User login
Child-to-Parent Violence Common in Court Record Review
BOSTON – Family violence is not limited to spousal or child abuse: Adolescents and preteens are also capable of violent, destructive behavior against family members, said an Australian investigator at the annual meeting of the American Academy of Psychiatry and the Law.
Nearly half of all restraining-order applications from a large children’s court in Australia were related to child-to-parent violence, reported Mr. Gennady Baksheev, a research fellow at the University of Melbourne.
Most of the violence was related to long-standing behavioral problems, with the perpetrators primarily being males and the victims primarily females. In 58% of the cases, the violent episodes occurred in single-parent households.
"Family violence perpetrated by children against their parents or siblings has received little attention, although it is increasingly being recognized as a serious problem for social services, law enforcement, and the courts," Mr. Baksheev said.
The medical literature has consistently shown that the "battered parent syndrome" is most frequently perpetrated by boys against their mothers, and that boys are more likely to engage in physically abusive behaviors, whereas girls are more likely to be emotionally or verbally abusive, he said.
Estimates of the prevalence of child-to-parent violence range from 7% to 56%, with differences in research methods and definitions accounting for the discrepancy. Explanations for this type of behavior include disturbances in family hierarchy, parents with harsh or punitive control strategies, familial conflict (including witnessing and modeling of parental violence), and psychiatric and/or behavioral disturbances among juveniles, Mr. Baksheev noted.
He and his colleagues conducted a retrospective audit of consecutive court records from the Melbourne Children’s Court, looking for applications for restraining orders against juvenile defendants. The records included the characteristics of the victims and perpetrators, the nature of the behavior prompting the applications, and the precipitants of the perpetrators’ behavior.
In all, 438 of the 928 applications filed during the study period met the criteria for juvenile family violence. Half of the applications (50%) were filed by the primary victim; most of the remaining half (49.4%) were filed by an adult on behalf of the victim. Nearly one-third of the applications (30%) were filed outside of normal court hours, suggesting emergencies.
Of the 438 perpetrators, 300 (69%) were boys. The mean age was 15.9 years (range, 12-18 years). Two-thirds of the sample (66%) were living in single-parent households, and 19.5% were living with both parents. (The remaining living arrangements were not specified.) In all, 14% of the perpetrators had a diagnosis of mental illness.
More than three-fourths of the victims (77%) were female, with a mean age of 40.2 years (range, 5-78 years). The victim was a parent in 78% of the cases, a sibling in 11%, and another relative, such as a stepsibling or grandparent, in 9%. (The remaining 2% were not specified.)
About 50% of the cases involved threats to the victim, 55% involved assaults, and 60% involved damage to property.
The motivation for violence was attributed to behavioral problems in 52% of cases, intimidation in 13%, family problems in 10%, retaliation in 9%, drug issues in 8%, mental disorders in 6%, and sexual predation in 2%.
In all, 56% of applications for restraining orders were not granted, but fewer than a third of these were attributable to court refusal. The majority were not granted because the victim refused to proceed. An analysis showed that not proceeding with a restraining order was significantly associated with the applicant being the primary victim (P less than .001).
In a post hoc analysis, the authors found that restraining orders were nearly 1.8 times more likely to be granted against male vs. female defendants. One-third of all restraining orders (32%) issued were subsequently breached, Mr. Baksheev said.
"The legal and social consequences of this are serious and sobering both for the family and the defendant who may be subject to criminal charges," Mr. Baksheev said.
Mr. Baksheev’s study was supported by the Ian Potter Foundation. He reported that he had no relevant financial disclosures.
BOSTON – Family violence is not limited to spousal or child abuse: Adolescents and preteens are also capable of violent, destructive behavior against family members, said an Australian investigator at the annual meeting of the American Academy of Psychiatry and the Law.
Nearly half of all restraining-order applications from a large children’s court in Australia were related to child-to-parent violence, reported Mr. Gennady Baksheev, a research fellow at the University of Melbourne.
Most of the violence was related to long-standing behavioral problems, with the perpetrators primarily being males and the victims primarily females. In 58% of the cases, the violent episodes occurred in single-parent households.
"Family violence perpetrated by children against their parents or siblings has received little attention, although it is increasingly being recognized as a serious problem for social services, law enforcement, and the courts," Mr. Baksheev said.
The medical literature has consistently shown that the "battered parent syndrome" is most frequently perpetrated by boys against their mothers, and that boys are more likely to engage in physically abusive behaviors, whereas girls are more likely to be emotionally or verbally abusive, he said.
Estimates of the prevalence of child-to-parent violence range from 7% to 56%, with differences in research methods and definitions accounting for the discrepancy. Explanations for this type of behavior include disturbances in family hierarchy, parents with harsh or punitive control strategies, familial conflict (including witnessing and modeling of parental violence), and psychiatric and/or behavioral disturbances among juveniles, Mr. Baksheev noted.
He and his colleagues conducted a retrospective audit of consecutive court records from the Melbourne Children’s Court, looking for applications for restraining orders against juvenile defendants. The records included the characteristics of the victims and perpetrators, the nature of the behavior prompting the applications, and the precipitants of the perpetrators’ behavior.
In all, 438 of the 928 applications filed during the study period met the criteria for juvenile family violence. Half of the applications (50%) were filed by the primary victim; most of the remaining half (49.4%) were filed by an adult on behalf of the victim. Nearly one-third of the applications (30%) were filed outside of normal court hours, suggesting emergencies.
Of the 438 perpetrators, 300 (69%) were boys. The mean age was 15.9 years (range, 12-18 years). Two-thirds of the sample (66%) were living in single-parent households, and 19.5% were living with both parents. (The remaining living arrangements were not specified.) In all, 14% of the perpetrators had a diagnosis of mental illness.
More than three-fourths of the victims (77%) were female, with a mean age of 40.2 years (range, 5-78 years). The victim was a parent in 78% of the cases, a sibling in 11%, and another relative, such as a stepsibling or grandparent, in 9%. (The remaining 2% were not specified.)
About 50% of the cases involved threats to the victim, 55% involved assaults, and 60% involved damage to property.
The motivation for violence was attributed to behavioral problems in 52% of cases, intimidation in 13%, family problems in 10%, retaliation in 9%, drug issues in 8%, mental disorders in 6%, and sexual predation in 2%.
In all, 56% of applications for restraining orders were not granted, but fewer than a third of these were attributable to court refusal. The majority were not granted because the victim refused to proceed. An analysis showed that not proceeding with a restraining order was significantly associated with the applicant being the primary victim (P less than .001).
In a post hoc analysis, the authors found that restraining orders were nearly 1.8 times more likely to be granted against male vs. female defendants. One-third of all restraining orders (32%) issued were subsequently breached, Mr. Baksheev said.
"The legal and social consequences of this are serious and sobering both for the family and the defendant who may be subject to criminal charges," Mr. Baksheev said.
Mr. Baksheev’s study was supported by the Ian Potter Foundation. He reported that he had no relevant financial disclosures.
BOSTON – Family violence is not limited to spousal or child abuse: Adolescents and preteens are also capable of violent, destructive behavior against family members, said an Australian investigator at the annual meeting of the American Academy of Psychiatry and the Law.
Nearly half of all restraining-order applications from a large children’s court in Australia were related to child-to-parent violence, reported Mr. Gennady Baksheev, a research fellow at the University of Melbourne.
Most of the violence was related to long-standing behavioral problems, with the perpetrators primarily being males and the victims primarily females. In 58% of the cases, the violent episodes occurred in single-parent households.
"Family violence perpetrated by children against their parents or siblings has received little attention, although it is increasingly being recognized as a serious problem for social services, law enforcement, and the courts," Mr. Baksheev said.
The medical literature has consistently shown that the "battered parent syndrome" is most frequently perpetrated by boys against their mothers, and that boys are more likely to engage in physically abusive behaviors, whereas girls are more likely to be emotionally or verbally abusive, he said.
Estimates of the prevalence of child-to-parent violence range from 7% to 56%, with differences in research methods and definitions accounting for the discrepancy. Explanations for this type of behavior include disturbances in family hierarchy, parents with harsh or punitive control strategies, familial conflict (including witnessing and modeling of parental violence), and psychiatric and/or behavioral disturbances among juveniles, Mr. Baksheev noted.
He and his colleagues conducted a retrospective audit of consecutive court records from the Melbourne Children’s Court, looking for applications for restraining orders against juvenile defendants. The records included the characteristics of the victims and perpetrators, the nature of the behavior prompting the applications, and the precipitants of the perpetrators’ behavior.
In all, 438 of the 928 applications filed during the study period met the criteria for juvenile family violence. Half of the applications (50%) were filed by the primary victim; most of the remaining half (49.4%) were filed by an adult on behalf of the victim. Nearly one-third of the applications (30%) were filed outside of normal court hours, suggesting emergencies.
Of the 438 perpetrators, 300 (69%) were boys. The mean age was 15.9 years (range, 12-18 years). Two-thirds of the sample (66%) were living in single-parent households, and 19.5% were living with both parents. (The remaining living arrangements were not specified.) In all, 14% of the perpetrators had a diagnosis of mental illness.
More than three-fourths of the victims (77%) were female, with a mean age of 40.2 years (range, 5-78 years). The victim was a parent in 78% of the cases, a sibling in 11%, and another relative, such as a stepsibling or grandparent, in 9%. (The remaining 2% were not specified.)
About 50% of the cases involved threats to the victim, 55% involved assaults, and 60% involved damage to property.
The motivation for violence was attributed to behavioral problems in 52% of cases, intimidation in 13%, family problems in 10%, retaliation in 9%, drug issues in 8%, mental disorders in 6%, and sexual predation in 2%.
In all, 56% of applications for restraining orders were not granted, but fewer than a third of these were attributable to court refusal. The majority were not granted because the victim refused to proceed. An analysis showed that not proceeding with a restraining order was significantly associated with the applicant being the primary victim (P less than .001).
In a post hoc analysis, the authors found that restraining orders were nearly 1.8 times more likely to be granted against male vs. female defendants. One-third of all restraining orders (32%) issued were subsequently breached, Mr. Baksheev said.
"The legal and social consequences of this are serious and sobering both for the family and the defendant who may be subject to criminal charges," Mr. Baksheev said.
Mr. Baksheev’s study was supported by the Ian Potter Foundation. He reported that he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: Some 47% of all restraining-order applications in a large Australian children’s court were to protect family members from a juvenile.
Data Source: A retrospective review of records from the Melbourne Children’s Court.
Disclosures: Mr. Baksheev’s study was supported by the Ian Potter Foundation. He reported that he had no relevant financial disclosures.
Caffeine Linked to Psychosis in Case Series
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.

Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.
Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.
Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: Caffeine-induced psychosis may lead to misdiagnosis, unnecessary treatment, or incarceration of susceptible individuals.
Data Source: Case series of patients in correctional and forensic settings.
Disclosures: The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
Don't Let Friends 'Friend' Patients on Facebook
BOSTON – Before hanging out a shingle on Facebook or other social networking sites, mental health providers should be aware of the pitfalls of TMI – too much information – warned a psychiatrist at the annual meeting of the American Academy of Psychiatry and the Law.
Roughly half of all medical students who posted on Facebook without thought to their privacy settings revealed personal information that did not reflect well on them, including profanity, intoxication, and discriminatory language, and more than a third posted sexually suggestive messages or images, reported Dr. Helen M. Farrell, a staff psychiatrist at Beth Israel Deaconess Medical Center in Boston.
In addition, indiscriminate postings can run afoul of HIPAA rules and leave clinicians liable to malpractice actions, Dr. Farrell cautioned.
Facebook can be useful for marketing a practice, but it can also be a professional and ethical minefield when used improperly, she noted in a poster presentation and an interview.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ the patients or establish any communication with them. They can also block patients from seeing their profiles and that would be recommended," she said.
She quoted a 2009 article in Entertainment Weekly which asked, "How on earth did we stalk our exes, remember our coworkers’ birthdays, bug our friends, and play a rousing game of Scrabulous before Facebook?"
Dr. Farrell did a PubMed search for articles on professionalism and Facebook, and found 12 studies that looked at how medical students and residents used the social medium.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ ... or establish any communication with them."
For example, a survey of Vanderbilt surgery residents and faculty found that 64% of the residents and 22% of the faculty had Facebook pages, and that 31% had publicly accessible sites with work-related comments posted (J. Surg. Educ. 2010;67:381-6). Of those comments, 14% made reference to patient care or to specific patient situations.
In a another study, investigators from the Wellington School of Medicine and Health Sciences in New Zealand, conducted a cross-sectional survey of Facebook use by recent medical graduates (Med. Educ. 2010;44:805-13).
