User login
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
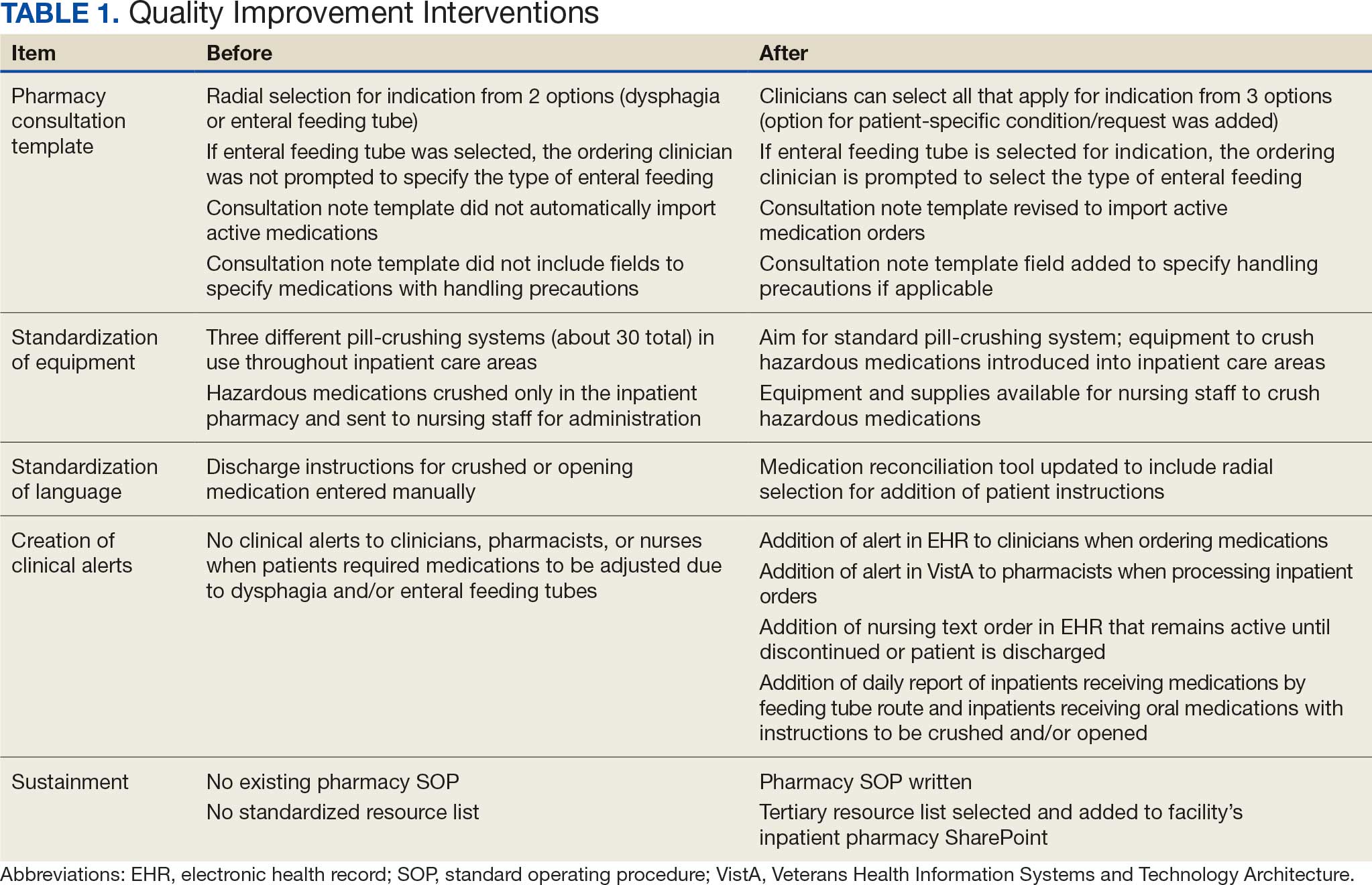
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
