User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Servier and French drug safety agency found guilty on diet drug
More than 10 years after the withdrawal of the weight-loss drug Mediator (benfluorex) from the market in France, the Paris Court issued its judgment on March 29, 2021, against Servier Laboratories and the French National Agency for the Safety of Medicines and Health Products (ANSM).
Servier Laboratories was convicted of “aggravated deception” and fined 2.7 million euros (approximately $3.2 million) but were found not guilty of fraud. ANSM will also have to pay a fine.
Mediator was brought to the market in 1976 for the treatment of hyperlipidemia and for overweight patients with type 2 diabetes but was used off label as an appetite suppressant. It was taken by 5 million people and was only removed from the market in France in 2009 because of its toxic effects.
Mediator was taken off the market in Spain 6 years earlier, and in Switzerland 12 years earlier, and more than 30 years before in Belgium. It was never marketed in the United States.
The number of deaths because of heart valve damage related to the drug in France has been estimated at 220-300 in the short term (2.5 years) and 1,300-1,800 in the long term. In addition, the drug has been responsible for 3,100-4,200 hospital admissions for valvular insufficiency and pulmonary arterial hypertension.
“Despite knowing the risks for very many years ... [Servier Laboratories] never took the necessary measures and thus deceived” consumers of Mediator, declared the president of the criminal court, Sylvie Daunois.
Servier has “weakened confidence in the health system,” she added.
“I am very happy that ‘aggravated deception,’ the heart of the case, has been recognized and condemned,” Irène Frachon, MD, a pulmonologist at Brest (France) University Hospital and whistleblower on the Mediator scandal, said in an interview.
However, Dr. Frachon continued: “The major problem, putting a toxic agent on the market for years, is a given. But the weakness of the sentences gives a mixed message.
“The judgment is too cautious in its punishments,” she added, pointing out that, “in the case of contaminated blood, there were prison sentences.”
Servier deceived doctors and patients
The French trial in September 2019 was extraordinary, with about 100 witnesses, nearly 400 lawyers, and 5,000 victims.
On June 23, 2020, the prosecutor, Aude Le Guilcher, requested at the end of her indictment that the six companies of the Servier group be fined, notably for “deception, homicide, involuntary injuries, and fraud,” to the tune of 20.3 million euros (approximately $23.8 million).
Against the former No. 2 of Servier, Jean-Philippe Seta, Ms. Le Guilcher requested 5 years in prison, with 2 years suspended, and a 200,000 euro (approximately $235,000) fine.
The same sum was requested against ANSM for homicide and unintentional injuries.
In the end, Mr. Seta, the former right hand of Jacques Servier, who died in 2004, was sentenced to 4 years in prison, suspended. For their part, ANSM was fined 303,000 euros(approximately $350,000).
It is now clearly established that Servier Laboratories knowingly concealed the similarity of Mediator to the fenfluramine family of compounds, which was banned in 1990 because of adverse effects.
The group also deceived doctors who prescribed the drug and patients who took it by hiding its toxicity.
Mediator should never have been authorized for use
In terms of the fraud charges, the prosecutor estimated that the losses incurred by the primary health insurance industry were in the region of several hundred million euros.
She argued that Mediator should never have been reimbursed, as “it should never have benefited from market authorization, which it received solely due to the fraudulent actions of the company.”
But because of the statute of limitations, this argument was not heard, explained Dr. Frachon, “and the same is true of conflicts of interest, where limitations led to them being discharged.
“We understand the legal difficulties, but it’s a shame in terms of the signal sent.”
“I hope the medical world will learn the lesson and not continue with ‘business as usual’ with people who are delinquents. I think it will be essential to restore public confidence,” concluded Dr. Frachon.
No conflicts of interest or funding were declared.
A version of this article first appeared on Medscape.com.
More than 10 years after the withdrawal of the weight-loss drug Mediator (benfluorex) from the market in France, the Paris Court issued its judgment on March 29, 2021, against Servier Laboratories and the French National Agency for the Safety of Medicines and Health Products (ANSM).
Servier Laboratories was convicted of “aggravated deception” and fined 2.7 million euros (approximately $3.2 million) but were found not guilty of fraud. ANSM will also have to pay a fine.
Mediator was brought to the market in 1976 for the treatment of hyperlipidemia and for overweight patients with type 2 diabetes but was used off label as an appetite suppressant. It was taken by 5 million people and was only removed from the market in France in 2009 because of its toxic effects.
