User login
30-Day Postop Mortality Higher in Low-BMI Patients
Low body mass index is a significant predictor of mortality within 30 days of surgery, according to a report published online in the Nov. 21 issue of Archives of Surgery.
Low BMI raises postoperative mortality risk even after allowances are made for the type of surgery and for the individual patient’s preoperative expected risk of death, said Florence E. Turrentine, Ph.D., R.N., of the department of surgery, University of Virginia, Charlottesville, and her associates.
In particular, the one-fifth of patients with the lowest BMI (less than 23.1 kg/m2) "demonstrated a significant increased risk of death, with 40% higher odds than the risk of death among patients in the middle range for BMI," they noted.
Most studies have reported no increase in postoperative mortality with increased BMI, but because these have had small numbers of patients and limited follow-up periods, the investigators undertook a larger analysis using the American College of Surgeons’ National Surgical Quality Improvement Program data set. "The analysis of such a large number of patients allowed us to [examine] individual procedures done by general surgeons to a level of specificity not previously available," Dr. Turrentine and her colleagues noted.
The study subjects were 189,533 patients who underwent a major general or vascular surgical procedure in 2005 and 2006 at 183 participating medical centers. All patients were examined preoperatively and were given a 30-day mortality probable risk score based on more than 30 demographic characteristics, comorbidities, and laboratory values (Arch. Surg. 2011 Nov. 21 [doi:10.1001/archsurg.2011.310]).
A total of 3,245 patients (1.7%) died within 30 days of their surgery.
Interestingly, compared with normal weight, obesity was associated with lower rather than higher postoperative surgical risk, but not to a statistically significant degree. Somewhat unexpectedly, it was low BMI that raised mortality risk.
Patients were divided into quintiles based on their BMI. After the data were adjusted to account for predicted mortality risk and type of surgery, the percentage of deaths among patients in the lowest BMI quintile (2.8%) was more than double that among patients in the highest BMI quintile (1.0%), which included patients with a BMI of 35.3 or greater.
Thirty-day mortality also was significantly higher among patients in the lowest quintile of BMI than among patients in the middle quintiles (1.8%, 1.5%, and 1.4%).
In this analysis, overweight and obese patients in the upper two quintiles had lower 30-day mortality than did normal-weight patients in the middle quintiles, but those differences did not attain statistical significance.
The investigators further analyzed the data by type of surgery, discriminating among 45 different procedures. Laparoscopy, which was selected as the reference procedure, had an overall mortality of 2.0%. In comparison with laparoscopy, exploratory laparotomy carried the highest 30-day mortality (13.9%).
The effect of BMI on 30-day mortality was found to be quite different for certain operations. High BMI raised 30-day mortality risk for colostomy formation, wound debridement, colorectal resection, hernia repair, and mastectomy.
No financial conflicts of interest were reported.
Low body mass index is a significant predictor of mortality within 30 days of surgery, according to a report published online in the Nov. 21 issue of Archives of Surgery.
Low BMI raises postoperative mortality risk even after allowances are made for the type of surgery and for the individual patient’s preoperative expected risk of death, said Florence E. Turrentine, Ph.D., R.N., of the department of surgery, University of Virginia, Charlottesville, and her associates.
In particular, the one-fifth of patients with the lowest BMI (less than 23.1 kg/m2) "demonstrated a significant increased risk of death, with 40% higher odds than the risk of death among patients in the middle range for BMI," they noted.
Most studies have reported no increase in postoperative mortality with increased BMI, but because these have had small numbers of patients and limited follow-up periods, the investigators undertook a larger analysis using the American College of Surgeons’ National Surgical Quality Improvement Program data set. "The analysis of such a large number of patients allowed us to [examine] individual procedures done by general surgeons to a level of specificity not previously available," Dr. Turrentine and her colleagues noted.
The study subjects were 189,533 patients who underwent a major general or vascular surgical procedure in 2005 and 2006 at 183 participating medical centers. All patients were examined preoperatively and were given a 30-day mortality probable risk score based on more than 30 demographic characteristics, comorbidities, and laboratory values (Arch. Surg. 2011 Nov. 21 [doi:10.1001/archsurg.2011.310]).
A total of 3,245 patients (1.7%) died within 30 days of their surgery.
Interestingly, compared with normal weight, obesity was associated with lower rather than higher postoperative surgical risk, but not to a statistically significant degree. Somewhat unexpectedly, it was low BMI that raised mortality risk.
Patients were divided into quintiles based on their BMI. After the data were adjusted to account for predicted mortality risk and type of surgery, the percentage of deaths among patients in the lowest BMI quintile (2.8%) was more than double that among patients in the highest BMI quintile (1.0%), which included patients with a BMI of 35.3 or greater.
Thirty-day mortality also was significantly higher among patients in the lowest quintile of BMI than among patients in the middle quintiles (1.8%, 1.5%, and 1.4%).
In this analysis, overweight and obese patients in the upper two quintiles had lower 30-day mortality than did normal-weight patients in the middle quintiles, but those differences did not attain statistical significance.
The investigators further analyzed the data by type of surgery, discriminating among 45 different procedures. Laparoscopy, which was selected as the reference procedure, had an overall mortality of 2.0%. In comparison with laparoscopy, exploratory laparotomy carried the highest 30-day mortality (13.9%).
The effect of BMI on 30-day mortality was found to be quite different for certain operations. High BMI raised 30-day mortality risk for colostomy formation, wound debridement, colorectal resection, hernia repair, and mastectomy.
No financial conflicts of interest were reported.
Low body mass index is a significant predictor of mortality within 30 days of surgery, according to a report published online in the Nov. 21 issue of Archives of Surgery.
Low BMI raises postoperative mortality risk even after allowances are made for the type of surgery and for the individual patient’s preoperative expected risk of death, said Florence E. Turrentine, Ph.D., R.N., of the department of surgery, University of Virginia, Charlottesville, and her associates.
In particular, the one-fifth of patients with the lowest BMI (less than 23.1 kg/m2) "demonstrated a significant increased risk of death, with 40% higher odds than the risk of death among patients in the middle range for BMI," they noted.
Most studies have reported no increase in postoperative mortality with increased BMI, but because these have had small numbers of patients and limited follow-up periods, the investigators undertook a larger analysis using the American College of Surgeons’ National Surgical Quality Improvement Program data set. "The analysis of such a large number of patients allowed us to [examine] individual procedures done by general surgeons to a level of specificity not previously available," Dr. Turrentine and her colleagues noted.
The study subjects were 189,533 patients who underwent a major general or vascular surgical procedure in 2005 and 2006 at 183 participating medical centers. All patients were examined preoperatively and were given a 30-day mortality probable risk score based on more than 30 demographic characteristics, comorbidities, and laboratory values (Arch. Surg. 2011 Nov. 21 [doi:10.1001/archsurg.2011.310]).
A total of 3,245 patients (1.7%) died within 30 days of their surgery.
Interestingly, compared with normal weight, obesity was associated with lower rather than higher postoperative surgical risk, but not to a statistically significant degree. Somewhat unexpectedly, it was low BMI that raised mortality risk.
Patients were divided into quintiles based on their BMI. After the data were adjusted to account for predicted mortality risk and type of surgery, the percentage of deaths among patients in the lowest BMI quintile (2.8%) was more than double that among patients in the highest BMI quintile (1.0%), which included patients with a BMI of 35.3 or greater.
Thirty-day mortality also was significantly higher among patients in the lowest quintile of BMI than among patients in the middle quintiles (1.8%, 1.5%, and 1.4%).
In this analysis, overweight and obese patients in the upper two quintiles had lower 30-day mortality than did normal-weight patients in the middle quintiles, but those differences did not attain statistical significance.
The investigators further analyzed the data by type of surgery, discriminating among 45 different procedures. Laparoscopy, which was selected as the reference procedure, had an overall mortality of 2.0%. In comparison with laparoscopy, exploratory laparotomy carried the highest 30-day mortality (13.9%).
The effect of BMI on 30-day mortality was found to be quite different for certain operations. High BMI raised 30-day mortality risk for colostomy formation, wound debridement, colorectal resection, hernia repair, and mastectomy.
No financial conflicts of interest were reported.
FROM ARCHIVES OF SURGERY
Mycophenolate Better Than Azathioprine for Lupus Nephritis Maintenance Therapy
Mycophenolate mofetil was more effective than azathioprine in maintaining renal response and preventing relapse in patients with active lupus nephritis, judging from the findings of a phase III clinical trial reported in the Nov. 17 issue of the New England Journal of Medicine.
Compared with azathioprine maintenance therapy, the use of mycophenolate mofetil prolonged the time to treatment failure, which was the study’s primary end point. It also extended the interval until individual components of this end point were reached, including a renal flare, the need for rescue therapy, sustained doubling time of the serum creatinine level, and the development of end-stage renal disease (ESRD), said Dr. Mary Anne Dooley of the University of North Carolina at Chapel Hill and her associates in the manufacturer-sponsored Aspreva Lupus Management Study (ALMS).
The investigators previously reported the results of the induction phase of ALMS, in which the efficacy and safety of mycophenolate mofetil were compared with that of intravenous cyclophosphamide as induction therapy for lupus nephritis. This latest report covers the results of the 3-year maintenance phase of ALMS, a prospective, double-blind trial comparing oral mycophenolate mofetil against oral azathioprine for maintenance of remission among the study subjects who responded to either induction therapy.
The 227 study subjects were aged 12-75 years at baseline and had class III, IV, or V lupus nephritis. They were enrolled at medical centers in Asia, Latin America, North America, Europe, South Africa, and Australia and were randomly assigned to receive mycophenolate mofetil (116 patients) or azathioprine (111 patients).
A total of 127 subjects (55.9% of the mycophenolate group and 48.6% of the azathioprine group) completed 36 months of treatment.
"Mycophenolate mofetil was significantly superior to azathioprine with respect to the primary end point, the time to treatment failure," and overall rates of treatment failure were 16.4% with mycophenolate, compared with 32.4% with azathioprine, regardless of which type of induction therapy had been used or where patients resided, Dr. Dooley and her colleagues said (N. Engl. J. Med. 2011;365:1886-95).
"Mycophenolate mofetil was significantly superior to azathioprine."
Among subjects who received mycophenolate mofetil maintenance, renal flares developed in 12.9%, rescue therapy was required in 7.8%, and a doubling of the serum creatinine level was reached in 0.9%. Among subjects who received azathioprine maintenance, renal flares developed in nearly twice as many (23.4%), rescue therapy was required in more than twice as many (17.1%), and a doubling of the serum creatinine level was reached in five times as many (4.5%).
Three patients on azathioprine developed ESRD, compared with none of those taking mycophenolate mofetil.
The overall incidence of adverse events was similar between the two groups, and infections were the most common adverse events in both. The rates of serious infection were low in both groups, at 9.6% with mycophenolate mofetil and 11.7% with azathioprine.
The percentage of patients who withdrew from treatment because of adverse effects was higher with azathioprine (39.6%) than with mycophenolate mofetil (25.2%).
"Although our trial included more patients and was substantially longer than many of the controlled trials involving patients with lupus nephritis, potential outcomes that might appear more frequently after 5-20 years [such as cardiovascular complications and ESRD] cannot be determined, since no further follow-up study is planned," they noted.
"The length of time that mycophenolate mofetil needs to be continued is unknown; hence, improved biomarkers of response are needed to distinguish disease remission from remission that occurs while the patient is receiving treatment," they added.
It is important to note that this maintenance study included only patients who responded well to induction therapy. Thus, the results may not apply to those whose disease is more difficult to treat, Dr. Dooley and her associates said.
The ALMS was supported by Vifor Pharma (formerly Aspreva Pharmaceuticals) as part of the Roche-Aspreva rare diseases collaboration, and by Caudex Medical.
Mycophenolate mofetil was more effective than azathioprine in maintaining renal response and preventing relapse in patients with active lupus nephritis, judging from the findings of a phase III clinical trial reported in the Nov. 17 issue of the New England Journal of Medicine.
Compared with azathioprine maintenance therapy, the use of mycophenolate mofetil prolonged the time to treatment failure, which was the study’s primary end point. It also extended the interval until individual components of this end point were reached, including a renal flare, the need for rescue therapy, sustained doubling time of the serum creatinine level, and the development of end-stage renal disease (ESRD), said Dr. Mary Anne Dooley of the University of North Carolina at Chapel Hill and her associates in the manufacturer-sponsored Aspreva Lupus Management Study (ALMS).
The investigators previously reported the results of the induction phase of ALMS, in which the efficacy and safety of mycophenolate mofetil were compared with that of intravenous cyclophosphamide as induction therapy for lupus nephritis. This latest report covers the results of the 3-year maintenance phase of ALMS, a prospective, double-blind trial comparing oral mycophenolate mofetil against oral azathioprine for maintenance of remission among the study subjects who responded to either induction therapy.
The 227 study subjects were aged 12-75 years at baseline and had class III, IV, or V lupus nephritis. They were enrolled at medical centers in Asia, Latin America, North America, Europe, South Africa, and Australia and were randomly assigned to receive mycophenolate mofetil (116 patients) or azathioprine (111 patients).
A total of 127 subjects (55.9% of the mycophenolate group and 48.6% of the azathioprine group) completed 36 months of treatment.
"Mycophenolate mofetil was significantly superior to azathioprine with respect to the primary end point, the time to treatment failure," and overall rates of treatment failure were 16.4% with mycophenolate, compared with 32.4% with azathioprine, regardless of which type of induction therapy had been used or where patients resided, Dr. Dooley and her colleagues said (N. Engl. J. Med. 2011;365:1886-95).
"Mycophenolate mofetil was significantly superior to azathioprine."
Among subjects who received mycophenolate mofetil maintenance, renal flares developed in 12.9%, rescue therapy was required in 7.8%, and a doubling of the serum creatinine level was reached in 0.9%. Among subjects who received azathioprine maintenance, renal flares developed in nearly twice as many (23.4%), rescue therapy was required in more than twice as many (17.1%), and a doubling of the serum creatinine level was reached in five times as many (4.5%).
Three patients on azathioprine developed ESRD, compared with none of those taking mycophenolate mofetil.
The overall incidence of adverse events was similar between the two groups, and infections were the most common adverse events in both. The rates of serious infection were low in both groups, at 9.6% with mycophenolate mofetil and 11.7% with azathioprine.
The percentage of patients who withdrew from treatment because of adverse effects was higher with azathioprine (39.6%) than with mycophenolate mofetil (25.2%).
"Although our trial included more patients and was substantially longer than many of the controlled trials involving patients with lupus nephritis, potential outcomes that might appear more frequently after 5-20 years [such as cardiovascular complications and ESRD] cannot be determined, since no further follow-up study is planned," they noted.
"The length of time that mycophenolate mofetil needs to be continued is unknown; hence, improved biomarkers of response are needed to distinguish disease remission from remission that occurs while the patient is receiving treatment," they added.
