User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Hypocalcemia Risk Warning Added to Osteoporosis Drug
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
Why Don’t Physicians Call In Sick?
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.

Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.
Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.
Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Testosterone Replacement May Cause ... Fracture?
This transcript has been edited for clarity.
I am showing you a graph without any labels.
What could this line represent? The stock price of some company that made a big splash but failed to live up to expectations? An outbreak curve charting the introduction of a new infectious agent to a population? The performance of a viral tweet?
I’ll tell you what it is in a moment, but I wanted you to recognize that there is something inherently wistful in this shape, something that speaks of past glory and inevitable declines. It’s a graph that induces a feeling of resistance — no, do not go gently into that good night.
The graph actually represents (roughly) the normal level of serum testosterone in otherwise-healthy men as they age.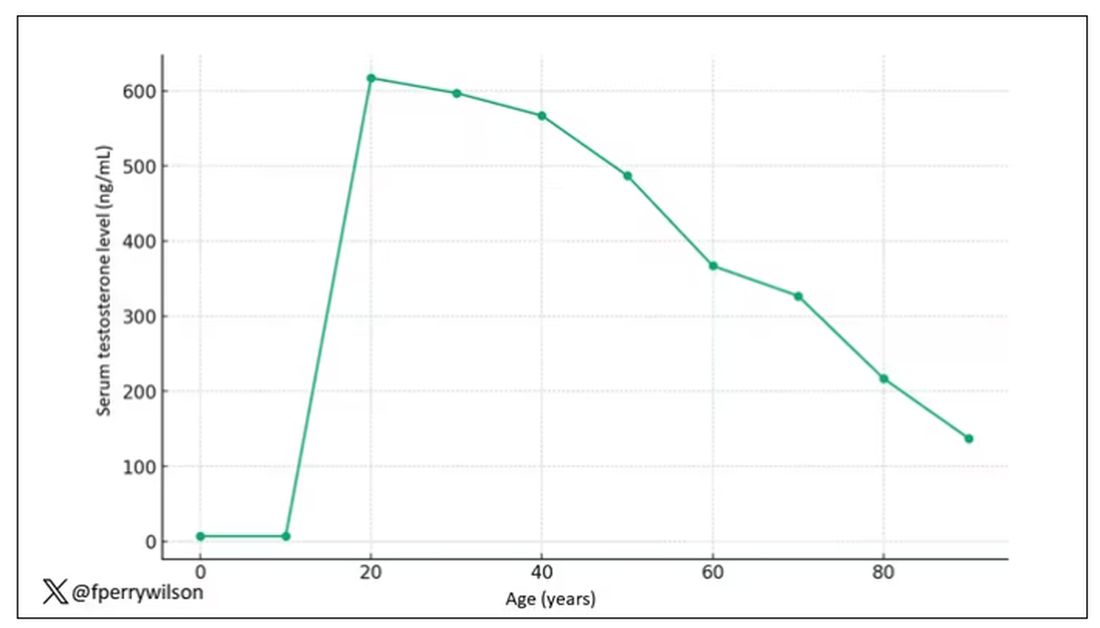
A caveat here: These numbers are not as well defined as I made them seem on this graph, particularly for those older than 65 years. But it is clear that testosterone levels decline with time, and the idea to supplement testosterone is hardly new. Like all treatments, testosterone supplementation has risks and benefits. Some risks are predictable, like exacerbating the symptoms of benign prostatic hyperplasia. Some risks seem to come completely out of left field. That’s what we have today, in a study suggesting that testosterone supplementation increases the risk for bone fractures.
Let me set the stage here by saying that nearly all prior research into the effects of testosterone supplementation has suggested that it is pretty good for bone health. It increases bone mineral density, bone strength, and improves bone architecture.
So if you were to do a randomized trial of testosterone supplementation and look at fracture risk in the testosterone group compared with the placebo group, you would expect the fracture risk would be much lower in those getting supplemented. Of course, this is why we actually do studies instead of assuming we know the answer already — because in this case, you’d be wrong.
I’m talking about this study, appearing in The New England Journal of Medicine.
It’s a prespecified secondary analysis of a randomized trial known as the TRAVERSE trial, which randomly assigned 5246 men with low testosterone levels to transdermal testosterone gel vs placebo. The primary goal of that trial was to assess the cardiovascular risk associated with testosterone supplementation, and the major take-home was that there was no difference in cardiovascular event rates between the testosterone and placebo groups.
This secondary analysis looked at fracture incidence. Researchers contacted participants multiple times in the first year of the study and yearly thereafter. Each time, they asked whether the participant had sustained a fracture. If they answered in the affirmative, a request for medical records was made and the researchers, still blinded to randomization status, adjudicated whether there was indeed a fracture or not, along with some details as to location, situation, and so on.
This was a big study, though, and that translates to just a 3.5% fracture rate in testosterone vs 2.5% in control, but the difference was statistically significant.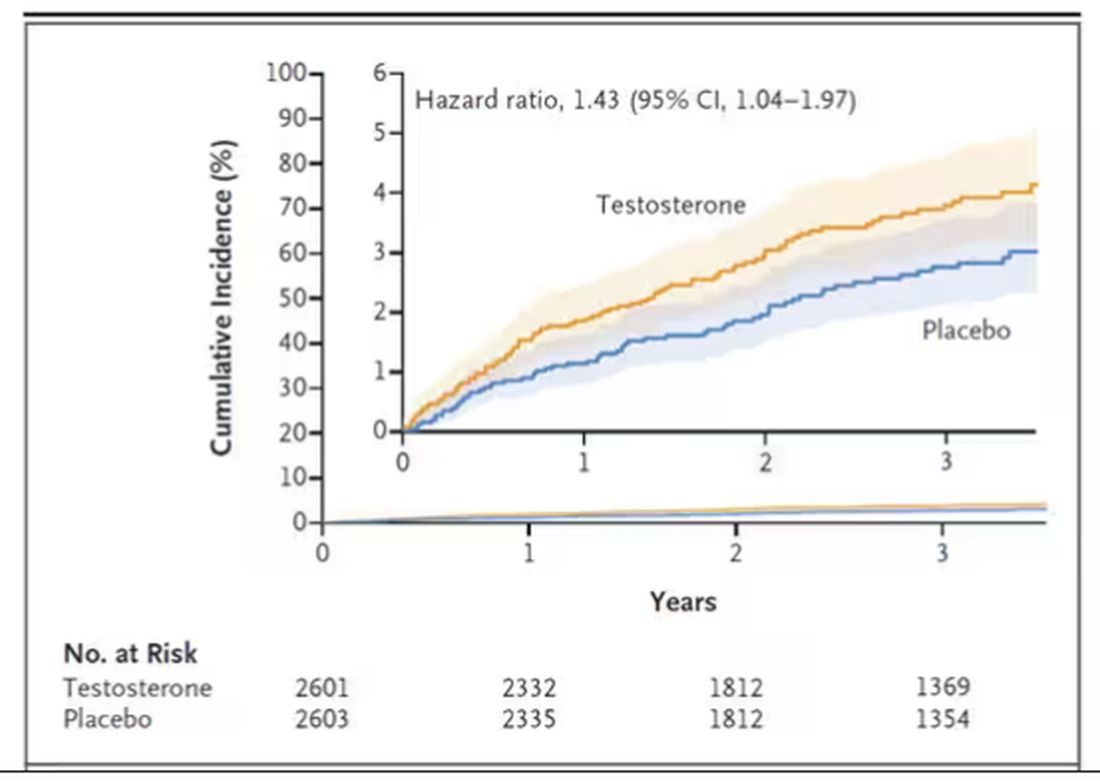
This difference persisted across various fracture types (non–high-impact fractures, for example) after excluding the small percentage of men taking osteoporosis medication.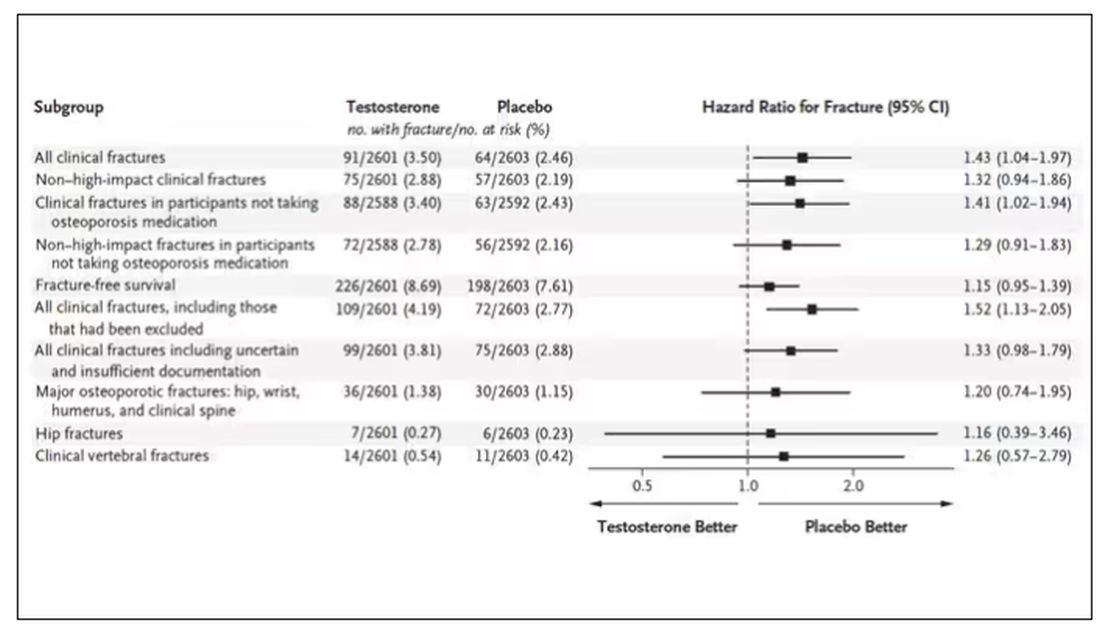
How does a drug that increases bone mineral density and bone strength increase the risk for fracture?
Well, one clue — and this was pointed out in a nice editorial by Matthis Grossman and Bradley Anawalt — is that the increased risk for fracture occurs quite soon after starting treatment, which is not consistent with direct bone effects. Rather, this might represent behavioral differences. Testosterone supplementation seems to increase energy levels; might it lead men to engage in activities that put them at higher risk for fracture?
Regardless of the cause, this adds to our knowledge about the rather complex mix of risks and benefits of testosterone supplementation and probably puts a bit more weight on the risks side. The truth is that testosterone levels do decline with age, as do many things, and it may not be appropriate to try to fight against that in all people. It’s worth noting that all of these studies use low levels of total serum testosterone as an entry criterion. But total testosterone is not what your body “sees.” It sees free testosterone, the portion not bound to sex hormone–binding globulin. And that binding protein is affected by lots of stuff — diabetes and obesity lower it, for example — making total testosterone levels seem low when free testosterone might be just fine.
In other words, testosterone supplementation is probably not terrible, but it is definitely not the cure for aging. In situations like this, we need better data to guide exactly who will benefit from the therapy and who will only be exposed to the risks.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I am showing you a graph without any labels.
What could this line represent? The stock price of some company that made a big splash but failed to live up to expectations? An outbreak curve charting the introduction of a new infectious agent to a population? The performance of a viral tweet?
I’ll tell you what it is in a moment, but I wanted you to recognize that there is something inherently wistful in this shape, something that speaks of past glory and inevitable declines. It’s a graph that induces a feeling of resistance — no, do not go gently into that good night.
The graph actually represents (roughly) the normal level of serum testosterone in otherwise-healthy men as they age.
A caveat here: These numbers are not as well defined as I made them seem on this graph, particularly for those older than 65 years. But it is clear that testosterone levels decline with time, and the idea to supplement testosterone is hardly new. Like all treatments, testosterone supplementation has risks and benefits. Some risks are predictable, like exacerbating the symptoms of benign prostatic hyperplasia. Some risks seem to come completely out of left field. That’s what we have today, in a study suggesting that testosterone supplementation increases the risk for bone fractures.
Let me set the stage here by saying that nearly all prior research into the effects of testosterone supplementation has suggested that it is pretty good for bone health. It increases bone mineral density, bone strength, and improves bone architecture.
So if you were to do a randomized trial of testosterone supplementation and look at fracture risk in the testosterone group compared with the placebo group, you would expect the fracture risk would be much lower in those getting supplemented. Of course, this is why we actually do studies instead of assuming we know the answer already — because in this case, you’d be wrong.
I’m talking about this study, appearing in The New England Journal of Medicine.
It’s a prespecified secondary analysis of a randomized trial known as the TRAVERSE trial, which randomly assigned 5246 men with low testosterone levels to transdermal testosterone gel vs placebo. The primary goal of that trial was to assess the cardiovascular risk associated with testosterone supplementation, and the major take-home was that there was no difference in cardiovascular event rates between the testosterone and placebo groups.
This secondary analysis looked at fracture incidence. Researchers contacted participants multiple times in the first year of the study and yearly thereafter. Each time, they asked whether the participant had sustained a fracture. If they answered in the affirmative, a request for medical records was made and the researchers, still blinded to randomization status, adjudicated whether there was indeed a fracture or not, along with some details as to location, situation, and so on.
