User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
First drug for desmoid tumors: ‘Impressive’ data for nirogacestat
PARIS –
Nirogacestat, under development by Connecticut-based SpringWorks Therapeutics, is an oral, selective, small-molecule gamma secretase inhibitor that targets the Notch signaling pathway, which is involved in cell differentiation. Desmoid tumors express high levels of Notch, so there is a “clear mechanistic rationale” for using such drugs in these patients.
Now, nirogacestat has shown a significant improvement in progression-free survival (PFS) and also a reduction in symptoms and better quality of life, when compared with placebo in the phase 3 DeFi trial.
The company has said that, by the end of this year, it will file these data for U.S. Food and Drug Administration approval of the drug for use in desmoid tumors.
Trial results were presented at the annual meeting of the European Society for Medical Oncology.
Overall, nirogacestat demonstrated “rapid, sustained, and statistically significant improvements in all primary and secondary endpoints,” study presenter Bernd Kasper, MD, PhD, sarcoma unit, Mannheim (Germany) Cancer Center, told a press conference.
There were “really impressive” reductions in pain scores and symptom burden, as well as improvements in health-related quality of life.
Dr. Kasper highlighted that this is the “first phase 3 trial … to demonstrate a clinical benefit with a gamma secretase inhibitor in any indication.”
With the drug showing a “manageable safety profile,” despite a high rate of ovarian dysfunction, Dr. Kasper believes it “has the potential to become the standard of care for patients with desmoid tumors requiring systemic treatment.”
Asked how long patients could take the drug, he replied, “Usually you take a drug as long as the patient benefits” from it.
“That means as long as there is no progression,” Dr. Kasper said, noting that there are patients from the earlier phase trials of nirogacestat who have been taking the drug “for years.”
However, there is a “very important question that is not answered” by the current study: “How long should we treat our patients?”
Dr. Kasper said to answer that question will require further trials, including those focused on treatment discontinuation.
Large trial in rare cancer
DeFi is a “unique study” and “very important in many aspects,” commented Jean-Yves Blay, MD, PhD, professor of medicine at the University Claude Bernard in Lyon, France, in an ESMO press release. Dr. Blay was not involved with the DeFi research.
“The results show benefit for the first time with a novel treatment with a new mode of action in patients where treatment options are currently limited,” he said, adding that the findings are “practice changing.”
Dr. Blay also praised the study for being “smart,” as it showed that large, placebo-controlled trials can be conducted in a rare cancer, and demonstrated the “importance of targeting the right patients with right drug.”
“The success of this study puts even more emphasis on the concept of having patients with rare cancers referred into reference centers, where clinical studies can be accomplished in record times, with the potential to deliver new treatments to patients with orphan diseases,” he said.
Discussing the results following their presentation, Dr. Blay said there are nevertheless a number of different treatment options for desmoid tumors, including sorafenib (Nexavar), and it is not clear whether patients with nonprogressive disease would experience any symptomatic benefit with nirogacestat.
Biomarkers of treatment efficacy and resistance are also required, he continued, and the drug’s long-term toxicity profile needs to be understood. In addition, its impact on ovarian dysfunction, as well as on future pregnancies, is currently unclear.
Details of the results
Presenting the study, Dr. Kasper explained that desmoid tumors have a variable presentation and an “unpredictable disease course,” and this together with the lack of approved therapies means they are “challenging to manage.”
Moreover, “due to local and aggressive growth, desmoid tumors can cause pain, disfigurement, and functional problems that can be a real burden for patients,” Dr. Kasper stressed.
Treatment should therefore be individualized to each patient to “optimize tumor control and improve the symptom burden,” he told the audience, including the impact on pain, physical function, and overall quality of life.
Indeed, a recent global consensus-based guideline for the management of desmoid tumors recommended a five-step model for treatment selection based on the level of evidence, overall response rate, PFS rate, ease of administration, and expected toxicity.
The DeFi trial enrolled patients with progressive desmoid tumors, stratified by target tumor location (intra-/extra-abdominal), who either were treatment-naive and not amenable to surgery, or were treatment refractory, or had recurrent disease after one prior line of therapy.
Dr. Kasper said in an interview that they required the patient to have at least 20% disease progression at the tumor sites so that they would include only those “who are in need of treatment.”
He explained that requirement was “quite strict” to ensure they excluded patients with “smaller-scale disease” and those with spontaneous regression, which can occur in desmoid tumors.
In all, 142 patients from 37 sites worldwide were randomly assigned to receive either nirogacestat 150 mg or placebo twice daily in 28-day cycles until radiographic progression, at which point patients were moved into an open-label phase and placebo patients could switch to nirogacestat.
The median age of the patients was 34 years, and two-thirds were female. Dr. Kasper underlined that there was a “rather high” prevalence of multifocal disease, at around 40%.
At the data cutoff for the primary analysis on April 7, nirogacestat was associated with a significant reduction in disease progression, at a median PFS that was not reached vs. 15.1 months for placebo, or a hazard ratio of 0.29 (P < .001).
This effect was seen across all subgroups included in the analysis, including when stratifying patients by age, gender, tumor characteristics, and prior treatment.
The objective response rate was also significantly higher with nirogacestat, at 41% vs. 8% in patients assigned to placebo (P < .001). A complete response was seen in 7% of patients given active treatment vs. 0% of those in the placebo group.
The median time to response was 5.6 months with nirogacestat and 11.1 months for patients given placebo.
Dr. Kasper also showed that nirogacestat was associated with significant reductions in pain severity, compared with placebo at treatment cycle 10, as measured on the Brief Pain Index-Short Form of –1.5 (P < .001).
There were also significant improvements with nirogacestat over placebo in the DT Symptom and DT Impact Scales (P < .001 for both), and on the global health status/quality of life scale (P = .007), physical functioning scale (P < .001), and role functioning scale (P < .001) of the EORTC Quality of Life Questionnaire-Core 30.
After a median exposure of 20.6 months, grade 3 or higher treatment-emergent adverse events were observed in 57% of patients treated with nirogacestat vs. 17% of those given placebo, who had a median treatment exposure of 11.4 months.
The most commonly reported adverse events of any grade with the active drug were diarrhea (84%), nausea (54%), fatigue (51%), and hypophosphatemia (42%), but Dr. Kasper noted that 95% of treatment-emergent adverse events were grade 1 or 2, with the first onset typically during cycle 1.
Ovarian dysfunction was observed in 75% of women of childbearing age, at a median onset at 9 weeks and a median duration of 21 weeks. However, the dysfunction resolved in 74% of patients, including those who continued active therapy.
The study was funded by SpringWorks Therapeutics. Dr. Kasper declares relationships with Bayer, Blueprint, Boehringer Ingelheim, SpringWorks, GSK, PharmaMar, and Ayala.
A version of this article first appeared on Medscape.com.
PARIS –
Nirogacestat, under development by Connecticut-based SpringWorks Therapeutics, is an oral, selective, small-molecule gamma secretase inhibitor that targets the Notch signaling pathway, which is involved in cell differentiation. Desmoid tumors express high levels of Notch, so there is a “clear mechanistic rationale” for using such drugs in these patients.
Now, nirogacestat has shown a significant improvement in progression-free survival (PFS) and also a reduction in symptoms and better quality of life, when compared with placebo in the phase 3 DeFi trial.
The company has said that, by the end of this year, it will file these data for U.S. Food and Drug Administration approval of the drug for use in desmoid tumors.
Trial results were presented at the annual meeting of the European Society for Medical Oncology.
Overall, nirogacestat demonstrated “rapid, sustained, and statistically significant improvements in all primary and secondary endpoints,” study presenter Bernd Kasper, MD, PhD, sarcoma unit, Mannheim (Germany) Cancer Center, told a press conference.
There were “really impressive” reductions in pain scores and symptom burden, as well as improvements in health-related quality of life.
Dr. Kasper highlighted that this is the “first phase 3 trial … to demonstrate a clinical benefit with a gamma secretase inhibitor in any indication.”
With the drug showing a “manageable safety profile,” despite a high rate of ovarian dysfunction, Dr. Kasper believes it “has the potential to become the standard of care for patients with desmoid tumors requiring systemic treatment.”
Asked how long patients could take the drug, he replied, “Usually you take a drug as long as the patient benefits” from it.
“That means as long as there is no progression,” Dr. Kasper said, noting that there are patients from the earlier phase trials of nirogacestat who have been taking the drug “for years.”
However, there is a “very important question that is not answered” by the current study: “How long should we treat our patients?”
Dr. Kasper said to answer that question will require further trials, including those focused on treatment discontinuation.
Large trial in rare cancer
DeFi is a “unique study” and “very important in many aspects,” commented Jean-Yves Blay, MD, PhD, professor of medicine at the University Claude Bernard in Lyon, France, in an ESMO press release. Dr. Blay was not involved with the DeFi research.
“The results show benefit for the first time with a novel treatment with a new mode of action in patients where treatment options are currently limited,” he said, adding that the findings are “practice changing.”
Dr. Blay also praised the study for being “smart,” as it showed that large, placebo-controlled trials can be conducted in a rare cancer, and demonstrated the “importance of targeting the right patients with right drug.”
“The success of this study puts even more emphasis on the concept of having patients with rare cancers referred into reference centers, where clinical studies can be accomplished in record times, with the potential to deliver new treatments to patients with orphan diseases,” he said.
Discussing the results following their presentation, Dr. Blay said there are nevertheless a number of different treatment options for desmoid tumors, including sorafenib (Nexavar), and it is not clear whether patients with nonprogressive disease would experience any symptomatic benefit with nirogacestat.
Biomarkers of treatment efficacy and resistance are also required, he continued, and the drug’s long-term toxicity profile needs to be understood. In addition, its impact on ovarian dysfunction, as well as on future pregnancies, is currently unclear.
Details of the results
Presenting the study, Dr. Kasper explained that desmoid tumors have a variable presentation and an “unpredictable disease course,” and this together with the lack of approved therapies means they are “challenging to manage.”
Moreover, “due to local and aggressive growth, desmoid tumors can cause pain, disfigurement, and functional problems that can be a real burden for patients,” Dr. Kasper stressed.
Treatment should therefore be individualized to each patient to “optimize tumor control and improve the symptom burden,” he told the audience, including the impact on pain, physical function, and overall quality of life.
Indeed, a recent global consensus-based guideline for the management of desmoid tumors recommended a five-step model for treatment selection based on the level of evidence, overall response rate, PFS rate, ease of administration, and expected toxicity.
The DeFi trial enrolled patients with progressive desmoid tumors, stratified by target tumor location (intra-/extra-abdominal), who either were treatment-naive and not amenable to surgery, or were treatment refractory, or had recurrent disease after one prior line of therapy.
Dr. Kasper said in an interview that they required the patient to have at least 20% disease progression at the tumor sites so that they would include only those “who are in need of treatment.”
He explained that requirement was “quite strict” to ensure they excluded patients with “smaller-scale disease” and those with spontaneous regression, which can occur in desmoid tumors.
In all, 142 patients from 37 sites worldwide were randomly assigned to receive either nirogacestat 150 mg or placebo twice daily in 28-day cycles until radiographic progression, at which point patients were moved into an open-label phase and placebo patients could switch to nirogacestat.
The median age of the patients was 34 years, and two-thirds were female. Dr. Kasper underlined that there was a “rather high” prevalence of multifocal disease, at around 40%.
At the data cutoff for the primary analysis on April 7, nirogacestat was associated with a significant reduction in disease progression, at a median PFS that was not reached vs. 15.1 months for placebo, or a hazard ratio of 0.29 (P < .001).
This effect was seen across all subgroups included in the analysis, including when stratifying patients by age, gender, tumor characteristics, and prior treatment.
The objective response rate was also significantly higher with nirogacestat, at 41% vs. 8% in patients assigned to placebo (P < .001). A complete response was seen in 7% of patients given active treatment vs. 0% of those in the placebo group.
The median time to response was 5.6 months with nirogacestat and 11.1 months for patients given placebo.
Dr. Kasper also showed that nirogacestat was associated with significant reductions in pain severity, compared with placebo at treatment cycle 10, as measured on the Brief Pain Index-Short Form of –1.5 (P < .001).
There were also significant improvements with nirogacestat over placebo in the DT Symptom and DT Impact Scales (P < .001 for both), and on the global health status/quality of life scale (P = .007), physical functioning scale (P < .001), and role functioning scale (P < .001) of the EORTC Quality of Life Questionnaire-Core 30.
After a median exposure of 20.6 months, grade 3 or higher treatment-emergent adverse events were observed in 57% of patients treated with nirogacestat vs. 17% of those given placebo, who had a median treatment exposure of 11.4 months.
The most commonly reported adverse events of any grade with the active drug were diarrhea (84%), nausea (54%), fatigue (51%), and hypophosphatemia (42%), but Dr. Kasper noted that 95% of treatment-emergent adverse events were grade 1 or 2, with the first onset typically during cycle 1.
Ovarian dysfunction was observed in 75% of women of childbearing age, at a median onset at 9 weeks and a median duration of 21 weeks. However, the dysfunction resolved in 74% of patients, including those who continued active therapy.
The study was funded by SpringWorks Therapeutics. Dr. Kasper declares relationships with Bayer, Blueprint, Boehringer Ingelheim, SpringWorks, GSK, PharmaMar, and Ayala.
A version of this article first appeared on Medscape.com.
PARIS –
Nirogacestat, under development by Connecticut-based SpringWorks Therapeutics, is an oral, selective, small-molecule gamma secretase inhibitor that targets the Notch signaling pathway, which is involved in cell differentiation. Desmoid tumors express high levels of Notch, so there is a “clear mechanistic rationale” for using such drugs in these patients.
Now, nirogacestat has shown a significant improvement in progression-free survival (PFS) and also a reduction in symptoms and better quality of life, when compared with placebo in the phase 3 DeFi trial.
The company has said that, by the end of this year, it will file these data for U.S. Food and Drug Administration approval of the drug for use in desmoid tumors.
Trial results were presented at the annual meeting of the European Society for Medical Oncology.
Overall, nirogacestat demonstrated “rapid, sustained, and statistically significant improvements in all primary and secondary endpoints,” study presenter Bernd Kasper, MD, PhD, sarcoma unit, Mannheim (Germany) Cancer Center, told a press conference.
There were “really impressive” reductions in pain scores and symptom burden, as well as improvements in health-related quality of life.
Dr. Kasper highlighted that this is the “first phase 3 trial … to demonstrate a clinical benefit with a gamma secretase inhibitor in any indication.”
With the drug showing a “manageable safety profile,” despite a high rate of ovarian dysfunction, Dr. Kasper believes it “has the potential to become the standard of care for patients with desmoid tumors requiring systemic treatment.”
Asked how long patients could take the drug, he replied, “Usually you take a drug as long as the patient benefits” from it.
“That means as long as there is no progression,” Dr. Kasper said, noting that there are patients from the earlier phase trials of nirogacestat who have been taking the drug “for years.”
However, there is a “very important question that is not answered” by the current study: “How long should we treat our patients?”
Dr. Kasper said to answer that question will require further trials, including those focused on treatment discontinuation.
Large trial in rare cancer
DeFi is a “unique study” and “very important in many aspects,” commented Jean-Yves Blay, MD, PhD, professor of medicine at the University Claude Bernard in Lyon, France, in an ESMO press release. Dr. Blay was not involved with the DeFi research.
“The results show benefit for the first time with a novel treatment with a new mode of action in patients where treatment options are currently limited,” he said, adding that the findings are “practice changing.”
Dr. Blay also praised the study for being “smart,” as it showed that large, placebo-controlled trials can be conducted in a rare cancer, and demonstrated the “importance of targeting the right patients with right drug.”
“The success of this study puts even more emphasis on the concept of having patients with rare cancers referred into reference centers, where clinical studies can be accomplished in record times, with the potential to deliver new treatments to patients with orphan diseases,” he said.
Discussing the results following their presentation, Dr. Blay said there are nevertheless a number of different treatment options for desmoid tumors, including sorafenib (Nexavar), and it is not clear whether patients with nonprogressive disease would experience any symptomatic benefit with nirogacestat.
Biomarkers of treatment efficacy and resistance are also required, he continued, and the drug’s long-term toxicity profile needs to be understood. In addition, its impact on ovarian dysfunction, as well as on future pregnancies, is currently unclear.
Details of the results
Presenting the study, Dr. Kasper explained that desmoid tumors have a variable presentation and an “unpredictable disease course,” and this together with the lack of approved therapies means they are “challenging to manage.”
Moreover, “due to local and aggressive growth, desmoid tumors can cause pain, disfigurement, and functional problems that can be a real burden for patients,” Dr. Kasper stressed.
Treatment should therefore be individualized to each patient to “optimize tumor control and improve the symptom burden,” he told the audience, including the impact on pain, physical function, and overall quality of life.
Indeed, a recent global consensus-based guideline for the management of desmoid tumors recommended a five-step model for treatment selection based on the level of evidence, overall response rate, PFS rate, ease of administration, and expected toxicity.
The DeFi trial enrolled patients with progressive desmoid tumors, stratified by target tumor location (intra-/extra-abdominal), who either were treatment-naive and not amenable to surgery, or were treatment refractory, or had recurrent disease after one prior line of therapy.
Dr. Kasper said in an interview that they required the patient to have at least 20% disease progression at the tumor sites so that they would include only those “who are in need of treatment.”
He explained that requirement was “quite strict” to ensure they excluded patients with “smaller-scale disease” and those with spontaneous regression, which can occur in desmoid tumors.
In all, 142 patients from 37 sites worldwide were randomly assigned to receive either nirogacestat 150 mg or placebo twice daily in 28-day cycles until radiographic progression, at which point patients were moved into an open-label phase and placebo patients could switch to nirogacestat.
The median age of the patients was 34 years, and two-thirds were female. Dr. Kasper underlined that there was a “rather high” prevalence of multifocal disease, at around 40%.
At the data cutoff for the primary analysis on April 7, nirogacestat was associated with a significant reduction in disease progression, at a median PFS that was not reached vs. 15.1 months for placebo, or a hazard ratio of 0.29 (P < .001).
This effect was seen across all subgroups included in the analysis, including when stratifying patients by age, gender, tumor characteristics, and prior treatment.
The objective response rate was also significantly higher with nirogacestat, at 41% vs. 8% in patients assigned to placebo (P < .001). A complete response was seen in 7% of patients given active treatment vs. 0% of those in the placebo group.
The median time to response was 5.6 months with nirogacestat and 11.1 months for patients given placebo.
Dr. Kasper also showed that nirogacestat was associated with significant reductions in pain severity, compared with placebo at treatment cycle 10, as measured on the Brief Pain Index-Short Form of –1.5 (P < .001).
There were also significant improvements with nirogacestat over placebo in the DT Symptom and DT Impact Scales (P < .001 for both), and on the global health status/quality of life scale (P = .007), physical functioning scale (P < .001), and role functioning scale (P < .001) of the EORTC Quality of Life Questionnaire-Core 30.
