User login
Lucas Franki is an associate editor for MDedge News, and has been with the company since 2014. He has a BA in English from Penn State University and is an Eagle Scout.
First treatment for LAL deficiency on track for European approval
Sebelipase alfa (Kanuma) has been recommended for approval to treat lysosomal acid lipase deficiency in infants, children, and adults, according to a press release from the European Medicine Agency.
Lysosomal acid lipase breaks down fatty material, and LAL deficiency causes a buildup of fatty material in important body organs such as the liver and blood vessels. Patients with LAL deficiency can experience symptoms such as growth failure, enlarged liver, diarrhea, and malabsorption. LAL deficiency is inherited, and is life threatening in its most severe form, especially in infants under 1 year old.
Sebelipase alfa is a long-term enzyme replacement therapy for all patients with LAL deficiency. In four small studies of 106 patients, sebelipase alfa proved effective at replacing the missing enzyme, and improvement was seen in several areas. Infant survival was improved, which is important as no treatment option for infants with LAL deficiency existed before.
Common side effects of the treatment include allergic reaction, transient hyperlipidemia, and development of antidrug antibodies. Any patients, particularly infants, showing signs of hypersensitivity should be monitored further.
Read the full press release on the European Medicine Agency’s website.
Sebelipase alfa (Kanuma) has been recommended for approval to treat lysosomal acid lipase deficiency in infants, children, and adults, according to a press release from the European Medicine Agency.
Lysosomal acid lipase breaks down fatty material, and LAL deficiency causes a buildup of fatty material in important body organs such as the liver and blood vessels. Patients with LAL deficiency can experience symptoms such as growth failure, enlarged liver, diarrhea, and malabsorption. LAL deficiency is inherited, and is life threatening in its most severe form, especially in infants under 1 year old.
Sebelipase alfa is a long-term enzyme replacement therapy for all patients with LAL deficiency. In four small studies of 106 patients, sebelipase alfa proved effective at replacing the missing enzyme, and improvement was seen in several areas. Infant survival was improved, which is important as no treatment option for infants with LAL deficiency existed before.
Common side effects of the treatment include allergic reaction, transient hyperlipidemia, and development of antidrug antibodies. Any patients, particularly infants, showing signs of hypersensitivity should be monitored further.
Read the full press release on the European Medicine Agency’s website.
Sebelipase alfa (Kanuma) has been recommended for approval to treat lysosomal acid lipase deficiency in infants, children, and adults, according to a press release from the European Medicine Agency.
Lysosomal acid lipase breaks down fatty material, and LAL deficiency causes a buildup of fatty material in important body organs such as the liver and blood vessels. Patients with LAL deficiency can experience symptoms such as growth failure, enlarged liver, diarrhea, and malabsorption. LAL deficiency is inherited, and is life threatening in its most severe form, especially in infants under 1 year old.
Sebelipase alfa is a long-term enzyme replacement therapy for all patients with LAL deficiency. In four small studies of 106 patients, sebelipase alfa proved effective at replacing the missing enzyme, and improvement was seen in several areas. Infant survival was improved, which is important as no treatment option for infants with LAL deficiency existed before.
Common side effects of the treatment include allergic reaction, transient hyperlipidemia, and development of antidrug antibodies. Any patients, particularly infants, showing signs of hypersensitivity should be monitored further.
Read the full press release on the European Medicine Agency’s website.
