User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Dapagliflozin’s T2D renal protection extends to ‘fast decline’ of eGFR
Treatment of patients with type 2 diabetes with the SGLT2 inhibitor dapagliflozin led to a significant drop in the occurrence of ‘fast decline’ of renal function in more than 15,000 patients enrolled in the drug’s main cardiovascular outcome trial, another example of the potent renal protective effects of agents from this drug class.

Among patients with type 2 diabetes enrolled in the DECLARE-TIMI 58 trial, the incidence of a fast decline in renal function, defined as a drop in estimated glomerular filtration rate (eGFR) of at least 3 mL/min per 1.73 m2, was 27% among patients treated with dapagliflozin and 37% in control patients who received placebo, a statistically significant difference for this post-hoc analysis, Itamar Raz, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
This finding, which adds to a long list of other renal function parameters reported to have been improved by treatment with sodium-glucose cotransporter 2 (SGLT2) inhibitors, “emphasizes the value of SGLT2 inhibitors as an important component of both prevention and treatment of chronic kidney disease among patients with type 2 diabetes,” said Dr. Raz, a diabetes researcher and professor of medicine at Hadassah University Hospital in Jerusalem.
The primary, prespecified renal outcomes in DECLARE-TIMI 58 were a cardiorenal composite outcome of sustained decline of at least 40% in eGFR to less than 60 mL/min per 1.73 m2, end-stage renal disease (defined as dialysis for at least 90 days, kidney transplantation, or confirmed sustained eGFR of less than 15 mL/min per 1.73 m2), or death from renal or cardiovascular causes; and a second prespecified renal-specific composite outcome that was the same except for excluding death from cardiovascular causes. The results showed that the cardiorenal outcome dropped by a statistically significant 24% with dapagliflozin treatment relative to control patients, and the renal-specific outcome fell by a statistically significant 47% with dapagliflozin relative to control patients (Lancet Diab Endocrinol. 2019 Aug 1;7[8];606-17).

The new findings on the incidence of fast decline in renal function help to further flesh out the scope of renal benefit exerted by SGLT2 inhibitors like dapagliflozin in patients with type 2 diabetes, said experts. Fast decline is a relatively recently devised measure of a high-risk, precipitous loss of renal function that has been defined as a drop of either 3 or 5 mL/min per 1.73 m2 per year (Kidney Int. 2017 Jun;91[6]:1300-11); for this analysis Dr. Raz and his associates used the less stringent definition.
Finding and treating ‘fast decliners’
The new report from Dr. Raz “confirms the original [renal] findings and looks to expand them to a particularly high risk group: the fast decliners,” commented Robert A. Gabbay, MD, chief science & medical officer of the ADA. “In some ways, the group of patients that we need to find a better treatment for most are those whose GFR declines quickly. We don’t always know who they are until after the fact, and studies have been looking for markers that might prospectively identify them,” he said in an interview.
The new analysis showed that dapagliflozin “was effective in this subgroup of patients. Furthermore, it didn’t matter if they had significant baseline disease or not. Even people with normal kidney function [at baseline] who were still fast decliners fared better with the drug than without it. This suggests that, if it can be confirmed in a prospective study, dapagliflozin might be effective very early in the course of treatment if we can identify who will be the fast decliners.”
Dr. Raz and his associates had the data necessary to calculate the rates of eGFR decline during the full follow-up period for 15,012 of the 17,160 patients enrolled in DECLARE-TIMI 58, and they found that 4,788 (32%) were fast decliners and 10,224 had a slower rate of renal deterioration. The average annual decline in eGFR during the period from 6 months after study entry through 4 years was 6.3 mL/min per 1.73 m2 per year (median of 5.1 mL/min per 1.73 m2 per year) among the fast decliners, and zero (median of 0.6 mL/min per 1.73 m2 per year) among the other patients.
Overcoming dapagliflozin’s initial eGFR reduction
The researchers focused on the 6-month to 4-year period of treatment as more representative of the impact of dapagliflozin because the SGLT2 inhibitors have an established pattern of triggering an initial, moderate decline in eGFR over roughly the first 6 months on the drug, which is similar to what happens to patients who start treatment with an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker.

“Some patients get as much as a 10% decline in eGFR” when SGLT2 inhibitor treatment starts, but “patients do better over time even with this initial hit,” the same way they do on drugs that act on the renin-angiotensin system, explained Silvio E. Inzucchi, MD, an endocrinologist and professor of medicine at Yale University in New Haven who has extensively studied the SGLT2 inhibitors.
The analyses reported by Dr. Raz showed that the protection against fast decline during the 6-month to 4-year period with dapagliflozin treatment was consistent across a range of patient subgroups regardless of age, duration of their type 2 diabetes, their baseline level of hyperglycemia, and their baseline eGFR. Nearly half the patients enrolled in DECLARE-TIMI 58 had an eGFR at baseline of at least 91 mL/min per 1.73 m2 and in this subgroup the incidence of fast decliners was 23% with dapagliflozin and 31% on placebo. Among the 45% of patients who began with an eGFR of 60-90 mL/min per 1.73 m2 the fast-decliner incidence was 32% and 43% when on or off dapagliflozin. Among the 7% of patients who entered with an eGFR below 60 mL/min per 1.73 m2, the fast-decliner incidence was 25% on dapagliflozin and 36% among controls. All the between-group differences were statistically significant.
The incidence of fast decliners was also lower with dapagliflozin treatment when the analysis included the entire first 4 years on treatment, including the first 6 months when SGLT2s usually spikes a loss of renal function. For the entire 4-year period, fast decline occurred among 34% of patients on dapagliflozin and in 37% of control patients, a statistically significant difference.
The mechanisms behind the consistent renal-protective effects of the SGLT2 inhibitors remain unclear right now, but likely seem related to the “perfect” diuretic action the drugs produce, said Dr. Inzucchi. “They’re not as hugely effective as diuretics, but they’re gentler.” While the SGLT2 inhibitors cause a modest amount of fluid loss ”for some reason they don’t activate the compensatory mechanisms that prevent further reductions in plasma volume,” a property that manifests as little or no change in catecholamines or renin-angiotensin activity, which sets this diuretic action apart from what happens with conventional diuretic drugs, he said in an interview.
In DECLARE-TIMI 58 treatment with dapagliflozin met its primary safety outcome of noninferiority to placebo with respect to major adverse cardiovascular events. The results failed to show statistically significant superiority for one of the primary efficacy endpoints, the rate of major adverse coronary events, but they did show significantly better performance for the second primary efficacy outcome of the rate of cardiovascular death or hospitalization for heart failure, which occurred in 4.9% of patients treated with dapagliflozin and in 5.8% of the control patients during a median follow-up of 4.2 years (N Engl J Med. 2019 Jan 24;380[4]:347-57).
DECLARE-TIMI 58 was sponsored by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. Raz has been an advisor to and speaker on behalf of AstraZeneca as well as several other companies. Dr. Gabbay had no relevant disclosures. Dr. Inzucchi has been a consultant to AstraZeneca, and also to Abbott, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics.
SOURCE: Raz I et al. ADA 2020, Abstract 303-OR.
Treatment of patients with type 2 diabetes with the SGLT2 inhibitor dapagliflozin led to a significant drop in the occurrence of ‘fast decline’ of renal function in more than 15,000 patients enrolled in the drug’s main cardiovascular outcome trial, another example of the potent renal protective effects of agents from this drug class.
Among patients with type 2 diabetes enrolled in the DECLARE-TIMI 58 trial, the incidence of a fast decline in renal function, defined as a drop in estimated glomerular filtration rate (eGFR) of at least 3 mL/min per 1.73 m2, was 27% among patients treated with dapagliflozin and 37% in control patients who received placebo, a statistically significant difference for this post-hoc analysis, Itamar Raz, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
This finding, which adds to a long list of other renal function parameters reported to have been improved by treatment with sodium-glucose cotransporter 2 (SGLT2) inhibitors, “emphasizes the value of SGLT2 inhibitors as an important component of both prevention and treatment of chronic kidney disease among patients with type 2 diabetes,” said Dr. Raz, a diabetes researcher and professor of medicine at Hadassah University Hospital in Jerusalem.
The primary, prespecified renal outcomes in DECLARE-TIMI 58 were a cardiorenal composite outcome of sustained decline of at least 40% in eGFR to less than 60 mL/min per 1.73 m2, end-stage renal disease (defined as dialysis for at least 90 days, kidney transplantation, or confirmed sustained eGFR of less than 15 mL/min per 1.73 m2), or death from renal or cardiovascular causes; and a second prespecified renal-specific composite outcome that was the same except for excluding death from cardiovascular causes. The results showed that the cardiorenal outcome dropped by a statistically significant 24% with dapagliflozin treatment relative to control patients, and the renal-specific outcome fell by a statistically significant 47% with dapagliflozin relative to control patients (Lancet Diab Endocrinol. 2019 Aug 1;7[8];606-17).
The new findings on the incidence of fast decline in renal function help to further flesh out the scope of renal benefit exerted by SGLT2 inhibitors like dapagliflozin in patients with type 2 diabetes, said experts. Fast decline is a relatively recently devised measure of a high-risk, precipitous loss of renal function that has been defined as a drop of either 3 or 5 mL/min per 1.73 m2 per year (Kidney Int. 2017 Jun;91[6]:1300-11); for this analysis Dr. Raz and his associates used the less stringent definition.
Finding and treating ‘fast decliners’
The new report from Dr. Raz “confirms the original [renal] findings and looks to expand them to a particularly high risk group: the fast decliners,” commented Robert A. Gabbay, MD, chief science & medical officer of the ADA. “In some ways, the group of patients that we need to find a better treatment for most are those whose GFR declines quickly. We don’t always know who they are until after the fact, and studies have been looking for markers that might prospectively identify them,” he said in an interview.
The new analysis showed that dapagliflozin “was effective in this subgroup of patients. Furthermore, it didn’t matter if they had significant baseline disease or not. Even people with normal kidney function [at baseline] who were still fast decliners fared better with the drug than without it. This suggests that, if it can be confirmed in a prospective study, dapagliflozin might be effective very early in the course of treatment if we can identify who will be the fast decliners.”
Dr. Raz and his associates had the data necessary to calculate the rates of eGFR decline during the full follow-up period for 15,012 of the 17,160 patients enrolled in DECLARE-TIMI 58, and they found that 4,788 (32%) were fast decliners and 10,224 had a slower rate of renal deterioration. The average annual decline in eGFR during the period from 6 months after study entry through 4 years was 6.3 mL/min per 1.73 m2 per year (median of 5.1 mL/min per 1.73 m2 per year) among the fast decliners, and zero (median of 0.6 mL/min per 1.73 m2 per year) among the other patients.
Overcoming dapagliflozin’s initial eGFR reduction
The researchers focused on the 6-month to 4-year period of treatment as more representative of the impact of dapagliflozin because the SGLT2 inhibitors have an established pattern of triggering an initial, moderate decline in eGFR over roughly the first 6 months on the drug, which is similar to what happens to patients who start treatment with an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker.
“Some patients get as much as a 10% decline in eGFR” when SGLT2 inhibitor treatment starts, but “patients do better over time even with this initial hit,” the same way they do on drugs that act on the renin-angiotensin system, explained Silvio E. Inzucchi, MD, an endocrinologist and professor of medicine at Yale University in New Haven who has extensively studied the SGLT2 inhibitors.
The analyses reported by Dr. Raz showed that the protection against fast decline during the 6-month to 4-year period with dapagliflozin treatment was consistent across a range of patient subgroups regardless of age, duration of their type 2 diabetes, their baseline level of hyperglycemia, and their baseline eGFR. Nearly half the patients enrolled in DECLARE-TIMI 58 had an eGFR at baseline of at least 91 mL/min per 1.73 m2 and in this subgroup the incidence of fast decliners was 23% with dapagliflozin and 31% on placebo. Among the 45% of patients who began with an eGFR of 60-90 mL/min per 1.73 m2 the fast-decliner incidence was 32% and 43% when on or off dapagliflozin. Among the 7% of patients who entered with an eGFR below 60 mL/min per 1.73 m2, the fast-decliner incidence was 25% on dapagliflozin and 36% among controls. All the between-group differences were statistically significant.
The incidence of fast decliners was also lower with dapagliflozin treatment when the analysis included the entire first 4 years on treatment, including the first 6 months when SGLT2s usually spikes a loss of renal function. For the entire 4-year period, fast decline occurred among 34% of patients on dapagliflozin and in 37% of control patients, a statistically significant difference.
The mechanisms behind the consistent renal-protective effects of the SGLT2 inhibitors remain unclear right now, but likely seem related to the “perfect” diuretic action the drugs produce, said Dr. Inzucchi. “They’re not as hugely effective as diuretics, but they’re gentler.” While the SGLT2 inhibitors cause a modest amount of fluid loss ”for some reason they don’t activate the compensatory mechanisms that prevent further reductions in plasma volume,” a property that manifests as little or no change in catecholamines or renin-angiotensin activity, which sets this diuretic action apart from what happens with conventional diuretic drugs, he said in an interview.
In DECLARE-TIMI 58 treatment with dapagliflozin met its primary safety outcome of noninferiority to placebo with respect to major adverse cardiovascular events. The results failed to show statistically significant superiority for one of the primary efficacy endpoints, the rate of major adverse coronary events, but they did show significantly better performance for the second primary efficacy outcome of the rate of cardiovascular death or hospitalization for heart failure, which occurred in 4.9% of patients treated with dapagliflozin and in 5.8% of the control patients during a median follow-up of 4.2 years (N Engl J Med. 2019 Jan 24;380[4]:347-57).
DECLARE-TIMI 58 was sponsored by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. Raz has been an advisor to and speaker on behalf of AstraZeneca as well as several other companies. Dr. Gabbay had no relevant disclosures. Dr. Inzucchi has been a consultant to AstraZeneca, and also to Abbott, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics.
SOURCE: Raz I et al. ADA 2020, Abstract 303-OR.
Treatment of patients with type 2 diabetes with the SGLT2 inhibitor dapagliflozin led to a significant drop in the occurrence of ‘fast decline’ of renal function in more than 15,000 patients enrolled in the drug’s main cardiovascular outcome trial, another example of the potent renal protective effects of agents from this drug class.
Among patients with type 2 diabetes enrolled in the DECLARE-TIMI 58 trial, the incidence of a fast decline in renal function, defined as a drop in estimated glomerular filtration rate (eGFR) of at least 3 mL/min per 1.73 m2, was 27% among patients treated with dapagliflozin and 37% in control patients who received placebo, a statistically significant difference for this post-hoc analysis, Itamar Raz, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
This finding, which adds to a long list of other renal function parameters reported to have been improved by treatment with sodium-glucose cotransporter 2 (SGLT2) inhibitors, “emphasizes the value of SGLT2 inhibitors as an important component of both prevention and treatment of chronic kidney disease among patients with type 2 diabetes,” said Dr. Raz, a diabetes researcher and professor of medicine at Hadassah University Hospital in Jerusalem.
The primary, prespecified renal outcomes in DECLARE-TIMI 58 were a cardiorenal composite outcome of sustained decline of at least 40% in eGFR to less than 60 mL/min per 1.73 m2, end-stage renal disease (defined as dialysis for at least 90 days, kidney transplantation, or confirmed sustained eGFR of less than 15 mL/min per 1.73 m2), or death from renal or cardiovascular causes; and a second prespecified renal-specific composite outcome that was the same except for excluding death from cardiovascular causes. The results showed that the cardiorenal outcome dropped by a statistically significant 24% with dapagliflozin treatment relative to control patients, and the renal-specific outcome fell by a statistically significant 47% with dapagliflozin relative to control patients (Lancet Diab Endocrinol. 2019 Aug 1;7[8];606-17).
The new findings on the incidence of fast decline in renal function help to further flesh out the scope of renal benefit exerted by SGLT2 inhibitors like dapagliflozin in patients with type 2 diabetes, said experts. Fast decline is a relatively recently devised measure of a high-risk, precipitous loss of renal function that has been defined as a drop of either 3 or 5 mL/min per 1.73 m2 per year (Kidney Int. 2017 Jun;91[6]:1300-11); for this analysis Dr. Raz and his associates used the less stringent definition.
Finding and treating ‘fast decliners’
The new report from Dr. Raz “confirms the original [renal] findings and looks to expand them to a particularly high risk group: the fast decliners,” commented Robert A. Gabbay, MD, chief science & medical officer of the ADA. “In some ways, the group of patients that we need to find a better treatment for most are those whose GFR declines quickly. We don’t always know who they are until after the fact, and studies have been looking for markers that might prospectively identify them,” he said in an interview.
The new analysis showed that dapagliflozin “was effective in this subgroup of patients. Furthermore, it didn’t matter if they had significant baseline disease or not. Even people with normal kidney function [at baseline] who were still fast decliners fared better with the drug than without it. This suggests that, if it can be confirmed in a prospective study, dapagliflozin might be effective very early in the course of treatment if we can identify who will be the fast decliners.”
Dr. Raz and his associates had the data necessary to calculate the rates of eGFR decline during the full follow-up period for 15,012 of the 17,160 patients enrolled in DECLARE-TIMI 58, and they found that 4,788 (32%) were fast decliners and 10,224 had a slower rate of renal deterioration. The average annual decline in eGFR during the period from 6 months after study entry through 4 years was 6.3 mL/min per 1.73 m2 per year (median of 5.1 mL/min per 1.73 m2 per year) among the fast decliners, and zero (median of 0.6 mL/min per 1.73 m2 per year) among the other patients.