After a median exposure of 20.6 months, grade 3 or higher treatment-emergent adverse events were observed in 57% of patients treated with nirogacestat vs. 17% of those given placebo, who had a median treatment exposure of 11.4 months.
The most commonly reported adverse events of any grade with the active drug were diarrhea (84%), nausea (54%), fatigue (51%), and hypophosphatemia (42%), but Dr. Kasper noted that 95% of treatment-emergent adverse events were grade 1 or 2, with the first onset typically during cycle 1.
Ovarian dysfunction was observed in 75% of women of childbearing age, at a median onset at 9 weeks and a median duration of 21 weeks. However, the dysfunction resolved in 74% of patients, including those who continued active therapy.
The study was funded by SpringWorks Therapeutics. Dr. Kasper declares relationships with Bayer, Blueprint, Boehringer Ingelheim, SpringWorks, GSK, PharmaMar, and Ayala.
A version of this article first appeared on Medscape.com.
FROM ESMO 2022
Sex is still a taboo subject for patients with breast cancer
and 20% noted a negative impact on their sex life. And while meeting with a specialist in psycho-oncology was universally viewed as an acceptable option, only one out of four patients considered consulting a sexologist. All these women should be encouraged to face and address issues related to sexuality so that they can truly regain a good quality of life, the study suggests.
The study, which was conducted at the breast unit of Santa Maria Goretti Hospital in Latina, Italy, enrolled 141 patients who had undergone breast cancer surgery. Participants were asked to complete a questionnaire that included questions regarding self-image, sexual activity, and sexual satisfaction, and it analyzed these aspects before and after treatment. The participants were then asked whether they felt that they needed to see a sexologist or a specialist in psycho-oncology.
The findings clearly showed a worsening in terms of body image perception. When the women were asked about the relationship they had with their body, femininity, and beauty prior to being diagnosed, 37.4% characterized it as very good and 58.9% as “normal,” with ups and downs but nothing that they would term “conflictual.” After diagnosis, 48.9% noted that the disease had an impact on their body image with a partial conditioning about their femininity and beauty. However, 7.2% had difficulty when it came to recognizing their own body, and their relationship with femininity also became difficult.
On the topic of sexuality, 71.2% of patients were completely satisfied with their sex life before they were diagnosed with breast cancer, 23.7% were partially satisfied, and 5.0% were unsatisfied. As for their sex life after diagnosis and surgery, 20.1% stated that it continued to be fulfilling and 55.4% said that it had gotten worse; 18.8% reported significant sexual dissatisfaction.
The participants were asked whether consulting a professional would be warranted, and whether that would provide useful support for overcoming the difficulties and challenges arising from the disease and the related treatments. In response, 97.1% said they would go to a specialist in psycho-oncology, but only 27.3% would seek help from a sexologist.
“Despite the negative impact on body image and on sexuality, few patients would seek the help of a sexologist; nearly all of the patients, however, would seek the help of a specialist in psycho-oncology. This was very surprising to us,” write the authors. They went on to note that they are carrying out another project to understand the reason for this disparity.
In addition, they advised clinicians to encourage communication about sexuality – a topic that is regularly overlooked and not included in discussions with patients, mostly because of cultural barriers. Often, physicians aren’t comfortable talking about sexuality, as they don’t feel they have the proper training to do so. Patients who are experiencing issues related to sexuality also often have difficulty asking for help. And so, in their conclusion, the authors point out that “collaborating together in the right direction is the basis of change and good communication.”
This article was translated from Univadis Italy and appeared on Medscape.com.
and 20% noted a negative impact on their sex life. And while meeting with a specialist in psycho-oncology was universally viewed as an acceptable option, only one out of four patients considered consulting a sexologist. All these women should be encouraged to face and address issues related to sexuality so that they can truly regain a good quality of life, the study suggests.
The study, which was conducted at the breast unit of Santa Maria Goretti Hospital in Latina, Italy, enrolled 141 patients who had undergone breast cancer surgery. Participants were asked to complete a questionnaire that included questions regarding self-image, sexual activity, and sexual satisfaction, and it analyzed these aspects before and after treatment. The participants were then asked whether they felt that they needed to see a sexologist or a specialist in psycho-oncology.
The findings clearly showed a worsening in terms of body image perception. When the women were asked about the relationship they had with their body, femininity, and beauty prior to being diagnosed, 37.4% characterized it as very good and 58.9% as “normal,” with ups and downs but nothing that they would term “conflictual.” After diagnosis, 48.9% noted that the disease had an impact on their body image with a partial conditioning about their femininity and beauty. However, 7.2% had difficulty when it came to recognizing their own body, and their relationship with femininity also became difficult.
On the topic of sexuality, 71.2% of patients were completely satisfied with their sex life before they were diagnosed with breast cancer, 23.7% were partially satisfied, and 5.0% were unsatisfied. As for their sex life after diagnosis and surgery, 20.1% stated that it continued to be fulfilling and 55.4% said that it had gotten worse; 18.8% reported significant sexual dissatisfaction.
The participants were asked whether consulting a professional would be warranted, and whether that would provide useful support for overcoming the difficulties and challenges arising from the disease and the related treatments. In response, 97.1% said they would go to a specialist in psycho-oncology, but only 27.3% would seek help from a sexologist.
“Despite the negative impact on body image and on sexuality, few patients would seek the help of a sexologist; nearly all of the patients, however, would seek the help of a specialist in psycho-oncology. This was very surprising to us,” write the authors. They went on to note that they are carrying out another project to understand the reason for this disparity.
In addition, they advised clinicians to encourage communication about sexuality – a topic that is regularly overlooked and not included in discussions with patients, mostly because of cultural barriers. Often, physicians aren’t comfortable talking about sexuality, as they don’t feel they have the proper training to do so. Patients who are experiencing issues related to sexuality also often have difficulty asking for help. And so, in their conclusion, the authors point out that “collaborating together in the right direction is the basis of change and good communication.”
This article was translated from Univadis Italy and appeared on Medscape.com.
and 20% noted a negative impact on their sex life. And while meeting with a specialist in psycho-oncology was universally viewed as an acceptable option, only one out of four patients considered consulting a sexologist. All these women should be encouraged to face and address issues related to sexuality so that they can truly regain a good quality of life, the study suggests.
The study, which was conducted at the breast unit of Santa Maria Goretti Hospital in Latina, Italy, enrolled 141 patients who had undergone breast cancer surgery. Participants were asked to complete a questionnaire that included questions regarding self-image, sexual activity, and sexual satisfaction, and it analyzed these aspects before and after treatment. The participants were then asked whether they felt that they needed to see a sexologist or a specialist in psycho-oncology.
The findings clearly showed a worsening in terms of body image perception. When the women were asked about the relationship they had with their body, femininity, and beauty prior to being diagnosed, 37.4% characterized it as very good and 58.9% as “normal,” with ups and downs but nothing that they would term “conflictual.” After diagnosis, 48.9% noted that the disease had an impact on their body image with a partial conditioning about their femininity and beauty. However, 7.2% had difficulty when it came to recognizing their own body, and their relationship with femininity also became difficult.
On the topic of sexuality, 71.2% of patients were completely satisfied with their sex life before they were diagnosed with breast cancer, 23.7% were partially satisfied, and 5.0% were unsatisfied. As for their sex life after diagnosis and surgery, 20.1% stated that it continued to be fulfilling and 55.4% said that it had gotten worse; 18.8% reported significant sexual dissatisfaction.
The participants were asked whether consulting a professional would be warranted, and whether that would provide useful support for overcoming the difficulties and challenges arising from the disease and the related treatments. In response, 97.1% said they would go to a specialist in psycho-oncology, but only 27.3% would seek help from a sexologist.
“Despite the negative impact on body image and on sexuality, few patients would seek the help of a sexologist; nearly all of the patients, however, would seek the help of a specialist in psycho-oncology. This was very surprising to us,” write the authors. They went on to note that they are carrying out another project to understand the reason for this disparity.
In addition, they advised clinicians to encourage communication about sexuality – a topic that is regularly overlooked and not included in discussions with patients, mostly because of cultural barriers. Often, physicians aren’t comfortable talking about sexuality, as they don’t feel they have the proper training to do so. Patients who are experiencing issues related to sexuality also often have difficulty asking for help. And so, in their conclusion, the authors point out that “collaborating together in the right direction is the basis of change and good communication.”
This article was translated from Univadis Italy and appeared on Medscape.com.
Blood test for multiple cancers: Many false positives
PARIS –
“As this technology develops, people must continue with their standard cancer screening, but this is a glimpse of what the future may hold,” commented study investigator Deborah Schrag, MD, MPH, chair, department of medicine, Memorial Sloan Kettering Cancer Center, New York.
For the PATHFINDER study, the Galleri blood test (developed by Grail) was used in 6,621 healthy individuals aged over 50, with or without additional cancer risk factors (such as history of smoking or genetic risk).
It found a positive cancer signal in 92 individuals (1.4%).
None of the individuals who tested positive was known to have cancer at the time of testing. Subsequent workup, which could include scans and/or biopsy, found cancer in 38% of those with a positive test.
“When the test was positive, the workups were typically done in less than 3 months,” Dr. Schrag commented, adding that “the blood test typically predicted the origin of the cancer.”
Dr. Schrag presented the findings at the annual meeting of the European Society for Medical Oncology (ESMO).
Approached for comment, Anthony J. Olszanski, MD, RPh, vice chair of research at the Fox Chase Cancer Center, Philadelphia, noted that the use of a blood test to “find” cancer has long been on the minds of patients. “It is not uncommon to hear oncology patients ask: ‘Why didn’t my doctor find my cancer earlier, on blood tests?’ ”
As this study suggests, finding a malignancy before it becomes apparent on imaging or because of symptoms is one step closer to becoming a reality. “But although this is an important study, it must be noted that only about 40% of patients with a positive test result were actually found to have cancer,” Dr. Olszanski said. “Conversely, about 60% of patients with a positive test result likely suffered from a considerable amount of anxiety that may persist even after further testing did not reveal a malignancy.”
Another important issue is that such testing may incur substantial health care cost. “Less than 2 participants per 100 had a positive test result, and those patients underwent further testing to interrogate the result,” he added. “It also remains unclear if detecting cancer early will lead to better outcomes.”
Whether or not the test will be cost-effective remains unknown, as Dr. Schrag emphasized they do not have a formal cost analysis at this time. “This technology is not ready for population-wide screening, but as the technology improves, costs will go down,” she said.
Dr. Schrag also added that this is a new concept and the trial shows it is feasible to detect cancer using a blood test. “It was not designed to determine if the test can decrease cancer mortality, which is obviously the purpose of screening, but it’s premature for that,” she said.
Details of the results
The Galleri test uses cell-free DNA and machine learning to detect a common cancer signal across more than 50 cancer types as well as to predict cancer signal origin.
Overall, the test detected a cancer signal in 1.4% (n = 92) of participants with analyzable samples.
A total of 90 participants underwent diagnostic testing (33 true positives and 57 false positives). Of the true positives, 81.8% underwent more than one invasive diagnostic test, as did 29.8% of false positives.
Specificity was 99.1%, positive predictive value (PPV) was approximately 40%, and 73% of those who were true positives had diagnostic resolution in less than 3 months.
Of the cancers that were diagnosed, 19 were solid tumors and 17 were hematologic cancers; 7 were diagnosed in a person with a history of cancer, 26 were cancer types without standard screening, and 14 were diagnosed at an early stage.
“What is exciting about this new paradigm is that many of these were cancers for which we don’t have standard screening,” said Dr. Schrag.
Dr. Schrag noted that given the immense interest in this study, the manufacturer is working toward refining the assay and improving the test. A reanalysis was conducted on all specimens using a refined version of the test.
“Importantly, the new analysis identified fewer patients with having positive signals, from 1.4% to 0.9%,” she said. “Specificity improved to 99.5% as did PPV – from 38% to 43.1% – and more people need to be screened to find a cancer – up to 263 from 189.”
False positives concerning
Previous, and very similar, results from the PATHFINDER trial were presented last year at the annual meeting of the American Society of Clinical Oncology.
Max Diehn, MD, PhD, associate professor of radiation oncology at Stanford (Calif.) University, was an invited discussant for the study.
He pointed out that there were more false positives than true positives and noted that “there were a significant number of invasive procedures in false positives, which could cause harm to these patients who don’t have cancer.”
Dr. Diehn also explained that most true positives were for lymphoid malignancies, not solid tumors, and it is not known whether early detection of lymphoid malignancy has clinical utility.
The Galleri test is already available in the United States and is being offered by a number of U.S. health networks. However, it is not approved by the U.S. Food and Drug Administration and is not covered by medical insurance, so individuals have to pay around $950 for it out of pocket.
Although some experts are excited by its potential, describing it as a “game-changer,” others are concerned that there are no clinical pathways in place yet to deal with the results of such a blood test, and say it is not ready for prime time.
The study was funded by Grail, a subsidiary of Illumina. Dr. Shrag has reported relationships with Grail, the Journal of the American Medical Association, and Pfizer. Several coauthors also have disclosed relationships with industry. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and Instil Bio, and running trials for them.
A version of this article first appeared on Medscape.com.
PARIS –
“As this technology develops, people must continue with their standard cancer screening, but this is a glimpse of what the future may hold,” commented study investigator Deborah Schrag, MD, MPH, chair, department of medicine, Memorial Sloan Kettering Cancer Center, New York.
For the PATHFINDER study, the Galleri blood test (developed by Grail) was used in 6,621 healthy individuals aged over 50, with or without additional cancer risk factors (such as history of smoking or genetic risk).
It found a positive cancer signal in 92 individuals (1.4%).
None of the individuals who tested positive was known to have cancer at the time of testing. Subsequent workup, which could include scans and/or biopsy, found cancer in 38% of those with a positive test.
“When the test was positive, the workups were typically done in less than 3 months,” Dr. Schrag commented, adding that “the blood test typically predicted the origin of the cancer.”
Dr. Schrag presented the findings at the annual meeting of the European Society for Medical Oncology (ESMO).
Approached for comment, Anthony J. Olszanski, MD, RPh, vice chair of research at the Fox Chase Cancer Center, Philadelphia, noted that the use of a blood test to “find” cancer has long been on the minds of patients. “It is not uncommon to hear oncology patients ask: ‘Why didn’t my doctor find my cancer earlier, on blood tests?’ ”
As this study suggests, finding a malignancy before it becomes apparent on imaging or because of symptoms is one step closer to becoming a reality. “But although this is an important study, it must be noted that only about 40% of patients with a positive test result were actually found to have cancer,” Dr. Olszanski said. “Conversely, about 60% of patients with a positive test result likely suffered from a considerable amount of anxiety that may persist even after further testing did not reveal a malignancy.”
Another important issue is that such testing may incur substantial health care cost. “Less than 2 participants per 100 had a positive test result, and those patients underwent further testing to interrogate the result,” he added. “It also remains unclear if detecting cancer early will lead to better outcomes.”
Whether or not the test will be cost-effective remains unknown, as Dr. Schrag emphasized they do not have a formal cost analysis at this time. “This technology is not ready for population-wide screening, but as the technology improves, costs will go down,” she said.
Dr. Schrag also added that this is a new concept and the trial shows it is feasible to detect cancer using a blood test. “It was not designed to determine if the test can decrease cancer mortality, which is obviously the purpose of screening, but it’s premature for that,” she said.
Details of the results
The Galleri test uses cell-free DNA and machine learning to detect a common cancer signal across more than 50 cancer types as well as to predict cancer signal origin.
Overall, the test detected a cancer signal in 1.4% (n = 92) of participants with analyzable samples.
A total of 90 participants underwent diagnostic testing (33 true positives and 57 false positives). Of the true positives, 81.8% underwent more than one invasive diagnostic test, as did 29.8% of false positives.
Specificity was 99.1%, positive predictive value (PPV) was approximately 40%, and 73% of those who were true positives had diagnostic resolution in less than 3 months.
Of the cancers that were diagnosed, 19 were solid tumors and 17 were hematologic cancers; 7 were diagnosed in a person with a history of cancer, 26 were cancer types without standard screening, and 14 were diagnosed at an early stage.
“What is exciting about this new paradigm is that many of these were cancers for which we don’t have standard screening,” said Dr. Schrag.
Dr. Schrag noted that given the immense interest in this study, the manufacturer is working toward refining the assay and improving the test. A reanalysis was conducted on all specimens using a refined version of the test.
“Importantly, the new analysis identified fewer patients with having positive signals, from 1.4% to 0.9%,” she said. “Specificity improved to 99.5% as did PPV – from 38% to 43.1% – and more people need to be screened to find a cancer – up to 263 from 189.”
False positives concerning
Previous, and very similar, results from the PATHFINDER trial were presented last year at the annual meeting of the American Society of Clinical Oncology.
Max Diehn, MD, PhD, associate professor of radiation oncology at Stanford (Calif.) University, was an invited discussant for the study.
He pointed out that there were more false positives than true positives and noted that “there were a significant number of invasive procedures in false positives, which could cause harm to these patients who don’t have cancer.”
Dr. Diehn also explained that most true positives were for lymphoid malignancies, not solid tumors, and it is not known whether early detection of lymphoid malignancy has clinical utility.
The Galleri test is already available in the United States and is being offered by a number of U.S. health networks. However, it is not approved by the U.S. Food and Drug Administration and is not covered by medical insurance, so individuals have to pay around $950 for it out of pocket.
Although some experts are excited by its potential, describing it as a “game-changer,” others are concerned that there are no clinical pathways in place yet to deal with the results of such a blood test, and say it is not ready for prime time.
The study was funded by Grail, a subsidiary of Illumina. Dr. Shrag has reported relationships with Grail, the Journal of the American Medical Association, and Pfizer. Several coauthors also have disclosed relationships with industry. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and Instil Bio, and running trials for them.
A version of this article first appeared on Medscape.com.
PARIS –
“As this technology develops, people must continue with their standard cancer screening, but this is a glimpse of what the future may hold,” commented study investigator Deborah Schrag, MD, MPH, chair, department of medicine, Memorial Sloan Kettering Cancer Center, New York.
For the PATHFINDER study, the Galleri blood test (developed by Grail) was used in 6,621 healthy individuals aged over 50, with or without additional cancer risk factors (such as history of smoking or genetic risk).
It found a positive cancer signal in 92 individuals (1.4%).
None of the individuals who tested positive was known to have cancer at the time of testing. Subsequent workup, which could include scans and/or biopsy, found cancer in 38% of those with a positive test.
“When the test was positive, the workups were typically done in less than 3 months,” Dr. Schrag commented, adding that “the blood test typically predicted the origin of the cancer.”
Dr. Schrag presented the findings at the annual meeting of the European Society for Medical Oncology (ESMO).
