User login
Clinical Endocrinology News is an independent news source that provides endocrinologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the endocrinologist's practice. Specialty topics include Diabetes, Lipid & Metabolic Disorders Menopause, Obesity, Osteoporosis, Pediatric Endocrinology, Pituitary, Thyroid & Adrenal Disorders, and Reproductive Endocrinology. Featured content includes Commentaries, Implementin Health Reform, Law & Medicine, and In the Loop, the blog of Clinical Endocrinology News. Clinical Endocrinology News is owned by Frontline Medical Communications.
addict
addicted
addicting
addiction
adult sites
alcohol
antibody
ass
attorney
audit
auditor
babies
babpa
baby
ban
banned
banning
best
bisexual
bitch
bleach
blog
blow job
bondage
boobs
booty
buy
cannabis
certificate
certification
certified
cheap
cheapest
class action
cocaine
cock
counterfeit drug
crack
crap
crime
criminal
cunt
curable
cure
dangerous
dangers
dead
deadly
death
defend
defended
depedent
dependence
dependent
detergent
dick
die
dildo
drug abuse
drug recall
dying
fag
fake
fatal
fatalities
fatality
free
fuck
gangs
gingivitis
guns
hardcore
herbal
herbs
heroin
herpes
home remedies
homo
horny
hypersensitivity
hypoglycemia treatment
illegal drug use
illegal use of prescription
incest
infant
infants
job
ketoacidosis
kill
killer
killing
kinky
law suit
lawsuit
lawyer
lesbian
marijuana
medicine for hypoglycemia
murder
naked
natural
newborn
nigger
noise
nude
nudity
orgy
over the counter
overdosage
overdose
overdosed
overdosing
penis
pimp
pistol
porn
porno
pornographic
pornography
prison
profanity
purchase
purchasing
pussy
queer
rape
rapist
recall
recreational drug
rob
robberies
sale
sales
sex
sexual
shit
shoot
slut
slutty
stole
stolen
store
sue
suicidal
suicide
supplements
supply company
theft
thief
thieves
tit
toddler
toddlers
toxic
toxin
tragedy
treating dka
treating hypoglycemia
treatment for hypoglycemia
vagina
violence
whore
withdrawal
without prescription
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-imn')]
div[contains(@class, 'pane-pub-home-imn')]
div[contains(@class, 'pane-pub-topic-imn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
New test for Lp(a) allows more accurate LDL-cholesterol results
A new study has drawn attention to inaccurate measurement of LDL-cholesterol levels in some patients with current assays, which could lead to incorrect therapeutic approaches.
The patient groups most affected are those with high levels of the lipoprotein Lp(a), in whom LDL-cholesterol levels are being overestimated in current laboratory tests, the authors say.
“Current laboratory assays all have the limitation that they cannot measure or report LDL cholesterol accurately. They are actually measuring the combination of LDL and Lp(a),” senior study author Sotirios Tsimikas, MD, University of California, San Diego, explained to this news organization.

“While this may not matter much in individuals with normal Lp(a) levels, in those with elevated Lp(a), the Lp(a) cholesterol may constitute a substantial proportion of the reported LDL cholesterol, and the actual LDL-cholesterol levels could be much lower that the value the lab is telling us,” he said.
Dr. Tsimikas gave the example of a patient with an LDL-cholesterol lab measurement of 75 mg/dL. “If that patient has an Lp(a) level of zero, then they do actually have an LDL level of 75. But as the Lp(a) increases, then the proportion of the result accounted for by LDL cholesterol decreases. So, if a patient with a measured LDL cholesterol of 75 has an Lp(a)-cholesterol level of 20, then their actual LDL level is 55.”
Dr. Tsimikas said it is important to know levels of both lipoproteins individually, so the correct therapeutic approach is used in situations where the Lp(a) cholesterol might be elevated.
“By understanding the actual values of LDL cholesterol and Lp(a) cholesterol, this will allow us to personalize the use of cholesterol-lowering medications and decide where to focus treatment. In the patient with a high level of Lp(a), their residual risk could be coming from Lp(a) cholesterol and less so from LDL cholesterol,” he added. “As we develop drugs to lower Lp(a), this patient might be better off on one of these rather than increasing efforts to lower LDL cholesterol, which might already be at goal.”
The study was published in the March 22 issue of the Journal of the American College of Cardiology.
Dr. Tsimikas noted that Lp(a) is now accepted as a genetic, independent, causal risk factor for cardiovascular disease, but current LDL-lowering drugs do not have much effect on Lp(a).
“Lp(a) can be lowered a little with niacin and PCSK9 inhibitors, but both have a quite a weak effect, and statins increase Lp(a). However, there are now multiple RNA-based therapeutics specifically targeting Lp(a) in clinical development,” he said.
At present, Lp(a) cholesterol has to be mathematically estimated, most commonly with the Dahlén formula, because of the lack of a validated, quantitative method to measure Lp(a) cholesterol, Dr. Tsimikas says.
For the current study, the researchers used a novel, quantitative, sensitive method to directly measure Lp(a) cholesterol, then applied this method to data from a recent study with the one of the new Lp(a)-lowering drugs in development – pelacarsen – which was conducted in patients with elevated Lp(a) levels.
Results showed that direct Lp(a)-cholesterol assessment, and subtracting this value from the laboratory LDL-cholesterol value, provides a more accurate reflection of the baseline and change in LDL cholesterol, the authors report. In the current study, corrected LDL cholesterol was 13 to 16 mg/dL lower than laboratory-reported LDL cholesterol.
Using the corrected LDL-cholesterol results, the study showed that pelacarsen significantly decreases Lp(a) cholesterol, with neutral to modest effects on LDL.
The study also suggests that the current method of calculating Lp(a) cholesterol, and then deriving a corrected LDL cholesterol – the Dahlén formula – is not accurate.
“The Dahlén formula relies on the assumption that Lp(a) cholesterol is universally a fixed 30% of Lp(a) mass, but this usually isn’t the case. The Dahlén formula needs to be discontinued. It can be highly inaccurate,” Dr. Tsimikas said.
Important implications
In an accompanying editorial, Guillaume Paré, MD, Michael Chong, PhD student, and Pedrum Mohammadi-Shemirani, BSc, all of McMaster University, Hamilton, Ont., say the current findings have three important clinical implications.
“First, they provide further proof that in individuals with elevated Lp(a), the contribution of Lp(a)-cholesterol to LDL-cholesterol is non-negligible using standard assays, with 13-16 mg/dL lower LDL-cholesterol post-correction.”
Secondly, the editorialists point out that these new findings confirm that the effect of Lp(a) inhibitors is likely to be mostly confined to Lp(a), “as would be expected.”
Finally, “and perhaps more importantly, the authors highlight the need to improve clinical reporting of lipid fractions to properly treat LDL-cholesterol and Lp(a) in high-risk patients,” they note.
“The report paves the way for future studies investigating the clinical utility of these additional measurements to initiate and monitor lipid-lowering therapy,” they conclude.
The clinical trial was funded by Ionis Pharmaceuticals, and the direct Lp(a)-cholesterol measurements were funded by Novartis through a research grant to the University of California, San Diego. Dr. Tsimikas is an employee of Ionis Pharmaceuticals and of the University of California, San Diego, and he is a cofounder of Covicept Therapeutics. He is also a coinventor and receives royalties from patents owned by UCSD on oxidation-specific antibodies and on biomarkers related to oxidized lipoproteins, as well as a cofounder and has equity interest in Oxitope and Kleanthi Diagnostics.
A version of this article first appeared on Medscape.com.
A new study has drawn attention to inaccurate measurement of LDL-cholesterol levels in some patients with current assays, which could lead to incorrect therapeutic approaches.
The patient groups most affected are those with high levels of the lipoprotein Lp(a), in whom LDL-cholesterol levels are being overestimated in current laboratory tests, the authors say.
“Current laboratory assays all have the limitation that they cannot measure or report LDL cholesterol accurately. They are actually measuring the combination of LDL and Lp(a),” senior study author Sotirios Tsimikas, MD, University of California, San Diego, explained to this news organization.
“While this may not matter much in individuals with normal Lp(a) levels, in those with elevated Lp(a), the Lp(a) cholesterol may constitute a substantial proportion of the reported LDL cholesterol, and the actual LDL-cholesterol levels could be much lower that the value the lab is telling us,” he said.
Dr. Tsimikas gave the example of a patient with an LDL-cholesterol lab measurement of 75 mg/dL. “If that patient has an Lp(a) level of zero, then they do actually have an LDL level of 75. But as the Lp(a) increases, then the proportion of the result accounted for by LDL cholesterol decreases. So, if a patient with a measured LDL cholesterol of 75 has an Lp(a)-cholesterol level of 20, then their actual LDL level is 55.”