Overcoming dapagliflozin’s initial eGFR reduction
The researchers focused on the 6-month to 4-year period of treatment as more representative of the impact of dapagliflozin because the SGLT2 inhibitors have an established pattern of triggering an initial, moderate decline in eGFR over roughly the first 6 months on the drug, which is similar to what happens to patients who start treatment with an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker.
“Some patients get as much as a 10% decline in eGFR” when SGLT2 inhibitor treatment starts, but “patients do better over time even with this initial hit,” the same way they do on drugs that act on the renin-angiotensin system, explained Silvio E. Inzucchi, MD, an endocrinologist and professor of medicine at Yale University in New Haven who has extensively studied the SGLT2 inhibitors.
The analyses reported by Dr. Raz showed that the protection against fast decline during the 6-month to 4-year period with dapagliflozin treatment was consistent across a range of patient subgroups regardless of age, duration of their type 2 diabetes, their baseline level of hyperglycemia, and their baseline eGFR. Nearly half the patients enrolled in DECLARE-TIMI 58 had an eGFR at baseline of at least 91 mL/min per 1.73 m2 and in this subgroup the incidence of fast decliners was 23% with dapagliflozin and 31% on placebo. Among the 45% of patients who began with an eGFR of 60-90 mL/min per 1.73 m2 the fast-decliner incidence was 32% and 43% when on or off dapagliflozin. Among the 7% of patients who entered with an eGFR below 60 mL/min per 1.73 m2, the fast-decliner incidence was 25% on dapagliflozin and 36% among controls. All the between-group differences were statistically significant.
The incidence of fast decliners was also lower with dapagliflozin treatment when the analysis included the entire first 4 years on treatment, including the first 6 months when SGLT2s usually spikes a loss of renal function. For the entire 4-year period, fast decline occurred among 34% of patients on dapagliflozin and in 37% of control patients, a statistically significant difference.
The mechanisms behind the consistent renal-protective effects of the SGLT2 inhibitors remain unclear right now, but likely seem related to the “perfect” diuretic action the drugs produce, said Dr. Inzucchi. “They’re not as hugely effective as diuretics, but they’re gentler.” While the SGLT2 inhibitors cause a modest amount of fluid loss ”for some reason they don’t activate the compensatory mechanisms that prevent further reductions in plasma volume,” a property that manifests as little or no change in catecholamines or renin-angiotensin activity, which sets this diuretic action apart from what happens with conventional diuretic drugs, he said in an interview.
In DECLARE-TIMI 58 treatment with dapagliflozin met its primary safety outcome of noninferiority to placebo with respect to major adverse cardiovascular events. The results failed to show statistically significant superiority for one of the primary efficacy endpoints, the rate of major adverse coronary events, but they did show significantly better performance for the second primary efficacy outcome of the rate of cardiovascular death or hospitalization for heart failure, which occurred in 4.9% of patients treated with dapagliflozin and in 5.8% of the control patients during a median follow-up of 4.2 years (N Engl J Med. 2019 Jan 24;380[4]:347-57).
DECLARE-TIMI 58 was sponsored by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. Raz has been an advisor to and speaker on behalf of AstraZeneca as well as several other companies. Dr. Gabbay had no relevant disclosures. Dr. Inzucchi has been a consultant to AstraZeneca, and also to Abbott, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics.
SOURCE: Raz I et al. ADA 2020, Abstract 303-OR.
FROM ADA 2020

Examining bias
I have an automatic preference for white people over black people. This isn’t my opinion; rather, it is my implicit bias test result. I didn’t believe it at first. Trying hard to not be biased, I took the test again and received the same outcome. My reaction – disbelief – is typical for those like me: White people who believe they are good human beings.

We’ve all watched in horror the acts of violence against blacks in the news. I was shocked and disgusted. It was easy to believe, however, that I am in no way complicit in the injustice and racism I was watching. I think I’m fair and without prejudice. I have never intentionally discriminated against someone. Wanting to help, I listened to my black colleagues, staff, and patients. What I learned made me uncomfortable.
Through all this news, I’d said little to my colleagues and friends. I cannot identify with how a black person has felt recently. What if I said the wrong thing or caused offense? The safe option is to say nothing. I learned that this is a common reaction and the least helpful. The advice from one black colleague was simple: “Just ask us.” Instead of ignoring the issue, she advised me to say: “I wonder what this experience has been like for you. Would you like to share?” And, if you mean it, to add, “I stand with you.” The latter should be followed by “What can I do to help?” Or, more powerfully, “What have I done that makes me complicit?”
Some of these conversations will be uncomfortable. If you want to help, then sit with that. Feeling uncomfortable might mean you are beginning to understand.
I also heard about the excellent book “White Fragility,” by Robin DiAngelo, PhD. In it, she argues that it is difficult for white people to talk about racism because of a tendency to react with defensiveness, guilt, and sometimes anger.
Many of the chapters in the book were easy to read because they didn’t apply to me: I don’t get angry in equity, inclusion, and diversity meetings. I don’t resent affirmative action programs. But then Dr. DiAngelo got me: I believed because I’m a good person and I have no intention of being racist, I’m absolved. Her argument was enlightening. Like all white people in the United States, I have benefited from white privilege. Yes, I’ve worked hard, but I also grew up in a white family with a college-educated father. That alone afforded me academic and financial advantages, which pushed me ahead. I’ve benefited from the status quo.
I have also failed to speak up when white friends carried on about how unnecessary affirmative action programs have become. I’ve sat with sealed lips when I’ve heard comments like “As a white male, it’s a lot harder to get into prestigious schools now.” Having no intention to harm doesn’t matter; plenty of harm is done unintentionally.
I also believed that because I have good intentions, I have no racial bias. I was wrong. The test I took online is an excellent tool to combat this blind spot. It was created by Harvard researchers and is available to everyone: Take a Test. It asks you to categorize faces as good or bad and records your tiny reaction times. Based on these and other questions, it provides feedback on your personal biases.
I was surprised that I have an implicit preference for white people over black people. That’s the point. Most of us are unaware of our biases and falsely believe we are free of them. I encourage you to take the test and learn about yourself. If the result makes you uncomfortable, then sit with it. Try not to be defensive, as I was, and accept that, even if you are a good person, you can become a better one.
Based on what I’ve learned and heard in the last few weeks, I’ve committed to a few things: To acknowledge the harm done to my black and brown colleagues and my complicity even by acts of omission. To not avoid uncomfortable feelings or uncomfortable conversations. As a leader, to use my organizational status to advocate. To stand by my partners of color not only in dramatic one-time marches but also against the everyday perpetrators of microaggressions. To create a safe space and invite my colleagues, staff, friends, and patients to share.
Standing up against racism is all our responsibility. As Dr. Martin Luther King Jr. reminds us: “In the end, we will remember not the words of our enemies, but the silence of our friends.”
Dr. Benabio is director of healthcare transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. He has no disclosures related to this column. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
I have an automatic preference for white people over black people. This isn’t my opinion; rather, it is my implicit bias test result. I didn’t believe it at first. Trying hard to not be biased, I took the test again and received the same outcome. My reaction – disbelief – is typical for those like me: White people who believe they are good human beings.
We’ve all watched in horror the acts of violence against blacks in the news. I was shocked and disgusted. It was easy to believe, however, that I am in no way complicit in the injustice and racism I was watching. I think I’m fair and without prejudice. I have never intentionally discriminated against someone. Wanting to help, I listened to my black colleagues, staff, and patients. What I learned made me uncomfortable.
Through all this news, I’d said little to my colleagues and friends. I cannot identify with how a black person has felt recently. What if I said the wrong thing or caused offense? The safe option is to say nothing. I learned that this is a common reaction and the least helpful. The advice from one black colleague was simple: “Just ask us.” Instead of ignoring the issue, she advised me to say: “I wonder what this experience has been like for you. Would you like to share?” And, if you mean it, to add, “I stand with you.” The latter should be followed by “What can I do to help?” Or, more powerfully, “What have I done that makes me complicit?”
Some of these conversations will be uncomfortable. If you want to help, then sit with that. Feeling uncomfortable might mean you are beginning to understand.
I also heard about the excellent book “White Fragility,” by Robin DiAngelo, PhD. In it, she argues that it is difficult for white people to talk about racism because of a tendency to react with defensiveness, guilt, and sometimes anger.
Many of the chapters in the book were easy to read because they didn’t apply to me: I don’t get angry in equity, inclusion, and diversity meetings. I don’t resent affirmative action programs. But then Dr. DiAngelo got me: I believed because I’m a good person and I have no intention of being racist, I’m absolved. Her argument was enlightening. Like all white people in the United States, I have benefited from white privilege. Yes, I’ve worked hard, but I also grew up in a white family with a college-educated father. That alone afforded me academic and financial advantages, which pushed me ahead. I’ve benefited from the status quo.
I have also failed to speak up when white friends carried on about how unnecessary affirmative action programs have become. I’ve sat with sealed lips when I’ve heard comments like “As a white male, it’s a lot harder to get into prestigious schools now.” Having no intention to harm doesn’t matter; plenty of harm is done unintentionally.
I also believed that because I have good intentions, I have no racial bias. I was wrong. The test I took online is an excellent tool to combat this blind spot. It was created by Harvard researchers and is available to everyone: Take a Test. It asks you to categorize faces as good or bad and records your tiny reaction times. Based on these and other questions, it provides feedback on your personal biases.
I was surprised that I have an implicit preference for white people over black people. That’s the point. Most of us are unaware of our biases and falsely believe we are free of them. I encourage you to take the test and learn about yourself. If the result makes you uncomfortable, then sit with it. Try not to be defensive, as I was, and accept that, even if you are a good person, you can become a better one.
Based on what I’ve learned and heard in the last few weeks, I’ve committed to a few things: To acknowledge the harm done to my black and brown colleagues and my complicity even by acts of omission. To not avoid uncomfortable feelings or uncomfortable conversations. As a leader, to use my organizational status to advocate. To stand by my partners of color not only in dramatic one-time marches but also against the everyday perpetrators of microaggressions. To create a safe space and invite my colleagues, staff, friends, and patients to share.
Standing up against racism is all our responsibility. As Dr. Martin Luther King Jr. reminds us: “In the end, we will remember not the words of our enemies, but the silence of our friends.”
Dr. Benabio is director of healthcare transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. He has no disclosures related to this column. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
I have an automatic preference for white people over black people. This isn’t my opinion; rather, it is my implicit bias test result. I didn’t believe it at first. Trying hard to not be biased, I took the test again and received the same outcome. My reaction – disbelief – is typical for those like me: White people who believe they are good human beings.
We’ve all watched in horror the acts of violence against blacks in the news. I was shocked and disgusted. It was easy to believe, however, that I am in no way complicit in the injustice and racism I was watching. I think I’m fair and without prejudice. I have never intentionally discriminated against someone. Wanting to help, I listened to my black colleagues, staff, and patients. What I learned made me uncomfortable.
Through all this news, I’d said little to my colleagues and friends. I cannot identify with how a black person has felt recently. What if I said the wrong thing or caused offense? The safe option is to say nothing. I learned that this is a common reaction and the least helpful. The advice from one black colleague was simple: “Just ask us.” Instead of ignoring the issue, she advised me to say: “I wonder what this experience has been like for you. Would you like to share?” And, if you mean it, to add, “I stand with you.” The latter should be followed by “What can I do to help?” Or, more powerfully, “What have I done that makes me complicit?”
Some of these conversations will be uncomfortable. If you want to help, then sit with that. Feeling uncomfortable might mean you are beginning to understand.
I also heard about the excellent book “White Fragility,” by Robin DiAngelo, PhD. In it, she argues that it is difficult for white people to talk about racism because of a tendency to react with defensiveness, guilt, and sometimes anger.
Many of the chapters in the book were easy to read because they didn’t apply to me: I don’t get angry in equity, inclusion, and diversity meetings. I don’t resent affirmative action programs. But then Dr. DiAngelo got me: I believed because I’m a good person and I have no intention of being racist, I’m absolved. Her argument was enlightening. Like all white people in the United States, I have benefited from white privilege. Yes, I’ve worked hard, but I also grew up in a white family with a college-educated father. That alone afforded me academic and financial advantages, which pushed me ahead. I’ve benefited from the status quo.
I have also failed to speak up when white friends carried on about how unnecessary affirmative action programs have become. I’ve sat with sealed lips when I’ve heard comments like “As a white male, it’s a lot harder to get into prestigious schools now.” Having no intention to harm doesn’t matter; plenty of harm is done unintentionally.
I also believed that because I have good intentions, I have no racial bias. I was wrong. The test I took online is an excellent tool to combat this blind spot. It was created by Harvard researchers and is available to everyone: Take a Test. It asks you to categorize faces as good or bad and records your tiny reaction times. Based on these and other questions, it provides feedback on your personal biases.
I was surprised that I have an implicit preference for white people over black people. That’s the point. Most of us are unaware of our biases and falsely believe we are free of them. I encourage you to take the test and learn about yourself. If the result makes you uncomfortable, then sit with it. Try not to be defensive, as I was, and accept that, even if you are a good person, you can become a better one.
Based on what I’ve learned and heard in the last few weeks, I’ve committed to a few things: To acknowledge the harm done to my black and brown colleagues and my complicity even by acts of omission. To not avoid uncomfortable feelings or uncomfortable conversations. As a leader, to use my organizational status to advocate. To stand by my partners of color not only in dramatic one-time marches but also against the everyday perpetrators of microaggressions. To create a safe space and invite my colleagues, staff, friends, and patients to share.
Standing up against racism is all our responsibility. As Dr. Martin Luther King Jr. reminds us: “In the end, we will remember not the words of our enemies, but the silence of our friends.”
Dr. Benabio is director of healthcare transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. He has no disclosures related to this column. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Lung ultrasound works well in children with COVID-19
researchers wrote in Pediatrics.
They also noted the benefits that modality provides over other imaging techniques.
Marco Denina, MD, and colleagues from the pediatric infectious diseases unit at Regina Margherita Children’s Hospital in Turin, Italy, performed an observational study of eight children aged 0-17 years who were admitted to the hospital for COVID-19 between March 8 and 26, 2020. In seven of eight patients, the findings were concordant between imaging modalities; in the remaining patient, lung ultrasound (LUS) found an interstitial B-lines pattern that was not seen on radiography. In seven patients with pathologic ultrasound findings at baseline, the improvement or resolution of the subpleural consolidations or interstitial patterns was consistent with concomitant radiologic findings.
The authors cited the benefits of using point-of-care ultrasound instead of other modalities, such as CT. “First, it may reduce the number of radiologic examinations, lowering the radiation exposure of the patients,” they wrote. “Secondly, when performed at the bedside, LUS allows for the reduction of the patient’s movement within the hospital; thus, it lowers the number of health care workers and medical devices exposed to [SARS-CoV-2].”
One limitation of the study is the small sample size; however, the researchers felt the high concordance still suggests LUS is a reasonable method for COVID-19 patients.
There was no external funding for this study and the investigators had no relevant financial disclosures.
SOURCE: Denina M et al. Pediatrics. 2020 Jun. doi: 10.1542/peds.2020-1157.
researchers wrote in Pediatrics.
They also noted the benefits that modality provides over other imaging techniques.
Marco Denina, MD, and colleagues from the pediatric infectious diseases unit at Regina Margherita Children’s Hospital in Turin, Italy, performed an observational study of eight children aged 0-17 years who were admitted to the hospital for COVID-19 between March 8 and 26, 2020. In seven of eight patients, the findings were concordant between imaging modalities; in the remaining patient, lung ultrasound (LUS) found an interstitial B-lines pattern that was not seen on radiography. In seven patients with pathologic ultrasound findings at baseline, the improvement or resolution of the subpleural consolidations or interstitial patterns was consistent with concomitant radiologic findings.
The authors cited the benefits of using point-of-care ultrasound instead of other modalities, such as CT. “First, it may reduce the number of radiologic examinations, lowering the radiation exposure of the patients,” they wrote. “Secondly, when performed at the bedside, LUS allows for the reduction of the patient’s movement within the hospital; thus, it lowers the number of health care workers and medical devices exposed to [SARS-CoV-2].”
One limitation of the study is the small sample size; however, the researchers felt the high concordance still suggests LUS is a reasonable method for COVID-19 patients.
There was no external funding for this study and the investigators had no relevant financial disclosures.
SOURCE: Denina M et al. Pediatrics. 2020 Jun. doi: 10.1542/peds.2020-1157.
researchers wrote in Pediatrics.
They also noted the benefits that modality provides over other imaging techniques.
Marco Denina, MD, and colleagues from the pediatric infectious diseases unit at Regina Margherita Children’s Hospital in Turin, Italy, performed an observational study of eight children aged 0-17 years who were admitted to the hospital for COVID-19 between March 8 and 26, 2020. In seven of eight patients, the findings were concordant between imaging modalities; in the remaining patient, lung ultrasound (LUS) found an interstitial B-lines pattern that was not seen on radiography. In seven patients with pathologic ultrasound findings at baseline, the improvement or resolution of the subpleural consolidations or interstitial patterns was consistent with concomitant radiologic findings.
