User login
Clinical Endocrinology News is an independent news source that provides endocrinologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the endocrinologist's practice. Specialty topics include Diabetes, Lipid & Metabolic Disorders Menopause, Obesity, Osteoporosis, Pediatric Endocrinology, Pituitary, Thyroid & Adrenal Disorders, and Reproductive Endocrinology. Featured content includes Commentaries, Implementin Health Reform, Law & Medicine, and In the Loop, the blog of Clinical Endocrinology News. Clinical Endocrinology News is owned by Frontline Medical Communications.
addict
addicted
addicting
addiction
adult sites
alcohol
antibody
ass
attorney
audit
auditor
babies
babpa
baby
ban
banned
banning
best
bisexual
bitch
bleach
blog
blow job
bondage
boobs
booty
buy
cannabis
certificate
certification
certified
cheap
cheapest
class action
cocaine
cock
counterfeit drug
crack
crap
crime
criminal
cunt
curable
cure
dangerous
dangers
dead
deadly
death
defend
defended
depedent
dependence
dependent
detergent
dick
die
dildo
drug abuse
drug recall
dying
fag
fake
fatal
fatalities
fatality
free
fuck
gangs
gingivitis
guns
hardcore
herbal
herbs
heroin
herpes
home remedies
homo
horny
hypersensitivity
hypoglycemia treatment
illegal drug use
illegal use of prescription
incest
infant
infants
job
ketoacidosis
kill
killer
killing
kinky
law suit
lawsuit
lawyer
lesbian
marijuana
medicine for hypoglycemia
murder
naked
natural
newborn
nigger
noise
nude
nudity
orgy
over the counter
overdosage
overdose
overdosed
overdosing
penis
pimp
pistol
porn
porno
pornographic
pornography
prison
profanity
purchase
purchasing
pussy
queer
rape
rapist
recall
recreational drug
rob
robberies
sale
sales
sex
sexual
shit
shoot
slut
slutty
stole
stolen
store
sue
suicidal
suicide
supplements
supply company
theft
thief
thieves
tit
toddler
toddlers
toxic
toxin
tragedy
treating dka
treating hypoglycemia
treatment for hypoglycemia
vagina
violence
whore
withdrawal
without prescription
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-imn')]
div[contains(@class, 'pane-pub-home-imn')]
div[contains(@class, 'pane-pub-topic-imn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Most rheumatology drugs don’t increase COVID-19 hospitalization risk
The vast majority of patients with rheumatic and musculoskeletal diseases who contract COVID-19 recover from the virus, regardless of which medication they receive for their rheumatic condition, new international research suggests.

“These results provide, for the first time, information about the outcome of COVID-19 in patients with rheumatic and musculoskeletal diseases,” said study investigator Pedro Machado, MD, PhD, from University College London. “They should provide some reassurance to patients and healthcare providers.”
Machado and his colleagues looked at 600 COVID-19 patients from 40 countries, and found that those taking TNF inhibitors for their rheumatic disease were less likely to be hospitalized for COVID-19. However, treatment with more than 10 mg of prednisone daily — considered a moderate to high dose — was associated with a higher probability of hospitalization.
In addition, hospitalization was not associated with biologics; JAK inhibitors; conventional disease-modifying antirheumatic drugs (DMARDs), such as methotrexate; antimalarials, such as hydroxychloroquine; or nonsteroidal anti-inflammatory drugs (NSAIDs) — either alone or in combination with other biologics, such as TNF-alpha inhibitors.
The findings were presented at the virtual European League Against Rheumatism (EULAR) 2020 Congress and were published online in Annals of the Rheumatic Diseases.
“Initially, there was a huge concern that these drugs could affect the outcome of patients getting COVID-19, but what this is showing is that probably these drugs do not increase their risk of severe outcome,” Machado, who is chair of the EULAR standing committee on epidemiology and health services research, told Medscape Medical News.
As of June 1, 1061 patients from 28 participating countries had been entered into the EULAR COVID-19 database, which was launched as part of the international Global Rheumatology Alliance registry. Patient data are categorized by factors such as top rheumatology diagnosis, comorbidities, top-five COVID-19 symptoms, and DMARD therapy at the time of virus infection. Anonymized data will be shared with an international register based in the United States.
Machado’s team combined data from the EULAR and Global Rheumatology Alliance COVID-19 registries from March 24 to April 20. They looked at patient factors — such as age, sex, smoking status, rheumatic diagnosis, comorbidities, and rheumatic therapies — to examine the association of rheumatic therapies with hospitalization rates and COVID-19 disease course.

Of the 277 patients (46%) in the study cohort who required hospitalization, 55 (9%) died. But this finding shouldn’t be viewed as the true rate of hospitalization or death in patients with rheumatic disease and COVID-19, said Gerd Burmester, MD, from Charité–University Medicine Berlin.
“There’s tremendous bias in terms of more serious cases of COVID-19 being reported to the registries,” he explained, “because the mild cases won’t even show up at their rheumatologist’s office.”
“This can skew the idea that COVID-19 is much more dangerous to rheumatic patients than to the regular population,” Burmester told Medscape Medical News. “It scares the patients, obviously, but we believe this is not justified.”
It’s still unclear whether rituximab use raises the risk for severe COVID-19, he said. “It appears to be the only biologic for which the jury is still out,” he said.
“Anti-TNFs and anti-IL-6 drugs may even be beneficial, although we don’t have robust data,” he added.
The study can only highlight associations between rheumatic drugs and COVID-19 outcomes. “We cannot say there is a causal relationship between the findings,” Machado said.
Longer-term data, when available, should illuminate “more granular” aspects of COVID-19 outcomes in rheumatic patients, including their risks of requiring ventilation or developing a cytokine storm, he noted.
Burmester and Machado agree that research needs to continue as the pandemic rages on. But so far, “there are no data suggesting that, if you’re on a targeted, dedicated immunomodulator, your risk is higher to have a worse course of COVID-19 than the general population,” Burmester said.
“We simply didn’t know that when the pandemic started, and some patients even discontinued their drugs out of this fear,” he added. “It’s more reassuring than we originally thought.”
This article first appeared on Medscape.com.
The vast majority of patients with rheumatic and musculoskeletal diseases who contract COVID-19 recover from the virus, regardless of which medication they receive for their rheumatic condition, new international research suggests.
“These results provide, for the first time, information about the outcome of COVID-19 in patients with rheumatic and musculoskeletal diseases,” said study investigator Pedro Machado, MD, PhD, from University College London. “They should provide some reassurance to patients and healthcare providers.”
Machado and his colleagues looked at 600 COVID-19 patients from 40 countries, and found that those taking TNF inhibitors for their rheumatic disease were less likely to be hospitalized for COVID-19. However, treatment with more than 10 mg of prednisone daily — considered a moderate to high dose — was associated with a higher probability of hospitalization.
In addition, hospitalization was not associated with biologics; JAK inhibitors; conventional disease-modifying antirheumatic drugs (DMARDs), such as methotrexate; antimalarials, such as hydroxychloroquine; or nonsteroidal anti-inflammatory drugs (NSAIDs) — either alone or in combination with other biologics, such as TNF-alpha inhibitors.
The findings were presented at the virtual European League Against Rheumatism (EULAR) 2020 Congress and were published online in Annals of the Rheumatic Diseases.
“Initially, there was a huge concern that these drugs could affect the outcome of patients getting COVID-19, but what this is showing is that probably these drugs do not increase their risk of severe outcome,” Machado, who is chair of the EULAR standing committee on epidemiology and health services research, told Medscape Medical News.
As of June 1, 1061 patients from 28 participating countries had been entered into the EULAR COVID-19 database, which was launched as part of the international Global Rheumatology Alliance registry. Patient data are categorized by factors such as top rheumatology diagnosis, comorbidities, top-five COVID-19 symptoms, and DMARD therapy at the time of virus infection. Anonymized data will be shared with an international register based in the United States.
Machado’s team combined data from the EULAR and Global Rheumatology Alliance COVID-19 registries from March 24 to April 20. They looked at patient factors — such as age, sex, smoking status, rheumatic diagnosis, comorbidities, and rheumatic therapies — to examine the association of rheumatic therapies with hospitalization rates and COVID-19 disease course.
Of the 277 patients (46%) in the study cohort who required hospitalization, 55 (9%) died. But this finding shouldn’t be viewed as the true rate of hospitalization or death in patients with rheumatic disease and COVID-19, said Gerd Burmester, MD, from Charité–University Medicine Berlin.
“There’s tremendous bias in terms of more serious cases of COVID-19 being reported to the registries,” he explained, “because the mild cases won’t even show up at their rheumatologist’s office.”
“This can skew the idea that COVID-19 is much more dangerous to rheumatic patients than to the regular population,” Burmester told Medscape Medical News. “It scares the patients, obviously, but we believe this is not justified.”
It’s still unclear whether rituximab use raises the risk for severe COVID-19, he said. “It appears to be the only biologic for which the jury is still out,” he said.
“Anti-TNFs and anti-IL-6 drugs may even be beneficial, although we don’t have robust data,” he added.
The study can only highlight associations between rheumatic drugs and COVID-19 outcomes. “We cannot say there is a causal relationship between the findings,” Machado said.
Longer-term data, when available, should illuminate “more granular” aspects of COVID-19 outcomes in rheumatic patients, including their risks of requiring ventilation or developing a cytokine storm, he noted.
Burmester and Machado agree that research needs to continue as the pandemic rages on. But so far, “there are no data suggesting that, if you’re on a targeted, dedicated immunomodulator, your risk is higher to have a worse course of COVID-19 than the general population,” Burmester said.
“We simply didn’t know that when the pandemic started, and some patients even discontinued their drugs out of this fear,” he added. “It’s more reassuring than we originally thought.”
This article first appeared on Medscape.com.
The vast majority of patients with rheumatic and musculoskeletal diseases who contract COVID-19 recover from the virus, regardless of which medication they receive for their rheumatic condition, new international research suggests.
“These results provide, for the first time, information about the outcome of COVID-19 in patients with rheumatic and musculoskeletal diseases,” said study investigator Pedro Machado, MD, PhD, from University College London. “They should provide some reassurance to patients and healthcare providers.”
Machado and his colleagues looked at 600 COVID-19 patients from 40 countries, and found that those taking TNF inhibitors for their rheumatic disease were less likely to be hospitalized for COVID-19. However, treatment with more than 10 mg of prednisone daily — considered a moderate to high dose — was associated with a higher probability of hospitalization.
In addition, hospitalization was not associated with biologics; JAK inhibitors; conventional disease-modifying antirheumatic drugs (DMARDs), such as methotrexate; antimalarials, such as hydroxychloroquine; or nonsteroidal anti-inflammatory drugs (NSAIDs) — either alone or in combination with other biologics, such as TNF-alpha inhibitors.
The findings were presented at the virtual European League Against Rheumatism (EULAR) 2020 Congress and were published online in Annals of the Rheumatic Diseases.
“Initially, there was a huge concern that these drugs could affect the outcome of patients getting COVID-19, but what this is showing is that probably these drugs do not increase their risk of severe outcome,” Machado, who is chair of the EULAR standing committee on epidemiology and health services research, told Medscape Medical News.
As of June 1, 1061 patients from 28 participating countries had been entered into the EULAR COVID-19 database, which was launched as part of the international Global Rheumatology Alliance registry. Patient data are categorized by factors such as top rheumatology diagnosis, comorbidities, top-five COVID-19 symptoms, and DMARD therapy at the time of virus infection. Anonymized data will be shared with an international register based in the United States.
Machado’s team combined data from the EULAR and Global Rheumatology Alliance COVID-19 registries from March 24 to April 20. They looked at patient factors — such as age, sex, smoking status, rheumatic diagnosis, comorbidities, and rheumatic therapies — to examine the association of rheumatic therapies with hospitalization rates and COVID-19 disease course.
Of the 277 patients (46%) in the study cohort who required hospitalization, 55 (9%) died. But this finding shouldn’t be viewed as the true rate of hospitalization or death in patients with rheumatic disease and COVID-19, said Gerd Burmester, MD, from Charité–University Medicine Berlin.