They found that 37% of the 220 graduates who had Facebook accounts had publicly available profiles, more than one-third of which (37%) revealed the poster’s sexual orientation, 46% showed them using alcohol, and 10% showed them being intoxicated.
It’s also unwise for clinicians to accept "friending" requests from patients. The patient may be exposed to possible unprofessional or embarrassing content that could tarnish the doctor-patient relationship, and there are concerns about boundary issues and potential liability, Dr. Farrell said.
The flip side of the Facebook coin is its promotional value, which can be used to market a school’s curriculum and share information about clinical and academic departments, schedules, etc.
In addition, public profiles that patients post can provide clues about their mental states, such as histrionic or narcissistic personality traits, antisocial moods, or behaviors such as the use of hostile language, libel, or cyberbullying.
The way in which patients react to Facebook also might provide clues to their thought processes or content. For example, patients who frequently, repeatedly check their Facebook accounts might have obsessive/compulsive traits, whereas postings by the patient might reveal psychosis or homicidal or suicidal ideation. Postings also may provide clues to patients’ perceptual disturbances, insight, and judgment, Dr. Farrell noted.
She recommends that Facebook users choose the highest privacy settings allowed, and that "e-professionalism" become part of the formal curriculum at professional schools and organizations.
The study was internally funded. Dr. Farrell reported that she had no relevant conflicts of interests.
BOSTON – Before hanging out a shingle on Facebook or other social networking sites, mental health providers should be aware of the pitfalls of TMI – too much information – warned a psychiatrist at the annual meeting of the American Academy of Psychiatry and the Law.
Roughly half of all medical students who posted on Facebook without thought to their privacy settings revealed personal information that did not reflect well on them, including profanity, intoxication, and discriminatory language, and more than a third posted sexually suggestive messages or images, reported Dr. Helen M. Farrell, a staff psychiatrist at Beth Israel Deaconess Medical Center in Boston.
In addition, indiscriminate postings can run afoul of HIPAA rules and leave clinicians liable to malpractice actions, Dr. Farrell cautioned.
Facebook can be useful for marketing a practice, but it can also be a professional and ethical minefield when used improperly, she noted in a poster presentation and an interview.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ the patients or establish any communication with them. They can also block patients from seeing their profiles and that would be recommended," she said.
She quoted a 2009 article in Entertainment Weekly which asked, "How on earth did we stalk our exes, remember our coworkers’ birthdays, bug our friends, and play a rousing game of Scrabulous before Facebook?"
Dr. Farrell did a PubMed search for articles on professionalism and Facebook, and found 12 studies that looked at how medical students and residents used the social medium.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ ... or establish any communication with them."
For example, a survey of Vanderbilt surgery residents and faculty found that 64% of the residents and 22% of the faculty had Facebook pages, and that 31% had publicly accessible sites with work-related comments posted (J. Surg. Educ. 2010;67:381-6). Of those comments, 14% made reference to patient care or to specific patient situations.
In a another study, investigators from the Wellington School of Medicine and Health Sciences in New Zealand, conducted a cross-sectional survey of Facebook use by recent medical graduates (Med. Educ. 2010;44:805-13).
They found that 37% of the 220 graduates who had Facebook accounts had publicly available profiles, more than one-third of which (37%) revealed the poster’s sexual orientation, 46% showed them using alcohol, and 10% showed them being intoxicated.
It’s also unwise for clinicians to accept "friending" requests from patients. The patient may be exposed to possible unprofessional or embarrassing content that could tarnish the doctor-patient relationship, and there are concerns about boundary issues and potential liability, Dr. Farrell said.
The flip side of the Facebook coin is its promotional value, which can be used to market a school’s curriculum and share information about clinical and academic departments, schedules, etc.
In addition, public profiles that patients post can provide clues about their mental states, such as histrionic or narcissistic personality traits, antisocial moods, or behaviors such as the use of hostile language, libel, or cyberbullying.
The way in which patients react to Facebook also might provide clues to their thought processes or content. For example, patients who frequently, repeatedly check their Facebook accounts might have obsessive/compulsive traits, whereas postings by the patient might reveal psychosis or homicidal or suicidal ideation. Postings also may provide clues to patients’ perceptual disturbances, insight, and judgment, Dr. Farrell noted.
She recommends that Facebook users choose the highest privacy settings allowed, and that "e-professionalism" become part of the formal curriculum at professional schools and organizations.
The study was internally funded. Dr. Farrell reported that she had no relevant conflicts of interests.
BOSTON – Before hanging out a shingle on Facebook or other social networking sites, mental health providers should be aware of the pitfalls of TMI – too much information – warned a psychiatrist at the annual meeting of the American Academy of Psychiatry and the Law.
Roughly half of all medical students who posted on Facebook without thought to their privacy settings revealed personal information that did not reflect well on them, including profanity, intoxication, and discriminatory language, and more than a third posted sexually suggestive messages or images, reported Dr. Helen M. Farrell, a staff psychiatrist at Beth Israel Deaconess Medical Center in Boston.
In addition, indiscriminate postings can run afoul of HIPAA rules and leave clinicians liable to malpractice actions, Dr. Farrell cautioned.
Facebook can be useful for marketing a practice, but it can also be a professional and ethical minefield when used improperly, she noted in a poster presentation and an interview.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ the patients or establish any communication with them. They can also block patients from seeing their profiles and that would be recommended," she said.
She quoted a 2009 article in Entertainment Weekly which asked, "How on earth did we stalk our exes, remember our coworkers’ birthdays, bug our friends, and play a rousing game of Scrabulous before Facebook?"
Dr. Farrell did a PubMed search for articles on professionalism and Facebook, and found 12 studies that looked at how medical students and residents used the social medium.
"If psychiatrists are contacted by patients on Facebook, they should not ‘friend’ ... or establish any communication with them."
For example, a survey of Vanderbilt surgery residents and faculty found that 64% of the residents and 22% of the faculty had Facebook pages, and that 31% had publicly accessible sites with work-related comments posted (J. Surg. Educ. 2010;67:381-6). Of those comments, 14% made reference to patient care or to specific patient situations.
In a another study, investigators from the Wellington School of Medicine and Health Sciences in New Zealand, conducted a cross-sectional survey of Facebook use by recent medical graduates (Med. Educ. 2010;44:805-13).
They found that 37% of the 220 graduates who had Facebook accounts had publicly available profiles, more than one-third of which (37%) revealed the poster’s sexual orientation, 46% showed them using alcohol, and 10% showed them being intoxicated.
It’s also unwise for clinicians to accept "friending" requests from patients. The patient may be exposed to possible unprofessional or embarrassing content that could tarnish the doctor-patient relationship, and there are concerns about boundary issues and potential liability, Dr. Farrell said.
The flip side of the Facebook coin is its promotional value, which can be used to market a school’s curriculum and share information about clinical and academic departments, schedules, etc.
In addition, public profiles that patients post can provide clues about their mental states, such as histrionic or narcissistic personality traits, antisocial moods, or behaviors such as the use of hostile language, libel, or cyberbullying.
The way in which patients react to Facebook also might provide clues to their thought processes or content. For example, patients who frequently, repeatedly check their Facebook accounts might have obsessive/compulsive traits, whereas postings by the patient might reveal psychosis or homicidal or suicidal ideation. Postings also may provide clues to patients’ perceptual disturbances, insight, and judgment, Dr. Farrell noted.
She recommends that Facebook users choose the highest privacy settings allowed, and that "e-professionalism" become part of the formal curriculum at professional schools and organizations.
The study was internally funded. Dr. Farrell reported that she had no relevant conflicts of interests.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: Approximately 50% of medical students who post publicly viewable profiles on Facebook publish unprofessional, unflattering, or potentially actionable content.
Data Source: Review of medical literature.
Disclosures: The study was internally funded. Dr. Farrell reported that she had no relevant conflicts of interests.
Lower Radiation Dose Improves Lung Cancer Survival
MIAMI BEACH – Less turned out to be better in a large clinical trial comparing radiation doses in patients treated with radiation and chemotherapy for stage III non–small cell lung cancer, investigators reported here.
The median overall survival rate at 1 year was 81% for patients treated with standard-dose (60 Gy) radiation, compared with 70.4% for those who received the high dose (74 Gy), according to preliminary findings from the radiation-dose arm of the ongoing phase III Radiation Therapy Oncology Group (RTOG) 0617 trial. The respective median survival rates were 21.7 months and 20.7 months (P = .02).
A planned interim analysis from the trial showed that the radiation comparison had crossed the prespecified boundary for futility, and the high-dose arm was stopped in June 2011, reported Dr. Jeffrey Bradley from Washington University in St. Louis at the annual meeting of the American Society for Radiation Oncology.
"I think this changes practice: If [cancer centers] weren’t using 60 Gray before, perhaps they should go back to using 60 Gray, because it does not appear that a higher dose is better," Dr. Bradley commented at the annual meeting of the American Society of Radiation Oncology (ASTRO).
Dr. Tim R. Williams, from the Lynn Cancer Institute at Boca Raton (Fla.) Regional Hospital, the immediate-past chairman of ASTRO, noted that his center has used high-dose radiation in stage III non–small cell lung cancer (NSCLC) patients for about 5 years. Although practice patterns vary, it’s likely that many treatment centers currently use the higher dose, he said.
In RTOG 0617, a total of 500 patients with stage IIIA/IIIB NSCLC were scheduled for randomization to one of four arms in a 2 x 2 factorial design with each patient assigned to receive either 74 Gy or 60 Gy radiation with or without cetuximab (Erbitux), on a background chemotherapy regimen of weekly paclitaxel (45 mg/m2) and carboplatin (titrated to an area-under-the-curve of 2).
The radiation was delivered in 2-Gy fractions over 30-37 fractions.
The analysis was performed on 426 patients who had been enrolled in the study before June 17, 2011.
Seeking to understand why the higher radiation dose was not better – the investigators had originally hypothesized that 74 Gy would result in a 7-month improvement in overall survival vs. 64 Gy – they performed univariate analyses, and found that significant predictors for better outcomes included continuous therapy, nonsquamous histology, and, female gender. In multivariate analysis, radiation dose (60 Gy vs. 74 Gy) was associated with a hazard ratio for overall survival of 1.48 (P = .038), nonsquamous histology versus squamous was associated with an HR of 1.52 (P = .025), and gross or internal tumor volume had a small but significant HR of 1.002 (P = .011).
Dr. Benjamin Movsas, chair of radiation oncology at the Henry Ford Health System in Detroit, the invited discussant, said that "as of 2011, level I evidence demonstrates no role for dose escalation in stage III non–small cell lung cancer."
He noted that although there were small differences between the radiation dose groups in terms of tumor histology, gross tumor volume, and other factors, they were not large enough to explain the differences in outcomes.
Citing the advice of his late father, also a physician, Dr. Movsas reminded the audience that "More is not always better."
The trial is continuing, but with patients assigned to 60 Gy radiation only, with the goal of evaluating the secondary study end point of overall survival of patients with or without cetuximab added to concurrent chemoradiotherapy.
The RTOG 0617 trial is supported by grants from the U.S. National Cancer Institute, with additional support from Bristol-Myers Squibb and ImClone.
Dr. Bradley and Dr. Williams had no disclosures. Dr. Movsas disclosed departmental research support from Varian and Philips. He also has served as a chair of an RTOG committee, but was not involved in the 0617 study.
MIAMI BEACH – Less turned out to be better in a large clinical trial comparing radiation doses in patients treated with radiation and chemotherapy for stage III non–small cell lung cancer, investigators reported here.
The median overall survival rate at 1 year was 81% for patients treated with standard-dose (60 Gy) radiation, compared with 70.4% for those who received the high dose (74 Gy), according to preliminary findings from the radiation-dose arm of the ongoing phase III Radiation Therapy Oncology Group (RTOG) 0617 trial. The respective median survival rates were 21.7 months and 20.7 months (P = .02).
A planned interim analysis from the trial showed that the radiation comparison had crossed the prespecified boundary for futility, and the high-dose arm was stopped in June 2011, reported Dr. Jeffrey Bradley from Washington University in St. Louis at the annual meeting of the American Society for Radiation Oncology.
"I think this changes practice: If [cancer centers] weren’t using 60 Gray before, perhaps they should go back to using 60 Gray, because it does not appear that a higher dose is better," Dr. Bradley commented at the annual meeting of the American Society of Radiation Oncology (ASTRO).