The authors cited the benefits of using point-of-care ultrasound instead of other modalities, such as CT. “First, it may reduce the number of radiologic examinations, lowering the radiation exposure of the patients,” they wrote. “Secondly, when performed at the bedside, LUS allows for the reduction of the patient’s movement within the hospital; thus, it lowers the number of health care workers and medical devices exposed to [SARS-CoV-2].”
One limitation of the study is the small sample size; however, the researchers felt the high concordance still suggests LUS is a reasonable method for COVID-19 patients.
There was no external funding for this study and the investigators had no relevant financial disclosures.
SOURCE: Denina M et al. Pediatrics. 2020 Jun. doi: 10.1542/peds.2020-1157.
FROM PEDIATRICS
VERTIS-CV: Ertugliflozin’s CV outcomes trial confirms SGLT2i benefits
The cardiovascular outcome trial results for a fourth sodium-glucose cotransporter 2 (SGLT2) inhibitor, ertugliflozin, were most notable for their consistency with the four prior, similar trials run on the three other drugs from this class on the U.S. market, canagliflozin, dapagliflozin, and empagliflozin, further solidifying the important role this drug class has recently taken on for patients with type 2 diabetes.

But the ertugliflozin results, which showed statistically significant superiority to placebo for just one endpoint, hospitalization for heart failure, made it unclear whether clinicians will regard ertugliflozin as the top agent from this class to prescribe.
“Our big takeaway is that the findings are consistent with what’s been seen in the other studies” of cardiovascular and renal outcomes in the EMPA-REG OUTCOME study of empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28 ), the CANVAS (N Engl J Med. 2017 Aug 17;377[7]:644-57) and CREDENCE (N Engl J Med. 2019 June 13;380[24]:2295-306 ) studies of canagliflozin, and the DECLARE-TIMI 58 trial with dapagliflozin (N Engl J Med. 2019 Jan 24;380[4]:347-57), Christopher P. Cannon, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
The cardiovascular outcome trials (CVOTs), mandated in 2008 by Food and Drug Administration guidance for type 2 diabetes drugs that is now in the process of undergoing an update, have had the main goal of proving safety, and the primary endpoint of the new ertugliflozin trial, VERTIS-CV, was noninferiority to placebo when used on top of standard type 2 diabetes medications for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke.
Key findings
Both of the tested dosages of ertugliflozin, 5 mg and 15 mg daily, met this endpoint, with event rates over a median 3.0 years of follow-up that ran very close to the placebo rate, clearly proving noninferiority. But the results showed no suggestion of superiority in a study that randomized 5,499 patients to either of the ertugliflozin regimens and 2,747 to placebo, reported Dr. Cannon, a cardiologist and professor of medicine at Harvard Medical School, Boston.
The primary outcome also showed similar event rates for each component of the composite endpoint, and subgroup analysis showed consistent results from ertugliflozin, compared with placebo, regardless of study-cohort subdivision by demographic, clinical, or treatment factors.
The trial design called for a hierarchical sequence of secondary-outcome superiority analyses, starting with the impact of ertugliflozin on cardiovascular death or heart failure hospitalization, and for this outcome ertugliflozin showed a point estimate of a 12% relative risk reduction, compared with placebo-treated patients, but this difference was not statistically significant. This meant that all subsequent superiority analyses in this trial could only be hypothesis generating and not definitive.
This negated the statistical validity of the only statistically significant treatment difference between ertugliflozin and placebo seen in VERTIS-CV, for the outcome of hospitalization for heart failure, where ertugliflozin treatment cut this outcome by 30%, compared with placebo patients. The rate of cardiovascular death alone, as well as a renal composite endpoint each showed no statistically significant benefit of ertugliflozin, compared with placebo, although the renal endpoint came close, with ertugliflozin reducing the combined rate of renal death, need for dialysis, need for renal transplant, or a doubling of serum creatinine from baseline by 19%, compared with placebo (P = .08).
How results compare with prior CVOTs
In some ways, these results seemed to contrast with outcomes from the CVOTs for the other SGLT2 inhibitors, which all showed at least two statistically significant benefits for major endpoints when compared with placebo.

As summarized in a new meta-analysis of all the CVOTs by Darren K. McGuire, MD, a cardiologist and professor of medicine at the University of Texas, Dallas, both empagliflozin and canagliflozin showed statistically significant superiority compared with placebo for their trial’s primary, combined major cardiovascular adverse event endpoint, but dapagliflozin and ertugliflozin did not. Empagliflozin was the sole SGLT2 inhibitor to show a statistically significant cut in cardiovascular deaths, compared with placebo.
The primary, composite renal efficacy endpoints used in these trials were hardest to compare because they differed from study to study, but unlike ertugliflozin, all the other three drugs in the class showed a statistically significant improvement, compared with placebo, for their respective renal outcomes. On the other hand, the pattern of estimated glomerular filtration rates measured at multiple times during the various trials showed a high level of consistency across the CVOTs.
The greatest consistently among the major endpoints across the trials was for heart failure hospitalization. All four agents showed statistically significant improvements, compared with placebo, and all four had roughly equal magnitudes of effect, a cut in event rates by about one-third.
“The greatest magnitude of benefit is for reductions in heart failure hospitalizations and for renal outcomes,” with the heart failure outcomes the “most consistent” across the studies and the renal outcomes “largely consistent,” concluded Dr. McGuire. All together, the five CVOTs for these four SGLT2 inhibitors involved more than 46,000 patients.

“A lot of data suggest these are all class effects,” that are roughly similar across all four of these SGLT2 inhibitors, commented Mark E. Cooper, MBBS, a professor and head of the department of diabetes at Monash University, Melbourne, and designated discussant for the study.
There was “clear homogeneity” between the VERTIS-CV results for hospitalization for heart failure and the other CVOTs, he noted. “I think there is a difference” in the cardiovascular death outcomes, specifically the sole statistically significant, 38% relative risk reduction with empagliflozin that stood out from the other CVOTs, but this difference is “totally unexplained,” added Dr. Cooper. “To really determine differences you’d need head-to-head studies that are unlikely to happen.”
The results of new SGLT2 inhibitor meta-analysis appeared to also “support contemporary society recommendations to prioritize the use of SGLT2 inhibitors independent of glucose-control considerations in patients with type 2 diabetes with or at high risk for cardiovascular and renal complications,” said Dr. McGuire.
“The guidelines have it right. Now it’s on us to implement these treatments to appropriate patients,” concluded Dr. Cannon.
Study details
VERTIS-CV (Cardiovascular Outcomes Following Ertugliflozin Treatment in Type 2 Diabetes Mellitus Participants With Vascular Disease) enrolled and followed patients with type 2 diabetes and established atherosclerotic cardiovascular disease at 531 centers in 34 countries during December 2013–December 2019. Other effects from ertugliflozin recorded during the trial were consistent with prior studies of the drug, which is already FDA approved for glycemic control: Compared with placebo, ertugliflozin treatment reduced hemoglobin A1c by an average of 0.5% after 1 year, cut average body weight by about 2.5 kg after 1 year with additional modest weight loss, during subsequent years on the drug, and reduced systolic blood pressure by about 3 mm Hg after 1 year.
The drug’s safety profile was generally reassuring and consistent with prior studies of this drug and others in the class, with overall no increase in total adverse events or serious adverse events, compared with placebo, and modestly increased rates of urinary tract and mycotic genital infections.
VERTIS-CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin (Steglatro). Dr. Cannon has received research funding and fees from Merck and Pfizer and from several other companies. Dr. McGuire has received honoraria from Merck, has been a consultant to Pfizer, and has had similar relationships with several other companies. Dr. Cooper has been an advisor to and received honoraria from Merck. He has also received honoraria from or been an adviser to AstraZeneca, Boehringer Ingelheim, Lilly, MundiPharma, Novartis, Reata, and Servier, and he has received research funding from Boehringer Ingelheim and Novo Nordisk.
The cardiovascular outcome trial results for a fourth sodium-glucose cotransporter 2 (SGLT2) inhibitor, ertugliflozin, were most notable for their consistency with the four prior, similar trials run on the three other drugs from this class on the U.S. market, canagliflozin, dapagliflozin, and empagliflozin, further solidifying the important role this drug class has recently taken on for patients with type 2 diabetes.
But the ertugliflozin results, which showed statistically significant superiority to placebo for just one endpoint, hospitalization for heart failure, made it unclear whether clinicians will regard ertugliflozin as the top agent from this class to prescribe.
“Our big takeaway is that the findings are consistent with what’s been seen in the other studies” of cardiovascular and renal outcomes in the EMPA-REG OUTCOME study of empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28 ), the CANVAS (N Engl J Med. 2017 Aug 17;377[7]:644-57) and CREDENCE (N Engl J Med. 2019 June 13;380[24]:2295-306 ) studies of canagliflozin, and the DECLARE-TIMI 58 trial with dapagliflozin (N Engl J Med. 2019 Jan 24;380[4]:347-57), Christopher P. Cannon, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
The cardiovascular outcome trials (CVOTs), mandated in 2008 by Food and Drug Administration guidance for type 2 diabetes drugs that is now in the process of undergoing an update, have had the main goal of proving safety, and the primary endpoint of the new ertugliflozin trial, VERTIS-CV, was noninferiority to placebo when used on top of standard type 2 diabetes medications for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke.
Key findings
Both of the tested dosages of ertugliflozin, 5 mg and 15 mg daily, met this endpoint, with event rates over a median 3.0 years of follow-up that ran very close to the placebo rate, clearly proving noninferiority. But the results showed no suggestion of superiority in a study that randomized 5,499 patients to either of the ertugliflozin regimens and 2,747 to placebo, reported Dr. Cannon, a cardiologist and professor of medicine at Harvard Medical School, Boston.
The primary outcome also showed similar event rates for each component of the composite endpoint, and subgroup analysis showed consistent results from ertugliflozin, compared with placebo, regardless of study-cohort subdivision by demographic, clinical, or treatment factors.
The trial design called for a hierarchical sequence of secondary-outcome superiority analyses, starting with the impact of ertugliflozin on cardiovascular death or heart failure hospitalization, and for this outcome ertugliflozin showed a point estimate of a 12% relative risk reduction, compared with placebo-treated patients, but this difference was not statistically significant. This meant that all subsequent superiority analyses in this trial could only be hypothesis generating and not definitive.
This negated the statistical validity of the only statistically significant treatment difference between ertugliflozin and placebo seen in VERTIS-CV, for the outcome of hospitalization for heart failure, where ertugliflozin treatment cut this outcome by 30%, compared with placebo patients. The rate of cardiovascular death alone, as well as a renal composite endpoint each showed no statistically significant benefit of ertugliflozin, compared with placebo, although the renal endpoint came close, with ertugliflozin reducing the combined rate of renal death, need for dialysis, need for renal transplant, or a doubling of serum creatinine from baseline by 19%, compared with placebo (P = .08).
How results compare with prior CVOTs
In some ways, these results seemed to contrast with outcomes from the CVOTs for the other SGLT2 inhibitors, which all showed at least two statistically significant benefits for major endpoints when compared with placebo.
As summarized in a new meta-analysis of all the CVOTs by Darren K. McGuire, MD, a cardiologist and professor of medicine at the University of Texas, Dallas, both empagliflozin and canagliflozin showed statistically significant superiority compared with placebo for their trial’s primary, combined major cardiovascular adverse event endpoint, but dapagliflozin and ertugliflozin did not. Empagliflozin was the sole SGLT2 inhibitor to show a statistically significant cut in cardiovascular deaths, compared with placebo.
The primary, composite renal efficacy endpoints used in these trials were hardest to compare because they differed from study to study, but unlike ertugliflozin, all the other three drugs in the class showed a statistically significant improvement, compared with placebo, for their respective renal outcomes. On the other hand, the pattern of estimated glomerular filtration rates measured at multiple times during the various trials showed a high level of consistency across the CVOTs.
The greatest consistently among the major endpoints across the trials was for heart failure hospitalization. All four agents showed statistically significant improvements, compared with placebo, and all four had roughly equal magnitudes of effect, a cut in event rates by about one-third.
“The greatest magnitude of benefit is for reductions in heart failure hospitalizations and for renal outcomes,” with the heart failure outcomes the “most consistent” across the studies and the renal outcomes “largely consistent,” concluded Dr. McGuire. All together, the five CVOTs for these four SGLT2 inhibitors involved more than 46,000 patients.
“A lot of data suggest these are all class effects,” that are roughly similar across all four of these SGLT2 inhibitors, commented Mark E. Cooper, MBBS, a professor and head of the department of diabetes at Monash University, Melbourne, and designated discussant for the study.
There was “clear homogeneity” between the VERTIS-CV results for hospitalization for heart failure and the other CVOTs, he noted. “I think there is a difference” in the cardiovascular death outcomes, specifically the sole statistically significant, 38% relative risk reduction with empagliflozin that stood out from the other CVOTs, but this difference is “totally unexplained,” added Dr. Cooper. “To really determine differences you’d need head-to-head studies that are unlikely to happen.”
The results of new SGLT2 inhibitor meta-analysis appeared to also “support contemporary society recommendations to prioritize the use of SGLT2 inhibitors independent of glucose-control considerations in patients with type 2 diabetes with or at high risk for cardiovascular and renal complications,” said Dr. McGuire.
“The guidelines have it right. Now it’s on us to implement these treatments to appropriate patients,” concluded Dr. Cannon.
Study details
VERTIS-CV (Cardiovascular Outcomes Following Ertugliflozin Treatment in Type 2 Diabetes Mellitus Participants With Vascular Disease) enrolled and followed patients with type 2 diabetes and established atherosclerotic cardiovascular disease at 531 centers in 34 countries during December 2013–December 2019. Other effects from ertugliflozin recorded during the trial were consistent with prior studies of the drug, which is already FDA approved for glycemic control: Compared with placebo, ertugliflozin treatment reduced hemoglobin A1c by an average of 0.5% after 1 year, cut average body weight by about 2.5 kg after 1 year with additional modest weight loss, during subsequent years on the drug, and reduced systolic blood pressure by about 3 mm Hg after 1 year.
The drug’s safety profile was generally reassuring and consistent with prior studies of this drug and others in the class, with overall no increase in total adverse events or serious adverse events, compared with placebo, and modestly increased rates of urinary tract and mycotic genital infections.
VERTIS-CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin (Steglatro). Dr. Cannon has received research funding and fees from Merck and Pfizer and from several other companies. Dr. McGuire has received honoraria from Merck, has been a consultant to Pfizer, and has had similar relationships with several other companies. Dr. Cooper has been an advisor to and received honoraria from Merck. He has also received honoraria from or been an adviser to AstraZeneca, Boehringer Ingelheim, Lilly, MundiPharma, Novartis, Reata, and Servier, and he has received research funding from Boehringer Ingelheim and Novo Nordisk.
The cardiovascular outcome trial results for a fourth sodium-glucose cotransporter 2 (SGLT2) inhibitor, ertugliflozin, were most notable for their consistency with the four prior, similar trials run on the three other drugs from this class on the U.S. market, canagliflozin, dapagliflozin, and empagliflozin, further solidifying the important role this drug class has recently taken on for patients with type 2 diabetes.
But the ertugliflozin results, which showed statistically significant superiority to placebo for just one endpoint, hospitalization for heart failure, made it unclear whether clinicians will regard ertugliflozin as the top agent from this class to prescribe.
“Our big takeaway is that the findings are consistent with what’s been seen in the other studies” of cardiovascular and renal outcomes in the EMPA-REG OUTCOME study of empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28 ), the CANVAS (N Engl J Med. 2017 Aug 17;377[7]:644-57) and CREDENCE (N Engl J Med. 2019 June 13;380[24]:2295-306 ) studies of canagliflozin, and the DECLARE-TIMI 58 trial with dapagliflozin (N Engl J Med. 2019 Jan 24;380[4]:347-57), Christopher P. Cannon, MD, said at the virtual annual scientific sessions of the American Diabetes Association.
The cardiovascular outcome trials (CVOTs), mandated in 2008 by Food and Drug Administration guidance for type 2 diabetes drugs that is now in the process of undergoing an update, have had the main goal of proving safety, and the primary endpoint of the new ertugliflozin trial, VERTIS-CV, was noninferiority to placebo when used on top of standard type 2 diabetes medications for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke.
Key findings
Both of the tested dosages of ertugliflozin, 5 mg and 15 mg daily, met this endpoint, with event rates over a median 3.0 years of follow-up that ran very close to the placebo rate, clearly proving noninferiority. But the results showed no suggestion of superiority in a study that randomized 5,499 patients to either of the ertugliflozin regimens and 2,747 to placebo, reported Dr. Cannon, a cardiologist and professor of medicine at Harvard Medical School, Boston.
The primary outcome also showed similar event rates for each component of the composite endpoint, and subgroup analysis showed consistent results from ertugliflozin, compared with placebo, regardless of study-cohort subdivision by demographic, clinical, or treatment factors.
The trial design called for a hierarchical sequence of secondary-outcome superiority analyses, starting with the impact of ertugliflozin on cardiovascular death or heart failure hospitalization, and for this outcome ertugliflozin showed a point estimate of a 12% relative risk reduction, compared with placebo-treated patients, but this difference was not statistically significant. This meant that all subsequent superiority analyses in this trial could only be hypothesis generating and not definitive.