“There’s tremendous bias in terms of more serious cases of COVID-19 being reported to the registries,” he explained, “because the mild cases won’t even show up at their rheumatologist’s office.”
“This can skew the idea that COVID-19 is much more dangerous to rheumatic patients than to the regular population,” Burmester told Medscape Medical News. “It scares the patients, obviously, but we believe this is not justified.”
It’s still unclear whether rituximab use raises the risk for severe COVID-19, he said. “It appears to be the only biologic for which the jury is still out,” he said.
“Anti-TNFs and anti-IL-6 drugs may even be beneficial, although we don’t have robust data,” he added.
The study can only highlight associations between rheumatic drugs and COVID-19 outcomes. “We cannot say there is a causal relationship between the findings,” Machado said.
Longer-term data, when available, should illuminate “more granular” aspects of COVID-19 outcomes in rheumatic patients, including their risks of requiring ventilation or developing a cytokine storm, he noted.
Burmester and Machado agree that research needs to continue as the pandemic rages on. But so far, “there are no data suggesting that, if you’re on a targeted, dedicated immunomodulator, your risk is higher to have a worse course of COVID-19 than the general population,” Burmester said.
“We simply didn’t know that when the pandemic started, and some patients even discontinued their drugs out of this fear,” he added. “It’s more reassuring than we originally thought.”
This article first appeared on Medscape.com.
More fatalities in heart transplant patients with COVID-19
COVID-19 infection is associated with a high risk for mortality in heart transplant (HT) recipients, a new case series suggests.
Investigators looked at data on 28 patients with a confirmed diagnosis of COVID-19 who received a HT between March 1, 2020, and April 24, 2020 and found a case-fatality rate of 25%.
“The high case fatality in our case series should alert physicians to the vulnerability of heart transplant recipients during the COVID-19 pandemic,” senior author Nir Uriel, MD, MSc, professor of medicine at Columbia University, New York, said in an interview.
“These patients require extra precautions to prevent the development of infection,” said Dr. Uriel, who is also a cardiologist at New York Presbyterian/Columbia University Irving Medical Center.
The study was published online May 13 in JAMA Cardiology.
Similar presentation
HT recipients can have several comorbidities after the procedure, including hypertension, diabetes, cardiac allograft vasculopathy, and ongoing immunosuppression, all of which can place them at risk for infection and adverse outcomes with COVID-19 infection, the authors wrote.
The researchers therefore embarked on a case series looking at 28 HT recipients with COVID-19 infection (median age, 64.0 years; interquartile range, 53.5-70.5; 79% male) to “describe the outcomes of recipients of HT who are chronically immunosuppressed and develop COVID-19 and raise important questions about the role of the immune system in the process.”
The median time from HT to study period was 8.6 (IQR, 4.2-14.5) years. Most patients had numerous comorbidities.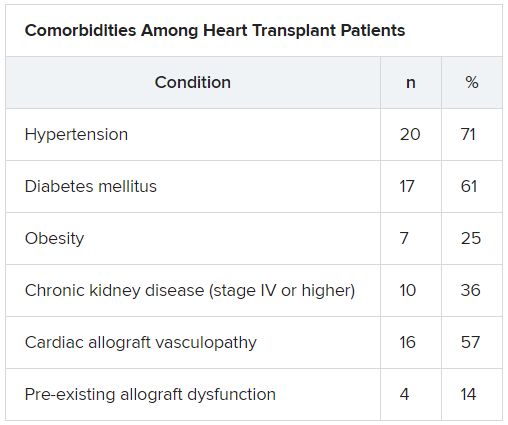
“The presentation of COVID-19 was similar to nontransplant patients with fever, dyspnea, cough, and GI symptoms,” Dr. Uriel reported.
No protective effect
Twenty-two patients (79%) required admission to the hospital, seven of whom (25%) required admission to the ICU and mechanical ventilation.
Despite the presence of immunosuppressive therapy, all patients had significant elevation of inflammatory biomarkers (median peak high-sensitivity C-reactive protein [hs-CRP], 11.83 mg/dL; IQR, 7.44-19.26; median peak interleukin [IL]-6, 105 pg/mL; IQR, 38-296).
Three-quarters had myocardial injury, with a median high-sensitivity troponin T of 0.055 (0.0205 - 0.1345) ng/mL.
Treatments of COVID-19 included hydroxychloroquine (18 patients; 78%), high-dose corticosteroids (eight patients; 47%), and IL-6 receptor antagonists (six patients; 26%).
Moreover, during hospitalization, mycophenolate mofetil was discontinued in most (70%) patients, and one-quarter had a reduction in their calcineurin inhibitor dose.
“Heart transplant recipients generally require more intense immunosuppressive therapy than most other solid organ transplant recipients, and this high baseline immunosuppression increases their propensity to develop infections and their likelihood of experiencing severe manifestations of infections,” Dr. Uriel commented.
“With COVID-19, in which the body’s inflammatory reaction appears to play a role in disease severity, there has been a question of whether immunosuppression may offer a protective effect,” he continued.
“This case series suggests that this is not the case, although this would need to be confirmed in larger studies,” he said.
Low threshold
Among the 22 patients who were admitted to the hospital, half were discharged home and four (18%) were still hospitalized at the end of the study.
Of the seven patients who died, two died at the study center, and five died in an outside institution.
“In the HT population, social distancing (or isolation), strict use of masks when in public, proper handwashing, and sanitization of surfaces are of paramount importance in the prevention of COVID-19 infection,” Dr. Uriel stated.
“In addition, we have restricted these patients’ contact with the hospital as much as possible during the pandemic,” he said.
However, “there should be a low threshold to hospitalize heart transplant patients who develop infection with COVID-19. Furthermore, in our series, outcomes were better for patients hospitalized at the transplant center; therefore, strong consideration should be given to transferring HT patients when hospitalized at another hospital,” he added.
The authors emphasized that COVID-19 patients “will require ongoing monitoring in the recovery phase, as an immunosuppression regimen is reintroduced and the consequences to the allograft itself become apparent.”
Vulnerable population
Commenting on the study, Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston, suggested that “in epidemiological terms, [the findings] might not look as bad as the way they are reflected in the paper.”
Given that Columbia is “one of the larger heart transplant centers in the U.S., following probably 1,000 patients, having only 22 out of perhaps thousands whom they transplanted or are actively following would actually represent a low serious infection rate,” said Dr. Mehra, who is also the executive director of the Center for Advanced Heart Disease at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, also in Boston.
“We must not forget to emphasize that, when assessing these case fatality rates, we must look at the entire population at risk, not only the handful that we were able to observe,” explained Dr. Mehra, who was not involved with the study.
Moreover, the patients were “older and had comorbidities, with poor underlying kidney function and other complications, and underlying coronary artery disease in the transplanted heart,” so “it would not surprise me that they had such a high fatality rate, since they had a high degree of vulnerability,” he said.
Dr. Mehra, who is also the editor-in-chief of the Journal of Heart and Lung Transplantation, said that the journal has received manuscripts still in the review process that suggest different fatality rates than those found in the current case series.
However, he acknowledged that, because these are patients with serious vulnerability due to underlying heart disease, “you can’t be lackadaisical and need to do everything to decrease this vulnerability.”
The authors noted that, although their study did not show a protective effect from immunosuppression against COVID-19, further studies are needed to assess each individual immunosuppressive agent and provide a definitive answer.
The study was supported by a grant to one of the investigators from the National Heart, Lung, and Blood Institute. Dr. Uriel reports no relevant financial relationships. The other authors’ disclosures are listed in the publication. Dr. Mehra reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 infection is associated with a high risk for mortality in heart transplant (HT) recipients, a new case series suggests.
Investigators looked at data on 28 patients with a confirmed diagnosis of COVID-19 who received a HT between March 1, 2020, and April 24, 2020 and found a case-fatality rate of 25%.
“The high case fatality in our case series should alert physicians to the vulnerability of heart transplant recipients during the COVID-19 pandemic,” senior author Nir Uriel, MD, MSc, professor of medicine at Columbia University, New York, said in an interview.
“These patients require extra precautions to prevent the development of infection,” said Dr. Uriel, who is also a cardiologist at New York Presbyterian/Columbia University Irving Medical Center.
The study was published online May 13 in JAMA Cardiology.
Similar presentation
HT recipients can have several comorbidities after the procedure, including hypertension, diabetes, cardiac allograft vasculopathy, and ongoing immunosuppression, all of which can place them at risk for infection and adverse outcomes with COVID-19 infection, the authors wrote.
The researchers therefore embarked on a case series looking at 28 HT recipients with COVID-19 infection (median age, 64.0 years; interquartile range, 53.5-70.5; 79% male) to “describe the outcomes of recipients of HT who are chronically immunosuppressed and develop COVID-19 and raise important questions about the role of the immune system in the process.”
The median time from HT to study period was 8.6 (IQR, 4.2-14.5) years. Most patients had numerous comorbidities.
“The presentation of COVID-19 was similar to nontransplant patients with fever, dyspnea, cough, and GI symptoms,” Dr. Uriel reported.
No protective effect
Twenty-two patients (79%) required admission to the hospital, seven of whom (25%) required admission to the ICU and mechanical ventilation.
Despite the presence of immunosuppressive therapy, all patients had significant elevation of inflammatory biomarkers (median peak high-sensitivity C-reactive protein [hs-CRP], 11.83 mg/dL; IQR, 7.44-19.26; median peak interleukin [IL]-6, 105 pg/mL; IQR, 38-296).
Three-quarters had myocardial injury, with a median high-sensitivity troponin T of 0.055 (0.0205 - 0.1345) ng/mL.
Treatments of COVID-19 included hydroxychloroquine (18 patients; 78%), high-dose corticosteroids (eight patients; 47%), and IL-6 receptor antagonists (six patients; 26%).
Moreover, during hospitalization, mycophenolate mofetil was discontinued in most (70%) patients, and one-quarter had a reduction in their calcineurin inhibitor dose.
“Heart transplant recipients generally require more intense immunosuppressive therapy than most other solid organ transplant recipients, and this high baseline immunosuppression increases their propensity to develop infections and their likelihood of experiencing severe manifestations of infections,” Dr. Uriel commented.
“With COVID-19, in which the body’s inflammatory reaction appears to play a role in disease severity, there has been a question of whether immunosuppression may offer a protective effect,” he continued.
“This case series suggests that this is not the case, although this would need to be confirmed in larger studies,” he said.
Low threshold
Among the 22 patients who were admitted to the hospital, half were discharged home and four (18%) were still hospitalized at the end of the study.
Of the seven patients who died, two died at the study center, and five died in an outside institution.
“In the HT population, social distancing (or isolation), strict use of masks when in public, proper handwashing, and sanitization of surfaces are of paramount importance in the prevention of COVID-19 infection,” Dr. Uriel stated.
“In addition, we have restricted these patients’ contact with the hospital as much as possible during the pandemic,” he said.
However, “there should be a low threshold to hospitalize heart transplant patients who develop infection with COVID-19. Furthermore, in our series, outcomes were better for patients hospitalized at the transplant center; therefore, strong consideration should be given to transferring HT patients when hospitalized at another hospital,” he added.
The authors emphasized that COVID-19 patients “will require ongoing monitoring in the recovery phase, as an immunosuppression regimen is reintroduced and the consequences to the allograft itself become apparent.”
Vulnerable population
Commenting on the study, Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston, suggested that “in epidemiological terms, [the findings] might not look as bad as the way they are reflected in the paper.”
Given that Columbia is “one of the larger heart transplant centers in the U.S., following probably 1,000 patients, having only 22 out of perhaps thousands whom they transplanted or are actively following would actually represent a low serious infection rate,” said Dr. Mehra, who is also the executive director of the Center for Advanced Heart Disease at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, also in Boston.
“We must not forget to emphasize that, when assessing these case fatality rates, we must look at the entire population at risk, not only the handful that we were able to observe,” explained Dr. Mehra, who was not involved with the study.
Moreover, the patients were “older and had comorbidities, with poor underlying kidney function and other complications, and underlying coronary artery disease in the transplanted heart,” so “it would not surprise me that they had such a high fatality rate, since they had a high degree of vulnerability,” he said.