Mediator was taken off the market in Spain 6 years earlier, and in Switzerland 12 years earlier, and more than 30 years before in Belgium. It was never marketed in the United States.
The number of deaths because of heart valve damage related to the drug in France has been estimated at 220-300 in the short term (2.5 years) and 1,300-1,800 in the long term. In addition, the drug has been responsible for 3,100-4,200 hospital admissions for valvular insufficiency and pulmonary arterial hypertension.
“Despite knowing the risks for very many years ... [Servier Laboratories] never took the necessary measures and thus deceived” consumers of Mediator, declared the president of the criminal court, Sylvie Daunois.
Servier has “weakened confidence in the health system,” she added.
“I am very happy that ‘aggravated deception,’ the heart of the case, has been recognized and condemned,” Irène Frachon, MD, a pulmonologist at Brest (France) University Hospital and whistleblower on the Mediator scandal, said in an interview.
However, Dr. Frachon continued: “The major problem, putting a toxic agent on the market for years, is a given. But the weakness of the sentences gives a mixed message.
“The judgment is too cautious in its punishments,” she added, pointing out that, “in the case of contaminated blood, there were prison sentences.”
Servier deceived doctors and patients
The French trial in September 2019 was extraordinary, with about 100 witnesses, nearly 400 lawyers, and 5,000 victims.
On June 23, 2020, the prosecutor, Aude Le Guilcher, requested at the end of her indictment that the six companies of the Servier group be fined, notably for “deception, homicide, involuntary injuries, and fraud,” to the tune of 20.3 million euros (approximately $23.8 million).
Against the former No. 2 of Servier, Jean-Philippe Seta, Ms. Le Guilcher requested 5 years in prison, with 2 years suspended, and a 200,000 euro (approximately $235,000) fine.
The same sum was requested against ANSM for homicide and unintentional injuries.
In the end, Mr. Seta, the former right hand of Jacques Servier, who died in 2004, was sentenced to 4 years in prison, suspended. For their part, ANSM was fined 303,000 euros(approximately $350,000).
It is now clearly established that Servier Laboratories knowingly concealed the similarity of Mediator to the fenfluramine family of compounds, which was banned in 1990 because of adverse effects.
The group also deceived doctors who prescribed the drug and patients who took it by hiding its toxicity.
Mediator should never have been authorized for use
In terms of the fraud charges, the prosecutor estimated that the losses incurred by the primary health insurance industry were in the region of several hundred million euros.
She argued that Mediator should never have been reimbursed, as “it should never have benefited from market authorization, which it received solely due to the fraudulent actions of the company.”
But because of the statute of limitations, this argument was not heard, explained Dr. Frachon, “and the same is true of conflicts of interest, where limitations led to them being discharged.
“We understand the legal difficulties, but it’s a shame in terms of the signal sent.”
“I hope the medical world will learn the lesson and not continue with ‘business as usual’ with people who are delinquents. I think it will be essential to restore public confidence,” concluded Dr. Frachon.
No conflicts of interest or funding were declared.
A version of this article first appeared on Medscape.com.
More than 10 years after the withdrawal of the weight-loss drug Mediator (benfluorex) from the market in France, the Paris Court issued its judgment on March 29, 2021, against Servier Laboratories and the French National Agency for the Safety of Medicines and Health Products (ANSM).
Servier Laboratories was convicted of “aggravated deception” and fined 2.7 million euros (approximately $3.2 million) but were found not guilty of fraud. ANSM will also have to pay a fine.
Mediator was brought to the market in 1976 for the treatment of hyperlipidemia and for overweight patients with type 2 diabetes but was used off label as an appetite suppressant. It was taken by 5 million people and was only removed from the market in France in 2009 because of its toxic effects.
Mediator was taken off the market in Spain 6 years earlier, and in Switzerland 12 years earlier, and more than 30 years before in Belgium. It was never marketed in the United States.
The number of deaths because of heart valve damage related to the drug in France has been estimated at 220-300 in the short term (2.5 years) and 1,300-1,800 in the long term. In addition, the drug has been responsible for 3,100-4,200 hospital admissions for valvular insufficiency and pulmonary arterial hypertension.
“Despite knowing the risks for very many years ... [Servier Laboratories] never took the necessary measures and thus deceived” consumers of Mediator, declared the president of the criminal court, Sylvie Daunois.