Cheaper Generics Keep Statin Expenditures in Check
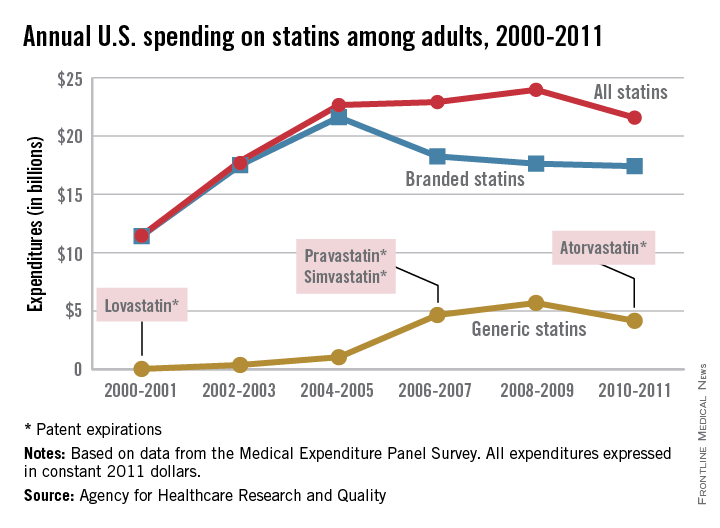
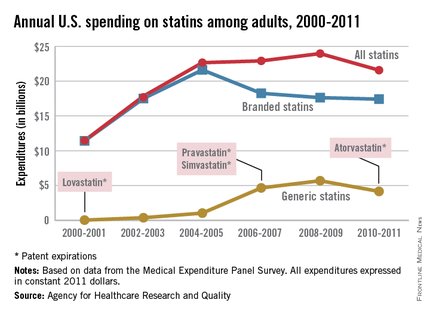
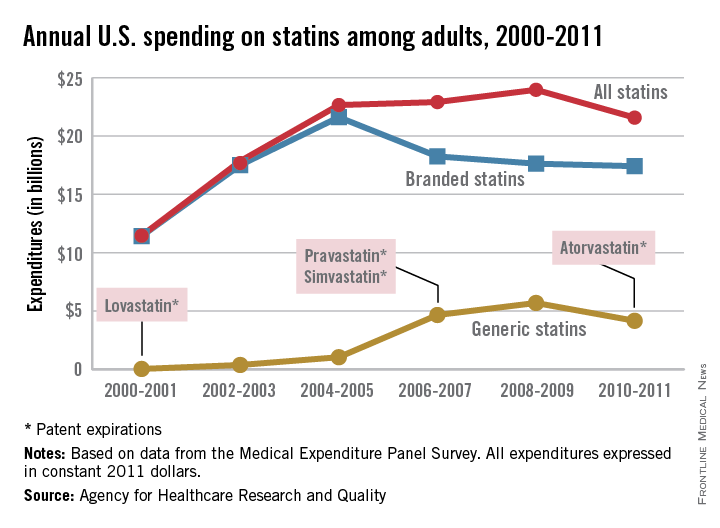
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
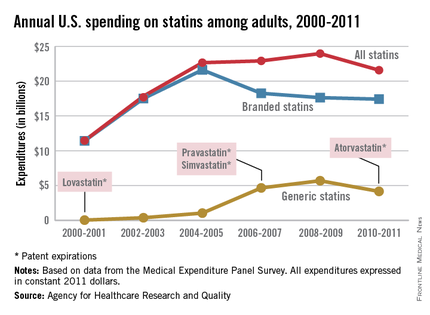
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Cheaper generics keep statin expenditures in check
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Total statin spending increased dramatically from 2000 to 2005, but has plateaued since as less expensive generic statins have entered the market, according to a report from the Agency for Healthcare Research and Quality.
In 2000-2001, total statin spending was $11.5 billion, nearly all of it on branded drugs. Lovastatin, the first statin approved by the Food and Drug Administration, went generic in 2001, and by 2004-2005, generic static spending was just over $1 billion and overall spending was at $22.7 billion.
Simvastatin and pravastatin both became generic in 2006 and spending on generic statins increased by over 300% by 2010-2011 to $4.2 billion. Overall spending for statins was $21.6 billion in 2010-2011, with branded drugs representing $17.4 billion of that total, the AHRQ reported.
The number of adults taking statins rose consistently from 2000 to 2011, from 17.6 million in 2000-2001 to 40.8 million in 2010-2011, despite the use of branded statins falling from 28.6 million people in 2004-2005 to 16.6 million in 2010-2011, as generic statin use increased from 2.4 million people to 26.5 million over the same time period.
The increased use of generics brought the annual cost per user for all statins down from $762 in 2002-2003 to $529 in 2010-2011. Spending per user on branded statins, however, rose considerably over that period, going from $774 annually in 2001-2002 to $1,051 in 2010-2011. The cost of generic statins dropped from a high of $425 in 2004-2005 to $157 per user in 2010-2011, the AHRQ noted.
All data were collected by the Medical Expenditure Panel Survey.
Beware of high blood pressure
High blood pressure may not have any symptoms except in the most extreme cases, but the effect it can have on the human body is real and severe.
The only symptom of high blood pressure is a very serious condition known as hypertensive crisis, which occurs only when blood pressure rises over 180/110 mm Hg. This condition requires immediate medical attention. High blood pressure can cause a series of other serious health issues, such as damage to the heart and arteries, stroke, kidney damage, vision loss, erectile dysfunction, memory loss, angina, and peripheral artery disease.