Dr. Tsimikas said it is important to know levels of both lipoproteins individually, so the correct therapeutic approach is used in situations where the Lp(a) cholesterol might be elevated.
“By understanding the actual values of LDL cholesterol and Lp(a) cholesterol, this will allow us to personalize the use of cholesterol-lowering medications and decide where to focus treatment. In the patient with a high level of Lp(a), their residual risk could be coming from Lp(a) cholesterol and less so from LDL cholesterol,” he added. “As we develop drugs to lower Lp(a), this patient might be better off on one of these rather than increasing efforts to lower LDL cholesterol, which might already be at goal.”
The study was published in the March 22 issue of the Journal of the American College of Cardiology.
Dr. Tsimikas noted that Lp(a) is now accepted as a genetic, independent, causal risk factor for cardiovascular disease, but current LDL-lowering drugs do not have much effect on Lp(a).
“Lp(a) can be lowered a little with niacin and PCSK9 inhibitors, but both have a quite a weak effect, and statins increase Lp(a). However, there are now multiple RNA-based therapeutics specifically targeting Lp(a) in clinical development,” he said.
At present, Lp(a) cholesterol has to be mathematically estimated, most commonly with the Dahlén formula, because of the lack of a validated, quantitative method to measure Lp(a) cholesterol, Dr. Tsimikas says.
For the current study, the researchers used a novel, quantitative, sensitive method to directly measure Lp(a) cholesterol, then applied this method to data from a recent study with the one of the new Lp(a)-lowering drugs in development – pelacarsen – which was conducted in patients with elevated Lp(a) levels.
Results showed that direct Lp(a)-cholesterol assessment, and subtracting this value from the laboratory LDL-cholesterol value, provides a more accurate reflection of the baseline and change in LDL cholesterol, the authors report. In the current study, corrected LDL cholesterol was 13 to 16 mg/dL lower than laboratory-reported LDL cholesterol.
Using the corrected LDL-cholesterol results, the study showed that pelacarsen significantly decreases Lp(a) cholesterol, with neutral to modest effects on LDL.
The study also suggests that the current method of calculating Lp(a) cholesterol, and then deriving a corrected LDL cholesterol – the Dahlén formula – is not accurate.
“The Dahlén formula relies on the assumption that Lp(a) cholesterol is universally a fixed 30% of Lp(a) mass, but this usually isn’t the case. The Dahlén formula needs to be discontinued. It can be highly inaccurate,” Dr. Tsimikas said.
Important implications
In an accompanying editorial, Guillaume Paré, MD, Michael Chong, PhD student, and Pedrum Mohammadi-Shemirani, BSc, all of McMaster University, Hamilton, Ont., say the current findings have three important clinical implications.
“First, they provide further proof that in individuals with elevated Lp(a), the contribution of Lp(a)-cholesterol to LDL-cholesterol is non-negligible using standard assays, with 13-16 mg/dL lower LDL-cholesterol post-correction.”
Secondly, the editorialists point out that these new findings confirm that the effect of Lp(a) inhibitors is likely to be mostly confined to Lp(a), “as would be expected.”
Finally, “and perhaps more importantly, the authors highlight the need to improve clinical reporting of lipid fractions to properly treat LDL-cholesterol and Lp(a) in high-risk patients,” they note.
“The report paves the way for future studies investigating the clinical utility of these additional measurements to initiate and monitor lipid-lowering therapy,” they conclude.
The clinical trial was funded by Ionis Pharmaceuticals, and the direct Lp(a)-cholesterol measurements were funded by Novartis through a research grant to the University of California, San Diego. Dr. Tsimikas is an employee of Ionis Pharmaceuticals and of the University of California, San Diego, and he is a cofounder of Covicept Therapeutics. He is also a coinventor and receives royalties from patents owned by UCSD on oxidation-specific antibodies and on biomarkers related to oxidized lipoproteins, as well as a cofounder and has equity interest in Oxitope and Kleanthi Diagnostics.
A version of this article first appeared on Medscape.com.
A new study has drawn attention to inaccurate measurement of LDL-cholesterol levels in some patients with current assays, which could lead to incorrect therapeutic approaches.
The patient groups most affected are those with high levels of the lipoprotein Lp(a), in whom LDL-cholesterol levels are being overestimated in current laboratory tests, the authors say.
“Current laboratory assays all have the limitation that they cannot measure or report LDL cholesterol accurately. They are actually measuring the combination of LDL and Lp(a),” senior study author Sotirios Tsimikas, MD, University of California, San Diego, explained to this news organization.
“While this may not matter much in individuals with normal Lp(a) levels, in those with elevated Lp(a), the Lp(a) cholesterol may constitute a substantial proportion of the reported LDL cholesterol, and the actual LDL-cholesterol levels could be much lower that the value the lab is telling us,” he said.
Dr. Tsimikas gave the example of a patient with an LDL-cholesterol lab measurement of 75 mg/dL. “If that patient has an Lp(a) level of zero, then they do actually have an LDL level of 75. But as the Lp(a) increases, then the proportion of the result accounted for by LDL cholesterol decreases. So, if a patient with a measured LDL cholesterol of 75 has an Lp(a)-cholesterol level of 20, then their actual LDL level is 55.”
Dr. Tsimikas said it is important to know levels of both lipoproteins individually, so the correct therapeutic approach is used in situations where the Lp(a) cholesterol might be elevated.
“By understanding the actual values of LDL cholesterol and Lp(a) cholesterol, this will allow us to personalize the use of cholesterol-lowering medications and decide where to focus treatment. In the patient with a high level of Lp(a), their residual risk could be coming from Lp(a) cholesterol and less so from LDL cholesterol,” he added. “As we develop drugs to lower Lp(a), this patient might be better off on one of these rather than increasing efforts to lower LDL cholesterol, which might already be at goal.”
The study was published in the March 22 issue of the Journal of the American College of Cardiology.
Dr. Tsimikas noted that Lp(a) is now accepted as a genetic, independent, causal risk factor for cardiovascular disease, but current LDL-lowering drugs do not have much effect on Lp(a).
“Lp(a) can be lowered a little with niacin and PCSK9 inhibitors, but both have a quite a weak effect, and statins increase Lp(a). However, there are now multiple RNA-based therapeutics specifically targeting Lp(a) in clinical development,” he said.
At present, Lp(a) cholesterol has to be mathematically estimated, most commonly with the Dahlén formula, because of the lack of a validated, quantitative method to measure Lp(a) cholesterol, Dr. Tsimikas says.
For the current study, the researchers used a novel, quantitative, sensitive method to directly measure Lp(a) cholesterol, then applied this method to data from a recent study with the one of the new Lp(a)-lowering drugs in development – pelacarsen – which was conducted in patients with elevated Lp(a) levels.
Results showed that direct Lp(a)-cholesterol assessment, and subtracting this value from the laboratory LDL-cholesterol value, provides a more accurate reflection of the baseline and change in LDL cholesterol, the authors report. In the current study, corrected LDL cholesterol was 13 to 16 mg/dL lower than laboratory-reported LDL cholesterol.
Using the corrected LDL-cholesterol results, the study showed that pelacarsen significantly decreases Lp(a) cholesterol, with neutral to modest effects on LDL.
The study also suggests that the current method of calculating Lp(a) cholesterol, and then deriving a corrected LDL cholesterol – the Dahlén formula – is not accurate.
“The Dahlén formula relies on the assumption that Lp(a) cholesterol is universally a fixed 30% of Lp(a) mass, but this usually isn’t the case. The Dahlén formula needs to be discontinued. It can be highly inaccurate,” Dr. Tsimikas said.
Important implications
In an accompanying editorial, Guillaume Paré, MD, Michael Chong, PhD student, and Pedrum Mohammadi-Shemirani, BSc, all of McMaster University, Hamilton, Ont., say the current findings have three important clinical implications.
“First, they provide further proof that in individuals with elevated Lp(a), the contribution of Lp(a)-cholesterol to LDL-cholesterol is non-negligible using standard assays, with 13-16 mg/dL lower LDL-cholesterol post-correction.”
Secondly, the editorialists point out that these new findings confirm that the effect of Lp(a) inhibitors is likely to be mostly confined to Lp(a), “as would be expected.”
Finally, “and perhaps more importantly, the authors highlight the need to improve clinical reporting of lipid fractions to properly treat LDL-cholesterol and Lp(a) in high-risk patients,” they note.
“The report paves the way for future studies investigating the clinical utility of these additional measurements to initiate and monitor lipid-lowering therapy,” they conclude.