This was a big study, though, and that translates to just a 3.5% fracture rate in testosterone vs 2.5% in control, but the difference was statistically significant.
This difference persisted across various fracture types (non–high-impact fractures, for example) after excluding the small percentage of men taking osteoporosis medication.
How does a drug that increases bone mineral density and bone strength increase the risk for fracture?
Well, one clue — and this was pointed out in a nice editorial by Matthis Grossman and Bradley Anawalt — is that the increased risk for fracture occurs quite soon after starting treatment, which is not consistent with direct bone effects. Rather, this might represent behavioral differences. Testosterone supplementation seems to increase energy levels; might it lead men to engage in activities that put them at higher risk for fracture?
Regardless of the cause, this adds to our knowledge about the rather complex mix of risks and benefits of testosterone supplementation and probably puts a bit more weight on the risks side. The truth is that testosterone levels do decline with age, as do many things, and it may not be appropriate to try to fight against that in all people. It’s worth noting that all of these studies use low levels of total serum testosterone as an entry criterion. But total testosterone is not what your body “sees.” It sees free testosterone, the portion not bound to sex hormone–binding globulin. And that binding protein is affected by lots of stuff — diabetes and obesity lower it, for example — making total testosterone levels seem low when free testosterone might be just fine.
In other words, testosterone supplementation is probably not terrible, but it is definitely not the cure for aging. In situations like this, we need better data to guide exactly who will benefit from the therapy and who will only be exposed to the risks.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I am showing you a graph without any labels.
What could this line represent? The stock price of some company that made a big splash but failed to live up to expectations? An outbreak curve charting the introduction of a new infectious agent to a population? The performance of a viral tweet?
I’ll tell you what it is in a moment, but I wanted you to recognize that there is something inherently wistful in this shape, something that speaks of past glory and inevitable declines. It’s a graph that induces a feeling of resistance — no, do not go gently into that good night.
The graph actually represents (roughly) the normal level of serum testosterone in otherwise-healthy men as they age.
A caveat here: These numbers are not as well defined as I made them seem on this graph, particularly for those older than 65 years. But it is clear that testosterone levels decline with time, and the idea to supplement testosterone is hardly new. Like all treatments, testosterone supplementation has risks and benefits. Some risks are predictable, like exacerbating the symptoms of benign prostatic hyperplasia. Some risks seem to come completely out of left field. That’s what we have today, in a study suggesting that testosterone supplementation increases the risk for bone fractures.
Let me set the stage here by saying that nearly all prior research into the effects of testosterone supplementation has suggested that it is pretty good for bone health. It increases bone mineral density, bone strength, and improves bone architecture.
So if you were to do a randomized trial of testosterone supplementation and look at fracture risk in the testosterone group compared with the placebo group, you would expect the fracture risk would be much lower in those getting supplemented. Of course, this is why we actually do studies instead of assuming we know the answer already — because in this case, you’d be wrong.
I’m talking about this study, appearing in The New England Journal of Medicine.
It’s a prespecified secondary analysis of a randomized trial known as the TRAVERSE trial, which randomly assigned 5246 men with low testosterone levels to transdermal testosterone gel vs placebo. The primary goal of that trial was to assess the cardiovascular risk associated with testosterone supplementation, and the major take-home was that there was no difference in cardiovascular event rates between the testosterone and placebo groups.
This secondary analysis looked at fracture incidence. Researchers contacted participants multiple times in the first year of the study and yearly thereafter. Each time, they asked whether the participant had sustained a fracture. If they answered in the affirmative, a request for medical records was made and the researchers, still blinded to randomization status, adjudicated whether there was indeed a fracture or not, along with some details as to location, situation, and so on.
This was a big study, though, and that translates to just a 3.5% fracture rate in testosterone vs 2.5% in control, but the difference was statistically significant.
This difference persisted across various fracture types (non–high-impact fractures, for example) after excluding the small percentage of men taking osteoporosis medication.
How does a drug that increases bone mineral density and bone strength increase the risk for fracture?
Well, one clue — and this was pointed out in a nice editorial by Matthis Grossman and Bradley Anawalt — is that the increased risk for fracture occurs quite soon after starting treatment, which is not consistent with direct bone effects. Rather, this might represent behavioral differences. Testosterone supplementation seems to increase energy levels; might it lead men to engage in activities that put them at higher risk for fracture?
Regardless of the cause, this adds to our knowledge about the rather complex mix of risks and benefits of testosterone supplementation and probably puts a bit more weight on the risks side. The truth is that testosterone levels do decline with age, as do many things, and it may not be appropriate to try to fight against that in all people. It’s worth noting that all of these studies use low levels of total serum testosterone as an entry criterion. But total testosterone is not what your body “sees.” It sees free testosterone, the portion not bound to sex hormone–binding globulin. And that binding protein is affected by lots of stuff — diabetes and obesity lower it, for example — making total testosterone levels seem low when free testosterone might be just fine.
In other words, testosterone supplementation is probably not terrible, but it is definitely not the cure for aging. In situations like this, we need better data to guide exactly who will benefit from the therapy and who will only be exposed to the risks.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Testosterone Supplements: Overcoming Current Misconceptions
Underdiagnosis, reluctant doctors, patient preconceptions: Treating low testosterone levels is a tricky business in France despite the proven benefits of replacement therapy. About 20% of patients with symptomatic low testosterone levels are treated for the deficiency, said Eric Huygue, MD, PhD, urologic surgeon at Toulouse University Hospital in France, at the 117th annual conference of the French Urology Association (AFU).
, said Dr. Huygue, who was involved in drawing up the first French recommendations on treating low testosterone in 2021.
“We must keep up communication efforts to make patients and doctors aware” of the benefits of supplementation, he said.
Testosterone Levels
Testosterone deficiency mostly affects men older than 40 years. A drop in androgen levels, which varies by individual, can lead to sexual problems (such as erectile dysfunction and low libido), physical symptoms (fatigue, hot flashes, loss of muscle mass, and osteoporosis), and mental disorders (anxiety, irritability, and depression).
There are an estimated 340,000 men with symptomatic testosterone deficiency in France. Just 70,000 of these are receiving replacement therapy (see box), which accounts for only 20% of those affected. For Dr. Huygue, this low treatment rate is due to underdiagnosis, as well as reluctance on the part of doctors and patients.
Although routine screening of low testosterone in the general population is not recommended, some individuals are particularly at risk, noted the urologist.
This is especially true for patients with metabolic disorders associated with insulin resistance (such as obesity and type 2 diabetes), cardiovascular diseases (hypertension, heart failure, and atrial fibrillation), or other chronic conditions (chronic obstructive pulmonary disease, cancer, and depression). Some medications (corticosteroids, antipsychotics, chemotherapy drugs, and antiretroviral therapies) can also lead to low testosterone.
Per the French recommendations for managing low testosterone, diagnosis must be based on free or bioavailable testosterone and not total testosterone levels, which can give a skewed result. Levels must be tested twice, 1 month apart, in the morning and while fasting. The reference range is determined by taking the lower threshold level of young men as measured in the laboratory.
Threshold Values
The current practice of using the reference range associated with the patient’s age group undoubtedly contributes to the underdiagnosis of low testosterone, said Dr. Huygue. According to a survey of AFU members in 2021, the year in which the recommendations were published, 77% of urologists interviewed reported referring to reference ranges for patients of the same age.
In their defense, “this method has long been in use, but it has eventually become apparent that symptomatic patients with an undiagnosed deficiency could be in the reference patients’ group,” Dr. Huygue explained.
Once a deficiency has been diagnosed, doctors may be reluctant to prescribe replacement therapy due to the perceived risk of developing prostate cancer. Several international studies have shown that “the risk of prostate cancer is the single biggest reason for doctors refusing to prescribe testosterone,” said Dr. Huygue.
Despite this reluctance, numerous studies have clearly shown that there is no link between a high testosterone level and the risk of developing prostate cancer. It even seems that a low testosterone level might expose a person to an increased risk for an aggressive form of cancer.
“This is a time of many surprising discoveries concerning the link between the prostate and testosterone, which go against what we have thought up to now. It has been observed that men with low testosterone develop more serious types of cancer,” said Dr. Huygue at a previous meeting of the AFU, during which he announced the publication of the French recommendations.
Prostate Cancer Recurrence
Urologists are also wary of testosterone supplementation in patients with a previous history of prostate cancer. According to the AFU’s survey, 40% of urologists questioned think that testosterone is contraindicated in this population. One in two urologists prescribe testosterone after radical prostatectomy for low or intermediate risk and most commonly after 3 years of undetectable prostate-specific antigen (PSA) levels.
Nevertheless, “several retrospective studies show the safety of testosterone replacement therapy in men who have undergone radical prostatectomy or radiotherapy or who are under active monitoring,” said Dr. Huygue. Testosterone “does not appear to increase the risk of relapse” after treatment of prostate cancer.
Dr. Huygue invited prescribing physicians to refer to the French recommendations, which specify that 1 year of undetectable PSA after prostatectomy is sufficient before prescribing replacement therapy. “This is clearly indicated in the recommendations for patients with a previous history of prostate cancer.”
Neither prostate cancer nor benign prostatic hyperplasia is a contraindication. According to the recommendations, the only contraindications to testosterone prescription are the following:
- Hematocrit > 54%
- Current breast or prostate cancer
- Cardiovascular event less than 3-6 months prior
- Trying to conceive
Cardiovascular Benefits
Another more commonly used argument by general practitioners and endocrinologists to justify their reluctance to prescribe testosterone is the risk to cardiovascular health. In early 2010, a series of American studies alerted clinicians to this risk when taking testosterone. Since then, other studies have had reassuring findings.
In response to the alert issued by the United States, the European Medicines Agency specified that “the data are not sufficient for a warning,” before the American Heart Association colleagues concluded that testosterone should only be avoided in the first 6 months following a severe cardiovascular event.
Conversely, in 2021, the European Society of Cardiology put forward the benefits of testosterone in an article in favor of replacement therapy to prevent cardiovascular risk. In particular, the hormone is thought to have a beneficial effect on arterial stiffness, the appearance of calcified plaques, and coronary artery dilatation.
The final hurdle to overcome before a testosterone prescription is filled relates to patients themselves, who often regard such treatment unfavorably. Many wrongly believe that androgens are hormones that “increase the risk of cancer, make you aggressive, cause weight gain, lead to hair loss, and cause body hair growth,” said Dr. Huygue.
Finally, breaks in the supply chain for Androtardyl, the only injectable form available for reimbursement by French social security schemes, were reported in the country in 2023, said Dr. Huygue. This situation only complicates further the prescription and use of testosterone replacement therapy.
Which Supplement?
Testosterone replacement therapies are available on the market in the following formulations:
Via transcutaneous administration: Testosterone-based gels, not covered by the French social security system (Androgel and Fortigel), to be applied daily. Users must be careful to avoid any potential transfer of the product to women or children in case of contact with the site after application.
Via an injection: Androtardyl (testosterone enanthate), covered by French social security, to be administered intramuscularly once a month. Nebido (testosterone undecanoate), not covered by French social security, with a more beneficial bioavailability profile, to be administered once every 3 months.
Pantestone (testosterone undecanoate), administered orally, is not marketed since 2021. It had the major disadvantage of requiring a high-fat diet to ensure optimal absorption.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
Underdiagnosis, reluctant doctors, patient preconceptions: Treating low testosterone levels is a tricky business in France despite the proven benefits of replacement therapy. About 20% of patients with symptomatic low testosterone levels are treated for the deficiency, said Eric Huygue, MD, PhD, urologic surgeon at Toulouse University Hospital in France, at the 117th annual conference of the French Urology Association (AFU).
, said Dr. Huygue, who was involved in drawing up the first French recommendations on treating low testosterone in 2021.
“We must keep up communication efforts to make patients and doctors aware” of the benefits of supplementation, he said.
Testosterone Levels
Testosterone deficiency mostly affects men older than 40 years. A drop in androgen levels, which varies by individual, can lead to sexual problems (such as erectile dysfunction and low libido), physical symptoms (fatigue, hot flashes, loss of muscle mass, and osteoporosis), and mental disorders (anxiety, irritability, and depression).
There are an estimated 340,000 men with symptomatic testosterone deficiency in France. Just 70,000 of these are receiving replacement therapy (see box), which accounts for only 20% of those affected. For Dr. Huygue, this low treatment rate is due to underdiagnosis, as well as reluctance on the part of doctors and patients.
Although routine screening of low testosterone in the general population is not recommended, some individuals are particularly at risk, noted the urologist.
This is especially true for patients with metabolic disorders associated with insulin resistance (such as obesity and type 2 diabetes), cardiovascular diseases (hypertension, heart failure, and atrial fibrillation), or other chronic conditions (chronic obstructive pulmonary disease, cancer, and depression). Some medications (corticosteroids, antipsychotics, chemotherapy drugs, and antiretroviral therapies) can also lead to low testosterone.
Per the French recommendations for managing low testosterone, diagnosis must be based on free or bioavailable testosterone and not total testosterone levels, which can give a skewed result. Levels must be tested twice, 1 month apart, in the morning and while fasting. The reference range is determined by taking the lower threshold level of young men as measured in the laboratory.
