User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Gender and Patient Satisfaction in a Veterans Health Administration Outpatient Chemotherapy Unit
Gender differences in patient satisfaction with medical care have been evaluated in multiple settings; however, studies specific to the unique population of women veterans with cancer are lacking. Women are reported to value privacy, psychosocial support, and communication to a higher degree compared with men.1 Factors affecting satisfaction include the following: discomfort in sharing treatment rooms with the opposite gender, a desire for privacy with treatment and restroom use, anatomic or illness differences, and a personal history of abuse.2-4 Regrettably, up to 1 in 3 women in the United States are victims of sexual trauma in their lifetimes, and up to 1 in 4 women in the military are victims of military sexual trauma. Incidence in both settings is suspected to be higher due to underreporting.5,6
Chemotherapy treatment units are often uniquely designed as an open space, with several patients sharing a treatment area. The design reduces isolation and facilitates quick nurse-patient access during potentially toxic treatments known to have frequent adverse effects. Data suggest that nursing staff prefer open models to facilitate quick patient assessments and interventions as needed; however, patients and families prefer private treatment rooms, especially among women patients or those receiving longer infusions.7
The Veterans Health Administration (VHA) patient population is male predominant, comprised only of 10% female patients.8 Although the proportion of female patients in the VHA is expected to rise annually to about 16% by 2043, the low percentage of female veterans will persist for the foreseeable future.8 This low percentage of female veterans is reflected in the Veterans Affairs Portland Health Care System (VAPHCS) cancer patient population and in the use of the chemotherapy infusion unit, which is used for the ambulatory treatment of veterans undergoing cancer therapy.
The VHA has previously explored gender differences in health care, such as with cardiovascular disease, transgender care, and access to mental health.9-11 However, to the best of our knowledge, no analysis has explored gender differences within the outpatient cancer treatment experience. Patient satisfaction with outpatient cancer care may be magnified in the VHA setting due to the uniquely unequal gender populations, shared treatment space design, and high incidence of sexual abuse among women veterans. Given this, we aimed to identify gender-related preferences in outpatient cancer care in our chemotherapy infusion unit.
In our study, we used the terms male and female to reflect statistical data from the literature or labeled data from the electronic health record (EHR); whereas the terms men and women were used to describe and encompass the cultural implications and context of gender.12
Methods
This study was designated as a quality improvement (QI) project by the VAPHCS research office and Institutional Review Board in accordance with VHA policies.
The VAPHCS outpatient chemotherapy infusion unit is designed with 6 rooms for chemotherapy administration. One room is a large open space with 6 chairs for patients. The other rooms are smaller with glass dividers between the rooms, and 3 chairs inside each for patients. There are 2 private bathrooms, each gender neutral. Direct patient care is provided by physicians, nurse practitioners (NPs), infusion unit nurses, and nurse coordinators. Men represent the majority of hematology and oncology physicians (13 of 20 total: 5 women fellow physicians and 2 women attending physicians), and 2 of 4 NPs. Women represent 10 of 12 infusion unit and cancer coordinator nurses. We used the VHA Computerized Patient Record System (CPRS) EHR, to create a list of veterans treated at the VAPHCS outpatient chemotherapy infusion unit for a 2-year period (January 1, 2018, to December 31, 2020).
Male and female patient lists were first generated based on CPRS categorization. We identified all female veterans treated in the ambulatory infusion unit during the study period. Male patients were then chosen at random, recording the most recent names for each year until a matched number per year compared with the female cohort was reached. Patients were recorded only once even though they had multiple infusion unit visits. Patients were excluded who were deceased, on hospice care, lost to follow-up, could not be reached by phone, refused to take the survey, had undeliverable email addresses, or lacked internet or email access.
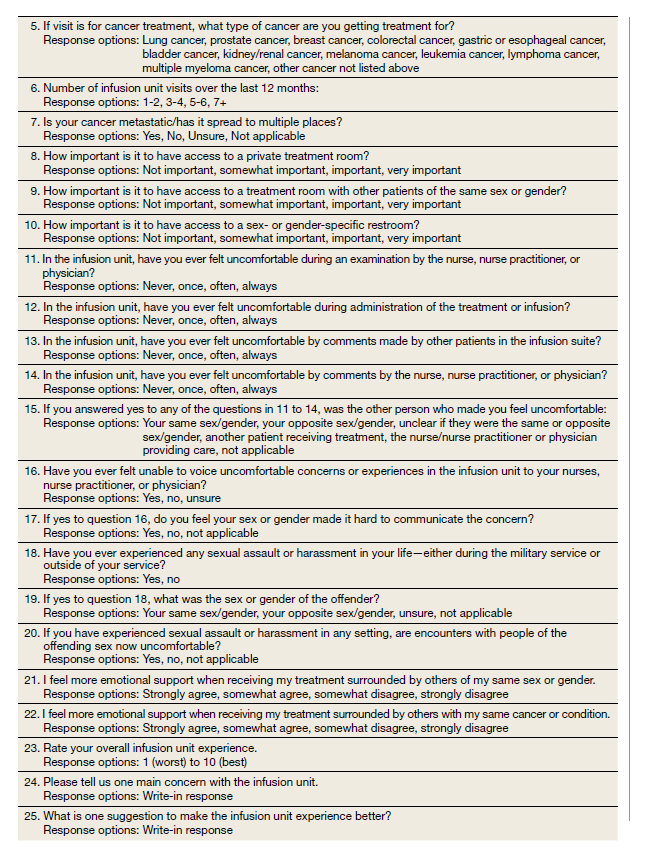
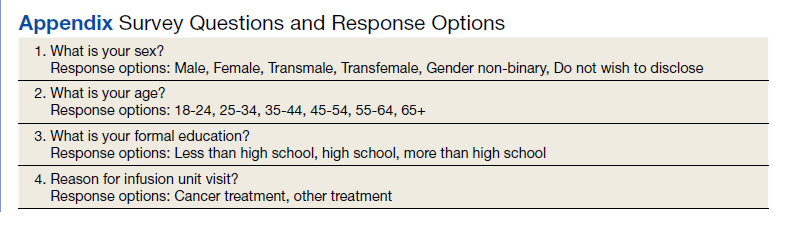
After filing the appropriate request through the VAPHCS Institutional Review Board committee in January 2021, patient records were reviewed for demographics data, contact information, and infusion treatment history. The survey was then conducted over a 2-week period during January and February 2021. Each patient was invited by phone to complete a 25-question anonymous online survey. The survey questions were created from patient-relayed experiences, then modeled into survey questions in a format similar to other patient satisfaction questionnaires described in cancer care and gender differences.2,13,14 The survey included self-identification of gender and was multiple choice for all except 2 questions, which allowed an open-ended response (Appendix). Only 1 answer per question was permitted. Only 1 survey link was sent to each veteran who gave permission for the survey. To protect anonymity for the small patient population, we excluded those identifying as gender nonbinary or transgender.
Statistical Analysis
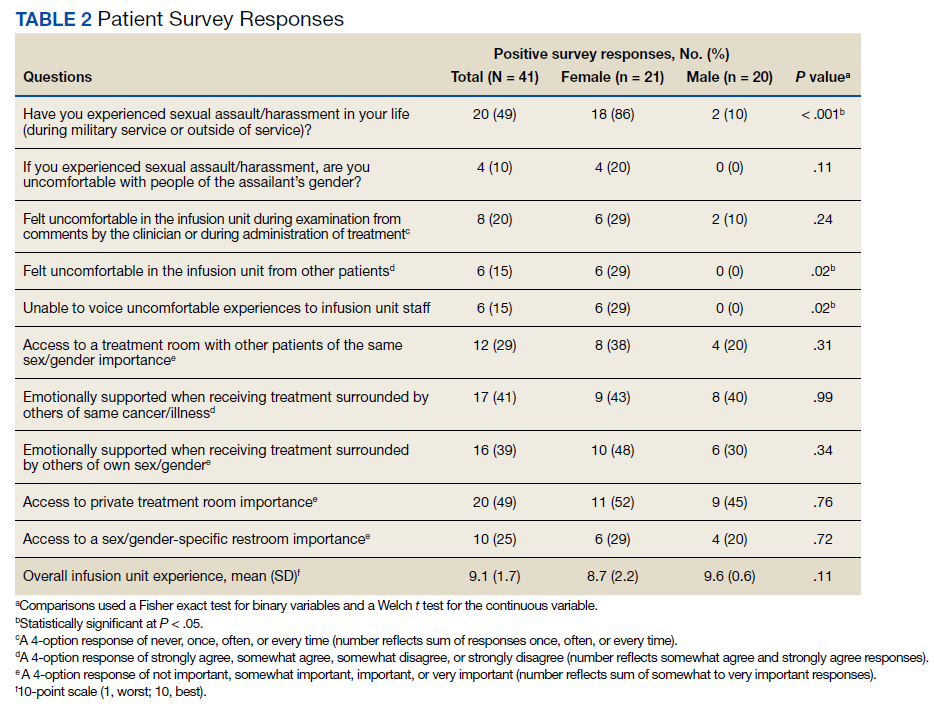
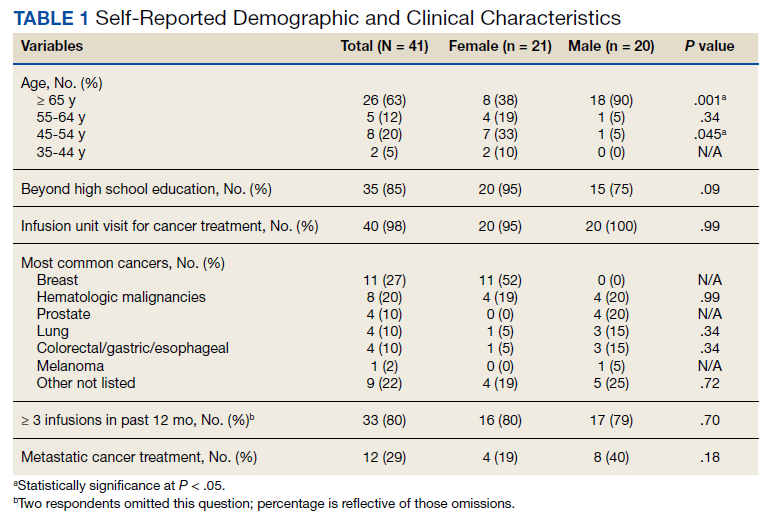
Patient, disease, and treatment features are separated by male and female cohorts to reflect information from the EHR (Table 1). Survey percentages were calculated to reflect the affirmative response of the question asked (Table 2). Questions with answer options of not important, minimally important, important, or very important were calculated to reflect the sum of any importance in both cohorts. Questions with answer options of never, once, often, or every time were calculated to reflect any occurrence (sum of once, often, or every time) in both patient groups. Questions with answer options of strongly agree, somewhat agree, somewhat disagree, and strongly disagree were calculated to reflect any agreement (somewhat agree and strongly agree summed together) for both groups. Comparisons between cohorts were then conducted using a Fisher exact test. A Welch t test was used to calculate the significance of the continuous variable and overall ranking of the infusion unit experience between groups.
Results
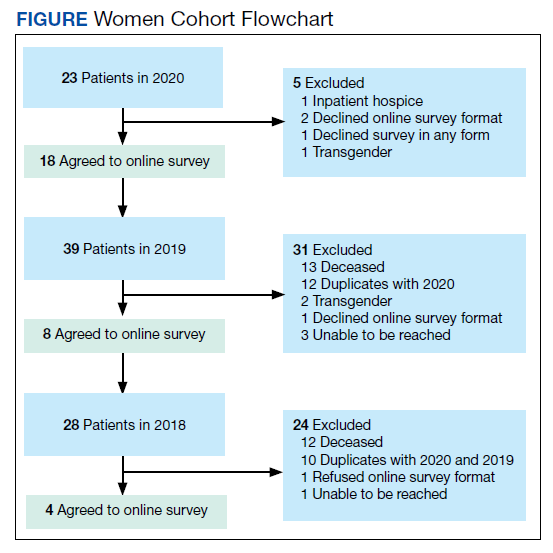
In 2020, 414 individual patients were treated at the VAPAHCS outpatient infusion unit. Of these, 23 (5.6%) were female, and 18 agreed to take the survey. After deceased and duplicate names from 2020 were removed, another 14 eligible 2019 female patients were invited and 6 agreed to participate; 6 eligible 2018 female patients were invited and 4 agreed to take the survey (Figure). Thirty female veterans were sent a survey link and 21 (70%) responses were collected. Twenty-one male 2020 patients were contacted and 18 agreed to take the survey. After removing duplicate names and deceased individuals, 17 of 21 eligible 2019 male patients and 4 of 6 eligible 2018 patients agreed to take the survey. Five additional male veterans declined the online-based survey method. In total, 39 male veterans were reached who agreed to have the survey link emailed, and 20 (51%) total responses were collected.
Most respondents answered all questions in the survey. The most frequently skipped questions included 3 questions that were contingent on a yes answer to a prior question, and 2 openended questions asking for a write-in response. Percentages for female and male respondents were adjusted for number of responses when applicable.
Thirteen (62%) female patients were aged < 65 years, while 18 (90%) of male patients were aged ≥ 65 years. Education beyond high school was reported in 20 female and 15 male respondents. Almost all treatment administered in the infusion unit was for cancer-directed treatment, with only 1 reporting a noncancer treatment (IV iron). The most common malignancy among female patients was breast cancer (n = 11, 52%); for male patients prostate cancer (n = 4, 20%) and hematologic malignancy (n = 4, 20%) were most common. Four (19%) female and 8 (40%) male respondents reported having a metastatic diagnosis. Overall patient satisfaction ranked high with an average score of 9.1 on a 10-point scale. The mean (SD) satisfaction score for female respondents was 1 point lower than that for men: 8.7 (2.2) vs 9.6 (0.6) in men (P = .11).
Eighteen (86%) women reported a history of sexual abuse or harassment compared with 2 (10%) men (P < .001). The sexual abuse assailant was a different gender for 17 of 18 female respondents and of the same gender for both male respondents. Of those with sexual abuse history, 4 women reported feeling uncomfortable around their assailant’s gender vs no men (P = .11), but this difference was not statistically significant. Six women (29%) and 2 (10%) men reported feeling uncomfortable during clinical examinations from comments made by the clinician or during treatment administration (P = .24). Six (29%) women and no men reported that they “felt uncomfortable in the infusion unit by other patients” (P = .02). Six (29%) women and no men reported feeling unable to “voice uncomfortable experiences” to the infusion unit clinician (P = .02).
Ten (48%) women and 6 (30%) men reported emotional support when receiving treatments provided by staff of the same gender (P = .34). Eight (38%) women and 4 (20%) men noted that access to treatment with the same gender was important (P = .31). Six (29%) women and 4 (20%) men indicated that access to a sex or gender-specific restroom was important (P = .72). No gender preferences were identified in the survey questions regarding importance of private treatment room access and level of emotional support when receiving treatment with others of the same malignancy. These relationships were not statistically significant.
In addition, 2 open-ended questions were asked. Seventeen women and 14 men responded. Contact the corresponding author for more information on the questions and responses.
Discussion
Overall patient satisfaction was high among the men and women veterans with cancer who received treatment in our outpatient infusion unit; however, notable gender differences existed. Three items in the survey revealed statistically significant differences in the patient experience between men and women veterans: history of sexual abuse or harassment, uncomfortable feelings among other patients, and discomfort in relaying uncomfortable feelings to a clinician. Other items in the survey did not reach statistical significance; however, we have included discussion of the findings as they may highlight important trends and be of clinical significance.
We suspect differences among genders in patient satisfaction to be related to the high incidence of sexual abuse or harassment history reported by women, much higher at 86% than the one-third to one-fourth incidence rates estimated by the existing literature for civilian or military sexual abuse in women.5,6 These high sexual abuse or harassment rates are present in a majority of women who receive cancer-directed treatment toward a gender-specific breast malignancy, surrounded predominantly among men in a shared treatment space. Together, these factors are likely key reasons behind the differences in satisfaction observed. This sentiment is expressed in our cohort, where one-fifth of women with a sexual abuse or harassment history continue to remain uncomfortable around men, and 29% of women reporting some uncomfortable feelings during their treatment experience compared with none of the men. Additionally, 6 (29%) women vs no men felt uncomfortable in reporting an uncomfortable experience with a clinician; this represents a significant barrier in providing care for these patients.
A key gender preference among women included access to shared treatment rooms with other women and that sharing a treatment space with other women resulted in feeling more emotional support during treatments. Access to gender-specific restrooms was also preferred by women more than men. Key findings in both genders were that about half of men and women valued access to a private treatment room and would derive more emotional support when surrounded by others with the same cancer.
Prior studies on gender and patient satisfaction in general medical care and cancer care have found women value privacy more than men.1-3 Wessels and colleagues performed an analysis of 386 patients with cancer in Europe and found gender to be the strongest influence in patient preferences within cancer care. Specifically, the highest statically significant association in care preferences among women included privacy, support/counseling/rehabilitation access, and decreased wait times.2 These findings were most pronounced in those with breast cancer compared with other malignancy type and highlights that malignancy type and gender predominance impact care satisfaction.
Traditionally a shared treatment space design has been used in outpatient chemotherapy units, similar to the design of the VAPHCS. However, recent data report on the patient preference for a private treatment space, which was especially prominent among women and those receiving longer infusions.7 In another study that evaluated 225 patients with cancer preferences in sharing a treatment space with those of a different sexual orientation or gender identify, differences were found. Both men and women had a similar level of comfort in sharing a treatment room with someone of a different sexual orientation; however, more women reported discomfort in sharing a treatment space with a transgender woman compared with men who felt more comfortable sharing a space with a transgender man.4 We noted a gender preference may be present to explain the difference. Within our cohort, women valued access to treatment with other women and derived more emotional support when with other women; however, we did not inquire about feelings in sharing a treatment space among transgender individuals or differing sexual orientation.
Gender differences for privacy and in shared room preferences may result from the lasting impacts of prior sexual abuse or harassment. A history of sexual abuse negatively impacts later medical care access and use.15 Those veterans who experienced sexual abuse/harrassment reported higher feelings of lack of control, vulnerability, depression, and pursued less medical care.15,16 Within cancer care, these feelings are most pronounced among women with gender-specific malignancies, such as gynecologic cancers or breast cancer. Treatment, screening, and physical examinations by clinicians who are of the same gender as the sexual abuse/harassment assailant can recreate traumatic feelings.15,16
A majority of women (n = 18, 86%) in our cohort reported a history of sexual abuse or harassment and breast malignancy was the most common cancer among women. However women represent just 5.6% of the VAPHCS infusion unit treatment population. This combination of factors may explain the reasons for women veterans’ preference for privacy during treatments, access to gender-specific restrooms, and feeling more emotional support when surrounded by other women. Strategies to help patients with a history of abuse have been described and include discussions from the clinician asking about abuse history, allowing time for the patient to express fears with an examination or test, and training on how to deliver sensitive care for those with trauma.17,18
Quality Improvement
Project In the VAPHCS infusion unit, several low-cost interventions have been undertaken as a result of our survey findings. We presented our survey data to the VAPHCS Cancer Committee, accredited through the national American College of Surgeons Commission on Cancer. The committee awarded support for a yearlong QI project, including a formal framework of quarterly multidisciplinary meetings to discuss project updates, challenges, and resources. The QI project centers on education to raise awareness of survey results as well as specific interventions for improvement.
