User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Post–COVID-19 lung injury: What we know so far
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
‘Praise Diabetes’: Support programs in Black churches yield lasting A1c changes
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.

Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.
Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.
Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
FROM ADA 2020
A pacemaker that 'just disappears' and a magnetic diet device
Ignore this pacemaker and it will go away
At some point – and now seems to be that point – we have to say enough is enough. The throwaway culture that produces phones, TVs, and computers that get tossed in the trash because they can’t be repaired has gone too far. That’s right, we’re looking at you, medical science!
This time, it’s a pacemaker that just disappears when it’s no longer needed. Some lazy heart surgeon decided that it was way too much trouble to do another surgery to remove the leads when a temporary pacemaker was no longer needed. You know the type: “It sure would be nice if the pacemaker components were biocompatible and were naturally absorbed by the body over the course of a few weeks and wouldn’t need to be surgically extracted.” Slacker.
Well, get a load of this. Researchers at Northwestern and George Washington universities say that they have come up with a transient pacemaker that “harvests energy from an external, remote antenna using near-field communication protocols – the same technology used in smartphones for electronic payments and in RFID tags.”
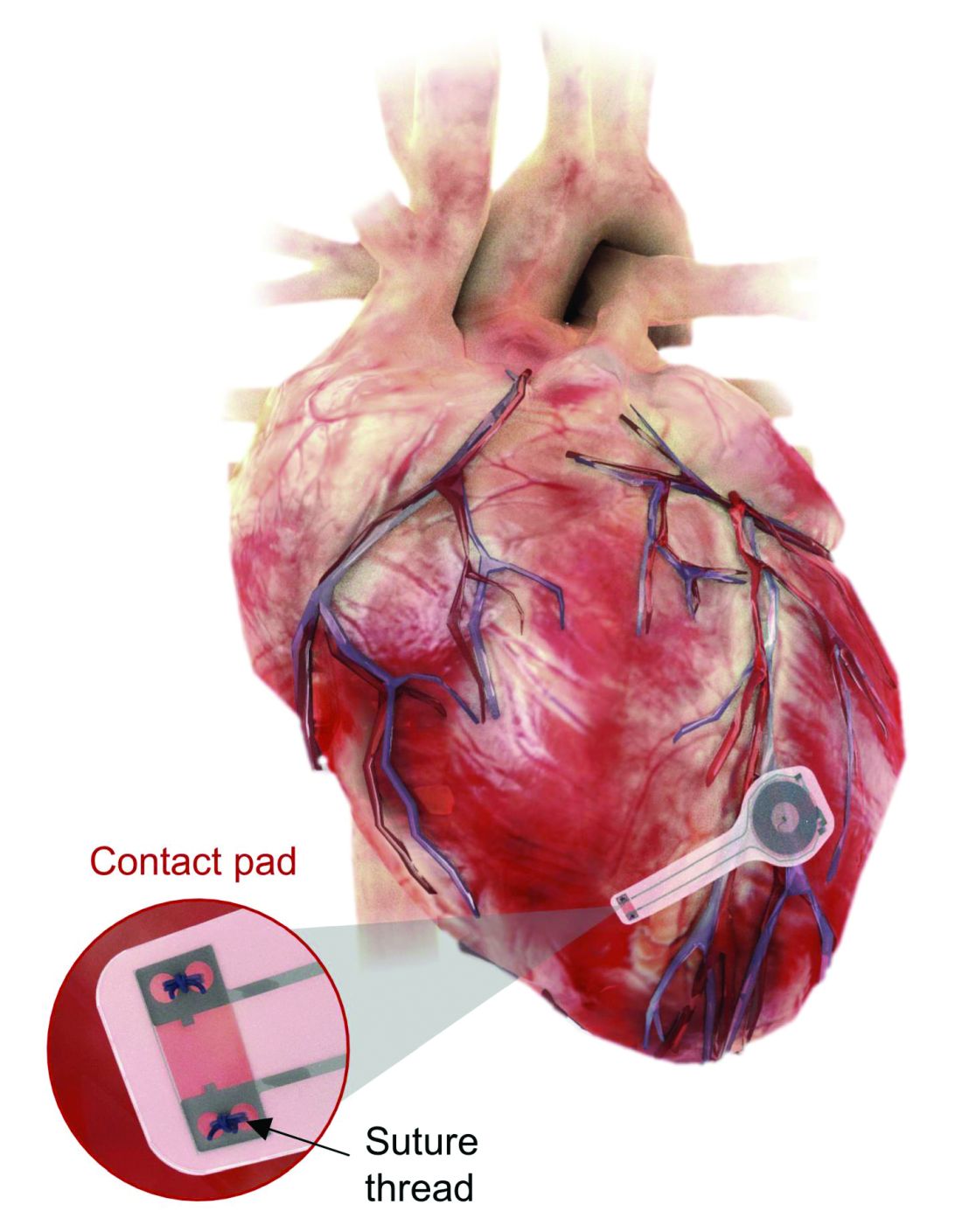
That means no batteries and no wires that have to be removed and can cause infections. Because the infectious disease docs also are too lazy to do their jobs, apparently.
The lack of onboard infrastructure means that the device can be very small – it weighs less than half a gram and is only 250 microns thick. And yes, it is bioresorbable and completely harmless. It fully degrades and disappears in 5-7 weeks through the body’s natural biologic processes, “thereby avoiding the need for physical removal of the pacemaker electrodes. This is potentially a major victory for postoperative patients,” said Dr. Rishi Arora, one of the investigators.
A victory for patients, he says. Not a word about the time and effort saved by the surgeons. Typical.
It’s a mask! No, it’s a COVID-19 test!
Mask wearing has gotten more lax as people get vaccinated for COVID-19, but as wearing masks for virus prevention is becoming more normalized in western society, some saw an opportunity to make them work for diagnosis.
Researchers from the Massachusetts Institute of Technology and the Wyss Institute for Biologically Inspired Engineering at Harvard University have found a way to do just that with their wearable freeze-dried cell-free (wFDCF) technology. A single push of a button releases water from a reservoir in the mask that sequentially activates three different freeze-dried biological reactions, which detect the SARS-CoV-2 virus in the wearer’s breath.
Initially meant as a tool for the Zika outbreak in 2015, the team made a quick pivot in May 2020. But this isn’t just some run-of-the-mill, at-home test. The data prove that the wFDCF mask is comparable to polymerase chain reactions tests, the standard in COVID-19 detection. Plus there aren’t any extra factors to deal with, like room or instrument temperature to ensure accuracy. In just 90 minutes, the mask gives results on a readout in a way similar to that of a pregnancy test. Voilà! To have COVID-19 or not to have COVID-19 is an easily answered question.

At LOTME, we think this is a big improvement from having dogs, or even three-foot rats, sniffing out coronavirus.
But wait, there’s more. “In addition to face masks, our programmable biosensors can be integrated into other garments to provide on-the-go detection of dangerous substances including viruses, bacteria, toxins, and chemical agents,” said Peter Nguyen, PhD, study coauthor and research scientist at the Wyss Institute. The technology can be used on lab coats, scrubs, military uniforms, and uniforms of first responders who may come in contact with hazardous pathogens and toxins. Think of all the lives saved and possible avoidances.
If only it could diagnose bad breath.
Finally, an excuse for the all-beer diet
Weight loss is hard work. Extremely hard work, and, as evidenced by the constant inundation and advertisement of quick fixes, crash diets, and expensive gym memberships, there’s not really a solid, 100% solution to the issue. Until now, thanks to a team of doctors from New Zealand, who’ve decided that the best way to combat obesity is to leave you in constant agony.
The DentalSlim Diet Control device is certainly a radical yet comically logical attempt to combat obesity. The creators say that the biggest problem with dieting is compliance, and, well, it’s difficult to eat too much if you can’t actually open your mouth. The metal contraption is mounted onto your teeth and uses magnetic locks to prevent the user from opening their mouths more than 2 mm. That’s less than a tenth of an inch. Which is not a lot. So not a lot that essentially all you can consume is liquid.

Oh, and they’ve got results to back up their madness. In a small study, seven otherwise healthy obese women lost an average of 5.1% of their body weight after using the DentalSlim for 2 weeks, though they did complain that the device was difficult to use, caused discomfort and difficulty speaking, made them more tense, and in general made life “less satisfying.” And one participant was able to cheat the system and consume nonhealthy food like chocolate by melting it.
So, there you are, if you want a weight-loss solution that tortures you and has far bigger holes than the one it leaves for your mouth, try the DentalSlim. Or, you know, don’t eat that eighth slice of pizza and maybe go for a walk later. Your choice.
Ignore this pacemaker and it will go away
At some point – and now seems to be that point – we have to say enough is enough. The throwaway culture that produces phones, TVs, and computers that get tossed in the trash because they can’t be repaired has gone too far. That’s right, we’re looking at you, medical science!
This time, it’s a pacemaker that just disappears when it’s no longer needed. Some lazy heart surgeon decided that it was way too much trouble to do another surgery to remove the leads when a temporary pacemaker was no longer needed. You know the type: “It sure would be nice if the pacemaker components were biocompatible and were naturally absorbed by the body over the course of a few weeks and wouldn’t need to be surgically extracted.” Slacker.
Well, get a load of this. Researchers at Northwestern and George Washington universities say that they have come up with a transient pacemaker that “harvests energy from an external, remote antenna using near-field communication protocols – the same technology used in smartphones for electronic payments and in RFID tags.”
That means no batteries and no wires that have to be removed and can cause infections. Because the infectious disease docs also are too lazy to do their jobs, apparently.
The lack of onboard infrastructure means that the device can be very small – it weighs less than half a gram and is only 250 microns thick. And yes, it is bioresorbable and completely harmless. It fully degrades and disappears in 5-7 weeks through the body’s natural biologic processes, “thereby avoiding the need for physical removal of the pacemaker electrodes. This is potentially a major victory for postoperative patients,” said Dr. Rishi Arora, one of the investigators.
A victory for patients, he says. Not a word about the time and effort saved by the surgeons. Typical.
It’s a mask! No, it’s a COVID-19 test!
Mask wearing has gotten more lax as people get vaccinated for COVID-19, but as wearing masks for virus prevention is becoming more normalized in western society, some saw an opportunity to make them work for diagnosis.
Researchers from the Massachusetts Institute of Technology and the Wyss Institute for Biologically Inspired Engineering at Harvard University have found a way to do just that with their wearable freeze-dried cell-free (wFDCF) technology. A single push of a button releases water from a reservoir in the mask that sequentially activates three different freeze-dried biological reactions, which detect the SARS-CoV-2 virus in the wearer’s breath.
Initially meant as a tool for the Zika outbreak in 2015, the team made a quick pivot in May 2020. But this isn’t just some run-of-the-mill, at-home test. The data prove that the wFDCF mask is comparable to polymerase chain reactions tests, the standard in COVID-19 detection. Plus there aren’t any extra factors to deal with, like room or instrument temperature to ensure accuracy. In just 90 minutes, the mask gives results on a readout in a way similar to that of a pregnancy test. Voilà! To have COVID-19 or not to have COVID-19 is an easily answered question.
At LOTME, we think this is a big improvement from having dogs, or even three-foot rats, sniffing out coronavirus.
But wait, there’s more. “In addition to face masks, our programmable biosensors can be integrated into other garments to provide on-the-go detection of dangerous substances including viruses, bacteria, toxins, and chemical agents,” said Peter Nguyen, PhD, study coauthor and research scientist at the Wyss Institute. The technology can be used on lab coats, scrubs, military uniforms, and uniforms of first responders who may come in contact with hazardous pathogens and toxins. Think of all the lives saved and possible avoidances.
If only it could diagnose bad breath.
Finally, an excuse for the all-beer diet
Weight loss is hard work. Extremely hard work, and, as evidenced by the constant inundation and advertisement of quick fixes, crash diets, and expensive gym memberships, there’s not really a solid, 100% solution to the issue. Until now, thanks to a team of doctors from New Zealand, who’ve decided that the best way to combat obesity is to leave you in constant agony.
The DentalSlim Diet Control device is certainly a radical yet comically logical attempt to combat obesity. The creators say that the biggest problem with dieting is compliance, and, well, it’s difficult to eat too much if you can’t actually open your mouth. The metal contraption is mounted onto your teeth and uses magnetic locks to prevent the user from opening their mouths more than 2 mm. That’s less than a tenth of an inch. Which is not a lot. So not a lot that essentially all you can consume is liquid.
Oh, and they’ve got results to back up their madness. In a small study, seven otherwise healthy obese women lost an average of 5.1% of their body weight after using the DentalSlim for 2 weeks, though they did complain that the device was difficult to use, caused discomfort and difficulty speaking, made them more tense, and in general made life “less satisfying.” And one participant was able to cheat the system and consume nonhealthy food like chocolate by melting it.
So, there you are, if you want a weight-loss solution that tortures you and has far bigger holes than the one it leaves for your mouth, try the DentalSlim. Or, you know, don’t eat that eighth slice of pizza and maybe go for a walk later. Your choice.
Ignore this pacemaker and it will go away
At some point – and now seems to be that point – we have to say enough is enough. The throwaway culture that produces phones, TVs, and computers that get tossed in the trash because they can’t be repaired has gone too far. That’s right, we’re looking at you, medical science!
This time, it’s a pacemaker that just disappears when it’s no longer needed. Some lazy heart surgeon decided that it was way too much trouble to do another surgery to remove the leads when a temporary pacemaker was no longer needed. You know the type: “It sure would be nice if the pacemaker components were biocompatible and were naturally absorbed by the body over the course of a few weeks and wouldn’t need to be surgically extracted.” Slacker.
Well, get a load of this. Researchers at Northwestern and George Washington universities say that they have come up with a transient pacemaker that “harvests energy from an external, remote antenna using near-field communication protocols – the same technology used in smartphones for electronic payments and in RFID tags.”
That means no batteries and no wires that have to be removed and can cause infections. Because the infectious disease docs also are too lazy to do their jobs, apparently.
The lack of onboard infrastructure means that the device can be very small – it weighs less than half a gram and is only 250 microns thick. And yes, it is bioresorbable and completely harmless. It fully degrades and disappears in 5-7 weeks through the body’s natural biologic processes, “thereby avoiding the need for physical removal of the pacemaker electrodes. This is potentially a major victory for postoperative patients,” said Dr. Rishi Arora, one of the investigators.
A victory for patients, he says. Not a word about the time and effort saved by the surgeons. Typical.
It’s a mask! No, it’s a COVID-19 test!
Mask wearing has gotten more lax as people get vaccinated for COVID-19, but as wearing masks for virus prevention is becoming more normalized in western society, some saw an opportunity to make them work for diagnosis.
Researchers from the Massachusetts Institute of Technology and the Wyss Institute for Biologically Inspired Engineering at Harvard University have found a way to do just that with their wearable freeze-dried cell-free (wFDCF) technology. A single push of a button releases water from a reservoir in the mask that sequentially activates three different freeze-dried biological reactions, which detect the SARS-CoV-2 virus in the wearer’s breath.
Initially meant as a tool for the Zika outbreak in 2015, the team made a quick pivot in May 2020. But this isn’t just some run-of-the-mill, at-home test. The data prove that the wFDCF mask is comparable to polymerase chain reactions tests, the standard in COVID-19 detection. Plus there aren’t any extra factors to deal with, like room or instrument temperature to ensure accuracy. In just 90 minutes, the mask gives results on a readout in a way similar to that of a pregnancy test. Voilà! To have COVID-19 or not to have COVID-19 is an easily answered question.
At LOTME, we think this is a big improvement from having dogs, or even three-foot rats, sniffing out coronavirus.
But wait, there’s more. “In addition to face masks, our programmable biosensors can be integrated into other garments to provide on-the-go detection of dangerous substances including viruses, bacteria, toxins, and chemical agents,” said Peter Nguyen, PhD, study coauthor and research scientist at the Wyss Institute. The technology can be used on lab coats, scrubs, military uniforms, and uniforms of first responders who may come in contact with hazardous pathogens and toxins. Think of all the lives saved and possible avoidances.
If only it could diagnose bad breath.
Finally, an excuse for the all-beer diet
Weight loss is hard work. Extremely hard work, and, as evidenced by the constant inundation and advertisement of quick fixes, crash diets, and expensive gym memberships, there’s not really a solid, 100% solution to the issue. Until now, thanks to a team of doctors from New Zealand, who’ve decided that the best way to combat obesity is to leave you in constant agony.
The DentalSlim Diet Control device is certainly a radical yet comically logical attempt to combat obesity. The creators say that the biggest problem with dieting is compliance, and, well, it’s difficult to eat too much if you can’t actually open your mouth. The metal contraption is mounted onto your teeth and uses magnetic locks to prevent the user from opening their mouths more than 2 mm. That’s less than a tenth of an inch. Which is not a lot. So not a lot that essentially all you can consume is liquid.
Oh, and they’ve got results to back up their madness. In a small study, seven otherwise healthy obese women lost an average of 5.1% of their body weight after using the DentalSlim for 2 weeks, though they did complain that the device was difficult to use, caused discomfort and difficulty speaking, made them more tense, and in general made life “less satisfying.” And one participant was able to cheat the system and consume nonhealthy food like chocolate by melting it.
So, there you are, if you want a weight-loss solution that tortures you and has far bigger holes than the one it leaves for your mouth, try the DentalSlim. Or, you know, don’t eat that eighth slice of pizza and maybe go for a walk later. Your choice.
Almost all U.S. COVID-19 deaths now in the unvaccinated
If you, a friend, or a loved one remain unvaccinated against COVID-19 at this point – for whatever reason – you are at higher risk of dying if you become infected.
That’s the conclusion of a new report released by the Associated Press looking at COVID-19 deaths during May 2021.
Of more than 18,000 people who died from COVID-19, for example, only about 150 were fully vaccinated. That’s less than 1%.
“Recently, I was working in the emergency room [and] I saw a 21-year-old African American who came in with shortness of breath,” said Vino K. Palli, MD, MPH, a physician specializing in emergency medicine, internal medicine, and urgent care.