It is important to note that this maintenance study included only patients who responded well to induction therapy. Thus, the results may not apply to those whose disease is more difficult to treat, Dr. Dooley and her associates said.
The ALMS was supported by Vifor Pharma (formerly Aspreva Pharmaceuticals) as part of the Roche-Aspreva rare diseases collaboration, and by Caudex Medical.
Mycophenolate mofetil was more effective than azathioprine in maintaining renal response and preventing relapse in patients with active lupus nephritis, judging from the findings of a phase III clinical trial reported in the Nov. 17 issue of the New England Journal of Medicine.
Compared with azathioprine maintenance therapy, the use of mycophenolate mofetil prolonged the time to treatment failure, which was the study’s primary end point. It also extended the interval until individual components of this end point were reached, including a renal flare, the need for rescue therapy, sustained doubling time of the serum creatinine level, and the development of end-stage renal disease (ESRD), said Dr. Mary Anne Dooley of the University of North Carolina at Chapel Hill and her associates in the manufacturer-sponsored Aspreva Lupus Management Study (ALMS).
The investigators previously reported the results of the induction phase of ALMS, in which the efficacy and safety of mycophenolate mofetil were compared with that of intravenous cyclophosphamide as induction therapy for lupus nephritis. This latest report covers the results of the 3-year maintenance phase of ALMS, a prospective, double-blind trial comparing oral mycophenolate mofetil against oral azathioprine for maintenance of remission among the study subjects who responded to either induction therapy.
The 227 study subjects were aged 12-75 years at baseline and had class III, IV, or V lupus nephritis. They were enrolled at medical centers in Asia, Latin America, North America, Europe, South Africa, and Australia and were randomly assigned to receive mycophenolate mofetil (116 patients) or azathioprine (111 patients).
A total of 127 subjects (55.9% of the mycophenolate group and 48.6% of the azathioprine group) completed 36 months of treatment.
"Mycophenolate mofetil was significantly superior to azathioprine with respect to the primary end point, the time to treatment failure," and overall rates of treatment failure were 16.4% with mycophenolate, compared with 32.4% with azathioprine, regardless of which type of induction therapy had been used or where patients resided, Dr. Dooley and her colleagues said (N. Engl. J. Med. 2011;365:1886-95).
"Mycophenolate mofetil was significantly superior to azathioprine."
Among subjects who received mycophenolate mofetil maintenance, renal flares developed in 12.9%, rescue therapy was required in 7.8%, and a doubling of the serum creatinine level was reached in 0.9%. Among subjects who received azathioprine maintenance, renal flares developed in nearly twice as many (23.4%), rescue therapy was required in more than twice as many (17.1%), and a doubling of the serum creatinine level was reached in five times as many (4.5%).
Three patients on azathioprine developed ESRD, compared with none of those taking mycophenolate mofetil.
The overall incidence of adverse events was similar between the two groups, and infections were the most common adverse events in both. The rates of serious infection were low in both groups, at 9.6% with mycophenolate mofetil and 11.7% with azathioprine.
The percentage of patients who withdrew from treatment because of adverse effects was higher with azathioprine (39.6%) than with mycophenolate mofetil (25.2%).
"Although our trial included more patients and was substantially longer than many of the controlled trials involving patients with lupus nephritis, potential outcomes that might appear more frequently after 5-20 years [such as cardiovascular complications and ESRD] cannot be determined, since no further follow-up study is planned," they noted.
"The length of time that mycophenolate mofetil needs to be continued is unknown; hence, improved biomarkers of response are needed to distinguish disease remission from remission that occurs while the patient is receiving treatment," they added.
It is important to note that this maintenance study included only patients who responded well to induction therapy. Thus, the results may not apply to those whose disease is more difficult to treat, Dr. Dooley and her associates said.
The ALMS was supported by Vifor Pharma (formerly Aspreva Pharmaceuticals) as part of the Roche-Aspreva rare diseases collaboration, and by Caudex Medical.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Mycophenolate mofetil was superior to azathioprine in rates of treatment failure (16.4% vs. 32.4%), renal flares (12.9% vs. 23.4%), need for rescue therapy (7.8% vs. 17.1%), doubling of serum creatinine level (0.9% vs. 4.5%), and development of ESRD (0% vs. 3%).
Data Source: The maintenance phase of an international, randomized, double-blind, phase III clinical trial involving 227 patients aged 12-75 years who had lupus nephritis and were followed for 3 years.
Disclosures: The ALMS was supported by Vifor Pharma (formerly Aspreva Pharmaceuticals) as part of the Roche-Aspreva rare diseases collaboration, and by Caudex Medical.
Obese Children Who Lose Weight Decrease Future CV Risks
Overweight or obese children who lose weight by the time they reach young adulthood markedly decrease their cardiovascular risks, according to a report in the Nov. 17 issue of the New England Journal of Medicine.
Although childhood overweight and obesity frequently persist into adulthood, some children lose weight, often during adolescence, and become nonobese adults. According to this analysis of four large cohort studies that tracked cardiovascular risk factors over two decades, such weight loss dramatically reduces their risk of type 2 diabetes, hypertension, dyslipidemia, and carotid-artery atherosclerosis in young adulthood, wrote Dr. Markus Juonala of the Research Center of Applied and Preventive Cardiovascular Medicine, University of Turku (Finland), and his associates.
"Although the observational nature of our study precludes making clinical recommendations, we hypothesize that reducing BMI [body mass index] in children and adolescents who are overweight or obese could reduce their cardiovascular risk. If this hypothesis is correct, primary care physicians should not take the pessimistic view that once childhood obesity is established, CV risk is also determined, but should recognize that CV risk may be substantially reduced if childhood obesity is successfully treated," said Dr. Juonala and his colleagues in the International Childhood Cardiovascular Cohort Consortium.
The consortium was created specifically to analyze the data pooled from four cohorts – the Bogalusa Heart Study and the Muscatine Study in the United States, the Childhood Determinants of Adult Health study in Australia, and the Cardiovascular Risk in Young Finns study in Finland – in which subjects underwent a baseline assessment of CV risk factors at ages 3-18 years and a follow-up assessment a mean of 23 years later.
"CV risk may be substantially reduced if childhood obesity is successfully treated."
There were 6,328 subjects, including 2,961 males and 3,367 females. At baseline during childhood, the prevalence of overweight or obesity was 12.2%, and that of obesity was 2.3%. At follow-up during young adulthood, the prevalence of overweight or obesity was 54.9%, and that of obesity was 20.7%.
As expected, "our data confirm both the increase in CV risk associated with childhood overweight or obesity and the tracking of adiposity between childhood and adulthood," the investigators said.
A total of 774 subjects had been overweight or obese as children, and 500 of them (64.6%) remained obese as adults. Another 147 subjects had been obese as children, and 121 (82.3%) of them remained obese as adults. In these subjects, overweight or obesity were strong predictors of type 2 diabetes, hypertension, poor cholesterol profiles, and reduced carotid-artery intima-media thickness (a proxy measure for incipient CV disease, since the cohorts were too young to have experienced CV events).
Among 5,554 subjects who had had normal weight as children, 812 (14.6%) were obese as adults. As expected, these subjects who were of normal weight in childhood but became overweight or obese as adults also had adverse CV risk profiles.
However, subjects who had been overweight or obese as children but became nonobese by young adulthood had CV risk profiles similar to those of subjects who had been of normal weight throughout their lives, Dr. Juonala and his associates wrote (N. Engl. J. Med. 2011;365:1876-85).
For example, the subjects who had been normal weight throughout the study and those who had been overweight or obese as children but became nonobese by young adulthood had no increased relative risk for developing type 2 diabetes, whereas those who were overweight or obese in childhood and remained so in young adulthood had a 5.4-fold increase in relative risk for developing type 2 diabetes, and those who were obese in childhood and remained so in young adulthood had a 4.5-fold increase in relative risk.
This study was limited in that the subjects were predominantly white, so the results cannot be generalized to other races or ethnic groups, the authors added.
This pooled analysis was supported by funding for the original four longitudinal cohort studies. Dr. Juonala reported no relevant financial disclosures. His coauthors reported ties to Pfizer, Merck, and AstraZeneca.
Juonala et al. found that during an interval of almost 25 years, "only 15% of subjects who were of normal weight as children [became] obese as adults, whereas 65% of those who were overweight or obese as children and 82% of those who were obese as children were obese as adults," said Dr. Albert P. Rocchini.
"These figures suggest that targeting interventions for obesity prevention and treatment specifically to children who are at high risk for becoming obese will prove to be a more valuable and more cost-effective strategy than targeting these interventions to whole populations of children," he noted.
Dr. Rocchini is in the pediatric cardiology division at C.S. Mott Children’s Hospital and the University of Michigan, Ann Arbor. These remarks were taken from his editorial comment accompanying the report of Dr. Juonala et al. (New Engl. J. Med. 2011;365:1927-9). Dr. Rocchini said he had no relevant financial disclosures.
Juonala et al. found that during an interval of almost 25 years, "only 15% of subjects who were of normal weight as children [became] obese as adults, whereas 65% of those who were overweight or obese as children and 82% of those who were obese as children were obese as adults," said Dr. Albert P. Rocchini.
"These figures suggest that targeting interventions for obesity prevention and treatment specifically to children who are at high risk for becoming obese will prove to be a more valuable and more cost-effective strategy than targeting these interventions to whole populations of children," he noted.
Dr. Rocchini is in the pediatric cardiology division at C.S. Mott Children’s Hospital and the University of Michigan, Ann Arbor. These remarks were taken from his editorial comment accompanying the report of Dr. Juonala et al. (New Engl. J. Med. 2011;365:1927-9). Dr. Rocchini said he had no relevant financial disclosures.
Juonala et al. found that during an interval of almost 25 years, "only 15% of subjects who were of normal weight as children [became] obese as adults, whereas 65% of those who were overweight or obese as children and 82% of those who were obese as children were obese as adults," said Dr. Albert P. Rocchini.
"These figures suggest that targeting interventions for obesity prevention and treatment specifically to children who are at high risk for becoming obese will prove to be a more valuable and more cost-effective strategy than targeting these interventions to whole populations of children," he noted.
Dr. Rocchini is in the pediatric cardiology division at C.S. Mott Children’s Hospital and the University of Michigan, Ann Arbor. These remarks were taken from his editorial comment accompanying the report of Dr. Juonala et al. (New Engl. J. Med. 2011;365:1927-9). Dr. Rocchini said he had no relevant financial disclosures.
Overweight or obese children who lose weight by the time they reach young adulthood markedly decrease their cardiovascular risks, according to a report in the Nov. 17 issue of the New England Journal of Medicine.
Although childhood overweight and obesity frequently persist into adulthood, some children lose weight, often during adolescence, and become nonobese adults. According to this analysis of four large cohort studies that tracked cardiovascular risk factors over two decades, such weight loss dramatically reduces their risk of type 2 diabetes, hypertension, dyslipidemia, and carotid-artery atherosclerosis in young adulthood, wrote Dr. Markus Juonala of the Research Center of Applied and Preventive Cardiovascular Medicine, University of Turku (Finland), and his associates.
"Although the observational nature of our study precludes making clinical recommendations, we hypothesize that reducing BMI [body mass index] in children and adolescents who are overweight or obese could reduce their cardiovascular risk. If this hypothesis is correct, primary care physicians should not take the pessimistic view that once childhood obesity is established, CV risk is also determined, but should recognize that CV risk may be substantially reduced if childhood obesity is successfully treated," said Dr. Juonala and his colleagues in the International Childhood Cardiovascular Cohort Consortium.
The consortium was created specifically to analyze the data pooled from four cohorts – the Bogalusa Heart Study and the Muscatine Study in the United States, the Childhood Determinants of Adult Health study in Australia, and the Cardiovascular Risk in Young Finns study in Finland – in which subjects underwent a baseline assessment of CV risk factors at ages 3-18 years and a follow-up assessment a mean of 23 years later.
"CV risk may be substantially reduced if childhood obesity is successfully treated."
There were 6,328 subjects, including 2,961 males and 3,367 females. At baseline during childhood, the prevalence of overweight or obesity was 12.2%, and that of obesity was 2.3%. At follow-up during young adulthood, the prevalence of overweight or obesity was 54.9%, and that of obesity was 20.7%.
As expected, "our data confirm both the increase in CV risk associated with childhood overweight or obesity and the tracking of adiposity between childhood and adulthood," the investigators said.
A total of 774 subjects had been overweight or obese as children, and 500 of them (64.6%) remained obese as adults. Another 147 subjects had been obese as children, and 121 (82.3%) of them remained obese as adults. In these subjects, overweight or obesity were strong predictors of type 2 diabetes, hypertension, poor cholesterol profiles, and reduced carotid-artery intima-media thickness (a proxy measure for incipient CV disease, since the cohorts were too young to have experienced CV events).
Among 5,554 subjects who had had normal weight as children, 812 (14.6%) were obese as adults. As expected, these subjects who were of normal weight in childhood but became overweight or obese as adults also had adverse CV risk profiles.
However, subjects who had been overweight or obese as children but became nonobese by young adulthood had CV risk profiles similar to those of subjects who had been of normal weight throughout their lives, Dr. Juonala and his associates wrote (N. Engl. J. Med. 2011;365:1876-85).
For example, the subjects who had been normal weight throughout the study and those who had been overweight or obese as children but became nonobese by young adulthood had no increased relative risk for developing type 2 diabetes, whereas those who were overweight or obese in childhood and remained so in young adulthood had a 5.4-fold increase in relative risk for developing type 2 diabetes, and those who were obese in childhood and remained so in young adulthood had a 4.5-fold increase in relative risk.
This study was limited in that the subjects were predominantly white, so the results cannot be generalized to other races or ethnic groups, the authors added.
This pooled analysis was supported by funding for the original four longitudinal cohort studies. Dr. Juonala reported no relevant financial disclosures. His coauthors reported ties to Pfizer, Merck, and AstraZeneca.
Overweight or obese children who lose weight by the time they reach young adulthood markedly decrease their cardiovascular risks, according to a report in the Nov. 17 issue of the New England Journal of Medicine.
Although childhood overweight and obesity frequently persist into adulthood, some children lose weight, often during adolescence, and become nonobese adults. According to this analysis of four large cohort studies that tracked cardiovascular risk factors over two decades, such weight loss dramatically reduces their risk of type 2 diabetes, hypertension, dyslipidemia, and carotid-artery atherosclerosis in young adulthood, wrote Dr. Markus Juonala of the Research Center of Applied and Preventive Cardiovascular Medicine, University of Turku (Finland), and his associates.