Servier has “weakened confidence in the health system,” she added.
“I am very happy that ‘aggravated deception,’ the heart of the case, has been recognized and condemned,” Irène Frachon, MD, a pulmonologist at Brest (France) University Hospital and whistleblower on the Mediator scandal, said in an interview.
However, Dr. Frachon continued: “The major problem, putting a toxic agent on the market for years, is a given. But the weakness of the sentences gives a mixed message.
“The judgment is too cautious in its punishments,” she added, pointing out that, “in the case of contaminated blood, there were prison sentences.”
Servier deceived doctors and patients
The French trial in September 2019 was extraordinary, with about 100 witnesses, nearly 400 lawyers, and 5,000 victims.
On June 23, 2020, the prosecutor, Aude Le Guilcher, requested at the end of her indictment that the six companies of the Servier group be fined, notably for “deception, homicide, involuntary injuries, and fraud,” to the tune of 20.3 million euros (approximately $23.8 million).
Against the former No. 2 of Servier, Jean-Philippe Seta, Ms. Le Guilcher requested 5 years in prison, with 2 years suspended, and a 200,000 euro (approximately $235,000) fine.
The same sum was requested against ANSM for homicide and unintentional injuries.
In the end, Mr. Seta, the former right hand of Jacques Servier, who died in 2004, was sentenced to 4 years in prison, suspended. For their part, ANSM was fined 303,000 euros(approximately $350,000).
It is now clearly established that Servier Laboratories knowingly concealed the similarity of Mediator to the fenfluramine family of compounds, which was banned in 1990 because of adverse effects.
The group also deceived doctors who prescribed the drug and patients who took it by hiding its toxicity.
Mediator should never have been authorized for use
In terms of the fraud charges, the prosecutor estimated that the losses incurred by the primary health insurance industry were in the region of several hundred million euros.
She argued that Mediator should never have been reimbursed, as “it should never have benefited from market authorization, which it received solely due to the fraudulent actions of the company.”
But because of the statute of limitations, this argument was not heard, explained Dr. Frachon, “and the same is true of conflicts of interest, where limitations led to them being discharged.
“We understand the legal difficulties, but it’s a shame in terms of the signal sent.”
“I hope the medical world will learn the lesson and not continue with ‘business as usual’ with people who are delinquents. I think it will be essential to restore public confidence,” concluded Dr. Frachon.
No conflicts of interest or funding were declared.
A version of this article first appeared on Medscape.com.
FDA okays new indication for alirocumab in homozygous FH
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
Starting April 5, patients can read your notes: 5 things to consider
Change in writing style is not mandated
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Change in writing style is not mandated
Change in writing style is not mandated
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 in 2020: Deaths and disparities
COVID-19 was the third-leading cause of death in the United States in 2020, but that mortality burden did not fall evenly along racial/ethnic lines, according to a provisional report from the Centers for Disease Control and Prevention.
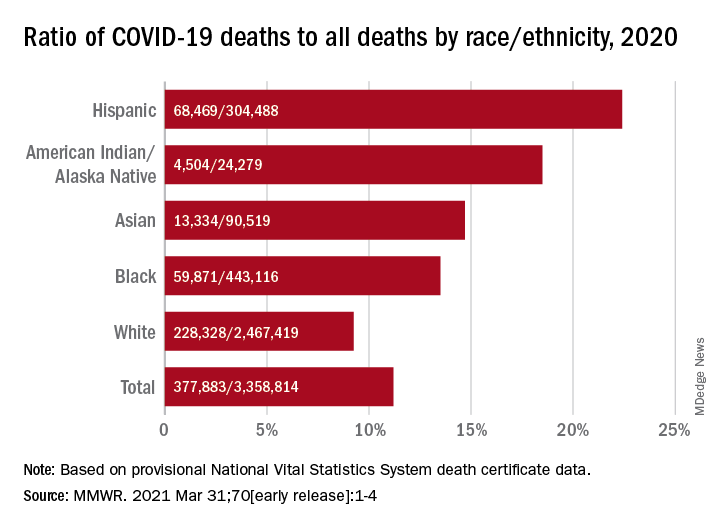
Only heart disease and cancer caused more deaths than SARS-CoV-2, which took the lives of almost 378,000 Americans last year, Farida B. Ahmad, MPH, and associates at the National Center for Health Statistics noted March 31 in the Morbidity and Mortality Weekly Report.
