO exposure. Additional protective factors were female sex, Black race, obesity, overweight, and HSCT. Older age, AUD, nicotine dependence, and greater comorbidity increased mortality risk.
Disscussion
Elucidating the pathophysiology and risk of transformation from MGUS to MM is an ongoing endeavor, even 35 years after the end of US involvement in the Vietnam War. Our study sought to understand a relationship between AO exposure, risk of MGUS transforming to MM, and associated mortality in US Vietnam War veterans. The rate of transformation (MGUS progressing to active MM) is well cited at 1% per year.15 Here, we found 12% of our cohort had undergone this transformation over 10 years.
Vietnam War era veterans who were exposed to AO during the Operation Ranch Hand period had 2.4 times greater risk of developing MGUS compared with veterans not exposed to AO.8 Our study was not designed to look at this association of AO exposure and MGUS/MM as this was a retrospective review to assess the difference in outcomes based on AO exposure. We found that AO exposure is associated with a decrease in mortality in contrast to a prior study showing worse survival with individuals with AO exposure.10 Another single center study found no association between AO exposure and overall survival, but it did identify an increased risk of progression from MGUS to MM.11 Our study did not show increased risk of transformation but did show positive effect on survival.
Black individuals have twice the risk of developing MM compared with White individuals and are diagnosed at a younger age (66 vs 70 years, respectively).16 Interestingly, Black race was a protective factor in our study. Given the length of time (35 years) elapsed since the Vietnam War ended, it is likely that most vulnerable Black veterans did not survive until our observation period.
HSCT, as expected, was a protective factor for veterans undergoing this treatment modality, but it is unclear why such a small number (8%) underwent HSCT as this is a standard of care in the management of MM. Obesity was also found to be a protective factor in a prior study, which was also seen in our study cohort.8
Limitations
This study was limited by its retrospective review of survivors among the Vietnam-era cohort several decades after the exposure of concern. Clinician notes and full historical data, such as date of onset for any disorder, were unavailable. These data also relied on the practitioners caring for the veterans to make the correct diagnosis with the associated code so that the data could be captured. Neither AO exposure nor diagnoses codes were verified against other sources of data; however, validation studies over the years have supported the accuracy of the diagnosis codes recorded in the VA EHR.
Conclusions
Because AO exposure is a nonmodifiable risk factor, focus should be placed on modifiable risk factors (eg, nicotine dependence, alcohol and substance use disorders, underlying comorbid conditions) as these were associated with worse outcomes. Future studies will look at the correlation of AO exposure, cytogenetics, and clinical outcomes in these veterans to learn how best to identify their disease course and optimize their care in the latter part of their life.
Acknowledgments
This research was supported by the Central Texas Veterans Health Care System and Baylor Scott and White Health, both in Temple and Veterans Affairs Central Western Massachusetts Healthcare System, Leeds.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30. doi:10.3322/caac.21442
2. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-e548. doi:10.1016/S1470-2045(14)70442-5
3. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. doi:10.4065/78.1.21
4. Kyle RA, Therneau TM, Rajkumar SV, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med. 2002;346(8):564- 569. doi:10.1056/NEJMoa01133202
5. International Myeloma Foundation. What Are MGUS, smoldering and active myeloma? Updated June 6, 2021. Accessed June 20, 2022. https://www.myeloma .org/what-are-mgus-smm-mm
6. Riedel DA, Pottern LM. The epidemiology of multiple myeloma. Hematol Oncol Clin North Am. 1992;6(2):225-247. doi:10.1016/S0889-8588(18)30341-1
7. Buckingham Jr WA. Operation Ranch Hand: The Air Force and herbicides in southeast Asia, 1961-1971. Washington, DC: Office of Air Force History, United States Air Force; 1982. Accessed June 20, 2022. https://apps.dtic.mil/sti /pdfs/ADA121709.pdf
8. Landgren O, Shim YK, Michalek J, et al. Agent Orange exposure and monoclonal gammopathy of undetermined significance: an Operation Ranch Hand veteran cohort study. JAMA Oncol. 2015;1(8):1061-1068. doi:10.1001/jamaoncol.2015.2938
9. Mescher C, Gilbertson D, Randall NM, et al. The impact of Agent Orange exposure on prognosis and management in patients with chronic lymphocytic leukemia: a National Veteran Affairs Tumor Registry Study. Leuk Lymphoma. 2018;59(6):1348-1355. doi:10.1080/10428194.2017.1375109
10. Callander NS, Freytes CO, Luo S, Carson KR. Previous Agent Orange exposure is correlated with worse outcome in patients with multiple myeloma (MM) [abstract]. Blood. 2015;126(23):4194. doi:10.1182/blood.V126.23.4194.4194
11. Bumma N, Nagasaka M, Kim S, Vankayala HM, Ahmed S, Jasti P. Incidence of monoclonal gammopathy of undetermined significance (MGUS) and subsequent transformation to multiple myeloma (MM) and effect of exposure to Agent Orange (AO): a single center experience from VA Detroit [abstract]. Blood. 2017;130(suppl 1):5383. doi:10.1182/blood.V130.Suppl_1.5383.5383
12. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. doi:10.1016/0021-9681(87)90171-8
13. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. doi:10.1016/0895-4356(92)90133-8
14. Copeland LA, Zeber JE, Sako EY, et al. Serious mental illnesses associated with receipt of surgery in retrospective analysis of patients in the Veterans Health Administration. BMC Surg. 2015;15:74. doi:10.1186/s12893-015-0064-7
15. Younes MA, Perez JD, Alirhayim Z, Ochoa C, Patel R, Dabak VS. MGUS Transformation into multiple myeloma in patients with solid organ transplantation [Abstract presented at American Society of Hematology Annual Meeting, November 15, 2013]. Blood. 2013;122(21):5325. doi:10.1182/blood.V122.21.5325.5325
16. Waxman AJ, Mink PJ, Devesa SS, et al. Racial disparities in incidence and outcome in multiple myeloma: a population- based study. Blood. 2010 Dec 16;116(25):5501-5506. doi:10.1182/blood-2010-07-298760
Multiple myeloma (MM) accounts for 1% to 2% of all cancers and slightly more than 17% of hematologic malignancies in the United States.1 MM is characterized by the neoplastic proliferation of immunoglobulin (Ig)-producing plasma cells with ≥ 10% clonal plasma cells in the bone marrow or biopsy-proven bony or soft tissue plasmacytoma, plus presence of related organ or tissue impairment or presence of a biomarker associated with near-inevitable progression to end-organ damage.2
Background
Up to 97% of patients with MM will have a monoclonal (M) protein produced and secreted by the malignant plasma cells, which can be detected by protein electrophoresis of the serum and an aliquot of urine from a 24-hour collection combined with immunofixation of the serum and urine. The M protein in MM usually consists of IgG 50% of the time and light chains 16% of the time. Patients who lack detectable M protein are considered to have nonsecretory myeloma. MM presents with end-organ damage, which includes hypercalcemia, renal dysfunction, anemia, or lytic bone lesions. Patients with MM frequently present with renal insufficiency due to cast nephropathy or light chain deposition disease.3
MM is thought to evolve from monoclonal gammopathy of uncertain significance (MGUS), an asymptomatic premalignant stage of clonal plasma cell proliferation with a risk of progression to active myeloma at 1% per year.4,5 Epidemiologic data suggest that people who develop MM have a genetic predisposition, but risk factors may develop or be acquired, such as age, immunosuppression, and environmental exposures. To better assess what causes transformation from MGUS to MM, it is important to identify agents that may cause this second hit.6
In November 1961, President John F. Kennedy authorized the start of Operation Ranch Hand, the US Air Force’s herbicide program during the Vietnam War. Twenty million gallons of various chemicals were sprayed in Vietnam, eastern Laos, and parts of Cambodia to defoliate rural land, depriving guerillas of their support base. Agent Orange (AO) was one of these chemicals; it is a mixed herbicide with traces of dioxin, a compound that has been associated with major health problems among exposed individuals.7 Several studies have evaluated exposure to AO and its potential harmful repercussions. Studies have assessed the link between AO and MGUS as well as AO to various leukemias, such as chronic lymphocytic leukemia.8,9 Other studies have shown the relationship between AO exposure and worse outcomes in persons with MM.10 To date, only a single abstract from a US Department of Veterans Affairs (VA) medical center has investigated the relationships between AO exposure and MGUS, MM, and the rate of transformation. The VA study of patients seen from 2005 to 2015 in Detroit, Michigan, found that AO exposure led to an increase in cumulative incidence rate of MGUS/MM, suggesting possible changes in disease biology and genetics.11
In this study, we aimed to determine the incidence of transformation of MGUS to MM in patients with and without exposure to AO. We then analyzed survival as a function of AO exposure, transformation, and clinical and sociodemographic variables. We also explored the impact of psychosocial variables and hematopoietic stem cell transplantation (HSCT), a standard of treatment for MM.
Methods
This retrospective cohort study assembled electronic health record (EHR) data from the Veterans Health Administration Corporate Data Warehouse (CDW). The VA Central Texas Veterans Healthcare System Institutional Review Board granted a waiver of consent for this record review. Eligible patients were Vietnam-era veterans who were in the military during the time that AO was used (1961-1971). Veterans were included if they were being cared for and received a diagnosis for MGUS or MM between October 1, 2009, and September 30, 2015 (all prevalent cases fiscal years 2010-2015). Cases were excluded if there was illogical death data or if age, race, ethnicity, body mass index (BMI), or prior-year diagnostic data were missing.
Measures
Patients were followed through April 2020. Presence of MGUS was defined by the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code 273.1. MM was identified by ICD-9 diagnosis codes 203.00, 203.01, and 203.02. The study index date was the earliest date of diagnosis of MGUS or MM in fiscal years 2010-2015. It was suspected that some patients with MM may have had a history of MGUS prior to this period. Therefore, for patients with MM, historical diagnosis of MGUS was extracted going back through the earliest data in the CDW (October 1999). Patients diagnosed with both MGUS and MM were considered transformation patients.
Other measures included age at index date, sex, race, ethnicity, VA priority status (a value 1 to 8 summarizing why the veteran qualified for VA care, such as military service-connected disability or very low income), and AO exposure authenticated per VA enrollment files and disability records. Service years were separated into 1961 to 1968 and 1969 to 1971 to match a change in the formulation of AO associated with decreased carcinogenic effect. Comorbidity data from the year prior to first MGUS/MM diagnosis in the observation period were extracted. Lifestyle factors associated with development of MGUS/MM were determined using the following codes: obesity per BMI calculation or diagnosis (ICD-9, 278.0), tobacco use per diagnosis (ICD-9, 305.1, V15.82), and survival from MGUS/MM diagnosis index date to date of death from any cause. Comorbidity was assessed using ICD-9 diagnosis codes to calculate the Charlson Comorbidity Index (CCI), which includes cardiovascular diseases, diabetes mellitus, liver and kidney diseases, cancers, and metastatic solid tumors. Cancers were omitted from our adapted CCI to avoid collinearity in the multivariable models. The theoretical maximum CCI score in this study was 25.12,13 Additional conditions known to be associated with variation in outcomes among veterans using the VA were indicated, including major depressive disorder, posttraumatic stress disorder (PTSD), alcohol use disorder (AUD), substance use disorder (SUD), and common chronic disease (hypertension, lipid disorders).14
Treatment with autologous HSCT was defined by Current Procedural Terminology and ICD-9 Clinical Modification procedure codes for bone marrow and autologous HSCT occurring at any time in the CDW (eAppendix). Days elapsed from MM diagnosis to HSCT were calculated.
Statistical Analysis
Sample characteristics were represented by frequencies and percentages for categorical variables and means and SDs (or medians and ranges where appropriate) for continuous variables. A χ2 test (or Fisher exact test when cell counts were low) assessed associations in bivariate comparisons. A 2-sample t test (or Wilcoxon rank sum test as appropriate) assessed differences in continuous variables between 2 groups. Kaplan-Meier curves depicted the unadjusted relationship of AO exposure to survival. Cox proportional hazards survival models examined an unadjusted model containing only the AO exposure indicator as a predictor and adjusted models were used for demographic and clinical factors for MGUS and patients with MM separately.
Predictors were age in decades, sex, Hispanic ethnicity, race, nicotine dependence, obesity, overweight, AUD, SUD, major depressive disorder, PTSD, and the adapted CCI. When modeling patients with MM, MGUS was added to the model to identify the transformation group. The interaction of AO with transformation was also analyzed for patients with MM. Results were reported as hazard ratios (HR) with their 95% CI.
Results
We identified 18,215 veterans diagnosed with either MGUS or MM during fiscal years 2010-2015 with 16,366 meeting inclusion criteria. Patients were excluded for missing data on exposure (n = 334), age (n = 12), race (n = 1058), ethnicity (n = 164), diagnosis (n = 47), treatment (n = 56), and BMI (n = 178). All were Vietnam War era veterans; 14 also served in other eras.
The cohort was 98.5% male (Table 1). Twenty-nine percent were Black veterans, 65% were White veterans, and 4% of individuals reported Hispanic ethnicity. Patients had a mean (SD) age of 66.7 (5.9) years (range, 52-96). Most patients were married (58%) or divorced/separated (27%). All were VA priority 1 to 5 (no 6, 7, or 8); 50% were priority 1 with 50% to 100% service-connected disability. Another 29% were eligible for VA care by reason of low income, 17% had 10% to 40% service-connected disability, and 4% were otherwise disabled.
During fiscal years 2010 to 2015, 68% of our cohort had a diagnosis of MGUS (n = 11,112; 9105 had MGUS only), 44% had MM (n = 7261; 5254 had MM only), and 12% of these were transformation patients (n = 2007). AO exposure characterized 3102 MGUS-only patients (34%), 1886 MM-only patients (36%), and 695 transformation patients (35%) (χ2 = 4.92, P = .09). Among 5683 AO-exposed patients, 695 (12.2%) underwent MGUS-to-MM transformation. Among 10,683 nonexposed veterans, 1312 (12.3%) experienced transformation.
Comorbidity in the year leading up to the index MGUS/MM date determined using CCI was a mean (SD) of 1.9 (2.1) (range, 0-14). Among disorders not included in the CCI, 71% were diagnosed with hypertension, 57% with lipid disorders, 22% with nicotine dependence, 14% with major depressive disorder, 13% with PTSD, and 9% with AUD. Overweight (BMI 25 to < 30) and obesity (BMI ≥ 30) were common (35% and 41%, respectively). For 98% of patients, weight was measured within 90 days of their index MGUS/MM date. Most of the cohort (70%) were in Vietnam in 1961 to 1968.
HSCT was provided to 632 patients with MM (8.7%), including 441 patients who were treated after their index date and 219 patients treated before their index date. From fiscal years 2010 to 2015, the median (IQR) number of days from MM index date to HSCT receipt was 349 (243-650) days. Historical HSCT occurred a median (IQR) of 857 (353-1592) days before the index date, per data available back to October 1999; this median suggests long histories of MM in this cohort.
The unadjusted survival model found a very small inverse association of mortality with AO exposure in the total sample, meaning patients with documented AO exposure lived longer (HR, 0.85; 95% CI, 0.81-0.89; Table 2; Figure). Among 11,112 MGUS patients, AO was similarly associated with mortality (HR, 0.79; 95% CI, 0.74-0.84). The effect was also seen among 7269 patients with MM (HR, 0.86; 95% CI, 0.81-0.91).
In the adjusted model of the total sample, the mortality hazard was greater for veterans who were older, with AUD and nicotine dependence, greater comorbidity per the CCI, diagnosis of MM, and transformation from MGUS to MM. Protective effects were noted for AO exposure, female sex, Black race, obesity, overweight, PTSD, and HSCT.
After adjusting for covariates, AO exposure was still associated with lower mortality among 11,112 patients with MGUS (HR, 0.85; 95% CI, 0.80-0.91). Risk factors were older age, nicotine dependence, AUD, the adapted CCI score (HR, 1.23 per point increase in the index; 95% CI, 1.22-1.25), and transformation to MM (HR, 1.76; 95% CI, 1.65-1.88). Additional protective factors were female sex, Black race, obesity, overweight, and PTSD.