Threshold Values
The current practice of using the reference range associated with the patient’s age group undoubtedly contributes to the underdiagnosis of low testosterone, said Dr. Huygue. According to a survey of AFU members in 2021, the year in which the recommendations were published, 77% of urologists interviewed reported referring to reference ranges for patients of the same age.
In their defense, “this method has long been in use, but it has eventually become apparent that symptomatic patients with an undiagnosed deficiency could be in the reference patients’ group,” Dr. Huygue explained.
Once a deficiency has been diagnosed, doctors may be reluctant to prescribe replacement therapy due to the perceived risk of developing prostate cancer. Several international studies have shown that “the risk of prostate cancer is the single biggest reason for doctors refusing to prescribe testosterone,” said Dr. Huygue.
Despite this reluctance, numerous studies have clearly shown that there is no link between a high testosterone level and the risk of developing prostate cancer. It even seems that a low testosterone level might expose a person to an increased risk for an aggressive form of cancer.
“This is a time of many surprising discoveries concerning the link between the prostate and testosterone, which go against what we have thought up to now. It has been observed that men with low testosterone develop more serious types of cancer,” said Dr. Huygue at a previous meeting of the AFU, during which he announced the publication of the French recommendations.
Prostate Cancer Recurrence
Urologists are also wary of testosterone supplementation in patients with a previous history of prostate cancer. According to the AFU’s survey, 40% of urologists questioned think that testosterone is contraindicated in this population. One in two urologists prescribe testosterone after radical prostatectomy for low or intermediate risk and most commonly after 3 years of undetectable prostate-specific antigen (PSA) levels.
Nevertheless, “several retrospective studies show the safety of testosterone replacement therapy in men who have undergone radical prostatectomy or radiotherapy or who are under active monitoring,” said Dr. Huygue. Testosterone “does not appear to increase the risk of relapse” after treatment of prostate cancer.
Dr. Huygue invited prescribing physicians to refer to the French recommendations, which specify that 1 year of undetectable PSA after prostatectomy is sufficient before prescribing replacement therapy. “This is clearly indicated in the recommendations for patients with a previous history of prostate cancer.”
Neither prostate cancer nor benign prostatic hyperplasia is a contraindication. According to the recommendations, the only contraindications to testosterone prescription are the following:
- Hematocrit > 54%
- Current breast or prostate cancer
- Cardiovascular event less than 3-6 months prior
- Trying to conceive
Cardiovascular Benefits
Another more commonly used argument by general practitioners and endocrinologists to justify their reluctance to prescribe testosterone is the risk to cardiovascular health. In early 2010, a series of American studies alerted clinicians to this risk when taking testosterone. Since then, other studies have had reassuring findings.
In response to the alert issued by the United States, the European Medicines Agency specified that “the data are not sufficient for a warning,” before the American Heart Association colleagues concluded that testosterone should only be avoided in the first 6 months following a severe cardiovascular event.
Conversely, in 2021, the European Society of Cardiology put forward the benefits of testosterone in an article in favor of replacement therapy to prevent cardiovascular risk. In particular, the hormone is thought to have a beneficial effect on arterial stiffness, the appearance of calcified plaques, and coronary artery dilatation.
The final hurdle to overcome before a testosterone prescription is filled relates to patients themselves, who often regard such treatment unfavorably. Many wrongly believe that androgens are hormones that “increase the risk of cancer, make you aggressive, cause weight gain, lead to hair loss, and cause body hair growth,” said Dr. Huygue.
Finally, breaks in the supply chain for Androtardyl, the only injectable form available for reimbursement by French social security schemes, were reported in the country in 2023, said Dr. Huygue. This situation only complicates further the prescription and use of testosterone replacement therapy.
Which Supplement?
Testosterone replacement therapies are available on the market in the following formulations:
Via transcutaneous administration: Testosterone-based gels, not covered by the French social security system (Androgel and Fortigel), to be applied daily. Users must be careful to avoid any potential transfer of the product to women or children in case of contact with the site after application.
Via an injection: Androtardyl (testosterone enanthate), covered by French social security, to be administered intramuscularly once a month. Nebido (testosterone undecanoate), not covered by French social security, with a more beneficial bioavailability profile, to be administered once every 3 months.
Pantestone (testosterone undecanoate), administered orally, is not marketed since 2021. It had the major disadvantage of requiring a high-fat diet to ensure optimal absorption.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
Underdiagnosis, reluctant doctors, patient preconceptions: Treating low testosterone levels is a tricky business in France despite the proven benefits of replacement therapy. About 20% of patients with symptomatic low testosterone levels are treated for the deficiency, said Eric Huygue, MD, PhD, urologic surgeon at Toulouse University Hospital in France, at the 117th annual conference of the French Urology Association (AFU).
, said Dr. Huygue, who was involved in drawing up the first French recommendations on treating low testosterone in 2021.
“We must keep up communication efforts to make patients and doctors aware” of the benefits of supplementation, he said.
Testosterone Levels
Testosterone deficiency mostly affects men older than 40 years. A drop in androgen levels, which varies by individual, can lead to sexual problems (such as erectile dysfunction and low libido), physical symptoms (fatigue, hot flashes, loss of muscle mass, and osteoporosis), and mental disorders (anxiety, irritability, and depression).
There are an estimated 340,000 men with symptomatic testosterone deficiency in France. Just 70,000 of these are receiving replacement therapy (see box), which accounts for only 20% of those affected. For Dr. Huygue, this low treatment rate is due to underdiagnosis, as well as reluctance on the part of doctors and patients.
Although routine screening of low testosterone in the general population is not recommended, some individuals are particularly at risk, noted the urologist.
This is especially true for patients with metabolic disorders associated with insulin resistance (such as obesity and type 2 diabetes), cardiovascular diseases (hypertension, heart failure, and atrial fibrillation), or other chronic conditions (chronic obstructive pulmonary disease, cancer, and depression). Some medications (corticosteroids, antipsychotics, chemotherapy drugs, and antiretroviral therapies) can also lead to low testosterone.
Per the French recommendations for managing low testosterone, diagnosis must be based on free or bioavailable testosterone and not total testosterone levels, which can give a skewed result. Levels must be tested twice, 1 month apart, in the morning and while fasting. The reference range is determined by taking the lower threshold level of young men as measured in the laboratory.
Threshold Values
The current practice of using the reference range associated with the patient’s age group undoubtedly contributes to the underdiagnosis of low testosterone, said Dr. Huygue. According to a survey of AFU members in 2021, the year in which the recommendations were published, 77% of urologists interviewed reported referring to reference ranges for patients of the same age.
In their defense, “this method has long been in use, but it has eventually become apparent that symptomatic patients with an undiagnosed deficiency could be in the reference patients’ group,” Dr. Huygue explained.
Once a deficiency has been diagnosed, doctors may be reluctant to prescribe replacement therapy due to the perceived risk of developing prostate cancer. Several international studies have shown that “the risk of prostate cancer is the single biggest reason for doctors refusing to prescribe testosterone,” said Dr. Huygue.
Despite this reluctance, numerous studies have clearly shown that there is no link between a high testosterone level and the risk of developing prostate cancer. It even seems that a low testosterone level might expose a person to an increased risk for an aggressive form of cancer.
“This is a time of many surprising discoveries concerning the link between the prostate and testosterone, which go against what we have thought up to now. It has been observed that men with low testosterone develop more serious types of cancer,” said Dr. Huygue at a previous meeting of the AFU, during which he announced the publication of the French recommendations.
Prostate Cancer Recurrence
Urologists are also wary of testosterone supplementation in patients with a previous history of prostate cancer. According to the AFU’s survey, 40% of urologists questioned think that testosterone is contraindicated in this population. One in two urologists prescribe testosterone after radical prostatectomy for low or intermediate risk and most commonly after 3 years of undetectable prostate-specific antigen (PSA) levels.
Nevertheless, “several retrospective studies show the safety of testosterone replacement therapy in men who have undergone radical prostatectomy or radiotherapy or who are under active monitoring,” said Dr. Huygue. Testosterone “does not appear to increase the risk of relapse” after treatment of prostate cancer.
Dr. Huygue invited prescribing physicians to refer to the French recommendations, which specify that 1 year of undetectable PSA after prostatectomy is sufficient before prescribing replacement therapy. “This is clearly indicated in the recommendations for patients with a previous history of prostate cancer.”
Neither prostate cancer nor benign prostatic hyperplasia is a contraindication. According to the recommendations, the only contraindications to testosterone prescription are the following:
- Hematocrit > 54%
- Current breast or prostate cancer
- Cardiovascular event less than 3-6 months prior
- Trying to conceive
Cardiovascular Benefits
Another more commonly used argument by general practitioners and endocrinologists to justify their reluctance to prescribe testosterone is the risk to cardiovascular health. In early 2010, a series of American studies alerted clinicians to this risk when taking testosterone. Since then, other studies have had reassuring findings.
In response to the alert issued by the United States, the European Medicines Agency specified that “the data are not sufficient for a warning,” before the American Heart Association colleagues concluded that testosterone should only be avoided in the first 6 months following a severe cardiovascular event.
Conversely, in 2021, the European Society of Cardiology put forward the benefits of testosterone in an article in favor of replacement therapy to prevent cardiovascular risk. In particular, the hormone is thought to have a beneficial effect on arterial stiffness, the appearance of calcified plaques, and coronary artery dilatation.
The final hurdle to overcome before a testosterone prescription is filled relates to patients themselves, who often regard such treatment unfavorably. Many wrongly believe that androgens are hormones that “increase the risk of cancer, make you aggressive, cause weight gain, lead to hair loss, and cause body hair growth,” said Dr. Huygue.
Finally, breaks in the supply chain for Androtardyl, the only injectable form available for reimbursement by French social security schemes, were reported in the country in 2023, said Dr. Huygue. This situation only complicates further the prescription and use of testosterone replacement therapy.
Which Supplement?
Testosterone replacement therapies are available on the market in the following formulations:
Via transcutaneous administration: Testosterone-based gels, not covered by the French social security system (Androgel and Fortigel), to be applied daily. Users must be careful to avoid any potential transfer of the product to women or children in case of contact with the site after application.
Via an injection: Androtardyl (testosterone enanthate), covered by French social security, to be administered intramuscularly once a month. Nebido (testosterone undecanoate), not covered by French social security, with a more beneficial bioavailability profile, to be administered once every 3 months.
Pantestone (testosterone undecanoate), administered orally, is not marketed since 2021. It had the major disadvantage of requiring a high-fat diet to ensure optimal absorption.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
How much would you bet on a diagnosis?
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.

With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.
With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.
With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
10 Weight-Loss Strategies to Help Patients With Obesity
This transcript has been edited for clarity.
According to the Centers for Disease Control and Prevention, the obesity prevalence in America was 41.9% between 2017 and 2020. Just 10 years ago, no state had an obesity prevalence above 35%.
Over the past 3 years, many patients gained weight during the COVID-19 pandemic as a result of adopting more sedentary lifestyles, staying at home, avoiding the gym owing to the potential for respiratory spread, and working remotely. For a long time, patients were avoiding attending social events and, as a result, were walking much less.
and other physicians to help patients with obesity realize their goal of achieving weight loss.
1. Embracing the GLP-1 Revolution, With Some Caveats
Glucagon-like peptide-1 (GLP-1) receptor agonists have become a popular treatment for type 2 diabetes and weight loss. These medications, which are given as an injection either weekly or daily depending on the type, have helped patients achieve weight loss with tremendous success.
They work by stimulating the body to produce insulin, which in turn lowers blood sugar. GLP-1 receptor agonists also slow peristalsis and the movement of food from the stomach into the small bowel, which allows patients to eat less by feeling fuller for longer and decreasing hunger.
Two GLP-1 receptor agonists are approved by the US Food and Drug Administration (FDA) for weight loss in patients without diabetes: liraglutide (Saxenda) and semaglutide (Wegovy). There are also lower-dose versions of these active ingredients with the trade names Ozempic and Victoza, designed to help patients with diabetes achieve better glucose and A1c control. In November 2023, the FDA approved a new medication called tirzepatide (Zepbound), which is a glucose-dependent insulinotropic polypeptide (GIP) plus GLP-1 receptor agonist.
This is a very exciting time for the management of type 2 diabetes and weight loss. Gastroenterologists can work with endocrinologists and primary care physicians to help patients choose appropriate weight loss medications.
However, gastroenterologists should also be aware of common GLP-1 receptor agonist side effects, including nausea, vomiting, diarrhea, and — in severe cases — hypoglycemia. These medications can also cause pancreatitis, acute kidney injury, worsening diabetes-related retinopathy, tachycardia, headaches, indigestion, gastroparesis, bowel obstruction, or ileus. We don’t use these medications in patients with a family or personal history of medullary thyroid cancer or multiple endocrine neoplasia. Consider avoiding their use as well in patients with a personal history of pancreatitis.
Recently, the American Society of Anesthesiologists (ASA) suggested holding off on the use of GLP-1 receptor agonists prior to elective endoscopy procedures owing to case reports of aspiration. Gastroenterologists and anesthesiologists are working together to make esophagogastroduodenoscopy (EGD) and colonoscopy as safe as possible in patients taking these treatments.