That represents 11.2% of the almost 3.36 million total deaths recorded in 2020. The racial/ethnics demographics, however, show that 22.4% of all deaths among Hispanic Americans were COVID-19–related, as were 18.6% of deaths in American Indians/Alaska Natives. Deaths among Asian persons, at 14.7%, and African Americans, at 13.5%, were closer but still above the national figure, while Whites (9.3%) were the only major subgroup below it, based on data from the National Vital Statistics System.
Age-adjusted death rates tell a somewhat different story: American Indian/Alaska native persons were highest with a rate of 187.8 COVID-19–associated deaths per 100,000 standard population, with Hispanic persons second at 164.3 per 100,000. Blacks were next at 151.1 deaths per 100,000, but Whites had a higher rate (72.5) than did Asian Americans (66.7), the CDC investigators reported.
“During January-December 2020, the estimated 2020 age-adjusted death rate increased for the first time since 2017, with an increase of 15.9% compared with 2019, from 715.2 to 828.7 deaths per 100,000 population,” they wrote, noting that “certain categories of race (i.e., AI/AN and Asian) and Hispanic ethnicity reported on death certificates might have been misclassified, possibly resulting in underestimates of death rates for some groups.”
COVID-19 was the third-leading cause of death in the United States in 2020, but that mortality burden did not fall evenly along racial/ethnic lines, according to a provisional report from the Centers for Disease Control and Prevention.
Only heart disease and cancer caused more deaths than SARS-CoV-2, which took the lives of almost 378,000 Americans last year, Farida B. Ahmad, MPH, and associates at the National Center for Health Statistics noted March 31 in the Morbidity and Mortality Weekly Report.
That represents 11.2% of the almost 3.36 million total deaths recorded in 2020. The racial/ethnics demographics, however, show that 22.4% of all deaths among Hispanic Americans were COVID-19–related, as were 18.6% of deaths in American Indians/Alaska Natives. Deaths among Asian persons, at 14.7%, and African Americans, at 13.5%, were closer but still above the national figure, while Whites (9.3%) were the only major subgroup below it, based on data from the National Vital Statistics System.
Age-adjusted death rates tell a somewhat different story: American Indian/Alaska native persons were highest with a rate of 187.8 COVID-19–associated deaths per 100,000 standard population, with Hispanic persons second at 164.3 per 100,000. Blacks were next at 151.1 deaths per 100,000, but Whites had a higher rate (72.5) than did Asian Americans (66.7), the CDC investigators reported.
“During January-December 2020, the estimated 2020 age-adjusted death rate increased for the first time since 2017, with an increase of 15.9% compared with 2019, from 715.2 to 828.7 deaths per 100,000 population,” they wrote, noting that “certain categories of race (i.e., AI/AN and Asian) and Hispanic ethnicity reported on death certificates might have been misclassified, possibly resulting in underestimates of death rates for some groups.”
COVID-19 was the third-leading cause of death in the United States in 2020, but that mortality burden did not fall evenly along racial/ethnic lines, according to a provisional report from the Centers for Disease Control and Prevention.
Only heart disease and cancer caused more deaths than SARS-CoV-2, which took the lives of almost 378,000 Americans last year, Farida B. Ahmad, MPH, and associates at the National Center for Health Statistics noted March 31 in the Morbidity and Mortality Weekly Report.
That represents 11.2% of the almost 3.36 million total deaths recorded in 2020. The racial/ethnics demographics, however, show that 22.4% of all deaths among Hispanic Americans were COVID-19–related, as were 18.6% of deaths in American Indians/Alaska Natives. Deaths among Asian persons, at 14.7%, and African Americans, at 13.5%, were closer but still above the national figure, while Whites (9.3%) were the only major subgroup below it, based on data from the National Vital Statistics System.
Age-adjusted death rates tell a somewhat different story: American Indian/Alaska native persons were highest with a rate of 187.8 COVID-19–associated deaths per 100,000 standard population, with Hispanic persons second at 164.3 per 100,000. Blacks were next at 151.1 deaths per 100,000, but Whites had a higher rate (72.5) than did Asian Americans (66.7), the CDC investigators reported.
“During January-December 2020, the estimated 2020 age-adjusted death rate increased for the first time since 2017, with an increase of 15.9% compared with 2019, from 715.2 to 828.7 deaths per 100,000 population,” they wrote, noting that “certain categories of race (i.e., AI/AN and Asian) and Hispanic ethnicity reported on death certificates might have been misclassified, possibly resulting in underestimates of death rates for some groups.”