Dr. Mehra, who is also the editor-in-chief of the Journal of Heart and Lung Transplantation, said that the journal has received manuscripts still in the review process that suggest different fatality rates than those found in the current case series.
However, he acknowledged that, because these are patients with serious vulnerability due to underlying heart disease, “you can’t be lackadaisical and need to do everything to decrease this vulnerability.”
The authors noted that, although their study did not show a protective effect from immunosuppression against COVID-19, further studies are needed to assess each individual immunosuppressive agent and provide a definitive answer.
The study was supported by a grant to one of the investigators from the National Heart, Lung, and Blood Institute. Dr. Uriel reports no relevant financial relationships. The other authors’ disclosures are listed in the publication. Dr. Mehra reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 infection is associated with a high risk for mortality in heart transplant (HT) recipients, a new case series suggests.
Investigators looked at data on 28 patients with a confirmed diagnosis of COVID-19 who received a HT between March 1, 2020, and April 24, 2020 and found a case-fatality rate of 25%.
“The high case fatality in our case series should alert physicians to the vulnerability of heart transplant recipients during the COVID-19 pandemic,” senior author Nir Uriel, MD, MSc, professor of medicine at Columbia University, New York, said in an interview.
“These patients require extra precautions to prevent the development of infection,” said Dr. Uriel, who is also a cardiologist at New York Presbyterian/Columbia University Irving Medical Center.
The study was published online May 13 in JAMA Cardiology.
Similar presentation
HT recipients can have several comorbidities after the procedure, including hypertension, diabetes, cardiac allograft vasculopathy, and ongoing immunosuppression, all of which can place them at risk for infection and adverse outcomes with COVID-19 infection, the authors wrote.
The researchers therefore embarked on a case series looking at 28 HT recipients with COVID-19 infection (median age, 64.0 years; interquartile range, 53.5-70.5; 79% male) to “describe the outcomes of recipients of HT who are chronically immunosuppressed and develop COVID-19 and raise important questions about the role of the immune system in the process.”
The median time from HT to study period was 8.6 (IQR, 4.2-14.5) years. Most patients had numerous comorbidities.
“The presentation of COVID-19 was similar to nontransplant patients with fever, dyspnea, cough, and GI symptoms,” Dr. Uriel reported.
No protective effect
Twenty-two patients (79%) required admission to the hospital, seven of whom (25%) required admission to the ICU and mechanical ventilation.
Despite the presence of immunosuppressive therapy, all patients had significant elevation of inflammatory biomarkers (median peak high-sensitivity C-reactive protein [hs-CRP], 11.83 mg/dL; IQR, 7.44-19.26; median peak interleukin [IL]-6, 105 pg/mL; IQR, 38-296).
Three-quarters had myocardial injury, with a median high-sensitivity troponin T of 0.055 (0.0205 - 0.1345) ng/mL.
Treatments of COVID-19 included hydroxychloroquine (18 patients; 78%), high-dose corticosteroids (eight patients; 47%), and IL-6 receptor antagonists (six patients; 26%).
Moreover, during hospitalization, mycophenolate mofetil was discontinued in most (70%) patients, and one-quarter had a reduction in their calcineurin inhibitor dose.
“Heart transplant recipients generally require more intense immunosuppressive therapy than most other solid organ transplant recipients, and this high baseline immunosuppression increases their propensity to develop infections and their likelihood of experiencing severe manifestations of infections,” Dr. Uriel commented.
“With COVID-19, in which the body’s inflammatory reaction appears to play a role in disease severity, there has been a question of whether immunosuppression may offer a protective effect,” he continued.
“This case series suggests that this is not the case, although this would need to be confirmed in larger studies,” he said.
Low threshold
Among the 22 patients who were admitted to the hospital, half were discharged home and four (18%) were still hospitalized at the end of the study.
Of the seven patients who died, two died at the study center, and five died in an outside institution.
“In the HT population, social distancing (or isolation), strict use of masks when in public, proper handwashing, and sanitization of surfaces are of paramount importance in the prevention of COVID-19 infection,” Dr. Uriel stated.
“In addition, we have restricted these patients’ contact with the hospital as much as possible during the pandemic,” he said.
However, “there should be a low threshold to hospitalize heart transplant patients who develop infection with COVID-19. Furthermore, in our series, outcomes were better for patients hospitalized at the transplant center; therefore, strong consideration should be given to transferring HT patients when hospitalized at another hospital,” he added.
The authors emphasized that COVID-19 patients “will require ongoing monitoring in the recovery phase, as an immunosuppression regimen is reintroduced and the consequences to the allograft itself become apparent.”
Vulnerable population
Commenting on the study, Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston, suggested that “in epidemiological terms, [the findings] might not look as bad as the way they are reflected in the paper.”
Given that Columbia is “one of the larger heart transplant centers in the U.S., following probably 1,000 patients, having only 22 out of perhaps thousands whom they transplanted or are actively following would actually represent a low serious infection rate,” said Dr. Mehra, who is also the executive director of the Center for Advanced Heart Disease at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, also in Boston.
“We must not forget to emphasize that, when assessing these case fatality rates, we must look at the entire population at risk, not only the handful that we were able to observe,” explained Dr. Mehra, who was not involved with the study.
Moreover, the patients were “older and had comorbidities, with poor underlying kidney function and other complications, and underlying coronary artery disease in the transplanted heart,” so “it would not surprise me that they had such a high fatality rate, since they had a high degree of vulnerability,” he said.
Dr. Mehra, who is also the editor-in-chief of the Journal of Heart and Lung Transplantation, said that the journal has received manuscripts still in the review process that suggest different fatality rates than those found in the current case series.
However, he acknowledged that, because these are patients with serious vulnerability due to underlying heart disease, “you can’t be lackadaisical and need to do everything to decrease this vulnerability.”
The authors noted that, although their study did not show a protective effect from immunosuppression against COVID-19, further studies are needed to assess each individual immunosuppressive agent and provide a definitive answer.
The study was supported by a grant to one of the investigators from the National Heart, Lung, and Blood Institute. Dr. Uriel reports no relevant financial relationships. The other authors’ disclosures are listed in the publication. Dr. Mehra reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
High out-of-pocket costs for type 1 diabetes patients: It’s not just insulin
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
Today’s top news highlights: COVID-19 could worsen gambling problems, food allergies less common than thought
Here are the stories our MDedge editors across specialties think you need to know about today:
Could COVID-19 worsen gambling problems?
Take isolation, add excess available time and anxiety about illness or finances and you get the potential to increase problem gambling behaviors during the COVID-19 pandemic. A call to action, recently published in the Journal of Addiction Medicine, says it’s essential to gather data and supply guidance on this issue. “People are likely to be experiencing stress at levels they haven’t experienced previously,” said coauthor Marc N. Potenza, MD, PhD, of Yale University, New Haven, Conn. While multiple factors can contribute to addictive behaviors, “with respect to the pandemic, one concern is that so-called negative reinforcement motivations – engaging in an addictive behavior to escape from depressed or negative mood states – may be a driving motivation for a significant number of people during this time,” he said. Read more.
Food allergies in children are less frequent than expected
Food allergies appear to be less common than previously reported among 6- to 10-year-olds in Europe, according to a recent study. Prevalance ranged from a low of 1.4% to a high of 3.8%, both of which are “considerably lower” than the 16% rate based on parental reports of symptoms such as rash, itching, or diarrhea, Linus Grabenhenrich, MD, MPH, and colleagues reported in Allergy. The most commonly reported allergies were to peanuts and hazelnuts, with a prevalence of just over 5% for both. Previous research on pediatric food allergy prevalence has largely consisted of single-center studies with heterogeneous designs, the researchers noted. Read more.
The grocery store hug
William G. Wilkoff, MD, grew up in a family that didn’t embrace hugging, but as a small-town pediatrician he warmed up to the concept so much that he would frequently hug a passing acquaintance at the grocery store. That’s something he misses in the current environment and that he doesn’t expect will return. “[N]early every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship,” Dr. Wilkoff wrote in a column on MDedge. “Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child. I’m sure you have your own list of people who send off that we-need-to-hug spark.” Read more.
Identifying structural lesions of axial spondyloarthritis
What constitutes a structural lesion of the sacroiliac joints on MRI that’s indicative of axial spondyloarthritis (axSpA) has long been a matter of conjecture, but the Assessment of SpondyloArthritis International Society (ASAS) MRI Working Group has developed new definitions that show a high degree of specificity in identifying such lesions in the disease. “Previous studies have described structural lesions in different ways, precluding meaningful comparisons between studies,” Walter P. Maksymowych, MD, said at the annual European Congress of Rheumatology, held online this year due to COVID-19. “The ASAS MRI group has generated updated consensus lesion definitions that describe each of the MRI lesions in the sacroiliac joint. These definitions have been validated by seven expert readers from the ASAS MRI group on MRI images from the ASAS classification cohort.” Read more.
Making the world’s skin crawl
Clinicians should be aware of the skin manifestations of COVID-19, especially when triaging patients. In a commentary published on MDedge, Kathleen M. Coerdt and Amor Khachemoune, MD, describe the dermatologic implications of COVID-19, including the clinical manifestations of the disease, risk reduction techniques for patients and providers, personal protective equipment-associated adverse reactions, and the financial impact on dermatologists. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Could COVID-19 worsen gambling problems?
Take isolation, add excess available time and anxiety about illness or finances and you get the potential to increase problem gambling behaviors during the COVID-19 pandemic. A call to action, recently published in the Journal of Addiction Medicine, says it’s essential to gather data and supply guidance on this issue. “People are likely to be experiencing stress at levels they haven’t experienced previously,” said coauthor Marc N. Potenza, MD, PhD, of Yale University, New Haven, Conn. While multiple factors can contribute to addictive behaviors, “with respect to the pandemic, one concern is that so-called negative reinforcement motivations – engaging in an addictive behavior to escape from depressed or negative mood states – may be a driving motivation for a significant number of people during this time,” he said. Read more.
Food allergies in children are less frequent than expected
Food allergies appear to be less common than previously reported among 6- to 10-year-olds in Europe, according to a recent study. Prevalance ranged from a low of 1.4% to a high of 3.8%, both of which are “considerably lower” than the 16% rate based on parental reports of symptoms such as rash, itching, or diarrhea, Linus Grabenhenrich, MD, MPH, and colleagues reported in Allergy. The most commonly reported allergies were to peanuts and hazelnuts, with a prevalence of just over 5% for both. Previous research on pediatric food allergy prevalence has largely consisted of single-center studies with heterogeneous designs, the researchers noted. Read more.
The grocery store hug
William G. Wilkoff, MD, grew up in a family that didn’t embrace hugging, but as a small-town pediatrician he warmed up to the concept so much that he would frequently hug a passing acquaintance at the grocery store. That’s something he misses in the current environment and that he doesn’t expect will return. “[N]early every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship,” Dr. Wilkoff wrote in a column on MDedge. “Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child. I’m sure you have your own list of people who send off that we-need-to-hug spark.” Read more.
Identifying structural lesions of axial spondyloarthritis
What constitutes a structural lesion of the sacroiliac joints on MRI that’s indicative of axial spondyloarthritis (axSpA) has long been a matter of conjecture, but the Assessment of SpondyloArthritis International Society (ASAS) MRI Working Group has developed new definitions that show a high degree of specificity in identifying such lesions in the disease. “Previous studies have described structural lesions in different ways, precluding meaningful comparisons between studies,” Walter P. Maksymowych, MD, said at the annual European Congress of Rheumatology, held online this year due to COVID-19. “The ASAS MRI group has generated updated consensus lesion definitions that describe each of the MRI lesions in the sacroiliac joint. These definitions have been validated by seven expert readers from the ASAS MRI group on MRI images from the ASAS classification cohort.” Read more.
Making the world’s skin crawl
Clinicians should be aware of the skin manifestations of COVID-19, especially when triaging patients. In a commentary published on MDedge, Kathleen M. Coerdt and Amor Khachemoune, MD, describe the dermatologic implications of COVID-19, including the clinical manifestations of the disease, risk reduction techniques for patients and providers, personal protective equipment-associated adverse reactions, and the financial impact on dermatologists. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Could COVID-19 worsen gambling problems?
