User login
Clinical Endocrinology News is an independent news source that provides endocrinologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the endocrinologist's practice. Specialty topics include Diabetes, Lipid & Metabolic Disorders Menopause, Obesity, Osteoporosis, Pediatric Endocrinology, Pituitary, Thyroid & Adrenal Disorders, and Reproductive Endocrinology. Featured content includes Commentaries, Implementin Health Reform, Law & Medicine, and In the Loop, the blog of Clinical Endocrinology News. Clinical Endocrinology News is owned by Frontline Medical Communications.
addict
addicted
addicting
addiction
adult sites
alcohol
antibody
ass
attorney
audit
auditor
babies
babpa
baby
ban
banned
banning
best
bisexual
bitch
bleach
blog
blow job
bondage
boobs
booty
buy
cannabis
certificate
certification
certified
cheap
cheapest
class action
cocaine
cock
counterfeit drug
crack
crap
crime
criminal
cunt
curable
cure
dangerous
dangers
dead
deadly
death
defend
defended
depedent
dependence
dependent
detergent
dick
die
dildo
drug abuse
drug recall
dying
fag
fake
fatal
fatalities
fatality
free
fuck
gangs
gingivitis
guns
hardcore
herbal
herbs
heroin
herpes
home remedies
homo
horny
hypersensitivity
hypoglycemia treatment
illegal drug use
illegal use of prescription
incest
infant
infants
job
ketoacidosis
kill
killer
killing
kinky
law suit
lawsuit
lawyer
lesbian
marijuana
medicine for hypoglycemia
murder
naked
natural
newborn
nigger
noise
nude
nudity
orgy
over the counter
overdosage
overdose
overdosed
overdosing
penis
pimp
pistol
porn
porno
pornographic
pornography
prison
profanity
purchase
purchasing
pussy
queer
rape
rapist
recall
recreational drug
rob
robberies
sale
sales
sex
sexual
shit
shoot
slut
slutty
stole
stolen
store
sue
suicidal
suicide
supplements
supply company
theft
thief
thieves
tit
toddler
toddlers
toxic
toxin
tragedy
treating dka
treating hypoglycemia
treatment for hypoglycemia
vagina
violence
whore
withdrawal
without prescription
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-imn')]
div[contains(@class, 'pane-pub-home-imn')]
div[contains(@class, 'pane-pub-topic-imn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
One of the keys to success on social media? Entertain and educate the public
Social media isn’t everyone’s cup of tea, but

“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
Social media isn’t everyone’s cup of tea, but
“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
Social media isn’t everyone’s cup of tea, but
“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
Why kids might reject sugar-free Halloween candy
Trick-or-treaters may not be so easily tricked into loving sugar-free treats, thanks to taste buds hard-wired to seek calorie-containing sweets, a new study suggests.
Taste isn’t all about choosing peanut butter cups over jelly beans. Since earliest humanity, our sense of taste has helped us detect salty, sweet, sour, savory, and bitter so that we can choose foods high in energy and low in poisons.
But these new findings suggest that our taste buds have another hidden talent: identifying foods that don’t give us any energy at all.
Scientists suspected this ability after research in mice showed that their taste buds could distinguish between sugar and calorie-free artificial sweeteners.
To test this possibility in humans, scientists asked people to drink a series of clear beverages and identify whether they were plain water or sweetened. The goal was to compare how people responded to glucose – a natural caloric sweetener in fruits, honey, and table sugar – and sucralose, a calorie-free artificial sweetener.
All participants wore nose plugs, ensuring that they would use only their taste buds and not their sense of smell for detection.
As expected, people could easily tell plain water from sweetened drinks, whether with glucose or sucralose, confirming that taste buds detect sweetness.
In a twist, researchers then mixed in flavorless chemicals that block taste buds from picking up sweetness. With these drinks, people could no longer distinguish sucralose-sweetened beverages from plain water. But they could still tell when they had a beverage sweetened with glucose.
This finding indicates that two separate pathways underlie the mouth’s response to sugar, researchers report in PLOS One. The first pathway identifies sweet flavors, and the second one detects foods that contain energy that can be used for fuel.
Scientists might one day come up with calorie-free sweets that trick taste buds into detecting the presence of calories, enhancing their appeal. But in the lab studies, the participants had no visual cues or smell to guide their reactions, meaning how these other sensory inputs would affect treat perception isn’t known.
A version of this article first appeared on WebMD.com.
Trick-or-treaters may not be so easily tricked into loving sugar-free treats, thanks to taste buds hard-wired to seek calorie-containing sweets, a new study suggests.
Taste isn’t all about choosing peanut butter cups over jelly beans. Since earliest humanity, our sense of taste has helped us detect salty, sweet, sour, savory, and bitter so that we can choose foods high in energy and low in poisons.
But these new findings suggest that our taste buds have another hidden talent: identifying foods that don’t give us any energy at all.
Scientists suspected this ability after research in mice showed that their taste buds could distinguish between sugar and calorie-free artificial sweeteners.
To test this possibility in humans, scientists asked people to drink a series of clear beverages and identify whether they were plain water or sweetened. The goal was to compare how people responded to glucose – a natural caloric sweetener in fruits, honey, and table sugar – and sucralose, a calorie-free artificial sweetener.
All participants wore nose plugs, ensuring that they would use only their taste buds and not their sense of smell for detection.
As expected, people could easily tell plain water from sweetened drinks, whether with glucose or sucralose, confirming that taste buds detect sweetness.
In a twist, researchers then mixed in flavorless chemicals that block taste buds from picking up sweetness. With these drinks, people could no longer distinguish sucralose-sweetened beverages from plain water. But they could still tell when they had a beverage sweetened with glucose.
This finding indicates that two separate pathways underlie the mouth’s response to sugar, researchers report in PLOS One. The first pathway identifies sweet flavors, and the second one detects foods that contain energy that can be used for fuel.
Scientists might one day come up with calorie-free sweets that trick taste buds into detecting the presence of calories, enhancing their appeal. But in the lab studies, the participants had no visual cues or smell to guide their reactions, meaning how these other sensory inputs would affect treat perception isn’t known.
A version of this article first appeared on WebMD.com.
Trick-or-treaters may not be so easily tricked into loving sugar-free treats, thanks to taste buds hard-wired to seek calorie-containing sweets, a new study suggests.
Taste isn’t all about choosing peanut butter cups over jelly beans. Since earliest humanity, our sense of taste has helped us detect salty, sweet, sour, savory, and bitter so that we can choose foods high in energy and low in poisons.
But these new findings suggest that our taste buds have another hidden talent: identifying foods that don’t give us any energy at all.
Scientists suspected this ability after research in mice showed that their taste buds could distinguish between sugar and calorie-free artificial sweeteners.
To test this possibility in humans, scientists asked people to drink a series of clear beverages and identify whether they were plain water or sweetened. The goal was to compare how people responded to glucose – a natural caloric sweetener in fruits, honey, and table sugar – and sucralose, a calorie-free artificial sweetener.
All participants wore nose plugs, ensuring that they would use only their taste buds and not their sense of smell for detection.
As expected, people could easily tell plain water from sweetened drinks, whether with glucose or sucralose, confirming that taste buds detect sweetness.
In a twist, researchers then mixed in flavorless chemicals that block taste buds from picking up sweetness. With these drinks, people could no longer distinguish sucralose-sweetened beverages from plain water. But they could still tell when they had a beverage sweetened with glucose.
This finding indicates that two separate pathways underlie the mouth’s response to sugar, researchers report in PLOS One. The first pathway identifies sweet flavors, and the second one detects foods that contain energy that can be used for fuel.
Scientists might one day come up with calorie-free sweets that trick taste buds into detecting the presence of calories, enhancing their appeal. But in the lab studies, the participants had no visual cues or smell to guide their reactions, meaning how these other sensory inputs would affect treat perception isn’t known.
A version of this article first appeared on WebMD.com.
SGLT2 inhibitors for diabetes: No link to fractures in older adults
Use of sodium-glucose cotransporter-2 (SGLT2) inhibitors does not appear to raise the risk for fractures in older adults, new research suggests.
The data come from a nationwide propensity score-matched study of U.S. Medicare recipients with type 2 diabetes who were new users of either an SGLT2 inhibitor, a dipeptidyl peptidase 4 (DPP-4) inhibitor, or a glucagon-like peptide (GLP-1) receptor agonist.
“The use of SGLT2 inhibitors was not associated with an increased risk of nontraumatic fractures compared with DPP-4 inhibitors or GLP-1 agonists. Results were consistent across categories of sex, frailty, age, and insulin use,” say Min Zhuo, MD, of Harvard Medical School, Boston, and colleagues, who published their work online October 27 in JAMA Network Open.
“Our results add to the evidence base evaluating the safety profile of SGLT2 inhibitors in older adults outside of [randomized controlled trials] and further characterize the risk-benefit balance of SGLT2 inhibitors in clinical practice,” they write.
Asked to comment, Simeon I. Taylor, MD, PhD, told this news organization, “This is a high-quality study that is generally reassuring that relatively short, less than 1 year, treatment with an SGLT2 inhibitor does not appear to significantly increase the risk of bone fractures.”
However, Dr. Taylor, of the Division of Endocrinology, Diabetes, and Nutrition, University of Maryland School of Medicine, Baltimore, also noted: “Notwithstanding these reassuring data, the paper also does a good job of pointing out important limitations.”
“Most importantly, these data do not address questions related to the risk of long-term chronic therapy. It is instructive to refer back to the published data demonstrating an approximately 2-year lag before a significant increase in the risk of fracture was observed in rosiglitazone-treated patients in the ADOPT study. The length of the lag is likely related to the baseline bone mineral density at the time drug therapy is initiated. These considerations may contribute to the observed variation in bone-related outcomes in different studies.”
Concern about SGLT2 inhibitors and fractures first arose in 2017 from the CANVAS study, in which the overall fracture risk with canagliflozin was a significant 26% higher than placebo. However, subsequent larger randomized trials of canagliflozin and other SGLT2 inhibitors did not find the same risk.
In addition, previous observational studies in younger adults have also not found use of SGLT2 inhibitors to be associated with increased fracture risk compared with DPP-4 inhibitors or GLP-1 agonists.
Understanding fracture risk with SGLT2 inhibitors is ‘critical’
Older adults with type 2 diabetes may benefit from reductions in atherosclerotic cardiovascular events, hospitalization for heart failure, end-stage kidney disease, and death associated with SGLT2 inhibitors, but the fact that aging may have negative effects on bone metabolism means “understanding the fracture risk associated with SGLT2 inhibitors in older adults with type 2 diabetes is critical,” say Dr. Zhuo and colleagues.
In the current study, they analyzed claims data for Medicare beneficiaries aged 66 years and older (1 year past Medicare eligibility) who were newly prescribed an SGLT2 inhibitor, DPP-4 inhibitor, or GLP-1 agonist between April 1, 2013 and Dec. 31, 2017.
A total of 45,889 patients from each treatment group were propensity-matched using 58 baseline characteristics, for a total of 137,667 patients.
After matching, there were 501 events of the primary composite outcome (nontraumatic pelvic fracture, hip fracture requiring surgery, or humerus, radius, or ulna fracture requiring intervention) within 30 days. By treatment group, fracture rates per 1,000 person-years were 4.69, 5.26, and 4.71 for SGLT2 inhibitors, DPP-4 inhibitors, and GLP-1 agonists respectively.
The differences between patients taking DPP-4 inhibitors or GLP-1 agonists compared with SGLT2 inhibitors were not significant, with hazard ratios of 0.90 and 1.00, respectively.
Results remained consistent in various sensitivity and subgroup analyses, including limiting the data to just the canagliflozin group. Overall, the fracture rate was greater with female sex, frailty, older age, and insulin use, consistent across drug classes.
The risks for falls and hypoglycemia were lower in the SGLT2 inhibitor versus matched DPP-4 inhibitor groups (hazard ratio, 0.82), and there was no difference in syncope. None of those differences were significant for the SGLT2 inhibitor group compared with the GLP-1 agonist group.
Consistent with previous data, the risk for diabetic ketoacidosis was higher with SGLT2 inhibitors versus DPP-4 inhibitors and GLP-1 agonists (HR, 1.29 and 1.58), and the risk for heart failure hospitalization was lower (HR, 0.42 and 0.69).
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, Harvard Medical School. Dr. Zhuo was supported by the National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Taylor is a consultant for Ionis Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Use of sodium-glucose cotransporter-2 (SGLT2) inhibitors does not appear to raise the risk for fractures in older adults, new research suggests.
The data come from a nationwide propensity score-matched study of U.S. Medicare recipients with type 2 diabetes who were new users of either an SGLT2 inhibitor, a dipeptidyl peptidase 4 (DPP-4) inhibitor, or a glucagon-like peptide (GLP-1) receptor agonist.
“The use of SGLT2 inhibitors was not associated with an increased risk of nontraumatic fractures compared with DPP-4 inhibitors or GLP-1 agonists. Results were consistent across categories of sex, frailty, age, and insulin use,” say Min Zhuo, MD, of Harvard Medical School, Boston, and colleagues, who published their work online October 27 in JAMA Network Open.
“Our results add to the evidence base evaluating the safety profile of SGLT2 inhibitors in older adults outside of [randomized controlled trials] and further characterize the risk-benefit balance of SGLT2 inhibitors in clinical practice,” they write.
Asked to comment, Simeon I. Taylor, MD, PhD, told this news organization, “This is a high-quality study that is generally reassuring that relatively short, less than 1 year, treatment with an SGLT2 inhibitor does not appear to significantly increase the risk of bone fractures.”
However, Dr. Taylor, of the Division of Endocrinology, Diabetes, and Nutrition, University of Maryland School of Medicine, Baltimore, also noted: “Notwithstanding these reassuring data, the paper also does a good job of pointing out important limitations.”
“Most importantly, these data do not address questions related to the risk of long-term chronic therapy. It is instructive to refer back to the published data demonstrating an approximately 2-year lag before a significant increase in the risk of fracture was observed in rosiglitazone-treated patients in the ADOPT study. The length of the lag is likely related to the baseline bone mineral density at the time drug therapy is initiated. These considerations may contribute to the observed variation in bone-related outcomes in different studies.”
Concern about SGLT2 inhibitors and fractures first arose in 2017 from the CANVAS study, in which the overall fracture risk with canagliflozin was a significant 26% higher than placebo. However, subsequent larger randomized trials of canagliflozin and other SGLT2 inhibitors did not find the same risk.
In addition, previous observational studies in younger adults have also not found use of SGLT2 inhibitors to be associated with increased fracture risk compared with DPP-4 inhibitors or GLP-1 agonists.
Understanding fracture risk with SGLT2 inhibitors is ‘critical’
Older adults with type 2 diabetes may benefit from reductions in atherosclerotic cardiovascular events, hospitalization for heart failure, end-stage kidney disease, and death associated with SGLT2 inhibitors, but the fact that aging may have negative effects on bone metabolism means “understanding the fracture risk associated with SGLT2 inhibitors in older adults with type 2 diabetes is critical,” say Dr. Zhuo and colleagues.
In the current study, they analyzed claims data for Medicare beneficiaries aged 66 years and older (1 year past Medicare eligibility) who were newly prescribed an SGLT2 inhibitor, DPP-4 inhibitor, or GLP-1 agonist between April 1, 2013 and Dec. 31, 2017.
A total of 45,889 patients from each treatment group were propensity-matched using 58 baseline characteristics, for a total of 137,667 patients.
After matching, there were 501 events of the primary composite outcome (nontraumatic pelvic fracture, hip fracture requiring surgery, or humerus, radius, or ulna fracture requiring intervention) within 30 days. By treatment group, fracture rates per 1,000 person-years were 4.69, 5.26, and 4.71 for SGLT2 inhibitors, DPP-4 inhibitors, and GLP-1 agonists respectively.
The differences between patients taking DPP-4 inhibitors or GLP-1 agonists compared with SGLT2 inhibitors were not significant, with hazard ratios of 0.90 and 1.00, respectively.
Results remained consistent in various sensitivity and subgroup analyses, including limiting the data to just the canagliflozin group. Overall, the fracture rate was greater with female sex, frailty, older age, and insulin use, consistent across drug classes.
The risks for falls and hypoglycemia were lower in the SGLT2 inhibitor versus matched DPP-4 inhibitor groups (hazard ratio, 0.82), and there was no difference in syncope. None of those differences were significant for the SGLT2 inhibitor group compared with the GLP-1 agonist group.
Consistent with previous data, the risk for diabetic ketoacidosis was higher with SGLT2 inhibitors versus DPP-4 inhibitors and GLP-1 agonists (HR, 1.29 and 1.58), and the risk for heart failure hospitalization was lower (HR, 0.42 and 0.69).
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, Harvard Medical School. Dr. Zhuo was supported by the National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Taylor is a consultant for Ionis Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Use of sodium-glucose cotransporter-2 (SGLT2) inhibitors does not appear to raise the risk for fractures in older adults, new research suggests.
The data come from a nationwide propensity score-matched study of U.S. Medicare recipients with type 2 diabetes who were new users of either an SGLT2 inhibitor, a dipeptidyl peptidase 4 (DPP-4) inhibitor, or a glucagon-like peptide (GLP-1) receptor agonist.
“The use of SGLT2 inhibitors was not associated with an increased risk of nontraumatic fractures compared with DPP-4 inhibitors or GLP-1 agonists. Results were consistent across categories of sex, frailty, age, and insulin use,” say Min Zhuo, MD, of Harvard Medical School, Boston, and colleagues, who published their work online October 27 in JAMA Network Open.
“Our results add to the evidence base evaluating the safety profile of SGLT2 inhibitors in older adults outside of [randomized controlled trials] and further characterize the risk-benefit balance of SGLT2 inhibitors in clinical practice,” they write.