The clinical trial was funded by Ionis Pharmaceuticals, and the direct Lp(a)-cholesterol measurements were funded by Novartis through a research grant to the University of California, San Diego. Dr. Tsimikas is an employee of Ionis Pharmaceuticals and of the University of California, San Diego, and he is a cofounder of Covicept Therapeutics. He is also a coinventor and receives royalties from patents owned by UCSD on oxidation-specific antibodies and on biomarkers related to oxidized lipoproteins, as well as a cofounder and has equity interest in Oxitope and Kleanthi Diagnostics.
A version of this article first appeared on Medscape.com.
Walking 10,000 steps a day: Desirable goal or urban myth?
Some myths never die. The idea of taking 10,000 steps a day is one of them. What started as a catchy marketing slogan has become a mantra for anyone promoting physical activity.
It all began in 1965 when the Japanese company Yamasa Tokei began selling a new step-counter which they called manpo-kei (ten-thousand steps meter). They coupled the product launch with an ad campaign – “Let’s walk 10,000 steps a day!” – in a bid to encourage physical activity. The threshold was always somewhat arbitrary, but the idea of 10,000 steps cemented itself in the public consciousness from that point forward.

To be fair, there is nothing wrong with taking 10,000 steps a day, and it does roughly correlate with the generally recommended amount of physical activity. Most people will take somewhere between 5,000 and 7,500 steps a day even if they lead largely sedentary lives. If you add 30 minutes of walking to your daily routine, that will account for an extra 3,000-4,000 steps and bring you close to that 10,000-step threshold. As such, setting a 10,000-step target is a potentially useful shorthand for people aspiring to achieve ideal levels of physical activity.
But walking fewer steps still has a benefit. A study in JAMA Network Open followed a cohort of 2,110 adults from the CARDIA study and found, rather unsurprisingly, that those with more steps per day had lower rates of all-cause mortality. But interestingly, those who averaged 7,000-10,000 steps per day did just as well as those who walked more than 10,000 steps, suggesting that the lower threshold was probably the inflection point.
Other research has shown that improving your step count is probably more important than achieving any specific threshold. In one Canadian study, patients with diabetes were randomized to usual care or to an exercise prescription from their physicians. The intervention group improved their daily step count from around 5,000 steps per day to about 6,200 steps per day. While the increase was less than the researchers had hoped for, it still resulted in improvements in blood sugar control. In another study, a 24-week walking program reduced blood pressure by 11 points in postmenopausal women, even though their increased daily step counts fell shy of the 10,000 goal at about 9,000 steps. Similarly, a small Japanese study found that enrolling postmenopausal women in a weekly exercise program helped improve their lipid profile even though they only increased their daily step count from 6,800 to 8,500 steps per day. And an analysis of U.S. NHANES data showed a mortality benefit when individuals taking more than 8,000 steps were compared with those taking fewer than 4,000 steps per day. The benefits largely plateaued beyond 9,000-10,000 steps.
The reality is that walking 10,000 steps a day is a laudable goal and is almost certainly beneficial. But even lower levels of physical activity have benefits. The trick is not so much to aim for some theoretical ideal but to improve upon your current baseline. Encouraging patients to get into the habit of taking a daily walk (be it in the morning, during lunchtime, or in the evening) is going to pay dividends regardless of their daily step count. The point is that when it comes to physical activity, the greatest benefit seems to be when we go from doing nothing to doing something.
Dr. Labos is a cardiologist at Queen Elizabeth Health Complex, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Some myths never die. The idea of taking 10,000 steps a day is one of them. What started as a catchy marketing slogan has become a mantra for anyone promoting physical activity.
It all began in 1965 when the Japanese company Yamasa Tokei began selling a new step-counter which they called manpo-kei (ten-thousand steps meter). They coupled the product launch with an ad campaign – “Let’s walk 10,000 steps a day!” – in a bid to encourage physical activity. The threshold was always somewhat arbitrary, but the idea of 10,000 steps cemented itself in the public consciousness from that point forward.
To be fair, there is nothing wrong with taking 10,000 steps a day, and it does roughly correlate with the generally recommended amount of physical activity. Most people will take somewhere between 5,000 and 7,500 steps a day even if they lead largely sedentary lives. If you add 30 minutes of walking to your daily routine, that will account for an extra 3,000-4,000 steps and bring you close to that 10,000-step threshold. As such, setting a 10,000-step target is a potentially useful shorthand for people aspiring to achieve ideal levels of physical activity.
But walking fewer steps still has a benefit. A study in JAMA Network Open followed a cohort of 2,110 adults from the CARDIA study and found, rather unsurprisingly, that those with more steps per day had lower rates of all-cause mortality. But interestingly, those who averaged 7,000-10,000 steps per day did just as well as those who walked more than 10,000 steps, suggesting that the lower threshold was probably the inflection point.
Other research has shown that improving your step count is probably more important than achieving any specific threshold. In one Canadian study, patients with diabetes were randomized to usual care or to an exercise prescription from their physicians. The intervention group improved their daily step count from around 5,000 steps per day to about 6,200 steps per day. While the increase was less than the researchers had hoped for, it still resulted in improvements in blood sugar control. In another study, a 24-week walking program reduced blood pressure by 11 points in postmenopausal women, even though their increased daily step counts fell shy of the 10,000 goal at about 9,000 steps. Similarly, a small Japanese study found that enrolling postmenopausal women in a weekly exercise program helped improve their lipid profile even though they only increased their daily step count from 6,800 to 8,500 steps per day. And an analysis of U.S. NHANES data showed a mortality benefit when individuals taking more than 8,000 steps were compared with those taking fewer than 4,000 steps per day. The benefits largely plateaued beyond 9,000-10,000 steps.
The reality is that walking 10,000 steps a day is a laudable goal and is almost certainly beneficial. But even lower levels of physical activity have benefits. The trick is not so much to aim for some theoretical ideal but to improve upon your current baseline. Encouraging patients to get into the habit of taking a daily walk (be it in the morning, during lunchtime, or in the evening) is going to pay dividends regardless of their daily step count. The point is that when it comes to physical activity, the greatest benefit seems to be when we go from doing nothing to doing something.
Dr. Labos is a cardiologist at Queen Elizabeth Health Complex, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Some myths never die. The idea of taking 10,000 steps a day is one of them. What started as a catchy marketing slogan has become a mantra for anyone promoting physical activity.
It all began in 1965 when the Japanese company Yamasa Tokei began selling a new step-counter which they called manpo-kei (ten-thousand steps meter). They coupled the product launch with an ad campaign – “Let’s walk 10,000 steps a day!” – in a bid to encourage physical activity. The threshold was always somewhat arbitrary, but the idea of 10,000 steps cemented itself in the public consciousness from that point forward.
To be fair, there is nothing wrong with taking 10,000 steps a day, and it does roughly correlate with the generally recommended amount of physical activity. Most people will take somewhere between 5,000 and 7,500 steps a day even if they lead largely sedentary lives. If you add 30 minutes of walking to your daily routine, that will account for an extra 3,000-4,000 steps and bring you close to that 10,000-step threshold. As such, setting a 10,000-step target is a potentially useful shorthand for people aspiring to achieve ideal levels of physical activity.
But walking fewer steps still has a benefit. A study in JAMA Network Open followed a cohort of 2,110 adults from the CARDIA study and found, rather unsurprisingly, that those with more steps per day had lower rates of all-cause mortality. But interestingly, those who averaged 7,000-10,000 steps per day did just as well as those who walked more than 10,000 steps, suggesting that the lower threshold was probably the inflection point.
Other research has shown that improving your step count is probably more important than achieving any specific threshold. In one Canadian study, patients with diabetes were randomized to usual care or to an exercise prescription from their physicians. The intervention group improved their daily step count from around 5,000 steps per day to about 6,200 steps per day. While the increase was less than the researchers had hoped for, it still resulted in improvements in blood sugar control. In another study, a 24-week walking program reduced blood pressure by 11 points in postmenopausal women, even though their increased daily step counts fell shy of the 10,000 goal at about 9,000 steps. Similarly, a small Japanese study found that enrolling postmenopausal women in a weekly exercise program helped improve their lipid profile even though they only increased their daily step count from 6,800 to 8,500 steps per day. And an analysis of U.S. NHANES data showed a mortality benefit when individuals taking more than 8,000 steps were compared with those taking fewer than 4,000 steps per day. The benefits largely plateaued beyond 9,000-10,000 steps.
The reality is that walking 10,000 steps a day is a laudable goal and is almost certainly beneficial. But even lower levels of physical activity have benefits. The trick is not so much to aim for some theoretical ideal but to improve upon your current baseline. Encouraging patients to get into the habit of taking a daily walk (be it in the morning, during lunchtime, or in the evening) is going to pay dividends regardless of their daily step count. The point is that when it comes to physical activity, the greatest benefit seems to be when we go from doing nothing to doing something.