"Although the observational nature of our study precludes making clinical recommendations, we hypothesize that reducing BMI [body mass index] in children and adolescents who are overweight or obese could reduce their cardiovascular risk. If this hypothesis is correct, primary care physicians should not take the pessimistic view that once childhood obesity is established, CV risk is also determined, but should recognize that CV risk may be substantially reduced if childhood obesity is successfully treated," said Dr. Juonala and his colleagues in the International Childhood Cardiovascular Cohort Consortium.
The consortium was created specifically to analyze the data pooled from four cohorts – the Bogalusa Heart Study and the Muscatine Study in the United States, the Childhood Determinants of Adult Health study in Australia, and the Cardiovascular Risk in Young Finns study in Finland – in which subjects underwent a baseline assessment of CV risk factors at ages 3-18 years and a follow-up assessment a mean of 23 years later.
"CV risk may be substantially reduced if childhood obesity is successfully treated."
There were 6,328 subjects, including 2,961 males and 3,367 females. At baseline during childhood, the prevalence of overweight or obesity was 12.2%, and that of obesity was 2.3%. At follow-up during young adulthood, the prevalence of overweight or obesity was 54.9%, and that of obesity was 20.7%.
As expected, "our data confirm both the increase in CV risk associated with childhood overweight or obesity and the tracking of adiposity between childhood and adulthood," the investigators said.
A total of 774 subjects had been overweight or obese as children, and 500 of them (64.6%) remained obese as adults. Another 147 subjects had been obese as children, and 121 (82.3%) of them remained obese as adults. In these subjects, overweight or obesity were strong predictors of type 2 diabetes, hypertension, poor cholesterol profiles, and reduced carotid-artery intima-media thickness (a proxy measure for incipient CV disease, since the cohorts were too young to have experienced CV events).
Among 5,554 subjects who had had normal weight as children, 812 (14.6%) were obese as adults. As expected, these subjects who were of normal weight in childhood but became overweight or obese as adults also had adverse CV risk profiles.
However, subjects who had been overweight or obese as children but became nonobese by young adulthood had CV risk profiles similar to those of subjects who had been of normal weight throughout their lives, Dr. Juonala and his associates wrote (N. Engl. J. Med. 2011;365:1876-85).
For example, the subjects who had been normal weight throughout the study and those who had been overweight or obese as children but became nonobese by young adulthood had no increased relative risk for developing type 2 diabetes, whereas those who were overweight or obese in childhood and remained so in young adulthood had a 5.4-fold increase in relative risk for developing type 2 diabetes, and those who were obese in childhood and remained so in young adulthood had a 4.5-fold increase in relative risk.
This study was limited in that the subjects were predominantly white, so the results cannot be generalized to other races or ethnic groups, the authors added.
This pooled analysis was supported by funding for the original four longitudinal cohort studies. Dr. Juonala reported no relevant financial disclosures. His coauthors reported ties to Pfizer, Merck, and AstraZeneca.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: The subjects who had been normal weight throughout the study and those who had been overweight or obese as children but became nonobese by young adulthood, had no increased relative risk for developing type 2 diabetes, whereas those who were overweight or obese in childhood and remained so in young adulthood had a 5.4-fold increase in relative risk for developing type 2 diabetes, and those who were obese in childhood and remained so in young adulthood had a 4.5-fold increase in relative risk for developing type 2 diabetes.
Data Source: A pooled analysis of data from four longitudinal cohort studies of CV risk factors in 6,328 subjects who were assessed at ages 3-18 years and again a mean of 23 years later during young adulthood.
Disclosures: This pooled analysis was supported by funding for the original four longitudinal cohort studies. Dr. Juonala reported no relevant financial disclosures. Dr. Juonala’s associates reported ties to Pfizer, Merck, and AstraZeneca.
Prostate: Denosumab Extends Bone Metastasis-Free Survival
The monoclonal antibody denosumab extended bone metastasis–free survival in an international, placebo-controlled phase III study involving 1,432 men with castration-resistant prostate cancer published online Nov. 16 in the Lancet Oncology.
Denosumab also prolonged the time to first bone metastasis and was associated with fewer symptomatic bone metastases in these high-risk patients, said Dr. Matthew R. Smith of the cancer center at the Massachusetts General Hospital, Boston, and his associates.
However, the agent did not improve overall survival, they noted.
The researchers assessed denosumab in a randomized, double-blind clinical trial conducted at 319 medical centers in 30 countries. Study subjects were men with castration-resistant prostate cancer who had no evidence of metastasis on radioisotope bone scanning, which was confirmed with subsequent imaging by CT, MRI, or plain radiography. All subjects were at high risk for disease progression based on elevated prostate-specific antigen results or short PSA doubling times.
The study subjects were randomly assigned to receive either subcutaneous denosumab 120 mg (716 patients) or placebo (716 patients) every 4 weeks until a study event (bone metastasis or death) was reached. All were strongly advised to take daily calcium and vitamin D supplements. They underwent further bone scans every 4 months to detect bone metastases.
Patients who developed a bone metastasis were discontinued from study treatment so that they could receive standard therapy, but were followed for up to an additional 3 years.
There were 605 bone metastases and 100 deaths during a median follow-up of 20 months.
The primary efficacy end point was bone metastasis–free survival. Compared with placebo, denosumab extended this end point by 4.2 months. Median bone metastasis–free survival was 29.5 months with denosumab and 25.2 months with placebo, "representing a decrease in risk of 15%," Dr. Smith and his colleagues said (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61226-9]).
The median time to bone metastasis was 33.2 months with denosumab, compared with 29.5 months with placebo. And the rate of symptomatic bone metastasis was 10% with denosumab, compared with 13% with placebo; the investigators reported a 33% reduction in the risk of symptomatic bone metastasis.
The median overall survival was similar between the two groups, however, at 43.9 months in the denosumab group and 44.8 months in the placebo group. Similarly, median progression-free survival was 21.7 months with denosumab and 19.3 months with placebo.
The investigators noted that their ability to assess survival was hampered by the requirement that patients who developed bone metastasis discontinue denosumab and undergo standard treatment to prevent bone-related events. "This requirement restricted our ability to evaluate overall survival with denosumab, since about 80% of the deaths occurred in patients who had discontinued the investigational product," they said.
"This same requirement also limited our ability to establish when asymptomatic bone metastases became symptomatic, since patients were removed from the study once a bone metastasis was detected and symptoms might not yet have occurred," they added.
The most common adverse events (back pain, constipation, arthralgia, diarrhea, and urinary tract infections) developed in a similar number of patients in both groups. Adverse events leading to withdrawal from the study developed in 11% of patients receiving denosumab and in 10% of those receiving placebo, a nonsignificant difference. And the rate of serious adverse events was 46% in both groups.
Denosumab was associated with an increased incidence of jaw osteonecrosis (5% vs. 0% with placebo), however, and an elevated rate of hypocalcemia (2% vs. less than 1% with placebo). Of note, the incidence of jaw necrosis increased over time from 1% in year 1 to 4% at the end of year 3, and 31 of 33 patients who developed this side effect had oral risk factors. A total of 64% of men who developed jaw necrosis required curettage and debridement, 6% required bone resection, and the remaining 30% were managed with oral rinses or antibiotics.
Denosumab specifically binds and inactivates RANK ligand, "an essential mediator of osteoclast formation, function, and survival." Activation of osteoclasts by RANK ligand is thought to promote the establishment of prostate cancer in the skeleton, and the expression of RANK ligand on prostate cancer cells may enhance the metastatic behavior of tumor cells, "with RANK ligand serving as a homing signal to bone marrow," Dr. Smith and his associates said.
Thus, "our finding that denosumab increases bone metastasis–free survival provides clinical evidence for the important role of the bone microenvironment and RANK ligand signaling in the development of bone metastases in men with prostate cancer," they noted.
Denosumab is approved as Xgeva for bone problems caused by solid tumors that have metastasized and as Prolia for osteoporosis in postmenopausal women at risk of breaking bones.
This study raises the question for clinicians of when to consider introducing denosumab for patients with prostate cancer, Dr. Christopher J. Logothetis said in an accompanying editorial (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61540-7]).
The results support the use of denosumab as an alternative to zoledronic acid, but the agent’s relatively small effect on bone metastasis–free survival and its lack of effect on overall survival "do not support its broad use as a preventive agent for bone metastases in prostate cancer," he said, urging "further investigations in this important area of research." Dr. Logothetis is chair of genitourinary medical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
Amgen funded this study, provided the denosumab, and participated in protocol design, data analysis, data interpretation, and preparation of the report. Dr. Smith and his associates reported ties to Amgen and Novartis. Dr. Logothetis reported no relevant financial disclosures.
The monoclonal antibody denosumab extended bone metastasis–free survival in an international, placebo-controlled phase III study involving 1,432 men with castration-resistant prostate cancer published online Nov. 16 in the Lancet Oncology.
Denosumab also prolonged the time to first bone metastasis and was associated with fewer symptomatic bone metastases in these high-risk patients, said Dr. Matthew R. Smith of the cancer center at the Massachusetts General Hospital, Boston, and his associates.
However, the agent did not improve overall survival, they noted.
The researchers assessed denosumab in a randomized, double-blind clinical trial conducted at 319 medical centers in 30 countries. Study subjects were men with castration-resistant prostate cancer who had no evidence of metastasis on radioisotope bone scanning, which was confirmed with subsequent imaging by CT, MRI, or plain radiography. All subjects were at high risk for disease progression based on elevated prostate-specific antigen results or short PSA doubling times.
The study subjects were randomly assigned to receive either subcutaneous denosumab 120 mg (716 patients) or placebo (716 patients) every 4 weeks until a study event (bone metastasis or death) was reached. All were strongly advised to take daily calcium and vitamin D supplements. They underwent further bone scans every 4 months to detect bone metastases.
Patients who developed a bone metastasis were discontinued from study treatment so that they could receive standard therapy, but were followed for up to an additional 3 years.
There were 605 bone metastases and 100 deaths during a median follow-up of 20 months.
The primary efficacy end point was bone metastasis–free survival. Compared with placebo, denosumab extended this end point by 4.2 months. Median bone metastasis–free survival was 29.5 months with denosumab and 25.2 months with placebo, "representing a decrease in risk of 15%," Dr. Smith and his colleagues said (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61226-9]).
The median time to bone metastasis was 33.2 months with denosumab, compared with 29.5 months with placebo. And the rate of symptomatic bone metastasis was 10% with denosumab, compared with 13% with placebo; the investigators reported a 33% reduction in the risk of symptomatic bone metastasis.
The median overall survival was similar between the two groups, however, at 43.9 months in the denosumab group and 44.8 months in the placebo group. Similarly, median progression-free survival was 21.7 months with denosumab and 19.3 months with placebo.
The investigators noted that their ability to assess survival was hampered by the requirement that patients who developed bone metastasis discontinue denosumab and undergo standard treatment to prevent bone-related events. "This requirement restricted our ability to evaluate overall survival with denosumab, since about 80% of the deaths occurred in patients who had discontinued the investigational product," they said.
"This same requirement also limited our ability to establish when asymptomatic bone metastases became symptomatic, since patients were removed from the study once a bone metastasis was detected and symptoms might not yet have occurred," they added.
The most common adverse events (back pain, constipation, arthralgia, diarrhea, and urinary tract infections) developed in a similar number of patients in both groups. Adverse events leading to withdrawal from the study developed in 11% of patients receiving denosumab and in 10% of those receiving placebo, a nonsignificant difference. And the rate of serious adverse events was 46% in both groups.
Denosumab was associated with an increased incidence of jaw osteonecrosis (5% vs. 0% with placebo), however, and an elevated rate of hypocalcemia (2% vs. less than 1% with placebo). Of note, the incidence of jaw necrosis increased over time from 1% in year 1 to 4% at the end of year 3, and 31 of 33 patients who developed this side effect had oral risk factors. A total of 64% of men who developed jaw necrosis required curettage and debridement, 6% required bone resection, and the remaining 30% were managed with oral rinses or antibiotics.
Denosumab specifically binds and inactivates RANK ligand, "an essential mediator of osteoclast formation, function, and survival." Activation of osteoclasts by RANK ligand is thought to promote the establishment of prostate cancer in the skeleton, and the expression of RANK ligand on prostate cancer cells may enhance the metastatic behavior of tumor cells, "with RANK ligand serving as a homing signal to bone marrow," Dr. Smith and his associates said.
Thus, "our finding that denosumab increases bone metastasis–free survival provides clinical evidence for the important role of the bone microenvironment and RANK ligand signaling in the development of bone metastases in men with prostate cancer," they noted.
Denosumab is approved as Xgeva for bone problems caused by solid tumors that have metastasized and as Prolia for osteoporosis in postmenopausal women at risk of breaking bones.
This study raises the question for clinicians of when to consider introducing denosumab for patients with prostate cancer, Dr. Christopher J. Logothetis said in an accompanying editorial (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61540-7]).
The results support the use of denosumab as an alternative to zoledronic acid, but the agent’s relatively small effect on bone metastasis–free survival and its lack of effect on overall survival "do not support its broad use as a preventive agent for bone metastases in prostate cancer," he said, urging "further investigations in this important area of research." Dr. Logothetis is chair of genitourinary medical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
Amgen funded this study, provided the denosumab, and participated in protocol design, data analysis, data interpretation, and preparation of the report. Dr. Smith and his associates reported ties to Amgen and Novartis. Dr. Logothetis reported no relevant financial disclosures.
The monoclonal antibody denosumab extended bone metastasis–free survival in an international, placebo-controlled phase III study involving 1,432 men with castration-resistant prostate cancer published online Nov. 16 in the Lancet Oncology.
Denosumab also prolonged the time to first bone metastasis and was associated with fewer symptomatic bone metastases in these high-risk patients, said Dr. Matthew R. Smith of the cancer center at the Massachusetts General Hospital, Boston, and his associates.
However, the agent did not improve overall survival, they noted.
The researchers assessed denosumab in a randomized, double-blind clinical trial conducted at 319 medical centers in 30 countries. Study subjects were men with castration-resistant prostate cancer who had no evidence of metastasis on radioisotope bone scanning, which was confirmed with subsequent imaging by CT, MRI, or plain radiography. All subjects were at high risk for disease progression based on elevated prostate-specific antigen results or short PSA doubling times.
The study subjects were randomly assigned to receive either subcutaneous denosumab 120 mg (716 patients) or placebo (716 patients) every 4 weeks until a study event (bone metastasis or death) was reached. All were strongly advised to take daily calcium and vitamin D supplements. They underwent further bone scans every 4 months to detect bone metastases.
Patients who developed a bone metastasis were discontinued from study treatment so that they could receive standard therapy, but were followed for up to an additional 3 years.
There were 605 bone metastases and 100 deaths during a median follow-up of 20 months.
The primary efficacy end point was bone metastasis–free survival. Compared with placebo, denosumab extended this end point by 4.2 months. Median bone metastasis–free survival was 29.5 months with denosumab and 25.2 months with placebo, "representing a decrease in risk of 15%," Dr. Smith and his colleagues said (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61226-9]).