Education efforts have been applied through multiple department-wide emails, in-person education to our chemotherapy unit staff, abstract submission to national oncology conferences, and grand rounds department presentations at VAPHCS and at other VHA-affiliated university programs. Additionally, education to clinicians with specific contact information for psychology and women’s health to support mental health, trauma, and sexual abuse histories has been given to each clinician who cares for veterans in the chemotherapy unit.
We also have implemented a mandatory cancer care navigation consultation for all women veterans who have a new cancer or infusion need. The cancer care navigator has received specialized training in sensitive history-taking and provides women veterans with a direct number to reach the cancer care navigation nurse. Cancer care navigation also provides a continuum of support and referral access for psychosocial needs as indicated between infusion or health care visits. Our hope is that these resources may help offset the sentiment reflected in our cohort of women feeling unable to voice concerns to a clinician.
Other interventions underway include offering designated scheduling time each week to women so they can receive infusions in an area with other women. This may help mitigate the finding that women veterans felt more uncomfortable around other patients during infusion treatments compared with how men felt in the chemotherapy unit. We also have implemented gender-specific restrooms labeled with a sign on each bathroom door so men and women can have access to a designated restroom. Offering private or semiprivate treatment rooms is currently limited by space and capacity; however, these may offer the greatest opportunity to improve patient satisfaction, especially among women veterans. Working with the support of the VAPHCS Cancer Committee, we aim to reevaluate the impact of the education and QI efforts on gender differences and patient satisfaction at completion of the 1-year award.
Limitations
Limitations to our study include the overall small sample size. This is due to the combination of the low number of women treated at VAPHCS and many with advanced cancer who, unfortunately, have a limited overall survival and hinders accrual of a larger sample size. Other limitations included age as a possible confounder in our findings, with women representing a younger demographic compared with men. We did not collect responses on duration of infusion time, which also may impact overall satisfaction and patient experience. We also acknowledge that biologic male or female sex may not correspond to a specific individual’s gender. Use of CPRS to obtain a matched number of male and female patients through random selection relied on labeled data from the EHR. This potentially may have excluded male patients who identify as another gender that would have been captured on the anonymous survey.
Last, we restricted survey responses to online only, which excluded a small percentage who declined this approach.
Conclusions
Our findings may have broad applications to other VHA facilities and other cancer-directed treatment centers where the patient demographic and open shared infusion unit design may be similar. The study also may serve as a model of survey design and implementation from which other centers may consider improving patient satisfaction. We hope these survey results and interventions can provide insight and be used to improve patient satisfaction among all cancer patients at infusion units serving veterans and nonveterans.
Acknowledgments
We are very thankful to our cancer patients who took the time to take the survey. We also are very grateful to the VHA infusion unit nurses, staff, nurse practitioners, and physicians who have embraced this project and welcomed any changes that may positively impact treatment of veterans. Also, thank you to Tia Kohs for statistical support and Sophie West for gender discussions. Last, we specifically thank Barbara, for her pursuit of better care for women and for all veterans.
1. Clarke SA, Booth L, Velikova G, Hewison J. Social support: gender differences in cancer patients in the United Kingdom. Cancer Nurs. 2006;29(1):66-72. doi:10.1097/00002820-200601000-00012
2. Wessels H, de Graeff A, Wynia K, et al. Gender-related needs and preferences in cancer care indicate the need for an individualized approach to cancer patients. Oncologist. 2010;15(6):648-655. doi:10.1634/theoncologist.2009-0337
3. Hartigan SM, Bonnet K, Chisholm L, et al. Why do women not use the bathroom? Women’s attitudes and beliefs on using public restrooms. Int J Environ Res Public Health. 2020;17(6):2053. doi:10.3390/ijerph17062053
4. Alexander K, Walters CB, Banerjee SC. Oncology patients’ preferences regarding sexual orientation and gender identity (SOGI) disclosure and room sharing sharing. Patient Educ Couns. 2020;103(5):1041-1048. doi:10.1016/j.pec.2019.12.006
5. Centers for Disease Control and Prevention. Facts about sexual violence. Updated July 5, 2022. Accessed July 13, 2022. https://www.cdc.gov/injury/features /sexual-violence/index.html
6. US Department of Veterans Affairs. Military sexual trauma. Updated May 16, 2022. Accessed July 13, 2022. https:// www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
7. Wang Z, Pukszta M. Private Rooms, Semi-open areas, or open areas for chemotherapy care: perspectives of cancer patients, families, and nursing staff. HERD. 2018;11(3):94- 108. doi:10.1177/1937586718758445
8. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Women veterans report: the past, present, and future of women veterans. Accessed July 13, 2022. https://www.va.gov/vetdata /docs/specialreports/women_veterans_2015_final.pdf
9. Driscoll MA, Higgins DM, Seng EK, et al. Trauma, social support, family conflict, and chronic pain in recent service veterans: does gender matter? Pain Med. 2015;16(6):1101- 1111. doi:10.1111/pme.12744
10. Fox AB, Meyer EC, Vogt D. Attitudes about the VA healthcare setting, mental illness, and mental health treatment and their relationship with VA mental health service use among female and male OEF/OIF veterans. Psychol Serv. 2015;12(1):49-58. doi:10.1037/a0038269
11. Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115(1):21-26. doi:10.1016/j.amjcard.2014.09.041
12. Tseng J. Sex, gender, and why the differences matter. Virtual Mentor. 2008;10(7):427-428. doi:10.1001/virtualmentor.2008.10.7.fred1-0807
13. Booij JC, Zegers M, Evers PMPJ, Hendricks M, Delnoij DMJ, Rademakers JJDJM. Improving cancer patient care: development of a generic cancer consumer quality index questionnaire for cancer patients. BMC Cancer. 2013;13(203). doi:10.1186/1471-2407-13-203
14. Meropol NJ, Egleston BL, Buzaglo JS, et al. Cancer patient preferences for quality and length of life. Cancer. 2008;113(12):3459-3466. doi:10.1002/cncr.23968 1
5. Schnur JB, Dillon MJ, Goldsmith RE, Montgomery GH. Cancer treatment experiences among survivors of childhood sexual abuse: a qualitative investigation of triggers and reactions to cumulative trauma. Palliat Support Care. 2018;16(6):767-776. doi:10.1017/S147895151700075X
16. Cadman L, Waller J, Ashdown-Barr L, Szarewski A. Barriers to cervical screening in women who have experienced sexual abuse: an exploratory study. J Fam Plann Reprod Health Care. 2012;38(4):214-220. doi:10.1136/jfprhc-2012-100378
17. Kelly S. The effects of childhood sexual abuse on women’s lives and their attitudes to cervical screening. J Fam Plann Reprod Health Care. 2012;38(4):212-213. doi:10.1136/jfprhc-2012-100418
18. McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep. 2006;121(4):435-444. doi:10.1177/003335490612100412
Gender differences in patient satisfaction with medical care have been evaluated in multiple settings; however, studies specific to the unique population of women veterans with cancer are lacking. Women are reported to value privacy, psychosocial support, and communication to a higher degree compared with men.1 Factors affecting satisfaction include the following: discomfort in sharing treatment rooms with the opposite gender, a desire for privacy with treatment and restroom use, anatomic or illness differences, and a personal history of abuse.2-4 Regrettably, up to 1 in 3 women in the United States are victims of sexual trauma in their lifetimes, and up to 1 in 4 women in the military are victims of military sexual trauma. Incidence in both settings is suspected to be higher due to underreporting.5,6
Chemotherapy treatment units are often uniquely designed as an open space, with several patients sharing a treatment area. The design reduces isolation and facilitates quick nurse-patient access during potentially toxic treatments known to have frequent adverse effects. Data suggest that nursing staff prefer open models to facilitate quick patient assessments and interventions as needed; however, patients and families prefer private treatment rooms, especially among women patients or those receiving longer infusions.7
The Veterans Health Administration (VHA) patient population is male predominant, comprised only of 10% female patients.8 Although the proportion of female patients in the VHA is expected to rise annually to about 16% by 2043, the low percentage of female veterans will persist for the foreseeable future.8 This low percentage of female veterans is reflected in the Veterans Affairs Portland Health Care System (VAPHCS) cancer patient population and in the use of the chemotherapy infusion unit, which is used for the ambulatory treatment of veterans undergoing cancer therapy.
The VHA has previously explored gender differences in health care, such as with cardiovascular disease, transgender care, and access to mental health.9-11 However, to the best of our knowledge, no analysis has explored gender differences within the outpatient cancer treatment experience. Patient satisfaction with outpatient cancer care may be magnified in the VHA setting due to the uniquely unequal gender populations, shared treatment space design, and high incidence of sexual abuse among women veterans. Given this, we aimed to identify gender-related preferences in outpatient cancer care in our chemotherapy infusion unit.
In our study, we used the terms male and female to reflect statistical data from the literature or labeled data from the electronic health record (EHR); whereas the terms men and women were used to describe and encompass the cultural implications and context of gender.12
Methods
This study was designated as a quality improvement (QI) project by the VAPHCS research office and Institutional Review Board in accordance with VHA policies.
The VAPHCS outpatient chemotherapy infusion unit is designed with 6 rooms for chemotherapy administration. One room is a large open space with 6 chairs for patients. The other rooms are smaller with glass dividers between the rooms, and 3 chairs inside each for patients. There are 2 private bathrooms, each gender neutral. Direct patient care is provided by physicians, nurse practitioners (NPs), infusion unit nurses, and nurse coordinators. Men represent the majority of hematology and oncology physicians (13 of 20 total: 5 women fellow physicians and 2 women attending physicians), and 2 of 4 NPs. Women represent 10 of 12 infusion unit and cancer coordinator nurses. We used the VHA Computerized Patient Record System (CPRS) EHR, to create a list of veterans treated at the VAPHCS outpatient chemotherapy infusion unit for a 2-year period (January 1, 2018, to December 31, 2020).
Male and female patient lists were first generated based on CPRS categorization. We identified all female veterans treated in the ambulatory infusion unit during the study period. Male patients were then chosen at random, recording the most recent names for each year until a matched number per year compared with the female cohort was reached. Patients were recorded only once even though they had multiple infusion unit visits. Patients were excluded who were deceased, on hospice care, lost to follow-up, could not be reached by phone, refused to take the survey, had undeliverable email addresses, or lacked internet or email access.
After filing the appropriate request through the VAPHCS Institutional Review Board committee in January 2021, patient records were reviewed for demographics data, contact information, and infusion treatment history. The survey was then conducted over a 2-week period during January and February 2021. Each patient was invited by phone to complete a 25-question anonymous online survey. The survey questions were created from patient-relayed experiences, then modeled into survey questions in a format similar to other patient satisfaction questionnaires described in cancer care and gender differences.2,13,14 The survey included self-identification of gender and was multiple choice for all except 2 questions, which allowed an open-ended response (Appendix). Only 1 answer per question was permitted. Only 1 survey link was sent to each veteran who gave permission for the survey. To protect anonymity for the small patient population, we excluded those identifying as gender nonbinary or transgender.
Statistical Analysis
Patient, disease, and treatment features are separated by male and female cohorts to reflect information from the EHR (Table 1). Survey percentages were calculated to reflect the affirmative response of the question asked (Table 2). Questions with answer options of not important, minimally important, important, or very important were calculated to reflect the sum of any importance in both cohorts. Questions with answer options of never, once, often, or every time were calculated to reflect any occurrence (sum of once, often, or every time) in both patient groups. Questions with answer options of strongly agree, somewhat agree, somewhat disagree, and strongly disagree were calculated to reflect any agreement (somewhat agree and strongly agree summed together) for both groups. Comparisons between cohorts were then conducted using a Fisher exact test. A Welch t test was used to calculate the significance of the continuous variable and overall ranking of the infusion unit experience between groups.
Results
In 2020, 414 individual patients were treated at the VAPAHCS outpatient infusion unit. Of these, 23 (5.6%) were female, and 18 agreed to take the survey. After deceased and duplicate names from 2020 were removed, another 14 eligible 2019 female patients were invited and 6 agreed to participate; 6 eligible 2018 female patients were invited and 4 agreed to take the survey (Figure). Thirty female veterans were sent a survey link and 21 (70%) responses were collected. Twenty-one male 2020 patients were contacted and 18 agreed to take the survey. After removing duplicate names and deceased individuals, 17 of 21 eligible 2019 male patients and 4 of 6 eligible 2018 patients agreed to take the survey. Five additional male veterans declined the online-based survey method. In total, 39 male veterans were reached who agreed to have the survey link emailed, and 20 (51%) total responses were collected.
Most respondents answered all questions in the survey. The most frequently skipped questions included 3 questions that were contingent on a yes answer to a prior question, and 2 openended questions asking for a write-in response. Percentages for female and male respondents were adjusted for number of responses when applicable.
Thirteen (62%) female patients were aged < 65 years, while 18 (90%) of male patients were aged ≥ 65 years. Education beyond high school was reported in 20 female and 15 male respondents. Almost all treatment administered in the infusion unit was for cancer-directed treatment, with only 1 reporting a noncancer treatment (IV iron). The most common malignancy among female patients was breast cancer (n = 11, 52%); for male patients prostate cancer (n = 4, 20%) and hematologic malignancy (n = 4, 20%) were most common. Four (19%) female and 8 (40%) male respondents reported having a metastatic diagnosis. Overall patient satisfaction ranked high with an average score of 9.1 on a 10-point scale. The mean (SD) satisfaction score for female respondents was 1 point lower than that for men: 8.7 (2.2) vs 9.6 (0.6) in men (P = .11).
Eighteen (86%) women reported a history of sexual abuse or harassment compared with 2 (10%) men (P < .001). The sexual abuse assailant was a different gender for 17 of 18 female respondents and of the same gender for both male respondents. Of those with sexual abuse history, 4 women reported feeling uncomfortable around their assailant’s gender vs no men (P = .11), but this difference was not statistically significant. Six women (29%) and 2 (10%) men reported feeling uncomfortable during clinical examinations from comments made by the clinician or during treatment administration (P = .24). Six (29%) women and no men reported that they “felt uncomfortable in the infusion unit by other patients” (P = .02). Six (29%) women and no men reported feeling unable to “voice uncomfortable experiences” to the infusion unit clinician (P = .02).
Ten (48%) women and 6 (30%) men reported emotional support when receiving treatments provided by staff of the same gender (P = .34). Eight (38%) women and 4 (20%) men noted that access to treatment with the same gender was important (P = .31). Six (29%) women and 4 (20%) men indicated that access to a sex or gender-specific restroom was important (P = .72). No gender preferences were identified in the survey questions regarding importance of private treatment room access and level of emotional support when receiving treatment with others of the same malignancy. These relationships were not statistically significant.
In addition, 2 open-ended questions were asked. Seventeen women and 14 men responded. Contact the corresponding author for more information on the questions and responses.
Discussion
Overall patient satisfaction was high among the men and women veterans with cancer who received treatment in our outpatient infusion unit; however, notable gender differences existed. Three items in the survey revealed statistically significant differences in the patient experience between men and women veterans: history of sexual abuse or harassment, uncomfortable feelings among other patients, and discomfort in relaying uncomfortable feelings to a clinician. Other items in the survey did not reach statistical significance; however, we have included discussion of the findings as they may highlight important trends and be of clinical significance.
We suspect differences among genders in patient satisfaction to be related to the high incidence of sexual abuse or harassment history reported by women, much higher at 86% than the one-third to one-fourth incidence rates estimated by the existing literature for civilian or military sexual abuse in women.5,6 These high sexual abuse or harassment rates are present in a majority of women who receive cancer-directed treatment toward a gender-specific breast malignancy, surrounded predominantly among men in a shared treatment space. Together, these factors are likely key reasons behind the differences in satisfaction observed. This sentiment is expressed in our cohort, where one-fifth of women with a sexual abuse or harassment history continue to remain uncomfortable around men, and 29% of women reporting some uncomfortable feelings during their treatment experience compared with none of the men. Additionally, 6 (29%) women vs no men felt uncomfortable in reporting an uncomfortable experience with a clinician; this represents a significant barrier in providing care for these patients.
A key gender preference among women included access to shared treatment rooms with other women and that sharing a treatment space with other women resulted in feeling more emotional support during treatments. Access to gender-specific restrooms was also preferred by women more than men. Key findings in both genders were that about half of men and women valued access to a private treatment room and would derive more emotional support when surrounded by others with the same cancer.
Prior studies on gender and patient satisfaction in general medical care and cancer care have found women value privacy more than men.1-3 Wessels and colleagues performed an analysis of 386 patients with cancer in Europe and found gender to be the strongest influence in patient preferences within cancer care. Specifically, the highest statically significant association in care preferences among women included privacy, support/counseling/rehabilitation access, and decreased wait times.2 These findings were most pronounced in those with breast cancer compared with other malignancy type and highlights that malignancy type and gender predominance impact care satisfaction.
Traditionally a shared treatment space design has been used in outpatient chemotherapy units, similar to the design of the VAPHCS. However, recent data report on the patient preference for a private treatment space, which was especially prominent among women and those receiving longer infusions.7 In another study that evaluated 225 patients with cancer preferences in sharing a treatment space with those of a different sexual orientation or gender identify, differences were found. Both men and women had a similar level of comfort in sharing a treatment room with someone of a different sexual orientation; however, more women reported discomfort in sharing a treatment space with a transgender woman compared with men who felt more comfortable sharing a space with a transgender man.4 We noted a gender preference may be present to explain the difference. Within our cohort, women valued access to treatment with other women and derived more emotional support when with other women; however, we did not inquire about feelings in sharing a treatment space among transgender individuals or differing sexual orientation.
Gender differences for privacy and in shared room preferences may result from the lasting impacts of prior sexual abuse or harassment. A history of sexual abuse negatively impacts later medical care access and use.15 Those veterans who experienced sexual abuse/harrassment reported higher feelings of lack of control, vulnerability, depression, and pursued less medical care.15,16 Within cancer care, these feelings are most pronounced among women with gender-specific malignancies, such as gynecologic cancers or breast cancer. Treatment, screening, and physical examinations by clinicians who are of the same gender as the sexual abuse/harassment assailant can recreate traumatic feelings.15,16
A majority of women (n = 18, 86%) in our cohort reported a history of sexual abuse or harassment and breast malignancy was the most common cancer among women. However women represent just 5.6% of the VAPHCS infusion unit treatment population. This combination of factors may explain the reasons for women veterans’ preference for privacy during treatments, access to gender-specific restrooms, and feeling more emotional support when surrounded by other women. Strategies to help patients with a history of abuse have been described and include discussions from the clinician asking about abuse history, allowing time for the patient to express fears with an examination or test, and training on how to deliver sensitive care for those with trauma.17,18
Quality Improvement
Project In the VAPHCS infusion unit, several low-cost interventions have been undertaken as a result of our survey findings. We presented our survey data to the VAPHCS Cancer Committee, accredited through the national American College of Surgeons Commission on Cancer. The committee awarded support for a yearlong QI project, including a formal framework of quarterly multidisciplinary meetings to discuss project updates, challenges, and resources. The QI project centers on education to raise awareness of survey results as well as specific interventions for improvement.
