User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Lomitapide shows promise in pediatric homozygous FH
MANNHEIM, Germany – Lomitapide, which reduces lipoprotein production in the liver, could help manage pediatric homozygous familial hypercholesterolemia (HoFH), suggest results of a trial that showed large reductions in circulating lipids.
The research was presented May 23 at the 91st European Atherosclerosis Society Congress.
Lomitapide inhibits microsomal triglyceride transfer protein, which plays a key role in apolipoprotein B-containing lipoprotein assembly and secretion in the liver and intestines. Crucially, the drug acts independently of the LDL cholesterol receptor.
It was approved in December 2012 by the U.S. Food and Drug Administration for use in adults with HoFH, sold under the name Juxtapid, and by the European Medicines Agency, where the brand name is Lojuxta.
The current trial involved more than 40 children and teenagers with HoFH aged 5-17 years; they were treated with the drug for 24 weeks, resulting in reductions of low density lipoprotein cholesterol of almost 54%, with nearly 42% reaching target levels.
The drug was also associated with marked reductions in other key lipids of at least 50%. However, 67% of patients also experienced gastrointestinal adverse events, and around 25% saw their levels of liver enzymes increase.
Early diagnosis ‘imperative’
The findings show that the “early diagnosis and treatment of HoFH is imperative,” said study presenter Luis Masana, MD, PhD, director of the Vascular Medicine and Metabolism Unit at Sant Joan de Reus University Hospital, Tarragona, Spain.
“I think that, with these results, we are bringing a new hope for this group of patients,” he continued. “I also think we will increase the quality of life, not just of the patients but also all the families involved in [managing] this problem.”
Session co-chair Andreas Zirlik, MD, PhD, head of the department of cardiology and chairman of the University Heart Center Graz, LKH-University Hospital, and Medical University of Graz (Austria), was more circumspect in his appraisal of the results.
He told this news organization that it is “always very difficult to establish therapy in pediatrics,” and believes that the drug “will give us an additional option” in managing HoFH.
However, Dr. Zirlik warned that he is a “little bit concerned” about lomitapide’s adverse event profile, and “would need to see a little bit deeper into the safety data.”
Highlighting the elevations in liver enzymes of around 25%, he asked: “What does it mean?” And how will it “play out in the long run?”
Beyond lomitapide, Dr. Zirlik pointed out that there are other drugs that have shown potential in managing HoFH and could potentially be used in the pediatric population, such as angiopoietin-like 3 protein (ANGPTL3) inhibitors and small interfering RNA (siRNA) compounds that target upstream production. “So, let’s see how they pan out,” he said.
Life-limiting condition
HoFH is an “ultra-rare, life-limiting condition,” with an estimated prevalence of approximately 3 per 1 million people, and a life expectancy in untreated patients of just 18 years, Dr. Masana said during his presentation.
Case series of lomitapide use in pediatric HoFH patients have shown encouraging results that are consistent with those seen in adults, he noted, with many able to achieve their LDL cholesterol target and stop or reduce apheresis.
To investigate further, a phase 3, single arm, open-label study was conducted. Following screening, 46 children and teenagers with HoFH underwent a 6- to 12-week run-in period, during which they were put on a low-fat diet with nutritional supplements.
“As you can imagine,” Dr. Masana said, “we are reducing the capacity for fat absorption with lomitapide, so the supplements and low-fat diet are necessary.”
Of these, 43 participants then entered a 24-week treatment period in which they were started on one of three doses, before undergoing dose escalation to the maximally tolerated dose. This was followed by an 80-week open-label safety phase, in which they continued on the maximally tolerated dose, then a follow-up period.
For the current presentation, Dr. Masana focused on the efficacy phase, showing that the mean age of participants was 10.7 years and that 55.8% were female. The HoFH diagnosis was confirmed genetically in 88.4% of cases.
Results showed that lomitapide was associated with a significant reduction in LDL cholesterol levels, from 435.8 mg/dL at baseline to 176.5 mg/dL at Week 24, which corresponded to a 53.5% overall reduction (P < .0001).
This meant that 41.9% of patients achieved their EAS LDL cholesterol target of less than 135 mg/dL at some point during the 24-week treatment period.
Stratifying by age, the reduction between baseline and week 24 was 538.5 mg/dL to 207.2 mg/dL, or 56.5%, in the 20 children aged 5-10 years, and 346.5 mg/dL to 149.9 mg/L, or 50.9%, in the 23 patients aged 11-17 years.
Dr. Masana explained that the results were “a little bit better in the younger group because they were receiving less treatment at this stage of the disease” than the older group.
He showed that lomitapide was associated with significant reductions in other lipid markers, including a 53.9% reduction in non–HDL cholesterol (P < .0001), a 50.1% drop in total cholesterol (P < .0001), and a 50.2% fall in very-low-density lipoprotein cholesterol (P < .0001).
Results showed 93% of patients experienced treatment-related adverse events, with 11.6% having serious events and 4.7% having events that led to study discontinuation. There was one (2.3%) major adverse cardiac event but no deaths.
He said that, despite these figures, the adverse events were “mostly mild or moderate.”
The majority (67%) of patients nevertheless had gastrointestinal adverse events, which were, “in general, associated with a lack of adherence to the low-fat diet.”
Aspartate aminotransferase levels were elevated in 23% of patients, while 28% had elevations in alanine aminotransferase, which were described by Dr. Masana as “moderate.”
The study was sponsored by Amryt Pharma. Dr. Masana declares relationships with Amarin, Amryt, Daiichi-Sankyo, Novartis, Sanofi, Servier, Servier, and Viatrix.
A version of this article first appeared on Medscape.com.
MANNHEIM, Germany – Lomitapide, which reduces lipoprotein production in the liver, could help manage pediatric homozygous familial hypercholesterolemia (HoFH), suggest results of a trial that showed large reductions in circulating lipids.
The research was presented May 23 at the 91st European Atherosclerosis Society Congress.
Lomitapide inhibits microsomal triglyceride transfer protein, which plays a key role in apolipoprotein B-containing lipoprotein assembly and secretion in the liver and intestines. Crucially, the drug acts independently of the LDL cholesterol receptor.
It was approved in December 2012 by the U.S. Food and Drug Administration for use in adults with HoFH, sold under the name Juxtapid, and by the European Medicines Agency, where the brand name is Lojuxta.
The current trial involved more than 40 children and teenagers with HoFH aged 5-17 years; they were treated with the drug for 24 weeks, resulting in reductions of low density lipoprotein cholesterol of almost 54%, with nearly 42% reaching target levels.
The drug was also associated with marked reductions in other key lipids of at least 50%. However, 67% of patients also experienced gastrointestinal adverse events, and around 25% saw their levels of liver enzymes increase.
Early diagnosis ‘imperative’
The findings show that the “early diagnosis and treatment of HoFH is imperative,” said study presenter Luis Masana, MD, PhD, director of the Vascular Medicine and Metabolism Unit at Sant Joan de Reus University Hospital, Tarragona, Spain.
“I think that, with these results, we are bringing a new hope for this group of patients,” he continued. “I also think we will increase the quality of life, not just of the patients but also all the families involved in [managing] this problem.”
Session co-chair Andreas Zirlik, MD, PhD, head of the department of cardiology and chairman of the University Heart Center Graz, LKH-University Hospital, and Medical University of Graz (Austria), was more circumspect in his appraisal of the results.
He told this news organization that it is “always very difficult to establish therapy in pediatrics,” and believes that the drug “will give us an additional option” in managing HoFH.
However, Dr. Zirlik warned that he is a “little bit concerned” about lomitapide’s adverse event profile, and “would need to see a little bit deeper into the safety data.”
Highlighting the elevations in liver enzymes of around 25%, he asked: “What does it mean?” And how will it “play out in the long run?”
Beyond lomitapide, Dr. Zirlik pointed out that there are other drugs that have shown potential in managing HoFH and could potentially be used in the pediatric population, such as angiopoietin-like 3 protein (ANGPTL3) inhibitors and small interfering RNA (siRNA) compounds that target upstream production. “So, let’s see how they pan out,” he said.
Life-limiting condition
HoFH is an “ultra-rare, life-limiting condition,” with an estimated prevalence of approximately 3 per 1 million people, and a life expectancy in untreated patients of just 18 years, Dr. Masana said during his presentation.
Case series of lomitapide use in pediatric HoFH patients have shown encouraging results that are consistent with those seen in adults, he noted, with many able to achieve their LDL cholesterol target and stop or reduce apheresis.
To investigate further, a phase 3, single arm, open-label study was conducted. Following screening, 46 children and teenagers with HoFH underwent a 6- to 12-week run-in period, during which they were put on a low-fat diet with nutritional supplements.
“As you can imagine,” Dr. Masana said, “we are reducing the capacity for fat absorption with lomitapide, so the supplements and low-fat diet are necessary.”
Of these, 43 participants then entered a 24-week treatment period in which they were started on one of three doses, before undergoing dose escalation to the maximally tolerated dose. This was followed by an 80-week open-label safety phase, in which they continued on the maximally tolerated dose, then a follow-up period.
For the current presentation, Dr. Masana focused on the efficacy phase, showing that the mean age of participants was 10.7 years and that 55.8% were female. The HoFH diagnosis was confirmed genetically in 88.4% of cases.
Results showed that lomitapide was associated with a significant reduction in LDL cholesterol levels, from 435.8 mg/dL at baseline to 176.5 mg/dL at Week 24, which corresponded to a 53.5% overall reduction (P < .0001).
This meant that 41.9% of patients achieved their EAS LDL cholesterol target of less than 135 mg/dL at some point during the 24-week treatment period.
Stratifying by age, the reduction between baseline and week 24 was 538.5 mg/dL to 207.2 mg/dL, or 56.5%, in the 20 children aged 5-10 years, and 346.5 mg/dL to 149.9 mg/L, or 50.9%, in the 23 patients aged 11-17 years.
Dr. Masana explained that the results were “a little bit better in the younger group because they were receiving less treatment at this stage of the disease” than the older group.
He showed that lomitapide was associated with significant reductions in other lipid markers, including a 53.9% reduction in non–HDL cholesterol (P < .0001), a 50.1% drop in total cholesterol (P < .0001), and a 50.2% fall in very-low-density lipoprotein cholesterol (P < .0001).
Results showed 93% of patients experienced treatment-related adverse events, with 11.6% having serious events and 4.7% having events that led to study discontinuation. There was one (2.3%) major adverse cardiac event but no deaths.
He said that, despite these figures, the adverse events were “mostly mild or moderate.”
The majority (67%) of patients nevertheless had gastrointestinal adverse events, which were, “in general, associated with a lack of adherence to the low-fat diet.”
Aspartate aminotransferase levels were elevated in 23% of patients, while 28% had elevations in alanine aminotransferase, which were described by Dr. Masana as “moderate.”
The study was sponsored by Amryt Pharma. Dr. Masana declares relationships with Amarin, Amryt, Daiichi-Sankyo, Novartis, Sanofi, Servier, Servier, and Viatrix.
A version of this article first appeared on Medscape.com.
MANNHEIM, Germany – Lomitapide, which reduces lipoprotein production in the liver, could help manage pediatric homozygous familial hypercholesterolemia (HoFH), suggest results of a trial that showed large reductions in circulating lipids.
The research was presented May 23 at the 91st European Atherosclerosis Society Congress.
Lomitapide inhibits microsomal triglyceride transfer protein, which plays a key role in apolipoprotein B-containing lipoprotein assembly and secretion in the liver and intestines. Crucially, the drug acts independently of the LDL cholesterol receptor.
It was approved in December 2012 by the U.S. Food and Drug Administration for use in adults with HoFH, sold under the name Juxtapid, and by the European Medicines Agency, where the brand name is Lojuxta.
The current trial involved more than 40 children and teenagers with HoFH aged 5-17 years; they were treated with the drug for 24 weeks, resulting in reductions of low density lipoprotein cholesterol of almost 54%, with nearly 42% reaching target levels.
The drug was also associated with marked reductions in other key lipids of at least 50%. However, 67% of patients also experienced gastrointestinal adverse events, and around 25% saw their levels of liver enzymes increase.
Early diagnosis ‘imperative’
The findings show that the “early diagnosis and treatment of HoFH is imperative,” said study presenter Luis Masana, MD, PhD, director of the Vascular Medicine and Metabolism Unit at Sant Joan de Reus University Hospital, Tarragona, Spain.
“I think that, with these results, we are bringing a new hope for this group of patients,” he continued. “I also think we will increase the quality of life, not just of the patients but also all the families involved in [managing] this problem.”
Session co-chair Andreas Zirlik, MD, PhD, head of the department of cardiology and chairman of the University Heart Center Graz, LKH-University Hospital, and Medical University of Graz (Austria), was more circumspect in his appraisal of the results.
He told this news organization that it is “always very difficult to establish therapy in pediatrics,” and believes that the drug “will give us an additional option” in managing HoFH.
However, Dr. Zirlik warned that he is a “little bit concerned” about lomitapide’s adverse event profile, and “would need to see a little bit deeper into the safety data.”
Highlighting the elevations in liver enzymes of around 25%, he asked: “What does it mean?” And how will it “play out in the long run?”
Beyond lomitapide, Dr. Zirlik pointed out that there are other drugs that have shown potential in managing HoFH and could potentially be used in the pediatric population, such as angiopoietin-like 3 protein (ANGPTL3) inhibitors and small interfering RNA (siRNA) compounds that target upstream production. “So, let’s see how they pan out,” he said.
Life-limiting condition
HoFH is an “ultra-rare, life-limiting condition,” with an estimated prevalence of approximately 3 per 1 million people, and a life expectancy in untreated patients of just 18 years, Dr. Masana said during his presentation.
Case series of lomitapide use in pediatric HoFH patients have shown encouraging results that are consistent with those seen in adults, he noted, with many able to achieve their LDL cholesterol target and stop or reduce apheresis.
To investigate further, a phase 3, single arm, open-label study was conducted. Following screening, 46 children and teenagers with HoFH underwent a 6- to 12-week run-in period, during which they were put on a low-fat diet with nutritional supplements.
“As you can imagine,” Dr. Masana said, “we are reducing the capacity for fat absorption with lomitapide, so the supplements and low-fat diet are necessary.”
Of these, 43 participants then entered a 24-week treatment period in which they were started on one of three doses, before undergoing dose escalation to the maximally tolerated dose. This was followed by an 80-week open-label safety phase, in which they continued on the maximally tolerated dose, then a follow-up period.
For the current presentation, Dr. Masana focused on the efficacy phase, showing that the mean age of participants was 10.7 years and that 55.8% were female. The HoFH diagnosis was confirmed genetically in 88.4% of cases.
Results showed that lomitapide was associated with a significant reduction in LDL cholesterol levels, from 435.8 mg/dL at baseline to 176.5 mg/dL at Week 24, which corresponded to a 53.5% overall reduction (P < .0001).
This meant that 41.9% of patients achieved their EAS LDL cholesterol target of less than 135 mg/dL at some point during the 24-week treatment period.
Stratifying by age, the reduction between baseline and week 24 was 538.5 mg/dL to 207.2 mg/dL, or 56.5%, in the 20 children aged 5-10 years, and 346.5 mg/dL to 149.9 mg/L, or 50.9%, in the 23 patients aged 11-17 years.
Dr. Masana explained that the results were “a little bit better in the younger group because they were receiving less treatment at this stage of the disease” than the older group.
He showed that lomitapide was associated with significant reductions in other lipid markers, including a 53.9% reduction in non–HDL cholesterol (P < .0001), a 50.1% drop in total cholesterol (P < .0001), and a 50.2% fall in very-low-density lipoprotein cholesterol (P < .0001).
Results showed 93% of patients experienced treatment-related adverse events, with 11.6% having serious events and 4.7% having events that led to study discontinuation. There was one (2.3%) major adverse cardiac event but no deaths.
He said that, despite these figures, the adverse events were “mostly mild or moderate.”
The majority (67%) of patients nevertheless had gastrointestinal adverse events, which were, “in general, associated with a lack of adherence to the low-fat diet.”
Aspartate aminotransferase levels were elevated in 23% of patients, while 28% had elevations in alanine aminotransferase, which were described by Dr. Masana as “moderate.”
The study was sponsored by Amryt Pharma. Dr. Masana declares relationships with Amarin, Amryt, Daiichi-Sankyo, Novartis, Sanofi, Servier, Servier, and Viatrix.
A version of this article first appeared on Medscape.com.
Preventive antipyretics, antibiotics not needed in stroke
“The results of PRECIOUS do not support preventive use of antiemetic, antipyretic, or antibiotic drugs in older patients with acute stroke,” senior study author Bart van der Worp, MD, professor of acute neurology at University Medical Center, Utrecht, the Netherlands, concluded.
“This trial was all about prevention,” trial co-investigator, Philip Bath, MD, professor of stroke medicine at the University of Nottingham (England), said in an interview.
“It was trying to improve outcomes by preventing infection, fever, and aspiration pneumonia, but the message from these results is that while we should be on the lookout for these complications and treat them early when they occur, we don’t need to give these medications on a prophylactic basis.”
The PREvention of Complications to Improve OUtcome in elderly patients with acute Stroke (PRECIOUS) trial was presented at the annual European Stroke Organisation Conference, held in Munich.