The median time to bone metastasis was 33.2 months with denosumab, compared with 29.5 months with placebo. And the rate of symptomatic bone metastasis was 10% with denosumab, compared with 13% with placebo; the investigators reported a 33% reduction in the risk of symptomatic bone metastasis.
The median overall survival was similar between the two groups, however, at 43.9 months in the denosumab group and 44.8 months in the placebo group. Similarly, median progression-free survival was 21.7 months with denosumab and 19.3 months with placebo.
The investigators noted that their ability to assess survival was hampered by the requirement that patients who developed bone metastasis discontinue denosumab and undergo standard treatment to prevent bone-related events. "This requirement restricted our ability to evaluate overall survival with denosumab, since about 80% of the deaths occurred in patients who had discontinued the investigational product," they said.
"This same requirement also limited our ability to establish when asymptomatic bone metastases became symptomatic, since patients were removed from the study once a bone metastasis was detected and symptoms might not yet have occurred," they added.
The most common adverse events (back pain, constipation, arthralgia, diarrhea, and urinary tract infections) developed in a similar number of patients in both groups. Adverse events leading to withdrawal from the study developed in 11% of patients receiving denosumab and in 10% of those receiving placebo, a nonsignificant difference. And the rate of serious adverse events was 46% in both groups.
Denosumab was associated with an increased incidence of jaw osteonecrosis (5% vs. 0% with placebo), however, and an elevated rate of hypocalcemia (2% vs. less than 1% with placebo). Of note, the incidence of jaw necrosis increased over time from 1% in year 1 to 4% at the end of year 3, and 31 of 33 patients who developed this side effect had oral risk factors. A total of 64% of men who developed jaw necrosis required curettage and debridement, 6% required bone resection, and the remaining 30% were managed with oral rinses or antibiotics.
Denosumab specifically binds and inactivates RANK ligand, "an essential mediator of osteoclast formation, function, and survival." Activation of osteoclasts by RANK ligand is thought to promote the establishment of prostate cancer in the skeleton, and the expression of RANK ligand on prostate cancer cells may enhance the metastatic behavior of tumor cells, "with RANK ligand serving as a homing signal to bone marrow," Dr. Smith and his associates said.
Thus, "our finding that denosumab increases bone metastasis–free survival provides clinical evidence for the important role of the bone microenvironment and RANK ligand signaling in the development of bone metastases in men with prostate cancer," they noted.
Denosumab is approved as Xgeva for bone problems caused by solid tumors that have metastasized and as Prolia for osteoporosis in postmenopausal women at risk of breaking bones.
This study raises the question for clinicians of when to consider introducing denosumab for patients with prostate cancer, Dr. Christopher J. Logothetis said in an accompanying editorial (Lancet Oncol. 2011 Nov. 16 [doi:10.1016/S0140-6736(11)61540-7]).
The results support the use of denosumab as an alternative to zoledronic acid, but the agent’s relatively small effect on bone metastasis–free survival and its lack of effect on overall survival "do not support its broad use as a preventive agent for bone metastases in prostate cancer," he said, urging "further investigations in this important area of research." Dr. Logothetis is chair of genitourinary medical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
Amgen funded this study, provided the denosumab, and participated in protocol design, data analysis, data interpretation, and preparation of the report. Dr. Smith and his associates reported ties to Amgen and Novartis. Dr. Logothetis reported no relevant financial disclosures.
FROM THE LANCET ONCOLOGY
Major Finding: Median bone metastasis–free survival was 29.5 months with denosumab and 25.2 months with placebo, representing a 15% increase with the monoclonal antibody.
Data Source: An international, phase III, randomized clinical trial comparing outcomes between 716 men with castration-resistant prostate cancer who received denosumab injections vs. 716 who received placebo injections.
Disclosures: Amgen funded this study, provided the denosumab, and participated in protocol design, data analysis, data interpretation, and preparation of the report. Dr. Smith and his associates reported ties to Amgen and Novartis.
Noncathartic CT Colonography Compares Well With Colonoscopy
When members of the general population were invited to participate in colon cancer screening, many more of them agreed to noncathartic computed tomographic colonography than to colonoscopy in a study published online Nov. 15 in the Lancet Oncology.
However, colonoscopy identified more advanced neoplasias than colonography did.
These two differences "more or less cancelled each other out" in terms of the diagnostic yield, said Dr. Esther M. Stoop of Erasmus University Medical Center, Rotterdam, and her associates.
These findings indicate that both noncathartic CT colonography and colonoscopy are appropriate for population-based screening, and other factors such as cost-effectiveness must be assessed to determine which method is preferable, the authors noted.
Dr. Stoop and her colleagues compared both the participation rate and the diagnostic yield of the two strategies among average-risk people aged 50-75 years in the general population residing in the areas around Amsterdam and Rotterdam. A total of 8,844 people were randomly assigned to be invited for screening colonoscopy (5,924 subjects) or CT colonography (2,920).
The noncathartic preparation method for CT colonography consisted of consuming small amounts of iodinated contrast agent.
Participation was markedly higher for noncathartic CT colonography (34%) than for colonoscopy (22%). The total number of invitees who participated was 1,276 for colonoscopy and 982 for CT colonography.
The final completion rates for the two procedures were similar, at 99% for CT colonography and 98% for colonoscopy. Initially, 4% of the CT colonography group had incomplete procedures because of inadequate distention, inadequate tagging, or both, but the procedure was successfully repeated in all but 11. Similarly, 3% of the colonoscopy group initially had incomplete procedures because of poor bowel preparation, pain during the procedure, bowel anatomy, colonic stricture, or other reasons, but the colonoscopy was successfully repeated in all but 28.
The diagnostic yield for all advanced neoplasia was significantly higher for colonoscopy: 8.7 per 100 colonoscopy subjects versus 6.1 per 100 CT colonography patients (P = .02). But when the data were analyzed another way, the diagnostic yield was 1.9 per 100 invitees for colonoscopy and 2.1 per 100 invitees for CT colonography; this difference was not statistically significant.
The diagnostic yield for advanced neoplasias of 10 mm or more, which included all cancers, was 1.5 per 100 invitees for colonoscopy and 2.0 per 100 invitees for CT colonography.
"Given the small number of colorectal cancers detected and the size of our study group, we were unable to obtain a precise comparison of the diagnostic yield for colorectal cancers," the investigators noted (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70283-2]).
Postpolypectomy bleeding developed in two colonoscopy subjects and in three CT colonography patients when they were referred for colonoscopy because of suspicious lesions.
In addition, CT colonography identified potentially important extracolonic abnormalities in 107 subjects, including four renal cell carcinomas, one duodenal carcinoma, seven abdominal aortic aneurysms, and three smaller aneurysms.
The study was funded by the Netherlands Organisation for Health Research and Development, the Centre for Translational Molecular Medicine, and the Nuts Ohra Foundation. Study materials were provided by Guerbet, Philips Healthcare, and Norgine. The study authors stated that they had no conflicts of interest.
Stoop and colleagues show "a significant 55% improvement in screening participation with CT colonography over colonoscopy, which is a crucial component to the overall success of a screening program," said Dr. Perry J. Pickhardt.
"By offering the additional option of CT colonography for screening, overall patient outcomes will be positively affected by the equivalent (or greater) yield for advanced neoplasia, coupled with a decrease in complications and costs," he said.
Dr. Pickhardt is in gastrointestinal imaging at the University of Wisconsin-Madison. He has been a consultant for Medicsight, Viatronix, and Bracco, and is a cofounder of VirtuoCTC. These remarks were taken from his editorial comment accompanying Dr. Stoop’s report (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70297-2]).
Stoop and colleagues show "a significant 55% improvement in screening participation with CT colonography over colonoscopy, which is a crucial component to the overall success of a screening program," said Dr. Perry J. Pickhardt.
"By offering the additional option of CT colonography for screening, overall patient outcomes will be positively affected by the equivalent (or greater) yield for advanced neoplasia, coupled with a decrease in complications and costs," he said.
Dr. Pickhardt is in gastrointestinal imaging at the University of Wisconsin-Madison. He has been a consultant for Medicsight, Viatronix, and Bracco, and is a cofounder of VirtuoCTC. These remarks were taken from his editorial comment accompanying Dr. Stoop’s report (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70297-2]).
Stoop and colleagues show "a significant 55% improvement in screening participation with CT colonography over colonoscopy, which is a crucial component to the overall success of a screening program," said Dr. Perry J. Pickhardt.
"By offering the additional option of CT colonography for screening, overall patient outcomes will be positively affected by the equivalent (or greater) yield for advanced neoplasia, coupled with a decrease in complications and costs," he said.
Dr. Pickhardt is in gastrointestinal imaging at the University of Wisconsin-Madison. He has been a consultant for Medicsight, Viatronix, and Bracco, and is a cofounder of VirtuoCTC. These remarks were taken from his editorial comment accompanying Dr. Stoop’s report (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70297-2]).
When members of the general population were invited to participate in colon cancer screening, many more of them agreed to noncathartic computed tomographic colonography than to colonoscopy in a study published online Nov. 15 in the Lancet Oncology.
However, colonoscopy identified more advanced neoplasias than colonography did.
These two differences "more or less cancelled each other out" in terms of the diagnostic yield, said Dr. Esther M. Stoop of Erasmus University Medical Center, Rotterdam, and her associates.
These findings indicate that both noncathartic CT colonography and colonoscopy are appropriate for population-based screening, and other factors such as cost-effectiveness must be assessed to determine which method is preferable, the authors noted.
Dr. Stoop and her colleagues compared both the participation rate and the diagnostic yield of the two strategies among average-risk people aged 50-75 years in the general population residing in the areas around Amsterdam and Rotterdam. A total of 8,844 people were randomly assigned to be invited for screening colonoscopy (5,924 subjects) or CT colonography (2,920).
The noncathartic preparation method for CT colonography consisted of consuming small amounts of iodinated contrast agent.
Participation was markedly higher for noncathartic CT colonography (34%) than for colonoscopy (22%). The total number of invitees who participated was 1,276 for colonoscopy and 982 for CT colonography.
The final completion rates for the two procedures were similar, at 99% for CT colonography and 98% for colonoscopy. Initially, 4% of the CT colonography group had incomplete procedures because of inadequate distention, inadequate tagging, or both, but the procedure was successfully repeated in all but 11. Similarly, 3% of the colonoscopy group initially had incomplete procedures because of poor bowel preparation, pain during the procedure, bowel anatomy, colonic stricture, or other reasons, but the colonoscopy was successfully repeated in all but 28.
The diagnostic yield for all advanced neoplasia was significantly higher for colonoscopy: 8.7 per 100 colonoscopy subjects versus 6.1 per 100 CT colonography patients (P = .02). But when the data were analyzed another way, the diagnostic yield was 1.9 per 100 invitees for colonoscopy and 2.1 per 100 invitees for CT colonography; this difference was not statistically significant.
The diagnostic yield for advanced neoplasias of 10 mm or more, which included all cancers, was 1.5 per 100 invitees for colonoscopy and 2.0 per 100 invitees for CT colonography.
"Given the small number of colorectal cancers detected and the size of our study group, we were unable to obtain a precise comparison of the diagnostic yield for colorectal cancers," the investigators noted (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70283-2]).
Postpolypectomy bleeding developed in two colonoscopy subjects and in three CT colonography patients when they were referred for colonoscopy because of suspicious lesions.
In addition, CT colonography identified potentially important extracolonic abnormalities in 107 subjects, including four renal cell carcinomas, one duodenal carcinoma, seven abdominal aortic aneurysms, and three smaller aneurysms.
The study was funded by the Netherlands Organisation for Health Research and Development, the Centre for Translational Molecular Medicine, and the Nuts Ohra Foundation. Study materials were provided by Guerbet, Philips Healthcare, and Norgine. The study authors stated that they had no conflicts of interest.
When members of the general population were invited to participate in colon cancer screening, many more of them agreed to noncathartic computed tomographic colonography than to colonoscopy in a study published online Nov. 15 in the Lancet Oncology.
However, colonoscopy identified more advanced neoplasias than colonography did.
These two differences "more or less cancelled each other out" in terms of the diagnostic yield, said Dr. Esther M. Stoop of Erasmus University Medical Center, Rotterdam, and her associates.
These findings indicate that both noncathartic CT colonography and colonoscopy are appropriate for population-based screening, and other factors such as cost-effectiveness must be assessed to determine which method is preferable, the authors noted.
Dr. Stoop and her colleagues compared both the participation rate and the diagnostic yield of the two strategies among average-risk people aged 50-75 years in the general population residing in the areas around Amsterdam and Rotterdam. A total of 8,844 people were randomly assigned to be invited for screening colonoscopy (5,924 subjects) or CT colonography (2,920).
The noncathartic preparation method for CT colonography consisted of consuming small amounts of iodinated contrast agent.
Participation was markedly higher for noncathartic CT colonography (34%) than for colonoscopy (22%). The total number of invitees who participated was 1,276 for colonoscopy and 982 for CT colonography.
The final completion rates for the two procedures were similar, at 99% for CT colonography and 98% for colonoscopy. Initially, 4% of the CT colonography group had incomplete procedures because of inadequate distention, inadequate tagging, or both, but the procedure was successfully repeated in all but 11. Similarly, 3% of the colonoscopy group initially had incomplete procedures because of poor bowel preparation, pain during the procedure, bowel anatomy, colonic stricture, or other reasons, but the colonoscopy was successfully repeated in all but 28.
The diagnostic yield for all advanced neoplasia was significantly higher for colonoscopy: 8.7 per 100 colonoscopy subjects versus 6.1 per 100 CT colonography patients (P = .02). But when the data were analyzed another way, the diagnostic yield was 1.9 per 100 invitees for colonoscopy and 2.1 per 100 invitees for CT colonography; this difference was not statistically significant.
The diagnostic yield for advanced neoplasias of 10 mm or more, which included all cancers, was 1.5 per 100 invitees for colonoscopy and 2.0 per 100 invitees for CT colonography.
"Given the small number of colorectal cancers detected and the size of our study group, we were unable to obtain a precise comparison of the diagnostic yield for colorectal cancers," the investigators noted (Lancet Oncol. 2011 Nov. 15 [doi:10.1016/S1470-2045(11)70283-2]).
Postpolypectomy bleeding developed in two colonoscopy subjects and in three CT colonography patients when they were referred for colonoscopy because of suspicious lesions.
In addition, CT colonography identified potentially important extracolonic abnormalities in 107 subjects, including four renal cell carcinomas, one duodenal carcinoma, seven abdominal aortic aneurysms, and three smaller aneurysms.
The study was funded by the Netherlands Organisation for Health Research and Development, the Centre for Translational Molecular Medicine, and the Nuts Ohra Foundation. Study materials were provided by Guerbet, Philips Healthcare, and Norgine. The study authors stated that they had no conflicts of interest.