Education efforts have been applied through multiple department-wide emails, in-person education to our chemotherapy unit staff, abstract submission to national oncology conferences, and grand rounds department presentations at VAPHCS and at other VHA-affiliated university programs. Additionally, education to clinicians with specific contact information for psychology and women’s health to support mental health, trauma, and sexual abuse histories has been given to each clinician who cares for veterans in the chemotherapy unit.
We also have implemented a mandatory cancer care navigation consultation for all women veterans who have a new cancer or infusion need. The cancer care navigator has received specialized training in sensitive history-taking and provides women veterans with a direct number to reach the cancer care navigation nurse. Cancer care navigation also provides a continuum of support and referral access for psychosocial needs as indicated between infusion or health care visits. Our hope is that these resources may help offset the sentiment reflected in our cohort of women feeling unable to voice concerns to a clinician.
Other interventions underway include offering designated scheduling time each week to women so they can receive infusions in an area with other women. This may help mitigate the finding that women veterans felt more uncomfortable around other patients during infusion treatments compared with how men felt in the chemotherapy unit. We also have implemented gender-specific restrooms labeled with a sign on each bathroom door so men and women can have access to a designated restroom. Offering private or semiprivate treatment rooms is currently limited by space and capacity; however, these may offer the greatest opportunity to improve patient satisfaction, especially among women veterans. Working with the support of the VAPHCS Cancer Committee, we aim to reevaluate the impact of the education and QI efforts on gender differences and patient satisfaction at completion of the 1-year award.
Limitations
Limitations to our study include the overall small sample size. This is due to the combination of the low number of women treated at VAPHCS and many with advanced cancer who, unfortunately, have a limited overall survival and hinders accrual of a larger sample size. Other limitations included age as a possible confounder in our findings, with women representing a younger demographic compared with men. We did not collect responses on duration of infusion time, which also may impact overall satisfaction and patient experience. We also acknowledge that biologic male or female sex may not correspond to a specific individual’s gender. Use of CPRS to obtain a matched number of male and female patients through random selection relied on labeled data from the EHR. This potentially may have excluded male patients who identify as another gender that would have been captured on the anonymous survey.
Last, we restricted survey responses to online only, which excluded a small percentage who declined this approach.
Conclusions
Our findings may have broad applications to other VHA facilities and other cancer-directed treatment centers where the patient demographic and open shared infusion unit design may be similar. The study also may serve as a model of survey design and implementation from which other centers may consider improving patient satisfaction. We hope these survey results and interventions can provide insight and be used to improve patient satisfaction among all cancer patients at infusion units serving veterans and nonveterans.
Acknowledgments
We are very thankful to our cancer patients who took the time to take the survey. We also are very grateful to the VHA infusion unit nurses, staff, nurse practitioners, and physicians who have embraced this project and welcomed any changes that may positively impact treatment of veterans. Also, thank you to Tia Kohs for statistical support and Sophie West for gender discussions. Last, we specifically thank Barbara, for her pursuit of better care for women and for all veterans.
Gender differences in patient satisfaction with medical care have been evaluated in multiple settings; however, studies specific to the unique population of women veterans with cancer are lacking. Women are reported to value privacy, psychosocial support, and communication to a higher degree compared with men.1 Factors affecting satisfaction include the following: discomfort in sharing treatment rooms with the opposite gender, a desire for privacy with treatment and restroom use, anatomic or illness differences, and a personal history of abuse.2-4 Regrettably, up to 1 in 3 women in the United States are victims of sexual trauma in their lifetimes, and up to 1 in 4 women in the military are victims of military sexual trauma. Incidence in both settings is suspected to be higher due to underreporting.5,6
Chemotherapy treatment units are often uniquely designed as an open space, with several patients sharing a treatment area. The design reduces isolation and facilitates quick nurse-patient access during potentially toxic treatments known to have frequent adverse effects. Data suggest that nursing staff prefer open models to facilitate quick patient assessments and interventions as needed; however, patients and families prefer private treatment rooms, especially among women patients or those receiving longer infusions.7
The Veterans Health Administration (VHA) patient population is male predominant, comprised only of 10% female patients.8 Although the proportion of female patients in the VHA is expected to rise annually to about 16% by 2043, the low percentage of female veterans will persist for the foreseeable future.8 This low percentage of female veterans is reflected in the Veterans Affairs Portland Health Care System (VAPHCS) cancer patient population and in the use of the chemotherapy infusion unit, which is used for the ambulatory treatment of veterans undergoing cancer therapy.
The VHA has previously explored gender differences in health care, such as with cardiovascular disease, transgender care, and access to mental health.9-11 However, to the best of our knowledge, no analysis has explored gender differences within the outpatient cancer treatment experience. Patient satisfaction with outpatient cancer care may be magnified in the VHA setting due to the uniquely unequal gender populations, shared treatment space design, and high incidence of sexual abuse among women veterans. Given this, we aimed to identify gender-related preferences in outpatient cancer care in our chemotherapy infusion unit.
In our study, we used the terms male and female to reflect statistical data from the literature or labeled data from the electronic health record (EHR); whereas the terms men and women were used to describe and encompass the cultural implications and context of gender.12
Methods
This study was designated as a quality improvement (QI) project by the VAPHCS research office and Institutional Review Board in accordance with VHA policies.
The VAPHCS outpatient chemotherapy infusion unit is designed with 6 rooms for chemotherapy administration. One room is a large open space with 6 chairs for patients. The other rooms are smaller with glass dividers between the rooms, and 3 chairs inside each for patients. There are 2 private bathrooms, each gender neutral. Direct patient care is provided by physicians, nurse practitioners (NPs), infusion unit nurses, and nurse coordinators. Men represent the majority of hematology and oncology physicians (13 of 20 total: 5 women fellow physicians and 2 women attending physicians), and 2 of 4 NPs. Women represent 10 of 12 infusion unit and cancer coordinator nurses. We used the VHA Computerized Patient Record System (CPRS) EHR, to create a list of veterans treated at the VAPHCS outpatient chemotherapy infusion unit for a 2-year period (January 1, 2018, to December 31, 2020).
Male and female patient lists were first generated based on CPRS categorization. We identified all female veterans treated in the ambulatory infusion unit during the study period. Male patients were then chosen at random, recording the most recent names for each year until a matched number per year compared with the female cohort was reached. Patients were recorded only once even though they had multiple infusion unit visits. Patients were excluded who were deceased, on hospice care, lost to follow-up, could not be reached by phone, refused to take the survey, had undeliverable email addresses, or lacked internet or email access.
After filing the appropriate request through the VAPHCS Institutional Review Board committee in January 2021, patient records were reviewed for demographics data, contact information, and infusion treatment history. The survey was then conducted over a 2-week period during January and February 2021. Each patient was invited by phone to complete a 25-question anonymous online survey. The survey questions were created from patient-relayed experiences, then modeled into survey questions in a format similar to other patient satisfaction questionnaires described in cancer care and gender differences.2,13,14 The survey included self-identification of gender and was multiple choice for all except 2 questions, which allowed an open-ended response (Appendix). Only 1 answer per question was permitted. Only 1 survey link was sent to each veteran who gave permission for the survey. To protect anonymity for the small patient population, we excluded those identifying as gender nonbinary or transgender.
Statistical Analysis
Patient, disease, and treatment features are separated by male and female cohorts to reflect information from the EHR (Table 1). Survey percentages were calculated to reflect the affirmative response of the question asked (Table 2). Questions with answer options of not important, minimally important, important, or very important were calculated to reflect the sum of any importance in both cohorts. Questions with answer options of never, once, often, or every time were calculated to reflect any occurrence (sum of once, often, or every time) in both patient groups. Questions with answer options of strongly agree, somewhat agree, somewhat disagree, and strongly disagree were calculated to reflect any agreement (somewhat agree and strongly agree summed together) for both groups. Comparisons between cohorts were then conducted using a Fisher exact test. A Welch t test was used to calculate the significance of the continuous variable and overall ranking of the infusion unit experience between groups.
Results
In 2020, 414 individual patients were treated at the VAPAHCS outpatient infusion unit. Of these, 23 (5.6%) were female, and 18 agreed to take the survey. After deceased and duplicate names from 2020 were removed, another 14 eligible 2019 female patients were invited and 6 agreed to participate; 6 eligible 2018 female patients were invited and 4 agreed to take the survey (Figure). Thirty female veterans were sent a survey link and 21 (70%) responses were collected. Twenty-one male 2020 patients were contacted and 18 agreed to take the survey. After removing duplicate names and deceased individuals, 17 of 21 eligible 2019 male patients and 4 of 6 eligible 2018 patients agreed to take the survey. Five additional male veterans declined the online-based survey method. In total, 39 male veterans were reached who agreed to have the survey link emailed, and 20 (51%) total responses were collected.
Most respondents answered all questions in the survey. The most frequently skipped questions included 3 questions that were contingent on a yes answer to a prior question, and 2 openended questions asking for a write-in response. Percentages for female and male respondents were adjusted for number of responses when applicable.
Thirteen (62%) female patients were aged < 65 years, while 18 (90%) of male patients were aged ≥ 65 years. Education beyond high school was reported in 20 female and 15 male respondents. Almost all treatment administered in the infusion unit was for cancer-directed treatment, with only 1 reporting a noncancer treatment (IV iron). The most common malignancy among female patients was breast cancer (n = 11, 52%); for male patients prostate cancer (n = 4, 20%) and hematologic malignancy (n = 4, 20%) were most common. Four (19%) female and 8 (40%) male respondents reported having a metastatic diagnosis. Overall patient satisfaction ranked high with an average score of 9.1 on a 10-point scale. The mean (SD) satisfaction score for female respondents was 1 point lower than that for men: 8.7 (2.2) vs 9.6 (0.6) in men (P = .11).
Eighteen (86%) women reported a history of sexual abuse or harassment compared with 2 (10%) men (P < .001). The sexual abuse assailant was a different gender for 17 of 18 female respondents and of the same gender for both male respondents. Of those with sexual abuse history, 4 women reported feeling uncomfortable around their assailant’s gender vs no men (P = .11), but this difference was not statistically significant. Six women (29%) and 2 (10%) men reported feeling uncomfortable during clinical examinations from comments made by the clinician or during treatment administration (P = .24). Six (29%) women and no men reported that they “felt uncomfortable in the infusion unit by other patients” (P = .02). Six (29%) women and no men reported feeling unable to “voice uncomfortable experiences” to the infusion unit clinician (P = .02).
Ten (48%) women and 6 (30%) men reported emotional support when receiving treatments provided by staff of the same gender (P = .34). Eight (38%) women and 4 (20%) men noted that access to treatment with the same gender was important (P = .31). Six (29%) women and 4 (20%) men indicated that access to a sex or gender-specific restroom was important (P = .72). No gender preferences were identified in the survey questions regarding importance of private treatment room access and level of emotional support when receiving treatment with others of the same malignancy. These relationships were not statistically significant.
In addition, 2 open-ended questions were asked. Seventeen women and 14 men responded. Contact the corresponding author for more information on the questions and responses.
Discussion
Overall patient satisfaction was high among the men and women veterans with cancer who received treatment in our outpatient infusion unit; however, notable gender differences existed. Three items in the survey revealed statistically significant differences in the patient experience between men and women veterans: history of sexual abuse or harassment, uncomfortable feelings among other patients, and discomfort in relaying uncomfortable feelings to a clinician. Other items in the survey did not reach statistical significance; however, we have included discussion of the findings as they may highlight important trends and be of clinical significance.
We suspect differences among genders in patient satisfaction to be related to the high incidence of sexual abuse or harassment history reported by women, much higher at 86% than the one-third to one-fourth incidence rates estimated by the existing literature for civilian or military sexual abuse in women.5,6 These high sexual abuse or harassment rates are present in a majority of women who receive cancer-directed treatment toward a gender-specific breast malignancy, surrounded predominantly among men in a shared treatment space. Together, these factors are likely key reasons behind the differences in satisfaction observed. This sentiment is expressed in our cohort, where one-fifth of women with a sexual abuse or harassment history continue to remain uncomfortable around men, and 29% of women reporting some uncomfortable feelings during their treatment experience compared with none of the men. Additionally, 6 (29%) women vs no men felt uncomfortable in reporting an uncomfortable experience with a clinician; this represents a significant barrier in providing care for these patients.
A key gender preference among women included access to shared treatment rooms with other women and that sharing a treatment space with other women resulted in feeling more emotional support during treatments. Access to gender-specific restrooms was also preferred by women more than men. Key findings in both genders were that about half of men and women valued access to a private treatment room and would derive more emotional support when surrounded by others with the same cancer.
Prior studies on gender and patient satisfaction in general medical care and cancer care have found women value privacy more than men.1-3 Wessels and colleagues performed an analysis of 386 patients with cancer in Europe and found gender to be the strongest influence in patient preferences within cancer care. Specifically, the highest statically significant association in care preferences among women included privacy, support/counseling/rehabilitation access, and decreased wait times.2 These findings were most pronounced in those with breast cancer compared with other malignancy type and highlights that malignancy type and gender predominance impact care satisfaction.
Traditionally a shared treatment space design has been used in outpatient chemotherapy units, similar to the design of the VAPHCS. However, recent data report on the patient preference for a private treatment space, which was especially prominent among women and those receiving longer infusions.7 In another study that evaluated 225 patients with cancer preferences in sharing a treatment space with those of a different sexual orientation or gender identify, differences were found. Both men and women had a similar level of comfort in sharing a treatment room with someone of a different sexual orientation; however, more women reported discomfort in sharing a treatment space with a transgender woman compared with men who felt more comfortable sharing a space with a transgender man.4 We noted a gender preference may be present to explain the difference. Within our cohort, women valued access to treatment with other women and derived more emotional support when with other women; however, we did not inquire about feelings in sharing a treatment space among transgender individuals or differing sexual orientation.
Gender differences for privacy and in shared room preferences may result from the lasting impacts of prior sexual abuse or harassment. A history of sexual abuse negatively impacts later medical care access and use.15 Those veterans who experienced sexual abuse/harrassment reported higher feelings of lack of control, vulnerability, depression, and pursued less medical care.15,16 Within cancer care, these feelings are most pronounced among women with gender-specific malignancies, such as gynecologic cancers or breast cancer. Treatment, screening, and physical examinations by clinicians who are of the same gender as the sexual abuse/harassment assailant can recreate traumatic feelings.15,16
A majority of women (n = 18, 86%) in our cohort reported a history of sexual abuse or harassment and breast malignancy was the most common cancer among women. However women represent just 5.6% of the VAPHCS infusion unit treatment population. This combination of factors may explain the reasons for women veterans’ preference for privacy during treatments, access to gender-specific restrooms, and feeling more emotional support when surrounded by other women. Strategies to help patients with a history of abuse have been described and include discussions from the clinician asking about abuse history, allowing time for the patient to express fears with an examination or test, and training on how to deliver sensitive care for those with trauma.17,18
Quality Improvement
Project In the VAPHCS infusion unit, several low-cost interventions have been undertaken as a result of our survey findings. We presented our survey data to the VAPHCS Cancer Committee, accredited through the national American College of Surgeons Commission on Cancer. The committee awarded support for a yearlong QI project, including a formal framework of quarterly multidisciplinary meetings to discuss project updates, challenges, and resources. The QI project centers on education to raise awareness of survey results as well as specific interventions for improvement.
Education efforts have been applied through multiple department-wide emails, in-person education to our chemotherapy unit staff, abstract submission to national oncology conferences, and grand rounds department presentations at VAPHCS and at other VHA-affiliated university programs. Additionally, education to clinicians with specific contact information for psychology and women’s health to support mental health, trauma, and sexual abuse histories has been given to each clinician who cares for veterans in the chemotherapy unit.
We also have implemented a mandatory cancer care navigation consultation for all women veterans who have a new cancer or infusion need. The cancer care navigator has received specialized training in sensitive history-taking and provides women veterans with a direct number to reach the cancer care navigation nurse. Cancer care navigation also provides a continuum of support and referral access for psychosocial needs as indicated between infusion or health care visits. Our hope is that these resources may help offset the sentiment reflected in our cohort of women feeling unable to voice concerns to a clinician.
Other interventions underway include offering designated scheduling time each week to women so they can receive infusions in an area with other women. This may help mitigate the finding that women veterans felt more uncomfortable around other patients during infusion treatments compared with how men felt in the chemotherapy unit. We also have implemented gender-specific restrooms labeled with a sign on each bathroom door so men and women can have access to a designated restroom. Offering private or semiprivate treatment rooms is currently limited by space and capacity; however, these may offer the greatest opportunity to improve patient satisfaction, especially among women veterans. Working with the support of the VAPHCS Cancer Committee, we aim to reevaluate the impact of the education and QI efforts on gender differences and patient satisfaction at completion of the 1-year award.
Limitations
Limitations to our study include the overall small sample size. This is due to the combination of the low number of women treated at VAPHCS and many with advanced cancer who, unfortunately, have a limited overall survival and hinders accrual of a larger sample size. Other limitations included age as a possible confounder in our findings, with women representing a younger demographic compared with men. We did not collect responses on duration of infusion time, which also may impact overall satisfaction and patient experience. We also acknowledge that biologic male or female sex may not correspond to a specific individual’s gender. Use of CPRS to obtain a matched number of male and female patients through random selection relied on labeled data from the EHR. This potentially may have excluded male patients who identify as another gender that would have been captured on the anonymous survey.
Last, we restricted survey responses to online only, which excluded a small percentage who declined this approach.
Conclusions
Our findings may have broad applications to other VHA facilities and other cancer-directed treatment centers where the patient demographic and open shared infusion unit design may be similar. The study also may serve as a model of survey design and implementation from which other centers may consider improving patient satisfaction. We hope these survey results and interventions can provide insight and be used to improve patient satisfaction among all cancer patients at infusion units serving veterans and nonveterans.
Acknowledgments
We are very thankful to our cancer patients who took the time to take the survey. We also are very grateful to the VHA infusion unit nurses, staff, nurse practitioners, and physicians who have embraced this project and welcomed any changes that may positively impact treatment of veterans. Also, thank you to Tia Kohs for statistical support and Sophie West for gender discussions. Last, we specifically thank Barbara, for her pursuit of better care for women and for all veterans.