The patient rapidly deteriorated and required intubation and ventilation. She was transferred to a specialized hospital for possible extracorporeal membrane oxygenation (ECMO) treatment.
“This patient was unvaccinated, along with her entire family. This would have been easily preventable,” added Dr. Palli, who is also founder and CEO of MiDoctor Urgent Care in New York City.
“Vaccine misinformation, compounded with vaccine inertia and vaccine access, have contributed to this,” he added. “Even though we have a surplus amount of vaccines at this time, we are only seeing 50% to 55% of completely vaccinated patients.”
Authors of the Associated Press report also acknowledge that some people who are fully vaccinated can get a breakthrough infection. These occurred in fewer than 1,200 of more than 853,000 people hospitalized for COVID-19 in May, or about 0.1%.
The Associated Press came up with these numbers using data from the Centers for Disease Control and Prevention. The CDC tracks the numbers of cases, hospitalizations, and deaths but does not breakdown rates by vaccination status.
Stronger argument for vaccination?
“The fact that only 0.8% of COVID-19 deaths are in the fully vaccinated should persuade those people still hesitant about vaccination,” said Hugh Cassiere, MD, medical director of Respiratory Therapy Services at North Shore University Hospital in Manhasset, New York.
Stuart C. Ray, MD, professor of medicine and oncology in the Division of Infectious Diseases at Johns Hopkins University, Baltimore, agreed. “It seems compelling, even for skeptics, that unvaccinated people represent 99% of those now dying from COVID-19 when they represent less than 50% of the adult population in the United States.”
The findings from the study could be more persuasive than previous arguments made in favor of immunization, Dr. Ray said. “These recent findings of striking reductions in risk of death in the vaccinated are more directly attributable and harder to ignore or dismiss.”
Brian Labus, PhD, MPH, of the University of Nevada Las Vegas (UNLV) is less convinced. “While this might change some peoples’ minds, it probably won’t make a major difference. People have many different reasons for not getting vaccinated, and this is only one of the things they consider.”
The study adds information that was not available before, said Dr. Labus, assistant professor in the Department of Epidemiology and Biostatistics at the UNLV School of Public Health. “We study the vaccine under tightly controlled, ideal conditions. This is the evidence that it works as well in the real world as it did in the trials, and that is what is most important in implementing a vaccination program,” added Dr. Labus.
“The scientific data has honed in on one thing: Vaccines are effective in preventing hospitalizations, ICU admissions, ventilations, and deaths,” agreed Dr. Palli.
“We now know that almost all deaths occurred in patients who were not vaccinated. We also know that all vaccines are effective against various strains that are in circulation right now, including the Delta variant, which is rapidly spreading,” Dr. Palli said.
Dr. Cassiere pointed out that the unvaccinated are not only at higher risk of developing COVID-19 but also of spreading, being hospitalized for, and dying from the infection. Avoiding “long hauler” symptoms is another argument in favor of immunization, he added.
As of June 28, the CDC reports that 63% of Americans 12 years and older have received at least one dose of a COVID-19 vaccine, and 54% are fully vaccinated.
Worldwide worry?
Although overall rates of U.S. COVID-19 hospitalizations and deaths are down, the outlook may not remain as encouraging. “I hope I’m wrong about this, but I anticipate that the coming fall and winter will bring increasingly localized versions of similar findings – severe disease and death due to SARS-CoV-2 infection in regions or groups with lower vaccination rates,” Dr. Ray said.
There could be a silver lining, he added: “If this unfortunate surge occurs, the health and economic consequences seem likely to erode much of the remaining hesitancy regarding vaccination.”
The rise of more infectious SARS-CoV-2 variants, such as the Delta variant, could also throw a wrench in controlling COVID-19. “This isn’t just a domestic issue,” Dr. Ray said. “We have learned that the world is a small place in pandemic times.”
The Associated Press investigators state that their findings support the high efficacy of the vaccine. Also, given the current widespread availability of COVID-19 vaccines in the United States, they believe many of the COVID-19 deaths now occurring are preventable.
Public health measures should have continued longer to protect unvaccinated individuals, especially Black Americans, Hispanic Americans, and other minorities, Dr. Palli said. “Only time will tell if re-opening and abandoning all public health measures by the CDC was premature.”
A version of this article first appeared on Medscape.com.
If you, a friend, or a loved one remain unvaccinated against COVID-19 at this point – for whatever reason – you are at higher risk of dying if you become infected.
That’s the conclusion of a new report released by the Associated Press looking at COVID-19 deaths during May 2021.
Of more than 18,000 people who died from COVID-19, for example, only about 150 were fully vaccinated. That’s less than 1%.
“Recently, I was working in the emergency room [and] I saw a 21-year-old African American who came in with shortness of breath,” said Vino K. Palli, MD, MPH, a physician specializing in emergency medicine, internal medicine, and urgent care.
The patient rapidly deteriorated and required intubation and ventilation. She was transferred to a specialized hospital for possible extracorporeal membrane oxygenation (ECMO) treatment.
“This patient was unvaccinated, along with her entire family. This would have been easily preventable,” added Dr. Palli, who is also founder and CEO of MiDoctor Urgent Care in New York City.
“Vaccine misinformation, compounded with vaccine inertia and vaccine access, have contributed to this,” he added. “Even though we have a surplus amount of vaccines at this time, we are only seeing 50% to 55% of completely vaccinated patients.”
Authors of the Associated Press report also acknowledge that some people who are fully vaccinated can get a breakthrough infection. These occurred in fewer than 1,200 of more than 853,000 people hospitalized for COVID-19 in May, or about 0.1%.
The Associated Press came up with these numbers using data from the Centers for Disease Control and Prevention. The CDC tracks the numbers of cases, hospitalizations, and deaths but does not breakdown rates by vaccination status.
Stronger argument for vaccination?
“The fact that only 0.8% of COVID-19 deaths are in the fully vaccinated should persuade those people still hesitant about vaccination,” said Hugh Cassiere, MD, medical director of Respiratory Therapy Services at North Shore University Hospital in Manhasset, New York.
Stuart C. Ray, MD, professor of medicine and oncology in the Division of Infectious Diseases at Johns Hopkins University, Baltimore, agreed. “It seems compelling, even for skeptics, that unvaccinated people represent 99% of those now dying from COVID-19 when they represent less than 50% of the adult population in the United States.”
The findings from the study could be more persuasive than previous arguments made in favor of immunization, Dr. Ray said. “These recent findings of striking reductions in risk of death in the vaccinated are more directly attributable and harder to ignore or dismiss.”
Brian Labus, PhD, MPH, of the University of Nevada Las Vegas (UNLV) is less convinced. “While this might change some peoples’ minds, it probably won’t make a major difference. People have many different reasons for not getting vaccinated, and this is only one of the things they consider.”
The study adds information that was not available before, said Dr. Labus, assistant professor in the Department of Epidemiology and Biostatistics at the UNLV School of Public Health. “We study the vaccine under tightly controlled, ideal conditions. This is the evidence that it works as well in the real world as it did in the trials, and that is what is most important in implementing a vaccination program,” added Dr. Labus.
“The scientific data has honed in on one thing: Vaccines are effective in preventing hospitalizations, ICU admissions, ventilations, and deaths,” agreed Dr. Palli.
“We now know that almost all deaths occurred in patients who were not vaccinated. We also know that all vaccines are effective against various strains that are in circulation right now, including the Delta variant, which is rapidly spreading,” Dr. Palli said.
Dr. Cassiere pointed out that the unvaccinated are not only at higher risk of developing COVID-19 but also of spreading, being hospitalized for, and dying from the infection. Avoiding “long hauler” symptoms is another argument in favor of immunization, he added.
As of June 28, the CDC reports that 63% of Americans 12 years and older have received at least one dose of a COVID-19 vaccine, and 54% are fully vaccinated.
Worldwide worry?
Although overall rates of U.S. COVID-19 hospitalizations and deaths are down, the outlook may not remain as encouraging. “I hope I’m wrong about this, but I anticipate that the coming fall and winter will bring increasingly localized versions of similar findings – severe disease and death due to SARS-CoV-2 infection in regions or groups with lower vaccination rates,” Dr. Ray said.
There could be a silver lining, he added: “If this unfortunate surge occurs, the health and economic consequences seem likely to erode much of the remaining hesitancy regarding vaccination.”
The rise of more infectious SARS-CoV-2 variants, such as the Delta variant, could also throw a wrench in controlling COVID-19. “This isn’t just a domestic issue,” Dr. Ray said. “We have learned that the world is a small place in pandemic times.”
The Associated Press investigators state that their findings support the high efficacy of the vaccine. Also, given the current widespread availability of COVID-19 vaccines in the United States, they believe many of the COVID-19 deaths now occurring are preventable.
Public health measures should have continued longer to protect unvaccinated individuals, especially Black Americans, Hispanic Americans, and other minorities, Dr. Palli said. “Only time will tell if re-opening and abandoning all public health measures by the CDC was premature.”
A version of this article first appeared on Medscape.com.
If you, a friend, or a loved one remain unvaccinated against COVID-19 at this point – for whatever reason – you are at higher risk of dying if you become infected.
That’s the conclusion of a new report released by the Associated Press looking at COVID-19 deaths during May 2021.
Of more than 18,000 people who died from COVID-19, for example, only about 150 were fully vaccinated. That’s less than 1%.
“Recently, I was working in the emergency room [and] I saw a 21-year-old African American who came in with shortness of breath,” said Vino K. Palli, MD, MPH, a physician specializing in emergency medicine, internal medicine, and urgent care.
The patient rapidly deteriorated and required intubation and ventilation. She was transferred to a specialized hospital for possible extracorporeal membrane oxygenation (ECMO) treatment.
“This patient was unvaccinated, along with her entire family. This would have been easily preventable,” added Dr. Palli, who is also founder and CEO of MiDoctor Urgent Care in New York City.
“Vaccine misinformation, compounded with vaccine inertia and vaccine access, have contributed to this,” he added. “Even though we have a surplus amount of vaccines at this time, we are only seeing 50% to 55% of completely vaccinated patients.”
Authors of the Associated Press report also acknowledge that some people who are fully vaccinated can get a breakthrough infection. These occurred in fewer than 1,200 of more than 853,000 people hospitalized for COVID-19 in May, or about 0.1%.
The Associated Press came up with these numbers using data from the Centers for Disease Control and Prevention. The CDC tracks the numbers of cases, hospitalizations, and deaths but does not breakdown rates by vaccination status.
Stronger argument for vaccination?
“The fact that only 0.8% of COVID-19 deaths are in the fully vaccinated should persuade those people still hesitant about vaccination,” said Hugh Cassiere, MD, medical director of Respiratory Therapy Services at North Shore University Hospital in Manhasset, New York.
Stuart C. Ray, MD, professor of medicine and oncology in the Division of Infectious Diseases at Johns Hopkins University, Baltimore, agreed. “It seems compelling, even for skeptics, that unvaccinated people represent 99% of those now dying from COVID-19 when they represent less than 50% of the adult population in the United States.”
The findings from the study could be more persuasive than previous arguments made in favor of immunization, Dr. Ray said. “These recent findings of striking reductions in risk of death in the vaccinated are more directly attributable and harder to ignore or dismiss.”
Brian Labus, PhD, MPH, of the University of Nevada Las Vegas (UNLV) is less convinced. “While this might change some peoples’ minds, it probably won’t make a major difference. People have many different reasons for not getting vaccinated, and this is only one of the things they consider.”
The study adds information that was not available before, said Dr. Labus, assistant professor in the Department of Epidemiology and Biostatistics at the UNLV School of Public Health. “We study the vaccine under tightly controlled, ideal conditions. This is the evidence that it works as well in the real world as it did in the trials, and that is what is most important in implementing a vaccination program,” added Dr. Labus.
“The scientific data has honed in on one thing: Vaccines are effective in preventing hospitalizations, ICU admissions, ventilations, and deaths,” agreed Dr. Palli.
“We now know that almost all deaths occurred in patients who were not vaccinated. We also know that all vaccines are effective against various strains that are in circulation right now, including the Delta variant, which is rapidly spreading,” Dr. Palli said.
Dr. Cassiere pointed out that the unvaccinated are not only at higher risk of developing COVID-19 but also of spreading, being hospitalized for, and dying from the infection. Avoiding “long hauler” symptoms is another argument in favor of immunization, he added.
As of June 28, the CDC reports that 63% of Americans 12 years and older have received at least one dose of a COVID-19 vaccine, and 54% are fully vaccinated.
Worldwide worry?
Although overall rates of U.S. COVID-19 hospitalizations and deaths are down, the outlook may not remain as encouraging. “I hope I’m wrong about this, but I anticipate that the coming fall and winter will bring increasingly localized versions of similar findings – severe disease and death due to SARS-CoV-2 infection in regions or groups with lower vaccination rates,” Dr. Ray said.
There could be a silver lining, he added: “If this unfortunate surge occurs, the health and economic consequences seem likely to erode much of the remaining hesitancy regarding vaccination.”
The rise of more infectious SARS-CoV-2 variants, such as the Delta variant, could also throw a wrench in controlling COVID-19. “This isn’t just a domestic issue,” Dr. Ray said. “We have learned that the world is a small place in pandemic times.”
The Associated Press investigators state that their findings support the high efficacy of the vaccine. Also, given the current widespread availability of COVID-19 vaccines in the United States, they believe many of the COVID-19 deaths now occurring are preventable.
Public health measures should have continued longer to protect unvaccinated individuals, especially Black Americans, Hispanic Americans, and other minorities, Dr. Palli said. “Only time will tell if re-opening and abandoning all public health measures by the CDC was premature.”
A version of this article first appeared on Medscape.com.
Physician fired after slurs, including ‘cannibalism,’ against Israel
Fidaa Wishah, MD, a pediatric radiologist at Phoenix Children’s Hospital in Arizona, has been fired after the hospital reviewed evidence that included her anti-Israel comments on social media, according to the hospital’s statement.
On May 26, Dr. Wishah posted, “We will uncover your thirst to kill our Palestinian children. … We sense your fear. The fear of your collapse. A state based on atrocity, inhumanity, racism and cannibalism never last long! Hey #israel … your end is coming sooner than you think.”
Phoenix Children’s Hospital did not respond to this news organization’s request for comment but said in a statement to the Jewish News Syndicate : “After a thorough review of the facts related to this matter, this individual is no longer providing care at Phoenix Children’s. All children in the care of Phoenix Children’s receive hope, healing and the best possible health care, regardless of race, color, disability, religion, gender, gender identity, sexual orientation or national origin.”
Dr. Wishah’s profile has been removed from the hospital website. Her LinkedIn profile indicates she had been a pediatric radiology fellow at Stanford (Calif.) University, specializing in advanced magnetic resonance imaging and fetal imaging and had been a senior staff pediatric radiologist at Henry Ford Health System in Detroit.
It wasn’t the first time antisemitic comments have led to the firing of a physician. Last year, this news organization wrote about Lara Kollab, DO, a first-year resident fired for her antisemitic tweets. She was subsequently barred from medicine.
In the same post from May 26, Dr. Wishah also wrote: “We will not be #censored anymore! Bomb our media buildings and we have the phones[.] Bribe the mainstream media and we have our small #socialmedia platforms[.] From our windows ... from our streets ... next the rubble we will expose you to the world[.] We will expose the #massacre and #genocide you #zionists are proud of[.]”
Today, CAIR-AZ, a group whose mission is to “enhance understanding of Islam, protect civil rights, promote justice, and empower American Muslims,” according to its website, announced that it, along with three private law firms, will represent Dr. Wishah in what they referred to as “her wrongful termination case against Phoenix Children’s Hospital.”
The announcement, which mentions that Dr. Wishah was born and raised in Gaza, said, “Dr. Wishah has been a medical doctor since 2010 and has spent the vast majority of her career as a pediatric physician. Despite caring for thousands of children, many of whom are Jewish, she has never been accused of discriminating against any of her patients or colleagues.”
The statement added, “PCH’s decision to terminate Dr. Wishah is shameful and an attack on freedom of speech.”
A version of this article first appeared on Medscape.com.
Fidaa Wishah, MD, a pediatric radiologist at Phoenix Children’s Hospital in Arizona, has been fired after the hospital reviewed evidence that included her anti-Israel comments on social media, according to the hospital’s statement.
On May 26, Dr. Wishah posted, “We will uncover your thirst to kill our Palestinian children. … We sense your fear. The fear of your collapse. A state based on atrocity, inhumanity, racism and cannibalism never last long! Hey #israel … your end is coming sooner than you think.”
Phoenix Children’s Hospital did not respond to this news organization’s request for comment but said in a statement to the Jewish News Syndicate : “After a thorough review of the facts related to this matter, this individual is no longer providing care at Phoenix Children’s. All children in the care of Phoenix Children’s receive hope, healing and the best possible health care, regardless of race, color, disability, religion, gender, gender identity, sexual orientation or national origin.”
Dr. Wishah’s profile has been removed from the hospital website. Her LinkedIn profile indicates she had been a pediatric radiology fellow at Stanford (Calif.) University, specializing in advanced magnetic resonance imaging and fetal imaging and had been a senior staff pediatric radiologist at Henry Ford Health System in Detroit.
It wasn’t the first time antisemitic comments have led to the firing of a physician. Last year, this news organization wrote about Lara Kollab, DO, a first-year resident fired for her antisemitic tweets. She was subsequently barred from medicine.
In the same post from May 26, Dr. Wishah also wrote: “We will not be #censored anymore! Bomb our media buildings and we have the phones[.] Bribe the mainstream media and we have our small #socialmedia platforms[.] From our windows ... from our streets ... next the rubble we will expose you to the world[.] We will expose the #massacre and #genocide you #zionists are proud of[.]”
Today, CAIR-AZ, a group whose mission is to “enhance understanding of Islam, protect civil rights, promote justice, and empower American Muslims,” according to its website, announced that it, along with three private law firms, will represent Dr. Wishah in what they referred to as “her wrongful termination case against Phoenix Children’s Hospital.”
The announcement, which mentions that Dr. Wishah was born and raised in Gaza, said, “Dr. Wishah has been a medical doctor since 2010 and has spent the vast majority of her career as a pediatric physician. Despite caring for thousands of children, many of whom are Jewish, she has never been accused of discriminating against any of her patients or colleagues.”