Take isolation, add excess available time and anxiety about illness or finances and you get the potential to increase problem gambling behaviors during the COVID-19 pandemic. A call to action, recently published in the Journal of Addiction Medicine, says it’s essential to gather data and supply guidance on this issue. “People are likely to be experiencing stress at levels they haven’t experienced previously,” said coauthor Marc N. Potenza, MD, PhD, of Yale University, New Haven, Conn. While multiple factors can contribute to addictive behaviors, “with respect to the pandemic, one concern is that so-called negative reinforcement motivations – engaging in an addictive behavior to escape from depressed or negative mood states – may be a driving motivation for a significant number of people during this time,” he said. Read more.
Food allergies in children are less frequent than expected
Food allergies appear to be less common than previously reported among 6- to 10-year-olds in Europe, according to a recent study. Prevalance ranged from a low of 1.4% to a high of 3.8%, both of which are “considerably lower” than the 16% rate based on parental reports of symptoms such as rash, itching, or diarrhea, Linus Grabenhenrich, MD, MPH, and colleagues reported in Allergy. The most commonly reported allergies were to peanuts and hazelnuts, with a prevalence of just over 5% for both. Previous research on pediatric food allergy prevalence has largely consisted of single-center studies with heterogeneous designs, the researchers noted. Read more.
The grocery store hug
William G. Wilkoff, MD, grew up in a family that didn’t embrace hugging, but as a small-town pediatrician he warmed up to the concept so much that he would frequently hug a passing acquaintance at the grocery store. That’s something he misses in the current environment and that he doesn’t expect will return. “[N]early every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship,” Dr. Wilkoff wrote in a column on MDedge. “Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child. I’m sure you have your own list of people who send off that we-need-to-hug spark.” Read more.
Identifying structural lesions of axial spondyloarthritis
What constitutes a structural lesion of the sacroiliac joints on MRI that’s indicative of axial spondyloarthritis (axSpA) has long been a matter of conjecture, but the Assessment of SpondyloArthritis International Society (ASAS) MRI Working Group has developed new definitions that show a high degree of specificity in identifying such lesions in the disease. “Previous studies have described structural lesions in different ways, precluding meaningful comparisons between studies,” Walter P. Maksymowych, MD, said at the annual European Congress of Rheumatology, held online this year due to COVID-19. “The ASAS MRI group has generated updated consensus lesion definitions that describe each of the MRI lesions in the sacroiliac joint. These definitions have been validated by seven expert readers from the ASAS MRI group on MRI images from the ASAS classification cohort.” Read more.
Making the world’s skin crawl
Clinicians should be aware of the skin manifestations of COVID-19, especially when triaging patients. In a commentary published on MDedge, Kathleen M. Coerdt and Amor Khachemoune, MD, describe the dermatologic implications of COVID-19, including the clinical manifestations of the disease, risk reduction techniques for patients and providers, personal protective equipment-associated adverse reactions, and the financial impact on dermatologists. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Americans avoided emergency departments early in the pandemic
compared with the corresponding period in 2019, according to a report from the Centers for Disease Control and Prevention.
“The striking decline in ED visits nationwide … suggests that the pandemic has altered the use of the ED by the public,” Kathleen P. Hartnett, PhD, and associates at the CDC said June 3 in the Mortality and Morbidity Weekly Report.
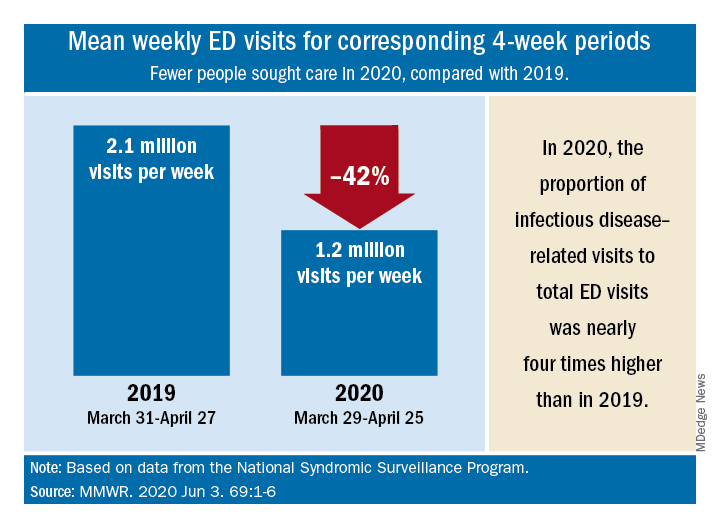
The weekly mean was just over 1.2 million ED visits for the 4 weeks from March 29 to April 25, 2020, compared with the nearly 2.2 million visits per week recorded from March 31 to April 27, 2019 – a drop of 42%, based on an analysis of data from the National Syndromic Surveillance Program.
Despite that drop, ED visits for infectious disease–related reasons, taken as a proportion of all 1.2 ED visits during the early pandemic period, were 3.8 times higher than the comparison period in 2019, the investigators reported.
ED visits also were higher in 2020 for specified and unspecified lower respiratory disease not including influenza, pneumonia, asthma, or bronchitis (prevalence ratio of 1.99, compared with 2019), cardiac arrest and ventricular fibrillation (PR, 1.98), and pneumonia not caused by tuberculosis (PR, 1.91), Dr. Hartnett and associates said.
Prevalence ratios for the early pandemic period were down for most other conditions, with some of the largest decreases seen for influenza (PR, 0.16), otitis media (PR, 0.35), and neoplasm-related encounters (PR, 0.40), they said.
Visits have increased each week since reaching their lowest point during April 12-18, but the number for the most recent full week, May 24-30, which was not included in the analysis, was still 26% lower than the corresponding week in 2019, the CDC team pointed out.
“Some persons could be delaying care for conditions that might result in additional mortality if left untreated,” the investigators noted, and those “who use the ED as a safety net because they lack access to primary care and telemedicine might be disproportionately affected if they avoid seeking care because of concerns about the infection risk in the ED.”
SOURCE: Hartnett KP et al. MMWR. 2020 Jun 3. 69:1-6.
compared with the corresponding period in 2019, according to a report from the Centers for Disease Control and Prevention.
“The striking decline in ED visits nationwide … suggests that the pandemic has altered the use of the ED by the public,” Kathleen P. Hartnett, PhD, and associates at the CDC said June 3 in the Mortality and Morbidity Weekly Report.
The weekly mean was just over 1.2 million ED visits for the 4 weeks from March 29 to April 25, 2020, compared with the nearly 2.2 million visits per week recorded from March 31 to April 27, 2019 – a drop of 42%, based on an analysis of data from the National Syndromic Surveillance Program.
Despite that drop, ED visits for infectious disease–related reasons, taken as a proportion of all 1.2 ED visits during the early pandemic period, were 3.8 times higher than the comparison period in 2019, the investigators reported.
ED visits also were higher in 2020 for specified and unspecified lower respiratory disease not including influenza, pneumonia, asthma, or bronchitis (prevalence ratio of 1.99, compared with 2019), cardiac arrest and ventricular fibrillation (PR, 1.98), and pneumonia not caused by tuberculosis (PR, 1.91), Dr. Hartnett and associates said.
Prevalence ratios for the early pandemic period were down for most other conditions, with some of the largest decreases seen for influenza (PR, 0.16), otitis media (PR, 0.35), and neoplasm-related encounters (PR, 0.40), they said.
Visits have increased each week since reaching their lowest point during April 12-18, but the number for the most recent full week, May 24-30, which was not included in the analysis, was still 26% lower than the corresponding week in 2019, the CDC team pointed out.
“Some persons could be delaying care for conditions that might result in additional mortality if left untreated,” the investigators noted, and those “who use the ED as a safety net because they lack access to primary care and telemedicine might be disproportionately affected if they avoid seeking care because of concerns about the infection risk in the ED.”
SOURCE: Hartnett KP et al. MMWR. 2020 Jun 3. 69:1-6.
compared with the corresponding period in 2019, according to a report from the Centers for Disease Control and Prevention.
“The striking decline in ED visits nationwide … suggests that the pandemic has altered the use of the ED by the public,” Kathleen P. Hartnett, PhD, and associates at the CDC said June 3 in the Mortality and Morbidity Weekly Report.
The weekly mean was just over 1.2 million ED visits for the 4 weeks from March 29 to April 25, 2020, compared with the nearly 2.2 million visits per week recorded from March 31 to April 27, 2019 – a drop of 42%, based on an analysis of data from the National Syndromic Surveillance Program.
Despite that drop, ED visits for infectious disease–related reasons, taken as a proportion of all 1.2 ED visits during the early pandemic period, were 3.8 times higher than the comparison period in 2019, the investigators reported.
ED visits also were higher in 2020 for specified and unspecified lower respiratory disease not including influenza, pneumonia, asthma, or bronchitis (prevalence ratio of 1.99, compared with 2019), cardiac arrest and ventricular fibrillation (PR, 1.98), and pneumonia not caused by tuberculosis (PR, 1.91), Dr. Hartnett and associates said.
Prevalence ratios for the early pandemic period were down for most other conditions, with some of the largest decreases seen for influenza (PR, 0.16), otitis media (PR, 0.35), and neoplasm-related encounters (PR, 0.40), they said.
Visits have increased each week since reaching their lowest point during April 12-18, but the number for the most recent full week, May 24-30, which was not included in the analysis, was still 26% lower than the corresponding week in 2019, the CDC team pointed out.
“Some persons could be delaying care for conditions that might result in additional mortality if left untreated,” the investigators noted, and those “who use the ED as a safety net because they lack access to primary care and telemedicine might be disproportionately affected if they avoid seeking care because of concerns about the infection risk in the ED.”
SOURCE: Hartnett KP et al. MMWR. 2020 Jun 3. 69:1-6.
FROM MMWR
The grocery store hug
I grew up in a family that was pretty much devoid of physical demonstrations of affection. I certainly felt that my folks loved me, but there was no hugging. I don’t recall ever seeing my parents kiss or touch each other. My dad would occasionally physically tease my mother. For example, I can remember one incident at the dinner table when he was playfully and gently laying a hand on my mother’s arm just as she was raising her fork to her mouth. After about three of these gentle holds, she lifted her water glass and tossed its contents in his face. This was the full extent of physicality in our family.

It wasn’t just my parents. I can’t remember aunts or uncles or cousins ever hugging us when we met. Grandmothers of course would request a hug. I never knew either of my grandfathers, but I suspect they would not have been the hugging kind.
I never felt I was missing out on anything, because in the generally WASPish atmosphere of the community in which I grew up I saw very few public displays of affection. But somewhere over time, hugging crept into the American repertoire of expression. This incursion may have been a ripple effect from the flower power, free love hippiedom of the ‘60s and ‘70s. Or it may have been a symptom of globalization as Americans became more familiar with other cultures in which physical expression was more common.
Whatever the reason for the more widespread adoption of hugging in our social vocabulary with my somewhat physically impoverished upbringing, it took me longer than most folks to comfortably include it in my greeting options. Although I may have come to the dance late, I have fully adopted hugging as a way to greet people with whom I have more than a passing acquaintance.
In fact, the ability to comfortably hug former coworkers, old friends I haven’t seen in years, and parents with whom I had shared a particularly troublesome child is what I miss most about the restrictions that have come with the COVID-19 pandemic. Now when I meet folks in the grocery store with whom I share a special affection that magnetic spark still leaps between our eyes, just visible over our face masks, but mentally and physically we take a step back and say to ourselves that this hug shouldn’t happen and it isn’t going to happen. And that makes me sad.

One of the great perks of practicing pediatrics in a small town and then remaining there in retirement is that nearly every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship. Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child.