Approached for comment, Anthony J. Olszanski, MD, RPh, vice chair of research at the Fox Chase Cancer Center, Philadelphia, noted that the use of a blood test to “find” cancer has long been on the minds of patients. “It is not uncommon to hear oncology patients ask: ‘Why didn’t my doctor find my cancer earlier, on blood tests?’ ”
As this study suggests, finding a malignancy before it becomes apparent on imaging or because of symptoms is one step closer to becoming a reality. “But although this is an important study, it must be noted that only about 40% of patients with a positive test result were actually found to have cancer,” Dr. Olszanski said. “Conversely, about 60% of patients with a positive test result likely suffered from a considerable amount of anxiety that may persist even after further testing did not reveal a malignancy.”
Another important issue is that such testing may incur substantial health care cost. “Less than 2 participants per 100 had a positive test result, and those patients underwent further testing to interrogate the result,” he added. “It also remains unclear if detecting cancer early will lead to better outcomes.”
Whether or not the test will be cost-effective remains unknown, as Dr. Schrag emphasized they do not have a formal cost analysis at this time. “This technology is not ready for population-wide screening, but as the technology improves, costs will go down,” she said.
Dr. Schrag also added that this is a new concept and the trial shows it is feasible to detect cancer using a blood test. “It was not designed to determine if the test can decrease cancer mortality, which is obviously the purpose of screening, but it’s premature for that,” she said.
Details of the results
The Galleri test uses cell-free DNA and machine learning to detect a common cancer signal across more than 50 cancer types as well as to predict cancer signal origin.
Overall, the test detected a cancer signal in 1.4% (n = 92) of participants with analyzable samples.
A total of 90 participants underwent diagnostic testing (33 true positives and 57 false positives). Of the true positives, 81.8% underwent more than one invasive diagnostic test, as did 29.8% of false positives.
Specificity was 99.1%, positive predictive value (PPV) was approximately 40%, and 73% of those who were true positives had diagnostic resolution in less than 3 months.
Of the cancers that were diagnosed, 19 were solid tumors and 17 were hematologic cancers; 7 were diagnosed in a person with a history of cancer, 26 were cancer types without standard screening, and 14 were diagnosed at an early stage.
“What is exciting about this new paradigm is that many of these were cancers for which we don’t have standard screening,” said Dr. Schrag.
Dr. Schrag noted that given the immense interest in this study, the manufacturer is working toward refining the assay and improving the test. A reanalysis was conducted on all specimens using a refined version of the test.
“Importantly, the new analysis identified fewer patients with having positive signals, from 1.4% to 0.9%,” she said. “Specificity improved to 99.5% as did PPV – from 38% to 43.1% – and more people need to be screened to find a cancer – up to 263 from 189.”
False positives concerning
Previous, and very similar, results from the PATHFINDER trial were presented last year at the annual meeting of the American Society of Clinical Oncology.
Max Diehn, MD, PhD, associate professor of radiation oncology at Stanford (Calif.) University, was an invited discussant for the study.
He pointed out that there were more false positives than true positives and noted that “there were a significant number of invasive procedures in false positives, which could cause harm to these patients who don’t have cancer.”
Dr. Diehn also explained that most true positives were for lymphoid malignancies, not solid tumors, and it is not known whether early detection of lymphoid malignancy has clinical utility.
The Galleri test is already available in the United States and is being offered by a number of U.S. health networks. However, it is not approved by the U.S. Food and Drug Administration and is not covered by medical insurance, so individuals have to pay around $950 for it out of pocket.
Although some experts are excited by its potential, describing it as a “game-changer,” others are concerned that there are no clinical pathways in place yet to deal with the results of such a blood test, and say it is not ready for prime time.
The study was funded by Grail, a subsidiary of Illumina. Dr. Shrag has reported relationships with Grail, the Journal of the American Medical Association, and Pfizer. Several coauthors also have disclosed relationships with industry. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and Instil Bio, and running trials for them.
A version of this article first appeared on Medscape.com.
AT ESMO 2022
Reporting Coronary Artery Calcium on Low-Dose Computed Tomography Impacts Statin Management in a Lung Cancer Screening Population
Cigarette smoking is an independent risk factor for lung cancer and atherosclerotic cardiovascular disease (ASCVD).1-3 The National Lung Screening Trial (NLST) demonstrated both lung cancer mortality reduction with the use of surveillance low-dose computed tomography (LDCT) and ASCVD as the most common cause of death among smokers.4,5 ASCVD remains the leading cause of death in the lung cancer screening (LCS) population.2,3 After publication of the NLST results, the US Preventive Services Task Force (USPSTF) established LCS eligibility among smokers and the Center for Medicare and Medicaid Services approved payment for annual LDCT in this group.1,6,7
Recently LDCT has been proposed as an adjunct diagnostic tool for detecting coronary artery calcium (CAC), which is independently associated with ASCVD and mortality.8-13 CAC scores have been recommended by the 2019 American College of Cardiology/American Heart Association cholesterol treatment guidelines and shown to be cost-effective in guiding statin therapy for patients with borderline to intermediate ASCVD risk.14-16 While CAC is conventionally quantified using electrocardiogram (ECG)-gated CT, these scans are not routinely performed in clinical practice because preventive CAC screening is neither recommended by the USPSTF nor covered by most insurance providers.17,18 LDCT, conversely, is reimbursable and a well-validated ASCVD risk predictor.18,19
In this study, we aimed to determine the validity of LDCT in identifying CAC among the military LCS population and whether it would impact statin recommendations based on 10-year ASCVD risk.
Methods
Participants were recruited from a retrospective cohort of 563 Military Health System (MHS) beneficiaries who received LCS with LDCT at Naval Medical Center Portsmouth (NMCP) in Virginia between January 1, 2019, and December 31, 2020. The 2013 USPSTF LCS guidelines were followed as the 2021 guidelines had not been published before the start of the study; thus, eligible participants included adults aged 55 to 80 years with at least a 30-pack-year smoking history and currently smoked or had quit within 15 years from the date of study consent.6,7
Between November 2020 and May 2021, study investigators screened 287 patient records and recruited 190 participants by telephone, starting with individuals who had the most recent LDCT and working backward until reaching the predetermined 170 subjects who had undergone in-office consents before ECG-gated CT scans. Since LDCT was not obtained simultaneously with the ECG-gated CT, participants were required to complete their gated CT within 24 months of their last LDCT. Of the 190 subjects initially recruited, those who were ineligible for LCS (n = 4), had a history of angioplasty, stent, or bypass revascularization procedure (n = 4), did not complete their ECG-gated CT within the specified time frame (n = 8), or withdrew from the study (n = 4) were excluded. While gated CT scans were scored for CAC in the present time, LDCT (previously only read for general lung pathology) was not scored until after participant consent. Patients were peripherally followed, via health record reviews, for 3 months after their gated CT to document any additional imaging ordered by their primary care practitioners. The study was approved by the NMCP Institutional Review Board.
Coronary Artery Calcification Scoring
We performed CT scans using Siemens SOMATOM Flash, a second-generation dual-source scanner; and GE LightSpeed VCT, a single-source, 64-slice scanner. A step-and-shoot prospective trigger technique was used, and contiguous axial images were reconstructed at 2.5-mm or 3-mm intervals for CAC quantification using the Agatston method.20 ECG-gated CT scans were electrocardiographically triggered at mid-diastole (70% of the R-R interval). Radiation dose reduction techniques involved adjustments of the mA according to body mass index and iterative reconstruction. LDCT scans were performed without ECG gating. We reconstructed contiguous axial images at 1-mm intervals for evaluation of the lung parenchyma. Similar dose-reduction techniques were used, to limit radiation exposure for each LDCT scan to < 1.5 mSv, per established guidelines.21 CAC on LDCT was also scored using the Agatston method. CAC was scored on the 2 scan types by different blinded reviewers.
Covariates
We reviewed outpatient health records to obtain participants’ age, sex, medical history, statin use, smoking status (current or former), and pack-years. International Classification of Diseases, Tenth Revision codes within medical encounters were used to document prevalent hypertension, hyperlipidemia, and diabetes mellitus. Participants’ most recent low-density lipoprotein value (within 24 months of ECG-gated CT) was recorded and 10-year ASCVD risk scores were calculated using the pooled cohorts equation.
Statistical Analysis
A power analysis performed before study initiation determined that a prospective sample size of 170 would be sufficient to provide strength of correlation between CAC scores calculated from ECG-gated CT and LDCT and achieve a statistical power of at least 80%. The Wilcoxon rank sum and Fisher exact tests were used to evaluate differences in continuous and categorical CAC scores, respectively. Given skewed distributions, Spearman rank correlations and Kendall W coefficient of concordance were respectively used to evaluate correlation and concordance of CAC scores between the 2 scan types. κ statistics were used to rate agreement between categorical CAC scores. Bland-Altman analysis was performed to determine the bias and limits of agreement between ECG-gated CT and LDCT.22 For categorical CAC score analysis, participants were categorized into 5 groups according to standard Agatston score cut-off points. We defined the 5 categories of CAC for both scan types based on previous analysis from Rumberger and colleagues: CAC = 0 (absent), CAC = 1-10 (minimal), CAC = 11-100 (mild), CAC = 101-400 (moderate), CAC > 400 (severe).23 Of note, LDCT reports at NMCP include a visual CAC score using these qualitative descriptors that were available to LDCT reviewers. Analyses were conducted using SAS version 9.4 and Microsoft Excel; P values < .05 were considered statistically significant.
Results
The 170 participants had a mean (SD) age of 62.1 (4.6) years and were 70.6% male (Table 1). Hyperlipidemia was the most prevalent cardiac risk factor with almost 70% of participants on a statin. There was no incidence of ischemic ASCVD during follow-up, although 1 participant was later diagnosed with lung cancer after evaluation of suspicious pulmonary findings on ECG-gated CT. CAC was identified on both scan types in 126 participants; however, LDCT was discordant with gated CT in identifying CAC in 24 subjects (P < .001).
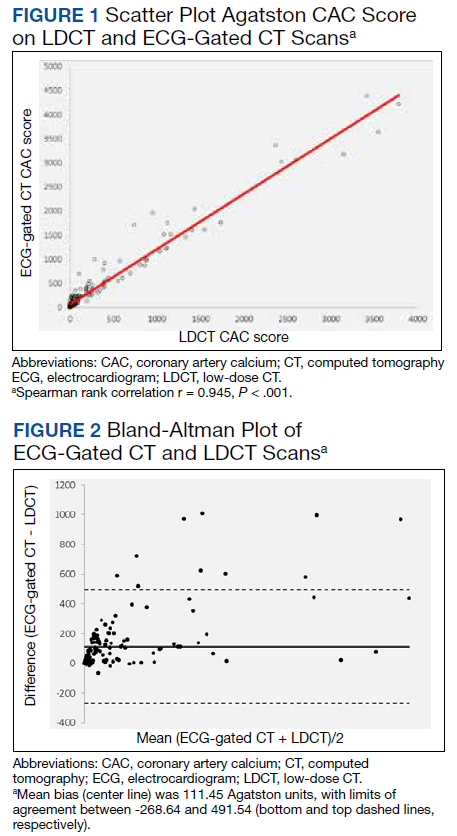
The correlation between CAC scores on ECG-gated CT and LDCT was 0.945 (P < .001) and the concordance was 0.643, indicating moderate agreement between CAC scores on the 2 different scans (Figure 1). Median CAC scores were significantly higher on ECG-gated CT when compared with LDCT (107.5 vs 48.1 Agatston units, respectively; P < .05). Table 2 shows the CAC score characteristics for both scan types. The κ statistic for agreement between categorical CAC scores on ECG-gated CT compared with LDCT was 0.49 (SEκ= 0.05; 95% CI, -0.73-1.71), and the weighted κ statistic was 0.71, indicating moderate to substantial agreement between the 2 scans using the specified cutoff points. The Bland-Altman analysis presented a mean bias of 111.45 Agatston units, with limits of agreement between -268.64 and 491.54, as shown in Figure 2, suggesting that CAC scores on ECG-gated CT were, on average, about 111 units higher than those on LDCT. Finally, there were 24 participants with CAC seen on ECG-gated CT but none identified on LDCT (P < .001); of this cohort 20 were already on a statin, and of the remaining 4 individuals, 1 met statin criteria based on a > 20% ASCVD risk score alone (regardless of CAC score), 1 with an intermediate risk score met statin criteria based on CAC score reporting, 1 did not meet criteria due to a low-risk score, and the last had no reportable ASCVD risk score.
In the study, there were 80 participants with reportable borderline to intermediate 10-year ASCVD risk scores (5% ≤ 10-year ASCVD risk < 20%), 49 of which were taking a statin. Of the remaining 31 participants not on a statin, 19 met statin criteria after CAC was identified on ECG-gated CT (of these 18 also had CAC identified on LDCT). Subsequently, the number of participants who met statin criteria after additional CAC reporting (on ECG-gated CT and LDCT) was statistically significant (P < .001 and P < .05, respectively). Of the 49 participants on a statin, only 1 individual no longer met statin criteria due to a CAC score < 1 on gated CT.
Discussion
In this study population of recruited MHS beneficiaries, there was a strong correlation and moderate to substantial agreement between CAC scores calculated from LDCT and conventional ECG-gated CT. The number of nonstatin participants who met statin criteria and would have benefited from additional CAC score reporting was statistically significant as compared to their statin counterparts who no longer met the criteria.
CAC screening using nongated CT has become an increasingly available and consistently reproducible means for stratifying ASCVD risk and guiding statin therapy in individuals with equivocal ASCVD risk scores.24-26 As has been demonstrated in previous studies, our study additionally highlights the effective use of LDCT in not only identifying CAC, but also in beneficially impacting statin decisions in the high-risk smoking population.24-26 Our results also showed LDCT missed CAC in participants, the majority of which were already on a statin, and only 1 nonstatin individual benefited from additional CAC reporting. CAC scoring on LDCT should be an adjunct, not a substitute, for ASCVD risk stratification to help guide statin management.25,27
Our results may provide cost considerate implications for preventive CAC screening. While TRICARE covers the cost of ECG-gated CT for MHS beneficiaries, the same is not true of most nonmilitary insurance providers. Concerns about cancer risk from radiation exposure may also lead to hesitation about receiving additional CTs in the smoking population. Since the LCS population already receives annual LDCT, these scans can also be used for CAC scoring to help primary care professionals risk stratify their patients, as has been previously shown.28-31 Clinicians should consider implementing CAC scoring with annual LDCT scans, which would curtail further risks and expenses from CAC-specified scans.
Although CAC is scored visually and routinely reported in the body of LDCT reports at our facility, this is not a universal practice and was performed in only 44% of subjects with known CAC by a previous study.32 In 2007, there were 600,000 CAC scoring scans and > 9 million routine chest CTs performed in the United States.33 Based on our results and the growing consensus in the existing literature, CAC scoring on nongated CT is not only valid and reliable, but also can estimate ASCVD risk and subsequent mortality.34-36 Routine chest CTs remain an available resource for providing additional ASCVD risk stratification.
As we demonstrated, median CAC scores on LDCT were on average significantly lower than those from gated CT. This could be due to slice thickness variability between the GE and Siemens scanners or CAC progression between the time of the retrospective LDCT and prospective ECG-gated CT. Aside from this potential limitation, LDCT has been shown to have a high level of agreement with gated CT in predicting CAC, both visually and by the Agatston technique.37-39 Our results further support previous recommendations of utilizing CAC score categories when determining ASCVD risk from LDCT and that establishing scoring cutoff points warrants further development for potential standardization.37-39 Readers should be mindful that LDCT may still be less sensitive and underestimate low CAC levels and that ECG-gated CT may occasionally be more optimal in determining ASCVD risk when considering the negative predictive value of CAC.40
Limitations
Our study cohort was composed of MHS beneficiaries. Compared with the general population, these individuals may have greater access to care and be more likely to receive statins after preventive screenings. Additional studies may be required to assess CAC-associated statin eligibility among the general population. As discussed previously LDCT was not performed concomitantly with the ECG-gated CT. Although there was moderate to substantial CAC agreement between the 2 scan types, the timing difference could have led to absolute differences in CAC scores across both scan types and impacted the ability to detect low-level CAC on LDCT. CAC values should be interpreted based on the respective scan type.
Conclusions
LDCT is a reliable diagnostic alternative to ECG-gated CT in predicting CAC. CAC scores from LDCT are highly correlated and concordant with those from gated CT and can help guide statin management in individuals with intermediate ASCVD risk. The proposed duality of LDCT to assess ASCVD risk in addition to lung cancer can reduce the need for unnecessary scans while optimizing preventive clinical care. While coronary calcium and elevated CAC scores can facilitate clinical decision making to initiate statin therapy for intermediate-risk patients, physicians must still determine whether additional cardiac testing is warranted to avoid unnecessary procedures and health care costs. Smokers undergoing annual LDCT may benefit from standardized CAC scoring to help further stratify ASCVD risk while limiting the expense and radiation of additional scans.
Acknowledgments
The authors thank Ms. Lorie Gower for her contributions to the study.