1. Clarke SA, Booth L, Velikova G, Hewison J. Social support: gender differences in cancer patients in the United Kingdom. Cancer Nurs. 2006;29(1):66-72. doi:10.1097/00002820-200601000-00012
2. Wessels H, de Graeff A, Wynia K, et al. Gender-related needs and preferences in cancer care indicate the need for an individualized approach to cancer patients. Oncologist. 2010;15(6):648-655. doi:10.1634/theoncologist.2009-0337
3. Hartigan SM, Bonnet K, Chisholm L, et al. Why do women not use the bathroom? Women’s attitudes and beliefs on using public restrooms. Int J Environ Res Public Health. 2020;17(6):2053. doi:10.3390/ijerph17062053
4. Alexander K, Walters CB, Banerjee SC. Oncology patients’ preferences regarding sexual orientation and gender identity (SOGI) disclosure and room sharing sharing. Patient Educ Couns. 2020;103(5):1041-1048. doi:10.1016/j.pec.2019.12.006
5. Centers for Disease Control and Prevention. Facts about sexual violence. Updated July 5, 2022. Accessed July 13, 2022. https://www.cdc.gov/injury/features /sexual-violence/index.html
6. US Department of Veterans Affairs. Military sexual trauma. Updated May 16, 2022. Accessed July 13, 2022. https:// www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
7. Wang Z, Pukszta M. Private Rooms, Semi-open areas, or open areas for chemotherapy care: perspectives of cancer patients, families, and nursing staff. HERD. 2018;11(3):94- 108. doi:10.1177/1937586718758445
8. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Women veterans report: the past, present, and future of women veterans. Accessed July 13, 2022. https://www.va.gov/vetdata /docs/specialreports/women_veterans_2015_final.pdf
9. Driscoll MA, Higgins DM, Seng EK, et al. Trauma, social support, family conflict, and chronic pain in recent service veterans: does gender matter? Pain Med. 2015;16(6):1101- 1111. doi:10.1111/pme.12744
10. Fox AB, Meyer EC, Vogt D. Attitudes about the VA healthcare setting, mental illness, and mental health treatment and their relationship with VA mental health service use among female and male OEF/OIF veterans. Psychol Serv. 2015;12(1):49-58. doi:10.1037/a0038269
11. Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115(1):21-26. doi:10.1016/j.amjcard.2014.09.041
12. Tseng J. Sex, gender, and why the differences matter. Virtual Mentor. 2008;10(7):427-428. doi:10.1001/virtualmentor.2008.10.7.fred1-0807
13. Booij JC, Zegers M, Evers PMPJ, Hendricks M, Delnoij DMJ, Rademakers JJDJM. Improving cancer patient care: development of a generic cancer consumer quality index questionnaire for cancer patients. BMC Cancer. 2013;13(203). doi:10.1186/1471-2407-13-203
14. Meropol NJ, Egleston BL, Buzaglo JS, et al. Cancer patient preferences for quality and length of life. Cancer. 2008;113(12):3459-3466. doi:10.1002/cncr.23968 1
5. Schnur JB, Dillon MJ, Goldsmith RE, Montgomery GH. Cancer treatment experiences among survivors of childhood sexual abuse: a qualitative investigation of triggers and reactions to cumulative trauma. Palliat Support Care. 2018;16(6):767-776. doi:10.1017/S147895151700075X
16. Cadman L, Waller J, Ashdown-Barr L, Szarewski A. Barriers to cervical screening in women who have experienced sexual abuse: an exploratory study. J Fam Plann Reprod Health Care. 2012;38(4):214-220. doi:10.1136/jfprhc-2012-100378
17. Kelly S. The effects of childhood sexual abuse on women’s lives and their attitudes to cervical screening. J Fam Plann Reprod Health Care. 2012;38(4):212-213. doi:10.1136/jfprhc-2012-100418
18. McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep. 2006;121(4):435-444. doi:10.1177/003335490612100412
1. Clarke SA, Booth L, Velikova G, Hewison J. Social support: gender differences in cancer patients in the United Kingdom. Cancer Nurs. 2006;29(1):66-72. doi:10.1097/00002820-200601000-00012
2. Wessels H, de Graeff A, Wynia K, et al. Gender-related needs and preferences in cancer care indicate the need for an individualized approach to cancer patients. Oncologist. 2010;15(6):648-655. doi:10.1634/theoncologist.2009-0337
3. Hartigan SM, Bonnet K, Chisholm L, et al. Why do women not use the bathroom? Women’s attitudes and beliefs on using public restrooms. Int J Environ Res Public Health. 2020;17(6):2053. doi:10.3390/ijerph17062053
4. Alexander K, Walters CB, Banerjee SC. Oncology patients’ preferences regarding sexual orientation and gender identity (SOGI) disclosure and room sharing sharing. Patient Educ Couns. 2020;103(5):1041-1048. doi:10.1016/j.pec.2019.12.006
5. Centers for Disease Control and Prevention. Facts about sexual violence. Updated July 5, 2022. Accessed July 13, 2022. https://www.cdc.gov/injury/features /sexual-violence/index.html
6. US Department of Veterans Affairs. Military sexual trauma. Updated May 16, 2022. Accessed July 13, 2022. https:// www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
7. Wang Z, Pukszta M. Private Rooms, Semi-open areas, or open areas for chemotherapy care: perspectives of cancer patients, families, and nursing staff. HERD. 2018;11(3):94- 108. doi:10.1177/1937586718758445
8. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Women veterans report: the past, present, and future of women veterans. Accessed July 13, 2022. https://www.va.gov/vetdata /docs/specialreports/women_veterans_2015_final.pdf
9. Driscoll MA, Higgins DM, Seng EK, et al. Trauma, social support, family conflict, and chronic pain in recent service veterans: does gender matter? Pain Med. 2015;16(6):1101- 1111. doi:10.1111/pme.12744
10. Fox AB, Meyer EC, Vogt D. Attitudes about the VA healthcare setting, mental illness, and mental health treatment and their relationship with VA mental health service use among female and male OEF/OIF veterans. Psychol Serv. 2015;12(1):49-58. doi:10.1037/a0038269
11. Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115(1):21-26. doi:10.1016/j.amjcard.2014.09.041
12. Tseng J. Sex, gender, and why the differences matter. Virtual Mentor. 2008;10(7):427-428. doi:10.1001/virtualmentor.2008.10.7.fred1-0807
13. Booij JC, Zegers M, Evers PMPJ, Hendricks M, Delnoij DMJ, Rademakers JJDJM. Improving cancer patient care: development of a generic cancer consumer quality index questionnaire for cancer patients. BMC Cancer. 2013;13(203). doi:10.1186/1471-2407-13-203
14. Meropol NJ, Egleston BL, Buzaglo JS, et al. Cancer patient preferences for quality and length of life. Cancer. 2008;113(12):3459-3466. doi:10.1002/cncr.23968 1
5. Schnur JB, Dillon MJ, Goldsmith RE, Montgomery GH. Cancer treatment experiences among survivors of childhood sexual abuse: a qualitative investigation of triggers and reactions to cumulative trauma. Palliat Support Care. 2018;16(6):767-776. doi:10.1017/S147895151700075X
16. Cadman L, Waller J, Ashdown-Barr L, Szarewski A. Barriers to cervical screening in women who have experienced sexual abuse: an exploratory study. J Fam Plann Reprod Health Care. 2012;38(4):214-220. doi:10.1136/jfprhc-2012-100378
17. Kelly S. The effects of childhood sexual abuse on women’s lives and their attitudes to cervical screening. J Fam Plann Reprod Health Care. 2012;38(4):212-213. doi:10.1136/jfprhc-2012-100418
18. McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep. 2006;121(4):435-444. doi:10.1177/003335490612100412
Pervasive ‘forever chemical’ linked to liver cancer
The correlation does not prove that PFOS causes this cancer, and more research is needed, but in the meantime, people should limit their exposure to it and others in its class, said Jesse Goodrich, PhD, a postdoctoral scholar in environmental medicine at the University of Southern California, Los Angeles.
“If you’re at risk for liver cancer because you have other risk factors, then these chemicals have the potential to kind of send you over the edge,” he told this news organization.
Dr. Goodrich and colleagues published their research online in JHEP Reports.
Dubbed “forever chemicals” because they can take thousands of years to break down, polyfluoroalkyl substances (PFAS) figure in makeup, food packaging, waterproof clothing, nonstick cookware, firefighting foams, and groundwater. They have spread through the atmosphere into rain and can be found in the blood of most Americans. PFOS is one of the most widely used PFAS.
“You can’t really escape them,” Dr. Goodrich said.
Previous research has linked PFAS to infertility, pregnancy complications, learning and behavioral problems in children, immune system issues, and higher cholesterol, as well as other cancers. Some experiments in animals suggested PFAS could cause liver cancer, and others showed a correlation between PFAS serum levels and biomarkers associated with liver cancer. But many of these health effects take a long time to develop.
“It wasn’t until we started to get really highly exposed groups of people that we started, as scientists, to be able to figure out what was going on,” said Dr. Goodrich.
High exposure, increased incidence
To measure the relationship between PFAS exposure and the incidence of hepatocellular carcinoma more definitively, Dr. Goodrich and colleagues analyzed data from the Multiethnic Cohort Study, a cohort of more than 200,000 people of African, Latin, Native Hawaiian, Japanese, and European ancestry tracked since the early 1990s in California and Hawaii. About 67,000 participants provided blood samples from 2001 to 2007.
From this cohort, the researchers found 50 people who later developed hepatocellular carcinoma. The researchers matched these patients with 50 controls of similar age at blood collection, sex, race, ethnicity, and study area who did not develop the cancer.
They found that people with more than 54.9 mcg/L of PFOS in their blood before any diagnosis of hepatocellular carcinoma were almost five times more likely to get the cancer (odds ratio 4.5; 95% confidence interval, 1.2-16.0), which was statistically significant (P = .02).
This level of PFOS corresponds to the 90th percentile found in the U.S. National Health and Nutrition Examination Survey (NHANES).
To get some idea of the mechanism by which PFOS might do its damage, the researchers also looked for linkage to levels of metabolites.
They found an overlap among high PFOS levels, hepatocellular carcinoma, and high levels of glucose, butyric acid (a short chain fatty acid), alpha-Ketoisovaleric acid (alpha branched-chain alpha-keto acid), and 7alpha-Hydroxy-3-oxo-4-cholestenoate (a bile acid). These metabolites have been associated in previous studies with metabolic disorders and liver disease.
Similarly, the researchers identified an association among the cancer, PFOS, and alterations in amino acid and glycan biosynthesis pathways.
Risk mitigation
The half-life of PFAS in the human body is about 3-7 years, said Dr. Goodrich.
“There’s not much you can do once they’re in there,” he said. “So, the focus needs to be on preventing the exposure in the first place.”
People can limit exposure by avoiding water contaminated with PFAS or filtering it out, Dr. Goodrich said. He recommended avoiding fish from contaminated waterways and nonstick cookware. The Environmental Protection Agency has more detailed recommendations.
But giving patients individualized recommendations is difficult, said Vincent Chen, MD, MS, a clinical instructor in gastroenterology at the University of Michigan, Ann Arbor, who was not involved in the study. Most clinicians don’t know their patients’ PFOS levels.
“It’s not that easy to get a test,” Dr. Chen told this news organization.
People can also mitigate their risk factors for hepatocellular carcinoma, such as a poor diet, a lack of exercise, and smoking, said Dr. Goodrich.
The researchers found that patients with hepatocellular carcinoma were more likely to be overweight and have diabetes, and PFOS was associated with higher fasting glucose levels. This raises the possibility that PFOS increases the risk for hepatocellular carcinoma by causing diabetes and obesity.
Dr. Goodrich and his colleagues tried to address this question by adjusting for baseline body mass index (BMI) and diabetes diagnosis in their statistical analysis.
After adjusting for BMI, they found that the association between PFOS and hepatocellular carcinoma diminished to a threefold risk (OR, 2.90; 95% CI, 0.78-10.00) and was no longer statistically significant (P = .11).
On the other hand, adjusting for diabetes did not change the significance of the relationship between PFOS and the cancer (OR, 5.7; 95% CI, 1.10-30.00; P = .04).
The sample size was probably too small to adequately tease out this relationship, Dr. Chen said. Still, he said, “I thought it was a very, very important study.”
The levels of PFOS found in the blood of Americans has been declining since the 1999-2000 NHANES, Dr. Chen pointed out. But that’s not as reassuring as it sounds.
“The problem is that if you put a regulation limiting the use of one PFAS, what people can do is just substitute with another PFAS or another molecule, which for all we know could be equally harmful,” Dr. Chen said.
Funding was provided by the Southern California Environmental Health Science Center supported by the National Institutes of Health. Dr. Goodrich and Dr. Chen report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The correlation does not prove that PFOS causes this cancer, and more research is needed, but in the meantime, people should limit their exposure to it and others in its class, said Jesse Goodrich, PhD, a postdoctoral scholar in environmental medicine at the University of Southern California, Los Angeles.
“If you’re at risk for liver cancer because you have other risk factors, then these chemicals have the potential to kind of send you over the edge,” he told this news organization.
Dr. Goodrich and colleagues published their research online in JHEP Reports.
Dubbed “forever chemicals” because they can take thousands of years to break down, polyfluoroalkyl substances (PFAS) figure in makeup, food packaging, waterproof clothing, nonstick cookware, firefighting foams, and groundwater. They have spread through the atmosphere into rain and can be found in the blood of most Americans. PFOS is one of the most widely used PFAS.
“You can’t really escape them,” Dr. Goodrich said.
Previous research has linked PFAS to infertility, pregnancy complications, learning and behavioral problems in children, immune system issues, and higher cholesterol, as well as other cancers. Some experiments in animals suggested PFAS could cause liver cancer, and others showed a correlation between PFAS serum levels and biomarkers associated with liver cancer. But many of these health effects take a long time to develop.
“It wasn’t until we started to get really highly exposed groups of people that we started, as scientists, to be able to figure out what was going on,” said Dr. Goodrich.
High exposure, increased incidence
To measure the relationship between PFAS exposure and the incidence of hepatocellular carcinoma more definitively, Dr. Goodrich and colleagues analyzed data from the Multiethnic Cohort Study, a cohort of more than 200,000 people of African, Latin, Native Hawaiian, Japanese, and European ancestry tracked since the early 1990s in California and Hawaii. About 67,000 participants provided blood samples from 2001 to 2007.
From this cohort, the researchers found 50 people who later developed hepatocellular carcinoma. The researchers matched these patients with 50 controls of similar age at blood collection, sex, race, ethnicity, and study area who did not develop the cancer.
They found that people with more than 54.9 mcg/L of PFOS in their blood before any diagnosis of hepatocellular carcinoma were almost five times more likely to get the cancer (odds ratio 4.5; 95% confidence interval, 1.2-16.0), which was statistically significant (P = .02).
This level of PFOS corresponds to the 90th percentile found in the U.S. National Health and Nutrition Examination Survey (NHANES).
To get some idea of the mechanism by which PFOS might do its damage, the researchers also looked for linkage to levels of metabolites.
They found an overlap among high PFOS levels, hepatocellular carcinoma, and high levels of glucose, butyric acid (a short chain fatty acid), alpha-Ketoisovaleric acid (alpha branched-chain alpha-keto acid), and 7alpha-Hydroxy-3-oxo-4-cholestenoate (a bile acid). These metabolites have been associated in previous studies with metabolic disorders and liver disease.
Similarly, the researchers identified an association among the cancer, PFOS, and alterations in amino acid and glycan biosynthesis pathways.
Risk mitigation
The half-life of PFAS in the human body is about 3-7 years, said Dr. Goodrich.
“There’s not much you can do once they’re in there,” he said. “So, the focus needs to be on preventing the exposure in the first place.”
People can limit exposure by avoiding water contaminated with PFAS or filtering it out, Dr. Goodrich said. He recommended avoiding fish from contaminated waterways and nonstick cookware. The Environmental Protection Agency has more detailed recommendations.
But giving patients individualized recommendations is difficult, said Vincent Chen, MD, MS, a clinical instructor in gastroenterology at the University of Michigan, Ann Arbor, who was not involved in the study. Most clinicians don’t know their patients’ PFOS levels.
“It’s not that easy to get a test,” Dr. Chen told this news organization.
People can also mitigate their risk factors for hepatocellular carcinoma, such as a poor diet, a lack of exercise, and smoking, said Dr. Goodrich.
The researchers found that patients with hepatocellular carcinoma were more likely to be overweight and have diabetes, and PFOS was associated with higher fasting glucose levels. This raises the possibility that PFOS increases the risk for hepatocellular carcinoma by causing diabetes and obesity.
Dr. Goodrich and his colleagues tried to address this question by adjusting for baseline body mass index (BMI) and diabetes diagnosis in their statistical analysis.
After adjusting for BMI, they found that the association between PFOS and hepatocellular carcinoma diminished to a threefold risk (OR, 2.90; 95% CI, 0.78-10.00) and was no longer statistically significant (P = .11).
On the other hand, adjusting for diabetes did not change the significance of the relationship between PFOS and the cancer (OR, 5.7; 95% CI, 1.10-30.00; P = .04).
The sample size was probably too small to adequately tease out this relationship, Dr. Chen said. Still, he said, “I thought it was a very, very important study.”
The levels of PFOS found in the blood of Americans has been declining since the 1999-2000 NHANES, Dr. Chen pointed out. But that’s not as reassuring as it sounds.
“The problem is that if you put a regulation limiting the use of one PFAS, what people can do is just substitute with another PFAS or another molecule, which for all we know could be equally harmful,” Dr. Chen said.
Funding was provided by the Southern California Environmental Health Science Center supported by the National Institutes of Health. Dr. Goodrich and Dr. Chen report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The correlation does not prove that PFOS causes this cancer, and more research is needed, but in the meantime, people should limit their exposure to it and others in its class, said Jesse Goodrich, PhD, a postdoctoral scholar in environmental medicine at the University of Southern California, Los Angeles.
“If you’re at risk for liver cancer because you have other risk factors, then these chemicals have the potential to kind of send you over the edge,” he told this news organization.
Dr. Goodrich and colleagues published their research online in JHEP Reports.
Dubbed “forever chemicals” because they can take thousands of years to break down, polyfluoroalkyl substances (PFAS) figure in makeup, food packaging, waterproof clothing, nonstick cookware, firefighting foams, and groundwater. They have spread through the atmosphere into rain and can be found in the blood of most Americans. PFOS is one of the most widely used PFAS.
“You can’t really escape them,” Dr. Goodrich said.
Previous research has linked PFAS to infertility, pregnancy complications, learning and behavioral problems in children, immune system issues, and higher cholesterol, as well as other cancers. Some experiments in animals suggested PFAS could cause liver cancer, and others showed a correlation between PFAS serum levels and biomarkers associated with liver cancer. But many of these health effects take a long time to develop.
“It wasn’t until we started to get really highly exposed groups of people that we started, as scientists, to be able to figure out what was going on,” said Dr. Goodrich.
High exposure, increased incidence
To measure the relationship between PFAS exposure and the incidence of hepatocellular carcinoma more definitively, Dr. Goodrich and colleagues analyzed data from the Multiethnic Cohort Study, a cohort of more than 200,000 people of African, Latin, Native Hawaiian, Japanese, and European ancestry tracked since the early 1990s in California and Hawaii. About 67,000 participants provided blood samples from 2001 to 2007.
From this cohort, the researchers found 50 people who later developed hepatocellular carcinoma. The researchers matched these patients with 50 controls of similar age at blood collection, sex, race, ethnicity, and study area who did not develop the cancer.
They found that people with more than 54.9 mcg/L of PFOS in their blood before any diagnosis of hepatocellular carcinoma were almost five times more likely to get the cancer (odds ratio 4.5; 95% confidence interval, 1.2-16.0), which was statistically significant (P = .02).
This level of PFOS corresponds to the 90th percentile found in the U.S. National Health and Nutrition Examination Survey (NHANES).
To get some idea of the mechanism by which PFOS might do its damage, the researchers also looked for linkage to levels of metabolites.
They found an overlap among high PFOS levels, hepatocellular carcinoma, and high levels of glucose, butyric acid (a short chain fatty acid), alpha-Ketoisovaleric acid (alpha branched-chain alpha-keto acid), and 7alpha-Hydroxy-3-oxo-4-cholestenoate (a bile acid). These metabolites have been associated in previous studies with metabolic disorders and liver disease.
Similarly, the researchers identified an association among the cancer, PFOS, and alterations in amino acid and glycan biosynthesis pathways.
Risk mitigation
The half-life of PFAS in the human body is about 3-7 years, said Dr. Goodrich.