The statement added, “PCH’s decision to terminate Dr. Wishah is shameful and an attack on freedom of speech.”
A version of this article first appeared on Medscape.com.
Fidaa Wishah, MD, a pediatric radiologist at Phoenix Children’s Hospital in Arizona, has been fired after the hospital reviewed evidence that included her anti-Israel comments on social media, according to the hospital’s statement.
On May 26, Dr. Wishah posted, “We will uncover your thirst to kill our Palestinian children. … We sense your fear. The fear of your collapse. A state based on atrocity, inhumanity, racism and cannibalism never last long! Hey #israel … your end is coming sooner than you think.”
Phoenix Children’s Hospital did not respond to this news organization’s request for comment but said in a statement to the Jewish News Syndicate : “After a thorough review of the facts related to this matter, this individual is no longer providing care at Phoenix Children’s. All children in the care of Phoenix Children’s receive hope, healing and the best possible health care, regardless of race, color, disability, religion, gender, gender identity, sexual orientation or national origin.”
Dr. Wishah’s profile has been removed from the hospital website. Her LinkedIn profile indicates she had been a pediatric radiology fellow at Stanford (Calif.) University, specializing in advanced magnetic resonance imaging and fetal imaging and had been a senior staff pediatric radiologist at Henry Ford Health System in Detroit.
It wasn’t the first time antisemitic comments have led to the firing of a physician. Last year, this news organization wrote about Lara Kollab, DO, a first-year resident fired for her antisemitic tweets. She was subsequently barred from medicine.
In the same post from May 26, Dr. Wishah also wrote: “We will not be #censored anymore! Bomb our media buildings and we have the phones[.] Bribe the mainstream media and we have our small #socialmedia platforms[.] From our windows ... from our streets ... next the rubble we will expose you to the world[.] We will expose the #massacre and #genocide you #zionists are proud of[.]”
Today, CAIR-AZ, a group whose mission is to “enhance understanding of Islam, protect civil rights, promote justice, and empower American Muslims,” according to its website, announced that it, along with three private law firms, will represent Dr. Wishah in what they referred to as “her wrongful termination case against Phoenix Children’s Hospital.”
The announcement, which mentions that Dr. Wishah was born and raised in Gaza, said, “Dr. Wishah has been a medical doctor since 2010 and has spent the vast majority of her career as a pediatric physician. Despite caring for thousands of children, many of whom are Jewish, she has never been accused of discriminating against any of her patients or colleagues.”
The statement added, “PCH’s decision to terminate Dr. Wishah is shameful and an attack on freedom of speech.”
A version of this article first appeared on Medscape.com.
EAS lipid guidance: Start high-risk patients on combo drug
Very-high-risk dyslipidemia patients unlikely to reach goal with a statin should be given combination statin–ezetimibe (Nustendi) therapy upfront, rather than wasting time and resources on trialing a statin alone, suggests a practical guidance document.
The document points out that, even with high-intensity statin therapy, patients achieve a reduction in low-density-lipoprotein (LDL) cholesterol levels of around 50%, which for many is not enough for them to achieve the stringent new guideline targets deemed necessary for risk reduction.
Instead, clinicians should determine at the first visit whether their patient, if they are not already on a statin, is likely to reach their goal with that drug alone, and if not, should immediately start them on the combination.
The guidance, which aims to offer a practical way to implement the 2019 European Society of Cardiology/EAS guidelines for the management of dyslipidemias, was published April 12 in Atherosclerosis .
Lead author Alberico L. Catapano, MD, PhD, discussed the new practical guidance at the recent European Atherosclerosis Society (EAS) 2021 Virtual Congress.
He explained that the motivation for creating the practical guidance was “very simple” and concerns something already embedded in the ESC/EAS guidelines; it’s just that “people didn’t notice” it.
Dr. Catapano, professor of pharmacology at the University of Milan and past president of the EAS, said the guidelines set out the average reduction in LDL-cholesterol levels “you can get by starting with high-intensity therapy and/or starting with a combination therapy.”
The guidelines, he said, suggest steps for achieving lipid control: Begin with a statin, add ezetimibe if the patient is still not at goal, and proceed to a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor if the patient is still not at target levels.
Dr. Catapano added that, “having said that, at the beginning, you can guess by knowing how far you are from the goal as to whether a statin by itself with help you get [there].”
If clinicians follow the new practical guidance of giving upfront combination statin–ezetimibe therapy in very-high-risk patients with high LDL-cholesterol levels, it will “save a lot of time, a lot of clinic visits, and will you get you to goal earlier.”
He gave the example of a patient who has an LDL-cholesterol level of 190 mg/dL, who would be classified as being at very high risk. With the target goal of 55 mg/dL, “you would never be able to get them to goal [with only] a high-intensity statin.”
The addition of ezetimibe to the regimen of this patient would have two advantages, Dr. Catapano said. The first is that “you get to goal more easily,” and the second is that, with the drugs available as a single-pill combination, it “makes it easier for the patient to be compliant.”
Consequently, there will be no “unnecessary back and forth,” he said. “Some of these are young people. They go to work; one less visit is less time lost at work.
“This is a practical issue,” he added. “It doesn’t contradict the guidelines,” it’s about “everyday clinical practice.”
Useful between updates
Responding to the guidance, Donald Lloyd-Jones, MD, president-elect of the American Heart Association (AHA), told this news organization that “this kind of document can be useful in periods between updates of the formal guidelines.”
New evidence comes out in between guidelines, and they “don’t often provide us with all of the practical solutions needed for everyday guidance when we’re dealing with individual patients with real-world problems.”
Dr. Lloyd-Jones, who is chair of the Department of Preventive Medicine at Northwestern University, Chicago, said the 2019 ESC/EAS guidelines set “quite aggressive targets, particularly for LDL cholesterol … but didn’t really provide much practical advice on how clinicians could get there for their patients.”
“While this document doesn’t completely address all patient groups, it does provide some good practical advice,” recognizing that “if you need to get to a certain LDL target, it’s unlikely you’re going to get there with just a statin in certain types of patients,” and “if you need a certain amount of LDL lowering, it’s certainly reasonable to start upfront with a statin and ezetimibe and see how you do.”
Crucially, Dr. Lloyd-Jones believes that the practical guidance does “flesh out some of the details the guidelines didn’t address.”
In terms of the aggressive LDL-cholesterol targets set out in the original guidelines, he said that “everyone agrees that lower is always better … and we’ve not get yet found a level that is too low.”
Further, “we’re certainly pushing patients lower and lower, especially with the use of PCSK9 inhibitors, so I think the general philosophy is consistent and correct,” although “it’s difficult to point to great evidence from clinical trials that specially says that 55 mg/dL or 40 mg/dL is the right target for a given group of patients.”
“There’s really very limited evidence for those specific numbers,” Dr. Lloyd-Jones added, “but I think everyone agrees, especially for patients at higher risk, the lower we can get them the better. What really matters, and what this document starts to address, is how we achieve as low as possible, and I think there are some important considerations that they take into account.”
Aside from how far patients need their LDL cholesterol lowered from baseline, there are issues like cost and patient preference for different types of medication, and these “weren’t particularly well addressed in the guidelines,” he added.
Scott D. Isaacs, MD, Secretary of the American Association of Clinical Endocrinologists (AACE), commented that the ESC/EAS recommendations echo the 2017 AACE/American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease.
He said that both guidelines “call for the need to lower LDL cholesterol as much as possible to prevent cardiovascular disease.”
He agreed, however, that high- or very-high-risk patients “have aggressive LDL targets that are often lower than what can be accomplished with high-dose, high-intensity statin monotherapy. Therefore, starting with combination therapy … will get more patients to goal more quickly and will prevent more cardiovascular events.”
Isaacs added: “It just makes sense that if you know a drug will not be strong enough, then you should start with two drugs.”
He noted that this approach is commonly used for conditions such as diabetes and hypertension, “when monotherapy is not expected to achieve the desired results.”
Dr. Isaacs also underlined that the combination of a statin plus ezetimibe “is appealing because of the price and ease of use.”
Although PCSK9 inhibitors are more potent and achieve even lower LDL levels, “the higher price and need to take an injection has limited their use,” he noted.
“One would expect that as the prices of PCSK9 inhibitors come down, their place in care pathways will move up since they are more effective and have proven cardiovascular benefit, but for now, statin plus ezetimibe is a potent and cost-effective way to achieve LDL targets in high- and very-high-risk patients,” Dr. Isaacs concluded.
One issue Dr. Lloyd-Jones raised with the ESC/EAS guidelines is that they seem to have put a lot of weight Mendelian randomization analysis.
“Those are useful in understanding whether having low LDL-cholesterol levels or triglycerides naturally are better for you – of course they are – but they actually provide no evidence about treatment effects, so I think what we need from that is actual data from the clinical trials to understand the treatment effects, both positive and negative.”
He added that that “really then helps us to drive to how and in whom we want to achieve the lowest levels possible.”
Dr. Lloyd-Jones said that Mendelian randomization analyses “continue to crop in a lot of these ESC and EAS documents,” and although they are “elegant and interesting,” they “don’t really inform treatment at all.”
No funding declared. Catapano declares relationships with Pfizer, Sanofi, Regeneron, Merck, Mediolanum, SigmaTau, Menarini, Kowa, Recordati, Eli Lilly, AstraZeneca, Merck, Aegerion and Amgen.
A version of this article first appeared on Medscape.com.
Very-high-risk dyslipidemia patients unlikely to reach goal with a statin should be given combination statin–ezetimibe (Nustendi) therapy upfront, rather than wasting time and resources on trialing a statin alone, suggests a practical guidance document.
The document points out that, even with high-intensity statin therapy, patients achieve a reduction in low-density-lipoprotein (LDL) cholesterol levels of around 50%, which for many is not enough for them to achieve the stringent new guideline targets deemed necessary for risk reduction.
Instead, clinicians should determine at the first visit whether their patient, if they are not already on a statin, is likely to reach their goal with that drug alone, and if not, should immediately start them on the combination.
The guidance, which aims to offer a practical way to implement the 2019 European Society of Cardiology/EAS guidelines for the management of dyslipidemias, was published April 12 in Atherosclerosis .
Lead author Alberico L. Catapano, MD, PhD, discussed the new practical guidance at the recent European Atherosclerosis Society (EAS) 2021 Virtual Congress.
He explained that the motivation for creating the practical guidance was “very simple” and concerns something already embedded in the ESC/EAS guidelines; it’s just that “people didn’t notice” it.
Dr. Catapano, professor of pharmacology at the University of Milan and past president of the EAS, said the guidelines set out the average reduction in LDL-cholesterol levels “you can get by starting with high-intensity therapy and/or starting with a combination therapy.”
The guidelines, he said, suggest steps for achieving lipid control: Begin with a statin, add ezetimibe if the patient is still not at goal, and proceed to a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor if the patient is still not at target levels.
Dr. Catapano added that, “having said that, at the beginning, you can guess by knowing how far you are from the goal as to whether a statin by itself with help you get [there].”
If clinicians follow the new practical guidance of giving upfront combination statin–ezetimibe therapy in very-high-risk patients with high LDL-cholesterol levels, it will “save a lot of time, a lot of clinic visits, and will you get you to goal earlier.”
He gave the example of a patient who has an LDL-cholesterol level of 190 mg/dL, who would be classified as being at very high risk. With the target goal of 55 mg/dL, “you would never be able to get them to goal [with only] a high-intensity statin.”
The addition of ezetimibe to the regimen of this patient would have two advantages, Dr. Catapano said. The first is that “you get to goal more easily,” and the second is that, with the drugs available as a single-pill combination, it “makes it easier for the patient to be compliant.”
Consequently, there will be no “unnecessary back and forth,” he said. “Some of these are young people. They go to work; one less visit is less time lost at work.
“This is a practical issue,” he added. “It doesn’t contradict the guidelines,” it’s about “everyday clinical practice.”
Useful between updates
Responding to the guidance, Donald Lloyd-Jones, MD, president-elect of the American Heart Association (AHA), told this news organization that “this kind of document can be useful in periods between updates of the formal guidelines.”
New evidence comes out in between guidelines, and they “don’t often provide us with all of the practical solutions needed for everyday guidance when we’re dealing with individual patients with real-world problems.”
Dr. Lloyd-Jones, who is chair of the Department of Preventive Medicine at Northwestern University, Chicago, said the 2019 ESC/EAS guidelines set “quite aggressive targets, particularly for LDL cholesterol … but didn’t really provide much practical advice on how clinicians could get there for their patients.”
“While this document doesn’t completely address all patient groups, it does provide some good practical advice,” recognizing that “if you need to get to a certain LDL target, it’s unlikely you’re going to get there with just a statin in certain types of patients,” and “if you need a certain amount of LDL lowering, it’s certainly reasonable to start upfront with a statin and ezetimibe and see how you do.”
Crucially, Dr. Lloyd-Jones believes that the practical guidance does “flesh out some of the details the guidelines didn’t address.”
In terms of the aggressive LDL-cholesterol targets set out in the original guidelines, he said that “everyone agrees that lower is always better … and we’ve not get yet found a level that is too low.”
Further, “we’re certainly pushing patients lower and lower, especially with the use of PCSK9 inhibitors, so I think the general philosophy is consistent and correct,” although “it’s difficult to point to great evidence from clinical trials that specially says that 55 mg/dL or 40 mg/dL is the right target for a given group of patients.”
“There’s really very limited evidence for those specific numbers,” Dr. Lloyd-Jones added, “but I think everyone agrees, especially for patients at higher risk, the lower we can get them the better. What really matters, and what this document starts to address, is how we achieve as low as possible, and I think there are some important considerations that they take into account.”
Aside from how far patients need their LDL cholesterol lowered from baseline, there are issues like cost and patient preference for different types of medication, and these “weren’t particularly well addressed in the guidelines,” he added.
Scott D. Isaacs, MD, Secretary of the American Association of Clinical Endocrinologists (AACE), commented that the ESC/EAS recommendations echo the 2017 AACE/American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease.
He said that both guidelines “call for the need to lower LDL cholesterol as much as possible to prevent cardiovascular disease.”
He agreed, however, that high- or very-high-risk patients “have aggressive LDL targets that are often lower than what can be accomplished with high-dose, high-intensity statin monotherapy. Therefore, starting with combination therapy … will get more patients to goal more quickly and will prevent more cardiovascular events.”
Isaacs added: “It just makes sense that if you know a drug will not be strong enough, then you should start with two drugs.”
He noted that this approach is commonly used for conditions such as diabetes and hypertension, “when monotherapy is not expected to achieve the desired results.”
Dr. Isaacs also underlined that the combination of a statin plus ezetimibe “is appealing because of the price and ease of use.”
Although PCSK9 inhibitors are more potent and achieve even lower LDL levels, “the higher price and need to take an injection has limited their use,” he noted.
“One would expect that as the prices of PCSK9 inhibitors come down, their place in care pathways will move up since they are more effective and have proven cardiovascular benefit, but for now, statin plus ezetimibe is a potent and cost-effective way to achieve LDL targets in high- and very-high-risk patients,” Dr. Isaacs concluded.
One issue Dr. Lloyd-Jones raised with the ESC/EAS guidelines is that they seem to have put a lot of weight Mendelian randomization analysis.
“Those are useful in understanding whether having low LDL-cholesterol levels or triglycerides naturally are better for you – of course they are – but they actually provide no evidence about treatment effects, so I think what we need from that is actual data from the clinical trials to understand the treatment effects, both positive and negative.”
He added that that “really then helps us to drive to how and in whom we want to achieve the lowest levels possible.”
Dr. Lloyd-Jones said that Mendelian randomization analyses “continue to crop in a lot of these ESC and EAS documents,” and although they are “elegant and interesting,” they “don’t really inform treatment at all.”
No funding declared. Catapano declares relationships with Pfizer, Sanofi, Regeneron, Merck, Mediolanum, SigmaTau, Menarini, Kowa, Recordati, Eli Lilly, AstraZeneca, Merck, Aegerion and Amgen.
A version of this article first appeared on Medscape.com.
Very-high-risk dyslipidemia patients unlikely to reach goal with a statin should be given combination statin–ezetimibe (Nustendi) therapy upfront, rather than wasting time and resources on trialing a statin alone, suggests a practical guidance document.
The document points out that, even with high-intensity statin therapy, patients achieve a reduction in low-density-lipoprotein (LDL) cholesterol levels of around 50%, which for many is not enough for them to achieve the stringent new guideline targets deemed necessary for risk reduction.
Instead, clinicians should determine at the first visit whether their patient, if they are not already on a statin, is likely to reach their goal with that drug alone, and if not, should immediately start them on the combination.
The guidance, which aims to offer a practical way to implement the 2019 European Society of Cardiology/EAS guidelines for the management of dyslipidemias, was published April 12 in Atherosclerosis .
Lead author Alberico L. Catapano, MD, PhD, discussed the new practical guidance at the recent European Atherosclerosis Society (EAS) 2021 Virtual Congress.
He explained that the motivation for creating the practical guidance was “very simple” and concerns something already embedded in the ESC/EAS guidelines; it’s just that “people didn’t notice” it.
Dr. Catapano, professor of pharmacology at the University of Milan and past president of the EAS, said the guidelines set out the average reduction in LDL-cholesterol levels “you can get by starting with high-intensity therapy and/or starting with a combination therapy.”
The guidelines, he said, suggest steps for achieving lipid control: Begin with a statin, add ezetimibe if the patient is still not at goal, and proceed to a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor if the patient is still not at target levels.
Dr. Catapano added that, “having said that, at the beginning, you can guess by knowing how far you are from the goal as to whether a statin by itself with help you get [there].”
If clinicians follow the new practical guidance of giving upfront combination statin–ezetimibe therapy in very-high-risk patients with high LDL-cholesterol levels, it will “save a lot of time, a lot of clinic visits, and will you get you to goal earlier.”
He gave the example of a patient who has an LDL-cholesterol level of 190 mg/dL, who would be classified as being at very high risk. With the target goal of 55 mg/dL, “you would never be able to get them to goal [with only] a high-intensity statin.”