1. Leigh A, McEvoy JW, Garg P, et al. Coronary artery calcium scores and atherosclerotic cardiovascular disease risk stratification in smokers. JACC Cardiovasc Imaging. 2019;12(5):852-861. doi:10.1016/j.jcmg.2017.12.017
2. Lu MT, Onuma OK, Massaro JM, D’Agostino RB Sr, O’Donnell CJ, Hoffmann U. Lung cancer screening eligibility in the community: cardiovascular risk factors, coronary artery calcification, and cardiovascular events. Circulation. 2016;134(12):897-899. doi:10.1161/CIRCULATIONAHA.116.023957
3. Tailor TD, Chiles C, Yeboah J, et al. Cardiovascular risk in the lung cancer screening population: a multicenter study evaluating the association between coronary artery calcification and preventive statin prescription. J Am Coll Radiol. 2021;18(9):1258-1266. doi:10.1016/j.jacr.2021.01.015
4. National Lung Screening Trial Research Team, Church TR, Black WC, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med. 2013;368(21):1980-1991. doi:10.1056/NEJMoa1209120
5. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322. doi:10.1161/CIR.0000000000000152
6. Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330-338. doi:10.7326/M13-2771
7. US Preventive Services Task Force, Krist AH, Davidson KW, et al. Screening for lung cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962-970. doi:10.1001/jama.2021.1117
8. Arcadi T, Maffei E, Sverzellati N, et al. Coronary artery calcium score on low-dose computed tomography for lung cancer screening. World J Radiol. 2014;6(6):381-387. doi:10.4329/wjr.v6.i6.381
9. Kim SM, Chung MJ, Lee KS, Choe YH, Yi CA, Choe BK. Coronary calcium screening using low-dose lung cancer screening: effectiveness of MDCT with retrospective reconstruction. AJR Am J Roentgenol. 2008;190(4):917-922. doi:10.2214/AJR.07.2979
10. Ruparel M, Quaife SL, Dickson JL, et al. Evaluation of cardiovascular risk in a lung cancer screening cohort. Thorax. 2019;74(12):1140-1146. doi:10.1136/thoraxjnl-2018-212812
11. Jacobs PC, Gondrie MJ, van der Graaf Y, et al. Coronary artery calcium can predict all-cause mortality and cardiovascular events on low-dose CT screening for lung cancer. AJR Am J Roentgenol. 2012;198(3):505-511. doi:10.2214/AJR.10.5577
12. Fan L, Fan K. Lung cancer screening CT-based coronary artery calcification in predicting cardiovascular events: A systematic review and meta-analysis. Medicine (Baltimore). 2018;97(20):e10461. doi:10.1097/MD.0000000000010461
13. Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary calcium score and cardiovascular risk. J Am Coll Cardiol. 2018;72(4):434-447. doi:10.1016/j.jacc.2018.05.027
14. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e563-e595. doi:10.1161/CIR.0000000000000677
15. Pletcher MJ, Pignone M, Earnshaw S, et al. Using the coronary artery calcium score to guide statin therapy: a cost-effectiveness analysis. Circ Cardiovasc Qual Outcomes. 2014;7(2):276-284. doi:10.1161/CIRCOUTCOMES.113.000799
16. Hong JC, Blankstein R, Shaw LJ, et al. Implications of coronary artery calcium testing for treatment decisions among statin candidates according to the ACC/AHA Cholesterol Management Guidelines: a cost-effectiveness analysis. JACC Cardiovasc Imaging. 2017;10(8):938-952. doi:10.1016/j.jcmg.2017.04.014
17. US Preventive Services Task Force, Curry SJ, Krist AH, et al. Risk assessment for cardiovascular disease with nontraditional risk factors: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320(3):272-280. doi:10.1001/jama.2018.8359
18. Hughes-Austin JM, Dominguez A 3rd, Allison MA, et al. Relationship of coronary calcium on standard chest CT scans with mortality. JACC Cardiovasc Imaging. 2016;9(2):152-159. doi:10.1016/j.jcmg.2015.06.030
19. Haller C, Vandehei A, Fisher R, et al. Incidence and implication of coronary artery calcium on non-gated chest computed tomography scans: a large observational cohort. Cureus. 2019;11(11):e6218. Published 2019 Nov 22. doi:10.7759/cureus.6218
20. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15(4):827-832. doi:10.1016/0735-1097(90)90282-t
21. Aberle D, Berg C, Black W, et al. The National Lung Screening Trial: overview and study design. Radiology. 2011;258(1):243-53. doi:10.1148/radiol.10091808
22. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135-160. doi:10.1177/096228029900800204
23. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc. 1999;74(3):243-252. doi:10.4065/74.3.243
24. Douthit NT, Wyatt N, Schwartz B. Clinical impact of reporting coronary artery calcium scores of non-gated chest computed tomography on statin management. Cureus. 2021;13(5):e14856. Published 2021 May 5. doi:10.7759/cureus.14856
25. Miedema MD, Dardari ZA, Kianoush S, et al. Statin eligibility, coronary artery calcium, and subsequent cardiovascular events according to the 2016 United States Preventive Services Task Force (USPSTF) Statin Guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Heart Assoc. 2018;7(12):e008920. Published 2018 Jun 13. doi:10.1161/JAHA.118.008920
26. Fisher R, Vandehei A, Haller C, et al. Reporting the presence of coronary artery calcium in the final impression of non-gated CT chest scans increases the appropriate utilization of statins. Cureus. 2020;12(9):e10579. Published 2020 Sep 21. doi:10.7759/cureus.10579
27. Blaha MJ, Budoff MJ, DeFilippis AP, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: implications for the JUPITER population from MESA, a population-based cohort study. Lancet. 2011;378(9792):684-692. doi:10.1016/S0140-6736(11)60784-8
28. Waheed S, Pollack S, Roth M, Reichek N, Guerci A, Cao JJ. Collective impact of conventional cardiovascular risk factors and coronary calcium score on clinical outcomes with or without statin therapy: the St Francis Heart Study. Atherosclerosis. 2016;255:193-199. doi:10.1016/j.atherosclerosis.2016.09.060
29. Mahabadi AA, Möhlenkamp S, Lehmann N, et al. CAC score improves coronary and CV risk assessment above statin indication by ESC and AHA/ACC Primary Prevention Guidelines. JACC Cardiovasc Imaging. 2017;10(2):143-153. doi:10.1016/j.jcmg.2016.03.022
30. Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849-858. doi:10.1161/CIRCULATIONAHA.115.018524
31. Hoffmann U, Massaro JM, D’Agostino RB Sr, Kathiresan S, Fox CS, O’Donnell CJ. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the Framingham Heart Study. J Am Heart Assoc. 2016;5(2):e003144. Published 2016 Feb 22. doi:10.1161/JAHA.115.003144
32. Williams KA Sr, Kim JT, Holohan KM. Frequency of unrecognized, unreported, or underreported coronary artery and cardiovascular calcification on noncardiac chest CT. J Cardiovasc Comput Tomogr. 2013;7(3):167-172. doi:10.1016/j.jcct.2013.05.003

33. Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077. doi:10.1001/archinternmed.2009.440
34. Azour L, Kadoch MA, Ward TJ, Eber CD, Jacobi AH. Estimation of cardiovascular risk on routine chest CT: Ordinal coronary artery calcium scoring as an accurate predictor of Agatston score ranges. J Cardiovasc Comput Tomogr. 2017;11(1):8-15. doi:10.1016/j.jcct.2016.10.001
35. Waltz J, Kocher M, Kahn J, Dirr M, Burt JR. The future of concurrent automated coronary artery calcium scoring on screening low-dose computed tomography. Cureus. 2020;12(6):e8574. Published 2020 Jun 12. doi:10.7759/cureus.8574
36. Huang YL, Wu FZ, Wang YC, et al. Reliable categorisation of visual scoring of coronary artery calcification on low-dose CT for lung cancer screening: validation with the standard Agatston score. Eur Radiol. 2013;23(5):1226-1233. doi:10.1007/s00330-012-2726-5
37. Kim YK, Sung YM, Cho SH, Park YN, Choi HY. Reliability analysis of visual ranking of coronary artery calcification on low-dose CT of the thorax for lung cancer screening: comparison with ECG-gated calcium scoring CT. Int J Cardiovasc Imaging. 2014;30 Suppl 2:81-87. doi:10.1007/s10554-014-0507-8
38. Xia C, Vonder M, Pelgrim GJ, et al. High-pitch dual-source CT for coronary artery calcium scoring: A head-to-head comparison of non-triggered chest versus triggered cardiac acquisition. J Cardiovasc Comput Tomogr. 2021;15(1):65-72. doi:10.1016/j.jcct.2020.04.013
39. Hutt A, Duhamel A, Deken V, et al. Coronary calcium screening with dual-source CT: reliability of ungated, high-pitch chest CT in comparison with dedicated calcium-scoring CT. Eur Radiol. 2016;26(6):1521-1528. doi:10.1007/s00330-015-3978-7
40. Blaha MJ, Budoff MJ, Tota-Maharaj R, et al. Improving the CAC score by addition of regional measures of calcium distribution: Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging. 2016;9(12):1407-1416. doi:10.1016/j.jcmg.2016.03.001
Cigarette smoking is an independent risk factor for lung cancer and atherosclerotic cardiovascular disease (ASCVD).1-3 The National Lung Screening Trial (NLST) demonstrated both lung cancer mortality reduction with the use of surveillance low-dose computed tomography (LDCT) and ASCVD as the most common cause of death among smokers.4,5 ASCVD remains the leading cause of death in the lung cancer screening (LCS) population.2,3 After publication of the NLST results, the US Preventive Services Task Force (USPSTF) established LCS eligibility among smokers and the Center for Medicare and Medicaid Services approved payment for annual LDCT in this group.1,6,7
Recently LDCT has been proposed as an adjunct diagnostic tool for detecting coronary artery calcium (CAC), which is independently associated with ASCVD and mortality.8-13 CAC scores have been recommended by the 2019 American College of Cardiology/American Heart Association cholesterol treatment guidelines and shown to be cost-effective in guiding statin therapy for patients with borderline to intermediate ASCVD risk.14-16 While CAC is conventionally quantified using electrocardiogram (ECG)-gated CT, these scans are not routinely performed in clinical practice because preventive CAC screening is neither recommended by the USPSTF nor covered by most insurance providers.17,18 LDCT, conversely, is reimbursable and a well-validated ASCVD risk predictor.18,19
In this study, we aimed to determine the validity of LDCT in identifying CAC among the military LCS population and whether it would impact statin recommendations based on 10-year ASCVD risk.
Methods
Participants were recruited from a retrospective cohort of 563 Military Health System (MHS) beneficiaries who received LCS with LDCT at Naval Medical Center Portsmouth (NMCP) in Virginia between January 1, 2019, and December 31, 2020. The 2013 USPSTF LCS guidelines were followed as the 2021 guidelines had not been published before the start of the study; thus, eligible participants included adults aged 55 to 80 years with at least a 30-pack-year smoking history and currently smoked or had quit within 15 years from the date of study consent.6,7
Between November 2020 and May 2021, study investigators screened 287 patient records and recruited 190 participants by telephone, starting with individuals who had the most recent LDCT and working backward until reaching the predetermined 170 subjects who had undergone in-office consents before ECG-gated CT scans. Since LDCT was not obtained simultaneously with the ECG-gated CT, participants were required to complete their gated CT within 24 months of their last LDCT. Of the 190 subjects initially recruited, those who were ineligible for LCS (n = 4), had a history of angioplasty, stent, or bypass revascularization procedure (n = 4), did not complete their ECG-gated CT within the specified time frame (n = 8), or withdrew from the study (n = 4) were excluded. While gated CT scans were scored for CAC in the present time, LDCT (previously only read for general lung pathology) was not scored until after participant consent. Patients were peripherally followed, via health record reviews, for 3 months after their gated CT to document any additional imaging ordered by their primary care practitioners. The study was approved by the NMCP Institutional Review Board.
Coronary Artery Calcification Scoring
We performed CT scans using Siemens SOMATOM Flash, a second-generation dual-source scanner; and GE LightSpeed VCT, a single-source, 64-slice scanner. A step-and-shoot prospective trigger technique was used, and contiguous axial images were reconstructed at 2.5-mm or 3-mm intervals for CAC quantification using the Agatston method.20 ECG-gated CT scans were electrocardiographically triggered at mid-diastole (70% of the R-R interval). Radiation dose reduction techniques involved adjustments of the mA according to body mass index and iterative reconstruction. LDCT scans were performed without ECG gating. We reconstructed contiguous axial images at 1-mm intervals for evaluation of the lung parenchyma. Similar dose-reduction techniques were used, to limit radiation exposure for each LDCT scan to < 1.5 mSv, per established guidelines.21 CAC on LDCT was also scored using the Agatston method. CAC was scored on the 2 scan types by different blinded reviewers.
Covariates
We reviewed outpatient health records to obtain participants’ age, sex, medical history, statin use, smoking status (current or former), and pack-years. International Classification of Diseases, Tenth Revision codes within medical encounters were used to document prevalent hypertension, hyperlipidemia, and diabetes mellitus. Participants’ most recent low-density lipoprotein value (within 24 months of ECG-gated CT) was recorded and 10-year ASCVD risk scores were calculated using the pooled cohorts equation.
Statistical Analysis
A power analysis performed before study initiation determined that a prospective sample size of 170 would be sufficient to provide strength of correlation between CAC scores calculated from ECG-gated CT and LDCT and achieve a statistical power of at least 80%. The Wilcoxon rank sum and Fisher exact tests were used to evaluate differences in continuous and categorical CAC scores, respectively. Given skewed distributions, Spearman rank correlations and Kendall W coefficient of concordance were respectively used to evaluate correlation and concordance of CAC scores between the 2 scan types. κ statistics were used to rate agreement between categorical CAC scores. Bland-Altman analysis was performed to determine the bias and limits of agreement between ECG-gated CT and LDCT.22 For categorical CAC score analysis, participants were categorized into 5 groups according to standard Agatston score cut-off points. We defined the 5 categories of CAC for both scan types based on previous analysis from Rumberger and colleagues: CAC = 0 (absent), CAC = 1-10 (minimal), CAC = 11-100 (mild), CAC = 101-400 (moderate), CAC > 400 (severe).23 Of note, LDCT reports at NMCP include a visual CAC score using these qualitative descriptors that were available to LDCT reviewers. Analyses were conducted using SAS version 9.4 and Microsoft Excel; P values < .05 were considered statistically significant.
Results
The 170 participants had a mean (SD) age of 62.1 (4.6) years and were 70.6% male (Table 1). Hyperlipidemia was the most prevalent cardiac risk factor with almost 70% of participants on a statin. There was no incidence of ischemic ASCVD during follow-up, although 1 participant was later diagnosed with lung cancer after evaluation of suspicious pulmonary findings on ECG-gated CT. CAC was identified on both scan types in 126 participants; however, LDCT was discordant with gated CT in identifying CAC in 24 subjects (P < .001).
The correlation between CAC scores on ECG-gated CT and LDCT was 0.945 (P < .001) and the concordance was 0.643, indicating moderate agreement between CAC scores on the 2 different scans (Figure 1). Median CAC scores were significantly higher on ECG-gated CT when compared with LDCT (107.5 vs 48.1 Agatston units, respectively; P < .05). Table 2 shows the CAC score characteristics for both scan types. The κ statistic for agreement between categorical CAC scores on ECG-gated CT compared with LDCT was 0.49 (SEκ= 0.05; 95% CI, -0.73-1.71), and the weighted κ statistic was 0.71, indicating moderate to substantial agreement between the 2 scans using the specified cutoff points. The Bland-Altman analysis presented a mean bias of 111.45 Agatston units, with limits of agreement between -268.64 and 491.54, as shown in Figure 2, suggesting that CAC scores on ECG-gated CT were, on average, about 111 units higher than those on LDCT. Finally, there were 24 participants with CAC seen on ECG-gated CT but none identified on LDCT (P < .001); of this cohort 20 were already on a statin, and of the remaining 4 individuals, 1 met statin criteria based on a > 20% ASCVD risk score alone (regardless of CAC score), 1 with an intermediate risk score met statin criteria based on CAC score reporting, 1 did not meet criteria due to a low-risk score, and the last had no reportable ASCVD risk score.
In the study, there were 80 participants with reportable borderline to intermediate 10-year ASCVD risk scores (5% ≤ 10-year ASCVD risk < 20%), 49 of which were taking a statin. Of the remaining 31 participants not on a statin, 19 met statin criteria after CAC was identified on ECG-gated CT (of these 18 also had CAC identified on LDCT). Subsequently, the number of participants who met statin criteria after additional CAC reporting (on ECG-gated CT and LDCT) was statistically significant (P < .001 and P < .05, respectively). Of the 49 participants on a statin, only 1 individual no longer met statin criteria due to a CAC score < 1 on gated CT.
Discussion
In this study population of recruited MHS beneficiaries, there was a strong correlation and moderate to substantial agreement between CAC scores calculated from LDCT and conventional ECG-gated CT. The number of nonstatin participants who met statin criteria and would have benefited from additional CAC score reporting was statistically significant as compared to their statin counterparts who no longer met the criteria.
CAC screening using nongated CT has become an increasingly available and consistently reproducible means for stratifying ASCVD risk and guiding statin therapy in individuals with equivocal ASCVD risk scores.24-26 As has been demonstrated in previous studies, our study additionally highlights the effective use of LDCT in not only identifying CAC, but also in beneficially impacting statin decisions in the high-risk smoking population.24-26 Our results also showed LDCT missed CAC in participants, the majority of which were already on a statin, and only 1 nonstatin individual benefited from additional CAC reporting. CAC scoring on LDCT should be an adjunct, not a substitute, for ASCVD risk stratification to help guide statin management.25,27
Our results may provide cost considerate implications for preventive CAC screening. While TRICARE covers the cost of ECG-gated CT for MHS beneficiaries, the same is not true of most nonmilitary insurance providers. Concerns about cancer risk from radiation exposure may also lead to hesitation about receiving additional CTs in the smoking population. Since the LCS population already receives annual LDCT, these scans can also be used for CAC scoring to help primary care professionals risk stratify their patients, as has been previously shown.28-31 Clinicians should consider implementing CAC scoring with annual LDCT scans, which would curtail further risks and expenses from CAC-specified scans.
Although CAC is scored visually and routinely reported in the body of LDCT reports at our facility, this is not a universal practice and was performed in only 44% of subjects with known CAC by a previous study.32 In 2007, there were 600,000 CAC scoring scans and > 9 million routine chest CTs performed in the United States.33 Based on our results and the growing consensus in the existing literature, CAC scoring on nongated CT is not only valid and reliable, but also can estimate ASCVD risk and subsequent mortality.34-36 Routine chest CTs remain an available resource for providing additional ASCVD risk stratification.
As we demonstrated, median CAC scores on LDCT were on average significantly lower than those from gated CT. This could be due to slice thickness variability between the GE and Siemens scanners or CAC progression between the time of the retrospective LDCT and prospective ECG-gated CT. Aside from this potential limitation, LDCT has been shown to have a high level of agreement with gated CT in predicting CAC, both visually and by the Agatston technique.37-39 Our results further support previous recommendations of utilizing CAC score categories when determining ASCVD risk from LDCT and that establishing scoring cutoff points warrants further development for potential standardization.37-39 Readers should be mindful that LDCT may still be less sensitive and underestimate low CAC levels and that ECG-gated CT may occasionally be more optimal in determining ASCVD risk when considering the negative predictive value of CAC.40
Limitations
Our study cohort was composed of MHS beneficiaries. Compared with the general population, these individuals may have greater access to care and be more likely to receive statins after preventive screenings. Additional studies may be required to assess CAC-associated statin eligibility among the general population. As discussed previously LDCT was not performed concomitantly with the ECG-gated CT. Although there was moderate to substantial CAC agreement between the 2 scan types, the timing difference could have led to absolute differences in CAC scores across both scan types and impacted the ability to detect low-level CAC on LDCT. CAC values should be interpreted based on the respective scan type.
Conclusions
LDCT is a reliable diagnostic alternative to ECG-gated CT in predicting CAC. CAC scores from LDCT are highly correlated and concordant with those from gated CT and can help guide statin management in individuals with intermediate ASCVD risk. The proposed duality of LDCT to assess ASCVD risk in addition to lung cancer can reduce the need for unnecessary scans while optimizing preventive clinical care. While coronary calcium and elevated CAC scores can facilitate clinical decision making to initiate statin therapy for intermediate-risk patients, physicians must still determine whether additional cardiac testing is warranted to avoid unnecessary procedures and health care costs. Smokers undergoing annual LDCT may benefit from standardized CAC scoring to help further stratify ASCVD risk while limiting the expense and radiation of additional scans.
Acknowledgments
The authors thank Ms. Lorie Gower for her contributions to the study.