FROM THE LANCET ONCOLOGY
Major Finding: The rate of detection of advanced neoplasia was 8.7 per 100 colonoscopy subjects and 6.1 per 100 CT colonography patients; however, the diagnostic yield was 1.9 per 100 invitees for colonoscopy and 2.1 per 100 invitees for CT colonography.
Data Source: A population-based randomized study of residents of Rotterdam and Amsterdam aged 50-75 years who were invited to undergo primary colorectal cancer screening by either colonoscopy (5,924 subjects) or CT colonography (2,920 subjects) during a 1-year period.
Disclosures: This study was funded by the Netherlands Organisation for Health Research and Development, the Centre for Translational Molecular Medicine, and the Nuts Ohra Foundation. Study materials were provided by Guerbet, Philips Healthcare, and Norgine. No financial conflicts of interest were reported.
Weight Loss Modest With Primary Care Program
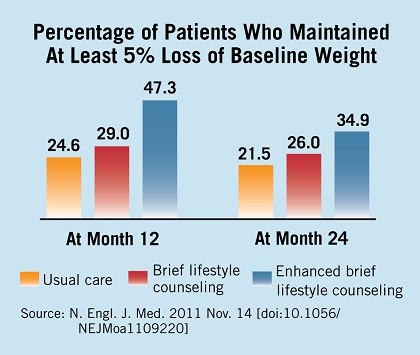
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than did either brief lifestyle counseling (2.9 kg) or usual care (1.7 kg).
Data Source: A randomized clinical trial comparing weight loss in 390 obese patients after 2 years of usual care, brief lifestyle counseling, and enhanced lifestyle counseling delivered by a primary care physician and staff medical assistants.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Earlier Liver Transplant Improves Survival in Alcoholic Hepatitis
Performing liver transplantation early in patients with severe alcoholic hepatitis unresponsive to medical therapy, rather than requiring that they demonstrate 6 months of sobriety before transplantation, improves their survival, according to a Nov. 10 report in the New England Journal of Medicine.
Six-month survival was 77% in a study of such patients who underwent early transplantation, compared with only 23% among matched control subjects who did not, said Dr. Philippe Mathurin of Hôpital Claude Huriez and Université Lille Nord de France, and his associates.
There were no alcoholic relapses during that 6 months. However, 3 of the 26 transplant patients resumed alcohol use during an extended 2-year follow-up; none of them developed graft dysfunction.
"Our findings challenge both the notion of a prescribed abstinence period as the only alcoholism-related criterion for transplant eligibility and the opinion of experts that alcoholic hepatitis is a contraindication for transplantation," the investigators noted.
Liver transplantation for alcoholic hepatitis usually has a favorable outcome but is controversial. Among those who oppose it, clinicians tend to think that the patient will resume drinking and eventually destroy the graft, and the public tends to prefer alloting scarce donor livers to nonalcoholic patients whom they perceive as more deserving.
The requirement that patients with severe alcoholic hepatitis demonstrate 6 months of sobriety is recognized as an arbitrary constraint, since the duration of abstinence is known to be a poor predictor of relapse of alcoholism. And 70%-80% of such patients die during that mandated interval.
Dr. Mathurin and his colleagues performed a comparative study to determine whether earlier transplantation would improve 6-month survival in patients whose severe alcoholic hepatitis was nonresponsive to medical management. They recruited patients at seven transplant centers in France.
A total of 26 patients were selected using very strict criteria to undergo early transplant. They were eligible only if the hepatitis was their first liver-decompensating event, if they had a good support network of family and friends, if they had no concomitant psychiatric disorders, and if they agreed to lifelong total alcohol abstinence.
"The stringency of our selection process resulted in our selecting a very small number of patients with alcoholic hepatitis for early transplantation" from a large pool of potential transplant recipients, the researchers noted.
The transplant patients were matched for age, sex, Maddrey’s discriminant function (a measure of liver disease severity), and Lille score (a predictor of likeliness to respond to medical therapy) to 26 control subjects.
Six-month survival was significantly higher among the transplant patients (77%) than among the controls (23%).
Eighteen of the 20 deaths among the control subjects (90%) occurred within 2 months of discovery that they were not responding to medical management – that is, well before the 6-month abstinence period had elapsed, the investigators said (N. Engl. J. Med. 2011;365:1790-1800).
When follow-up was extended to 2 years, early transplantation remained associated with significantly improved survival (72%), compared with control subjects (23%).
Investigators had also sought to measure the rate of posttransplantation alcohol relapse in patients selected free of the 6-month rule. None of the transplant recipients resumed drinking during the 6-month follow-up, but three did so later, at 720 days, 740 days, and 1,140 days. None of these three grafts has yet demonstrated dysfunction.
"Previous studies of patients with alcoholism who underwent transplantation suggest that the rate of relapse over the long term may be approximately 25%-35%," Dr. Mathurin and his associates noted.
In weighing the burden of early transplantation on the overall transplantation activity of participating centers, investigators said that only 2.9% of the grafts used during the study period were for early liver transplantation. While some observers contend that the public may be less willing to donate if guidelines are modified regarding alcoholic patients, the authors said that has not happened where transplantation is offered to intravenous drug users or patients who have voluntarily overdosed on acetaminophen.
The findings show that "early liver transplantation may be an appropriate rescue option for selected patients whose first episode of severe alcoholic hepatitis is not responsive to medical therapy, after careful assessment of their addiction profile," the investigators said.
This study was supported by the Société Nationale Française de Gastroentérologie. Dr. Mathurin and his associates reported numerous ties to industry sources.
The argument against allowing patients with severe alcoholic hepatitis to receive liver transplants – that alcoholism is self-inflicted – is invalid. "Alcoholism is a disease, and it should not be used to exclude patients from transplantation," said Dr. Robert S. Brown Jr.
"When one looks at the causes of liver disease, much of it could be perceived as self-inflicted, such as prior drug use resulting in viral hepatitis or obesity leading to NAFLD," he noted.
"I do think this study highlights the need to rethink our approach to transplantation for alcoholic liver disease, including applying better rules for selecting patients who are at low risk for recidivism that can be applied in a uniform and fair way."
Dr. Brown is at the Center for Liver Disease and Transplantation at Columbia University College of Physicians and Surgeons, New York. He reported having no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Mathurin’s report (N. Engl. J. Med. 2011;365:1836-8).
The argument against allowing patients with severe alcoholic hepatitis to receive liver transplants – that alcoholism is self-inflicted – is invalid. "Alcoholism is a disease, and it should not be used to exclude patients from transplantation," said Dr. Robert S. Brown Jr.
"When one looks at the causes of liver disease, much of it could be perceived as self-inflicted, such as prior drug use resulting in viral hepatitis or obesity leading to NAFLD," he noted.
"I do think this study highlights the need to rethink our approach to transplantation for alcoholic liver disease, including applying better rules for selecting patients who are at low risk for recidivism that can be applied in a uniform and fair way."
Dr. Brown is at the Center for Liver Disease and Transplantation at Columbia University College of Physicians and Surgeons, New York. He reported having no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Mathurin’s report (N. Engl. J. Med. 2011;365:1836-8).
The argument against allowing patients with severe alcoholic hepatitis to receive liver transplants – that alcoholism is self-inflicted – is invalid. "Alcoholism is a disease, and it should not be used to exclude patients from transplantation," said Dr. Robert S. Brown Jr.
"When one looks at the causes of liver disease, much of it could be perceived as self-inflicted, such as prior drug use resulting in viral hepatitis or obesity leading to NAFLD," he noted.
"I do think this study highlights the need to rethink our approach to transplantation for alcoholic liver disease, including applying better rules for selecting patients who are at low risk for recidivism that can be applied in a uniform and fair way."
Dr. Brown is at the Center for Liver Disease and Transplantation at Columbia University College of Physicians and Surgeons, New York. He reported having no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Mathurin’s report (N. Engl. J. Med. 2011;365:1836-8).
Performing liver transplantation early in patients with severe alcoholic hepatitis unresponsive to medical therapy, rather than requiring that they demonstrate 6 months of sobriety before transplantation, improves their survival, according to a Nov. 10 report in the New England Journal of Medicine.
Six-month survival was 77% in a study of such patients who underwent early transplantation, compared with only 23% among matched control subjects who did not, said Dr. Philippe Mathurin of Hôpital Claude Huriez and Université Lille Nord de France, and his associates.
There were no alcoholic relapses during that 6 months. However, 3 of the 26 transplant patients resumed alcohol use during an extended 2-year follow-up; none of them developed graft dysfunction.
"Our findings challenge both the notion of a prescribed abstinence period as the only alcoholism-related criterion for transplant eligibility and the opinion of experts that alcoholic hepatitis is a contraindication for transplantation," the investigators noted.
Liver transplantation for alcoholic hepatitis usually has a favorable outcome but is controversial. Among those who oppose it, clinicians tend to think that the patient will resume drinking and eventually destroy the graft, and the public tends to prefer alloting scarce donor livers to nonalcoholic patients whom they perceive as more deserving.
The requirement that patients with severe alcoholic hepatitis demonstrate 6 months of sobriety is recognized as an arbitrary constraint, since the duration of abstinence is known to be a poor predictor of relapse of alcoholism. And 70%-80% of such patients die during that mandated interval.
Dr. Mathurin and his colleagues performed a comparative study to determine whether earlier transplantation would improve 6-month survival in patients whose severe alcoholic hepatitis was nonresponsive to medical management. They recruited patients at seven transplant centers in France.
A total of 26 patients were selected using very strict criteria to undergo early transplant. They were eligible only if the hepatitis was their first liver-decompensating event, if they had a good support network of family and friends, if they had no concomitant psychiatric disorders, and if they agreed to lifelong total alcohol abstinence.
"The stringency of our selection process resulted in our selecting a very small number of patients with alcoholic hepatitis for early transplantation" from a large pool of potential transplant recipients, the researchers noted.
The transplant patients were matched for age, sex, Maddrey’s discriminant function (a measure of liver disease severity), and Lille score (a predictor of likeliness to respond to medical therapy) to 26 control subjects.
Six-month survival was significantly higher among the transplant patients (77%) than among the controls (23%).
Eighteen of the 20 deaths among the control subjects (90%) occurred within 2 months of discovery that they were not responding to medical management – that is, well before the 6-month abstinence period had elapsed, the investigators said (N. Engl. J. Med. 2011;365:1790-1800).
When follow-up was extended to 2 years, early transplantation remained associated with significantly improved survival (72%), compared with control subjects (23%).
Investigators had also sought to measure the rate of posttransplantation alcohol relapse in patients selected free of the 6-month rule. None of the transplant recipients resumed drinking during the 6-month follow-up, but three did so later, at 720 days, 740 days, and 1,140 days. None of these three grafts has yet demonstrated dysfunction.
"Previous studies of patients with alcoholism who underwent transplantation suggest that the rate of relapse over the long term may be approximately 25%-35%," Dr. Mathurin and his associates noted.
In weighing the burden of early transplantation on the overall transplantation activity of participating centers, investigators said that only 2.9% of the grafts used during the study period were for early liver transplantation. While some observers contend that the public may be less willing to donate if guidelines are modified regarding alcoholic patients, the authors said that has not happened where transplantation is offered to intravenous drug users or patients who have voluntarily overdosed on acetaminophen.
The findings show that "early liver transplantation may be an appropriate rescue option for selected patients whose first episode of severe alcoholic hepatitis is not responsive to medical therapy, after careful assessment of their addiction profile," the investigators said.
This study was supported by the Société Nationale Française de Gastroentérologie. Dr. Mathurin and his associates reported numerous ties to industry sources.
Performing liver transplantation early in patients with severe alcoholic hepatitis unresponsive to medical therapy, rather than requiring that they demonstrate 6 months of sobriety before transplantation, improves their survival, according to a Nov. 10 report in the New England Journal of Medicine.
Six-month survival was 77% in a study of such patients who underwent early transplantation, compared with only 23% among matched control subjects who did not, said Dr. Philippe Mathurin of Hôpital Claude Huriez and Université Lille Nord de France, and his associates.
There were no alcoholic relapses during that 6 months. However, 3 of the 26 transplant patients resumed alcohol use during an extended 2-year follow-up; none of them developed graft dysfunction.
"Our findings challenge both the notion of a prescribed abstinence period as the only alcoholism-related criterion for transplant eligibility and the opinion of experts that alcoholic hepatitis is a contraindication for transplantation," the investigators noted.
Liver transplantation for alcoholic hepatitis usually has a favorable outcome but is controversial. Among those who oppose it, clinicians tend to think that the patient will resume drinking and eventually destroy the graft, and the public tends to prefer alloting scarce donor livers to nonalcoholic patients whom they perceive as more deserving.
The requirement that patients with severe alcoholic hepatitis demonstrate 6 months of sobriety is recognized as an arbitrary constraint, since the duration of abstinence is known to be a poor predictor of relapse of alcoholism. And 70%-80% of such patients die during that mandated interval.
Dr. Mathurin and his colleagues performed a comparative study to determine whether earlier transplantation would improve 6-month survival in patients whose severe alcoholic hepatitis was nonresponsive to medical management. They recruited patients at seven transplant centers in France.
A total of 26 patients were selected using very strict criteria to undergo early transplant. They were eligible only if the hepatitis was their first liver-decompensating event, if they had a good support network of family and friends, if they had no concomitant psychiatric disorders, and if they agreed to lifelong total alcohol abstinence.
"The stringency of our selection process resulted in our selecting a very small number of patients with alcoholic hepatitis for early transplantation" from a large pool of potential transplant recipients, the researchers noted.
The transplant patients were matched for age, sex, Maddrey’s discriminant function (a measure of liver disease severity), and Lille score (a predictor of likeliness to respond to medical therapy) to 26 control subjects.
Six-month survival was significantly higher among the transplant patients (77%) than among the controls (23%).
Eighteen of the 20 deaths among the control subjects (90%) occurred within 2 months of discovery that they were not responding to medical management – that is, well before the 6-month abstinence period had elapsed, the investigators said (N. Engl. J. Med. 2011;365:1790-1800).
When follow-up was extended to 2 years, early transplantation remained associated with significantly improved survival (72%), compared with control subjects (23%).
Investigators had also sought to measure the rate of posttransplantation alcohol relapse in patients selected free of the 6-month rule. None of the transplant recipients resumed drinking during the 6-month follow-up, but three did so later, at 720 days, 740 days, and 1,140 days. None of these three grafts has yet demonstrated dysfunction.
"Previous studies of patients with alcoholism who underwent transplantation suggest that the rate of relapse over the long term may be approximately 25%-35%," Dr. Mathurin and his associates noted.