According to the ASA recommendations, GLP-1 receptor agonists that are given at a daily dose should be held on the day of their procedure. Weekly-dose versions are supposed to be held for 1 week prior to colonoscopy or EGD. During EGD procedures, I also recommend keeping the head of the bed at a 45° angle to help prevent aspiration even further.
Gastroenterologists are eagerly awaiting additional studies to determine whether holding GLP-1 receptor agonists prior to endoscopy is really necessary. But for now, we recommend following the ASA guidelines.
2. Substituting Out Sugary Drinks
Gastroenterologists and primary care physicians constantly advise their patients to avoid consuming sugary drinks, such as soda, fruit juices, calorie-laden coffee drinks, sweetened tea, hot chocolate, and, of course, alcohol. Many of our patients drink three to six of these sugary drinks a day.
As a gastroenterologist, it’s important to counsel our overweight patients and obtain an accurate history about their daily and weekly consumption of excess calories.
Recommend substituting sugary drinks with water, unsweetened tea (either hot or cold), and coffee.
To prevent constipation, encourage patients to drink at least eight 8-ounce glasses of fluid per day. Drinking water, tea, and coffee can also help keep patients feeling fuller for longer and avoid those tempting snacks.
3. Adopting the Right Diet
Every day, I encourage my patients to avoid eating fried fatty foods and processed meats. We also advise patients to avoid junk food filled with carbohydrates and salt.
Instead, patients should try to eat a piece of fruit or some vegetables with every single meal, which keeps patients feeling fuller for longer, prevents diverticulitis from forming, and can even help prevent colon cancer.
Making small dietary changes can dramatically reduce daily calorie consumption, which adds up over time and can help patients lose weight in a safe way.
Meal prepping for the week ahead, perhaps on a Sunday, is a very simple way to eat more nutritious foods instead of constantly getting takeout and fast food.
Many of our patients have also successfully lost weight through intermittent fasting, although I recommend working with a nutritionist on this one.
A Mediterranean diet is also a great option.
4. Getting Active
I encourage patients to take daily walks, swim, play sports, take fitness classes, do yoga or Pilates, and use weights at a gym.
Exercise burns calories, which is great for our hearts, prevents hepatic steatosis, and helps relieve stress. Exercise also stimulates peristalsis, which can help our constipated patients achieve more regular bowel movements.
There are a few other things to keep in mind in this area. Try to avoid strenuous exercise right after eating, because this will help prevent both heartburn and gastroesophageal reflux disease (GERD).
5. Reducing Stomach Volume With a Gastric Balloon
A gastric balloon procedure is a temporary obesity treatment that helps patients lose weight by reducing the volume of the stomach so that they feel full more easily. This can be accomplished endoscopically through the mouth without the need for surgery.
Basically, a deflated balloon is placed through the mouth using an endoscope and advanced into the stomach by a gastroenterologist or surgeon. The balloon is inflated with salt water and can remain in the stomach for 6 months before it is removed.
This procedure can help patients feel full and consequently eat less, thereby leading to gradual and safe weight loss.
6. Using the Accordion Procedure
An endoscopic sleeve gastroplasty procedure, sometimes called an accordion procedure, is used for patients with a body mass index ≥ 30 when diet and exercise alone have failed. An EGD tube is equipped with small stitching instruments that are used to reduce the size of the stomach.
This procedure has less complications than open or laparoscopic surgery and can be reversed.
7. Injecting Botulinum Toxin
Another technique is having the gastroenterologist inject botulinum toxin into the stomach wall. This works by relaxing the stomach propulsion muscles, which delays gastric emptying so that patients feel fuller longer and more easily.
This approach is good for achieving moderate weight loss of approximately 5%-10% of body weight. It works best in combination with a good diet and exercise. The effects of the botulinum toxin can last for 3 months, and the procedure can be repeated every 6 months.
8. Adjusting Certain Lifestyle Factors
Gastroenterologists should also counsel our patients about exercise, stress management, and the importance of sleep to prevent overeating. Self-care is extremely important for patients. Walk, swim, lift weights, and play sports; I personally love basketball and tennis.
I also recommend allocating enough time for sleep each night. At least 7-9 hours of sleep is ideal. Good sleep hygiene can help keep a stable schedule. Create a comfortable bedroom that is free of disruptions like TV watching or playing on your phone or computer.
Gastroenterologists can provide simple instructions to their patients on how to achieve this. For example, unplug from electronics 30-60 minutes prior to sleep. Try also to avoid eating late at night, which will help patients prevent GERD and heartburn symptoms too.
9. Considering Orlistat as an Option
Orlistat is an oral over-the-counter lipase inhibitor that inhibits fat absorption in the intestines. This drug can interfere with the absorption of fat-soluble vitamins A, D, E, and K. Therefore, it’s important to take a multivitamin 2 hours before or 2 hours after taking orlistat.
However, orlistat can cause steatorrhea, so it’s often not our first choice.
10. Working With Dietitians
I highly recommend that gastroenterologists regularly refer patients to a registered dietitian for medical nutrition therapy. Dietitians help patients establish nutritional goals with calorie limits. I find that many of my patients like the nutritional counseling the dietitians provide, and this can even be done via telemedicine.
A dietitian will examine a patient’s eating habits and help them set weight loss goals that are both realistic and achievable. Having a dietitian motivate a patient through several clinic visits is important for success. A dietitian can plan how many calories a patient should consume in a day while maintaining food, protein, and vitamin intake.
With this therapy, many patients are able to lose approximately 1-1.5 pounds each week. A dietitian can help keep patients accountable for their weight loss goals. I encourage my patients to use their dietitian as a weight loss teacher and a coach who can personalize a diet plan that tastes great.
Some of our patients also have overlapping gastrointestinal issues, such as celiac disease or irritable bowel syndrome. Dietitians can also formulate diets that are great for these other diagnoses too.
There are also apps available on our phones to help with diet and weight loss.
Having a Difficult Conversation to Prevent Long-Term Disease
It’s important for gastroenterologists to work with patients to achieve weight loss. Addressing obesity is sometimes a difficult topic to bring up with patients, but it’s nonetheless very important.
Together, we can help treat obesity plus improve and prevent hepatic steatosis, metabolic dysfunction–associated steatotic liver disease (MASLD), and metabolic dysfunction–associated steatohepatitis (MASH). The estimated global prevalence of MASLD is 32% in adults, so gastroenterologists and hepatologists are working together to try to treat obesity and to prevent long-term liver disease.
Dr. Levy is a gastroenterologist at the University of Chicago. In 2017, Levy, a previous Fulbright Fellow in France, also started a gastroenterology clinic for refugees resettling in Chicago. His clinical projects focus on the development of colorectal cancer screening campaigns. Levy, who recently gave a TEDx Talk about building health education campaigns using music and concerts, organizes Tune It Up: A Concert To Raise Colorectal Cancer Awareness with the American College of Gastroenterology (ACG). He frequently publishes on a variety of gastroenterology topics and serves on ACG’s Public Relations Committee and FDA-Related Matters Committee. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
According to the Centers for Disease Control and Prevention, the obesity prevalence in America was 41.9% between 2017 and 2020. Just 10 years ago, no state had an obesity prevalence above 35%.
Over the past 3 years, many patients gained weight during the COVID-19 pandemic as a result of adopting more sedentary lifestyles, staying at home, avoiding the gym owing to the potential for respiratory spread, and working remotely. For a long time, patients were avoiding attending social events and, as a result, were walking much less.
and other physicians to help patients with obesity realize their goal of achieving weight loss.
1. Embracing the GLP-1 Revolution, With Some Caveats
Glucagon-like peptide-1 (GLP-1) receptor agonists have become a popular treatment for type 2 diabetes and weight loss. These medications, which are given as an injection either weekly or daily depending on the type, have helped patients achieve weight loss with tremendous success.
They work by stimulating the body to produce insulin, which in turn lowers blood sugar. GLP-1 receptor agonists also slow peristalsis and the movement of food from the stomach into the small bowel, which allows patients to eat less by feeling fuller for longer and decreasing hunger.
Two GLP-1 receptor agonists are approved by the US Food and Drug Administration (FDA) for weight loss in patients without diabetes: liraglutide (Saxenda) and semaglutide (Wegovy). There are also lower-dose versions of these active ingredients with the trade names Ozempic and Victoza, designed to help patients with diabetes achieve better glucose and A1c control. In November 2023, the FDA approved a new medication called tirzepatide (Zepbound), which is a glucose-dependent insulinotropic polypeptide (GIP) plus GLP-1 receptor agonist.
This is a very exciting time for the management of type 2 diabetes and weight loss. Gastroenterologists can work with endocrinologists and primary care physicians to help patients choose appropriate weight loss medications.
However, gastroenterologists should also be aware of common GLP-1 receptor agonist side effects, including nausea, vomiting, diarrhea, and — in severe cases — hypoglycemia. These medications can also cause pancreatitis, acute kidney injury, worsening diabetes-related retinopathy, tachycardia, headaches, indigestion, gastroparesis, bowel obstruction, or ileus. We don’t use these medications in patients with a family or personal history of medullary thyroid cancer or multiple endocrine neoplasia. Consider avoiding their use as well in patients with a personal history of pancreatitis.
Recently, the American Society of Anesthesiologists (ASA) suggested holding off on the use of GLP-1 receptor agonists prior to elective endoscopy procedures owing to case reports of aspiration. Gastroenterologists and anesthesiologists are working together to make esophagogastroduodenoscopy (EGD) and colonoscopy as safe as possible in patients taking these treatments.
According to the ASA recommendations, GLP-1 receptor agonists that are given at a daily dose should be held on the day of their procedure. Weekly-dose versions are supposed to be held for 1 week prior to colonoscopy or EGD. During EGD procedures, I also recommend keeping the head of the bed at a 45° angle to help prevent aspiration even further.
Gastroenterologists are eagerly awaiting additional studies to determine whether holding GLP-1 receptor agonists prior to endoscopy is really necessary. But for now, we recommend following the ASA guidelines.
2. Substituting Out Sugary Drinks
Gastroenterologists and primary care physicians constantly advise their patients to avoid consuming sugary drinks, such as soda, fruit juices, calorie-laden coffee drinks, sweetened tea, hot chocolate, and, of course, alcohol. Many of our patients drink three to six of these sugary drinks a day.
As a gastroenterologist, it’s important to counsel our overweight patients and obtain an accurate history about their daily and weekly consumption of excess calories.
Recommend substituting sugary drinks with water, unsweetened tea (either hot or cold), and coffee.
To prevent constipation, encourage patients to drink at least eight 8-ounce glasses of fluid per day. Drinking water, tea, and coffee can also help keep patients feeling fuller for longer and avoid those tempting snacks.
3. Adopting the Right Diet
Every day, I encourage my patients to avoid eating fried fatty foods and processed meats. We also advise patients to avoid junk food filled with carbohydrates and salt.
Instead, patients should try to eat a piece of fruit or some vegetables with every single meal, which keeps patients feeling fuller for longer, prevents diverticulitis from forming, and can even help prevent colon cancer.
Making small dietary changes can dramatically reduce daily calorie consumption, which adds up over time and can help patients lose weight in a safe way.
Meal prepping for the week ahead, perhaps on a Sunday, is a very simple way to eat more nutritious foods instead of constantly getting takeout and fast food.
Many of our patients have also successfully lost weight through intermittent fasting, although I recommend working with a nutritionist on this one.
A Mediterranean diet is also a great option.
4. Getting Active
I encourage patients to take daily walks, swim, play sports, take fitness classes, do yoga or Pilates, and use weights at a gym.
Exercise burns calories, which is great for our hearts, prevents hepatic steatosis, and helps relieve stress. Exercise also stimulates peristalsis, which can help our constipated patients achieve more regular bowel movements.
There are a few other things to keep in mind in this area. Try to avoid strenuous exercise right after eating, because this will help prevent both heartburn and gastroesophageal reflux disease (GERD).
5. Reducing Stomach Volume With a Gastric Balloon
A gastric balloon procedure is a temporary obesity treatment that helps patients lose weight by reducing the volume of the stomach so that they feel full more easily. This can be accomplished endoscopically through the mouth without the need for surgery.
Basically, a deflated balloon is placed through the mouth using an endoscope and advanced into the stomach by a gastroenterologist or surgeon. The balloon is inflated with salt water and can remain in the stomach for 6 months before it is removed.
This procedure can help patients feel full and consequently eat less, thereby leading to gradual and safe weight loss.
6. Using the Accordion Procedure
An endoscopic sleeve gastroplasty procedure, sometimes called an accordion procedure, is used for patients with a body mass index ≥ 30 when diet and exercise alone have failed. An EGD tube is equipped with small stitching instruments that are used to reduce the size of the stomach.
This procedure has less complications than open or laparoscopic surgery and can be reversed.
7. Injecting Botulinum Toxin
Another technique is having the gastroenterologist inject botulinum toxin into the stomach wall. This works by relaxing the stomach propulsion muscles, which delays gastric emptying so that patients feel fuller longer and more easily.
This approach is good for achieving moderate weight loss of approximately 5%-10% of body weight. It works best in combination with a good diet and exercise. The effects of the botulinum toxin can last for 3 months, and the procedure can be repeated every 6 months.