High blood pressure in combination with other risk factors such as age, heredity, gender, obesity, smoking, high cholesterol, diabetes, and physical inactivity can further increase risk of major health issues. Diet and exercise changes, however, can help lessen that risk.
Learn more at the American Heart Association website.
High blood pressure may not have any symptoms except in the most extreme cases, but the effect it can have on the human body is real and severe.
The only symptom of high blood pressure is a very serious condition known as hypertensive crisis, which occurs only when blood pressure rises over 180/110 mm Hg. This condition requires immediate medical attention. High blood pressure can cause a series of other serious health issues, such as damage to the heart and arteries, stroke, kidney damage, vision loss, erectile dysfunction, memory loss, angina, and peripheral artery disease.
High blood pressure in combination with other risk factors such as age, heredity, gender, obesity, smoking, high cholesterol, diabetes, and physical inactivity can further increase risk of major health issues. Diet and exercise changes, however, can help lessen that risk.
Learn more at the American Heart Association website.
High blood pressure may not have any symptoms except in the most extreme cases, but the effect it can have on the human body is real and severe.
The only symptom of high blood pressure is a very serious condition known as hypertensive crisis, which occurs only when blood pressure rises over 180/110 mm Hg. This condition requires immediate medical attention. High blood pressure can cause a series of other serious health issues, such as damage to the heart and arteries, stroke, kidney damage, vision loss, erectile dysfunction, memory loss, angina, and peripheral artery disease.
High blood pressure in combination with other risk factors such as age, heredity, gender, obesity, smoking, high cholesterol, diabetes, and physical inactivity can further increase risk of major health issues. Diet and exercise changes, however, can help lessen that risk.
Learn more at the American Heart Association website.
Impulsivity related to medication nonadherence in bipolar patients
Euthymic bipolar disorder patients with poor medication adherence are more likely to experience nonplanning impulsivity, according to Dr. Raoul Belzeaux and his associates.
Dr. Belzeaux and his associates conducted a cross-sectional study at nine centers across France. They collected data from 260 outpatients in symptomatic remission who had been diagnosed with bipolar disorder type I, type II, or not otherwise specified based on DSM-IV criteria.
The Medication Adherence Rating Scale total mean score for the study was 7.6, which is suboptimal. The standardized coefficient between nonplanning impulsivity score and MARS score was 0.156. Factors outside medication adherence, such as lifetime anxiety disorders, had little effect on impulsivity and medication adherence.
“The association between impulsivity and adherence to medication may lead to systematically evaluate impulsivity” for example, with standardized questionnaires such as the Barratt Impulsiveness Scale “in clinical practice to better predict risk of nonadherence and, thus, contribute to promote personalized treatment strategy,” the investigators concluded.
Find the full study in the Journal of Affective Disorders (doi: 10.1016/j.jad.2015.05.041).
Euthymic bipolar disorder patients with poor medication adherence are more likely to experience nonplanning impulsivity, according to Dr. Raoul Belzeaux and his associates.
Dr. Belzeaux and his associates conducted a cross-sectional study at nine centers across France. They collected data from 260 outpatients in symptomatic remission who had been diagnosed with bipolar disorder type I, type II, or not otherwise specified based on DSM-IV criteria.
The Medication Adherence Rating Scale total mean score for the study was 7.6, which is suboptimal. The standardized coefficient between nonplanning impulsivity score and MARS score was 0.156. Factors outside medication adherence, such as lifetime anxiety disorders, had little effect on impulsivity and medication adherence.
“The association between impulsivity and adherence to medication may lead to systematically evaluate impulsivity” for example, with standardized questionnaires such as the Barratt Impulsiveness Scale “in clinical practice to better predict risk of nonadherence and, thus, contribute to promote personalized treatment strategy,” the investigators concluded.
Find the full study in the Journal of Affective Disorders (doi: 10.1016/j.jad.2015.05.041).
Euthymic bipolar disorder patients with poor medication adherence are more likely to experience nonplanning impulsivity, according to Dr. Raoul Belzeaux and his associates.
Dr. Belzeaux and his associates conducted a cross-sectional study at nine centers across France. They collected data from 260 outpatients in symptomatic remission who had been diagnosed with bipolar disorder type I, type II, or not otherwise specified based on DSM-IV criteria.
The Medication Adherence Rating Scale total mean score for the study was 7.6, which is suboptimal. The standardized coefficient between nonplanning impulsivity score and MARS score was 0.156. Factors outside medication adherence, such as lifetime anxiety disorders, had little effect on impulsivity and medication adherence.