In weighing the burden of early transplantation on the overall transplantation activity of participating centers, investigators said that only 2.9% of the grafts used during the study period were for early liver transplantation. While some observers contend that the public may be less willing to donate if guidelines are modified regarding alcoholic patients, the authors said that has not happened where transplantation is offered to intravenous drug users or patients who have voluntarily overdosed on acetaminophen.
The findings show that "early liver transplantation may be an appropriate rescue option for selected patients whose first episode of severe alcoholic hepatitis is not responsive to medical therapy, after careful assessment of their addiction profile," the investigators said.
This study was supported by the Société Nationale Française de Gastroentérologie. Dr. Mathurin and his associates reported numerous ties to industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Six-month survival was significantly higher among transplant recipients (77%) than among control subjects (23%).
Data Source: A prospective multicenter case-control study of 26 patients with severe alcoholic hepatitis resistant to medical therapy who underwent early liver transplant at seven French medical centers and 26 matched control subjects who did not.
Disclosures: This study was supported by the Société Nationale Française de Gastroentérologie. Dr. Mathurin and his associates reported numerous ties to industry sources.
Alcoholic Hepatitis Survival No Better With N-acetylcysteine
Adding N-acetylcysteine to prednisolone therapy failed to significantly improve 6-month survival in patients who had severe acute alcoholic hepatitis, according to a report in the Nov. 10 New England Journal of Medicine.
The combination therapy did improve 1-month survival compared with standard prednisolone treatment alone, but that benefit did not persist, said Dr. Eric Nguyen-Khac of Amiens (France) University Hospital, and his associates.
Severe acute alcoholic hepatitis is accompanied by mitochondrial depletion of glutathione, a major cellular antioxidant. Researchers have proposed that adding an antioxidant such as N-acetylcysteine to standard glucocorticoid therapy for this condition "would have the advantage of both acting on the inflammatory process and reconstituting cellular glutathione reserves," Dr. Nguyen-Khac and his colleagues said (N. Engl. J. Med. 2011;365:1,781-9).
In addition, N-acetylcysteine has been shown to protect the liver in chronic alcoholic hepatitis and in mouse models of acute alcoholic hepatitis.
The investigators tested this theory in a trial involving 180 patients treated over a 5-year period at 11 university hospitals in France. Study subjects were randomly assigned to receive oral prednisolone plus 5 days of intravenous N-acetylcysteine (89 patients) or oral prednisolone plus 5 days of intravenous glucose solution (91 patients serving as controls) and were followed at intervals for 6 months.
All study subjects were allowed concomitant therapy with diuretics, albumin, and sodium restriction for ascites and with beta-blockers for portal hypertension, as needed. A total of 57 subjects died during the study.
The final analysis included 174 study subjects. The primary end point, mortality at 6 months, occurred among 23 of 85 patients (27%) in the combined-therapy group and 34 of 89 patients (38%) in the control group, a difference that was not significant.
A secondary end point, mortality at 1 month, was significantly better with combined therapy (7 of 85 patients, or 8%) than with prednisolone alone (21 of 89 patients, or 24%).
The researchers noted that the study may have lacked sufficient power to detect a significant difference at 6 months. "It is also possible that 5 days of N-acetylcysteine was not enough. A longer period of intravenous N-acetylcysteine combined with prednisolone could perhaps be considered, with subsequent oral administration of N-acetylcysteine until 1 month," they said.
Regarding adverse events at 6 months, the rate of hepatorenal syndrome was 12% with combined therapy and 25% in the control group; that of infection was 19% with combined therapy and 42% in the control group. Other complications did not differ between the two groups.
This study was supported by Programme Hospitalier de Recherche Clinique. No conflicts of interest were reported.
Adding N-acetylcysteine to prednisolone therapy failed to significantly improve 6-month survival in patients who had severe acute alcoholic hepatitis, according to a report in the Nov. 10 New England Journal of Medicine.
The combination therapy did improve 1-month survival compared with standard prednisolone treatment alone, but that benefit did not persist, said Dr. Eric Nguyen-Khac of Amiens (France) University Hospital, and his associates.
Severe acute alcoholic hepatitis is accompanied by mitochondrial depletion of glutathione, a major cellular antioxidant. Researchers have proposed that adding an antioxidant such as N-acetylcysteine to standard glucocorticoid therapy for this condition "would have the advantage of both acting on the inflammatory process and reconstituting cellular glutathione reserves," Dr. Nguyen-Khac and his colleagues said (N. Engl. J. Med. 2011;365:1,781-9).
In addition, N-acetylcysteine has been shown to protect the liver in chronic alcoholic hepatitis and in mouse models of acute alcoholic hepatitis.
The investigators tested this theory in a trial involving 180 patients treated over a 5-year period at 11 university hospitals in France. Study subjects were randomly assigned to receive oral prednisolone plus 5 days of intravenous N-acetylcysteine (89 patients) or oral prednisolone plus 5 days of intravenous glucose solution (91 patients serving as controls) and were followed at intervals for 6 months.
All study subjects were allowed concomitant therapy with diuretics, albumin, and sodium restriction for ascites and with beta-blockers for portal hypertension, as needed. A total of 57 subjects died during the study.
The final analysis included 174 study subjects. The primary end point, mortality at 6 months, occurred among 23 of 85 patients (27%) in the combined-therapy group and 34 of 89 patients (38%) in the control group, a difference that was not significant.
A secondary end point, mortality at 1 month, was significantly better with combined therapy (7 of 85 patients, or 8%) than with prednisolone alone (21 of 89 patients, or 24%).
The researchers noted that the study may have lacked sufficient power to detect a significant difference at 6 months. "It is also possible that 5 days of N-acetylcysteine was not enough. A longer period of intravenous N-acetylcysteine combined with prednisolone could perhaps be considered, with subsequent oral administration of N-acetylcysteine until 1 month," they said.
Regarding adverse events at 6 months, the rate of hepatorenal syndrome was 12% with combined therapy and 25% in the control group; that of infection was 19% with combined therapy and 42% in the control group. Other complications did not differ between the two groups.
This study was supported by Programme Hospitalier de Recherche Clinique. No conflicts of interest were reported.
Adding N-acetylcysteine to prednisolone therapy failed to significantly improve 6-month survival in patients who had severe acute alcoholic hepatitis, according to a report in the Nov. 10 New England Journal of Medicine.
The combination therapy did improve 1-month survival compared with standard prednisolone treatment alone, but that benefit did not persist, said Dr. Eric Nguyen-Khac of Amiens (France) University Hospital, and his associates.
Severe acute alcoholic hepatitis is accompanied by mitochondrial depletion of glutathione, a major cellular antioxidant. Researchers have proposed that adding an antioxidant such as N-acetylcysteine to standard glucocorticoid therapy for this condition "would have the advantage of both acting on the inflammatory process and reconstituting cellular glutathione reserves," Dr. Nguyen-Khac and his colleagues said (N. Engl. J. Med. 2011;365:1,781-9).
In addition, N-acetylcysteine has been shown to protect the liver in chronic alcoholic hepatitis and in mouse models of acute alcoholic hepatitis.
The investigators tested this theory in a trial involving 180 patients treated over a 5-year period at 11 university hospitals in France. Study subjects were randomly assigned to receive oral prednisolone plus 5 days of intravenous N-acetylcysteine (89 patients) or oral prednisolone plus 5 days of intravenous glucose solution (91 patients serving as controls) and were followed at intervals for 6 months.
All study subjects were allowed concomitant therapy with diuretics, albumin, and sodium restriction for ascites and with beta-blockers for portal hypertension, as needed. A total of 57 subjects died during the study.
The final analysis included 174 study subjects. The primary end point, mortality at 6 months, occurred among 23 of 85 patients (27%) in the combined-therapy group and 34 of 89 patients (38%) in the control group, a difference that was not significant.
A secondary end point, mortality at 1 month, was significantly better with combined therapy (7 of 85 patients, or 8%) than with prednisolone alone (21 of 89 patients, or 24%).
The researchers noted that the study may have lacked sufficient power to detect a significant difference at 6 months. "It is also possible that 5 days of N-acetylcysteine was not enough. A longer period of intravenous N-acetylcysteine combined with prednisolone could perhaps be considered, with subsequent oral administration of N-acetylcysteine until 1 month," they said.
Regarding adverse events at 6 months, the rate of hepatorenal syndrome was 12% with combined therapy and 25% in the control group; that of infection was 19% with combined therapy and 42% in the control group. Other complications did not differ between the two groups.
This study was supported by Programme Hospitalier de Recherche Clinique. No conflicts of interest were reported.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Six-month mortality was not significantly better among patients who had severe alcoholic hepatitis treated with prednisolone plus N-acetylcysteine (27%), compared with those given prednisolone only (38%).
Data Source: A prospective multicenter randomized controlled trial involving 180 patients in France.
Disclosures: This study was supported by Programme Hospitalier de Recherche Clinique. No conflicts of interest were reported.
Autistic Brains Have an Excess of Prefrontal Neurons
Brains from seven boys with autism had a mean of 67% more neurons in the dorsolateral and mesial prefrontal cortex than did those of six age-matched control subjects in a postmortem study reported in the Nov. 9 issue of JAMA.
"To our knowledge, this study is the first direct quantitative test and confirmation of the theory that a pathological overabundance of neurons in critical brain regions is present at a young age in autism," said Eric Courchesne, Ph.D., of the department of neuroscience, National Institutes of Health–University of California, San Diego, Autism Center of Excellence, University of California San Diego, La Jolla, and his associates.
"Because cortical neurons are generated in prenatal, not postnatal life, pathological overabundance of neurons indicates early developmental disturbances in molecular and genetic mechanisms that govern proliferation, cell cycle regulation, and apoptosis," they noted (JAMA 2011;306:2001-10).
Among autistic children, brain overgrowth (excess weight and size) and neuronal dysfunction have long been observed in many regions involved in higher-order social, emotional, communication, and cognitive development. But the neural basis of these abnormalities was unknown because it could only be explored in "direct quantitative studies of the young postmortem autistic brain" – specimens that are very rarely available.
Dr. Courchesne and his colleagues were able to perform such a study when they received access to entire dorsolateral and mesial sections of the prefrontal cortex in seven autistic and six control male subjects who had been aged 2-16 years when they died. Valid cell counts cannot be obtained using density estimates from small blocks of cortical tissue, the researchers explained.
They used stereological methods to count neurons, sampling 100 or more locations within 8-12 sections per reference space, and they calculated the total number of neurons using the optical fractionator method. Neurons were distinguished from microglia and satellite oligodendrocytes by doing detailed morphological examination, not just by estimating cell size.
The control cases were free of mental illness, intellectual disability, and neurological disorders. The autistic cases displayed a wide range of intellectual abilities, social skills, communication abilities, and functional impairments. All had been born at term after unremarkable perinatal courses.
Most of the study subjects had died of acute global ischemic hypoxia from accidental trauma (drowning, hanging, or electrocution); 1 died in a car accident, 1 of rhabdomyosarcoma, and 1 of possible cardiac arrest.
There had been no abnormalities on gross examination of most of the brains, according to medical examiner or neuropathology reports. The mean weight of autistic brains was 1,484 g, and was 17.6% greater than the normative mean weight for same-aged subjects reported in the literature. The control brains were significantly lighter and deviated from the norm by only 0.2%.
There were 79% more neurons in the dorsolateral prefrontal cortex among autistic brains than control brains, and 29% more neurons in the mesial prefrontal cortex. "Together, these 2 subdivisions gave a total combined prefrontal neuron count that was 67% greater in the autistic children (mean, 1.94 billion) compared with controls (mean, 1.16 billion)," Dr. Courchesne and his associates said.
This significant difference remained robust when the data were adjusted to account for subject age and postmortem interval.
The greater excess of neurons in the dorsolateral than in the mesial prefrontal cortex "parallels MRI volumetric data showing greater deviance in the dorsolateral prefrontal cortex than the mesial prefrontal cortex in living autistic toddlers," the investigators said.
Moreover, "these global increases in prefrontal neuron numbers were not apparent either at low or high magnification, and thus [were] undetectable by neuropathology visual inspection and neuron density measurement without formal quantitative stereological procedures," they noted.
There were no differences between autistic and control brains in the size of neurons, nor in counts of glial cells in the same brain regions.
It remains to be determined whether excess numbers of neurons occur in other regions of the brain besides "these two major prefrontal subdivisions," they added.
As has been noted in previous studies, this study found that the average weight of the autistic brains was heaver than that of the control brains. This indicates that the pathological increase in neuron numbers may be an important contributor to the brain overgrowth that has long been known to occur in autism.
However, the autistic brains did not show the linear correlation between number of neurons and brain weight that has been described in normal brains and was found in the control brains in this study. "Neuron counts in the autistic children should have been accompanied by brain weights considerably larger than was observed, reaching 29.4% enlargement rather than the observed 17.6% enlargement. Thus, the size of the autistic brain, overlarge as it is, might actually underestimate the pathology of excess neuron numbers," Dr. Courchesne and his colleagues noted.
"It would be invaluable to study larger samples of autistic and control cases at a younger and narrower age range to confirm excess counts in autism at the youngest ages, as well as to study larger samples across a wider age range to identify patterns of age-related changes in autism. It [also] will be important to include female cases in future studies, as etiological mechanisms may be discordant between the sexes," they said.
Future studies with a greater number of subjects also would allow researchers to explore relationships between brain morphology and behavior, possibly revealing whether neuron counts relate to symptom severity or intellectual ability, they added.
This study was supported by Autism Speaks, Cure Autism Now, the Peter Emch Family Foundation, the Simons Foundation, and the Thursday Club Juniors. Also, a grant from the National Institutes of Health–University of California, San Diego Autism Center of Excellence was awarded to Dr. Courchesne and a National Institute of Mental Health grant was awarded to Dr. Courchesne’s associated Dr. Peter R. Moulton. Brain specimens were provided by the National Institute of Child Health and Human Development Brain and Tissue Bank for Developmental Disorders, Autism Tissue Program, and direct donations to the Courchesne laboratory. Dr. Courchesne’s associate, Dr. Michael E. Calhoun, is the principal owner of Sinq Systems, a contract research organization that performed data collection and analysis for this study and he is an applicant on a pending patent on file with the U.S. Patent and Trademark Office related to analysis of microscopic structure.
These findings "add significantly to the mounting biological evidence that the developmental neuropathology of idiopathic autism begins before birth in some, possibly all, cases," said Dr. Janet E. Lainhart and Nicholas Lange, Sc.D.
"Factors that normally organize the brain appear to be disrupted," they said.
Regions of the brain other than the prefrontal cortex, such as the temporal lobes, also deserve investigation by postmortem tissue analysis, they added.
Dr. Lainhart is in the departments of psychiatry, pediatrics, and neuroscience at the University of Utah’s Brain Institute, Salt Lake City. Dr. Lange is in the departments of psychiatry and biostatistics at Harvard University Schools of Medicine and Public Health, Boston. Both reported no relevant financial disclosures. These remarks were taken from their editorial accompanying Dr. Courchesne’s report (JAMA 2011;306:2031-2).