After adjusting for covariates and limiting the analytic cohort to MM patients, the effect of AO exposure persisted (HR, 0.89; 95% CI, 0.84-0.95). Mortality risk factors were older age, nicotine dependence, AUD, and higher CCI score. Also protective were female sex, Black race, obesity, overweight, diagnosis of MGUS (transformation), and HSCT.
In the final model on patients with MM, the interaction term of AO exposure with transformation was significant. The combination of AO exposure with MGUS transformation had a greater protective effect than either AO exposure alone or MGUS without prior AO exposure. Additional protective factors were female sex, Black race, obesity, overweight, and HSCT. Older age, AUD, nicotine dependence, and greater comorbidity increased mortality risk.
Disscussion
Elucidating the pathophysiology and risk of transformation from MGUS to MM is an ongoing endeavor, even 35 years after the end of US involvement in the Vietnam War. Our study sought to understand a relationship between AO exposure, risk of MGUS transforming to MM, and associated mortality in US Vietnam War veterans. The rate of transformation (MGUS progressing to active MM) is well cited at 1% per year.15 Here, we found 12% of our cohort had undergone this transformation over 10 years.
Vietnam War era veterans who were exposed to AO during the Operation Ranch Hand period had 2.4 times greater risk of developing MGUS compared with veterans not exposed to AO.8 Our study was not designed to look at this association of AO exposure and MGUS/MM as this was a retrospective review to assess the difference in outcomes based on AO exposure. We found that AO exposure is associated with a decrease in mortality in contrast to a prior study showing worse survival with individuals with AO exposure.10 Another single center study found no association between AO exposure and overall survival, but it did identify an increased risk of progression from MGUS to MM.11 Our study did not show increased risk of transformation but did show positive effect on survival.
Black individuals have twice the risk of developing MM compared with White individuals and are diagnosed at a younger age (66 vs 70 years, respectively).16 Interestingly, Black race was a protective factor in our study. Given the length of time (35 years) elapsed since the Vietnam War ended, it is likely that most vulnerable Black veterans did not survive until our observation period.
HSCT, as expected, was a protective factor for veterans undergoing this treatment modality, but it is unclear why such a small number (8%) underwent HSCT as this is a standard of care in the management of MM. Obesity was also found to be a protective factor in a prior study, which was also seen in our study cohort.8
Limitations
This study was limited by its retrospective review of survivors among the Vietnam-era cohort several decades after the exposure of concern. Clinician notes and full historical data, such as date of onset for any disorder, were unavailable. These data also relied on the practitioners caring for the veterans to make the correct diagnosis with the associated code so that the data could be captured. Neither AO exposure nor diagnoses codes were verified against other sources of data; however, validation studies over the years have supported the accuracy of the diagnosis codes recorded in the VA EHR.
Conclusions
Because AO exposure is a nonmodifiable risk factor, focus should be placed on modifiable risk factors (eg, nicotine dependence, alcohol and substance use disorders, underlying comorbid conditions) as these were associated with worse outcomes. Future studies will look at the correlation of AO exposure, cytogenetics, and clinical outcomes in these veterans to learn how best to identify their disease course and optimize their care in the latter part of their life.
Acknowledgments
This research was supported by the Central Texas Veterans Health Care System and Baylor Scott and White Health, both in Temple and Veterans Affairs Central Western Massachusetts Healthcare System, Leeds.
Multiple myeloma (MM) accounts for 1% to 2% of all cancers and slightly more than 17% of hematologic malignancies in the United States.1 MM is characterized by the neoplastic proliferation of immunoglobulin (Ig)-producing plasma cells with ≥ 10% clonal plasma cells in the bone marrow or biopsy-proven bony or soft tissue plasmacytoma, plus presence of related organ or tissue impairment or presence of a biomarker associated with near-inevitable progression to end-organ damage.2
Background
Up to 97% of patients with MM will have a monoclonal (M) protein produced and secreted by the malignant plasma cells, which can be detected by protein electrophoresis of the serum and an aliquot of urine from a 24-hour collection combined with immunofixation of the serum and urine. The M protein in MM usually consists of IgG 50% of the time and light chains 16% of the time. Patients who lack detectable M protein are considered to have nonsecretory myeloma. MM presents with end-organ damage, which includes hypercalcemia, renal dysfunction, anemia, or lytic bone lesions. Patients with MM frequently present with renal insufficiency due to cast nephropathy or light chain deposition disease.3
MM is thought to evolve from monoclonal gammopathy of uncertain significance (MGUS), an asymptomatic premalignant stage of clonal plasma cell proliferation with a risk of progression to active myeloma at 1% per year.4,5 Epidemiologic data suggest that people who develop MM have a genetic predisposition, but risk factors may develop or be acquired, such as age, immunosuppression, and environmental exposures. To better assess what causes transformation from MGUS to MM, it is important to identify agents that may cause this second hit.6
In November 1961, President John F. Kennedy authorized the start of Operation Ranch Hand, the US Air Force’s herbicide program during the Vietnam War. Twenty million gallons of various chemicals were sprayed in Vietnam, eastern Laos, and parts of Cambodia to defoliate rural land, depriving guerillas of their support base. Agent Orange (AO) was one of these chemicals; it is a mixed herbicide with traces of dioxin, a compound that has been associated with major health problems among exposed individuals.7 Several studies have evaluated exposure to AO and its potential harmful repercussions. Studies have assessed the link between AO and MGUS as well as AO to various leukemias, such as chronic lymphocytic leukemia.8,9 Other studies have shown the relationship between AO exposure and worse outcomes in persons with MM.10 To date, only a single abstract from a US Department of Veterans Affairs (VA) medical center has investigated the relationships between AO exposure and MGUS, MM, and the rate of transformation. The VA study of patients seen from 2005 to 2015 in Detroit, Michigan, found that AO exposure led to an increase in cumulative incidence rate of MGUS/MM, suggesting possible changes in disease biology and genetics.11
In this study, we aimed to determine the incidence of transformation of MGUS to MM in patients with and without exposure to AO. We then analyzed survival as a function of AO exposure, transformation, and clinical and sociodemographic variables. We also explored the impact of psychosocial variables and hematopoietic stem cell transplantation (HSCT), a standard of treatment for MM.
Methods
This retrospective cohort study assembled electronic health record (EHR) data from the Veterans Health Administration Corporate Data Warehouse (CDW). The VA Central Texas Veterans Healthcare System Institutional Review Board granted a waiver of consent for this record review. Eligible patients were Vietnam-era veterans who were in the military during the time that AO was used (1961-1971). Veterans were included if they were being cared for and received a diagnosis for MGUS or MM between October 1, 2009, and September 30, 2015 (all prevalent cases fiscal years 2010-2015). Cases were excluded if there was illogical death data or if age, race, ethnicity, body mass index (BMI), or prior-year diagnostic data were missing.
Measures
Patients were followed through April 2020. Presence of MGUS was defined by the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code 273.1. MM was identified by ICD-9 diagnosis codes 203.00, 203.01, and 203.02. The study index date was the earliest date of diagnosis of MGUS or MM in fiscal years 2010-2015. It was suspected that some patients with MM may have had a history of MGUS prior to this period. Therefore, for patients with MM, historical diagnosis of MGUS was extracted going back through the earliest data in the CDW (October 1999). Patients diagnosed with both MGUS and MM were considered transformation patients.
Other measures included age at index date, sex, race, ethnicity, VA priority status (a value 1 to 8 summarizing why the veteran qualified for VA care, such as military service-connected disability or very low income), and AO exposure authenticated per VA enrollment files and disability records. Service years were separated into 1961 to 1968 and 1969 to 1971 to match a change in the formulation of AO associated with decreased carcinogenic effect. Comorbidity data from the year prior to first MGUS/MM diagnosis in the observation period were extracted. Lifestyle factors associated with development of MGUS/MM were determined using the following codes: obesity per BMI calculation or diagnosis (ICD-9, 278.0), tobacco use per diagnosis (ICD-9, 305.1, V15.82), and survival from MGUS/MM diagnosis index date to date of death from any cause. Comorbidity was assessed using ICD-9 diagnosis codes to calculate the Charlson Comorbidity Index (CCI), which includes cardiovascular diseases, diabetes mellitus, liver and kidney diseases, cancers, and metastatic solid tumors. Cancers were omitted from our adapted CCI to avoid collinearity in the multivariable models. The theoretical maximum CCI score in this study was 25.12,13 Additional conditions known to be associated with variation in outcomes among veterans using the VA were indicated, including major depressive disorder, posttraumatic stress disorder (PTSD), alcohol use disorder (AUD), substance use disorder (SUD), and common chronic disease (hypertension, lipid disorders).14
Treatment with autologous HSCT was defined by Current Procedural Terminology and ICD-9 Clinical Modification procedure codes for bone marrow and autologous HSCT occurring at any time in the CDW (eAppendix). Days elapsed from MM diagnosis to HSCT were calculated.
Statistical Analysis
Sample characteristics were represented by frequencies and percentages for categorical variables and means and SDs (or medians and ranges where appropriate) for continuous variables. A χ2 test (or Fisher exact test when cell counts were low) assessed associations in bivariate comparisons. A 2-sample t test (or Wilcoxon rank sum test as appropriate) assessed differences in continuous variables between 2 groups. Kaplan-Meier curves depicted the unadjusted relationship of AO exposure to survival. Cox proportional hazards survival models examined an unadjusted model containing only the AO exposure indicator as a predictor and adjusted models were used for demographic and clinical factors for MGUS and patients with MM separately.
Predictors were age in decades, sex, Hispanic ethnicity, race, nicotine dependence, obesity, overweight, AUD, SUD, major depressive disorder, PTSD, and the adapted CCI. When modeling patients with MM, MGUS was added to the model to identify the transformation group. The interaction of AO with transformation was also analyzed for patients with MM. Results were reported as hazard ratios (HR) with their 95% CI.
Results
We identified 18,215 veterans diagnosed with either MGUS or MM during fiscal years 2010-2015 with 16,366 meeting inclusion criteria. Patients were excluded for missing data on exposure (n = 334), age (n = 12), race (n = 1058), ethnicity (n = 164), diagnosis (n = 47), treatment (n = 56), and BMI (n = 178). All were Vietnam War era veterans; 14 also served in other eras.
The cohort was 98.5% male (Table 1). Twenty-nine percent were Black veterans, 65% were White veterans, and 4% of individuals reported Hispanic ethnicity. Patients had a mean (SD) age of 66.7 (5.9) years (range, 52-96). Most patients were married (58%) or divorced/separated (27%). All were VA priority 1 to 5 (no 6, 7, or 8); 50% were priority 1 with 50% to 100% service-connected disability. Another 29% were eligible for VA care by reason of low income, 17% had 10% to 40% service-connected disability, and 4% were otherwise disabled.
During fiscal years 2010 to 2015, 68% of our cohort had a diagnosis of MGUS (n = 11,112; 9105 had MGUS only), 44% had MM (n = 7261; 5254 had MM only), and 12% of these were transformation patients (n = 2007). AO exposure characterized 3102 MGUS-only patients (34%), 1886 MM-only patients (36%), and 695 transformation patients (35%) (χ2 = 4.92, P = .09). Among 5683 AO-exposed patients, 695 (12.2%) underwent MGUS-to-MM transformation. Among 10,683 nonexposed veterans, 1312 (12.3%) experienced transformation.
Comorbidity in the year leading up to the index MGUS/MM date determined using CCI was a mean (SD) of 1.9 (2.1) (range, 0-14). Among disorders not included in the CCI, 71% were diagnosed with hypertension, 57% with lipid disorders, 22% with nicotine dependence, 14% with major depressive disorder, 13% with PTSD, and 9% with AUD. Overweight (BMI 25 to < 30) and obesity (BMI ≥ 30) were common (35% and 41%, respectively). For 98% of patients, weight was measured within 90 days of their index MGUS/MM date. Most of the cohort (70%) were in Vietnam in 1961 to 1968.
HSCT was provided to 632 patients with MM (8.7%), including 441 patients who were treated after their index date and 219 patients treated before their index date. From fiscal years 2010 to 2015, the median (IQR) number of days from MM index date to HSCT receipt was 349 (243-650) days. Historical HSCT occurred a median (IQR) of 857 (353-1592) days before the index date, per data available back to October 1999; this median suggests long histories of MM in this cohort.
The unadjusted survival model found a very small inverse association of mortality with AO exposure in the total sample, meaning patients with documented AO exposure lived longer (HR, 0.85; 95% CI, 0.81-0.89; Table 2; Figure). Among 11,112 MGUS patients, AO was similarly associated with mortality (HR, 0.79; 95% CI, 0.74-0.84). The effect was also seen among 7269 patients with MM (HR, 0.86; 95% CI, 0.81-0.91).
In the adjusted model of the total sample, the mortality hazard was greater for veterans who were older, with AUD and nicotine dependence, greater comorbidity per the CCI, diagnosis of MM, and transformation from MGUS to MM. Protective effects were noted for AO exposure, female sex, Black race, obesity, overweight, PTSD, and HSCT.
After adjusting for covariates, AO exposure was still associated with lower mortality among 11,112 patients with MGUS (HR, 0.85; 95% CI, 0.80-0.91). Risk factors were older age, nicotine dependence, AUD, the adapted CCI score (HR, 1.23 per point increase in the index; 95% CI, 1.22-1.25), and transformation to MM (HR, 1.76; 95% CI, 1.65-1.88). Additional protective factors were female sex, Black race, obesity, overweight, and PTSD.
After adjusting for covariates and limiting the analytic cohort to MM patients, the effect of AO exposure persisted (HR, 0.89; 95% CI, 0.84-0.95). Mortality risk factors were older age, nicotine dependence, AUD, and higher CCI score. Also protective were female sex, Black race, obesity, overweight, diagnosis of MGUS (transformation), and HSCT.
In the final model on patients with MM, the interaction term of AO exposure with transformation was significant. The combination of AO exposure with MGUS transformation had a greater protective effect than either AO exposure alone or MGUS without prior AO exposure. Additional protective factors were female sex, Black race, obesity, overweight, and HSCT. Older age, AUD, nicotine dependence, and greater comorbidity increased mortality risk.
Disscussion
Elucidating the pathophysiology and risk of transformation from MGUS to MM is an ongoing endeavor, even 35 years after the end of US involvement in the Vietnam War. Our study sought to understand a relationship between AO exposure, risk of MGUS transforming to MM, and associated mortality in US Vietnam War veterans. The rate of transformation (MGUS progressing to active MM) is well cited at 1% per year.15 Here, we found 12% of our cohort had undergone this transformation over 10 years.
Vietnam War era veterans who were exposed to AO during the Operation Ranch Hand period had 2.4 times greater risk of developing MGUS compared with veterans not exposed to AO.8 Our study was not designed to look at this association of AO exposure and MGUS/MM as this was a retrospective review to assess the difference in outcomes based on AO exposure. We found that AO exposure is associated with a decrease in mortality in contrast to a prior study showing worse survival with individuals with AO exposure.10 Another single center study found no association between AO exposure and overall survival, but it did identify an increased risk of progression from MGUS to MM.11 Our study did not show increased risk of transformation but did show positive effect on survival.
Black individuals have twice the risk of developing MM compared with White individuals and are diagnosed at a younger age (66 vs 70 years, respectively).16 Interestingly, Black race was a protective factor in our study. Given the length of time (35 years) elapsed since the Vietnam War ended, it is likely that most vulnerable Black veterans did not survive until our observation period.
HSCT, as expected, was a protective factor for veterans undergoing this treatment modality, but it is unclear why such a small number (8%) underwent HSCT as this is a standard of care in the management of MM. Obesity was also found to be a protective factor in a prior study, which was also seen in our study cohort.8
Limitations
This study was limited by its retrospective review of survivors among the Vietnam-era cohort several decades after the exposure of concern. Clinician notes and full historical data, such as date of onset for any disorder, were unavailable. These data also relied on the practitioners caring for the veterans to make the correct diagnosis with the associated code so that the data could be captured. Neither AO exposure nor diagnoses codes were verified against other sources of data; however, validation studies over the years have supported the accuracy of the diagnosis codes recorded in the VA EHR.