“The association between impulsivity and adherence to medication may lead to systematically evaluate impulsivity” for example, with standardized questionnaires such as the Barratt Impulsiveness Scale “in clinical practice to better predict risk of nonadherence and, thus, contribute to promote personalized treatment strategy,” the investigators concluded.
Find the full study in the Journal of Affective Disorders (doi: 10.1016/j.jad.2015.05.041).
In recent-onset bipolar disorder, tailored CBT reduced relapses
Recovery-focused cognitive-behavioral therapy can delay and reduce relapses for patients with recent-onset bipolar disorder, Steven H. Jones, Ph.D., and his associates reported in a pilot study that compared 33 patients who received up to 18 hours of tailored CBT and 34 patients who received treatment as usual (TAU).
“This study highlights the potential benefits of taking a formulation-based approach to bipolar disorder, in which a range of evidence-informed techniques are available to the clinician but the relative emphasis given to each is determined on an individual client basis,” the researchers noted in the British Journal of Psychiatry (doi:10.1192/bjp.bp.113.141259).

Dr. Jones of Lancaster (England) University and his colleagues studied participants who met the DSM-IV diagnosis of primary bipolar with onset within the past 5 years. The recovery-focused CBT approach included core items whose use was determined by individual patient needs. The recovery approach was explained, information was gathered about current and historical mood and functioning, the meaning and relevance of the diagnosis were discussed, recovery-informed therapy goals were identified, relationships between mood experiences and progress towards recovery goals were addressed, CBT techniques were identified and applied to facilitate positive coping, and wider functioning issues in relation to recovery were considered. The information was used to develop a recovery plan and lessons from therapy were shared with key stakeholders.
Unlike standard CBT for bipolar disorder, which focuses on preventing relapse, the tailored CBT approach elicited client-focused goals and the freedom to work within whatever model the client brings. The model could address functioning and comorbidity issues as well as mood problems, and emphasized supporting clients to move away from self-critical and stigmatizing language, especially around diagnosis and behavior in acute episodes.
The primary clinical outcomes were measured using the Bipolar Recovery Questionnaire (33-item version, 0-100 scale with higher score indicating higher personal recovery), time to bipolar relapse measured by the Structural Clinical Interview for DSM-IV (SCID)-LIFE, and mood symptoms as measured by the Hamilton Rating Scale for Depression and Bech-Rafaelsen Mania Scale.
After 12 months, the CBT group’s Bipolar Recovery Questionnaire mean score was 2,351 – a 30% improvement from baseline (1,797), while the TAU group’s mean score was 2,193 – an 8% improvement from baseline(1,935).
Both manic and depressive relapses were less common and took longer to occur in the CBT group. There were 11 depressive relapses in the CBT group, occurring after a median of 60 weeks. There were 19 relapses in the TAU group, occurring after a median of 18 weeks. There were 3 manic relapses in the CBT group, occurring after a median of 60 weeks, and 10 manic relapses in the TAU group occurring after a median of 33 weeks.
Recovery-focused cognitive-behavioral therapy can delay and reduce relapses for patients with recent-onset bipolar disorder, Steven H. Jones, Ph.D., and his associates reported in a pilot study that compared 33 patients who received up to 18 hours of tailored CBT and 34 patients who received treatment as usual (TAU).
“This study highlights the potential benefits of taking a formulation-based approach to bipolar disorder, in which a range of evidence-informed techniques are available to the clinician but the relative emphasis given to each is determined on an individual client basis,” the researchers noted in the British Journal of Psychiatry (doi:10.1192/bjp.bp.113.141259).
Dr. Jones of Lancaster (England) University and his colleagues studied participants who met the DSM-IV diagnosis of primary bipolar with onset within the past 5 years. The recovery-focused CBT approach included core items whose use was determined by individual patient needs. The recovery approach was explained, information was gathered about current and historical mood and functioning, the meaning and relevance of the diagnosis were discussed, recovery-informed therapy goals were identified, relationships between mood experiences and progress towards recovery goals were addressed, CBT techniques were identified and applied to facilitate positive coping, and wider functioning issues in relation to recovery were considered. The information was used to develop a recovery plan and lessons from therapy were shared with key stakeholders.
Unlike standard CBT for bipolar disorder, which focuses on preventing relapse, the tailored CBT approach elicited client-focused goals and the freedom to work within whatever model the client brings. The model could address functioning and comorbidity issues as well as mood problems, and emphasized supporting clients to move away from self-critical and stigmatizing language, especially around diagnosis and behavior in acute episodes.