I can envision a day sometime in the relatively near future that I will be able to hug my two grandchildren whom I haven’t hugged even though they live a short 10-minute walk away. But I have trouble imagining when I will again be able to enjoy and be enriched by those special grocery store hugs that I have grown to savor.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I grew up in a family that was pretty much devoid of physical demonstrations of affection. I certainly felt that my folks loved me, but there was no hugging. I don’t recall ever seeing my parents kiss or touch each other. My dad would occasionally physically tease my mother. For example, I can remember one incident at the dinner table when he was playfully and gently laying a hand on my mother’s arm just as she was raising her fork to her mouth. After about three of these gentle holds, she lifted her water glass and tossed its contents in his face. This was the full extent of physicality in our family.
It wasn’t just my parents. I can’t remember aunts or uncles or cousins ever hugging us when we met. Grandmothers of course would request a hug. I never knew either of my grandfathers, but I suspect they would not have been the hugging kind.
I never felt I was missing out on anything, because in the generally WASPish atmosphere of the community in which I grew up I saw very few public displays of affection. But somewhere over time, hugging crept into the American repertoire of expression. This incursion may have been a ripple effect from the flower power, free love hippiedom of the ‘60s and ‘70s. Or it may have been a symptom of globalization as Americans became more familiar with other cultures in which physical expression was more common.
Whatever the reason for the more widespread adoption of hugging in our social vocabulary with my somewhat physically impoverished upbringing, it took me longer than most folks to comfortably include it in my greeting options. Although I may have come to the dance late, I have fully adopted hugging as a way to greet people with whom I have more than a passing acquaintance.
In fact, the ability to comfortably hug former coworkers, old friends I haven’t seen in years, and parents with whom I had shared a particularly troublesome child is what I miss most about the restrictions that have come with the COVID-19 pandemic. Now when I meet folks in the grocery store with whom I share a special affection that magnetic spark still leaps between our eyes, just visible over our face masks, but mentally and physically we take a step back and say to ourselves that this hug shouldn’t happen and it isn’t going to happen. And that makes me sad.
One of the great perks of practicing pediatrics in a small town and then remaining there in retirement is that nearly every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship. Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child.
I can envision a day sometime in the relatively near future that I will be able to hug my two grandchildren whom I haven’t hugged even though they live a short 10-minute walk away. But I have trouble imagining when I will again be able to enjoy and be enriched by those special grocery store hugs that I have grown to savor.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I grew up in a family that was pretty much devoid of physical demonstrations of affection. I certainly felt that my folks loved me, but there was no hugging. I don’t recall ever seeing my parents kiss or touch each other. My dad would occasionally physically tease my mother. For example, I can remember one incident at the dinner table when he was playfully and gently laying a hand on my mother’s arm just as she was raising her fork to her mouth. After about three of these gentle holds, she lifted her water glass and tossed its contents in his face. This was the full extent of physicality in our family.
It wasn’t just my parents. I can’t remember aunts or uncles or cousins ever hugging us when we met. Grandmothers of course would request a hug. I never knew either of my grandfathers, but I suspect they would not have been the hugging kind.
I never felt I was missing out on anything, because in the generally WASPish atmosphere of the community in which I grew up I saw very few public displays of affection. But somewhere over time, hugging crept into the American repertoire of expression. This incursion may have been a ripple effect from the flower power, free love hippiedom of the ‘60s and ‘70s. Or it may have been a symptom of globalization as Americans became more familiar with other cultures in which physical expression was more common.
Whatever the reason for the more widespread adoption of hugging in our social vocabulary with my somewhat physically impoverished upbringing, it took me longer than most folks to comfortably include it in my greeting options. Although I may have come to the dance late, I have fully adopted hugging as a way to greet people with whom I have more than a passing acquaintance.
In fact, the ability to comfortably hug former coworkers, old friends I haven’t seen in years, and parents with whom I had shared a particularly troublesome child is what I miss most about the restrictions that have come with the COVID-19 pandemic. Now when I meet folks in the grocery store with whom I share a special affection that magnetic spark still leaps between our eyes, just visible over our face masks, but mentally and physically we take a step back and say to ourselves that this hug shouldn’t happen and it isn’t going to happen. And that makes me sad.
One of the great perks of practicing pediatrics in a small town and then remaining there in retirement is that nearly every week I encounter one or two people with whom I have a long and sometimes emotionally charged relationship. Nurses with whom I sweated over difficult delivery room resuscitations. Parents for whom their anxiety was getting in the way of their ability to parent. Parents and caregivers of complex multiply disabled children who are now adults. Peers who have lost a spouse or a child.
I can envision a day sometime in the relatively near future that I will be able to hug my two grandchildren whom I haven’t hugged even though they live a short 10-minute walk away. But I have trouble imagining when I will again be able to enjoy and be enriched by those special grocery store hugs that I have grown to savor.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Today’s top news highlights: Addressing racism in maternity care, group forms to protect health professionals from retaliation
Here are the stories our MDedge editors across specialties think you need to know about today:
Addressing racism in the maternal mortality crisis
The emerging racial disparities in COVID-19 incidence and outcomes in the United States are on a collision course with long-standing racial disparities in U.S. maternal care and mortality. “The saying is that ‘the virus doesn’t discriminate,’ but it understands our biases, right? So, the virus takes advantage of the weaknesses in our system,” said Joia A. Crear-Perry, MD, an ob.gyn. and founder and president of the National Birth Equity Collaborative, a New Orleans–based research, training, and advocacy organization working to optimize black maternal and infant health. This article is part of an ongoing feature series on the crisis in maternal mortality in the United States. Here we explore potential solutions for addressing the inequities as proposed by thought leaders and key stakeholders. Read more.
A ‘Beacon’ for physicians, nurses facing retaliation
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy. Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality. The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment supply and other matters of public concern related to coronavirus. “There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.” Read more.
COVID-19 ravages the Navajo Nation
The Navajo Nation has the most cases of the COVID-19 virus of any tribe in the United States, and numbers as of May 31, 2020, are 5,348, with 246 confirmed deaths. These devastating numbers, which might be leveling off, are associated with Navajo people having higher-than-average rates of diabetes, heart disease, and cancer. This is compounded with 30%-40% of homes having no electricity or running water, and a poverty rate of about 38%. “We endured and learned from each Naayee, hunger, and death to name a few adversities. The COVID-19 pandemic, or “Big Cough” (Dikos Nitsaa’igii -19 in Navajo language), is a monster confronting the Navajo today. It has had significant impact on our nation and people,” Mary Hasbah Roessel, MD, a Navajo board-certified psychiatrist practicing in Santa Fe, N.M., wrote in a commentary on MDedge. Read more.
Heart pump system authorized for COVID-19 patients
The Food and Drug Administration issued an emergency use authorization (EUA) for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation. The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including pulmonary embolism. Read more.
Deprescribing hypertension meds looks safe for older adults
Some patients aged 80 years or older can potentially cut back on their number of antihypertensive meds, under physician guidance, without an important loss of blood pressure control, researchers concluded based on findings from a randomized multicenter trial. The study, called Optimising Treatment for Mild Systolic Hypertension in the Elderly (OPTIMISE), entered “patients in whom the benefits of taking blood pressure-lowering treatments might start to be outweighed by the potential harms,” said James P. Sheppard, PhD, of University of Oxford (England). The report was published in JAMA. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Addressing racism in the maternal mortality crisis
The emerging racial disparities in COVID-19 incidence and outcomes in the United States are on a collision course with long-standing racial disparities in U.S. maternal care and mortality. “The saying is that ‘the virus doesn’t discriminate,’ but it understands our biases, right? So, the virus takes advantage of the weaknesses in our system,” said Joia A. Crear-Perry, MD, an ob.gyn. and founder and president of the National Birth Equity Collaborative, a New Orleans–based research, training, and advocacy organization working to optimize black maternal and infant health. This article is part of an ongoing feature series on the crisis in maternal mortality in the United States. Here we explore potential solutions for addressing the inequities as proposed by thought leaders and key stakeholders. Read more.
A ‘Beacon’ for physicians, nurses facing retaliation
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy. Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality. The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment supply and other matters of public concern related to coronavirus. “There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.” Read more.
COVID-19 ravages the Navajo Nation
The Navajo Nation has the most cases of the COVID-19 virus of any tribe in the United States, and numbers as of May 31, 2020, are 5,348, with 246 confirmed deaths. These devastating numbers, which might be leveling off, are associated with Navajo people having higher-than-average rates of diabetes, heart disease, and cancer. This is compounded with 30%-40% of homes having no electricity or running water, and a poverty rate of about 38%. “We endured and learned from each Naayee, hunger, and death to name a few adversities. The COVID-19 pandemic, or “Big Cough” (Dikos Nitsaa’igii -19 in Navajo language), is a monster confronting the Navajo today. It has had significant impact on our nation and people,” Mary Hasbah Roessel, MD, a Navajo board-certified psychiatrist practicing in Santa Fe, N.M., wrote in a commentary on MDedge. Read more.
Heart pump system authorized for COVID-19 patients
The Food and Drug Administration issued an emergency use authorization (EUA) for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation. The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including pulmonary embolism. Read more.
Deprescribing hypertension meds looks safe for older adults
Some patients aged 80 years or older can potentially cut back on their number of antihypertensive meds, under physician guidance, without an important loss of blood pressure control, researchers concluded based on findings from a randomized multicenter trial. The study, called Optimising Treatment for Mild Systolic Hypertension in the Elderly (OPTIMISE), entered “patients in whom the benefits of taking blood pressure-lowering treatments might start to be outweighed by the potential harms,” said James P. Sheppard, PhD, of University of Oxford (England). The report was published in JAMA. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Addressing racism in the maternal mortality crisis
The emerging racial disparities in COVID-19 incidence and outcomes in the United States are on a collision course with long-standing racial disparities in U.S. maternal care and mortality. “The saying is that ‘the virus doesn’t discriminate,’ but it understands our biases, right? So, the virus takes advantage of the weaknesses in our system,” said Joia A. Crear-Perry, MD, an ob.gyn. and founder and president of the National Birth Equity Collaborative, a New Orleans–based research, training, and advocacy organization working to optimize black maternal and infant health. This article is part of an ongoing feature series on the crisis in maternal mortality in the United States. Here we explore potential solutions for addressing the inequities as proposed by thought leaders and key stakeholders. Read more.
A ‘Beacon’ for physicians, nurses facing retaliation
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy. Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality. The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment supply and other matters of public concern related to coronavirus. “There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.” Read more.
COVID-19 ravages the Navajo Nation
The Navajo Nation has the most cases of the COVID-19 virus of any tribe in the United States, and numbers as of May 31, 2020, are 5,348, with 246 confirmed deaths. These devastating numbers, which might be leveling off, are associated with Navajo people having higher-than-average rates of diabetes, heart disease, and cancer. This is compounded with 30%-40% of homes having no electricity or running water, and a poverty rate of about 38%. “We endured and learned from each Naayee, hunger, and death to name a few adversities. The COVID-19 pandemic, or “Big Cough” (Dikos Nitsaa’igii -19 in Navajo language), is a monster confronting the Navajo today. It has had significant impact on our nation and people,” Mary Hasbah Roessel, MD, a Navajo board-certified psychiatrist practicing in Santa Fe, N.M., wrote in a commentary on MDedge. Read more.
Heart pump system authorized for COVID-19 patients
The Food and Drug Administration issued an emergency use authorization (EUA) for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation. The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including pulmonary embolism. Read more.
Deprescribing hypertension meds looks safe for older adults
Some patients aged 80 years or older can potentially cut back on their number of antihypertensive meds, under physician guidance, without an important loss of blood pressure control, researchers concluded based on findings from a randomized multicenter trial. The study, called Optimising Treatment for Mild Systolic Hypertension in the Elderly (OPTIMISE), entered “patients in whom the benefits of taking blood pressure-lowering treatments might start to be outweighed by the potential harms,” said James P. Sheppard, PhD, of University of Oxford (England). The report was published in JAMA. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
COVID-19: New group stands up for health professionals facing retaliation
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy.

Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality.
“When COVID came around, we began talking about where we could make a difference and help people where help was needed most,” said Dr. Hathi, an internal medicine resident at Massachusetts General Hospital in Boston. “We decided the PPE issue makes a good first focus.”