This negated the statistical validity of the only statistically significant treatment difference between ertugliflozin and placebo seen in VERTIS-CV, for the outcome of hospitalization for heart failure, where ertugliflozin treatment cut this outcome by 30%, compared with placebo patients. The rate of cardiovascular death alone, as well as a renal composite endpoint each showed no statistically significant benefit of ertugliflozin, compared with placebo, although the renal endpoint came close, with ertugliflozin reducing the combined rate of renal death, need for dialysis, need for renal transplant, or a doubling of serum creatinine from baseline by 19%, compared with placebo (P = .08).
How results compare with prior CVOTs
In some ways, these results seemed to contrast with outcomes from the CVOTs for the other SGLT2 inhibitors, which all showed at least two statistically significant benefits for major endpoints when compared with placebo.
As summarized in a new meta-analysis of all the CVOTs by Darren K. McGuire, MD, a cardiologist and professor of medicine at the University of Texas, Dallas, both empagliflozin and canagliflozin showed statistically significant superiority compared with placebo for their trial’s primary, combined major cardiovascular adverse event endpoint, but dapagliflozin and ertugliflozin did not. Empagliflozin was the sole SGLT2 inhibitor to show a statistically significant cut in cardiovascular deaths, compared with placebo.
The primary, composite renal efficacy endpoints used in these trials were hardest to compare because they differed from study to study, but unlike ertugliflozin, all the other three drugs in the class showed a statistically significant improvement, compared with placebo, for their respective renal outcomes. On the other hand, the pattern of estimated glomerular filtration rates measured at multiple times during the various trials showed a high level of consistency across the CVOTs.
The greatest consistently among the major endpoints across the trials was for heart failure hospitalization. All four agents showed statistically significant improvements, compared with placebo, and all four had roughly equal magnitudes of effect, a cut in event rates by about one-third.
“The greatest magnitude of benefit is for reductions in heart failure hospitalizations and for renal outcomes,” with the heart failure outcomes the “most consistent” across the studies and the renal outcomes “largely consistent,” concluded Dr. McGuire. All together, the five CVOTs for these four SGLT2 inhibitors involved more than 46,000 patients.
“A lot of data suggest these are all class effects,” that are roughly similar across all four of these SGLT2 inhibitors, commented Mark E. Cooper, MBBS, a professor and head of the department of diabetes at Monash University, Melbourne, and designated discussant for the study.
There was “clear homogeneity” between the VERTIS-CV results for hospitalization for heart failure and the other CVOTs, he noted. “I think there is a difference” in the cardiovascular death outcomes, specifically the sole statistically significant, 38% relative risk reduction with empagliflozin that stood out from the other CVOTs, but this difference is “totally unexplained,” added Dr. Cooper. “To really determine differences you’d need head-to-head studies that are unlikely to happen.”
The results of new SGLT2 inhibitor meta-analysis appeared to also “support contemporary society recommendations to prioritize the use of SGLT2 inhibitors independent of glucose-control considerations in patients with type 2 diabetes with or at high risk for cardiovascular and renal complications,” said Dr. McGuire.
“The guidelines have it right. Now it’s on us to implement these treatments to appropriate patients,” concluded Dr. Cannon.
Study details
VERTIS-CV (Cardiovascular Outcomes Following Ertugliflozin Treatment in Type 2 Diabetes Mellitus Participants With Vascular Disease) enrolled and followed patients with type 2 diabetes and established atherosclerotic cardiovascular disease at 531 centers in 34 countries during December 2013–December 2019. Other effects from ertugliflozin recorded during the trial were consistent with prior studies of the drug, which is already FDA approved for glycemic control: Compared with placebo, ertugliflozin treatment reduced hemoglobin A1c by an average of 0.5% after 1 year, cut average body weight by about 2.5 kg after 1 year with additional modest weight loss, during subsequent years on the drug, and reduced systolic blood pressure by about 3 mm Hg after 1 year.
The drug’s safety profile was generally reassuring and consistent with prior studies of this drug and others in the class, with overall no increase in total adverse events or serious adverse events, compared with placebo, and modestly increased rates of urinary tract and mycotic genital infections.
VERTIS-CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin (Steglatro). Dr. Cannon has received research funding and fees from Merck and Pfizer and from several other companies. Dr. McGuire has received honoraria from Merck, has been a consultant to Pfizer, and has had similar relationships with several other companies. Dr. Cooper has been an advisor to and received honoraria from Merck. He has also received honoraria from or been an adviser to AstraZeneca, Boehringer Ingelheim, Lilly, MundiPharma, Novartis, Reata, and Servier, and he has received research funding from Boehringer Ingelheim and Novo Nordisk.
FROM ADA 2020
Face mask type matters when sterilizing, study finds
according to researchers. The greatest reduction in filtration efficiency after sterilization occurred with surgical face masks.
With plasma vapor hydrogen peroxide (H2O2) sterilization, filtration efficiency of N95 and KN95 masks was maintained at more than 95%, but for surgical face masks, filtration efficiency was reduced to less than 95%. With chlorine dioxide (ClO2) sterilization, on the other hand, filtration efficiency was maintained at above 95% for N95 masks, but for KN95 and surgical face masks, filtration efficiency was reduced to less than 80%.
In a research letter published online June 15 in JAMA Network Open, researchers from the University of Oklahoma Health Sciences Center, Oklahoma City, report the results of a study of the two sterilization techniques on the pressure drop and filtration efficiency of N95, KN95, and surgical face masks.
“The H2O2 treatment showed a small effect on the overall filtration efficiency of the tested masks, but the ClO2 treatment showed marked reduction in the overall filtration efficiency of the KN95s and surgical face masks. All pressure drop changes were within the acceptable range,” the researchers write.
The study did not evaluate the effect of repeated sterilizations on face masks.
Five masks of each type were sterilized with either H2O2 or ClO2. Masks were then placed in a test chamber, and a salt aerosol was nebulized to assess both upstream and downstream filtration as well as pressure drop. The researchers used a mobility particle sizer to measure particle number concentration from 16.8 nm to 514 nm. An acceptable pressure drop was defined as a drop of less than 1.38 inches of water (35 mm) for inhalation.
Although pressure drop changes were within the acceptable range for all three mask types following sterilization with either method, H2O2 sterilization yielded the least reduction in filtration efficacy in all cases. After sterilization with H2O2, filtration efficiencies were 96.6%, 97.1%, and 91.6% for the N95s, KN95s, and the surgical face masks, respectively. In contrast, filtration efficiencies after ClO2 sterilization were 95.1%, 76.2%, and 77.9%, respectively.
The researchers note that, although overall filtration efficiency was maintained with ClO2 sterilization, there was a significant drop in efficiency with respect to particles of approximately 300 nm (0.3 microns) in size. For particles of that size, mean filtration efficiency decreased to 86.2% for N95s, 40.8% for KN95s, and 47.1% for surgical face masks.
The testing described in the report is “quite affordable at $350 per mask type, so it is hard to imagine any health care provider cannot set aside a small budget to conduct such an important test,” author Evan Floyd, PhD, told Medscape Medical News.
Given the high demand for effective face masks and the current risk for counterfeit products, Floyd suggested that individual facilities test all masks intended for use by healthcare workers before and after sterilization procedures.
“However, if for some reason testing is not an option, we would recommend sticking to established brands and suppliers, perhaps reach out to your state health department or a local representative of the strategic stockpile of PPE,” he noted.
The authors acknowledge that further studies using a larger sample size and a greater variety of masks, as well as studies to evaluate different sterilization techniques, are required. Further, “measuring the respirator’s filtration efficiency by aerosol size instead of only measuring the overall filtration efficiency” should also be considered. Such an approach would enable researchers to evaluate the degree to which masks protect against specific infectious agents.
This article first appeared on Medscape.com.
according to researchers. The greatest reduction in filtration efficiency after sterilization occurred with surgical face masks.
With plasma vapor hydrogen peroxide (H2O2) sterilization, filtration efficiency of N95 and KN95 masks was maintained at more than 95%, but for surgical face masks, filtration efficiency was reduced to less than 95%. With chlorine dioxide (ClO2) sterilization, on the other hand, filtration efficiency was maintained at above 95% for N95 masks, but for KN95 and surgical face masks, filtration efficiency was reduced to less than 80%.
In a research letter published online June 15 in JAMA Network Open, researchers from the University of Oklahoma Health Sciences Center, Oklahoma City, report the results of a study of the two sterilization techniques on the pressure drop and filtration efficiency of N95, KN95, and surgical face masks.
“The H2O2 treatment showed a small effect on the overall filtration efficiency of the tested masks, but the ClO2 treatment showed marked reduction in the overall filtration efficiency of the KN95s and surgical face masks. All pressure drop changes were within the acceptable range,” the researchers write.
The study did not evaluate the effect of repeated sterilizations on face masks.
Five masks of each type were sterilized with either H2O2 or ClO2. Masks were then placed in a test chamber, and a salt aerosol was nebulized to assess both upstream and downstream filtration as well as pressure drop. The researchers used a mobility particle sizer to measure particle number concentration from 16.8 nm to 514 nm. An acceptable pressure drop was defined as a drop of less than 1.38 inches of water (35 mm) for inhalation.
Although pressure drop changes were within the acceptable range for all three mask types following sterilization with either method, H2O2 sterilization yielded the least reduction in filtration efficacy in all cases. After sterilization with H2O2, filtration efficiencies were 96.6%, 97.1%, and 91.6% for the N95s, KN95s, and the surgical face masks, respectively. In contrast, filtration efficiencies after ClO2 sterilization were 95.1%, 76.2%, and 77.9%, respectively.
The researchers note that, although overall filtration efficiency was maintained with ClO2 sterilization, there was a significant drop in efficiency with respect to particles of approximately 300 nm (0.3 microns) in size. For particles of that size, mean filtration efficiency decreased to 86.2% for N95s, 40.8% for KN95s, and 47.1% for surgical face masks.
The testing described in the report is “quite affordable at $350 per mask type, so it is hard to imagine any health care provider cannot set aside a small budget to conduct such an important test,” author Evan Floyd, PhD, told Medscape Medical News.
Given the high demand for effective face masks and the current risk for counterfeit products, Floyd suggested that individual facilities test all masks intended for use by healthcare workers before and after sterilization procedures.
“However, if for some reason testing is not an option, we would recommend sticking to established brands and suppliers, perhaps reach out to your state health department or a local representative of the strategic stockpile of PPE,” he noted.
The authors acknowledge that further studies using a larger sample size and a greater variety of masks, as well as studies to evaluate different sterilization techniques, are required. Further, “measuring the respirator’s filtration efficiency by aerosol size instead of only measuring the overall filtration efficiency” should also be considered. Such an approach would enable researchers to evaluate the degree to which masks protect against specific infectious agents.
This article first appeared on Medscape.com.
according to researchers. The greatest reduction in filtration efficiency after sterilization occurred with surgical face masks.
With plasma vapor hydrogen peroxide (H2O2) sterilization, filtration efficiency of N95 and KN95 masks was maintained at more than 95%, but for surgical face masks, filtration efficiency was reduced to less than 95%. With chlorine dioxide (ClO2) sterilization, on the other hand, filtration efficiency was maintained at above 95% for N95 masks, but for KN95 and surgical face masks, filtration efficiency was reduced to less than 80%.
In a research letter published online June 15 in JAMA Network Open, researchers from the University of Oklahoma Health Sciences Center, Oklahoma City, report the results of a study of the two sterilization techniques on the pressure drop and filtration efficiency of N95, KN95, and surgical face masks.
“The H2O2 treatment showed a small effect on the overall filtration efficiency of the tested masks, but the ClO2 treatment showed marked reduction in the overall filtration efficiency of the KN95s and surgical face masks. All pressure drop changes were within the acceptable range,” the researchers write.
The study did not evaluate the effect of repeated sterilizations on face masks.
Five masks of each type were sterilized with either H2O2 or ClO2. Masks were then placed in a test chamber, and a salt aerosol was nebulized to assess both upstream and downstream filtration as well as pressure drop. The researchers used a mobility particle sizer to measure particle number concentration from 16.8 nm to 514 nm. An acceptable pressure drop was defined as a drop of less than 1.38 inches of water (35 mm) for inhalation.
Although pressure drop changes were within the acceptable range for all three mask types following sterilization with either method, H2O2 sterilization yielded the least reduction in filtration efficacy in all cases. After sterilization with H2O2, filtration efficiencies were 96.6%, 97.1%, and 91.6% for the N95s, KN95s, and the surgical face masks, respectively. In contrast, filtration efficiencies after ClO2 sterilization were 95.1%, 76.2%, and 77.9%, respectively.
The researchers note that, although overall filtration efficiency was maintained with ClO2 sterilization, there was a significant drop in efficiency with respect to particles of approximately 300 nm (0.3 microns) in size. For particles of that size, mean filtration efficiency decreased to 86.2% for N95s, 40.8% for KN95s, and 47.1% for surgical face masks.
The testing described in the report is “quite affordable at $350 per mask type, so it is hard to imagine any health care provider cannot set aside a small budget to conduct such an important test,” author Evan Floyd, PhD, told Medscape Medical News.
Given the high demand for effective face masks and the current risk for counterfeit products, Floyd suggested that individual facilities test all masks intended for use by healthcare workers before and after sterilization procedures.
“However, if for some reason testing is not an option, we would recommend sticking to established brands and suppliers, perhaps reach out to your state health department or a local representative of the strategic stockpile of PPE,” he noted.
The authors acknowledge that further studies using a larger sample size and a greater variety of masks, as well as studies to evaluate different sterilization techniques, are required. Further, “measuring the respirator’s filtration efficiency by aerosol size instead of only measuring the overall filtration efficiency” should also be considered. Such an approach would enable researchers to evaluate the degree to which masks protect against specific infectious agents.
This article first appeared on Medscape.com.
Frequent hypoglycemic episodes raise cardiac event risk
Frequent hypoglycemic episodes were linked to a raised incidence of cardiovascular events in adults with type 2 diabetes in a recent retrospective study, suggesting certain hypoglycemia-associated diabetes drugs should be avoided, an investigator said.
Patients who had more than five hypoglycemic episodes per year had a 61% greater risk of cardiovascular (CV) events, compared with patients with less frequent episodes, according to results of the study.
Although there were fewer strokes among younger patients, the overall increase in cardiovascular event risk held up regardless of age group, according to investigator Aman Rajpal, MD, of Louis Stokes Veterans Affairs Medical Center and Case Western Reserve University, both in Cleveland.
On the basis of these and earlier studies tying hypoglycemia to CV risk, health care providers need to “pay close attention” to low blood sugar and personalize glycemic control targets for each patient based on risk of hypoglycemia, Dr. Rajpal said in a presentation of the study at the virtual annual scientific sessions of the American Diabetes Association.
“Also, this suggests that avoidance of drugs associated with increased risk of hypoglycemia – namely insulin, sulfonylureas, or others – is essential to avoid and minimize the risk of cardiovascular events in this patient population with type 2 diabetes,” said Dr. Rajpal. “Let us remember part of our Hippocratic oath: ‘Above all, do no harm.’ ”
Tailoring treatment to mitigate risk
Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, said that results of this study suggest a need to carefully select medical therapy for each individual patient with diabetes in order to mitigate CV risk.
“It’s really about tailoring their drugs to their personal situation,” Dr. Schutta said in an interview.
Although newer diabetes drug classes are associated with low to no risk of hypoglycemia, Dr. Schutta said that there is still a place for drugs such as sulfonylureas in certain situations.
Among sulfonylureas, glyburide comes with a much higher incidence of hypoglycemia, compared with glipizide and glimepiride, according to Dr. Schutta. “I think there’s a role for both drugs, but you have to be very careful, and you have to get the data from your patients.”
Hypoglycemia frequency and outcomes
Speculation that hypoglycemia could be linked to adverse CV outcomes was sparked years ago by trials such as ADVANCE. Severe hypoglycemia in that study was associated with a 168% increased risk of death from a CV cause (N Engl J Med. 2010 Oct 7;363:1410-8).
At the time, ADVANCE investigators said they were unable to find evidence that multiple severe hypoglycemia episodes conferred a greater risk of CV events versus a single hypoglycemia episode, though they added that few patients had recurrent events.
“In other words, the association between the number of hypoglycemia events, and adverse CV outcomes is still unclear,” said Dr. Rajpal in his virtual ADA presentation.
Potential elevated risks with more than five episodes
To evaluate the association between frequent hypoglycemic episodes (i.e., more than five per year, compared with one to five episodes) and CV events, Dr. Rajpal and colleagues evaluated outcomes data for 4.9 million adults with type 2 diabetes found in a large commercial database including information on patients in 27 U.S. health care networks.
Database records indicated that about 182,000 patients, or nearly 4%, had episodes of hyperglycemia, which Dr. Rajpal said was presumed to mean a plasma glucose level of less than 70 mg/dL.
Characteristics of the patients with more than five hypoglycemic episodes were similar to those with one to five episodes, although they were more likely to be 65 years or older, and were “slightly more likely” to be on insulin, which could possibly precipitate more hypoglycemic episodes in that group, Dr. Rajpal said.
Key findings
In the main analysis, Dr. Rajpal said, risk of CV events was significantly increased in those with more than five hypoglycemic episodes, compared with those with one to five episodes, with an odds ratio of 1.61 (95% confidence interval, 1.56-1.66). The incidence of cardiovascular events was 33.1% in those with more than five episodes and 23.5% in those with one to five episodes, according to the data presented.