Dr. Labos is a cardiologist at Queen Elizabeth Health Complex, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Empagliflozin scores topline win in EMPA-KIDNEY trial
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.

In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Excess weight over lifetime hikes risk for colorectal cancer
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.

Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
FROM JAMA ONCOLOGY
COVID surge in Western Europe puts U.S. health experts on alert
, even as states and cities continue to lift restrictions amid low case numbers.
Infectious disease experts are watching BA.2, the Omicron subvariant that appears to be more transmissible than the original strain. BA.2 is fueling outbreaks across Europe and is growing in dominance across the United States.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” Eric Topol, MD, director of the Scripps Research Translational Institute, told The Washington Post.
He has been following the surge and has posted recent charts of the outbreak on Twitter. Hospitalizations appear to be increasing in some places as well, he noted, despite the higher vaccination rates of many Western European countries.
“There’s no question there’s a significant wave there,” Dr. Topol said.
Germany recorded more than 260,000 new cases on March 15, according to the data tracker from the New York Times, but coronavirus restrictions are still being lifted this week. The U.K. is reporting more than 75,000 daily cases, and the Netherlands is reporting more than 60,000 daily cases, which are considered major numbers, compared to their population sizes. Meanwhile, France, Italy, and Switzerland are also reporting large increases in infections.
During the past 2 years, widespread outbreaks in Europe have been followed by similar surges in the U.S. weeks later. Most experts interviewed by the Post predicted that it’s likely to happen again.
In the United States, the BA.2 subvariant accounted for 23% of new COVID-19 cases for the week ending March 12, according to the latest estimate from the Centers for Disease Control and Prevention, while the original Omicron strain made up about 66% of cases. The BA.2 percentage is up from 13.7% of new cases for the week ending March 5, 7.1% the previous week, and 4.1% the week before that. In parts of the Northeast and New England, BA.2 makes up more than 38% of new cases.
At the same time, the 7 -day average of COVID-19 cases continues to drop in the United States, with about 31,000 daily cases currently, the New York Times data tracker shows. About 25,000 COVID-19 patients are hospitalized across the country, which has fallen 44% in the past 2 weeks, and about 1,200 deaths are being reported daily.
Several variables could affect the course of a future surge, the Post reported. Vaccination rates, coronavirus safety protocols, and access to antiviral medications could dictate how another wave unfolds across the country.
About 82% of the eligible U.S. population has received at least one vaccine dose, and 69% is fully vaccinated, according to the latest CDC data. About half of those who are eligible for booster doses have received one. In Germany, nearly 76% of people are fully vaccinated, the newspaper reported, and in the United Kingdom, about 74% are fully vaccinated.
Health experts are also considering how natural immunity from a previous infection could affect a BA.2 surge. Millions of Americans were infected with the original Omicron strain, BA.1, which could provide protection. That said, researchers aren’t quite sure whether BA.1 infection protects against BA.2.
“It’s like a weather alert. Right now, the skies are sunny and bright, and we hope they stay that way,” Michael Osterholm, PhD, director of the University of Minnesota’s Center for Infectious Disease Research and Policy, told CNN.
“But we could have some bad weather by evening,” he said. “We just don’t know.”
A version of this article first appeared on WebMD.com.
, even as states and cities continue to lift restrictions amid low case numbers.
Infectious disease experts are watching BA.2, the Omicron subvariant that appears to be more transmissible than the original strain. BA.2 is fueling outbreaks across Europe and is growing in dominance across the United States.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” Eric Topol, MD, director of the Scripps Research Translational Institute, told The Washington Post.
He has been following the surge and has posted recent charts of the outbreak on Twitter. Hospitalizations appear to be increasing in some places as well, he noted, despite the higher vaccination rates of many Western European countries.
“There’s no question there’s a significant wave there,” Dr. Topol said.
Germany recorded more than 260,000 new cases on March 15, according to the data tracker from the New York Times, but coronavirus restrictions are still being lifted this week. The U.K. is reporting more than 75,000 daily cases, and the Netherlands is reporting more than 60,000 daily cases, which are considered major numbers, compared to their population sizes. Meanwhile, France, Italy, and Switzerland are also reporting large increases in infections.
During the past 2 years, widespread outbreaks in Europe have been followed by similar surges in the U.S. weeks later. Most experts interviewed by the Post predicted that it’s likely to happen again.
In the United States, the BA.2 subvariant accounted for 23% of new COVID-19 cases for the week ending March 12, according to the latest estimate from the Centers for Disease Control and Prevention, while the original Omicron strain made up about 66% of cases. The BA.2 percentage is up from 13.7% of new cases for the week ending March 5, 7.1% the previous week, and 4.1% the week before that. In parts of the Northeast and New England, BA.2 makes up more than 38% of new cases.
At the same time, the 7 -day average of COVID-19 cases continues to drop in the United States, with about 31,000 daily cases currently, the New York Times data tracker shows. About 25,000 COVID-19 patients are hospitalized across the country, which has fallen 44% in the past 2 weeks, and about 1,200 deaths are being reported daily.
Several variables could affect the course of a future surge, the Post reported. Vaccination rates, coronavirus safety protocols, and access to antiviral medications could dictate how another wave unfolds across the country.
About 82% of the eligible U.S. population has received at least one vaccine dose, and 69% is fully vaccinated, according to the latest CDC data. About half of those who are eligible for booster doses have received one. In Germany, nearly 76% of people are fully vaccinated, the newspaper reported, and in the United Kingdom, about 74% are fully vaccinated.
Health experts are also considering how natural immunity from a previous infection could affect a BA.2 surge. Millions of Americans were infected with the original Omicron strain, BA.1, which could provide protection. That said, researchers aren’t quite sure whether BA.1 infection protects against BA.2.
“It’s like a weather alert. Right now, the skies are sunny and bright, and we hope they stay that way,” Michael Osterholm, PhD, director of the University of Minnesota’s Center for Infectious Disease Research and Policy, told CNN.
“But we could have some bad weather by evening,” he said. “We just don’t know.”
A version of this article first appeared on WebMD.com.
, even as states and cities continue to lift restrictions amid low case numbers.
Infectious disease experts are watching BA.2, the Omicron subvariant that appears to be more transmissible than the original strain. BA.2 is fueling outbreaks across Europe and is growing in dominance across the United States.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” Eric Topol, MD, director of the Scripps Research Translational Institute, told The Washington Post.
He has been following the surge and has posted recent charts of the outbreak on Twitter. Hospitalizations appear to be increasing in some places as well, he noted, despite the higher vaccination rates of many Western European countries.
“There’s no question there’s a significant wave there,” Dr. Topol said.
Germany recorded more than 260,000 new cases on March 15, according to the data tracker from the New York Times, but coronavirus restrictions are still being lifted this week. The U.K. is reporting more than 75,000 daily cases, and the Netherlands is reporting more than 60,000 daily cases, which are considered major numbers, compared to their population sizes. Meanwhile, France, Italy, and Switzerland are also reporting large increases in infections.
During the past 2 years, widespread outbreaks in Europe have been followed by similar surges in the U.S. weeks later. Most experts interviewed by the Post predicted that it’s likely to happen again.
In the United States, the BA.2 subvariant accounted for 23% of new COVID-19 cases for the week ending March 12, according to the latest estimate from the Centers for Disease Control and Prevention, while the original Omicron strain made up about 66% of cases. The BA.2 percentage is up from 13.7% of new cases for the week ending March 5, 7.1% the previous week, and 4.1% the week before that. In parts of the Northeast and New England, BA.2 makes up more than 38% of new cases.
At the same time, the 7 -day average of COVID-19 cases continues to drop in the United States, with about 31,000 daily cases currently, the New York Times data tracker shows. About 25,000 COVID-19 patients are hospitalized across the country, which has fallen 44% in the past 2 weeks, and about 1,200 deaths are being reported daily.
Several variables could affect the course of a future surge, the Post reported. Vaccination rates, coronavirus safety protocols, and access to antiviral medications could dictate how another wave unfolds across the country.
About 82% of the eligible U.S. population has received at least one vaccine dose, and 69% is fully vaccinated, according to the latest CDC data. About half of those who are eligible for booster doses have received one. In Germany, nearly 76% of people are fully vaccinated, the newspaper reported, and in the United Kingdom, about 74% are fully vaccinated.
Health experts are also considering how natural immunity from a previous infection could affect a BA.2 surge. Millions of Americans were infected with the original Omicron strain, BA.1, which could provide protection. That said, researchers aren’t quite sure whether BA.1 infection protects against BA.2.