Conclusions
Because AO exposure is a nonmodifiable risk factor, focus should be placed on modifiable risk factors (eg, nicotine dependence, alcohol and substance use disorders, underlying comorbid conditions) as these were associated with worse outcomes. Future studies will look at the correlation of AO exposure, cytogenetics, and clinical outcomes in these veterans to learn how best to identify their disease course and optimize their care in the latter part of their life.
Acknowledgments
This research was supported by the Central Texas Veterans Health Care System and Baylor Scott and White Health, both in Temple and Veterans Affairs Central Western Massachusetts Healthcare System, Leeds.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30. doi:10.3322/caac.21442
2. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-e548. doi:10.1016/S1470-2045(14)70442-5
3. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. doi:10.4065/78.1.21
4. Kyle RA, Therneau TM, Rajkumar SV, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med. 2002;346(8):564- 569. doi:10.1056/NEJMoa01133202
5. International Myeloma Foundation. What Are MGUS, smoldering and active myeloma? Updated June 6, 2021. Accessed June 20, 2022. https://www.myeloma .org/what-are-mgus-smm-mm
6. Riedel DA, Pottern LM. The epidemiology of multiple myeloma. Hematol Oncol Clin North Am. 1992;6(2):225-247. doi:10.1016/S0889-8588(18)30341-1
7. Buckingham Jr WA. Operation Ranch Hand: The Air Force and herbicides in southeast Asia, 1961-1971. Washington, DC: Office of Air Force History, United States Air Force; 1982. Accessed June 20, 2022. https://apps.dtic.mil/sti /pdfs/ADA121709.pdf
8. Landgren O, Shim YK, Michalek J, et al. Agent Orange exposure and monoclonal gammopathy of undetermined significance: an Operation Ranch Hand veteran cohort study. JAMA Oncol. 2015;1(8):1061-1068. doi:10.1001/jamaoncol.2015.2938
9. Mescher C, Gilbertson D, Randall NM, et al. The impact of Agent Orange exposure on prognosis and management in patients with chronic lymphocytic leukemia: a National Veteran Affairs Tumor Registry Study. Leuk Lymphoma. 2018;59(6):1348-1355. doi:10.1080/10428194.2017.1375109
10. Callander NS, Freytes CO, Luo S, Carson KR. Previous Agent Orange exposure is correlated with worse outcome in patients with multiple myeloma (MM) [abstract]. Blood. 2015;126(23):4194. doi:10.1182/blood.V126.23.4194.4194
11. Bumma N, Nagasaka M, Kim S, Vankayala HM, Ahmed S, Jasti P. Incidence of monoclonal gammopathy of undetermined significance (MGUS) and subsequent transformation to multiple myeloma (MM) and effect of exposure to Agent Orange (AO): a single center experience from VA Detroit [abstract]. Blood. 2017;130(suppl 1):5383. doi:10.1182/blood.V130.Suppl_1.5383.5383
12. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. doi:10.1016/0021-9681(87)90171-8
13. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. doi:10.1016/0895-4356(92)90133-8
14. Copeland LA, Zeber JE, Sako EY, et al. Serious mental illnesses associated with receipt of surgery in retrospective analysis of patients in the Veterans Health Administration. BMC Surg. 2015;15:74. doi:10.1186/s12893-015-0064-7
15. Younes MA, Perez JD, Alirhayim Z, Ochoa C, Patel R, Dabak VS. MGUS Transformation into multiple myeloma in patients with solid organ transplantation [Abstract presented at American Society of Hematology Annual Meeting, November 15, 2013]. Blood. 2013;122(21):5325. doi:10.1182/blood.V122.21.5325.5325
16. Waxman AJ, Mink PJ, Devesa SS, et al. Racial disparities in incidence and outcome in multiple myeloma: a population- based study. Blood. 2010 Dec 16;116(25):5501-5506. doi:10.1182/blood-2010-07-298760
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30. doi:10.3322/caac.21442
2. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-e548. doi:10.1016/S1470-2045(14)70442-5
3. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. doi:10.4065/78.1.21
4. Kyle RA, Therneau TM, Rajkumar SV, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med. 2002;346(8):564- 569. doi:10.1056/NEJMoa01133202
5. International Myeloma Foundation. What Are MGUS, smoldering and active myeloma? Updated June 6, 2021. Accessed June 20, 2022. https://www.myeloma .org/what-are-mgus-smm-mm
6. Riedel DA, Pottern LM. The epidemiology of multiple myeloma. Hematol Oncol Clin North Am. 1992;6(2):225-247. doi:10.1016/S0889-8588(18)30341-1
7. Buckingham Jr WA. Operation Ranch Hand: The Air Force and herbicides in southeast Asia, 1961-1971. Washington, DC: Office of Air Force History, United States Air Force; 1982. Accessed June 20, 2022. https://apps.dtic.mil/sti /pdfs/ADA121709.pdf
8. Landgren O, Shim YK, Michalek J, et al. Agent Orange exposure and monoclonal gammopathy of undetermined significance: an Operation Ranch Hand veteran cohort study. JAMA Oncol. 2015;1(8):1061-1068. doi:10.1001/jamaoncol.2015.2938
9. Mescher C, Gilbertson D, Randall NM, et al. The impact of Agent Orange exposure on prognosis and management in patients with chronic lymphocytic leukemia: a National Veteran Affairs Tumor Registry Study. Leuk Lymphoma. 2018;59(6):1348-1355. doi:10.1080/10428194.2017.1375109
10. Callander NS, Freytes CO, Luo S, Carson KR. Previous Agent Orange exposure is correlated with worse outcome in patients with multiple myeloma (MM) [abstract]. Blood. 2015;126(23):4194. doi:10.1182/blood.V126.23.4194.4194
11. Bumma N, Nagasaka M, Kim S, Vankayala HM, Ahmed S, Jasti P. Incidence of monoclonal gammopathy of undetermined significance (MGUS) and subsequent transformation to multiple myeloma (MM) and effect of exposure to Agent Orange (AO): a single center experience from VA Detroit [abstract]. Blood. 2017;130(suppl 1):5383. doi:10.1182/blood.V130.Suppl_1.5383.5383
12. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. doi:10.1016/0021-9681(87)90171-8
13. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. doi:10.1016/0895-4356(92)90133-8
14. Copeland LA, Zeber JE, Sako EY, et al. Serious mental illnesses associated with receipt of surgery in retrospective analysis of patients in the Veterans Health Administration. BMC Surg. 2015;15:74. doi:10.1186/s12893-015-0064-7
15. Younes MA, Perez JD, Alirhayim Z, Ochoa C, Patel R, Dabak VS. MGUS Transformation into multiple myeloma in patients with solid organ transplantation [Abstract presented at American Society of Hematology Annual Meeting, November 15, 2013]. Blood. 2013;122(21):5325. doi:10.1182/blood.V122.21.5325.5325
16. Waxman AJ, Mink PJ, Devesa SS, et al. Racial disparities in incidence and outcome in multiple myeloma: a population- based study. Blood. 2010 Dec 16;116(25):5501-5506. doi:10.1182/blood-2010-07-298760
Is prostasin a clue to diabetes/cancer link?
People with elevated levels of protein prostasin seem to have a higher risk of developing diabetes and dying from cancer, according to a large, prospective, population-based study. The finding may provide new insights into why people with diabetes have an increased risk of cancer.
The study claims to be the first to investigate the link between plasma prostasin levels and cancer mortality, the study authors wrote in Diabetologia. The study analyzed plasma prostasin samples from 4,297 older adults (average age, 57.5 years) from the Malmö (Sweden) Diet and Cancer Study Cardiovascular Cohort.

“This study from the general population shows that prostasin, a protein that could be measured in blood, is associated with increased risk of developing diabetes,” senior author Gunnar Engström, MD, PhD, professor of epidemiology at Lund University in Malmö, Sweden, said in a comment. “Furthermore, it was associated with increased risk of death from cancer, especially in individuals with elevated glucose levels in the prediabetic range.
“The relationship between diabetes and cancer is poorly understood,” Dr. Engström said. “To our knowledge, this is the first big population study of prostasin and risk of diabetes.”
He noted previous studies have found a relationship between prostasin and cancer outcomes. “Prostasin could be a possible shared link between the two diseases and the results could help us understand why individuals with diabetes have increased risk of cancer.”
Patients in the study were assigned to quartiles based on prostasin levels. Those in the highest quartile had almost twice the risk of prevalent diabetes than did those in the lowest quartile (adjusted odds ratio, 1.95; 95% confidence interval, 1.39-2.76; P < .0001).
During the follow-up periods of 21.9 years for diabetes and 23.5 years for cancer, on average, 702 participants developed diabetes and 651 died from cancer. Again, the analysis found a significantly higher adjusted hazard ratio for participants in the fourth quartile: about 75% higher for diabetes (HR, 1.76; 95% CI, 1.41-2.19; P < .0001), and, after multivariable analysis, about 40% higher for death from cancer (HR, 1.43; 95% CI, 1.14-1.8; P = .0008).
Potential diabetes-cancer ‘interaction’
The study also identified what it called “a significant interaction” between prostasin and fasting blood glucose for cancer mortality risk (P = .022). In patients with impaired fasting blood glucose levels at baseline, the risk for cancer mortality was about 50% greater with each standard deviation increase in prostasin (HR, 1.52; 95% CI, 1.07-2.16; P = .019). Those with normal fasting blood glucose at baseline had a significantly lower risk with each SD increase in prostasin (HR, 1.11; 95% CI, 1.01-1.21; P = .025).
Further research is needed to validate the potential of prostasin as a biomarker for diabetes and cancer risks, Dr. Engström said. “The results need to be replicated in other studies. A study of cancer mortality in a big cohort of diabetes patients would be of great interest. We also need to examine whether prostasin is causally related to cancer and/or diabetes, or whether prostasin could act as a valuable risk marker in clinical settings. If causal, there could a possible molecular target for treatment.”
He added: “Biomarkers of diabetes and cancer are of great interest in the era of personalized medicine, both for disease prevention and for treatment of those with established disease.”
Li-Mei Chen, MD, PhD, a research associate professor at the University of Central Florida, Orlando, has studied the role of prostasin in epidemiology. She noted that one of the challenges of using prostasin in clinical or research settings is the lack of a standardized assay, which the Malmö study acknowledged. Dr. Engström and colleagues wrote that “prostasin levels were measured in arbitrary units (NPX values), and thus could not be compared directly with absolute values.”
Dr. Chen pointed out that the study reported a lower range of 0.24 pg/mL and an upper range of 7,800 pg/mL.
This means that, “in different groups that measure prostasin, the absolute quantity could have a difference in the thousands or tens of thousands,” she said. “That makes the judgment difficult of whether for this person you have a high level of prostasin in the blood and the other one you don’t if the difference is over a thousandfold.”
The Malmö study used the Proseek Multiplex Oncology I panel to determine plasma prostasin concentration, but Dr. Chen noted that she couldn’t find any data validating the panel for measuring prostasin. “It’s really hard for me to say whether this is of value or not because if the method that generated the data is not verified by another method, you don’t really know what you’re measuring.
“If the data are questionable, it’s really hard to say whether it means whether it’s a marker for cancer or diabetes,” Dr. Chen added. “That’s the biggest question I have, but actually the authors realize that.”
Dr. Engström confirmed that, “if prostasin is used to identify patients with increased risk of diabetes and cancer mortality, we also need to develop standardized assays for clinical use.”
Dr. Engström and coauthors had no disclosures. The study received funding from the Swedish Heart Lung Foundation, the National Natural Science Foundation of China, and the Natural Science Foundation of Jiangsu Province. The Malmö Diet and Cancer study received grants from the Swedish Cancer Society, the Swedish Medical Research Council, AFA Insurance, the Albert Påhlsson and Gunnar Nilsson Foundations, Malmö City Council, and Lund University. Dr. Chen had no relevant disclosures.
People with elevated levels of protein prostasin seem to have a higher risk of developing diabetes and dying from cancer, according to a large, prospective, population-based study. The finding may provide new insights into why people with diabetes have an increased risk of cancer.
The study claims to be the first to investigate the link between plasma prostasin levels and cancer mortality, the study authors wrote in Diabetologia. The study analyzed plasma prostasin samples from 4,297 older adults (average age, 57.5 years) from the Malmö (Sweden) Diet and Cancer Study Cardiovascular Cohort.
“This study from the general population shows that prostasin, a protein that could be measured in blood, is associated with increased risk of developing diabetes,” senior author Gunnar Engström, MD, PhD, professor of epidemiology at Lund University in Malmö, Sweden, said in a comment. “Furthermore, it was associated with increased risk of death from cancer, especially in individuals with elevated glucose levels in the prediabetic range.
“The relationship between diabetes and cancer is poorly understood,” Dr. Engström said. “To our knowledge, this is the first big population study of prostasin and risk of diabetes.”
He noted previous studies have found a relationship between prostasin and cancer outcomes. “Prostasin could be a possible shared link between the two diseases and the results could help us understand why individuals with diabetes have increased risk of cancer.”
Patients in the study were assigned to quartiles based on prostasin levels. Those in the highest quartile had almost twice the risk of prevalent diabetes than did those in the lowest quartile (adjusted odds ratio, 1.95; 95% confidence interval, 1.39-2.76; P < .0001).
During the follow-up periods of 21.9 years for diabetes and 23.5 years for cancer, on average, 702 participants developed diabetes and 651 died from cancer. Again, the analysis found a significantly higher adjusted hazard ratio for participants in the fourth quartile: about 75% higher for diabetes (HR, 1.76; 95% CI, 1.41-2.19; P < .0001), and, after multivariable analysis, about 40% higher for death from cancer (HR, 1.43; 95% CI, 1.14-1.8; P = .0008).
Potential diabetes-cancer ‘interaction’
The study also identified what it called “a significant interaction” between prostasin and fasting blood glucose for cancer mortality risk (P = .022). In patients with impaired fasting blood glucose levels at baseline, the risk for cancer mortality was about 50% greater with each standard deviation increase in prostasin (HR, 1.52; 95% CI, 1.07-2.16; P = .019). Those with normal fasting blood glucose at baseline had a significantly lower risk with each SD increase in prostasin (HR, 1.11; 95% CI, 1.01-1.21; P = .025).
Further research is needed to validate the potential of prostasin as a biomarker for diabetes and cancer risks, Dr. Engström said. “The results need to be replicated in other studies. A study of cancer mortality in a big cohort of diabetes patients would be of great interest. We also need to examine whether prostasin is causally related to cancer and/or diabetes, or whether prostasin could act as a valuable risk marker in clinical settings. If causal, there could a possible molecular target for treatment.”
He added: “Biomarkers of diabetes and cancer are of great interest in the era of personalized medicine, both for disease prevention and for treatment of those with established disease.”
Li-Mei Chen, MD, PhD, a research associate professor at the University of Central Florida, Orlando, has studied the role of prostasin in epidemiology. She noted that one of the challenges of using prostasin in clinical or research settings is the lack of a standardized assay, which the Malmö study acknowledged. Dr. Engström and colleagues wrote that “prostasin levels were measured in arbitrary units (NPX values), and thus could not be compared directly with absolute values.”
Dr. Chen pointed out that the study reported a lower range of 0.24 pg/mL and an upper range of 7,800 pg/mL.
This means that, “in different groups that measure prostasin, the absolute quantity could have a difference in the thousands or tens of thousands,” she said. “That makes the judgment difficult of whether for this person you have a high level of prostasin in the blood and the other one you don’t if the difference is over a thousandfold.”
The Malmö study used the Proseek Multiplex Oncology I panel to determine plasma prostasin concentration, but Dr. Chen noted that she couldn’t find any data validating the panel for measuring prostasin. “It’s really hard for me to say whether this is of value or not because if the method that generated the data is not verified by another method, you don’t really know what you’re measuring.
“If the data are questionable, it’s really hard to say whether it means whether it’s a marker for cancer or diabetes,” Dr. Chen added. “That’s the biggest question I have, but actually the authors realize that.”
Dr. Engström confirmed that, “if prostasin is used to identify patients with increased risk of diabetes and cancer mortality, we also need to develop standardized assays for clinical use.”