FROM MMWR
CDC adds new medical conditions to COVID-19 high-risk list
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
Vaccine mismatch: What to do after dose 1 when plans change
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.

After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.
After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.
After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
COVID vaccines could lose their punch within a year, experts say

In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
National Psoriasis Foundation recommends some stop methotrexate for 2 weeks after J&J vaccine
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.

The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.
The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.
The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
FROM INNOVATIONS IN DERMATOLOGY
Use of complimentary and alternative medicine common in diabetes patients
An updated worldwide estimate of complementary and alternative medicine (CAM) use among individuals with diabetes found widespread use, though it varied greatly by region and is sometimes hard to define.

The report is the first literature review of the subject since 2007. The researchers looked at CAM use by region, as well as by patient categories such as those with advanced diabetes and by length of time since diagnosis. The most commonly reported CAMs in use were herbal medicine, acupuncture, homeopathy, and spiritual healing.
Only about one-third of patients disclosed their CAM use to their physician or health care provider. “We suggest that health care professionals should carefully anticipate the likelihood of their [patients’] diabetic CAM use in order to enhance treatment optimization and promote medication adherence, as well as to provide a fully informed consultation,” said first author Abdulaziz S. Alzahrani, a PhD student at the University of Birmingham (England). The study was published March 8, 2021, in the European Journal of Clinical Pharmacology.
Patients also have a responsibility, said Gregory Rhee, PhD, assistant professor of public health sciences at the University of Connecticut, Farmington. He was the lead author of a 2018 survey of CAM use in adults aged 65 years and older with diabetes in the United States using data from the 2012 National Health Interview Survey, and found that 25% had used CAM in some form in the prior year. “They need to be more up front, more proactive talking about CAM use with their doctors, and the second part is the physician. They also should be better educated in terms of CAM use. Traditionally, the physician in Western societies have pretty much ignored CAM use. But they are getting aware of CAM use and also we know that people are coming from multiple cultural backgrounds. The physicians and other health care providers should be better informed about CAM, and they should be better educated about it to provide patients better practice,” said Dr. Rhee.
He also distinguished between approaches like yoga or Tai Chi, which are physically oriented and not particularly controversial, and herbal medicines or dietary supplements. “Those can be controversial because we do not have strong scientific evidence to support those modalities for effectiveness on diabetes management,” Dr. Rhee added.
Mr. Alzahrani and colleagues conducted a meta-analysis of 38 studies, which included data from 25 countries. The included studies varied in their approach. For example, 16 studies focused exclusively on herbal and nutritional supplements. The most commonly mentioned CAMs were acupuncture and mind-body therapies (each named in six studies), religious and spiritual healing (five studies), and homeopathy (four studies). Among 31 studies focusing on herbal and nutritional supplements, the most common herbs mentioned were cinnamon and fenugreek (mentioned in 18 studies), garlic (17 studies), aloe vera (14 studies), and black seed (12 studies).
Prevalence of CAM use varied widely, ranging from 17% in Jordan to 89% in India and in a separate study in Jordan. The pooled prevalence of CAM use was 51% (95% confidence interval, 43%-59%). Subgroup analyses found the highest rate of CAM use in Europe (76%) and Africa (55%), and the lowest in North America (45%).
When the researchers examined patient characteristics, they found no significant relationship between CAM use and established ethnicity groups, or between type 1 and type 2 diabetes. The prevalence ratio was lower among men (PR, 0.86; 95% CI, 0.81-0.91). PRs for CAM use were lower among those with diabetic complications (PR, 0.81; 95% CI, 0.66-0.99). Individuals with diabetes of at least 5 years’ duration were more likely to use CAM than those with shorter duration of illness (PR, 1.71; 95% CI, 1.04-1.32).
Most (78%) CAM users employed it as an addition to their treatment regimen (95% CI, 56-94%), while 21% used it as an alternative to prescribed medicine (95% CI, 12-31%). More than two-thirds (67%) of individuals did not disclose CAM use to health care professionals (95% CI, 58-76%).