Cigarette smoking is an independent risk factor for lung cancer and atherosclerotic cardiovascular disease (ASCVD).1-3 The National Lung Screening Trial (NLST) demonstrated both lung cancer mortality reduction with the use of surveillance low-dose computed tomography (LDCT) and ASCVD as the most common cause of death among smokers.4,5 ASCVD remains the leading cause of death in the lung cancer screening (LCS) population.2,3 After publication of the NLST results, the US Preventive Services Task Force (USPSTF) established LCS eligibility among smokers and the Center for Medicare and Medicaid Services approved payment for annual LDCT in this group.1,6,7
Recently LDCT has been proposed as an adjunct diagnostic tool for detecting coronary artery calcium (CAC), which is independently associated with ASCVD and mortality.8-13 CAC scores have been recommended by the 2019 American College of Cardiology/American Heart Association cholesterol treatment guidelines and shown to be cost-effective in guiding statin therapy for patients with borderline to intermediate ASCVD risk.14-16 While CAC is conventionally quantified using electrocardiogram (ECG)-gated CT, these scans are not routinely performed in clinical practice because preventive CAC screening is neither recommended by the USPSTF nor covered by most insurance providers.17,18 LDCT, conversely, is reimbursable and a well-validated ASCVD risk predictor.18,19
In this study, we aimed to determine the validity of LDCT in identifying CAC among the military LCS population and whether it would impact statin recommendations based on 10-year ASCVD risk.
Methods
Participants were recruited from a retrospective cohort of 563 Military Health System (MHS) beneficiaries who received LCS with LDCT at Naval Medical Center Portsmouth (NMCP) in Virginia between January 1, 2019, and December 31, 2020. The 2013 USPSTF LCS guidelines were followed as the 2021 guidelines had not been published before the start of the study; thus, eligible participants included adults aged 55 to 80 years with at least a 30-pack-year smoking history and currently smoked or had quit within 15 years from the date of study consent.6,7
Between November 2020 and May 2021, study investigators screened 287 patient records and recruited 190 participants by telephone, starting with individuals who had the most recent LDCT and working backward until reaching the predetermined 170 subjects who had undergone in-office consents before ECG-gated CT scans. Since LDCT was not obtained simultaneously with the ECG-gated CT, participants were required to complete their gated CT within 24 months of their last LDCT. Of the 190 subjects initially recruited, those who were ineligible for LCS (n = 4), had a history of angioplasty, stent, or bypass revascularization procedure (n = 4), did not complete their ECG-gated CT within the specified time frame (n = 8), or withdrew from the study (n = 4) were excluded. While gated CT scans were scored for CAC in the present time, LDCT (previously only read for general lung pathology) was not scored until after participant consent. Patients were peripherally followed, via health record reviews, for 3 months after their gated CT to document any additional imaging ordered by their primary care practitioners. The study was approved by the NMCP Institutional Review Board.
Coronary Artery Calcification Scoring
We performed CT scans using Siemens SOMATOM Flash, a second-generation dual-source scanner; and GE LightSpeed VCT, a single-source, 64-slice scanner. A step-and-shoot prospective trigger technique was used, and contiguous axial images were reconstructed at 2.5-mm or 3-mm intervals for CAC quantification using the Agatston method.20 ECG-gated CT scans were electrocardiographically triggered at mid-diastole (70% of the R-R interval). Radiation dose reduction techniques involved adjustments of the mA according to body mass index and iterative reconstruction. LDCT scans were performed without ECG gating. We reconstructed contiguous axial images at 1-mm intervals for evaluation of the lung parenchyma. Similar dose-reduction techniques were used, to limit radiation exposure for each LDCT scan to < 1.5 mSv, per established guidelines.21 CAC on LDCT was also scored using the Agatston method. CAC was scored on the 2 scan types by different blinded reviewers.
Covariates
We reviewed outpatient health records to obtain participants’ age, sex, medical history, statin use, smoking status (current or former), and pack-years. International Classification of Diseases, Tenth Revision codes within medical encounters were used to document prevalent hypertension, hyperlipidemia, and diabetes mellitus. Participants’ most recent low-density lipoprotein value (within 24 months of ECG-gated CT) was recorded and 10-year ASCVD risk scores were calculated using the pooled cohorts equation.
Statistical Analysis
A power analysis performed before study initiation determined that a prospective sample size of 170 would be sufficient to provide strength of correlation between CAC scores calculated from ECG-gated CT and LDCT and achieve a statistical power of at least 80%. The Wilcoxon rank sum and Fisher exact tests were used to evaluate differences in continuous and categorical CAC scores, respectively. Given skewed distributions, Spearman rank correlations and Kendall W coefficient of concordance were respectively used to evaluate correlation and concordance of CAC scores between the 2 scan types. κ statistics were used to rate agreement between categorical CAC scores. Bland-Altman analysis was performed to determine the bias and limits of agreement between ECG-gated CT and LDCT.22 For categorical CAC score analysis, participants were categorized into 5 groups according to standard Agatston score cut-off points. We defined the 5 categories of CAC for both scan types based on previous analysis from Rumberger and colleagues: CAC = 0 (absent), CAC = 1-10 (minimal), CAC = 11-100 (mild), CAC = 101-400 (moderate), CAC > 400 (severe).23 Of note, LDCT reports at NMCP include a visual CAC score using these qualitative descriptors that were available to LDCT reviewers. Analyses were conducted using SAS version 9.4 and Microsoft Excel; P values < .05 were considered statistically significant.
Results
The 170 participants had a mean (SD) age of 62.1 (4.6) years and were 70.6% male (Table 1). Hyperlipidemia was the most prevalent cardiac risk factor with almost 70% of participants on a statin. There was no incidence of ischemic ASCVD during follow-up, although 1 participant was later diagnosed with lung cancer after evaluation of suspicious pulmonary findings on ECG-gated CT. CAC was identified on both scan types in 126 participants; however, LDCT was discordant with gated CT in identifying CAC in 24 subjects (P < .001).
The correlation between CAC scores on ECG-gated CT and LDCT was 0.945 (P < .001) and the concordance was 0.643, indicating moderate agreement between CAC scores on the 2 different scans (Figure 1). Median CAC scores were significantly higher on ECG-gated CT when compared with LDCT (107.5 vs 48.1 Agatston units, respectively; P < .05). Table 2 shows the CAC score characteristics for both scan types. The κ statistic for agreement between categorical CAC scores on ECG-gated CT compared with LDCT was 0.49 (SEκ= 0.05; 95% CI, -0.73-1.71), and the weighted κ statistic was 0.71, indicating moderate to substantial agreement between the 2 scans using the specified cutoff points. The Bland-Altman analysis presented a mean bias of 111.45 Agatston units, with limits of agreement between -268.64 and 491.54, as shown in Figure 2, suggesting that CAC scores on ECG-gated CT were, on average, about 111 units higher than those on LDCT. Finally, there were 24 participants with CAC seen on ECG-gated CT but none identified on LDCT (P < .001); of this cohort 20 were already on a statin, and of the remaining 4 individuals, 1 met statin criteria based on a > 20% ASCVD risk score alone (regardless of CAC score), 1 with an intermediate risk score met statin criteria based on CAC score reporting, 1 did not meet criteria due to a low-risk score, and the last had no reportable ASCVD risk score.
In the study, there were 80 participants with reportable borderline to intermediate 10-year ASCVD risk scores (5% ≤ 10-year ASCVD risk < 20%), 49 of which were taking a statin. Of the remaining 31 participants not on a statin, 19 met statin criteria after CAC was identified on ECG-gated CT (of these 18 also had CAC identified on LDCT). Subsequently, the number of participants who met statin criteria after additional CAC reporting (on ECG-gated CT and LDCT) was statistically significant (P < .001 and P < .05, respectively). Of the 49 participants on a statin, only 1 individual no longer met statin criteria due to a CAC score < 1 on gated CT.
Discussion
In this study population of recruited MHS beneficiaries, there was a strong correlation and moderate to substantial agreement between CAC scores calculated from LDCT and conventional ECG-gated CT. The number of nonstatin participants who met statin criteria and would have benefited from additional CAC score reporting was statistically significant as compared to their statin counterparts who no longer met the criteria.
CAC screening using nongated CT has become an increasingly available and consistently reproducible means for stratifying ASCVD risk and guiding statin therapy in individuals with equivocal ASCVD risk scores.24-26 As has been demonstrated in previous studies, our study additionally highlights the effective use of LDCT in not only identifying CAC, but also in beneficially impacting statin decisions in the high-risk smoking population.24-26 Our results also showed LDCT missed CAC in participants, the majority of which were already on a statin, and only 1 nonstatin individual benefited from additional CAC reporting. CAC scoring on LDCT should be an adjunct, not a substitute, for ASCVD risk stratification to help guide statin management.25,27
Our results may provide cost considerate implications for preventive CAC screening. While TRICARE covers the cost of ECG-gated CT for MHS beneficiaries, the same is not true of most nonmilitary insurance providers. Concerns about cancer risk from radiation exposure may also lead to hesitation about receiving additional CTs in the smoking population. Since the LCS population already receives annual LDCT, these scans can also be used for CAC scoring to help primary care professionals risk stratify their patients, as has been previously shown.28-31 Clinicians should consider implementing CAC scoring with annual LDCT scans, which would curtail further risks and expenses from CAC-specified scans.
Although CAC is scored visually and routinely reported in the body of LDCT reports at our facility, this is not a universal practice and was performed in only 44% of subjects with known CAC by a previous study.32 In 2007, there were 600,000 CAC scoring scans and > 9 million routine chest CTs performed in the United States.33 Based on our results and the growing consensus in the existing literature, CAC scoring on nongated CT is not only valid and reliable, but also can estimate ASCVD risk and subsequent mortality.34-36 Routine chest CTs remain an available resource for providing additional ASCVD risk stratification.
As we demonstrated, median CAC scores on LDCT were on average significantly lower than those from gated CT. This could be due to slice thickness variability between the GE and Siemens scanners or CAC progression between the time of the retrospective LDCT and prospective ECG-gated CT. Aside from this potential limitation, LDCT has been shown to have a high level of agreement with gated CT in predicting CAC, both visually and by the Agatston technique.37-39 Our results further support previous recommendations of utilizing CAC score categories when determining ASCVD risk from LDCT and that establishing scoring cutoff points warrants further development for potential standardization.37-39 Readers should be mindful that LDCT may still be less sensitive and underestimate low CAC levels and that ECG-gated CT may occasionally be more optimal in determining ASCVD risk when considering the negative predictive value of CAC.40
Limitations
Our study cohort was composed of MHS beneficiaries. Compared with the general population, these individuals may have greater access to care and be more likely to receive statins after preventive screenings. Additional studies may be required to assess CAC-associated statin eligibility among the general population. As discussed previously LDCT was not performed concomitantly with the ECG-gated CT. Although there was moderate to substantial CAC agreement between the 2 scan types, the timing difference could have led to absolute differences in CAC scores across both scan types and impacted the ability to detect low-level CAC on LDCT. CAC values should be interpreted based on the respective scan type.
Conclusions
LDCT is a reliable diagnostic alternative to ECG-gated CT in predicting CAC. CAC scores from LDCT are highly correlated and concordant with those from gated CT and can help guide statin management in individuals with intermediate ASCVD risk. The proposed duality of LDCT to assess ASCVD risk in addition to lung cancer can reduce the need for unnecessary scans while optimizing preventive clinical care. While coronary calcium and elevated CAC scores can facilitate clinical decision making to initiate statin therapy for intermediate-risk patients, physicians must still determine whether additional cardiac testing is warranted to avoid unnecessary procedures and health care costs. Smokers undergoing annual LDCT may benefit from standardized CAC scoring to help further stratify ASCVD risk while limiting the expense and radiation of additional scans.
Acknowledgments
The authors thank Ms. Lorie Gower for her contributions to the study.
1. Leigh A, McEvoy JW, Garg P, et al. Coronary artery calcium scores and atherosclerotic cardiovascular disease risk stratification in smokers. JACC Cardiovasc Imaging. 2019;12(5):852-861. doi:10.1016/j.jcmg.2017.12.017
2. Lu MT, Onuma OK, Massaro JM, D’Agostino RB Sr, O’Donnell CJ, Hoffmann U. Lung cancer screening eligibility in the community: cardiovascular risk factors, coronary artery calcification, and cardiovascular events. Circulation. 2016;134(12):897-899. doi:10.1161/CIRCULATIONAHA.116.023957
3. Tailor TD, Chiles C, Yeboah J, et al. Cardiovascular risk in the lung cancer screening population: a multicenter study evaluating the association between coronary artery calcification and preventive statin prescription. J Am Coll Radiol. 2021;18(9):1258-1266. doi:10.1016/j.jacr.2021.01.015
4. National Lung Screening Trial Research Team, Church TR, Black WC, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med. 2013;368(21):1980-1991. doi:10.1056/NEJMoa1209120
5. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322. doi:10.1161/CIR.0000000000000152
6. Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330-338. doi:10.7326/M13-2771
7. US Preventive Services Task Force, Krist AH, Davidson KW, et al. Screening for lung cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962-970. doi:10.1001/jama.2021.1117
8. Arcadi T, Maffei E, Sverzellati N, et al. Coronary artery calcium score on low-dose computed tomography for lung cancer screening. World J Radiol. 2014;6(6):381-387. doi:10.4329/wjr.v6.i6.381
9. Kim SM, Chung MJ, Lee KS, Choe YH, Yi CA, Choe BK. Coronary calcium screening using low-dose lung cancer screening: effectiveness of MDCT with retrospective reconstruction. AJR Am J Roentgenol. 2008;190(4):917-922. doi:10.2214/AJR.07.2979
10. Ruparel M, Quaife SL, Dickson JL, et al. Evaluation of cardiovascular risk in a lung cancer screening cohort. Thorax. 2019;74(12):1140-1146. doi:10.1136/thoraxjnl-2018-212812
11. Jacobs PC, Gondrie MJ, van der Graaf Y, et al. Coronary artery calcium can predict all-cause mortality and cardiovascular events on low-dose CT screening for lung cancer. AJR Am J Roentgenol. 2012;198(3):505-511. doi:10.2214/AJR.10.5577
12. Fan L, Fan K. Lung cancer screening CT-based coronary artery calcification in predicting cardiovascular events: A systematic review and meta-analysis. Medicine (Baltimore). 2018;97(20):e10461. doi:10.1097/MD.0000000000010461
13. Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary calcium score and cardiovascular risk. J Am Coll Cardiol. 2018;72(4):434-447. doi:10.1016/j.jacc.2018.05.027
14. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e563-e595. doi:10.1161/CIR.0000000000000677
15. Pletcher MJ, Pignone M, Earnshaw S, et al. Using the coronary artery calcium score to guide statin therapy: a cost-effectiveness analysis. Circ Cardiovasc Qual Outcomes. 2014;7(2):276-284. doi:10.1161/CIRCOUTCOMES.113.000799
16. Hong JC, Blankstein R, Shaw LJ, et al. Implications of coronary artery calcium testing for treatment decisions among statin candidates according to the ACC/AHA Cholesterol Management Guidelines: a cost-effectiveness analysis. JACC Cardiovasc Imaging. 2017;10(8):938-952. doi:10.1016/j.jcmg.2017.04.014
17. US Preventive Services Task Force, Curry SJ, Krist AH, et al. Risk assessment for cardiovascular disease with nontraditional risk factors: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320(3):272-280. doi:10.1001/jama.2018.8359
18. Hughes-Austin JM, Dominguez A 3rd, Allison MA, et al. Relationship of coronary calcium on standard chest CT scans with mortality. JACC Cardiovasc Imaging. 2016;9(2):152-159. doi:10.1016/j.jcmg.2015.06.030
19. Haller C, Vandehei A, Fisher R, et al. Incidence and implication of coronary artery calcium on non-gated chest computed tomography scans: a large observational cohort. Cureus. 2019;11(11):e6218. Published 2019 Nov 22. doi:10.7759/cureus.6218
20. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15(4):827-832. doi:10.1016/0735-1097(90)90282-t
21. Aberle D, Berg C, Black W, et al. The National Lung Screening Trial: overview and study design. Radiology. 2011;258(1):243-53. doi:10.1148/radiol.10091808
22. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135-160. doi:10.1177/096228029900800204
23. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc. 1999;74(3):243-252. doi:10.4065/74.3.243
24. Douthit NT, Wyatt N, Schwartz B. Clinical impact of reporting coronary artery calcium scores of non-gated chest computed tomography on statin management. Cureus. 2021;13(5):e14856. Published 2021 May 5. doi:10.7759/cureus.14856
25. Miedema MD, Dardari ZA, Kianoush S, et al. Statin eligibility, coronary artery calcium, and subsequent cardiovascular events according to the 2016 United States Preventive Services Task Force (USPSTF) Statin Guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Heart Assoc. 2018;7(12):e008920. Published 2018 Jun 13. doi:10.1161/JAHA.118.008920
26. Fisher R, Vandehei A, Haller C, et al. Reporting the presence of coronary artery calcium in the final impression of non-gated CT chest scans increases the appropriate utilization of statins. Cureus. 2020;12(9):e10579. Published 2020 Sep 21. doi:10.7759/cureus.10579
27. Blaha MJ, Budoff MJ, DeFilippis AP, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: implications for the JUPITER population from MESA, a population-based cohort study. Lancet. 2011;378(9792):684-692. doi:10.1016/S0140-6736(11)60784-8
28. Waheed S, Pollack S, Roth M, Reichek N, Guerci A, Cao JJ. Collective impact of conventional cardiovascular risk factors and coronary calcium score on clinical outcomes with or without statin therapy: the St Francis Heart Study. Atherosclerosis. 2016;255:193-199. doi:10.1016/j.atherosclerosis.2016.09.060
29. Mahabadi AA, Möhlenkamp S, Lehmann N, et al. CAC score improves coronary and CV risk assessment above statin indication by ESC and AHA/ACC Primary Prevention Guidelines. JACC Cardiovasc Imaging. 2017;10(2):143-153. doi:10.1016/j.jcmg.2016.03.022
30. Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849-858. doi:10.1161/CIRCULATIONAHA.115.018524
31. Hoffmann U, Massaro JM, D’Agostino RB Sr, Kathiresan S, Fox CS, O’Donnell CJ. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the Framingham Heart Study. J Am Heart Assoc. 2016;5(2):e003144. Published 2016 Feb 22. doi:10.1161/JAHA.115.003144