Dr. Tim R. Williams, from the Lynn Cancer Institute at Boca Raton (Fla.) Regional Hospital, the immediate-past chairman of ASTRO, noted that his center has used high-dose radiation in stage III non–small cell lung cancer (NSCLC) patients for about 5 years. Although practice patterns vary, it’s likely that many treatment centers currently use the higher dose, he said.
In RTOG 0617, a total of 500 patients with stage IIIA/IIIB NSCLC were scheduled for randomization to one of four arms in a 2 x 2 factorial design with each patient assigned to receive either 74 Gy or 60 Gy radiation with or without cetuximab (Erbitux), on a background chemotherapy regimen of weekly paclitaxel (45 mg/m2) and carboplatin (titrated to an area-under-the-curve of 2).
The radiation was delivered in 2-Gy fractions over 30-37 fractions.
The analysis was performed on 426 patients who had been enrolled in the study before June 17, 2011.
Seeking to understand why the higher radiation dose was not better – the investigators had originally hypothesized that 74 Gy would result in a 7-month improvement in overall survival vs. 64 Gy – they performed univariate analyses, and found that significant predictors for better outcomes included continuous therapy, nonsquamous histology, and, female gender. In multivariate analysis, radiation dose (60 Gy vs. 74 Gy) was associated with a hazard ratio for overall survival of 1.48 (P = .038), nonsquamous histology versus squamous was associated with an HR of 1.52 (P = .025), and gross or internal tumor volume had a small but significant HR of 1.002 (P = .011).
Dr. Benjamin Movsas, chair of radiation oncology at the Henry Ford Health System in Detroit, the invited discussant, said that "as of 2011, level I evidence demonstrates no role for dose escalation in stage III non–small cell lung cancer."
He noted that although there were small differences between the radiation dose groups in terms of tumor histology, gross tumor volume, and other factors, they were not large enough to explain the differences in outcomes.
Citing the advice of his late father, also a physician, Dr. Movsas reminded the audience that "More is not always better."
The trial is continuing, but with patients assigned to 60 Gy radiation only, with the goal of evaluating the secondary study end point of overall survival of patients with or without cetuximab added to concurrent chemoradiotherapy.
The RTOG 0617 trial is supported by grants from the U.S. National Cancer Institute, with additional support from Bristol-Myers Squibb and ImClone.
Dr. Bradley and Dr. Williams had no disclosures. Dr. Movsas disclosed departmental research support from Varian and Philips. He also has served as a chair of an RTOG committee, but was not involved in the 0617 study.
MIAMI BEACH – Less turned out to be better in a large clinical trial comparing radiation doses in patients treated with radiation and chemotherapy for stage III non–small cell lung cancer, investigators reported here.
The median overall survival rate at 1 year was 81% for patients treated with standard-dose (60 Gy) radiation, compared with 70.4% for those who received the high dose (74 Gy), according to preliminary findings from the radiation-dose arm of the ongoing phase III Radiation Therapy Oncology Group (RTOG) 0617 trial. The respective median survival rates were 21.7 months and 20.7 months (P = .02).
A planned interim analysis from the trial showed that the radiation comparison had crossed the prespecified boundary for futility, and the high-dose arm was stopped in June 2011, reported Dr. Jeffrey Bradley from Washington University in St. Louis at the annual meeting of the American Society for Radiation Oncology.
"I think this changes practice: If [cancer centers] weren’t using 60 Gray before, perhaps they should go back to using 60 Gray, because it does not appear that a higher dose is better," Dr. Bradley commented at the annual meeting of the American Society of Radiation Oncology (ASTRO).
Dr. Tim R. Williams, from the Lynn Cancer Institute at Boca Raton (Fla.) Regional Hospital, the immediate-past chairman of ASTRO, noted that his center has used high-dose radiation in stage III non–small cell lung cancer (NSCLC) patients for about 5 years. Although practice patterns vary, it’s likely that many treatment centers currently use the higher dose, he said.
In RTOG 0617, a total of 500 patients with stage IIIA/IIIB NSCLC were scheduled for randomization to one of four arms in a 2 x 2 factorial design with each patient assigned to receive either 74 Gy or 60 Gy radiation with or without cetuximab (Erbitux), on a background chemotherapy regimen of weekly paclitaxel (45 mg/m2) and carboplatin (titrated to an area-under-the-curve of 2).
The radiation was delivered in 2-Gy fractions over 30-37 fractions.
The analysis was performed on 426 patients who had been enrolled in the study before June 17, 2011.
Seeking to understand why the higher radiation dose was not better – the investigators had originally hypothesized that 74 Gy would result in a 7-month improvement in overall survival vs. 64 Gy – they performed univariate analyses, and found that significant predictors for better outcomes included continuous therapy, nonsquamous histology, and, female gender. In multivariate analysis, radiation dose (60 Gy vs. 74 Gy) was associated with a hazard ratio for overall survival of 1.48 (P = .038), nonsquamous histology versus squamous was associated with an HR of 1.52 (P = .025), and gross or internal tumor volume had a small but significant HR of 1.002 (P = .011).
Dr. Benjamin Movsas, chair of radiation oncology at the Henry Ford Health System in Detroit, the invited discussant, said that "as of 2011, level I evidence demonstrates no role for dose escalation in stage III non–small cell lung cancer."
He noted that although there were small differences between the radiation dose groups in terms of tumor histology, gross tumor volume, and other factors, they were not large enough to explain the differences in outcomes.
Citing the advice of his late father, also a physician, Dr. Movsas reminded the audience that "More is not always better."
The trial is continuing, but with patients assigned to 60 Gy radiation only, with the goal of evaluating the secondary study end point of overall survival of patients with or without cetuximab added to concurrent chemoradiotherapy.
The RTOG 0617 trial is supported by grants from the U.S. National Cancer Institute, with additional support from Bristol-Myers Squibb and ImClone.
Dr. Bradley and Dr. Williams had no disclosures. Dr. Movsas disclosed departmental research support from Varian and Philips. He also has served as a chair of an RTOG committee, but was not involved in the 0617 study.
Major Finding: Median overall survival among patients with stage III NSCLC treated with chemotherapy was 20.7 months with high-dose radiation (74 Gy), vs. 21.7 months with standard-dose radiation (60 Gy; P =.02).
Data Source: 426 patients enrolled in the randomized controlled RTOG 0617 trial.
Disclosures: Dr. Bradley and Dr. Williams had no disclosures. Dr. Movsas disclosed departmental research support from Varian and Philips. He also has served as a chair of an RTOG committee, but was not involved in the 0617 study.
Bullying Victims Suffer Long-Term Depression
BOSTON – Children singled out for abuse either in person or through cyberbullying are more prone to long-term depression, significantly poorer mental and physical health, and suicidal thoughts and actions than their peers who are spared from bullying, said investigators at the annual meeting of the American Academy of Psychiatry and the Law.
Children seen as outsiders by their peers – those with developmental disabilities, mental health problems, and gays or lesbians – are the most common targets of bullies both in the schoolyard and online, said Dr. Eileen P. Ryan from the University of Virginia in Charlottesville.
With cyberbullying – a term that encompasses remote, electronic bullying done on e-mail, role-playing game sites, YouTube, Facebook, and other online venues – the perpetrator doesn’t need to be in the same room or the same town as the victim. In addition, the bully can be physically weaker than his target.
"This is where the little red-headed, freckled, pale child is able to bully the quarterback of the high school football team," said Dr. Bradley Freeman of Vanderbilt University in Nashville, Tenn.
Dr. Ryan cited a definition of bullying by Dan Olweus, Ph.D., a Swedish psychologist and bullying expert: "A person is bullied when he or she is subjected repeatedly and over time to negative action on the part of one or more people."
The U.S. attorney general’s office defines cyberbullying as "use of electronic devices and information such as e-mail instant messaging, text messages, mobile phones, pager, and websites to send or post cruel or harmful messages or images about an individual or group."

Both forms of bullying can have severe mental health consequences for both the victim and the bully, Dr. Ryan said. Although it is widely thought to become less prevalent with age, 20%-30% of 8th through 12th graders have reported frequent involvement in bullying as a victim, bully, or both. A 2001 study from the National Institute for Child Health and Human Development found that nearly 30% of a representative sample of 15,686 6th through 10th graders reported moderate or frequent involvement in bullying: 13% as bullies, 10.6% as victims, and 6.3% as both, with boys more frequently being both the bully and the bullied (JAMA 2001;285:2094-100).
In the Pittsburgh Youth Study, a prospective cohort study of 503 boys followed from ages 6 through 19, being a bully at age 10 was the strongest predictor of delinquency. The study showed that 32.6% of bullies become delinquents, compared with 22.5% of nonbullies. In addition, being a victim at age 19 was the strongest predictor of depression, with 32% of victims having depression, compared with 22.7% of nonvictims, Dr. Ryan said (J. Aggress. Confl. Peace Res. 2011 June 9 [10.1108/17596591111132882]).
A recent meta-analysis from investigators at the University of Cambridge (England), found that the probability of being depressed up to 36 years later was much higher among people who had been bullied at school, compared with nonvictims. The authors also found that the probability of offending up to 11 years later was much higher for school bullies than noninvolved students, she noted (Crim. Behav. Ment. Health 2011;21:80-9).
Girls who bully, even infrequently, appear to be at increased risk for suicide, while among boys, only those who bully frequently are at increased risk.
"Suicidal behavior among male bullies may be a function of psychopathology rather than bullying, per se," Dr. Ryan said.
Equal Opportunity Bullies
Cyberbullies often carry out their abuse anonymously, but according to a 2004 survey of Internet users, 84% of cyberbullies knew their victim in person, and 31% of victims said they knew the bullies.
Cyberbullying increases with age, with males about twice as likely as females to be the electronic bullies (22% to 12%, respectively), Dr. Freeman said. He pointed to a 2007 studywhich found that 38% of cyberbullies said they participated in the activity for fun, 25% for retaliation, and 6% because they felt bad about themselves (J. Adolesc. Health 2007;41[6 suppl. 1]:S1-5).
As with old-fashioned bullying, victims might experience loss of self-esteem, depression, hopelessness, psychosomatic symptoms, or attempted or actual suicide.
Antibullying Legislation

At least 23 states have enacted laws directing school districts to draft policies against bullying, harassment, and intimidation among students; seven states require schools to have disciplinary procedures or consequences, said Dr. Karen Rosenbaum, of New York University.
Many of the laws have been enacted in response to high profile cases of teens who committed suicide after being bullied online and in person.
For example, after the 2010 bullying-induced suicide of Phoebe Prince, a 15-year-old Irish immigrant who had recently enrolled at a high school in South Hadley, Mass., the state of Massachusetts enacted a law that bans bullying on all school grounds, buses, and activities. The law also mandates that every incident be investigated by school officials and reported to the parents of the students involved.
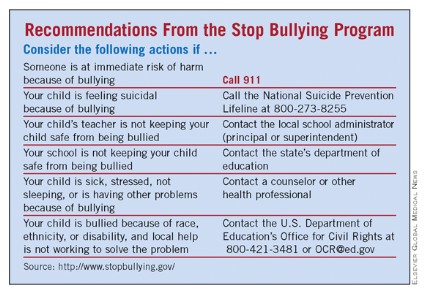
StopBullying.gov, a federal government website, recommends a number of steps to prevent or stop bullying.
The researchers did not disclose funding sources for their studies. Dr. Ryan, Dr. Freeman, and Dr. Rosenbaum each declared that they have no financial conflicts of interest.
BOSTON – Children singled out for abuse either in person or through cyberbullying are more prone to long-term depression, significantly poorer mental and physical health, and suicidal thoughts and actions than their peers who are spared from bullying, said investigators at the annual meeting of the American Academy of Psychiatry and the Law.
Children seen as outsiders by their peers – those with developmental disabilities, mental health problems, and gays or lesbians – are the most common targets of bullies both in the schoolyard and online, said Dr. Eileen P. Ryan from the University of Virginia in Charlottesville.
With cyberbullying – a term that encompasses remote, electronic bullying done on e-mail, role-playing game sites, YouTube, Facebook, and other online venues – the perpetrator doesn’t need to be in the same room or the same town as the victim. In addition, the bully can be physically weaker than his target.
"This is where the little red-headed, freckled, pale child is able to bully the quarterback of the high school football team," said Dr. Bradley Freeman of Vanderbilt University in Nashville, Tenn.
Dr. Ryan cited a definition of bullying by Dan Olweus, Ph.D., a Swedish psychologist and bullying expert: "A person is bullied when he or she is subjected repeatedly and over time to negative action on the part of one or more people."
The U.S. attorney general’s office defines cyberbullying as "use of electronic devices and information such as e-mail instant messaging, text messages, mobile phones, pager, and websites to send or post cruel or harmful messages or images about an individual or group."