Dr. Van der Worp explained that infections, fever, and aspiration pneumonia frequently occur following stroke, particularly in older patients, and these poststroke complications are associated with an increased risk of death and poor functional outcome.
“We assessed whether a pharmacological strategy to reduce the risk of infections and fever improves outcomes of elderly patients with moderately severe or severe stroke,” he said.
Previous studies looking at this approach have been performed in broad populations of stroke patients who had a relatively low risk of poststroke complications, thereby reducing the potential for benefit from these interventions.
The current PRECIOUS trial was therefore conducted in a more selective elderly population with more severe strokes, a group believed to be at higher risk of infection and fever.
The trial included patients aged 66 years or older with moderately severe to severe ischemic stroke (National Institutes of Health Stroke Scale score ≥ 6) or intracerebral hemorrhage.
They were randomized in a 3 x 2 factorial design to oral, rectal, or intravenous metoclopramide (10 mg three times a day); intravenous ceftriaxone (2,000 mg once daily); oral, rectal, or intravenous paracetamol (1,000 mg four times daily); or usual care.
Medications were started within 24 hours after symptom onset and continued for 4 days or until complete recovery or discharge from hospital, if earlier.
“We assessed these three simple, safe, and inexpensive therapies – paracetamol to prevent fever; the antiemetic, metoclopramide, to prevent aspiration; and ceftriaxone, which is the preferred antibiotic for post-stroke pneumonia in the Netherlands,” Dr. van der Worp said.
The primary outcome was modified Rankin Scale (mRS) score at 90 days.
The trial was aiming to enroll 3,800 patients from 67 European sites but was stopped after 1,493 patients had been included because of lack of funding. After excluding patients who withdrew consent or were lost to follow-up, 1,471 patients were included in the intention-to-treat analysis.
Results showed no effect on the primary outcome of any of the prophylactic treatments.
“None of the medications had any effect on the functional outcome at 90 days. This was a surprise to me,” Dr. Van der Worp commented. “I had expected that at least one of the medications would have been of benefit.”
A secondary outcome was the diagnosis of pneumonia, which again was not reduced by any of the medications.
“Remarkably, neither ceftriaxone nor metoclopramide had any effect on the risk of developing pneumonia. It was all quite disappointing,” van der Worp said.
There was, however, a reduction in the incidence of urinary tract infections in the ceftriaxone group.
Trying to explain why there was a reduction in urinary tract infections but not pneumonia with the antibiotic, Dr. Van der Worp pointed out that poststroke pneumonia is to a large extent caused by a mechanical process (aspiration), and bacteria may only play a minor role in its development.
He said he was therefore surprised that metoclopramide, which should prevent the mechanical process of aspiration, did not reduce the development of pneumonia.
He suggested that some patients may have already experienced aspiration before the metoclopramide was started, noting that many patients with acute stroke already have signs of pneumonia on CT scan in the first few hours after symptom onset.
A previous smaller study (MAPS) had shown a lower rate of pneumonia in stroke patients given metoclopramide, but in this study the drug was given for 3 weeks.
Discussing the PRECIOUS trial at the ESOC meeting, Christine Roffe, MD, professor of stroke medicine at Keele (England) University, and senior investigator of the MAPS study, suggested that a longer period of metoclopramide treatment may be needed than the 4 days given in the PRECIOUS study, as the risk of pneumonia persists for longer than just a few days.
She noted that another trial (MAPS-2) is now underway in the United Kingdom to try and confirm the first MAPS result with longer duration metoclopramide.
Dr. Van der Worp responded: “Certainly, I think that the MAPS-2 study should be continued. It is investigating a much longer duration of treatment, which may be beneficial, especially in patients with more severe strokes.”
On the reason for the disappointing results with paracetamol, Dr. Van der Worp elaborated: “We found that only a very few of these older patients developed a fever – only about 5% in the control group. Paracetamol did reduce the risk of fever, but because the proportion of patients who developed fever was so small, this may have been why it didn’t translate into any effect on the functional outcome.”
Dr. Roffe concluded that PRECIOUS was an important study. “There is also a positive message here. We have all been worried about using too many antibiotics. We need to make sure we use these drugs responsibly. I think this trial has told us there is little point in using antibiotics in a preventative way in these patients.”
She added that although the trial was stopped prematurely, it had produced decisive results.
“Yes, I believe that even if the trial was much larger, we still would not have shown an effect,” Dr. Van der Worp agreed.
A version of this article first appeared on Medscape.com.
“The results of PRECIOUS do not support preventive use of antiemetic, antipyretic, or antibiotic drugs in older patients with acute stroke,” senior study author Bart van der Worp, MD, professor of acute neurology at University Medical Center, Utrecht, the Netherlands, concluded.
“This trial was all about prevention,” trial co-investigator, Philip Bath, MD, professor of stroke medicine at the University of Nottingham (England), said in an interview.
“It was trying to improve outcomes by preventing infection, fever, and aspiration pneumonia, but the message from these results is that while we should be on the lookout for these complications and treat them early when they occur, we don’t need to give these medications on a prophylactic basis.”
The PREvention of Complications to Improve OUtcome in elderly patients with acute Stroke (PRECIOUS) trial was presented at the annual European Stroke Organisation Conference, held in Munich.
Dr. Van der Worp explained that infections, fever, and aspiration pneumonia frequently occur following stroke, particularly in older patients, and these poststroke complications are associated with an increased risk of death and poor functional outcome.
“We assessed whether a pharmacological strategy to reduce the risk of infections and fever improves outcomes of elderly patients with moderately severe or severe stroke,” he said.
Previous studies looking at this approach have been performed in broad populations of stroke patients who had a relatively low risk of poststroke complications, thereby reducing the potential for benefit from these interventions.
The current PRECIOUS trial was therefore conducted in a more selective elderly population with more severe strokes, a group believed to be at higher risk of infection and fever.
The trial included patients aged 66 years or older with moderately severe to severe ischemic stroke (National Institutes of Health Stroke Scale score ≥ 6) or intracerebral hemorrhage.
They were randomized in a 3 x 2 factorial design to oral, rectal, or intravenous metoclopramide (10 mg three times a day); intravenous ceftriaxone (2,000 mg once daily); oral, rectal, or intravenous paracetamol (1,000 mg four times daily); or usual care.
Medications were started within 24 hours after symptom onset and continued for 4 days or until complete recovery or discharge from hospital, if earlier.
“We assessed these three simple, safe, and inexpensive therapies – paracetamol to prevent fever; the antiemetic, metoclopramide, to prevent aspiration; and ceftriaxone, which is the preferred antibiotic for post-stroke pneumonia in the Netherlands,” Dr. van der Worp said.
The primary outcome was modified Rankin Scale (mRS) score at 90 days.
The trial was aiming to enroll 3,800 patients from 67 European sites but was stopped after 1,493 patients had been included because of lack of funding. After excluding patients who withdrew consent or were lost to follow-up, 1,471 patients were included in the intention-to-treat analysis.
Results showed no effect on the primary outcome of any of the prophylactic treatments.
“None of the medications had any effect on the functional outcome at 90 days. This was a surprise to me,” Dr. Van der Worp commented. “I had expected that at least one of the medications would have been of benefit.”
A secondary outcome was the diagnosis of pneumonia, which again was not reduced by any of the medications.
“Remarkably, neither ceftriaxone nor metoclopramide had any effect on the risk of developing pneumonia. It was all quite disappointing,” van der Worp said.
There was, however, a reduction in the incidence of urinary tract infections in the ceftriaxone group.
Trying to explain why there was a reduction in urinary tract infections but not pneumonia with the antibiotic, Dr. Van der Worp pointed out that poststroke pneumonia is to a large extent caused by a mechanical process (aspiration), and bacteria may only play a minor role in its development.
He said he was therefore surprised that metoclopramide, which should prevent the mechanical process of aspiration, did not reduce the development of pneumonia.
He suggested that some patients may have already experienced aspiration before the metoclopramide was started, noting that many patients with acute stroke already have signs of pneumonia on CT scan in the first few hours after symptom onset.
A previous smaller study (MAPS) had shown a lower rate of pneumonia in stroke patients given metoclopramide, but in this study the drug was given for 3 weeks.
Discussing the PRECIOUS trial at the ESOC meeting, Christine Roffe, MD, professor of stroke medicine at Keele (England) University, and senior investigator of the MAPS study, suggested that a longer period of metoclopramide treatment may be needed than the 4 days given in the PRECIOUS study, as the risk of pneumonia persists for longer than just a few days.
She noted that another trial (MAPS-2) is now underway in the United Kingdom to try and confirm the first MAPS result with longer duration metoclopramide.
Dr. Van der Worp responded: “Certainly, I think that the MAPS-2 study should be continued. It is investigating a much longer duration of treatment, which may be beneficial, especially in patients with more severe strokes.”
On the reason for the disappointing results with paracetamol, Dr. Van der Worp elaborated: “We found that only a very few of these older patients developed a fever – only about 5% in the control group. Paracetamol did reduce the risk of fever, but because the proportion of patients who developed fever was so small, this may have been why it didn’t translate into any effect on the functional outcome.”
Dr. Roffe concluded that PRECIOUS was an important study. “There is also a positive message here. We have all been worried about using too many antibiotics. We need to make sure we use these drugs responsibly. I think this trial has told us there is little point in using antibiotics in a preventative way in these patients.”
She added that although the trial was stopped prematurely, it had produced decisive results.
“Yes, I believe that even if the trial was much larger, we still would not have shown an effect,” Dr. Van der Worp agreed.
A version of this article first appeared on Medscape.com.
“The results of PRECIOUS do not support preventive use of antiemetic, antipyretic, or antibiotic drugs in older patients with acute stroke,” senior study author Bart van der Worp, MD, professor of acute neurology at University Medical Center, Utrecht, the Netherlands, concluded.
“This trial was all about prevention,” trial co-investigator, Philip Bath, MD, professor of stroke medicine at the University of Nottingham (England), said in an interview.
“It was trying to improve outcomes by preventing infection, fever, and aspiration pneumonia, but the message from these results is that while we should be on the lookout for these complications and treat them early when they occur, we don’t need to give these medications on a prophylactic basis.”
The PREvention of Complications to Improve OUtcome in elderly patients with acute Stroke (PRECIOUS) trial was presented at the annual European Stroke Organisation Conference, held in Munich.
Dr. Van der Worp explained that infections, fever, and aspiration pneumonia frequently occur following stroke, particularly in older patients, and these poststroke complications are associated with an increased risk of death and poor functional outcome.
“We assessed whether a pharmacological strategy to reduce the risk of infections and fever improves outcomes of elderly patients with moderately severe or severe stroke,” he said.
Previous studies looking at this approach have been performed in broad populations of stroke patients who had a relatively low risk of poststroke complications, thereby reducing the potential for benefit from these interventions.
The current PRECIOUS trial was therefore conducted in a more selective elderly population with more severe strokes, a group believed to be at higher risk of infection and fever.
The trial included patients aged 66 years or older with moderately severe to severe ischemic stroke (National Institutes of Health Stroke Scale score ≥ 6) or intracerebral hemorrhage.
They were randomized in a 3 x 2 factorial design to oral, rectal, or intravenous metoclopramide (10 mg three times a day); intravenous ceftriaxone (2,000 mg once daily); oral, rectal, or intravenous paracetamol (1,000 mg four times daily); or usual care.
Medications were started within 24 hours after symptom onset and continued for 4 days or until complete recovery or discharge from hospital, if earlier.
“We assessed these three simple, safe, and inexpensive therapies – paracetamol to prevent fever; the antiemetic, metoclopramide, to prevent aspiration; and ceftriaxone, which is the preferred antibiotic for post-stroke pneumonia in the Netherlands,” Dr. van der Worp said.
The primary outcome was modified Rankin Scale (mRS) score at 90 days.
The trial was aiming to enroll 3,800 patients from 67 European sites but was stopped after 1,493 patients had been included because of lack of funding. After excluding patients who withdrew consent or were lost to follow-up, 1,471 patients were included in the intention-to-treat analysis.
Results showed no effect on the primary outcome of any of the prophylactic treatments.
“None of the medications had any effect on the functional outcome at 90 days. This was a surprise to me,” Dr. Van der Worp commented. “I had expected that at least one of the medications would have been of benefit.”
A secondary outcome was the diagnosis of pneumonia, which again was not reduced by any of the medications.
“Remarkably, neither ceftriaxone nor metoclopramide had any effect on the risk of developing pneumonia. It was all quite disappointing,” van der Worp said.
There was, however, a reduction in the incidence of urinary tract infections in the ceftriaxone group.
Trying to explain why there was a reduction in urinary tract infections but not pneumonia with the antibiotic, Dr. Van der Worp pointed out that poststroke pneumonia is to a large extent caused by a mechanical process (aspiration), and bacteria may only play a minor role in its development.
He said he was therefore surprised that metoclopramide, which should prevent the mechanical process of aspiration, did not reduce the development of pneumonia.
He suggested that some patients may have already experienced aspiration before the metoclopramide was started, noting that many patients with acute stroke already have signs of pneumonia on CT scan in the first few hours after symptom onset.
A previous smaller study (MAPS) had shown a lower rate of pneumonia in stroke patients given metoclopramide, but in this study the drug was given for 3 weeks.
Discussing the PRECIOUS trial at the ESOC meeting, Christine Roffe, MD, professor of stroke medicine at Keele (England) University, and senior investigator of the MAPS study, suggested that a longer period of metoclopramide treatment may be needed than the 4 days given in the PRECIOUS study, as the risk of pneumonia persists for longer than just a few days.
She noted that another trial (MAPS-2) is now underway in the United Kingdom to try and confirm the first MAPS result with longer duration metoclopramide.
Dr. Van der Worp responded: “Certainly, I think that the MAPS-2 study should be continued. It is investigating a much longer duration of treatment, which may be beneficial, especially in patients with more severe strokes.”
On the reason for the disappointing results with paracetamol, Dr. Van der Worp elaborated: “We found that only a very few of these older patients developed a fever – only about 5% in the control group. Paracetamol did reduce the risk of fever, but because the proportion of patients who developed fever was so small, this may have been why it didn’t translate into any effect on the functional outcome.”
Dr. Roffe concluded that PRECIOUS was an important study. “There is also a positive message here. We have all been worried about using too many antibiotics. We need to make sure we use these drugs responsibly. I think this trial has told us there is little point in using antibiotics in a preventative way in these patients.”
She added that although the trial was stopped prematurely, it had produced decisive results.
“Yes, I believe that even if the trial was much larger, we still would not have shown an effect,” Dr. Van der Worp agreed.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
Intensive BP reduction after stroke recanalization harmful
MUNICH, GERMANY – suggests results from the OPTIMAL-BP trial.
The research, presented at the annual European Stroke Organisation Conference, supports the latest U.S. and European guidelines, which recommend a relatively high upper SBP limit.
For the trial, which was halted early, more than 300 patients who successfully underwent IAT for acute ischemic stroke were randomly assigned to intensive or conventional BP management within 2 hours of recanalization.
Patients in the intensive group were 44% less likely than those assigned to conventional management to have a favorable outcome of a modified Rankin Scale (mRS) score of 0-2 at 3 months, while having similar rates of adverse outcomes.
The results suggest that intensive BP lowering in the 24 hours after recanalization leads to an increased risk of disability without decreasing the risk of intracerebral hemorrhage (ICH) or death, said study presenter Hyo Suk Nam, MD, PhD, department of neurology, Yonsei (South Korea) University.
Consequently, the trial “does not support intensive blood pressure management” in that early post-IAT period, although the “optimal blood pressure range remains unclear and requires more investigation,” he said.
Dr. Nam added that the results suggest, “despite recanalization, some areas in the ischemic brain may have already been damaged,” or that surrounding areas continue to have reduced blood circulation.
He believes that these areas may have reduced capacity for autoregulation and so “may not effectively counteract sudden drops in blood pressure.
“Thus, intensive blood pressure lowering may further reduce blood flow ... and exacerbate ischemic injury.”
On the other hand, the conventional group confirmed prior studies indicating that high SBP is associated with poor outcomes.
Dr. Nam suggested that increased BP “may be a physiological response to the acute stress of stroke,” but that the adverse outcomes in some patients “might reflect stroke severity rather than being a direct effect of raised blood pressure.”
Session cochair Carlos Molina, MD, director of the stroke unit and brain hemodynamics at Vall d’Hebron Hospital, Barcelona, commented that “it’s very important to remember that the guidances are endorsed by the results of this study.
He said in an interview that “intensive blood pressure lowering harms the brain, especially just after reperfusion.
“So, the results are in line with the previous concept that we need to be careful, as intensive blood pressure lowering is associated with clinical deterioration and poor outcomes.”
He agreed with Dr. Nam that, with high BP also being harmful, the optimal range is currently unclear.
Dr. Molina underlined, however, that, in the absence of further studies, “we have to stick to the guidelines.”
Dr. Nam pointed out that, while high BP can result in reperfusion injury or ICH, “too low blood pressure can worsen cerebral ischemia.”
Yet the management of BP after successful recanalization with IAT is “largely unknown.”
He noted that, while both the European Stroke Organisation and American Heart Association/American Stroke Association guidelines recommend that BP should be kept below 180/105 mm Hg in patients who have undergone successful recanalization, the evidence class for this recommendation is “weak.”