The addition of ezetimibe to the regimen of this patient would have two advantages, Dr. Catapano said. The first is that “you get to goal more easily,” and the second is that, with the drugs available as a single-pill combination, it “makes it easier for the patient to be compliant.”
Consequently, there will be no “unnecessary back and forth,” he said. “Some of these are young people. They go to work; one less visit is less time lost at work.
“This is a practical issue,” he added. “It doesn’t contradict the guidelines,” it’s about “everyday clinical practice.”
Useful between updates
Responding to the guidance, Donald Lloyd-Jones, MD, president-elect of the American Heart Association (AHA), told this news organization that “this kind of document can be useful in periods between updates of the formal guidelines.”
New evidence comes out in between guidelines, and they “don’t often provide us with all of the practical solutions needed for everyday guidance when we’re dealing with individual patients with real-world problems.”
Dr. Lloyd-Jones, who is chair of the Department of Preventive Medicine at Northwestern University, Chicago, said the 2019 ESC/EAS guidelines set “quite aggressive targets, particularly for LDL cholesterol … but didn’t really provide much practical advice on how clinicians could get there for their patients.”
“While this document doesn’t completely address all patient groups, it does provide some good practical advice,” recognizing that “if you need to get to a certain LDL target, it’s unlikely you’re going to get there with just a statin in certain types of patients,” and “if you need a certain amount of LDL lowering, it’s certainly reasonable to start upfront with a statin and ezetimibe and see how you do.”
Crucially, Dr. Lloyd-Jones believes that the practical guidance does “flesh out some of the details the guidelines didn’t address.”
In terms of the aggressive LDL-cholesterol targets set out in the original guidelines, he said that “everyone agrees that lower is always better … and we’ve not get yet found a level that is too low.”
Further, “we’re certainly pushing patients lower and lower, especially with the use of PCSK9 inhibitors, so I think the general philosophy is consistent and correct,” although “it’s difficult to point to great evidence from clinical trials that specially says that 55 mg/dL or 40 mg/dL is the right target for a given group of patients.”
“There’s really very limited evidence for those specific numbers,” Dr. Lloyd-Jones added, “but I think everyone agrees, especially for patients at higher risk, the lower we can get them the better. What really matters, and what this document starts to address, is how we achieve as low as possible, and I think there are some important considerations that they take into account.”
Aside from how far patients need their LDL cholesterol lowered from baseline, there are issues like cost and patient preference for different types of medication, and these “weren’t particularly well addressed in the guidelines,” he added.
Scott D. Isaacs, MD, Secretary of the American Association of Clinical Endocrinologists (AACE), commented that the ESC/EAS recommendations echo the 2017 AACE/American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease.
He said that both guidelines “call for the need to lower LDL cholesterol as much as possible to prevent cardiovascular disease.”
He agreed, however, that high- or very-high-risk patients “have aggressive LDL targets that are often lower than what can be accomplished with high-dose, high-intensity statin monotherapy. Therefore, starting with combination therapy … will get more patients to goal more quickly and will prevent more cardiovascular events.”
Isaacs added: “It just makes sense that if you know a drug will not be strong enough, then you should start with two drugs.”
He noted that this approach is commonly used for conditions such as diabetes and hypertension, “when monotherapy is not expected to achieve the desired results.”
Dr. Isaacs also underlined that the combination of a statin plus ezetimibe “is appealing because of the price and ease of use.”
Although PCSK9 inhibitors are more potent and achieve even lower LDL levels, “the higher price and need to take an injection has limited their use,” he noted.
“One would expect that as the prices of PCSK9 inhibitors come down, their place in care pathways will move up since they are more effective and have proven cardiovascular benefit, but for now, statin plus ezetimibe is a potent and cost-effective way to achieve LDL targets in high- and very-high-risk patients,” Dr. Isaacs concluded.
One issue Dr. Lloyd-Jones raised with the ESC/EAS guidelines is that they seem to have put a lot of weight Mendelian randomization analysis.
“Those are useful in understanding whether having low LDL-cholesterol levels or triglycerides naturally are better for you – of course they are – but they actually provide no evidence about treatment effects, so I think what we need from that is actual data from the clinical trials to understand the treatment effects, both positive and negative.”
He added that that “really then helps us to drive to how and in whom we want to achieve the lowest levels possible.”
Dr. Lloyd-Jones said that Mendelian randomization analyses “continue to crop in a lot of these ESC and EAS documents,” and although they are “elegant and interesting,” they “don’t really inform treatment at all.”
No funding declared. Catapano declares relationships with Pfizer, Sanofi, Regeneron, Merck, Mediolanum, SigmaTau, Menarini, Kowa, Recordati, Eli Lilly, AstraZeneca, Merck, Aegerion and Amgen.
A version of this article first appeared on Medscape.com.
AMPLITUDE-O: Efpeglenatide benefits in high-risk diabetes
The AMPLITUDE-O phase 3 trial showed that investigational drug efpeglenatide (Sanofi/Hanmi Pharmaceutical) – an exendin-based glucagonlike peptide-1 receptor agonist – was safe and reduced the risk of worsening renal and cardiovascular outcomes in patients with type 2 diabetes at high cardiovascular risk.

That is, in patients with type 2 diabetes and a high prevalence of cardiovascular and kidney disease with a high hemoglobin A1c and moderate use of a sodium-glucose cotransporter 2 inhibitor, subcutaneous efpeglenatide (4 or 6 mg/week) significantly and safely reduced cardiovascular and renal outcomes, said study investigator Naveed Sattar, MD.
Dr. Sattar, of the University of Glasgow, summarized the results during a symposium at the annual scientific sessions of the American Diabetes Association. The study was simultaneously published online in the New England Journal of Medicine.
AMPLITUDE-O was a cardiovascular outcome trial (CVOT) in more than 4,000 high-risk patients with type 2 diabetes followed for a mean of 1.8 years.
Compared with patients who received placebo, those who received either dose of efpeglenatide had a 27% lower risk of a major adverse cardiovascular event, defined as nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular or undetermined causes; a 21% lower risk of expanded MACE (MACE, coronary revascularization, or hospitalization for unstable angina); a 32% lower risk of a composite renal outcome (decrease in kidney function or macroalbuminuria); and a 27% lower risk of MACE or noncardiovascular death.
And “these effects were independent of baseline SGLT2 inhibitors, estimated glomerular filtration rate (eGFR), or metformin use,” Dr. Sattar pointed out.
New and important findings, but Sanofi no longer developing drug
The trial’s primary investigator, Hertzel C. Gerstein, MD, pointed out several new and important findings of the drug and study, compared with CVOTs of seven other GLP-1 receptor agonists.

The trial included more patients (32%) with renal disease (eGFR, 25-60 mL/min) than the other trials.
There were enough patients taking SGLT2 inhibitors at baseline (15%) to show no difference in the effect of a GLP-1 receptor agonist in the presence/absence of an SGLT2 inhibitor.
So this is the first clearly positive GLP-1 receptor agonist CVOT with an exendin-4–based GLP-1 receptor agonist showing that the GLP-1 receptor agonist class is cardioprotective whether or not it is based on a human or animal GLP-1 structure.
And there was a significant reduction in MACE or noncardiovascular death.
“This would be good for people with type 2 diabetes and either cardiovascular or renal disease at high risk for cardiovascular and/or renal outcomes,” said Dr. Gerstein, professor of medicine at McMaster University, Hamilton, Ont.
However, the trial sponsor, Sanofi, is no longer developing the drug. The company returned the rights back to Hanmi, which had started this line of research. “Hopefully” Hanmi or another company will develop the drug further, said Dr. Gerstein.
Sicker patients than in 7 other GLP-1 agonist CVOTs
Efpeglenatide – like two other drugs in the class, exenatide and lixisenatide – is an exendin-based GLP-1 agonist. (Exendin-4 is a peptide found in the saliva of the Gila monster lizard.) In contrast, liraglutide, dulaglutide, albiglutide, and semaglutide are human-analog GLP-1 agonists.
A meta-analysis of the seven CVOTs of these other drugs in this class reported, among other things, that “overall, GLP-1 agonist treatment reduced MACE by 12%.”
Amanda I. Adler, MD, PhD, professor of diabetic medicine and health policy, University of Oxford, (England), and the assigned independent commenter at the symposium, cited many things “the investigators did well.”
Compared with the CVOTs of the other GLP-1 receptor agonists – ELIXA (lixisenatide), LEADER (liraglutide), SUSTAIN-6 (semaglutide), EXSCEL (exenatide), Harmony Outcomes (albiglutide), REWIND (dulaglutide), and PIONEER 6 (oral semaglutide) – patients in the AMPLITUDE-O trial were sicker, she noted.
AMPLITUDE-O participants had the longest duration of diabetes (15 years), lowest mean eGFR of 72 ml/min per 1.73 m2, highest A1c (8.9%), and highest percentage of insulin use (62%), she noted.
The study was primarily a safety and noninferiority trial, she pointed out, although a series of superiority analyses were prespecified that would be conducted if the drug was found to be noninferior to placebo for the primary outcome of 3-point MACE.
It was good that patients were stratified according to SGLT2 inhibitor use – into current user, likely future user, and not likely future user – although “likely future user” may have misclassified some patients.
The various stakeholders – patients, regulators, doctors, payers, statisticians, and the marketing department of any company providing the drug – would want to know more, such as quality of life, long-term effects, and cost, she observed.
Meta-analysis of 8 CVOTs shows stronger class benefit
Dr. Sattar presented an eight-trial meta-analysis (an update of the seven-trial meta-analysis that included data from AMPLITUDE-O), which showed patients with type 2 diabetes who received GLP-1 agonists had a decreased rate of the 3-component MACE and decreased individual components (stroke more so than MI) – regardless of the structure of these drugs (exenatide or human analogs).
The updated meta-analysis also showed that, overall, GLP-1 agonists decreased all-cause mortality and possibly reduced the risk of heart failure hospitalization (perhaps linked to atherosclerotic benefits) as well as renal dysfunction.
There was no increase in risk of severe hypoglycemia, retinopathy, or pancreatic adverse effects.
AMPLITUDE-O: Design and findings
AMPLITUDE-O included 4,076 adults with type 2 diabetes from 344 sites in 28 countries who were screened from May 2018 to April 2019. Participants also had cardiovascular disease or kidney disease (eGFR, 25-60 mL/min) plus at least one other cardiovascular risk factor. They were randomized 1:1:1 to receive subcutaneous efpeglenatide (4 or 6 mg/week) or placebo.
Patients were a mean age of 65, most (87%) were White, and 33% were female. They had a mean A1c of 8.9%. Most (90%) had a history of cardiovascular disease and 31% had current kidney disease.
MACE occurred in 189 participants (7.0%) assigned to efpeglenatide and 125 participants (9.2%) assigned to receive placebo (3.9 vs. 5.3 events/100 person-years) (hazard ratio, 0.73; 95% confidence interval, 0.58-0.92; P < .001 for noninferiority; P = .007 for superiority).
The composite renal outcome event (decreased kidney function or macroalbuminuria) occurred in 353 participants (13.0%) assigned to receive efpeglenatide and in 250 participants (18.4%) assigned to receive placebo (HR, 0.68; 95% CI, 0.57-0.79; P < .001).
Diarrhea, constipation, nausea, vomiting, or bloating occurred more frequently with efpeglenatide than placebo.
The study was funded by Sanofi. Dr. Sattar has reported being on advisory panels for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi, and receiving research support from Boehringer Ingelheim. Dr. Gerstein has reported being a member of advisory panels for Novo Nordisk, Pfizer, and Sanofi, and a consultant for Abbott, Covance, Eli Lilly, Kowa, and Sanofi. He reported receiving research support from AstraZeneca, Eli Lilly, Merck, Novo Nordisk, and Sanofi, and having other relationships with Boehringer Ingelheim, DKSH, Eli Lilly, Sanofi, and Zuellig Pharma. Dr. Adler has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The AMPLITUDE-O phase 3 trial showed that investigational drug efpeglenatide (Sanofi/Hanmi Pharmaceutical) – an exendin-based glucagonlike peptide-1 receptor agonist – was safe and reduced the risk of worsening renal and cardiovascular outcomes in patients with type 2 diabetes at high cardiovascular risk.
That is, in patients with type 2 diabetes and a high prevalence of cardiovascular and kidney disease with a high hemoglobin A1c and moderate use of a sodium-glucose cotransporter 2 inhibitor, subcutaneous efpeglenatide (4 or 6 mg/week) significantly and safely reduced cardiovascular and renal outcomes, said study investigator Naveed Sattar, MD.
Dr. Sattar, of the University of Glasgow, summarized the results during a symposium at the annual scientific sessions of the American Diabetes Association. The study was simultaneously published online in the New England Journal of Medicine.
AMPLITUDE-O was a cardiovascular outcome trial (CVOT) in more than 4,000 high-risk patients with type 2 diabetes followed for a mean of 1.8 years.
Compared with patients who received placebo, those who received either dose of efpeglenatide had a 27% lower risk of a major adverse cardiovascular event, defined as nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular or undetermined causes; a 21% lower risk of expanded MACE (MACE, coronary revascularization, or hospitalization for unstable angina); a 32% lower risk of a composite renal outcome (decrease in kidney function or macroalbuminuria); and a 27% lower risk of MACE or noncardiovascular death.
And “these effects were independent of baseline SGLT2 inhibitors, estimated glomerular filtration rate (eGFR), or metformin use,” Dr. Sattar pointed out.
New and important findings, but Sanofi no longer developing drug
The trial’s primary investigator, Hertzel C. Gerstein, MD, pointed out several new and important findings of the drug and study, compared with CVOTs of seven other GLP-1 receptor agonists.
The trial included more patients (32%) with renal disease (eGFR, 25-60 mL/min) than the other trials.
There were enough patients taking SGLT2 inhibitors at baseline (15%) to show no difference in the effect of a GLP-1 receptor agonist in the presence/absence of an SGLT2 inhibitor.
So this is the first clearly positive GLP-1 receptor agonist CVOT with an exendin-4–based GLP-1 receptor agonist showing that the GLP-1 receptor agonist class is cardioprotective whether or not it is based on a human or animal GLP-1 structure.
And there was a significant reduction in MACE or noncardiovascular death.
“This would be good for people with type 2 diabetes and either cardiovascular or renal disease at high risk for cardiovascular and/or renal outcomes,” said Dr. Gerstein, professor of medicine at McMaster University, Hamilton, Ont.
However, the trial sponsor, Sanofi, is no longer developing the drug. The company returned the rights back to Hanmi, which had started this line of research. “Hopefully” Hanmi or another company will develop the drug further, said Dr. Gerstein.
Sicker patients than in 7 other GLP-1 agonist CVOTs
Efpeglenatide – like two other drugs in the class, exenatide and lixisenatide – is an exendin-based GLP-1 agonist. (Exendin-4 is a peptide found in the saliva of the Gila monster lizard.) In contrast, liraglutide, dulaglutide, albiglutide, and semaglutide are human-analog GLP-1 agonists.
A meta-analysis of the seven CVOTs of these other drugs in this class reported, among other things, that “overall, GLP-1 agonist treatment reduced MACE by 12%.”
Amanda I. Adler, MD, PhD, professor of diabetic medicine and health policy, University of Oxford, (England), and the assigned independent commenter at the symposium, cited many things “the investigators did well.”
Compared with the CVOTs of the other GLP-1 receptor agonists – ELIXA (lixisenatide), LEADER (liraglutide), SUSTAIN-6 (semaglutide), EXSCEL (exenatide), Harmony Outcomes (albiglutide), REWIND (dulaglutide), and PIONEER 6 (oral semaglutide) – patients in the AMPLITUDE-O trial were sicker, she noted.
AMPLITUDE-O participants had the longest duration of diabetes (15 years), lowest mean eGFR of 72 ml/min per 1.73 m2, highest A1c (8.9%), and highest percentage of insulin use (62%), she noted.
The study was primarily a safety and noninferiority trial, she pointed out, although a series of superiority analyses were prespecified that would be conducted if the drug was found to be noninferior to placebo for the primary outcome of 3-point MACE.
It was good that patients were stratified according to SGLT2 inhibitor use – into current user, likely future user, and not likely future user – although “likely future user” may have misclassified some patients.
The various stakeholders – patients, regulators, doctors, payers, statisticians, and the marketing department of any company providing the drug – would want to know more, such as quality of life, long-term effects, and cost, she observed.
Meta-analysis of 8 CVOTs shows stronger class benefit
Dr. Sattar presented an eight-trial meta-analysis (an update of the seven-trial meta-analysis that included data from AMPLITUDE-O), which showed patients with type 2 diabetes who received GLP-1 agonists had a decreased rate of the 3-component MACE and decreased individual components (stroke more so than MI) – regardless of the structure of these drugs (exenatide or human analogs).
The updated meta-analysis also showed that, overall, GLP-1 agonists decreased all-cause mortality and possibly reduced the risk of heart failure hospitalization (perhaps linked to atherosclerotic benefits) as well as renal dysfunction.
There was no increase in risk of severe hypoglycemia, retinopathy, or pancreatic adverse effects.
AMPLITUDE-O: Design and findings
AMPLITUDE-O included 4,076 adults with type 2 diabetes from 344 sites in 28 countries who were screened from May 2018 to April 2019. Participants also had cardiovascular disease or kidney disease (eGFR, 25-60 mL/min) plus at least one other cardiovascular risk factor. They were randomized 1:1:1 to receive subcutaneous efpeglenatide (4 or 6 mg/week) or placebo.
Patients were a mean age of 65, most (87%) were White, and 33% were female. They had a mean A1c of 8.9%. Most (90%) had a history of cardiovascular disease and 31% had current kidney disease.
MACE occurred in 189 participants (7.0%) assigned to efpeglenatide and 125 participants (9.2%) assigned to receive placebo (3.9 vs. 5.3 events/100 person-years) (hazard ratio, 0.73; 95% confidence interval, 0.58-0.92; P < .001 for noninferiority; P = .007 for superiority).