Both forms of bullying can have severe mental health consequences for both the victim and the bully, Dr. Ryan said. Although it is widely thought to become less prevalent with age, 20%-30% of 8th through 12th graders have reported frequent involvement in bullying as a victim, bully, or both. A 2001 study from the National Institute for Child Health and Human Development found that nearly 30% of a representative sample of 15,686 6th through 10th graders reported moderate or frequent involvement in bullying: 13% as bullies, 10.6% as victims, and 6.3% as both, with boys more frequently being both the bully and the bullied (JAMA 2001;285:2094-100).
In the Pittsburgh Youth Study, a prospective cohort study of 503 boys followed from ages 6 through 19, being a bully at age 10 was the strongest predictor of delinquency. The study showed that 32.6% of bullies become delinquents, compared with 22.5% of nonbullies. In addition, being a victim at age 19 was the strongest predictor of depression, with 32% of victims having depression, compared with 22.7% of nonvictims, Dr. Ryan said (J. Aggress. Confl. Peace Res. 2011 June 9 [10.1108/17596591111132882]).
A recent meta-analysis from investigators at the University of Cambridge (England), found that the probability of being depressed up to 36 years later was much higher among people who had been bullied at school, compared with nonvictims. The authors also found that the probability of offending up to 11 years later was much higher for school bullies than noninvolved students, she noted (Crim. Behav. Ment. Health 2011;21:80-9).
Girls who bully, even infrequently, appear to be at increased risk for suicide, while among boys, only those who bully frequently are at increased risk.
"Suicidal behavior among male bullies may be a function of psychopathology rather than bullying, per se," Dr. Ryan said.
Equal Opportunity Bullies
Cyberbullies often carry out their abuse anonymously, but according to a 2004 survey of Internet users, 84% of cyberbullies knew their victim in person, and 31% of victims said they knew the bullies.
Cyberbullying increases with age, with males about twice as likely as females to be the electronic bullies (22% to 12%, respectively), Dr. Freeman said. He pointed to a 2007 studywhich found that 38% of cyberbullies said they participated in the activity for fun, 25% for retaliation, and 6% because they felt bad about themselves (J. Adolesc. Health 2007;41[6 suppl. 1]:S1-5).
As with old-fashioned bullying, victims might experience loss of self-esteem, depression, hopelessness, psychosomatic symptoms, or attempted or actual suicide.
Antibullying Legislation
At least 23 states have enacted laws directing school districts to draft policies against bullying, harassment, and intimidation among students; seven states require schools to have disciplinary procedures or consequences, said Dr. Karen Rosenbaum, of New York University.
Many of the laws have been enacted in response to high profile cases of teens who committed suicide after being bullied online and in person.
For example, after the 2010 bullying-induced suicide of Phoebe Prince, a 15-year-old Irish immigrant who had recently enrolled at a high school in South Hadley, Mass., the state of Massachusetts enacted a law that bans bullying on all school grounds, buses, and activities. The law also mandates that every incident be investigated by school officials and reported to the parents of the students involved.
StopBullying.gov, a federal government website, recommends a number of steps to prevent or stop bullying.
The researchers did not disclose funding sources for their studies. Dr. Ryan, Dr. Freeman, and Dr. Rosenbaum each declared that they have no financial conflicts of interest.
BOSTON – Children singled out for abuse either in person or through cyberbullying are more prone to long-term depression, significantly poorer mental and physical health, and suicidal thoughts and actions than their peers who are spared from bullying, said investigators at the annual meeting of the American Academy of Psychiatry and the Law.
Children seen as outsiders by their peers – those with developmental disabilities, mental health problems, and gays or lesbians – are the most common targets of bullies both in the schoolyard and online, said Dr. Eileen P. Ryan from the University of Virginia in Charlottesville.
With cyberbullying – a term that encompasses remote, electronic bullying done on e-mail, role-playing game sites, YouTube, Facebook, and other online venues – the perpetrator doesn’t need to be in the same room or the same town as the victim. In addition, the bully can be physically weaker than his target.
"This is where the little red-headed, freckled, pale child is able to bully the quarterback of the high school football team," said Dr. Bradley Freeman of Vanderbilt University in Nashville, Tenn.
Dr. Ryan cited a definition of bullying by Dan Olweus, Ph.D., a Swedish psychologist and bullying expert: "A person is bullied when he or she is subjected repeatedly and over time to negative action on the part of one or more people."
The U.S. attorney general’s office defines cyberbullying as "use of electronic devices and information such as e-mail instant messaging, text messages, mobile phones, pager, and websites to send or post cruel or harmful messages or images about an individual or group."
Both forms of bullying can have severe mental health consequences for both the victim and the bully, Dr. Ryan said. Although it is widely thought to become less prevalent with age, 20%-30% of 8th through 12th graders have reported frequent involvement in bullying as a victim, bully, or both. A 2001 study from the National Institute for Child Health and Human Development found that nearly 30% of a representative sample of 15,686 6th through 10th graders reported moderate or frequent involvement in bullying: 13% as bullies, 10.6% as victims, and 6.3% as both, with boys more frequently being both the bully and the bullied (JAMA 2001;285:2094-100).
In the Pittsburgh Youth Study, a prospective cohort study of 503 boys followed from ages 6 through 19, being a bully at age 10 was the strongest predictor of delinquency. The study showed that 32.6% of bullies become delinquents, compared with 22.5% of nonbullies. In addition, being a victim at age 19 was the strongest predictor of depression, with 32% of victims having depression, compared with 22.7% of nonvictims, Dr. Ryan said (J. Aggress. Confl. Peace Res. 2011 June 9 [10.1108/17596591111132882]).
A recent meta-analysis from investigators at the University of Cambridge (England), found that the probability of being depressed up to 36 years later was much higher among people who had been bullied at school, compared with nonvictims. The authors also found that the probability of offending up to 11 years later was much higher for school bullies than noninvolved students, she noted (Crim. Behav. Ment. Health 2011;21:80-9).
Girls who bully, even infrequently, appear to be at increased risk for suicide, while among boys, only those who bully frequently are at increased risk.
"Suicidal behavior among male bullies may be a function of psychopathology rather than bullying, per se," Dr. Ryan said.
Equal Opportunity Bullies
Cyberbullies often carry out their abuse anonymously, but according to a 2004 survey of Internet users, 84% of cyberbullies knew their victim in person, and 31% of victims said they knew the bullies.
Cyberbullying increases with age, with males about twice as likely as females to be the electronic bullies (22% to 12%, respectively), Dr. Freeman said. He pointed to a 2007 studywhich found that 38% of cyberbullies said they participated in the activity for fun, 25% for retaliation, and 6% because they felt bad about themselves (J. Adolesc. Health 2007;41[6 suppl. 1]:S1-5).
As with old-fashioned bullying, victims might experience loss of self-esteem, depression, hopelessness, psychosomatic symptoms, or attempted or actual suicide.
Antibullying Legislation
At least 23 states have enacted laws directing school districts to draft policies against bullying, harassment, and intimidation among students; seven states require schools to have disciplinary procedures or consequences, said Dr. Karen Rosenbaum, of New York University.
Many of the laws have been enacted in response to high profile cases of teens who committed suicide after being bullied online and in person.
For example, after the 2010 bullying-induced suicide of Phoebe Prince, a 15-year-old Irish immigrant who had recently enrolled at a high school in South Hadley, Mass., the state of Massachusetts enacted a law that bans bullying on all school grounds, buses, and activities. The law also mandates that every incident be investigated by school officials and reported to the parents of the students involved.
StopBullying.gov, a federal government website, recommends a number of steps to prevent or stop bullying.
The researchers did not disclose funding sources for their studies. Dr. Ryan, Dr. Freeman, and Dr. Rosenbaum each declared that they have no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Study Finds Fault With Sex-Offender Restriction Laws
BOSTON – Laws intended to keep convicted sex offenders far away from schools, playgrounds, shopping malls, and other places where children might gather don’t appear to work or aren’t being vigorously enforced in parts of the United States. And when the laws are adhered to, they often keep offenders far away from needed psychiatric services, job prospects, and social support, researchers said at the annual meeting of the American Academy of Psychiatry and the Law.
In Buffalo, N.Y., sex offenders are legally barred from living in all but 6.5% of the city’s total area, but more than 90% of sex offenders in the county live within that city’s limits, said Dr. Jacqueline A. Berenson, a forensic psychiatrist in private practice in New York City.

"One of the conclusions that has come from a number of studies is that the legislation is not only not helping with the recidivism rate of sex offenders in the community, but may actually be worsening recidivism rates, and that the collateral damage being done by this legislation nationally is self-defeating," she said.
Residence restriction laws vary considerably in their components (who is an offender, where can’t they live, how far they must stay away), and in terms of complexity and ambiguity of the statutes, which vary in their definition, measurement of distance, and enforcement, Dr. Berenson noted.
For example, in Erie County, N.Y., alone, rules vary from one municipality to the next. In the city of Lackawanna, level 3 registered sex offenders or any registered offender over the age of 17 convicted of an offense (including statutory rape) upon a child age 16 or under is forbidden from living within 2,000 feet of any school, park, playground, athletic field, or day care center. In contrast, the Town of Evans and the Village of Sloan set a 1,500-foot boundary, with Sloan bylaws adding teen/community centers, dance halls, and skating rinks to exclusion zones. The law does not specify what constitutes a "teen/community center" or "dance hall."
Such laws, Dr. Berenson said, often force offenders to live in more rural areas where they might not have community or social support or access to services, or to violate the laws by living within an off-limits area and risk parole violation, rearrest, and imprisonment.
"Do they understand what the legislation means? Do their parole officers understand? And if they don’t understand, does that make them not culpable if they’re living in a restricted area? And the answer to that is ‘No’; if they’re living in a restricted area, the potential for being arrested and charged with a felony is real," she said.
A researcher who also studies housing issues of sex offenders, Andrew J. Harris, Ph.D., from the University of Massachusetts Lowell, cited the example of Miami-Dade County, Fla., where sex offenders were living in a makeshift encampment under a bridge on the Julia Tuttle Causeway, the only place they could find that didn’t violate that county’s residence restrictions. Some offenders even received state-issued IDs listing the causeway as their place of residence.
Mapping Offenders
Dr. Berenson reported results of a study that she and Dr. Paul S. Appelbaum of Columbia University, New York, conducted on the effect of residence statutes on the availability of residences for registered sex offenders in both urban and rural areas of Erie and Schenectady counties in New York.
They collected parcel data from the New York State Department of Cyber Security and the Schenectady County geographic information services department, and created overlay maps showing restricted locations according to statute, and residential locations of registered sex offenders.
Although they expected to find that most offenders were living in rural areas, where schools and playgrounds are more widely dispersed, they found that the opposite was true. In Erie County, 90% of offenders were living in restricted areas, and nearly all were within the city limits of Buffalo (91% of the city dwellers were living in restricted areas of Buffalo). Similarly, 90% of offenders in Schenectady County were living in restricted zones, and 100% of offenders living within the City of Schenectady were doing so afoul of the law.
In both counties, only a small percentage of rural residences were in restricted zones, whereas the large majority of multiple family residences or apartments, more commonly found in urban areas, were not legally available to offenders.
The implications of these findings, Dr. Berenson said, are that there may be inadequate resources or an unwillingness on the part of law enforcement agencies to follow the restriction statutes. She noted that courts have overturned sex offender residency laws in eight New York counties, and that the Washington County board of supervisors recently voted to repeal that county’s law.
"Policy makers should be pulling out the [geographic information services] software themselves and asking, ‘What is the actual impact of this legislation? What’s going to happen? Where are these guys going to go?’ " Dr. Harris said. "Housing is a matter of managing this inherent risk that people have for public safety and minimizing the collateral risk."
Dr. Berenson’s study was internally funded. Dr. Berenson and Dr. Harris reported that they had no relevant financial disclosures.
BOSTON – Laws intended to keep convicted sex offenders far away from schools, playgrounds, shopping malls, and other places where children might gather don’t appear to work or aren’t being vigorously enforced in parts of the United States. And when the laws are adhered to, they often keep offenders far away from needed psychiatric services, job prospects, and social support, researchers said at the annual meeting of the American Academy of Psychiatry and the Law.
In Buffalo, N.Y., sex offenders are legally barred from living in all but 6.5% of the city’s total area, but more than 90% of sex offenders in the county live within that city’s limits, said Dr. Jacqueline A. Berenson, a forensic psychiatrist in private practice in New York City.