“There’s not much you can do once they’re in there,” he said. “So, the focus needs to be on preventing the exposure in the first place.”
People can limit exposure by avoiding water contaminated with PFAS or filtering it out, Dr. Goodrich said. He recommended avoiding fish from contaminated waterways and nonstick cookware. The Environmental Protection Agency has more detailed recommendations.
But giving patients individualized recommendations is difficult, said Vincent Chen, MD, MS, a clinical instructor in gastroenterology at the University of Michigan, Ann Arbor, who was not involved in the study. Most clinicians don’t know their patients’ PFOS levels.
“It’s not that easy to get a test,” Dr. Chen told this news organization.
People can also mitigate their risk factors for hepatocellular carcinoma, such as a poor diet, a lack of exercise, and smoking, said Dr. Goodrich.
The researchers found that patients with hepatocellular carcinoma were more likely to be overweight and have diabetes, and PFOS was associated with higher fasting glucose levels. This raises the possibility that PFOS increases the risk for hepatocellular carcinoma by causing diabetes and obesity.
Dr. Goodrich and his colleagues tried to address this question by adjusting for baseline body mass index (BMI) and diabetes diagnosis in their statistical analysis.
After adjusting for BMI, they found that the association between PFOS and hepatocellular carcinoma diminished to a threefold risk (OR, 2.90; 95% CI, 0.78-10.00) and was no longer statistically significant (P = .11).
On the other hand, adjusting for diabetes did not change the significance of the relationship between PFOS and the cancer (OR, 5.7; 95% CI, 1.10-30.00; P = .04).
The sample size was probably too small to adequately tease out this relationship, Dr. Chen said. Still, he said, “I thought it was a very, very important study.”
The levels of PFOS found in the blood of Americans has been declining since the 1999-2000 NHANES, Dr. Chen pointed out. But that’s not as reassuring as it sounds.
“The problem is that if you put a regulation limiting the use of one PFAS, what people can do is just substitute with another PFAS or another molecule, which for all we know could be equally harmful,” Dr. Chen said.
Funding was provided by the Southern California Environmental Health Science Center supported by the National Institutes of Health. Dr. Goodrich and Dr. Chen report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JHEP REPORTS
Leukemia rates two to three times higher in children born near fracking
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Lung adverse effects in patients taking trastuzumab deruxtecan
although the benefit-to-risk relationship with use of the drug is still positive, say researchers who report a review of early clinical trials with the drug.
T-DXd is a monoclonal antibody that targets HER2. It is approved for use in HER2-positive breast, gastric, and lung cancers.
In the new study, investigators analyzed data from early clinical trials that involved patients with advanced cancers who had been heavily pretreated. They found an incidence of just over 15% for interstitial lung disease (ILD)/pneumonitis associated with the drug. Most patients (77.4%) had grade 1 or 2 ILD, but 2.2% of patients had grade 5 ILD.
“Interstitial lung disease is a known risk factor in patients treated with antibody conjugates for cancer,” commented lead author Charles Powell, MD, Icahn School of Medicine at Mount Sinai, New York. This adverse effect can lead to lung fibrosis and can become severe, life threatening, and even fatal, the authors warned.
The authors also discussed management of the event, which involves corticosteroids, and recommended that any patient who develops ILD of grade 3 or higher be hospitalized.
Close monitoring and proactive management may reduce the risk of ILD, they suggested.
Indeed, the incidence of this adverse effect was lower in a later phase 3 trial of the drug (10.5% in the DESTINY-Breast03 trial) and that the adverse events were less severe in this patient population (none of these events were of grade 4 or 5).
“Increased knowledge ... and implementation of ILD/pneumonitis monitoring, diagnosis, and management guidelines” may have resulted in this adverse effect being identified early and treated before it progressed, they commented.
ILD is highlighted in a boxed warning on the product label.
The study was published online in ESMO Open.
In their review, the investigators evaluated nine early-stage monotherapy clinical trials (phases 1 and 2) involving a total of 1,150 patients (breast cancer, 44.3%; gastric cancer, 25.6%; lung cancer, 17.7%; colorectal cancer, 9.3%, other cancers, 3.0%).
These patients had advanced cancer and had been heavily pretreated with a median of four prior lines of therapy. They received one or more doses of at least 5.4 mg/kg of T-DXd.
Nearly half of the cohort were treated for more than 6 months. A total of 276 potential ILD/pneumonitis events were sent for adjudication; of those, 85% were adjudicated as ILD/pneumonitis.
The overall incidence of adjudicated ILD/pneumonitis events was 15.4%; most were low-grade events. Some 87% of patients experienced their first ILD event within 12 months of treatment. The median time to experiencing an ILD/pneumonitis event was 5.4 months.
Some of the patients who developed grade 1 ILD/pneumonitis were treated and the adverse event resolved. These patients were then rechallenged with the drug. Only 3 of the 47 rechallenged patients experienced recurrence of ILD/pneumonitis, the authors noted.
“Rechallenge with T-DXd after complete resolution of grade 1 events is possible and warrants further investigation,” they commented. They cautioned, however, that rechallenge is not recommended for all patients, at least not for those with grade 2 or higher ILD/pneumonitis.
Overall, the authors concluded that the “benefit-risk of T-DXd treatment is positive,” but they warned that some patients may be at increased risk of developing ILD/pneumonitis
Baseline factors that increase the risk of developing an ILD/pneumonitis event include the following: being younger than 65 years, receiving a T-DXd dose of more than6.4 mg/kg, having a baseline oxygen saturation level of less than 95%, having moderate to severe renal impairment, and having lung comorbidities. In addition, patients who had initially been diagnosed with cancer more than 4 years before receiving the drug were at higher risk of developing ILD/pneumonitis.
“Using learnings from the early clinical trials experience, physician education and patient management protocols were revised and disseminated by the study sponsors [and] more recent trial data in earlier lines of therapy has demonstrated lower rates of ILD events, suggesting close monitoring and proactive management of ILD/pneumonitis is warranted for all patients,” Dr. Powell said in a statement.
The T-DXd clinical trials were sponsored by AstraZeneca and Daiichi Sankyo. Dr. Powell has received fees from Daiichi Sankyo, AstraZeneca, and Voluntis.
A version of this article first appeared on Medscape.com.
although the benefit-to-risk relationship with use of the drug is still positive, say researchers who report a review of early clinical trials with the drug.
T-DXd is a monoclonal antibody that targets HER2. It is approved for use in HER2-positive breast, gastric, and lung cancers.
In the new study, investigators analyzed data from early clinical trials that involved patients with advanced cancers who had been heavily pretreated. They found an incidence of just over 15% for interstitial lung disease (ILD)/pneumonitis associated with the drug. Most patients (77.4%) had grade 1 or 2 ILD, but 2.2% of patients had grade 5 ILD.
“Interstitial lung disease is a known risk factor in patients treated with antibody conjugates for cancer,” commented lead author Charles Powell, MD, Icahn School of Medicine at Mount Sinai, New York. This adverse effect can lead to lung fibrosis and can become severe, life threatening, and even fatal, the authors warned.
The authors also discussed management of the event, which involves corticosteroids, and recommended that any patient who develops ILD of grade 3 or higher be hospitalized.
Close monitoring and proactive management may reduce the risk of ILD, they suggested.
Indeed, the incidence of this adverse effect was lower in a later phase 3 trial of the drug (10.5% in the DESTINY-Breast03 trial) and that the adverse events were less severe in this patient population (none of these events were of grade 4 or 5).
“Increased knowledge ... and implementation of ILD/pneumonitis monitoring, diagnosis, and management guidelines” may have resulted in this adverse effect being identified early and treated before it progressed, they commented.
ILD is highlighted in a boxed warning on the product label.
The study was published online in ESMO Open.
In their review, the investigators evaluated nine early-stage monotherapy clinical trials (phases 1 and 2) involving a total of 1,150 patients (breast cancer, 44.3%; gastric cancer, 25.6%; lung cancer, 17.7%; colorectal cancer, 9.3%, other cancers, 3.0%).
These patients had advanced cancer and had been heavily pretreated with a median of four prior lines of therapy. They received one or more doses of at least 5.4 mg/kg of T-DXd.
Nearly half of the cohort were treated for more than 6 months. A total of 276 potential ILD/pneumonitis events were sent for adjudication; of those, 85% were adjudicated as ILD/pneumonitis.
The overall incidence of adjudicated ILD/pneumonitis events was 15.4%; most were low-grade events. Some 87% of patients experienced their first ILD event within 12 months of treatment. The median time to experiencing an ILD/pneumonitis event was 5.4 months.
Some of the patients who developed grade 1 ILD/pneumonitis were treated and the adverse event resolved. These patients were then rechallenged with the drug. Only 3 of the 47 rechallenged patients experienced recurrence of ILD/pneumonitis, the authors noted.
“Rechallenge with T-DXd after complete resolution of grade 1 events is possible and warrants further investigation,” they commented. They cautioned, however, that rechallenge is not recommended for all patients, at least not for those with grade 2 or higher ILD/pneumonitis.
Overall, the authors concluded that the “benefit-risk of T-DXd treatment is positive,” but they warned that some patients may be at increased risk of developing ILD/pneumonitis
Baseline factors that increase the risk of developing an ILD/pneumonitis event include the following: being younger than 65 years, receiving a T-DXd dose of more than6.4 mg/kg, having a baseline oxygen saturation level of less than 95%, having moderate to severe renal impairment, and having lung comorbidities. In addition, patients who had initially been diagnosed with cancer more than 4 years before receiving the drug were at higher risk of developing ILD/pneumonitis.
“Using learnings from the early clinical trials experience, physician education and patient management protocols were revised and disseminated by the study sponsors [and] more recent trial data in earlier lines of therapy has demonstrated lower rates of ILD events, suggesting close monitoring and proactive management of ILD/pneumonitis is warranted for all patients,” Dr. Powell said in a statement.
The T-DXd clinical trials were sponsored by AstraZeneca and Daiichi Sankyo. Dr. Powell has received fees from Daiichi Sankyo, AstraZeneca, and Voluntis.
A version of this article first appeared on Medscape.com.
although the benefit-to-risk relationship with use of the drug is still positive, say researchers who report a review of early clinical trials with the drug.
T-DXd is a monoclonal antibody that targets HER2. It is approved for use in HER2-positive breast, gastric, and lung cancers.
In the new study, investigators analyzed data from early clinical trials that involved patients with advanced cancers who had been heavily pretreated. They found an incidence of just over 15% for interstitial lung disease (ILD)/pneumonitis associated with the drug. Most patients (77.4%) had grade 1 or 2 ILD, but 2.2% of patients had grade 5 ILD.
“Interstitial lung disease is a known risk factor in patients treated with antibody conjugates for cancer,” commented lead author Charles Powell, MD, Icahn School of Medicine at Mount Sinai, New York. This adverse effect can lead to lung fibrosis and can become severe, life threatening, and even fatal, the authors warned.
The authors also discussed management of the event, which involves corticosteroids, and recommended that any patient who develops ILD of grade 3 or higher be hospitalized.
Close monitoring and proactive management may reduce the risk of ILD, they suggested.
Indeed, the incidence of this adverse effect was lower in a later phase 3 trial of the drug (10.5% in the DESTINY-Breast03 trial) and that the adverse events were less severe in this patient population (none of these events were of grade 4 or 5).
“Increased knowledge ... and implementation of ILD/pneumonitis monitoring, diagnosis, and management guidelines” may have resulted in this adverse effect being identified early and treated before it progressed, they commented.
ILD is highlighted in a boxed warning on the product label.
The study was published online in ESMO Open.
In their review, the investigators evaluated nine early-stage monotherapy clinical trials (phases 1 and 2) involving a total of 1,150 patients (breast cancer, 44.3%; gastric cancer, 25.6%; lung cancer, 17.7%; colorectal cancer, 9.3%, other cancers, 3.0%).
These patients had advanced cancer and had been heavily pretreated with a median of four prior lines of therapy. They received one or more doses of at least 5.4 mg/kg of T-DXd.
Nearly half of the cohort were treated for more than 6 months. A total of 276 potential ILD/pneumonitis events were sent for adjudication; of those, 85% were adjudicated as ILD/pneumonitis.
The overall incidence of adjudicated ILD/pneumonitis events was 15.4%; most were low-grade events. Some 87% of patients experienced their first ILD event within 12 months of treatment. The median time to experiencing an ILD/pneumonitis event was 5.4 months.
Some of the patients who developed grade 1 ILD/pneumonitis were treated and the adverse event resolved. These patients were then rechallenged with the drug. Only 3 of the 47 rechallenged patients experienced recurrence of ILD/pneumonitis, the authors noted.
“Rechallenge with T-DXd after complete resolution of grade 1 events is possible and warrants further investigation,” they commented. They cautioned, however, that rechallenge is not recommended for all patients, at least not for those with grade 2 or higher ILD/pneumonitis.
Overall, the authors concluded that the “benefit-risk of T-DXd treatment is positive,” but they warned that some patients may be at increased risk of developing ILD/pneumonitis
Baseline factors that increase the risk of developing an ILD/pneumonitis event include the following: being younger than 65 years, receiving a T-DXd dose of more than6.4 mg/kg, having a baseline oxygen saturation level of less than 95%, having moderate to severe renal impairment, and having lung comorbidities. In addition, patients who had initially been diagnosed with cancer more than 4 years before receiving the drug were at higher risk of developing ILD/pneumonitis.
“Using learnings from the early clinical trials experience, physician education and patient management protocols were revised and disseminated by the study sponsors [and] more recent trial data in earlier lines of therapy has demonstrated lower rates of ILD events, suggesting close monitoring and proactive management of ILD/pneumonitis is warranted for all patients,” Dr. Powell said in a statement.
The T-DXd clinical trials were sponsored by AstraZeneca and Daiichi Sankyo. Dr. Powell has received fees from Daiichi Sankyo, AstraZeneca, and Voluntis.
A version of this article first appeared on Medscape.com.
FROM ESMO OPEN
The ‘great dynamism’ of radiation oncology
The field of radiation oncology has rapidly evolved in recent years, thanks in large part to findings from randomized clinical trials (RCTs) that have helped shift therapeutic standards, a review of the literature shows.
Highlights from this research reveal how high-tech radiotherapy, such as hypofractionation and stereotactic body radiotherapy, has improved care for many patients, how personalized radiotherapy using image-based guidance has helped tailor treatments, and how endpoints that focus on quality of life and patient satisfaction are emerging.
For instance, Charles B. Simone II, MD, FACRO, who was not involved in the current work, pointed to “a proliferation of trials assessing hypofractionation in the curative setting and stereotactic body radiation therapy in the curative and poly- and oligometastatic settings that have allowed for increased patient convenience and dose intensification, respectively.”
Dr. Simone, chief medical officer, New York Proton Center, Memorial Sloan Kettering Cancer Center, also noted that the first personalized radiotherapy trials using imaging and biological markers have “the profound potential to individualize treatment and improve patient outcomes.”
The review was published in the European Journal of Cancer.
An evolving field
Given the fast-changing landscape for cancer therapeutics and a deluge of research studies, the authors wanted to understand the most notable advances established in recent trials as well as caveats to some approaches and emerging areas to watch.
In the review, Sophie Espenel, MD, from the department of radiation oncology, Gustave Roussy Cancer Campus, Villejuif, France, and colleagues identified 1,347 radiotherapy RCTs that were conducted from January 2018 to December 2021. Of these, the authors selected 110 large phase 2 or 3 RCTs that contained data showing practice-changing or emerging concepts.
Overall, the studies showed “great dynamism” in radiation oncology research and covered a wide range of radiotherapy practices, according to Dr. Espenel and coauthors.
A central area of research has focused on radioimmunotherapy, an approach that aims to enhance the antitumor immune response. One RCT in the preoperative setting showed, for instance, that concurrent stereotactic body radiotherapy delivered at 24 Gy over eight fractions, along with the anti–PD-L1 agent durvalumab, increased major pathologic complete response rates almost eightfold in comparison with durvalumab alone for patients with early-stage lung cancer (53.3% vs. 6.7%).
Although promising, not all trials that evaluated a concurrent chemoradiotherapy-immunotherapy strategy showed positive results. One RCT of locally advanced head and neck squamous cell carcinoma, for instance, found that median progression-free survival was not reached when adding the anti–PD-L1 avelumab to chemoradiotherapy. In addition, trials in the metastatic setting have shown conflicting results, the authors note.
Another topic of interest is that of newer radiosensitizers. A trial that evaluated high-risk locoregionally advanced head and neck squamous cell carcinoma highlighted the efficacy of xevinapant, a pro-apoptotic agent that inhibits apoptosis proteins. Xevinapant was used for the first time in conjunction with a standard high-dose cisplatin chemoradiotherapy. In this study, locoregional control at 18 months was achieved for 54% of patients who received xevinapant vs. 33% of those who received standard care. The toxicity profiles were similar.
The use of high-tech radiotherapy is gaining ground. It allows patients to receive more targeted treatments at lower doses and in shorter time frames. One trial found, for instance, that a more hypofractionated adjuvant whole breast approach, using 26 Gy in five fractions over a week, is as effective and safe as 40 Gy in 15 fractions over 3 weeks. The researchers found that there was no difference in the incidence of locoregional relapses, disease-free survival, and overall survival between the regimens.
Dr. Simone also noted that advanced treatment modalities, such as intensity-modulated radiotherapy, stereotactic radiosurgery, and proton therapy, have the potential to improve patient-reported adverse events and clinical outcomes. “I have seen this both in my clinical practice and in several recent publications,” he says.
Personalization of radiotherapy is also an emerging area that may allow for more tailored treatments with improved outcomes. The authors highlighted a study that found that PMSA PET-CT was better than conventional CT for accurately staging prostate cancer. This approach was also less expensive and led to less radiation exposure.
On the basis of this research, “PMSA PET-CT has since become the [standard of care] for prostate cancer staging,” the authors explain.
Dr. Espenel and colleagues note that as patients survive longer, quality of life and patient satisfaction are increasingly becoming endpoints in RCTs. Experts are focusing more attention on sequelae of treatments and advances in technology that can spare critical organs from radiation and reduce overall treatment time.
Shared decision-making is becoming increasingly possible in many cases as well. For example, with some clinical trials that involved different treatment modalities, outcomes were equivalent, but toxicity profiles differed, allowing patients to choose therapeutic options tailored to their preferences.
Overall, these data demonstrate “a great dynamism of radiation oncology research in most primary tumor types,” the researchers write.
The study received no outside financial support. The authors have disclosed no relevant financial relationships. Dr. Simone is chair of the American Society for Radiation Oncology Lung Resource Panel and the American Society for Radiation Oncology Veteran Affairs Radiation Oncology Quality Surveillance Blue Ribbon Lung Panel and has received honorarium from Varian Medical Systems.
A version of this article first appeared on Medscape.com.
The field of radiation oncology has rapidly evolved in recent years, thanks in large part to findings from randomized clinical trials (RCTs) that have helped shift therapeutic standards, a review of the literature shows.
Highlights from this research reveal how high-tech radiotherapy, such as hypofractionation and stereotactic body radiotherapy, has improved care for many patients, how personalized radiotherapy using image-based guidance has helped tailor treatments, and how endpoints that focus on quality of life and patient satisfaction are emerging.