Risks were also significantly increased specifically for cardiac arrhythmias, cerebrovascular accidents, and MI, Dr. Rajpal said, with ORs of 1.65 (95% CI, 1.9-1.71), 1.38 (95% CI, 1.22-1.56), and 1.43 (95% CI, 1.36-1.50), respectively.
Because individuals in the group with more than five hypoglycemic episodes were more likely to be elderly, Dr. Rajpal said that he and coinvestigators decided to perform an age-specific stratified analysis.
Although cerebral vascular incidence was low in younger patients, risk of CV events overall was nevertheless significantly elevated for those aged 65 years or older, 45-64 years, and 18-44 years, with ORs of 1.69 (95% CI, 1.61-1.7), 1.58 (95% CI, 1.48-1.69), and 1.62 (95% CI, 1.33-1.97).
“The results were still valid in stratified analysis based on different age groups,” Dr. Rajpal said.
Dr. Rajpal and coauthors reported that he had no conflicts of interest related to the research.
SOURCE: Rajpal A et al. ADA 2020, Abstract 161-OR.
Frequent hypoglycemic episodes were linked to a raised incidence of cardiovascular events in adults with type 2 diabetes in a recent retrospective study, suggesting certain hypoglycemia-associated diabetes drugs should be avoided, an investigator said.
Patients who had more than five hypoglycemic episodes per year had a 61% greater risk of cardiovascular (CV) events, compared with patients with less frequent episodes, according to results of the study.
Although there were fewer strokes among younger patients, the overall increase in cardiovascular event risk held up regardless of age group, according to investigator Aman Rajpal, MD, of Louis Stokes Veterans Affairs Medical Center and Case Western Reserve University, both in Cleveland.
On the basis of these and earlier studies tying hypoglycemia to CV risk, health care providers need to “pay close attention” to low blood sugar and personalize glycemic control targets for each patient based on risk of hypoglycemia, Dr. Rajpal said in a presentation of the study at the virtual annual scientific sessions of the American Diabetes Association.
“Also, this suggests that avoidance of drugs associated with increased risk of hypoglycemia – namely insulin, sulfonylureas, or others – is essential to avoid and minimize the risk of cardiovascular events in this patient population with type 2 diabetes,” said Dr. Rajpal. “Let us remember part of our Hippocratic oath: ‘Above all, do no harm.’ ”
Tailoring treatment to mitigate risk
Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, said that results of this study suggest a need to carefully select medical therapy for each individual patient with diabetes in order to mitigate CV risk.
“It’s really about tailoring their drugs to their personal situation,” Dr. Schutta said in an interview.
Although newer diabetes drug classes are associated with low to no risk of hypoglycemia, Dr. Schutta said that there is still a place for drugs such as sulfonylureas in certain situations.
Among sulfonylureas, glyburide comes with a much higher incidence of hypoglycemia, compared with glipizide and glimepiride, according to Dr. Schutta. “I think there’s a role for both drugs, but you have to be very careful, and you have to get the data from your patients.”
Hypoglycemia frequency and outcomes
Speculation that hypoglycemia could be linked to adverse CV outcomes was sparked years ago by trials such as ADVANCE. Severe hypoglycemia in that study was associated with a 168% increased risk of death from a CV cause (N Engl J Med. 2010 Oct 7;363:1410-8).
At the time, ADVANCE investigators said they were unable to find evidence that multiple severe hypoglycemia episodes conferred a greater risk of CV events versus a single hypoglycemia episode, though they added that few patients had recurrent events.
“In other words, the association between the number of hypoglycemia events, and adverse CV outcomes is still unclear,” said Dr. Rajpal in his virtual ADA presentation.
Potential elevated risks with more than five episodes
To evaluate the association between frequent hypoglycemic episodes (i.e., more than five per year, compared with one to five episodes) and CV events, Dr. Rajpal and colleagues evaluated outcomes data for 4.9 million adults with type 2 diabetes found in a large commercial database including information on patients in 27 U.S. health care networks.
Database records indicated that about 182,000 patients, or nearly 4%, had episodes of hyperglycemia, which Dr. Rajpal said was presumed to mean a plasma glucose level of less than 70 mg/dL.
Characteristics of the patients with more than five hypoglycemic episodes were similar to those with one to five episodes, although they were more likely to be 65 years or older, and were “slightly more likely” to be on insulin, which could possibly precipitate more hypoglycemic episodes in that group, Dr. Rajpal said.
Key findings
In the main analysis, Dr. Rajpal said, risk of CV events was significantly increased in those with more than five hypoglycemic episodes, compared with those with one to five episodes, with an odds ratio of 1.61 (95% confidence interval, 1.56-1.66). The incidence of cardiovascular events was 33.1% in those with more than five episodes and 23.5% in those with one to five episodes, according to the data presented.
Risks were also significantly increased specifically for cardiac arrhythmias, cerebrovascular accidents, and MI, Dr. Rajpal said, with ORs of 1.65 (95% CI, 1.9-1.71), 1.38 (95% CI, 1.22-1.56), and 1.43 (95% CI, 1.36-1.50), respectively.
Because individuals in the group with more than five hypoglycemic episodes were more likely to be elderly, Dr. Rajpal said that he and coinvestigators decided to perform an age-specific stratified analysis.
Although cerebral vascular incidence was low in younger patients, risk of CV events overall was nevertheless significantly elevated for those aged 65 years or older, 45-64 years, and 18-44 years, with ORs of 1.69 (95% CI, 1.61-1.7), 1.58 (95% CI, 1.48-1.69), and 1.62 (95% CI, 1.33-1.97).
“The results were still valid in stratified analysis based on different age groups,” Dr. Rajpal said.
Dr. Rajpal and coauthors reported that he had no conflicts of interest related to the research.
SOURCE: Rajpal A et al. ADA 2020, Abstract 161-OR.
Frequent hypoglycemic episodes were linked to a raised incidence of cardiovascular events in adults with type 2 diabetes in a recent retrospective study, suggesting certain hypoglycemia-associated diabetes drugs should be avoided, an investigator said.
Patients who had more than five hypoglycemic episodes per year had a 61% greater risk of cardiovascular (CV) events, compared with patients with less frequent episodes, according to results of the study.
Although there were fewer strokes among younger patients, the overall increase in cardiovascular event risk held up regardless of age group, according to investigator Aman Rajpal, MD, of Louis Stokes Veterans Affairs Medical Center and Case Western Reserve University, both in Cleveland.
On the basis of these and earlier studies tying hypoglycemia to CV risk, health care providers need to “pay close attention” to low blood sugar and personalize glycemic control targets for each patient based on risk of hypoglycemia, Dr. Rajpal said in a presentation of the study at the virtual annual scientific sessions of the American Diabetes Association.
“Also, this suggests that avoidance of drugs associated with increased risk of hypoglycemia – namely insulin, sulfonylureas, or others – is essential to avoid and minimize the risk of cardiovascular events in this patient population with type 2 diabetes,” said Dr. Rajpal. “Let us remember part of our Hippocratic oath: ‘Above all, do no harm.’ ”
Tailoring treatment to mitigate risk
Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, said that results of this study suggest a need to carefully select medical therapy for each individual patient with diabetes in order to mitigate CV risk.
“It’s really about tailoring their drugs to their personal situation,” Dr. Schutta said in an interview.
Although newer diabetes drug classes are associated with low to no risk of hypoglycemia, Dr. Schutta said that there is still a place for drugs such as sulfonylureas in certain situations.
Among sulfonylureas, glyburide comes with a much higher incidence of hypoglycemia, compared with glipizide and glimepiride, according to Dr. Schutta. “I think there’s a role for both drugs, but you have to be very careful, and you have to get the data from your patients.”
Hypoglycemia frequency and outcomes
Speculation that hypoglycemia could be linked to adverse CV outcomes was sparked years ago by trials such as ADVANCE. Severe hypoglycemia in that study was associated with a 168% increased risk of death from a CV cause (N Engl J Med. 2010 Oct 7;363:1410-8).
At the time, ADVANCE investigators said they were unable to find evidence that multiple severe hypoglycemia episodes conferred a greater risk of CV events versus a single hypoglycemia episode, though they added that few patients had recurrent events.
“In other words, the association between the number of hypoglycemia events, and adverse CV outcomes is still unclear,” said Dr. Rajpal in his virtual ADA presentation.
Potential elevated risks with more than five episodes
To evaluate the association between frequent hypoglycemic episodes (i.e., more than five per year, compared with one to five episodes) and CV events, Dr. Rajpal and colleagues evaluated outcomes data for 4.9 million adults with type 2 diabetes found in a large commercial database including information on patients in 27 U.S. health care networks.
Database records indicated that about 182,000 patients, or nearly 4%, had episodes of hyperglycemia, which Dr. Rajpal said was presumed to mean a plasma glucose level of less than 70 mg/dL.
Characteristics of the patients with more than five hypoglycemic episodes were similar to those with one to five episodes, although they were more likely to be 65 years or older, and were “slightly more likely” to be on insulin, which could possibly precipitate more hypoglycemic episodes in that group, Dr. Rajpal said.
Key findings
In the main analysis, Dr. Rajpal said, risk of CV events was significantly increased in those with more than five hypoglycemic episodes, compared with those with one to five episodes, with an odds ratio of 1.61 (95% confidence interval, 1.56-1.66). The incidence of cardiovascular events was 33.1% in those with more than five episodes and 23.5% in those with one to five episodes, according to the data presented.
Risks were also significantly increased specifically for cardiac arrhythmias, cerebrovascular accidents, and MI, Dr. Rajpal said, with ORs of 1.65 (95% CI, 1.9-1.71), 1.38 (95% CI, 1.22-1.56), and 1.43 (95% CI, 1.36-1.50), respectively.
Because individuals in the group with more than five hypoglycemic episodes were more likely to be elderly, Dr. Rajpal said that he and coinvestigators decided to perform an age-specific stratified analysis.
Although cerebral vascular incidence was low in younger patients, risk of CV events overall was nevertheless significantly elevated for those aged 65 years or older, 45-64 years, and 18-44 years, with ORs of 1.69 (95% CI, 1.61-1.7), 1.58 (95% CI, 1.48-1.69), and 1.62 (95% CI, 1.33-1.97).
“The results were still valid in stratified analysis based on different age groups,” Dr. Rajpal said.
Dr. Rajpal and coauthors reported that he had no conflicts of interest related to the research.
SOURCE: Rajpal A et al. ADA 2020, Abstract 161-OR.
FROM ADA 2020
Hospitalist well-being during the pandemic
Navigating COVID-19 requires self-care
The global COVID-19 pandemic has escalated everyone’s stress levels, especially clinicians caring for hospitalized patients. New pressures have added to everyday stress, new studies have revised prior patient care recommendations, and the world generally seems upside down. What can a busy hospitalist do to maintain a modicum of sanity in all the craziness?
The stressors facing hospitalists
Uncertainty

Of all the burdens COVID-19 has unleashed, the biggest may be uncertainty. Not only is there unease about the virus itself, there also is legitimate concern about the future of medicine, said Elizabeth Harry, MD, SFHM, a hospitalist and senior director of clinical affairs at the University of Colorado Hospital in Aurora.
“What does it look like after an event like this, particularly in areas like academic medicine and teaching our next generation and getting funding for research? And how do we continue to produce physicians that can provide excellent care?” she asked.
There is also uncertainty in the best way to care for patients, said Eileen Barrett, MD, MPH, SFHM, a hospitalist at the University of New Mexico, Albuquerque.
“There are some models that are emerging to predict who will have a worse outcome, but they’re still not great models, so we have uncertainty for a given patient.” And, she noted, as the science continues to evolve, there exists a constant worry that “you might have inadvertently caused someone harm.”

The financial implications of the pandemic are creating uncertainty too. “When you fund a health care system with elective procedures and you can’t do those, and instead have to shift to the most essential services, a lot of places are seeing a massive deficit, which is going to affect staff morale and some physician offices are going to close,” said Elisabeth Poorman, MD, MPH, a primary care and internal medicine physician and chair of the King County Medical Society Physician Wellness Committee in Seattle.
Fear
When the pandemic began in the United States, “fear of the unknown was perhaps the scariest part, particularly as it pertained to personal protective equipment,” said Mark Rudolph, MD, SFHM, chief experience officer and vice president of patient experience and physician development at Sound Physicians in Tacoma, Wash. “For most clinicians, this is the first time that they are themselves in harm’s way while they do their jobs. And worse, they risk bringing the virus home to their families. That is the concern I hear most.”
Anxiety
Worrying about being able to provide excellent patient care is a big stressor, especially since this is the heart and soul of why most hospitalists have gone into their line of work.
“Part of providing excellent care to your patients is providing excellent supportive care to their families,” Dr. Harry said. “There’s some dissonance there in not being able to allow the family to come visit, but wanting to keep them safe, and it feels really hard to support your patients and support their families in the best way. It can feel like you’re just watching and waiting to see what will happen, and that we don’t have a lot of agency over which direction things take.”
There is concern for health care team members as well, Dr. Harry added. “Physicians care a lot about their teams and how they’re doing. I think there’s a sense of esprit de corps among folks and worry for each other there.”
Guilt
Although you may be at the hospital all day, you may feel guilty when you are not providing direct patient care. Or maybe you or someone on your team has an immunodeficiency and can’t be on the front line. Perhaps one of your team members contracted COVID-19 and you did not. Whatever the case, guilt is another emotion that is rampant among hospitalists right now, Dr. Barrett said.
Burnout
Unfortunately, burnout is a potential reality in times of high stress. “Burnout is dynamic,” said Dr. Poorman. “It’s a process by which your emotional and cognitive reserves are exhausted. The people with the highest burnout are the ones who are still trying to provide the standard of care, or above the standard of care in dysfunctional systems.”
Dr. Harry noted that burnout presents in different ways for different people, but Dr. Rudolph added that it’s crucial for hospitalist team members to watch for signs of burnout so they can intervene and/or get help for their colleagues.
Warning signs in yourself or others that burnout could be on the horizon include:
- Fatigue/exhaustion – Whether emotional or physical (or both), this can become a problem if it “just doesn’t seem to go away despite rest and time away from work,” said Dr. Rudolph.
- Behavioral changes – Any behavior that’s out of the ordinary may be a red flag, like lashing out at someone at work.
- Overwork – Working too much can be caused by an inability to let go of patient care, Dr. Barrett said.
- Not working enough – This may include avoiding tasks and having difficulty meeting deadlines.
- Maladaptive coping behaviors – Excessive consumption of alcohol or drugs is a common coping mechanism. “Even excessive consumption of news is something that people are using to numb out a little bit,” said Dr. Harry.
- Depersonalization – “This is where you start to look at patients, colleagues, or administrators as ‘them’ and you can’t connect as deeply,” Dr. Harry said. “Part of that’s protective and a normal thing to do during a big trauma like this, but it’s also incredibly distancing. Any language that people start using that feels like ‘us’ or ‘them’ is a warning sign.”
- Disengagement – Many people disengage from their work, but Dr. Poorman said physicians tend to disengage from other parts of their lives, such as exercise and family interaction.
Protecting yourself while supporting others
Like the illustration of putting the oxygen mask on yourself first so you can help others, it’s important to protect your own mental and physical health as you support your fellow physicians. Here’s what the experts suggest.
Focus on basic needs
“When you’re in the midst of a trauma, which we are, you don’t want to open all of that up and go to the depths of your thoughts about the grief of all of it because it can actually make the trauma worse,” said Dr. Harry. “There’s a lot of literature that debriefing is really helpful after the event, but if you do it during the event, it can be really dangerous.”
Instead, she said, the goal should be focusing on your basic needs and what you need to do to get through each day, like keeping you and your family in good health. “What is your purpose? Staying connected to why you do this and staying focused on the present is really important,” Dr. Harry noted.
Do your best to get a good night’s sleep, exercise as much as you can, talk to others, and see a mental health provider if your anxiety is too high, advises Dr. Barrett. “Even avoiding blue light from phones and screens within 2 hours of bedtime, parking further away from the hospital and walking, and taking the stairs are things that add up in a big way.”
Keep up your normal routine
“Right now, it’s really critical for clinicians to keep up components of their routine that feel ‘normal,’ ” Dr. Rudolph said. “Whether it’s exercise, playing board games with their kids, or spending time on a hobby, it’s critical to allow yourself these comfortable, predictable, and rewarding detours.”
Set limits
People under stress tend to find unhealthy ways to cope. Instead, try being intentional about what you are consuming by putting limits on things like your news, alcohol consumption, and the number of hours you work, said Dr. Harry.
Implement a culture of wellness
Dr. Barrett believes in creating the work culture we want to be in, one that ensures people have psychological safety, allows them to ask for help, encourages them to disconnect completely from work, and makes them feel valued and listened to. She likes the example of “the pause,” which is called by a team member right after a patient expires.

“It’s a 30-second moment of silence where we reflect on the patient, their loved ones, and every member of the health care team who helped support and treat them,” said Dr. Barrett. “At the conclusion, you say: ‘Thank you. Is there anything you need to be able to go back to the care of other patients?’ Because it’s unnatural to have this terrible thing that happened and then just act like nothing happened.”