"One of the conclusions that has come from a number of studies is that the legislation is not only not helping with the recidivism rate of sex offenders in the community, but may actually be worsening recidivism rates, and that the collateral damage being done by this legislation nationally is self-defeating," she said.
Residence restriction laws vary considerably in their components (who is an offender, where can’t they live, how far they must stay away), and in terms of complexity and ambiguity of the statutes, which vary in their definition, measurement of distance, and enforcement, Dr. Berenson noted.
For example, in Erie County, N.Y., alone, rules vary from one municipality to the next. In the city of Lackawanna, level 3 registered sex offenders or any registered offender over the age of 17 convicted of an offense (including statutory rape) upon a child age 16 or under is forbidden from living within 2,000 feet of any school, park, playground, athletic field, or day care center. In contrast, the Town of Evans and the Village of Sloan set a 1,500-foot boundary, with Sloan bylaws adding teen/community centers, dance halls, and skating rinks to exclusion zones. The law does not specify what constitutes a "teen/community center" or "dance hall."
Such laws, Dr. Berenson said, often force offenders to live in more rural areas where they might not have community or social support or access to services, or to violate the laws by living within an off-limits area and risk parole violation, rearrest, and imprisonment.
"Do they understand what the legislation means? Do their parole officers understand? And if they don’t understand, does that make them not culpable if they’re living in a restricted area? And the answer to that is ‘No’; if they’re living in a restricted area, the potential for being arrested and charged with a felony is real," she said.
A researcher who also studies housing issues of sex offenders, Andrew J. Harris, Ph.D., from the University of Massachusetts Lowell, cited the example of Miami-Dade County, Fla., where sex offenders were living in a makeshift encampment under a bridge on the Julia Tuttle Causeway, the only place they could find that didn’t violate that county’s residence restrictions. Some offenders even received state-issued IDs listing the causeway as their place of residence.
Mapping Offenders
Dr. Berenson reported results of a study that she and Dr. Paul S. Appelbaum of Columbia University, New York, conducted on the effect of residence statutes on the availability of residences for registered sex offenders in both urban and rural areas of Erie and Schenectady counties in New York.
They collected parcel data from the New York State Department of Cyber Security and the Schenectady County geographic information services department, and created overlay maps showing restricted locations according to statute, and residential locations of registered sex offenders.
Although they expected to find that most offenders were living in rural areas, where schools and playgrounds are more widely dispersed, they found that the opposite was true. In Erie County, 90% of offenders were living in restricted areas, and nearly all were within the city limits of Buffalo (91% of the city dwellers were living in restricted areas of Buffalo). Similarly, 90% of offenders in Schenectady County were living in restricted zones, and 100% of offenders living within the City of Schenectady were doing so afoul of the law.
In both counties, only a small percentage of rural residences were in restricted zones, whereas the large majority of multiple family residences or apartments, more commonly found in urban areas, were not legally available to offenders.
The implications of these findings, Dr. Berenson said, are that there may be inadequate resources or an unwillingness on the part of law enforcement agencies to follow the restriction statutes. She noted that courts have overturned sex offender residency laws in eight New York counties, and that the Washington County board of supervisors recently voted to repeal that county’s law.
"Policy makers should be pulling out the [geographic information services] software themselves and asking, ‘What is the actual impact of this legislation? What’s going to happen? Where are these guys going to go?’ " Dr. Harris said. "Housing is a matter of managing this inherent risk that people have for public safety and minimizing the collateral risk."
Dr. Berenson’s study was internally funded. Dr. Berenson and Dr. Harris reported that they had no relevant financial disclosures.
BOSTON – Laws intended to keep convicted sex offenders far away from schools, playgrounds, shopping malls, and other places where children might gather don’t appear to work or aren’t being vigorously enforced in parts of the United States. And when the laws are adhered to, they often keep offenders far away from needed psychiatric services, job prospects, and social support, researchers said at the annual meeting of the American Academy of Psychiatry and the Law.
In Buffalo, N.Y., sex offenders are legally barred from living in all but 6.5% of the city’s total area, but more than 90% of sex offenders in the county live within that city’s limits, said Dr. Jacqueline A. Berenson, a forensic psychiatrist in private practice in New York City.
"One of the conclusions that has come from a number of studies is that the legislation is not only not helping with the recidivism rate of sex offenders in the community, but may actually be worsening recidivism rates, and that the collateral damage being done by this legislation nationally is self-defeating," she said.
Residence restriction laws vary considerably in their components (who is an offender, where can’t they live, how far they must stay away), and in terms of complexity and ambiguity of the statutes, which vary in their definition, measurement of distance, and enforcement, Dr. Berenson noted.
For example, in Erie County, N.Y., alone, rules vary from one municipality to the next. In the city of Lackawanna, level 3 registered sex offenders or any registered offender over the age of 17 convicted of an offense (including statutory rape) upon a child age 16 or under is forbidden from living within 2,000 feet of any school, park, playground, athletic field, or day care center. In contrast, the Town of Evans and the Village of Sloan set a 1,500-foot boundary, with Sloan bylaws adding teen/community centers, dance halls, and skating rinks to exclusion zones. The law does not specify what constitutes a "teen/community center" or "dance hall."
Such laws, Dr. Berenson said, often force offenders to live in more rural areas where they might not have community or social support or access to services, or to violate the laws by living within an off-limits area and risk parole violation, rearrest, and imprisonment.
"Do they understand what the legislation means? Do their parole officers understand? And if they don’t understand, does that make them not culpable if they’re living in a restricted area? And the answer to that is ‘No’; if they’re living in a restricted area, the potential for being arrested and charged with a felony is real," she said.
A researcher who also studies housing issues of sex offenders, Andrew J. Harris, Ph.D., from the University of Massachusetts Lowell, cited the example of Miami-Dade County, Fla., where sex offenders were living in a makeshift encampment under a bridge on the Julia Tuttle Causeway, the only place they could find that didn’t violate that county’s residence restrictions. Some offenders even received state-issued IDs listing the causeway as their place of residence.
Mapping Offenders
Dr. Berenson reported results of a study that she and Dr. Paul S. Appelbaum of Columbia University, New York, conducted on the effect of residence statutes on the availability of residences for registered sex offenders in both urban and rural areas of Erie and Schenectady counties in New York.
They collected parcel data from the New York State Department of Cyber Security and the Schenectady County geographic information services department, and created overlay maps showing restricted locations according to statute, and residential locations of registered sex offenders.
Although they expected to find that most offenders were living in rural areas, where schools and playgrounds are more widely dispersed, they found that the opposite was true. In Erie County, 90% of offenders were living in restricted areas, and nearly all were within the city limits of Buffalo (91% of the city dwellers were living in restricted areas of Buffalo). Similarly, 90% of offenders in Schenectady County were living in restricted zones, and 100% of offenders living within the City of Schenectady were doing so afoul of the law.
In both counties, only a small percentage of rural residences were in restricted zones, whereas the large majority of multiple family residences or apartments, more commonly found in urban areas, were not legally available to offenders.
The implications of these findings, Dr. Berenson said, are that there may be inadequate resources or an unwillingness on the part of law enforcement agencies to follow the restriction statutes. She noted that courts have overturned sex offender residency laws in eight New York counties, and that the Washington County board of supervisors recently voted to repeal that county’s law.
"Policy makers should be pulling out the [geographic information services] software themselves and asking, ‘What is the actual impact of this legislation? What’s going to happen? Where are these guys going to go?’ " Dr. Harris said. "Housing is a matter of managing this inherent risk that people have for public safety and minimizing the collateral risk."
Dr. Berenson’s study was internally funded. Dr. Berenson and Dr. Harris reported that they had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: In Erie County, N.Y., 90% of registered sex offenders were living in restricted areas (for example, near a school or park), and nearly all were within the city limits of Buffalo; 91% of those living in that city resided in restricted areas.
Data Source: Single-center study of geographic and demographic data.
Disclosures: Dr. Berenson’s study was internally funded. Dr. Berenson and Dr. Harris reported that they had no relevant financial disclosures.
Quetiapine Abuse Common in Prison Populations
BOSTON – Quetiapine might be a drug of choice among substance abusers behind bars, said researchers at the annual meeting of the American Academy of Psychiatry and the Law.
An atypical antipsychotic with potent sedative and anxiolytic properties, quetiapine (Seroquel) is, along with olanzapine (Zyprexa), one of only two agents in its class to have a "street value," said Dr. Amanda Pearce Roper and Dr. Leonard Mulbry Jr., from the Medical University of South Carolina, Charleston.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it," Dr. Mulbry said in an interview.
He said he also has heard anecdotal reports of quetiapine misuse and abuse in the community but has seen little in the way of evidence to support it.
"We had seen so much desire for it in the correctional system, but then when we did the literature search, there was virtually nothing there," he said.
Quetiapine is an antagonist of dopamine, serotonin, and adrenergic receptors, and it is a potent antihistamine with only negligible anticholinergic effects. It strongly binds serotonin receptors but is rapidly dissociated from D2 receptors, which minimizes its effects on the nigrostriatal and tuberoinfundibular pathways, said Dr. Roper.
Stopping the drug abruptly can lead to withdrawal symptoms because of compensatory changes in the aforementioned receptors. The British National formulary recommends that patients on quetiapine be gradually withdrawn from the drug to avoid withdrawal symptoms, Dr. Roper noted.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it."
The drug is approved by the Food and Drug Administration for the treatment of bipolar affective disorder in the depressed phase and in mania maintenance, schizophrenia, and as an adjunct to treatment for major depressive disorder.
"Its impact on these symptoms may explain why its misuse is so widespread institutionally and on the street," Dr. Roper commented.
She pointed to a 2004 report that found that about 30% of inmates in the Los Angeles County Jail faked symptoms in order to obtain quetiapine, and that many of the malingerers were substance abusers who would snort the crushed tablets (Am. J. Psychiatry 2004;161:1718).
Other observers reported inmates or patients intravenously injecting crushed tablets or inserting them into the rectum (Am. J. Psychiatry 2005;162:1755-6; Pain Med. 2007;8:171-83).
"We have also gotten anecdotal reports of people using quetiapine on the outside and mixing it with other drugs, particularly cocaine," Dr. Mulbry said.
Dr. Roper noted that several correctional facilities have reported either removing quetiapine from their formulary or restricting its access in attempts to reduce abuse of the drug.
For example, the Santa Rita, Calif., jail removed quetiapine and several other drugs from its formulary out of concerns about abuse. The result was a drop in both medication abuse case reports and the cost of psychotropic agents for the jail, as well as a stabilizing of overall medication costs.
The prescribing information for quetiapine extended-release formulation states in part that "patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of misuse or abuse of SEROQUEL, e.g., development of tolerance, increases in dose, drug-seeking behavior."
The study was internally funded. Dr. Mulbry and Dr. Roper each reported that they had no relevant financial disclosures.
BOSTON – Quetiapine might be a drug of choice among substance abusers behind bars, said researchers at the annual meeting of the American Academy of Psychiatry and the Law.
An atypical antipsychotic with potent sedative and anxiolytic properties, quetiapine (Seroquel) is, along with olanzapine (Zyprexa), one of only two agents in its class to have a "street value," said Dr. Amanda Pearce Roper and Dr. Leonard Mulbry Jr., from the Medical University of South Carolina, Charleston.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it," Dr. Mulbry said in an interview.
He said he also has heard anecdotal reports of quetiapine misuse and abuse in the community but has seen little in the way of evidence to support it.
"We had seen so much desire for it in the correctional system, but then when we did the literature search, there was virtually nothing there," he said.
Quetiapine is an antagonist of dopamine, serotonin, and adrenergic receptors, and it is a potent antihistamine with only negligible anticholinergic effects. It strongly binds serotonin receptors but is rapidly dissociated from D2 receptors, which minimizes its effects on the nigrostriatal and tuberoinfundibular pathways, said Dr. Roper.
Stopping the drug abruptly can lead to withdrawal symptoms because of compensatory changes in the aforementioned receptors. The British National formulary recommends that patients on quetiapine be gradually withdrawn from the drug to avoid withdrawal symptoms, Dr. Roper noted.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it."
The drug is approved by the Food and Drug Administration for the treatment of bipolar affective disorder in the depressed phase and in mania maintenance, schizophrenia, and as an adjunct to treatment for major depressive disorder.
"Its impact on these symptoms may explain why its misuse is so widespread institutionally and on the street," Dr. Roper commented.
She pointed to a 2004 report that found that about 30% of inmates in the Los Angeles County Jail faked symptoms in order to obtain quetiapine, and that many of the malingerers were substance abusers who would snort the crushed tablets (Am. J. Psychiatry 2004;161:1718).