Although CAM use can be a source of friction between patients and physicians, Dr. Rhee also sees it as an opportunity. Patients from diverse backgrounds may be using CAM, often as a result of different cultural backgrounds. He cited the belief in some Asian countries that the balance of Yin and Yang is key to health, which many patients believe can be addressed through CAM. “If we want to promote cultural diversity, if we really care about patient diversity, I think CAM is one of the potential sources where the doctors should know [more about] the issue,” said Dr. Rhee.
The study was funded by the University of Birmingham. Dr. Rhee and Mr. Alzahrani have no relevant financial disclosures.
An updated worldwide estimate of complementary and alternative medicine (CAM) use among individuals with diabetes found widespread use, though it varied greatly by region and is sometimes hard to define.
The report is the first literature review of the subject since 2007. The researchers looked at CAM use by region, as well as by patient categories such as those with advanced diabetes and by length of time since diagnosis. The most commonly reported CAMs in use were herbal medicine, acupuncture, homeopathy, and spiritual healing.
Only about one-third of patients disclosed their CAM use to their physician or health care provider. “We suggest that health care professionals should carefully anticipate the likelihood of their [patients’] diabetic CAM use in order to enhance treatment optimization and promote medication adherence, as well as to provide a fully informed consultation,” said first author Abdulaziz S. Alzahrani, a PhD student at the University of Birmingham (England). The study was published March 8, 2021, in the European Journal of Clinical Pharmacology.
Patients also have a responsibility, said Gregory Rhee, PhD, assistant professor of public health sciences at the University of Connecticut, Farmington. He was the lead author of a 2018 survey of CAM use in adults aged 65 years and older with diabetes in the United States using data from the 2012 National Health Interview Survey, and found that 25% had used CAM in some form in the prior year. “They need to be more up front, more proactive talking about CAM use with their doctors, and the second part is the physician. They also should be better educated in terms of CAM use. Traditionally, the physician in Western societies have pretty much ignored CAM use. But they are getting aware of CAM use and also we know that people are coming from multiple cultural backgrounds. The physicians and other health care providers should be better informed about CAM, and they should be better educated about it to provide patients better practice,” said Dr. Rhee.
He also distinguished between approaches like yoga or Tai Chi, which are physically oriented and not particularly controversial, and herbal medicines or dietary supplements. “Those can be controversial because we do not have strong scientific evidence to support those modalities for effectiveness on diabetes management,” Dr. Rhee added.
Mr. Alzahrani and colleagues conducted a meta-analysis of 38 studies, which included data from 25 countries. The included studies varied in their approach. For example, 16 studies focused exclusively on herbal and nutritional supplements. The most commonly mentioned CAMs were acupuncture and mind-body therapies (each named in six studies), religious and spiritual healing (five studies), and homeopathy (four studies). Among 31 studies focusing on herbal and nutritional supplements, the most common herbs mentioned were cinnamon and fenugreek (mentioned in 18 studies), garlic (17 studies), aloe vera (14 studies), and black seed (12 studies).
Prevalence of CAM use varied widely, ranging from 17% in Jordan to 89% in India and in a separate study in Jordan. The pooled prevalence of CAM use was 51% (95% confidence interval, 43%-59%). Subgroup analyses found the highest rate of CAM use in Europe (76%) and Africa (55%), and the lowest in North America (45%).
When the researchers examined patient characteristics, they found no significant relationship between CAM use and established ethnicity groups, or between type 1 and type 2 diabetes. The prevalence ratio was lower among men (PR, 0.86; 95% CI, 0.81-0.91). PRs for CAM use were lower among those with diabetic complications (PR, 0.81; 95% CI, 0.66-0.99). Individuals with diabetes of at least 5 years’ duration were more likely to use CAM than those with shorter duration of illness (PR, 1.71; 95% CI, 1.04-1.32).
Most (78%) CAM users employed it as an addition to their treatment regimen (95% CI, 56-94%), while 21% used it as an alternative to prescribed medicine (95% CI, 12-31%). More than two-thirds (67%) of individuals did not disclose CAM use to health care professionals (95% CI, 58-76%).
Although CAM use can be a source of friction between patients and physicians, Dr. Rhee also sees it as an opportunity. Patients from diverse backgrounds may be using CAM, often as a result of different cultural backgrounds. He cited the belief in some Asian countries that the balance of Yin and Yang is key to health, which many patients believe can be addressed through CAM. “If we want to promote cultural diversity, if we really care about patient diversity, I think CAM is one of the potential sources where the doctors should know [more about] the issue,” said Dr. Rhee.