Dr. Engström and coauthors had no disclosures. The study received funding from the Swedish Heart Lung Foundation, the National Natural Science Foundation of China, and the Natural Science Foundation of Jiangsu Province. The Malmö Diet and Cancer study received grants from the Swedish Cancer Society, the Swedish Medical Research Council, AFA Insurance, the Albert Påhlsson and Gunnar Nilsson Foundations, Malmö City Council, and Lund University. Dr. Chen had no relevant disclosures.
People with elevated levels of protein prostasin seem to have a higher risk of developing diabetes and dying from cancer, according to a large, prospective, population-based study. The finding may provide new insights into why people with diabetes have an increased risk of cancer.
The study claims to be the first to investigate the link between plasma prostasin levels and cancer mortality, the study authors wrote in Diabetologia. The study analyzed plasma prostasin samples from 4,297 older adults (average age, 57.5 years) from the Malmö (Sweden) Diet and Cancer Study Cardiovascular Cohort.
“This study from the general population shows that prostasin, a protein that could be measured in blood, is associated with increased risk of developing diabetes,” senior author Gunnar Engström, MD, PhD, professor of epidemiology at Lund University in Malmö, Sweden, said in a comment. “Furthermore, it was associated with increased risk of death from cancer, especially in individuals with elevated glucose levels in the prediabetic range.
“The relationship between diabetes and cancer is poorly understood,” Dr. Engström said. “To our knowledge, this is the first big population study of prostasin and risk of diabetes.”
He noted previous studies have found a relationship between prostasin and cancer outcomes. “Prostasin could be a possible shared link between the two diseases and the results could help us understand why individuals with diabetes have increased risk of cancer.”
Patients in the study were assigned to quartiles based on prostasin levels. Those in the highest quartile had almost twice the risk of prevalent diabetes than did those in the lowest quartile (adjusted odds ratio, 1.95; 95% confidence interval, 1.39-2.76; P < .0001).
During the follow-up periods of 21.9 years for diabetes and 23.5 years for cancer, on average, 702 participants developed diabetes and 651 died from cancer. Again, the analysis found a significantly higher adjusted hazard ratio for participants in the fourth quartile: about 75% higher for diabetes (HR, 1.76; 95% CI, 1.41-2.19; P < .0001), and, after multivariable analysis, about 40% higher for death from cancer (HR, 1.43; 95% CI, 1.14-1.8; P = .0008).
Potential diabetes-cancer ‘interaction’
The study also identified what it called “a significant interaction” between prostasin and fasting blood glucose for cancer mortality risk (P = .022). In patients with impaired fasting blood glucose levels at baseline, the risk for cancer mortality was about 50% greater with each standard deviation increase in prostasin (HR, 1.52; 95% CI, 1.07-2.16; P = .019). Those with normal fasting blood glucose at baseline had a significantly lower risk with each SD increase in prostasin (HR, 1.11; 95% CI, 1.01-1.21; P = .025).
Further research is needed to validate the potential of prostasin as a biomarker for diabetes and cancer risks, Dr. Engström said. “The results need to be replicated in other studies. A study of cancer mortality in a big cohort of diabetes patients would be of great interest. We also need to examine whether prostasin is causally related to cancer and/or diabetes, or whether prostasin could act as a valuable risk marker in clinical settings. If causal, there could a possible molecular target for treatment.”
He added: “Biomarkers of diabetes and cancer are of great interest in the era of personalized medicine, both for disease prevention and for treatment of those with established disease.”
Li-Mei Chen, MD, PhD, a research associate professor at the University of Central Florida, Orlando, has studied the role of prostasin in epidemiology. She noted that one of the challenges of using prostasin in clinical or research settings is the lack of a standardized assay, which the Malmö study acknowledged. Dr. Engström and colleagues wrote that “prostasin levels were measured in arbitrary units (NPX values), and thus could not be compared directly with absolute values.”
Dr. Chen pointed out that the study reported a lower range of 0.24 pg/mL and an upper range of 7,800 pg/mL.
This means that, “in different groups that measure prostasin, the absolute quantity could have a difference in the thousands or tens of thousands,” she said. “That makes the judgment difficult of whether for this person you have a high level of prostasin in the blood and the other one you don’t if the difference is over a thousandfold.”
The Malmö study used the Proseek Multiplex Oncology I panel to determine plasma prostasin concentration, but Dr. Chen noted that she couldn’t find any data validating the panel for measuring prostasin. “It’s really hard for me to say whether this is of value or not because if the method that generated the data is not verified by another method, you don’t really know what you’re measuring.
“If the data are questionable, it’s really hard to say whether it means whether it’s a marker for cancer or diabetes,” Dr. Chen added. “That’s the biggest question I have, but actually the authors realize that.”
Dr. Engström confirmed that, “if prostasin is used to identify patients with increased risk of diabetes and cancer mortality, we also need to develop standardized assays for clinical use.”
Dr. Engström and coauthors had no disclosures. The study received funding from the Swedish Heart Lung Foundation, the National Natural Science Foundation of China, and the Natural Science Foundation of Jiangsu Province. The Malmö Diet and Cancer study received grants from the Swedish Cancer Society, the Swedish Medical Research Council, AFA Insurance, the Albert Påhlsson and Gunnar Nilsson Foundations, Malmö City Council, and Lund University. Dr. Chen had no relevant disclosures.
FROM DIABETOLOGIA
New blood test could reshape early CRC screening
A simple blood test that looks for a combination of specific RNA snippets may become a novel way to screen for early-onset colorectal cancer, suggests a new study published online in Gastroenterology.
Researchers identified four microRNAs that together comprise a signature biomarker that can be used to detect and diagnose the presence of colorectal cancer from a liquid biopsy in a younger population.
MicroRNAs, or miRNAs, are small RNA molecules that do not encode proteins but are used instead to regulate gene expression. The study authors developed and validated a panel that detects four miRNAs occurring at higher levels in plasma samples from patients with early-onset colorectal cancer, with high sensitivity and specificity.
“The point would be to use this test as a routine part of annual healthcare, or for people in high-risk families every 6 months,” study senior author Ajay Goel, PhD, MS, chair of the department of molecular diagnostics and experimental therapeutics at the City of Hope Comprehensive Cancer Center, Duarte, Calif., said in an interview.
“It’s affordable, it can be done easily from a small tube of blood, and as long as that test stays negative, you’re good,” Dr. Goel said, because even if patients miss a test, the next one, whether it’s 6 months or a year later, will catch any potential cancer.
“Colon cancer is not going to kill somebody overnight, so this should be used as a precursor to colonoscopy. As long as that test is negative, you can postpone a colonoscopy,” he said.
Andrew T. Chan, MD, MPH, a professor of medicine at Harvard Medical School and vice chair of gastroenterology at Massachusetts General Hospital, both in Boston, who was not involved in the research, said in an interview that the findings are exciting.
“It would be really value-added to have a blood-based screening test,” Dr. Chan said, adding that researchers have pursued multiple different avenues in pursuit of one. “It’s very nice to see that area progress and to actually have some evidence that microRNAs could be a potential biomarker for colorectal cancer.”
Screening now insufficient for early-onset disease
The U.S. Preventive Services Task Force recently lowered the recommended age to 45 years to begin screening for colorectal cancer. Part of the rationale for the change came from the rising rates of early-onset colorectal cancer, a distinct clinical and molecular entity that tends to have poorer survival than late-onset disease, the authors noted.
Early-onset disease, occurring primarily in people under 50 without a family or genetic history of colorectal cancer, now makes up about 10%-15% of all new cases and continues to rise, they write.
“Early-onset colorectal cancer patients are more likely to exhibit an advanced stage tumor at initial presentation, distal tumor localization, signet ring histology, and a disease presentation with concurrent metastasis,” the authors wrote. “This raises the logistical clinical concern that, since the tumors in early-onset colorectal cancer patients are often more aggressive than those with late-onset colorectal cancer, a delayed diagnosis could have a significant adverse impact and can lead to early death.”
Yet current screening strategies are insufficient for detecting enough early-onset cases, the authors assert.
Colonoscopies are invasive, carry a risk for complications, and are cost- and time-prohibitive for people at average risk. Meanwhile, existing fecal and blood tests “lack adequate diagnostic performance for the early detection of colorectal cancer, especially early-onset colorectal cancer, as these assays have yet to be explored or developed in this population,” they wrote.
The ideal “diagnostic modality should preferably be acceptable to healthy individuals, inexpensive, rapid, and preferably noninvasive,” they note.
Finding and validating miRNA
The researchers therefore turned to the concept of a liquid biopsy, focusing on identifying miRNAs associated with colorectal cancer, because their expression tends to be stable in tissues, blood, stool, and other body fluids.
They first analyzed an miRNA expression profiling dataset from 1,061 individuals to look for miRNAs whose expression was higher in colorectal cancer patients. The dataset included 42 patients with stage 1-2 early-onset colorectal cancer, 370 patients with stage 1-2 late-onset colorectal cancer, 62 patients younger than 50 years without cancer, and 587 patients aged 50 years or older without cancer.
The researchers found 28 miRNAs that were significantly unregulated in early-onset colorectal cancer tissue samples, compared with cancer-free samples and 11 miRNAs unregulated specifically in only the early-onset colorectal cancer samples. Four of these 11 miRNAs were adequately distinct from one another and were detectable in the plasma samples that the researchers would use to train and validate them as a combination biomarker.
The researchers used 117 plasma samples from Japan, including 72 from people with early-onset colorectal cancer and 45 from healthy donors, to develop and train an assay detecting the four miRNAs. They then validated the assay using 142 plasma samples from Spain, including 77 with early-onset colorectal cancer and 65 healthy donors.
In the Japan cohort, the four-miRNA assay had a sensitivity of 90% and a specificity of 80%, with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 84%. In the Spain cohort used for validation, the assay performed with a sensitivity of 82%, a specificity of 86%, a PPV of 88%, and an NPV of 80%.
“Taken together, the genome-wide transcriptomic profiling approach was indeed robust, as it identified the biomarkers that were successfully trained and validated in plasma specimens from independent cohorts of patients with early-onset colorectal cancer, hence highlighting their translational potential in the clinic for the detection of this malignancy in early stages,” the authors wrote.
By disease stage, the four-miRNA panel identified both early-stage (stage 1-2; sensitivity, 92%; specificity, 80%) and late-stage (stage 3-4; sensitivity, 79%; specificity, 86%) early-onset colorectal cancer in the validation cohort.
Clinical benefit of blood test
The researchers also assessed the benefit-harm trade-off of this liquid biopsy assay compared with other screening modalities, taking into consideration the risk for false positives and false negatives.
A decision curve analysis “revealed that the miRNA panel achieved a higher net benefit regardless of threshold probability in comparison to intervention for all patients or none of the patients,” the researchers reported. “These findings suggest that this miRNA panel might offer more clinical benefit with regards to the avoidance of physical harm and misdiagnosis.”
They also found that expression levels of these four miRNAs significantly decreased after surgical removal of the colorectal cancer, strongly suggesting that the miRNAs do originate with the tumor.
“To have a relatively inexpensive and noninvasive means of screening a younger population is a very important unmet need,” said Dr. Chan.
It’s not feasible to recommend colonoscopies in people younger than 45 years because of resource constraints, he said, so “this is a wonderful new development to actually have the possibility of a blood-based screening test for younger individuals, especially given that rising incidence of young-onset colorectal cancer.”
Dr. Goel pointed out that only half of those recommended to get screened for colorectal cancer actually undergo screening, and a large reason for that is the desire to avoid colonoscopy, a concern echoed in the findings of a recent study by Christopher V. Almario, MD, MSHPM, and colleagues.
Dr. Goel expects that this strategy would increase compliance with screening because it’s less invasive and more affordable, particularly for younger patients. He estimates that a commercial assay using this panel, if approved by the Food and Drug Administration, should cost less than $100.
Dr. Almario, an assistant professor of medicine at the Cedars-Sinai Karsh Division of Gastroenterology and Hepatology in Los Angeles, agreed that an FDA-approved blood-based screening test would be a “game-changer,” as long as it’s accurate and effective.
Though Dr. Almario did not review the data in Goel’s study, he said in an interview that a blood test for colorectal cancer screening would be “the holy grail, so to speak, in terms of really moving the needle on screening uptake.”
Next steps
Dr. Chan noted that one caveat to consider with this study is that it was done in a relatively small population of individuals, even though the test was validated in a second set of plasma samples.
“Additional validation needs to be done in larger numbers of patients to really understand the performance characteristics because it is possible that some of these signatures may, when they’re using a broader group of individuals, not perform as well,” Dr. Chan said.
Dr. Goel said he is working with several companies right now to develop and further test a commercial product. He anticipates it may be shelf-ready in 2-5 years.
“The take-home message is that clinicians need to be more cognizant of the fact that incidence of this disease is rising, and we need to do something about it,” Dr. Goel said, particularly for those younger than 45 years who currently don’t have a screening option.
“Now we have at least a sliver of hope for those who might be suffering from this disease, for those for whom we have zero screening or diagnostic tests,” he said.
The research was funded by the National Cancer Institute and Fundación MAPFRE Guanarteme. Dr. Goel, Dr. Chan, and Dr. Almario reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
A simple blood test that looks for a combination of specific RNA snippets may become a novel way to screen for early-onset colorectal cancer, suggests a new study published online in Gastroenterology.
Researchers identified four microRNAs that together comprise a signature biomarker that can be used to detect and diagnose the presence of colorectal cancer from a liquid biopsy in a younger population.
MicroRNAs, or miRNAs, are small RNA molecules that do not encode proteins but are used instead to regulate gene expression. The study authors developed and validated a panel that detects four miRNAs occurring at higher levels in plasma samples from patients with early-onset colorectal cancer, with high sensitivity and specificity.
“The point would be to use this test as a routine part of annual healthcare, or for people in high-risk families every 6 months,” study senior author Ajay Goel, PhD, MS, chair of the department of molecular diagnostics and experimental therapeutics at the City of Hope Comprehensive Cancer Center, Duarte, Calif., said in an interview.
“It’s affordable, it can be done easily from a small tube of blood, and as long as that test stays negative, you’re good,” Dr. Goel said, because even if patients miss a test, the next one, whether it’s 6 months or a year later, will catch any potential cancer.
“Colon cancer is not going to kill somebody overnight, so this should be used as a precursor to colonoscopy. As long as that test is negative, you can postpone a colonoscopy,” he said.
Andrew T. Chan, MD, MPH, a professor of medicine at Harvard Medical School and vice chair of gastroenterology at Massachusetts General Hospital, both in Boston, who was not involved in the research, said in an interview that the findings are exciting.
“It would be really value-added to have a blood-based screening test,” Dr. Chan said, adding that researchers have pursued multiple different avenues in pursuit of one. “It’s very nice to see that area progress and to actually have some evidence that microRNAs could be a potential biomarker for colorectal cancer.”
Screening now insufficient for early-onset disease
The U.S. Preventive Services Task Force recently lowered the recommended age to 45 years to begin screening for colorectal cancer. Part of the rationale for the change came from the rising rates of early-onset colorectal cancer, a distinct clinical and molecular entity that tends to have poorer survival than late-onset disease, the authors noted.
Early-onset disease, occurring primarily in people under 50 without a family or genetic history of colorectal cancer, now makes up about 10%-15% of all new cases and continues to rise, they write.
“Early-onset colorectal cancer patients are more likely to exhibit an advanced stage tumor at initial presentation, distal tumor localization, signet ring histology, and a disease presentation with concurrent metastasis,” the authors wrote. “This raises the logistical clinical concern that, since the tumors in early-onset colorectal cancer patients are often more aggressive than those with late-onset colorectal cancer, a delayed diagnosis could have a significant adverse impact and can lead to early death.”
Yet current screening strategies are insufficient for detecting enough early-onset cases, the authors assert.
Colonoscopies are invasive, carry a risk for complications, and are cost- and time-prohibitive for people at average risk. Meanwhile, existing fecal and blood tests “lack adequate diagnostic performance for the early detection of colorectal cancer, especially early-onset colorectal cancer, as these assays have yet to be explored or developed in this population,” they wrote.
The ideal “diagnostic modality should preferably be acceptable to healthy individuals, inexpensive, rapid, and preferably noninvasive,” they note.
Finding and validating miRNA
The researchers therefore turned to the concept of a liquid biopsy, focusing on identifying miRNAs associated with colorectal cancer, because their expression tends to be stable in tissues, blood, stool, and other body fluids.