The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment (PPE) supply and other matters of public concern related to coronavirus.
In recent months, health care professionals have reported being reprimanded or even terminated for publicly discussing PPE shortages or sharing safety concerns. Other clinicians say they can’t share their experiences for fear of reprisal by their hospitals.

“The centrality of adequate PPE is pretty undeniable at this point,” said John Paul Schnapper-Casteras, JD, an attorney and cofounder of the organization. “In terms of speaking up about matters of workplace safety and public concern, when health care workers share knowledge, correct problems – and in some cases, blow the whistle – it affirmatively benefits medical science, disease control, and the public interest,” he said in an interview. “We have seen in other countries, the disastrous consequences that can stem from silencing medical professionals who try to speak out.”
Letter highlights hospitals’ obligations
As part of their efforts, Beacon leaders drafted a strongly worded letter on behalf of health care workers outlining the legal obligations of hospitals to ensure workplace safety, underscoring the federal protections that bar retaliation against employees who exercise their workplace rights. Whistleblower protections under the Occupational Safety and Health Act, the False Claims Act, and the National Labor Relations Act, for instance, prohibit retaliation against employees for blowing the whistle on unsafe or unlawful conditions.
Beacon’s letter urges hospitals to adopt a uniform policy that recognizes “the importance and legitimacy of doctors, nurses, and medical professionals who research, write, and speak about the use and supply of PPE in addressing coronavirus.”
“We are deeply troubled by reports that medical professionals are being fired, retaliated against, disciplined, or threatened for speaking (or potentially speaking) about PPE shortages and related safety conditions that directly place their and their patients’ lives in danger,” the letter states. “As a matter of law, medical personnel have a wide range of rights that protect their employment status and ability to comment on matters of public concern (and provide a cause of action in court if these rights are violated).”
Dr. Hathi, who over the last decade has founded two social enterprises advancing women’s rights, said organizers have sent the letter to hospitals and health systems that were publicly reported or otherwise known to have threatened, terminated, or retaliated against employees for protesting PPE shortages or speaking up about unsafe working conditions during this crisis. The letter is available on the Beacon website.
“Many letters have been written [recently] criticizing hospitals for retaliating against their workers,” Dr. Hathi said. “Ours amplifies this voice. But it also serves as a tool for self-empowerment, a stark warning to health systems that their actions bear consequences, and an assurance to health workers across the country that we’re listening and we’re here to help them safeguard their rights and their dignity at work.”
Dr. Hathi and her colleagues have also circulated the letter on social media and other platforms as a petition that health care professionals and others can sign in support of fair and safe treatment of employees with respect to PPE. So far, the group has collected signatures from individuals, communities, and organizations representing about 35,000 people, Dr. Hathi said.
Workplace rights, legal options
Beacon leaders have also begun counseling and advising health care workers who have experienced retaliation or discipline associated with PPE issues. Educating medical professionals about their workplace rights and legal options is another key focus of the group, according to its founders.
“There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.”
In one instance, they heard from a physician who wanted to protect nurses at his hospital because they did not have masks and were being coughed on by COVID-19 patients. The doctor requested that his hospital supply masks to the nurses. After making the request, the physician was disciplined by hospital leadership, Dr. Hathi said. In another case, a physician assistant told the group she was terminated because she wanted to wear her own mask in a hospital that was treating COVID patients.
“She was not allowed to, and she was fired for even bringing it up,” said Sheel Tyle, JD, an attorney and Beacon cofounder.
Beacon intends to assist health care workers who face such retaliation and discipline in a number of ways, Mr. Tyle said. For instance, by helping an individual get compensation for what happened, aiding the professional in getting their job back, or helping the worker retain a severance package of some kind, he said.
“And then there is the larger public policy issue of preventing the hospital from being a bad actor,” Mr. Tyle said. “That can be done through state or federal complaints, largely under different statutes related to workplace protection or OSHA. Our group [has] lawyers that could represent clients individually as well as a number of friends who are attorneys in various states who we could partner with, depending on the situation.”
While the organization is positioned to represent health professionals in lawsuits if necessary, Mr. Tyle emphasized that litigation is not the intended goal of the group. Rather, they are seeking to deter hospitals and others from being “bad actors,” through any number of methods, including communication, advocacy, or complaints.
Ultimately, Dr. Hathi said she hopes the organization’s efforts activate health care workers as an organizing body and in the process, spark policy change at the federal level to better protect health care workers.
“The challenges we’re facing now – protecting workplace safety, employee voice, a living wage, adequate sick and family leave – long predate this pandemic,” Dr. Hathi said. “But they’ve deepened and acquired existential significance as, battered by policy failures and the unsparing virus itself, physicians shed their political indifference and join a growing nationwide chorus to restore workers’ rights and to fundamentally reimagine our broken healthcare system. Now, more than ever before, organizations like Beacon are vital for arming health workers in this fight.”
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy.
Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality.
“When COVID came around, we began talking about where we could make a difference and help people where help was needed most,” said Dr. Hathi, an internal medicine resident at Massachusetts General Hospital in Boston. “We decided the PPE issue makes a good first focus.”
The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment (PPE) supply and other matters of public concern related to coronavirus.
In recent months, health care professionals have reported being reprimanded or even terminated for publicly discussing PPE shortages or sharing safety concerns. Other clinicians say they can’t share their experiences for fear of reprisal by their hospitals.
“The centrality of adequate PPE is pretty undeniable at this point,” said John Paul Schnapper-Casteras, JD, an attorney and cofounder of the organization. “In terms of speaking up about matters of workplace safety and public concern, when health care workers share knowledge, correct problems – and in some cases, blow the whistle – it affirmatively benefits medical science, disease control, and the public interest,” he said in an interview. “We have seen in other countries, the disastrous consequences that can stem from silencing medical professionals who try to speak out.”
Letter highlights hospitals’ obligations
As part of their efforts, Beacon leaders drafted a strongly worded letter on behalf of health care workers outlining the legal obligations of hospitals to ensure workplace safety, underscoring the federal protections that bar retaliation against employees who exercise their workplace rights. Whistleblower protections under the Occupational Safety and Health Act, the False Claims Act, and the National Labor Relations Act, for instance, prohibit retaliation against employees for blowing the whistle on unsafe or unlawful conditions.
Beacon’s letter urges hospitals to adopt a uniform policy that recognizes “the importance and legitimacy of doctors, nurses, and medical professionals who research, write, and speak about the use and supply of PPE in addressing coronavirus.”
“We are deeply troubled by reports that medical professionals are being fired, retaliated against, disciplined, or threatened for speaking (or potentially speaking) about PPE shortages and related safety conditions that directly place their and their patients’ lives in danger,” the letter states. “As a matter of law, medical personnel have a wide range of rights that protect their employment status and ability to comment on matters of public concern (and provide a cause of action in court if these rights are violated).”
Dr. Hathi, who over the last decade has founded two social enterprises advancing women’s rights, said organizers have sent the letter to hospitals and health systems that were publicly reported or otherwise known to have threatened, terminated, or retaliated against employees for protesting PPE shortages or speaking up about unsafe working conditions during this crisis. The letter is available on the Beacon website.
“Many letters have been written [recently] criticizing hospitals for retaliating against their workers,” Dr. Hathi said. “Ours amplifies this voice. But it also serves as a tool for self-empowerment, a stark warning to health systems that their actions bear consequences, and an assurance to health workers across the country that we’re listening and we’re here to help them safeguard their rights and their dignity at work.”
Dr. Hathi and her colleagues have also circulated the letter on social media and other platforms as a petition that health care professionals and others can sign in support of fair and safe treatment of employees with respect to PPE. So far, the group has collected signatures from individuals, communities, and organizations representing about 35,000 people, Dr. Hathi said.
Workplace rights, legal options
Beacon leaders have also begun counseling and advising health care workers who have experienced retaliation or discipline associated with PPE issues. Educating medical professionals about their workplace rights and legal options is another key focus of the group, according to its founders.
“There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.”
In one instance, they heard from a physician who wanted to protect nurses at his hospital because they did not have masks and were being coughed on by COVID-19 patients. The doctor requested that his hospital supply masks to the nurses. After making the request, the physician was disciplined by hospital leadership, Dr. Hathi said. In another case, a physician assistant told the group she was terminated because she wanted to wear her own mask in a hospital that was treating COVID patients.
“She was not allowed to, and she was fired for even bringing it up,” said Sheel Tyle, JD, an attorney and Beacon cofounder.
Beacon intends to assist health care workers who face such retaliation and discipline in a number of ways, Mr. Tyle said. For instance, by helping an individual get compensation for what happened, aiding the professional in getting their job back, or helping the worker retain a severance package of some kind, he said.
“And then there is the larger public policy issue of preventing the hospital from being a bad actor,” Mr. Tyle said. “That can be done through state or federal complaints, largely under different statutes related to workplace protection or OSHA. Our group [has] lawyers that could represent clients individually as well as a number of friends who are attorneys in various states who we could partner with, depending on the situation.”
While the organization is positioned to represent health professionals in lawsuits if necessary, Mr. Tyle emphasized that litigation is not the intended goal of the group. Rather, they are seeking to deter hospitals and others from being “bad actors,” through any number of methods, including communication, advocacy, or complaints.
Ultimately, Dr. Hathi said she hopes the organization’s efforts activate health care workers as an organizing body and in the process, spark policy change at the federal level to better protect health care workers.
“The challenges we’re facing now – protecting workplace safety, employee voice, a living wage, adequate sick and family leave – long predate this pandemic,” Dr. Hathi said. “But they’ve deepened and acquired existential significance as, battered by policy failures and the unsparing virus itself, physicians shed their political indifference and join a growing nationwide chorus to restore workers’ rights and to fundamentally reimagine our broken healthcare system. Now, more than ever before, organizations like Beacon are vital for arming health workers in this fight.”
Sejal Hathi, MD, and two colleagues had long kicked around the idea of starting a nonprofit group that would center on civic and legal advocacy.
Once the COVID-19 pandemic hit, the three friends – who have a mix of legal, medical, and advocacy backgrounds – began chatting by email and through Zoom video meetings about how to make the plan a reality.
“When COVID came around, we began talking about where we could make a difference and help people where help was needed most,” said Dr. Hathi, an internal medicine resident at Massachusetts General Hospital in Boston. “We decided the PPE issue makes a good first focus.”
The new organization – named Beacon – quickly mobilized, assembled their team, and launched a website. Beacon’s first project now aims to highlight and protect the legal rights of medical professionals who speak out about personal protection equipment (PPE) supply and other matters of public concern related to coronavirus.
In recent months, health care professionals have reported being reprimanded or even terminated for publicly discussing PPE shortages or sharing safety concerns. Other clinicians say they can’t share their experiences for fear of reprisal by their hospitals.
“The centrality of adequate PPE is pretty undeniable at this point,” said John Paul Schnapper-Casteras, JD, an attorney and cofounder of the organization. “In terms of speaking up about matters of workplace safety and public concern, when health care workers share knowledge, correct problems – and in some cases, blow the whistle – it affirmatively benefits medical science, disease control, and the public interest,” he said in an interview. “We have seen in other countries, the disastrous consequences that can stem from silencing medical professionals who try to speak out.”
Letter highlights hospitals’ obligations
As part of their efforts, Beacon leaders drafted a strongly worded letter on behalf of health care workers outlining the legal obligations of hospitals to ensure workplace safety, underscoring the federal protections that bar retaliation against employees who exercise their workplace rights. Whistleblower protections under the Occupational Safety and Health Act, the False Claims Act, and the National Labor Relations Act, for instance, prohibit retaliation against employees for blowing the whistle on unsafe or unlawful conditions.
Beacon’s letter urges hospitals to adopt a uniform policy that recognizes “the importance and legitimacy of doctors, nurses, and medical professionals who research, write, and speak about the use and supply of PPE in addressing coronavirus.”
“We are deeply troubled by reports that medical professionals are being fired, retaliated against, disciplined, or threatened for speaking (or potentially speaking) about PPE shortages and related safety conditions that directly place their and their patients’ lives in danger,” the letter states. “As a matter of law, medical personnel have a wide range of rights that protect their employment status and ability to comment on matters of public concern (and provide a cause of action in court if these rights are violated).”