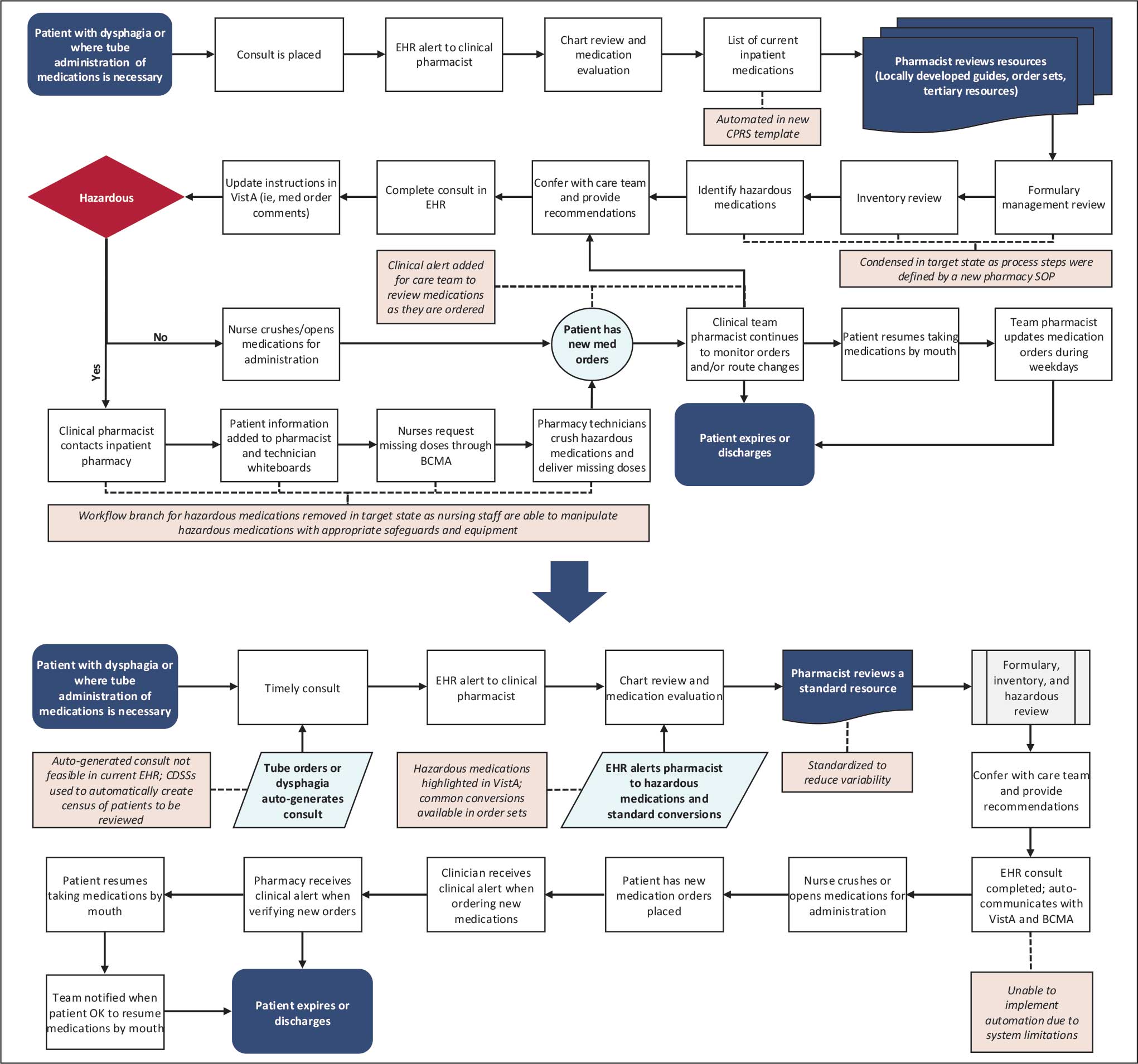
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).

Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