Asked to comment, Simeon I. Taylor, MD, PhD, told this news organization, “This is a high-quality study that is generally reassuring that relatively short, less than 1 year, treatment with an SGLT2 inhibitor does not appear to significantly increase the risk of bone fractures.”
However, Dr. Taylor, of the Division of Endocrinology, Diabetes, and Nutrition, University of Maryland School of Medicine, Baltimore, also noted: “Notwithstanding these reassuring data, the paper also does a good job of pointing out important limitations.”
“Most importantly, these data do not address questions related to the risk of long-term chronic therapy. It is instructive to refer back to the published data demonstrating an approximately 2-year lag before a significant increase in the risk of fracture was observed in rosiglitazone-treated patients in the ADOPT study. The length of the lag is likely related to the baseline bone mineral density at the time drug therapy is initiated. These considerations may contribute to the observed variation in bone-related outcomes in different studies.”
Concern about SGLT2 inhibitors and fractures first arose in 2017 from the CANVAS study, in which the overall fracture risk with canagliflozin was a significant 26% higher than placebo. However, subsequent larger randomized trials of canagliflozin and other SGLT2 inhibitors did not find the same risk.
In addition, previous observational studies in younger adults have also not found use of SGLT2 inhibitors to be associated with increased fracture risk compared with DPP-4 inhibitors or GLP-1 agonists.
Understanding fracture risk with SGLT2 inhibitors is ‘critical’
Older adults with type 2 diabetes may benefit from reductions in atherosclerotic cardiovascular events, hospitalization for heart failure, end-stage kidney disease, and death associated with SGLT2 inhibitors, but the fact that aging may have negative effects on bone metabolism means “understanding the fracture risk associated with SGLT2 inhibitors in older adults with type 2 diabetes is critical,” say Dr. Zhuo and colleagues.
In the current study, they analyzed claims data for Medicare beneficiaries aged 66 years and older (1 year past Medicare eligibility) who were newly prescribed an SGLT2 inhibitor, DPP-4 inhibitor, or GLP-1 agonist between April 1, 2013 and Dec. 31, 2017.
A total of 45,889 patients from each treatment group were propensity-matched using 58 baseline characteristics, for a total of 137,667 patients.
After matching, there were 501 events of the primary composite outcome (nontraumatic pelvic fracture, hip fracture requiring surgery, or humerus, radius, or ulna fracture requiring intervention) within 30 days. By treatment group, fracture rates per 1,000 person-years were 4.69, 5.26, and 4.71 for SGLT2 inhibitors, DPP-4 inhibitors, and GLP-1 agonists respectively.
The differences between patients taking DPP-4 inhibitors or GLP-1 agonists compared with SGLT2 inhibitors were not significant, with hazard ratios of 0.90 and 1.00, respectively.
Results remained consistent in various sensitivity and subgroup analyses, including limiting the data to just the canagliflozin group. Overall, the fracture rate was greater with female sex, frailty, older age, and insulin use, consistent across drug classes.
The risks for falls and hypoglycemia were lower in the SGLT2 inhibitor versus matched DPP-4 inhibitor groups (hazard ratio, 0.82), and there was no difference in syncope. None of those differences were significant for the SGLT2 inhibitor group compared with the GLP-1 agonist group.
Consistent with previous data, the risk for diabetic ketoacidosis was higher with SGLT2 inhibitors versus DPP-4 inhibitors and GLP-1 agonists (HR, 1.29 and 1.58), and the risk for heart failure hospitalization was lower (HR, 0.42 and 0.69).
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, Harvard Medical School. Dr. Zhuo was supported by the National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Taylor is a consultant for Ionis Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Nondiabetes hospitalization is wrong time to up diabetes meds
“Short-term hospitalization [for reasons other than diabetes] may not be the time to intervene in long-term diabetes management,” researchers conclude.
They found that, in a national cohort of older almost entirely male veterans with non–insulin-treated type 2 diabetes who were hospitalized for non–diabetes-related common medical conditions, intensified diabetes treatment on hospital discharge was linked to an increased risk of severe hypoglycemia in the immediate postdischarge period.
However, diabetes treatment intensification – that is, receiving a prescription for a new or higher dose of diabetes medicine – was not associated with decreased risks of severe hyperglycemia or with improved glycemic (hemoglobin A1c) control at 30 days or 1 year, according to study results, published in JAMA Network Open.
“We didn’t see a reduction in diabetes emergencies in more intensively treated patients,” lead investigator Timothy S. Anderson, MD, said in an interview.
Also, importantly, there was a low rate of persistence with the new treatment. “Half of the patients were no longer taking these [intensified diabetes medicines] at 1 year, which tells me that context is key,” he pointed out. “If a patient is in the hospital for diabetes [unlike the patients in this study], I think it makes a lot of sense to modify and adjust their regimen to try to help them right then and there.”
The overall risk of severe hyperglycemia or severe hypoglycemia was pretty small in the overall cohort, Dr. Anderson noted, “but we do put people at risk of leaving the hospital and ending up back in the hospital with low blood sugar when we intensify medications, and there’s not necessarily a good signal to suggest that it’s all that urgent to change these medicines.”
Instead, the “safer path” may be to make recommendations to the patient’s outpatient physician and also inform the patient – for example, “We saw some concerns about your diabetes while you were in the hospital, and this is really something that should be looked at when you’re recovered and feeling better from the rest of your health standpoint” – rather than making a diabetes medication change while the person is acutely ill or recovering from illness, said Dr. Anderson, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston.
The researchers also found an “unexpected” significant decrease in 30-day mortality in the patients with intensified diabetes treatment, which was probably because of confounding that was not accounted for, Dr. Anderson speculated, since clinical trials have consistently shown that benefits from diabetes medications take a longer time to show an effect.
‘Important study,’ but lacked newer meds
This is an “important” study for primary care and in-hospital physicians that shows that “hospitalization is really not the time and the place” to intensify diabetes medication, Rozalina G. McCoy, MD, coauthor of an invited commentary, told this news organization in an interview.
“While overcoming treatment inertia is important, [it should be] done appropriately, so that we don’t overtreat patients,” Dr. McCoy, of the Mayo Clinic in Rochester, Minn., stressed.
The very low rate of persistence of taking intensified medications is a major finding, she agreed. Hospitalized patients “are not in their usual state of health, so if we make long-term treatment decisions based on their acute abnormal situation, that may not be appropriate.”
However, patients with high A1c may benefit from a change at hospital discharge rather than when they see their primary care provider, with the caveat that they need close follow-up as an outpatient.
The study emphasizes the “need for longitudinal patient care rather than episodic patches,” according to Dr. McCoy.
For example, a patient who is hospitalized for a chronic obstructive pulmonary disease or asthma exacerbation may be receiving steroids that cause high blood glucose levels but as soon as they’re done with their steroid course, blood glucose will decrease, so the “need for close outpatient follow-up is very important.”
One limitation of the current work is that an earlier study in the same population by the research group showed that 49% of patients whose treatment regimens were intensified had limited life expectancy or were at or below their A1c goal, so they would not have benefited from the stepped-up treatment, she noted.
Another limitation is that the findings cannot be generalized to women or younger patients, or to patients treated with glucagonlike peptide 1 (GLP-1)–receptor agonists or sodium-glucose cotransporter 2 (SGLT2) inhibitors.
The study patients were seen in the U.S. Veterans Health Administration health system when these newer agents were not used. Three-quarters of patients received intensified treatment with sulfonylurea or insulin, and only one patient received a new GLP-1–receptor agonist.
Ideally, Dr. McCoy said, patients should have been prescribed a GLP-1–receptor agonist if they had atherosclerotic cardiovascular disease or kidney disease, or an SGLT2 inhibitor if they had kidney disease or heart failure, which may have led to different results, and would need to be determined in further study.
Dr. Anderson agreed that “SGLT2 inhibitors and GLP1 agonists are broadly much safer than the older diabetes medicines, at least when it comes to risk of hypoglycemia, and may have more clear benefits in heart disease and mortality. So I would not want to extrapolate our findings to those new classes,” he said. “A similar set of studies would need to be done.”
Study rationale and findings
Hospitalized older adults with diabetes commonly have transiently elevated blood glucose levels that might lead clinicians to discharge them from hospital with a prescription for more intensive diabetes medications than they were on before they were hospitalized, but it is not clear if these diabetes medication changes would improve outcomes.
To investigate this, the researchers analyzed data from patients with diabetes who were 65 and older and hospitalized for common medical conditions in VHA hospitals during January 2011–September 2016, and then discharged to the community.
They excluded patients who were hospitalized for things that require immediate change in diabetes treatment and patients who were using insulin before their hospitalization (because instructions to modify insulin dosing frequently don’t have a new prescription).
The researchers identified 28,198 adults with diabetes who were not on insulin and were hospitalized in the VHA health system for heart failure (18%), coronary artery disease (13%), chronic obstructive pulmonary disease (10%), pneumonia (9.6%), and urinary tract infection (7.5%), and less often and not in decreasing order, for acute coronary syndrome, arrhythmia, asthma, chest pain, conduction disorders, heart valve disorders, sepsis, skin infection, stroke, and transient ischemic attack.
Of these patients, 2,768 patients (9.8%) received diabetes medication intensification, and the researchers matched 2,648 of these patients with an equal number of patients who did not receive this treatment intensification.
The patients in each group had a mean age of 73 and 98.5% were male; 78% were White.
They had a mean A1c of 7.9%. Most were receiving sulfonylurea (43%) or metformin (39%), and few were receiving thiazolidinediones (4.1%), alpha-glucosidase inhibitors (2.7%), dipeptidyl peptidase 4 inhibitors (2.0%), or other types of diabetes drugs (0.1%).
Of the 2,768 patients who received intensified diabetes medication, most received a prescription for insulin (51%) or sulfonylurea (23%).
In the propensity-matched cohort, patients with intensified diabetes medication had a higher rate of severe hypoglycemia at 30 days (1% vs. 0.5%), which translated into a significant twofold higher risk (hazard ratio, 2.17).
The rates of severe hypoglycemia at 1 year were similar in both groups (3.1% and 2.9%).
The incidence of severe hyperglycemia was the same in both groups at 30 days (0.3%) and 1 year (1.3%).
In secondary outcomes, at 1 year, 48% of new oral diabetes medications and 39% of new insulin prescriptions were no longer being filled.
Overall, patients who were discharged with intensified diabetes medication were significantly less likely to die within 30 days than the other patients (1.3% vs. 2.4%; HR, 0.55).
However, this mortality benefit was found only in the subgroup of 2,524 patients who had uncontrolled diabetes when they were admitted to hospital (A1c >7.5%; mean A1c, 9.1%), and not in the propensity-matched subgroup of 2,672 patients who had controlled diabetes then (A1c up to 7.5%; mean A1c, 6.8%).
There was no significant difference in 1-year mortality in patients with versus without intensified treatment (15.8% vs. 17.8%).
There were also no significant between-group difference in rates of hospital readmission at 30 days (roughly 17%) or 1 year (roughly 51%).
The decreases in mean A1c from hospital discharge to 1 year later were also the same in both groups (going from 7.9% to 7.7%).
The study was funded by grants from the National Institute on Aging and the American College of Cardiology. Dr. Anderson has no relevant financial disclosures. Dr. McCoy reported receiving grants from the National Institute of Diabetes and Digestive and Kidney Diseases, AARP, and the Patient-Centered Outcomes Research Institute outside the submitted work. The disclosures of the other authors and the editorial coauthor are available with the article and commentary.
“Short-term hospitalization [for reasons other than diabetes] may not be the time to intervene in long-term diabetes management,” researchers conclude.
They found that, in a national cohort of older almost entirely male veterans with non–insulin-treated type 2 diabetes who were hospitalized for non–diabetes-related common medical conditions, intensified diabetes treatment on hospital discharge was linked to an increased risk of severe hypoglycemia in the immediate postdischarge period.
However, diabetes treatment intensification – that is, receiving a prescription for a new or higher dose of diabetes medicine – was not associated with decreased risks of severe hyperglycemia or with improved glycemic (hemoglobin A1c) control at 30 days or 1 year, according to study results, published in JAMA Network Open.
“We didn’t see a reduction in diabetes emergencies in more intensively treated patients,” lead investigator Timothy S. Anderson, MD, said in an interview.
Also, importantly, there was a low rate of persistence with the new treatment. “Half of the patients were no longer taking these [intensified diabetes medicines] at 1 year, which tells me that context is key,” he pointed out. “If a patient is in the hospital for diabetes [unlike the patients in this study], I think it makes a lot of sense to modify and adjust their regimen to try to help them right then and there.”
The overall risk of severe hyperglycemia or severe hypoglycemia was pretty small in the overall cohort, Dr. Anderson noted, “but we do put people at risk of leaving the hospital and ending up back in the hospital with low blood sugar when we intensify medications, and there’s not necessarily a good signal to suggest that it’s all that urgent to change these medicines.”
Instead, the “safer path” may be to make recommendations to the patient’s outpatient physician and also inform the patient – for example, “We saw some concerns about your diabetes while you were in the hospital, and this is really something that should be looked at when you’re recovered and feeling better from the rest of your health standpoint” – rather than making a diabetes medication change while the person is acutely ill or recovering from illness, said Dr. Anderson, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston.
The researchers also found an “unexpected” significant decrease in 30-day mortality in the patients with intensified diabetes treatment, which was probably because of confounding that was not accounted for, Dr. Anderson speculated, since clinical trials have consistently shown that benefits from diabetes medications take a longer time to show an effect.
‘Important study,’ but lacked newer meds
This is an “important” study for primary care and in-hospital physicians that shows that “hospitalization is really not the time and the place” to intensify diabetes medication, Rozalina G. McCoy, MD, coauthor of an invited commentary, told this news organization in an interview.
“While overcoming treatment inertia is important, [it should be] done appropriately, so that we don’t overtreat patients,” Dr. McCoy, of the Mayo Clinic in Rochester, Minn., stressed.
The very low rate of persistence of taking intensified medications is a major finding, she agreed. Hospitalized patients “are not in their usual state of health, so if we make long-term treatment decisions based on their acute abnormal situation, that may not be appropriate.”
However, patients with high A1c may benefit from a change at hospital discharge rather than when they see their primary care provider, with the caveat that they need close follow-up as an outpatient.
The study emphasizes the “need for longitudinal patient care rather than episodic patches,” according to Dr. McCoy.
For example, a patient who is hospitalized for a chronic obstructive pulmonary disease or asthma exacerbation may be receiving steroids that cause high blood glucose levels but as soon as they’re done with their steroid course, blood glucose will decrease, so the “need for close outpatient follow-up is very important.”
One limitation of the current work is that an earlier study in the same population by the research group showed that 49% of patients whose treatment regimens were intensified had limited life expectancy or were at or below their A1c goal, so they would not have benefited from the stepped-up treatment, she noted.
Another limitation is that the findings cannot be generalized to women or younger patients, or to patients treated with glucagonlike peptide 1 (GLP-1)–receptor agonists or sodium-glucose cotransporter 2 (SGLT2) inhibitors.
The study patients were seen in the U.S. Veterans Health Administration health system when these newer agents were not used. Three-quarters of patients received intensified treatment with sulfonylurea or insulin, and only one patient received a new GLP-1–receptor agonist.
Ideally, Dr. McCoy said, patients should have been prescribed a GLP-1–receptor agonist if they had atherosclerotic cardiovascular disease or kidney disease, or an SGLT2 inhibitor if they had kidney disease or heart failure, which may have led to different results, and would need to be determined in further study.
Dr. Anderson agreed that “SGLT2 inhibitors and GLP1 agonists are broadly much safer than the older diabetes medicines, at least when it comes to risk of hypoglycemia, and may have more clear benefits in heart disease and mortality. So I would not want to extrapolate our findings to those new classes,” he said. “A similar set of studies would need to be done.”
Study rationale and findings
Hospitalized older adults with diabetes commonly have transiently elevated blood glucose levels that might lead clinicians to discharge them from hospital with a prescription for more intensive diabetes medications than they were on before they were hospitalized, but it is not clear if these diabetes medication changes would improve outcomes.
To investigate this, the researchers analyzed data from patients with diabetes who were 65 and older and hospitalized for common medical conditions in VHA hospitals during January 2011–September 2016, and then discharged to the community.
They excluded patients who were hospitalized for things that require immediate change in diabetes treatment and patients who were using insulin before their hospitalization (because instructions to modify insulin dosing frequently don’t have a new prescription).
The researchers identified 28,198 adults with diabetes who were not on insulin and were hospitalized in the VHA health system for heart failure (18%), coronary artery disease (13%), chronic obstructive pulmonary disease (10%), pneumonia (9.6%), and urinary tract infection (7.5%), and less often and not in decreasing order, for acute coronary syndrome, arrhythmia, asthma, chest pain, conduction disorders, heart valve disorders, sepsis, skin infection, stroke, and transient ischemic attack.
Of these patients, 2,768 patients (9.8%) received diabetes medication intensification, and the researchers matched 2,648 of these patients with an equal number of patients who did not receive this treatment intensification.
The patients in each group had a mean age of 73 and 98.5% were male; 78% were White.
They had a mean A1c of 7.9%. Most were receiving sulfonylurea (43%) or metformin (39%), and few were receiving thiazolidinediones (4.1%), alpha-glucosidase inhibitors (2.7%), dipeptidyl peptidase 4 inhibitors (2.0%), or other types of diabetes drugs (0.1%).
Of the 2,768 patients who received intensified diabetes medication, most received a prescription for insulin (51%) or sulfonylurea (23%).
In the propensity-matched cohort, patients with intensified diabetes medication had a higher rate of severe hypoglycemia at 30 days (1% vs. 0.5%), which translated into a significant twofold higher risk (hazard ratio, 2.17).