These findings "add significantly to the mounting biological evidence that the developmental neuropathology of idiopathic autism begins before birth in some, possibly all, cases," said Dr. Janet E. Lainhart and Nicholas Lange, Sc.D.
"Factors that normally organize the brain appear to be disrupted," they said.
Regions of the brain other than the prefrontal cortex, such as the temporal lobes, also deserve investigation by postmortem tissue analysis, they added.
Dr. Lainhart is in the departments of psychiatry, pediatrics, and neuroscience at the University of Utah’s Brain Institute, Salt Lake City. Dr. Lange is in the departments of psychiatry and biostatistics at Harvard University Schools of Medicine and Public Health, Boston. Both reported no relevant financial disclosures. These remarks were taken from their editorial accompanying Dr. Courchesne’s report (JAMA 2011;306:2031-2).
These findings "add significantly to the mounting biological evidence that the developmental neuropathology of idiopathic autism begins before birth in some, possibly all, cases," said Dr. Janet E. Lainhart and Nicholas Lange, Sc.D.
"Factors that normally organize the brain appear to be disrupted," they said.
Regions of the brain other than the prefrontal cortex, such as the temporal lobes, also deserve investigation by postmortem tissue analysis, they added.
Dr. Lainhart is in the departments of psychiatry, pediatrics, and neuroscience at the University of Utah’s Brain Institute, Salt Lake City. Dr. Lange is in the departments of psychiatry and biostatistics at Harvard University Schools of Medicine and Public Health, Boston. Both reported no relevant financial disclosures. These remarks were taken from their editorial accompanying Dr. Courchesne’s report (JAMA 2011;306:2031-2).
Brains from seven boys with autism had a mean of 67% more neurons in the dorsolateral and mesial prefrontal cortex than did those of six age-matched control subjects in a postmortem study reported in the Nov. 9 issue of JAMA.
"To our knowledge, this study is the first direct quantitative test and confirmation of the theory that a pathological overabundance of neurons in critical brain regions is present at a young age in autism," said Eric Courchesne, Ph.D., of the department of neuroscience, National Institutes of Health–University of California, San Diego, Autism Center of Excellence, University of California San Diego, La Jolla, and his associates.
"Because cortical neurons are generated in prenatal, not postnatal life, pathological overabundance of neurons indicates early developmental disturbances in molecular and genetic mechanisms that govern proliferation, cell cycle regulation, and apoptosis," they noted (JAMA 2011;306:2001-10).
Among autistic children, brain overgrowth (excess weight and size) and neuronal dysfunction have long been observed in many regions involved in higher-order social, emotional, communication, and cognitive development. But the neural basis of these abnormalities was unknown because it could only be explored in "direct quantitative studies of the young postmortem autistic brain" – specimens that are very rarely available.
Dr. Courchesne and his colleagues were able to perform such a study when they received access to entire dorsolateral and mesial sections of the prefrontal cortex in seven autistic and six control male subjects who had been aged 2-16 years when they died. Valid cell counts cannot be obtained using density estimates from small blocks of cortical tissue, the researchers explained.
They used stereological methods to count neurons, sampling 100 or more locations within 8-12 sections per reference space, and they calculated the total number of neurons using the optical fractionator method. Neurons were distinguished from microglia and satellite oligodendrocytes by doing detailed morphological examination, not just by estimating cell size.
The control cases were free of mental illness, intellectual disability, and neurological disorders. The autistic cases displayed a wide range of intellectual abilities, social skills, communication abilities, and functional impairments. All had been born at term after unremarkable perinatal courses.
Most of the study subjects had died of acute global ischemic hypoxia from accidental trauma (drowning, hanging, or electrocution); 1 died in a car accident, 1 of rhabdomyosarcoma, and 1 of possible cardiac arrest.
There had been no abnormalities on gross examination of most of the brains, according to medical examiner or neuropathology reports. The mean weight of autistic brains was 1,484 g, and was 17.6% greater than the normative mean weight for same-aged subjects reported in the literature. The control brains were significantly lighter and deviated from the norm by only 0.2%.
There were 79% more neurons in the dorsolateral prefrontal cortex among autistic brains than control brains, and 29% more neurons in the mesial prefrontal cortex. "Together, these 2 subdivisions gave a total combined prefrontal neuron count that was 67% greater in the autistic children (mean, 1.94 billion) compared with controls (mean, 1.16 billion)," Dr. Courchesne and his associates said.
This significant difference remained robust when the data were adjusted to account for subject age and postmortem interval.
The greater excess of neurons in the dorsolateral than in the mesial prefrontal cortex "parallels MRI volumetric data showing greater deviance in the dorsolateral prefrontal cortex than the mesial prefrontal cortex in living autistic toddlers," the investigators said.
Moreover, "these global increases in prefrontal neuron numbers were not apparent either at low or high magnification, and thus [were] undetectable by neuropathology visual inspection and neuron density measurement without formal quantitative stereological procedures," they noted.
There were no differences between autistic and control brains in the size of neurons, nor in counts of glial cells in the same brain regions.
It remains to be determined whether excess numbers of neurons occur in other regions of the brain besides "these two major prefrontal subdivisions," they added.
As has been noted in previous studies, this study found that the average weight of the autistic brains was heaver than that of the control brains. This indicates that the pathological increase in neuron numbers may be an important contributor to the brain overgrowth that has long been known to occur in autism.
However, the autistic brains did not show the linear correlation between number of neurons and brain weight that has been described in normal brains and was found in the control brains in this study. "Neuron counts in the autistic children should have been accompanied by brain weights considerably larger than was observed, reaching 29.4% enlargement rather than the observed 17.6% enlargement. Thus, the size of the autistic brain, overlarge as it is, might actually underestimate the pathology of excess neuron numbers," Dr. Courchesne and his colleagues noted.
"It would be invaluable to study larger samples of autistic and control cases at a younger and narrower age range to confirm excess counts in autism at the youngest ages, as well as to study larger samples across a wider age range to identify patterns of age-related changes in autism. It [also] will be important to include female cases in future studies, as etiological mechanisms may be discordant between the sexes," they said.
Future studies with a greater number of subjects also would allow researchers to explore relationships between brain morphology and behavior, possibly revealing whether neuron counts relate to symptom severity or intellectual ability, they added.
This study was supported by Autism Speaks, Cure Autism Now, the Peter Emch Family Foundation, the Simons Foundation, and the Thursday Club Juniors. Also, a grant from the National Institutes of Health–University of California, San Diego Autism Center of Excellence was awarded to Dr. Courchesne and a National Institute of Mental Health grant was awarded to Dr. Courchesne’s associated Dr. Peter R. Moulton. Brain specimens were provided by the National Institute of Child Health and Human Development Brain and Tissue Bank for Developmental Disorders, Autism Tissue Program, and direct donations to the Courchesne laboratory. Dr. Courchesne’s associate, Dr. Michael E. Calhoun, is the principal owner of Sinq Systems, a contract research organization that performed data collection and analysis for this study and he is an applicant on a pending patent on file with the U.S. Patent and Trademark Office related to analysis of microscopic structure.
Brains from seven boys with autism had a mean of 67% more neurons in the dorsolateral and mesial prefrontal cortex than did those of six age-matched control subjects in a postmortem study reported in the Nov. 9 issue of JAMA.
"To our knowledge, this study is the first direct quantitative test and confirmation of the theory that a pathological overabundance of neurons in critical brain regions is present at a young age in autism," said Eric Courchesne, Ph.D., of the department of neuroscience, National Institutes of Health–University of California, San Diego, Autism Center of Excellence, University of California San Diego, La Jolla, and his associates.
"Because cortical neurons are generated in prenatal, not postnatal life, pathological overabundance of neurons indicates early developmental disturbances in molecular and genetic mechanisms that govern proliferation, cell cycle regulation, and apoptosis," they noted (JAMA 2011;306:2001-10).
Among autistic children, brain overgrowth (excess weight and size) and neuronal dysfunction have long been observed in many regions involved in higher-order social, emotional, communication, and cognitive development. But the neural basis of these abnormalities was unknown because it could only be explored in "direct quantitative studies of the young postmortem autistic brain" – specimens that are very rarely available.
Dr. Courchesne and his colleagues were able to perform such a study when they received access to entire dorsolateral and mesial sections of the prefrontal cortex in seven autistic and six control male subjects who had been aged 2-16 years when they died. Valid cell counts cannot be obtained using density estimates from small blocks of cortical tissue, the researchers explained.
They used stereological methods to count neurons, sampling 100 or more locations within 8-12 sections per reference space, and they calculated the total number of neurons using the optical fractionator method. Neurons were distinguished from microglia and satellite oligodendrocytes by doing detailed morphological examination, not just by estimating cell size.
The control cases were free of mental illness, intellectual disability, and neurological disorders. The autistic cases displayed a wide range of intellectual abilities, social skills, communication abilities, and functional impairments. All had been born at term after unremarkable perinatal courses.
Most of the study subjects had died of acute global ischemic hypoxia from accidental trauma (drowning, hanging, or electrocution); 1 died in a car accident, 1 of rhabdomyosarcoma, and 1 of possible cardiac arrest.
There had been no abnormalities on gross examination of most of the brains, according to medical examiner or neuropathology reports. The mean weight of autistic brains was 1,484 g, and was 17.6% greater than the normative mean weight for same-aged subjects reported in the literature. The control brains were significantly lighter and deviated from the norm by only 0.2%.
There were 79% more neurons in the dorsolateral prefrontal cortex among autistic brains than control brains, and 29% more neurons in the mesial prefrontal cortex. "Together, these 2 subdivisions gave a total combined prefrontal neuron count that was 67% greater in the autistic children (mean, 1.94 billion) compared with controls (mean, 1.16 billion)," Dr. Courchesne and his associates said.
This significant difference remained robust when the data were adjusted to account for subject age and postmortem interval.
The greater excess of neurons in the dorsolateral than in the mesial prefrontal cortex "parallels MRI volumetric data showing greater deviance in the dorsolateral prefrontal cortex than the mesial prefrontal cortex in living autistic toddlers," the investigators said.
Moreover, "these global increases in prefrontal neuron numbers were not apparent either at low or high magnification, and thus [were] undetectable by neuropathology visual inspection and neuron density measurement without formal quantitative stereological procedures," they noted.
There were no differences between autistic and control brains in the size of neurons, nor in counts of glial cells in the same brain regions.
It remains to be determined whether excess numbers of neurons occur in other regions of the brain besides "these two major prefrontal subdivisions," they added.
As has been noted in previous studies, this study found that the average weight of the autistic brains was heaver than that of the control brains. This indicates that the pathological increase in neuron numbers may be an important contributor to the brain overgrowth that has long been known to occur in autism.
However, the autistic brains did not show the linear correlation between number of neurons and brain weight that has been described in normal brains and was found in the control brains in this study. "Neuron counts in the autistic children should have been accompanied by brain weights considerably larger than was observed, reaching 29.4% enlargement rather than the observed 17.6% enlargement. Thus, the size of the autistic brain, overlarge as it is, might actually underestimate the pathology of excess neuron numbers," Dr. Courchesne and his colleagues noted.
"It would be invaluable to study larger samples of autistic and control cases at a younger and narrower age range to confirm excess counts in autism at the youngest ages, as well as to study larger samples across a wider age range to identify patterns of age-related changes in autism. It [also] will be important to include female cases in future studies, as etiological mechanisms may be discordant between the sexes," they said.
Future studies with a greater number of subjects also would allow researchers to explore relationships between brain morphology and behavior, possibly revealing whether neuron counts relate to symptom severity or intellectual ability, they added.
This study was supported by Autism Speaks, Cure Autism Now, the Peter Emch Family Foundation, the Simons Foundation, and the Thursday Club Juniors. Also, a grant from the National Institutes of Health–University of California, San Diego Autism Center of Excellence was awarded to Dr. Courchesne and a National Institute of Mental Health grant was awarded to Dr. Courchesne’s associated Dr. Peter R. Moulton. Brain specimens were provided by the National Institute of Child Health and Human Development Brain and Tissue Bank for Developmental Disorders, Autism Tissue Program, and direct donations to the Courchesne laboratory. Dr. Courchesne’s associate, Dr. Michael E. Calhoun, is the principal owner of Sinq Systems, a contract research organization that performed data collection and analysis for this study and he is an applicant on a pending patent on file with the U.S. Patent and Trademark Office related to analysis of microscopic structure.
FROM JAMA
Major Finding: There were 79% more neurons in the dorsolateral prefrontal cortex of autistic brains than in control brains, and 29% more neurons in the mesial prefrontal cortex; together, the total combined prefrontal neuron count was 67% greater in the autistic brains (mean, 1.94 billion neurons), compared with controls (mean, 1.16 billion neurons).
Data Source: A postmortem study of brains from seven autistic boys aged 2-16 years and six age-matched control boys who had no mental illness, intellectual disability, or neurologic disorders.
Disclosures: This study was supported by Autism Speaks, Cure Autism Now, the Peter Emch Family Foundation, the Simons Foundation, and the Thursday Club Juniors. Also, a grant from the National Institutes of Health–University of California, San Diego, Autism Center of Excellence was awarded to Dr. Courchesne and a National Institute of Mental Health grant was awarded to Dr. Courchesne’s associate Dr. Peter R. Moulton. Brain specimens were provided by the National Institute of Child Health and Human Development Brain and Tissue Bank for Developmental Disorders, Autism Tissue Program, and direct donations to the Courchesne laboratory. Dr. Courchesne’s associate, Dr. Michael E. Calhoun, is the principal owner of Sinq Systems, a contract research organization that performed data collection and analysis for this study, and he is an applicant on a pending patent on file with the U.S. Patent and Trademark Office related to analysis of microscopic structure.
Bypass Proves No Better Than Drugs in Preventing Stroke
Extracranial-intracranial arterial bypass surgery failed to prevent the recurrence of ischemic stroke any better than did medical therapy alone in a large clinical trial of patients with atherosclerotic internal carotid artery occlusion.
Even though graft patency was deemed "excellent" and the surgery clearly improved cerebral hemodynamics, the rate of ipsilateral recurrent stroke after 2 years was approximately 21%, which was not significantly different from the 23% rate among patients who received only medical therapy, Dr. William J. Powers of the department of neurology at the University of North Carolina at Chapel Hill, and his associates reported online Nov. 8 in JAMA.
Extracranial-intracranial (EC-IC) bypass surgery is designed to prevent recurrent stroke by improving hemodynamics distal to an index atherosclerotic occlusion in the internal carotid artery. Dr. Powers and his colleagues conducted the COSS (Carotid Occlusion Surgery Study) to determine whether the procedure, when added to optimal medical therapy, further reduced the rate of ipsilateral ischemic stroke.