Other observers reported inmates or patients intravenously injecting crushed tablets or inserting them into the rectum (Am. J. Psychiatry 2005;162:1755-6; Pain Med. 2007;8:171-83).
"We have also gotten anecdotal reports of people using quetiapine on the outside and mixing it with other drugs, particularly cocaine," Dr. Mulbry said.
Dr. Roper noted that several correctional facilities have reported either removing quetiapine from their formulary or restricting its access in attempts to reduce abuse of the drug.
For example, the Santa Rita, Calif., jail removed quetiapine and several other drugs from its formulary out of concerns about abuse. The result was a drop in both medication abuse case reports and the cost of psychotropic agents for the jail, as well as a stabilizing of overall medication costs.
The prescribing information for quetiapine extended-release formulation states in part that "patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of misuse or abuse of SEROQUEL, e.g., development of tolerance, increases in dose, drug-seeking behavior."
The study was internally funded. Dr. Mulbry and Dr. Roper each reported that they had no relevant financial disclosures.
BOSTON – Quetiapine might be a drug of choice among substance abusers behind bars, said researchers at the annual meeting of the American Academy of Psychiatry and the Law.
An atypical antipsychotic with potent sedative and anxiolytic properties, quetiapine (Seroquel) is, along with olanzapine (Zyprexa), one of only two agents in its class to have a "street value," said Dr. Amanda Pearce Roper and Dr. Leonard Mulbry Jr., from the Medical University of South Carolina, Charleston.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it," Dr. Mulbry said in an interview.
He said he also has heard anecdotal reports of quetiapine misuse and abuse in the community but has seen little in the way of evidence to support it.
"We had seen so much desire for it in the correctional system, but then when we did the literature search, there was virtually nothing there," he said.
Quetiapine is an antagonist of dopamine, serotonin, and adrenergic receptors, and it is a potent antihistamine with only negligible anticholinergic effects. It strongly binds serotonin receptors but is rapidly dissociated from D2 receptors, which minimizes its effects on the nigrostriatal and tuberoinfundibular pathways, said Dr. Roper.
Stopping the drug abruptly can lead to withdrawal symptoms because of compensatory changes in the aforementioned receptors. The British National formulary recommends that patients on quetiapine be gradually withdrawn from the drug to avoid withdrawal symptoms, Dr. Roper noted.
"In any given institution where Seroquel is available, there will be hundreds of guys trying to get it."
The drug is approved by the Food and Drug Administration for the treatment of bipolar affective disorder in the depressed phase and in mania maintenance, schizophrenia, and as an adjunct to treatment for major depressive disorder.
"Its impact on these symptoms may explain why its misuse is so widespread institutionally and on the street," Dr. Roper commented.
She pointed to a 2004 report that found that about 30% of inmates in the Los Angeles County Jail faked symptoms in order to obtain quetiapine, and that many of the malingerers were substance abusers who would snort the crushed tablets (Am. J. Psychiatry 2004;161:1718).
Other observers reported inmates or patients intravenously injecting crushed tablets or inserting them into the rectum (Am. J. Psychiatry 2005;162:1755-6; Pain Med. 2007;8:171-83).
"We have also gotten anecdotal reports of people using quetiapine on the outside and mixing it with other drugs, particularly cocaine," Dr. Mulbry said.
Dr. Roper noted that several correctional facilities have reported either removing quetiapine from their formulary or restricting its access in attempts to reduce abuse of the drug.
For example, the Santa Rita, Calif., jail removed quetiapine and several other drugs from its formulary out of concerns about abuse. The result was a drop in both medication abuse case reports and the cost of psychotropic agents for the jail, as well as a stabilizing of overall medication costs.
The prescribing information for quetiapine extended-release formulation states in part that "patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of misuse or abuse of SEROQUEL, e.g., development of tolerance, increases in dose, drug-seeking behavior."
The study was internally funded. Dr. Mulbry and Dr. Roper each reported that they had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: An estimated 30% of inmates in the Los Angeles County Jail malingered to obtain quetiapine; many of the malingerers were substance abusers who would snort the crushed tablets.
Data Source: Review of case reports from the medical literature.
Disclosures: The study was internally funded. Dr. Mulbry and Dr. Roper each reported that they had no relevant financial disclosures.
Does H. pylori Impair Glucose Tolerance?
Major Finding: Helicobacter pylori infection was associated with a hazard ratio of 2.69 for diabetes among Latinos older than 60 years.
Data Source: Epidemiologic studies examining the relationship between H. pylori infections, glycated hemoglobin levels, and diabetes.
Disclosures: Dr. Jeon's study was supported by grants from the National Institutes of Health. Dr. Chen did not disclose a funding source. Both investigators reported that they had no relevant financial disclosures.
BOSTON – Already convicted for its role in causing peptic ulcers, Helicobacter pylori is also being indicted as a possible co-conspirator in the development of diabetes, investigators from two separate studies said at the meeting.
In a study of nearly 1,800 older Latinos in California, H. pylori infection was associated with a more than twofold greater risk for diabetes, reported Dr. Christine Y. Jeon of the Columbia University School of Nursing, New York.
In addition, a separate study of National Health and Nutrition Examination Survey (NHANES) data found that, after excluding for diabetes and controlling for other risk factors, H. pylori seropositivity was positively associated with hemoglobin A1c levels – suggesting that the bacterium may play a role in impaired glucose tolerance, said Dr. Yu Chen of New York University Langone Medical Center, New York.
Dr. Jeon noted that, although the mechanism for the association between H. pylori infection and diabetes is unknown, it does not appear to be mediated by either the inflammatory pathway or insulin resistance.
“This highlights the need for future studies on how the timing and severity of H. pylori infection affect glucose control in younger individuals, and how H. pylori alters gut microbiota and subsequent host gene expression and energy uptake,” she said.
Dr. Jeon and her colleagues conducted a study to examine whether risk of diabetes changes with various common chronic infections, including herpes simplex virus 1, varicella virus, cytomegalovirus, Toxoplasma gondii, and H. pylori.
The study and its focus on H. pylori in particular were motivated in part by observation of a racial gradient in both diabetes prevalence and H. pylori infection in the United States, with Mexican Americans having a higher prevalence of both than either whites or non-Hispanic blacks.
Additionally, studies have found evidence of association between periodontal bacteria and increased diabetes risk, as well as links between decreased insulin sensitivity and higher antibody titers to herpes simplex virus 2 and Chlamydia pneumoniae.
Other studies, however, have not shown an association between common infections and insulin resistance or diabetes.
Dr. Jeon and colleagues analyzed data on 1,789 men and women older than 60 years who were enrolled in the Sacramento Area Latino Study on Aging (SALSA). Of that group, 782 people did not have diabetes and had available baseline pathogen data.
During the 10-year study, 144 of those 782 people developed diabetes (18% incidence rate), with diabetes defined as self-report of a physician's diagnosis of diabetes or of taking hypoglycemic medication, including insulin, at semiannual interviews; fasting glucose of at least 126 mg/dL at four follow-up visits; or death certificate inclusion of diabetes as a cause of death.
In bivariate analysis adjusted for gender and education, none of the pathogens reached statistical significance for an association with diabetes.
In multivariate analysis, however, the only significant association seen with diabetes was H. pylori (hazard ratio, 2.69). The association was stronger than that for either vascular disease (HR, 1.78) or being a former smoker (HR of 1.34 in bivariate analysis).
Possible explanations for the association include H. pylori–induced alterations in gut microbiota, changes in nutrient metabolism in the gut, increased energy harvesting, or altered host gene expression, Dr. Jeon said.
In the second study, Dr. Chen and her colleague Dr. Martin Blaser looked at data from NHANES III (1988-1994) and IV (1999-2004).
In NHANES III, they found a positive association between H. pylori infection and HbA1c in the overall cohort and in people with body mass indexes (BMIs) both below 25 and 25 and higher (P for interaction for each comparison less than .01).
They also saw a synergistic interaction between H. pylori and higher levels of BMI in both NHANES III and IV (P for interaction less than .01), suggesting that H. pylori exacerbated the rise in HbA1c often seen with weight increase.
In addition, in NHANES III but not NHANES IV, the synergistic effect was seen among patients seropositive for the cagA strain of H. pylori, which has been associated with virulence.
The investigators did not, however, find an association between self-reported diabetes and H. pylori infection.
{kind=link}
The H. pylori association was stronger than that for either vascular disease or being a former smoker.
Source DR. JEON
{kind=link}
H. pylori was associated with diabetes and increased HbA1c in two separate investigations. A mechanism to explain the curious finding is unknown.
Source ©3drenderings/Fotolia.com
Major Finding: Helicobacter pylori infection was associated with a hazard ratio of 2.69 for diabetes among Latinos older than 60 years.
Data Source: Epidemiologic studies examining the relationship between H. pylori infections, glycated hemoglobin levels, and diabetes.
Disclosures: Dr. Jeon's study was supported by grants from the National Institutes of Health. Dr. Chen did not disclose a funding source. Both investigators reported that they had no relevant financial disclosures.
BOSTON – Already convicted for its role in causing peptic ulcers, Helicobacter pylori is also being indicted as a possible co-conspirator in the development of diabetes, investigators from two separate studies said at the meeting.
In a study of nearly 1,800 older Latinos in California, H. pylori infection was associated with a more than twofold greater risk for diabetes, reported Dr. Christine Y. Jeon of the Columbia University School of Nursing, New York.
In addition, a separate study of National Health and Nutrition Examination Survey (NHANES) data found that, after excluding for diabetes and controlling for other risk factors, H. pylori seropositivity was positively associated with hemoglobin A1c levels – suggesting that the bacterium may play a role in impaired glucose tolerance, said Dr. Yu Chen of New York University Langone Medical Center, New York.
Dr. Jeon noted that, although the mechanism for the association between H. pylori infection and diabetes is unknown, it does not appear to be mediated by either the inflammatory pathway or insulin resistance.
“This highlights the need for future studies on how the timing and severity of H. pylori infection affect glucose control in younger individuals, and how H. pylori alters gut microbiota and subsequent host gene expression and energy uptake,” she said.
Dr. Jeon and her colleagues conducted a study to examine whether risk of diabetes changes with various common chronic infections, including herpes simplex virus 1, varicella virus, cytomegalovirus, Toxoplasma gondii, and H. pylori.
The study and its focus on H. pylori in particular were motivated in part by observation of a racial gradient in both diabetes prevalence and H. pylori infection in the United States, with Mexican Americans having a higher prevalence of both than either whites or non-Hispanic blacks.
Additionally, studies have found evidence of association between periodontal bacteria and increased diabetes risk, as well as links between decreased insulin sensitivity and higher antibody titers to herpes simplex virus 2 and Chlamydia pneumoniae.
Other studies, however, have not shown an association between common infections and insulin resistance or diabetes.
Dr. Jeon and colleagues analyzed data on 1,789 men and women older than 60 years who were enrolled in the Sacramento Area Latino Study on Aging (SALSA). Of that group, 782 people did not have diabetes and had available baseline pathogen data.
During the 10-year study, 144 of those 782 people developed diabetes (18% incidence rate), with diabetes defined as self-report of a physician's diagnosis of diabetes or of taking hypoglycemic medication, including insulin, at semiannual interviews; fasting glucose of at least 126 mg/dL at four follow-up visits; or death certificate inclusion of diabetes as a cause of death.
In bivariate analysis adjusted for gender and education, none of the pathogens reached statistical significance for an association with diabetes.
In multivariate analysis, however, the only significant association seen with diabetes was H. pylori (hazard ratio, 2.69). The association was stronger than that for either vascular disease (HR, 1.78) or being a former smoker (HR of 1.34 in bivariate analysis).
Possible explanations for the association include H. pylori–induced alterations in gut microbiota, changes in nutrient metabolism in the gut, increased energy harvesting, or altered host gene expression, Dr. Jeon said.
In the second study, Dr. Chen and her colleague Dr. Martin Blaser looked at data from NHANES III (1988-1994) and IV (1999-2004).
In NHANES III, they found a positive association between H. pylori infection and HbA1c in the overall cohort and in people with body mass indexes (BMIs) both below 25 and 25 and higher (P for interaction for each comparison less than .01).
They also saw a synergistic interaction between H. pylori and higher levels of BMI in both NHANES III and IV (P for interaction less than .01), suggesting that H. pylori exacerbated the rise in HbA1c often seen with weight increase.
In addition, in NHANES III but not NHANES IV, the synergistic effect was seen among patients seropositive for the cagA strain of H. pylori, which has been associated with virulence.
The investigators did not, however, find an association between self-reported diabetes and H. pylori infection.