8. Adjusting Certain Lifestyle Factors
Gastroenterologists should also counsel our patients about exercise, stress management, and the importance of sleep to prevent overeating. Self-care is extremely important for patients. Walk, swim, lift weights, and play sports; I personally love basketball and tennis.
I also recommend allocating enough time for sleep each night. At least 7-9 hours of sleep is ideal. Good sleep hygiene can help keep a stable schedule. Create a comfortable bedroom that is free of disruptions like TV watching or playing on your phone or computer.
Gastroenterologists can provide simple instructions to their patients on how to achieve this. For example, unplug from electronics 30-60 minutes prior to sleep. Try also to avoid eating late at night, which will help patients prevent GERD and heartburn symptoms too.
9. Considering Orlistat as an Option
Orlistat is an oral over-the-counter lipase inhibitor that inhibits fat absorption in the intestines. This drug can interfere with the absorption of fat-soluble vitamins A, D, E, and K. Therefore, it’s important to take a multivitamin 2 hours before or 2 hours after taking orlistat.
However, orlistat can cause steatorrhea, so it’s often not our first choice.
10. Working With Dietitians
I highly recommend that gastroenterologists regularly refer patients to a registered dietitian for medical nutrition therapy. Dietitians help patients establish nutritional goals with calorie limits. I find that many of my patients like the nutritional counseling the dietitians provide, and this can even be done via telemedicine.
A dietitian will examine a patient’s eating habits and help them set weight loss goals that are both realistic and achievable. Having a dietitian motivate a patient through several clinic visits is important for success. A dietitian can plan how many calories a patient should consume in a day while maintaining food, protein, and vitamin intake.
With this therapy, many patients are able to lose approximately 1-1.5 pounds each week. A dietitian can help keep patients accountable for their weight loss goals. I encourage my patients to use their dietitian as a weight loss teacher and a coach who can personalize a diet plan that tastes great.
Some of our patients also have overlapping gastrointestinal issues, such as celiac disease or irritable bowel syndrome. Dietitians can also formulate diets that are great for these other diagnoses too.
There are also apps available on our phones to help with diet and weight loss.
Having a Difficult Conversation to Prevent Long-Term Disease
It’s important for gastroenterologists to work with patients to achieve weight loss. Addressing obesity is sometimes a difficult topic to bring up with patients, but it’s nonetheless very important.
Together, we can help treat obesity plus improve and prevent hepatic steatosis, metabolic dysfunction–associated steatotic liver disease (MASLD), and metabolic dysfunction–associated steatohepatitis (MASH). The estimated global prevalence of MASLD is 32% in adults, so gastroenterologists and hepatologists are working together to try to treat obesity and to prevent long-term liver disease.
Dr. Levy is a gastroenterologist at the University of Chicago. In 2017, Levy, a previous Fulbright Fellow in France, also started a gastroenterology clinic for refugees resettling in Chicago. His clinical projects focus on the development of colorectal cancer screening campaigns. Levy, who recently gave a TEDx Talk about building health education campaigns using music and concerts, organizes Tune It Up: A Concert To Raise Colorectal Cancer Awareness with the American College of Gastroenterology (ACG). He frequently publishes on a variety of gastroenterology topics and serves on ACG’s Public Relations Committee and FDA-Related Matters Committee. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
According to the Centers for Disease Control and Prevention, the obesity prevalence in America was 41.9% between 2017 and 2020. Just 10 years ago, no state had an obesity prevalence above 35%.
Over the past 3 years, many patients gained weight during the COVID-19 pandemic as a result of adopting more sedentary lifestyles, staying at home, avoiding the gym owing to the potential for respiratory spread, and working remotely. For a long time, patients were avoiding attending social events and, as a result, were walking much less.
and other physicians to help patients with obesity realize their goal of achieving weight loss.
1. Embracing the GLP-1 Revolution, With Some Caveats
Glucagon-like peptide-1 (GLP-1) receptor agonists have become a popular treatment for type 2 diabetes and weight loss. These medications, which are given as an injection either weekly or daily depending on the type, have helped patients achieve weight loss with tremendous success.
They work by stimulating the body to produce insulin, which in turn lowers blood sugar. GLP-1 receptor agonists also slow peristalsis and the movement of food from the stomach into the small bowel, which allows patients to eat less by feeling fuller for longer and decreasing hunger.
Two GLP-1 receptor agonists are approved by the US Food and Drug Administration (FDA) for weight loss in patients without diabetes: liraglutide (Saxenda) and semaglutide (Wegovy). There are also lower-dose versions of these active ingredients with the trade names Ozempic and Victoza, designed to help patients with diabetes achieve better glucose and A1c control. In November 2023, the FDA approved a new medication called tirzepatide (Zepbound), which is a glucose-dependent insulinotropic polypeptide (GIP) plus GLP-1 receptor agonist.
This is a very exciting time for the management of type 2 diabetes and weight loss. Gastroenterologists can work with endocrinologists and primary care physicians to help patients choose appropriate weight loss medications.
However, gastroenterologists should also be aware of common GLP-1 receptor agonist side effects, including nausea, vomiting, diarrhea, and — in severe cases — hypoglycemia. These medications can also cause pancreatitis, acute kidney injury, worsening diabetes-related retinopathy, tachycardia, headaches, indigestion, gastroparesis, bowel obstruction, or ileus. We don’t use these medications in patients with a family or personal history of medullary thyroid cancer or multiple endocrine neoplasia. Consider avoiding their use as well in patients with a personal history of pancreatitis.
Recently, the American Society of Anesthesiologists (ASA) suggested holding off on the use of GLP-1 receptor agonists prior to elective endoscopy procedures owing to case reports of aspiration. Gastroenterologists and anesthesiologists are working together to make esophagogastroduodenoscopy (EGD) and colonoscopy as safe as possible in patients taking these treatments.
According to the ASA recommendations, GLP-1 receptor agonists that are given at a daily dose should be held on the day of their procedure. Weekly-dose versions are supposed to be held for 1 week prior to colonoscopy or EGD. During EGD procedures, I also recommend keeping the head of the bed at a 45° angle to help prevent aspiration even further.
Gastroenterologists are eagerly awaiting additional studies to determine whether holding GLP-1 receptor agonists prior to endoscopy is really necessary. But for now, we recommend following the ASA guidelines.
2. Substituting Out Sugary Drinks
Gastroenterologists and primary care physicians constantly advise their patients to avoid consuming sugary drinks, such as soda, fruit juices, calorie-laden coffee drinks, sweetened tea, hot chocolate, and, of course, alcohol. Many of our patients drink three to six of these sugary drinks a day.
As a gastroenterologist, it’s important to counsel our overweight patients and obtain an accurate history about their daily and weekly consumption of excess calories.
Recommend substituting sugary drinks with water, unsweetened tea (either hot or cold), and coffee.
To prevent constipation, encourage patients to drink at least eight 8-ounce glasses of fluid per day. Drinking water, tea, and coffee can also help keep patients feeling fuller for longer and avoid those tempting snacks.
3. Adopting the Right Diet
Every day, I encourage my patients to avoid eating fried fatty foods and processed meats. We also advise patients to avoid junk food filled with carbohydrates and salt.
Instead, patients should try to eat a piece of fruit or some vegetables with every single meal, which keeps patients feeling fuller for longer, prevents diverticulitis from forming, and can even help prevent colon cancer.
Making small dietary changes can dramatically reduce daily calorie consumption, which adds up over time and can help patients lose weight in a safe way.
Meal prepping for the week ahead, perhaps on a Sunday, is a very simple way to eat more nutritious foods instead of constantly getting takeout and fast food.
Many of our patients have also successfully lost weight through intermittent fasting, although I recommend working with a nutritionist on this one.
A Mediterranean diet is also a great option.
4. Getting Active
I encourage patients to take daily walks, swim, play sports, take fitness classes, do yoga or Pilates, and use weights at a gym.
Exercise burns calories, which is great for our hearts, prevents hepatic steatosis, and helps relieve stress. Exercise also stimulates peristalsis, which can help our constipated patients achieve more regular bowel movements.
There are a few other things to keep in mind in this area. Try to avoid strenuous exercise right after eating, because this will help prevent both heartburn and gastroesophageal reflux disease (GERD).
5. Reducing Stomach Volume With a Gastric Balloon
A gastric balloon procedure is a temporary obesity treatment that helps patients lose weight by reducing the volume of the stomach so that they feel full more easily. This can be accomplished endoscopically through the mouth without the need for surgery.
Basically, a deflated balloon is placed through the mouth using an endoscope and advanced into the stomach by a gastroenterologist or surgeon. The balloon is inflated with salt water and can remain in the stomach for 6 months before it is removed.
This procedure can help patients feel full and consequently eat less, thereby leading to gradual and safe weight loss.
6. Using the Accordion Procedure
An endoscopic sleeve gastroplasty procedure, sometimes called an accordion procedure, is used for patients with a body mass index ≥ 30 when diet and exercise alone have failed. An EGD tube is equipped with small stitching instruments that are used to reduce the size of the stomach.
This procedure has less complications than open or laparoscopic surgery and can be reversed.
7. Injecting Botulinum Toxin
Another technique is having the gastroenterologist inject botulinum toxin into the stomach wall. This works by relaxing the stomach propulsion muscles, which delays gastric emptying so that patients feel fuller longer and more easily.
This approach is good for achieving moderate weight loss of approximately 5%-10% of body weight. It works best in combination with a good diet and exercise. The effects of the botulinum toxin can last for 3 months, and the procedure can be repeated every 6 months.
8. Adjusting Certain Lifestyle Factors
Gastroenterologists should also counsel our patients about exercise, stress management, and the importance of sleep to prevent overeating. Self-care is extremely important for patients. Walk, swim, lift weights, and play sports; I personally love basketball and tennis.
I also recommend allocating enough time for sleep each night. At least 7-9 hours of sleep is ideal. Good sleep hygiene can help keep a stable schedule. Create a comfortable bedroom that is free of disruptions like TV watching or playing on your phone or computer.
Gastroenterologists can provide simple instructions to their patients on how to achieve this. For example, unplug from electronics 30-60 minutes prior to sleep. Try also to avoid eating late at night, which will help patients prevent GERD and heartburn symptoms too.
9. Considering Orlistat as an Option
Orlistat is an oral over-the-counter lipase inhibitor that inhibits fat absorption in the intestines. This drug can interfere with the absorption of fat-soluble vitamins A, D, E, and K. Therefore, it’s important to take a multivitamin 2 hours before or 2 hours after taking orlistat.
However, orlistat can cause steatorrhea, so it’s often not our first choice.
10. Working With Dietitians
I highly recommend that gastroenterologists regularly refer patients to a registered dietitian for medical nutrition therapy. Dietitians help patients establish nutritional goals with calorie limits. I find that many of my patients like the nutritional counseling the dietitians provide, and this can even be done via telemedicine.
A dietitian will examine a patient’s eating habits and help them set weight loss goals that are both realistic and achievable. Having a dietitian motivate a patient through several clinic visits is important for success. A dietitian can plan how many calories a patient should consume in a day while maintaining food, protein, and vitamin intake.
With this therapy, many patients are able to lose approximately 1-1.5 pounds each week. A dietitian can help keep patients accountable for their weight loss goals. I encourage my patients to use their dietitian as a weight loss teacher and a coach who can personalize a diet plan that tastes great.
Some of our patients also have overlapping gastrointestinal issues, such as celiac disease or irritable bowel syndrome. Dietitians can also formulate diets that are great for these other diagnoses too.
There are also apps available on our phones to help with diet and weight loss.
Having a Difficult Conversation to Prevent Long-Term Disease
It’s important for gastroenterologists to work with patients to achieve weight loss. Addressing obesity is sometimes a difficult topic to bring up with patients, but it’s nonetheless very important.
Together, we can help treat obesity plus improve and prevent hepatic steatosis, metabolic dysfunction–associated steatotic liver disease (MASLD), and metabolic dysfunction–associated steatohepatitis (MASH). The estimated global prevalence of MASLD is 32% in adults, so gastroenterologists and hepatologists are working together to try to treat obesity and to prevent long-term liver disease.
Dr. Levy is a gastroenterologist at the University of Chicago. In 2017, Levy, a previous Fulbright Fellow in France, also started a gastroenterology clinic for refugees resettling in Chicago. His clinical projects focus on the development of colorectal cancer screening campaigns. Levy, who recently gave a TEDx Talk about building health education campaigns using music and concerts, organizes Tune It Up: A Concert To Raise Colorectal Cancer Awareness with the American College of Gastroenterology (ACG). He frequently publishes on a variety of gastroenterology topics and serves on ACG’s Public Relations Committee and FDA-Related Matters Committee. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Prostate Risks Similar for Testosterone Therapy and Placebo
TOPLINE:
including cancer.
METHODOLOGY:
- Uncertainty and concern exist about a link between prostate cancer risk and testosterone levels. Most professional society guidelines recommend against TRT in men with a history of or an increased risk for prostate cancer.
- The Testosterone Replacement Therapy for Assessment of Long-Term Vascular Events and Efficacy Response in Hypogonadal Men included 5204 men (ages 45-80, 17% Black, 80% White), randomly assigned to receive testosterone gel or placebo.