Furthermore, observational studies have indicated that higher maximum or average SBP is associated with poor outcomes, but two multicenter clinical trials of intensive BP lowering after IAT, BP-TARGET and ENCHANTED2/MT, had conflicting results.
The researchers therefore investigated whether intensive BP management would result in better clinical outcomes in the 24 hours after successful recanalization with IAT.
They conducted a multicenter, open-label trial in which patients aged 20 years and older who underwent IAT for acute ischemic stroke with large cerebrovascular occlusion and had an SBP of at least 140 mm Hg were recruited from 19 centers in South Korea between June 2020 and November 2022.
The patients were randomly assigned within 2 hours of successful recanalization to intensive BP management, targeting an SBP less than 140 mm Hg, or conventional management, targeting an SBP of 140-180 mm Hg.
Clinicians could use local treatment protocols based on available intravenous BP-lowering drugs. BP was measured every 15 minutes for the first hour after randomization and then hourly for 24 hours.
The trial was terminated early because of safety concerns after the ENCHANTED2/MT trial revealed a negative impact on mRS scores at 3 months with intensive BP management.
Of 1,606 potentially eligible patients with acute ischemic stroke treated with IAT, 306 were randomly assigned, with 155 in the intensive group and 150 in the conventional group included in the primary analysis.
The mean age was 73.1 years, and 40.3% were women. The average National Institutes of Health Stroke Scale (NIHSS) score prior to IAT was 13. The mean time from stroke onset to randomization was 480 minutes (interquartile range, 320-820 minutes).
At 24 hours, the mean SBP in the intensive group was 129.2 mm Hg versus 138.0 mm Hg in the conventional group, for a between-group difference of 9.6 mm Hg (95% confidence interval, –12.2 to –6.9, P < .001).
Patients in the intensive group spent 80.3% of the first 24 hours with SBP less than 140 mm Hg versus 54.2% in the conventional group (P < .001). In contrast, conventional group patients spent 42.1% of the first 24 hours with SBP 140-180 mm Hg versus 14.2% in the intensive group.
Crucially, Dr. Nam showed that patients in the intensive BP-lowering group were significantly less likely than those in the conventional group to have a favorable outcome, defined as an mRS score of 0-2, at 3 months, at 39.4% versus 54.4%, or an adjusted odds ratio of 0.56 (95% CI, 0.33-0.96, P = .034).
Moreover, a poor outcome was 1.84 (95% CI, 1.17-2.91) times more common in the intervention group than the conventional group, Dr. Nam reported, with a number needed to harm of 6.6.
In terms of safety, there was no significant difference in rates of symptomatic ICH between the groups, at 9% in the intensive versus 8.1% in the conventional groups, or an aOR of 1.10 (95% CI, 0.48-2.53, P = .816).
There was also no difference in the rate of death related to the index stroke within 90 days, at 7.7% versus 5.4% (AOR, 1.73; 95% CI, 0.61-4.92, P = .307).
There were also no significant differences between the groups in key secondary outcomes, such as NIHSS score at 24 hours, recanalization at 24 hours, favorable outcome on the mRS at 1 month, and the EQ-5D-3L quality of life score.
However, patients in the intensive group were substantially more likely to experience malignant brain edema, at 7.7% versus 1.3% in the conventional group (aOR, 7.88; 95% CI, 1.57-39.39, P = .012).
Restricted cubic spline regression analysis indicated that there was a U-shaped relationship between mean SBP during the 24 hours following IAT and the odds ratio of a poor outcome, in which both a low and a high BPe were unfavorable.
Dr. Nam cautioned that, when interpreting the results, the early termination of the study may have reduced its statistical power and increased the likelihood of random and exaggerated treatment effects.
He also noted that the study was conducted in South Korea, and so the results may not be generalizable to other populations.
The study received a grant from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health and Welfare. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggests results from the OPTIMAL-BP trial.
The research, presented at the annual European Stroke Organisation Conference, supports the latest U.S. and European guidelines, which recommend a relatively high upper SBP limit.
For the trial, which was halted early, more than 300 patients who successfully underwent IAT for acute ischemic stroke were randomly assigned to intensive or conventional BP management within 2 hours of recanalization.
Patients in the intensive group were 44% less likely than those assigned to conventional management to have a favorable outcome of a modified Rankin Scale (mRS) score of 0-2 at 3 months, while having similar rates of adverse outcomes.
The results suggest that intensive BP lowering in the 24 hours after recanalization leads to an increased risk of disability without decreasing the risk of intracerebral hemorrhage (ICH) or death, said study presenter Hyo Suk Nam, MD, PhD, department of neurology, Yonsei (South Korea) University.
Consequently, the trial “does not support intensive blood pressure management” in that early post-IAT period, although the “optimal blood pressure range remains unclear and requires more investigation,” he said.
Dr. Nam added that the results suggest, “despite recanalization, some areas in the ischemic brain may have already been damaged,” or that surrounding areas continue to have reduced blood circulation.
He believes that these areas may have reduced capacity for autoregulation and so “may not effectively counteract sudden drops in blood pressure.
“Thus, intensive blood pressure lowering may further reduce blood flow ... and exacerbate ischemic injury.”
On the other hand, the conventional group confirmed prior studies indicating that high SBP is associated with poor outcomes.
Dr. Nam suggested that increased BP “may be a physiological response to the acute stress of stroke,” but that the adverse outcomes in some patients “might reflect stroke severity rather than being a direct effect of raised blood pressure.”
Session cochair Carlos Molina, MD, director of the stroke unit and brain hemodynamics at Vall d’Hebron Hospital, Barcelona, commented that “it’s very important to remember that the guidances are endorsed by the results of this study.
He said in an interview that “intensive blood pressure lowering harms the brain, especially just after reperfusion.
“So, the results are in line with the previous concept that we need to be careful, as intensive blood pressure lowering is associated with clinical deterioration and poor outcomes.”
He agreed with Dr. Nam that, with high BP also being harmful, the optimal range is currently unclear.
Dr. Molina underlined, however, that, in the absence of further studies, “we have to stick to the guidelines.”
Dr. Nam pointed out that, while high BP can result in reperfusion injury or ICH, “too low blood pressure can worsen cerebral ischemia.”
Yet the management of BP after successful recanalization with IAT is “largely unknown.”
He noted that, while both the European Stroke Organisation and American Heart Association/American Stroke Association guidelines recommend that BP should be kept below 180/105 mm Hg in patients who have undergone successful recanalization, the evidence class for this recommendation is “weak.”
Furthermore, observational studies have indicated that higher maximum or average SBP is associated with poor outcomes, but two multicenter clinical trials of intensive BP lowering after IAT, BP-TARGET and ENCHANTED2/MT, had conflicting results.
The researchers therefore investigated whether intensive BP management would result in better clinical outcomes in the 24 hours after successful recanalization with IAT.
They conducted a multicenter, open-label trial in which patients aged 20 years and older who underwent IAT for acute ischemic stroke with large cerebrovascular occlusion and had an SBP of at least 140 mm Hg were recruited from 19 centers in South Korea between June 2020 and November 2022.
The patients were randomly assigned within 2 hours of successful recanalization to intensive BP management, targeting an SBP less than 140 mm Hg, or conventional management, targeting an SBP of 140-180 mm Hg.
Clinicians could use local treatment protocols based on available intravenous BP-lowering drugs. BP was measured every 15 minutes for the first hour after randomization and then hourly for 24 hours.
The trial was terminated early because of safety concerns after the ENCHANTED2/MT trial revealed a negative impact on mRS scores at 3 months with intensive BP management.
Of 1,606 potentially eligible patients with acute ischemic stroke treated with IAT, 306 were randomly assigned, with 155 in the intensive group and 150 in the conventional group included in the primary analysis.
The mean age was 73.1 years, and 40.3% were women. The average National Institutes of Health Stroke Scale (NIHSS) score prior to IAT was 13. The mean time from stroke onset to randomization was 480 minutes (interquartile range, 320-820 minutes).
At 24 hours, the mean SBP in the intensive group was 129.2 mm Hg versus 138.0 mm Hg in the conventional group, for a between-group difference of 9.6 mm Hg (95% confidence interval, –12.2 to –6.9, P < .001).
Patients in the intensive group spent 80.3% of the first 24 hours with SBP less than 140 mm Hg versus 54.2% in the conventional group (P < .001). In contrast, conventional group patients spent 42.1% of the first 24 hours with SBP 140-180 mm Hg versus 14.2% in the intensive group.
Crucially, Dr. Nam showed that patients in the intensive BP-lowering group were significantly less likely than those in the conventional group to have a favorable outcome, defined as an mRS score of 0-2, at 3 months, at 39.4% versus 54.4%, or an adjusted odds ratio of 0.56 (95% CI, 0.33-0.96, P = .034).
Moreover, a poor outcome was 1.84 (95% CI, 1.17-2.91) times more common in the intervention group than the conventional group, Dr. Nam reported, with a number needed to harm of 6.6.
In terms of safety, there was no significant difference in rates of symptomatic ICH between the groups, at 9% in the intensive versus 8.1% in the conventional groups, or an aOR of 1.10 (95% CI, 0.48-2.53, P = .816).
There was also no difference in the rate of death related to the index stroke within 90 days, at 7.7% versus 5.4% (AOR, 1.73; 95% CI, 0.61-4.92, P = .307).
There were also no significant differences between the groups in key secondary outcomes, such as NIHSS score at 24 hours, recanalization at 24 hours, favorable outcome on the mRS at 1 month, and the EQ-5D-3L quality of life score.
However, patients in the intensive group were substantially more likely to experience malignant brain edema, at 7.7% versus 1.3% in the conventional group (aOR, 7.88; 95% CI, 1.57-39.39, P = .012).
Restricted cubic spline regression analysis indicated that there was a U-shaped relationship between mean SBP during the 24 hours following IAT and the odds ratio of a poor outcome, in which both a low and a high BPe were unfavorable.
Dr. Nam cautioned that, when interpreting the results, the early termination of the study may have reduced its statistical power and increased the likelihood of random and exaggerated treatment effects.
He also noted that the study was conducted in South Korea, and so the results may not be generalizable to other populations.
The study received a grant from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health and Welfare. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggests results from the OPTIMAL-BP trial.
The research, presented at the annual European Stroke Organisation Conference, supports the latest U.S. and European guidelines, which recommend a relatively high upper SBP limit.
For the trial, which was halted early, more than 300 patients who successfully underwent IAT for acute ischemic stroke were randomly assigned to intensive or conventional BP management within 2 hours of recanalization.
Patients in the intensive group were 44% less likely than those assigned to conventional management to have a favorable outcome of a modified Rankin Scale (mRS) score of 0-2 at 3 months, while having similar rates of adverse outcomes.
The results suggest that intensive BP lowering in the 24 hours after recanalization leads to an increased risk of disability without decreasing the risk of intracerebral hemorrhage (ICH) or death, said study presenter Hyo Suk Nam, MD, PhD, department of neurology, Yonsei (South Korea) University.
Consequently, the trial “does not support intensive blood pressure management” in that early post-IAT period, although the “optimal blood pressure range remains unclear and requires more investigation,” he said.
Dr. Nam added that the results suggest, “despite recanalization, some areas in the ischemic brain may have already been damaged,” or that surrounding areas continue to have reduced blood circulation.
He believes that these areas may have reduced capacity for autoregulation and so “may not effectively counteract sudden drops in blood pressure.
“Thus, intensive blood pressure lowering may further reduce blood flow ... and exacerbate ischemic injury.”
On the other hand, the conventional group confirmed prior studies indicating that high SBP is associated with poor outcomes.
Dr. Nam suggested that increased BP “may be a physiological response to the acute stress of stroke,” but that the adverse outcomes in some patients “might reflect stroke severity rather than being a direct effect of raised blood pressure.”
Session cochair Carlos Molina, MD, director of the stroke unit and brain hemodynamics at Vall d’Hebron Hospital, Barcelona, commented that “it’s very important to remember that the guidances are endorsed by the results of this study.
He said in an interview that “intensive blood pressure lowering harms the brain, especially just after reperfusion.
“So, the results are in line with the previous concept that we need to be careful, as intensive blood pressure lowering is associated with clinical deterioration and poor outcomes.”
He agreed with Dr. Nam that, with high BP also being harmful, the optimal range is currently unclear.
Dr. Molina underlined, however, that, in the absence of further studies, “we have to stick to the guidelines.”
Dr. Nam pointed out that, while high BP can result in reperfusion injury or ICH, “too low blood pressure can worsen cerebral ischemia.”
Yet the management of BP after successful recanalization with IAT is “largely unknown.”
He noted that, while both the European Stroke Organisation and American Heart Association/American Stroke Association guidelines recommend that BP should be kept below 180/105 mm Hg in patients who have undergone successful recanalization, the evidence class for this recommendation is “weak.”
Furthermore, observational studies have indicated that higher maximum or average SBP is associated with poor outcomes, but two multicenter clinical trials of intensive BP lowering after IAT, BP-TARGET and ENCHANTED2/MT, had conflicting results.
The researchers therefore investigated whether intensive BP management would result in better clinical outcomes in the 24 hours after successful recanalization with IAT.
They conducted a multicenter, open-label trial in which patients aged 20 years and older who underwent IAT for acute ischemic stroke with large cerebrovascular occlusion and had an SBP of at least 140 mm Hg were recruited from 19 centers in South Korea between June 2020 and November 2022.
The patients were randomly assigned within 2 hours of successful recanalization to intensive BP management, targeting an SBP less than 140 mm Hg, or conventional management, targeting an SBP of 140-180 mm Hg.
Clinicians could use local treatment protocols based on available intravenous BP-lowering drugs. BP was measured every 15 minutes for the first hour after randomization and then hourly for 24 hours.
The trial was terminated early because of safety concerns after the ENCHANTED2/MT trial revealed a negative impact on mRS scores at 3 months with intensive BP management.
Of 1,606 potentially eligible patients with acute ischemic stroke treated with IAT, 306 were randomly assigned, with 155 in the intensive group and 150 in the conventional group included in the primary analysis.
The mean age was 73.1 years, and 40.3% were women. The average National Institutes of Health Stroke Scale (NIHSS) score prior to IAT was 13. The mean time from stroke onset to randomization was 480 minutes (interquartile range, 320-820 minutes).
At 24 hours, the mean SBP in the intensive group was 129.2 mm Hg versus 138.0 mm Hg in the conventional group, for a between-group difference of 9.6 mm Hg (95% confidence interval, –12.2 to –6.9, P < .001).
Patients in the intensive group spent 80.3% of the first 24 hours with SBP less than 140 mm Hg versus 54.2% in the conventional group (P < .001). In contrast, conventional group patients spent 42.1% of the first 24 hours with SBP 140-180 mm Hg versus 14.2% in the intensive group.
Crucially, Dr. Nam showed that patients in the intensive BP-lowering group were significantly less likely than those in the conventional group to have a favorable outcome, defined as an mRS score of 0-2, at 3 months, at 39.4% versus 54.4%, or an adjusted odds ratio of 0.56 (95% CI, 0.33-0.96, P = .034).
Moreover, a poor outcome was 1.84 (95% CI, 1.17-2.91) times more common in the intervention group than the conventional group, Dr. Nam reported, with a number needed to harm of 6.6.
In terms of safety, there was no significant difference in rates of symptomatic ICH between the groups, at 9% in the intensive versus 8.1% in the conventional groups, or an aOR of 1.10 (95% CI, 0.48-2.53, P = .816).
There was also no difference in the rate of death related to the index stroke within 90 days, at 7.7% versus 5.4% (AOR, 1.73; 95% CI, 0.61-4.92, P = .307).
There were also no significant differences between the groups in key secondary outcomes, such as NIHSS score at 24 hours, recanalization at 24 hours, favorable outcome on the mRS at 1 month, and the EQ-5D-3L quality of life score.
However, patients in the intensive group were substantially more likely to experience malignant brain edema, at 7.7% versus 1.3% in the conventional group (aOR, 7.88; 95% CI, 1.57-39.39, P = .012).
Restricted cubic spline regression analysis indicated that there was a U-shaped relationship between mean SBP during the 24 hours following IAT and the odds ratio of a poor outcome, in which both a low and a high BPe were unfavorable.
Dr. Nam cautioned that, when interpreting the results, the early termination of the study may have reduced its statistical power and increased the likelihood of random and exaggerated treatment effects.
He also noted that the study was conducted in South Korea, and so the results may not be generalizable to other populations.
The study received a grant from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health and Welfare. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
AT ESOC 2023
Tenecteplase late after stroke misses endpoint: TIMELESS
However, there were some encouraging trends, and there did not appear to be an increase in intracranial hemorrhage (ICH), leading to hope that the option of late thrombolysis in this group of patients may still have potential.
The TIMELESS study tested the approach of giving thrombolysis with tenecteplase (TNK) to patients with a large-vessel occlusion stroke up to 24 hours after symptom onset. Patients were selected by perfusion imaging, and those who had a stroke with a small core and large amount of salvageable brain tissue were included in the placebo-controlled study.
“This is first trial to try giving a thrombolytic so late – up to 24 hours after last known well. While we did not meet the primary outcome, there were some promising findings,” lead author, Gregory Albers, MD, director of the Stanford (Calif.) Stroke Center and professor of neurology at Stanford University, said in an interview.
“The most encouraging observation was that we did not show any safety issues with giving TNK to this population at such a late time. Many people thought this would be too high risk but there was no increase in ICH, which was very low and the same in both groups,” Dr. Albers said.