They first analyzed an miRNA expression profiling dataset from 1,061 individuals to look for miRNAs whose expression was higher in colorectal cancer patients. The dataset included 42 patients with stage 1-2 early-onset colorectal cancer, 370 patients with stage 1-2 late-onset colorectal cancer, 62 patients younger than 50 years without cancer, and 587 patients aged 50 years or older without cancer.
The researchers found 28 miRNAs that were significantly unregulated in early-onset colorectal cancer tissue samples, compared with cancer-free samples and 11 miRNAs unregulated specifically in only the early-onset colorectal cancer samples. Four of these 11 miRNAs were adequately distinct from one another and were detectable in the plasma samples that the researchers would use to train and validate them as a combination biomarker.
The researchers used 117 plasma samples from Japan, including 72 from people with early-onset colorectal cancer and 45 from healthy donors, to develop and train an assay detecting the four miRNAs. They then validated the assay using 142 plasma samples from Spain, including 77 with early-onset colorectal cancer and 65 healthy donors.
In the Japan cohort, the four-miRNA assay had a sensitivity of 90% and a specificity of 80%, with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 84%. In the Spain cohort used for validation, the assay performed with a sensitivity of 82%, a specificity of 86%, a PPV of 88%, and an NPV of 80%.
“Taken together, the genome-wide transcriptomic profiling approach was indeed robust, as it identified the biomarkers that were successfully trained and validated in plasma specimens from independent cohorts of patients with early-onset colorectal cancer, hence highlighting their translational potential in the clinic for the detection of this malignancy in early stages,” the authors wrote.
By disease stage, the four-miRNA panel identified both early-stage (stage 1-2; sensitivity, 92%; specificity, 80%) and late-stage (stage 3-4; sensitivity, 79%; specificity, 86%) early-onset colorectal cancer in the validation cohort.
Clinical benefit of blood test
The researchers also assessed the benefit-harm trade-off of this liquid biopsy assay compared with other screening modalities, taking into consideration the risk for false positives and false negatives.
A decision curve analysis “revealed that the miRNA panel achieved a higher net benefit regardless of threshold probability in comparison to intervention for all patients or none of the patients,” the researchers reported. “These findings suggest that this miRNA panel might offer more clinical benefit with regards to the avoidance of physical harm and misdiagnosis.”
They also found that expression levels of these four miRNAs significantly decreased after surgical removal of the colorectal cancer, strongly suggesting that the miRNAs do originate with the tumor.
“To have a relatively inexpensive and noninvasive means of screening a younger population is a very important unmet need,” said Dr. Chan.
It’s not feasible to recommend colonoscopies in people younger than 45 years because of resource constraints, he said, so “this is a wonderful new development to actually have the possibility of a blood-based screening test for younger individuals, especially given that rising incidence of young-onset colorectal cancer.”
Dr. Goel pointed out that only half of those recommended to get screened for colorectal cancer actually undergo screening, and a large reason for that is the desire to avoid colonoscopy, a concern echoed in the findings of a recent study by Christopher V. Almario, MD, MSHPM, and colleagues.
Dr. Goel expects that this strategy would increase compliance with screening because it’s less invasive and more affordable, particularly for younger patients. He estimates that a commercial assay using this panel, if approved by the Food and Drug Administration, should cost less than $100.
Dr. Almario, an assistant professor of medicine at the Cedars-Sinai Karsh Division of Gastroenterology and Hepatology in Los Angeles, agreed that an FDA-approved blood-based screening test would be a “game-changer,” as long as it’s accurate and effective.
Though Dr. Almario did not review the data in Goel’s study, he said in an interview that a blood test for colorectal cancer screening would be “the holy grail, so to speak, in terms of really moving the needle on screening uptake.”
Next steps
Dr. Chan noted that one caveat to consider with this study is that it was done in a relatively small population of individuals, even though the test was validated in a second set of plasma samples.
“Additional validation needs to be done in larger numbers of patients to really understand the performance characteristics because it is possible that some of these signatures may, when they’re using a broader group of individuals, not perform as well,” Dr. Chan said.
Dr. Goel said he is working with several companies right now to develop and further test a commercial product. He anticipates it may be shelf-ready in 2-5 years.
“The take-home message is that clinicians need to be more cognizant of the fact that incidence of this disease is rising, and we need to do something about it,” Dr. Goel said, particularly for those younger than 45 years who currently don’t have a screening option.
“Now we have at least a sliver of hope for those who might be suffering from this disease, for those for whom we have zero screening or diagnostic tests,” he said.
The research was funded by the National Cancer Institute and Fundación MAPFRE Guanarteme. Dr. Goel, Dr. Chan, and Dr. Almario reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
A simple blood test that looks for a combination of specific RNA snippets may become a novel way to screen for early-onset colorectal cancer, suggests a new study published online in Gastroenterology.
Researchers identified four microRNAs that together comprise a signature biomarker that can be used to detect and diagnose the presence of colorectal cancer from a liquid biopsy in a younger population.
MicroRNAs, or miRNAs, are small RNA molecules that do not encode proteins but are used instead to regulate gene expression. The study authors developed and validated a panel that detects four miRNAs occurring at higher levels in plasma samples from patients with early-onset colorectal cancer, with high sensitivity and specificity.
“The point would be to use this test as a routine part of annual healthcare, or for people in high-risk families every 6 months,” study senior author Ajay Goel, PhD, MS, chair of the department of molecular diagnostics and experimental therapeutics at the City of Hope Comprehensive Cancer Center, Duarte, Calif., said in an interview.
“It’s affordable, it can be done easily from a small tube of blood, and as long as that test stays negative, you’re good,” Dr. Goel said, because even if patients miss a test, the next one, whether it’s 6 months or a year later, will catch any potential cancer.
“Colon cancer is not going to kill somebody overnight, so this should be used as a precursor to colonoscopy. As long as that test is negative, you can postpone a colonoscopy,” he said.
Andrew T. Chan, MD, MPH, a professor of medicine at Harvard Medical School and vice chair of gastroenterology at Massachusetts General Hospital, both in Boston, who was not involved in the research, said in an interview that the findings are exciting.
“It would be really value-added to have a blood-based screening test,” Dr. Chan said, adding that researchers have pursued multiple different avenues in pursuit of one. “It’s very nice to see that area progress and to actually have some evidence that microRNAs could be a potential biomarker for colorectal cancer.”
Screening now insufficient for early-onset disease
The U.S. Preventive Services Task Force recently lowered the recommended age to 45 years to begin screening for colorectal cancer. Part of the rationale for the change came from the rising rates of early-onset colorectal cancer, a distinct clinical and molecular entity that tends to have poorer survival than late-onset disease, the authors noted.
Early-onset disease, occurring primarily in people under 50 without a family or genetic history of colorectal cancer, now makes up about 10%-15% of all new cases and continues to rise, they write.
“Early-onset colorectal cancer patients are more likely to exhibit an advanced stage tumor at initial presentation, distal tumor localization, signet ring histology, and a disease presentation with concurrent metastasis,” the authors wrote. “This raises the logistical clinical concern that, since the tumors in early-onset colorectal cancer patients are often more aggressive than those with late-onset colorectal cancer, a delayed diagnosis could have a significant adverse impact and can lead to early death.”
Yet current screening strategies are insufficient for detecting enough early-onset cases, the authors assert.
Colonoscopies are invasive, carry a risk for complications, and are cost- and time-prohibitive for people at average risk. Meanwhile, existing fecal and blood tests “lack adequate diagnostic performance for the early detection of colorectal cancer, especially early-onset colorectal cancer, as these assays have yet to be explored or developed in this population,” they wrote.
The ideal “diagnostic modality should preferably be acceptable to healthy individuals, inexpensive, rapid, and preferably noninvasive,” they note.
Finding and validating miRNA
The researchers therefore turned to the concept of a liquid biopsy, focusing on identifying miRNAs associated with colorectal cancer, because their expression tends to be stable in tissues, blood, stool, and other body fluids.
They first analyzed an miRNA expression profiling dataset from 1,061 individuals to look for miRNAs whose expression was higher in colorectal cancer patients. The dataset included 42 patients with stage 1-2 early-onset colorectal cancer, 370 patients with stage 1-2 late-onset colorectal cancer, 62 patients younger than 50 years without cancer, and 587 patients aged 50 years or older without cancer.
The researchers found 28 miRNAs that were significantly unregulated in early-onset colorectal cancer tissue samples, compared with cancer-free samples and 11 miRNAs unregulated specifically in only the early-onset colorectal cancer samples. Four of these 11 miRNAs were adequately distinct from one another and were detectable in the plasma samples that the researchers would use to train and validate them as a combination biomarker.
The researchers used 117 plasma samples from Japan, including 72 from people with early-onset colorectal cancer and 45 from healthy donors, to develop and train an assay detecting the four miRNAs. They then validated the assay using 142 plasma samples from Spain, including 77 with early-onset colorectal cancer and 65 healthy donors.
In the Japan cohort, the four-miRNA assay had a sensitivity of 90% and a specificity of 80%, with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 84%. In the Spain cohort used for validation, the assay performed with a sensitivity of 82%, a specificity of 86%, a PPV of 88%, and an NPV of 80%.
“Taken together, the genome-wide transcriptomic profiling approach was indeed robust, as it identified the biomarkers that were successfully trained and validated in plasma specimens from independent cohorts of patients with early-onset colorectal cancer, hence highlighting their translational potential in the clinic for the detection of this malignancy in early stages,” the authors wrote.
By disease stage, the four-miRNA panel identified both early-stage (stage 1-2; sensitivity, 92%; specificity, 80%) and late-stage (stage 3-4; sensitivity, 79%; specificity, 86%) early-onset colorectal cancer in the validation cohort.
Clinical benefit of blood test
The researchers also assessed the benefit-harm trade-off of this liquid biopsy assay compared with other screening modalities, taking into consideration the risk for false positives and false negatives.
A decision curve analysis “revealed that the miRNA panel achieved a higher net benefit regardless of threshold probability in comparison to intervention for all patients or none of the patients,” the researchers reported. “These findings suggest that this miRNA panel might offer more clinical benefit with regards to the avoidance of physical harm and misdiagnosis.”
They also found that expression levels of these four miRNAs significantly decreased after surgical removal of the colorectal cancer, strongly suggesting that the miRNAs do originate with the tumor.
“To have a relatively inexpensive and noninvasive means of screening a younger population is a very important unmet need,” said Dr. Chan.
It’s not feasible to recommend colonoscopies in people younger than 45 years because of resource constraints, he said, so “this is a wonderful new development to actually have the possibility of a blood-based screening test for younger individuals, especially given that rising incidence of young-onset colorectal cancer.”
Dr. Goel pointed out that only half of those recommended to get screened for colorectal cancer actually undergo screening, and a large reason for that is the desire to avoid colonoscopy, a concern echoed in the findings of a recent study by Christopher V. Almario, MD, MSHPM, and colleagues.
Dr. Goel expects that this strategy would increase compliance with screening because it’s less invasive and more affordable, particularly for younger patients. He estimates that a commercial assay using this panel, if approved by the Food and Drug Administration, should cost less than $100.
Dr. Almario, an assistant professor of medicine at the Cedars-Sinai Karsh Division of Gastroenterology and Hepatology in Los Angeles, agreed that an FDA-approved blood-based screening test would be a “game-changer,” as long as it’s accurate and effective.
Though Dr. Almario did not review the data in Goel’s study, he said in an interview that a blood test for colorectal cancer screening would be “the holy grail, so to speak, in terms of really moving the needle on screening uptake.”
Next steps
Dr. Chan noted that one caveat to consider with this study is that it was done in a relatively small population of individuals, even though the test was validated in a second set of plasma samples.
“Additional validation needs to be done in larger numbers of patients to really understand the performance characteristics because it is possible that some of these signatures may, when they’re using a broader group of individuals, not perform as well,” Dr. Chan said.
Dr. Goel said he is working with several companies right now to develop and further test a commercial product. He anticipates it may be shelf-ready in 2-5 years.
“The take-home message is that clinicians need to be more cognizant of the fact that incidence of this disease is rising, and we need to do something about it,” Dr. Goel said, particularly for those younger than 45 years who currently don’t have a screening option.
“Now we have at least a sliver of hope for those who might be suffering from this disease, for those for whom we have zero screening or diagnostic tests,” he said.
The research was funded by the National Cancer Institute and Fundación MAPFRE Guanarteme. Dr. Goel, Dr. Chan, and Dr. Almario reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM GASTROENTEROLOGY
One in four NSCLC patients respond poorly to COVID-19 vaccine
according to a new study.
The study was published in the Journal of Clinical Oncology.
“Booster vaccination increased binding and neutralizing antibody titers to Omicron, but antibody titers declined after 3 months. These data highlight the concern for patients with cancer given the rapid spread of SARS-CoV-2 Omicron variant,” wrote the authors, who were led by Rafi Ahmed, PhD, Emory University, Atlanta.
Researchers found that 18% had no detectable antibody at all and active treatment type had no association with vaccine response.
Researchers examined antibody titers among 82 NSCLC patients and 53 healthy volunteers. They collected blood samples longitudinally for analysis. While most patients had binding and neutralizing antibody titers that were comparable with healthy volunteers, 25% had poor responses, which led to six- to sevenfold lower titers than healthy controls. There was no association between worse vaccine responses and history of programmed death–1 monotherapy, chemotherapy, or both in combination. Receipt of a booster vaccine improved binding and neutralizing antibody titers to both the wild type and the Omicron variant, but 2-4 months after the booster there was a five- to sevenfold decrease in neutralizing titers to both the wild type and Omicron variant.
“This study indicates both the need to monitor our patients with lung cancer for response to COVID-19 mRNA vaccines, identify the nonresponders for follow-up and further attempts at immunization, and continue collecting and analyzing clinicodemographic information and biospecimens from our patients,” wrote the authors of an accompanying editorial.
Although the findings reveal potential concerns, the good news is that most patients NSCLC patients do respond normally to COVID-19 vaccination, said John D. Minna, MD, University of Texas Southwestern Medical Center, Dallas, lead author of the editorial.
He offered some advice to physicians. “You can test your patients using currently available [Clinical Laboratory Improvement Amendments]–approved lab tests to determine what their antibody titers are. This should be done after boosting since titers will go down after time. We know that if a patient has lung cancer and they do get infected with SARS-CoV-2 that potentially they could develop serious COVID-19 disease. Besides giving antiviral treatment, it is important that they be closely monitored for symptoms of progression so if they need to be hospitalized it can be done in a prudent manner,” said Dr. Minna, who is director of the Hamon Center for Therapeutic Oncology Research at the University of Texas Southwestern Medical Center.
No clinical details have emerged that might predict which patients have an insufficient response to vaccination. “When we started these studies, a lot of us thought that anyone who did not develop a good antibody response would be weak or sicker. For example, [patients with] late-stage disease, or having had a lot of therapy, or perhaps immune checkpoint blockade. However, none of these things are correlated. The main advice we are giving our lung cancer patients are to get vaccinated, get boosted (double boosted), and just do the smart thing to protect yourself from exposure,” he said.
For example, when traveling on a plane, patients should wear a mask. They should also avoid large indoor events. He also recommended that, following vaccination and boosters, patients seek out CLIA-certified tests to get their titer checked.
“Upon any COVID infection, even if their titer is at or above 80%, patients should see their physician to consider treatment with Paxlovid (nirmatrelvir/ritonavir), which has emergency use authorization. For patients with a lower titer, it’s important to seek out a physician and consider Paxlovid and possibly antibody therapy. But these are individual decisions to be made with your doctor,” Dr. Minna said.
The next important research question is what happens to T-cell immune response following vaccination. “We know that a good cellular immune response is also important in preventing infection and severe infection, but we don’t yet know which persons (with or without cancer) have good T-cell responses. This information will also likely impact what we tell our patients and will add to the antibody data,” he said.
Studies are ongoing to determine specific T-cell responses to mRNA vaccines, and how well those T-cell responses respond to SARS-CoV-2 infection in the laboratory.
according to a new study.
The study was published in the Journal of Clinical Oncology.