Target resources
Be proactive and know where to find resources before you need them, advised Dr. Harry. “Most institutions have free mental health resources, either through their employee assistance programs or HR, plus there’s lots of national organizations that are offering free resources to health care providers.”
Focus on what you can control
Separating what is under your control from what is not is a struggle for everyone, Dr. Poorman said, but it’s helpful to think about the ways you can have an impact and what you’re able to control.
“There was a woman who was diagnosed with early-onset Parkinson’s that I heard giving an interview at the beginning of this pandemic,” she said. “It was the most helpful advice I got, which was: ‘Think of the next good thing you can do.’ You can’t fix everything, so what’s the next good thing you can do?”
Maintain connectivity
Make sure you are utilizing your support circle and staying connected. “That sense of connection is incredibly protective on multiple fronts for depression, for burnout, for suicide ideation, etc.,” Dr. Harry said.
“It doesn’t matter if it’s your teammates at work, your family at home, your best friend from medical school – whomever you can debrief with, vent with, and just share your thoughts and feelings with, these outlets are critical for all of us to process our emotions and diffuse stress and anxiety,” said Dr. Rudolph.
Dr. Poorman is concerned that there could be a spike in physician suicides caused by increased stress, so she also encourages talking openly about what is going on and about getting help when it’s necessary. “Many of us are afraid to seek care because we can actually have our ability to practice medicine questioned, but now is not the time for heroes. Now is the time for people who are willing to recognize their own strengths and limitations to take care of one another.”
Be compassionate toward others
Keep in mind that everyone is stressed out and offer empathy and compassion. “I think everybody’s struggling to try to figure this out and the more that we can give each other the benefit of the doubt and a little grace, the more protective that is,” said Dr. Harry.

Listening is meaningful too. “Recognizing opportunities to validate and acknowledge the feelings that are being shared with you by your colleagues is critical,” Dr. Rudolph said. “We all need to know that we’re not alone, that our thoughts and feelings are okay, and when we share a difficult story, the value of someone saying something as simple as, ‘wow, that sounds like it was really hard,’ is immense.”
Be compassionate toward yourself
Try to give yourself a break and be as compassionate with yourself as you would with others. It’s okay that you’re not getting in shape, publishing prolifically, or redesigning your house right now.
“There’s a lot of data linking lack of self-compassion to burnout,” said Dr. Harry. She says there are courses on self-compassion available that help you work on being kinder to yourself.
Get a “battle buddy”
The American Medical Association has a free “buddy system” program called PeerRx to help physicians cope during the pandemic. Dr. Rudolph said that now is a great time to use this military-developed intervention in which each team member checks in with a chosen partner at agreed-upon intervals.
For example, “You can tell that person: ‘If I don’t call my family for a week that’s a red flag for me.’ And then you hold each other accountable to those things,” Dr. Harry said.
The buddy system is another way to harness that sense of connection that is so vital to our health and well-being.
“The simple act of showing that you care … can make all the difference when you’re doing this kind of work that is both challenging and dangerous,” said Dr. Rudolph.
Navigating COVID-19 requires self-care
Navigating COVID-19 requires self-care
The global COVID-19 pandemic has escalated everyone’s stress levels, especially clinicians caring for hospitalized patients. New pressures have added to everyday stress, new studies have revised prior patient care recommendations, and the world generally seems upside down. What can a busy hospitalist do to maintain a modicum of sanity in all the craziness?
The stressors facing hospitalists
Uncertainty
Of all the burdens COVID-19 has unleashed, the biggest may be uncertainty. Not only is there unease about the virus itself, there also is legitimate concern about the future of medicine, said Elizabeth Harry, MD, SFHM, a hospitalist and senior director of clinical affairs at the University of Colorado Hospital in Aurora.
“What does it look like after an event like this, particularly in areas like academic medicine and teaching our next generation and getting funding for research? And how do we continue to produce physicians that can provide excellent care?” she asked.
There is also uncertainty in the best way to care for patients, said Eileen Barrett, MD, MPH, SFHM, a hospitalist at the University of New Mexico, Albuquerque.
“There are some models that are emerging to predict who will have a worse outcome, but they’re still not great models, so we have uncertainty for a given patient.” And, she noted, as the science continues to evolve, there exists a constant worry that “you might have inadvertently caused someone harm.”
The financial implications of the pandemic are creating uncertainty too. “When you fund a health care system with elective procedures and you can’t do those, and instead have to shift to the most essential services, a lot of places are seeing a massive deficit, which is going to affect staff morale and some physician offices are going to close,” said Elisabeth Poorman, MD, MPH, a primary care and internal medicine physician and chair of the King County Medical Society Physician Wellness Committee in Seattle.
Fear
When the pandemic began in the United States, “fear of the unknown was perhaps the scariest part, particularly as it pertained to personal protective equipment,” said Mark Rudolph, MD, SFHM, chief experience officer and vice president of patient experience and physician development at Sound Physicians in Tacoma, Wash. “For most clinicians, this is the first time that they are themselves in harm’s way while they do their jobs. And worse, they risk bringing the virus home to their families. That is the concern I hear most.”
Anxiety
Worrying about being able to provide excellent patient care is a big stressor, especially since this is the heart and soul of why most hospitalists have gone into their line of work.
“Part of providing excellent care to your patients is providing excellent supportive care to their families,” Dr. Harry said. “There’s some dissonance there in not being able to allow the family to come visit, but wanting to keep them safe, and it feels really hard to support your patients and support their families in the best way. It can feel like you’re just watching and waiting to see what will happen, and that we don’t have a lot of agency over which direction things take.”
There is concern for health care team members as well, Dr. Harry added. “Physicians care a lot about their teams and how they’re doing. I think there’s a sense of esprit de corps among folks and worry for each other there.”
Guilt
Although you may be at the hospital all day, you may feel guilty when you are not providing direct patient care. Or maybe you or someone on your team has an immunodeficiency and can’t be on the front line. Perhaps one of your team members contracted COVID-19 and you did not. Whatever the case, guilt is another emotion that is rampant among hospitalists right now, Dr. Barrett said.
Burnout
Unfortunately, burnout is a potential reality in times of high stress. “Burnout is dynamic,” said Dr. Poorman. “It’s a process by which your emotional and cognitive reserves are exhausted. The people with the highest burnout are the ones who are still trying to provide the standard of care, or above the standard of care in dysfunctional systems.”
Dr. Harry noted that burnout presents in different ways for different people, but Dr. Rudolph added that it’s crucial for hospitalist team members to watch for signs of burnout so they can intervene and/or get help for their colleagues.
Warning signs in yourself or others that burnout could be on the horizon include:
- Fatigue/exhaustion – Whether emotional or physical (or both), this can become a problem if it “just doesn’t seem to go away despite rest and time away from work,” said Dr. Rudolph.
- Behavioral changes – Any behavior that’s out of the ordinary may be a red flag, like lashing out at someone at work.
- Overwork – Working too much can be caused by an inability to let go of patient care, Dr. Barrett said.
- Not working enough – This may include avoiding tasks and having difficulty meeting deadlines.
- Maladaptive coping behaviors – Excessive consumption of alcohol or drugs is a common coping mechanism. “Even excessive consumption of news is something that people are using to numb out a little bit,” said Dr. Harry.
- Depersonalization – “This is where you start to look at patients, colleagues, or administrators as ‘them’ and you can’t connect as deeply,” Dr. Harry said. “Part of that’s protective and a normal thing to do during a big trauma like this, but it’s also incredibly distancing. Any language that people start using that feels like ‘us’ or ‘them’ is a warning sign.”
- Disengagement – Many people disengage from their work, but Dr. Poorman said physicians tend to disengage from other parts of their lives, such as exercise and family interaction.
Protecting yourself while supporting others
Like the illustration of putting the oxygen mask on yourself first so you can help others, it’s important to protect your own mental and physical health as you support your fellow physicians. Here’s what the experts suggest.
Focus on basic needs
“When you’re in the midst of a trauma, which we are, you don’t want to open all of that up and go to the depths of your thoughts about the grief of all of it because it can actually make the trauma worse,” said Dr. Harry. “There’s a lot of literature that debriefing is really helpful after the event, but if you do it during the event, it can be really dangerous.”
Instead, she said, the goal should be focusing on your basic needs and what you need to do to get through each day, like keeping you and your family in good health. “What is your purpose? Staying connected to why you do this and staying focused on the present is really important,” Dr. Harry noted.
Do your best to get a good night’s sleep, exercise as much as you can, talk to others, and see a mental health provider if your anxiety is too high, advises Dr. Barrett. “Even avoiding blue light from phones and screens within 2 hours of bedtime, parking further away from the hospital and walking, and taking the stairs are things that add up in a big way.”
Keep up your normal routine
“Right now, it’s really critical for clinicians to keep up components of their routine that feel ‘normal,’ ” Dr. Rudolph said. “Whether it’s exercise, playing board games with their kids, or spending time on a hobby, it’s critical to allow yourself these comfortable, predictable, and rewarding detours.”
Set limits
People under stress tend to find unhealthy ways to cope. Instead, try being intentional about what you are consuming by putting limits on things like your news, alcohol consumption, and the number of hours you work, said Dr. Harry.
Implement a culture of wellness
Dr. Barrett believes in creating the work culture we want to be in, one that ensures people have psychological safety, allows them to ask for help, encourages them to disconnect completely from work, and makes them feel valued and listened to. She likes the example of “the pause,” which is called by a team member right after a patient expires.
“It’s a 30-second moment of silence where we reflect on the patient, their loved ones, and every member of the health care team who helped support and treat them,” said Dr. Barrett. “At the conclusion, you say: ‘Thank you. Is there anything you need to be able to go back to the care of other patients?’ Because it’s unnatural to have this terrible thing that happened and then just act like nothing happened.”
Target resources
Be proactive and know where to find resources before you need them, advised Dr. Harry. “Most institutions have free mental health resources, either through their employee assistance programs or HR, plus there’s lots of national organizations that are offering free resources to health care providers.”
Focus on what you can control
Separating what is under your control from what is not is a struggle for everyone, Dr. Poorman said, but it’s helpful to think about the ways you can have an impact and what you’re able to control.
“There was a woman who was diagnosed with early-onset Parkinson’s that I heard giving an interview at the beginning of this pandemic,” she said. “It was the most helpful advice I got, which was: ‘Think of the next good thing you can do.’ You can’t fix everything, so what’s the next good thing you can do?”
Maintain connectivity
Make sure you are utilizing your support circle and staying connected. “That sense of connection is incredibly protective on multiple fronts for depression, for burnout, for suicide ideation, etc.,” Dr. Harry said.
“It doesn’t matter if it’s your teammates at work, your family at home, your best friend from medical school – whomever you can debrief with, vent with, and just share your thoughts and feelings with, these outlets are critical for all of us to process our emotions and diffuse stress and anxiety,” said Dr. Rudolph.
Dr. Poorman is concerned that there could be a spike in physician suicides caused by increased stress, so she also encourages talking openly about what is going on and about getting help when it’s necessary. “Many of us are afraid to seek care because we can actually have our ability to practice medicine questioned, but now is not the time for heroes. Now is the time for people who are willing to recognize their own strengths and limitations to take care of one another.”
Be compassionate toward others
Keep in mind that everyone is stressed out and offer empathy and compassion. “I think everybody’s struggling to try to figure this out and the more that we can give each other the benefit of the doubt and a little grace, the more protective that is,” said Dr. Harry.
Listening is meaningful too. “Recognizing opportunities to validate and acknowledge the feelings that are being shared with you by your colleagues is critical,” Dr. Rudolph said. “We all need to know that we’re not alone, that our thoughts and feelings are okay, and when we share a difficult story, the value of someone saying something as simple as, ‘wow, that sounds like it was really hard,’ is immense.”
Be compassionate toward yourself
Try to give yourself a break and be as compassionate with yourself as you would with others. It’s okay that you’re not getting in shape, publishing prolifically, or redesigning your house right now.
“There’s a lot of data linking lack of self-compassion to burnout,” said Dr. Harry. She says there are courses on self-compassion available that help you work on being kinder to yourself.
Get a “battle buddy”
The American Medical Association has a free “buddy system” program called PeerRx to help physicians cope during the pandemic. Dr. Rudolph said that now is a great time to use this military-developed intervention in which each team member checks in with a chosen partner at agreed-upon intervals.
For example, “You can tell that person: ‘If I don’t call my family for a week that’s a red flag for me.’ And then you hold each other accountable to those things,” Dr. Harry said.
The buddy system is another way to harness that sense of connection that is so vital to our health and well-being.
“The simple act of showing that you care … can make all the difference when you’re doing this kind of work that is both challenging and dangerous,” said Dr. Rudolph.
The global COVID-19 pandemic has escalated everyone’s stress levels, especially clinicians caring for hospitalized patients. New pressures have added to everyday stress, new studies have revised prior patient care recommendations, and the world generally seems upside down. What can a busy hospitalist do to maintain a modicum of sanity in all the craziness?
The stressors facing hospitalists
Uncertainty
Of all the burdens COVID-19 has unleashed, the biggest may be uncertainty. Not only is there unease about the virus itself, there also is legitimate concern about the future of medicine, said Elizabeth Harry, MD, SFHM, a hospitalist and senior director of clinical affairs at the University of Colorado Hospital in Aurora.
“What does it look like after an event like this, particularly in areas like academic medicine and teaching our next generation and getting funding for research? And how do we continue to produce physicians that can provide excellent care?” she asked.
There is also uncertainty in the best way to care for patients, said Eileen Barrett, MD, MPH, SFHM, a hospitalist at the University of New Mexico, Albuquerque.
“There are some models that are emerging to predict who will have a worse outcome, but they’re still not great models, so we have uncertainty for a given patient.” And, she noted, as the science continues to evolve, there exists a constant worry that “you might have inadvertently caused someone harm.”
The financial implications of the pandemic are creating uncertainty too. “When you fund a health care system with elective procedures and you can’t do those, and instead have to shift to the most essential services, a lot of places are seeing a massive deficit, which is going to affect staff morale and some physician offices are going to close,” said Elisabeth Poorman, MD, MPH, a primary care and internal medicine physician and chair of the King County Medical Society Physician Wellness Committee in Seattle.
Fear
When the pandemic began in the United States, “fear of the unknown was perhaps the scariest part, particularly as it pertained to personal protective equipment,” said Mark Rudolph, MD, SFHM, chief experience officer and vice president of patient experience and physician development at Sound Physicians in Tacoma, Wash. “For most clinicians, this is the first time that they are themselves in harm’s way while they do their jobs. And worse, they risk bringing the virus home to their families. That is the concern I hear most.”
Anxiety
Worrying about being able to provide excellent patient care is a big stressor, especially since this is the heart and soul of why most hospitalists have gone into their line of work.
“Part of providing excellent care to your patients is providing excellent supportive care to their families,” Dr. Harry said. “There’s some dissonance there in not being able to allow the family to come visit, but wanting to keep them safe, and it feels really hard to support your patients and support their families in the best way. It can feel like you’re just watching and waiting to see what will happen, and that we don’t have a lot of agency over which direction things take.”
There is concern for health care team members as well, Dr. Harry added. “Physicians care a lot about their teams and how they’re doing. I think there’s a sense of esprit de corps among folks and worry for each other there.”
Guilt
Although you may be at the hospital all day, you may feel guilty when you are not providing direct patient care. Or maybe you or someone on your team has an immunodeficiency and can’t be on the front line. Perhaps one of your team members contracted COVID-19 and you did not. Whatever the case, guilt is another emotion that is rampant among hospitalists right now, Dr. Barrett said.
Burnout
Unfortunately, burnout is a potential reality in times of high stress. “Burnout is dynamic,” said Dr. Poorman. “It’s a process by which your emotional and cognitive reserves are exhausted. The people with the highest burnout are the ones who are still trying to provide the standard of care, or above the standard of care in dysfunctional systems.”
Dr. Harry noted that burnout presents in different ways for different people, but Dr. Rudolph added that it’s crucial for hospitalist team members to watch for signs of burnout so they can intervene and/or get help for their colleagues.
Warning signs in yourself or others that burnout could be on the horizon include:
- Fatigue/exhaustion – Whether emotional or physical (or both), this can become a problem if it “just doesn’t seem to go away despite rest and time away from work,” said Dr. Rudolph.
- Behavioral changes – Any behavior that’s out of the ordinary may be a red flag, like lashing out at someone at work.
- Overwork – Working too much can be caused by an inability to let go of patient care, Dr. Barrett said.
- Not working enough – This may include avoiding tasks and having difficulty meeting deadlines.
- Maladaptive coping behaviors – Excessive consumption of alcohol or drugs is a common coping mechanism. “Even excessive consumption of news is something that people are using to numb out a little bit,” said Dr. Harry.
- Depersonalization – “This is where you start to look at patients, colleagues, or administrators as ‘them’ and you can’t connect as deeply,” Dr. Harry said. “Part of that’s protective and a normal thing to do during a big trauma like this, but it’s also incredibly distancing. Any language that people start using that feels like ‘us’ or ‘them’ is a warning sign.”
- Disengagement – Many people disengage from their work, but Dr. Poorman said physicians tend to disengage from other parts of their lives, such as exercise and family interaction.
Protecting yourself while supporting others
Like the illustration of putting the oxygen mask on yourself first so you can help others, it’s important to protect your own mental and physical health as you support your fellow physicians. Here’s what the experts suggest.