The primary clinical outcomes were measured using the Bipolar Recovery Questionnaire (33-item version, 0-100 scale with higher score indicating higher personal recovery), time to bipolar relapse measured by the Structural Clinical Interview for DSM-IV (SCID)-LIFE, and mood symptoms as measured by the Hamilton Rating Scale for Depression and Bech-Rafaelsen Mania Scale.
After 12 months, the CBT group’s Bipolar Recovery Questionnaire mean score was 2,351 – a 30% improvement from baseline (1,797), while the TAU group’s mean score was 2,193 – an 8% improvement from baseline(1,935).
Both manic and depressive relapses were less common and took longer to occur in the CBT group. There were 11 depressive relapses in the CBT group, occurring after a median of 60 weeks. There were 19 relapses in the TAU group, occurring after a median of 18 weeks. There were 3 manic relapses in the CBT group, occurring after a median of 60 weeks, and 10 manic relapses in the TAU group occurring after a median of 33 weeks.
Recovery-focused cognitive-behavioral therapy can delay and reduce relapses for patients with recent-onset bipolar disorder, Steven H. Jones, Ph.D., and his associates reported in a pilot study that compared 33 patients who received up to 18 hours of tailored CBT and 34 patients who received treatment as usual (TAU).
“This study highlights the potential benefits of taking a formulation-based approach to bipolar disorder, in which a range of evidence-informed techniques are available to the clinician but the relative emphasis given to each is determined on an individual client basis,” the researchers noted in the British Journal of Psychiatry (doi:10.1192/bjp.bp.113.141259).
Dr. Jones of Lancaster (England) University and his colleagues studied participants who met the DSM-IV diagnosis of primary bipolar with onset within the past 5 years. The recovery-focused CBT approach included core items whose use was determined by individual patient needs. The recovery approach was explained, information was gathered about current and historical mood and functioning, the meaning and relevance of the diagnosis were discussed, recovery-informed therapy goals were identified, relationships between mood experiences and progress towards recovery goals were addressed, CBT techniques were identified and applied to facilitate positive coping, and wider functioning issues in relation to recovery were considered. The information was used to develop a recovery plan and lessons from therapy were shared with key stakeholders.
Unlike standard CBT for bipolar disorder, which focuses on preventing relapse, the tailored CBT approach elicited client-focused goals and the freedom to work within whatever model the client brings. The model could address functioning and comorbidity issues as well as mood problems, and emphasized supporting clients to move away from self-critical and stigmatizing language, especially around diagnosis and behavior in acute episodes.
The primary clinical outcomes were measured using the Bipolar Recovery Questionnaire (33-item version, 0-100 scale with higher score indicating higher personal recovery), time to bipolar relapse measured by the Structural Clinical Interview for DSM-IV (SCID)-LIFE, and mood symptoms as measured by the Hamilton Rating Scale for Depression and Bech-Rafaelsen Mania Scale.
After 12 months, the CBT group’s Bipolar Recovery Questionnaire mean score was 2,351 – a 30% improvement from baseline (1,797), while the TAU group’s mean score was 2,193 – an 8% improvement from baseline(1,935).
Both manic and depressive relapses were less common and took longer to occur in the CBT group. There were 11 depressive relapses in the CBT group, occurring after a median of 60 weeks. There were 19 relapses in the TAU group, occurring after a median of 18 weeks. There were 3 manic relapses in the CBT group, occurring after a median of 60 weeks, and 10 manic relapses in the TAU group occurring after a median of 33 weeks.
Key clinical point: Patient-focused CBT may reduce relapses in recent-onset bipolar disorder.
Major finding: After 12 months, the CBT group’s Bipolar Recovery Questionnaire mean score was 2,351 – a 30% improvement from baseline (1,797), while the usual treatment group’s mean score was 2,193 – an 8% improvement from baseline(1,935).
Data source: A prospective study of 67 patients with recent-onset bipolar disorder, 33 given CBT and 34 given usual therapy.
Disclosures: The researchers had no relevant financial disclosures.

‘Dabbing’ on the rise: Is this marijuana use dangerous?
The use of butane hash oil and the inhalation of concentrated tetrahydrocannabinol created through butane extraction, otherwise known as “dabbing,” seems to be on the rise in the United States, and might carry risks beyond that of traditional marijuana, according to John M. Stogner, Ph.D., and Bryan Lee Miller, Ph.D.