“And we saw some evidence of drug effect. There appeared to be a benefit in patients with M1 occlusions, the most common type of large-vessel occlusion, who represented half the patients in the study,” he added.
The researchers also gained information on the logistics and timing of TNK administration in this late period which they hope can guide the design of a future trial.
Dr. Albers presented the TIMELESS trial at the annual European Stroke Organisation Conference.
He explained that there is increasing evidence that intravenous thrombolysis can improve outcome in selected patients even beyond the traditional 4.5-hour time window.
The phase 3, double-blind, randomized, placebo-controlled TIMELESS study sought to investigate whether tenecteplase administered to patients with ischemic stroke with large-vessel occlusion presenting between 4.5 and 24 hours after last known well would improve clinical outcome as measured by modified Rankin Scale (mRS) at day 90.
The trial included 458 patients with an internal carotid artery occlusion or middle cerebral artery segment 1 or 2 occlusion and presenting with salvageable tissue on imaging. They were randomly assigned 1:1 to either intravenous tenecteplase (0.25 mg/kg; maximum, 25 mg) or placebo.
The proportion of patients treated with mechanical thrombectomy were similar between the two treatment arms (around 77%). The study completion rate was higher than 96% in both treatment arms.
The primary endpoint analyses showed no significant difference in the odds of a lower mRS score at day 90, but there was a slight trend toward benefit in the TNK group in the shift analysis, with a common odds ratio of 1.13 (95% confidence interval, 0.81-1.56; P = .48).
The percentage of patients achieving a favorable outcome, defined as an mRS of 0-2, was not significantly different between the treatment groups: 46% in the TNK group versus 42% in the placebo group (nominal P = .41).
Promising safety data
There were no significant safety issues, and the risk for bleeding was not significantly increased in the tenecteplase group. Symptomatic ICH occurred in 3.2% of the TNK group versus 2.3% of the placebo group, a nonsignificant difference.
“The low rate of ICH with TNK at this late time point is very reassuring,” Dr. Albers said. “We believe the reason for the low ICH rate is probably because these patients were selected for small core strokes. We also found that there was a trend towards the most benefit from TNK in patients with the smallest cores, supporting the use of imaging to select patients.”
The secondary endpoint of complete recanalization at 24-hours post randomization was higher in the TNK group at 76.7%, compared with 63.9% in the placebo group (P = .006).
Benefit in M1 occlusions?
Subgroup analysis showed that there appeared to be a benefit of TNK in the 227 patients included who had an M1 occlusion. In this group, the common odds ratio for a more favorable outcome in the mRS shift analysis with TNK was 1.59 (95% CI, 1.00-2.52; adjusted nominal P = .051).
The percentage of patients with a favorable outcome (mRS, 0-2) at 90 days in the M1 occlusion subgroup was 45.9% for TNK versus 31.4% for placebo, giving an adjusted odds ratio of 2.03 (95% CI, 1.14-3.66; nominal P = .017).
But Dr. Albers cautioned that this was an exploratory analysis, and no formal conclusions should be drawn from these data.
“We saw very strong results in favor of giving thrombolysis in the patients with M1 occlusions. We had preliminary pilot data suggesting this approach may work in these patients,” he commented.
“But we included the smaller M2 occlusions as well, because we thought that as there should be less clot in an M2 occlusion it might be easier to dissolve with thrombolysis,” he added. “But surprisingly, the M2 occlusion patients seemed to do worse with TNK than placebo, and the M1 patients did better.”
Timing of TNK
Dr. Albers said that there was also information from in the study on the timing of TNK administration.
In patients who also received thrombectomy, who made up of the majority of those in the study, the average time of TNK administration was only 20 minutes before the thrombectomy procedure.
“We had hoped to have a longer time between thrombolysis and thrombectomy so the drug would have more time to work. The idea was that patients would be given TNK at the primary stroke center before being transferred for thrombectomy, but actually only a few patients received TNK at the primary stroke center,” Dr. Albers explained.
“But, again surprisingly, we found that patients given TNK right at the time of the thrombectomy procedure seemed to show a trend toward benefit over placebo,” he reported.
He suggested that this may be caused by the thrombolytic dissolving the small fragments that can sometimes break off and cause further occlusions when the clot is removed by thrombectomy.
“We have learned a lot from this study, and we are planning to go forward with the information gained to plan a second study, in which we will focus on patients with M1 occlusions and try to get the drug on board at primary stroke centers, so it has more time to work before thrombectomy,” he added.
Commenting on the TIMELESS study at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that he thought the trial had shown three important results: “Firstly, TNK appeared to be safe in this late window in these selected patients – that is a very important observation. Secondly, reperfusion rates at 24 hours were increased with TNK and we know that this translates into clinical benefit. And thirdly, there was a neutral effect on primary outcomes, but I think the sample size of 438 patients was not large enough to show efficacy.”
Dr. Tsivgoulis concluded that these points need to be addressed in future trials.
The TIMELESS trial was funded by Genentech.
A version of this article first appeared on Medscape.com.
However, there were some encouraging trends, and there did not appear to be an increase in intracranial hemorrhage (ICH), leading to hope that the option of late thrombolysis in this group of patients may still have potential.
The TIMELESS study tested the approach of giving thrombolysis with tenecteplase (TNK) to patients with a large-vessel occlusion stroke up to 24 hours after symptom onset. Patients were selected by perfusion imaging, and those who had a stroke with a small core and large amount of salvageable brain tissue were included in the placebo-controlled study.
“This is first trial to try giving a thrombolytic so late – up to 24 hours after last known well. While we did not meet the primary outcome, there were some promising findings,” lead author, Gregory Albers, MD, director of the Stanford (Calif.) Stroke Center and professor of neurology at Stanford University, said in an interview.
“The most encouraging observation was that we did not show any safety issues with giving TNK to this population at such a late time. Many people thought this would be too high risk but there was no increase in ICH, which was very low and the same in both groups,” Dr. Albers said.
“And we saw some evidence of drug effect. There appeared to be a benefit in patients with M1 occlusions, the most common type of large-vessel occlusion, who represented half the patients in the study,” he added.
The researchers also gained information on the logistics and timing of TNK administration in this late period which they hope can guide the design of a future trial.
Dr. Albers presented the TIMELESS trial at the annual European Stroke Organisation Conference.
He explained that there is increasing evidence that intravenous thrombolysis can improve outcome in selected patients even beyond the traditional 4.5-hour time window.
The phase 3, double-blind, randomized, placebo-controlled TIMELESS study sought to investigate whether tenecteplase administered to patients with ischemic stroke with large-vessel occlusion presenting between 4.5 and 24 hours after last known well would improve clinical outcome as measured by modified Rankin Scale (mRS) at day 90.
The trial included 458 patients with an internal carotid artery occlusion or middle cerebral artery segment 1 or 2 occlusion and presenting with salvageable tissue on imaging. They were randomly assigned 1:1 to either intravenous tenecteplase (0.25 mg/kg; maximum, 25 mg) or placebo.
The proportion of patients treated with mechanical thrombectomy were similar between the two treatment arms (around 77%). The study completion rate was higher than 96% in both treatment arms.
The primary endpoint analyses showed no significant difference in the odds of a lower mRS score at day 90, but there was a slight trend toward benefit in the TNK group in the shift analysis, with a common odds ratio of 1.13 (95% confidence interval, 0.81-1.56; P = .48).
The percentage of patients achieving a favorable outcome, defined as an mRS of 0-2, was not significantly different between the treatment groups: 46% in the TNK group versus 42% in the placebo group (nominal P = .41).
Promising safety data
There were no significant safety issues, and the risk for bleeding was not significantly increased in the tenecteplase group. Symptomatic ICH occurred in 3.2% of the TNK group versus 2.3% of the placebo group, a nonsignificant difference.
“The low rate of ICH with TNK at this late time point is very reassuring,” Dr. Albers said. “We believe the reason for the low ICH rate is probably because these patients were selected for small core strokes. We also found that there was a trend towards the most benefit from TNK in patients with the smallest cores, supporting the use of imaging to select patients.”
The secondary endpoint of complete recanalization at 24-hours post randomization was higher in the TNK group at 76.7%, compared with 63.9% in the placebo group (P = .006).
Benefit in M1 occlusions?
Subgroup analysis showed that there appeared to be a benefit of TNK in the 227 patients included who had an M1 occlusion. In this group, the common odds ratio for a more favorable outcome in the mRS shift analysis with TNK was 1.59 (95% CI, 1.00-2.52; adjusted nominal P = .051).
The percentage of patients with a favorable outcome (mRS, 0-2) at 90 days in the M1 occlusion subgroup was 45.9% for TNK versus 31.4% for placebo, giving an adjusted odds ratio of 2.03 (95% CI, 1.14-3.66; nominal P = .017).
But Dr. Albers cautioned that this was an exploratory analysis, and no formal conclusions should be drawn from these data.
“We saw very strong results in favor of giving thrombolysis in the patients with M1 occlusions. We had preliminary pilot data suggesting this approach may work in these patients,” he commented.
“But we included the smaller M2 occlusions as well, because we thought that as there should be less clot in an M2 occlusion it might be easier to dissolve with thrombolysis,” he added. “But surprisingly, the M2 occlusion patients seemed to do worse with TNK than placebo, and the M1 patients did better.”
Timing of TNK
Dr. Albers said that there was also information from in the study on the timing of TNK administration.
In patients who also received thrombectomy, who made up of the majority of those in the study, the average time of TNK administration was only 20 minutes before the thrombectomy procedure.
“We had hoped to have a longer time between thrombolysis and thrombectomy so the drug would have more time to work. The idea was that patients would be given TNK at the primary stroke center before being transferred for thrombectomy, but actually only a few patients received TNK at the primary stroke center,” Dr. Albers explained.
“But, again surprisingly, we found that patients given TNK right at the time of the thrombectomy procedure seemed to show a trend toward benefit over placebo,” he reported.
He suggested that this may be caused by the thrombolytic dissolving the small fragments that can sometimes break off and cause further occlusions when the clot is removed by thrombectomy.
“We have learned a lot from this study, and we are planning to go forward with the information gained to plan a second study, in which we will focus on patients with M1 occlusions and try to get the drug on board at primary stroke centers, so it has more time to work before thrombectomy,” he added.
Commenting on the TIMELESS study at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that he thought the trial had shown three important results: “Firstly, TNK appeared to be safe in this late window in these selected patients – that is a very important observation. Secondly, reperfusion rates at 24 hours were increased with TNK and we know that this translates into clinical benefit. And thirdly, there was a neutral effect on primary outcomes, but I think the sample size of 438 patients was not large enough to show efficacy.”
Dr. Tsivgoulis concluded that these points need to be addressed in future trials.
The TIMELESS trial was funded by Genentech.
A version of this article first appeared on Medscape.com.
However, there were some encouraging trends, and there did not appear to be an increase in intracranial hemorrhage (ICH), leading to hope that the option of late thrombolysis in this group of patients may still have potential.
The TIMELESS study tested the approach of giving thrombolysis with tenecteplase (TNK) to patients with a large-vessel occlusion stroke up to 24 hours after symptom onset. Patients were selected by perfusion imaging, and those who had a stroke with a small core and large amount of salvageable brain tissue were included in the placebo-controlled study.
“This is first trial to try giving a thrombolytic so late – up to 24 hours after last known well. While we did not meet the primary outcome, there were some promising findings,” lead author, Gregory Albers, MD, director of the Stanford (Calif.) Stroke Center and professor of neurology at Stanford University, said in an interview.
“The most encouraging observation was that we did not show any safety issues with giving TNK to this population at such a late time. Many people thought this would be too high risk but there was no increase in ICH, which was very low and the same in both groups,” Dr. Albers said.
“And we saw some evidence of drug effect. There appeared to be a benefit in patients with M1 occlusions, the most common type of large-vessel occlusion, who represented half the patients in the study,” he added.
The researchers also gained information on the logistics and timing of TNK administration in this late period which they hope can guide the design of a future trial.
Dr. Albers presented the TIMELESS trial at the annual European Stroke Organisation Conference.
He explained that there is increasing evidence that intravenous thrombolysis can improve outcome in selected patients even beyond the traditional 4.5-hour time window.
The phase 3, double-blind, randomized, placebo-controlled TIMELESS study sought to investigate whether tenecteplase administered to patients with ischemic stroke with large-vessel occlusion presenting between 4.5 and 24 hours after last known well would improve clinical outcome as measured by modified Rankin Scale (mRS) at day 90.
The trial included 458 patients with an internal carotid artery occlusion or middle cerebral artery segment 1 or 2 occlusion and presenting with salvageable tissue on imaging. They were randomly assigned 1:1 to either intravenous tenecteplase (0.25 mg/kg; maximum, 25 mg) or placebo.
The proportion of patients treated with mechanical thrombectomy were similar between the two treatment arms (around 77%). The study completion rate was higher than 96% in both treatment arms.
The primary endpoint analyses showed no significant difference in the odds of a lower mRS score at day 90, but there was a slight trend toward benefit in the TNK group in the shift analysis, with a common odds ratio of 1.13 (95% confidence interval, 0.81-1.56; P = .48).
The percentage of patients achieving a favorable outcome, defined as an mRS of 0-2, was not significantly different between the treatment groups: 46% in the TNK group versus 42% in the placebo group (nominal P = .41).
Promising safety data
There were no significant safety issues, and the risk for bleeding was not significantly increased in the tenecteplase group. Symptomatic ICH occurred in 3.2% of the TNK group versus 2.3% of the placebo group, a nonsignificant difference.
“The low rate of ICH with TNK at this late time point is very reassuring,” Dr. Albers said. “We believe the reason for the low ICH rate is probably because these patients were selected for small core strokes. We also found that there was a trend towards the most benefit from TNK in patients with the smallest cores, supporting the use of imaging to select patients.”
The secondary endpoint of complete recanalization at 24-hours post randomization was higher in the TNK group at 76.7%, compared with 63.9% in the placebo group (P = .006).
Benefit in M1 occlusions?
Subgroup analysis showed that there appeared to be a benefit of TNK in the 227 patients included who had an M1 occlusion. In this group, the common odds ratio for a more favorable outcome in the mRS shift analysis with TNK was 1.59 (95% CI, 1.00-2.52; adjusted nominal P = .051).
The percentage of patients with a favorable outcome (mRS, 0-2) at 90 days in the M1 occlusion subgroup was 45.9% for TNK versus 31.4% for placebo, giving an adjusted odds ratio of 2.03 (95% CI, 1.14-3.66; nominal P = .017).
But Dr. Albers cautioned that this was an exploratory analysis, and no formal conclusions should be drawn from these data.
“We saw very strong results in favor of giving thrombolysis in the patients with M1 occlusions. We had preliminary pilot data suggesting this approach may work in these patients,” he commented.
“But we included the smaller M2 occlusions as well, because we thought that as there should be less clot in an M2 occlusion it might be easier to dissolve with thrombolysis,” he added. “But surprisingly, the M2 occlusion patients seemed to do worse with TNK than placebo, and the M1 patients did better.”
Timing of TNK
Dr. Albers said that there was also information from in the study on the timing of TNK administration.
In patients who also received thrombectomy, who made up of the majority of those in the study, the average time of TNK administration was only 20 minutes before the thrombectomy procedure.
“We had hoped to have a longer time between thrombolysis and thrombectomy so the drug would have more time to work. The idea was that patients would be given TNK at the primary stroke center before being transferred for thrombectomy, but actually only a few patients received TNK at the primary stroke center,” Dr. Albers explained.
“But, again surprisingly, we found that patients given TNK right at the time of the thrombectomy procedure seemed to show a trend toward benefit over placebo,” he reported.
He suggested that this may be caused by the thrombolytic dissolving the small fragments that can sometimes break off and cause further occlusions when the clot is removed by thrombectomy.
“We have learned a lot from this study, and we are planning to go forward with the information gained to plan a second study, in which we will focus on patients with M1 occlusions and try to get the drug on board at primary stroke centers, so it has more time to work before thrombectomy,” he added.
Commenting on the TIMELESS study at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that he thought the trial had shown three important results: “Firstly, TNK appeared to be safe in this late window in these selected patients – that is a very important observation. Secondly, reperfusion rates at 24 hours were increased with TNK and we know that this translates into clinical benefit. And thirdly, there was a neutral effect on primary outcomes, but I think the sample size of 438 patients was not large enough to show efficacy.”
Dr. Tsivgoulis concluded that these points need to be addressed in future trials.
The TIMELESS trial was funded by Genentech.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
ECG implant tightens AFib management, improves outcomes in MONITOR-AF
Chronic conditions like diabetes or hypertension “often require long-term care through long-term monitoring,” observed a researcher, and “we know that continuous monitoring is superior to intermittent monitoring for long-term outcomes.”
So maybe practice should rely more on continuous ECG monitoring for patients with atrial fibrillation (AFib), also a chronic condition, proposed Dhanunjaya R. Lakkireddy, MD, of the Kansas City Heart Rhythm Institute, Overland Park, Kan., in presenting a new analysis at the annual scientific sessions of the Heart Rhythm Society.
(ILRs), compared with standard care. The latter could include intermittent 12-lead ECG, Holter, or other intermittent monitoring at physicians’ discretion.