The composite renal outcome event (decreased kidney function or macroalbuminuria) occurred in 353 participants (13.0%) assigned to receive efpeglenatide and in 250 participants (18.4%) assigned to receive placebo (HR, 0.68; 95% CI, 0.57-0.79; P < .001).
Diarrhea, constipation, nausea, vomiting, or bloating occurred more frequently with efpeglenatide than placebo.
The study was funded by Sanofi. Dr. Sattar has reported being on advisory panels for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi, and receiving research support from Boehringer Ingelheim. Dr. Gerstein has reported being a member of advisory panels for Novo Nordisk, Pfizer, and Sanofi, and a consultant for Abbott, Covance, Eli Lilly, Kowa, and Sanofi. He reported receiving research support from AstraZeneca, Eli Lilly, Merck, Novo Nordisk, and Sanofi, and having other relationships with Boehringer Ingelheim, DKSH, Eli Lilly, Sanofi, and Zuellig Pharma. Dr. Adler has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The AMPLITUDE-O phase 3 trial showed that investigational drug efpeglenatide (Sanofi/Hanmi Pharmaceutical) – an exendin-based glucagonlike peptide-1 receptor agonist – was safe and reduced the risk of worsening renal and cardiovascular outcomes in patients with type 2 diabetes at high cardiovascular risk.
That is, in patients with type 2 diabetes and a high prevalence of cardiovascular and kidney disease with a high hemoglobin A1c and moderate use of a sodium-glucose cotransporter 2 inhibitor, subcutaneous efpeglenatide (4 or 6 mg/week) significantly and safely reduced cardiovascular and renal outcomes, said study investigator Naveed Sattar, MD.
Dr. Sattar, of the University of Glasgow, summarized the results during a symposium at the annual scientific sessions of the American Diabetes Association. The study was simultaneously published online in the New England Journal of Medicine.
AMPLITUDE-O was a cardiovascular outcome trial (CVOT) in more than 4,000 high-risk patients with type 2 diabetes followed for a mean of 1.8 years.
Compared with patients who received placebo, those who received either dose of efpeglenatide had a 27% lower risk of a major adverse cardiovascular event, defined as nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular or undetermined causes; a 21% lower risk of expanded MACE (MACE, coronary revascularization, or hospitalization for unstable angina); a 32% lower risk of a composite renal outcome (decrease in kidney function or macroalbuminuria); and a 27% lower risk of MACE or noncardiovascular death.
And “these effects were independent of baseline SGLT2 inhibitors, estimated glomerular filtration rate (eGFR), or metformin use,” Dr. Sattar pointed out.
New and important findings, but Sanofi no longer developing drug
The trial’s primary investigator, Hertzel C. Gerstein, MD, pointed out several new and important findings of the drug and study, compared with CVOTs of seven other GLP-1 receptor agonists.
The trial included more patients (32%) with renal disease (eGFR, 25-60 mL/min) than the other trials.
There were enough patients taking SGLT2 inhibitors at baseline (15%) to show no difference in the effect of a GLP-1 receptor agonist in the presence/absence of an SGLT2 inhibitor.
So this is the first clearly positive GLP-1 receptor agonist CVOT with an exendin-4–based GLP-1 receptor agonist showing that the GLP-1 receptor agonist class is cardioprotective whether or not it is based on a human or animal GLP-1 structure.
And there was a significant reduction in MACE or noncardiovascular death.
“This would be good for people with type 2 diabetes and either cardiovascular or renal disease at high risk for cardiovascular and/or renal outcomes,” said Dr. Gerstein, professor of medicine at McMaster University, Hamilton, Ont.
However, the trial sponsor, Sanofi, is no longer developing the drug. The company returned the rights back to Hanmi, which had started this line of research. “Hopefully” Hanmi or another company will develop the drug further, said Dr. Gerstein.
Sicker patients than in 7 other GLP-1 agonist CVOTs
Efpeglenatide – like two other drugs in the class, exenatide and lixisenatide – is an exendin-based GLP-1 agonist. (Exendin-4 is a peptide found in the saliva of the Gila monster lizard.) In contrast, liraglutide, dulaglutide, albiglutide, and semaglutide are human-analog GLP-1 agonists.
A meta-analysis of the seven CVOTs of these other drugs in this class reported, among other things, that “overall, GLP-1 agonist treatment reduced MACE by 12%.”
Amanda I. Adler, MD, PhD, professor of diabetic medicine and health policy, University of Oxford, (England), and the assigned independent commenter at the symposium, cited many things “the investigators did well.”
Compared with the CVOTs of the other GLP-1 receptor agonists – ELIXA (lixisenatide), LEADER (liraglutide), SUSTAIN-6 (semaglutide), EXSCEL (exenatide), Harmony Outcomes (albiglutide), REWIND (dulaglutide), and PIONEER 6 (oral semaglutide) – patients in the AMPLITUDE-O trial were sicker, she noted.
AMPLITUDE-O participants had the longest duration of diabetes (15 years), lowest mean eGFR of 72 ml/min per 1.73 m2, highest A1c (8.9%), and highest percentage of insulin use (62%), she noted.
The study was primarily a safety and noninferiority trial, she pointed out, although a series of superiority analyses were prespecified that would be conducted if the drug was found to be noninferior to placebo for the primary outcome of 3-point MACE.
It was good that patients were stratified according to SGLT2 inhibitor use – into current user, likely future user, and not likely future user – although “likely future user” may have misclassified some patients.
The various stakeholders – patients, regulators, doctors, payers, statisticians, and the marketing department of any company providing the drug – would want to know more, such as quality of life, long-term effects, and cost, she observed.
Meta-analysis of 8 CVOTs shows stronger class benefit
Dr. Sattar presented an eight-trial meta-analysis (an update of the seven-trial meta-analysis that included data from AMPLITUDE-O), which showed patients with type 2 diabetes who received GLP-1 agonists had a decreased rate of the 3-component MACE and decreased individual components (stroke more so than MI) – regardless of the structure of these drugs (exenatide or human analogs).
The updated meta-analysis also showed that, overall, GLP-1 agonists decreased all-cause mortality and possibly reduced the risk of heart failure hospitalization (perhaps linked to atherosclerotic benefits) as well as renal dysfunction.
There was no increase in risk of severe hypoglycemia, retinopathy, or pancreatic adverse effects.
AMPLITUDE-O: Design and findings
AMPLITUDE-O included 4,076 adults with type 2 diabetes from 344 sites in 28 countries who were screened from May 2018 to April 2019. Participants also had cardiovascular disease or kidney disease (eGFR, 25-60 mL/min) plus at least one other cardiovascular risk factor. They were randomized 1:1:1 to receive subcutaneous efpeglenatide (4 or 6 mg/week) or placebo.
Patients were a mean age of 65, most (87%) were White, and 33% were female. They had a mean A1c of 8.9%. Most (90%) had a history of cardiovascular disease and 31% had current kidney disease.
MACE occurred in 189 participants (7.0%) assigned to efpeglenatide and 125 participants (9.2%) assigned to receive placebo (3.9 vs. 5.3 events/100 person-years) (hazard ratio, 0.73; 95% confidence interval, 0.58-0.92; P < .001 for noninferiority; P = .007 for superiority).
The composite renal outcome event (decreased kidney function or macroalbuminuria) occurred in 353 participants (13.0%) assigned to receive efpeglenatide and in 250 participants (18.4%) assigned to receive placebo (HR, 0.68; 95% CI, 0.57-0.79; P < .001).
Diarrhea, constipation, nausea, vomiting, or bloating occurred more frequently with efpeglenatide than placebo.
The study was funded by Sanofi. Dr. Sattar has reported being on advisory panels for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi, and receiving research support from Boehringer Ingelheim. Dr. Gerstein has reported being a member of advisory panels for Novo Nordisk, Pfizer, and Sanofi, and a consultant for Abbott, Covance, Eli Lilly, Kowa, and Sanofi. He reported receiving research support from AstraZeneca, Eli Lilly, Merck, Novo Nordisk, and Sanofi, and having other relationships with Boehringer Ingelheim, DKSH, Eli Lilly, Sanofi, and Zuellig Pharma. Dr. Adler has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Semaglutide 2.4 mg ‘likely to usher in a new era’ in obesity treatment
The recently licensed weight-loss drug semaglutide 2.4 mg/week (Wegovy, Novo Nordisk) “is likely to usher in a new era in the medical treatment of obesity,” Lee M. Kaplan, MD, PhD, stated at the annual scientific sessions of the American Diabetes Association, held virtually.

Dr. Kaplan discussed the clinical implications of caring for patients with obesity now that the glucagon-like peptide-1 (GLP-1) receptor agonist is approved in the United States for weight loss.
Weight loss with semaglutide 2.4 mg was twice that achieved with liraglutide 3 mg (Saxenda, Novo Nordisk) – that is, roughly a 10%-15% weight loss at 68 weeks, said Dr. Kaplan, who was not involved in the pivotal STEP clinical trials of the agent.
“I think as we start to see more data come in over the next couple of years,” including from the cardiovascular outcome trial SELECT, he continued, “we’ll be able to use the data to create a nuanced [individualized patient treatment] approach, but we’ll also be able to use our clinical experience, which will grow rapidly over the next few years.”
In the future, semaglutide is likely to be combined with other drugs to provide even greater weight loss, predicts Dr. Kaplan, director of the Obesity, Metabolism, and Nutrition Institute at Massachusetts General Hospital in Boston.
In the meantime, “to be effective, semaglutide needs to be used,” he stressed, while noting that responses to the drug vary by individual, and so this will need to be taken into account.
“Obesity needs to be recognized as a disease in its own right, as well as a risk factor for numerous other diseases, [and] equitable access to obesity treatment needs to be broadened,” he emphasized.
Four pivotal phase 3 trials
As previously reported, four pivotal 68-week, phase 3 clinical trials in the Semaglutide Treatment Effect in People With Obesity (STEP) program tested the safety and efficacy of subcutaneous semaglutide 2.4 mg/week in more than 4,500 adults with overweight or obesity.
The trials have been published in high profile journals – the New England Journal of Medicine (STEP 1), The Lancet (STEP 2), and JAMA (STEP 3 and STEP 4) – said Robert F. Kushner, MD.
“I would encourage all of you to download and read each of these trials on your own,” Dr. Kushner, professor of medicine and medicine education at Northwestern University, Chicago, and coauthor of STEP 1, said before presenting a top-level review of key results.
STEP 1 examined weight management, STEP 3 added a background of intensive behavioral therapy, STEP 4 investigated sustained weight management, and STEP 2 (unlike the others) investigated weight management in patients with type 2 diabetes, he summarized.
In STEP 1, patients who received semaglutide had an average 15% weight loss, and those who stayed on the drug had a 17% weight loss, compared with the 2.4% weight loss in the placebo group.
“One-third of individuals in the trial achieved at least a 20% weight loss or more,” Dr. Kushner said, which is “really phenomenal.”
The results of STEP 3 “suggest that semaglutide with monthly brief lifestyle counseling alone is sufficient to produce a mean weight loss of 15%,” he noted, as adding a low-calorie diet and intensive behavior therapy sped up the initial weight loss but did not increase the final weight loss.
A post hoc analysis of STEP 2 showed “it’s clear that improvement in A1c” is greater with at least a 10% weight loss versus a smaller weight loss, Dr. Kushner said. A1c dropped by 2.2% versus 1.3%, with these two weight losses, respectively.
In STEP 4, after dose escalation to 2.4 mg at 20 weeks, patients had lost 10.6% of their initial weight. At 68 weeks, those who were switched to placebo at 20 weeks had lost 5.4% of their initial weight, whereas those who remained on semaglutide had lost 17.7% of their initial weight.
This shows that “if you remove the drug, the disease starts to come back,” Dr. Kushner pointed out.
Nausea, the most common side effect, occurred in 20% of patients, but was mostly mild or moderate, and gastrointestinal effects including constipation, vomiting, and diarrhea were transient and occurred early in the dose escalation phase.
Large individual variability, combination therapies on horizon
Dr. Kaplan pointed out, however, that “like [with] other antiobesity therapies ... there’s a large patient-to-patient variability.”
A third of patients exhibit more than 20% weight loss, and 10% exhibit more than 30% weight loss – approaching the efficacy of bariatric surgery.
However, nearly 10% of patients without diabetes and upwards of 30% of patients with diabetes will experience less than 5% weight loss, he said.
Therefore, “success or failure in one patient doesn’t predict response in another, and we should always remember that as we treat different patients with these medications,” Dr. Kaplan advised.
A recent phase 1b study suggests that combination therapy with semaglutide and the amylin agonist cagrilintide ups weight loss, as previously reported.
In this short trial with no lifestyle modification, it took 16 weeks for patients to reach full dosing, and at 20 weeks, patients on semaglutide had lost 8% of their initial weight, whereas those on combination therapy had lost 17% of their initial weight.
“There’s hope that, in combination with cagrilintide and probably with several other agents that are still in early development, we’ll be seeing average weight loss that is in the range of that seen with bariatric surgery,” Dr. Kushner said.
Doctors discuss two hypothetical cases
Session moderator Julio Rosenstock, MD, of the University of Texas, Dallas, a coinvestigator in several of the STEP trials, invited Dr. Kaplan and two other panelists to explain how they would manage two hypothetical patients.
Case 1
You have a patient with type 2 diabetes, a body mass index of 32, 33 kg/m2, and an A1c of 7.5% or 8% on metformin. Would you use semaglutide 1 mg (Ozempic, Novo Nordisk) that is indicated for type 2 diabetes, or would you use semaglutide 2.4 mg that is indicated for obesity and risk factors?
“We have the answer to that from STEP 2,” said Melanie J. Davies, MB ChB, MD, professor of diabetes medicine at the University of Leicester, England, who led the STEP 2 trial.

“For some patients, the 1-mg dose, which we use routinely in the clinic, may be reasonable to get good glycemic control for cardiovascular protection and will obviously achieve some weight loss. But if you really want to go for the weight-related comorbidities, then the 2.4-mg dose is what you need,” she said.
“A lot of [clinicians] might say: ‘I’ll see how [the patient goes] with the 1-mg dose, and then maybe if they’re not losing the weight and not getting to glycemic target, then maybe I’ll switch to 2.4 mg,’” said John Wilding, MD, who leads clinical research into obesity, diabetes, and endocrinology at the University of Liverpool, England, and led the STEP 1 trial.
“But the STEP 2 data show very clearly that you get almost the same A1c,” Dr. Rosenstock interjected. “I would go for 2.4 mg. The patient has a BMI of 32, 33 kg/m2. I would hit hard the BMI. We need to change that paradigm.”
“For other diseases we don’t always go to the maximum dose that’s available. We go to the dose that’s necessary to achieve the clinical endpoint that we want,” Dr. Kaplan noted. “I think one of the challenges is going to be to learn how to clinically nuance our therapy the way we do for other diseases.”
“That is the usual thinking,” Dr. Rosenstock agreed. But “with the 2.4-mg dose, one third get a 20% reduction of BMI, and 10% get almost a 30% reduction – and you [aren’t] going to see that with semaglutide 1 mg!”
“That’s true,” Dr. Kaplan conceded. However, a patient with a relatively low BMI of 32, 33 kg/m2 may not need the higher dose, unlike a patient who has a BMI of 45 kg/m2 and diabetes. But we’re going to find that out over the next couple of years, he expects.
Case 2
You have a patient with a BMI of 31 kg/m2 who is newly diagnosed with type 2 diabetes. Why should you start that patient with metformin? Why won’t you start with something that will directly tackle obesity and get the patient to lose 20 pounds and for sure the blood sugar is going to be better?
“I think if I have someone who is really keen to put their diabetes into remission,” Dr. Wilding said, “this would be a fantastic approach because they would have a really high chance of doing that.”
The prediabetes data from STEP showed that “we can put a lot of people from prediabetes back to normal glucose tolerance,” Dr. Wilding noted. “Maybe we can put people with early diabetes back to normal as well. I think that’s a trial that really does need to be done,” he said.
“We’re going to have to figure out the best pathway forward,” Dr. Kaplan observed, noting that multiple stakeholders, including payers, patients, and providers, play a role in the uptake of new obesity drugs.
“Do you think we will see less bariatric surgery with these drugs?” Dr. Rosenstock asked Dr. Kaplan.
“I think you have to remember that of the millions and millions of people with obesity, a very small portion are currently treated with antiobesity medication, and an even smaller portion are getting bariatric surgery,” Dr. Kaplan replied.
“In the United States, 90% of people who get bariatric surgery are self-referred,” he said, so, “I think initially we are not going to see much of a change” in rates of bariatric surgery.
Dr. Rosenstock, Dr. Kaplan, Dr. Wilding, and Dr. Davies disclosed ties with Novo Nordisk and numerous other companies.
A version of this article first appeared on Medscape.com.
The recently licensed weight-loss drug semaglutide 2.4 mg/week (Wegovy, Novo Nordisk) “is likely to usher in a new era in the medical treatment of obesity,” Lee M. Kaplan, MD, PhD, stated at the annual scientific sessions of the American Diabetes Association, held virtually.
Dr. Kaplan discussed the clinical implications of caring for patients with obesity now that the glucagon-like peptide-1 (GLP-1) receptor agonist is approved in the United States for weight loss.
Weight loss with semaglutide 2.4 mg was twice that achieved with liraglutide 3 mg (Saxenda, Novo Nordisk) – that is, roughly a 10%-15% weight loss at 68 weeks, said Dr. Kaplan, who was not involved in the pivotal STEP clinical trials of the agent.
“I think as we start to see more data come in over the next couple of years,” including from the cardiovascular outcome trial SELECT, he continued, “we’ll be able to use the data to create a nuanced [individualized patient treatment] approach, but we’ll also be able to use our clinical experience, which will grow rapidly over the next few years.”
In the future, semaglutide is likely to be combined with other drugs to provide even greater weight loss, predicts Dr. Kaplan, director of the Obesity, Metabolism, and Nutrition Institute at Massachusetts General Hospital in Boston.
In the meantime, “to be effective, semaglutide needs to be used,” he stressed, while noting that responses to the drug vary by individual, and so this will need to be taken into account.