They enrolled 195 patients who demonstrated complete occlusion of an internal carotid artery on vascular imaging, had experienced a transient ischemic attack (TIA) or ischemic stroke in the hemispheric territory of the occluded artery during the preceding 120 days, and showed hemodynamic cerebral ischemia on PET measurement of oxygen extraction fraction. The study subjects were randomly assigned to receive medical therapy (98 patients) or medical therapy plus EC-IC bypass surgery (97 patients) at 49 clinical centers and 18 PET centers in the United States and Canada.
The bypass surgery clearly improved cerebral hemodynamics on follow-up assessments, and overall graft patency was 98% after 30 days and 96% at last follow-up.
The 21% rate of recurrent ipsilateral ischemic stroke in the surgical group was very close to the rate of 24% that was predicted when the trial was designed, but the nonsurgical group’s rate of 23% was markedly lower than the 40% rate that had been predicted for it, based on the results of prospective observational studies performed in the 1990s. So even though the EC-IC bypass surgery cut the risk of recurrent stroke, "the better-than-expected efficacy of medical therapy in the nonsurgical group was sufficient to nullify any overall benefit of surgery," the investigators wrote (JAMA 2011;306:1983-92).
"Interpretation of the study is limited by the relatively small number of outcomes events," they added.
The COSS trial was terminated early when an interim analysis showed that given the unexpectedly low number of primary end points in the nonsurgical group, a clinically meaningful difference in favor of surgery would not be detectable unless the sample size were markedly increased. Since this wasn’t feasible, the investigators ended the study.
Later, a significant error was discovered in the interim analysis. However, it was still "highly unlikely that the COSS would have shown a statistically significant benefit for surgery if taken to completion," Dr. Powers and his associates noted.
The COSS trial was funded by grants from the National Institute of Neurological Disorders and Stroke and the U.S. Public Health Service. Several of Dr. Powers’ associates reported receiving personal compensation as a consultant for Merck, Medtronic, and W.L. Gore and Associates.
Dr. Broderick and Dr. Meyers are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough.
The failure of extracranial-intracranial arterial bypass surgery to improve clinical outcome at 2 years despite the improvement of an important biologic marker of brain perfusion – improved oxygen extraction ratio after the bypass procedure – is another addition to the list of failed surrogate end points in trials of cerebrovascular disease. These include recombinant factor VIIa to slow and stop bleeding in patients with intracerebral hemorrhage and intracranial stenting for stroke prevention in patients with symptomatic high-grade intracranial artery stenosis.
These and other trials of endovascular therapy for stroke consistently show that clinical outcomes after revascularization are highly dependent on minimizing the time interval between stroke onset and revascularization. These outcomes suggest that recanalization is an excellent surrogate end point in the first hours after stroke onset but is a poor surrogate at later time intervals and does not capture the entire effect of the endovascular procedure. Since the better-than-expected outcomes of the nonsurgical group in the COSS trial might possibly reflect improvements in the medical prevention of stroke during the conduct of the trial, Dr. Powers and his coauthors suggested that their results "reaffirm the hazard of using even the most carefully studied historical controls to infer therapeutic efficacy and the necessity of performing randomized controlled trials to establish clinical benefit."
Reimbursement for use of endovascular devices that have been approved only for the clearance of thrombus in acute stroke but not as clinically effective treatments for acute stroke – such as the MERCI Concentric Retriever and the Penumbra aspiration system – has increased their use by physicians in U.S. hospitals despite the lack of clinical effectiveness. Both of these devices received clearance by the Food and Drug Administration based on single-group, nonrandomized trials comparing device treatment with historical controls. Reimbursement for such devices makes it harder to recruit patients into randomized clinical trials that might clarify their effectiveness. Physicians who care for patients with acute stroke should enroll patients in randomized clinical trials in order to balance and align the standards of evidence for clinical effectiveness with reimbursement.
Dr. Joseph P. Broderick of the University of Cincinnati and Dr. Philip M. Meyers of Columbia University, New York, are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough. These remarks were adapted from their editorial comment accompanying the COSS trial report (JAMA 2011;306:2026-8).
The failure of extracranial-intracranial arterial bypass surgery to improve clinical outcome at 2 years despite the improvement of an important biologic marker of brain perfusion – improved oxygen extraction ratio after the bypass procedure – is another addition to the list of failed surrogate end points in trials of cerebrovascular disease. These include recombinant factor VIIa to slow and stop bleeding in patients with intracerebral hemorrhage and intracranial stenting for stroke prevention in patients with symptomatic high-grade intracranial artery stenosis.
These and other trials of endovascular therapy for stroke consistently show that clinical outcomes after revascularization are highly dependent on minimizing the time interval between stroke onset and revascularization. These outcomes suggest that recanalization is an excellent surrogate end point in the first hours after stroke onset but is a poor surrogate at later time intervals and does not capture the entire effect of the endovascular procedure. Since the better-than-expected outcomes of the nonsurgical group in the COSS trial might possibly reflect improvements in the medical prevention of stroke during the conduct of the trial, Dr. Powers and his coauthors suggested that their results "reaffirm the hazard of using even the most carefully studied historical controls to infer therapeutic efficacy and the necessity of performing randomized controlled trials to establish clinical benefit."
Reimbursement for use of endovascular devices that have been approved only for the clearance of thrombus in acute stroke but not as clinically effective treatments for acute stroke – such as the MERCI Concentric Retriever and the Penumbra aspiration system – has increased their use by physicians in U.S. hospitals despite the lack of clinical effectiveness. Both of these devices received clearance by the Food and Drug Administration based on single-group, nonrandomized trials comparing device treatment with historical controls. Reimbursement for such devices makes it harder to recruit patients into randomized clinical trials that might clarify their effectiveness. Physicians who care for patients with acute stroke should enroll patients in randomized clinical trials in order to balance and align the standards of evidence for clinical effectiveness with reimbursement.
Dr. Joseph P. Broderick of the University of Cincinnati and Dr. Philip M. Meyers of Columbia University, New York, are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough. These remarks were adapted from their editorial comment accompanying the COSS trial report (JAMA 2011;306:2026-8).
The failure of extracranial-intracranial arterial bypass surgery to improve clinical outcome at 2 years despite the improvement of an important biologic marker of brain perfusion – improved oxygen extraction ratio after the bypass procedure – is another addition to the list of failed surrogate end points in trials of cerebrovascular disease. These include recombinant factor VIIa to slow and stop bleeding in patients with intracerebral hemorrhage and intracranial stenting for stroke prevention in patients with symptomatic high-grade intracranial artery stenosis.
These and other trials of endovascular therapy for stroke consistently show that clinical outcomes after revascularization are highly dependent on minimizing the time interval between stroke onset and revascularization. These outcomes suggest that recanalization is an excellent surrogate end point in the first hours after stroke onset but is a poor surrogate at later time intervals and does not capture the entire effect of the endovascular procedure. Since the better-than-expected outcomes of the nonsurgical group in the COSS trial might possibly reflect improvements in the medical prevention of stroke during the conduct of the trial, Dr. Powers and his coauthors suggested that their results "reaffirm the hazard of using even the most carefully studied historical controls to infer therapeutic efficacy and the necessity of performing randomized controlled trials to establish clinical benefit."
Reimbursement for use of endovascular devices that have been approved only for the clearance of thrombus in acute stroke but not as clinically effective treatments for acute stroke – such as the MERCI Concentric Retriever and the Penumbra aspiration system – has increased their use by physicians in U.S. hospitals despite the lack of clinical effectiveness. Both of these devices received clearance by the Food and Drug Administration based on single-group, nonrandomized trials comparing device treatment with historical controls. Reimbursement for such devices makes it harder to recruit patients into randomized clinical trials that might clarify their effectiveness. Physicians who care for patients with acute stroke should enroll patients in randomized clinical trials in order to balance and align the standards of evidence for clinical effectiveness with reimbursement.
Dr. Joseph P. Broderick of the University of Cincinnati and Dr. Philip M. Meyers of Columbia University, New York, are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough. These remarks were adapted from their editorial comment accompanying the COSS trial report (JAMA 2011;306:2026-8).
Extracranial-intracranial arterial bypass surgery failed to prevent the recurrence of ischemic stroke any better than did medical therapy alone in a large clinical trial of patients with atherosclerotic internal carotid artery occlusion.
Even though graft patency was deemed "excellent" and the surgery clearly improved cerebral hemodynamics, the rate of ipsilateral recurrent stroke after 2 years was approximately 21%, which was not significantly different from the 23% rate among patients who received only medical therapy, Dr. William J. Powers of the department of neurology at the University of North Carolina at Chapel Hill, and his associates reported online Nov. 8 in JAMA.
Extracranial-intracranial (EC-IC) bypass surgery is designed to prevent recurrent stroke by improving hemodynamics distal to an index atherosclerotic occlusion in the internal carotid artery. Dr. Powers and his colleagues conducted the COSS (Carotid Occlusion Surgery Study) to determine whether the procedure, when added to optimal medical therapy, further reduced the rate of ipsilateral ischemic stroke.
They enrolled 195 patients who demonstrated complete occlusion of an internal carotid artery on vascular imaging, had experienced a transient ischemic attack (TIA) or ischemic stroke in the hemispheric territory of the occluded artery during the preceding 120 days, and showed hemodynamic cerebral ischemia on PET measurement of oxygen extraction fraction. The study subjects were randomly assigned to receive medical therapy (98 patients) or medical therapy plus EC-IC bypass surgery (97 patients) at 49 clinical centers and 18 PET centers in the United States and Canada.
The bypass surgery clearly improved cerebral hemodynamics on follow-up assessments, and overall graft patency was 98% after 30 days and 96% at last follow-up.
The 21% rate of recurrent ipsilateral ischemic stroke in the surgical group was very close to the rate of 24% that was predicted when the trial was designed, but the nonsurgical group’s rate of 23% was markedly lower than the 40% rate that had been predicted for it, based on the results of prospective observational studies performed in the 1990s. So even though the EC-IC bypass surgery cut the risk of recurrent stroke, "the better-than-expected efficacy of medical therapy in the nonsurgical group was sufficient to nullify any overall benefit of surgery," the investigators wrote (JAMA 2011;306:1983-92).
"Interpretation of the study is limited by the relatively small number of outcomes events," they added.
The COSS trial was terminated early when an interim analysis showed that given the unexpectedly low number of primary end points in the nonsurgical group, a clinically meaningful difference in favor of surgery would not be detectable unless the sample size were markedly increased. Since this wasn’t feasible, the investigators ended the study.
Later, a significant error was discovered in the interim analysis. However, it was still "highly unlikely that the COSS would have shown a statistically significant benefit for surgery if taken to completion," Dr. Powers and his associates noted.
The COSS trial was funded by grants from the National Institute of Neurological Disorders and Stroke and the U.S. Public Health Service. Several of Dr. Powers’ associates reported receiving personal compensation as a consultant for Merck, Medtronic, and W.L. Gore and Associates.
Dr. Broderick and Dr. Meyers are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough.
Extracranial-intracranial arterial bypass surgery failed to prevent the recurrence of ischemic stroke any better than did medical therapy alone in a large clinical trial of patients with atherosclerotic internal carotid artery occlusion.
Even though graft patency was deemed "excellent" and the surgery clearly improved cerebral hemodynamics, the rate of ipsilateral recurrent stroke after 2 years was approximately 21%, which was not significantly different from the 23% rate among patients who received only medical therapy, Dr. William J. Powers of the department of neurology at the University of North Carolina at Chapel Hill, and his associates reported online Nov. 8 in JAMA.
Extracranial-intracranial (EC-IC) bypass surgery is designed to prevent recurrent stroke by improving hemodynamics distal to an index atherosclerotic occlusion in the internal carotid artery. Dr. Powers and his colleagues conducted the COSS (Carotid Occlusion Surgery Study) to determine whether the procedure, when added to optimal medical therapy, further reduced the rate of ipsilateral ischemic stroke.
They enrolled 195 patients who demonstrated complete occlusion of an internal carotid artery on vascular imaging, had experienced a transient ischemic attack (TIA) or ischemic stroke in the hemispheric territory of the occluded artery during the preceding 120 days, and showed hemodynamic cerebral ischemia on PET measurement of oxygen extraction fraction. The study subjects were randomly assigned to receive medical therapy (98 patients) or medical therapy plus EC-IC bypass surgery (97 patients) at 49 clinical centers and 18 PET centers in the United States and Canada.
The bypass surgery clearly improved cerebral hemodynamics on follow-up assessments, and overall graft patency was 98% after 30 days and 96% at last follow-up.
The 21% rate of recurrent ipsilateral ischemic stroke in the surgical group was very close to the rate of 24% that was predicted when the trial was designed, but the nonsurgical group’s rate of 23% was markedly lower than the 40% rate that had been predicted for it, based on the results of prospective observational studies performed in the 1990s. So even though the EC-IC bypass surgery cut the risk of recurrent stroke, "the better-than-expected efficacy of medical therapy in the nonsurgical group was sufficient to nullify any overall benefit of surgery," the investigators wrote (JAMA 2011;306:1983-92).
"Interpretation of the study is limited by the relatively small number of outcomes events," they added.
The COSS trial was terminated early when an interim analysis showed that given the unexpectedly low number of primary end points in the nonsurgical group, a clinically meaningful difference in favor of surgery would not be detectable unless the sample size were markedly increased. Since this wasn’t feasible, the investigators ended the study.
Later, a significant error was discovered in the interim analysis. However, it was still "highly unlikely that the COSS would have shown a statistically significant benefit for surgery if taken to completion," Dr. Powers and his associates noted.
The COSS trial was funded by grants from the National Institute of Neurological Disorders and Stroke and the U.S. Public Health Service. Several of Dr. Powers’ associates reported receiving personal compensation as a consultant for Merck, Medtronic, and W.L. Gore and Associates.
Dr. Broderick and Dr. Meyers are involved in the IMS III trial, which receives or has received interventional devices or drugs from Genentech, EKOS Corp., Concentric, and Johnson & Johnson. Dr. Broderick also reported serving as a consultant to Genentech and receiving investigational drug supply for the ongoing CLEARER trial from Schering Plough.
FROM JAMA
Major Finding: Even though EC-IC bypass surgery improved cerebral hemodynamics, the 2-year rate of recurrent ischemic stroke was not significantly better after the procedure (21%) than after optimal medical therapy alone (23%).
Data Source: The COSS was an open-label, randomized clinical trial involving 195 patients with atherosclerotic internal carotid artery occlusion treated at 67 centers in the United States and Canada.
Disclosures: The COSS trial was funded by grants from the National Institute of Neurological Disorders and Stroke and the U.S. Public Health Service. Several of Dr. Powers’ associates reported receiving personal compensation as a consultant for Merck, Medtronic, and W.L. Gore & Associates.