32. Williams KA Sr, Kim JT, Holohan KM. Frequency of unrecognized, unreported, or underreported coronary artery and cardiovascular calcification on noncardiac chest CT. J Cardiovasc Comput Tomogr. 2013;7(3):167-172. doi:10.1016/j.jcct.2013.05.003
33. Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077. doi:10.1001/archinternmed.2009.440
34. Azour L, Kadoch MA, Ward TJ, Eber CD, Jacobi AH. Estimation of cardiovascular risk on routine chest CT: Ordinal coronary artery calcium scoring as an accurate predictor of Agatston score ranges. J Cardiovasc Comput Tomogr. 2017;11(1):8-15. doi:10.1016/j.jcct.2016.10.001
35. Waltz J, Kocher M, Kahn J, Dirr M, Burt JR. The future of concurrent automated coronary artery calcium scoring on screening low-dose computed tomography. Cureus. 2020;12(6):e8574. Published 2020 Jun 12. doi:10.7759/cureus.8574
36. Huang YL, Wu FZ, Wang YC, et al. Reliable categorisation of visual scoring of coronary artery calcification on low-dose CT for lung cancer screening: validation with the standard Agatston score. Eur Radiol. 2013;23(5):1226-1233. doi:10.1007/s00330-012-2726-5
37. Kim YK, Sung YM, Cho SH, Park YN, Choi HY. Reliability analysis of visual ranking of coronary artery calcification on low-dose CT of the thorax for lung cancer screening: comparison with ECG-gated calcium scoring CT. Int J Cardiovasc Imaging. 2014;30 Suppl 2:81-87. doi:10.1007/s10554-014-0507-8
38. Xia C, Vonder M, Pelgrim GJ, et al. High-pitch dual-source CT for coronary artery calcium scoring: A head-to-head comparison of non-triggered chest versus triggered cardiac acquisition. J Cardiovasc Comput Tomogr. 2021;15(1):65-72. doi:10.1016/j.jcct.2020.04.013
39. Hutt A, Duhamel A, Deken V, et al. Coronary calcium screening with dual-source CT: reliability of ungated, high-pitch chest CT in comparison with dedicated calcium-scoring CT. Eur Radiol. 2016;26(6):1521-1528. doi:10.1007/s00330-015-3978-7
40. Blaha MJ, Budoff MJ, Tota-Maharaj R, et al. Improving the CAC score by addition of regional measures of calcium distribution: Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging. 2016;9(12):1407-1416. doi:10.1016/j.jcmg.2016.03.001
1. Leigh A, McEvoy JW, Garg P, et al. Coronary artery calcium scores and atherosclerotic cardiovascular disease risk stratification in smokers. JACC Cardiovasc Imaging. 2019;12(5):852-861. doi:10.1016/j.jcmg.2017.12.017
2. Lu MT, Onuma OK, Massaro JM, D’Agostino RB Sr, O’Donnell CJ, Hoffmann U. Lung cancer screening eligibility in the community: cardiovascular risk factors, coronary artery calcification, and cardiovascular events. Circulation. 2016;134(12):897-899. doi:10.1161/CIRCULATIONAHA.116.023957
3. Tailor TD, Chiles C, Yeboah J, et al. Cardiovascular risk in the lung cancer screening population: a multicenter study evaluating the association between coronary artery calcification and preventive statin prescription. J Am Coll Radiol. 2021;18(9):1258-1266. doi:10.1016/j.jacr.2021.01.015
4. National Lung Screening Trial Research Team, Church TR, Black WC, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med. 2013;368(21):1980-1991. doi:10.1056/NEJMoa1209120
5. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322. doi:10.1161/CIR.0000000000000152
6. Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330-338. doi:10.7326/M13-2771
7. US Preventive Services Task Force, Krist AH, Davidson KW, et al. Screening for lung cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962-970. doi:10.1001/jama.2021.1117
8. Arcadi T, Maffei E, Sverzellati N, et al. Coronary artery calcium score on low-dose computed tomography for lung cancer screening. World J Radiol. 2014;6(6):381-387. doi:10.4329/wjr.v6.i6.381
9. Kim SM, Chung MJ, Lee KS, Choe YH, Yi CA, Choe BK. Coronary calcium screening using low-dose lung cancer screening: effectiveness of MDCT with retrospective reconstruction. AJR Am J Roentgenol. 2008;190(4):917-922. doi:10.2214/AJR.07.2979
10. Ruparel M, Quaife SL, Dickson JL, et al. Evaluation of cardiovascular risk in a lung cancer screening cohort. Thorax. 2019;74(12):1140-1146. doi:10.1136/thoraxjnl-2018-212812
11. Jacobs PC, Gondrie MJ, van der Graaf Y, et al. Coronary artery calcium can predict all-cause mortality and cardiovascular events on low-dose CT screening for lung cancer. AJR Am J Roentgenol. 2012;198(3):505-511. doi:10.2214/AJR.10.5577
12. Fan L, Fan K. Lung cancer screening CT-based coronary artery calcification in predicting cardiovascular events: A systematic review and meta-analysis. Medicine (Baltimore). 2018;97(20):e10461. doi:10.1097/MD.0000000000010461
13. Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary calcium score and cardiovascular risk. J Am Coll Cardiol. 2018;72(4):434-447. doi:10.1016/j.jacc.2018.05.027
14. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e563-e595. doi:10.1161/CIR.0000000000000677
15. Pletcher MJ, Pignone M, Earnshaw S, et al. Using the coronary artery calcium score to guide statin therapy: a cost-effectiveness analysis. Circ Cardiovasc Qual Outcomes. 2014;7(2):276-284. doi:10.1161/CIRCOUTCOMES.113.000799
16. Hong JC, Blankstein R, Shaw LJ, et al. Implications of coronary artery calcium testing for treatment decisions among statin candidates according to the ACC/AHA Cholesterol Management Guidelines: a cost-effectiveness analysis. JACC Cardiovasc Imaging. 2017;10(8):938-952. doi:10.1016/j.jcmg.2017.04.014
17. US Preventive Services Task Force, Curry SJ, Krist AH, et al. Risk assessment for cardiovascular disease with nontraditional risk factors: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320(3):272-280. doi:10.1001/jama.2018.8359
18. Hughes-Austin JM, Dominguez A 3rd, Allison MA, et al. Relationship of coronary calcium on standard chest CT scans with mortality. JACC Cardiovasc Imaging. 2016;9(2):152-159. doi:10.1016/j.jcmg.2015.06.030
19. Haller C, Vandehei A, Fisher R, et al. Incidence and implication of coronary artery calcium on non-gated chest computed tomography scans: a large observational cohort. Cureus. 2019;11(11):e6218. Published 2019 Nov 22. doi:10.7759/cureus.6218
20. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15(4):827-832. doi:10.1016/0735-1097(90)90282-t
21. Aberle D, Berg C, Black W, et al. The National Lung Screening Trial: overview and study design. Radiology. 2011;258(1):243-53. doi:10.1148/radiol.10091808
22. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135-160. doi:10.1177/096228029900800204
23. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc. 1999;74(3):243-252. doi:10.4065/74.3.243
24. Douthit NT, Wyatt N, Schwartz B. Clinical impact of reporting coronary artery calcium scores of non-gated chest computed tomography on statin management. Cureus. 2021;13(5):e14856. Published 2021 May 5. doi:10.7759/cureus.14856
25. Miedema MD, Dardari ZA, Kianoush S, et al. Statin eligibility, coronary artery calcium, and subsequent cardiovascular events according to the 2016 United States Preventive Services Task Force (USPSTF) Statin Guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Heart Assoc. 2018;7(12):e008920. Published 2018 Jun 13. doi:10.1161/JAHA.118.008920
26. Fisher R, Vandehei A, Haller C, et al. Reporting the presence of coronary artery calcium in the final impression of non-gated CT chest scans increases the appropriate utilization of statins. Cureus. 2020;12(9):e10579. Published 2020 Sep 21. doi:10.7759/cureus.10579
27. Blaha MJ, Budoff MJ, DeFilippis AP, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: implications for the JUPITER population from MESA, a population-based cohort study. Lancet. 2011;378(9792):684-692. doi:10.1016/S0140-6736(11)60784-8
28. Waheed S, Pollack S, Roth M, Reichek N, Guerci A, Cao JJ. Collective impact of conventional cardiovascular risk factors and coronary calcium score on clinical outcomes with or without statin therapy: the St Francis Heart Study. Atherosclerosis. 2016;255:193-199. doi:10.1016/j.atherosclerosis.2016.09.060
29. Mahabadi AA, Möhlenkamp S, Lehmann N, et al. CAC score improves coronary and CV risk assessment above statin indication by ESC and AHA/ACC Primary Prevention Guidelines. JACC Cardiovasc Imaging. 2017;10(2):143-153. doi:10.1016/j.jcmg.2016.03.022
30. Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849-858. doi:10.1161/CIRCULATIONAHA.115.018524
31. Hoffmann U, Massaro JM, D’Agostino RB Sr, Kathiresan S, Fox CS, O’Donnell CJ. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the Framingham Heart Study. J Am Heart Assoc. 2016;5(2):e003144. Published 2016 Feb 22. doi:10.1161/JAHA.115.003144
32. Williams KA Sr, Kim JT, Holohan KM. Frequency of unrecognized, unreported, or underreported coronary artery and cardiovascular calcification on noncardiac chest CT. J Cardiovasc Comput Tomogr. 2013;7(3):167-172. doi:10.1016/j.jcct.2013.05.003
33. Berrington de González A, Mahesh M, Kim KP, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071-2077. doi:10.1001/archinternmed.2009.440
34. Azour L, Kadoch MA, Ward TJ, Eber CD, Jacobi AH. Estimation of cardiovascular risk on routine chest CT: Ordinal coronary artery calcium scoring as an accurate predictor of Agatston score ranges. J Cardiovasc Comput Tomogr. 2017;11(1):8-15. doi:10.1016/j.jcct.2016.10.001
35. Waltz J, Kocher M, Kahn J, Dirr M, Burt JR. The future of concurrent automated coronary artery calcium scoring on screening low-dose computed tomography. Cureus. 2020;12(6):e8574. Published 2020 Jun 12. doi:10.7759/cureus.8574
36. Huang YL, Wu FZ, Wang YC, et al. Reliable categorisation of visual scoring of coronary artery calcification on low-dose CT for lung cancer screening: validation with the standard Agatston score. Eur Radiol. 2013;23(5):1226-1233. doi:10.1007/s00330-012-2726-5
37. Kim YK, Sung YM, Cho SH, Park YN, Choi HY. Reliability analysis of visual ranking of coronary artery calcification on low-dose CT of the thorax for lung cancer screening: comparison with ECG-gated calcium scoring CT. Int J Cardiovasc Imaging. 2014;30 Suppl 2:81-87. doi:10.1007/s10554-014-0507-8
38. Xia C, Vonder M, Pelgrim GJ, et al. High-pitch dual-source CT for coronary artery calcium scoring: A head-to-head comparison of non-triggered chest versus triggered cardiac acquisition. J Cardiovasc Comput Tomogr. 2021;15(1):65-72. doi:10.1016/j.jcct.2020.04.013
39. Hutt A, Duhamel A, Deken V, et al. Coronary calcium screening with dual-source CT: reliability of ungated, high-pitch chest CT in comparison with dedicated calcium-scoring CT. Eur Radiol. 2016;26(6):1521-1528. doi:10.1007/s00330-015-3978-7
40. Blaha MJ, Budoff MJ, Tota-Maharaj R, et al. Improving the CAC score by addition of regional measures of calcium distribution: Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging. 2016;9(12):1407-1416. doi:10.1016/j.jcmg.2016.03.001
Overall survival dips with vitamin D deficiency in melanoma
, according to research presented at the annual congress of the European Academy of Dermatology and Venereology.
Whereas the 5-year overall survival was 90% when vitamin D serum levels were above a 10 ng/mL threshold, it was 84% when levels fell below it. Notably, the gap in overall survival between those above and below the threshold appeared to widen as time went on.
The research adds to existing evidence that “vitamin D levels can play an important and independent role in patients’ survival outcomes,” study investigator Inés Gracia-Darder, MD, told this news organization. “The important application in clinical practice would be to know if vitamin D supplementation influences the survival of melanoma patients,” said Dr. Gracia-Darder, a clinical specialist in dermatology at the Hospital Universitari Son Espases, Mallorca, Spain.

Known association, but not much data
“It is not a new finding,” but there are limited data, especially in melanoma, said Julie De Smedt, MD, of KU Leuven, Belgium, who was asked to comment on the results. Other groups have shown, certainly for cancer in general, that vitamin D can have an effect on overall survival.
“Low levels of vitamin D are associated with the pathological parameters of the melanoma, such as the thickness of the tumor,” Dr. De Smedt said in an interview, indicating that it’s not just overall survival that might be affected.
“So we assume that also has an effect on melanoma-specific survival,” she added.
That assumption, however, is not supported by the data Dr. Gracia-Darder presented, as there was no difference in melanoma-specific survival among the two groups of patients that had been studied.
Retrospective cohort analysis
Vitamin D levels had been studied in 264 patients who were included in the retrospective cohort analysis. All had invasive melanomas, and all had been seen at the Hospital Clinic of Barcelona between January 1998 and June 2021. Their mean age was 57 years, and the median follow-up was 6.7 years.
For inclusion, all patients had to have had their vitamin D levels measured after being diagnosed with melanoma; those with a 25-hydroxyvitamin D3 serum level of less than 10 ng/mL were deemed to be vitamin D deficient, whereas those with levels of 10 ng/mL and above were deemed normal or insufficient.
A measurement less than 10 ng/mL is considered vitamin D deficiency, Dr. De Smedt said. “But there is a difference between countries, and there’s also a difference between societies,” noting the cut-off used in the lab where she works is 20 ng/mL. This makes it difficult to compare studies, she said.
Independent association with overall survival
Seasonal variation in vitamin D levels were considered as a possible confounding factor, but Dr. Gracia-Darder noted that there was a similar distribution of measurements taken between October to March and April to September.
Univariate and multivariate analyses established vitamin D deficiency as being independently associated with overall survival with hazard ratios of 2.34 and 2.45, respectively.
Other predictive factors were having a higher Breslow index, as well as older age and gender.
Time to recommend vitamin D supplementation?
So should patients with melanoma have their vitamin D levels routinely checked? And what about advising them to take vitamin D supplements?
“In our practice, we analyze the vitamin D levels of our patients,” Dr. Gracia-Darder said. Patients are told to limit their exposure to the sun because of their skin cancer, so they are very likely to become vitamin D deficient.
While dietary changes or supplements might be suggested, there’s no real evidence to support upping vitamin D levels to date, so “future prospective studies are needed,” Dr. Gracia-Darder added.
Such studies have already started, including one in Italy, one in Australia, and another study that Dr. De Smedt has been involved with for the past few years.
Called the ViDMe study, it’s a multicenter, randomized, double-blind trial in which patients are being given a high-dose oral vitamin D supplement or placebo once a month for at least 1 year. About 430 patients with a first cutaneous malignant melanoma have been included in the trial, which started in December 2012.
It is hoped that the results will show that the supplementation will have had a protective effect on the risk of relapse and that there will be a correlation between vitamin D levels in the blood and vitamin D receptor immunoreactivity in the tumor.
“The study is still blinded,” Dr. De Smedt said. “We will unblind in the coming months and then at the end of the year, maybe next year, we will have the results.”
The study reported by Dr. Gracia-Darder did not receive any specific funding. Dr. Gracia-Darder disclosed that the melanoma unit where the study was performed receives many grants and funds to carry out research. She reported no other relevant financial relationships. Dr. De Smedt had no relevant financial relationships. The ViDMe study is sponsored by the Universitaire Ziekenhuizen Leuven.
A version of this article first appeared on Medscape.com.
, according to research presented at the annual congress of the European Academy of Dermatology and Venereology.
Whereas the 5-year overall survival was 90% when vitamin D serum levels were above a 10 ng/mL threshold, it was 84% when levels fell below it. Notably, the gap in overall survival between those above and below the threshold appeared to widen as time went on.
The research adds to existing evidence that “vitamin D levels can play an important and independent role in patients’ survival outcomes,” study investigator Inés Gracia-Darder, MD, told this news organization. “The important application in clinical practice would be to know if vitamin D supplementation influences the survival of melanoma patients,” said Dr. Gracia-Darder, a clinical specialist in dermatology at the Hospital Universitari Son Espases, Mallorca, Spain.
Known association, but not much data
“It is not a new finding,” but there are limited data, especially in melanoma, said Julie De Smedt, MD, of KU Leuven, Belgium, who was asked to comment on the results. Other groups have shown, certainly for cancer in general, that vitamin D can have an effect on overall survival.
“Low levels of vitamin D are associated with the pathological parameters of the melanoma, such as the thickness of the tumor,” Dr. De Smedt said in an interview, indicating that it’s not just overall survival that might be affected.
“So we assume that also has an effect on melanoma-specific survival,” she added.
That assumption, however, is not supported by the data Dr. Gracia-Darder presented, as there was no difference in melanoma-specific survival among the two groups of patients that had been studied.
Retrospective cohort analysis
Vitamin D levels had been studied in 264 patients who were included in the retrospective cohort analysis. All had invasive melanomas, and all had been seen at the Hospital Clinic of Barcelona between January 1998 and June 2021. Their mean age was 57 years, and the median follow-up was 6.7 years.
For inclusion, all patients had to have had their vitamin D levels measured after being diagnosed with melanoma; those with a 25-hydroxyvitamin D3 serum level of less than 10 ng/mL were deemed to be vitamin D deficient, whereas those with levels of 10 ng/mL and above were deemed normal or insufficient.
A measurement less than 10 ng/mL is considered vitamin D deficiency, Dr. De Smedt said. “But there is a difference between countries, and there’s also a difference between societies,” noting the cut-off used in the lab where she works is 20 ng/mL. This makes it difficult to compare studies, she said.
Independent association with overall survival
Seasonal variation in vitamin D levels were considered as a possible confounding factor, but Dr. Gracia-Darder noted that there was a similar distribution of measurements taken between October to March and April to September.
Univariate and multivariate analyses established vitamin D deficiency as being independently associated with overall survival with hazard ratios of 2.34 and 2.45, respectively.
Other predictive factors were having a higher Breslow index, as well as older age and gender.
Time to recommend vitamin D supplementation?
So should patients with melanoma have their vitamin D levels routinely checked? And what about advising them to take vitamin D supplements?
“In our practice, we analyze the vitamin D levels of our patients,” Dr. Gracia-Darder said. Patients are told to limit their exposure to the sun because of their skin cancer, so they are very likely to become vitamin D deficient.
While dietary changes or supplements might be suggested, there’s no real evidence to support upping vitamin D levels to date, so “future prospective studies are needed,” Dr. Gracia-Darder added.
Such studies have already started, including one in Italy, one in Australia, and another study that Dr. De Smedt has been involved with for the past few years.
Called the ViDMe study, it’s a multicenter, randomized, double-blind trial in which patients are being given a high-dose oral vitamin D supplement or placebo once a month for at least 1 year. About 430 patients with a first cutaneous malignant melanoma have been included in the trial, which started in December 2012.
It is hoped that the results will show that the supplementation will have had a protective effect on the risk of relapse and that there will be a correlation between vitamin D levels in the blood and vitamin D receptor immunoreactivity in the tumor.
“The study is still blinded,” Dr. De Smedt said. “We will unblind in the coming months and then at the end of the year, maybe next year, we will have the results.”