“Obesity needs to be recognized as a disease in its own right, as well as a risk factor for numerous other diseases, [and] equitable access to obesity treatment needs to be broadened,” he emphasized.
Four pivotal phase 3 trials
As previously reported, four pivotal 68-week, phase 3 clinical trials in the Semaglutide Treatment Effect in People With Obesity (STEP) program tested the safety and efficacy of subcutaneous semaglutide 2.4 mg/week in more than 4,500 adults with overweight or obesity.
The trials have been published in high profile journals – the New England Journal of Medicine (STEP 1), The Lancet (STEP 2), and JAMA (STEP 3 and STEP 4) – said Robert F. Kushner, MD.
“I would encourage all of you to download and read each of these trials on your own,” Dr. Kushner, professor of medicine and medicine education at Northwestern University, Chicago, and coauthor of STEP 1, said before presenting a top-level review of key results.
STEP 1 examined weight management, STEP 3 added a background of intensive behavioral therapy, STEP 4 investigated sustained weight management, and STEP 2 (unlike the others) investigated weight management in patients with type 2 diabetes, he summarized.
In STEP 1, patients who received semaglutide had an average 15% weight loss, and those who stayed on the drug had a 17% weight loss, compared with the 2.4% weight loss in the placebo group.
“One-third of individuals in the trial achieved at least a 20% weight loss or more,” Dr. Kushner said, which is “really phenomenal.”
The results of STEP 3 “suggest that semaglutide with monthly brief lifestyle counseling alone is sufficient to produce a mean weight loss of 15%,” he noted, as adding a low-calorie diet and intensive behavior therapy sped up the initial weight loss but did not increase the final weight loss.
A post hoc analysis of STEP 2 showed “it’s clear that improvement in A1c” is greater with at least a 10% weight loss versus a smaller weight loss, Dr. Kushner said. A1c dropped by 2.2% versus 1.3%, with these two weight losses, respectively.
In STEP 4, after dose escalation to 2.4 mg at 20 weeks, patients had lost 10.6% of their initial weight. At 68 weeks, those who were switched to placebo at 20 weeks had lost 5.4% of their initial weight, whereas those who remained on semaglutide had lost 17.7% of their initial weight.
This shows that “if you remove the drug, the disease starts to come back,” Dr. Kushner pointed out.
Nausea, the most common side effect, occurred in 20% of patients, but was mostly mild or moderate, and gastrointestinal effects including constipation, vomiting, and diarrhea were transient and occurred early in the dose escalation phase.
Large individual variability, combination therapies on horizon
Dr. Kaplan pointed out, however, that “like [with] other antiobesity therapies ... there’s a large patient-to-patient variability.”
A third of patients exhibit more than 20% weight loss, and 10% exhibit more than 30% weight loss – approaching the efficacy of bariatric surgery.
However, nearly 10% of patients without diabetes and upwards of 30% of patients with diabetes will experience less than 5% weight loss, he said.
Therefore, “success or failure in one patient doesn’t predict response in another, and we should always remember that as we treat different patients with these medications,” Dr. Kaplan advised.
A recent phase 1b study suggests that combination therapy with semaglutide and the amylin agonist cagrilintide ups weight loss, as previously reported.
In this short trial with no lifestyle modification, it took 16 weeks for patients to reach full dosing, and at 20 weeks, patients on semaglutide had lost 8% of their initial weight, whereas those on combination therapy had lost 17% of their initial weight.
“There’s hope that, in combination with cagrilintide and probably with several other agents that are still in early development, we’ll be seeing average weight loss that is in the range of that seen with bariatric surgery,” Dr. Kushner said.
Doctors discuss two hypothetical cases
Session moderator Julio Rosenstock, MD, of the University of Texas, Dallas, a coinvestigator in several of the STEP trials, invited Dr. Kaplan and two other panelists to explain how they would manage two hypothetical patients.
Case 1
You have a patient with type 2 diabetes, a body mass index of 32, 33 kg/m2, and an A1c of 7.5% or 8% on metformin. Would you use semaglutide 1 mg (Ozempic, Novo Nordisk) that is indicated for type 2 diabetes, or would you use semaglutide 2.4 mg that is indicated for obesity and risk factors?
“We have the answer to that from STEP 2,” said Melanie J. Davies, MB ChB, MD, professor of diabetes medicine at the University of Leicester, England, who led the STEP 2 trial.
“For some patients, the 1-mg dose, which we use routinely in the clinic, may be reasonable to get good glycemic control for cardiovascular protection and will obviously achieve some weight loss. But if you really want to go for the weight-related comorbidities, then the 2.4-mg dose is what you need,” she said.
“A lot of [clinicians] might say: ‘I’ll see how [the patient goes] with the 1-mg dose, and then maybe if they’re not losing the weight and not getting to glycemic target, then maybe I’ll switch to 2.4 mg,’” said John Wilding, MD, who leads clinical research into obesity, diabetes, and endocrinology at the University of Liverpool, England, and led the STEP 1 trial.
“But the STEP 2 data show very clearly that you get almost the same A1c,” Dr. Rosenstock interjected. “I would go for 2.4 mg. The patient has a BMI of 32, 33 kg/m2. I would hit hard the BMI. We need to change that paradigm.”
“For other diseases we don’t always go to the maximum dose that’s available. We go to the dose that’s necessary to achieve the clinical endpoint that we want,” Dr. Kaplan noted. “I think one of the challenges is going to be to learn how to clinically nuance our therapy the way we do for other diseases.”
“That is the usual thinking,” Dr. Rosenstock agreed. But “with the 2.4-mg dose, one third get a 20% reduction of BMI, and 10% get almost a 30% reduction – and you [aren’t] going to see that with semaglutide 1 mg!”
“That’s true,” Dr. Kaplan conceded. However, a patient with a relatively low BMI of 32, 33 kg/m2 may not need the higher dose, unlike a patient who has a BMI of 45 kg/m2 and diabetes. But we’re going to find that out over the next couple of years, he expects.
Case 2
You have a patient with a BMI of 31 kg/m2 who is newly diagnosed with type 2 diabetes. Why should you start that patient with metformin? Why won’t you start with something that will directly tackle obesity and get the patient to lose 20 pounds and for sure the blood sugar is going to be better?
“I think if I have someone who is really keen to put their diabetes into remission,” Dr. Wilding said, “this would be a fantastic approach because they would have a really high chance of doing that.”
The prediabetes data from STEP showed that “we can put a lot of people from prediabetes back to normal glucose tolerance,” Dr. Wilding noted. “Maybe we can put people with early diabetes back to normal as well. I think that’s a trial that really does need to be done,” he said.
“We’re going to have to figure out the best pathway forward,” Dr. Kaplan observed, noting that multiple stakeholders, including payers, patients, and providers, play a role in the uptake of new obesity drugs.
“Do you think we will see less bariatric surgery with these drugs?” Dr. Rosenstock asked Dr. Kaplan.
“I think you have to remember that of the millions and millions of people with obesity, a very small portion are currently treated with antiobesity medication, and an even smaller portion are getting bariatric surgery,” Dr. Kaplan replied.
“In the United States, 90% of people who get bariatric surgery are self-referred,” he said, so, “I think initially we are not going to see much of a change” in rates of bariatric surgery.
Dr. Rosenstock, Dr. Kaplan, Dr. Wilding, and Dr. Davies disclosed ties with Novo Nordisk and numerous other companies.
A version of this article first appeared on Medscape.com.
The recently licensed weight-loss drug semaglutide 2.4 mg/week (Wegovy, Novo Nordisk) “is likely to usher in a new era in the medical treatment of obesity,” Lee M. Kaplan, MD, PhD, stated at the annual scientific sessions of the American Diabetes Association, held virtually.
Dr. Kaplan discussed the clinical implications of caring for patients with obesity now that the glucagon-like peptide-1 (GLP-1) receptor agonist is approved in the United States for weight loss.
Weight loss with semaglutide 2.4 mg was twice that achieved with liraglutide 3 mg (Saxenda, Novo Nordisk) – that is, roughly a 10%-15% weight loss at 68 weeks, said Dr. Kaplan, who was not involved in the pivotal STEP clinical trials of the agent.
“I think as we start to see more data come in over the next couple of years,” including from the cardiovascular outcome trial SELECT, he continued, “we’ll be able to use the data to create a nuanced [individualized patient treatment] approach, but we’ll also be able to use our clinical experience, which will grow rapidly over the next few years.”
In the future, semaglutide is likely to be combined with other drugs to provide even greater weight loss, predicts Dr. Kaplan, director of the Obesity, Metabolism, and Nutrition Institute at Massachusetts General Hospital in Boston.
In the meantime, “to be effective, semaglutide needs to be used,” he stressed, while noting that responses to the drug vary by individual, and so this will need to be taken into account.
“Obesity needs to be recognized as a disease in its own right, as well as a risk factor for numerous other diseases, [and] equitable access to obesity treatment needs to be broadened,” he emphasized.
Four pivotal phase 3 trials
As previously reported, four pivotal 68-week, phase 3 clinical trials in the Semaglutide Treatment Effect in People With Obesity (STEP) program tested the safety and efficacy of subcutaneous semaglutide 2.4 mg/week in more than 4,500 adults with overweight or obesity.
The trials have been published in high profile journals – the New England Journal of Medicine (STEP 1), The Lancet (STEP 2), and JAMA (STEP 3 and STEP 4) – said Robert F. Kushner, MD.
“I would encourage all of you to download and read each of these trials on your own,” Dr. Kushner, professor of medicine and medicine education at Northwestern University, Chicago, and coauthor of STEP 1, said before presenting a top-level review of key results.
STEP 1 examined weight management, STEP 3 added a background of intensive behavioral therapy, STEP 4 investigated sustained weight management, and STEP 2 (unlike the others) investigated weight management in patients with type 2 diabetes, he summarized.
In STEP 1, patients who received semaglutide had an average 15% weight loss, and those who stayed on the drug had a 17% weight loss, compared with the 2.4% weight loss in the placebo group.
“One-third of individuals in the trial achieved at least a 20% weight loss or more,” Dr. Kushner said, which is “really phenomenal.”
The results of STEP 3 “suggest that semaglutide with monthly brief lifestyle counseling alone is sufficient to produce a mean weight loss of 15%,” he noted, as adding a low-calorie diet and intensive behavior therapy sped up the initial weight loss but did not increase the final weight loss.
A post hoc analysis of STEP 2 showed “it’s clear that improvement in A1c” is greater with at least a 10% weight loss versus a smaller weight loss, Dr. Kushner said. A1c dropped by 2.2% versus 1.3%, with these two weight losses, respectively.
In STEP 4, after dose escalation to 2.4 mg at 20 weeks, patients had lost 10.6% of their initial weight. At 68 weeks, those who were switched to placebo at 20 weeks had lost 5.4% of their initial weight, whereas those who remained on semaglutide had lost 17.7% of their initial weight.
This shows that “if you remove the drug, the disease starts to come back,” Dr. Kushner pointed out.
Nausea, the most common side effect, occurred in 20% of patients, but was mostly mild or moderate, and gastrointestinal effects including constipation, vomiting, and diarrhea were transient and occurred early in the dose escalation phase.
Large individual variability, combination therapies on horizon
Dr. Kaplan pointed out, however, that “like [with] other antiobesity therapies ... there’s a large patient-to-patient variability.”
A third of patients exhibit more than 20% weight loss, and 10% exhibit more than 30% weight loss – approaching the efficacy of bariatric surgery.
However, nearly 10% of patients without diabetes and upwards of 30% of patients with diabetes will experience less than 5% weight loss, he said.
Therefore, “success or failure in one patient doesn’t predict response in another, and we should always remember that as we treat different patients with these medications,” Dr. Kaplan advised.
A recent phase 1b study suggests that combination therapy with semaglutide and the amylin agonist cagrilintide ups weight loss, as previously reported.
In this short trial with no lifestyle modification, it took 16 weeks for patients to reach full dosing, and at 20 weeks, patients on semaglutide had lost 8% of their initial weight, whereas those on combination therapy had lost 17% of their initial weight.
“There’s hope that, in combination with cagrilintide and probably with several other agents that are still in early development, we’ll be seeing average weight loss that is in the range of that seen with bariatric surgery,” Dr. Kushner said.
Doctors discuss two hypothetical cases
Session moderator Julio Rosenstock, MD, of the University of Texas, Dallas, a coinvestigator in several of the STEP trials, invited Dr. Kaplan and two other panelists to explain how they would manage two hypothetical patients.
Case 1
You have a patient with type 2 diabetes, a body mass index of 32, 33 kg/m2, and an A1c of 7.5% or 8% on metformin. Would you use semaglutide 1 mg (Ozempic, Novo Nordisk) that is indicated for type 2 diabetes, or would you use semaglutide 2.4 mg that is indicated for obesity and risk factors?
“We have the answer to that from STEP 2,” said Melanie J. Davies, MB ChB, MD, professor of diabetes medicine at the University of Leicester, England, who led the STEP 2 trial.
“For some patients, the 1-mg dose, which we use routinely in the clinic, may be reasonable to get good glycemic control for cardiovascular protection and will obviously achieve some weight loss. But if you really want to go for the weight-related comorbidities, then the 2.4-mg dose is what you need,” she said.
“A lot of [clinicians] might say: ‘I’ll see how [the patient goes] with the 1-mg dose, and then maybe if they’re not losing the weight and not getting to glycemic target, then maybe I’ll switch to 2.4 mg,’” said John Wilding, MD, who leads clinical research into obesity, diabetes, and endocrinology at the University of Liverpool, England, and led the STEP 1 trial.
“But the STEP 2 data show very clearly that you get almost the same A1c,” Dr. Rosenstock interjected. “I would go for 2.4 mg. The patient has a BMI of 32, 33 kg/m2. I would hit hard the BMI. We need to change that paradigm.”
“For other diseases we don’t always go to the maximum dose that’s available. We go to the dose that’s necessary to achieve the clinical endpoint that we want,” Dr. Kaplan noted. “I think one of the challenges is going to be to learn how to clinically nuance our therapy the way we do for other diseases.”
“That is the usual thinking,” Dr. Rosenstock agreed. But “with the 2.4-mg dose, one third get a 20% reduction of BMI, and 10% get almost a 30% reduction – and you [aren’t] going to see that with semaglutide 1 mg!”
“That’s true,” Dr. Kaplan conceded. However, a patient with a relatively low BMI of 32, 33 kg/m2 may not need the higher dose, unlike a patient who has a BMI of 45 kg/m2 and diabetes. But we’re going to find that out over the next couple of years, he expects.
Case 2
You have a patient with a BMI of 31 kg/m2 who is newly diagnosed with type 2 diabetes. Why should you start that patient with metformin? Why won’t you start with something that will directly tackle obesity and get the patient to lose 20 pounds and for sure the blood sugar is going to be better?
“I think if I have someone who is really keen to put their diabetes into remission,” Dr. Wilding said, “this would be a fantastic approach because they would have a really high chance of doing that.”
The prediabetes data from STEP showed that “we can put a lot of people from prediabetes back to normal glucose tolerance,” Dr. Wilding noted. “Maybe we can put people with early diabetes back to normal as well. I think that’s a trial that really does need to be done,” he said.
“We’re going to have to figure out the best pathway forward,” Dr. Kaplan observed, noting that multiple stakeholders, including payers, patients, and providers, play a role in the uptake of new obesity drugs.
“Do you think we will see less bariatric surgery with these drugs?” Dr. Rosenstock asked Dr. Kaplan.
“I think you have to remember that of the millions and millions of people with obesity, a very small portion are currently treated with antiobesity medication, and an even smaller portion are getting bariatric surgery,” Dr. Kaplan replied.
“In the United States, 90% of people who get bariatric surgery are self-referred,” he said, so, “I think initially we are not going to see much of a change” in rates of bariatric surgery.
Dr. Rosenstock, Dr. Kaplan, Dr. Wilding, and Dr. Davies disclosed ties with Novo Nordisk and numerous other companies.
A version of this article first appeared on Medscape.com.
Maintain OMT for 5 years after revascularization, boost survival at 10 years: SYNTAXES
When it comes to medical therapy after a coronary revascularization procedure, more is better. Patients started and then maintained indefinitely on more rather than fewer of the drugs identified as optimal medical therapy (OMT) achieve a major survival benefit 10 years later, according to long-term follow-up from an extended analysis of the SYNTAX trial.

For the survival benefit at 10 years, “the present study suggests that at least three types of optimal medical therapy should be maintained for at least 5 years after revascularization,” reported a multinational team of cardiovascular specialists led by Hideyuki Kawashima, MD and Patrick Serruys, MD, who both have affiliations with the department of cardiology of the National University of Ireland, Galway.
The SYNTAX trial was conducted to compare percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) for patients with previously untreated three-vessel and/or left main disease (N Engl J Med 2009;360:961-72). The conclusion from that study, published in 2009 and subsequently reinforced by a 5-year follow-up, was that CABG should remain the standard of care for complex lesions.
Optimal medical therapy defined
In the course of SYNTAX, the impact of OMT on outcome was also evaluated in a subanalysis. At 5 years, there was a mortality advantage for those receiving an antiplatelet drug, a statin, a renin-angiotensin system inhibitor (ACE inhibitor or angiotensin receptor blocker), and a beta-blocker when compared with fewer of these agents.
When an investigator-initiated extension of SYNTAX, called SYNTAXES, was conducted to compare the outcomes of PCI and CABG at 10 years, it also permitted an extended analysis of OMT. Although the primary comparison of SYNTAXES, reported 2 years ago, did not show a significant difference between PCI and CABG for mortality at 10 years, there was a difference for OMT.
When investigators compared treatment with three or more OMT agents with that with two or fewer OMT drugs at 5 years, the result for all-cause death at 10 years translated into a more than 50% relative reduction (hazard ratio, 0.47; P = .002). The absolute difference in mortality was a more than 6% reduction (13.1% vs. 19.9%).
OMT data offer major message
The current study is considered to have a major message for patients as well as physicians.
“OMT even outweighs the survival benefit from revascularization alone, so our patients should convince themselves of the value of rigorous adherence and compliance,” Dr. Serruys said in an interview. According to him, these are compelling data for telling patients that OMT “is the best insurance for extended survival.” We now know from these data “the longer, the better.”