“It’s like a weather alert. Right now, the skies are sunny and bright, and we hope they stay that way,” Michael Osterholm, PhD, director of the University of Minnesota’s Center for Infectious Disease Research and Policy, told CNN.
“But we could have some bad weather by evening,” he said. “We just don’t know.”
A version of this article first appeared on WebMD.com.
Obesity linked to combined OSA syndrome and severe asthma
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
FROM RESPIRATORY MEDICINE AND RESEARCH
Doctors treat osteoporosis with hormone therapy against guidelines
This type of hormone therapy (HT) can be given as estrogen or a combination of hormones including estrogen. The physicians interviewed for this piece who prescribe HT for osteoporosis suggest the benefits outweigh the downsides to its use for some of their patients. But such doctors may be a minority group, suggests Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center, Portland.

According to Dr. McClung, HT is now rarely prescribed as treatment – as opposed to prevention – for osteoporosis in the absence of additional benefits such as reducing vasomotor symptoms.
Researchers’ findings on HT use in women with osteoporosis are complex. While HT is approved for menopausal prevention of osteoporosis, it is not indicated as a treatment for the disease by the Food and Drug Administration. See the prescribing information for Premarin tablets, which contain a mixture of estrogen hormones, for an example of the FDA’s indications and usage for the type of HT addressed in this article.
Women’s Health Initiative findings
The Women’s Health Initiative (WHI) hormone therapy trials showed that HT reduces the incidence of all osteoporosis-related fractures in postmenopausal women, even those at low risk of fracture, but osteoporosis-related fractures was not a study endpoint. These trials also revealed that HT was associated with increased risks of cardiovascular and cerebrovascular events, an increased risk of breast cancer, and other adverse health outcomes.
The release of the interim results of the WHI trials in 2002 led to a fair amount of fear and confusion about the use of HT after menopause. After the WHI findings were published, estrogen use dropped dramatically, but for everything, including for vasomotor symptoms and the prevention and treatment of osteoporosis.
Prior to the WHI study, it was very common for hormone therapy to be prescribed as women neared or entered menopause, said Risa Kagan MD, clinical professor of obstetrics, gynecology, and reproductive sciences, University of California, San Francisco.

“When a woman turned 50, that was one of the first things we did – was to put her on hormone therapy. All that changed with the WHI, but now we are coming full circle,” noted Dr. Kagan, who currently prescribes HT as first line treatment for osteoporosis to some women.
Hormone therapy’s complex history
HT’s ability to reduce bone loss in postmenopausal women is well-documented in many papers, including one published March 8, 2018, in Osteoporosis International, by Dr. Kagan and colleagues. This reduced bone loss has been shown to significantly reduce fractures in patients with low bone mass and osteoporosis.
While a growing number of therapies are now available to treat osteoporosis, HT was traditionally viewed as a standard method of preventing fractures in this population. It was also widely used to prevent other types of symptoms associated with the menopause, such as hot flashes, night sweats, and sleep disturbances, and multiple observational studies had demonstrated that its use appeared to reduce the incidence of cardiovascular disease (CVD) in symptomatic menopausal women who initiated HT in early menopause.
Even though the WHI studies were the largest randomized trials ever performed in postmenopausal women, they had notable limitations, according to Dr. Kagan.
“The women were older – the average age was 63 years,” she said. “And they only investigated one route and one dose of estrogen.”
Since then, many different formulations and routes of administration with more favorable safety profiles than what was used in the WHI have become available.
It’s both scientifically and clinically unsound to extrapolate the unfavorable risk-benefit profile of HT seen in the WHI trials to all women regardless of age, HT dosage or formulation, or the length of time they’re on it, she added.
Today’s use of HT in women with osteoporosis
Re-analyses and follow-up studies from the WHI trials, along with data from other studies, have suggested that the benefit-risk profiles of HT are affected by a variety of factors. These include the timing of use in relation to menopause and chronological age and the type of hormone regimen.
“Clinically, many advocate for [hormone therapy] use, especially in the newer younger postmenopausal women to prevent bone loss, but also in younger women who are diagnosed with osteoporosis and then as they get older transition to more bone specific agents,” noted Dr. Kagan.
“Some advocate preserving bone mass and preventing osteoporosis and even treating the younger newly postmenopausal women who have no contraindications with hormone therapy initially, and then gradually transitioning them to a bone specific agent as they get older and at risk for fracture.
“If a woman is already fractured and/or has very low bone density with no other obvious secondary metabolic reason, we also often advocate anabolic agents for 1-2 years then consider estrogen for maintenance – again, if [there is] no contraindication to using HT,” she added.
Thus, an individualized approach is recommended to determine a woman’s risk-benefit ratio of HT use based on the absolute risk of adverse effects, Dr. Kagan noted.
“Transdermal and low/ultra-low doses of HT, have a favorable risk profile, and are effective in preserving bone mineral density and bone quality in many women,” she said.
According to Dr. McClung, HT “is most often used for treatment in women in whom hormone therapy was begun for hot flashes and then, when osteoporosis was found later, was simply continued.
“Society guidelines are cautious about recommending hormone therapy for osteoporosis treatment since estrogen is not approved for treatment, despite the clear fracture protection benefit observed in the WHI study,” he said. “Since [women in the WHI trials] were not recruited as having osteoporosis, those results do not meet the FDA requirement for treatment approval, namely the reduction in fracture risk in patients with osteoporosis. However, knowing what we know about the salutary skeletal effects of estrogen, many of us do use them in our patients with osteoporosis – although not prescribed for that purpose.”
Additional scenarios when doctors may advise HT
“I often recommend – and I think colleagues do as well – that women with recent menopause and menopausal symptoms who also have low bone mineral density or even scores showing osteoporosis see their gynecologist to discuss HT for a few years, perhaps until age 60 if no contraindications, and if it is well tolerated,” said Ethel S. Siris, MD, professor of medicine at Columbia University Medical Center in New York.
“Once they stop it we can then give one of our other bone drugs, but it delays the need to start them since on adequate estrogen the bone density should remain stable while they take it,” added Dr. Siris, an endocrinologist and internist, and director of the Toni Stabile Osteoporosis Center in New York. “They may need a bisphosphonate or another bone drug to further protect them from bone loss and future fracture [after stopping HT].”
Victor L. Roberts, MD, founder of Endocrine Associates of Florida, Lake Mary, pointed out that women now have many options for treatment of osteoporosis.

“If a woman is in early menopause and is having other symptoms, then estrogen is warranted,” he said. “If she has osteoporosis, then it’s a bonus.”
“We have better agents that are bone specific,” for a patient who presents with osteoporosis and no other symptoms, he said.
“If a woman is intolerant of alendronate or other similar drugs, or chooses not to have an injectable, then estrogen or a SERM [selective estrogen receptor modulator] would be an option.”
Dr. Roberts added that HT would be more of a niche drug.
“It has a role and documented benefit and works,” he said. “There is good scientific data for the use of estrogen.”
Dr. Kagan is a consultant for Pfizer, Therapeutics MD, Amgen, on the Medical and Scientific Advisory Board of American Bone Health. The other experts interviewed for this piece reported no conflicts.
This type of hormone therapy (HT) can be given as estrogen or a combination of hormones including estrogen. The physicians interviewed for this piece who prescribe HT for osteoporosis suggest the benefits outweigh the downsides to its use for some of their patients. But such doctors may be a minority group, suggests Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center, Portland.
According to Dr. McClung, HT is now rarely prescribed as treatment – as opposed to prevention – for osteoporosis in the absence of additional benefits such as reducing vasomotor symptoms.
Researchers’ findings on HT use in women with osteoporosis are complex. While HT is approved for menopausal prevention of osteoporosis, it is not indicated as a treatment for the disease by the Food and Drug Administration. See the prescribing information for Premarin tablets, which contain a mixture of estrogen hormones, for an example of the FDA’s indications and usage for the type of HT addressed in this article.
Women’s Health Initiative findings
The Women’s Health Initiative (WHI) hormone therapy trials showed that HT reduces the incidence of all osteoporosis-related fractures in postmenopausal women, even those at low risk of fracture, but osteoporosis-related fractures was not a study endpoint. These trials also revealed that HT was associated with increased risks of cardiovascular and cerebrovascular events, an increased risk of breast cancer, and other adverse health outcomes.
The release of the interim results of the WHI trials in 2002 led to a fair amount of fear and confusion about the use of HT after menopause. After the WHI findings were published, estrogen use dropped dramatically, but for everything, including for vasomotor symptoms and the prevention and treatment of osteoporosis.
Prior to the WHI study, it was very common for hormone therapy to be prescribed as women neared or entered menopause, said Risa Kagan MD, clinical professor of obstetrics, gynecology, and reproductive sciences, University of California, San Francisco.