The rates of severe hypoglycemia at 1 year were similar in both groups (3.1% and 2.9%).
The incidence of severe hyperglycemia was the same in both groups at 30 days (0.3%) and 1 year (1.3%).
In secondary outcomes, at 1 year, 48% of new oral diabetes medications and 39% of new insulin prescriptions were no longer being filled.
Overall, patients who were discharged with intensified diabetes medication were significantly less likely to die within 30 days than the other patients (1.3% vs. 2.4%; HR, 0.55).
However, this mortality benefit was found only in the subgroup of 2,524 patients who had uncontrolled diabetes when they were admitted to hospital (A1c >7.5%; mean A1c, 9.1%), and not in the propensity-matched subgroup of 2,672 patients who had controlled diabetes then (A1c up to 7.5%; mean A1c, 6.8%).
There was no significant difference in 1-year mortality in patients with versus without intensified treatment (15.8% vs. 17.8%).
There were also no significant between-group difference in rates of hospital readmission at 30 days (roughly 17%) or 1 year (roughly 51%).
The decreases in mean A1c from hospital discharge to 1 year later were also the same in both groups (going from 7.9% to 7.7%).
The study was funded by grants from the National Institute on Aging and the American College of Cardiology. Dr. Anderson has no relevant financial disclosures. Dr. McCoy reported receiving grants from the National Institute of Diabetes and Digestive and Kidney Diseases, AARP, and the Patient-Centered Outcomes Research Institute outside the submitted work. The disclosures of the other authors and the editorial coauthor are available with the article and commentary.
“Short-term hospitalization [for reasons other than diabetes] may not be the time to intervene in long-term diabetes management,” researchers conclude.
They found that, in a national cohort of older almost entirely male veterans with non–insulin-treated type 2 diabetes who were hospitalized for non–diabetes-related common medical conditions, intensified diabetes treatment on hospital discharge was linked to an increased risk of severe hypoglycemia in the immediate postdischarge period.
However, diabetes treatment intensification – that is, receiving a prescription for a new or higher dose of diabetes medicine – was not associated with decreased risks of severe hyperglycemia or with improved glycemic (hemoglobin A1c) control at 30 days or 1 year, according to study results, published in JAMA Network Open.
“We didn’t see a reduction in diabetes emergencies in more intensively treated patients,” lead investigator Timothy S. Anderson, MD, said in an interview.
Also, importantly, there was a low rate of persistence with the new treatment. “Half of the patients were no longer taking these [intensified diabetes medicines] at 1 year, which tells me that context is key,” he pointed out. “If a patient is in the hospital for diabetes [unlike the patients in this study], I think it makes a lot of sense to modify and adjust their regimen to try to help them right then and there.”
The overall risk of severe hyperglycemia or severe hypoglycemia was pretty small in the overall cohort, Dr. Anderson noted, “but we do put people at risk of leaving the hospital and ending up back in the hospital with low blood sugar when we intensify medications, and there’s not necessarily a good signal to suggest that it’s all that urgent to change these medicines.”
Instead, the “safer path” may be to make recommendations to the patient’s outpatient physician and also inform the patient – for example, “We saw some concerns about your diabetes while you were in the hospital, and this is really something that should be looked at when you’re recovered and feeling better from the rest of your health standpoint” – rather than making a diabetes medication change while the person is acutely ill or recovering from illness, said Dr. Anderson, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston.
The researchers also found an “unexpected” significant decrease in 30-day mortality in the patients with intensified diabetes treatment, which was probably because of confounding that was not accounted for, Dr. Anderson speculated, since clinical trials have consistently shown that benefits from diabetes medications take a longer time to show an effect.
‘Important study,’ but lacked newer meds
This is an “important” study for primary care and in-hospital physicians that shows that “hospitalization is really not the time and the place” to intensify diabetes medication, Rozalina G. McCoy, MD, coauthor of an invited commentary, told this news organization in an interview.
“While overcoming treatment inertia is important, [it should be] done appropriately, so that we don’t overtreat patients,” Dr. McCoy, of the Mayo Clinic in Rochester, Minn., stressed.
The very low rate of persistence of taking intensified medications is a major finding, she agreed. Hospitalized patients “are not in their usual state of health, so if we make long-term treatment decisions based on their acute abnormal situation, that may not be appropriate.”
However, patients with high A1c may benefit from a change at hospital discharge rather than when they see their primary care provider, with the caveat that they need close follow-up as an outpatient.
The study emphasizes the “need for longitudinal patient care rather than episodic patches,” according to Dr. McCoy.
For example, a patient who is hospitalized for a chronic obstructive pulmonary disease or asthma exacerbation may be receiving steroids that cause high blood glucose levels but as soon as they’re done with their steroid course, blood glucose will decrease, so the “need for close outpatient follow-up is very important.”
One limitation of the current work is that an earlier study in the same population by the research group showed that 49% of patients whose treatment regimens were intensified had limited life expectancy or were at or below their A1c goal, so they would not have benefited from the stepped-up treatment, she noted.
Another limitation is that the findings cannot be generalized to women or younger patients, or to patients treated with glucagonlike peptide 1 (GLP-1)–receptor agonists or sodium-glucose cotransporter 2 (SGLT2) inhibitors.
The study patients were seen in the U.S. Veterans Health Administration health system when these newer agents were not used. Three-quarters of patients received intensified treatment with sulfonylurea or insulin, and only one patient received a new GLP-1–receptor agonist.
Ideally, Dr. McCoy said, patients should have been prescribed a GLP-1–receptor agonist if they had atherosclerotic cardiovascular disease or kidney disease, or an SGLT2 inhibitor if they had kidney disease or heart failure, which may have led to different results, and would need to be determined in further study.
Dr. Anderson agreed that “SGLT2 inhibitors and GLP1 agonists are broadly much safer than the older diabetes medicines, at least when it comes to risk of hypoglycemia, and may have more clear benefits in heart disease and mortality. So I would not want to extrapolate our findings to those new classes,” he said. “A similar set of studies would need to be done.”
Study rationale and findings
Hospitalized older adults with diabetes commonly have transiently elevated blood glucose levels that might lead clinicians to discharge them from hospital with a prescription for more intensive diabetes medications than they were on before they were hospitalized, but it is not clear if these diabetes medication changes would improve outcomes.
To investigate this, the researchers analyzed data from patients with diabetes who were 65 and older and hospitalized for common medical conditions in VHA hospitals during January 2011–September 2016, and then discharged to the community.
They excluded patients who were hospitalized for things that require immediate change in diabetes treatment and patients who were using insulin before their hospitalization (because instructions to modify insulin dosing frequently don’t have a new prescription).
The researchers identified 28,198 adults with diabetes who were not on insulin and were hospitalized in the VHA health system for heart failure (18%), coronary artery disease (13%), chronic obstructive pulmonary disease (10%), pneumonia (9.6%), and urinary tract infection (7.5%), and less often and not in decreasing order, for acute coronary syndrome, arrhythmia, asthma, chest pain, conduction disorders, heart valve disorders, sepsis, skin infection, stroke, and transient ischemic attack.
Of these patients, 2,768 patients (9.8%) received diabetes medication intensification, and the researchers matched 2,648 of these patients with an equal number of patients who did not receive this treatment intensification.
The patients in each group had a mean age of 73 and 98.5% were male; 78% were White.
They had a mean A1c of 7.9%. Most were receiving sulfonylurea (43%) or metformin (39%), and few were receiving thiazolidinediones (4.1%), alpha-glucosidase inhibitors (2.7%), dipeptidyl peptidase 4 inhibitors (2.0%), or other types of diabetes drugs (0.1%).
Of the 2,768 patients who received intensified diabetes medication, most received a prescription for insulin (51%) or sulfonylurea (23%).
In the propensity-matched cohort, patients with intensified diabetes medication had a higher rate of severe hypoglycemia at 30 days (1% vs. 0.5%), which translated into a significant twofold higher risk (hazard ratio, 2.17).
The rates of severe hypoglycemia at 1 year were similar in both groups (3.1% and 2.9%).
The incidence of severe hyperglycemia was the same in both groups at 30 days (0.3%) and 1 year (1.3%).
In secondary outcomes, at 1 year, 48% of new oral diabetes medications and 39% of new insulin prescriptions were no longer being filled.
Overall, patients who were discharged with intensified diabetes medication were significantly less likely to die within 30 days than the other patients (1.3% vs. 2.4%; HR, 0.55).
However, this mortality benefit was found only in the subgroup of 2,524 patients who had uncontrolled diabetes when they were admitted to hospital (A1c >7.5%; mean A1c, 9.1%), and not in the propensity-matched subgroup of 2,672 patients who had controlled diabetes then (A1c up to 7.5%; mean A1c, 6.8%).
There was no significant difference in 1-year mortality in patients with versus without intensified treatment (15.8% vs. 17.8%).
There were also no significant between-group difference in rates of hospital readmission at 30 days (roughly 17%) or 1 year (roughly 51%).
The decreases in mean A1c from hospital discharge to 1 year later were also the same in both groups (going from 7.9% to 7.7%).
The study was funded by grants from the National Institute on Aging and the American College of Cardiology. Dr. Anderson has no relevant financial disclosures. Dr. McCoy reported receiving grants from the National Institute of Diabetes and Digestive and Kidney Diseases, AARP, and the Patient-Centered Outcomes Research Institute outside the submitted work. The disclosures of the other authors and the editorial coauthor are available with the article and commentary.
FROM JAMA NETWORK OPEN
Free vitamin D no better at predicting death in men than standard testing
In the clinical assessment of vitamin D concentrations, free 25-hydroxyvitamin D shows little added benefit to the current standard of total 25(OH)D, with deficiencies in each associated with at least a twofold risk of all-cause mortality, new research shows.

“In this prospective, population-based study of middle-aged and older European men, total 25(OH)D levels below 20 mcg/L were independently associated with a twofold increased all-cause mortality,” the researchers reported.
“Lower concentrations of free 25(OH)D were also predictive of mortality, but did not provide any additional information,” they noted. “The data do not support routine measurement of free 25(OH)D or 1,25(OH)2D [1,25-dihydroxyvitamin D] over total 25(OH)D levels.”
Despite vitamin D deficiency being well established as playing a role in a wide range of adverse health effects, including cardiovascular disease and mortality, there has been a lack of consensus on the optimal concentration of total 25(OH)D, with studies showing inconsistent levels to define insufficiency and deficiency.
One aspect of the debate has focused on precisely how to measure the concentrations, with some evidence supporting the “free hormone hypothesis,” which suggests that free 25(OH)D could represent a better indicator than the standard total 25(OH)D of functional availability of vitamin D, and have stronger clinical utility.
To investigate both issues, Marian Dejaeger, MD, PhD, and colleagues evaluated prospective data on 1,915 men recruited from eight centers around Europe in the European Male Aging Study in a report published in the Journal of Clinical Endocrinology & Metabolism
The men, who were aged between 40 and 79 years, had a mean follow-up of 12.3 years; during that time, about a quarter (23.5%) of them died.
In addition to other factors, including being older, having a higher body mass index, and having at least two comorbidities, men who died had significantly lower levels of total 25(OH)D, total 1,25(OH)2D, free 25(OH)D, and free 1,25(OH)2D, as well as higher parathyroid hormone and creatinine values.
After adjustment for key confounders, including body mass index, smoking, alcohol consumption, kidney function, number of comorbidities at baseline and other factors, men with a total 25(OH)D below 20 mcg/L had a significantly increased risk of mortality, compared with those who had normal levels of vitamin D, defined as above 30 mcg/L (hazard ratio, 2.03; P < .001).
In terms of free 25(OH)D, the lowest three free 25(OH)D quintiles (under 4.43 ng/L) similarly had a significantly higher mortality risk, compared with the highest quintile (HR, 2.09; P < .01) after adjustment for the confounders.
Further observations of all quintiles of other measures of 1,25(OH)2D and vitamin D binding protein (DBP) showed no associations with mortality after adjusting for confounders.
Methods of measurement
An important caveat of the study is the type of method used to measure free 25(OH)D. The authors calculated free 25(OH)D using a formula, as opposed to the alternative of direct measurement with an enzyme-linked immunosorbent assay kit, and there can be important differences between the two approaches, said Daniel Bikle, MD, PhD, a professor of medicine and dermatology at the San Francisco Veterans Affairs Medical Center and University of California, San Francisco, in a comment on the research.
“The biggest problem is that calculating free 25(OH)D does not give an accurate estimate of the real free level, so making conclusions regarding its role in clinical situations is subject to error,” said Dr. Bikle, who recently authored a review of the free hormone hypothesis.
A calculation approach “depends heavily on the total 25(OH)D level, so in a population with reasonably normal DBP and albumin levels, the correlation with total 25(OH)D is very high, so I am not surprised by the results showing no additional value,” he said in an interview.
The authors addressed their use of the calculation over the direct measurement in the study, noting that there is a “high correlation between both methods.”
But they added that, “as no equilibrium analysis method is available for free 25(OH)D, nor for free 1,25(OH)2D, no method can be considered superior.”
Dr. Dejaeger, of the department of public health and primary care, Katholieke Universiteit Leuven (Belgium), added that she agreed that high or low DBP could potentially shift some correlations, but noted that other research has shown calculated and direct measures to match relatively well.
“So we partly agree [with Dr. Bikle] not being surprised that we did not find an added value because we also found little variation in DBP, but we are not convinced that a different measurement method could make the difference here.”
Another caveat of the study is that, despite half of the measurements being taken in the summer, more than 90% of subjects in the study’s cohort had vitamin D insufficiency, defined in the study as total 25(OH)D levels below 30 mcg/L, and as many as 70% had deficiency, with levels below 20 mcg/L.
Therefore, “as the number of participants with high levels of total 25(OH)D in our study is small, a true threshold concentration for optimal vitamin D status cannot be defined on basis of our data,” the authors noted.
Under current recommendations, the Endocrine Society indicates that concentrations below 30 mcg/L are insufficient, while other groups, including the Institute of Medicine, suggest concentrations of 20 mcg/L or above are adequate.
Free hormone hypothesis
Under the free hormone hypothesis, which is observed with thyroid hormones and sex steroids, the very small fraction of free hormones that are not bound to protein carriers can enter cells and help facilitate biologic activity.
The hypothesis of a role of free 25(OH)D in mortality was supported by a recent study, in which free 25(OH)D levels – but not total 25(OH)D levels, were found to be independently associated with an increased risk of all-cause and cardiovascular mortality among patients with coronary artery disease.
However, two other studies are more consistent with the new findings, including one study showing no added value of free 25(OH)D as a marker for bone mineral density in older women, and another study showing no value as a marker of metabolic variables in healthy children.
“Currently, there are no hard data to support routine measurements of free 25(OH)D or 1,25(OH)2D over total 25(OH)D, the current standard of assessing vitamin D status, as stated in guidelines from different scientific bodies,” Dr. Dejaeger said in an interview.
The study received support from Versus Arthritis and the National Institute for Health Research Manchester Biomedical Research Centre. Dr. Dejaeger and Dr. Bikle had no disclosures to report.
In the clinical assessment of vitamin D concentrations, free 25-hydroxyvitamin D shows little added benefit to the current standard of total 25(OH)D, with deficiencies in each associated with at least a twofold risk of all-cause mortality, new research shows.
“In this prospective, population-based study of middle-aged and older European men, total 25(OH)D levels below 20 mcg/L were independently associated with a twofold increased all-cause mortality,” the researchers reported.
“Lower concentrations of free 25(OH)D were also predictive of mortality, but did not provide any additional information,” they noted. “The data do not support routine measurement of free 25(OH)D or 1,25(OH)2D [1,25-dihydroxyvitamin D] over total 25(OH)D levels.”
Despite vitamin D deficiency being well established as playing a role in a wide range of adverse health effects, including cardiovascular disease and mortality, there has been a lack of consensus on the optimal concentration of total 25(OH)D, with studies showing inconsistent levels to define insufficiency and deficiency.
One aspect of the debate has focused on precisely how to measure the concentrations, with some evidence supporting the “free hormone hypothesis,” which suggests that free 25(OH)D could represent a better indicator than the standard total 25(OH)D of functional availability of vitamin D, and have stronger clinical utility.
To investigate both issues, Marian Dejaeger, MD, PhD, and colleagues evaluated prospective data on 1,915 men recruited from eight centers around Europe in the European Male Aging Study in a report published in the Journal of Clinical Endocrinology & Metabolism
The men, who were aged between 40 and 79 years, had a mean follow-up of 12.3 years; during that time, about a quarter (23.5%) of them died.
In addition to other factors, including being older, having a higher body mass index, and having at least two comorbidities, men who died had significantly lower levels of total 25(OH)D, total 1,25(OH)2D, free 25(OH)D, and free 1,25(OH)2D, as well as higher parathyroid hormone and creatinine values.
After adjustment for key confounders, including body mass index, smoking, alcohol consumption, kidney function, number of comorbidities at baseline and other factors, men with a total 25(OH)D below 20 mcg/L had a significantly increased risk of mortality, compared with those who had normal levels of vitamin D, defined as above 30 mcg/L (hazard ratio, 2.03; P < .001).
In terms of free 25(OH)D, the lowest three free 25(OH)D quintiles (under 4.43 ng/L) similarly had a significantly higher mortality risk, compared with the highest quintile (HR, 2.09; P < .01) after adjustment for the confounders.
Further observations of all quintiles of other measures of 1,25(OH)2D and vitamin D binding protein (DBP) showed no associations with mortality after adjusting for confounders.
Methods of measurement
An important caveat of the study is the type of method used to measure free 25(OH)D. The authors calculated free 25(OH)D using a formula, as opposed to the alternative of direct measurement with an enzyme-linked immunosorbent assay kit, and there can be important differences between the two approaches, said Daniel Bikle, MD, PhD, a professor of medicine and dermatology at the San Francisco Veterans Affairs Medical Center and University of California, San Francisco, in a comment on the research.