The study was funded by the University of Birmingham. Dr. Rhee and Mr. Alzahrani have no relevant financial disclosures.
An updated worldwide estimate of complementary and alternative medicine (CAM) use among individuals with diabetes found widespread use, though it varied greatly by region and is sometimes hard to define.
The report is the first literature review of the subject since 2007. The researchers looked at CAM use by region, as well as by patient categories such as those with advanced diabetes and by length of time since diagnosis. The most commonly reported CAMs in use were herbal medicine, acupuncture, homeopathy, and spiritual healing.
Only about one-third of patients disclosed their CAM use to their physician or health care provider. “We suggest that health care professionals should carefully anticipate the likelihood of their [patients’] diabetic CAM use in order to enhance treatment optimization and promote medication adherence, as well as to provide a fully informed consultation,” said first author Abdulaziz S. Alzahrani, a PhD student at the University of Birmingham (England). The study was published March 8, 2021, in the European Journal of Clinical Pharmacology.
Patients also have a responsibility, said Gregory Rhee, PhD, assistant professor of public health sciences at the University of Connecticut, Farmington. He was the lead author of a 2018 survey of CAM use in adults aged 65 years and older with diabetes in the United States using data from the 2012 National Health Interview Survey, and found that 25% had used CAM in some form in the prior year. “They need to be more up front, more proactive talking about CAM use with their doctors, and the second part is the physician. They also should be better educated in terms of CAM use. Traditionally, the physician in Western societies have pretty much ignored CAM use. But they are getting aware of CAM use and also we know that people are coming from multiple cultural backgrounds. The physicians and other health care providers should be better informed about CAM, and they should be better educated about it to provide patients better practice,” said Dr. Rhee.
He also distinguished between approaches like yoga or Tai Chi, which are physically oriented and not particularly controversial, and herbal medicines or dietary supplements. “Those can be controversial because we do not have strong scientific evidence to support those modalities for effectiveness on diabetes management,” Dr. Rhee added.
Mr. Alzahrani and colleagues conducted a meta-analysis of 38 studies, which included data from 25 countries. The included studies varied in their approach. For example, 16 studies focused exclusively on herbal and nutritional supplements. The most commonly mentioned CAMs were acupuncture and mind-body therapies (each named in six studies), religious and spiritual healing (five studies), and homeopathy (four studies). Among 31 studies focusing on herbal and nutritional supplements, the most common herbs mentioned were cinnamon and fenugreek (mentioned in 18 studies), garlic (17 studies), aloe vera (14 studies), and black seed (12 studies).
Prevalence of CAM use varied widely, ranging from 17% in Jordan to 89% in India and in a separate study in Jordan. The pooled prevalence of CAM use was 51% (95% confidence interval, 43%-59%). Subgroup analyses found the highest rate of CAM use in Europe (76%) and Africa (55%), and the lowest in North America (45%).
When the researchers examined patient characteristics, they found no significant relationship between CAM use and established ethnicity groups, or between type 1 and type 2 diabetes. The prevalence ratio was lower among men (PR, 0.86; 95% CI, 0.81-0.91). PRs for CAM use were lower among those with diabetic complications (PR, 0.81; 95% CI, 0.66-0.99). Individuals with diabetes of at least 5 years’ duration were more likely to use CAM than those with shorter duration of illness (PR, 1.71; 95% CI, 1.04-1.32).
Most (78%) CAM users employed it as an addition to their treatment regimen (95% CI, 56-94%), while 21% used it as an alternative to prescribed medicine (95% CI, 12-31%). More than two-thirds (67%) of individuals did not disclose CAM use to health care professionals (95% CI, 58-76%).
Although CAM use can be a source of friction between patients and physicians, Dr. Rhee also sees it as an opportunity. Patients from diverse backgrounds may be using CAM, often as a result of different cultural backgrounds. He cited the belief in some Asian countries that the balance of Yin and Yang is key to health, which many patients believe can be addressed through CAM. “If we want to promote cultural diversity, if we really care about patient diversity, I think CAM is one of the potential sources where the doctors should know [more about] the issue,” said Dr. Rhee.
The study was funded by the University of Birmingham. Dr. Rhee and Mr. Alzahrani have no relevant financial disclosures.
FROM THE EUROPEAN JOURNAL OF CLINICAL PHARMACOLOGY
Many unknowns on fertility preservation in transgender patients
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.