For instance, Charles B. Simone II, MD, FACRO, who was not involved in the current work, pointed to “a proliferation of trials assessing hypofractionation in the curative setting and stereotactic body radiation therapy in the curative and poly- and oligometastatic settings that have allowed for increased patient convenience and dose intensification, respectively.”
Dr. Simone, chief medical officer, New York Proton Center, Memorial Sloan Kettering Cancer Center, also noted that the first personalized radiotherapy trials using imaging and biological markers have “the profound potential to individualize treatment and improve patient outcomes.”
The review was published in the European Journal of Cancer.
An evolving field
Given the fast-changing landscape for cancer therapeutics and a deluge of research studies, the authors wanted to understand the most notable advances established in recent trials as well as caveats to some approaches and emerging areas to watch.
In the review, Sophie Espenel, MD, from the department of radiation oncology, Gustave Roussy Cancer Campus, Villejuif, France, and colleagues identified 1,347 radiotherapy RCTs that were conducted from January 2018 to December 2021. Of these, the authors selected 110 large phase 2 or 3 RCTs that contained data showing practice-changing or emerging concepts.
Overall, the studies showed “great dynamism” in radiation oncology research and covered a wide range of radiotherapy practices, according to Dr. Espenel and coauthors.
A central area of research has focused on radioimmunotherapy, an approach that aims to enhance the antitumor immune response. One RCT in the preoperative setting showed, for instance, that concurrent stereotactic body radiotherapy delivered at 24 Gy over eight fractions, along with the anti–PD-L1 agent durvalumab, increased major pathologic complete response rates almost eightfold in comparison with durvalumab alone for patients with early-stage lung cancer (53.3% vs. 6.7%).
Although promising, not all trials that evaluated a concurrent chemoradiotherapy-immunotherapy strategy showed positive results. One RCT of locally advanced head and neck squamous cell carcinoma, for instance, found that median progression-free survival was not reached when adding the anti–PD-L1 avelumab to chemoradiotherapy. In addition, trials in the metastatic setting have shown conflicting results, the authors note.
Another topic of interest is that of newer radiosensitizers. A trial that evaluated high-risk locoregionally advanced head and neck squamous cell carcinoma highlighted the efficacy of xevinapant, a pro-apoptotic agent that inhibits apoptosis proteins. Xevinapant was used for the first time in conjunction with a standard high-dose cisplatin chemoradiotherapy. In this study, locoregional control at 18 months was achieved for 54% of patients who received xevinapant vs. 33% of those who received standard care. The toxicity profiles were similar.
The use of high-tech radiotherapy is gaining ground. It allows patients to receive more targeted treatments at lower doses and in shorter time frames. One trial found, for instance, that a more hypofractionated adjuvant whole breast approach, using 26 Gy in five fractions over a week, is as effective and safe as 40 Gy in 15 fractions over 3 weeks. The researchers found that there was no difference in the incidence of locoregional relapses, disease-free survival, and overall survival between the regimens.
Dr. Simone also noted that advanced treatment modalities, such as intensity-modulated radiotherapy, stereotactic radiosurgery, and proton therapy, have the potential to improve patient-reported adverse events and clinical outcomes. “I have seen this both in my clinical practice and in several recent publications,” he says.
Personalization of radiotherapy is also an emerging area that may allow for more tailored treatments with improved outcomes. The authors highlighted a study that found that PMSA PET-CT was better than conventional CT for accurately staging prostate cancer. This approach was also less expensive and led to less radiation exposure.
On the basis of this research, “PMSA PET-CT has since become the [standard of care] for prostate cancer staging,” the authors explain.
Dr. Espenel and colleagues note that as patients survive longer, quality of life and patient satisfaction are increasingly becoming endpoints in RCTs. Experts are focusing more attention on sequelae of treatments and advances in technology that can spare critical organs from radiation and reduce overall treatment time.
Shared decision-making is becoming increasingly possible in many cases as well. For example, with some clinical trials that involved different treatment modalities, outcomes were equivalent, but toxicity profiles differed, allowing patients to choose therapeutic options tailored to their preferences.
Overall, these data demonstrate “a great dynamism of radiation oncology research in most primary tumor types,” the researchers write.
The study received no outside financial support. The authors have disclosed no relevant financial relationships. Dr. Simone is chair of the American Society for Radiation Oncology Lung Resource Panel and the American Society for Radiation Oncology Veteran Affairs Radiation Oncology Quality Surveillance Blue Ribbon Lung Panel and has received honorarium from Varian Medical Systems.
A version of this article first appeared on Medscape.com.
The field of radiation oncology has rapidly evolved in recent years, thanks in large part to findings from randomized clinical trials (RCTs) that have helped shift therapeutic standards, a review of the literature shows.
Highlights from this research reveal how high-tech radiotherapy, such as hypofractionation and stereotactic body radiotherapy, has improved care for many patients, how personalized radiotherapy using image-based guidance has helped tailor treatments, and how endpoints that focus on quality of life and patient satisfaction are emerging.
For instance, Charles B. Simone II, MD, FACRO, who was not involved in the current work, pointed to “a proliferation of trials assessing hypofractionation in the curative setting and stereotactic body radiation therapy in the curative and poly- and oligometastatic settings that have allowed for increased patient convenience and dose intensification, respectively.”
Dr. Simone, chief medical officer, New York Proton Center, Memorial Sloan Kettering Cancer Center, also noted that the first personalized radiotherapy trials using imaging and biological markers have “the profound potential to individualize treatment and improve patient outcomes.”
The review was published in the European Journal of Cancer.
An evolving field
Given the fast-changing landscape for cancer therapeutics and a deluge of research studies, the authors wanted to understand the most notable advances established in recent trials as well as caveats to some approaches and emerging areas to watch.
In the review, Sophie Espenel, MD, from the department of radiation oncology, Gustave Roussy Cancer Campus, Villejuif, France, and colleagues identified 1,347 radiotherapy RCTs that were conducted from January 2018 to December 2021. Of these, the authors selected 110 large phase 2 or 3 RCTs that contained data showing practice-changing or emerging concepts.
Overall, the studies showed “great dynamism” in radiation oncology research and covered a wide range of radiotherapy practices, according to Dr. Espenel and coauthors.
A central area of research has focused on radioimmunotherapy, an approach that aims to enhance the antitumor immune response. One RCT in the preoperative setting showed, for instance, that concurrent stereotactic body radiotherapy delivered at 24 Gy over eight fractions, along with the anti–PD-L1 agent durvalumab, increased major pathologic complete response rates almost eightfold in comparison with durvalumab alone for patients with early-stage lung cancer (53.3% vs. 6.7%).
Although promising, not all trials that evaluated a concurrent chemoradiotherapy-immunotherapy strategy showed positive results. One RCT of locally advanced head and neck squamous cell carcinoma, for instance, found that median progression-free survival was not reached when adding the anti–PD-L1 avelumab to chemoradiotherapy. In addition, trials in the metastatic setting have shown conflicting results, the authors note.
Another topic of interest is that of newer radiosensitizers. A trial that evaluated high-risk locoregionally advanced head and neck squamous cell carcinoma highlighted the efficacy of xevinapant, a pro-apoptotic agent that inhibits apoptosis proteins. Xevinapant was used for the first time in conjunction with a standard high-dose cisplatin chemoradiotherapy. In this study, locoregional control at 18 months was achieved for 54% of patients who received xevinapant vs. 33% of those who received standard care. The toxicity profiles were similar.
The use of high-tech radiotherapy is gaining ground. It allows patients to receive more targeted treatments at lower doses and in shorter time frames. One trial found, for instance, that a more hypofractionated adjuvant whole breast approach, using 26 Gy in five fractions over a week, is as effective and safe as 40 Gy in 15 fractions over 3 weeks. The researchers found that there was no difference in the incidence of locoregional relapses, disease-free survival, and overall survival between the regimens.
Dr. Simone also noted that advanced treatment modalities, such as intensity-modulated radiotherapy, stereotactic radiosurgery, and proton therapy, have the potential to improve patient-reported adverse events and clinical outcomes. “I have seen this both in my clinical practice and in several recent publications,” he says.
Personalization of radiotherapy is also an emerging area that may allow for more tailored treatments with improved outcomes. The authors highlighted a study that found that PMSA PET-CT was better than conventional CT for accurately staging prostate cancer. This approach was also less expensive and led to less radiation exposure.
On the basis of this research, “PMSA PET-CT has since become the [standard of care] for prostate cancer staging,” the authors explain.
Dr. Espenel and colleagues note that as patients survive longer, quality of life and patient satisfaction are increasingly becoming endpoints in RCTs. Experts are focusing more attention on sequelae of treatments and advances in technology that can spare critical organs from radiation and reduce overall treatment time.
Shared decision-making is becoming increasingly possible in many cases as well. For example, with some clinical trials that involved different treatment modalities, outcomes were equivalent, but toxicity profiles differed, allowing patients to choose therapeutic options tailored to their preferences.
Overall, these data demonstrate “a great dynamism of radiation oncology research in most primary tumor types,” the researchers write.
The study received no outside financial support. The authors have disclosed no relevant financial relationships. Dr. Simone is chair of the American Society for Radiation Oncology Lung Resource Panel and the American Society for Radiation Oncology Veteran Affairs Radiation Oncology Quality Surveillance Blue Ribbon Lung Panel and has received honorarium from Varian Medical Systems.
A version of this article first appeared on Medscape.com.
FROM THE EUROPEAN JOURNAL OF CANCER
Where women’s voices still get heard less
“Our study provides the first analysis of gender and early-career faculty disparities in speakers at hematology and medical oncology board review meetings,” the authors reported in research published in Blood Advances.
“We covered six major board reviews over the last 5 years that are either conducted yearly or every other year, [and] the general trend across all meetings showed skewness toward men speakers,” the authors reported.
Recent data from 2021 suggests a closing of the gender gap in oncology, with women making up 44.6% of oncologists in training. However, they still only represented 35.2% of practicing oncologists and are underrepresented in leadership positions in academic oncology, the authors reported.
With speaking roles at academic meetings potentially marking a key step in career advancement and improved opportunities, the authors sought to investigate the balance of gender, as well as early-career faculty among speakers at prominent hematology and/or oncology board review lecture series taking place in the United States between 2017 and 2021.
The five institutions and one society presenting the board review lecture series included Baylor College of Medicine/MD Anderson Cancer Center, both in Houston; Dana-Farber Brigham Cancer Center, Boston; George Washington University, Washington; Memorial Sloan Kettering Cancer Center, New York; Seattle Cancer Care Alliance; and the hematology board review series from the American Society of Hematology.
During the period in question, among 1,224 board review lectures presented, women constituted only 37.7% of the speakers. In lectures presented by American Board of Internal Medicine–certified speakers (n = 1,016, 83%), women were found to have made up fewer than 50% of speakers in five of six courses.
Men were also more likely to be recurrent speakers; across all courses, 13 men but only 2 women conducted 10 or more lectures. And while 35 men gave six or more lectures across all courses, only 12 women did so.
The lecture topics with the lowest rates of women presenters included malignant hematology (24.8%), solid tumors (38.9%), and benign hematology lectures (44.1%).

“We suspected [the imbalance in malignant hematology] since multiple recurrent roles were concentrated in the malignant hematology,” senior author Samer Al Hadidi, MD, of the Myeloma Center, Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, AK, said in an interview.
He noted that “there are no regulations that such courses need to follow to ensure certain proportions of women and junior faculty are involved.”
Early-career faculty
In terms of early-career representation, more than 50% of lectures were given by faculty who had received their initial certifications more than 15 years earlier. The median time from initial certification was 12.5 years for hematology and 14 years for medical oncology.
The findings that more than half of the board review lectures were presented by faculty with more than 15 years’ experience since initial certification “reflects a lack of appropriate involvement of early-career faculty, who arguably may have more recent experience with board certification,” the authors wrote.
While being underrepresented in such roles is detrimental, there are no regulations that such courses follow to ensure certain proportions of women and junior faculty are involved, Dr. Al Hadidi noted.
Equal representation remains elusive
The study does suggest some notable gains. In a previous study of 181 academic conferences in the United States and Canada between 2007 and 2017, the rate of women speakers was only 15%, compared with 37.7% in the new study.
And an overall trend analysis in the study shows an approximately 10% increase in representation of women in all of the board reviews. However, only the ASH hematology board review achieved more than 50% women in their two courses.
“Overall, the proportion of women speakers is improving over the years, though it remains suboptimal,” Dr. Al Hadidi said.
The authors noted that oncology is clearly not the only specialty with gender disparities. They documented a lack of women speakers at conferences involving otolaryngology head and neck meetings, radiation oncology, emergency medicine, and research conferences.
They pointed to the work of ASH’s Women in Hematology Working Group as an important example of the needed effort to improve the balance of women hematologists.

Ariela Marshall, MD, director of women’s thrombosis and hemostasis at Penn Medicine in Philadelphia and a leader of ASH’s Women in Hematology Working Group, agreed that more efforts are needed to address both gender disparities as well as those of early career speakers. She asserted that the two disparities appear to be connected.
“If you broke down gender representation over time and the faculty/time since initial certification, the findings may mirror the percent of women in hematology-oncology at that given point in time,” Dr. Marshall said in an interview.
“If an institution is truly committed to taking action on gender equity, it needs to look at gender and experience equity of speakers,” she said. “Perhaps it’s the time to say ‘Dr. X has been doing this review course for 15 years. Let’s give someone else a chance.’
“This is not even just from a gender equity perspective but from a career development perspective overall,” she added. “Junior faculty need these speaking engagements a lot more than senior faculty.”
Meanwhile, the higher number of female trainees is a trend that ideally will be sustained as those trainees move into positions of leadership, Dr. Marshall noted.
“We do see that over time, we have achieved gender equity in the percent of women matriculating to medical school. And my hope is that, 20 years down the line, we will see the effects of this reflected in increased equity in leadership positions such as division/department chair, dean, and hospital CEO,” she said. “However, we have a lot of work to do because there are still huge inequities in the culture of medicine (institutional and more broadly), including gender-based discrimination, maternal discrimination, and high attrition rates for women physicians, compared to male physicians.
“It’s not enough to simply say ‘well, we have fixed the problem because our incoming medical student classes are now equitable in gender distribution,’ ”
The authors and Dr. Marshall had no disclosures to report.
“Our study provides the first analysis of gender and early-career faculty disparities in speakers at hematology and medical oncology board review meetings,” the authors reported in research published in Blood Advances.
“We covered six major board reviews over the last 5 years that are either conducted yearly or every other year, [and] the general trend across all meetings showed skewness toward men speakers,” the authors reported.
Recent data from 2021 suggests a closing of the gender gap in oncology, with women making up 44.6% of oncologists in training. However, they still only represented 35.2% of practicing oncologists and are underrepresented in leadership positions in academic oncology, the authors reported.
With speaking roles at academic meetings potentially marking a key step in career advancement and improved opportunities, the authors sought to investigate the balance of gender, as well as early-career faculty among speakers at prominent hematology and/or oncology board review lecture series taking place in the United States between 2017 and 2021.
The five institutions and one society presenting the board review lecture series included Baylor College of Medicine/MD Anderson Cancer Center, both in Houston; Dana-Farber Brigham Cancer Center, Boston; George Washington University, Washington; Memorial Sloan Kettering Cancer Center, New York; Seattle Cancer Care Alliance; and the hematology board review series from the American Society of Hematology.
During the period in question, among 1,224 board review lectures presented, women constituted only 37.7% of the speakers. In lectures presented by American Board of Internal Medicine–certified speakers (n = 1,016, 83%), women were found to have made up fewer than 50% of speakers in five of six courses.
Men were also more likely to be recurrent speakers; across all courses, 13 men but only 2 women conducted 10 or more lectures. And while 35 men gave six or more lectures across all courses, only 12 women did so.
The lecture topics with the lowest rates of women presenters included malignant hematology (24.8%), solid tumors (38.9%), and benign hematology lectures (44.1%).
“We suspected [the imbalance in malignant hematology] since multiple recurrent roles were concentrated in the malignant hematology,” senior author Samer Al Hadidi, MD, of the Myeloma Center, Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, AK, said in an interview.
He noted that “there are no regulations that such courses need to follow to ensure certain proportions of women and junior faculty are involved.”
Early-career faculty
In terms of early-career representation, more than 50% of lectures were given by faculty who had received their initial certifications more than 15 years earlier. The median time from initial certification was 12.5 years for hematology and 14 years for medical oncology.
The findings that more than half of the board review lectures were presented by faculty with more than 15 years’ experience since initial certification “reflects a lack of appropriate involvement of early-career faculty, who arguably may have more recent experience with board certification,” the authors wrote.
While being underrepresented in such roles is detrimental, there are no regulations that such courses follow to ensure certain proportions of women and junior faculty are involved, Dr. Al Hadidi noted.
Equal representation remains elusive
The study does suggest some notable gains. In a previous study of 181 academic conferences in the United States and Canada between 2007 and 2017, the rate of women speakers was only 15%, compared with 37.7% in the new study.
And an overall trend analysis in the study shows an approximately 10% increase in representation of women in all of the board reviews. However, only the ASH hematology board review achieved more than 50% women in their two courses.
“Overall, the proportion of women speakers is improving over the years, though it remains suboptimal,” Dr. Al Hadidi said.
The authors noted that oncology is clearly not the only specialty with gender disparities. They documented a lack of women speakers at conferences involving otolaryngology head and neck meetings, radiation oncology, emergency medicine, and research conferences.
They pointed to the work of ASH’s Women in Hematology Working Group as an important example of the needed effort to improve the balance of women hematologists.
Ariela Marshall, MD, director of women’s thrombosis and hemostasis at Penn Medicine in Philadelphia and a leader of ASH’s Women in Hematology Working Group, agreed that more efforts are needed to address both gender disparities as well as those of early career speakers. She asserted that the two disparities appear to be connected.
“If you broke down gender representation over time and the faculty/time since initial certification, the findings may mirror the percent of women in hematology-oncology at that given point in time,” Dr. Marshall said in an interview.
“If an institution is truly committed to taking action on gender equity, it needs to look at gender and experience equity of speakers,” she said. “Perhaps it’s the time to say ‘Dr. X has been doing this review course for 15 years. Let’s give someone else a chance.’
“This is not even just from a gender equity perspective but from a career development perspective overall,” she added. “Junior faculty need these speaking engagements a lot more than senior faculty.”
Meanwhile, the higher number of female trainees is a trend that ideally will be sustained as those trainees move into positions of leadership, Dr. Marshall noted.
“We do see that over time, we have achieved gender equity in the percent of women matriculating to medical school. And my hope is that, 20 years down the line, we will see the effects of this reflected in increased equity in leadership positions such as division/department chair, dean, and hospital CEO,” she said. “However, we have a lot of work to do because there are still huge inequities in the culture of medicine (institutional and more broadly), including gender-based discrimination, maternal discrimination, and high attrition rates for women physicians, compared to male physicians.
“It’s not enough to simply say ‘well, we have fixed the problem because our incoming medical student classes are now equitable in gender distribution,’ ”
The authors and Dr. Marshall had no disclosures to report.
“Our study provides the first analysis of gender and early-career faculty disparities in speakers at hematology and medical oncology board review meetings,” the authors reported in research published in Blood Advances.
“We covered six major board reviews over the last 5 years that are either conducted yearly or every other year, [and] the general trend across all meetings showed skewness toward men speakers,” the authors reported.