“When a woman turned 50, that was one of the first things we did – was to put her on hormone therapy. All that changed with the WHI, but now we are coming full circle,” noted Dr. Kagan, who currently prescribes HT as first line treatment for osteoporosis to some women.
Hormone therapy’s complex history
HT’s ability to reduce bone loss in postmenopausal women is well-documented in many papers, including one published March 8, 2018, in Osteoporosis International, by Dr. Kagan and colleagues. This reduced bone loss has been shown to significantly reduce fractures in patients with low bone mass and osteoporosis.
While a growing number of therapies are now available to treat osteoporosis, HT was traditionally viewed as a standard method of preventing fractures in this population. It was also widely used to prevent other types of symptoms associated with the menopause, such as hot flashes, night sweats, and sleep disturbances, and multiple observational studies had demonstrated that its use appeared to reduce the incidence of cardiovascular disease (CVD) in symptomatic menopausal women who initiated HT in early menopause.
Even though the WHI studies were the largest randomized trials ever performed in postmenopausal women, they had notable limitations, according to Dr. Kagan.
“The women were older – the average age was 63 years,” she said. “And they only investigated one route and one dose of estrogen.”
Since then, many different formulations and routes of administration with more favorable safety profiles than what was used in the WHI have become available.
It’s both scientifically and clinically unsound to extrapolate the unfavorable risk-benefit profile of HT seen in the WHI trials to all women regardless of age, HT dosage or formulation, or the length of time they’re on it, she added.
Today’s use of HT in women with osteoporosis
Re-analyses and follow-up studies from the WHI trials, along with data from other studies, have suggested that the benefit-risk profiles of HT are affected by a variety of factors. These include the timing of use in relation to menopause and chronological age and the type of hormone regimen.
“Clinically, many advocate for [hormone therapy] use, especially in the newer younger postmenopausal women to prevent bone loss, but also in younger women who are diagnosed with osteoporosis and then as they get older transition to more bone specific agents,” noted Dr. Kagan.
“Some advocate preserving bone mass and preventing osteoporosis and even treating the younger newly postmenopausal women who have no contraindications with hormone therapy initially, and then gradually transitioning them to a bone specific agent as they get older and at risk for fracture.
“If a woman is already fractured and/or has very low bone density with no other obvious secondary metabolic reason, we also often advocate anabolic agents for 1-2 years then consider estrogen for maintenance – again, if [there is] no contraindication to using HT,” she added.
Thus, an individualized approach is recommended to determine a woman’s risk-benefit ratio of HT use based on the absolute risk of adverse effects, Dr. Kagan noted.
“Transdermal and low/ultra-low doses of HT, have a favorable risk profile, and are effective in preserving bone mineral density and bone quality in many women,” she said.
According to Dr. McClung, HT “is most often used for treatment in women in whom hormone therapy was begun for hot flashes and then, when osteoporosis was found later, was simply continued.
“Society guidelines are cautious about recommending hormone therapy for osteoporosis treatment since estrogen is not approved for treatment, despite the clear fracture protection benefit observed in the WHI study,” he said. “Since [women in the WHI trials] were not recruited as having osteoporosis, those results do not meet the FDA requirement for treatment approval, namely the reduction in fracture risk in patients with osteoporosis. However, knowing what we know about the salutary skeletal effects of estrogen, many of us do use them in our patients with osteoporosis – although not prescribed for that purpose.”
Additional scenarios when doctors may advise HT
“I often recommend – and I think colleagues do as well – that women with recent menopause and menopausal symptoms who also have low bone mineral density or even scores showing osteoporosis see their gynecologist to discuss HT for a few years, perhaps until age 60 if no contraindications, and if it is well tolerated,” said Ethel S. Siris, MD, professor of medicine at Columbia University Medical Center in New York.
“Once they stop it we can then give one of our other bone drugs, but it delays the need to start them since on adequate estrogen the bone density should remain stable while they take it,” added Dr. Siris, an endocrinologist and internist, and director of the Toni Stabile Osteoporosis Center in New York. “They may need a bisphosphonate or another bone drug to further protect them from bone loss and future fracture [after stopping HT].”
Victor L. Roberts, MD, founder of Endocrine Associates of Florida, Lake Mary, pointed out that women now have many options for treatment of osteoporosis.
“If a woman is in early menopause and is having other symptoms, then estrogen is warranted,” he said. “If she has osteoporosis, then it’s a bonus.”
“We have better agents that are bone specific,” for a patient who presents with osteoporosis and no other symptoms, he said.
“If a woman is intolerant of alendronate or other similar drugs, or chooses not to have an injectable, then estrogen or a SERM [selective estrogen receptor modulator] would be an option.”
Dr. Roberts added that HT would be more of a niche drug.
“It has a role and documented benefit and works,” he said. “There is good scientific data for the use of estrogen.”
Dr. Kagan is a consultant for Pfizer, Therapeutics MD, Amgen, on the Medical and Scientific Advisory Board of American Bone Health. The other experts interviewed for this piece reported no conflicts.
This type of hormone therapy (HT) can be given as estrogen or a combination of hormones including estrogen. The physicians interviewed for this piece who prescribe HT for osteoporosis suggest the benefits outweigh the downsides to its use for some of their patients. But such doctors may be a minority group, suggests Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center, Portland.
According to Dr. McClung, HT is now rarely prescribed as treatment – as opposed to prevention – for osteoporosis in the absence of additional benefits such as reducing vasomotor symptoms.
Researchers’ findings on HT use in women with osteoporosis are complex. While HT is approved for menopausal prevention of osteoporosis, it is not indicated as a treatment for the disease by the Food and Drug Administration. See the prescribing information for Premarin tablets, which contain a mixture of estrogen hormones, for an example of the FDA’s indications and usage for the type of HT addressed in this article.
Women’s Health Initiative findings
The Women’s Health Initiative (WHI) hormone therapy trials showed that HT reduces the incidence of all osteoporosis-related fractures in postmenopausal women, even those at low risk of fracture, but osteoporosis-related fractures was not a study endpoint. These trials also revealed that HT was associated with increased risks of cardiovascular and cerebrovascular events, an increased risk of breast cancer, and other adverse health outcomes.
The release of the interim results of the WHI trials in 2002 led to a fair amount of fear and confusion about the use of HT after menopause. After the WHI findings were published, estrogen use dropped dramatically, but for everything, including for vasomotor symptoms and the prevention and treatment of osteoporosis.
Prior to the WHI study, it was very common for hormone therapy to be prescribed as women neared or entered menopause, said Risa Kagan MD, clinical professor of obstetrics, gynecology, and reproductive sciences, University of California, San Francisco.
“When a woman turned 50, that was one of the first things we did – was to put her on hormone therapy. All that changed with the WHI, but now we are coming full circle,” noted Dr. Kagan, who currently prescribes HT as first line treatment for osteoporosis to some women.
Hormone therapy’s complex history
HT’s ability to reduce bone loss in postmenopausal women is well-documented in many papers, including one published March 8, 2018, in Osteoporosis International, by Dr. Kagan and colleagues. This reduced bone loss has been shown to significantly reduce fractures in patients with low bone mass and osteoporosis.
While a growing number of therapies are now available to treat osteoporosis, HT was traditionally viewed as a standard method of preventing fractures in this population. It was also widely used to prevent other types of symptoms associated with the menopause, such as hot flashes, night sweats, and sleep disturbances, and multiple observational studies had demonstrated that its use appeared to reduce the incidence of cardiovascular disease (CVD) in symptomatic menopausal women who initiated HT in early menopause.
Even though the WHI studies were the largest randomized trials ever performed in postmenopausal women, they had notable limitations, according to Dr. Kagan.
“The women were older – the average age was 63 years,” she said. “And they only investigated one route and one dose of estrogen.”
Since then, many different formulations and routes of administration with more favorable safety profiles than what was used in the WHI have become available.
It’s both scientifically and clinically unsound to extrapolate the unfavorable risk-benefit profile of HT seen in the WHI trials to all women regardless of age, HT dosage or formulation, or the length of time they’re on it, she added.
Today’s use of HT in women with osteoporosis
Re-analyses and follow-up studies from the WHI trials, along with data from other studies, have suggested that the benefit-risk profiles of HT are affected by a variety of factors. These include the timing of use in relation to menopause and chronological age and the type of hormone regimen.
“Clinically, many advocate for [hormone therapy] use, especially in the newer younger postmenopausal women to prevent bone loss, but also in younger women who are diagnosed with osteoporosis and then as they get older transition to more bone specific agents,” noted Dr. Kagan.