“Booster vaccination increased binding and neutralizing antibody titers to Omicron, but antibody titers declined after 3 months. These data highlight the concern for patients with cancer given the rapid spread of SARS-CoV-2 Omicron variant,” wrote the authors, who were led by Rafi Ahmed, PhD, Emory University, Atlanta.
Researchers found that 18% had no detectable antibody at all and active treatment type had no association with vaccine response.
Researchers examined antibody titers among 82 NSCLC patients and 53 healthy volunteers. They collected blood samples longitudinally for analysis. While most patients had binding and neutralizing antibody titers that were comparable with healthy volunteers, 25% had poor responses, which led to six- to sevenfold lower titers than healthy controls. There was no association between worse vaccine responses and history of programmed death–1 monotherapy, chemotherapy, or both in combination. Receipt of a booster vaccine improved binding and neutralizing antibody titers to both the wild type and the Omicron variant, but 2-4 months after the booster there was a five- to sevenfold decrease in neutralizing titers to both the wild type and Omicron variant.
“This study indicates both the need to monitor our patients with lung cancer for response to COVID-19 mRNA vaccines, identify the nonresponders for follow-up and further attempts at immunization, and continue collecting and analyzing clinicodemographic information and biospecimens from our patients,” wrote the authors of an accompanying editorial.
Although the findings reveal potential concerns, the good news is that most patients NSCLC patients do respond normally to COVID-19 vaccination, said John D. Minna, MD, University of Texas Southwestern Medical Center, Dallas, lead author of the editorial.
He offered some advice to physicians. “You can test your patients using currently available [Clinical Laboratory Improvement Amendments]–approved lab tests to determine what their antibody titers are. This should be done after boosting since titers will go down after time. We know that if a patient has lung cancer and they do get infected with SARS-CoV-2 that potentially they could develop serious COVID-19 disease. Besides giving antiviral treatment, it is important that they be closely monitored for symptoms of progression so if they need to be hospitalized it can be done in a prudent manner,” said Dr. Minna, who is director of the Hamon Center for Therapeutic Oncology Research at the University of Texas Southwestern Medical Center.
No clinical details have emerged that might predict which patients have an insufficient response to vaccination. “When we started these studies, a lot of us thought that anyone who did not develop a good antibody response would be weak or sicker. For example, [patients with] late-stage disease, or having had a lot of therapy, or perhaps immune checkpoint blockade. However, none of these things are correlated. The main advice we are giving our lung cancer patients are to get vaccinated, get boosted (double boosted), and just do the smart thing to protect yourself from exposure,” he said.
For example, when traveling on a plane, patients should wear a mask. They should also avoid large indoor events. He also recommended that, following vaccination and boosters, patients seek out CLIA-certified tests to get their titer checked.
“Upon any COVID infection, even if their titer is at or above 80%, patients should see their physician to consider treatment with Paxlovid (nirmatrelvir/ritonavir), which has emergency use authorization. For patients with a lower titer, it’s important to seek out a physician and consider Paxlovid and possibly antibody therapy. But these are individual decisions to be made with your doctor,” Dr. Minna said.
The next important research question is what happens to T-cell immune response following vaccination. “We know that a good cellular immune response is also important in preventing infection and severe infection, but we don’t yet know which persons (with or without cancer) have good T-cell responses. This information will also likely impact what we tell our patients and will add to the antibody data,” he said.
Studies are ongoing to determine specific T-cell responses to mRNA vaccines, and how well those T-cell responses respond to SARS-CoV-2 infection in the laboratory.
according to a new study.
The study was published in the Journal of Clinical Oncology.
“Booster vaccination increased binding and neutralizing antibody titers to Omicron, but antibody titers declined after 3 months. These data highlight the concern for patients with cancer given the rapid spread of SARS-CoV-2 Omicron variant,” wrote the authors, who were led by Rafi Ahmed, PhD, Emory University, Atlanta.
Researchers found that 18% had no detectable antibody at all and active treatment type had no association with vaccine response.
Researchers examined antibody titers among 82 NSCLC patients and 53 healthy volunteers. They collected blood samples longitudinally for analysis. While most patients had binding and neutralizing antibody titers that were comparable with healthy volunteers, 25% had poor responses, which led to six- to sevenfold lower titers than healthy controls. There was no association between worse vaccine responses and history of programmed death–1 monotherapy, chemotherapy, or both in combination. Receipt of a booster vaccine improved binding and neutralizing antibody titers to both the wild type and the Omicron variant, but 2-4 months after the booster there was a five- to sevenfold decrease in neutralizing titers to both the wild type and Omicron variant.
“This study indicates both the need to monitor our patients with lung cancer for response to COVID-19 mRNA vaccines, identify the nonresponders for follow-up and further attempts at immunization, and continue collecting and analyzing clinicodemographic information and biospecimens from our patients,” wrote the authors of an accompanying editorial.
Although the findings reveal potential concerns, the good news is that most patients NSCLC patients do respond normally to COVID-19 vaccination, said John D. Minna, MD, University of Texas Southwestern Medical Center, Dallas, lead author of the editorial.
He offered some advice to physicians. “You can test your patients using currently available [Clinical Laboratory Improvement Amendments]–approved lab tests to determine what their antibody titers are. This should be done after boosting since titers will go down after time. We know that if a patient has lung cancer and they do get infected with SARS-CoV-2 that potentially they could develop serious COVID-19 disease. Besides giving antiviral treatment, it is important that they be closely monitored for symptoms of progression so if they need to be hospitalized it can be done in a prudent manner,” said Dr. Minna, who is director of the Hamon Center for Therapeutic Oncology Research at the University of Texas Southwestern Medical Center.
No clinical details have emerged that might predict which patients have an insufficient response to vaccination. “When we started these studies, a lot of us thought that anyone who did not develop a good antibody response would be weak or sicker. For example, [patients with] late-stage disease, or having had a lot of therapy, or perhaps immune checkpoint blockade. However, none of these things are correlated. The main advice we are giving our lung cancer patients are to get vaccinated, get boosted (double boosted), and just do the smart thing to protect yourself from exposure,” he said.
For example, when traveling on a plane, patients should wear a mask. They should also avoid large indoor events. He also recommended that, following vaccination and boosters, patients seek out CLIA-certified tests to get their titer checked.
“Upon any COVID infection, even if their titer is at or above 80%, patients should see their physician to consider treatment with Paxlovid (nirmatrelvir/ritonavir), which has emergency use authorization. For patients with a lower titer, it’s important to seek out a physician and consider Paxlovid and possibly antibody therapy. But these are individual decisions to be made with your doctor,” Dr. Minna said.
The next important research question is what happens to T-cell immune response following vaccination. “We know that a good cellular immune response is also important in preventing infection and severe infection, but we don’t yet know which persons (with or without cancer) have good T-cell responses. This information will also likely impact what we tell our patients and will add to the antibody data,” he said.
Studies are ongoing to determine specific T-cell responses to mRNA vaccines, and how well those T-cell responses respond to SARS-CoV-2 infection in the laboratory.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Treatment combo shows ‘clinical benefit’ in liver cancer trial
in patients with hepatocellular carcinoma, shows a new study.
While the combination has been shown to be beneficial in renal cell carcinoma and other solid tumor types, it has never before been tested in a phase 3 clinical trial for hepatocellular carcinoma until now.
The new study, published in The Lancet Oncology, included 837 patients from 178 hospital in 32 countries who were enrolled in the study (called COSMIC-312) between December 2018 and August 2020. 432 patients were randomly assigned to receive a combination of cabozantinib (Cabometyx, Exelixis), a tyrosine kinase inhibitor (TKI), and atezolizumab (Tecentriq, Genentech), a PD-L1 inhibitor. While 217 patients were treated with sorafenib (Nexavar, Bayer) alone and 188 patients were treated with cabozantinib.
Clinically meaningful improvements in progression-free survival, increased disease control and lower primary progression were seen in patients who received the cabozantinib and atezolizumab combination therapy over patients who were treated with sorafenib. However, there was no improvement in overall survival.
“The improvement in progression-free survival with cabozantinib plus atezolizumab in this study shows that the combination confers clinical benefit for patients with advanced hepatocellular carcinoma previously untreated with systemic anticancer therapy,” wrote the authors of the study, led by Robin Kate Kelley, MD, a gastrointestinal oncologist with the University of California, San Francisco, and Lorenza Rimassa, MD, a gastrointestinal oncologist with Humanitas University, Milan. “The absence of a benefit in overall survival, along with the availability of atezolizumab in combination with bevacizumab, indicates the need for additional studies to determine if cabozantinib plus atezolizumab would be an appropriate first-line treatment option in select patient populations.”
For symptomatic patients with high disease burden or main portal vein occlusion who are at risk for impending complications, controlling the disease as quickly as possible is vital, the authors wrote. “Underlying chronic liver disease is nearly universal in patients with hepatocellular carcinoma and the risk of gastrointestinal bleeding is high in this population, particularly if portal vein tumor thrombus is present.”
Hepatocellular carcinoma (HCC) is an angiogenic tumor, making it a logical target for TKIs that target vascular endothelial growth factor. The TKI sorafenib was the first to be approved as a first-line treatment for HCC, and since then immune checkpoint inhibitors have been shown to induce durable responses in the first-line setting, but have not improved overall survival in randomized trials.
Study methodology
In the study, after a median follow-up of 15.8 months, median progression-free survival was 6.8 months in the combination group and 4.2 months in the sorafenib group (hazard ratio, 0.63; P = .0012). The median overall survival was 15.4 months in the combination group and 15.5 months in the sorafenib group (not significant). Grade 3-4 adverse events included an increase in ALT, which occurred in 9% of the combination group, 3% of the sorafenib group, and 6% of the cabozantinib only group; hypertension (9%, 8%, and 12%, respectively); an increase in AST increase (9%, 4%, 10%); and palmar-plantar erythrodysesthesia (8%, 8%, 9%). Serious treatment-related adverse events occurred in 18% of patients in the combination arm, 8% in the sorafenib arm, and 13% in the cabozantinib arm.
There were no excess serious bleeding events in the treatment groups containing cabozantinib, compared with sorafenib which is noteworthy because HCC patients are at high risk for gastrointestinal bleeding.
Treatment-related grade 5 events were rare, occurring in 1% (six patients) of the combination group, and in just one patient in both the sorafenib and cabozantinib groups.
Although the results suggest promising clinical benefit, the lack of overall survival benefit limit the implications of these findings. Since atezolizumab combined with bevacizumab is also available for this patient population, more research is needed to determine if cabozantinib plus atezolizumab can become a first-line option.
The study had some limitations: Participants had to have a Child-Pugh class of A, though there was no requirement to assess for fibrosis or cirrhosis. Otherwise there were few barriers to study entry.
The study was sponsored by Exelixis (Alameda) and Ipsen (Boulogne-Billancourt, France).
in patients with hepatocellular carcinoma, shows a new study.
While the combination has been shown to be beneficial in renal cell carcinoma and other solid tumor types, it has never before been tested in a phase 3 clinical trial for hepatocellular carcinoma until now.
The new study, published in The Lancet Oncology, included 837 patients from 178 hospital in 32 countries who were enrolled in the study (called COSMIC-312) between December 2018 and August 2020. 432 patients were randomly assigned to receive a combination of cabozantinib (Cabometyx, Exelixis), a tyrosine kinase inhibitor (TKI), and atezolizumab (Tecentriq, Genentech), a PD-L1 inhibitor. While 217 patients were treated with sorafenib (Nexavar, Bayer) alone and 188 patients were treated with cabozantinib.
Clinically meaningful improvements in progression-free survival, increased disease control and lower primary progression were seen in patients who received the cabozantinib and atezolizumab combination therapy over patients who were treated with sorafenib. However, there was no improvement in overall survival.
“The improvement in progression-free survival with cabozantinib plus atezolizumab in this study shows that the combination confers clinical benefit for patients with advanced hepatocellular carcinoma previously untreated with systemic anticancer therapy,” wrote the authors of the study, led by Robin Kate Kelley, MD, a gastrointestinal oncologist with the University of California, San Francisco, and Lorenza Rimassa, MD, a gastrointestinal oncologist with Humanitas University, Milan. “The absence of a benefit in overall survival, along with the availability of atezolizumab in combination with bevacizumab, indicates the need for additional studies to determine if cabozantinib plus atezolizumab would be an appropriate first-line treatment option in select patient populations.”
For symptomatic patients with high disease burden or main portal vein occlusion who are at risk for impending complications, controlling the disease as quickly as possible is vital, the authors wrote. “Underlying chronic liver disease is nearly universal in patients with hepatocellular carcinoma and the risk of gastrointestinal bleeding is high in this population, particularly if portal vein tumor thrombus is present.”
Hepatocellular carcinoma (HCC) is an angiogenic tumor, making it a logical target for TKIs that target vascular endothelial growth factor. The TKI sorafenib was the first to be approved as a first-line treatment for HCC, and since then immune checkpoint inhibitors have been shown to induce durable responses in the first-line setting, but have not improved overall survival in randomized trials.
Study methodology
In the study, after a median follow-up of 15.8 months, median progression-free survival was 6.8 months in the combination group and 4.2 months in the sorafenib group (hazard ratio, 0.63; P = .0012). The median overall survival was 15.4 months in the combination group and 15.5 months in the sorafenib group (not significant). Grade 3-4 adverse events included an increase in ALT, which occurred in 9% of the combination group, 3% of the sorafenib group, and 6% of the cabozantinib only group; hypertension (9%, 8%, and 12%, respectively); an increase in AST increase (9%, 4%, 10%); and palmar-plantar erythrodysesthesia (8%, 8%, 9%). Serious treatment-related adverse events occurred in 18% of patients in the combination arm, 8% in the sorafenib arm, and 13% in the cabozantinib arm.
There were no excess serious bleeding events in the treatment groups containing cabozantinib, compared with sorafenib which is noteworthy because HCC patients are at high risk for gastrointestinal bleeding.
Treatment-related grade 5 events were rare, occurring in 1% (six patients) of the combination group, and in just one patient in both the sorafenib and cabozantinib groups.
Although the results suggest promising clinical benefit, the lack of overall survival benefit limit the implications of these findings. Since atezolizumab combined with bevacizumab is also available for this patient population, more research is needed to determine if cabozantinib plus atezolizumab can become a first-line option.
The study had some limitations: Participants had to have a Child-Pugh class of A, though there was no requirement to assess for fibrosis or cirrhosis. Otherwise there were few barriers to study entry.
The study was sponsored by Exelixis (Alameda) and Ipsen (Boulogne-Billancourt, France).
in patients with hepatocellular carcinoma, shows a new study.
While the combination has been shown to be beneficial in renal cell carcinoma and other solid tumor types, it has never before been tested in a phase 3 clinical trial for hepatocellular carcinoma until now.
The new study, published in The Lancet Oncology, included 837 patients from 178 hospital in 32 countries who were enrolled in the study (called COSMIC-312) between December 2018 and August 2020. 432 patients were randomly assigned to receive a combination of cabozantinib (Cabometyx, Exelixis), a tyrosine kinase inhibitor (TKI), and atezolizumab (Tecentriq, Genentech), a PD-L1 inhibitor. While 217 patients were treated with sorafenib (Nexavar, Bayer) alone and 188 patients were treated with cabozantinib.
Clinically meaningful improvements in progression-free survival, increased disease control and lower primary progression were seen in patients who received the cabozantinib and atezolizumab combination therapy over patients who were treated with sorafenib. However, there was no improvement in overall survival.
“The improvement in progression-free survival with cabozantinib plus atezolizumab in this study shows that the combination confers clinical benefit for patients with advanced hepatocellular carcinoma previously untreated with systemic anticancer therapy,” wrote the authors of the study, led by Robin Kate Kelley, MD, a gastrointestinal oncologist with the University of California, San Francisco, and Lorenza Rimassa, MD, a gastrointestinal oncologist with Humanitas University, Milan. “The absence of a benefit in overall survival, along with the availability of atezolizumab in combination with bevacizumab, indicates the need for additional studies to determine if cabozantinib plus atezolizumab would be an appropriate first-line treatment option in select patient populations.”
For symptomatic patients with high disease burden or main portal vein occlusion who are at risk for impending complications, controlling the disease as quickly as possible is vital, the authors wrote. “Underlying chronic liver disease is nearly universal in patients with hepatocellular carcinoma and the risk of gastrointestinal bleeding is high in this population, particularly if portal vein tumor thrombus is present.”