“The biggest problem is that calculating free 25(OH)D does not give an accurate estimate of the real free level, so making conclusions regarding its role in clinical situations is subject to error,” said Dr. Bikle, who recently authored a review of the free hormone hypothesis.
A calculation approach “depends heavily on the total 25(OH)D level, so in a population with reasonably normal DBP and albumin levels, the correlation with total 25(OH)D is very high, so I am not surprised by the results showing no additional value,” he said in an interview.
The authors addressed their use of the calculation over the direct measurement in the study, noting that there is a “high correlation between both methods.”
But they added that, “as no equilibrium analysis method is available for free 25(OH)D, nor for free 1,25(OH)2D, no method can be considered superior.”
Dr. Dejaeger, of the department of public health and primary care, Katholieke Universiteit Leuven (Belgium), added that she agreed that high or low DBP could potentially shift some correlations, but noted that other research has shown calculated and direct measures to match relatively well.
“So we partly agree [with Dr. Bikle] not being surprised that we did not find an added value because we also found little variation in DBP, but we are not convinced that a different measurement method could make the difference here.”
Another caveat of the study is that, despite half of the measurements being taken in the summer, more than 90% of subjects in the study’s cohort had vitamin D insufficiency, defined in the study as total 25(OH)D levels below 30 mcg/L, and as many as 70% had deficiency, with levels below 20 mcg/L.
Therefore, “as the number of participants with high levels of total 25(OH)D in our study is small, a true threshold concentration for optimal vitamin D status cannot be defined on basis of our data,” the authors noted.
Under current recommendations, the Endocrine Society indicates that concentrations below 30 mcg/L are insufficient, while other groups, including the Institute of Medicine, suggest concentrations of 20 mcg/L or above are adequate.
Free hormone hypothesis
Under the free hormone hypothesis, which is observed with thyroid hormones and sex steroids, the very small fraction of free hormones that are not bound to protein carriers can enter cells and help facilitate biologic activity.
The hypothesis of a role of free 25(OH)D in mortality was supported by a recent study, in which free 25(OH)D levels – but not total 25(OH)D levels, were found to be independently associated with an increased risk of all-cause and cardiovascular mortality among patients with coronary artery disease.
However, two other studies are more consistent with the new findings, including one study showing no added value of free 25(OH)D as a marker for bone mineral density in older women, and another study showing no value as a marker of metabolic variables in healthy children.
“Currently, there are no hard data to support routine measurements of free 25(OH)D or 1,25(OH)2D over total 25(OH)D, the current standard of assessing vitamin D status, as stated in guidelines from different scientific bodies,” Dr. Dejaeger said in an interview.
The study received support from Versus Arthritis and the National Institute for Health Research Manchester Biomedical Research Centre. Dr. Dejaeger and Dr. Bikle had no disclosures to report.
In the clinical assessment of vitamin D concentrations, free 25-hydroxyvitamin D shows little added benefit to the current standard of total 25(OH)D, with deficiencies in each associated with at least a twofold risk of all-cause mortality, new research shows.
“In this prospective, population-based study of middle-aged and older European men, total 25(OH)D levels below 20 mcg/L were independently associated with a twofold increased all-cause mortality,” the researchers reported.
“Lower concentrations of free 25(OH)D were also predictive of mortality, but did not provide any additional information,” they noted. “The data do not support routine measurement of free 25(OH)D or 1,25(OH)2D [1,25-dihydroxyvitamin D] over total 25(OH)D levels.”
Despite vitamin D deficiency being well established as playing a role in a wide range of adverse health effects, including cardiovascular disease and mortality, there has been a lack of consensus on the optimal concentration of total 25(OH)D, with studies showing inconsistent levels to define insufficiency and deficiency.
One aspect of the debate has focused on precisely how to measure the concentrations, with some evidence supporting the “free hormone hypothesis,” which suggests that free 25(OH)D could represent a better indicator than the standard total 25(OH)D of functional availability of vitamin D, and have stronger clinical utility.
To investigate both issues, Marian Dejaeger, MD, PhD, and colleagues evaluated prospective data on 1,915 men recruited from eight centers around Europe in the European Male Aging Study in a report published in the Journal of Clinical Endocrinology & Metabolism
The men, who were aged between 40 and 79 years, had a mean follow-up of 12.3 years; during that time, about a quarter (23.5%) of them died.
In addition to other factors, including being older, having a higher body mass index, and having at least two comorbidities, men who died had significantly lower levels of total 25(OH)D, total 1,25(OH)2D, free 25(OH)D, and free 1,25(OH)2D, as well as higher parathyroid hormone and creatinine values.
After adjustment for key confounders, including body mass index, smoking, alcohol consumption, kidney function, number of comorbidities at baseline and other factors, men with a total 25(OH)D below 20 mcg/L had a significantly increased risk of mortality, compared with those who had normal levels of vitamin D, defined as above 30 mcg/L (hazard ratio, 2.03; P < .001).
In terms of free 25(OH)D, the lowest three free 25(OH)D quintiles (under 4.43 ng/L) similarly had a significantly higher mortality risk, compared with the highest quintile (HR, 2.09; P < .01) after adjustment for the confounders.
Further observations of all quintiles of other measures of 1,25(OH)2D and vitamin D binding protein (DBP) showed no associations with mortality after adjusting for confounders.
Methods of measurement
An important caveat of the study is the type of method used to measure free 25(OH)D. The authors calculated free 25(OH)D using a formula, as opposed to the alternative of direct measurement with an enzyme-linked immunosorbent assay kit, and there can be important differences between the two approaches, said Daniel Bikle, MD, PhD, a professor of medicine and dermatology at the San Francisco Veterans Affairs Medical Center and University of California, San Francisco, in a comment on the research.
“The biggest problem is that calculating free 25(OH)D does not give an accurate estimate of the real free level, so making conclusions regarding its role in clinical situations is subject to error,” said Dr. Bikle, who recently authored a review of the free hormone hypothesis.
A calculation approach “depends heavily on the total 25(OH)D level, so in a population with reasonably normal DBP and albumin levels, the correlation with total 25(OH)D is very high, so I am not surprised by the results showing no additional value,” he said in an interview.
The authors addressed their use of the calculation over the direct measurement in the study, noting that there is a “high correlation between both methods.”
But they added that, “as no equilibrium analysis method is available for free 25(OH)D, nor for free 1,25(OH)2D, no method can be considered superior.”
Dr. Dejaeger, of the department of public health and primary care, Katholieke Universiteit Leuven (Belgium), added that she agreed that high or low DBP could potentially shift some correlations, but noted that other research has shown calculated and direct measures to match relatively well.
“So we partly agree [with Dr. Bikle] not being surprised that we did not find an added value because we also found little variation in DBP, but we are not convinced that a different measurement method could make the difference here.”
Another caveat of the study is that, despite half of the measurements being taken in the summer, more than 90% of subjects in the study’s cohort had vitamin D insufficiency, defined in the study as total 25(OH)D levels below 30 mcg/L, and as many as 70% had deficiency, with levels below 20 mcg/L.
Therefore, “as the number of participants with high levels of total 25(OH)D in our study is small, a true threshold concentration for optimal vitamin D status cannot be defined on basis of our data,” the authors noted.
Under current recommendations, the Endocrine Society indicates that concentrations below 30 mcg/L are insufficient, while other groups, including the Institute of Medicine, suggest concentrations of 20 mcg/L or above are adequate.
Free hormone hypothesis
Under the free hormone hypothesis, which is observed with thyroid hormones and sex steroids, the very small fraction of free hormones that are not bound to protein carriers can enter cells and help facilitate biologic activity.
The hypothesis of a role of free 25(OH)D in mortality was supported by a recent study, in which free 25(OH)D levels – but not total 25(OH)D levels, were found to be independently associated with an increased risk of all-cause and cardiovascular mortality among patients with coronary artery disease.
However, two other studies are more consistent with the new findings, including one study showing no added value of free 25(OH)D as a marker for bone mineral density in older women, and another study showing no value as a marker of metabolic variables in healthy children.
“Currently, there are no hard data to support routine measurements of free 25(OH)D or 1,25(OH)2D over total 25(OH)D, the current standard of assessing vitamin D status, as stated in guidelines from different scientific bodies,” Dr. Dejaeger said in an interview.
The study received support from Versus Arthritis and the National Institute for Health Research Manchester Biomedical Research Centre. Dr. Dejaeger and Dr. Bikle had no disclosures to report.
FROM JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
The devil in the (masking) details
The Devil’s own face covering?
It’s been over a year and a half since the COVID-19 emergency was declared in the United States, and we’ve been starting to wonder what our good friend SARS-CoV-2 has left to give. The collective cynic/optimist in us figures that the insanity can’t last forever, right?

Maybe not forever, but …
A group of parents is suing the Central Bucks (Pa.) School District over school mask mandates, suggesting that the district has no legal authority to enforce such measures. Most of their arguments, Philadelphia Magazine says, are pretty standard stuff: Masks are causing depression, anxiety, and discomfort in their children; masks are a violation of their constitutional rights; and “masks are being used as a control mechanism over the population.”
There are some unusual claims, though. One of the parents, Shannon Harris, said that “wearing masks interferes with their religious duty to spread the word of God and forces them to participate in a satanic ritual,” according to the Philadelphia Inquirer.
Philadelphia Magazine decided to check on that “satanic ritual” claim by asking an expert, in this case a spokesperson for the Church of Satan. The Reverend Raul Antony said that “simply ‘wearing a mask’ is not a Satanic ritual, and anyone that genuinely thinks otherwise is a blithering idiot,” adding that the group’s rituals were available on its website.
COVID, you never let us down.
You’re the (hurricane) wind beneath my wings
Marriage isn’t easy. From finances to everyday stressors like work and children, maintaining a solid relationship is tough. Then a natural disaster shows up on top of everything else, and marriages actually improve, researchers found.

In a study published by Psychological Science, researchers surveyed 231 newlywed couples about the satisfaction of their marriage before and after Hurricane Harvey in 2017. They found after the hurricane couples had a “significant boost” in the satisfaction of their relationship.
One would think something like this would create what researchers call a “stress spillover,” creating a decrease in relationship satisfaction. Destruction to your home or even displacement after a natural disaster seems pretty stressful. But, “a natural disaster can really put things in perspective. People realize how important their partner is to them when they are jolted out of the day-to-day stress of life,” said Hannah Williamson, PhD, the lead author of the study.
And although everyone saw an increase, the biggest jumps in relationship satisfaction belonged to the people who were most unhappy before the hurricane. Unfortunately, the researchers also found that the effects were only temporary and the dissatisfaction came back within a year.
Dr. Williamson thinks there may be something to these findings that can be beneficial from a therapy standpoint where “couples can shift their perspective in a similar way without having to go through a natural disaster.”
Let’s hope she’s right, because the alternative is to seek out a rampaging hurricane every time your relationship is on the rocks, and that just seems impractical after the second or third year.
Not-so-essential oils
Many people use essential oils as a way to unwind and relax. Stressed? Can’t sleep? There’s probably an essential oil for that. However, it seems like these days a lot of things we love and/or think are good for us have a side that’s not so.

According to the Centers for Disease Control and Prevention, a woman from Georgia died from a rare bacteria called Burkholderia pseudomallei. There have been three previous infections in Kansas, Minnesota, and Texas throughout 2021; two of the four infections were in children. Melioidosis, the disease caused by B. pseudomallei, is usually found in southeast Asia and isn’t obvious or easy to diagnose, especially in places like decidedly untropical Minnesota.
The Georgia case was the real break in this medical mystery, as the infection was traced back to a Walmart product called “Better Homes and Gardens Essential Oil Infused Aromatherapy Room Spray with Gemstones” (a very pithy name). The bacteria were in the lavender and chamomile scent. The CDC is investigating all other product scents, and Walmart has recalled all lots of the product.
If you’ve got that particular essential oil, it’s probably for the best that you stop using it. Don’t worry, we’re sure there’s plenty of other essential oil–infused aromatherapy room sprays with gemstones out there for your scent-based needs.
Welcome to the Ministry of Sleep-Deprived Walks
Walking is simple, right? You put one foot in front of the other, and soon you’re walking out the door. Little kids can do it. Even zombies can walk, and they don’t even have brains.

Research from MIT and the University of São Paulo has shown that walking is a little trickier than we might think. One researcher in particular noticed that student volunteers tended to perform worse toward the end of semesters, as project deadlines and multiple exams crashed over their heads and they were deprived of solid sleep schedules.
In a study published in Scientific Reports, our intrepid walking researchers had a collection of students monitor their sleep patterns for 2 weeks; on average, the students got 6 hours per night, though some were able to compensate on weekends. On the final day of a 14-day period, some students pulled all-nighters while the rest were allowed to sleep as usual. Then all students performed a walking test involving keeping time with a metronome.
To absolutely no one’s surprise, the students who performed all-nighters before being tested walked the worst, but between the other students, the ones who compensated for sleep deprivation on weekends did better than those who got 6 hours every night, despite getting a similar amount of sleep overall. This effect persisted even when the compensating students performed their walking tests late in the week, just before they got their weekend beauty sleep.
The moral of the story? Sleep is good, and you should get more of it. But if you can’t, sleep in on weekends. Science has given you permission. All those suburban dads looking to get their teenagers up at 8 in the morning must be sweating right now.
The Devil’s own face covering?
It’s been over a year and a half since the COVID-19 emergency was declared in the United States, and we’ve been starting to wonder what our good friend SARS-CoV-2 has left to give. The collective cynic/optimist in us figures that the insanity can’t last forever, right?
Maybe not forever, but …
A group of parents is suing the Central Bucks (Pa.) School District over school mask mandates, suggesting that the district has no legal authority to enforce such measures. Most of their arguments, Philadelphia Magazine says, are pretty standard stuff: Masks are causing depression, anxiety, and discomfort in their children; masks are a violation of their constitutional rights; and “masks are being used as a control mechanism over the population.”
There are some unusual claims, though. One of the parents, Shannon Harris, said that “wearing masks interferes with their religious duty to spread the word of God and forces them to participate in a satanic ritual,” according to the Philadelphia Inquirer.
Philadelphia Magazine decided to check on that “satanic ritual” claim by asking an expert, in this case a spokesperson for the Church of Satan. The Reverend Raul Antony said that “simply ‘wearing a mask’ is not a Satanic ritual, and anyone that genuinely thinks otherwise is a blithering idiot,” adding that the group’s rituals were available on its website.
COVID, you never let us down.
You’re the (hurricane) wind beneath my wings
Marriage isn’t easy. From finances to everyday stressors like work and children, maintaining a solid relationship is tough. Then a natural disaster shows up on top of everything else, and marriages actually improve, researchers found.
In a study published by Psychological Science, researchers surveyed 231 newlywed couples about the satisfaction of their marriage before and after Hurricane Harvey in 2017. They found after the hurricane couples had a “significant boost” in the satisfaction of their relationship.
One would think something like this would create what researchers call a “stress spillover,” creating a decrease in relationship satisfaction. Destruction to your home or even displacement after a natural disaster seems pretty stressful. But, “a natural disaster can really put things in perspective. People realize how important their partner is to them when they are jolted out of the day-to-day stress of life,” said Hannah Williamson, PhD, the lead author of the study.
And although everyone saw an increase, the biggest jumps in relationship satisfaction belonged to the people who were most unhappy before the hurricane. Unfortunately, the researchers also found that the effects were only temporary and the dissatisfaction came back within a year.
Dr. Williamson thinks there may be something to these findings that can be beneficial from a therapy standpoint where “couples can shift their perspective in a similar way without having to go through a natural disaster.”
Let’s hope she’s right, because the alternative is to seek out a rampaging hurricane every time your relationship is on the rocks, and that just seems impractical after the second or third year.
Not-so-essential oils
Many people use essential oils as a way to unwind and relax. Stressed? Can’t sleep? There’s probably an essential oil for that. However, it seems like these days a lot of things we love and/or think are good for us have a side that’s not so.
According to the Centers for Disease Control and Prevention, a woman from Georgia died from a rare bacteria called Burkholderia pseudomallei. There have been three previous infections in Kansas, Minnesota, and Texas throughout 2021; two of the four infections were in children. Melioidosis, the disease caused by B. pseudomallei, is usually found in southeast Asia and isn’t obvious or easy to diagnose, especially in places like decidedly untropical Minnesota.
The Georgia case was the real break in this medical mystery, as the infection was traced back to a Walmart product called “Better Homes and Gardens Essential Oil Infused Aromatherapy Room Spray with Gemstones” (a very pithy name). The bacteria were in the lavender and chamomile scent. The CDC is investigating all other product scents, and Walmart has recalled all lots of the product.
If you’ve got that particular essential oil, it’s probably for the best that you stop using it. Don’t worry, we’re sure there’s plenty of other essential oil–infused aromatherapy room sprays with gemstones out there for your scent-based needs.
Welcome to the Ministry of Sleep-Deprived Walks
Walking is simple, right? You put one foot in front of the other, and soon you’re walking out the door. Little kids can do it. Even zombies can walk, and they don’t even have brains.
Research from MIT and the University of São Paulo has shown that walking is a little trickier than we might think. One researcher in particular noticed that student volunteers tended to perform worse toward the end of semesters, as project deadlines and multiple exams crashed over their heads and they were deprived of solid sleep schedules.
In a study published in Scientific Reports, our intrepid walking researchers had a collection of students monitor their sleep patterns for 2 weeks; on average, the students got 6 hours per night, though some were able to compensate on weekends. On the final day of a 14-day period, some students pulled all-nighters while the rest were allowed to sleep as usual. Then all students performed a walking test involving keeping time with a metronome.