Dr. Hathi, who over the last decade has founded two social enterprises advancing women’s rights, said organizers have sent the letter to hospitals and health systems that were publicly reported or otherwise known to have threatened, terminated, or retaliated against employees for protesting PPE shortages or speaking up about unsafe working conditions during this crisis. The letter is available on the Beacon website.
“Many letters have been written [recently] criticizing hospitals for retaliating against their workers,” Dr. Hathi said. “Ours amplifies this voice. But it also serves as a tool for self-empowerment, a stark warning to health systems that their actions bear consequences, and an assurance to health workers across the country that we’re listening and we’re here to help them safeguard their rights and their dignity at work.”
Dr. Hathi and her colleagues have also circulated the letter on social media and other platforms as a petition that health care professionals and others can sign in support of fair and safe treatment of employees with respect to PPE. So far, the group has collected signatures from individuals, communities, and organizations representing about 35,000 people, Dr. Hathi said.
Workplace rights, legal options
Beacon leaders have also begun counseling and advising health care workers who have experienced retaliation or discipline associated with PPE issues. Educating medical professionals about their workplace rights and legal options is another key focus of the group, according to its founders.
“There are a flurry of reports coming our way about physicians and nurses, as well as other health care workers, who are for whatever reason being disciplined or retaliated against for simply seeking appropriate safety policies at their workplaces,” Dr. Hathi said. “What we’ve found is that many of them don’t even know what their options look like. Doctors, nurses, health care workers are not the typical type to engage politically, to speak out, [or to] advocate for themselves.”
In one instance, they heard from a physician who wanted to protect nurses at his hospital because they did not have masks and were being coughed on by COVID-19 patients. The doctor requested that his hospital supply masks to the nurses. After making the request, the physician was disciplined by hospital leadership, Dr. Hathi said. In another case, a physician assistant told the group she was terminated because she wanted to wear her own mask in a hospital that was treating COVID patients.
“She was not allowed to, and she was fired for even bringing it up,” said Sheel Tyle, JD, an attorney and Beacon cofounder.
Beacon intends to assist health care workers who face such retaliation and discipline in a number of ways, Mr. Tyle said. For instance, by helping an individual get compensation for what happened, aiding the professional in getting their job back, or helping the worker retain a severance package of some kind, he said.
“And then there is the larger public policy issue of preventing the hospital from being a bad actor,” Mr. Tyle said. “That can be done through state or federal complaints, largely under different statutes related to workplace protection or OSHA. Our group [has] lawyers that could represent clients individually as well as a number of friends who are attorneys in various states who we could partner with, depending on the situation.”
While the organization is positioned to represent health professionals in lawsuits if necessary, Mr. Tyle emphasized that litigation is not the intended goal of the group. Rather, they are seeking to deter hospitals and others from being “bad actors,” through any number of methods, including communication, advocacy, or complaints.
Ultimately, Dr. Hathi said she hopes the organization’s efforts activate health care workers as an organizing body and in the process, spark policy change at the federal level to better protect health care workers.
“The challenges we’re facing now – protecting workplace safety, employee voice, a living wage, adequate sick and family leave – long predate this pandemic,” Dr. Hathi said. “But they’ve deepened and acquired existential significance as, battered by policy failures and the unsparing virus itself, physicians shed their political indifference and join a growing nationwide chorus to restore workers’ rights and to fundamentally reimagine our broken healthcare system. Now, more than ever before, organizations like Beacon are vital for arming health workers in this fight.”
FDA okays emergency use for Impella RP in COVID-19 right heart failure
The Food and Drug Administration issued an emergency use authorization for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation, Abiomed announced June 1.
“Based on extrapolation of data from the approved indication and reported clinical experience, FDA has concluded that the Impella RP may be effective at providing temporary right ventricular support for the treatment of acute right heart failure or decompensation caused by COVID-19 complications, including PE [pulmonary embolism],” the letter noted.
It cited, for example, use of the temporary heart pump in a 59-year-old woman suffering from COVID-19 who went into right ventricular failure and became hypotensive after an acute PE was removed. After placement of the device, the patient experienced a “dramatic and immediate” improvement in arterial pressure and the device was removed on the fifth day, according to Amir Kaki, MD, and Ted Schreiber, MD, of Ascension St. John Hospital, Detroit, whose review of the case has been posted online.
“Acute pulmonary embolism is clearly being recognized as a life-threatening manifestation of COVID-19. Impella RP is an important tool to help cardiologists save lives during this pandemic,” Dr. Kaki said in the letter. “As we have demonstrated in our series of patients, early recognition of right ventricular dysfunction and early placement of the Impella RP for patients who are hypotensive can be lifesaving.”
Other data cited in support of the Impella RP emergency use authorization (EUA) include a 2019 series of hemodynamically unstable patients with PE in Japan and a 2017 case report of a 47-year-old man with right ventricular failure, profound shock, and a massive PE.
The FDA granted premarket approval of the Impella RP system in 2017 to provide temporary right ventricular support for up to 14 days in patients with a body surface area of at least 1.5 m2 who develop acute right heart failure or decompensation following left ventricular assist device implantation, MI, heart transplant, or open-heart surgery.
The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including PE.
The Impella RP is authorized only for emergency use under the EUA and only for the duration of the circumstances justifying use of EUAs, the letter noted.
Last year, concerns were raised about off-indication use after interim results from a postapproval study suggested a higher risk for death than seen in premarket studies treated with the temporary heart pump.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration issued an emergency use authorization for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation, Abiomed announced June 1.
“Based on extrapolation of data from the approved indication and reported clinical experience, FDA has concluded that the Impella RP may be effective at providing temporary right ventricular support for the treatment of acute right heart failure or decompensation caused by COVID-19 complications, including PE [pulmonary embolism],” the letter noted.
It cited, for example, use of the temporary heart pump in a 59-year-old woman suffering from COVID-19 who went into right ventricular failure and became hypotensive after an acute PE was removed. After placement of the device, the patient experienced a “dramatic and immediate” improvement in arterial pressure and the device was removed on the fifth day, according to Amir Kaki, MD, and Ted Schreiber, MD, of Ascension St. John Hospital, Detroit, whose review of the case has been posted online.
“Acute pulmonary embolism is clearly being recognized as a life-threatening manifestation of COVID-19. Impella RP is an important tool to help cardiologists save lives during this pandemic,” Dr. Kaki said in the letter. “As we have demonstrated in our series of patients, early recognition of right ventricular dysfunction and early placement of the Impella RP for patients who are hypotensive can be lifesaving.”
Other data cited in support of the Impella RP emergency use authorization (EUA) include a 2019 series of hemodynamically unstable patients with PE in Japan and a 2017 case report of a 47-year-old man with right ventricular failure, profound shock, and a massive PE.
The FDA granted premarket approval of the Impella RP system in 2017 to provide temporary right ventricular support for up to 14 days in patients with a body surface area of at least 1.5 m2 who develop acute right heart failure or decompensation following left ventricular assist device implantation, MI, heart transplant, or open-heart surgery.
The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including PE.
The Impella RP is authorized only for emergency use under the EUA and only for the duration of the circumstances justifying use of EUAs, the letter noted.
Last year, concerns were raised about off-indication use after interim results from a postapproval study suggested a higher risk for death than seen in premarket studies treated with the temporary heart pump.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration issued an emergency use authorization for use of the Impella RP heart pump system in COVID-19 patients with right heart failure or decompensation, Abiomed announced June 1.
“Based on extrapolation of data from the approved indication and reported clinical experience, FDA has concluded that the Impella RP may be effective at providing temporary right ventricular support for the treatment of acute right heart failure or decompensation caused by COVID-19 complications, including PE [pulmonary embolism],” the letter noted.
It cited, for example, use of the temporary heart pump in a 59-year-old woman suffering from COVID-19 who went into right ventricular failure and became hypotensive after an acute PE was removed. After placement of the device, the patient experienced a “dramatic and immediate” improvement in arterial pressure and the device was removed on the fifth day, according to Amir Kaki, MD, and Ted Schreiber, MD, of Ascension St. John Hospital, Detroit, whose review of the case has been posted online.
“Acute pulmonary embolism is clearly being recognized as a life-threatening manifestation of COVID-19. Impella RP is an important tool to help cardiologists save lives during this pandemic,” Dr. Kaki said in the letter. “As we have demonstrated in our series of patients, early recognition of right ventricular dysfunction and early placement of the Impella RP for patients who are hypotensive can be lifesaving.”
Other data cited in support of the Impella RP emergency use authorization (EUA) include a 2019 series of hemodynamically unstable patients with PE in Japan and a 2017 case report of a 47-year-old man with right ventricular failure, profound shock, and a massive PE.
The FDA granted premarket approval of the Impella RP system in 2017 to provide temporary right ventricular support for up to 14 days in patients with a body surface area of at least 1.5 m2 who develop acute right heart failure or decompensation following left ventricular assist device implantation, MI, heart transplant, or open-heart surgery.
The EUA indication for the Impella RP system is to provide temporary right ventricular support for up to 14 days in critical care patients with a body surface area of at least 1.5 m2 for the treatment of acute right heart failure or decompensation caused by complications related to COVID-19, including PE.
The Impella RP is authorized only for emergency use under the EUA and only for the duration of the circumstances justifying use of EUAs, the letter noted.
Last year, concerns were raised about off-indication use after interim results from a postapproval study suggested a higher risk for death than seen in premarket studies treated with the temporary heart pump.
A version of this article originally appeared on Medscape.com.
Distancing works, N95 respirators work better
A study that claims to be the first review of all the available evidence of the effectiveness of physical distancing, face masks, and eye protection to prevent spread of COVID-19 and other respiratory diseases has quantified the effectiveness of these protective measures. The study found that greater physical distancing from an exposed person significantly reduces risk of transmission and that N95 masks, particularly for health care workers, are more effective than other face coverings.
The meta-analysis, published online in The Lancet (2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9) also marks the first evaluation of these protective measures in both community and health care settings for COVID-19, the study authors stated.
“The risk for infection is highly dependent on distance to the individual infected and the type of face mask and eye protection worn,” wrote Derek K. Chu, MD, PhD, of McMaster University in Hamilton, Ont., and colleagues, reporting on behalf of the COVID-19 Systematic Urgent Review Group Effort, or SURGE.
The study reported that physical distancing of at least 1 meter, or about a yard, “seems to be strongly associated with a large protective effect,” but that distancing of 2 meters or about 6 feet could be more effective.
The study involved a systematic review of 172 observational studies across six continents that evaluated distance measures, face masks, and eye protection to prevent transmission between patients with confirmed or probable COVID-19, other severe acute respiratory syndrome (SARS) disease, and Middle East respiratory syndrome (MERS), and their family members, caregivers and health care workers up to May 3, 2020. The meta-analysis involved pooled estimates from 44 comparative studies with 25,697 participants, including seven studies of COVID-19 with 6,674 participants. None of the studies included in the meta-analysis were randomized clinical trials.
A subanalysis of 29 unadjusted and 9 adjusted studies found that the absolute risk of infection in proximity to an exposed individual was 12.8% at 1 m and 2.6% at 2 m. The risk remained constant even when the six COVID-19 studies in this subanalysis were isolated and regardless of being in a health care or non–health-care setting. Each meter of increased distance resulted in a doubling in the change in relative risk (P = .041).
The study also identified what Dr. Chu and colleagues characterized as a “large reduction” in infection risk with the use of both N95 or similar respirators or face masks, with an adjusted risk of infection of 3.1% with a face covering vs. a 17.4% without. The researchers also found a stronger association in health care settings vs. non–health care settings, with a relative risk of 0.3 vs. 0.56, respectively (P = .049). The protective effect of N95 or similar respirators was greater than other masks, with adjusted odds ratios of 0.04 vs. 0.33 (P = .09).
Eye protection was found to reduce the risk of infection to 5.5% vs. 16% without eye protection.
The study also identified potential barriers to social distancing and use of masks and eye protection: discomfort, resource use “linked with potentially decreased equity,” less clear communication, and a perceived lack of empathy on the part of providers toward patients.