“Some advocate preserving bone mass and preventing osteoporosis and even treating the younger newly postmenopausal women who have no contraindications with hormone therapy initially, and then gradually transitioning them to a bone specific agent as they get older and at risk for fracture.
“If a woman is already fractured and/or has very low bone density with no other obvious secondary metabolic reason, we also often advocate anabolic agents for 1-2 years then consider estrogen for maintenance – again, if [there is] no contraindication to using HT,” she added.
Thus, an individualized approach is recommended to determine a woman’s risk-benefit ratio of HT use based on the absolute risk of adverse effects, Dr. Kagan noted.
“Transdermal and low/ultra-low doses of HT, have a favorable risk profile, and are effective in preserving bone mineral density and bone quality in many women,” she said.
According to Dr. McClung, HT “is most often used for treatment in women in whom hormone therapy was begun for hot flashes and then, when osteoporosis was found later, was simply continued.
“Society guidelines are cautious about recommending hormone therapy for osteoporosis treatment since estrogen is not approved for treatment, despite the clear fracture protection benefit observed in the WHI study,” he said. “Since [women in the WHI trials] were not recruited as having osteoporosis, those results do not meet the FDA requirement for treatment approval, namely the reduction in fracture risk in patients with osteoporosis. However, knowing what we know about the salutary skeletal effects of estrogen, many of us do use them in our patients with osteoporosis – although not prescribed for that purpose.”
Additional scenarios when doctors may advise HT
“I often recommend – and I think colleagues do as well – that women with recent menopause and menopausal symptoms who also have low bone mineral density or even scores showing osteoporosis see their gynecologist to discuss HT for a few years, perhaps until age 60 if no contraindications, and if it is well tolerated,” said Ethel S. Siris, MD, professor of medicine at Columbia University Medical Center in New York.
“Once they stop it we can then give one of our other bone drugs, but it delays the need to start them since on adequate estrogen the bone density should remain stable while they take it,” added Dr. Siris, an endocrinologist and internist, and director of the Toni Stabile Osteoporosis Center in New York. “They may need a bisphosphonate or another bone drug to further protect them from bone loss and future fracture [after stopping HT].”
Victor L. Roberts, MD, founder of Endocrine Associates of Florida, Lake Mary, pointed out that women now have many options for treatment of osteoporosis.
“If a woman is in early menopause and is having other symptoms, then estrogen is warranted,” he said. “If she has osteoporosis, then it’s a bonus.”
“We have better agents that are bone specific,” for a patient who presents with osteoporosis and no other symptoms, he said.
“If a woman is intolerant of alendronate or other similar drugs, or chooses not to have an injectable, then estrogen or a SERM [selective estrogen receptor modulator] would be an option.”
Dr. Roberts added that HT would be more of a niche drug.
“It has a role and documented benefit and works,” he said. “There is good scientific data for the use of estrogen.”
Dr. Kagan is a consultant for Pfizer, Therapeutics MD, Amgen, on the Medical and Scientific Advisory Board of American Bone Health. The other experts interviewed for this piece reported no conflicts.
New ACC guidance on cardiovascular consequences of COVID-19
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
Doctors have failed them, say those with transgender regret
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
Don’t drink calories: Artificial sweeteners beat sugar in new analysis
This transcript of Impact Factor with F. Perry Wilson has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
When I counsel patients who are trying to lose weight, there is something I always discuss: “Don’t drink calories.” The idea is that it is so easy to consume sweetened beverages (and alcoholic ones, for that matter) and we don’t really get a sense of how many calories we’re taking in.
Some patients balk at the idea, saying they can’t stand the taste of water or just can’t bring themselves to drink it. While, as a nephrologist, this pains me deeply to hear, I often suggest going for low- or zero-calorie flavored drinks instead of the sugary stuff.
And yet ... I need to admit that recently I’ve been more nervous about that advice. A very nice study in Nature, for example, found that artificial sweeteners induce glucose intolerance and weight gain – in mice.
Several observational studies have suggested that the use of nonnutritive sweeteners – sucralose, aspartame, and so on – are associated with higher body weight and type 2 diabetes. Of course,
Randomized trials, as ever, are the key to deeper understanding, but most trials in this space are relatively small. That makes a good case for this study, appearing in JAMA Network Open, which combines data from 17 randomized trials to determine what effects substituting sugary drinks with low- and zero-calorie drinks truly has.
So, what’s the bottom line? Should I ditch the Splenda in my morning coffee and drop in some sugar cubes?
It turns out that the effects of drinking low- or zero-calorie drinks instead of sugary ones is modest, but overall beneficial, depending on the outcome you’re trying to achieve.
Randomized trials show that switching to low-cal drinks reduces body weight by about a kilogram, and BMI by 0.3 points. It also reduces body fat by about half a percent.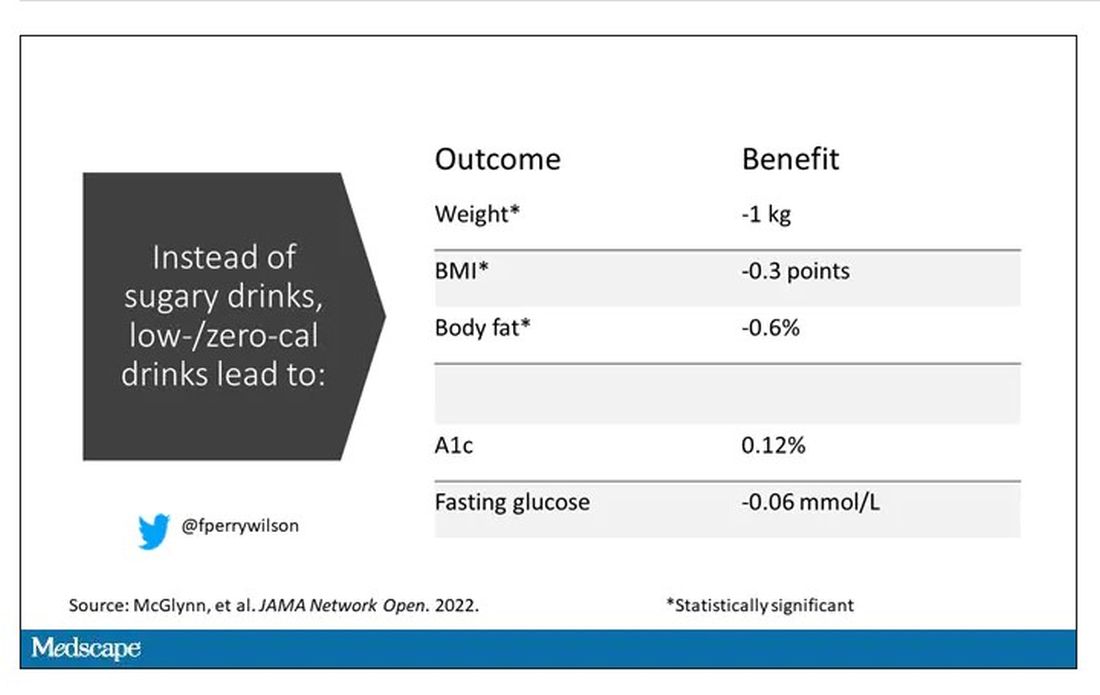
Effects on glucose homeostasis – hemoglobin A1c level and fasting glucose – were not that impressive, though.