Patients with AFib and the ECG implants in the MONITOR-AF study, which was not randomized and therefore only suggestive, were managed “more efficiently” with greater access to electrophysiologists (P < .01) and adherence to oral anticoagulants (P = .020) and other medications.
Followed for a mean of 2 years, patients with ILRs were more likely to undergo catheter ablation, and their time to a catheter ablation “was impressively shorter, 153 days versus 426 days” (P < .001), Dr. Lakkireddy said.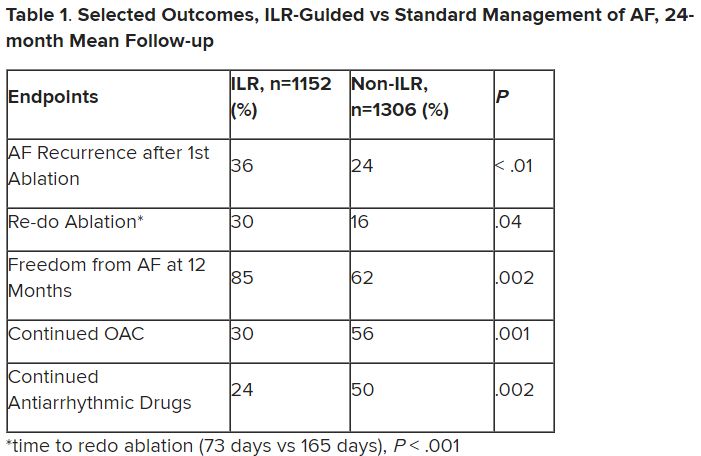
The ILR group also had fewer strokes and bleeding complications and were less likely to be hospitalized for AFib-related reasons, he said, because “a lot of these patients were caught ahead of time through the remote monitoring.”
For example, ILR patients had fewer heart failure (HF) hospitalizations, likely because “you’re not allowing these patients to remain with untreated rapid ventricular rates for a long period of time. You intervene early, thereby mitigating the onset of heart failure.”
Indeed, Dr. Lakkireddy said, their cumulative rate of any cardiovascular complication was “dramatically lower” – 3.4 versus 10.4 events per 100 person-years (P < .001).
Certainly, a routine recommendation to consider AFib patients for continuous monitoring would require randomized-trial evidence, he acknowledged. “This is an observation registry and proof of concept from a very heterogeneous cohort of patients. There were no obvious set criteria for ILR implantation.”
Nonetheless, “continuous and dynamic monitoring enabled quicker decision-making and patient management,” Dr. Lakkireddy said. “Especially in those patients who may have silent atrial fibrillation, an ILR could significantly mitigate the risk of complications from stroke and heart failure exacerbations.”
Several randomized trials have supported “earlier, more aggressive treatment” for AFib, including EAST-AFNET4, EARLY-AF, and CABANA, observed Daniel Morin, MD, MPH, of Ochsner Medical Center, New Orleans, as the invited discussant for Dr. Lakkireddy’s presentation.
So, he continued, if the goal is to “get every single AFib patient to ablation just as soon as possible,” then maybe MONITOR-AF supports the use of ILRs in such cases.
Indeed, it is “certainly possible” that the continuous stream of data from ILRs “allows faster progression of therapy and possibly even better outcomes” as MONITOR-AF suggests, said Dr. Morin, who is director of electrophysiology research at his center.
Moreover, ILR data could potentially “support shared decision-making perhaps by convincing the patient, and maybe their insurers, that we should move forward with ablation.”
But given the study’s observational, registry-based nature, the MONITOR-AF analysis is limited by potential confounders that complicate its interpretation.
For example, Dr. Morin continued, all ILR patients but only 60% of those on standard care˙ had access to an electrophysiologist (P = .001). That means “less access to some antiarrhythmic medications and certainly far less access to ablation therapy.”
Moreover, “during shared decision-making, a patient who sees the results of their ILR monitoring may be more prone to seek out or to accept earlier, more definitive therapy via ablation,” he said. “The presence of an ILR may then be a good way to move the needle toward ablation.”
Of note, an overwhelming majority of ILR patients received ablation, 93.5%, compared with 58.6% of standard-care patients. “It’s unclear how much of that association was caused by the ILR’s presence vs. other factors, such as physician availability, physician aggressiveness, or patient willingness for intervention,” Dr. Morin noted.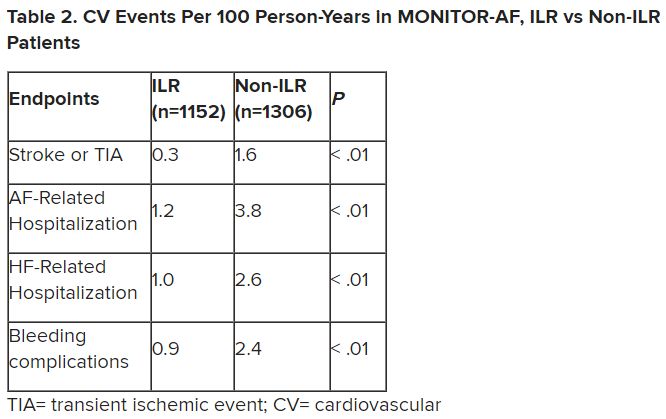
MONITOR-AF included 2,458 patients with paroxysmal or persistent AFib who either were implanted with or did not receive an ILR from 2018 to 2021 and were followed for at least 12 months.
The two groups were similar, Dr. Lakkireddy reported, with respect to demographics and baseline history AFib, hypertension, hyperlipidemia, diabetes, coronary disease, neurovascular events, peripheral artery disease, and obstructive sleep apnea.
Dr. Lakkireddy said a subgroup analysis is forthcoming, but that he’d “intuitively” think that the 15%-20% of AFib patients who are asymptomatic would gain the most from the ILR monitoring approach. There is already evidence that such patients tend to have the worst AFib outcomes, often receiving an AFib diagnosis only after presenting with consequences such as stroke or heart failure.
Dr. Lakkireddy disclosed receiving research grants, modest honoraria, or consulting fees from Abbott, Janssen, Boston Scientific, Johnson & Johnson, Biotronik, Bristol-Myers Squibb, Pfizer, Atricure, Northeast Scientific, and Acutus. Dr. Morin disclosed receiving research grants, honoraria, or consulting fees from Abbott and serving on a speakers’ bureau for Boston Scientific, Medtronic, and Zoll Medical.
A version of this article first appeared on Medscape.com.
Chronic conditions like diabetes or hypertension “often require long-term care through long-term monitoring,” observed a researcher, and “we know that continuous monitoring is superior to intermittent monitoring for long-term outcomes.”
So maybe practice should rely more on continuous ECG monitoring for patients with atrial fibrillation (AFib), also a chronic condition, proposed Dhanunjaya R. Lakkireddy, MD, of the Kansas City Heart Rhythm Institute, Overland Park, Kan., in presenting a new analysis at the annual scientific sessions of the Heart Rhythm Society.
(ILRs), compared with standard care. The latter could include intermittent 12-lead ECG, Holter, or other intermittent monitoring at physicians’ discretion.
Patients with AFib and the ECG implants in the MONITOR-AF study, which was not randomized and therefore only suggestive, were managed “more efficiently” with greater access to electrophysiologists (P < .01) and adherence to oral anticoagulants (P = .020) and other medications.
Followed for a mean of 2 years, patients with ILRs were more likely to undergo catheter ablation, and their time to a catheter ablation “was impressively shorter, 153 days versus 426 days” (P < .001), Dr. Lakkireddy said.
The ILR group also had fewer strokes and bleeding complications and were less likely to be hospitalized for AFib-related reasons, he said, because “a lot of these patients were caught ahead of time through the remote monitoring.”
For example, ILR patients had fewer heart failure (HF) hospitalizations, likely because “you’re not allowing these patients to remain with untreated rapid ventricular rates for a long period of time. You intervene early, thereby mitigating the onset of heart failure.”
Indeed, Dr. Lakkireddy said, their cumulative rate of any cardiovascular complication was “dramatically lower” – 3.4 versus 10.4 events per 100 person-years (P < .001).
Certainly, a routine recommendation to consider AFib patients for continuous monitoring would require randomized-trial evidence, he acknowledged. “This is an observation registry and proof of concept from a very heterogeneous cohort of patients. There were no obvious set criteria for ILR implantation.”
Nonetheless, “continuous and dynamic monitoring enabled quicker decision-making and patient management,” Dr. Lakkireddy said. “Especially in those patients who may have silent atrial fibrillation, an ILR could significantly mitigate the risk of complications from stroke and heart failure exacerbations.”
Several randomized trials have supported “earlier, more aggressive treatment” for AFib, including EAST-AFNET4, EARLY-AF, and CABANA, observed Daniel Morin, MD, MPH, of Ochsner Medical Center, New Orleans, as the invited discussant for Dr. Lakkireddy’s presentation.
So, he continued, if the goal is to “get every single AFib patient to ablation just as soon as possible,” then maybe MONITOR-AF supports the use of ILRs in such cases.
Indeed, it is “certainly possible” that the continuous stream of data from ILRs “allows faster progression of therapy and possibly even better outcomes” as MONITOR-AF suggests, said Dr. Morin, who is director of electrophysiology research at his center.
Moreover, ILR data could potentially “support shared decision-making perhaps by convincing the patient, and maybe their insurers, that we should move forward with ablation.”
But given the study’s observational, registry-based nature, the MONITOR-AF analysis is limited by potential confounders that complicate its interpretation.
For example, Dr. Morin continued, all ILR patients but only 60% of those on standard care˙ had access to an electrophysiologist (P = .001). That means “less access to some antiarrhythmic medications and certainly far less access to ablation therapy.”
Moreover, “during shared decision-making, a patient who sees the results of their ILR monitoring may be more prone to seek out or to accept earlier, more definitive therapy via ablation,” he said. “The presence of an ILR may then be a good way to move the needle toward ablation.”
Of note, an overwhelming majority of ILR patients received ablation, 93.5%, compared with 58.6% of standard-care patients. “It’s unclear how much of that association was caused by the ILR’s presence vs. other factors, such as physician availability, physician aggressiveness, or patient willingness for intervention,” Dr. Morin noted.
MONITOR-AF included 2,458 patients with paroxysmal or persistent AFib who either were implanted with or did not receive an ILR from 2018 to 2021 and were followed for at least 12 months.
The two groups were similar, Dr. Lakkireddy reported, with respect to demographics and baseline history AFib, hypertension, hyperlipidemia, diabetes, coronary disease, neurovascular events, peripheral artery disease, and obstructive sleep apnea.
Dr. Lakkireddy said a subgroup analysis is forthcoming, but that he’d “intuitively” think that the 15%-20% of AFib patients who are asymptomatic would gain the most from the ILR monitoring approach. There is already evidence that such patients tend to have the worst AFib outcomes, often receiving an AFib diagnosis only after presenting with consequences such as stroke or heart failure.
Dr. Lakkireddy disclosed receiving research grants, modest honoraria, or consulting fees from Abbott, Janssen, Boston Scientific, Johnson & Johnson, Biotronik, Bristol-Myers Squibb, Pfizer, Atricure, Northeast Scientific, and Acutus. Dr. Morin disclosed receiving research grants, honoraria, or consulting fees from Abbott and serving on a speakers’ bureau for Boston Scientific, Medtronic, and Zoll Medical.
A version of this article first appeared on Medscape.com.
Chronic conditions like diabetes or hypertension “often require long-term care through long-term monitoring,” observed a researcher, and “we know that continuous monitoring is superior to intermittent monitoring for long-term outcomes.”
So maybe practice should rely more on continuous ECG monitoring for patients with atrial fibrillation (AFib), also a chronic condition, proposed Dhanunjaya R. Lakkireddy, MD, of the Kansas City Heart Rhythm Institute, Overland Park, Kan., in presenting a new analysis at the annual scientific sessions of the Heart Rhythm Society.
(ILRs), compared with standard care. The latter could include intermittent 12-lead ECG, Holter, or other intermittent monitoring at physicians’ discretion.
Patients with AFib and the ECG implants in the MONITOR-AF study, which was not randomized and therefore only suggestive, were managed “more efficiently” with greater access to electrophysiologists (P < .01) and adherence to oral anticoagulants (P = .020) and other medications.
Followed for a mean of 2 years, patients with ILRs were more likely to undergo catheter ablation, and their time to a catheter ablation “was impressively shorter, 153 days versus 426 days” (P < .001), Dr. Lakkireddy said.
The ILR group also had fewer strokes and bleeding complications and were less likely to be hospitalized for AFib-related reasons, he said, because “a lot of these patients were caught ahead of time through the remote monitoring.”
For example, ILR patients had fewer heart failure (HF) hospitalizations, likely because “you’re not allowing these patients to remain with untreated rapid ventricular rates for a long period of time. You intervene early, thereby mitigating the onset of heart failure.”
Indeed, Dr. Lakkireddy said, their cumulative rate of any cardiovascular complication was “dramatically lower” – 3.4 versus 10.4 events per 100 person-years (P < .001).
Certainly, a routine recommendation to consider AFib patients for continuous monitoring would require randomized-trial evidence, he acknowledged. “This is an observation registry and proof of concept from a very heterogeneous cohort of patients. There were no obvious set criteria for ILR implantation.”
Nonetheless, “continuous and dynamic monitoring enabled quicker decision-making and patient management,” Dr. Lakkireddy said. “Especially in those patients who may have silent atrial fibrillation, an ILR could significantly mitigate the risk of complications from stroke and heart failure exacerbations.”
Several randomized trials have supported “earlier, more aggressive treatment” for AFib, including EAST-AFNET4, EARLY-AF, and CABANA, observed Daniel Morin, MD, MPH, of Ochsner Medical Center, New Orleans, as the invited discussant for Dr. Lakkireddy’s presentation.
So, he continued, if the goal is to “get every single AFib patient to ablation just as soon as possible,” then maybe MONITOR-AF supports the use of ILRs in such cases.
Indeed, it is “certainly possible” that the continuous stream of data from ILRs “allows faster progression of therapy and possibly even better outcomes” as MONITOR-AF suggests, said Dr. Morin, who is director of electrophysiology research at his center.
Moreover, ILR data could potentially “support shared decision-making perhaps by convincing the patient, and maybe their insurers, that we should move forward with ablation.”
But given the study’s observational, registry-based nature, the MONITOR-AF analysis is limited by potential confounders that complicate its interpretation.
For example, Dr. Morin continued, all ILR patients but only 60% of those on standard care˙ had access to an electrophysiologist (P = .001). That means “less access to some antiarrhythmic medications and certainly far less access to ablation therapy.”
Moreover, “during shared decision-making, a patient who sees the results of their ILR monitoring may be more prone to seek out or to accept earlier, more definitive therapy via ablation,” he said. “The presence of an ILR may then be a good way to move the needle toward ablation.”
Of note, an overwhelming majority of ILR patients received ablation, 93.5%, compared with 58.6% of standard-care patients. “It’s unclear how much of that association was caused by the ILR’s presence vs. other factors, such as physician availability, physician aggressiveness, or patient willingness for intervention,” Dr. Morin noted.
MONITOR-AF included 2,458 patients with paroxysmal or persistent AFib who either were implanted with or did not receive an ILR from 2018 to 2021 and were followed for at least 12 months.
The two groups were similar, Dr. Lakkireddy reported, with respect to demographics and baseline history AFib, hypertension, hyperlipidemia, diabetes, coronary disease, neurovascular events, peripheral artery disease, and obstructive sleep apnea.
Dr. Lakkireddy said a subgroup analysis is forthcoming, but that he’d “intuitively” think that the 15%-20% of AFib patients who are asymptomatic would gain the most from the ILR monitoring approach. There is already evidence that such patients tend to have the worst AFib outcomes, often receiving an AFib diagnosis only after presenting with consequences such as stroke or heart failure.
Dr. Lakkireddy disclosed receiving research grants, modest honoraria, or consulting fees from Abbott, Janssen, Boston Scientific, Johnson & Johnson, Biotronik, Bristol-Myers Squibb, Pfizer, Atricure, Northeast Scientific, and Acutus. Dr. Morin disclosed receiving research grants, honoraria, or consulting fees from Abbott and serving on a speakers’ bureau for Boston Scientific, Medtronic, and Zoll Medical.
A version of this article first appeared on Medscape.com.
FROM HEART RHYTHM 2023
Ancient plague, cyclical pandemics … history lesson?
Even the plague wanted to visit Stonehenge
We’re about to blow your mind: The history you learned in school was often inaccurate. Shocking, we know, so we’ll give you a minute to process this incredible news.
Better? Good. Now, let’s look back at high school European history. The Black Death, specifically. The common narrative is that the Mongols, while besieging a Crimean city belonging to the Genoese, catapulted dead bodies infected with some mystery disease that turned out to be the plague. The Genoese then brought the plague back to Italy, and from there, we all know the rest of the story.
The Black Death was certainly extremely important to the development of modern Europe as we know it, but the history books gloss over the much longer history of the plague. Yersinia pestis did not suddenly appear unbidden in a Mongol war camp in 1347. The Black Death wasn’t even the first horrific, continent-wide pandemic caused by the plague; the Plague of Justinian 800 years earlier crippled the Byzantine Empire during an expansionist phase and killed anywhere between 15 million and 100 million.