- Men with a history of cardiovascular disease or increased cardiovascular risk were evaluated to exclude those at increased prostate cancer risk (fasting testosterone < 300 ng/dL, ≥ 1 hypogonadal symptoms).
- The primary prostate safety endpoint was high-grade prostate cancer incidence (Gleason score, ≥ 4 + 3).
- Secondary endpoints were incidences of any prostate cancer, acute urinary retention, invasive procedure for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms.
TAKEAWAY:
- During 14,304 person-years of follow-up, high-grade prostate cancer incidence did not differ significantly between the TRT and placebo (0.19% vs 0.12%; P = .51) groups.
- The incidences of prostate cancer, acute urinary retention, invasive procedures for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms were also similar between the groups.
- TRT did not lead to an increase in lower urinary tract symptoms.
- The increase in prostate-specific antigen (PSA) levels was higher in the TRT group than in the placebo group (P < .001). However, the between-group difference did not widen after 12 months.
IN PRACTICE:
For “clinicians and patients who are considering testosterone replacement therapy for hypogonadism,” wrote the authors, “the study’s findings will facilitate a more informed appraisal of the potential prostate risks of testosterone replacement therapy.”
SOURCE:
Shalender Bhasin, MB, BS, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, led the study. It was published online in JAMA Network Open.
LIMITATIONS:
- The study findings do not apply to men with known prostate cancer or higher PSA values or those without confirmed hypogonadism.
- Although the TRAVERSE study was longer than many contemporary trials, carcinogens may require many years to induce malignant neoplasms.
- The trial’s structured evaluation of men after PSA testing did not include prostate imaging or other biomarker tests, which could affect the decision to perform a biopsy.
DISCLOSURES:
This study was funded by a consortium of testosterone manufacturers led by AbbVie Inc with additional financial support from Endo Pharmaceuticals, Acerus Pharmaceuticals Corp, and Upsher-Smith Laboratories. Mr. Bhasin and two coauthors declared receiving grants, consulting and personal fees, and other ties with pharmaceutical and device companies and other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
including cancer.
METHODOLOGY:
- Uncertainty and concern exist about a link between prostate cancer risk and testosterone levels. Most professional society guidelines recommend against TRT in men with a history of or an increased risk for prostate cancer.
- The Testosterone Replacement Therapy for Assessment of Long-Term Vascular Events and Efficacy Response in Hypogonadal Men included 5204 men (ages 45-80, 17% Black, 80% White), randomly assigned to receive testosterone gel or placebo.
- Men with a history of cardiovascular disease or increased cardiovascular risk were evaluated to exclude those at increased prostate cancer risk (fasting testosterone < 300 ng/dL, ≥ 1 hypogonadal symptoms).
- The primary prostate safety endpoint was high-grade prostate cancer incidence (Gleason score, ≥ 4 + 3).
- Secondary endpoints were incidences of any prostate cancer, acute urinary retention, invasive procedure for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms.
TAKEAWAY:
- During 14,304 person-years of follow-up, high-grade prostate cancer incidence did not differ significantly between the TRT and placebo (0.19% vs 0.12%; P = .51) groups.
- The incidences of prostate cancer, acute urinary retention, invasive procedures for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms were also similar between the groups.
- TRT did not lead to an increase in lower urinary tract symptoms.
- The increase in prostate-specific antigen (PSA) levels was higher in the TRT group than in the placebo group (P < .001). However, the between-group difference did not widen after 12 months.
IN PRACTICE:
For “clinicians and patients who are considering testosterone replacement therapy for hypogonadism,” wrote the authors, “the study’s findings will facilitate a more informed appraisal of the potential prostate risks of testosterone replacement therapy.”
SOURCE:
Shalender Bhasin, MB, BS, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, led the study. It was published online in JAMA Network Open.
LIMITATIONS:
- The study findings do not apply to men with known prostate cancer or higher PSA values or those without confirmed hypogonadism.
- Although the TRAVERSE study was longer than many contemporary trials, carcinogens may require many years to induce malignant neoplasms.
- The trial’s structured evaluation of men after PSA testing did not include prostate imaging or other biomarker tests, which could affect the decision to perform a biopsy.
DISCLOSURES:
This study was funded by a consortium of testosterone manufacturers led by AbbVie Inc with additional financial support from Endo Pharmaceuticals, Acerus Pharmaceuticals Corp, and Upsher-Smith Laboratories. Mr. Bhasin and two coauthors declared receiving grants, consulting and personal fees, and other ties with pharmaceutical and device companies and other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
including cancer.
METHODOLOGY:
- Uncertainty and concern exist about a link between prostate cancer risk and testosterone levels. Most professional society guidelines recommend against TRT in men with a history of or an increased risk for prostate cancer.
- The Testosterone Replacement Therapy for Assessment of Long-Term Vascular Events and Efficacy Response in Hypogonadal Men included 5204 men (ages 45-80, 17% Black, 80% White), randomly assigned to receive testosterone gel or placebo.
- Men with a history of cardiovascular disease or increased cardiovascular risk were evaluated to exclude those at increased prostate cancer risk (fasting testosterone < 300 ng/dL, ≥ 1 hypogonadal symptoms).
- The primary prostate safety endpoint was high-grade prostate cancer incidence (Gleason score, ≥ 4 + 3).
- Secondary endpoints were incidences of any prostate cancer, acute urinary retention, invasive procedure for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms.
TAKEAWAY:
- During 14,304 person-years of follow-up, high-grade prostate cancer incidence did not differ significantly between the TRT and placebo (0.19% vs 0.12%; P = .51) groups.
- The incidences of prostate cancer, acute urinary retention, invasive procedures for benign prostatic hyperplasia, prostate biopsy, and new pharmacologic treatment for lower urinary tract symptoms were also similar between the groups.
- TRT did not lead to an increase in lower urinary tract symptoms.
- The increase in prostate-specific antigen (PSA) levels was higher in the TRT group than in the placebo group (P < .001). However, the between-group difference did not widen after 12 months.
IN PRACTICE:
For “clinicians and patients who are considering testosterone replacement therapy for hypogonadism,” wrote the authors, “the study’s findings will facilitate a more informed appraisal of the potential prostate risks of testosterone replacement therapy.”
SOURCE:
Shalender Bhasin, MB, BS, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, led the study. It was published online in JAMA Network Open.
LIMITATIONS:
- The study findings do not apply to men with known prostate cancer or higher PSA values or those without confirmed hypogonadism.
- Although the TRAVERSE study was longer than many contemporary trials, carcinogens may require many years to induce malignant neoplasms.
- The trial’s structured evaluation of men after PSA testing did not include prostate imaging or other biomarker tests, which could affect the decision to perform a biopsy.
DISCLOSURES:
This study was funded by a consortium of testosterone manufacturers led by AbbVie Inc with additional financial support from Endo Pharmaceuticals, Acerus Pharmaceuticals Corp, and Upsher-Smith Laboratories. Mr. Bhasin and two coauthors declared receiving grants, consulting and personal fees, and other ties with pharmaceutical and device companies and other sources.
A version of this article appeared on Medscape.com.
‘Stop Teaching’ Children It’s Their Fault They’re Fat
The US Preventive Services Task Force (USPSTF) has published draft recommendations that 6-year-olds with obesity be lectured to about diet and exercise.
Never mind that there are no reproducible or scalable studies demonstrating durable and clinically meaningful benefits of this for adults let alone children. Never mind that children are not household decision-makers on matters of grocery shopping, cooking, or exercise. Never mind the corollary that many children so lectured who fail to see an impact on their weight will perceive that as their own personal failures. And of course, never mind that we’re privileged to be in an era with safe, effective, pharmacotherapeutic options for obesity. No. We must teach children it’s their fault if they’re fat. Because ultimately that’s what many of them will learn.
That’s not to say there’s no room for counseling. But with children as young as 6, that counseling should be delivered exclusively to their parents and caregivers. That counseling should focus as much if not more so on the impact of weight bias and the biological basis of obesity rather than diet and exercise, while explicitly teaching parents the means to discuss nutrition without risking their children feeling worse about themselves, increasing the risk for conflict over changes, or heightening their children’s chance of developing eating disorders or maladaptive relationships with food.
But back to the USPSTF’s actual recommendation for those 6 years old and up. They’re recommending “at least” 26 hours of lectures over a year-long interprofessional intervention. Putting aside the reality that this isn’t scalable time-wise or cost-wise to reach even a fraction of the roughly 15 million US children with obesity, there is also the issue of service provision. Because when it comes to obesity, if the intervention is purely educational, even if you want to believe there is a syllabus out there that would have a dramatic impact, its impact will vary wildly depending on the skill and approach of the service providers. This inconvenient truth is also the one that makes it impossible to meaningfully compare program outcomes even when they share the same content.
The USPSTF’s draft recommendations also explicitly avoid what the American Academy of Pediatrics has rightly embraced: the use where appropriate of medications or surgery. While opponents of the use of pharmacotherapy for childhood obesity tend to point to a lack of long-term data as rationale for its denial, something that the USPSTF has done, again, we have long-term data demonstrating a lack of scalable, clinically meaningful efficacy for service only based programs.
Childhood obesity is a flood and its ongoing current is relentless. Given its tremendous impact, especially at its extremes, on both physical and mental health, this is yet another example of systemic weight bias in action — it’s as if the USPSTF is recommending a swimming lesson–only approach while actively fearmongering, despite an absence of plausible mechanistic risk, about the long-term use of life jackets.
Dr. Freedhoff is associate professor, Department of Family Medicine, University of Ottawa; Medical Director, Bariatric Medical Institute, Ottawa, Ontario, Canada. Dr. Freedhoff has disclosed ties with Bariatric Medical Institute, Constant Health, and Novo Nordisk.
A version of this article appeared on Medscape.com.
The US Preventive Services Task Force (USPSTF) has published draft recommendations that 6-year-olds with obesity be lectured to about diet and exercise.
Never mind that there are no reproducible or scalable studies demonstrating durable and clinically meaningful benefits of this for adults let alone children. Never mind that children are not household decision-makers on matters of grocery shopping, cooking, or exercise. Never mind the corollary that many children so lectured who fail to see an impact on their weight will perceive that as their own personal failures. And of course, never mind that we’re privileged to be in an era with safe, effective, pharmacotherapeutic options for obesity. No. We must teach children it’s their fault if they’re fat. Because ultimately that’s what many of them will learn.
That’s not to say there’s no room for counseling. But with children as young as 6, that counseling should be delivered exclusively to their parents and caregivers. That counseling should focus as much if not more so on the impact of weight bias and the biological basis of obesity rather than diet and exercise, while explicitly teaching parents the means to discuss nutrition without risking their children feeling worse about themselves, increasing the risk for conflict over changes, or heightening their children’s chance of developing eating disorders or maladaptive relationships with food.
But back to the USPSTF’s actual recommendation for those 6 years old and up. They’re recommending “at least” 26 hours of lectures over a year-long interprofessional intervention. Putting aside the reality that this isn’t scalable time-wise or cost-wise to reach even a fraction of the roughly 15 million US children with obesity, there is also the issue of service provision. Because when it comes to obesity, if the intervention is purely educational, even if you want to believe there is a syllabus out there that would have a dramatic impact, its impact will vary wildly depending on the skill and approach of the service providers. This inconvenient truth is also the one that makes it impossible to meaningfully compare program outcomes even when they share the same content.
The USPSTF’s draft recommendations also explicitly avoid what the American Academy of Pediatrics has rightly embraced: the use where appropriate of medications or surgery. While opponents of the use of pharmacotherapy for childhood obesity tend to point to a lack of long-term data as rationale for its denial, something that the USPSTF has done, again, we have long-term data demonstrating a lack of scalable, clinically meaningful efficacy for service only based programs.
Childhood obesity is a flood and its ongoing current is relentless. Given its tremendous impact, especially at its extremes, on both physical and mental health, this is yet another example of systemic weight bias in action — it’s as if the USPSTF is recommending a swimming lesson–only approach while actively fearmongering, despite an absence of plausible mechanistic risk, about the long-term use of life jackets.
Dr. Freedhoff is associate professor, Department of Family Medicine, University of Ottawa; Medical Director, Bariatric Medical Institute, Ottawa, Ontario, Canada. Dr. Freedhoff has disclosed ties with Bariatric Medical Institute, Constant Health, and Novo Nordisk.
A version of this article appeared on Medscape.com.
The US Preventive Services Task Force (USPSTF) has published draft recommendations that 6-year-olds with obesity be lectured to about diet and exercise.
Never mind that there are no reproducible or scalable studies demonstrating durable and clinically meaningful benefits of this for adults let alone children. Never mind that children are not household decision-makers on matters of grocery shopping, cooking, or exercise. Never mind the corollary that many children so lectured who fail to see an impact on their weight will perceive that as their own personal failures. And of course, never mind that we’re privileged to be in an era with safe, effective, pharmacotherapeutic options for obesity. No. We must teach children it’s their fault if they’re fat. Because ultimately that’s what many of them will learn.
That’s not to say there’s no room for counseling. But with children as young as 6, that counseling should be delivered exclusively to their parents and caregivers. That counseling should focus as much if not more so on the impact of weight bias and the biological basis of obesity rather than diet and exercise, while explicitly teaching parents the means to discuss nutrition without risking their children feeling worse about themselves, increasing the risk for conflict over changes, or heightening their children’s chance of developing eating disorders or maladaptive relationships with food.