Dr. Chu and colleagues wrote that more “high-quality” research, including randomized trials of the optimal physical distance and evaluation of different mask types in non–health care settings “is urgently needed.” They added, “Policymakers at all levels should, therefore, strive to address equity implications for groups with currently limited access to face masks and eye protection.”
The goal of this study was to “inform WHO guidance documents,” the study noted. “Governments and the public health community can use our results to give clear advice for community settings and healthcare workers on these protective measures to reduce infection risk,” said study co-leader Holger Schünemann, MD, MSc, PhD, of McMaster University.
Prof. Raina MacIntyre, MBBS, PhD, head of the biosecurity research program at the Kirby Institute at the University of New South Wales in Sydney, who authored the comment that accompanied the article, said that this study provides evidence for stronger PPE guidelines.
“The Centers for Disease Control and Prevention initially recommended N95s for health workers treating COVID-19 patients, but later downgraded this to surgical masks and even cloth masks and bandannas when there was a supply shortage,” she said. “This study shows that N95s are superior masks and should prompt a review of guidelines that recommend anything less for health workers.”
Recommending anything less than N95 masks for health workers is like sending troops into battle “unarmed or with bows and arrows against a fully armed enemy,” she said. “We are not talking about a device that costs hundreds or thousands of dollars; a N95 costs less than a dollar to produce. All that is needed to address the supply shortage is political will.”
While the study has some shortcomings – namely that it didn’t provide a breakdown of positive tests among COVID-19 participants – it does provide important insight for physicians, Sachin Gupta, MD, a pulmonary and critical care specialist in San Francisco, said in an interview. “The strength of a meta-analysis is that you’re able to get a composite idea; that’s one up side to this,” he said. “They’re confirming what we knew: that distance matters; that more protective masks reduce risk of infection; and that eye protection has an important role.”
Dr. Chu and colleagues have no relevant financial relationships to disclose. One member of SURGE is participating in a clinical trial comparing medical masks and N95 respirators. The World Health Organization provided partial funding for the study.
SOURCE: Chu DK et al. Lancet. 2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9 .
A study that claims to be the first review of all the available evidence of the effectiveness of physical distancing, face masks, and eye protection to prevent spread of COVID-19 and other respiratory diseases has quantified the effectiveness of these protective measures. The study found that greater physical distancing from an exposed person significantly reduces risk of transmission and that N95 masks, particularly for health care workers, are more effective than other face coverings.
The meta-analysis, published online in The Lancet (2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9) also marks the first evaluation of these protective measures in both community and health care settings for COVID-19, the study authors stated.
“The risk for infection is highly dependent on distance to the individual infected and the type of face mask and eye protection worn,” wrote Derek K. Chu, MD, PhD, of McMaster University in Hamilton, Ont., and colleagues, reporting on behalf of the COVID-19 Systematic Urgent Review Group Effort, or SURGE.
The study reported that physical distancing of at least 1 meter, or about a yard, “seems to be strongly associated with a large protective effect,” but that distancing of 2 meters or about 6 feet could be more effective.
The study involved a systematic review of 172 observational studies across six continents that evaluated distance measures, face masks, and eye protection to prevent transmission between patients with confirmed or probable COVID-19, other severe acute respiratory syndrome (SARS) disease, and Middle East respiratory syndrome (MERS), and their family members, caregivers and health care workers up to May 3, 2020. The meta-analysis involved pooled estimates from 44 comparative studies with 25,697 participants, including seven studies of COVID-19 with 6,674 participants. None of the studies included in the meta-analysis were randomized clinical trials.
A subanalysis of 29 unadjusted and 9 adjusted studies found that the absolute risk of infection in proximity to an exposed individual was 12.8% at 1 m and 2.6% at 2 m. The risk remained constant even when the six COVID-19 studies in this subanalysis were isolated and regardless of being in a health care or non–health-care setting. Each meter of increased distance resulted in a doubling in the change in relative risk (P = .041).
The study also identified what Dr. Chu and colleagues characterized as a “large reduction” in infection risk with the use of both N95 or similar respirators or face masks, with an adjusted risk of infection of 3.1% with a face covering vs. a 17.4% without. The researchers also found a stronger association in health care settings vs. non–health care settings, with a relative risk of 0.3 vs. 0.56, respectively (P = .049). The protective effect of N95 or similar respirators was greater than other masks, with adjusted odds ratios of 0.04 vs. 0.33 (P = .09).
Eye protection was found to reduce the risk of infection to 5.5% vs. 16% without eye protection.
The study also identified potential barriers to social distancing and use of masks and eye protection: discomfort, resource use “linked with potentially decreased equity,” less clear communication, and a perceived lack of empathy on the part of providers toward patients.
Dr. Chu and colleagues wrote that more “high-quality” research, including randomized trials of the optimal physical distance and evaluation of different mask types in non–health care settings “is urgently needed.” They added, “Policymakers at all levels should, therefore, strive to address equity implications for groups with currently limited access to face masks and eye protection.”
The goal of this study was to “inform WHO guidance documents,” the study noted. “Governments and the public health community can use our results to give clear advice for community settings and healthcare workers on these protective measures to reduce infection risk,” said study co-leader Holger Schünemann, MD, MSc, PhD, of McMaster University.
Prof. Raina MacIntyre, MBBS, PhD, head of the biosecurity research program at the Kirby Institute at the University of New South Wales in Sydney, who authored the comment that accompanied the article, said that this study provides evidence for stronger PPE guidelines.
“The Centers for Disease Control and Prevention initially recommended N95s for health workers treating COVID-19 patients, but later downgraded this to surgical masks and even cloth masks and bandannas when there was a supply shortage,” she said. “This study shows that N95s are superior masks and should prompt a review of guidelines that recommend anything less for health workers.”
Recommending anything less than N95 masks for health workers is like sending troops into battle “unarmed or with bows and arrows against a fully armed enemy,” she said. “We are not talking about a device that costs hundreds or thousands of dollars; a N95 costs less than a dollar to produce. All that is needed to address the supply shortage is political will.”
While the study has some shortcomings – namely that it didn’t provide a breakdown of positive tests among COVID-19 participants – it does provide important insight for physicians, Sachin Gupta, MD, a pulmonary and critical care specialist in San Francisco, said in an interview. “The strength of a meta-analysis is that you’re able to get a composite idea; that’s one up side to this,” he said. “They’re confirming what we knew: that distance matters; that more protective masks reduce risk of infection; and that eye protection has an important role.”
Dr. Chu and colleagues have no relevant financial relationships to disclose. One member of SURGE is participating in a clinical trial comparing medical masks and N95 respirators. The World Health Organization provided partial funding for the study.
SOURCE: Chu DK et al. Lancet. 2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9 .
A study that claims to be the first review of all the available evidence of the effectiveness of physical distancing, face masks, and eye protection to prevent spread of COVID-19 and other respiratory diseases has quantified the effectiveness of these protective measures. The study found that greater physical distancing from an exposed person significantly reduces risk of transmission and that N95 masks, particularly for health care workers, are more effective than other face coverings.
The meta-analysis, published online in The Lancet (2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9) also marks the first evaluation of these protective measures in both community and health care settings for COVID-19, the study authors stated.
“The risk for infection is highly dependent on distance to the individual infected and the type of face mask and eye protection worn,” wrote Derek K. Chu, MD, PhD, of McMaster University in Hamilton, Ont., and colleagues, reporting on behalf of the COVID-19 Systematic Urgent Review Group Effort, or SURGE.
The study reported that physical distancing of at least 1 meter, or about a yard, “seems to be strongly associated with a large protective effect,” but that distancing of 2 meters or about 6 feet could be more effective.
The study involved a systematic review of 172 observational studies across six continents that evaluated distance measures, face masks, and eye protection to prevent transmission between patients with confirmed or probable COVID-19, other severe acute respiratory syndrome (SARS) disease, and Middle East respiratory syndrome (MERS), and their family members, caregivers and health care workers up to May 3, 2020. The meta-analysis involved pooled estimates from 44 comparative studies with 25,697 participants, including seven studies of COVID-19 with 6,674 participants. None of the studies included in the meta-analysis were randomized clinical trials.
A subanalysis of 29 unadjusted and 9 adjusted studies found that the absolute risk of infection in proximity to an exposed individual was 12.8% at 1 m and 2.6% at 2 m. The risk remained constant even when the six COVID-19 studies in this subanalysis were isolated and regardless of being in a health care or non–health-care setting. Each meter of increased distance resulted in a doubling in the change in relative risk (P = .041).
The study also identified what Dr. Chu and colleagues characterized as a “large reduction” in infection risk with the use of both N95 or similar respirators or face masks, with an adjusted risk of infection of 3.1% with a face covering vs. a 17.4% without. The researchers also found a stronger association in health care settings vs. non–health care settings, with a relative risk of 0.3 vs. 0.56, respectively (P = .049). The protective effect of N95 or similar respirators was greater than other masks, with adjusted odds ratios of 0.04 vs. 0.33 (P = .09).
Eye protection was found to reduce the risk of infection to 5.5% vs. 16% without eye protection.
The study also identified potential barriers to social distancing and use of masks and eye protection: discomfort, resource use “linked with potentially decreased equity,” less clear communication, and a perceived lack of empathy on the part of providers toward patients.
Dr. Chu and colleagues wrote that more “high-quality” research, including randomized trials of the optimal physical distance and evaluation of different mask types in non–health care settings “is urgently needed.” They added, “Policymakers at all levels should, therefore, strive to address equity implications for groups with currently limited access to face masks and eye protection.”
The goal of this study was to “inform WHO guidance documents,” the study noted. “Governments and the public health community can use our results to give clear advice for community settings and healthcare workers on these protective measures to reduce infection risk,” said study co-leader Holger Schünemann, MD, MSc, PhD, of McMaster University.
Prof. Raina MacIntyre, MBBS, PhD, head of the biosecurity research program at the Kirby Institute at the University of New South Wales in Sydney, who authored the comment that accompanied the article, said that this study provides evidence for stronger PPE guidelines.
“The Centers for Disease Control and Prevention initially recommended N95s for health workers treating COVID-19 patients, but later downgraded this to surgical masks and even cloth masks and bandannas when there was a supply shortage,” she said. “This study shows that N95s are superior masks and should prompt a review of guidelines that recommend anything less for health workers.”
Recommending anything less than N95 masks for health workers is like sending troops into battle “unarmed or with bows and arrows against a fully armed enemy,” she said. “We are not talking about a device that costs hundreds or thousands of dollars; a N95 costs less than a dollar to produce. All that is needed to address the supply shortage is political will.”
While the study has some shortcomings – namely that it didn’t provide a breakdown of positive tests among COVID-19 participants – it does provide important insight for physicians, Sachin Gupta, MD, a pulmonary and critical care specialist in San Francisco, said in an interview. “The strength of a meta-analysis is that you’re able to get a composite idea; that’s one up side to this,” he said. “They’re confirming what we knew: that distance matters; that more protective masks reduce risk of infection; and that eye protection has an important role.”
Dr. Chu and colleagues have no relevant financial relationships to disclose. One member of SURGE is participating in a clinical trial comparing medical masks and N95 respirators. The World Health Organization provided partial funding for the study.
SOURCE: Chu DK et al. Lancet. 2020 Jun 2; doi.org/10.1016/ S0140-6736(20)31142-9 .
FROM THE LANCET
Key clinical point: Meta-analysis confirms protective measures reduce risk of spread of COVID-19.
Major finding: Adjusted risk of infection was 3.1% with a face covering vs. 17.4% without.
Study details: Systematic review and meta-analysis of 172 observational studies with 25,697 participants assessing measures to prevent spread of respiratory disease up to May 3, 2020.
Disclosures: Dr. Chu and colleagues have no relevant financial relationships to disclose. One member of SURGE is participating in a clinical trial comparing medical masks and N95 respirators. The study was in part funded by the World Health Organization.
Source: Chu DK et al. Lancet. 2020 Jun 1. doi. org/10.1016/ S0140-6736(20)31142-9.