Focus on basic needs
“When you’re in the midst of a trauma, which we are, you don’t want to open all of that up and go to the depths of your thoughts about the grief of all of it because it can actually make the trauma worse,” said Dr. Harry. “There’s a lot of literature that debriefing is really helpful after the event, but if you do it during the event, it can be really dangerous.”
Instead, she said, the goal should be focusing on your basic needs and what you need to do to get through each day, like keeping you and your family in good health. “What is your purpose? Staying connected to why you do this and staying focused on the present is really important,” Dr. Harry noted.
Do your best to get a good night’s sleep, exercise as much as you can, talk to others, and see a mental health provider if your anxiety is too high, advises Dr. Barrett. “Even avoiding blue light from phones and screens within 2 hours of bedtime, parking further away from the hospital and walking, and taking the stairs are things that add up in a big way.”
Keep up your normal routine
“Right now, it’s really critical for clinicians to keep up components of their routine that feel ‘normal,’ ” Dr. Rudolph said. “Whether it’s exercise, playing board games with their kids, or spending time on a hobby, it’s critical to allow yourself these comfortable, predictable, and rewarding detours.”
Set limits
People under stress tend to find unhealthy ways to cope. Instead, try being intentional about what you are consuming by putting limits on things like your news, alcohol consumption, and the number of hours you work, said Dr. Harry.
Implement a culture of wellness
Dr. Barrett believes in creating the work culture we want to be in, one that ensures people have psychological safety, allows them to ask for help, encourages them to disconnect completely from work, and makes them feel valued and listened to. She likes the example of “the pause,” which is called by a team member right after a patient expires.
“It’s a 30-second moment of silence where we reflect on the patient, their loved ones, and every member of the health care team who helped support and treat them,” said Dr. Barrett. “At the conclusion, you say: ‘Thank you. Is there anything you need to be able to go back to the care of other patients?’ Because it’s unnatural to have this terrible thing that happened and then just act like nothing happened.”
Target resources
Be proactive and know where to find resources before you need them, advised Dr. Harry. “Most institutions have free mental health resources, either through their employee assistance programs or HR, plus there’s lots of national organizations that are offering free resources to health care providers.”
Focus on what you can control
Separating what is under your control from what is not is a struggle for everyone, Dr. Poorman said, but it’s helpful to think about the ways you can have an impact and what you’re able to control.
“There was a woman who was diagnosed with early-onset Parkinson’s that I heard giving an interview at the beginning of this pandemic,” she said. “It was the most helpful advice I got, which was: ‘Think of the next good thing you can do.’ You can’t fix everything, so what’s the next good thing you can do?”
Maintain connectivity
Make sure you are utilizing your support circle and staying connected. “That sense of connection is incredibly protective on multiple fronts for depression, for burnout, for suicide ideation, etc.,” Dr. Harry said.
“It doesn’t matter if it’s your teammates at work, your family at home, your best friend from medical school – whomever you can debrief with, vent with, and just share your thoughts and feelings with, these outlets are critical for all of us to process our emotions and diffuse stress and anxiety,” said Dr. Rudolph.
Dr. Poorman is concerned that there could be a spike in physician suicides caused by increased stress, so she also encourages talking openly about what is going on and about getting help when it’s necessary. “Many of us are afraid to seek care because we can actually have our ability to practice medicine questioned, but now is not the time for heroes. Now is the time for people who are willing to recognize their own strengths and limitations to take care of one another.”
Be compassionate toward others
Keep in mind that everyone is stressed out and offer empathy and compassion. “I think everybody’s struggling to try to figure this out and the more that we can give each other the benefit of the doubt and a little grace, the more protective that is,” said Dr. Harry.
Listening is meaningful too. “Recognizing opportunities to validate and acknowledge the feelings that are being shared with you by your colleagues is critical,” Dr. Rudolph said. “We all need to know that we’re not alone, that our thoughts and feelings are okay, and when we share a difficult story, the value of someone saying something as simple as, ‘wow, that sounds like it was really hard,’ is immense.”
Be compassionate toward yourself
Try to give yourself a break and be as compassionate with yourself as you would with others. It’s okay that you’re not getting in shape, publishing prolifically, or redesigning your house right now.
“There’s a lot of data linking lack of self-compassion to burnout,” said Dr. Harry. She says there are courses on self-compassion available that help you work on being kinder to yourself.
Get a “battle buddy”
The American Medical Association has a free “buddy system” program called PeerRx to help physicians cope during the pandemic. Dr. Rudolph said that now is a great time to use this military-developed intervention in which each team member checks in with a chosen partner at agreed-upon intervals.
For example, “You can tell that person: ‘If I don’t call my family for a week that’s a red flag for me.’ And then you hold each other accountable to those things,” Dr. Harry said.
The buddy system is another way to harness that sense of connection that is so vital to our health and well-being.
“The simple act of showing that you care … can make all the difference when you’re doing this kind of work that is both challenging and dangerous,” said Dr. Rudolph.
Robotics lightens load for bariatric surgeons in super obese
Use of a robotics platform provides a surgeon with more information so they can make better decisions, especially in challenging situations of primary and revisional bariatric surgery, according to Cheguevara Afaneh, MD, of New York–Presbyterian Hospital and Weill Cornell Medical Center, New York.
“The value of modern technology is to be able to do the most difficult cases in a much simpler format,” he said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Dr. Afaneh shared examples of how robotic assistance can help surgeons address challenges in bariatric surgery clinical practice, including managing super- and super-super-obese patients, dealing with gastroesophageal reflux disease (GERD), and negating the impact of surgical assistant experience.
“Super-obese patients pose more of a challenge interoperatively for both the surgeon and the assistant,” Dr. Afaneh noted. He and colleagues conducted a study of perioperative outcomes and found no significant differences between morbidly obese and super-obese patients in perioperative morbidity or operating time when a robotic platform was used.
The benefits to the surgeon when using robotic assistance in super-obese patients include effortless navigation of the abdominal wall, the ability to execute complex maneuvers in a challenging environment, and the security of a stable platform with no assistant fatigue, Dr. Afaneh emphasized. “When you are using the robotic platform, you are negating a lot of the patient factors” and fatigue factors that make bariatric surgery in super-obese and super-super-obese patients especially difficult, he said.
For example, in a patient who weighed nearly 500 pounds, pulling up on the stomach to get behind the actual stomach is easier because assistant fatigue is not a factor, so the surgeon can take more time and prevent a more difficult dissection, he said. In addition, Dr. Afaneh’s research showed no difference in operative time, and that the robot assistance outcomes were reproducible across a range of body mass index categories.
Robotic assistance also allows for comparable outcomes in surgeons with less experience, notably in revisional surgery, said Dr. Afaneh. He reviewed data from his first year of experience in revisional procedures using robotic assistance to his partners’ more than 20 years of laparoscopic experience. He found no significant differences in operative time, complications, or conversions to open procedures.
However, the more important message from the study was that less experienced surgeons were able to safely perform some of the most difficult revisional procedures without increasing morbidity, compared with more experienced surgeons. The data suggest that, with robotic assistance, surgeons early in their career can take on some of the bigger cases and expect outcomes similar to those of more experienced surgeons, Dr. Afaneh said.
Robotics has demonstrated improved outcomes in managing patients with GERD, which has become a common problem after bariatric surgery, noted Dr. Afaneh. When he and his colleagues reviewed data from their center on robotic-assisted approaches to GERD after bariatric surgery, they found that, even in primary magnetic sphincter operations, “robotics maintains comparable outcomes in revisional sleeve gastrectomy fields,” he said.
Another notable benefit of robotics in bariatric surgery is the negation of the “assistant effect,” said Dr. Afaneh. Often, less experienced surgeons are matched with less experienced assistants. “We took a look at the use of the robotic in cases of complex GI surgeries,” he said. They compared laparoscopic and robotic cases and stratified them by third-year assistant or fellow. “If you had a fellow, the operative time dropped by half an hour for laparoscopic cases, but the time was no different in robotics cases,” regardless of the use of fellow or third-year assistant, he said.
“The robotic platform allows you to assist yourself,” and allows for full surgeon autonomy, Dr. Afaneh emphasized. “You are the best person at predicting your next step.” The robotics platform also serves as a teaching tool. “For those who teach, there is no added morbidity based on the assistance of the trainee,” he said. In addition, the improved visualization of robotics “allows for better appreciation of scarred tissue planes and more precise suturing,” he noted.
Overall, “one of the values of the robotic platform is shortening the learning curve,” Dr. Afaneh said. He reviewed data from his fellows and himself, and found no difference in operative times. “My mentee was able to achieve operative times as good as my third year in practice. The robotic platform shaved off several years of learning experience,” he said. Dr. Afaneh’s operative times also decreased with robotics, which shows how experienced surgeons learn from this technology, he said.
Dr. Afaneh disclosed serving as a consultant for Intuitive Surgical.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Use of a robotics platform provides a surgeon with more information so they can make better decisions, especially in challenging situations of primary and revisional bariatric surgery, according to Cheguevara Afaneh, MD, of New York–Presbyterian Hospital and Weill Cornell Medical Center, New York.
“The value of modern technology is to be able to do the most difficult cases in a much simpler format,” he said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Dr. Afaneh shared examples of how robotic assistance can help surgeons address challenges in bariatric surgery clinical practice, including managing super- and super-super-obese patients, dealing with gastroesophageal reflux disease (GERD), and negating the impact of surgical assistant experience.
“Super-obese patients pose more of a challenge interoperatively for both the surgeon and the assistant,” Dr. Afaneh noted. He and colleagues conducted a study of perioperative outcomes and found no significant differences between morbidly obese and super-obese patients in perioperative morbidity or operating time when a robotic platform was used.
The benefits to the surgeon when using robotic assistance in super-obese patients include effortless navigation of the abdominal wall, the ability to execute complex maneuvers in a challenging environment, and the security of a stable platform with no assistant fatigue, Dr. Afaneh emphasized. “When you are using the robotic platform, you are negating a lot of the patient factors” and fatigue factors that make bariatric surgery in super-obese and super-super-obese patients especially difficult, he said.
For example, in a patient who weighed nearly 500 pounds, pulling up on the stomach to get behind the actual stomach is easier because assistant fatigue is not a factor, so the surgeon can take more time and prevent a more difficult dissection, he said. In addition, Dr. Afaneh’s research showed no difference in operative time, and that the robot assistance outcomes were reproducible across a range of body mass index categories.
Robotic assistance also allows for comparable outcomes in surgeons with less experience, notably in revisional surgery, said Dr. Afaneh. He reviewed data from his first year of experience in revisional procedures using robotic assistance to his partners’ more than 20 years of laparoscopic experience. He found no significant differences in operative time, complications, or conversions to open procedures.
However, the more important message from the study was that less experienced surgeons were able to safely perform some of the most difficult revisional procedures without increasing morbidity, compared with more experienced surgeons. The data suggest that, with robotic assistance, surgeons early in their career can take on some of the bigger cases and expect outcomes similar to those of more experienced surgeons, Dr. Afaneh said.
Robotics has demonstrated improved outcomes in managing patients with GERD, which has become a common problem after bariatric surgery, noted Dr. Afaneh. When he and his colleagues reviewed data from their center on robotic-assisted approaches to GERD after bariatric surgery, they found that, even in primary magnetic sphincter operations, “robotics maintains comparable outcomes in revisional sleeve gastrectomy fields,” he said.
Another notable benefit of robotics in bariatric surgery is the negation of the “assistant effect,” said Dr. Afaneh. Often, less experienced surgeons are matched with less experienced assistants. “We took a look at the use of the robotic in cases of complex GI surgeries,” he said. They compared laparoscopic and robotic cases and stratified them by third-year assistant or fellow. “If you had a fellow, the operative time dropped by half an hour for laparoscopic cases, but the time was no different in robotics cases,” regardless of the use of fellow or third-year assistant, he said.
“The robotic platform allows you to assist yourself,” and allows for full surgeon autonomy, Dr. Afaneh emphasized. “You are the best person at predicting your next step.” The robotics platform also serves as a teaching tool. “For those who teach, there is no added morbidity based on the assistance of the trainee,” he said. In addition, the improved visualization of robotics “allows for better appreciation of scarred tissue planes and more precise suturing,” he noted.
Overall, “one of the values of the robotic platform is shortening the learning curve,” Dr. Afaneh said. He reviewed data from his fellows and himself, and found no difference in operative times. “My mentee was able to achieve operative times as good as my third year in practice. The robotic platform shaved off several years of learning experience,” he said. Dr. Afaneh’s operative times also decreased with robotics, which shows how experienced surgeons learn from this technology, he said.
Dr. Afaneh disclosed serving as a consultant for Intuitive Surgical.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Use of a robotics platform provides a surgeon with more information so they can make better decisions, especially in challenging situations of primary and revisional bariatric surgery, according to Cheguevara Afaneh, MD, of New York–Presbyterian Hospital and Weill Cornell Medical Center, New York.
“The value of modern technology is to be able to do the most difficult cases in a much simpler format,” he said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Dr. Afaneh shared examples of how robotic assistance can help surgeons address challenges in bariatric surgery clinical practice, including managing super- and super-super-obese patients, dealing with gastroesophageal reflux disease (GERD), and negating the impact of surgical assistant experience.
“Super-obese patients pose more of a challenge interoperatively for both the surgeon and the assistant,” Dr. Afaneh noted. He and colleagues conducted a study of perioperative outcomes and found no significant differences between morbidly obese and super-obese patients in perioperative morbidity or operating time when a robotic platform was used.
The benefits to the surgeon when using robotic assistance in super-obese patients include effortless navigation of the abdominal wall, the ability to execute complex maneuvers in a challenging environment, and the security of a stable platform with no assistant fatigue, Dr. Afaneh emphasized. “When you are using the robotic platform, you are negating a lot of the patient factors” and fatigue factors that make bariatric surgery in super-obese and super-super-obese patients especially difficult, he said.
For example, in a patient who weighed nearly 500 pounds, pulling up on the stomach to get behind the actual stomach is easier because assistant fatigue is not a factor, so the surgeon can take more time and prevent a more difficult dissection, he said. In addition, Dr. Afaneh’s research showed no difference in operative time, and that the robot assistance outcomes were reproducible across a range of body mass index categories.
Robotic assistance also allows for comparable outcomes in surgeons with less experience, notably in revisional surgery, said Dr. Afaneh. He reviewed data from his first year of experience in revisional procedures using robotic assistance to his partners’ more than 20 years of laparoscopic experience. He found no significant differences in operative time, complications, or conversions to open procedures.
However, the more important message from the study was that less experienced surgeons were able to safely perform some of the most difficult revisional procedures without increasing morbidity, compared with more experienced surgeons. The data suggest that, with robotic assistance, surgeons early in their career can take on some of the bigger cases and expect outcomes similar to those of more experienced surgeons, Dr. Afaneh said.
Robotics has demonstrated improved outcomes in managing patients with GERD, which has become a common problem after bariatric surgery, noted Dr. Afaneh. When he and his colleagues reviewed data from their center on robotic-assisted approaches to GERD after bariatric surgery, they found that, even in primary magnetic sphincter operations, “robotics maintains comparable outcomes in revisional sleeve gastrectomy fields,” he said.
Another notable benefit of robotics in bariatric surgery is the negation of the “assistant effect,” said Dr. Afaneh. Often, less experienced surgeons are matched with less experienced assistants. “We took a look at the use of the robotic in cases of complex GI surgeries,” he said. They compared laparoscopic and robotic cases and stratified them by third-year assistant or fellow. “If you had a fellow, the operative time dropped by half an hour for laparoscopic cases, but the time was no different in robotics cases,” regardless of the use of fellow or third-year assistant, he said.
“The robotic platform allows you to assist yourself,” and allows for full surgeon autonomy, Dr. Afaneh emphasized. “You are the best person at predicting your next step.” The robotics platform also serves as a teaching tool. “For those who teach, there is no added morbidity based on the assistance of the trainee,” he said. In addition, the improved visualization of robotics “allows for better appreciation of scarred tissue planes and more precise suturing,” he noted.
Overall, “one of the values of the robotic platform is shortening the learning curve,” Dr. Afaneh said. He reviewed data from his fellows and himself, and found no difference in operative times. “My mentee was able to achieve operative times as good as my third year in practice. The robotic platform shaved off several years of learning experience,” he said. Dr. Afaneh’s operative times also decreased with robotics, which shows how experienced surgeons learn from this technology, he said.
Dr. Afaneh disclosed serving as a consultant for Intuitive Surgical.
Global Academy for Medical Education and this news organization are owned by the same parent company.
FROM MISS
Comorbidities increase COVID-19 deaths by factor of 12
, compared with those who have no such condition, according to the Centers for Disease Control and Prevention.