To absolutely no one’s surprise, the students who performed all-nighters before being tested walked the worst, but between the other students, the ones who compensated for sleep deprivation on weekends did better than those who got 6 hours every night, despite getting a similar amount of sleep overall. This effect persisted even when the compensating students performed their walking tests late in the week, just before they got their weekend beauty sleep.
The moral of the story? Sleep is good, and you should get more of it. But if you can’t, sleep in on weekends. Science has given you permission. All those suburban dads looking to get their teenagers up at 8 in the morning must be sweating right now.
The Devil’s own face covering?
It’s been over a year and a half since the COVID-19 emergency was declared in the United States, and we’ve been starting to wonder what our good friend SARS-CoV-2 has left to give. The collective cynic/optimist in us figures that the insanity can’t last forever, right?
Maybe not forever, but …
A group of parents is suing the Central Bucks (Pa.) School District over school mask mandates, suggesting that the district has no legal authority to enforce such measures. Most of their arguments, Philadelphia Magazine says, are pretty standard stuff: Masks are causing depression, anxiety, and discomfort in their children; masks are a violation of their constitutional rights; and “masks are being used as a control mechanism over the population.”
There are some unusual claims, though. One of the parents, Shannon Harris, said that “wearing masks interferes with their religious duty to spread the word of God and forces them to participate in a satanic ritual,” according to the Philadelphia Inquirer.
Philadelphia Magazine decided to check on that “satanic ritual” claim by asking an expert, in this case a spokesperson for the Church of Satan. The Reverend Raul Antony said that “simply ‘wearing a mask’ is not a Satanic ritual, and anyone that genuinely thinks otherwise is a blithering idiot,” adding that the group’s rituals were available on its website.
COVID, you never let us down.
You’re the (hurricane) wind beneath my wings
Marriage isn’t easy. From finances to everyday stressors like work and children, maintaining a solid relationship is tough. Then a natural disaster shows up on top of everything else, and marriages actually improve, researchers found.
In a study published by Psychological Science, researchers surveyed 231 newlywed couples about the satisfaction of their marriage before and after Hurricane Harvey in 2017. They found after the hurricane couples had a “significant boost” in the satisfaction of their relationship.
One would think something like this would create what researchers call a “stress spillover,” creating a decrease in relationship satisfaction. Destruction to your home or even displacement after a natural disaster seems pretty stressful. But, “a natural disaster can really put things in perspective. People realize how important their partner is to them when they are jolted out of the day-to-day stress of life,” said Hannah Williamson, PhD, the lead author of the study.
And although everyone saw an increase, the biggest jumps in relationship satisfaction belonged to the people who were most unhappy before the hurricane. Unfortunately, the researchers also found that the effects were only temporary and the dissatisfaction came back within a year.
Dr. Williamson thinks there may be something to these findings that can be beneficial from a therapy standpoint where “couples can shift their perspective in a similar way without having to go through a natural disaster.”
Let’s hope she’s right, because the alternative is to seek out a rampaging hurricane every time your relationship is on the rocks, and that just seems impractical after the second or third year.
Not-so-essential oils
Many people use essential oils as a way to unwind and relax. Stressed? Can’t sleep? There’s probably an essential oil for that. However, it seems like these days a lot of things we love and/or think are good for us have a side that’s not so.
According to the Centers for Disease Control and Prevention, a woman from Georgia died from a rare bacteria called Burkholderia pseudomallei. There have been three previous infections in Kansas, Minnesota, and Texas throughout 2021; two of the four infections were in children. Melioidosis, the disease caused by B. pseudomallei, is usually found in southeast Asia and isn’t obvious or easy to diagnose, especially in places like decidedly untropical Minnesota.
The Georgia case was the real break in this medical mystery, as the infection was traced back to a Walmart product called “Better Homes and Gardens Essential Oil Infused Aromatherapy Room Spray with Gemstones” (a very pithy name). The bacteria were in the lavender and chamomile scent. The CDC is investigating all other product scents, and Walmart has recalled all lots of the product.
If you’ve got that particular essential oil, it’s probably for the best that you stop using it. Don’t worry, we’re sure there’s plenty of other essential oil–infused aromatherapy room sprays with gemstones out there for your scent-based needs.
Welcome to the Ministry of Sleep-Deprived Walks
Walking is simple, right? You put one foot in front of the other, and soon you’re walking out the door. Little kids can do it. Even zombies can walk, and they don’t even have brains.
Research from MIT and the University of São Paulo has shown that walking is a little trickier than we might think. One researcher in particular noticed that student volunteers tended to perform worse toward the end of semesters, as project deadlines and multiple exams crashed over their heads and they were deprived of solid sleep schedules.
In a study published in Scientific Reports, our intrepid walking researchers had a collection of students monitor their sleep patterns for 2 weeks; on average, the students got 6 hours per night, though some were able to compensate on weekends. On the final day of a 14-day period, some students pulled all-nighters while the rest were allowed to sleep as usual. Then all students performed a walking test involving keeping time with a metronome.
To absolutely no one’s surprise, the students who performed all-nighters before being tested walked the worst, but between the other students, the ones who compensated for sleep deprivation on weekends did better than those who got 6 hours every night, despite getting a similar amount of sleep overall. This effect persisted even when the compensating students performed their walking tests late in the week, just before they got their weekend beauty sleep.
The moral of the story? Sleep is good, and you should get more of it. But if you can’t, sleep in on weekends. Science has given you permission. All those suburban dads looking to get their teenagers up at 8 in the morning must be sweating right now.
Which specialties get the biggest markups over Medicare rates?
Anesthesiologists charge private insurers more than 300% above Medicare rates, a markup that is higher than that of 16 other specialties, according to a study released by the Urban Institute.
The Washington-based nonprofit institute found that the lowest markups were in psychiatry, ophthalmology, ob.gyn., family medicine, gastroenterology, and internal medicine, at 110%-120% of Medicare rates. .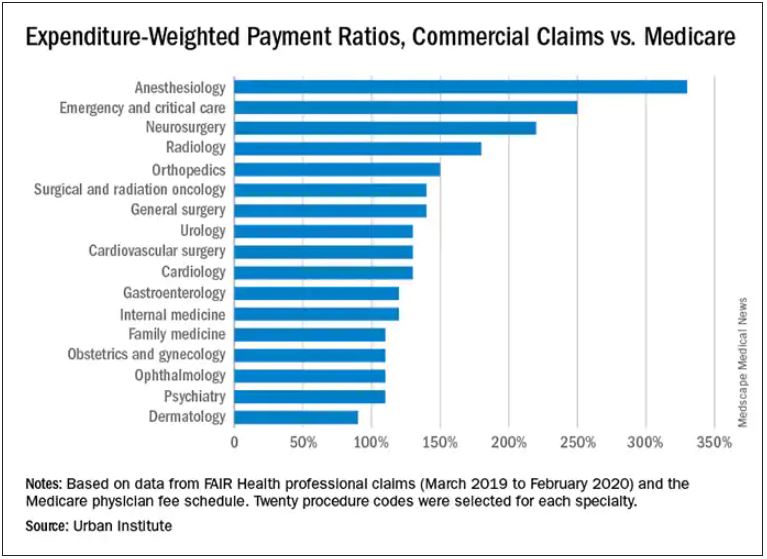
In the middle are cardiology and cardiovascular surgery (130%), urology (130%), general surgery, surgical and radiation oncology (all at 140%), and orthopedics (150%).
At the top end were radiology (180%), neurosurgery (220%), emergency and critical care (250%), and anesthesiology (330%).
The wide variation in payments could be cited in support of the idea of applying Medicare rates across all physician specialties, say the study authors. Although lowering practitioner payments might lead to savings, it “will also create more pushback from providers, especially if these rates are introduced in the employer market,” write researchers Stacey McMorrow, PhD, Robert A. Berenson, MD, and John Holahan, PhD.
It is not known whether lowering commercial payment rates might decrease patient access, they write.
The authors also note that specialties in which the potential for a fee reduction was greatest were also the specialties for which baseline compensation was highest – from $350,000 annually for emergency physicians to $800,000 a year for neurosurgeons. Annual compensation for ob.gyns., dermatologists, and opthalmologists is about $350,000 a year, which suggests that “these specialties are similarly well compensated by both Medicare and commercial insurers,” the authors write.
The investigators assessed the top 20 procedure codes by expenditure in each of 17 physician specialties. They estimated the commercial-to-Medicare payment ratio for each service and constructed weighted averages across services for each specialty at the national level and for 12 states for which data for all the specialties and services were available.
The researchers analyzed claims from the FAIR Health database between March 2019 and March 2020. That database represents 60 insurers covering 150 million people.
Pediatric and geriatric specialties, nonphysician practitioners, out-of-network clinicians, and ambulatory surgery center claims were excluded. Codes with modifiers, J codes, and clinical laboratory services were also not included.
The charges used in the study were not the actual contracted rates. The authors instead used “imputed allowed amounts” for each claim line. That method was used to protect the confidentiality of the negotiated rates.
With regard to all specialties, the lowest compensated services were procedures, evaluation and management, and tests, which received 140%-150% of the Medicare rate. Treatments and imaging were marked up 160%. Anesthesia was reimbursed at a rate 330% higher than the rate Medicare would pay.
The authors also assessed geographic variation for the 12 states for which they had data.
Similar to findings in other studies, the researchers found that the markup was lowest in Pennsylvania (120%) and highest in Wisconsin (260%). The U.S. average was 160%. California and Missouri were at 150%; Michigan was right at the average.
For physicians in Illinois, Louisiana, Colorado, Texas, and New York, markups were 170%-180% over the Medicare rate. Markups for clinicians in New Jersey (190%) and Arizona (200%) were closest to the Wisconsin rate.
The authors note some study limitations, including the fact that they excluded out-of-network practitioners, “and such payments may disproportionately affect certain specialties.”
A version of this article first appeared on Medscape.com.
Anesthesiologists charge private insurers more than 300% above Medicare rates, a markup that is higher than that of 16 other specialties, according to a study released by the Urban Institute.
The Washington-based nonprofit institute found that the lowest markups were in psychiatry, ophthalmology, ob.gyn., family medicine, gastroenterology, and internal medicine, at 110%-120% of Medicare rates. .
In the middle are cardiology and cardiovascular surgery (130%), urology (130%), general surgery, surgical and radiation oncology (all at 140%), and orthopedics (150%).
At the top end were radiology (180%), neurosurgery (220%), emergency and critical care (250%), and anesthesiology (330%).
The wide variation in payments could be cited in support of the idea of applying Medicare rates across all physician specialties, say the study authors. Although lowering practitioner payments might lead to savings, it “will also create more pushback from providers, especially if these rates are introduced in the employer market,” write researchers Stacey McMorrow, PhD, Robert A. Berenson, MD, and John Holahan, PhD.
It is not known whether lowering commercial payment rates might decrease patient access, they write.
The authors also note that specialties in which the potential for a fee reduction was greatest were also the specialties for which baseline compensation was highest – from $350,000 annually for emergency physicians to $800,000 a year for neurosurgeons. Annual compensation for ob.gyns., dermatologists, and opthalmologists is about $350,000 a year, which suggests that “these specialties are similarly well compensated by both Medicare and commercial insurers,” the authors write.
The investigators assessed the top 20 procedure codes by expenditure in each of 17 physician specialties. They estimated the commercial-to-Medicare payment ratio for each service and constructed weighted averages across services for each specialty at the national level and for 12 states for which data for all the specialties and services were available.
The researchers analyzed claims from the FAIR Health database between March 2019 and March 2020. That database represents 60 insurers covering 150 million people.
Pediatric and geriatric specialties, nonphysician practitioners, out-of-network clinicians, and ambulatory surgery center claims were excluded. Codes with modifiers, J codes, and clinical laboratory services were also not included.
The charges used in the study were not the actual contracted rates. The authors instead used “imputed allowed amounts” for each claim line. That method was used to protect the confidentiality of the negotiated rates.
With regard to all specialties, the lowest compensated services were procedures, evaluation and management, and tests, which received 140%-150% of the Medicare rate. Treatments and imaging were marked up 160%. Anesthesia was reimbursed at a rate 330% higher than the rate Medicare would pay.
The authors also assessed geographic variation for the 12 states for which they had data.
Similar to findings in other studies, the researchers found that the markup was lowest in Pennsylvania (120%) and highest in Wisconsin (260%). The U.S. average was 160%. California and Missouri were at 150%; Michigan was right at the average.
For physicians in Illinois, Louisiana, Colorado, Texas, and New York, markups were 170%-180% over the Medicare rate. Markups for clinicians in New Jersey (190%) and Arizona (200%) were closest to the Wisconsin rate.
The authors note some study limitations, including the fact that they excluded out-of-network practitioners, “and such payments may disproportionately affect certain specialties.”
A version of this article first appeared on Medscape.com.
Anesthesiologists charge private insurers more than 300% above Medicare rates, a markup that is higher than that of 16 other specialties, according to a study released by the Urban Institute.
The Washington-based nonprofit institute found that the lowest markups were in psychiatry, ophthalmology, ob.gyn., family medicine, gastroenterology, and internal medicine, at 110%-120% of Medicare rates. .
In the middle are cardiology and cardiovascular surgery (130%), urology (130%), general surgery, surgical and radiation oncology (all at 140%), and orthopedics (150%).
At the top end were radiology (180%), neurosurgery (220%), emergency and critical care (250%), and anesthesiology (330%).
The wide variation in payments could be cited in support of the idea of applying Medicare rates across all physician specialties, say the study authors. Although lowering practitioner payments might lead to savings, it “will also create more pushback from providers, especially if these rates are introduced in the employer market,” write researchers Stacey McMorrow, PhD, Robert A. Berenson, MD, and John Holahan, PhD.
It is not known whether lowering commercial payment rates might decrease patient access, they write.
The authors also note that specialties in which the potential for a fee reduction was greatest were also the specialties for which baseline compensation was highest – from $350,000 annually for emergency physicians to $800,000 a year for neurosurgeons. Annual compensation for ob.gyns., dermatologists, and opthalmologists is about $350,000 a year, which suggests that “these specialties are similarly well compensated by both Medicare and commercial insurers,” the authors write.
The investigators assessed the top 20 procedure codes by expenditure in each of 17 physician specialties. They estimated the commercial-to-Medicare payment ratio for each service and constructed weighted averages across services for each specialty at the national level and for 12 states for which data for all the specialties and services were available.
The researchers analyzed claims from the FAIR Health database between March 2019 and March 2020. That database represents 60 insurers covering 150 million people.
Pediatric and geriatric specialties, nonphysician practitioners, out-of-network clinicians, and ambulatory surgery center claims were excluded. Codes with modifiers, J codes, and clinical laboratory services were also not included.
The charges used in the study were not the actual contracted rates. The authors instead used “imputed allowed amounts” for each claim line. That method was used to protect the confidentiality of the negotiated rates.
With regard to all specialties, the lowest compensated services were procedures, evaluation and management, and tests, which received 140%-150% of the Medicare rate. Treatments and imaging were marked up 160%. Anesthesia was reimbursed at a rate 330% higher than the rate Medicare would pay.
The authors also assessed geographic variation for the 12 states for which they had data.
Similar to findings in other studies, the researchers found that the markup was lowest in Pennsylvania (120%) and highest in Wisconsin (260%). The U.S. average was 160%. California and Missouri were at 150%; Michigan was right at the average.
For physicians in Illinois, Louisiana, Colorado, Texas, and New York, markups were 170%-180% over the Medicare rate. Markups for clinicians in New Jersey (190%) and Arizona (200%) were closest to the Wisconsin rate.
The authors note some study limitations, including the fact that they excluded out-of-network practitioners, “and such payments may disproportionately affect certain specialties.”
A version of this article first appeared on Medscape.com.
Hot temperatures in outdoor lockboxes increase sample errors
, according to results from a recent study published in the American Journal of Clinical Pathology.
“Our findings indicate that samples (centrifuged or not centrifuged) were impacted by extreme summer temperatures when stored for short periods of time inside commonly used steel lockboxes,” Joseph R. Wiencek, PhD, medical director of clinical chemistry, Vanderbilt University School of Medicine Core Laboratory in Nashville, said in an interview.
Dr. Wiencek and colleagues picked two dates during the summer of 2019 in a mid-Atlantic state to place two courier lockboxes (LabLocker-KF300) outside in hot temperatures (32º C) starting at 11 a.m., with one lockbox containing two 24-oz cold packs (Nordic NI24) and the other containing no cold packs. The researchers monitored the temperatures of each lockbox over the course of 4 hours.
Overall, eight participants had seven samples in lithium heparin drawn for two studies evaluating centrifuged or not centrifuged samples. In the first study, four participants had seven samples drawn, with one centrifuged sample serving as a control for each patient. The other six samples were wrapped in paper towels, placed in resealable plastic bags, and distributed evenly in the warm and cold lockboxes. The samples did not directly touch the cold packs in the cold lockbox. At 1 hour, 2 hours, and 4 hours, a participant’s sample was removed from each lockbox and centrifuged.
In the second study, another four participants had seven samples drawn. As in the first study, all samples were centrifuged and placed in the lockboxes. For both studies, when samples were centrifuged, plasma from samples was left on the gel barrier when analyzed for concentrations of C-reactive protein, a comprehensive metabolic panel, lactate dehydrogenase (LDH), a lipid panel, magnesium, and phosphorus (Abbott Architect c16000).
In the study of uncentrifuged samples, Dr. Wiencek and colleagues found that when the temperature outside ranged from 28.2º to 44.0º C (mean 40.4º C), the temperature of the cold lockbox was between 16.5º to 22.3º C (mean 22.3º C). The temperature ranged between 34.4º to 46.9º C (mean 42.6º C) in the warm lockbox. For centrifuged samples, the cold lockbox temperature was between 12.2º to 23.0º C (mean 18.0º C) and the warm lockbox was between 25. to 40.8º C (mean 35.2º C) when the outdoor temperature ranged from 27.2º to 46.3º C (mean 37.9º C).