Hepatocellular carcinoma (HCC) is an angiogenic tumor, making it a logical target for TKIs that target vascular endothelial growth factor. The TKI sorafenib was the first to be approved as a first-line treatment for HCC, and since then immune checkpoint inhibitors have been shown to induce durable responses in the first-line setting, but have not improved overall survival in randomized trials.
Study methodology
In the study, after a median follow-up of 15.8 months, median progression-free survival was 6.8 months in the combination group and 4.2 months in the sorafenib group (hazard ratio, 0.63; P = .0012). The median overall survival was 15.4 months in the combination group and 15.5 months in the sorafenib group (not significant). Grade 3-4 adverse events included an increase in ALT, which occurred in 9% of the combination group, 3% of the sorafenib group, and 6% of the cabozantinib only group; hypertension (9%, 8%, and 12%, respectively); an increase in AST increase (9%, 4%, 10%); and palmar-plantar erythrodysesthesia (8%, 8%, 9%). Serious treatment-related adverse events occurred in 18% of patients in the combination arm, 8% in the sorafenib arm, and 13% in the cabozantinib arm.
There were no excess serious bleeding events in the treatment groups containing cabozantinib, compared with sorafenib which is noteworthy because HCC patients are at high risk for gastrointestinal bleeding.
Treatment-related grade 5 events were rare, occurring in 1% (six patients) of the combination group, and in just one patient in both the sorafenib and cabozantinib groups.
Although the results suggest promising clinical benefit, the lack of overall survival benefit limit the implications of these findings. Since atezolizumab combined with bevacizumab is also available for this patient population, more research is needed to determine if cabozantinib plus atezolizumab can become a first-line option.
The study had some limitations: Participants had to have a Child-Pugh class of A, though there was no requirement to assess for fibrosis or cirrhosis. Otherwise there were few barriers to study entry.
The study was sponsored by Exelixis (Alameda) and Ipsen (Boulogne-Billancourt, France).
FROM THE LANCET
Taste dysfunction in head and neck cancer due to radiation dose
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
FROM JAMA OTOLARYNGOLOGY–HEAD AND NECK SURGERY
Devices to detect skin cancer: FDA advisers offer mixed views
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.

Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.

Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.
Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.
Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
Many die waiting for `last-chance’ therapy
Some patients with blood cancers for whom all other therapeutic options have been exhausted have one final chance of getting rid of their disease: treatment with chimeric antigen-receptor (CAR) T cells.
Described as a “living drug,” the treatment involves genetically engineering the patient’s own blood cells and reinfusing them back into their system. These CAR T cells then hunt down and destroy cancer cells; in some cases, they manage to eradicate the disease completely.
About half of patients with leukemia or lymphoma and about a third of those with multiple myeloma who receive this treatment have a complete remission and achieve a functional “cure.”
But not all patients who could benefit from this therapy are able to get it. Some are spending months on waiting lists, often deteriorating while they wait. These patients have exhausted all other therapeutic options, and many are facing hospice and death.
The scope of this problem was illustrated by a recent survey of the centers that are certified to deliver this complex therapy.
The survey was led by Yi Lin, MD, PhD, associate professor of medicine at the Mayo Clinic, Rochester, Minn., and medical director for the cellular therapy program. It was published as an abstract at the annual meeting of the American Society of Clinical Oncology recently, although it was not presented there.
“We wanted to find out just how widespread this problem is,” Dr. Lin said, adding: “There had been nothing in the literature thus far about it.”
The team contacted 20 centers across the United States and received responses from 17. Results showed that the median time on the waiting list was 6 months and that only 25% of patients eventually received CAR T-cell therapy. An additional 25% were able to enter a CAR T clinical trial. The remaining 50% of patients either were enrolled in a different type of trial, entered hospice, or died.
For patient selection, all centers reported using a committee of experienced physicians to ensure consistency. They employed different ethical principles for selection. Some centers sought to maximize the total benefit, such as selecting the patients most likely to achieve leukapheresis or a clinical response, while others based their decisions on the time patients spent on waiting list or gave priority to the patients who were the “worst off” with the most limited therapeutic options.
Shortage affecting mostly myeloma patients
The shortages in CAR T-cell therapies primarily involve the products used for patients with multiple myeloma.
The problem has not, as yet, noticeably spilled over to lymphoma and leukemia treatments, which use a slightly different type of CAR T-cell therapy (it targets CD19, whereas the cell therapies used for myeloma target BCMA).
“We have backlog of myeloma patients who don’t have access,” said Nina Shah, MD, a hematologist and professor of medicine at the University of California, San Francisco. “We have only four slots for the two myeloma products but about 50-60 eligible patients.”
Long waiting times for CAR T cells for myeloma have been an issue ever since the first of these products appeared on the market: idecabtagene vicleucel (ide-cel; Abecma), developed by Bluebird Bio and Bristol-Myers Squibb. “As soon as it became available in March 2021, we had people waiting and limits on our access to it,” Dr. Shah said.
A second CAR T-cell therapy for myeloma, ciltacabtagene autoleucel (cilta-cel, Carvykti), developed by Janssen and Legend Biotech, received approval in February 2022. While that helped provide centers with a few more slots, it wasn’t sufficient to cut waiting times, and the demand for these myeloma therapies continues to outstrip the capacity to produce CAR-T products in a timely manner.
“For myeloma, the demand is very high, as most patients are not cured from any other existing myeloma therapies, and most patients will make it to fifth-line therapy where the two CAR T-cell products are approved right now,” said Krina K. Patel, MD, medical director of the department of lymphoma/myeloma in the division of cancer medicine at the University of Texas MD Anderson Cancer Center, Houston.
“We likely have 10 eligible CAR-T myeloma patients each month at our center,” she said, “but were getting two slots per month for the past 8 months, and now are getting four slots a month.”
“Our clinic has also experienced the impact of the low number of manufacturing slots offered to each cancer center for some CAR T-cell products,” said David Maloney, MD, PhD, medical director, Cellular Immunotherapy and Bezos Family Immunotherapy Clinic, Seattle Cancer Care Alliance.
He noted that, as with other cancer centers, for multiple myeloma they are provided a specific number of manufacturing slots for each treatment. “Our providers discuss which patients are most appropriate for available slots for that month,” said Dr. Maloney.
“Additionally, juggling patient schedules may be required to address the extended manufacturing time for some products. In some cases, clinical trials may be available in a more timely fashion for appropriate patients, and in some cases, switching to an alternative product is possible,” he commented.
Complex causes behind bottleneck
The cause of the current bottleneck for myeloma patients is complex. It stems from a shortage of raw materials and supply chain restraints, among other things.
While the biggest impact of shortages has been on patients with multiple myeloma, Dr. Patel pointed out that these constraints are also affecting patients with lymphoma at her institution, but to a lesser degree.
“This is multifactorial as to why, but most of the issues arise from manufacturing,” Dr. Patel said in an interview. “Initially, the FDA limited how many slots each new product could have per month, then there was a viral vector shortage, and then the quality-control process the FDA requires takes longer than the manufacturing of the cells actually do.”
On top of that, “we have about a 5% manufacturing fail rate so far,” she added. Such failures occur when the cells taken from a patient cannot be converted into CAR T cells for therapy.
Matthew J. Frigault, MD, from the Center for Cellular Therapies, Mass General Cancer Center, Boston, explained that the growing excitement about the potential for cellular therapy and recent approvals for these products for use in earlier lines of treatment have increased demand for them.
There are also problems regarding supply. Manufacture and delivery of CAR T is complicated and takes time to scale up, Dr. Frigault pointed out. “Therefore, we are seeing limited access, more so for the BCMA-directed therapies [which are used for myeloma].”
The shortages and delays likely involve two main factors. “For the newer indications, there is a significant backlog of patients who have been waiting for these therapies and have not been able to access them in the clinical trial setting, and manufacturing is extremely complicated and not easily scaled up,” he said.
“That being said, manufacturers are trying to increase the number of available manufacturing slots and decrease the time needed to manufacture cells,” Dr. Frigault commented.
Delays in access to myeloma CAR T-cell therapy are also affecting patient care at Fox Chase Cancer Center in Philadelphia. “We have had about one slot every 2 months for Abecma,” noted Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase. “For Carvykti, there are only 32 certified centers in [the] U.S., and access is very limited.”
Dr. Fung explained that they have had to offer alternative treatments to many of their patients. “There are rumors that there’s shortage in obtaining raw materials, such as the virus used for transduction, although we have not encountered any problems in other CAR T products used for lymphomas.”
Pharma companies trying to meet the demand
This news organization reached out to the manufacturers of CAR T products. All have reported that they are doing what they feasibly can to ramp up production.
“The complexity of delivering CAR T-cell therapies is unlike any other traditional biologic or small-molecule medicine, using a patient’s own cells to start a highly sophisticated and personalized manufacturing process,” commented a spokesperson for BMS, which has two CAR T-cell products currently on the market.
“In this nascent field of cell therapy, we continue to evolve every day, addressing supply and manufacturing challenges head on by applying key learnings across our three state-of-the-art cell therapy facilities and two new facilities in progress.
“We have been encouraged by a steady increase in our manufacturing capacity, and we continue efforts to ramp up further to meet the demand for our cell therapies,” the BMS spokesperson commented. “We have already seen improvements in the stabilization of vector supply and expect additional improvements in capacity in the second half of 2022.”
Novartis said much the same thing. They have a “comprehensive, integrated global CAR-T manufacturing footprint that strengthens the flexibility, resilience, and sustainability of the Novartis manufacturing and supply chain. Together with an improved manufacturing process, we are confident in our ability to meet patient demand with timely delivery,” according to a Novartis spokesperson.
The spokesperson also pointed out that the company has continuously incorporated process improvements that have significantly increased manufacturing capacity and success rates for patients in need of CAR T cells.
“Data presented at [the] American Society of Hematology annual meeting in 2021 showed the Novartis Morris Plains facility, our flagship CAR T manufacturing site, had commercial manufacturing and shipping success rates of 96% and 99%, respectively, between January and August 2021,” according to the spokesperson.
Legend and Janssen, the companies behind Carvykti, one of the two approved cell products for myeloma, which launched earlier in 2022, said that they have continued to activate certified treatment centers in a phased approach that will enable them to expand availability throughout 2022 and beyond.
“This phased approach was designed to ensure the highest level of predictability and reliability for the patient and the certified treatment centers,” the spokesperson said. “We understand the urgency for patients in need of Carvyki and are committed to doing everything we can to accelerate our ability to deliver this important cell therapy in a reliable and timely manner.”
With regard to the industry-wide supply shortage of lentivirus, Legend and Janssen say they have put in place multiple processes to address the shortage, “including enhancing our own internal manufacturing capabilities of this essential drug substance, to ensure sufficient and sustained supply.”
Incredibly exciting potential
Given the immense potential of CAR T-cell therapy, the supply shortage that myeloma patients are experiencing is all the more poignant and distressing. While not everyone benefits, some patients for whom every other therapy failed and who were facing hospice have had dramatic results.
“Incredibly exciting with unbelievable potential” was how one expert described these new therapies when the first product was about to enter the marketplace. Since then, six CAR T-cell therapies have received regulatory approval for an ever-increasing range of hematologic malignancies.
But these CAR T-cell therapies have their own set of adverse events, which can be serious and even life-threatening. In addition, not all patients become cancer free, although long-term data are impressive.
A study that included one of the longest follow-ups to date was reported at the 2020 annual meeting of the American Society of Clinical Oncology. The researchers reported that remissions lasted over 9 years for patients with relapsed/refractory B-cell lymphoma or chronic lymphocytic leukemia who underwent treatment with Kite’s axicaptagene cilleucel (Yescarta). This review included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved for 54% of patients, and partial remission was achieved for 22%.
The results with CAR T-cell therapy in multiple myeloma are not quite as impressive, but even so, the clinical data that supported the approval of Abecma showed that a third of patients, who had previously received a median of six prior therapies, achieved a complete response.
At the time of the Abecma approval, the lead investigator of the study, Nikhil Munshi, MD, of Dana-Farber Cancer Institute, Boston, commented: “The results of this trial represent a true turning point in the treatment of this disease. In my 30 years of treating myeloma, I have not seen any other therapy as effective in this group of patients.”
A version of this article first appeared on Medscape.com.
Some patients with blood cancers for whom all other therapeutic options have been exhausted have one final chance of getting rid of their disease: treatment with chimeric antigen-receptor (CAR) T cells.
Described as a “living drug,” the treatment involves genetically engineering the patient’s own blood cells and reinfusing them back into their system. These CAR T cells then hunt down and destroy cancer cells; in some cases, they manage to eradicate the disease completely.
About half of patients with leukemia or lymphoma and about a third of those with multiple myeloma who receive this treatment have a complete remission and achieve a functional “cure.”
But not all patients who could benefit from this therapy are able to get it. Some are spending months on waiting lists, often deteriorating while they wait. These patients have exhausted all other therapeutic options, and many are facing hospice and death.
The scope of this problem was illustrated by a recent survey of the centers that are certified to deliver this complex therapy.
The survey was led by Yi Lin, MD, PhD, associate professor of medicine at the Mayo Clinic, Rochester, Minn., and medical director for the cellular therapy program. It was published as an abstract at the annual meeting of the American Society of Clinical Oncology recently, although it was not presented there.
“We wanted to find out just how widespread this problem is,” Dr. Lin said, adding: “There had been nothing in the literature thus far about it.”
The team contacted 20 centers across the United States and received responses from 17. Results showed that the median time on the waiting list was 6 months and that only 25% of patients eventually received CAR T-cell therapy. An additional 25% were able to enter a CAR T clinical trial. The remaining 50% of patients either were enrolled in a different type of trial, entered hospice, or died.
For patient selection, all centers reported using a committee of experienced physicians to ensure consistency. They employed different ethical principles for selection. Some centers sought to maximize the total benefit, such as selecting the patients most likely to achieve leukapheresis or a clinical response, while others based their decisions on the time patients spent on waiting list or gave priority to the patients who were the “worst off” with the most limited therapeutic options.
Shortage affecting mostly myeloma patients
The shortages in CAR T-cell therapies primarily involve the products used for patients with multiple myeloma.
The problem has not, as yet, noticeably spilled over to lymphoma and leukemia treatments, which use a slightly different type of CAR T-cell therapy (it targets CD19, whereas the cell therapies used for myeloma target BCMA).
“We have backlog of myeloma patients who don’t have access,” said Nina Shah, MD, a hematologist and professor of medicine at the University of California, San Francisco. “We have only four slots for the two myeloma products but about 50-60 eligible patients.”
Long waiting times for CAR T cells for myeloma have been an issue ever since the first of these products appeared on the market: idecabtagene vicleucel (ide-cel; Abecma), developed by Bluebird Bio and Bristol-Myers Squibb. “As soon as it became available in March 2021, we had people waiting and limits on our access to it,” Dr. Shah said.
A second CAR T-cell therapy for myeloma, ciltacabtagene autoleucel (cilta-cel, Carvykti), developed by Janssen and Legend Biotech, received approval in February 2022. While that helped provide centers with a few more slots, it wasn’t sufficient to cut waiting times, and the demand for these myeloma therapies continues to outstrip the capacity to produce CAR-T products in a timely manner.
“For myeloma, the demand is very high, as most patients are not cured from any other existing myeloma therapies, and most patients will make it to fifth-line therapy where the two CAR T-cell products are approved right now,” said Krina K. Patel, MD, medical director of the department of lymphoma/myeloma in the division of cancer medicine at the University of Texas MD Anderson Cancer Center, Houston.
“We likely have 10 eligible CAR-T myeloma patients each month at our center,” she said, “but were getting two slots per month for the past 8 months, and now are getting four slots a month.”
“Our clinic has also experienced the impact of the low number of manufacturing slots offered to each cancer center for some CAR T-cell products,” said David Maloney, MD, PhD, medical director, Cellular Immunotherapy and Bezos Family Immunotherapy Clinic, Seattle Cancer Care Alliance.
He noted that, as with other cancer centers, for multiple myeloma they are provided a specific number of manufacturing slots for each treatment. “Our providers discuss which patients are most appropriate for available slots for that month,” said Dr. Maloney.