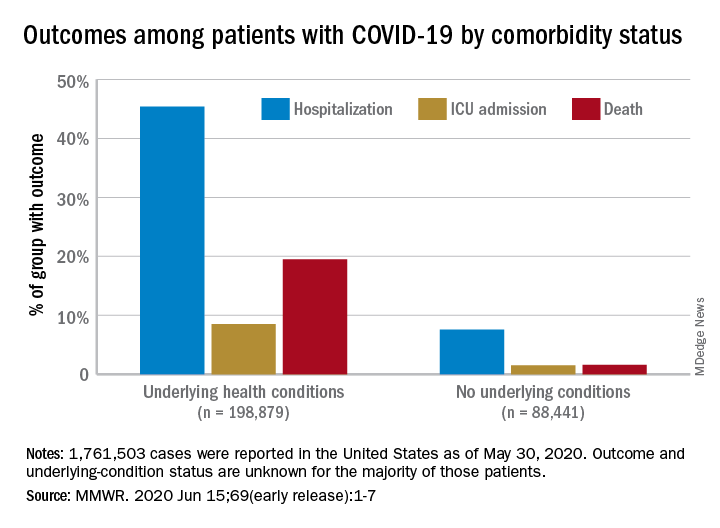
Among those with underlying conditions such as cardiovascular disease or diabetes, 45.4% of patients with COVID-19 were hospitalized, versus 7.6% of patients without an underlying condition, said Erin K. Stokes, MPH, and associates of the CDC COVID-19 Emergency Response team.
The difference in deaths was even greater over the study period of Jan. 22–May 30, 2020: 19.5% of COVID-19 patients with underlying conditions died, compared with 1.6% of those with no underlying condition. The gap narrowed, however, for ICU admissions, with corresponding rates of 8.5% and 1.5%, the investigators reported June 15 in the Morbidity and Mortality Weekly Report.
“The COVID-19 pandemic continues to be severe, particularly in certain population groups,” they said.
The cumulative incidence of laboratory-confirmed cases up to May 30, for instance, was nearly twice as high for those aged 80 years and over (902 per 100,000 population) than for those aged 70-79 years (464.2 per 100,000). Those aged 50-59 years had the second-highest incidence, 550.5 per 100,000, Ms. Stokes and associates said.
“Among cases with known race and ethnicity, 33% of persons were Hispanic, 22% were black, and 1.3% were [American Indian/Alaska Native]. These findings suggest that persons in these groups, who account for 18%, 13%, and 0.7% of the U.S. population, respectively, are disproportionately affected by the COVID-19 pandemic,” they wrote.
Another source of disparity: “Incidence among males and females was similar overall, [but] severe outcomes were more commonly reported among males,” the investigators noted. Cumulative incidence was 401.1 per 100,000 for males and 406.0 for females, but 6.0% of male patients died, compared with 4.8% of females.
As of May 30, a total of 1,761,503 cases and 103,700 deaths had been reported to the CDC. Of those cases, approximately 1.3 million were included in the analysis, with data on individual underlying health conditions available for 287,320 (22%). The split on those cases was 198,879 with health conditions and 88,411 without, the CDC data show.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females, Ms. Stokes and associates said.
The pandemic “is an ongoing public health crisis in the United States that continues to affect all populations and result in severe outcomes including death,” they said, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.”
SOURCE: Stokes EK et al. MMWR. 2020 Jun 15;69(early release):1-7.
, compared with those who have no such condition, according to the Centers for Disease Control and Prevention.
Among those with underlying conditions such as cardiovascular disease or diabetes, 45.4% of patients with COVID-19 were hospitalized, versus 7.6% of patients without an underlying condition, said Erin K. Stokes, MPH, and associates of the CDC COVID-19 Emergency Response team.
The difference in deaths was even greater over the study period of Jan. 22–May 30, 2020: 19.5% of COVID-19 patients with underlying conditions died, compared with 1.6% of those with no underlying condition. The gap narrowed, however, for ICU admissions, with corresponding rates of 8.5% and 1.5%, the investigators reported June 15 in the Morbidity and Mortality Weekly Report.
“The COVID-19 pandemic continues to be severe, particularly in certain population groups,” they said.
The cumulative incidence of laboratory-confirmed cases up to May 30, for instance, was nearly twice as high for those aged 80 years and over (902 per 100,000 population) than for those aged 70-79 years (464.2 per 100,000). Those aged 50-59 years had the second-highest incidence, 550.5 per 100,000, Ms. Stokes and associates said.
“Among cases with known race and ethnicity, 33% of persons were Hispanic, 22% were black, and 1.3% were [American Indian/Alaska Native]. These findings suggest that persons in these groups, who account for 18%, 13%, and 0.7% of the U.S. population, respectively, are disproportionately affected by the COVID-19 pandemic,” they wrote.
Another source of disparity: “Incidence among males and females was similar overall, [but] severe outcomes were more commonly reported among males,” the investigators noted. Cumulative incidence was 401.1 per 100,000 for males and 406.0 for females, but 6.0% of male patients died, compared with 4.8% of females.
As of May 30, a total of 1,761,503 cases and 103,700 deaths had been reported to the CDC. Of those cases, approximately 1.3 million were included in the analysis, with data on individual underlying health conditions available for 287,320 (22%). The split on those cases was 198,879 with health conditions and 88,411 without, the CDC data show.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females, Ms. Stokes and associates said.
The pandemic “is an ongoing public health crisis in the United States that continues to affect all populations and result in severe outcomes including death,” they said, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.”
SOURCE: Stokes EK et al. MMWR. 2020 Jun 15;69(early release):1-7.
, compared with those who have no such condition, according to the Centers for Disease Control and Prevention.
Among those with underlying conditions such as cardiovascular disease or diabetes, 45.4% of patients with COVID-19 were hospitalized, versus 7.6% of patients without an underlying condition, said Erin K. Stokes, MPH, and associates of the CDC COVID-19 Emergency Response team.
The difference in deaths was even greater over the study period of Jan. 22–May 30, 2020: 19.5% of COVID-19 patients with underlying conditions died, compared with 1.6% of those with no underlying condition. The gap narrowed, however, for ICU admissions, with corresponding rates of 8.5% and 1.5%, the investigators reported June 15 in the Morbidity and Mortality Weekly Report.
“The COVID-19 pandemic continues to be severe, particularly in certain population groups,” they said.
The cumulative incidence of laboratory-confirmed cases up to May 30, for instance, was nearly twice as high for those aged 80 years and over (902 per 100,000 population) than for those aged 70-79 years (464.2 per 100,000). Those aged 50-59 years had the second-highest incidence, 550.5 per 100,000, Ms. Stokes and associates said.
“Among cases with known race and ethnicity, 33% of persons were Hispanic, 22% were black, and 1.3% were [American Indian/Alaska Native]. These findings suggest that persons in these groups, who account for 18%, 13%, and 0.7% of the U.S. population, respectively, are disproportionately affected by the COVID-19 pandemic,” they wrote.
Another source of disparity: “Incidence among males and females was similar overall, [but] severe outcomes were more commonly reported among males,” the investigators noted. Cumulative incidence was 401.1 per 100,000 for males and 406.0 for females, but 6.0% of male patients died, compared with 4.8% of females.
As of May 30, a total of 1,761,503 cases and 103,700 deaths had been reported to the CDC. Of those cases, approximately 1.3 million were included in the analysis, with data on individual underlying health conditions available for 287,320 (22%). The split on those cases was 198,879 with health conditions and 88,411 without, the CDC data show.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females, Ms. Stokes and associates said.
The pandemic “is an ongoing public health crisis in the United States that continues to affect all populations and result in severe outcomes including death,” they said, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.”
SOURCE: Stokes EK et al. MMWR. 2020 Jun 15;69(early release):1-7.
FROM MMWR
Weight loss stays consistent in one- and two-step in gastric band conversion
with either a one- or two-step procedure, a study of 78 patients showed.
“Laparoscopic adjustable gastric banding (LAGB) has largely fallen out of favor, likely related to variable efficacy in weight reduction coupled with poor effectiveness in reducing obesity related comorbidities like type 2 diabetes and hypercholesterolemia,” Vasu Chirumamilla, MD, of Westchester Medical Center, Valhalla, N.Y., and colleagues wrote in a poster presented at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
LAGB also can cause complications including, slippage, erosion, and gastric pouch dilation; subsequently many patients undergo conversion to laparoscopic sleeve gastrectomy (LSG). However, the impact of a one-step vs. two-step conversion procedure on patient weight loss remains unclear, the researchers said.
To compare weight loss after the two types of procedures, the researchers reviewed data from 78 patients (71 women) aged 15-74 years treated between 2013 and 2018 at a multi-surgeon, private practice bariatric surgery center. All patients had a history of LAGB; 31 underwent conversion to LSG in one stage, and 47 underwent conversion in two stages. Weight loss, defined as the percentage excess weight loss, was the primary endpoint.
The average excess weight loss was 44% for patients in both the one-stage and two-stage groups, and body mass index decreased by 8.9 points and 8.8 points, respectively, in the two groups, the researchers wrote.
Patients in the two-stage group experienced a significant increase in body mass index (P = .008) during the time between band removal to sleeve gastrectomy, which was an average of 207 days, they said.
The findings were limited in part by the small sample size and retrospective design, and more data are needed to compare complication rates in one-stage and two-stage procedures, the researchers noted. However, the results showed “no difference in excess weight loss in patients converted from laparoscopic adjustable gastric band to sleeve gastrectomy in one-stage versus a two-stage procedure,” they concluded.
“LAGB used to be a very popular weight loss procedure – bands were placed in a great deal of patients,” Dr. Chirumamilla said in an interview. “Now those patients are presenting with increasing frequency to bariatric surgeons with band complications or weight regain. The volume for LSG is increasing and results in percentage excess weight loss of approximately 65% versus approximately 42% for LAGB,” he said. A goal of the study was to provide patients and the surgeons with a more informed approach to performing and consenting to the particular operation, he added.
“The results have not surprised us, because as long as done by experienced surgeons on compliant patients the weight loss outcomes from the day of surgery onward should be equivalent,” Dr. Chirumamilla explained. “We were also not surprised to find that patients undergoing a two-stage conversion gained weight before their second-stage sleeve gastrectomy.”
The bottom line for clinicians is that “patients getting a conversion from band to sleeve in one-stage versus two-stages experience the same percentage excess body weight loss from time of surgery,” although two-stage patients do gain weight while awaiting their second-stage sleeve gastrectomy, Dr. Chirumamilla said.
“More research is needed to compare short- and long-term complications rates between one-stage and two-stage conversions. The ideal research situation would be a randomized, multicenter, large volume study to reduce bias,” he noted.
Dr. Chirumamilla’s collaborators included Akia Caine MD, Zachary Ballinger, Rebecca Castro, Thomas Cerabona MD, and Ashutosh Kaul MD, of the surgical group Advanced Surgeons at nygetfit.com.
Global Academy for Medical Education and this news organization are owned by the same parent company. The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Chirumamilla V et al. MISS 2020. Poster PA-14.
with either a one- or two-step procedure, a study of 78 patients showed.
“Laparoscopic adjustable gastric banding (LAGB) has largely fallen out of favor, likely related to variable efficacy in weight reduction coupled with poor effectiveness in reducing obesity related comorbidities like type 2 diabetes and hypercholesterolemia,” Vasu Chirumamilla, MD, of Westchester Medical Center, Valhalla, N.Y., and colleagues wrote in a poster presented at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
LAGB also can cause complications including, slippage, erosion, and gastric pouch dilation; subsequently many patients undergo conversion to laparoscopic sleeve gastrectomy (LSG). However, the impact of a one-step vs. two-step conversion procedure on patient weight loss remains unclear, the researchers said.
To compare weight loss after the two types of procedures, the researchers reviewed data from 78 patients (71 women) aged 15-74 years treated between 2013 and 2018 at a multi-surgeon, private practice bariatric surgery center. All patients had a history of LAGB; 31 underwent conversion to LSG in one stage, and 47 underwent conversion in two stages. Weight loss, defined as the percentage excess weight loss, was the primary endpoint.
The average excess weight loss was 44% for patients in both the one-stage and two-stage groups, and body mass index decreased by 8.9 points and 8.8 points, respectively, in the two groups, the researchers wrote.
Patients in the two-stage group experienced a significant increase in body mass index (P = .008) during the time between band removal to sleeve gastrectomy, which was an average of 207 days, they said.
The findings were limited in part by the small sample size and retrospective design, and more data are needed to compare complication rates in one-stage and two-stage procedures, the researchers noted. However, the results showed “no difference in excess weight loss in patients converted from laparoscopic adjustable gastric band to sleeve gastrectomy in one-stage versus a two-stage procedure,” they concluded.
“LAGB used to be a very popular weight loss procedure – bands were placed in a great deal of patients,” Dr. Chirumamilla said in an interview. “Now those patients are presenting with increasing frequency to bariatric surgeons with band complications or weight regain. The volume for LSG is increasing and results in percentage excess weight loss of approximately 65% versus approximately 42% for LAGB,” he said. A goal of the study was to provide patients and the surgeons with a more informed approach to performing and consenting to the particular operation, he added.
“The results have not surprised us, because as long as done by experienced surgeons on compliant patients the weight loss outcomes from the day of surgery onward should be equivalent,” Dr. Chirumamilla explained. “We were also not surprised to find that patients undergoing a two-stage conversion gained weight before their second-stage sleeve gastrectomy.”
The bottom line for clinicians is that “patients getting a conversion from band to sleeve in one-stage versus two-stages experience the same percentage excess body weight loss from time of surgery,” although two-stage patients do gain weight while awaiting their second-stage sleeve gastrectomy, Dr. Chirumamilla said.
“More research is needed to compare short- and long-term complications rates between one-stage and two-stage conversions. The ideal research situation would be a randomized, multicenter, large volume study to reduce bias,” he noted.
Dr. Chirumamilla’s collaborators included Akia Caine MD, Zachary Ballinger, Rebecca Castro, Thomas Cerabona MD, and Ashutosh Kaul MD, of the surgical group Advanced Surgeons at nygetfit.com.
Global Academy for Medical Education and this news organization are owned by the same parent company. The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Chirumamilla V et al. MISS 2020. Poster PA-14.
with either a one- or two-step procedure, a study of 78 patients showed.
“Laparoscopic adjustable gastric banding (LAGB) has largely fallen out of favor, likely related to variable efficacy in weight reduction coupled with poor effectiveness in reducing obesity related comorbidities like type 2 diabetes and hypercholesterolemia,” Vasu Chirumamilla, MD, of Westchester Medical Center, Valhalla, N.Y., and colleagues wrote in a poster presented at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
LAGB also can cause complications including, slippage, erosion, and gastric pouch dilation; subsequently many patients undergo conversion to laparoscopic sleeve gastrectomy (LSG). However, the impact of a one-step vs. two-step conversion procedure on patient weight loss remains unclear, the researchers said.
To compare weight loss after the two types of procedures, the researchers reviewed data from 78 patients (71 women) aged 15-74 years treated between 2013 and 2018 at a multi-surgeon, private practice bariatric surgery center. All patients had a history of LAGB; 31 underwent conversion to LSG in one stage, and 47 underwent conversion in two stages. Weight loss, defined as the percentage excess weight loss, was the primary endpoint.
The average excess weight loss was 44% for patients in both the one-stage and two-stage groups, and body mass index decreased by 8.9 points and 8.8 points, respectively, in the two groups, the researchers wrote.
Patients in the two-stage group experienced a significant increase in body mass index (P = .008) during the time between band removal to sleeve gastrectomy, which was an average of 207 days, they said.
The findings were limited in part by the small sample size and retrospective design, and more data are needed to compare complication rates in one-stage and two-stage procedures, the researchers noted. However, the results showed “no difference in excess weight loss in patients converted from laparoscopic adjustable gastric band to sleeve gastrectomy in one-stage versus a two-stage procedure,” they concluded.
“LAGB used to be a very popular weight loss procedure – bands were placed in a great deal of patients,” Dr. Chirumamilla said in an interview. “Now those patients are presenting with increasing frequency to bariatric surgeons with band complications or weight regain. The volume for LSG is increasing and results in percentage excess weight loss of approximately 65% versus approximately 42% for LAGB,” he said. A goal of the study was to provide patients and the surgeons with a more informed approach to performing and consenting to the particular operation, he added.
“The results have not surprised us, because as long as done by experienced surgeons on compliant patients the weight loss outcomes from the day of surgery onward should be equivalent,” Dr. Chirumamilla explained. “We were also not surprised to find that patients undergoing a two-stage conversion gained weight before their second-stage sleeve gastrectomy.”
The bottom line for clinicians is that “patients getting a conversion from band to sleeve in one-stage versus two-stages experience the same percentage excess body weight loss from time of surgery,” although two-stage patients do gain weight while awaiting their second-stage sleeve gastrectomy, Dr. Chirumamilla said.
“More research is needed to compare short- and long-term complications rates between one-stage and two-stage conversions. The ideal research situation would be a randomized, multicenter, large volume study to reduce bias,” he noted.
Dr. Chirumamilla’s collaborators included Akia Caine MD, Zachary Ballinger, Rebecca Castro, Thomas Cerabona MD, and Ashutosh Kaul MD, of the surgical group Advanced Surgeons at nygetfit.com.
Global Academy for Medical Education and this news organization are owned by the same parent company. The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Chirumamilla V et al. MISS 2020. Poster PA-14.
FROM MISS
Key clinical point: Weight loss was the same for patients after conversions from LAGB to LSG in both one-step and two-step procedures.
Major finding: The average excess weight loss was 44% for patients in both one-step and two-step conversion groups, and body mass index decreased by approximately 9 points in both groups.
Study details: The data come from a retrospective study of 78 adults who underwent conversion from LABG to LSG.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Chirumamilla V et al. MISS 2020. Poster PA-14.