The study reported by Dr. Gracia-Darder did not receive any specific funding. Dr. Gracia-Darder disclosed that the melanoma unit where the study was performed receives many grants and funds to carry out research. She reported no other relevant financial relationships. Dr. De Smedt had no relevant financial relationships. The ViDMe study is sponsored by the Universitaire Ziekenhuizen Leuven.
A version of this article first appeared on Medscape.com.
, according to research presented at the annual congress of the European Academy of Dermatology and Venereology.
Whereas the 5-year overall survival was 90% when vitamin D serum levels were above a 10 ng/mL threshold, it was 84% when levels fell below it. Notably, the gap in overall survival between those above and below the threshold appeared to widen as time went on.
The research adds to existing evidence that “vitamin D levels can play an important and independent role in patients’ survival outcomes,” study investigator Inés Gracia-Darder, MD, told this news organization. “The important application in clinical practice would be to know if vitamin D supplementation influences the survival of melanoma patients,” said Dr. Gracia-Darder, a clinical specialist in dermatology at the Hospital Universitari Son Espases, Mallorca, Spain.
Known association, but not much data
“It is not a new finding,” but there are limited data, especially in melanoma, said Julie De Smedt, MD, of KU Leuven, Belgium, who was asked to comment on the results. Other groups have shown, certainly for cancer in general, that vitamin D can have an effect on overall survival.
“Low levels of vitamin D are associated with the pathological parameters of the melanoma, such as the thickness of the tumor,” Dr. De Smedt said in an interview, indicating that it’s not just overall survival that might be affected.
“So we assume that also has an effect on melanoma-specific survival,” she added.
That assumption, however, is not supported by the data Dr. Gracia-Darder presented, as there was no difference in melanoma-specific survival among the two groups of patients that had been studied.
Retrospective cohort analysis
Vitamin D levels had been studied in 264 patients who were included in the retrospective cohort analysis. All had invasive melanomas, and all had been seen at the Hospital Clinic of Barcelona between January 1998 and June 2021. Their mean age was 57 years, and the median follow-up was 6.7 years.
For inclusion, all patients had to have had their vitamin D levels measured after being diagnosed with melanoma; those with a 25-hydroxyvitamin D3 serum level of less than 10 ng/mL were deemed to be vitamin D deficient, whereas those with levels of 10 ng/mL and above were deemed normal or insufficient.
A measurement less than 10 ng/mL is considered vitamin D deficiency, Dr. De Smedt said. “But there is a difference between countries, and there’s also a difference between societies,” noting the cut-off used in the lab where she works is 20 ng/mL. This makes it difficult to compare studies, she said.
Independent association with overall survival
Seasonal variation in vitamin D levels were considered as a possible confounding factor, but Dr. Gracia-Darder noted that there was a similar distribution of measurements taken between October to March and April to September.
Univariate and multivariate analyses established vitamin D deficiency as being independently associated with overall survival with hazard ratios of 2.34 and 2.45, respectively.
Other predictive factors were having a higher Breslow index, as well as older age and gender.
Time to recommend vitamin D supplementation?
So should patients with melanoma have their vitamin D levels routinely checked? And what about advising them to take vitamin D supplements?
“In our practice, we analyze the vitamin D levels of our patients,” Dr. Gracia-Darder said. Patients are told to limit their exposure to the sun because of their skin cancer, so they are very likely to become vitamin D deficient.
While dietary changes or supplements might be suggested, there’s no real evidence to support upping vitamin D levels to date, so “future prospective studies are needed,” Dr. Gracia-Darder added.
Such studies have already started, including one in Italy, one in Australia, and another study that Dr. De Smedt has been involved with for the past few years.
Called the ViDMe study, it’s a multicenter, randomized, double-blind trial in which patients are being given a high-dose oral vitamin D supplement or placebo once a month for at least 1 year. About 430 patients with a first cutaneous malignant melanoma have been included in the trial, which started in December 2012.
It is hoped that the results will show that the supplementation will have had a protective effect on the risk of relapse and that there will be a correlation between vitamin D levels in the blood and vitamin D receptor immunoreactivity in the tumor.
“The study is still blinded,” Dr. De Smedt said. “We will unblind in the coming months and then at the end of the year, maybe next year, we will have the results.”
The study reported by Dr. Gracia-Darder did not receive any specific funding. Dr. Gracia-Darder disclosed that the melanoma unit where the study was performed receives many grants and funds to carry out research. She reported no other relevant financial relationships. Dr. De Smedt had no relevant financial relationships. The ViDMe study is sponsored by the Universitaire Ziekenhuizen Leuven.
A version of this article first appeared on Medscape.com.
FROM THE EADV CONGRESS
Implementation of a Bone Marrow Biopsy Clinic: Effect on Wait Times for the Procedure, Diagnosis and Treatment Initiation
Clinical Situation
Bone marrow biopsies often need to be performed expeditiously in order to alleviate patient concerns and quickly determine a diagnosis and treatment plan. However, with increasing subspecialization there are fewer hematology/oncology providers available to perform this procedure.
Literature
Our VA previously addressed this issue by having all bone marrow biopsies performed through Interventional Radiology (IR). The average time from order to procedure, though, was 18.6 days (Arfons LM, AVAHO 2016).
Intervention
A weekly bone marrow biopsy clinic was formed, utilizing a small group (heme/onc physician, nurse practitioner and key nursing staff). In collaboration with pathology, interior design, pharmacy, facilities and environmental services, a standard operating procedure was developed, which included a staffing model, procedural checklist, documentation template, scheduling and ordering system.
Outcomes/Implications
Bone marrow biopsies performed before and after initiation of the bone marrow biopsy clinic were tracked for time from order placement to: procedure being done; diagnosis rendered; and for those whose biopsy result needed therapy, initiation of treatment. From 8/4/2020 to 8/12/2021 there were 140 bone marrow biopsies performed, all through IR. The average time from order to the procedure was 23.1 days; from order to diagnosis was 27.8 days and from order to treatment was 54.8 days. After implementation of the bone marrow biopsy clinic, from 9/8/2021 to 5/25/2022 there have been 61 bone marrow biopsies performed (those ordered through IR were excluded). The average time from order to the procedure was 6.8 days; from order to diagnosis was 11.4 days and from order to treatment was 27.3 days. The differences in the average wait times for all 3 measures (time to procedure, diagnosis and treatment) were highly statistically significant (P < .001 for each), in favor of shorter wait times for those performed in the bone marrow clinic as compared to those done through IR. Implementation of a dedicated weekly bone marrow biopsy clinic significantly reduced wait times for the procedure, diagnosis and treatment initiation. This should be considered at other VA centers to improve the care of our veterans.
Clinical Situation
Bone marrow biopsies often need to be performed expeditiously in order to alleviate patient concerns and quickly determine a diagnosis and treatment plan. However, with increasing subspecialization there are fewer hematology/oncology providers available to perform this procedure.
Literature
Our VA previously addressed this issue by having all bone marrow biopsies performed through Interventional Radiology (IR). The average time from order to procedure, though, was 18.6 days (Arfons LM, AVAHO 2016).
Intervention
A weekly bone marrow biopsy clinic was formed, utilizing a small group (heme/onc physician, nurse practitioner and key nursing staff). In collaboration with pathology, interior design, pharmacy, facilities and environmental services, a standard operating procedure was developed, which included a staffing model, procedural checklist, documentation template, scheduling and ordering system.
Outcomes/Implications
Bone marrow biopsies performed before and after initiation of the bone marrow biopsy clinic were tracked for time from order placement to: procedure being done; diagnosis rendered; and for those whose biopsy result needed therapy, initiation of treatment. From 8/4/2020 to 8/12/2021 there were 140 bone marrow biopsies performed, all through IR. The average time from order to the procedure was 23.1 days; from order to diagnosis was 27.8 days and from order to treatment was 54.8 days. After implementation of the bone marrow biopsy clinic, from 9/8/2021 to 5/25/2022 there have been 61 bone marrow biopsies performed (those ordered through IR were excluded). The average time from order to the procedure was 6.8 days; from order to diagnosis was 11.4 days and from order to treatment was 27.3 days. The differences in the average wait times for all 3 measures (time to procedure, diagnosis and treatment) were highly statistically significant (P < .001 for each), in favor of shorter wait times for those performed in the bone marrow clinic as compared to those done through IR. Implementation of a dedicated weekly bone marrow biopsy clinic significantly reduced wait times for the procedure, diagnosis and treatment initiation. This should be considered at other VA centers to improve the care of our veterans.
Clinical Situation
Bone marrow biopsies often need to be performed expeditiously in order to alleviate patient concerns and quickly determine a diagnosis and treatment plan. However, with increasing subspecialization there are fewer hematology/oncology providers available to perform this procedure.
Literature
Our VA previously addressed this issue by having all bone marrow biopsies performed through Interventional Radiology (IR). The average time from order to procedure, though, was 18.6 days (Arfons LM, AVAHO 2016).
Intervention
A weekly bone marrow biopsy clinic was formed, utilizing a small group (heme/onc physician, nurse practitioner and key nursing staff). In collaboration with pathology, interior design, pharmacy, facilities and environmental services, a standard operating procedure was developed, which included a staffing model, procedural checklist, documentation template, scheduling and ordering system.
Outcomes/Implications
Bone marrow biopsies performed before and after initiation of the bone marrow biopsy clinic were tracked for time from order placement to: procedure being done; diagnosis rendered; and for those whose biopsy result needed therapy, initiation of treatment. From 8/4/2020 to 8/12/2021 there were 140 bone marrow biopsies performed, all through IR. The average time from order to the procedure was 23.1 days; from order to diagnosis was 27.8 days and from order to treatment was 54.8 days. After implementation of the bone marrow biopsy clinic, from 9/8/2021 to 5/25/2022 there have been 61 bone marrow biopsies performed (those ordered through IR were excluded). The average time from order to the procedure was 6.8 days; from order to diagnosis was 11.4 days and from order to treatment was 27.3 days. The differences in the average wait times for all 3 measures (time to procedure, diagnosis and treatment) were highly statistically significant (P < .001 for each), in favor of shorter wait times for those performed in the bone marrow clinic as compared to those done through IR. Implementation of a dedicated weekly bone marrow biopsy clinic significantly reduced wait times for the procedure, diagnosis and treatment initiation. This should be considered at other VA centers to improve the care of our veterans.
NP-Led Suspicion of Cancer Clinic Improves Timeliness of Care for Veterans
Clinical Situation
Delays in diagnosis affect outcomes in veterans with cancer. Veterans sent into the community for suspected cancer frequently experience delays in diagnosis and treatment. This is further complicated by inappropriate workup, resulting in additional delays. Retaining veterans within the VA system for care and providing guidance to primary care providers (PCPs) to assist with expedited workup was an identified need. The Suspicion of Cancer Clinic (SOCC) was developed to address barriers to timely cancer diagnosis and care.
Literature
Researched private sector models of rapid cancer diagnostic and suspicion clinics. Literature analyzed showed improved outcomes through reduction of diagnostic delay. Nurse practitioner (NP)-led clinics were determined to be effective in expediting diagnosis and reducing cancer care delays.
Intervention
The Suspicion of Cancer Clinic is a tele-clinic, staffed with a NP. Diagnostic consult for the NP to assume the workup upon discovery of high suspicion of cancer, or via non-visit consult (NVC) to provide diagnostic guidance are available to PCPs. Outreach and education were performed prior initial clinic launch and post-launch, when need for further clarification of role and scope of the clinic was identified, based on consult trends.
Outcomes/Implications
The SOCC received 133 consults between 9/1/2021 and 6/6/2022 for veterans ranging age 29-94 years. Of these consults, 25 were expedited, diagnostic workups, 47 were NVCs, eliminating unnecessary or incomplete workups, yielding 23 veterans diagnosed with one of 8 types cancer. An additional 34 consults were forwarded to other appropriate service, and 27 were not appropriate for clinic and cancelled. Further outreach and education resulted in a 55% decrease in inappropriate consults. The NP retained 10 veterans (50%) within the VA for diagnostics, who had planned to receive community workup, which is an average four-week delay to schedule in the community. The SOCC was developed utilizing existing staff. The tele-clinic relieves workspace burden. Veterans received timely and appropriate cancer workups, reducing diagnostic delays. PCPs received additional support and guidance. Veterans retained within the VA system is more cost-effective and avoids community care delays. NP-led suspicion/rapid diagnostic clinic effectively reduced care delays by immediate initiation of further diagnostics and appropriate utilization of resources.
References
Campbell C, Nowell A, Karagheusian K, Giroux J, Kiteley C, Martelli L, McQuestion M, Quinn M, Rowe Samadhin YP, Touw M, Moody L. Practical innovation: Advanced practice nurses in cancer care. Can Oncol Nurs J. 2020 Jan 1;30(1):9-15. doi:10.5737/23688076301915. PMID: 33119001; PMCID: PMC7585714.
Drudge-Coates L, Khati V, Ballesteros R, Martyn-Hemphill C, Brown C, Green J, Challacombe B, Muir G. A nurse practitioner model for the assessment of suspected prostate cancer referrals is safe, cost and time efficient. Ecancermedicalscience. 2019 Dec 18;13:994. doi:10.3332/ecancer.2019.994. PMID: 32010218; PMCID: PMC6974368.
Nixon S, Bezverbnaya K, Maganti M, Gullane P, Reedijk M, Kuruvilla J, Prica A, Kridel R, Kukreti V, Bennett S, Rogalla P, Delabie J, Pintilie M, Crump M. Evaluation of Lymphadenopathy and Suspected Lymphoma in a Lymphoma Rapid Diagnosis Clinic. JCO Oncol Pract. 2020 Jan;16(1):e29-e36. doi:10.1200/JOP.19.00202. Epub 2019 Oct 1. PMID: 31573831.
Vasilakis C, Forte P. Setting up a rapid diagnostic clinic for patients with vague symptoms of cancer: a mixed method process evaluation study. BMC Health Serv Res. 2021 Apr 17;21(1):357. doi: 10.1186/s12913-021-06360-0. PMID: 33865373; PMCID: PMC8052708.
Clinical Situation
Delays in diagnosis affect outcomes in veterans with cancer. Veterans sent into the community for suspected cancer frequently experience delays in diagnosis and treatment. This is further complicated by inappropriate workup, resulting in additional delays. Retaining veterans within the VA system for care and providing guidance to primary care providers (PCPs) to assist with expedited workup was an identified need. The Suspicion of Cancer Clinic (SOCC) was developed to address barriers to timely cancer diagnosis and care.
Literature
Researched private sector models of rapid cancer diagnostic and suspicion clinics. Literature analyzed showed improved outcomes through reduction of diagnostic delay. Nurse practitioner (NP)-led clinics were determined to be effective in expediting diagnosis and reducing cancer care delays.
Intervention
The Suspicion of Cancer Clinic is a tele-clinic, staffed with a NP. Diagnostic consult for the NP to assume the workup upon discovery of high suspicion of cancer, or via non-visit consult (NVC) to provide diagnostic guidance are available to PCPs. Outreach and education were performed prior initial clinic launch and post-launch, when need for further clarification of role and scope of the clinic was identified, based on consult trends.
Outcomes/Implications
The SOCC received 133 consults between 9/1/2021 and 6/6/2022 for veterans ranging age 29-94 years. Of these consults, 25 were expedited, diagnostic workups, 47 were NVCs, eliminating unnecessary or incomplete workups, yielding 23 veterans diagnosed with one of 8 types cancer. An additional 34 consults were forwarded to other appropriate service, and 27 were not appropriate for clinic and cancelled. Further outreach and education resulted in a 55% decrease in inappropriate consults. The NP retained 10 veterans (50%) within the VA for diagnostics, who had planned to receive community workup, which is an average four-week delay to schedule in the community. The SOCC was developed utilizing existing staff. The tele-clinic relieves workspace burden. Veterans received timely and appropriate cancer workups, reducing diagnostic delays. PCPs received additional support and guidance. Veterans retained within the VA system is more cost-effective and avoids community care delays. NP-led suspicion/rapid diagnostic clinic effectively reduced care delays by immediate initiation of further diagnostics and appropriate utilization of resources.
References
Campbell C, Nowell A, Karagheusian K, Giroux J, Kiteley C, Martelli L, McQuestion M, Quinn M, Rowe Samadhin YP, Touw M, Moody L. Practical innovation: Advanced practice nurses in cancer care. Can Oncol Nurs J. 2020 Jan 1;30(1):9-15. doi:10.5737/23688076301915. PMID: 33119001; PMCID: PMC7585714.
Drudge-Coates L, Khati V, Ballesteros R, Martyn-Hemphill C, Brown C, Green J, Challacombe B, Muir G. A nurse practitioner model for the assessment of suspected prostate cancer referrals is safe, cost and time efficient. Ecancermedicalscience. 2019 Dec 18;13:994. doi:10.3332/ecancer.2019.994. PMID: 32010218; PMCID: PMC6974368.
Nixon S, Bezverbnaya K, Maganti M, Gullane P, Reedijk M, Kuruvilla J, Prica A, Kridel R, Kukreti V, Bennett S, Rogalla P, Delabie J, Pintilie M, Crump M. Evaluation of Lymphadenopathy and Suspected Lymphoma in a Lymphoma Rapid Diagnosis Clinic. JCO Oncol Pract. 2020 Jan;16(1):e29-e36. doi:10.1200/JOP.19.00202. Epub 2019 Oct 1. PMID: 31573831.
Vasilakis C, Forte P. Setting up a rapid diagnostic clinic for patients with vague symptoms of cancer: a mixed method process evaluation study. BMC Health Serv Res. 2021 Apr 17;21(1):357. doi: 10.1186/s12913-021-06360-0. PMID: 33865373; PMCID: PMC8052708.
Clinical Situation
Delays in diagnosis affect outcomes in veterans with cancer. Veterans sent into the community for suspected cancer frequently experience delays in diagnosis and treatment. This is further complicated by inappropriate workup, resulting in additional delays. Retaining veterans within the VA system for care and providing guidance to primary care providers (PCPs) to assist with expedited workup was an identified need. The Suspicion of Cancer Clinic (SOCC) was developed to address barriers to timely cancer diagnosis and care.
Literature
Researched private sector models of rapid cancer diagnostic and suspicion clinics. Literature analyzed showed improved outcomes through reduction of diagnostic delay. Nurse practitioner (NP)-led clinics were determined to be effective in expediting diagnosis and reducing cancer care delays.
Intervention
The Suspicion of Cancer Clinic is a tele-clinic, staffed with a NP. Diagnostic consult for the NP to assume the workup upon discovery of high suspicion of cancer, or via non-visit consult (NVC) to provide diagnostic guidance are available to PCPs. Outreach and education were performed prior initial clinic launch and post-launch, when need for further clarification of role and scope of the clinic was identified, based on consult trends.