The H. pylori association was stronger than that for either vascular disease or being a former smoker.
Source DR. JEON
H. pylori was associated with diabetes and increased HbA1c in two separate investigations. A mechanism to explain the curious finding is unknown.
Source ©3drenderings/Fotolia.com
Major Finding: Helicobacter pylori infection was associated with a hazard ratio of 2.69 for diabetes among Latinos older than 60 years.
Data Source: Epidemiologic studies examining the relationship between H. pylori infections, glycated hemoglobin levels, and diabetes.
Disclosures: Dr. Jeon's study was supported by grants from the National Institutes of Health. Dr. Chen did not disclose a funding source. Both investigators reported that they had no relevant financial disclosures.
BOSTON – Already convicted for its role in causing peptic ulcers, Helicobacter pylori is also being indicted as a possible co-conspirator in the development of diabetes, investigators from two separate studies said at the meeting.
In a study of nearly 1,800 older Latinos in California, H. pylori infection was associated with a more than twofold greater risk for diabetes, reported Dr. Christine Y. Jeon of the Columbia University School of Nursing, New York.
In addition, a separate study of National Health and Nutrition Examination Survey (NHANES) data found that, after excluding for diabetes and controlling for other risk factors, H. pylori seropositivity was positively associated with hemoglobin A1c levels – suggesting that the bacterium may play a role in impaired glucose tolerance, said Dr. Yu Chen of New York University Langone Medical Center, New York.
Dr. Jeon noted that, although the mechanism for the association between H. pylori infection and diabetes is unknown, it does not appear to be mediated by either the inflammatory pathway or insulin resistance.
“This highlights the need for future studies on how the timing and severity of H. pylori infection affect glucose control in younger individuals, and how H. pylori alters gut microbiota and subsequent host gene expression and energy uptake,” she said.
Dr. Jeon and her colleagues conducted a study to examine whether risk of diabetes changes with various common chronic infections, including herpes simplex virus 1, varicella virus, cytomegalovirus, Toxoplasma gondii, and H. pylori.
The study and its focus on H. pylori in particular were motivated in part by observation of a racial gradient in both diabetes prevalence and H. pylori infection in the United States, with Mexican Americans having a higher prevalence of both than either whites or non-Hispanic blacks.
Additionally, studies have found evidence of association between periodontal bacteria and increased diabetes risk, as well as links between decreased insulin sensitivity and higher antibody titers to herpes simplex virus 2 and Chlamydia pneumoniae.
Other studies, however, have not shown an association between common infections and insulin resistance or diabetes.
Dr. Jeon and colleagues analyzed data on 1,789 men and women older than 60 years who were enrolled in the Sacramento Area Latino Study on Aging (SALSA). Of that group, 782 people did not have diabetes and had available baseline pathogen data.
During the 10-year study, 144 of those 782 people developed diabetes (18% incidence rate), with diabetes defined as self-report of a physician's diagnosis of diabetes or of taking hypoglycemic medication, including insulin, at semiannual interviews; fasting glucose of at least 126 mg/dL at four follow-up visits; or death certificate inclusion of diabetes as a cause of death.
In bivariate analysis adjusted for gender and education, none of the pathogens reached statistical significance for an association with diabetes.
In multivariate analysis, however, the only significant association seen with diabetes was H. pylori (hazard ratio, 2.69). The association was stronger than that for either vascular disease (HR, 1.78) or being a former smoker (HR of 1.34 in bivariate analysis).
Possible explanations for the association include H. pylori–induced alterations in gut microbiota, changes in nutrient metabolism in the gut, increased energy harvesting, or altered host gene expression, Dr. Jeon said.
In the second study, Dr. Chen and her colleague Dr. Martin Blaser looked at data from NHANES III (1988-1994) and IV (1999-2004).
In NHANES III, they found a positive association between H. pylori infection and HbA1c in the overall cohort and in people with body mass indexes (BMIs) both below 25 and 25 and higher (P for interaction for each comparison less than .01).
They also saw a synergistic interaction between H. pylori and higher levels of BMI in both NHANES III and IV (P for interaction less than .01), suggesting that H. pylori exacerbated the rise in HbA1c often seen with weight increase.
In addition, in NHANES III but not NHANES IV, the synergistic effect was seen among patients seropositive for the cagA strain of H. pylori, which has been associated with virulence.
The investigators did not, however, find an association between self-reported diabetes and H. pylori infection.
The H. pylori association was stronger than that for either vascular disease or being a former smoker.
Source DR. JEON
H. pylori was associated with diabetes and increased HbA1c in two separate investigations. A mechanism to explain the curious finding is unknown.
Source ©3drenderings/Fotolia.com
From the Annual Meeting of the Infectious Diseases Society of America
HIV Care Faces Uncertain Future
BOSTON – Comprehensive HIV care in the United States has resulted in a dramatic reduction in AIDS-related morbidity and mortality, but the future of that care is clouded by uncertainties surrounding health care reform and financing, HIV specialists said at the annual meeting of the Infectious Diseases Society of America.
While they applaud expanded access to care, members of the HIV Medicine Association of the IDSA and the Ryan White Medical Providers Coalition expressed concern that the quality of care for HIV-positive patients could suffer if that care was moved out of Ryan White clinics and into Medicaid-based community health centers without clinical expertise in HIV, said Dr. Joel Gallant from the division of infectious diseases at Johns Hopkins University, Baltimore.

"The multidisciplinary integrated care provided by these clinics has really been critical to their success, and they have become models of high-quality health care for underserved people and for the concept of the medical home. Unfortunately, this model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform," he said at a briefing discussing the groups’ joint policy statement on the essential components of effective HIV care.
The Ryan White program, established by Congress in 1990, is the third largest funder of HIV care in the United States, after Medicare and Medicaid. According to the Kaiser Family Foundation, the program serves more than 500,000 people with HIV each year, and pays for the care of people with limited or no insurance or other financial resources.
In their policy statement, the authors optimistically state that President Obama’s health care reform plan "provides an unprecedented opportunity to improve access to HIV care and develop more sustainable funding streams that can be used to expand access to the effective HIV care model developed by the Ryan White program."
But if such change is to succeed – and it’s a very big "if" – Dr. Gallant and colleagues acknowledged that it "will require Medicaid, Medicare, and private insurers to adopt delivery systems and risk-adjusted payment mechanisms that support access to effective HIV care."
The authors say that whatever shape health care takes in the future, the elements required for effective HIV care include access to:
• Routine HIV testing.
• Early diagnosis.
• Care provided by an expert in HIV.
• Subspecialists with HIV experience.
• HIV medications.
• Support for adherence to treatment and health care.
• Access to social work services, substance abuse treatment, and mental health services.
"Weakening of this model by fragmenting care, decreasing access to essential services or decreasing provider expertise could really have devastating consequences to infected individuals and to society as a whole," Dr. Gallant said.
"[The HIV care] model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform."
He noted that although HIV medications are expensive, they are life-saving, highly cost-effective, and prevent illness, disability, hospitalization, and death when properly used.
"In addition, now we know that successful HIV treatment prevents transmission. In the recently published HPTN 052 study, treating the affected partner in a sero-discordant partner reduced transmission to the uninfected partner by 96%, so providing quality HIV care to HIV-infected is really critical to our efforts to reduce the size of the epidemic in this country," he added (N. Engl. J. Med. 2011;365:493-505).
The Ryan White model also has broader application to the treatment of other chronic conditions, commented coauthor Dr. Mari Kitahata from the department of medicine at the University of Washington, Seattle.
"A key component is coordination of care, and a care coordinator could be a qualified nurse, case manager or social worker responsible for communicating and coordinating with other providers, as well as bringing access to services throughout the continuum. Medication management is an essential component of primary care, as it is in other chronic diseases," she said.
The policy statement was developed by a joint working group of the HIV Medicine Association’s board of directors and the Ryan White Medical Providers Coalition with support from HIV Medicine Association staff.
Dr. Gallant disclosed that he has received honoraria or consulting fees from Bristol-Myers Squibb, Merck, Janssen Therapeutics, RAPID Pharmaceuticals and Gilead Sciences, and payment for review activities from Gilead and Sangamo Biosciences. Dr. Kitahata disclosed no potential conflicts of interest.
BOSTON – Comprehensive HIV care in the United States has resulted in a dramatic reduction in AIDS-related morbidity and mortality, but the future of that care is clouded by uncertainties surrounding health care reform and financing, HIV specialists said at the annual meeting of the Infectious Diseases Society of America.
While they applaud expanded access to care, members of the HIV Medicine Association of the IDSA and the Ryan White Medical Providers Coalition expressed concern that the quality of care for HIV-positive patients could suffer if that care was moved out of Ryan White clinics and into Medicaid-based community health centers without clinical expertise in HIV, said Dr. Joel Gallant from the division of infectious diseases at Johns Hopkins University, Baltimore.
"The multidisciplinary integrated care provided by these clinics has really been critical to their success, and they have become models of high-quality health care for underserved people and for the concept of the medical home. Unfortunately, this model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform," he said at a briefing discussing the groups’ joint policy statement on the essential components of effective HIV care.
The Ryan White program, established by Congress in 1990, is the third largest funder of HIV care in the United States, after Medicare and Medicaid. According to the Kaiser Family Foundation, the program serves more than 500,000 people with HIV each year, and pays for the care of people with limited or no insurance or other financial resources.
In their policy statement, the authors optimistically state that President Obama’s health care reform plan "provides an unprecedented opportunity to improve access to HIV care and develop more sustainable funding streams that can be used to expand access to the effective HIV care model developed by the Ryan White program."
But if such change is to succeed – and it’s a very big "if" – Dr. Gallant and colleagues acknowledged that it "will require Medicaid, Medicare, and private insurers to adopt delivery systems and risk-adjusted payment mechanisms that support access to effective HIV care."
The authors say that whatever shape health care takes in the future, the elements required for effective HIV care include access to:
• Routine HIV testing.
• Early diagnosis.
• Care provided by an expert in HIV.
• Subspecialists with HIV experience.
• HIV medications.
• Support for adherence to treatment and health care.
• Access to social work services, substance abuse treatment, and mental health services.
"Weakening of this model by fragmenting care, decreasing access to essential services or decreasing provider expertise could really have devastating consequences to infected individuals and to society as a whole," Dr. Gallant said.
"[The HIV care] model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform."
He noted that although HIV medications are expensive, they are life-saving, highly cost-effective, and prevent illness, disability, hospitalization, and death when properly used.
"In addition, now we know that successful HIV treatment prevents transmission. In the recently published HPTN 052 study, treating the affected partner in a sero-discordant partner reduced transmission to the uninfected partner by 96%, so providing quality HIV care to HIV-infected is really critical to our efforts to reduce the size of the epidemic in this country," he added (N. Engl. J. Med. 2011;365:493-505).
The Ryan White model also has broader application to the treatment of other chronic conditions, commented coauthor Dr. Mari Kitahata from the department of medicine at the University of Washington, Seattle.
"A key component is coordination of care, and a care coordinator could be a qualified nurse, case manager or social worker responsible for communicating and coordinating with other providers, as well as bringing access to services throughout the continuum. Medication management is an essential component of primary care, as it is in other chronic diseases," she said.
The policy statement was developed by a joint working group of the HIV Medicine Association’s board of directors and the Ryan White Medical Providers Coalition with support from HIV Medicine Association staff.
Dr. Gallant disclosed that he has received honoraria or consulting fees from Bristol-Myers Squibb, Merck, Janssen Therapeutics, RAPID Pharmaceuticals and Gilead Sciences, and payment for review activities from Gilead and Sangamo Biosciences. Dr. Kitahata disclosed no potential conflicts of interest.
BOSTON – Comprehensive HIV care in the United States has resulted in a dramatic reduction in AIDS-related morbidity and mortality, but the future of that care is clouded by uncertainties surrounding health care reform and financing, HIV specialists said at the annual meeting of the Infectious Diseases Society of America.
While they applaud expanded access to care, members of the HIV Medicine Association of the IDSA and the Ryan White Medical Providers Coalition expressed concern that the quality of care for HIV-positive patients could suffer if that care was moved out of Ryan White clinics and into Medicaid-based community health centers without clinical expertise in HIV, said Dr. Joel Gallant from the division of infectious diseases at Johns Hopkins University, Baltimore.
"The multidisciplinary integrated care provided by these clinics has really been critical to their success, and they have become models of high-quality health care for underserved people and for the concept of the medical home. Unfortunately, this model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform," he said at a briefing discussing the groups’ joint policy statement on the essential components of effective HIV care.