Today, though, LOTME looks even deeper into history, nearly beyond even history itself, back into the depths of early Bronze Age northern Europe. Specifically, to two ancient burial sites in England, where researchers have identified three 4,000-year-old cases of Y. pestis, the first recorded incidence of the disease in Britain.
Two of the individuals, identified through analysis of dental pulp, were young children buried at a mass grave in Somerset, while the third, a middle-aged woman, was found in a ring cairn in Cumbria. These sites are hundreds of miles apart, yet carbon dating suggests all three people lived and died at roughly the same time. The strain found is very similar to other samples of plague found across central and western Europe starting around 3,000 BCE, suggesting a single, easily spread disease affecting a large area in a relatively small period of time. In other words, a pandemic. Even in these ancient times, the world was connected. Not even the island of Britain could escape.
Beyond that though, the research helps confirm the cyclical nature of the plague; over time, it loses its effectiveness and goes into hiding, only to mutate and come roaring back. This is a story with absolutely no relevance at all to the modern world. Nope, no plagues or pandemics going around right now, no viruses fading into the background in any way. What a ridiculous inference to make.
Uncovering the invisible with artificial intelligence
This week in “What Else Can AI Do?” new research shows that a computer program can reveal brain injury that couldn’t be seen before with typical MRI.
The hot new AI, birthed by researchers at New York University, could potentially be a game changer by linking repeated head impacts with tiny, structural changes in the brains of athletes who have not been diagnosed with a concussion. By using machine learning to train the AI, the researchers were, for the first time, able to distinguish the brain of athletes who played contact sports (football, soccer, lacrosse) from those participating in noncontact sports such as baseball, basketball, and cross-country.
How did they do it? The investigators “designed statistical techniques that gave their computer program the ability to ‘learn’ how to predict exposure to repeated head impacts using mathematical models,” they explained in a written statement. Adding in data from the MRI scans of 81 male athletes with no known concussion diagnosis and the ability to identify unusual brain features between athletes with and without head trauma allowed the AI to predict results with accuracy even Miss Cleo would envy.
“This method may provide an important diagnostic tool not only for concussion, but also for detecting the damage that stems from subtler and more frequent head impacts,” said lead author Junbo Chen, an engineering doctoral candidate at NYU. That could make this new AI a valuable asset to science and medicine.
There are many things the human brain can do that AI can’t, and delegation could be one of them. Examining the data that represent the human brain in minute detail? Maybe we leave that to the machine.
Talk about your field promotions
If you’re a surgeon doing an amputation, the list of possible assistants pretty much starts and ends in only one place: Not the closest available janitor.
That may seem like an oddly obvious thing for us to say, but there’s at least one former Mainz (Germany) University Hospital physician who really needed to get this bit of advice before he attempted an unassisted toe amputation back in October of 2020. Yes, that does seem like kind of a long time ago for us to be reporting it now, but the details of the incident only just came to light a few days ago, thanks to German public broadcaster SWR.
Since it was just a toe, the surgeon thought he could perform the operation without any help. The toe, unfortunately, had other plans. The partially anesthetized patient got restless in the operating room, but with no actual trained nurse in the vicinity, the surgeon asked the closest available person – that would be the janitor – to lend a hand.
The surgical manager heard about these goings-on and got to the operating room too late to stop the procedure but soon enough to see the cleaning staffer “at the operating table with a bloody suction cup and a bloody compress in their hands,” SWR recently reported.
The incident was reported to the hospital’s medical director and the surgeon was fired, but since the patient experienced no complications not much fuss was made about it at the time.
Well, guess what? It’s toe-tally our job to make a fuss about these kinds of things. Or could it be that our job, much like the surgeon’s employment and the patient’s digit, is here toe-day and gone toe-morrow?
Even the plague wanted to visit Stonehenge
We’re about to blow your mind: The history you learned in school was often inaccurate. Shocking, we know, so we’ll give you a minute to process this incredible news.
Better? Good. Now, let’s look back at high school European history. The Black Death, specifically. The common narrative is that the Mongols, while besieging a Crimean city belonging to the Genoese, catapulted dead bodies infected with some mystery disease that turned out to be the plague. The Genoese then brought the plague back to Italy, and from there, we all know the rest of the story.
The Black Death was certainly extremely important to the development of modern Europe as we know it, but the history books gloss over the much longer history of the plague. Yersinia pestis did not suddenly appear unbidden in a Mongol war camp in 1347. The Black Death wasn’t even the first horrific, continent-wide pandemic caused by the plague; the Plague of Justinian 800 years earlier crippled the Byzantine Empire during an expansionist phase and killed anywhere between 15 million and 100 million.
Today, though, LOTME looks even deeper into history, nearly beyond even history itself, back into the depths of early Bronze Age northern Europe. Specifically, to two ancient burial sites in England, where researchers have identified three 4,000-year-old cases of Y. pestis, the first recorded incidence of the disease in Britain.
Two of the individuals, identified through analysis of dental pulp, were young children buried at a mass grave in Somerset, while the third, a middle-aged woman, was found in a ring cairn in Cumbria. These sites are hundreds of miles apart, yet carbon dating suggests all three people lived and died at roughly the same time. The strain found is very similar to other samples of plague found across central and western Europe starting around 3,000 BCE, suggesting a single, easily spread disease affecting a large area in a relatively small period of time. In other words, a pandemic. Even in these ancient times, the world was connected. Not even the island of Britain could escape.
Beyond that though, the research helps confirm the cyclical nature of the plague; over time, it loses its effectiveness and goes into hiding, only to mutate and come roaring back. This is a story with absolutely no relevance at all to the modern world. Nope, no plagues or pandemics going around right now, no viruses fading into the background in any way. What a ridiculous inference to make.
Uncovering the invisible with artificial intelligence
This week in “What Else Can AI Do?” new research shows that a computer program can reveal brain injury that couldn’t be seen before with typical MRI.
The hot new AI, birthed by researchers at New York University, could potentially be a game changer by linking repeated head impacts with tiny, structural changes in the brains of athletes who have not been diagnosed with a concussion. By using machine learning to train the AI, the researchers were, for the first time, able to distinguish the brain of athletes who played contact sports (football, soccer, lacrosse) from those participating in noncontact sports such as baseball, basketball, and cross-country.
How did they do it? The investigators “designed statistical techniques that gave their computer program the ability to ‘learn’ how to predict exposure to repeated head impacts using mathematical models,” they explained in a written statement. Adding in data from the MRI scans of 81 male athletes with no known concussion diagnosis and the ability to identify unusual brain features between athletes with and without head trauma allowed the AI to predict results with accuracy even Miss Cleo would envy.
“This method may provide an important diagnostic tool not only for concussion, but also for detecting the damage that stems from subtler and more frequent head impacts,” said lead author Junbo Chen, an engineering doctoral candidate at NYU. That could make this new AI a valuable asset to science and medicine.
There are many things the human brain can do that AI can’t, and delegation could be one of them. Examining the data that represent the human brain in minute detail? Maybe we leave that to the machine.
Talk about your field promotions
If you’re a surgeon doing an amputation, the list of possible assistants pretty much starts and ends in only one place: Not the closest available janitor.
That may seem like an oddly obvious thing for us to say, but there’s at least one former Mainz (Germany) University Hospital physician who really needed to get this bit of advice before he attempted an unassisted toe amputation back in October of 2020. Yes, that does seem like kind of a long time ago for us to be reporting it now, but the details of the incident only just came to light a few days ago, thanks to German public broadcaster SWR.
Since it was just a toe, the surgeon thought he could perform the operation without any help. The toe, unfortunately, had other plans. The partially anesthetized patient got restless in the operating room, but with no actual trained nurse in the vicinity, the surgeon asked the closest available person – that would be the janitor – to lend a hand.
The surgical manager heard about these goings-on and got to the operating room too late to stop the procedure but soon enough to see the cleaning staffer “at the operating table with a bloody suction cup and a bloody compress in their hands,” SWR recently reported.
The incident was reported to the hospital’s medical director and the surgeon was fired, but since the patient experienced no complications not much fuss was made about it at the time.
Well, guess what? It’s toe-tally our job to make a fuss about these kinds of things. Or could it be that our job, much like the surgeon’s employment and the patient’s digit, is here toe-day and gone toe-morrow?
Even the plague wanted to visit Stonehenge
We’re about to blow your mind: The history you learned in school was often inaccurate. Shocking, we know, so we’ll give you a minute to process this incredible news.
Better? Good. Now, let’s look back at high school European history. The Black Death, specifically. The common narrative is that the Mongols, while besieging a Crimean city belonging to the Genoese, catapulted dead bodies infected with some mystery disease that turned out to be the plague. The Genoese then brought the plague back to Italy, and from there, we all know the rest of the story.
The Black Death was certainly extremely important to the development of modern Europe as we know it, but the history books gloss over the much longer history of the plague. Yersinia pestis did not suddenly appear unbidden in a Mongol war camp in 1347. The Black Death wasn’t even the first horrific, continent-wide pandemic caused by the plague; the Plague of Justinian 800 years earlier crippled the Byzantine Empire during an expansionist phase and killed anywhere between 15 million and 100 million.
Today, though, LOTME looks even deeper into history, nearly beyond even history itself, back into the depths of early Bronze Age northern Europe. Specifically, to two ancient burial sites in England, where researchers have identified three 4,000-year-old cases of Y. pestis, the first recorded incidence of the disease in Britain.
Two of the individuals, identified through analysis of dental pulp, were young children buried at a mass grave in Somerset, while the third, a middle-aged woman, was found in a ring cairn in Cumbria. These sites are hundreds of miles apart, yet carbon dating suggests all three people lived and died at roughly the same time. The strain found is very similar to other samples of plague found across central and western Europe starting around 3,000 BCE, suggesting a single, easily spread disease affecting a large area in a relatively small period of time. In other words, a pandemic. Even in these ancient times, the world was connected. Not even the island of Britain could escape.
Beyond that though, the research helps confirm the cyclical nature of the plague; over time, it loses its effectiveness and goes into hiding, only to mutate and come roaring back. This is a story with absolutely no relevance at all to the modern world. Nope, no plagues or pandemics going around right now, no viruses fading into the background in any way. What a ridiculous inference to make.
Uncovering the invisible with artificial intelligence
This week in “What Else Can AI Do?” new research shows that a computer program can reveal brain injury that couldn’t be seen before with typical MRI.
The hot new AI, birthed by researchers at New York University, could potentially be a game changer by linking repeated head impacts with tiny, structural changes in the brains of athletes who have not been diagnosed with a concussion. By using machine learning to train the AI, the researchers were, for the first time, able to distinguish the brain of athletes who played contact sports (football, soccer, lacrosse) from those participating in noncontact sports such as baseball, basketball, and cross-country.
How did they do it? The investigators “designed statistical techniques that gave their computer program the ability to ‘learn’ how to predict exposure to repeated head impacts using mathematical models,” they explained in a written statement. Adding in data from the MRI scans of 81 male athletes with no known concussion diagnosis and the ability to identify unusual brain features between athletes with and without head trauma allowed the AI to predict results with accuracy even Miss Cleo would envy.
“This method may provide an important diagnostic tool not only for concussion, but also for detecting the damage that stems from subtler and more frequent head impacts,” said lead author Junbo Chen, an engineering doctoral candidate at NYU. That could make this new AI a valuable asset to science and medicine.
There are many things the human brain can do that AI can’t, and delegation could be one of them. Examining the data that represent the human brain in minute detail? Maybe we leave that to the machine.
Talk about your field promotions
If you’re a surgeon doing an amputation, the list of possible assistants pretty much starts and ends in only one place: Not the closest available janitor.
That may seem like an oddly obvious thing for us to say, but there’s at least one former Mainz (Germany) University Hospital physician who really needed to get this bit of advice before he attempted an unassisted toe amputation back in October of 2020. Yes, that does seem like kind of a long time ago for us to be reporting it now, but the details of the incident only just came to light a few days ago, thanks to German public broadcaster SWR.
Since it was just a toe, the surgeon thought he could perform the operation without any help. The toe, unfortunately, had other plans. The partially anesthetized patient got restless in the operating room, but with no actual trained nurse in the vicinity, the surgeon asked the closest available person – that would be the janitor – to lend a hand.
The surgical manager heard about these goings-on and got to the operating room too late to stop the procedure but soon enough to see the cleaning staffer “at the operating table with a bloody suction cup and a bloody compress in their hands,” SWR recently reported.
The incident was reported to the hospital’s medical director and the surgeon was fired, but since the patient experienced no complications not much fuss was made about it at the time.
Well, guess what? It’s toe-tally our job to make a fuss about these kinds of things. Or could it be that our job, much like the surgeon’s employment and the patient’s digit, is here toe-day and gone toe-morrow?
Troponin to ID diabetes patients with silent heart disease?
– based on data from a representative sample of more than 10,000 U.S. adults.
The finding suggests hs-cTnT maybe a useful marker for adults with diabetes who could benefit from more aggressive CVD risk reduction despite having no clinical indications of CVD.
The results “highlight the substantial burden of subclinical CVD in persons with diabetes and emphasize the importance of early detection and treatment of CVD for this high-risk population,” say the authors of the research, published in the Journal of the American Heart Association.

“This is the first study to examine subclinical CVD, defined by elevated cardiac biomarkers, in a nationally representative population of adults with or without diabetes. It provides novel information on the high burden of subclinical CVD [in American adults with diabetes] and the potential utility of hs-cTnT for monitoring this risk in people with diabetes,” said Elizabeth Selvin, PhD, senior author and a professor of epidemiology at Johns Hopkins University, Baltimore.
“What we are seeing is that many people with type 2 diabetes who have not had a heart attack or a history of cardiovascular disease are at high risk for cardiovascular complications,” added Dr. Selvin in an AHA press release. “When we look at the whole population of people diagnosed with type 2 diabetes, about 27 million adults in the U.S., according to the [Centers for Disease Control and Prevention], some are at low risk and some are at high risk for cardiovascular disease, so the open question is: ‘Who is most at risk?’ These cardiac biomarkers give us a window into cardiovascular risk in people who otherwise might not be recognized as highest risk.”
“Our results provide evidence to support use of cardiac biomarkers for routine risk monitoring in high-risk populations such as people with diabetes,” Dr. Selvin noted in an interview.
Need for aggressive CVD risk reduction
The findings also indicate that people with diabetes and an elevated hs-cTnT “should be targeted for aggressive cardiovascular risk reduction, including lifestyle interventions, weight loss, and treatment with statins, blood pressure medications, and cardioprotective therapies such as sodium-glucose cotransporter 2 (SGLT-2) inhibitors and glucagonlike peptide-1 (GLP-1) receptor agonists,” Dr. Selvin added.
“Cholesterol is often the factor that we target to reduce the risk of cardiovascular disease in people with type 2 diabetes,” she observed. “However, type 2 diabetes may have a direct effect on the heart not related to cholesterol levels. If type 2 diabetes is directly causing damage to the small vessels in the heart unrelated to cholesterol plaque buildup, then cholesterol-lowering medications are not going to prevent cardiac damage,” Dr. Selvin explained. “Our research suggests that additional non–statin-related therapies are needed to lower the cardiovascular disease risk in people with type 2 diabetes.”
However, she noted that a necessary step prior to formally recommending such a strategy is to run clinical trials to assess the efficacy of specific treatments, such as SGLT-2 inhibitors and GLP-1 agonists, in people with diabetes and elevated hs-cTnT.

“Randomized controlled trials would be best to test the relevance of measuring these biomarkers to assess risk in asymptomatic people with diabetes,” as well as prospective study of the value of hs-cTnT to guide treatment, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado at Denver, Aurora.
“I doubt measurements [of hs-cTnT] would be reimbursed [by third-party payers] if carried out without such outcome data,” he added.
Dr. Eckel also highlights the need to further validate in additional cohorts the link between elevations in hs-cTnT and CVD events in adults with diabetes, and to confirm that elevated levels of another cardiac biomarker – N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) – do not work as well as troponin as a risk marker for people with diabetes, another finding of the study.
ADA report already recommends testing these biomarkers for HF
However, a consensus report published in 2022 by the American Diabetes Association laid out the case for routinely and regularly measuring levels of both high sensitivity cardiac troponin and natriuretic peptides in people with diabetes for early identification of incident heart failure.
“Among individuals with diabetes, measurement of a natriuretic peptide or high-sensitivity cardiac troponin is recommended on at least a yearly basis to identify the earliest heart failure stages and implement strategies to prevent transition to symptomatic heart failure,” noted the ADA consensus report on heart failure.
The new study run by Dr. Selvin and coauthors used data collected by the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004 from U.S. adults who were at least 20 years old and had no history of CVD: myocardial infarction, stroke, coronary heart disease, or heart failure. This included 9,273 people without diabetes and 1,031 with diabetes, defined as a prior diagnosis or hemoglobin A1c of at least 6.5%.
“Cardiovascular risk varies substantially in adults with type 2 diabetes, highlighting the need for accurate risk stratification,” the authors observed.
All study participants had recorded measures of hs-cTnT and NT-proBNP.
The researchers considered an hs-cTnT level of greater than 14 ng/L and an NT-proBNP level of greater than 125 pg/mL as indicators of subclinical CVD.
The crude prevalence of elevated NT-proBNP was 33.4% among those with diabetes and 16.1% in those without diabetes. Elevated hs-cTnT occurred in 19% of those with diabetes and in 5% of those without diabetes. Elevated levels of both markers existed in 9% of those with diabetes and in 3% of those without diabetes.