The same message from these data extends to physicians.
“I wish I could understand the apparent blind spot physicians have with respect to prescribing OMT despite the overwhelming benefit from multiple clinical trials,” said William E. Boden, MD, professor of medicine, Boston University.
Dr. Boden was a coauthor of an editorial accompanying the newly published SYNTAXES subanalysis. In the editorial, he noted that OMT following revascularization and in other high-risk patients “has been unacceptably low,” but he was asked to expand on the lessons from the newly released SYNTAXES subanalysis in an interview.
“There has often been a belief that revascularization negates the need for OMT and that’s why the SYNTAXES trial 10-year mortality reduction – which builds upon an earlier 5-year mortality reduction analysis – is so important,” he said.
Patients should take OMT long term
These data “should be both a motivator for physicians to prescribe OMT and for patients to remain adherent to OMT,” he said. “It is the best warranty to blunt the progression of atherosclerosis and to reduce subsequent cardiac events.”
For the 10-year subanalysis of OMT in SYNTAXES, the patients were stratified by the number of OMTs they were taking at 5 years after revascularization and then evaluated for survival at 10 years. Of the 1,472 patients available for analysis at 5 years, only 678 (46%) were on OMT. The other 794 patients were not.
Graphically, the Kaplan-Meier survival curve for those on three types of OMT was consistently beneath that of those on four OMTs, but the gap narrowed over time. At the end of 10 years, the advantage of the four-drug OMT was not statistically significant relative to three or fewer (13.1% vs. 12.7%).
Statins and antiplatelets show largest effect
When analyzed individually and in different combinations, the agents with OMT did not appear to be equal. For example, the biggest survival gap at 10 years was for those who were on an antiplatelet therapy and a statin at 5 years relative to those who were not on either (13.2% vs. 22.6%; P = .006). Even after adjustment, there was nearly 45% survival benefit for these two agents (HR, 0.556; P = .02).
Conversely, the 10-year survival advantage for being on a renin-angiotensin system inhibitor at 5 years versus not being exposed to this therapy was small and nonsignificant (14.7% vs. 13.7%; P = .651).
The precise proportion of patients who were prescribed and adhered to OMT between 5 years and 10 years is unknown, acknowledged the authors, so conclusions are limited about the added benefit of 10- versus 5-year OMT, although the authors presume that a substantial proportion of those adherent for 5 years would likely continue on these therapies.
It can be said with confidence that those adherent for at least 5 years are more likely to be alive at 10 years than those who are not, according to Dr. Boden. He considers these data a call for physicians and all high-risk patients, not just those who have undergone revascularization, to take these standard therapies.
There are plenty of data to “show how poorly we treat patients with OMT,” said Dr. Boden, citing several studies. In one, which looked at OMT in a nationally representative sample in the United States, only a third of patients with angina were taking an antiplatelet, a statin, and a beta-blocker, all of which are indicated.
“Hospitalization for revascularization provides an opportune time to capture the attention of patients and their physicians,” he wrote in his editorial. He called OMT “an imperative to optimize clinical outcomes.”
Many of the investigators involved in the SYNTAXES subanalysis, including Dr. Serruys, have financial relationships with multiple pharmaceutical companies, including Boston Scientific, which provided the initial funding for the SYNTAX trial. Dr. Boden reports no potential conflicts of interest.
When it comes to medical therapy after a coronary revascularization procedure, more is better. Patients started and then maintained indefinitely on more rather than fewer of the drugs identified as optimal medical therapy (OMT) achieve a major survival benefit 10 years later, according to long-term follow-up from an extended analysis of the SYNTAX trial.
For the survival benefit at 10 years, “the present study suggests that at least three types of optimal medical therapy should be maintained for at least 5 years after revascularization,” reported a multinational team of cardiovascular specialists led by Hideyuki Kawashima, MD and Patrick Serruys, MD, who both have affiliations with the department of cardiology of the National University of Ireland, Galway.
The SYNTAX trial was conducted to compare percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) for patients with previously untreated three-vessel and/or left main disease (N Engl J Med 2009;360:961-72). The conclusion from that study, published in 2009 and subsequently reinforced by a 5-year follow-up, was that CABG should remain the standard of care for complex lesions.
Optimal medical therapy defined
In the course of SYNTAX, the impact of OMT on outcome was also evaluated in a subanalysis. At 5 years, there was a mortality advantage for those receiving an antiplatelet drug, a statin, a renin-angiotensin system inhibitor (ACE inhibitor or angiotensin receptor blocker), and a beta-blocker when compared with fewer of these agents.
When an investigator-initiated extension of SYNTAX, called SYNTAXES, was conducted to compare the outcomes of PCI and CABG at 10 years, it also permitted an extended analysis of OMT. Although the primary comparison of SYNTAXES, reported 2 years ago, did not show a significant difference between PCI and CABG for mortality at 10 years, there was a difference for OMT.
When investigators compared treatment with three or more OMT agents with that with two or fewer OMT drugs at 5 years, the result for all-cause death at 10 years translated into a more than 50% relative reduction (hazard ratio, 0.47; P = .002). The absolute difference in mortality was a more than 6% reduction (13.1% vs. 19.9%).
OMT data offer major message
The current study is considered to have a major message for patients as well as physicians.
“OMT even outweighs the survival benefit from revascularization alone, so our patients should convince themselves of the value of rigorous adherence and compliance,” Dr. Serruys said in an interview. According to him, these are compelling data for telling patients that OMT “is the best insurance for extended survival.” We now know from these data “the longer, the better.”
The same message from these data extends to physicians.
“I wish I could understand the apparent blind spot physicians have with respect to prescribing OMT despite the overwhelming benefit from multiple clinical trials,” said William E. Boden, MD, professor of medicine, Boston University.
Dr. Boden was a coauthor of an editorial accompanying the newly published SYNTAXES subanalysis. In the editorial, he noted that OMT following revascularization and in other high-risk patients “has been unacceptably low,” but he was asked to expand on the lessons from the newly released SYNTAXES subanalysis in an interview.
“There has often been a belief that revascularization negates the need for OMT and that’s why the SYNTAXES trial 10-year mortality reduction – which builds upon an earlier 5-year mortality reduction analysis – is so important,” he said.
Patients should take OMT long term
These data “should be both a motivator for physicians to prescribe OMT and for patients to remain adherent to OMT,” he said. “It is the best warranty to blunt the progression of atherosclerosis and to reduce subsequent cardiac events.”
For the 10-year subanalysis of OMT in SYNTAXES, the patients were stratified by the number of OMTs they were taking at 5 years after revascularization and then evaluated for survival at 10 years. Of the 1,472 patients available for analysis at 5 years, only 678 (46%) were on OMT. The other 794 patients were not.
Graphically, the Kaplan-Meier survival curve for those on three types of OMT was consistently beneath that of those on four OMTs, but the gap narrowed over time. At the end of 10 years, the advantage of the four-drug OMT was not statistically significant relative to three or fewer (13.1% vs. 12.7%).
Statins and antiplatelets show largest effect
When analyzed individually and in different combinations, the agents with OMT did not appear to be equal. For example, the biggest survival gap at 10 years was for those who were on an antiplatelet therapy and a statin at 5 years relative to those who were not on either (13.2% vs. 22.6%; P = .006). Even after adjustment, there was nearly 45% survival benefit for these two agents (HR, 0.556; P = .02).
Conversely, the 10-year survival advantage for being on a renin-angiotensin system inhibitor at 5 years versus not being exposed to this therapy was small and nonsignificant (14.7% vs. 13.7%; P = .651).
The precise proportion of patients who were prescribed and adhered to OMT between 5 years and 10 years is unknown, acknowledged the authors, so conclusions are limited about the added benefit of 10- versus 5-year OMT, although the authors presume that a substantial proportion of those adherent for 5 years would likely continue on these therapies.
It can be said with confidence that those adherent for at least 5 years are more likely to be alive at 10 years than those who are not, according to Dr. Boden. He considers these data a call for physicians and all high-risk patients, not just those who have undergone revascularization, to take these standard therapies.
There are plenty of data to “show how poorly we treat patients with OMT,” said Dr. Boden, citing several studies. In one, which looked at OMT in a nationally representative sample in the United States, only a third of patients with angina were taking an antiplatelet, a statin, and a beta-blocker, all of which are indicated.
“Hospitalization for revascularization provides an opportune time to capture the attention of patients and their physicians,” he wrote in his editorial. He called OMT “an imperative to optimize clinical outcomes.”
Many of the investigators involved in the SYNTAXES subanalysis, including Dr. Serruys, have financial relationships with multiple pharmaceutical companies, including Boston Scientific, which provided the initial funding for the SYNTAX trial. Dr. Boden reports no potential conflicts of interest.
When it comes to medical therapy after a coronary revascularization procedure, more is better. Patients started and then maintained indefinitely on more rather than fewer of the drugs identified as optimal medical therapy (OMT) achieve a major survival benefit 10 years later, according to long-term follow-up from an extended analysis of the SYNTAX trial.
For the survival benefit at 10 years, “the present study suggests that at least three types of optimal medical therapy should be maintained for at least 5 years after revascularization,” reported a multinational team of cardiovascular specialists led by Hideyuki Kawashima, MD and Patrick Serruys, MD, who both have affiliations with the department of cardiology of the National University of Ireland, Galway.
The SYNTAX trial was conducted to compare percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) for patients with previously untreated three-vessel and/or left main disease (N Engl J Med 2009;360:961-72). The conclusion from that study, published in 2009 and subsequently reinforced by a 5-year follow-up, was that CABG should remain the standard of care for complex lesions.
Optimal medical therapy defined
In the course of SYNTAX, the impact of OMT on outcome was also evaluated in a subanalysis. At 5 years, there was a mortality advantage for those receiving an antiplatelet drug, a statin, a renin-angiotensin system inhibitor (ACE inhibitor or angiotensin receptor blocker), and a beta-blocker when compared with fewer of these agents.
When an investigator-initiated extension of SYNTAX, called SYNTAXES, was conducted to compare the outcomes of PCI and CABG at 10 years, it also permitted an extended analysis of OMT. Although the primary comparison of SYNTAXES, reported 2 years ago, did not show a significant difference between PCI and CABG for mortality at 10 years, there was a difference for OMT.
When investigators compared treatment with three or more OMT agents with that with two or fewer OMT drugs at 5 years, the result for all-cause death at 10 years translated into a more than 50% relative reduction (hazard ratio, 0.47; P = .002). The absolute difference in mortality was a more than 6% reduction (13.1% vs. 19.9%).
OMT data offer major message
The current study is considered to have a major message for patients as well as physicians.
“OMT even outweighs the survival benefit from revascularization alone, so our patients should convince themselves of the value of rigorous adherence and compliance,” Dr. Serruys said in an interview. According to him, these are compelling data for telling patients that OMT “is the best insurance for extended survival.” We now know from these data “the longer, the better.”
The same message from these data extends to physicians.
“I wish I could understand the apparent blind spot physicians have with respect to prescribing OMT despite the overwhelming benefit from multiple clinical trials,” said William E. Boden, MD, professor of medicine, Boston University.
Dr. Boden was a coauthor of an editorial accompanying the newly published SYNTAXES subanalysis. In the editorial, he noted that OMT following revascularization and in other high-risk patients “has been unacceptably low,” but he was asked to expand on the lessons from the newly released SYNTAXES subanalysis in an interview.
“There has often been a belief that revascularization negates the need for OMT and that’s why the SYNTAXES trial 10-year mortality reduction – which builds upon an earlier 5-year mortality reduction analysis – is so important,” he said.
Patients should take OMT long term
These data “should be both a motivator for physicians to prescribe OMT and for patients to remain adherent to OMT,” he said. “It is the best warranty to blunt the progression of atherosclerosis and to reduce subsequent cardiac events.”
For the 10-year subanalysis of OMT in SYNTAXES, the patients were stratified by the number of OMTs they were taking at 5 years after revascularization and then evaluated for survival at 10 years. Of the 1,472 patients available for analysis at 5 years, only 678 (46%) were on OMT. The other 794 patients were not.
Graphically, the Kaplan-Meier survival curve for those on three types of OMT was consistently beneath that of those on four OMTs, but the gap narrowed over time. At the end of 10 years, the advantage of the four-drug OMT was not statistically significant relative to three or fewer (13.1% vs. 12.7%).
Statins and antiplatelets show largest effect
When analyzed individually and in different combinations, the agents with OMT did not appear to be equal. For example, the biggest survival gap at 10 years was for those who were on an antiplatelet therapy and a statin at 5 years relative to those who were not on either (13.2% vs. 22.6%; P = .006). Even after adjustment, there was nearly 45% survival benefit for these two agents (HR, 0.556; P = .02).
Conversely, the 10-year survival advantage for being on a renin-angiotensin system inhibitor at 5 years versus not being exposed to this therapy was small and nonsignificant (14.7% vs. 13.7%; P = .651).
The precise proportion of patients who were prescribed and adhered to OMT between 5 years and 10 years is unknown, acknowledged the authors, so conclusions are limited about the added benefit of 10- versus 5-year OMT, although the authors presume that a substantial proportion of those adherent for 5 years would likely continue on these therapies.
It can be said with confidence that those adherent for at least 5 years are more likely to be alive at 10 years than those who are not, according to Dr. Boden. He considers these data a call for physicians and all high-risk patients, not just those who have undergone revascularization, to take these standard therapies.
There are plenty of data to “show how poorly we treat patients with OMT,” said Dr. Boden, citing several studies. In one, which looked at OMT in a nationally representative sample in the United States, only a third of patients with angina were taking an antiplatelet, a statin, and a beta-blocker, all of which are indicated.
“Hospitalization for revascularization provides an opportune time to capture the attention of patients and their physicians,” he wrote in his editorial. He called OMT “an imperative to optimize clinical outcomes.”
Many of the investigators involved in the SYNTAXES subanalysis, including Dr. Serruys, have financial relationships with multiple pharmaceutical companies, including Boston Scientific, which provided the initial funding for the SYNTAX trial. Dr. Boden reports no potential conflicts of interest.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Nocturnal hypoglycemia halved with insulin degludec vs. glargine
Patients with type 1 diabetes who used insulin degludec as their basal insulin had fewer than half the number of nocturnal hypoglycemia events, compared with patients who used insulin glargine U100, in a head-to-head crossover study with 51 patients who had a history of nighttime hypoglycemia episodes.
Patients with type 1 diabetes who are “struggling with nocturnal hypoglycemia would benefit from insulin degludec treatment,” said Julie M. Brøsen, MD, at the annual scientific sessions of the American Diabetes Association.
Accumulating evidence for less hypoglycemia with insulin degludec
Results from several studies comparing insulin degludec (Tresiba), a second-generation, longer-acting insulin with more stable steady-state performance, with the first-generation basal insulin analogue glargine (Lantus), have built the case that degludec produces fewer hypoglycemia events.
The landmark SWITCH 1 crossover study published in 2017 showed in about 500 patients with type 1 diabetes and a risk factor for hypoglycemia that treatment with insulin degludec led to significantly few total hypoglycemia episodes and significantly fewer nocturnal episodes, compared with insulin glargine.
Next came similar findings from ReFLeCT, a multicenter observational study that followed 556 unselected patients with type 1 diabetes in routine practice settings who switched to insulin degludec following treatment with a different basal insulin. The results again showed a significant drop-off in total, nonsevere, severe, and nocturnal hypoglycemia events.
Homing in on higher-risk patients
The current study, HypoDeg (Insulin Degludec and Symptomatic Nocturnal Hypoglycaemia), ran at 10 Danish centers and enrolled 149 adults with type 1 diabetes who had at least one episode of severe nocturnal hypoglycemia within the prior 2 years, focusing on patients most at risk for future nocturnal hypoglycemia events. In an unusual study design, researchers identified nocturnal hypoglycemic episodes with hourly venous blood samples drawn from a subcutaneous line.
They randomized the patients to basal insulin treatment with either insulin degludec or to insulin glargine U100, allowed their treatment to stabilize for 3 months, and then tallied nocturnal hypoglycemia events for 9 months. They then crossed patients to the alternative basal insulin and repeated the process.
Results from the full study have not yet appeared in published form but were in a pair of reports at the 2020 scientific sessions of the ADA.
One report included findings based on 136 episodes of severe hypoglycemia identified clinically and showed these events occurred 35% less often during treatment with insulin degludec, a significant difference. The overall finding was primarily driven by 48% fewer episodes of severe nocturnal hypoglycemia, but this difference was not significant.
The second report identified hypoglycemia events with continuous glucose monitoring in 74 of the study participants, which identified 193 episodes of nonsevere nocturnal hypoglycemia and found that treatment with insulin degludec cut the rate by 47%, primarily by reducing asymptomatic episodes.
Hourly blood draws track overnight hypoglycemia
The current study included 51 of the 149 HypoDeg patients who agreed to undergo overnight blood sampling and had this done at least once while treated with each of the two study insulins. (The study design called for two blood sampling nights for each willing patient during each of the two treatment periods.) The 51 patients had type 1 diabetes for an average of 28 years and an average age of 58 years. Two-thirds were men, their baseline A1c was 7.8%, and on average had 2.6 episodes of severe nocturnal hypoglycemia during the prior 2 years.
The researchers drew hourly blood specimens on a total of 196 nights from the 51 participating patients and identified 57 nights when blood glucose levels reached hypoglycemia thresholds in 33 patients. One-third of the events occurred when patients were on insulin degludec treatment, and two-thirds when they were on insulin glargine, reported Dr. Brøsen.
She presented three separate analyses of the data. One analysis focused on level 1 hypoglycemia events, when blood glucose dips to 70 mg/dL or less, which occurred 54% less often when patients were on insulin degludec. A second analysis looked at level 2 events, when blood glucose falls below 54 mg/dL, and treatment with insulin degludec cut this by 64% compared with insulin glargine. The third analysis focused on symptomatic events when blood glucose was 70 mg/dL or less, and treatment with insulin degludec linked with a 62% cut in this metric. All three between-group differences were significant.