The researchers also calculated the significant change limit (SCL) for each analyte in each sample, finding that aspartate aminotransferase, glucose, LDH, and potassium significantly exceeded the SCL in both the centrifuged and uncentrifuged samples, with the greatest changes seen at the 4-hour timepoint for samples in the warm lockbox (P < .05 for all).
Lockbox instructions are “consistently inconsistent”
In viewing instructions for lockboxes across institutions, Dr. Wiencek said the “outdoor courier lockbox instructions among private, academic and reference laboratories were consistently inconsistent.” For example, no laboratories cited time restrictions for samples in lockboxes, and their descriptions on the number of cold packs a laboratory should use and where the lockbox should be placed varied. The inconsistencies “highlighted the emergent need for standardization and guidance documents for institutions to implement,” Dr. Wiencek said.
One unanswered question is how widespread the problem is. It is unclear how many outdoor courier lockboxes are currently in use in the United States or globally; however, experts agreed it was a common occurrence, with some of the largest laboratory service providers offering outdoor courier lockboxes to their clients.
“Courier lockboxes are everywhere. All you need to do is walk around your clinics that are at your hospitals or clinics located around your grocery store to find them,” Dr. Wiencek said. “Some hang on doors, while others can be found on the ground in direct sunlight on a hot summer day.”
What’s more, institutions may not realize how leaving samples outdoors for extended periods can affect results. “Care teams are commonly unaware that samples placed in these poorly designed lockboxes can experience extreme summer or winter temperatures that may lead to incorrect results,” Dr. Wiencek said. “Healthcare providers need to understand the hidden dangers courier lockboxes have on the quality of their patient’s test results.”
Amy L. Pyle-Eilola, PhD, clinical chemistry director at Nationwide Children’s Hospital in Columbus, Ohio, said a major strength of the study by Dr. Wiencek and colleagues “is just that it was done at all.”
“I appreciate the real-world nature of this study and that it provides a snapshot of what conditions are really like in a lockbox in the summer,” she said in an interview.
In the clinical lab, receiving samples that had been sitting in a courier lockbox “is not uncommon,” Dr. Pyle-Eilola said.
“When I have encountered these situations, I have struggled to decide if it is still appropriate to run the tests. I always look to the medical literature for assistance with these situations, but there has been a paucity of information available on the impact of lockbox storage,” she explained.
The study by Dr. Wiencek and colleagues “provides some much-needed evidence for what is acceptable for lockbox storage conditions,” she said.
Areas of future research
Rodney E. Rohde, PhD, university distinguished chair and professor of the Clinical Laboratory Science (CLS) Program at Texas State University in San Marcos, said in an interview that the study “does a nice job of looking at multiple analytes and controlling for several variables,” but the sample size is small and the results may be difficult to generalize.
Dr. Pyle-Eilola highlighted another limitation — “a common shortcoming of these kinds of studies” — in the use of healthy donors for patient samples, which narrows the range of assay results.
“It is possible that more significant variation in results may be observed in additional analytes if the samples had higher concentrations of those analytes,” she said. “Moreover, this is clinically relevant as the samples stored in such lockboxes are not always from healthy individuals and have abnormal concentrations of analytes.”
Mario Plebani, MD, professor of clinical biochemistry and clinical molecular biology and chief of the department of laboratory medicine at University Hospital of Padova in Padova, Italy, agreed with that assessment.
“[T]he risks for errors and patient safety are higher for values near to the upper or lower reference value, and in general for samples collected in patients with particular diseases and clinical conditions,” he said in an interview.
“This paper deserves a commenting editorial to better highlight the urgent need for further studies on the same issue and in general on the risk in the pre-pre-analytical phase, including sample storage and transportation,” he noted.
Another area of future research is studying patient samples exposed to hotter or colder temperatures in outdoor courier lockboxes outside the mid-Atlantic area. “Here in Texas, temperatures can reach extreme heat levels,” Dr. Rohde said, who added that use of outdoor lockboxes is “very common in my region.”
Dr. Wiencek disclosed he has been a consultant on this research topic for Roche Diagnostics and received an honorarium for speaking on the subject from the American Association for Clinical Chemistry and American Society of Clinical Pathology. The other authors have no relevant conflict of interest. Dr. Pyle-Eilola, Dr. Rohde, and Dr. Plebani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to results from a recent study published in the American Journal of Clinical Pathology.
“Our findings indicate that samples (centrifuged or not centrifuged) were impacted by extreme summer temperatures when stored for short periods of time inside commonly used steel lockboxes,” Joseph R. Wiencek, PhD, medical director of clinical chemistry, Vanderbilt University School of Medicine Core Laboratory in Nashville, said in an interview.
Dr. Wiencek and colleagues picked two dates during the summer of 2019 in a mid-Atlantic state to place two courier lockboxes (LabLocker-KF300) outside in hot temperatures (32º C) starting at 11 a.m., with one lockbox containing two 24-oz cold packs (Nordic NI24) and the other containing no cold packs. The researchers monitored the temperatures of each lockbox over the course of 4 hours.
Overall, eight participants had seven samples in lithium heparin drawn for two studies evaluating centrifuged or not centrifuged samples. In the first study, four participants had seven samples drawn, with one centrifuged sample serving as a control for each patient. The other six samples were wrapped in paper towels, placed in resealable plastic bags, and distributed evenly in the warm and cold lockboxes. The samples did not directly touch the cold packs in the cold lockbox. At 1 hour, 2 hours, and 4 hours, a participant’s sample was removed from each lockbox and centrifuged.
In the second study, another four participants had seven samples drawn. As in the first study, all samples were centrifuged and placed in the lockboxes. For both studies, when samples were centrifuged, plasma from samples was left on the gel barrier when analyzed for concentrations of C-reactive protein, a comprehensive metabolic panel, lactate dehydrogenase (LDH), a lipid panel, magnesium, and phosphorus (Abbott Architect c16000).
In the study of uncentrifuged samples, Dr. Wiencek and colleagues found that when the temperature outside ranged from 28.2º to 44.0º C (mean 40.4º C), the temperature of the cold lockbox was between 16.5º to 22.3º C (mean 22.3º C). The temperature ranged between 34.4º to 46.9º C (mean 42.6º C) in the warm lockbox. For centrifuged samples, the cold lockbox temperature was between 12.2º to 23.0º C (mean 18.0º C) and the warm lockbox was between 25. to 40.8º C (mean 35.2º C) when the outdoor temperature ranged from 27.2º to 46.3º C (mean 37.9º C).
The researchers also calculated the significant change limit (SCL) for each analyte in each sample, finding that aspartate aminotransferase, glucose, LDH, and potassium significantly exceeded the SCL in both the centrifuged and uncentrifuged samples, with the greatest changes seen at the 4-hour timepoint for samples in the warm lockbox (P < .05 for all).
Lockbox instructions are “consistently inconsistent”
In viewing instructions for lockboxes across institutions, Dr. Wiencek said the “outdoor courier lockbox instructions among private, academic and reference laboratories were consistently inconsistent.” For example, no laboratories cited time restrictions for samples in lockboxes, and their descriptions on the number of cold packs a laboratory should use and where the lockbox should be placed varied. The inconsistencies “highlighted the emergent need for standardization and guidance documents for institutions to implement,” Dr. Wiencek said.
One unanswered question is how widespread the problem is. It is unclear how many outdoor courier lockboxes are currently in use in the United States or globally; however, experts agreed it was a common occurrence, with some of the largest laboratory service providers offering outdoor courier lockboxes to their clients.
“Courier lockboxes are everywhere. All you need to do is walk around your clinics that are at your hospitals or clinics located around your grocery store to find them,” Dr. Wiencek said. “Some hang on doors, while others can be found on the ground in direct sunlight on a hot summer day.”
What’s more, institutions may not realize how leaving samples outdoors for extended periods can affect results. “Care teams are commonly unaware that samples placed in these poorly designed lockboxes can experience extreme summer or winter temperatures that may lead to incorrect results,” Dr. Wiencek said. “Healthcare providers need to understand the hidden dangers courier lockboxes have on the quality of their patient’s test results.”
Amy L. Pyle-Eilola, PhD, clinical chemistry director at Nationwide Children’s Hospital in Columbus, Ohio, said a major strength of the study by Dr. Wiencek and colleagues “is just that it was done at all.”
“I appreciate the real-world nature of this study and that it provides a snapshot of what conditions are really like in a lockbox in the summer,” she said in an interview.
In the clinical lab, receiving samples that had been sitting in a courier lockbox “is not uncommon,” Dr. Pyle-Eilola said.
“When I have encountered these situations, I have struggled to decide if it is still appropriate to run the tests. I always look to the medical literature for assistance with these situations, but there has been a paucity of information available on the impact of lockbox storage,” she explained.
The study by Dr. Wiencek and colleagues “provides some much-needed evidence for what is acceptable for lockbox storage conditions,” she said.
Areas of future research
Rodney E. Rohde, PhD, university distinguished chair and professor of the Clinical Laboratory Science (CLS) Program at Texas State University in San Marcos, said in an interview that the study “does a nice job of looking at multiple analytes and controlling for several variables,” but the sample size is small and the results may be difficult to generalize.
Dr. Pyle-Eilola highlighted another limitation — “a common shortcoming of these kinds of studies” — in the use of healthy donors for patient samples, which narrows the range of assay results.
“It is possible that more significant variation in results may be observed in additional analytes if the samples had higher concentrations of those analytes,” she said. “Moreover, this is clinically relevant as the samples stored in such lockboxes are not always from healthy individuals and have abnormal concentrations of analytes.”
Mario Plebani, MD, professor of clinical biochemistry and clinical molecular biology and chief of the department of laboratory medicine at University Hospital of Padova in Padova, Italy, agreed with that assessment.
“[T]he risks for errors and patient safety are higher for values near to the upper or lower reference value, and in general for samples collected in patients with particular diseases and clinical conditions,” he said in an interview.
“This paper deserves a commenting editorial to better highlight the urgent need for further studies on the same issue and in general on the risk in the pre-pre-analytical phase, including sample storage and transportation,” he noted.
Another area of future research is studying patient samples exposed to hotter or colder temperatures in outdoor courier lockboxes outside the mid-Atlantic area. “Here in Texas, temperatures can reach extreme heat levels,” Dr. Rohde said, who added that use of outdoor lockboxes is “very common in my region.”
Dr. Wiencek disclosed he has been a consultant on this research topic for Roche Diagnostics and received an honorarium for speaking on the subject from the American Association for Clinical Chemistry and American Society of Clinical Pathology. The other authors have no relevant conflict of interest. Dr. Pyle-Eilola, Dr. Rohde, and Dr. Plebani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to results from a recent study published in the American Journal of Clinical Pathology.
“Our findings indicate that samples (centrifuged or not centrifuged) were impacted by extreme summer temperatures when stored for short periods of time inside commonly used steel lockboxes,” Joseph R. Wiencek, PhD, medical director of clinical chemistry, Vanderbilt University School of Medicine Core Laboratory in Nashville, said in an interview.
Dr. Wiencek and colleagues picked two dates during the summer of 2019 in a mid-Atlantic state to place two courier lockboxes (LabLocker-KF300) outside in hot temperatures (32º C) starting at 11 a.m., with one lockbox containing two 24-oz cold packs (Nordic NI24) and the other containing no cold packs. The researchers monitored the temperatures of each lockbox over the course of 4 hours.
Overall, eight participants had seven samples in lithium heparin drawn for two studies evaluating centrifuged or not centrifuged samples. In the first study, four participants had seven samples drawn, with one centrifuged sample serving as a control for each patient. The other six samples were wrapped in paper towels, placed in resealable plastic bags, and distributed evenly in the warm and cold lockboxes. The samples did not directly touch the cold packs in the cold lockbox. At 1 hour, 2 hours, and 4 hours, a participant’s sample was removed from each lockbox and centrifuged.
In the second study, another four participants had seven samples drawn. As in the first study, all samples were centrifuged and placed in the lockboxes. For both studies, when samples were centrifuged, plasma from samples was left on the gel barrier when analyzed for concentrations of C-reactive protein, a comprehensive metabolic panel, lactate dehydrogenase (LDH), a lipid panel, magnesium, and phosphorus (Abbott Architect c16000).
In the study of uncentrifuged samples, Dr. Wiencek and colleagues found that when the temperature outside ranged from 28.2º to 44.0º C (mean 40.4º C), the temperature of the cold lockbox was between 16.5º to 22.3º C (mean 22.3º C). The temperature ranged between 34.4º to 46.9º C (mean 42.6º C) in the warm lockbox. For centrifuged samples, the cold lockbox temperature was between 12.2º to 23.0º C (mean 18.0º C) and the warm lockbox was between 25. to 40.8º C (mean 35.2º C) when the outdoor temperature ranged from 27.2º to 46.3º C (mean 37.9º C).
The researchers also calculated the significant change limit (SCL) for each analyte in each sample, finding that aspartate aminotransferase, glucose, LDH, and potassium significantly exceeded the SCL in both the centrifuged and uncentrifuged samples, with the greatest changes seen at the 4-hour timepoint for samples in the warm lockbox (P < .05 for all).
Lockbox instructions are “consistently inconsistent”
In viewing instructions for lockboxes across institutions, Dr. Wiencek said the “outdoor courier lockbox instructions among private, academic and reference laboratories were consistently inconsistent.” For example, no laboratories cited time restrictions for samples in lockboxes, and their descriptions on the number of cold packs a laboratory should use and where the lockbox should be placed varied. The inconsistencies “highlighted the emergent need for standardization and guidance documents for institutions to implement,” Dr. Wiencek said.
One unanswered question is how widespread the problem is. It is unclear how many outdoor courier lockboxes are currently in use in the United States or globally; however, experts agreed it was a common occurrence, with some of the largest laboratory service providers offering outdoor courier lockboxes to their clients.
“Courier lockboxes are everywhere. All you need to do is walk around your clinics that are at your hospitals or clinics located around your grocery store to find them,” Dr. Wiencek said. “Some hang on doors, while others can be found on the ground in direct sunlight on a hot summer day.”
What’s more, institutions may not realize how leaving samples outdoors for extended periods can affect results. “Care teams are commonly unaware that samples placed in these poorly designed lockboxes can experience extreme summer or winter temperatures that may lead to incorrect results,” Dr. Wiencek said. “Healthcare providers need to understand the hidden dangers courier lockboxes have on the quality of their patient’s test results.”
Amy L. Pyle-Eilola, PhD, clinical chemistry director at Nationwide Children’s Hospital in Columbus, Ohio, said a major strength of the study by Dr. Wiencek and colleagues “is just that it was done at all.”
“I appreciate the real-world nature of this study and that it provides a snapshot of what conditions are really like in a lockbox in the summer,” she said in an interview.
In the clinical lab, receiving samples that had been sitting in a courier lockbox “is not uncommon,” Dr. Pyle-Eilola said.
“When I have encountered these situations, I have struggled to decide if it is still appropriate to run the tests. I always look to the medical literature for assistance with these situations, but there has been a paucity of information available on the impact of lockbox storage,” she explained.
The study by Dr. Wiencek and colleagues “provides some much-needed evidence for what is acceptable for lockbox storage conditions,” she said.
Areas of future research
Rodney E. Rohde, PhD, university distinguished chair and professor of the Clinical Laboratory Science (CLS) Program at Texas State University in San Marcos, said in an interview that the study “does a nice job of looking at multiple analytes and controlling for several variables,” but the sample size is small and the results may be difficult to generalize.
Dr. Pyle-Eilola highlighted another limitation — “a common shortcoming of these kinds of studies” — in the use of healthy donors for patient samples, which narrows the range of assay results.
“It is possible that more significant variation in results may be observed in additional analytes if the samples had higher concentrations of those analytes,” she said. “Moreover, this is clinically relevant as the samples stored in such lockboxes are not always from healthy individuals and have abnormal concentrations of analytes.”
Mario Plebani, MD, professor of clinical biochemistry and clinical molecular biology and chief of the department of laboratory medicine at University Hospital of Padova in Padova, Italy, agreed with that assessment.
“[T]he risks for errors and patient safety are higher for values near to the upper or lower reference value, and in general for samples collected in patients with particular diseases and clinical conditions,” he said in an interview.
“This paper deserves a commenting editorial to better highlight the urgent need for further studies on the same issue and in general on the risk in the pre-pre-analytical phase, including sample storage and transportation,” he noted.
Another area of future research is studying patient samples exposed to hotter or colder temperatures in outdoor courier lockboxes outside the mid-Atlantic area. “Here in Texas, temperatures can reach extreme heat levels,” Dr. Rohde said, who added that use of outdoor lockboxes is “very common in my region.”
Dr. Wiencek disclosed he has been a consultant on this research topic for Roche Diagnostics and received an honorarium for speaking on the subject from the American Association for Clinical Chemistry and American Society of Clinical Pathology. The other authors have no relevant conflict of interest. Dr. Pyle-Eilola, Dr. Rohde, and Dr. Plebani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA panel votes to approve Pfizer’s vaccine for children
Seventeen of the 18 members of the Vaccines and Related Biological Products Advisory Committee (VRBPAC) on Oct. 26 voted to recommend the 10-microgram shot for kids, which is one-third the dose given to adults.
One member, Michael Kurilla, MD, director of the division of clinical innovation at the National Institutes of Health, Bethesda, Md., abstained from voting.
If the FDA follows the recommendation, as it typically does, and issues an Emergency Use Authorization for the vaccine, the shots could be available within days.