Recent data from 2021 suggests a closing of the gender gap in oncology, with women making up 44.6% of oncologists in training. However, they still only represented 35.2% of practicing oncologists and are underrepresented in leadership positions in academic oncology, the authors reported.
With speaking roles at academic meetings potentially marking a key step in career advancement and improved opportunities, the authors sought to investigate the balance of gender, as well as early-career faculty among speakers at prominent hematology and/or oncology board review lecture series taking place in the United States between 2017 and 2021.
The five institutions and one society presenting the board review lecture series included Baylor College of Medicine/MD Anderson Cancer Center, both in Houston; Dana-Farber Brigham Cancer Center, Boston; George Washington University, Washington; Memorial Sloan Kettering Cancer Center, New York; Seattle Cancer Care Alliance; and the hematology board review series from the American Society of Hematology.
During the period in question, among 1,224 board review lectures presented, women constituted only 37.7% of the speakers. In lectures presented by American Board of Internal Medicine–certified speakers (n = 1,016, 83%), women were found to have made up fewer than 50% of speakers in five of six courses.
Men were also more likely to be recurrent speakers; across all courses, 13 men but only 2 women conducted 10 or more lectures. And while 35 men gave six or more lectures across all courses, only 12 women did so.
The lecture topics with the lowest rates of women presenters included malignant hematology (24.8%), solid tumors (38.9%), and benign hematology lectures (44.1%).
“We suspected [the imbalance in malignant hematology] since multiple recurrent roles were concentrated in the malignant hematology,” senior author Samer Al Hadidi, MD, of the Myeloma Center, Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, AK, said in an interview.
He noted that “there are no regulations that such courses need to follow to ensure certain proportions of women and junior faculty are involved.”
Early-career faculty
In terms of early-career representation, more than 50% of lectures were given by faculty who had received their initial certifications more than 15 years earlier. The median time from initial certification was 12.5 years for hematology and 14 years for medical oncology.
The findings that more than half of the board review lectures were presented by faculty with more than 15 years’ experience since initial certification “reflects a lack of appropriate involvement of early-career faculty, who arguably may have more recent experience with board certification,” the authors wrote.
While being underrepresented in such roles is detrimental, there are no regulations that such courses follow to ensure certain proportions of women and junior faculty are involved, Dr. Al Hadidi noted.
Equal representation remains elusive
The study does suggest some notable gains. In a previous study of 181 academic conferences in the United States and Canada between 2007 and 2017, the rate of women speakers was only 15%, compared with 37.7% in the new study.
And an overall trend analysis in the study shows an approximately 10% increase in representation of women in all of the board reviews. However, only the ASH hematology board review achieved more than 50% women in their two courses.
“Overall, the proportion of women speakers is improving over the years, though it remains suboptimal,” Dr. Al Hadidi said.
The authors noted that oncology is clearly not the only specialty with gender disparities. They documented a lack of women speakers at conferences involving otolaryngology head and neck meetings, radiation oncology, emergency medicine, and research conferences.
They pointed to the work of ASH’s Women in Hematology Working Group as an important example of the needed effort to improve the balance of women hematologists.
Ariela Marshall, MD, director of women’s thrombosis and hemostasis at Penn Medicine in Philadelphia and a leader of ASH’s Women in Hematology Working Group, agreed that more efforts are needed to address both gender disparities as well as those of early career speakers. She asserted that the two disparities appear to be connected.
“If you broke down gender representation over time and the faculty/time since initial certification, the findings may mirror the percent of women in hematology-oncology at that given point in time,” Dr. Marshall said in an interview.
“If an institution is truly committed to taking action on gender equity, it needs to look at gender and experience equity of speakers,” she said. “Perhaps it’s the time to say ‘Dr. X has been doing this review course for 15 years. Let’s give someone else a chance.’
“This is not even just from a gender equity perspective but from a career development perspective overall,” she added. “Junior faculty need these speaking engagements a lot more than senior faculty.”
Meanwhile, the higher number of female trainees is a trend that ideally will be sustained as those trainees move into positions of leadership, Dr. Marshall noted.
“We do see that over time, we have achieved gender equity in the percent of women matriculating to medical school. And my hope is that, 20 years down the line, we will see the effects of this reflected in increased equity in leadership positions such as division/department chair, dean, and hospital CEO,” she said. “However, we have a lot of work to do because there are still huge inequities in the culture of medicine (institutional and more broadly), including gender-based discrimination, maternal discrimination, and high attrition rates for women physicians, compared to male physicians.
“It’s not enough to simply say ‘well, we have fixed the problem because our incoming medical student classes are now equitable in gender distribution,’ ”
The authors and Dr. Marshall had no disclosures to report.
FROM BLOOD ADVANCES
AML’s seasonal peak suggests viral or environmental etiology
Most diagnoses of acute myeloid leukemia (AML) are made during January. This finding strongly implies that seasonal factors, such as infectious agents or environmental triggers, influence the development or proliferation of the disease, which points to prevention opportunities. This was the conclusion of an international study led by a team from the Jiménez Díaz Foundation University Hospital Health Research Institute (IIS-FJD) in Madrid, in collaboration with colleagues from the University of Bristol, England. Their work was published in the British Journal of Haematology.
The study’s aim was to investigate the potential seasonal and long-term trends in AML diagnosis in an overall population and in subgroups according to sex and age. To do so, the researchers examined 26,472 cases of AML diagnosed in Spain between 2004 and 2015. They found seasonality in the diagnosis of this type of leukemia. This “could point to there being an underlying seasonal etiology at play,” noted one of the main authors of the study, Juan Manuel Alonso, MD, a physician in the IIS-FJD’s department of hematology and hemotherapy.
“The environmental triggers involved could be radiation, pollution, allergens, or infectious agents like viruses. We’re leaning toward viruses, because there are already distinct solid tumor and hematologic cancers that are caused by them and because, in the winter months, there’s an increased incidence of cancers due to viral infections,” Dr. Alonso said in an interview. “The etiological mechanism should be different from that exerted by chronic viral pressure, because here we’re dealing with an acute and aggressive disease that probably needs a short incubation period.”
Various hypotheses
In an interview, David Martínez, MD, a hematologist at La Fe University Hospital in Valencia, Spain, described the research as “an extremely well done and much-discussed study on AML, a disease that appears to be diagnosed more frequently at a certain time of year – namely, January.
“There’s no clear explanation for this finding,” Dr. Martínez said. “Several possible reasons have been put forward and are being talked about. The one that seems to hold the most water is the hypothesis that infectious agents and environmental factors may have a greater influence. This is because the idea that they’re involved in neoplastic diseases is nothing new. In fact, there are a lot of publications and a good amount of scientific evidence that link viral infections and environmental factors with the development of oncologic diseases.”
AML is a rare disease yet is responsible for many cancer-related deaths. Mutations that cause AML can occur due to an inherited mutant gene or exposure to certain carcinogens, such as chemotherapy, radiotherapy, ionizing radiation, tobacco, and benzene. These findings are broadly similar to those of a large U.S.-based study by Calip et al., who found a peak of adult AML diagnoses during December and January from 1992 to 2008. Previous smaller studies have provided conflicting evidence, likely due to lower power or to the use of less advanced statistical approaches.
Seasonal factors involved?
Demonstration of seasonal variation in the occurrence of AML would, firstly, provide supportive evidence of etiology by seasonal factors, such as infectious agents or environmental factors, and, secondly, focus research onto the etiologic role of such factors.
The current study used population-based data on cases of AML occurring in Spain from a nationwide hospital discharge registry for the years 2004 to 2015. “This is, to our knowledge, the largest study aimed at investigating the potential seasonal and long-term trends in AML incidence in an overall population and in subgroups according to sex and age while employing novel statistical models with serial dependence for discrete-valued time series,” wrote the researchers.
They extracted information from the register of each case about the date of admission, discharge date, the anonymous identifier for each patient, International Classification of Diseases (ICD)–9 codes, sex, and date of birth, from which they derived age groups as described for the at-risk population. For patients hospitalized on more than one occasion, only the record corresponding to their first diagnosis of AML was selected.
AML cases per month were standardized to months of equal length.
Age/sex-standardized monthly incidence rates of AML were calculated using the census of Spanish population in 2010 as a “standard” population. Age-standardized and sex-standardized monthly incidence rates of AML were calculated.
Nine separate time-series decompositions were performed as an initial exploratory analysis on the monthly incidence rates of AML using data for all cases and data for each sex and age group. Nine separate Poisson generalized linear autoregressive moving average (GLARMA) models were fitted to evaluate the temporal dynamics in AML incidence using data for all cases, and data for each sex and age group.
Long-term trend
A total of 26,472 patients with a first diagnosis of active AML were hospitalized in Spain and registered at the country’s Minimum Basic Data Set (CMBD) during 2004-2015. In the end, there were 26,475 patients in the study population; a greater proportion of cases were male (56.0%), and the median age at diagnosis was 67 years.
Seasonal and trend decomposition using Loess decomposition of the incidence rates observed in the overall population exhibited seasonal fluctuation with a peak in January. A slight upward trend was apparent from visual inspection with an upturn in early 2005 and a downturn at the end of 2013. As for the differences by sex groups and age groups, Dr. Alonso said, “For both sexes and in age groups 5-19, 20-49, and 50-64 years, we found that the results were identical to those found in the overall population.”
The final model included an upward linear long-term trend, as well as the variables monthly seasonality and December 2015. The estimated monthly long-term trend implies that the monthly incidence rates of AML diagnoses annually increased by 0.4% (95% confidence interval [CI], 0.2%-0.6%; P = .0011), given that the other covariates are held constant.
January displayed the highest incidence rate of AML, with a minimum average difference of 7%, when compared with February (95% CI, 2%-12%; P = .0143) and a maximum average difference of 16%, compared with November (95% CI, 11%-21%; P < .0001) and August (95% CI, 10%-21%; P < .0001).
The incidence rate of AML for December 2015 was 0.43 (95% CI, 0.34-0.54; P < .0001) times the average incidence rate for the rest of the study period.
Potential role of viruses
“We have to keep in mind that infectious agents (viral infections) and environmental factors (allergens) don’t disappear in the warmer months,” Dr. Martínez added. “There are just other viruses and different factors. We don’t know the role or the weight that each one of the factors has, either individually or specifically, in the development of AML. In addition, we know that AML is a very heterogeneous disease and that various factors, including genetic ones, can be involved in its etiopathogenesis.”
With respect to the stem cell theory in this leukemia, Dr. Alonso emphasized that, “in theory, the virus could fit into it with no problem. That said, any other environmental agent could also produce the described phenomenon where the rapid proliferation of quiescent leukemic stem cells is stimulated, thereby hastening the diagnosis.”
“Should the etiological factor be found,” Dr. Martínez noted, “we can try to reduce exposure and thereby decrease the incidence of AML. On the other hand, discovering how the environmental factor stimulates the proliferation of quiescent leukemic [stem] cells could enhance our knowledge about the regulation of that.”
As to whether there is evidence for the involvement of infections in other hematologic malignancies, Dr. Martínez reported, “This has already been seen. And this study shows other examples (Epstein-Barr virus and human T-cell lymphotropic virus type 1 with lymphomas), and there could also be Helicobacter pylori and lymphomas.”
Outside of hematology, human papillomavirus has been associated with cervical cancer, tobacco with lung cancer, sun with skin cancer, and diet with the development of some solid neoplasms.
“The study speaks about the concept of a latency period. To accept the idea that a factor or virus that’s more prevalent in winter produces, on its own, AML in a few weeks or months means accepting the idea of a very short latency period – something that’s not usually the case. For that, another explanation is given: An abnormal immune response or that a seasonal infectious agent can be capable of promoting leukemogenesis. These are also hypotheses to be explored in the future,” suggested Dr. Martínez.
New research network
Several potential limitations of this study should be considered. One limitation is that AML cases were obtained from the CMBD registry as defined by ICD-9, and no other AML classifications were available. Another limitation is that information on the date of onset of clinical symptoms was not available for analysis. In addition, a further limitation related to the source of their data may have led the researchers to underestimate the incidence rates of AML in older patients, as only hospitalized patients were captured in their study.
As for continuing the research, the results make it necessary to carry out complementary epidemiologic studies that will examine the association between seasonal risk factors and the increased diagnosis of AML during winter months.
To go forward, the first step would be to secure funding. For this purpose, a network is being put together featuring collaborators from other world-renowned research groups that are at the top of their respective disciplines. Through this network, they hope to be able to apply together for public research grants from countries in Europe and elsewhere as well as to establish collaborations with various companies in the private sector.
“This could open up new therapeutic avenues in the future, as we could try to force leukemic stem cells to divide, thereby reducing the resistance that the standard treatments usually demonstrate,” Dr. Alonso concluded.
Dr. Alonso received research funding from Incyte, Pfizer International, and Astellas Pharma outside the present work. Dr. Martínez disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition. A version of the article appeared on Medscape.com.
Most diagnoses of acute myeloid leukemia (AML) are made during January. This finding strongly implies that seasonal factors, such as infectious agents or environmental triggers, influence the development or proliferation of the disease, which points to prevention opportunities. This was the conclusion of an international study led by a team from the Jiménez Díaz Foundation University Hospital Health Research Institute (IIS-FJD) in Madrid, in collaboration with colleagues from the University of Bristol, England. Their work was published in the British Journal of Haematology.
The study’s aim was to investigate the potential seasonal and long-term trends in AML diagnosis in an overall population and in subgroups according to sex and age. To do so, the researchers examined 26,472 cases of AML diagnosed in Spain between 2004 and 2015. They found seasonality in the diagnosis of this type of leukemia. This “could point to there being an underlying seasonal etiology at play,” noted one of the main authors of the study, Juan Manuel Alonso, MD, a physician in the IIS-FJD’s department of hematology and hemotherapy.
“The environmental triggers involved could be radiation, pollution, allergens, or infectious agents like viruses. We’re leaning toward viruses, because there are already distinct solid tumor and hematologic cancers that are caused by them and because, in the winter months, there’s an increased incidence of cancers due to viral infections,” Dr. Alonso said in an interview. “The etiological mechanism should be different from that exerted by chronic viral pressure, because here we’re dealing with an acute and aggressive disease that probably needs a short incubation period.”
Various hypotheses
In an interview, David Martínez, MD, a hematologist at La Fe University Hospital in Valencia, Spain, described the research as “an extremely well done and much-discussed study on AML, a disease that appears to be diagnosed more frequently at a certain time of year – namely, January.
“There’s no clear explanation for this finding,” Dr. Martínez said. “Several possible reasons have been put forward and are being talked about. The one that seems to hold the most water is the hypothesis that infectious agents and environmental factors may have a greater influence. This is because the idea that they’re involved in neoplastic diseases is nothing new. In fact, there are a lot of publications and a good amount of scientific evidence that link viral infections and environmental factors with the development of oncologic diseases.”
AML is a rare disease yet is responsible for many cancer-related deaths. Mutations that cause AML can occur due to an inherited mutant gene or exposure to certain carcinogens, such as chemotherapy, radiotherapy, ionizing radiation, tobacco, and benzene. These findings are broadly similar to those of a large U.S.-based study by Calip et al., who found a peak of adult AML diagnoses during December and January from 1992 to 2008. Previous smaller studies have provided conflicting evidence, likely due to lower power or to the use of less advanced statistical approaches.
Seasonal factors involved?
Demonstration of seasonal variation in the occurrence of AML would, firstly, provide supportive evidence of etiology by seasonal factors, such as infectious agents or environmental factors, and, secondly, focus research onto the etiologic role of such factors.
The current study used population-based data on cases of AML occurring in Spain from a nationwide hospital discharge registry for the years 2004 to 2015. “This is, to our knowledge, the largest study aimed at investigating the potential seasonal and long-term trends in AML incidence in an overall population and in subgroups according to sex and age while employing novel statistical models with serial dependence for discrete-valued time series,” wrote the researchers.
They extracted information from the register of each case about the date of admission, discharge date, the anonymous identifier for each patient, International Classification of Diseases (ICD)–9 codes, sex, and date of birth, from which they derived age groups as described for the at-risk population. For patients hospitalized on more than one occasion, only the record corresponding to their first diagnosis of AML was selected.
AML cases per month were standardized to months of equal length.
Age/sex-standardized monthly incidence rates of AML were calculated using the census of Spanish population in 2010 as a “standard” population. Age-standardized and sex-standardized monthly incidence rates of AML were calculated.
Nine separate time-series decompositions were performed as an initial exploratory analysis on the monthly incidence rates of AML using data for all cases and data for each sex and age group. Nine separate Poisson generalized linear autoregressive moving average (GLARMA) models were fitted to evaluate the temporal dynamics in AML incidence using data for all cases, and data for each sex and age group.
Long-term trend
A total of 26,472 patients with a first diagnosis of active AML were hospitalized in Spain and registered at the country’s Minimum Basic Data Set (CMBD) during 2004-2015. In the end, there were 26,475 patients in the study population; a greater proportion of cases were male (56.0%), and the median age at diagnosis was 67 years.
Seasonal and trend decomposition using Loess decomposition of the incidence rates observed in the overall population exhibited seasonal fluctuation with a peak in January. A slight upward trend was apparent from visual inspection with an upturn in early 2005 and a downturn at the end of 2013. As for the differences by sex groups and age groups, Dr. Alonso said, “For both sexes and in age groups 5-19, 20-49, and 50-64 years, we found that the results were identical to those found in the overall population.”
The final model included an upward linear long-term trend, as well as the variables monthly seasonality and December 2015. The estimated monthly long-term trend implies that the monthly incidence rates of AML diagnoses annually increased by 0.4% (95% confidence interval [CI], 0.2%-0.6%; P = .0011), given that the other covariates are held constant.
January displayed the highest incidence rate of AML, with a minimum average difference of 7%, when compared with February (95% CI, 2%-12%; P = .0143) and a maximum average difference of 16%, compared with November (95% CI, 11%-21%; P < .0001) and August (95% CI, 10%-21%; P < .0001).
The incidence rate of AML for December 2015 was 0.43 (95% CI, 0.34-0.54; P < .0001) times the average incidence rate for the rest of the study period.
Potential role of viruses
“We have to keep in mind that infectious agents (viral infections) and environmental factors (allergens) don’t disappear in the warmer months,” Dr. Martínez added. “There are just other viruses and different factors. We don’t know the role or the weight that each one of the factors has, either individually or specifically, in the development of AML. In addition, we know that AML is a very heterogeneous disease and that various factors, including genetic ones, can be involved in its etiopathogenesis.”
With respect to the stem cell theory in this leukemia, Dr. Alonso emphasized that, “in theory, the virus could fit into it with no problem. That said, any other environmental agent could also produce the described phenomenon where the rapid proliferation of quiescent leukemic stem cells is stimulated, thereby hastening the diagnosis.”
“Should the etiological factor be found,” Dr. Martínez noted, “we can try to reduce exposure and thereby decrease the incidence of AML. On the other hand, discovering how the environmental factor stimulates the proliferation of quiescent leukemic [stem] cells could enhance our knowledge about the regulation of that.”
As to whether there is evidence for the involvement of infections in other hematologic malignancies, Dr. Martínez reported, “This has already been seen. And this study shows other examples (Epstein-Barr virus and human T-cell lymphotropic virus type 1 with lymphomas), and there could also be Helicobacter pylori and lymphomas.”