Evidence supports already-changed practice
This new evidence “supports recommending” insulin degludec over insulin glargine, commented Bastiaan E. de Galan, MD, PhD, an endocrinologist and professor at Maastrict (the Netherlands) University Medical Center. The new results “extend those from previous trials in populations with type 1 diabetes that were unselected for the risk of hypoglycemia. In clinical practice, insulin degludec is already considered for patients who reported nocturnal hypoglycemia while on insulin glargine U100, but it’s great this study provides the scientific evidence,” said Dr. de Galan in an interview.

“The lower rate of nocturnal hypoglycemia with degludec, compared with glargine U100 is well established. Inpatient assessment of hypoglycemia with measurement of hourly plasma glucose allowed HypoDeg to provide stronger evidence than prior studies. The benefit of delgudec versus glargine U100 was significant and clinically meaningful, in hypo-prone patients who would benefit the most” by using insulin degludec, commented Gian Paolo Fadini, MD, an endocrinologist at the University of Padova (Italy), and a lead investigator on the ReFLeCT study.
But insulin degludec is not a completely silver bullet. Its prolonged duration of action and stability that may in part explain why it limits hypoglycemia events can also be a drawback: “It probably offers fewer options for flexibility. Any change in dose takes at least a day or 2 to settle, which may be unfavorable in certain circumstances,” noted Dr. de Galan.
“I wouldn’t recommend insulin degludec for all patients with type 1 diabetes. It’s an individual evaluation in each patient,” said Dr. Brøsen. “We will be looking into whether some patients are better off on insulin glargine.”
Cost makes a difference
Another, potentially more consequential flaw is insulin degludec’s relative expense.
“To date, use of degludec in routine practice has been limited by its cost, compared with older basal insulins,” observed Dr. Fadini in an interview. “In several countries, including the United States, degludec is substantially more expensive than glargine.”
The ADA’s Standards of Medical Care in Diabetes–2021 includes table 9.3 that lists the costs of various insulins and shows the median average wholesale price of insulin glargine U100 follow-on products as $190/vial, compared with a $407 price for a similar vial of insulin degludec.

Insulin degludec “is clearly superior from a hypoglycemia standpoint. Patients with type 1 diabetes like the reduction because hypoglycemia is scary, and dangerous. The main issue is cost, and the extent to which it may be covered by insurance,” commented Lisa Chow, MD, an endocrinologist at the University of Minnesota, Minneapolis. “We generally won’t prescribe degludec unless it is at a price affordable to the patient. We try to use patient assistance programs sponsored by the company [that markets insulin degludec: Novo Nordisk] to try to make it more affordable.”
Dr. Chow also highlighted that a new wrinkle has been introduction of a more concentrated formulation of insulin glargine, U300, which appears to cause less hypoglycemia than insulin glargine U100. Recent study results indicated that no significant difference exists in the incidence of hypoglycemia among patients treated with insulin glargine U300 and those treated with insulin degludec, such as findings from the BRIGHT trial, which included just over 900 patients, and in the CONCLUDE trial, which randomized more than 1,600 patients.
The HypoDeg study was sponsored by Novo Nordisk, the company that markets insulin degludec. Dr. Brøsen had no personal disclosures, but several of her coauthors were either Novo Nordisk employees or had financial relationships with the company. Dr. de Galan has received research funding from Novo Nordisk. Dr. Fadini has received lecture fees and research funding from Novo Nordisk, from Sanofi, the company that markets insulin glargine, and from several other companies. Dr. Chow has received research funding from Dexcom.
Patients with type 1 diabetes who used insulin degludec as their basal insulin had fewer than half the number of nocturnal hypoglycemia events, compared with patients who used insulin glargine U100, in a head-to-head crossover study with 51 patients who had a history of nighttime hypoglycemia episodes.
Patients with type 1 diabetes who are “struggling with nocturnal hypoglycemia would benefit from insulin degludec treatment,” said Julie M. Brøsen, MD, at the annual scientific sessions of the American Diabetes Association.
Accumulating evidence for less hypoglycemia with insulin degludec
Results from several studies comparing insulin degludec (Tresiba), a second-generation, longer-acting insulin with more stable steady-state performance, with the first-generation basal insulin analogue glargine (Lantus), have built the case that degludec produces fewer hypoglycemia events.
The landmark SWITCH 1 crossover study published in 2017 showed in about 500 patients with type 1 diabetes and a risk factor for hypoglycemia that treatment with insulin degludec led to significantly few total hypoglycemia episodes and significantly fewer nocturnal episodes, compared with insulin glargine.
Next came similar findings from ReFLeCT, a multicenter observational study that followed 556 unselected patients with type 1 diabetes in routine practice settings who switched to insulin degludec following treatment with a different basal insulin. The results again showed a significant drop-off in total, nonsevere, severe, and nocturnal hypoglycemia events.
Homing in on higher-risk patients
The current study, HypoDeg (Insulin Degludec and Symptomatic Nocturnal Hypoglycaemia), ran at 10 Danish centers and enrolled 149 adults with type 1 diabetes who had at least one episode of severe nocturnal hypoglycemia within the prior 2 years, focusing on patients most at risk for future nocturnal hypoglycemia events. In an unusual study design, researchers identified nocturnal hypoglycemic episodes with hourly venous blood samples drawn from a subcutaneous line.
They randomized the patients to basal insulin treatment with either insulin degludec or to insulin glargine U100, allowed their treatment to stabilize for 3 months, and then tallied nocturnal hypoglycemia events for 9 months. They then crossed patients to the alternative basal insulin and repeated the process.
Results from the full study have not yet appeared in published form but were in a pair of reports at the 2020 scientific sessions of the ADA.
One report included findings based on 136 episodes of severe hypoglycemia identified clinically and showed these events occurred 35% less often during treatment with insulin degludec, a significant difference. The overall finding was primarily driven by 48% fewer episodes of severe nocturnal hypoglycemia, but this difference was not significant.
The second report identified hypoglycemia events with continuous glucose monitoring in 74 of the study participants, which identified 193 episodes of nonsevere nocturnal hypoglycemia and found that treatment with insulin degludec cut the rate by 47%, primarily by reducing asymptomatic episodes.
Hourly blood draws track overnight hypoglycemia
The current study included 51 of the 149 HypoDeg patients who agreed to undergo overnight blood sampling and had this done at least once while treated with each of the two study insulins. (The study design called for two blood sampling nights for each willing patient during each of the two treatment periods.) The 51 patients had type 1 diabetes for an average of 28 years and an average age of 58 years. Two-thirds were men, their baseline A1c was 7.8%, and on average had 2.6 episodes of severe nocturnal hypoglycemia during the prior 2 years.
The researchers drew hourly blood specimens on a total of 196 nights from the 51 participating patients and identified 57 nights when blood glucose levels reached hypoglycemia thresholds in 33 patients. One-third of the events occurred when patients were on insulin degludec treatment, and two-thirds when they were on insulin glargine, reported Dr. Brøsen.
She presented three separate analyses of the data. One analysis focused on level 1 hypoglycemia events, when blood glucose dips to 70 mg/dL or less, which occurred 54% less often when patients were on insulin degludec. A second analysis looked at level 2 events, when blood glucose falls below 54 mg/dL, and treatment with insulin degludec cut this by 64% compared with insulin glargine. The third analysis focused on symptomatic events when blood glucose was 70 mg/dL or less, and treatment with insulin degludec linked with a 62% cut in this metric. All three between-group differences were significant.
Evidence supports already-changed practice
This new evidence “supports recommending” insulin degludec over insulin glargine, commented Bastiaan E. de Galan, MD, PhD, an endocrinologist and professor at Maastrict (the Netherlands) University Medical Center. The new results “extend those from previous trials in populations with type 1 diabetes that were unselected for the risk of hypoglycemia. In clinical practice, insulin degludec is already considered for patients who reported nocturnal hypoglycemia while on insulin glargine U100, but it’s great this study provides the scientific evidence,” said Dr. de Galan in an interview.
“The lower rate of nocturnal hypoglycemia with degludec, compared with glargine U100 is well established. Inpatient assessment of hypoglycemia with measurement of hourly plasma glucose allowed HypoDeg to provide stronger evidence than prior studies. The benefit of delgudec versus glargine U100 was significant and clinically meaningful, in hypo-prone patients who would benefit the most” by using insulin degludec, commented Gian Paolo Fadini, MD, an endocrinologist at the University of Padova (Italy), and a lead investigator on the ReFLeCT study.
But insulin degludec is not a completely silver bullet. Its prolonged duration of action and stability that may in part explain why it limits hypoglycemia events can also be a drawback: “It probably offers fewer options for flexibility. Any change in dose takes at least a day or 2 to settle, which may be unfavorable in certain circumstances,” noted Dr. de Galan.
“I wouldn’t recommend insulin degludec for all patients with type 1 diabetes. It’s an individual evaluation in each patient,” said Dr. Brøsen. “We will be looking into whether some patients are better off on insulin glargine.”
Cost makes a difference
Another, potentially more consequential flaw is insulin degludec’s relative expense.
“To date, use of degludec in routine practice has been limited by its cost, compared with older basal insulins,” observed Dr. Fadini in an interview. “In several countries, including the United States, degludec is substantially more expensive than glargine.”
The ADA’s Standards of Medical Care in Diabetes–2021 includes table 9.3 that lists the costs of various insulins and shows the median average wholesale price of insulin glargine U100 follow-on products as $190/vial, compared with a $407 price for a similar vial of insulin degludec.
Insulin degludec “is clearly superior from a hypoglycemia standpoint. Patients with type 1 diabetes like the reduction because hypoglycemia is scary, and dangerous. The main issue is cost, and the extent to which it may be covered by insurance,” commented Lisa Chow, MD, an endocrinologist at the University of Minnesota, Minneapolis. “We generally won’t prescribe degludec unless it is at a price affordable to the patient. We try to use patient assistance programs sponsored by the company [that markets insulin degludec: Novo Nordisk] to try to make it more affordable.”
Dr. Chow also highlighted that a new wrinkle has been introduction of a more concentrated formulation of insulin glargine, U300, which appears to cause less hypoglycemia than insulin glargine U100. Recent study results indicated that no significant difference exists in the incidence of hypoglycemia among patients treated with insulin glargine U300 and those treated with insulin degludec, such as findings from the BRIGHT trial, which included just over 900 patients, and in the CONCLUDE trial, which randomized more than 1,600 patients.
The HypoDeg study was sponsored by Novo Nordisk, the company that markets insulin degludec. Dr. Brøsen had no personal disclosures, but several of her coauthors were either Novo Nordisk employees or had financial relationships with the company. Dr. de Galan has received research funding from Novo Nordisk. Dr. Fadini has received lecture fees and research funding from Novo Nordisk, from Sanofi, the company that markets insulin glargine, and from several other companies. Dr. Chow has received research funding from Dexcom.
Patients with type 1 diabetes who used insulin degludec as their basal insulin had fewer than half the number of nocturnal hypoglycemia events, compared with patients who used insulin glargine U100, in a head-to-head crossover study with 51 patients who had a history of nighttime hypoglycemia episodes.
Patients with type 1 diabetes who are “struggling with nocturnal hypoglycemia would benefit from insulin degludec treatment,” said Julie M. Brøsen, MD, at the annual scientific sessions of the American Diabetes Association.
Accumulating evidence for less hypoglycemia with insulin degludec
Results from several studies comparing insulin degludec (Tresiba), a second-generation, longer-acting insulin with more stable steady-state performance, with the first-generation basal insulin analogue glargine (Lantus), have built the case that degludec produces fewer hypoglycemia events.
The landmark SWITCH 1 crossover study published in 2017 showed in about 500 patients with type 1 diabetes and a risk factor for hypoglycemia that treatment with insulin degludec led to significantly few total hypoglycemia episodes and significantly fewer nocturnal episodes, compared with insulin glargine.
Next came similar findings from ReFLeCT, a multicenter observational study that followed 556 unselected patients with type 1 diabetes in routine practice settings who switched to insulin degludec following treatment with a different basal insulin. The results again showed a significant drop-off in total, nonsevere, severe, and nocturnal hypoglycemia events.
Homing in on higher-risk patients
The current study, HypoDeg (Insulin Degludec and Symptomatic Nocturnal Hypoglycaemia), ran at 10 Danish centers and enrolled 149 adults with type 1 diabetes who had at least one episode of severe nocturnal hypoglycemia within the prior 2 years, focusing on patients most at risk for future nocturnal hypoglycemia events. In an unusual study design, researchers identified nocturnal hypoglycemic episodes with hourly venous blood samples drawn from a subcutaneous line.
They randomized the patients to basal insulin treatment with either insulin degludec or to insulin glargine U100, allowed their treatment to stabilize for 3 months, and then tallied nocturnal hypoglycemia events for 9 months. They then crossed patients to the alternative basal insulin and repeated the process.
Results from the full study have not yet appeared in published form but were in a pair of reports at the 2020 scientific sessions of the ADA.
One report included findings based on 136 episodes of severe hypoglycemia identified clinically and showed these events occurred 35% less often during treatment with insulin degludec, a significant difference. The overall finding was primarily driven by 48% fewer episodes of severe nocturnal hypoglycemia, but this difference was not significant.
The second report identified hypoglycemia events with continuous glucose monitoring in 74 of the study participants, which identified 193 episodes of nonsevere nocturnal hypoglycemia and found that treatment with insulin degludec cut the rate by 47%, primarily by reducing asymptomatic episodes.
Hourly blood draws track overnight hypoglycemia
The current study included 51 of the 149 HypoDeg patients who agreed to undergo overnight blood sampling and had this done at least once while treated with each of the two study insulins. (The study design called for two blood sampling nights for each willing patient during each of the two treatment periods.) The 51 patients had type 1 diabetes for an average of 28 years and an average age of 58 years. Two-thirds were men, their baseline A1c was 7.8%, and on average had 2.6 episodes of severe nocturnal hypoglycemia during the prior 2 years.
The researchers drew hourly blood specimens on a total of 196 nights from the 51 participating patients and identified 57 nights when blood glucose levels reached hypoglycemia thresholds in 33 patients. One-third of the events occurred when patients were on insulin degludec treatment, and two-thirds when they were on insulin glargine, reported Dr. Brøsen.
She presented three separate analyses of the data. One analysis focused on level 1 hypoglycemia events, when blood glucose dips to 70 mg/dL or less, which occurred 54% less often when patients were on insulin degludec. A second analysis looked at level 2 events, when blood glucose falls below 54 mg/dL, and treatment with insulin degludec cut this by 64% compared with insulin glargine. The third analysis focused on symptomatic events when blood glucose was 70 mg/dL or less, and treatment with insulin degludec linked with a 62% cut in this metric. All three between-group differences were significant.
Evidence supports already-changed practice
This new evidence “supports recommending” insulin degludec over insulin glargine, commented Bastiaan E. de Galan, MD, PhD, an endocrinologist and professor at Maastrict (the Netherlands) University Medical Center. The new results “extend those from previous trials in populations with type 1 diabetes that were unselected for the risk of hypoglycemia. In clinical practice, insulin degludec is already considered for patients who reported nocturnal hypoglycemia while on insulin glargine U100, but it’s great this study provides the scientific evidence,” said Dr. de Galan in an interview.
“The lower rate of nocturnal hypoglycemia with degludec, compared with glargine U100 is well established. Inpatient assessment of hypoglycemia with measurement of hourly plasma glucose allowed HypoDeg to provide stronger evidence than prior studies. The benefit of delgudec versus glargine U100 was significant and clinically meaningful, in hypo-prone patients who would benefit the most” by using insulin degludec, commented Gian Paolo Fadini, MD, an endocrinologist at the University of Padova (Italy), and a lead investigator on the ReFLeCT study.
But insulin degludec is not a completely silver bullet. Its prolonged duration of action and stability that may in part explain why it limits hypoglycemia events can also be a drawback: “It probably offers fewer options for flexibility. Any change in dose takes at least a day or 2 to settle, which may be unfavorable in certain circumstances,” noted Dr. de Galan.
“I wouldn’t recommend insulin degludec for all patients with type 1 diabetes. It’s an individual evaluation in each patient,” said Dr. Brøsen. “We will be looking into whether some patients are better off on insulin glargine.”
Cost makes a difference
Another, potentially more consequential flaw is insulin degludec’s relative expense.
“To date, use of degludec in routine practice has been limited by its cost, compared with older basal insulins,” observed Dr. Fadini in an interview. “In several countries, including the United States, degludec is substantially more expensive than glargine.”
The ADA’s Standards of Medical Care in Diabetes–2021 includes table 9.3 that lists the costs of various insulins and shows the median average wholesale price of insulin glargine U100 follow-on products as $190/vial, compared with a $407 price for a similar vial of insulin degludec.
Insulin degludec “is clearly superior from a hypoglycemia standpoint. Patients with type 1 diabetes like the reduction because hypoglycemia is scary, and dangerous. The main issue is cost, and the extent to which it may be covered by insurance,” commented Lisa Chow, MD, an endocrinologist at the University of Minnesota, Minneapolis. “We generally won’t prescribe degludec unless it is at a price affordable to the patient. We try to use patient assistance programs sponsored by the company [that markets insulin degludec: Novo Nordisk] to try to make it more affordable.”
Dr. Chow also highlighted that a new wrinkle has been introduction of a more concentrated formulation of insulin glargine, U300, which appears to cause less hypoglycemia than insulin glargine U100. Recent study results indicated that no significant difference exists in the incidence of hypoglycemia among patients treated with insulin glargine U300 and those treated with insulin degludec, such as findings from the BRIGHT trial, which included just over 900 patients, and in the CONCLUDE trial, which randomized more than 1,600 patients.
The HypoDeg study was sponsored by Novo Nordisk, the company that markets insulin degludec. Dr. Brøsen had no personal disclosures, but several of her coauthors were either Novo Nordisk employees or had financial relationships with the company. Dr. de Galan has received research funding from Novo Nordisk. Dr. Fadini has received lecture fees and research funding from Novo Nordisk, from Sanofi, the company that markets insulin glargine, and from several other companies. Dr. Chow has received research funding from Dexcom.
FROM ADA 2021