But back to the USPSTF’s actual recommendation for those 6 years old and up. They’re recommending “at least” 26 hours of lectures over a year-long interprofessional intervention. Putting aside the reality that this isn’t scalable time-wise or cost-wise to reach even a fraction of the roughly 15 million US children with obesity, there is also the issue of service provision. Because when it comes to obesity, if the intervention is purely educational, even if you want to believe there is a syllabus out there that would have a dramatic impact, its impact will vary wildly depending on the skill and approach of the service providers. This inconvenient truth is also the one that makes it impossible to meaningfully compare program outcomes even when they share the same content.
The USPSTF’s draft recommendations also explicitly avoid what the American Academy of Pediatrics has rightly embraced: the use where appropriate of medications or surgery. While opponents of the use of pharmacotherapy for childhood obesity tend to point to a lack of long-term data as rationale for its denial, something that the USPSTF has done, again, we have long-term data demonstrating a lack of scalable, clinically meaningful efficacy for service only based programs.
Childhood obesity is a flood and its ongoing current is relentless. Given its tremendous impact, especially at its extremes, on both physical and mental health, this is yet another example of systemic weight bias in action — it’s as if the USPSTF is recommending a swimming lesson–only approach while actively fearmongering, despite an absence of plausible mechanistic risk, about the long-term use of life jackets.
Dr. Freedhoff is associate professor, Department of Family Medicine, University of Ottawa; Medical Director, Bariatric Medical Institute, Ottawa, Ontario, Canada. Dr. Freedhoff has disclosed ties with Bariatric Medical Institute, Constant Health, and Novo Nordisk.
A version of this article appeared on Medscape.com.
EHR Tool Enhances Primary Aldosteronism Screening in Hypertensive Patients
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Oncologists Sound the Alarm About Rise of White Bagging
For years, oncologist John DiPersio, MD, PhD, had faced frustrating encounters with insurers that only cover medications through a process called white bagging.
Instead of the traditional buy-and-bill pathway where oncologists purchase specialty drugs, such as infusion medications, directly from the distributor or manufacturer, white bagging requires physicians to receive these drugs from a specialty pharmacy.
On its face, the differences may seem minor. However, as Dr. DiPersio knows well, the consequences for oncologists and patients are not.
That is why Dr. DiPersio’s cancer center does not allow white bagging.
And when insurers refuse to reconsider the white bagging policy, his cancer team is left with few options.
“Sometimes, we have to redirect patients to other places,” said Dr. DiPersio, a bone marrow transplant specialist at Siteman Cancer Center, Washington University, St. Louis.
In emergency instances where patients cannot wait, Dr. DiPersio’s team will administer their own stock of a drug. In such cases, “we accept the fact that by not allowing white bagging, there may be nonpayment. We take the hit as far as cost.”
Increasingly, white bagging mandates are becoming harder for practices to avoid.
In a 2021 survey, 87% of Association of Community Cancer Centers members said white bagging has become an insurer mandate for some of their patients.
A 2023 analysis from Adam J. Fein, PhD, of Drug Channels Institute, Philadelphia, found that white bagging accounted for 17% of infused oncology product sourcing from clinics and 38% from hospital outpatient departments, up from 15% to 28% in 2019. Another practice called brown bagging, where specialty pharmacies send drugs directly to patients, creates many of the same issues but is much less prevalent than white bagging.
This change reflects “the broader battle over oncology margins” and insurers’ “attempts to shift costs to providers, patients, and manufacturers,” Dr. Fein wrote in his 2023 report.
White Bagging: Who Benefits?
At its core, white bagging changes how drugs are covered and reimbursed. Under buy and bill, drugs fall under a patient’s medical benefit. Oncologists purchase drugs directly from the manufacturer or distributor and receive reimbursement from the insurance company for both the cost of the drug as well as for administering it to patients.
Under white bagging, drugs fall under a patient’s pharmacy benefit. In these instances, a specialty pharmacy prepares the infusion ahead of time and ships it directly to the physician’s office or clinic. Because oncologists do not purchase the drug directly, they cannot bill insurers for it; instead, the pharmacy receives reimbursement for the drug and the provider is reimbursed for administering it.
Insurance companies argue that white bagging reduces patients’ out-of-pocket costs “by preventing hospitals and physicians from charging exorbitant fees to buy and store specialty medicines themselves,” according to advocacy group America’s Health Insurance Plans (AHIP).
Data from AHIP suggested that hospitals mark up the price of cancer drugs considerably, charging about twice as much as a specialty pharmacy, and that physician’s offices also charge about 23% more. However, these figures highlight how much insurers are billed, not necessarily how much patients ultimately pay.
Other evidence shows that white bagging raises costs for patients while reducing reimbursement for oncologists and saving insurance companies money.
A recent analysis in JAMA Network Open, which looked at 50 cancer drugs associated with the highest total spending from the 2020 Medicare Part B, found that mean insurance payments to providers were more than $2000 lower for drugs distributed under bagging than traditional buy and bill: $7405 vs $9547 per patient per month. Investigators found the same pattern in median insurance payments: $5746 vs $6681. Patients also paid more out-of-pocket each month with bagging vs buy and bill: $315 vs $145.
For patients with private insurance, “out-of-pocket costs were higher under bagging practice than the traditional buy-and-bill practice,” said lead author Ya-Chen Tina Shih, PhD, a professor in the department of radiation oncology at UCLA Health, Los Angeles.
White bagging is entirely for the profit of health insurers, specialty pharmacies, and pharmacy benefit managers, the middlemen who negotiate drug prices on behalf of payers.
Many people may not realize the underlying money-making strategies behind white bagging, explained Ted Okon, executive director for Community Oncology Alliance, which opposes the practice. Often, an insurer, pharmacy benefit manager, and mail order pharmacy involved in the process are all affiliated with the same corporation. In such cases, an insurer has a financial motive to control the source of medications and steer business to its affiliated pharmacies, Mr. Okon said.
When a single corporation owns numerous parts of the drug supply chain, insurers end up having “sway over what drug to use and then how the patient is going to get it,” Mr. Okon said. If the specialty pharmacy is a 340B contract pharmacy, it likely also receives a sizable discount on the drug and can make more money through white bagging.
Dangerous to Patients?
On the safety front, proponents of white bagging say the process is safe and efficient.
Specialty pharmacies are used only for prescription drugs that can be safely delivered, said AHIP spokesman David Allen.
In addition to having the same supply chain safety requirements as any other dispensing pharmacy, “specialty pharmacies also must meet additional safety requirements for specialty drugs” to ensure “the safe storage, handling, and dispensing of the drugs,” Mr. Allen explained.
However, oncologists argue that white bagging can be dangerous.
With white bagging, specialty pharmacies send a specified dose to practices, which does not allow practices to source and mix the drug themselves or make essential last-minute dose-related changes — something that happens every day in the clinic, said Debra Patt, MD, PhD, MBA, executive vice president for policy and strategy for Texas Oncology, Dallas.
White bagging also increases the risk for drug contamination, results in drug waste if the medication can’t be used, and can create delays in care.
Essentially, white bagging takes control away from oncologists and makes patient care more unpredictable and complex, explained Dr. Patt, president of the Texas Society of Clinical Oncology, Rockville, Maryland.
Dr. Patt, who does not allow white bagging in her practice, recalled a recent patient with metastatic breast cancer who came to the clinic for trastuzumab deruxtecan. The patient had been experiencing acute abdominal pain. After an exam and CT, Dr. Patt found the breast cancer had grown and moved into the patient’s liver.
“I had to discontinue that plan and change to a different chemotherapy,” she said. “If we had white bagged, that would have been a waste of several thousand dollars. Also, the patient would have to wait for the new medication to be white bagged, a delay that would be at least a week and the patient would have to come back at another time.”
When asked about the safety concerns associated with white bagging, Lemrey “Al” Carter, MS, PharmD, RPh, executive director of the National Association of Boards of Pharmacy (NABP), said the NABP “acknowledges that all these issues exist.
“It is unfortunate if patient care or costs are negatively impacted,” Dr. Carter said, adding that “boards of pharmacy can investigate if they are made aware of safety concerns at the pharmacy level. If a violation of the pharmacy laws or rules is found, boards can take action.”
More Legislation to Prevent Bagging
As white bagging mandates from insurance companies ramp up, more practices and states are banning it.
In the Association of Community Cancer Centers’ 2021 survey, 59% of members said their cancer program or practice does not allow white bagging.
At least 15 states have introduced legislation that restricts and/or prohibits white and brown bagging practices, according to a 2023 report by the Institute for Clinical and Economic Review. Some of the proposed laws would restrict mandates by stipulating that physicians are reimbursed at the contracted amount for clinician-administered drugs, whether obtained from a pharmacy or the manufacturer.
Louisiana, Vermont, and Minnesota were the first to enact anti–white bagging laws. Louisiana’s law, for example, enacted in 2021, bans white bagging and requires insurers to reimburse providers for physician-administered drugs if obtained from out-of-network pharmacies.
When the legislation passed, white bagging was just starting to enter the healthcare market in Louisiana, and the state wanted to act proactively, said Kathy W. Oubre, MS, CEO of the Pontchartrain Cancer Center, Covington, Louisiana, and president of the Coalition of Hematology and Oncology Practices, Mountain View, California.
“We recognized the growing concern around it,” Ms. Oubre said. The state legislature at the time included physicians and pharmacists who “really understood from a practice and patient perspective, the harm that policy could do.”
Ms. Oubre would like to see more legislation in other states and believes Louisiana’s law is a good model.
At the federal level, the American Hospital Association and American Society of Health-System Pharmacists have also urged the US Food and Drug Administration to take appropriate enforcement action to protect patients from white bagging.
Legislation that bars white bagging mandates is the most reasonable way to support timely and appropriate access to cancer care, Dr. Patt said. In the absence of such legislation, she said oncologists can only opt out of insurance contracts that may require the practice.
“That is a difficult position to put oncologists in,” she said.
A version of this article appeared on Medscape.com.
For years, oncologist John DiPersio, MD, PhD, had faced frustrating encounters with insurers that only cover medications through a process called white bagging.
Instead of the traditional buy-and-bill pathway where oncologists purchase specialty drugs, such as infusion medications, directly from the distributor or manufacturer, white bagging requires physicians to receive these drugs from a specialty pharmacy.
On its face, the differences may seem minor. However, as Dr. DiPersio knows well, the consequences for oncologists and patients are not.
That is why Dr. DiPersio’s cancer center does not allow white bagging.
And when insurers refuse to reconsider the white bagging policy, his cancer team is left with few options.
“Sometimes, we have to redirect patients to other places,” said Dr. DiPersio, a bone marrow transplant specialist at Siteman Cancer Center, Washington University, St. Louis.
In emergency instances where patients cannot wait, Dr. DiPersio’s team will administer their own stock of a drug. In such cases, “we accept the fact that by not allowing white bagging, there may be nonpayment. We take the hit as far as cost.”
Increasingly, white bagging mandates are becoming harder for practices to avoid.
In a 2021 survey, 87% of Association of Community Cancer Centers members said white bagging has become an insurer mandate for some of their patients.
A 2023 analysis from Adam J. Fein, PhD, of Drug Channels Institute, Philadelphia, found that white bagging accounted for 17% of infused oncology product sourcing from clinics and 38% from hospital outpatient departments, up from 15% to 28% in 2019. Another practice called brown bagging, where specialty pharmacies send drugs directly to patients, creates many of the same issues but is much less prevalent than white bagging.
This change reflects “the broader battle over oncology margins” and insurers’ “attempts to shift costs to providers, patients, and manufacturers,” Dr. Fein wrote in his 2023 report.
White Bagging: Who Benefits?
At its core, white bagging changes how drugs are covered and reimbursed. Under buy and bill, drugs fall under a patient’s medical benefit. Oncologists purchase drugs directly from the manufacturer or distributor and receive reimbursement from the insurance company for both the cost of the drug as well as for administering it to patients.
Under white bagging, drugs fall under a patient’s pharmacy benefit. In these instances, a specialty pharmacy prepares the infusion ahead of time and ships it directly to the physician’s office or clinic. Because oncologists do not purchase the drug directly, they cannot bill insurers for it; instead, the pharmacy receives reimbursement for the drug and the provider is reimbursed for administering it.
Insurance companies argue that white bagging reduces patients’ out-of-pocket costs “by preventing hospitals and physicians from charging exorbitant fees to buy and store specialty medicines themselves,” according to advocacy group America’s Health Insurance Plans (AHIP).
Data from AHIP suggested that hospitals mark up the price of cancer drugs considerably, charging about twice as much as a specialty pharmacy, and that physician’s offices also charge about 23% more. However, these figures highlight how much insurers are billed, not necessarily how much patients ultimately pay.
Other evidence shows that white bagging raises costs for patients while reducing reimbursement for oncologists and saving insurance companies money.
A recent analysis in JAMA Network Open, which looked at 50 cancer drugs associated with the highest total spending from the 2020 Medicare Part B, found that mean insurance payments to providers were more than $2000 lower for drugs distributed under bagging than traditional buy and bill: $7405 vs $9547 per patient per month. Investigators found the same pattern in median insurance payments: $5746 vs $6681. Patients also paid more out-of-pocket each month with bagging vs buy and bill: $315 vs $145.