Outside of hematology, human papillomavirus has been associated with cervical cancer, tobacco with lung cancer, sun with skin cancer, and diet with the development of some solid neoplasms.
“The study speaks about the concept of a latency period. To accept the idea that a factor or virus that’s more prevalent in winter produces, on its own, AML in a few weeks or months means accepting the idea of a very short latency period – something that’s not usually the case. For that, another explanation is given: An abnormal immune response or that a seasonal infectious agent can be capable of promoting leukemogenesis. These are also hypotheses to be explored in the future,” suggested Dr. Martínez.
New research network
Several potential limitations of this study should be considered. One limitation is that AML cases were obtained from the CMBD registry as defined by ICD-9, and no other AML classifications were available. Another limitation is that information on the date of onset of clinical symptoms was not available for analysis. In addition, a further limitation related to the source of their data may have led the researchers to underestimate the incidence rates of AML in older patients, as only hospitalized patients were captured in their study.
As for continuing the research, the results make it necessary to carry out complementary epidemiologic studies that will examine the association between seasonal risk factors and the increased diagnosis of AML during winter months.
To go forward, the first step would be to secure funding. For this purpose, a network is being put together featuring collaborators from other world-renowned research groups that are at the top of their respective disciplines. Through this network, they hope to be able to apply together for public research grants from countries in Europe and elsewhere as well as to establish collaborations with various companies in the private sector.
“This could open up new therapeutic avenues in the future, as we could try to force leukemic stem cells to divide, thereby reducing the resistance that the standard treatments usually demonstrate,” Dr. Alonso concluded.
Dr. Alonso received research funding from Incyte, Pfizer International, and Astellas Pharma outside the present work. Dr. Martínez disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition. A version of the article appeared on Medscape.com.
Most diagnoses of acute myeloid leukemia (AML) are made during January. This finding strongly implies that seasonal factors, such as infectious agents or environmental triggers, influence the development or proliferation of the disease, which points to prevention opportunities. This was the conclusion of an international study led by a team from the Jiménez Díaz Foundation University Hospital Health Research Institute (IIS-FJD) in Madrid, in collaboration with colleagues from the University of Bristol, England. Their work was published in the British Journal of Haematology.
The study’s aim was to investigate the potential seasonal and long-term trends in AML diagnosis in an overall population and in subgroups according to sex and age. To do so, the researchers examined 26,472 cases of AML diagnosed in Spain between 2004 and 2015. They found seasonality in the diagnosis of this type of leukemia. This “could point to there being an underlying seasonal etiology at play,” noted one of the main authors of the study, Juan Manuel Alonso, MD, a physician in the IIS-FJD’s department of hematology and hemotherapy.
“The environmental triggers involved could be radiation, pollution, allergens, or infectious agents like viruses. We’re leaning toward viruses, because there are already distinct solid tumor and hematologic cancers that are caused by them and because, in the winter months, there’s an increased incidence of cancers due to viral infections,” Dr. Alonso said in an interview. “The etiological mechanism should be different from that exerted by chronic viral pressure, because here we’re dealing with an acute and aggressive disease that probably needs a short incubation period.”
Various hypotheses
In an interview, David Martínez, MD, a hematologist at La Fe University Hospital in Valencia, Spain, described the research as “an extremely well done and much-discussed study on AML, a disease that appears to be diagnosed more frequently at a certain time of year – namely, January.
“There’s no clear explanation for this finding,” Dr. Martínez said. “Several possible reasons have been put forward and are being talked about. The one that seems to hold the most water is the hypothesis that infectious agents and environmental factors may have a greater influence. This is because the idea that they’re involved in neoplastic diseases is nothing new. In fact, there are a lot of publications and a good amount of scientific evidence that link viral infections and environmental factors with the development of oncologic diseases.”
AML is a rare disease yet is responsible for many cancer-related deaths. Mutations that cause AML can occur due to an inherited mutant gene or exposure to certain carcinogens, such as chemotherapy, radiotherapy, ionizing radiation, tobacco, and benzene. These findings are broadly similar to those of a large U.S.-based study by Calip et al., who found a peak of adult AML diagnoses during December and January from 1992 to 2008. Previous smaller studies have provided conflicting evidence, likely due to lower power or to the use of less advanced statistical approaches.
Seasonal factors involved?
Demonstration of seasonal variation in the occurrence of AML would, firstly, provide supportive evidence of etiology by seasonal factors, such as infectious agents or environmental factors, and, secondly, focus research onto the etiologic role of such factors.
The current study used population-based data on cases of AML occurring in Spain from a nationwide hospital discharge registry for the years 2004 to 2015. “This is, to our knowledge, the largest study aimed at investigating the potential seasonal and long-term trends in AML incidence in an overall population and in subgroups according to sex and age while employing novel statistical models with serial dependence for discrete-valued time series,” wrote the researchers.
They extracted information from the register of each case about the date of admission, discharge date, the anonymous identifier for each patient, International Classification of Diseases (ICD)–9 codes, sex, and date of birth, from which they derived age groups as described for the at-risk population. For patients hospitalized on more than one occasion, only the record corresponding to their first diagnosis of AML was selected.
AML cases per month were standardized to months of equal length.
Age/sex-standardized monthly incidence rates of AML were calculated using the census of Spanish population in 2010 as a “standard” population. Age-standardized and sex-standardized monthly incidence rates of AML were calculated.
Nine separate time-series decompositions were performed as an initial exploratory analysis on the monthly incidence rates of AML using data for all cases and data for each sex and age group. Nine separate Poisson generalized linear autoregressive moving average (GLARMA) models were fitted to evaluate the temporal dynamics in AML incidence using data for all cases, and data for each sex and age group.
Long-term trend
A total of 26,472 patients with a first diagnosis of active AML were hospitalized in Spain and registered at the country’s Minimum Basic Data Set (CMBD) during 2004-2015. In the end, there were 26,475 patients in the study population; a greater proportion of cases were male (56.0%), and the median age at diagnosis was 67 years.
Seasonal and trend decomposition using Loess decomposition of the incidence rates observed in the overall population exhibited seasonal fluctuation with a peak in January. A slight upward trend was apparent from visual inspection with an upturn in early 2005 and a downturn at the end of 2013. As for the differences by sex groups and age groups, Dr. Alonso said, “For both sexes and in age groups 5-19, 20-49, and 50-64 years, we found that the results were identical to those found in the overall population.”
The final model included an upward linear long-term trend, as well as the variables monthly seasonality and December 2015. The estimated monthly long-term trend implies that the monthly incidence rates of AML diagnoses annually increased by 0.4% (95% confidence interval [CI], 0.2%-0.6%; P = .0011), given that the other covariates are held constant.
January displayed the highest incidence rate of AML, with a minimum average difference of 7%, when compared with February (95% CI, 2%-12%; P = .0143) and a maximum average difference of 16%, compared with November (95% CI, 11%-21%; P < .0001) and August (95% CI, 10%-21%; P < .0001).
The incidence rate of AML for December 2015 was 0.43 (95% CI, 0.34-0.54; P < .0001) times the average incidence rate for the rest of the study period.
Potential role of viruses
“We have to keep in mind that infectious agents (viral infections) and environmental factors (allergens) don’t disappear in the warmer months,” Dr. Martínez added. “There are just other viruses and different factors. We don’t know the role or the weight that each one of the factors has, either individually or specifically, in the development of AML. In addition, we know that AML is a very heterogeneous disease and that various factors, including genetic ones, can be involved in its etiopathogenesis.”
With respect to the stem cell theory in this leukemia, Dr. Alonso emphasized that, “in theory, the virus could fit into it with no problem. That said, any other environmental agent could also produce the described phenomenon where the rapid proliferation of quiescent leukemic stem cells is stimulated, thereby hastening the diagnosis.”
“Should the etiological factor be found,” Dr. Martínez noted, “we can try to reduce exposure and thereby decrease the incidence of AML. On the other hand, discovering how the environmental factor stimulates the proliferation of quiescent leukemic [stem] cells could enhance our knowledge about the regulation of that.”
As to whether there is evidence for the involvement of infections in other hematologic malignancies, Dr. Martínez reported, “This has already been seen. And this study shows other examples (Epstein-Barr virus and human T-cell lymphotropic virus type 1 with lymphomas), and there could also be Helicobacter pylori and lymphomas.”
Outside of hematology, human papillomavirus has been associated with cervical cancer, tobacco with lung cancer, sun with skin cancer, and diet with the development of some solid neoplasms.
“The study speaks about the concept of a latency period. To accept the idea that a factor or virus that’s more prevalent in winter produces, on its own, AML in a few weeks or months means accepting the idea of a very short latency period – something that’s not usually the case. For that, another explanation is given: An abnormal immune response or that a seasonal infectious agent can be capable of promoting leukemogenesis. These are also hypotheses to be explored in the future,” suggested Dr. Martínez.
New research network
Several potential limitations of this study should be considered. One limitation is that AML cases were obtained from the CMBD registry as defined by ICD-9, and no other AML classifications were available. Another limitation is that information on the date of onset of clinical symptoms was not available for analysis. In addition, a further limitation related to the source of their data may have led the researchers to underestimate the incidence rates of AML in older patients, as only hospitalized patients were captured in their study.
As for continuing the research, the results make it necessary to carry out complementary epidemiologic studies that will examine the association between seasonal risk factors and the increased diagnosis of AML during winter months.
To go forward, the first step would be to secure funding. For this purpose, a network is being put together featuring collaborators from other world-renowned research groups that are at the top of their respective disciplines. Through this network, they hope to be able to apply together for public research grants from countries in Europe and elsewhere as well as to establish collaborations with various companies in the private sector.
“This could open up new therapeutic avenues in the future, as we could try to force leukemic stem cells to divide, thereby reducing the resistance that the standard treatments usually demonstrate,” Dr. Alonso concluded.
Dr. Alonso received research funding from Incyte, Pfizer International, and Astellas Pharma outside the present work. Dr. Martínez disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition. A version of the article appeared on Medscape.com.
FROM THE BRITISH JOURNAL OF HEMATOLOGY
Estrogen replacement therapy in endometrial cancer survivors
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.

If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.
If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.
If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
Annual PSA screening important for Black men
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
FROM JAMA ONCOLOGY
Oncologists’ wealth and debt: COVID had little impact
concludes the latest Medscape Oncologist Wealth & Debt Report 2022.
Comparing the findings with those in the larger Medscape Physician Wealth & Debt Report 2022, which surveyed more than 13,000 physicians in 29 specialties, the findings for oncologists show how they compare with those who chose other paths in medicine.
Oncologists’ income rose, on average, by 2% in the past year and now stands at an average of $411,000 annually, up from $403,000 in the 2021 report.
This puts oncologists in the top third of specialties, with plastic surgeons again in the top slot (with average income of $576,000 in 2022).
One-fifth (20%) of oncologists surveyed reported a family worth of more than $5 million, which represents substantial family wealth, the report comments.
However, 22% of oncologists reported that their family net worth was less than $500,000, and another 10% estimated that it to fall between $500,000 and $1 million.
For comparison, the average U.S. family net worth is about $749,000, according to data from the Federal Reserve.
Most live ‘within their means’
Most oncologists (94%) and also most (94%) of all of the physicians surveyed said that they live within or below their means.
How does one do this? Just paying off credit cards each month and contributing enough to a 401(k) account to receive an employer match does not meet this standard, said Joel Greenwald MD, CFP, a wealth management advisor for physicians. To live within or below your means, you also need to be saving at least 20% toward retirement, pay down student loans, contribute to your kids’ college savings, and set aside rainy day cash, he explained.
When physicians were asked about their favorite cost-cutting tactics, replies included bringing lunch to work, keeping a car for 15 years, and carrying out their own household maintenance and repairs. One doctor described a “24-hour rule” when it comes to shopping: “Revisit the desired purchase after 24 hours to see if it’s still desired.”
But how well do these tactics go down with ‘the other half’ and the rest of the household? Two-thirds (66%) of oncologists, and a similar proportion of all physicians, said that they argue with their significant other about spending. This appears to be high in comparison with the finding from a recent survey that across the United States, about one in four couples (25%) argue about money at least once a month.
Regarding spending, the top expense among oncologists was for childcare (16%), private tuition for offspring (14%), mortgage on a second home (14%), college tuition for offspring (14%), and a car lease (12%).
Around 17% of oncologists reported that they are still paying off their own college or medical school loans. For this statistic, they are about in the middle of all specialties.
The report notes that freeing oneself from medical school debt is very costly. Physicians in the United States pay an average of $356,000-$440,000, about half of which is interest.
Little change over 2021
The COVID pandemic had much less of an impact on physicians than it had on the general population when it comes to keeping up with payments, and most physicians were not affected. Only 3% of oncologists said they fell behind with payments for mortgage; 6% fell behind with payments for other bills.
In comparison, nearly half (46%) of Americans missed one or more payments of rent or mortgage because of COVID, according to a 2021 industry survey.
Over the past year, most oncologists (70%) did not change their spending habits, and only 11% cut expenses by deferring or refinancing loans. Also, most oncologists (75%) avoided major financial loses. Only 8% reported financial losses because of problems at their medical practice.
However, a slightly higher percentage of oncologists reported a stock or company investment that had turned sour in 2022 (37%) in comparison with 2021 (28%).
A version of this article first appeared on Medscape.com.
concludes the latest Medscape Oncologist Wealth & Debt Report 2022.
Comparing the findings with those in the larger Medscape Physician Wealth & Debt Report 2022, which surveyed more than 13,000 physicians in 29 specialties, the findings for oncologists show how they compare with those who chose other paths in medicine.
Oncologists’ income rose, on average, by 2% in the past year and now stands at an average of $411,000 annually, up from $403,000 in the 2021 report.
This puts oncologists in the top third of specialties, with plastic surgeons again in the top slot (with average income of $576,000 in 2022).
One-fifth (20%) of oncologists surveyed reported a family worth of more than $5 million, which represents substantial family wealth, the report comments.
However, 22% of oncologists reported that their family net worth was less than $500,000, and another 10% estimated that it to fall between $500,000 and $1 million.
For comparison, the average U.S. family net worth is about $749,000, according to data from the Federal Reserve.
Most live ‘within their means’
Most oncologists (94%) and also most (94%) of all of the physicians surveyed said that they live within or below their means.
How does one do this? Just paying off credit cards each month and contributing enough to a 401(k) account to receive an employer match does not meet this standard, said Joel Greenwald MD, CFP, a wealth management advisor for physicians. To live within or below your means, you also need to be saving at least 20% toward retirement, pay down student loans, contribute to your kids’ college savings, and set aside rainy day cash, he explained.
When physicians were asked about their favorite cost-cutting tactics, replies included bringing lunch to work, keeping a car for 15 years, and carrying out their own household maintenance and repairs. One doctor described a “24-hour rule” when it comes to shopping: “Revisit the desired purchase after 24 hours to see if it’s still desired.”
But how well do these tactics go down with ‘the other half’ and the rest of the household? Two-thirds (66%) of oncologists, and a similar proportion of all physicians, said that they argue with their significant other about spending. This appears to be high in comparison with the finding from a recent survey that across the United States, about one in four couples (25%) argue about money at least once a month.
Regarding spending, the top expense among oncologists was for childcare (16%), private tuition for offspring (14%), mortgage on a second home (14%), college tuition for offspring (14%), and a car lease (12%).
Around 17% of oncologists reported that they are still paying off their own college or medical school loans. For this statistic, they are about in the middle of all specialties.
The report notes that freeing oneself from medical school debt is very costly. Physicians in the United States pay an average of $356,000-$440,000, about half of which is interest.
Little change over 2021
The COVID pandemic had much less of an impact on physicians than it had on the general population when it comes to keeping up with payments, and most physicians were not affected. Only 3% of oncologists said they fell behind with payments for mortgage; 6% fell behind with payments for other bills.
In comparison, nearly half (46%) of Americans missed one or more payments of rent or mortgage because of COVID, according to a 2021 industry survey.
Over the past year, most oncologists (70%) did not change their spending habits, and only 11% cut expenses by deferring or refinancing loans. Also, most oncologists (75%) avoided major financial loses. Only 8% reported financial losses because of problems at their medical practice.
However, a slightly higher percentage of oncologists reported a stock or company investment that had turned sour in 2022 (37%) in comparison with 2021 (28%).
A version of this article first appeared on Medscape.com.
concludes the latest Medscape Oncologist Wealth & Debt Report 2022.
Comparing the findings with those in the larger Medscape Physician Wealth & Debt Report 2022, which surveyed more than 13,000 physicians in 29 specialties, the findings for oncologists show how they compare with those who chose other paths in medicine.
Oncologists’ income rose, on average, by 2% in the past year and now stands at an average of $411,000 annually, up from $403,000 in the 2021 report.
This puts oncologists in the top third of specialties, with plastic surgeons again in the top slot (with average income of $576,000 in 2022).
One-fifth (20%) of oncologists surveyed reported a family worth of more than $5 million, which represents substantial family wealth, the report comments.
However, 22% of oncologists reported that their family net worth was less than $500,000, and another 10% estimated that it to fall between $500,000 and $1 million.
For comparison, the average U.S. family net worth is about $749,000, according to data from the Federal Reserve.
Most live ‘within their means’
Most oncologists (94%) and also most (94%) of all of the physicians surveyed said that they live within or below their means.
How does one do this? Just paying off credit cards each month and contributing enough to a 401(k) account to receive an employer match does not meet this standard, said Joel Greenwald MD, CFP, a wealth management advisor for physicians. To live within or below your means, you also need to be saving at least 20% toward retirement, pay down student loans, contribute to your kids’ college savings, and set aside rainy day cash, he explained.
When physicians were asked about their favorite cost-cutting tactics, replies included bringing lunch to work, keeping a car for 15 years, and carrying out their own household maintenance and repairs. One doctor described a “24-hour rule” when it comes to shopping: “Revisit the desired purchase after 24 hours to see if it’s still desired.”
But how well do these tactics go down with ‘the other half’ and the rest of the household? Two-thirds (66%) of oncologists, and a similar proportion of all physicians, said that they argue with their significant other about spending. This appears to be high in comparison with the finding from a recent survey that across the United States, about one in four couples (25%) argue about money at least once a month.
Regarding spending, the top expense among oncologists was for childcare (16%), private tuition for offspring (14%), mortgage on a second home (14%), college tuition for offspring (14%), and a car lease (12%).
Around 17% of oncologists reported that they are still paying off their own college or medical school loans. For this statistic, they are about in the middle of all specialties.
The report notes that freeing oneself from medical school debt is very costly. Physicians in the United States pay an average of $356,000-$440,000, about half of which is interest.
Little change over 2021
The COVID pandemic had much less of an impact on physicians than it had on the general population when it comes to keeping up with payments, and most physicians were not affected. Only 3% of oncologists said they fell behind with payments for mortgage; 6% fell behind with payments for other bills.
In comparison, nearly half (46%) of Americans missed one or more payments of rent or mortgage because of COVID, according to a 2021 industry survey.
Over the past year, most oncologists (70%) did not change their spending habits, and only 11% cut expenses by deferring or refinancing loans. Also, most oncologists (75%) avoided major financial loses. Only 8% reported financial losses because of problems at their medical practice.
However, a slightly higher percentage of oncologists reported a stock or company investment that had turned sour in 2022 (37%) in comparison with 2021 (28%).
A version of this article first appeared on Medscape.com.