After the FDA’s final decision, the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet to make specific recommendations for its use. The CDC committee must stick closely to the conditions for use spelled out in the EUA, so their recommendations are likely to be similar to those made by the FDA. Their next meeting is scheduled for Nov. 2 and 3.
In the end, some on the panel felt uneasy with their decision.
“I voted yes primarily because I wanted to make sure that children who really need this vaccine, the Black and brown children of our country, get the vaccine,” said James Hildreth, MD, PhD, president and CEO of Meharry Medical College in Nashville.
“But to be honest, the best way to protect the health of some children will be to do nothing because they will be just fine,” he said.
Others said they were surprised by how difficult the decision had been.
“This is a much tougher one than we had expected going into it,” said committee member Eric Rubin, MD, editor and chief of the New England Journal of Medicine, during the FDA advisory committee’s meeting.
Ahead of the vote, the committee heard presentations outlining the expected benefits of vaccinating children along with potential risks.
“Children have been greatly impacted by the pandemic,” said Fiona Havers, MD, a medical officer with the CDC in Atlanta who reviewed the epidemiology of COVID-19 in kids.
In the second year of the pandemic, as more seniors have been vaccinated against the virus, COVID cases have largely shifted from older to younger age groups.
So far, there have been more than 1.9 million COVID-19 cases in children ages 5 through 11 in the United States.. Cases in kids saw a big jump in July and August with summer travel, schools reopening, and the dominance of the Delta variant.
And those are just the cases reported to the CDC. Regular testing of anonymous blood samples collected at sites across the United States indicates that 6 times as many kids have had COVID than what is reflected in official counts.
Last winter, blood sample testing showed about 13% of children had antibodies against the virus, suggesting they’d been infected. By this summer, that number had risen to 42%.
That figure clearly made an impression on many members of the committee who asked the FDA’s vaccine reviewers if they had tried to account for immunity from past infections in their modeling. They had not.
Some felt that even with a highly effective vaccine — new data presented by Pfizer showed the children’s dose was 90% effective at preventing symptomatic infections in kids — caution was warranted as much is still unknown about myocarditis, a rare side effect of the mRNA vaccines.
Myocarditis has been more common in younger age groups. It usually goes away over time but requires hospital care. It’s not known if myocarditis could have lingering effects for those who experience it.
There were no cases of myocarditis seen in Pfizer’s studies of the vaccine in children, and no other serious events were seen. Vaccine side effects reported in the Pfizer studies were mostly mild and included fatigue, headache, and pain at the injection site.
“We think we have optimized the immune response and minimized our reactions,” said William Gruber, MD, senior vice president vaccine research and clinical development at Pfizer.
But the studies didn’t include enough participants to pick up rare, but serious adverse events like myocarditis.
“We’re worried about a side effect that we can’t measure yet, but it’s probably real, and we see a benefit that isn’t the same as it is in older age groups,” said Dr. Rubin.
Benefits vs. risks
FDA modeled the benefits and risks for children under a variety of scenarios. The benefits of the vaccines to children very much depend on the amount of transmission in the community.
When transmission is high, the benefits to children — in terms of infections, hospitalizations, ICU admissions — clearly outweigh its risks.
But when COVID-19 rates are low in the community, as they were in June, FDA analysts predicted the vaccines might send more children to the hospital for myocarditis than the virus would.
The FDA noted that kids who are hospitalized for myocarditis tend not to be as ill as children with COVID-19, however.
“If the trends continue the way they are going, the emergency for children is not what we might think it would be. That was my concern,” Dr. Hildreth said.
But others warned against complacency.
“Thinking that this is going to be the end of the wave permanently may be a little overly optimistic,” said committee chairman Arnold Monto, MD, a professor of public health and epidemiology at the University of Michigan, Ann Arbor.
The majority of COVID-19 cases in children are mild. Only about 1% of kids are hospitalized for their infections, according to CDC data. But the rates of hospitalizations in kids are about 3 times higher for people of color — including Blacks, Hispanics, and Native Americans, as compared to Whites and Asian Americans.
Since the start of the pandemic, 94 children ages 5 to 11 have died, making it the eighth leading cause of death for kids this age last year.
More than 5,200 children have developed a delayed complication from their infections called Multi-System Inflammatory Syndrome (MIS-C).
MIS-C can be severe and require hospital care and can lead to myocarditis. Children ages 5 to 11 are the age group at greatest risk for this complication.
Kids can also get long COVID. There’s not a lot of data on how often this happens, though it appears to be less frequent in children than in adults.
But a survey in the United Kingdom found that 7%-8% of kids have symptoms from their infections that last longer than 12 weeks, Dr. Havers said. Symptoms that can linger for kids include fatigue, cough, muscle and joint pain, headaches, and insomnia.
More than 1 million children have been impacted by school closures so far this year, and quarantines have had lasting impacts on learning, social development, and mental health.
Even though kids aren’t usually COVID superspreaders, they can still pass the infection on to others.
“What is clear is that secondary transmission from children, both to other children and to adults, does occur,” Dr. Havers said.
For that reason, they can continue the spread of the virus and give it opportunities to mutate and become more dangerous.
Safety monitoring to continue
Some committee members referenced thousands of letters they had received within the past few days urging them to vote against the vaccine.
Jay Portnoy, MD, a professor of pediatrics at Children’s Mercy Hospital in Kansas City, Mo., said he had personally received about 4,000 emails.
“But I feel like I need to also represent the consumers, the parents that I see every day in the clinic who are terrified of sending their children to school because they’re not protected against COVID,” he said, explaining his vote to recommend authorization.
“Our kids are going to be dealing with this virus for many years to come. It’s going to come repeatedly. Getting this vaccine is just the first step that they can take to protect themselves from having bad outcomes,” Dr. Portnoy said.
Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, reminded members of the committee that there were several government surveillance systems in place to catch any potential safety issues in near real time.
“I really appreciate very much the concern here. The safety monitoring of this vaccine will continue,” Dr. Marks said. “I do view this as one of our greatest responsibilities.”
“I really am so grateful that we had this discussion and voted to approve,” said Capt. Amanda Cohn, MD, chief medical officer at the National Center for Immunization and Respiratory Diseases.
“I think the benefits in this age group really are super important even if they are lower than for other age groups.”
This article was updated 10/27/21.
A version of this article first appeared on WebMD.com.
Seventeen of the 18 members of the Vaccines and Related Biological Products Advisory Committee (VRBPAC) on Oct. 26 voted to recommend the 10-microgram shot for kids, which is one-third the dose given to adults.
One member, Michael Kurilla, MD, director of the division of clinical innovation at the National Institutes of Health, Bethesda, Md., abstained from voting.
If the FDA follows the recommendation, as it typically does, and issues an Emergency Use Authorization for the vaccine, the shots could be available within days.
After the FDA’s final decision, the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet to make specific recommendations for its use. The CDC committee must stick closely to the conditions for use spelled out in the EUA, so their recommendations are likely to be similar to those made by the FDA. Their next meeting is scheduled for Nov. 2 and 3.
In the end, some on the panel felt uneasy with their decision.
“I voted yes primarily because I wanted to make sure that children who really need this vaccine, the Black and brown children of our country, get the vaccine,” said James Hildreth, MD, PhD, president and CEO of Meharry Medical College in Nashville.
“But to be honest, the best way to protect the health of some children will be to do nothing because they will be just fine,” he said.
Others said they were surprised by how difficult the decision had been.
“This is a much tougher one than we had expected going into it,” said committee member Eric Rubin, MD, editor and chief of the New England Journal of Medicine, during the FDA advisory committee’s meeting.
Ahead of the vote, the committee heard presentations outlining the expected benefits of vaccinating children along with potential risks.
“Children have been greatly impacted by the pandemic,” said Fiona Havers, MD, a medical officer with the CDC in Atlanta who reviewed the epidemiology of COVID-19 in kids.
In the second year of the pandemic, as more seniors have been vaccinated against the virus, COVID cases have largely shifted from older to younger age groups.
So far, there have been more than 1.9 million COVID-19 cases in children ages 5 through 11 in the United States.. Cases in kids saw a big jump in July and August with summer travel, schools reopening, and the dominance of the Delta variant.
And those are just the cases reported to the CDC. Regular testing of anonymous blood samples collected at sites across the United States indicates that 6 times as many kids have had COVID than what is reflected in official counts.
Last winter, blood sample testing showed about 13% of children had antibodies against the virus, suggesting they’d been infected. By this summer, that number had risen to 42%.
That figure clearly made an impression on many members of the committee who asked the FDA’s vaccine reviewers if they had tried to account for immunity from past infections in their modeling. They had not.
Some felt that even with a highly effective vaccine — new data presented by Pfizer showed the children’s dose was 90% effective at preventing symptomatic infections in kids — caution was warranted as much is still unknown about myocarditis, a rare side effect of the mRNA vaccines.
Myocarditis has been more common in younger age groups. It usually goes away over time but requires hospital care. It’s not known if myocarditis could have lingering effects for those who experience it.
There were no cases of myocarditis seen in Pfizer’s studies of the vaccine in children, and no other serious events were seen. Vaccine side effects reported in the Pfizer studies were mostly mild and included fatigue, headache, and pain at the injection site.
“We think we have optimized the immune response and minimized our reactions,” said William Gruber, MD, senior vice president vaccine research and clinical development at Pfizer.
But the studies didn’t include enough participants to pick up rare, but serious adverse events like myocarditis.
“We’re worried about a side effect that we can’t measure yet, but it’s probably real, and we see a benefit that isn’t the same as it is in older age groups,” said Dr. Rubin.
Benefits vs. risks
FDA modeled the benefits and risks for children under a variety of scenarios. The benefits of the vaccines to children very much depend on the amount of transmission in the community.
When transmission is high, the benefits to children — in terms of infections, hospitalizations, ICU admissions — clearly outweigh its risks.
But when COVID-19 rates are low in the community, as they were in June, FDA analysts predicted the vaccines might send more children to the hospital for myocarditis than the virus would.
The FDA noted that kids who are hospitalized for myocarditis tend not to be as ill as children with COVID-19, however.
“If the trends continue the way they are going, the emergency for children is not what we might think it would be. That was my concern,” Dr. Hildreth said.
But others warned against complacency.
“Thinking that this is going to be the end of the wave permanently may be a little overly optimistic,” said committee chairman Arnold Monto, MD, a professor of public health and epidemiology at the University of Michigan, Ann Arbor.
The majority of COVID-19 cases in children are mild. Only about 1% of kids are hospitalized for their infections, according to CDC data. But the rates of hospitalizations in kids are about 3 times higher for people of color — including Blacks, Hispanics, and Native Americans, as compared to Whites and Asian Americans.
Since the start of the pandemic, 94 children ages 5 to 11 have died, making it the eighth leading cause of death for kids this age last year.
More than 5,200 children have developed a delayed complication from their infections called Multi-System Inflammatory Syndrome (MIS-C).
MIS-C can be severe and require hospital care and can lead to myocarditis. Children ages 5 to 11 are the age group at greatest risk for this complication.
Kids can also get long COVID. There’s not a lot of data on how often this happens, though it appears to be less frequent in children than in adults.
But a survey in the United Kingdom found that 7%-8% of kids have symptoms from their infections that last longer than 12 weeks, Dr. Havers said. Symptoms that can linger for kids include fatigue, cough, muscle and joint pain, headaches, and insomnia.
More than 1 million children have been impacted by school closures so far this year, and quarantines have had lasting impacts on learning, social development, and mental health.
Even though kids aren’t usually COVID superspreaders, they can still pass the infection on to others.
“What is clear is that secondary transmission from children, both to other children and to adults, does occur,” Dr. Havers said.
For that reason, they can continue the spread of the virus and give it opportunities to mutate and become more dangerous.
Safety monitoring to continue
Some committee members referenced thousands of letters they had received within the past few days urging them to vote against the vaccine.
Jay Portnoy, MD, a professor of pediatrics at Children’s Mercy Hospital in Kansas City, Mo., said he had personally received about 4,000 emails.
“But I feel like I need to also represent the consumers, the parents that I see every day in the clinic who are terrified of sending their children to school because they’re not protected against COVID,” he said, explaining his vote to recommend authorization.
“Our kids are going to be dealing with this virus for many years to come. It’s going to come repeatedly. Getting this vaccine is just the first step that they can take to protect themselves from having bad outcomes,” Dr. Portnoy said.
Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, reminded members of the committee that there were several government surveillance systems in place to catch any potential safety issues in near real time.
“I really appreciate very much the concern here. The safety monitoring of this vaccine will continue,” Dr. Marks said. “I do view this as one of our greatest responsibilities.”
“I really am so grateful that we had this discussion and voted to approve,” said Capt. Amanda Cohn, MD, chief medical officer at the National Center for Immunization and Respiratory Diseases.
“I think the benefits in this age group really are super important even if they are lower than for other age groups.”
This article was updated 10/27/21.
A version of this article first appeared on WebMD.com.
Seventeen of the 18 members of the Vaccines and Related Biological Products Advisory Committee (VRBPAC) on Oct. 26 voted to recommend the 10-microgram shot for kids, which is one-third the dose given to adults.
One member, Michael Kurilla, MD, director of the division of clinical innovation at the National Institutes of Health, Bethesda, Md., abstained from voting.
If the FDA follows the recommendation, as it typically does, and issues an Emergency Use Authorization for the vaccine, the shots could be available within days.
After the FDA’s final decision, the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet to make specific recommendations for its use. The CDC committee must stick closely to the conditions for use spelled out in the EUA, so their recommendations are likely to be similar to those made by the FDA. Their next meeting is scheduled for Nov. 2 and 3.
In the end, some on the panel felt uneasy with their decision.
“I voted yes primarily because I wanted to make sure that children who really need this vaccine, the Black and brown children of our country, get the vaccine,” said James Hildreth, MD, PhD, president and CEO of Meharry Medical College in Nashville.
“But to be honest, the best way to protect the health of some children will be to do nothing because they will be just fine,” he said.
Others said they were surprised by how difficult the decision had been.
“This is a much tougher one than we had expected going into it,” said committee member Eric Rubin, MD, editor and chief of the New England Journal of Medicine, during the FDA advisory committee’s meeting.
Ahead of the vote, the committee heard presentations outlining the expected benefits of vaccinating children along with potential risks.
“Children have been greatly impacted by the pandemic,” said Fiona Havers, MD, a medical officer with the CDC in Atlanta who reviewed the epidemiology of COVID-19 in kids.
In the second year of the pandemic, as more seniors have been vaccinated against the virus, COVID cases have largely shifted from older to younger age groups.
So far, there have been more than 1.9 million COVID-19 cases in children ages 5 through 11 in the United States.. Cases in kids saw a big jump in July and August with summer travel, schools reopening, and the dominance of the Delta variant.
And those are just the cases reported to the CDC. Regular testing of anonymous blood samples collected at sites across the United States indicates that 6 times as many kids have had COVID than what is reflected in official counts.
Last winter, blood sample testing showed about 13% of children had antibodies against the virus, suggesting they’d been infected. By this summer, that number had risen to 42%.
That figure clearly made an impression on many members of the committee who asked the FDA’s vaccine reviewers if they had tried to account for immunity from past infections in their modeling. They had not.
Some felt that even with a highly effective vaccine — new data presented by Pfizer showed the children’s dose was 90% effective at preventing symptomatic infections in kids — caution was warranted as much is still unknown about myocarditis, a rare side effect of the mRNA vaccines.
Myocarditis has been more common in younger age groups. It usually goes away over time but requires hospital care. It’s not known if myocarditis could have lingering effects for those who experience it.
There were no cases of myocarditis seen in Pfizer’s studies of the vaccine in children, and no other serious events were seen. Vaccine side effects reported in the Pfizer studies were mostly mild and included fatigue, headache, and pain at the injection site.
“We think we have optimized the immune response and minimized our reactions,” said William Gruber, MD, senior vice president vaccine research and clinical development at Pfizer.
But the studies didn’t include enough participants to pick up rare, but serious adverse events like myocarditis.
“We’re worried about a side effect that we can’t measure yet, but it’s probably real, and we see a benefit that isn’t the same as it is in older age groups,” said Dr. Rubin.
Benefits vs. risks
FDA modeled the benefits and risks for children under a variety of scenarios. The benefits of the vaccines to children very much depend on the amount of transmission in the community.
When transmission is high, the benefits to children — in terms of infections, hospitalizations, ICU admissions — clearly outweigh its risks.
But when COVID-19 rates are low in the community, as they were in June, FDA analysts predicted the vaccines might send more children to the hospital for myocarditis than the virus would.
The FDA noted that kids who are hospitalized for myocarditis tend not to be as ill as children with COVID-19, however.
“If the trends continue the way they are going, the emergency for children is not what we might think it would be. That was my concern,” Dr. Hildreth said.
But others warned against complacency.
“Thinking that this is going to be the end of the wave permanently may be a little overly optimistic,” said committee chairman Arnold Monto, MD, a professor of public health and epidemiology at the University of Michigan, Ann Arbor.
The majority of COVID-19 cases in children are mild. Only about 1% of kids are hospitalized for their infections, according to CDC data. But the rates of hospitalizations in kids are about 3 times higher for people of color — including Blacks, Hispanics, and Native Americans, as compared to Whites and Asian Americans.
Since the start of the pandemic, 94 children ages 5 to 11 have died, making it the eighth leading cause of death for kids this age last year.
More than 5,200 children have developed a delayed complication from their infections called Multi-System Inflammatory Syndrome (MIS-C).
MIS-C can be severe and require hospital care and can lead to myocarditis. Children ages 5 to 11 are the age group at greatest risk for this complication.
Kids can also get long COVID. There’s not a lot of data on how often this happens, though it appears to be less frequent in children than in adults.
But a survey in the United Kingdom found that 7%-8% of kids have symptoms from their infections that last longer than 12 weeks, Dr. Havers said. Symptoms that can linger for kids include fatigue, cough, muscle and joint pain, headaches, and insomnia.