“Additionally, juggling patient schedules may be required to address the extended manufacturing time for some products. In some cases, clinical trials may be available in a more timely fashion for appropriate patients, and in some cases, switching to an alternative product is possible,” he commented.
Complex causes behind bottleneck
The cause of the current bottleneck for myeloma patients is complex. It stems from a shortage of raw materials and supply chain restraints, among other things.
While the biggest impact of shortages has been on patients with multiple myeloma, Dr. Patel pointed out that these constraints are also affecting patients with lymphoma at her institution, but to a lesser degree.
“This is multifactorial as to why, but most of the issues arise from manufacturing,” Dr. Patel said in an interview. “Initially, the FDA limited how many slots each new product could have per month, then there was a viral vector shortage, and then the quality-control process the FDA requires takes longer than the manufacturing of the cells actually do.”
On top of that, “we have about a 5% manufacturing fail rate so far,” she added. Such failures occur when the cells taken from a patient cannot be converted into CAR T cells for therapy.
Matthew J. Frigault, MD, from the Center for Cellular Therapies, Mass General Cancer Center, Boston, explained that the growing excitement about the potential for cellular therapy and recent approvals for these products for use in earlier lines of treatment have increased demand for them.
There are also problems regarding supply. Manufacture and delivery of CAR T is complicated and takes time to scale up, Dr. Frigault pointed out. “Therefore, we are seeing limited access, more so for the BCMA-directed therapies [which are used for myeloma].”
The shortages and delays likely involve two main factors. “For the newer indications, there is a significant backlog of patients who have been waiting for these therapies and have not been able to access them in the clinical trial setting, and manufacturing is extremely complicated and not easily scaled up,” he said.
“That being said, manufacturers are trying to increase the number of available manufacturing slots and decrease the time needed to manufacture cells,” Dr. Frigault commented.
Delays in access to myeloma CAR T-cell therapy are also affecting patient care at Fox Chase Cancer Center in Philadelphia. “We have had about one slot every 2 months for Abecma,” noted Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase. “For Carvykti, there are only 32 certified centers in [the] U.S., and access is very limited.”
Dr. Fung explained that they have had to offer alternative treatments to many of their patients. “There are rumors that there’s shortage in obtaining raw materials, such as the virus used for transduction, although we have not encountered any problems in other CAR T products used for lymphomas.”
Pharma companies trying to meet the demand
This news organization reached out to the manufacturers of CAR T products. All have reported that they are doing what they feasibly can to ramp up production.
“The complexity of delivering CAR T-cell therapies is unlike any other traditional biologic or small-molecule medicine, using a patient’s own cells to start a highly sophisticated and personalized manufacturing process,” commented a spokesperson for BMS, which has two CAR T-cell products currently on the market.
“In this nascent field of cell therapy, we continue to evolve every day, addressing supply and manufacturing challenges head on by applying key learnings across our three state-of-the-art cell therapy facilities and two new facilities in progress.
“We have been encouraged by a steady increase in our manufacturing capacity, and we continue efforts to ramp up further to meet the demand for our cell therapies,” the BMS spokesperson commented. “We have already seen improvements in the stabilization of vector supply and expect additional improvements in capacity in the second half of 2022.”
Novartis said much the same thing. They have a “comprehensive, integrated global CAR-T manufacturing footprint that strengthens the flexibility, resilience, and sustainability of the Novartis manufacturing and supply chain. Together with an improved manufacturing process, we are confident in our ability to meet patient demand with timely delivery,” according to a Novartis spokesperson.
The spokesperson also pointed out that the company has continuously incorporated process improvements that have significantly increased manufacturing capacity and success rates for patients in need of CAR T cells.
“Data presented at [the] American Society of Hematology annual meeting in 2021 showed the Novartis Morris Plains facility, our flagship CAR T manufacturing site, had commercial manufacturing and shipping success rates of 96% and 99%, respectively, between January and August 2021,” according to the spokesperson.
Legend and Janssen, the companies behind Carvykti, one of the two approved cell products for myeloma, which launched earlier in 2022, said that they have continued to activate certified treatment centers in a phased approach that will enable them to expand availability throughout 2022 and beyond.
“This phased approach was designed to ensure the highest level of predictability and reliability for the patient and the certified treatment centers,” the spokesperson said. “We understand the urgency for patients in need of Carvyki and are committed to doing everything we can to accelerate our ability to deliver this important cell therapy in a reliable and timely manner.”
With regard to the industry-wide supply shortage of lentivirus, Legend and Janssen say they have put in place multiple processes to address the shortage, “including enhancing our own internal manufacturing capabilities of this essential drug substance, to ensure sufficient and sustained supply.”
Incredibly exciting potential
Given the immense potential of CAR T-cell therapy, the supply shortage that myeloma patients are experiencing is all the more poignant and distressing. While not everyone benefits, some patients for whom every other therapy failed and who were facing hospice have had dramatic results.
“Incredibly exciting with unbelievable potential” was how one expert described these new therapies when the first product was about to enter the marketplace. Since then, six CAR T-cell therapies have received regulatory approval for an ever-increasing range of hematologic malignancies.
But these CAR T-cell therapies have their own set of adverse events, which can be serious and even life-threatening. In addition, not all patients become cancer free, although long-term data are impressive.
A study that included one of the longest follow-ups to date was reported at the 2020 annual meeting of the American Society of Clinical Oncology. The researchers reported that remissions lasted over 9 years for patients with relapsed/refractory B-cell lymphoma or chronic lymphocytic leukemia who underwent treatment with Kite’s axicaptagene cilleucel (Yescarta). This review included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved for 54% of patients, and partial remission was achieved for 22%.
The results with CAR T-cell therapy in multiple myeloma are not quite as impressive, but even so, the clinical data that supported the approval of Abecma showed that a third of patients, who had previously received a median of six prior therapies, achieved a complete response.
At the time of the Abecma approval, the lead investigator of the study, Nikhil Munshi, MD, of Dana-Farber Cancer Institute, Boston, commented: “The results of this trial represent a true turning point in the treatment of this disease. In my 30 years of treating myeloma, I have not seen any other therapy as effective in this group of patients.”
A version of this article first appeared on Medscape.com.
Some patients with blood cancers for whom all other therapeutic options have been exhausted have one final chance of getting rid of their disease: treatment with chimeric antigen-receptor (CAR) T cells.
Described as a “living drug,” the treatment involves genetically engineering the patient’s own blood cells and reinfusing them back into their system. These CAR T cells then hunt down and destroy cancer cells; in some cases, they manage to eradicate the disease completely.
About half of patients with leukemia or lymphoma and about a third of those with multiple myeloma who receive this treatment have a complete remission and achieve a functional “cure.”
But not all patients who could benefit from this therapy are able to get it. Some are spending months on waiting lists, often deteriorating while they wait. These patients have exhausted all other therapeutic options, and many are facing hospice and death.
The scope of this problem was illustrated by a recent survey of the centers that are certified to deliver this complex therapy.
The survey was led by Yi Lin, MD, PhD, associate professor of medicine at the Mayo Clinic, Rochester, Minn., and medical director for the cellular therapy program. It was published as an abstract at the annual meeting of the American Society of Clinical Oncology recently, although it was not presented there.
“We wanted to find out just how widespread this problem is,” Dr. Lin said, adding: “There had been nothing in the literature thus far about it.”
The team contacted 20 centers across the United States and received responses from 17. Results showed that the median time on the waiting list was 6 months and that only 25% of patients eventually received CAR T-cell therapy. An additional 25% were able to enter a CAR T clinical trial. The remaining 50% of patients either were enrolled in a different type of trial, entered hospice, or died.
For patient selection, all centers reported using a committee of experienced physicians to ensure consistency. They employed different ethical principles for selection. Some centers sought to maximize the total benefit, such as selecting the patients most likely to achieve leukapheresis or a clinical response, while others based their decisions on the time patients spent on waiting list or gave priority to the patients who were the “worst off” with the most limited therapeutic options.
Shortage affecting mostly myeloma patients
The shortages in CAR T-cell therapies primarily involve the products used for patients with multiple myeloma.
The problem has not, as yet, noticeably spilled over to lymphoma and leukemia treatments, which use a slightly different type of CAR T-cell therapy (it targets CD19, whereas the cell therapies used for myeloma target BCMA).
“We have backlog of myeloma patients who don’t have access,” said Nina Shah, MD, a hematologist and professor of medicine at the University of California, San Francisco. “We have only four slots for the two myeloma products but about 50-60 eligible patients.”
Long waiting times for CAR T cells for myeloma have been an issue ever since the first of these products appeared on the market: idecabtagene vicleucel (ide-cel; Abecma), developed by Bluebird Bio and Bristol-Myers Squibb. “As soon as it became available in March 2021, we had people waiting and limits on our access to it,” Dr. Shah said.
A second CAR T-cell therapy for myeloma, ciltacabtagene autoleucel (cilta-cel, Carvykti), developed by Janssen and Legend Biotech, received approval in February 2022. While that helped provide centers with a few more slots, it wasn’t sufficient to cut waiting times, and the demand for these myeloma therapies continues to outstrip the capacity to produce CAR-T products in a timely manner.
“For myeloma, the demand is very high, as most patients are not cured from any other existing myeloma therapies, and most patients will make it to fifth-line therapy where the two CAR T-cell products are approved right now,” said Krina K. Patel, MD, medical director of the department of lymphoma/myeloma in the division of cancer medicine at the University of Texas MD Anderson Cancer Center, Houston.
“We likely have 10 eligible CAR-T myeloma patients each month at our center,” she said, “but were getting two slots per month for the past 8 months, and now are getting four slots a month.”
“Our clinic has also experienced the impact of the low number of manufacturing slots offered to each cancer center for some CAR T-cell products,” said David Maloney, MD, PhD, medical director, Cellular Immunotherapy and Bezos Family Immunotherapy Clinic, Seattle Cancer Care Alliance.
He noted that, as with other cancer centers, for multiple myeloma they are provided a specific number of manufacturing slots for each treatment. “Our providers discuss which patients are most appropriate for available slots for that month,” said Dr. Maloney.
“Additionally, juggling patient schedules may be required to address the extended manufacturing time for some products. In some cases, clinical trials may be available in a more timely fashion for appropriate patients, and in some cases, switching to an alternative product is possible,” he commented.
Complex causes behind bottleneck
The cause of the current bottleneck for myeloma patients is complex. It stems from a shortage of raw materials and supply chain restraints, among other things.
While the biggest impact of shortages has been on patients with multiple myeloma, Dr. Patel pointed out that these constraints are also affecting patients with lymphoma at her institution, but to a lesser degree.
“This is multifactorial as to why, but most of the issues arise from manufacturing,” Dr. Patel said in an interview. “Initially, the FDA limited how many slots each new product could have per month, then there was a viral vector shortage, and then the quality-control process the FDA requires takes longer than the manufacturing of the cells actually do.”
On top of that, “we have about a 5% manufacturing fail rate so far,” she added. Such failures occur when the cells taken from a patient cannot be converted into CAR T cells for therapy.
Matthew J. Frigault, MD, from the Center for Cellular Therapies, Mass General Cancer Center, Boston, explained that the growing excitement about the potential for cellular therapy and recent approvals for these products for use in earlier lines of treatment have increased demand for them.
There are also problems regarding supply. Manufacture and delivery of CAR T is complicated and takes time to scale up, Dr. Frigault pointed out. “Therefore, we are seeing limited access, more so for the BCMA-directed therapies [which are used for myeloma].”
The shortages and delays likely involve two main factors. “For the newer indications, there is a significant backlog of patients who have been waiting for these therapies and have not been able to access them in the clinical trial setting, and manufacturing is extremely complicated and not easily scaled up,” he said.
“That being said, manufacturers are trying to increase the number of available manufacturing slots and decrease the time needed to manufacture cells,” Dr. Frigault commented.
Delays in access to myeloma CAR T-cell therapy are also affecting patient care at Fox Chase Cancer Center in Philadelphia. “We have had about one slot every 2 months for Abecma,” noted Henry Fung, MD, chair of the department of bone marrow transplant and cellular therapies at Fox Chase. “For Carvykti, there are only 32 certified centers in [the] U.S., and access is very limited.”
Dr. Fung explained that they have had to offer alternative treatments to many of their patients. “There are rumors that there’s shortage in obtaining raw materials, such as the virus used for transduction, although we have not encountered any problems in other CAR T products used for lymphomas.”
Pharma companies trying to meet the demand
This news organization reached out to the manufacturers of CAR T products. All have reported that they are doing what they feasibly can to ramp up production.
“The complexity of delivering CAR T-cell therapies is unlike any other traditional biologic or small-molecule medicine, using a patient’s own cells to start a highly sophisticated and personalized manufacturing process,” commented a spokesperson for BMS, which has two CAR T-cell products currently on the market.
“In this nascent field of cell therapy, we continue to evolve every day, addressing supply and manufacturing challenges head on by applying key learnings across our three state-of-the-art cell therapy facilities and two new facilities in progress.
“We have been encouraged by a steady increase in our manufacturing capacity, and we continue efforts to ramp up further to meet the demand for our cell therapies,” the BMS spokesperson commented. “We have already seen improvements in the stabilization of vector supply and expect additional improvements in capacity in the second half of 2022.”
Novartis said much the same thing. They have a “comprehensive, integrated global CAR-T manufacturing footprint that strengthens the flexibility, resilience, and sustainability of the Novartis manufacturing and supply chain. Together with an improved manufacturing process, we are confident in our ability to meet patient demand with timely delivery,” according to a Novartis spokesperson.
The spokesperson also pointed out that the company has continuously incorporated process improvements that have significantly increased manufacturing capacity and success rates for patients in need of CAR T cells.
“Data presented at [the] American Society of Hematology annual meeting in 2021 showed the Novartis Morris Plains facility, our flagship CAR T manufacturing site, had commercial manufacturing and shipping success rates of 96% and 99%, respectively, between January and August 2021,” according to the spokesperson.
Legend and Janssen, the companies behind Carvykti, one of the two approved cell products for myeloma, which launched earlier in 2022, said that they have continued to activate certified treatment centers in a phased approach that will enable them to expand availability throughout 2022 and beyond.
“This phased approach was designed to ensure the highest level of predictability and reliability for the patient and the certified treatment centers,” the spokesperson said. “We understand the urgency for patients in need of Carvyki and are committed to doing everything we can to accelerate our ability to deliver this important cell therapy in a reliable and timely manner.”
With regard to the industry-wide supply shortage of lentivirus, Legend and Janssen say they have put in place multiple processes to address the shortage, “including enhancing our own internal manufacturing capabilities of this essential drug substance, to ensure sufficient and sustained supply.”
Incredibly exciting potential
Given the immense potential of CAR T-cell therapy, the supply shortage that myeloma patients are experiencing is all the more poignant and distressing. While not everyone benefits, some patients for whom every other therapy failed and who were facing hospice have had dramatic results.
“Incredibly exciting with unbelievable potential” was how one expert described these new therapies when the first product was about to enter the marketplace. Since then, six CAR T-cell therapies have received regulatory approval for an ever-increasing range of hematologic malignancies.
But these CAR T-cell therapies have their own set of adverse events, which can be serious and even life-threatening. In addition, not all patients become cancer free, although long-term data are impressive.
A study that included one of the longest follow-ups to date was reported at the 2020 annual meeting of the American Society of Clinical Oncology. The researchers reported that remissions lasted over 9 years for patients with relapsed/refractory B-cell lymphoma or chronic lymphocytic leukemia who underwent treatment with Kite’s axicaptagene cilleucel (Yescarta). This review included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved for 54% of patients, and partial remission was achieved for 22%.
The results with CAR T-cell therapy in multiple myeloma are not quite as impressive, but even so, the clinical data that supported the approval of Abecma showed that a third of patients, who had previously received a median of six prior therapies, achieved a complete response.
At the time of the Abecma approval, the lead investigator of the study, Nikhil Munshi, MD, of Dana-Farber Cancer Institute, Boston, commented: “The results of this trial represent a true turning point in the treatment of this disease. In my 30 years of treating myeloma, I have not seen any other therapy as effective in this group of patients.”
A version of this article first appeared on Medscape.com.