“Approximately one in three adults with diabetes had subclinical CVD, with 19% having elevated levels of hs-cTnT, 23% having elevated NT-proBNP, and 9% having elevations in both cardiac biomarkers,” the researchers noted.
Diabetes linked with a doubled prevalence of elevated hs-cTnT
After adjustment for several demographic variables as well as traditional CVD risk factors, people with diabetes had a significant 98% higher rate of elevated hs-cTnT, compared with those without diabetes. But after similar adjustments, the rate of elevated NT-proBNP was significantly lower among people with diabetes, compared with controls, by a relative reduction of 24%.
“Our findings suggest that, in people with diabetes, hs-cTnT may be more useful [than NT-proBNP] for general risk monitoring, as its interpretation is less complicated,” said Dr. Selvin, who explained that “NT-proBNP is affected by overweight and obesity.”
In people with diabetes, the age-adjusted prevalence of elevated hs-cTnT ran higher in those with longer duration diabetes, and in those with less well-controlled diabetes based on a higher level of A1c. Neither of these factors showed any significant relationship with measured levels of NT-proBNP.
Further analysis linked the NHANES findings during 1999-2004 with U.S. national death records through the end of 2019. This showed that elevated levels of both hs-cTnT and NT-proBNP significantly linked with subsequently higher rates of all-cause mortality among people with diabetes. Elevated hs-cTnT linked with a 77% increased mortality and NT-proBNP linked with a 78% increased rate, compared with people with diabetes and no elevations in these markers, after adjustment for demographic variables and CVD risk factors.
However, for the outcome of cardiovascular death, elevated hs-cTnT linked with a nonsignificant 54% relative increase, while elevated NT-proBNP linked with a significant 2.46-fold relative increase.
The study “adds new data on biomarkers that are not routinely measured in asymptomatic people with or without diabetes” and the relationships of these markers to CVD mortality and all-cause mortality, Dr. Eckel concluded.
The study received no commercial funding, but used reagents donated by Abbott Laboratories, Ortho Clinical Diagnostics, Roche Diagnostics, and Siemens Healthcare Diagnostics. Dr. Selvin and Dr. Eckel had no disclosures.
A version of this article first appeared on Medscape.com.
– based on data from a representative sample of more than 10,000 U.S. adults.
The finding suggests hs-cTnT maybe a useful marker for adults with diabetes who could benefit from more aggressive CVD risk reduction despite having no clinical indications of CVD.
The results “highlight the substantial burden of subclinical CVD in persons with diabetes and emphasize the importance of early detection and treatment of CVD for this high-risk population,” say the authors of the research, published in the Journal of the American Heart Association.
“This is the first study to examine subclinical CVD, defined by elevated cardiac biomarkers, in a nationally representative population of adults with or without diabetes. It provides novel information on the high burden of subclinical CVD [in American adults with diabetes] and the potential utility of hs-cTnT for monitoring this risk in people with diabetes,” said Elizabeth Selvin, PhD, senior author and a professor of epidemiology at Johns Hopkins University, Baltimore.
“What we are seeing is that many people with type 2 diabetes who have not had a heart attack or a history of cardiovascular disease are at high risk for cardiovascular complications,” added Dr. Selvin in an AHA press release. “When we look at the whole population of people diagnosed with type 2 diabetes, about 27 million adults in the U.S., according to the [Centers for Disease Control and Prevention], some are at low risk and some are at high risk for cardiovascular disease, so the open question is: ‘Who is most at risk?’ These cardiac biomarkers give us a window into cardiovascular risk in people who otherwise might not be recognized as highest risk.”
“Our results provide evidence to support use of cardiac biomarkers for routine risk monitoring in high-risk populations such as people with diabetes,” Dr. Selvin noted in an interview.
Need for aggressive CVD risk reduction
The findings also indicate that people with diabetes and an elevated hs-cTnT “should be targeted for aggressive cardiovascular risk reduction, including lifestyle interventions, weight loss, and treatment with statins, blood pressure medications, and cardioprotective therapies such as sodium-glucose cotransporter 2 (SGLT-2) inhibitors and glucagonlike peptide-1 (GLP-1) receptor agonists,” Dr. Selvin added.
“Cholesterol is often the factor that we target to reduce the risk of cardiovascular disease in people with type 2 diabetes,” she observed. “However, type 2 diabetes may have a direct effect on the heart not related to cholesterol levels. If type 2 diabetes is directly causing damage to the small vessels in the heart unrelated to cholesterol plaque buildup, then cholesterol-lowering medications are not going to prevent cardiac damage,” Dr. Selvin explained. “Our research suggests that additional non–statin-related therapies are needed to lower the cardiovascular disease risk in people with type 2 diabetes.”
However, she noted that a necessary step prior to formally recommending such a strategy is to run clinical trials to assess the efficacy of specific treatments, such as SGLT-2 inhibitors and GLP-1 agonists, in people with diabetes and elevated hs-cTnT.
“Randomized controlled trials would be best to test the relevance of measuring these biomarkers to assess risk in asymptomatic people with diabetes,” as well as prospective study of the value of hs-cTnT to guide treatment, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado at Denver, Aurora.
“I doubt measurements [of hs-cTnT] would be reimbursed [by third-party payers] if carried out without such outcome data,” he added.
Dr. Eckel also highlights the need to further validate in additional cohorts the link between elevations in hs-cTnT and CVD events in adults with diabetes, and to confirm that elevated levels of another cardiac biomarker – N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) – do not work as well as troponin as a risk marker for people with diabetes, another finding of the study.
ADA report already recommends testing these biomarkers for HF
However, a consensus report published in 2022 by the American Diabetes Association laid out the case for routinely and regularly measuring levels of both high sensitivity cardiac troponin and natriuretic peptides in people with diabetes for early identification of incident heart failure.
“Among individuals with diabetes, measurement of a natriuretic peptide or high-sensitivity cardiac troponin is recommended on at least a yearly basis to identify the earliest heart failure stages and implement strategies to prevent transition to symptomatic heart failure,” noted the ADA consensus report on heart failure.
The new study run by Dr. Selvin and coauthors used data collected by the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004 from U.S. adults who were at least 20 years old and had no history of CVD: myocardial infarction, stroke, coronary heart disease, or heart failure. This included 9,273 people without diabetes and 1,031 with diabetes, defined as a prior diagnosis or hemoglobin A1c of at least 6.5%.
“Cardiovascular risk varies substantially in adults with type 2 diabetes, highlighting the need for accurate risk stratification,” the authors observed.
All study participants had recorded measures of hs-cTnT and NT-proBNP.
The researchers considered an hs-cTnT level of greater than 14 ng/L and an NT-proBNP level of greater than 125 pg/mL as indicators of subclinical CVD.
The crude prevalence of elevated NT-proBNP was 33.4% among those with diabetes and 16.1% in those without diabetes. Elevated hs-cTnT occurred in 19% of those with diabetes and in 5% of those without diabetes. Elevated levels of both markers existed in 9% of those with diabetes and in 3% of those without diabetes.
“Approximately one in three adults with diabetes had subclinical CVD, with 19% having elevated levels of hs-cTnT, 23% having elevated NT-proBNP, and 9% having elevations in both cardiac biomarkers,” the researchers noted.
Diabetes linked with a doubled prevalence of elevated hs-cTnT
After adjustment for several demographic variables as well as traditional CVD risk factors, people with diabetes had a significant 98% higher rate of elevated hs-cTnT, compared with those without diabetes. But after similar adjustments, the rate of elevated NT-proBNP was significantly lower among people with diabetes, compared with controls, by a relative reduction of 24%.
“Our findings suggest that, in people with diabetes, hs-cTnT may be more useful [than NT-proBNP] for general risk monitoring, as its interpretation is less complicated,” said Dr. Selvin, who explained that “NT-proBNP is affected by overweight and obesity.”
In people with diabetes, the age-adjusted prevalence of elevated hs-cTnT ran higher in those with longer duration diabetes, and in those with less well-controlled diabetes based on a higher level of A1c. Neither of these factors showed any significant relationship with measured levels of NT-proBNP.
Further analysis linked the NHANES findings during 1999-2004 with U.S. national death records through the end of 2019. This showed that elevated levels of both hs-cTnT and NT-proBNP significantly linked with subsequently higher rates of all-cause mortality among people with diabetes. Elevated hs-cTnT linked with a 77% increased mortality and NT-proBNP linked with a 78% increased rate, compared with people with diabetes and no elevations in these markers, after adjustment for demographic variables and CVD risk factors.
However, for the outcome of cardiovascular death, elevated hs-cTnT linked with a nonsignificant 54% relative increase, while elevated NT-proBNP linked with a significant 2.46-fold relative increase.
The study “adds new data on biomarkers that are not routinely measured in asymptomatic people with or without diabetes” and the relationships of these markers to CVD mortality and all-cause mortality, Dr. Eckel concluded.
The study received no commercial funding, but used reagents donated by Abbott Laboratories, Ortho Clinical Diagnostics, Roche Diagnostics, and Siemens Healthcare Diagnostics. Dr. Selvin and Dr. Eckel had no disclosures.
A version of this article first appeared on Medscape.com.
– based on data from a representative sample of more than 10,000 U.S. adults.
The finding suggests hs-cTnT maybe a useful marker for adults with diabetes who could benefit from more aggressive CVD risk reduction despite having no clinical indications of CVD.
The results “highlight the substantial burden of subclinical CVD in persons with diabetes and emphasize the importance of early detection and treatment of CVD for this high-risk population,” say the authors of the research, published in the Journal of the American Heart Association.
“This is the first study to examine subclinical CVD, defined by elevated cardiac biomarkers, in a nationally representative population of adults with or without diabetes. It provides novel information on the high burden of subclinical CVD [in American adults with diabetes] and the potential utility of hs-cTnT for monitoring this risk in people with diabetes,” said Elizabeth Selvin, PhD, senior author and a professor of epidemiology at Johns Hopkins University, Baltimore.
“What we are seeing is that many people with type 2 diabetes who have not had a heart attack or a history of cardiovascular disease are at high risk for cardiovascular complications,” added Dr. Selvin in an AHA press release. “When we look at the whole population of people diagnosed with type 2 diabetes, about 27 million adults in the U.S., according to the [Centers for Disease Control and Prevention], some are at low risk and some are at high risk for cardiovascular disease, so the open question is: ‘Who is most at risk?’ These cardiac biomarkers give us a window into cardiovascular risk in people who otherwise might not be recognized as highest risk.”
“Our results provide evidence to support use of cardiac biomarkers for routine risk monitoring in high-risk populations such as people with diabetes,” Dr. Selvin noted in an interview.
Need for aggressive CVD risk reduction
The findings also indicate that people with diabetes and an elevated hs-cTnT “should be targeted for aggressive cardiovascular risk reduction, including lifestyle interventions, weight loss, and treatment with statins, blood pressure medications, and cardioprotective therapies such as sodium-glucose cotransporter 2 (SGLT-2) inhibitors and glucagonlike peptide-1 (GLP-1) receptor agonists,” Dr. Selvin added.
“Cholesterol is often the factor that we target to reduce the risk of cardiovascular disease in people with type 2 diabetes,” she observed. “However, type 2 diabetes may have a direct effect on the heart not related to cholesterol levels. If type 2 diabetes is directly causing damage to the small vessels in the heart unrelated to cholesterol plaque buildup, then cholesterol-lowering medications are not going to prevent cardiac damage,” Dr. Selvin explained. “Our research suggests that additional non–statin-related therapies are needed to lower the cardiovascular disease risk in people with type 2 diabetes.”
However, she noted that a necessary step prior to formally recommending such a strategy is to run clinical trials to assess the efficacy of specific treatments, such as SGLT-2 inhibitors and GLP-1 agonists, in people with diabetes and elevated hs-cTnT.
“Randomized controlled trials would be best to test the relevance of measuring these biomarkers to assess risk in asymptomatic people with diabetes,” as well as prospective study of the value of hs-cTnT to guide treatment, commented Robert H. Eckel, MD, an endocrinologist affiliated with the University of Colorado at Denver, Aurora.
“I doubt measurements [of hs-cTnT] would be reimbursed [by third-party payers] if carried out without such outcome data,” he added.
Dr. Eckel also highlights the need to further validate in additional cohorts the link between elevations in hs-cTnT and CVD events in adults with diabetes, and to confirm that elevated levels of another cardiac biomarker – N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) – do not work as well as troponin as a risk marker for people with diabetes, another finding of the study.
ADA report already recommends testing these biomarkers for HF
However, a consensus report published in 2022 by the American Diabetes Association laid out the case for routinely and regularly measuring levels of both high sensitivity cardiac troponin and natriuretic peptides in people with diabetes for early identification of incident heart failure.
“Among individuals with diabetes, measurement of a natriuretic peptide or high-sensitivity cardiac troponin is recommended on at least a yearly basis to identify the earliest heart failure stages and implement strategies to prevent transition to symptomatic heart failure,” noted the ADA consensus report on heart failure.
The new study run by Dr. Selvin and coauthors used data collected by the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004 from U.S. adults who were at least 20 years old and had no history of CVD: myocardial infarction, stroke, coronary heart disease, or heart failure. This included 9,273 people without diabetes and 1,031 with diabetes, defined as a prior diagnosis or hemoglobin A1c of at least 6.5%.
“Cardiovascular risk varies substantially in adults with type 2 diabetes, highlighting the need for accurate risk stratification,” the authors observed.
All study participants had recorded measures of hs-cTnT and NT-proBNP.
The researchers considered an hs-cTnT level of greater than 14 ng/L and an NT-proBNP level of greater than 125 pg/mL as indicators of subclinical CVD.
The crude prevalence of elevated NT-proBNP was 33.4% among those with diabetes and 16.1% in those without diabetes. Elevated hs-cTnT occurred in 19% of those with diabetes and in 5% of those without diabetes. Elevated levels of both markers existed in 9% of those with diabetes and in 3% of those without diabetes.
“Approximately one in three adults with diabetes had subclinical CVD, with 19% having elevated levels of hs-cTnT, 23% having elevated NT-proBNP, and 9% having elevations in both cardiac biomarkers,” the researchers noted.
Diabetes linked with a doubled prevalence of elevated hs-cTnT
After adjustment for several demographic variables as well as traditional CVD risk factors, people with diabetes had a significant 98% higher rate of elevated hs-cTnT, compared with those without diabetes. But after similar adjustments, the rate of elevated NT-proBNP was significantly lower among people with diabetes, compared with controls, by a relative reduction of 24%.
“Our findings suggest that, in people with diabetes, hs-cTnT may be more useful [than NT-proBNP] for general risk monitoring, as its interpretation is less complicated,” said Dr. Selvin, who explained that “NT-proBNP is affected by overweight and obesity.”
In people with diabetes, the age-adjusted prevalence of elevated hs-cTnT ran higher in those with longer duration diabetes, and in those with less well-controlled diabetes based on a higher level of A1c. Neither of these factors showed any significant relationship with measured levels of NT-proBNP.
Further analysis linked the NHANES findings during 1999-2004 with U.S. national death records through the end of 2019. This showed that elevated levels of both hs-cTnT and NT-proBNP significantly linked with subsequently higher rates of all-cause mortality among people with diabetes. Elevated hs-cTnT linked with a 77% increased mortality and NT-proBNP linked with a 78% increased rate, compared with people with diabetes and no elevations in these markers, after adjustment for demographic variables and CVD risk factors.
However, for the outcome of cardiovascular death, elevated hs-cTnT linked with a nonsignificant 54% relative increase, while elevated NT-proBNP linked with a significant 2.46-fold relative increase.
The study “adds new data on biomarkers that are not routinely measured in asymptomatic people with or without diabetes” and the relationships of these markers to CVD mortality and all-cause mortality, Dr. Eckel concluded.
The study received no commercial funding, but used reagents donated by Abbott Laboratories, Ortho Clinical Diagnostics, Roche Diagnostics, and Siemens Healthcare Diagnostics. Dr. Selvin and Dr. Eckel had no disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Overweight in heterozygous FH tied to even higher CAD risk
MANNHEIM, GERMANY – – rates that appear to have a substantial impact on these patients’ already increased risk of coronary artery disease, a registry analysis suggests.
Data on almost 36,000 individuals with FH were collated from an international registry, revealing that 55% of adults and 25% of children and adolescents with the homozygous form of FH had overweight or obesity. The figures for heterozygous FH were 52% and 27%, respectively.
Crucially, overweight or obesity was associated with substantially increased rates of coronary artery disease, particularly in persons with heterozygous FH, among whom adults with obesity faced a twofold increased risk, rising to more than sixfold in children and adolescents.
Moreover, “obesity is associated with a worse lipid profile, even from childhood, regardless of whether a patient is on medication,” said study presenter Amany Elshorbagy, DPhil, Cardiovascular Epidemiologist, department of primary care and public health, Imperial College London.
She added that, with the increased risk of coronary artery disease associated with heterozygous FH, the results showed that “together with lipid-lowering medication, weight management is needed.”
The research was presented at the annual meeting of the European Atherosclerosis Society.
Tended to be thin
Alberico L. Catapano, MD, PhD, director of cardiovascular research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, and past president of the EAS, said in an interview that, historically, few FH patients were overweight or obese; rather, they tended to be thin.