More than 1 million children have been impacted by school closures so far this year, and quarantines have had lasting impacts on learning, social development, and mental health.
Even though kids aren’t usually COVID superspreaders, they can still pass the infection on to others.
“What is clear is that secondary transmission from children, both to other children and to adults, does occur,” Dr. Havers said.
For that reason, they can continue the spread of the virus and give it opportunities to mutate and become more dangerous.
Safety monitoring to continue
Some committee members referenced thousands of letters they had received within the past few days urging them to vote against the vaccine.
Jay Portnoy, MD, a professor of pediatrics at Children’s Mercy Hospital in Kansas City, Mo., said he had personally received about 4,000 emails.
“But I feel like I need to also represent the consumers, the parents that I see every day in the clinic who are terrified of sending their children to school because they’re not protected against COVID,” he said, explaining his vote to recommend authorization.
“Our kids are going to be dealing with this virus for many years to come. It’s going to come repeatedly. Getting this vaccine is just the first step that they can take to protect themselves from having bad outcomes,” Dr. Portnoy said.
Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, reminded members of the committee that there were several government surveillance systems in place to catch any potential safety issues in near real time.
“I really appreciate very much the concern here. The safety monitoring of this vaccine will continue,” Dr. Marks said. “I do view this as one of our greatest responsibilities.”
“I really am so grateful that we had this discussion and voted to approve,” said Capt. Amanda Cohn, MD, chief medical officer at the National Center for Immunization and Respiratory Diseases.
“I think the benefits in this age group really are super important even if they are lower than for other age groups.”
This article was updated 10/27/21.
A version of this article first appeared on WebMD.com.
Vitamin D status may play a pivotal role in colon cancer prevention
This is according to an observational study published in the journal Gastroenterology. The study included 94,205 women (aged 25-42 years) who were followed between 1991 and 2015 during which 111 incident cases of early-onset colorectal cancer were diagnosed. Among 29,186 women who had at least one lower endoscopy from 1991 to 2011, 1,439 newly diagnosed conventional adenomas and 1,878 serrated polyps were found.
Women who consumed the highest average levels of total vitamin D of 450 IU per day, compared with those consuming less than 300 IU per day, showed a significantly reduced risk of early-onset colorectal cancer. Consuming 400 IU each day was associated with a 54% reduced risk of early-onset colorectal cancer.
“If confirmed, our findings could potentially lead to recommendations for higher vitamin D intake as an inexpensive low-risk complement to colorectal cancer screening as a prevention strategy for adults younger than age 50,” wrote the study authors, led by Edward L. Giovannucci, MD, ScD, of the Harvard School of Public Health, Boston.
Associations between vitamin D levels and colorectal cancer have been documented in review articles over the years. The link is the subject of 10 recently completed or ongoing clinical trials. Few studies have focused on early colorectal cancer and vitamin D intake. Unlike advanced colorectal cancer, the early-onset form of the disease is not as strongly associated with the traditional risk factors of a family history of colorectal cancer and it is therefore believed to be more strongly linked to other factors, such as lifestyle and diet – including vitamin D supplementation.
The evidence is in, but it’s incomplete
In addition to the new study in Gastroenterology, other observational studies, as well as laboratory and animal studies, suggest that vitamin D plays a role in inhibiting carcinogenesis. Vitamin D, researchers theorize, contains anti-inflammatory, immunomodulatory, and tumor angiogenesis properties that can slow the growth of tumors, but the evidence is mixed.
A meta-analysis of 137,567 patients published in 2013 in Preventive Medicine found an inverse association between 25-hydroxyvitamin D (25[OH]D) and total cancer mortality in women, but not among men. Three meta-analyses published in 2014 and 2019 found that vitamin D supplementation does not affect cancer incidence but does significantly reduce total cancer mortality rates by 12%-13%.
In 2019, researchers led by Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research for the American Cancer Society, described a causal relationship between circulating vitamin D and colorectal cancer risk among 17 cohorts from a pooled analysis. “Our study suggests that optimal circulating 25(OH)D concentrations for colorectal cancer risk reduction are 75-100 nmol/L, [which is] higher than current Institute of Medicine recommendations for bone health,” she and colleagues wrote. Their findings were published in the Journal of the National Cancer Institute.
The Vitamin D and Omega-3 Trial (VITAL) published in 2019 in the New England Journal of Medicine, showed no significant effect of vitamin D3 supplementation of 2,000 IU/day in lowering the risk of invasive cancer or cardiovascular events.
Despite the mixed results, studies offer valuable insights into cancer risks, said Scott Kopetz, MD, PhD, codirector of the colorectal cancer moon shot research program at the University of Texas MD Anderson Cancer Center, Houston.
The Gastroenterology study is noteworthy because it focuses on early-onset colorectal cancer, he said.
“[The authors] demonstrate for the first time that there is an association of vitamin D intake with early-onset colorectal incidence, especially in the left side of the colon and rectum where the increase in early onset colorectal cancer manifests,” Dr. Kopetz said. “The analysis suggests that it may require long-term vitamin D intake to derive the benefit, which may explain why some shorter-term randomized studies failed to demonstrate.”
In animal models, vitamin D3 is “estimated to lower the incidence of colorectal cancer by 50%,” according to Lidija Klampfer, PhD, formerly a molecular biologist and senior research scientist with the Southern Research Institute, Birmingham, Ala.
Dr. Klampfer, a founding partner of ProteXase Therapeutics, is the author of an article on vitamin D and colon cancer published in 2014 in the World Journal of Gastrointestinal Oncology.
“The levels of vitamin D3 appear to be an essential determinant for the development and progression of colon cancer and supplementation with vitamin D3 is effective in suppressing intestinal tumorigenesis in animal models,” she wrote. “Studies have shown that 1,25 dihydroxyvitamin D3 can inhibit tumor-promoting inflammation leading to the development and progression of colon cancer.”
The hazards of a vitamin D deficiency
A severe vitamin D deficiency is associated with compromised bone and muscle health, calcium absorption, immunity, heart function and it can affect mood. Other studies have linked vitamin D deficiency to colorectal cancer, blood cancers, and bowel cancer.
Serum 25(OH)D is the primary circulating form of vitamin D and is considered the best marker for assessing vitamin D status, says Karin Amrein, MD, MSc, an endocrinologist with the Medical University of Graz (Austria). She was the lead author of a review on vitamin D deficiency published in January 2020 in the European Journal of Clinical Nutrition.
The Global Consensus Recommendations define vitamin D insufficiency as 12-20 ng/mL (30-50 nmol/L) and a deficiency as a serum 25OHD concentration less than 12 ng/mL (30 nmol/L). A deficiency in adults is usually treated with 50,000 IU of vitamin D2 or D3 once weekly for 8 weeks followed by maintenance dosages of cholecalciferol (vitamin D3) at 800-1,000 IU daily from dietary and supplemental sources.
Screening is recommended for individuals who exhibit symptoms and conditions associated with a vitamin D deficiency, but there is little agreement on recommended serum levels because every individual is different, according to the U.S. Preventive Services Task Force which updated its vitamin D recommendations in April for the first time in 7 years.
This is according to an observational study published in the journal Gastroenterology. The study included 94,205 women (aged 25-42 years) who were followed between 1991 and 2015 during which 111 incident cases of early-onset colorectal cancer were diagnosed. Among 29,186 women who had at least one lower endoscopy from 1991 to 2011, 1,439 newly diagnosed conventional adenomas and 1,878 serrated polyps were found.
Women who consumed the highest average levels of total vitamin D of 450 IU per day, compared with those consuming less than 300 IU per day, showed a significantly reduced risk of early-onset colorectal cancer. Consuming 400 IU each day was associated with a 54% reduced risk of early-onset colorectal cancer.
“If confirmed, our findings could potentially lead to recommendations for higher vitamin D intake as an inexpensive low-risk complement to colorectal cancer screening as a prevention strategy for adults younger than age 50,” wrote the study authors, led by Edward L. Giovannucci, MD, ScD, of the Harvard School of Public Health, Boston.
Associations between vitamin D levels and colorectal cancer have been documented in review articles over the years. The link is the subject of 10 recently completed or ongoing clinical trials. Few studies have focused on early colorectal cancer and vitamin D intake. Unlike advanced colorectal cancer, the early-onset form of the disease is not as strongly associated with the traditional risk factors of a family history of colorectal cancer and it is therefore believed to be more strongly linked to other factors, such as lifestyle and diet – including vitamin D supplementation.
The evidence is in, but it’s incomplete
In addition to the new study in Gastroenterology, other observational studies, as well as laboratory and animal studies, suggest that vitamin D plays a role in inhibiting carcinogenesis. Vitamin D, researchers theorize, contains anti-inflammatory, immunomodulatory, and tumor angiogenesis properties that can slow the growth of tumors, but the evidence is mixed.
A meta-analysis of 137,567 patients published in 2013 in Preventive Medicine found an inverse association between 25-hydroxyvitamin D (25[OH]D) and total cancer mortality in women, but not among men. Three meta-analyses published in 2014 and 2019 found that vitamin D supplementation does not affect cancer incidence but does significantly reduce total cancer mortality rates by 12%-13%.
In 2019, researchers led by Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research for the American Cancer Society, described a causal relationship between circulating vitamin D and colorectal cancer risk among 17 cohorts from a pooled analysis. “Our study suggests that optimal circulating 25(OH)D concentrations for colorectal cancer risk reduction are 75-100 nmol/L, [which is] higher than current Institute of Medicine recommendations for bone health,” she and colleagues wrote. Their findings were published in the Journal of the National Cancer Institute.
The Vitamin D and Omega-3 Trial (VITAL) published in 2019 in the New England Journal of Medicine, showed no significant effect of vitamin D3 supplementation of 2,000 IU/day in lowering the risk of invasive cancer or cardiovascular events.
Despite the mixed results, studies offer valuable insights into cancer risks, said Scott Kopetz, MD, PhD, codirector of the colorectal cancer moon shot research program at the University of Texas MD Anderson Cancer Center, Houston.
The Gastroenterology study is noteworthy because it focuses on early-onset colorectal cancer, he said.
“[The authors] demonstrate for the first time that there is an association of vitamin D intake with early-onset colorectal incidence, especially in the left side of the colon and rectum where the increase in early onset colorectal cancer manifests,” Dr. Kopetz said. “The analysis suggests that it may require long-term vitamin D intake to derive the benefit, which may explain why some shorter-term randomized studies failed to demonstrate.”
In animal models, vitamin D3 is “estimated to lower the incidence of colorectal cancer by 50%,” according to Lidija Klampfer, PhD, formerly a molecular biologist and senior research scientist with the Southern Research Institute, Birmingham, Ala.
Dr. Klampfer, a founding partner of ProteXase Therapeutics, is the author of an article on vitamin D and colon cancer published in 2014 in the World Journal of Gastrointestinal Oncology.
“The levels of vitamin D3 appear to be an essential determinant for the development and progression of colon cancer and supplementation with vitamin D3 is effective in suppressing intestinal tumorigenesis in animal models,” she wrote. “Studies have shown that 1,25 dihydroxyvitamin D3 can inhibit tumor-promoting inflammation leading to the development and progression of colon cancer.”
The hazards of a vitamin D deficiency
A severe vitamin D deficiency is associated with compromised bone and muscle health, calcium absorption, immunity, heart function and it can affect mood. Other studies have linked vitamin D deficiency to colorectal cancer, blood cancers, and bowel cancer.
Serum 25(OH)D is the primary circulating form of vitamin D and is considered the best marker for assessing vitamin D status, says Karin Amrein, MD, MSc, an endocrinologist with the Medical University of Graz (Austria). She was the lead author of a review on vitamin D deficiency published in January 2020 in the European Journal of Clinical Nutrition.
The Global Consensus Recommendations define vitamin D insufficiency as 12-20 ng/mL (30-50 nmol/L) and a deficiency as a serum 25OHD concentration less than 12 ng/mL (30 nmol/L). A deficiency in adults is usually treated with 50,000 IU of vitamin D2 or D3 once weekly for 8 weeks followed by maintenance dosages of cholecalciferol (vitamin D3) at 800-1,000 IU daily from dietary and supplemental sources.
Screening is recommended for individuals who exhibit symptoms and conditions associated with a vitamin D deficiency, but there is little agreement on recommended serum levels because every individual is different, according to the U.S. Preventive Services Task Force which updated its vitamin D recommendations in April for the first time in 7 years.
This is according to an observational study published in the journal Gastroenterology. The study included 94,205 women (aged 25-42 years) who were followed between 1991 and 2015 during which 111 incident cases of early-onset colorectal cancer were diagnosed. Among 29,186 women who had at least one lower endoscopy from 1991 to 2011, 1,439 newly diagnosed conventional adenomas and 1,878 serrated polyps were found.
Women who consumed the highest average levels of total vitamin D of 450 IU per day, compared with those consuming less than 300 IU per day, showed a significantly reduced risk of early-onset colorectal cancer. Consuming 400 IU each day was associated with a 54% reduced risk of early-onset colorectal cancer.
“If confirmed, our findings could potentially lead to recommendations for higher vitamin D intake as an inexpensive low-risk complement to colorectal cancer screening as a prevention strategy for adults younger than age 50,” wrote the study authors, led by Edward L. Giovannucci, MD, ScD, of the Harvard School of Public Health, Boston.
Associations between vitamin D levels and colorectal cancer have been documented in review articles over the years. The link is the subject of 10 recently completed or ongoing clinical trials. Few studies have focused on early colorectal cancer and vitamin D intake. Unlike advanced colorectal cancer, the early-onset form of the disease is not as strongly associated with the traditional risk factors of a family history of colorectal cancer and it is therefore believed to be more strongly linked to other factors, such as lifestyle and diet – including vitamin D supplementation.
The evidence is in, but it’s incomplete
In addition to the new study in Gastroenterology, other observational studies, as well as laboratory and animal studies, suggest that vitamin D plays a role in inhibiting carcinogenesis. Vitamin D, researchers theorize, contains anti-inflammatory, immunomodulatory, and tumor angiogenesis properties that can slow the growth of tumors, but the evidence is mixed.
A meta-analysis of 137,567 patients published in 2013 in Preventive Medicine found an inverse association between 25-hydroxyvitamin D (25[OH]D) and total cancer mortality in women, but not among men. Three meta-analyses published in 2014 and 2019 found that vitamin D supplementation does not affect cancer incidence but does significantly reduce total cancer mortality rates by 12%-13%.
In 2019, researchers led by Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research for the American Cancer Society, described a causal relationship between circulating vitamin D and colorectal cancer risk among 17 cohorts from a pooled analysis. “Our study suggests that optimal circulating 25(OH)D concentrations for colorectal cancer risk reduction are 75-100 nmol/L, [which is] higher than current Institute of Medicine recommendations for bone health,” she and colleagues wrote. Their findings were published in the Journal of the National Cancer Institute.
The Vitamin D and Omega-3 Trial (VITAL) published in 2019 in the New England Journal of Medicine, showed no significant effect of vitamin D3 supplementation of 2,000 IU/day in lowering the risk of invasive cancer or cardiovascular events.
Despite the mixed results, studies offer valuable insights into cancer risks, said Scott Kopetz, MD, PhD, codirector of the colorectal cancer moon shot research program at the University of Texas MD Anderson Cancer Center, Houston.
The Gastroenterology study is noteworthy because it focuses on early-onset colorectal cancer, he said.
“[The authors] demonstrate for the first time that there is an association of vitamin D intake with early-onset colorectal incidence, especially in the left side of the colon and rectum where the increase in early onset colorectal cancer manifests,” Dr. Kopetz said. “The analysis suggests that it may require long-term vitamin D intake to derive the benefit, which may explain why some shorter-term randomized studies failed to demonstrate.”
In animal models, vitamin D3 is “estimated to lower the incidence of colorectal cancer by 50%,” according to Lidija Klampfer, PhD, formerly a molecular biologist and senior research scientist with the Southern Research Institute, Birmingham, Ala.
Dr. Klampfer, a founding partner of ProteXase Therapeutics, is the author of an article on vitamin D and colon cancer published in 2014 in the World Journal of Gastrointestinal Oncology.
“The levels of vitamin D3 appear to be an essential determinant for the development and progression of colon cancer and supplementation with vitamin D3 is effective in suppressing intestinal tumorigenesis in animal models,” she wrote. “Studies have shown that 1,25 dihydroxyvitamin D3 can inhibit tumor-promoting inflammation leading to the development and progression of colon cancer.”
The hazards of a vitamin D deficiency
A severe vitamin D deficiency is associated with compromised bone and muscle health, calcium absorption, immunity, heart function and it can affect mood. Other studies have linked vitamin D deficiency to colorectal cancer, blood cancers, and bowel cancer.
Serum 25(OH)D is the primary circulating form of vitamin D and is considered the best marker for assessing vitamin D status, says Karin Amrein, MD, MSc, an endocrinologist with the Medical University of Graz (Austria). She was the lead author of a review on vitamin D deficiency published in January 2020 in the European Journal of Clinical Nutrition.
The Global Consensus Recommendations define vitamin D insufficiency as 12-20 ng/mL (30-50 nmol/L) and a deficiency as a serum 25OHD concentration less than 12 ng/mL (30 nmol/L). A deficiency in adults is usually treated with 50,000 IU of vitamin D2 or D3 once weekly for 8 weeks followed by maintenance dosages of cholecalciferol (vitamin D3) at 800-1,000 IU daily from dietary and supplemental sources.
Screening is recommended for individuals who exhibit symptoms and conditions associated with a vitamin D deficiency, but there is little agreement on recommended serum levels because every individual is different, according to the U.S. Preventive Services Task Force which updated its vitamin D recommendations in April for the first time in 7 years.
FROM GASTROENTEROLOGY