For patients with private insurance, “out-of-pocket costs were higher under bagging practice than the traditional buy-and-bill practice,” said lead author Ya-Chen Tina Shih, PhD, a professor in the department of radiation oncology at UCLA Health, Los Angeles.
White bagging is entirely for the profit of health insurers, specialty pharmacies, and pharmacy benefit managers, the middlemen who negotiate drug prices on behalf of payers.
Many people may not realize the underlying money-making strategies behind white bagging, explained Ted Okon, executive director for Community Oncology Alliance, which opposes the practice. Often, an insurer, pharmacy benefit manager, and mail order pharmacy involved in the process are all affiliated with the same corporation. In such cases, an insurer has a financial motive to control the source of medications and steer business to its affiliated pharmacies, Mr. Okon said.
When a single corporation owns numerous parts of the drug supply chain, insurers end up having “sway over what drug to use and then how the patient is going to get it,” Mr. Okon said. If the specialty pharmacy is a 340B contract pharmacy, it likely also receives a sizable discount on the drug and can make more money through white bagging.
Dangerous to Patients?
On the safety front, proponents of white bagging say the process is safe and efficient.
Specialty pharmacies are used only for prescription drugs that can be safely delivered, said AHIP spokesman David Allen.
In addition to having the same supply chain safety requirements as any other dispensing pharmacy, “specialty pharmacies also must meet additional safety requirements for specialty drugs” to ensure “the safe storage, handling, and dispensing of the drugs,” Mr. Allen explained.
However, oncologists argue that white bagging can be dangerous.
With white bagging, specialty pharmacies send a specified dose to practices, which does not allow practices to source and mix the drug themselves or make essential last-minute dose-related changes — something that happens every day in the clinic, said Debra Patt, MD, PhD, MBA, executive vice president for policy and strategy for Texas Oncology, Dallas.
White bagging also increases the risk for drug contamination, results in drug waste if the medication can’t be used, and can create delays in care.
Essentially, white bagging takes control away from oncologists and makes patient care more unpredictable and complex, explained Dr. Patt, president of the Texas Society of Clinical Oncology, Rockville, Maryland.
Dr. Patt, who does not allow white bagging in her practice, recalled a recent patient with metastatic breast cancer who came to the clinic for trastuzumab deruxtecan. The patient had been experiencing acute abdominal pain. After an exam and CT, Dr. Patt found the breast cancer had grown and moved into the patient’s liver.
“I had to discontinue that plan and change to a different chemotherapy,” she said. “If we had white bagged, that would have been a waste of several thousand dollars. Also, the patient would have to wait for the new medication to be white bagged, a delay that would be at least a week and the patient would have to come back at another time.”
When asked about the safety concerns associated with white bagging, Lemrey “Al” Carter, MS, PharmD, RPh, executive director of the National Association of Boards of Pharmacy (NABP), said the NABP “acknowledges that all these issues exist.
“It is unfortunate if patient care or costs are negatively impacted,” Dr. Carter said, adding that “boards of pharmacy can investigate if they are made aware of safety concerns at the pharmacy level. If a violation of the pharmacy laws or rules is found, boards can take action.”
More Legislation to Prevent Bagging
As white bagging mandates from insurance companies ramp up, more practices and states are banning it.
In the Association of Community Cancer Centers’ 2021 survey, 59% of members said their cancer program or practice does not allow white bagging.
At least 15 states have introduced legislation that restricts and/or prohibits white and brown bagging practices, according to a 2023 report by the Institute for Clinical and Economic Review. Some of the proposed laws would restrict mandates by stipulating that physicians are reimbursed at the contracted amount for clinician-administered drugs, whether obtained from a pharmacy or the manufacturer.
Louisiana, Vermont, and Minnesota were the first to enact anti–white bagging laws. Louisiana’s law, for example, enacted in 2021, bans white bagging and requires insurers to reimburse providers for physician-administered drugs if obtained from out-of-network pharmacies.
When the legislation passed, white bagging was just starting to enter the healthcare market in Louisiana, and the state wanted to act proactively, said Kathy W. Oubre, MS, CEO of the Pontchartrain Cancer Center, Covington, Louisiana, and president of the Coalition of Hematology and Oncology Practices, Mountain View, California.
“We recognized the growing concern around it,” Ms. Oubre said. The state legislature at the time included physicians and pharmacists who “really understood from a practice and patient perspective, the harm that policy could do.”
Ms. Oubre would like to see more legislation in other states and believes Louisiana’s law is a good model.
At the federal level, the American Hospital Association and American Society of Health-System Pharmacists have also urged the US Food and Drug Administration to take appropriate enforcement action to protect patients from white bagging.
Legislation that bars white bagging mandates is the most reasonable way to support timely and appropriate access to cancer care, Dr. Patt said. In the absence of such legislation, she said oncologists can only opt out of insurance contracts that may require the practice.
“That is a difficult position to put oncologists in,” she said.
A version of this article appeared on Medscape.com.
For years, oncologist John DiPersio, MD, PhD, had faced frustrating encounters with insurers that only cover medications through a process called white bagging.
Instead of the traditional buy-and-bill pathway where oncologists purchase specialty drugs, such as infusion medications, directly from the distributor or manufacturer, white bagging requires physicians to receive these drugs from a specialty pharmacy.
On its face, the differences may seem minor. However, as Dr. DiPersio knows well, the consequences for oncologists and patients are not.
That is why Dr. DiPersio’s cancer center does not allow white bagging.
And when insurers refuse to reconsider the white bagging policy, his cancer team is left with few options.
“Sometimes, we have to redirect patients to other places,” said Dr. DiPersio, a bone marrow transplant specialist at Siteman Cancer Center, Washington University, St. Louis.
In emergency instances where patients cannot wait, Dr. DiPersio’s team will administer their own stock of a drug. In such cases, “we accept the fact that by not allowing white bagging, there may be nonpayment. We take the hit as far as cost.”
Increasingly, white bagging mandates are becoming harder for practices to avoid.
In a 2021 survey, 87% of Association of Community Cancer Centers members said white bagging has become an insurer mandate for some of their patients.
A 2023 analysis from Adam J. Fein, PhD, of Drug Channels Institute, Philadelphia, found that white bagging accounted for 17% of infused oncology product sourcing from clinics and 38% from hospital outpatient departments, up from 15% to 28% in 2019. Another practice called brown bagging, where specialty pharmacies send drugs directly to patients, creates many of the same issues but is much less prevalent than white bagging.
This change reflects “the broader battle over oncology margins” and insurers’ “attempts to shift costs to providers, patients, and manufacturers,” Dr. Fein wrote in his 2023 report.
White Bagging: Who Benefits?
At its core, white bagging changes how drugs are covered and reimbursed. Under buy and bill, drugs fall under a patient’s medical benefit. Oncologists purchase drugs directly from the manufacturer or distributor and receive reimbursement from the insurance company for both the cost of the drug as well as for administering it to patients.
Under white bagging, drugs fall under a patient’s pharmacy benefit. In these instances, a specialty pharmacy prepares the infusion ahead of time and ships it directly to the physician’s office or clinic. Because oncologists do not purchase the drug directly, they cannot bill insurers for it; instead, the pharmacy receives reimbursement for the drug and the provider is reimbursed for administering it.
Insurance companies argue that white bagging reduces patients’ out-of-pocket costs “by preventing hospitals and physicians from charging exorbitant fees to buy and store specialty medicines themselves,” according to advocacy group America’s Health Insurance Plans (AHIP).
Data from AHIP suggested that hospitals mark up the price of cancer drugs considerably, charging about twice as much as a specialty pharmacy, and that physician’s offices also charge about 23% more. However, these figures highlight how much insurers are billed, not necessarily how much patients ultimately pay.
Other evidence shows that white bagging raises costs for patients while reducing reimbursement for oncologists and saving insurance companies money.
A recent analysis in JAMA Network Open, which looked at 50 cancer drugs associated with the highest total spending from the 2020 Medicare Part B, found that mean insurance payments to providers were more than $2000 lower for drugs distributed under bagging than traditional buy and bill: $7405 vs $9547 per patient per month. Investigators found the same pattern in median insurance payments: $5746 vs $6681. Patients also paid more out-of-pocket each month with bagging vs buy and bill: $315 vs $145.
For patients with private insurance, “out-of-pocket costs were higher under bagging practice than the traditional buy-and-bill practice,” said lead author Ya-Chen Tina Shih, PhD, a professor in the department of radiation oncology at UCLA Health, Los Angeles.
White bagging is entirely for the profit of health insurers, specialty pharmacies, and pharmacy benefit managers, the middlemen who negotiate drug prices on behalf of payers.
Many people may not realize the underlying money-making strategies behind white bagging, explained Ted Okon, executive director for Community Oncology Alliance, which opposes the practice. Often, an insurer, pharmacy benefit manager, and mail order pharmacy involved in the process are all affiliated with the same corporation. In such cases, an insurer has a financial motive to control the source of medications and steer business to its affiliated pharmacies, Mr. Okon said.
When a single corporation owns numerous parts of the drug supply chain, insurers end up having “sway over what drug to use and then how the patient is going to get it,” Mr. Okon said. If the specialty pharmacy is a 340B contract pharmacy, it likely also receives a sizable discount on the drug and can make more money through white bagging.
Dangerous to Patients?
On the safety front, proponents of white bagging say the process is safe and efficient.
Specialty pharmacies are used only for prescription drugs that can be safely delivered, said AHIP spokesman David Allen.
In addition to having the same supply chain safety requirements as any other dispensing pharmacy, “specialty pharmacies also must meet additional safety requirements for specialty drugs” to ensure “the safe storage, handling, and dispensing of the drugs,” Mr. Allen explained.
However, oncologists argue that white bagging can be dangerous.
With white bagging, specialty pharmacies send a specified dose to practices, which does not allow practices to source and mix the drug themselves or make essential last-minute dose-related changes — something that happens every day in the clinic, said Debra Patt, MD, PhD, MBA, executive vice president for policy and strategy for Texas Oncology, Dallas.
White bagging also increases the risk for drug contamination, results in drug waste if the medication can’t be used, and can create delays in care.
Essentially, white bagging takes control away from oncologists and makes patient care more unpredictable and complex, explained Dr. Patt, president of the Texas Society of Clinical Oncology, Rockville, Maryland.
Dr. Patt, who does not allow white bagging in her practice, recalled a recent patient with metastatic breast cancer who came to the clinic for trastuzumab deruxtecan. The patient had been experiencing acute abdominal pain. After an exam and CT, Dr. Patt found the breast cancer had grown and moved into the patient’s liver.
“I had to discontinue that plan and change to a different chemotherapy,” she said. “If we had white bagged, that would have been a waste of several thousand dollars. Also, the patient would have to wait for the new medication to be white bagged, a delay that would be at least a week and the patient would have to come back at another time.”
When asked about the safety concerns associated with white bagging, Lemrey “Al” Carter, MS, PharmD, RPh, executive director of the National Association of Boards of Pharmacy (NABP), said the NABP “acknowledges that all these issues exist.
“It is unfortunate if patient care or costs are negatively impacted,” Dr. Carter said, adding that “boards of pharmacy can investigate if they are made aware of safety concerns at the pharmacy level. If a violation of the pharmacy laws or rules is found, boards can take action.”
More Legislation to Prevent Bagging
As white bagging mandates from insurance companies ramp up, more practices and states are banning it.
In the Association of Community Cancer Centers’ 2021 survey, 59% of members said their cancer program or practice does not allow white bagging.
At least 15 states have introduced legislation that restricts and/or prohibits white and brown bagging practices, according to a 2023 report by the Institute for Clinical and Economic Review. Some of the proposed laws would restrict mandates by stipulating that physicians are reimbursed at the contracted amount for clinician-administered drugs, whether obtained from a pharmacy or the manufacturer.
Louisiana, Vermont, and Minnesota were the first to enact anti–white bagging laws. Louisiana’s law, for example, enacted in 2021, bans white bagging and requires insurers to reimburse providers for physician-administered drugs if obtained from out-of-network pharmacies.
When the legislation passed, white bagging was just starting to enter the healthcare market in Louisiana, and the state wanted to act proactively, said Kathy W. Oubre, MS, CEO of the Pontchartrain Cancer Center, Covington, Louisiana, and president of the Coalition of Hematology and Oncology Practices, Mountain View, California.
“We recognized the growing concern around it,” Ms. Oubre said. The state legislature at the time included physicians and pharmacists who “really understood from a practice and patient perspective, the harm that policy could do.”
Ms. Oubre would like to see more legislation in other states and believes Louisiana’s law is a good model.
At the federal level, the American Hospital Association and American Society of Health-System Pharmacists have also urged the US Food and Drug Administration to take appropriate enforcement action to protect patients from white bagging.
Legislation that bars white bagging mandates is the most reasonable way to support timely and appropriate access to cancer care, Dr. Patt said. In the absence of such legislation, she said oncologists can only opt out of insurance contracts that may require the practice.
“That is a difficult position to put oncologists in,” she said.
A version of this article appeared on Medscape.com.