However, there is now “a trend for people with FH to show more diabetes and obesity,” with the “bottom line” being that, as they are already at increased risk of coronary artery disease, it pushes their risk up even further.
In other words, if a risk factor such as obesity is added “on top of the strongest risk factor, that is LDL cholesterol, it is not one plus one makes two, it is one plus one makes three,” he said.
As such, Dr. Catapano believes that the study is “very interesting,” because it further underlines the importance of weight management for individuals with increased LDL cholesterol, “especially when you have genetic forms, like FH.”
Dr. Catapano’s comments were echoed by session co-chair Ulrike Schatz, MD, leader of the lipidology specialty department at the University Hospital Carl Gustav Carus, Technical University of Dresden (Germany).
Indeed, she told Dr. Elshorbagy before her presentation that she finds “a lot of my FH patients have a tendency towards anorexia.”
In an interview, Dr. Elshorbagy said that that reaction was typical of “most of the clinicians” she had spoken to. Upon seeing her data, especially for homozygous FH patients, they say, “They are on the lean side.”
Consequently, the research team went into the study “with the expectation that they might have a lower prevalence of obesity and overweight than the general population,” but “that’s not what we’re seeing.”
Dr. Elshorbagy noted that it would be helpful to have longitudinal data to determine whether, 50 years ago, patients with HF “were leaner, along with the rest of the population.”
The registry data are cross-sectional, and the team is now reaching out to the respective national lead investigators to submit follow-up data on their patients, with the aim of looking at changes in body weight and the impact on outcomes over time.
Another key question for the researchers is in regard to fat distribution, as body mass index “is not the best predictor of heart disease,” Dr. Elshorbagy said, but is rather central obesity.
Although they have also asked investigators to share waist circumference data, she conceded that it is a measurement that “is a lot harder to standardize across centers and countries; it’s not like putting patients on a scale.”
Overall, Dr. Elshorbagy believes that her findings indicate that clinicians should take a broader, more holistic approach toward their patients – in other words, an approach in which lipid lowering medication is “key but is just one of several things we need to do to make sure the coronary event rate goes down.”
More with than without
Dr. Elshorbagy began her presentation by highlighting that the prevalence of overweight and obesity ranges from 50% to 70% and that it is “the only health condition where you’ve got more people worldwide with the condition than without.”
Crucially, overweight increases the risk of coronary artery disease by approximately 20%. Among patients with obesity, the risk rises to 50%.
Given that FH patients “already have a very high risk of cardiovascular disease from their high cholesterol levels,” the team set out to determine rates of obesity and overweight in this population and their impact on coronary artery disease risk.
They used cross-sectional data from the EAS FH Studies Collaboration Global Registry, which involves 29,262 adults aged greater than or equal to 18 years and 6,275 children and adolescents aged 5 to 17 years with heterozygous FH, and 325 adults and 57 children with homozygous FH.
Dividing the adults into standard BMI categories, they found that 16% of heterozygous and 23% of homozygous FH patients had obesity, while 52% and 55%, respectively, had overweight or obesity.
For children, the team used World Health Organization z score cutoffs, which indicated that 9% of patients with heterozygous FH and 7% of patients with homozygous FH had obesity. Rates of overweight or obesity were 27% and 25%, respectively.
Among patients with heterozygous FH, rates of overweight or obesity among adults were 50% in high-income countries and 63% in other countries; among children, the rates were and 27% and 29%, respectively.
Stratified by region, the team found that the lowest rate of overweight or obesity among adult patients with heterozygous FH was in Eastern Asia, at 27%, while the highest was in Northern Africa/Western Asia (the Middle East), at 82%.
In North America, 56% of adult patients had overweight or obesity. The prevalence of coronary artery disease rose with increasing BMI.
Among adult patients with heterozygous FH, 11.3% of those with normal weight had coronary artery disease; the percentage rose to 22.9% among those with overweight, and 30.9% among those with obesity. Among children, the corresponding figures were 0.1%, 0.2%, and 0.7%.
Putting adults and children with homozygous FH together, the researchers found that 29.0% of patients with normal weight had coronary artery disease, compared with 31.3% of those with overweight and 49.3% of those with obesity.
Moreover, the results showed that levels of LDL and remnant cholesterol were significantly associated with BMI in adults and children with heterozygous FH, even after adjusting for age, sex, and lipid-lowering medication (P < .001 for all).
Multivariate analysis that took into account age, sex, lipid-lowering medication, and LDL cholesterol revealed that having obesity, compared with not having obesity, was associated with a substantial increase in the risk of coronary artery disease among patients with heterozygous FH.
Among adults with the condition, the odds ratio was 2.16 (95% confidence interval, 1.97-2.36), while among children and adolescents, it was 6.87 (95% CI, 1.55-30.46).
The results remained similar after further adjustment for the presence of diabetes and when considering peripheral artery disease and stroke.
No funding for the study was declared. Dr. Elshorbagy has relationships with Amgen, Daiichi Sankyo, and Regeneron.
A version of this article first appeared on Medscape.com.
MANNHEIM, GERMANY – – rates that appear to have a substantial impact on these patients’ already increased risk of coronary artery disease, a registry analysis suggests.
Data on almost 36,000 individuals with FH were collated from an international registry, revealing that 55% of adults and 25% of children and adolescents with the homozygous form of FH had overweight or obesity. The figures for heterozygous FH were 52% and 27%, respectively.
Crucially, overweight or obesity was associated with substantially increased rates of coronary artery disease, particularly in persons with heterozygous FH, among whom adults with obesity faced a twofold increased risk, rising to more than sixfold in children and adolescents.
Moreover, “obesity is associated with a worse lipid profile, even from childhood, regardless of whether a patient is on medication,” said study presenter Amany Elshorbagy, DPhil, Cardiovascular Epidemiologist, department of primary care and public health, Imperial College London.
She added that, with the increased risk of coronary artery disease associated with heterozygous FH, the results showed that “together with lipid-lowering medication, weight management is needed.”
The research was presented at the annual meeting of the European Atherosclerosis Society.
Tended to be thin
Alberico L. Catapano, MD, PhD, director of cardiovascular research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, and past president of the EAS, said in an interview that, historically, few FH patients were overweight or obese; rather, they tended to be thin.
However, there is now “a trend for people with FH to show more diabetes and obesity,” with the “bottom line” being that, as they are already at increased risk of coronary artery disease, it pushes their risk up even further.
In other words, if a risk factor such as obesity is added “on top of the strongest risk factor, that is LDL cholesterol, it is not one plus one makes two, it is one plus one makes three,” he said.
As such, Dr. Catapano believes that the study is “very interesting,” because it further underlines the importance of weight management for individuals with increased LDL cholesterol, “especially when you have genetic forms, like FH.”
Dr. Catapano’s comments were echoed by session co-chair Ulrike Schatz, MD, leader of the lipidology specialty department at the University Hospital Carl Gustav Carus, Technical University of Dresden (Germany).
Indeed, she told Dr. Elshorbagy before her presentation that she finds “a lot of my FH patients have a tendency towards anorexia.”
In an interview, Dr. Elshorbagy said that that reaction was typical of “most of the clinicians” she had spoken to. Upon seeing her data, especially for homozygous FH patients, they say, “They are on the lean side.”
Consequently, the research team went into the study “with the expectation that they might have a lower prevalence of obesity and overweight than the general population,” but “that’s not what we’re seeing.”
Dr. Elshorbagy noted that it would be helpful to have longitudinal data to determine whether, 50 years ago, patients with HF “were leaner, along with the rest of the population.”
The registry data are cross-sectional, and the team is now reaching out to the respective national lead investigators to submit follow-up data on their patients, with the aim of looking at changes in body weight and the impact on outcomes over time.
Another key question for the researchers is in regard to fat distribution, as body mass index “is not the best predictor of heart disease,” Dr. Elshorbagy said, but is rather central obesity.
Although they have also asked investigators to share waist circumference data, she conceded that it is a measurement that “is a lot harder to standardize across centers and countries; it’s not like putting patients on a scale.”
Overall, Dr. Elshorbagy believes that her findings indicate that clinicians should take a broader, more holistic approach toward their patients – in other words, an approach in which lipid lowering medication is “key but is just one of several things we need to do to make sure the coronary event rate goes down.”
More with than without
Dr. Elshorbagy began her presentation by highlighting that the prevalence of overweight and obesity ranges from 50% to 70% and that it is “the only health condition where you’ve got more people worldwide with the condition than without.”
Crucially, overweight increases the risk of coronary artery disease by approximately 20%. Among patients with obesity, the risk rises to 50%.
Given that FH patients “already have a very high risk of cardiovascular disease from their high cholesterol levels,” the team set out to determine rates of obesity and overweight in this population and their impact on coronary artery disease risk.
They used cross-sectional data from the EAS FH Studies Collaboration Global Registry, which involves 29,262 adults aged greater than or equal to 18 years and 6,275 children and adolescents aged 5 to 17 years with heterozygous FH, and 325 adults and 57 children with homozygous FH.
Dividing the adults into standard BMI categories, they found that 16% of heterozygous and 23% of homozygous FH patients had obesity, while 52% and 55%, respectively, had overweight or obesity.
For children, the team used World Health Organization z score cutoffs, which indicated that 9% of patients with heterozygous FH and 7% of patients with homozygous FH had obesity. Rates of overweight or obesity were 27% and 25%, respectively.
Among patients with heterozygous FH, rates of overweight or obesity among adults were 50% in high-income countries and 63% in other countries; among children, the rates were and 27% and 29%, respectively.
Stratified by region, the team found that the lowest rate of overweight or obesity among adult patients with heterozygous FH was in Eastern Asia, at 27%, while the highest was in Northern Africa/Western Asia (the Middle East), at 82%.
In North America, 56% of adult patients had overweight or obesity. The prevalence of coronary artery disease rose with increasing BMI.
Among adult patients with heterozygous FH, 11.3% of those with normal weight had coronary artery disease; the percentage rose to 22.9% among those with overweight, and 30.9% among those with obesity. Among children, the corresponding figures were 0.1%, 0.2%, and 0.7%.
Putting adults and children with homozygous FH together, the researchers found that 29.0% of patients with normal weight had coronary artery disease, compared with 31.3% of those with overweight and 49.3% of those with obesity.
Moreover, the results showed that levels of LDL and remnant cholesterol were significantly associated with BMI in adults and children with heterozygous FH, even after adjusting for age, sex, and lipid-lowering medication (P < .001 for all).
Multivariate analysis that took into account age, sex, lipid-lowering medication, and LDL cholesterol revealed that having obesity, compared with not having obesity, was associated with a substantial increase in the risk of coronary artery disease among patients with heterozygous FH.
Among adults with the condition, the odds ratio was 2.16 (95% confidence interval, 1.97-2.36), while among children and adolescents, it was 6.87 (95% CI, 1.55-30.46).
The results remained similar after further adjustment for the presence of diabetes and when considering peripheral artery disease and stroke.
No funding for the study was declared. Dr. Elshorbagy has relationships with Amgen, Daiichi Sankyo, and Regeneron.
A version of this article first appeared on Medscape.com.
MANNHEIM, GERMANY – – rates that appear to have a substantial impact on these patients’ already increased risk of coronary artery disease, a registry analysis suggests.
Data on almost 36,000 individuals with FH were collated from an international registry, revealing that 55% of adults and 25% of children and adolescents with the homozygous form of FH had overweight or obesity. The figures for heterozygous FH were 52% and 27%, respectively.
Crucially, overweight or obesity was associated with substantially increased rates of coronary artery disease, particularly in persons with heterozygous FH, among whom adults with obesity faced a twofold increased risk, rising to more than sixfold in children and adolescents.
Moreover, “obesity is associated with a worse lipid profile, even from childhood, regardless of whether a patient is on medication,” said study presenter Amany Elshorbagy, DPhil, Cardiovascular Epidemiologist, department of primary care and public health, Imperial College London.
She added that, with the increased risk of coronary artery disease associated with heterozygous FH, the results showed that “together with lipid-lowering medication, weight management is needed.”
The research was presented at the annual meeting of the European Atherosclerosis Society.
Tended to be thin
Alberico L. Catapano, MD, PhD, director of cardiovascular research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, and past president of the EAS, said in an interview that, historically, few FH patients were overweight or obese; rather, they tended to be thin.
However, there is now “a trend for people with FH to show more diabetes and obesity,” with the “bottom line” being that, as they are already at increased risk of coronary artery disease, it pushes their risk up even further.
In other words, if a risk factor such as obesity is added “on top of the strongest risk factor, that is LDL cholesterol, it is not one plus one makes two, it is one plus one makes three,” he said.
As such, Dr. Catapano believes that the study is “very interesting,” because it further underlines the importance of weight management for individuals with increased LDL cholesterol, “especially when you have genetic forms, like FH.”
Dr. Catapano’s comments were echoed by session co-chair Ulrike Schatz, MD, leader of the lipidology specialty department at the University Hospital Carl Gustav Carus, Technical University of Dresden (Germany).
Indeed, she told Dr. Elshorbagy before her presentation that she finds “a lot of my FH patients have a tendency towards anorexia.”
In an interview, Dr. Elshorbagy said that that reaction was typical of “most of the clinicians” she had spoken to. Upon seeing her data, especially for homozygous FH patients, they say, “They are on the lean side.”
Consequently, the research team went into the study “with the expectation that they might have a lower prevalence of obesity and overweight than the general population,” but “that’s not what we’re seeing.”
Dr. Elshorbagy noted that it would be helpful to have longitudinal data to determine whether, 50 years ago, patients with HF “were leaner, along with the rest of the population.”
The registry data are cross-sectional, and the team is now reaching out to the respective national lead investigators to submit follow-up data on their patients, with the aim of looking at changes in body weight and the impact on outcomes over time.
Another key question for the researchers is in regard to fat distribution, as body mass index “is not the best predictor of heart disease,” Dr. Elshorbagy said, but is rather central obesity.
Although they have also asked investigators to share waist circumference data, she conceded that it is a measurement that “is a lot harder to standardize across centers and countries; it’s not like putting patients on a scale.”
Overall, Dr. Elshorbagy believes that her findings indicate that clinicians should take a broader, more holistic approach toward their patients – in other words, an approach in which lipid lowering medication is “key but is just one of several things we need to do to make sure the coronary event rate goes down.”
More with than without
Dr. Elshorbagy began her presentation by highlighting that the prevalence of overweight and obesity ranges from 50% to 70% and that it is “the only health condition where you’ve got more people worldwide with the condition than without.”
Crucially, overweight increases the risk of coronary artery disease by approximately 20%. Among patients with obesity, the risk rises to 50%.
Given that FH patients “already have a very high risk of cardiovascular disease from their high cholesterol levels,” the team set out to determine rates of obesity and overweight in this population and their impact on coronary artery disease risk.
They used cross-sectional data from the EAS FH Studies Collaboration Global Registry, which involves 29,262 adults aged greater than or equal to 18 years and 6,275 children and adolescents aged 5 to 17 years with heterozygous FH, and 325 adults and 57 children with homozygous FH.
Dividing the adults into standard BMI categories, they found that 16% of heterozygous and 23% of homozygous FH patients had obesity, while 52% and 55%, respectively, had overweight or obesity.
For children, the team used World Health Organization z score cutoffs, which indicated that 9% of patients with heterozygous FH and 7% of patients with homozygous FH had obesity. Rates of overweight or obesity were 27% and 25%, respectively.
Among patients with heterozygous FH, rates of overweight or obesity among adults were 50% in high-income countries and 63% in other countries; among children, the rates were and 27% and 29%, respectively.
Stratified by region, the team found that the lowest rate of overweight or obesity among adult patients with heterozygous FH was in Eastern Asia, at 27%, while the highest was in Northern Africa/Western Asia (the Middle East), at 82%.
In North America, 56% of adult patients had overweight or obesity. The prevalence of coronary artery disease rose with increasing BMI.
Among adult patients with heterozygous FH, 11.3% of those with normal weight had coronary artery disease; the percentage rose to 22.9% among those with overweight, and 30.9% among those with obesity. Among children, the corresponding figures were 0.1%, 0.2%, and 0.7%.
Putting adults and children with homozygous FH together, the researchers found that 29.0% of patients with normal weight had coronary artery disease, compared with 31.3% of those with overweight and 49.3% of those with obesity.
Moreover, the results showed that levels of LDL and remnant cholesterol were significantly associated with BMI in adults and children with heterozygous FH, even after adjusting for age, sex, and lipid-lowering medication (P < .001 for all).
Multivariate analysis that took into account age, sex, lipid-lowering medication, and LDL cholesterol revealed that having obesity, compared with not having obesity, was associated with a substantial increase in the risk of coronary artery disease among patients with heterozygous FH.
Among adults with the condition, the odds ratio was 2.16 (95% confidence interval, 1.97-2.36), while among children and adolescents, it was 6.87 (95% CI, 1.55-30.46).
The results remained similar after further adjustment for the presence of diabetes and when considering peripheral artery disease and stroke.
No funding for the study was declared. Dr. Elshorbagy has relationships with Amgen, Daiichi Sankyo, and Regeneron.
A version of this article first appeared on Medscape.com.
AT EAS 2023
Cardiopathy no basis for choosing anticoagulation in ESUS
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.

The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.
The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.
The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
No added benefit from revascularization in low-risk CAS
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023