The authors also compared sugar-sweetened beverages with plain old water. I expected this analysis to show more dramatic benefits. After all, we’re all just ugly, giant bags of mostly water. Interestingly, the effects of switching to water were not as dramatic and largely nonsignificant with respect to most outcomes evaluated.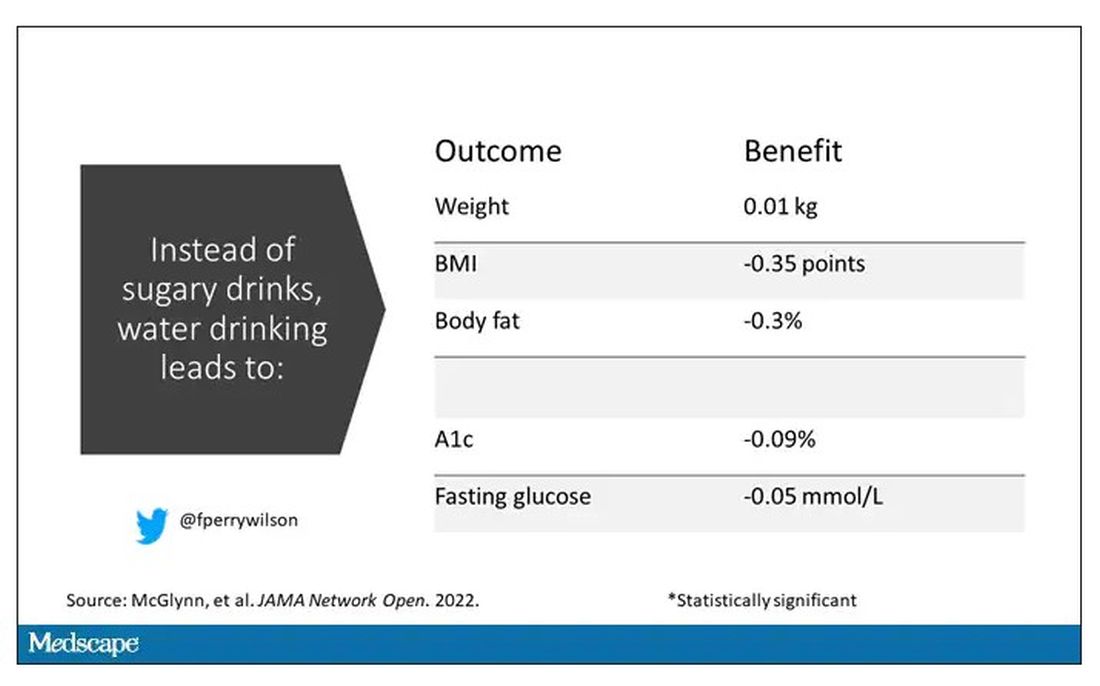
So, what do we make of this? If someone is a habitual drinker of sugar-sweetened beverages, is it preferable to switch to a zero-calorie flavored drink, compared with plain water?
One possibility is that in the trials where people are randomized to switch to water, they aren’t as adherent. Just because we ask someone to drink water doesn’t mean they do it, and so there may be a tendency to “cheat” with sugar-sweetened beverages. However, if told that low- or zero-calorie flavored drinks are okay, maybe it’s easier to stick to the plan? This is essentially the argument you get from people who say that vaping is a good way to quit smoking. It may or may not be true.
It could also be that we just don’t have enough rigorous data to make a firm conclusion. Of the 17 trials examined, only three of them used water substitution as an intervention.
All in all, these data provide some reassurance that the zero-calorie sweeteners aren’t secretly exacerbating the obesity epidemic. I’d certainly rather my patients drink Diet Coke than regular Coke. That said, these studies are necessarily short term; the longer-term effects of sugar substitutes, while perhaps not as bad as the long-term effects of sugar, must necessarily be worse than the long-term effects of drinking water. Maybe this is the nephrologist in me talking again, but I doubt that there could possibly be a fluid better for the human body than good old H2O. Except coffee, of course.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript of Impact Factor with F. Perry Wilson has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
When I counsel patients who are trying to lose weight, there is something I always discuss: “Don’t drink calories.” The idea is that it is so easy to consume sweetened beverages (and alcoholic ones, for that matter) and we don’t really get a sense of how many calories we’re taking in.
Some patients balk at the idea, saying they can’t stand the taste of water or just can’t bring themselves to drink it. While, as a nephrologist, this pains me deeply to hear, I often suggest going for low- or zero-calorie flavored drinks instead of the sugary stuff.
And yet ... I need to admit that recently I’ve been more nervous about that advice. A very nice study in Nature, for example, found that artificial sweeteners induce glucose intolerance and weight gain – in mice.
Several observational studies have suggested that the use of nonnutritive sweeteners – sucralose, aspartame, and so on – are associated with higher body weight and type 2 diabetes. Of course,
Randomized trials, as ever, are the key to deeper understanding, but most trials in this space are relatively small. That makes a good case for this study, appearing in JAMA Network Open, which combines data from 17 randomized trials to determine what effects substituting sugary drinks with low- and zero-calorie drinks truly has.
So, what’s the bottom line? Should I ditch the Splenda in my morning coffee and drop in some sugar cubes?
It turns out that the effects of drinking low- or zero-calorie drinks instead of sugary ones is modest, but overall beneficial, depending on the outcome you’re trying to achieve.
Randomized trials show that switching to low-cal drinks reduces body weight by about a kilogram, and BMI by 0.3 points. It also reduces body fat by about half a percent.
Effects on glucose homeostasis – hemoglobin A1c level and fasting glucose – were not that impressive, though.
The authors also compared sugar-sweetened beverages with plain old water. I expected this analysis to show more dramatic benefits. After all, we’re all just ugly, giant bags of mostly water. Interestingly, the effects of switching to water were not as dramatic and largely nonsignificant with respect to most outcomes evaluated.
So, what do we make of this? If someone is a habitual drinker of sugar-sweetened beverages, is it preferable to switch to a zero-calorie flavored drink, compared with plain water?
One possibility is that in the trials where people are randomized to switch to water, they aren’t as adherent. Just because we ask someone to drink water doesn’t mean they do it, and so there may be a tendency to “cheat” with sugar-sweetened beverages. However, if told that low- or zero-calorie flavored drinks are okay, maybe it’s easier to stick to the plan? This is essentially the argument you get from people who say that vaping is a good way to quit smoking. It may or may not be true.
It could also be that we just don’t have enough rigorous data to make a firm conclusion. Of the 17 trials examined, only three of them used water substitution as an intervention.
All in all, these data provide some reassurance that the zero-calorie sweeteners aren’t secretly exacerbating the obesity epidemic. I’d certainly rather my patients drink Diet Coke than regular Coke. That said, these studies are necessarily short term; the longer-term effects of sugar substitutes, while perhaps not as bad as the long-term effects of sugar, must necessarily be worse than the long-term effects of drinking water. Maybe this is the nephrologist in me talking again, but I doubt that there could possibly be a fluid better for the human body than good old H2O. Except coffee, of course.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript of Impact Factor with F. Perry Wilson has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
When I counsel patients who are trying to lose weight, there is something I always discuss: “Don’t drink calories.” The idea is that it is so easy to consume sweetened beverages (and alcoholic ones, for that matter) and we don’t really get a sense of how many calories we’re taking in.
Some patients balk at the idea, saying they can’t stand the taste of water or just can’t bring themselves to drink it. While, as a nephrologist, this pains me deeply to hear, I often suggest going for low- or zero-calorie flavored drinks instead of the sugary stuff.
And yet ... I need to admit that recently I’ve been more nervous about that advice. A very nice study in Nature, for example, found that artificial sweeteners induce glucose intolerance and weight gain – in mice.
Several observational studies have suggested that the use of nonnutritive sweeteners – sucralose, aspartame, and so on – are associated with higher body weight and type 2 diabetes. Of course,
Randomized trials, as ever, are the key to deeper understanding, but most trials in this space are relatively small. That makes a good case for this study, appearing in JAMA Network Open, which combines data from 17 randomized trials to determine what effects substituting sugary drinks with low- and zero-calorie drinks truly has.
So, what’s the bottom line? Should I ditch the Splenda in my morning coffee and drop in some sugar cubes?
It turns out that the effects of drinking low- or zero-calorie drinks instead of sugary ones is modest, but overall beneficial, depending on the outcome you’re trying to achieve.
Randomized trials show that switching to low-cal drinks reduces body weight by about a kilogram, and BMI by 0.3 points. It also reduces body fat by about half a percent.
Effects on glucose homeostasis – hemoglobin A1c level and fasting glucose – were not that impressive, though.
The authors also compared sugar-sweetened beverages with plain old water. I expected this analysis to show more dramatic benefits. After all, we’re all just ugly, giant bags of mostly water. Interestingly, the effects of switching to water were not as dramatic and largely nonsignificant with respect to most outcomes evaluated.
So, what do we make of this? If someone is a habitual drinker of sugar-sweetened beverages, is it preferable to switch to a zero-calorie flavored drink, compared with plain water?
One possibility is that in the trials where people are randomized to switch to water, they aren’t as adherent. Just because we ask someone to drink water doesn’t mean they do it, and so there may be a tendency to “cheat” with sugar-sweetened beverages. However, if told that low- or zero-calorie flavored drinks are okay, maybe it’s easier to stick to the plan? This is essentially the argument you get from people who say that vaping is a good way to quit smoking. It may or may not be true.
It could also be that we just don’t have enough rigorous data to make a firm conclusion. Of the 17 trials examined, only three of them used water substitution as an intervention.
All in all, these data provide some reassurance that the zero-calorie sweeteners aren’t secretly exacerbating the obesity epidemic. I’d certainly rather my patients drink Diet Coke than regular Coke. That said, these studies are necessarily short term; the longer-term effects of sugar substitutes, while perhaps not as bad as the long-term effects of sugar, must necessarily be worse than the long-term effects of drinking water. Maybe this is the nephrologist in me talking again, but I doubt that there could possibly be a fluid better for the human body than good old H2O. Except coffee, of course.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.