The Ryan White program, established by Congress in 1990, is the third largest funder of HIV care in the United States, after Medicare and Medicaid. According to the Kaiser Family Foundation, the program serves more than 500,000 people with HIV each year, and pays for the care of people with limited or no insurance or other financial resources.
In their policy statement, the authors optimistically state that President Obama’s health care reform plan "provides an unprecedented opportunity to improve access to HIV care and develop more sustainable funding streams that can be used to expand access to the effective HIV care model developed by the Ryan White program."
But if such change is to succeed – and it’s a very big "if" – Dr. Gallant and colleagues acknowledged that it "will require Medicaid, Medicare, and private insurers to adopt delivery systems and risk-adjusted payment mechanisms that support access to effective HIV care."
The authors say that whatever shape health care takes in the future, the elements required for effective HIV care include access to:
• Routine HIV testing.
• Early diagnosis.
• Care provided by an expert in HIV.
• Subspecialists with HIV experience.
• HIV medications.
• Support for adherence to treatment and health care.
• Access to social work services, substance abuse treatment, and mental health services.
"Weakening of this model by fragmenting care, decreasing access to essential services or decreasing provider expertise could really have devastating consequences to infected individuals and to society as a whole," Dr. Gallant said.
"[The HIV care] model is now in jeopardy, in part because of the current economic climate and in part because of the potential successes of health care reform."
He noted that although HIV medications are expensive, they are life-saving, highly cost-effective, and prevent illness, disability, hospitalization, and death when properly used.
"In addition, now we know that successful HIV treatment prevents transmission. In the recently published HPTN 052 study, treating the affected partner in a sero-discordant partner reduced transmission to the uninfected partner by 96%, so providing quality HIV care to HIV-infected is really critical to our efforts to reduce the size of the epidemic in this country," he added (N. Engl. J. Med. 2011;365:493-505).
The Ryan White model also has broader application to the treatment of other chronic conditions, commented coauthor Dr. Mari Kitahata from the department of medicine at the University of Washington, Seattle.
"A key component is coordination of care, and a care coordinator could be a qualified nurse, case manager or social worker responsible for communicating and coordinating with other providers, as well as bringing access to services throughout the continuum. Medication management is an essential component of primary care, as it is in other chronic diseases," she said.
The policy statement was developed by a joint working group of the HIV Medicine Association’s board of directors and the Ryan White Medical Providers Coalition with support from HIV Medicine Association staff.
Dr. Gallant disclosed that he has received honoraria or consulting fees from Bristol-Myers Squibb, Merck, Janssen Therapeutics, RAPID Pharmaceuticals and Gilead Sciences, and payment for review activities from Gilead and Sangamo Biosciences. Dr. Kitahata disclosed no potential conflicts of interest.
FROM THE ANNUAL MEETING OF THE INFECTIOUS DISEASES SOCIETY OF AMERICA
Major Finding: Coordinated HIV care services may be jeopardized by fragmentation of services unless new health care models adopt the comprehensive care program embodied by the Congressionally established Ryan White Program.
Data Source: Joint policy statement from the HIV Medicine Association of the IDSA and the Ryan White Medical Providers Coalition.
Disclosures: The policy statement was developed by a joint working group of the HIV Medicine Association board of directors and the Ryan White Medical Providers Coalition with support from HIV Medicine Association staff. Dr. Gallant disclosed that he has received honoraria or consulting fees from Bristol-Myers Squibb, Merck, Janssen Therapeutics, RAPID Pharmaceuticals and Gilead Sciences, and payment for review activities from Gilead and Sangamo Biosciences. Dr. Kitahata disclosed no potential conflicts of interest.
Community-Acquired Pneumonia Prevention Starts in the Mouth
BOSTON – Community-dwelling seniors who brush their teeth, keep as active as their infirmities permit, and shun cigarettes may be able to significantly lower their risk for serious pneumonia, investigators reported at the annual meeting of the Infectious Diseases Society of America.
Among 1,575 adults aged 70 years and older who were followed in an ongoing prospective study, a higher oral plaque burden was associated with a 1.43-fold greater risk for pneumonia that required hospitalization; the development of a mobility limitation was linked to 1.84-fold increased risk, and an active smoking status effectively doubled the risk (1.95-fold), reported Dr. Manisha Juthani-Mehta of Yale University in New Haven, Conn.
"The novel and interesting thing from this study is that these findings are consistent with the emerging theme linking oral bacteria (and therefore, potentially, the oral microbiome) to pneumonia risk in many different clinical settings – not only hospital-acquired pneumonia and ventilator-associated pneumonia, but now potentially ... community-acquired pneumonia, where aspiration may be a predominant mechanism for risk pneumonia in community-dwelling older adults as well," she said.
Dental plaque has been identified as a reservoir for respiratory pathogens implicated in hospital-acquired and ventilator-associated pneumonia, and her group has identified inadequate oral care as a risk factor for nursing home–acquired pneumonia, Dr. Juthani-Mehta said.
Whether dental plaque or poor oral hygiene also puts presumably healthy, community-dwelling older adults at greater risk for developing serious pneumonia was unclear, however.
The investigators hypothesized that in addition to inadequate dental care, modifiable risk factors for pneumonia would include lack of influenza and Pneumovax vaccinations, poor nutrition (body mass index loss), and cigarette smoking.
The overall Health ABC study cohort included 3,075 community-dwelling adults in Pittsburgh and Memphis who were aged 70-79 years at baseline. Of that group, 1,575 had a study interview within 6 months of a dental exam and had an available plaque score.
The authors defined poor oral hygiene as a mean oral plaque score of 1 or greater on a scale of 0-3 (0 = no plaque; 1 = plaque identified by a probe; 2 = visible plaque; 3 = abundant plaque).
The rate of pneumonia cases requiring hospitalization (the primary outcome) was 169.8 per 10,000 person-years, which was similar to that of the overall population rate for people aged 65 years and older (161.0 per 10,000 person-years in 2007, according to a 2010 National Health Statistics Report).
In a multivariate analysis, modifiable risk factors were mean oral plaque score (hazard ratio, 1.43), incident mobility limitation (HR, 1.84), and active smoking (HR, 1.95).
Nonmodifiable risk factors included male sex (HR, 2.08), white race (HR, 1.67), and age older than 75 years (HR, 1.32).
Looking at the average attributable fraction for each of the risk factors, the investigators found that the plaque score accounted for 13.1% of pneumonias, mobility limitation accounted for 12.2%, and smoking for 1.1%.
The study was supported by grants from the National Institutes for Health. Dr. Juthani-Mehta reported that she had no relevant financial disclosures.
BOSTON – Community-dwelling seniors who brush their teeth, keep as active as their infirmities permit, and shun cigarettes may be able to significantly lower their risk for serious pneumonia, investigators reported at the annual meeting of the Infectious Diseases Society of America.
Among 1,575 adults aged 70 years and older who were followed in an ongoing prospective study, a higher oral plaque burden was associated with a 1.43-fold greater risk for pneumonia that required hospitalization; the development of a mobility limitation was linked to 1.84-fold increased risk, and an active smoking status effectively doubled the risk (1.95-fold), reported Dr. Manisha Juthani-Mehta of Yale University in New Haven, Conn.
"The novel and interesting thing from this study is that these findings are consistent with the emerging theme linking oral bacteria (and therefore, potentially, the oral microbiome) to pneumonia risk in many different clinical settings – not only hospital-acquired pneumonia and ventilator-associated pneumonia, but now potentially ... community-acquired pneumonia, where aspiration may be a predominant mechanism for risk pneumonia in community-dwelling older adults as well," she said.
Dental plaque has been identified as a reservoir for respiratory pathogens implicated in hospital-acquired and ventilator-associated pneumonia, and her group has identified inadequate oral care as a risk factor for nursing home–acquired pneumonia, Dr. Juthani-Mehta said.
Whether dental plaque or poor oral hygiene also puts presumably healthy, community-dwelling older adults at greater risk for developing serious pneumonia was unclear, however.
The investigators hypothesized that in addition to inadequate dental care, modifiable risk factors for pneumonia would include lack of influenza and Pneumovax vaccinations, poor nutrition (body mass index loss), and cigarette smoking.
The overall Health ABC study cohort included 3,075 community-dwelling adults in Pittsburgh and Memphis who were aged 70-79 years at baseline. Of that group, 1,575 had a study interview within 6 months of a dental exam and had an available plaque score.
The authors defined poor oral hygiene as a mean oral plaque score of 1 or greater on a scale of 0-3 (0 = no plaque; 1 = plaque identified by a probe; 2 = visible plaque; 3 = abundant plaque).
The rate of pneumonia cases requiring hospitalization (the primary outcome) was 169.8 per 10,000 person-years, which was similar to that of the overall population rate for people aged 65 years and older (161.0 per 10,000 person-years in 2007, according to a 2010 National Health Statistics Report).
In a multivariate analysis, modifiable risk factors were mean oral plaque score (hazard ratio, 1.43), incident mobility limitation (HR, 1.84), and active smoking (HR, 1.95).
Nonmodifiable risk factors included male sex (HR, 2.08), white race (HR, 1.67), and age older than 75 years (HR, 1.32).
Looking at the average attributable fraction for each of the risk factors, the investigators found that the plaque score accounted for 13.1% of pneumonias, mobility limitation accounted for 12.2%, and smoking for 1.1%.
The study was supported by grants from the National Institutes for Health. Dr. Juthani-Mehta reported that she had no relevant financial disclosures.
BOSTON – Community-dwelling seniors who brush their teeth, keep as active as their infirmities permit, and shun cigarettes may be able to significantly lower their risk for serious pneumonia, investigators reported at the annual meeting of the Infectious Diseases Society of America.
Among 1,575 adults aged 70 years and older who were followed in an ongoing prospective study, a higher oral plaque burden was associated with a 1.43-fold greater risk for pneumonia that required hospitalization; the development of a mobility limitation was linked to 1.84-fold increased risk, and an active smoking status effectively doubled the risk (1.95-fold), reported Dr. Manisha Juthani-Mehta of Yale University in New Haven, Conn.
"The novel and interesting thing from this study is that these findings are consistent with the emerging theme linking oral bacteria (and therefore, potentially, the oral microbiome) to pneumonia risk in many different clinical settings – not only hospital-acquired pneumonia and ventilator-associated pneumonia, but now potentially ... community-acquired pneumonia, where aspiration may be a predominant mechanism for risk pneumonia in community-dwelling older adults as well," she said.
Dental plaque has been identified as a reservoir for respiratory pathogens implicated in hospital-acquired and ventilator-associated pneumonia, and her group has identified inadequate oral care as a risk factor for nursing home–acquired pneumonia, Dr. Juthani-Mehta said.
Whether dental plaque or poor oral hygiene also puts presumably healthy, community-dwelling older adults at greater risk for developing serious pneumonia was unclear, however.
The investigators hypothesized that in addition to inadequate dental care, modifiable risk factors for pneumonia would include lack of influenza and Pneumovax vaccinations, poor nutrition (body mass index loss), and cigarette smoking.
The overall Health ABC study cohort included 3,075 community-dwelling adults in Pittsburgh and Memphis who were aged 70-79 years at baseline. Of that group, 1,575 had a study interview within 6 months of a dental exam and had an available plaque score.
The authors defined poor oral hygiene as a mean oral plaque score of 1 or greater on a scale of 0-3 (0 = no plaque; 1 = plaque identified by a probe; 2 = visible plaque; 3 = abundant plaque).
The rate of pneumonia cases requiring hospitalization (the primary outcome) was 169.8 per 10,000 person-years, which was similar to that of the overall population rate for people aged 65 years and older (161.0 per 10,000 person-years in 2007, according to a 2010 National Health Statistics Report).
In a multivariate analysis, modifiable risk factors were mean oral plaque score (hazard ratio, 1.43), incident mobility limitation (HR, 1.84), and active smoking (HR, 1.95).
Nonmodifiable risk factors included male sex (HR, 2.08), white race (HR, 1.67), and age older than 75 years (HR, 1.32).
Looking at the average attributable fraction for each of the risk factors, the investigators found that the plaque score accounted for 13.1% of pneumonias, mobility limitation accounted for 12.2%, and smoking for 1.1%.
The study was supported by grants from the National Institutes for Health. Dr. Juthani-Mehta reported that she had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE INFECTIOUS DISEASES SOCIETY OF AMERICA
Major Finding: Community-dwelling older adults with a mean oral plaque score equal to or greater than 1 were 43% more likely to develop pneumonia that required hospitalization.
Data Source: A prospective cohort study.
Disclosures: The study was supported by grants from the National Institutes for Health. Dr. Juthani-Mehta reported that she had no relevant financial disclosures.