Outcomes/Implications
The SOCC received 133 consults between 9/1/2021 and 6/6/2022 for veterans ranging age 29-94 years. Of these consults, 25 were expedited, diagnostic workups, 47 were NVCs, eliminating unnecessary or incomplete workups, yielding 23 veterans diagnosed with one of 8 types cancer. An additional 34 consults were forwarded to other appropriate service, and 27 were not appropriate for clinic and cancelled. Further outreach and education resulted in a 55% decrease in inappropriate consults. The NP retained 10 veterans (50%) within the VA for diagnostics, who had planned to receive community workup, which is an average four-week delay to schedule in the community. The SOCC was developed utilizing existing staff. The tele-clinic relieves workspace burden. Veterans received timely and appropriate cancer workups, reducing diagnostic delays. PCPs received additional support and guidance. Veterans retained within the VA system is more cost-effective and avoids community care delays. NP-led suspicion/rapid diagnostic clinic effectively reduced care delays by immediate initiation of further diagnostics and appropriate utilization of resources.
References
Campbell C, Nowell A, Karagheusian K, Giroux J, Kiteley C, Martelli L, McQuestion M, Quinn M, Rowe Samadhin YP, Touw M, Moody L. Practical innovation: Advanced practice nurses in cancer care. Can Oncol Nurs J. 2020 Jan 1;30(1):9-15. doi:10.5737/23688076301915. PMID: 33119001; PMCID: PMC7585714.
Drudge-Coates L, Khati V, Ballesteros R, Martyn-Hemphill C, Brown C, Green J, Challacombe B, Muir G. A nurse practitioner model for the assessment of suspected prostate cancer referrals is safe, cost and time efficient. Ecancermedicalscience. 2019 Dec 18;13:994. doi:10.3332/ecancer.2019.994. PMID: 32010218; PMCID: PMC6974368.
Nixon S, Bezverbnaya K, Maganti M, Gullane P, Reedijk M, Kuruvilla J, Prica A, Kridel R, Kukreti V, Bennett S, Rogalla P, Delabie J, Pintilie M, Crump M. Evaluation of Lymphadenopathy and Suspected Lymphoma in a Lymphoma Rapid Diagnosis Clinic. JCO Oncol Pract. 2020 Jan;16(1):e29-e36. doi:10.1200/JOP.19.00202. Epub 2019 Oct 1. PMID: 31573831.
Vasilakis C, Forte P. Setting up a rapid diagnostic clinic for patients with vague symptoms of cancer: a mixed method process evaluation study. BMC Health Serv Res. 2021 Apr 17;21(1):357. doi: 10.1186/s12913-021-06360-0. PMID: 33865373; PMCID: PMC8052708.
An Open-Label Feasibility and Acceptability Pilot of Hypnosis and Mindfulness Meditation for Cancer Pain in Veterans
Purpose
This was an open label trial to determine feasibility and acceptability of 2 complementary and integrative interventions (self-hypnosis [HYP] and mindfulness meditation [MM]) for pain in veterans undergoing treatment for head and neck cancer (HNC) at VA Puget Sound.
Background
HNC is associated with pain prior to and during treatment. HYP and MM have shown promise for procedural, acute, and chronic pain and may be a helpful addition to cancer treatment.
Methods
All veterans initiating treatment during the study window (2018-2020) were offered study treatment in addition to usual care. After providing informed consent and hearing a brief description of the interventions, participants selected either the HYP or MM intervention or a control condition (ie, complete assessments but no intervention). Participants met with a study clinician who introduced the intervention and provided audio recordings and a workbook and instructed them to listen to the recordings as often as they deemed helpful. Participants completed survey assessments at baseline, week 4, and at study completion (8 weeks). Measures included patient-reported satisfaction and perceived treatment helpfulness, frequency of practice, and likeliness of using skills going forward.
Data Analysis
Descriptive statistics were computed for all measures collected. No statistical tests were conducted due to small sample size.
Results
Of the 15 veterans who enrolled, 7 selected HYP, 7 selected MM, none selected the control condition, and 1 withdrew prior to treatment selection. Of the 14 completers, 79% reported that their chosen treatment was helpful and that they practiced at least once a week; 71% reported that they are likely to use these skills going forward. No adverse events were reported.
Conclusions/Implications
Self-guided HYP and MM interventions can be administered feasibly and are highly acceptable to veterans undergoing HNC treatment in a VA setting. HYP or MM interventions are feasible to implement with little demand on resources, and that listening to recordings is acceptable and helpful for veterans with pain related to cancer and cancer treatment. Further research is warranted to formally evaluate the efficacy of these interventions in this population in a well-powered study.
Purpose
This was an open label trial to determine feasibility and acceptability of 2 complementary and integrative interventions (self-hypnosis [HYP] and mindfulness meditation [MM]) for pain in veterans undergoing treatment for head and neck cancer (HNC) at VA Puget Sound.
Background
HNC is associated with pain prior to and during treatment. HYP and MM have shown promise for procedural, acute, and chronic pain and may be a helpful addition to cancer treatment.
Methods
All veterans initiating treatment during the study window (2018-2020) were offered study treatment in addition to usual care. After providing informed consent and hearing a brief description of the interventions, participants selected either the HYP or MM intervention or a control condition (ie, complete assessments but no intervention). Participants met with a study clinician who introduced the intervention and provided audio recordings and a workbook and instructed them to listen to the recordings as often as they deemed helpful. Participants completed survey assessments at baseline, week 4, and at study completion (8 weeks). Measures included patient-reported satisfaction and perceived treatment helpfulness, frequency of practice, and likeliness of using skills going forward.
Data Analysis
Descriptive statistics were computed for all measures collected. No statistical tests were conducted due to small sample size.
Results
Of the 15 veterans who enrolled, 7 selected HYP, 7 selected MM, none selected the control condition, and 1 withdrew prior to treatment selection. Of the 14 completers, 79% reported that their chosen treatment was helpful and that they practiced at least once a week; 71% reported that they are likely to use these skills going forward. No adverse events were reported.
Conclusions/Implications
Self-guided HYP and MM interventions can be administered feasibly and are highly acceptable to veterans undergoing HNC treatment in a VA setting. HYP or MM interventions are feasible to implement with little demand on resources, and that listening to recordings is acceptable and helpful for veterans with pain related to cancer and cancer treatment. Further research is warranted to formally evaluate the efficacy of these interventions in this population in a well-powered study.
Purpose
This was an open label trial to determine feasibility and acceptability of 2 complementary and integrative interventions (self-hypnosis [HYP] and mindfulness meditation [MM]) for pain in veterans undergoing treatment for head and neck cancer (HNC) at VA Puget Sound.
Background
HNC is associated with pain prior to and during treatment. HYP and MM have shown promise for procedural, acute, and chronic pain and may be a helpful addition to cancer treatment.
Methods
All veterans initiating treatment during the study window (2018-2020) were offered study treatment in addition to usual care. After providing informed consent and hearing a brief description of the interventions, participants selected either the HYP or MM intervention or a control condition (ie, complete assessments but no intervention). Participants met with a study clinician who introduced the intervention and provided audio recordings and a workbook and instructed them to listen to the recordings as often as they deemed helpful. Participants completed survey assessments at baseline, week 4, and at study completion (8 weeks). Measures included patient-reported satisfaction and perceived treatment helpfulness, frequency of practice, and likeliness of using skills going forward.
Data Analysis
Descriptive statistics were computed for all measures collected. No statistical tests were conducted due to small sample size.
Results
Of the 15 veterans who enrolled, 7 selected HYP, 7 selected MM, none selected the control condition, and 1 withdrew prior to treatment selection. Of the 14 completers, 79% reported that their chosen treatment was helpful and that they practiced at least once a week; 71% reported that they are likely to use these skills going forward. No adverse events were reported.
Conclusions/Implications
Self-guided HYP and MM interventions can be administered feasibly and are highly acceptable to veterans undergoing HNC treatment in a VA setting. HYP or MM interventions are feasible to implement with little demand on resources, and that listening to recordings is acceptable and helpful for veterans with pain related to cancer and cancer treatment. Further research is warranted to formally evaluate the efficacy of these interventions in this population in a well-powered study.
The Use of Aromatherapy as a Complementary Alternative Medicine in the Management of Cancer-Related Pain
Purpose
To identify the effectiveness of aromatherapy as an adjunct in improving pain and overall sense of well-being among patients with cancer receiving hospice care.
Background
There is limited data available on the use of aromatherapy for pain management among patients with cancer receiving end-of-life care. This project identifies the benefits of aromatherapy in a population where it was not previously evaluated.
Methods
Patients with cancer who were admitted to the hospice unit of a local hospital within a large healthcare system for at least 24 hours and taking opioids for neoplasm related pain at least once a day were included in the study. Patients with allergy to essential oils, and those suffering from allergic rhinitis and common cold, and a history of asthma were excluded. Patients who were unable to consent for study participation were also excluded.
Data Analysis
Retrospective chart analysis and surveys were used to collect the data. Univariate descriptive statistics were used for patient characteristics. A Wilcoxon Signed Rank Test was used to determine opioid use before and after aromatherapy. The t test was used to compare pain scores before and after aromatherapy. A 5-point Likert scale was used to evaluate how soothing the participants found the treatment to be. The Numeric Pain Intensity Scale was used for pain scores.
Results
There was a total of 40 participants, all of whom were male with an average age of 69 years. Pain scores before and after treatment were found to be statistically significant at an average of 5.15/10 vs 3.68/10, respectively. On a scale from 1-5 with 5 being the most soothing, there was an average rating of 3.87 among participants. There was not a statistically significant decline in opioid use from pre-treatment to post-treatment. Higher pain scores before intervention were associated with rating the lotion as more soothing.
Conclusions
The use of aromatherapy as a complement to opioids for cancer-related pain in the end-of-life was associated with an increase sense of well-being, resulted in lower pain scores and seems to have subjective comfort merit.
Implications
This study shows the potential benefits of using aromatherapy in end-of-life care among patients with cancer.
Purpose
To identify the effectiveness of aromatherapy as an adjunct in improving pain and overall sense of well-being among patients with cancer receiving hospice care.
Background
There is limited data available on the use of aromatherapy for pain management among patients with cancer receiving end-of-life care. This project identifies the benefits of aromatherapy in a population where it was not previously evaluated.
Methods
Patients with cancer who were admitted to the hospice unit of a local hospital within a large healthcare system for at least 24 hours and taking opioids for neoplasm related pain at least once a day were included in the study. Patients with allergy to essential oils, and those suffering from allergic rhinitis and common cold, and a history of asthma were excluded. Patients who were unable to consent for study participation were also excluded.
Data Analysis
Retrospective chart analysis and surveys were used to collect the data. Univariate descriptive statistics were used for patient characteristics. A Wilcoxon Signed Rank Test was used to determine opioid use before and after aromatherapy. The t test was used to compare pain scores before and after aromatherapy. A 5-point Likert scale was used to evaluate how soothing the participants found the treatment to be. The Numeric Pain Intensity Scale was used for pain scores.
Results
There was a total of 40 participants, all of whom were male with an average age of 69 years. Pain scores before and after treatment were found to be statistically significant at an average of 5.15/10 vs 3.68/10, respectively. On a scale from 1-5 with 5 being the most soothing, there was an average rating of 3.87 among participants. There was not a statistically significant decline in opioid use from pre-treatment to post-treatment. Higher pain scores before intervention were associated with rating the lotion as more soothing.
Conclusions
The use of aromatherapy as a complement to opioids for cancer-related pain in the end-of-life was associated with an increase sense of well-being, resulted in lower pain scores and seems to have subjective comfort merit.
Implications
This study shows the potential benefits of using aromatherapy in end-of-life care among patients with cancer.
Purpose
To identify the effectiveness of aromatherapy as an adjunct in improving pain and overall sense of well-being among patients with cancer receiving hospice care.
Background
There is limited data available on the use of aromatherapy for pain management among patients with cancer receiving end-of-life care. This project identifies the benefits of aromatherapy in a population where it was not previously evaluated.
Methods
Patients with cancer who were admitted to the hospice unit of a local hospital within a large healthcare system for at least 24 hours and taking opioids for neoplasm related pain at least once a day were included in the study. Patients with allergy to essential oils, and those suffering from allergic rhinitis and common cold, and a history of asthma were excluded. Patients who were unable to consent for study participation were also excluded.
Data Analysis
Retrospective chart analysis and surveys were used to collect the data. Univariate descriptive statistics were used for patient characteristics. A Wilcoxon Signed Rank Test was used to determine opioid use before and after aromatherapy. The t test was used to compare pain scores before and after aromatherapy. A 5-point Likert scale was used to evaluate how soothing the participants found the treatment to be. The Numeric Pain Intensity Scale was used for pain scores.
Results
There was a total of 40 participants, all of whom were male with an average age of 69 years. Pain scores before and after treatment were found to be statistically significant at an average of 5.15/10 vs 3.68/10, respectively. On a scale from 1-5 with 5 being the most soothing, there was an average rating of 3.87 among participants. There was not a statistically significant decline in opioid use from pre-treatment to post-treatment. Higher pain scores before intervention were associated with rating the lotion as more soothing.
Conclusions
The use of aromatherapy as a complement to opioids for cancer-related pain in the end-of-life was associated with an increase sense of well-being, resulted in lower pain scores and seems to have subjective comfort merit.
Implications
This study shows the potential benefits of using aromatherapy in end-of-life care among patients with cancer.
Palliative Care Disparities in Small Cell Carcinoma of the Prostate: An Analysis of the National Cancer Database
Purpose
This study addresses a gap in knowledge regarding palliative care utilization patterns in smallcell carcinoma of the prostate.
Background
Prostate cancer is the most common cancer affecting males. One of the most aggressive malignancies of the prostate is small cell carcinoma (SCC) of the prostate. Almost 70% of patients diagnosed with SCC present with the disseminated disease with a low 5-year survival rate of less than 2%. The role of palliative care can be beneficial in metastatic prostate cancer given its largely incurable course. Despite evidence favoring palliative care for prostate cancer in several patient populations, it remains under-utilized. Palliative care utilization patterns in SCC of the prostate have not yet been studied.
Methods
This is a retrospective study of patients diagnosed with all subtypes of AJCC staged metastatic SCC of the prostate between 2004 and 2017 in the National Cancer Database (NCDB) to determine palliative care usage (n = 615). Exclusion criteria included missing data.
Data Analysis
Variables were evaluated for significance (P < .05) in relation to the receipt of palliative care using Pearson Chi-Square, ANOVA, and Kaplan- Meier tests. Multivariate analysis was performed via binary logistics regression.
Results
Among the 961 patients diagnosed with SCC of the prostate, 64% had metastatic disease (n = 615). The metastatic cohort was more likely to receive palliative care than those that did not have distant metastasis (24.2% vs 5.7%, P < .001). Palliative care use has grown between 2004 (n = 6) and 2017 (n = 20). Patients that were uninsured were more likely than insured patients to receive palliative care (50% vs 23.5%, P = .003; 95% CI, 0.051- 0.546). Non-Hispanic patients were also more likely than Hispanic patients to receive palliative care (P = .033; 95% CI, 1.154-28.140). New England locations had the highest utilization of palliative care (43.%, P = .009). Factors that impacted palliative care use included facility region, insurance status, and Hispanic status. As palliative care continues to be utilized more frequently, we hope that this study can provide a starting point in studying and preventing palliative treatment disparities.
Purpose
This study addresses a gap in knowledge regarding palliative care utilization patterns in smallcell carcinoma of the prostate.
Background
Prostate cancer is the most common cancer affecting males. One of the most aggressive malignancies of the prostate is small cell carcinoma (SCC) of the prostate. Almost 70% of patients diagnosed with SCC present with the disseminated disease with a low 5-year survival rate of less than 2%. The role of palliative care can be beneficial in metastatic prostate cancer given its largely incurable course. Despite evidence favoring palliative care for prostate cancer in several patient populations, it remains under-utilized. Palliative care utilization patterns in SCC of the prostate have not yet been studied.
Methods
This is a retrospective study of patients diagnosed with all subtypes of AJCC staged metastatic SCC of the prostate between 2004 and 2017 in the National Cancer Database (NCDB) to determine palliative care usage (n = 615). Exclusion criteria included missing data.
Data Analysis
Variables were evaluated for significance (P < .05) in relation to the receipt of palliative care using Pearson Chi-Square, ANOVA, and Kaplan- Meier tests. Multivariate analysis was performed via binary logistics regression.
Results
Among the 961 patients diagnosed with SCC of the prostate, 64% had metastatic disease (n = 615). The metastatic cohort was more likely to receive palliative care than those that did not have distant metastasis (24.2% vs 5.7%, P < .001). Palliative care use has grown between 2004 (n = 6) and 2017 (n = 20). Patients that were uninsured were more likely than insured patients to receive palliative care (50% vs 23.5%, P = .003; 95% CI, 0.051- 0.546). Non-Hispanic patients were also more likely than Hispanic patients to receive palliative care (P = .033; 95% CI, 1.154-28.140). New England locations had the highest utilization of palliative care (43.%, P = .009). Factors that impacted palliative care use included facility region, insurance status, and Hispanic status. As palliative care continues to be utilized more frequently, we hope that this study can provide a starting point in studying and preventing palliative treatment disparities.
Purpose
This study addresses a gap in knowledge regarding palliative care utilization patterns in smallcell carcinoma of the prostate.
Background
Prostate cancer is the most common cancer affecting males. One of the most aggressive malignancies of the prostate is small cell carcinoma (SCC) of the prostate. Almost 70% of patients diagnosed with SCC present with the disseminated disease with a low 5-year survival rate of less than 2%. The role of palliative care can be beneficial in metastatic prostate cancer given its largely incurable course. Despite evidence favoring palliative care for prostate cancer in several patient populations, it remains under-utilized. Palliative care utilization patterns in SCC of the prostate have not yet been studied.
Methods
This is a retrospective study of patients diagnosed with all subtypes of AJCC staged metastatic SCC of the prostate between 2004 and 2017 in the National Cancer Database (NCDB) to determine palliative care usage (n = 615). Exclusion criteria included missing data.
Data Analysis
Variables were evaluated for significance (P < .05) in relation to the receipt of palliative care using Pearson Chi-Square, ANOVA, and Kaplan- Meier tests. Multivariate analysis was performed via binary logistics regression.
Results
Among the 961 patients diagnosed with SCC of the prostate, 64% had metastatic disease (n = 615). The metastatic cohort was more likely to receive palliative care than those that did not have distant metastasis (24.2% vs 5.7%, P < .001). Palliative care use has grown between 2004 (n = 6) and 2017 (n = 20). Patients that were uninsured were more likely than insured patients to receive palliative care (50% vs 23.5%, P = .003; 95% CI, 0.051- 0.546). Non-Hispanic patients were also more likely than Hispanic patients to receive palliative care (P = .033; 95% CI, 1.154-28.140). New England locations had the highest utilization of palliative care (43.%, P = .009). Factors that impacted palliative care use included facility region, insurance status, and Hispanic status. As palliative care continues to be utilized more frequently, we hope that this study can provide a starting point in studying and preventing palliative treatment disparities.