Butane hash oil (BHO) is produced by passing butane through a tube filled with cannabis trimmings. The tetrahydrocannabinol (THC) dissolves in the butane, and the mixture is collected. The butane evaporates off, leaving crystals that can be up to 80% THC. This process, known as blasting, can be done at home. However, butane is a dangerous and flammable substance, and the risks tied to blasting are similar to those of methamphetamine production.
Dabbing itself involves inhaling vaporized THC crystals through a glass water pipe using a hollow titanium rod heated by a blowtorch. Aside from the obvious health risk of using a blowtorch while mentally impaired, dabbing also can involve inhalation of off-gassing solder, rust from oxidized metal, and benzene.
There has been little research into the health effects of dabbing. Some sources suggest that substances that cause lung damage are not smoked and there is no risk of bacterial or fungal infection; others suggest that adverse side effects such as loss of consciousness and falls are more common, and that dabbing carries an increased risk of addiction.
Primary care physicians should inform patients of potential risk, but they “should avoid hyperbolic arguments like those of the media that describe dabbing as ‘the crack of pot,’ and instead urge caution. Patients should be advised that research is lacking, information is still largely anecdotal, and the safest option is to refrain from use when definitive answers are absent,” Dr. Stogner and Dr. Miller noted.
Find the full perspective in Pediatrics (doi:10.1542/peds.2015-0454).
The use of butane hash oil and the inhalation of concentrated tetrahydrocannabinol created through butane extraction, otherwise known as “dabbing,” seems to be on the rise in the United States, and might carry risks beyond that of traditional marijuana, according to John M. Stogner, Ph.D., and Bryan Lee Miller, Ph.D.
Butane hash oil (BHO) is produced by passing butane through a tube filled with cannabis trimmings. The tetrahydrocannabinol (THC) dissolves in the butane, and the mixture is collected. The butane evaporates off, leaving crystals that can be up to 80% THC. This process, known as blasting, can be done at home. However, butane is a dangerous and flammable substance, and the risks tied to blasting are similar to those of methamphetamine production.
Dabbing itself involves inhaling vaporized THC crystals through a glass water pipe using a hollow titanium rod heated by a blowtorch. Aside from the obvious health risk of using a blowtorch while mentally impaired, dabbing also can involve inhalation of off-gassing solder, rust from oxidized metal, and benzene.
There has been little research into the health effects of dabbing. Some sources suggest that substances that cause lung damage are not smoked and there is no risk of bacterial or fungal infection; others suggest that adverse side effects such as loss of consciousness and falls are more common, and that dabbing carries an increased risk of addiction.
Primary care physicians should inform patients of potential risk, but they “should avoid hyperbolic arguments like those of the media that describe dabbing as ‘the crack of pot,’ and instead urge caution. Patients should be advised that research is lacking, information is still largely anecdotal, and the safest option is to refrain from use when definitive answers are absent,” Dr. Stogner and Dr. Miller noted.
Find the full perspective in Pediatrics (doi:10.1542/peds.2015-0454).
The use of butane hash oil and the inhalation of concentrated tetrahydrocannabinol created through butane extraction, otherwise known as “dabbing,” seems to be on the rise in the United States, and might carry risks beyond that of traditional marijuana, according to John M. Stogner, Ph.D., and Bryan Lee Miller, Ph.D.
Butane hash oil (BHO) is produced by passing butane through a tube filled with cannabis trimmings. The tetrahydrocannabinol (THC) dissolves in the butane, and the mixture is collected. The butane evaporates off, leaving crystals that can be up to 80% THC. This process, known as blasting, can be done at home. However, butane is a dangerous and flammable substance, and the risks tied to blasting are similar to those of methamphetamine production.
Dabbing itself involves inhaling vaporized THC crystals through a glass water pipe using a hollow titanium rod heated by a blowtorch. Aside from the obvious health risk of using a blowtorch while mentally impaired, dabbing also can involve inhalation of off-gassing solder, rust from oxidized metal, and benzene.
There has been little research into the health effects of dabbing. Some sources suggest that substances that cause lung damage are not smoked and there is no risk of bacterial or fungal infection; others suggest that adverse side effects such as loss of consciousness and falls are more common, and that dabbing carries an increased risk of addiction.
Primary care physicians should inform patients of potential risk, but they “should avoid hyperbolic arguments like those of the media that describe dabbing as ‘the crack of pot,’ and instead urge caution. Patients should be advised that research is lacking, information is still largely anecdotal, and the safest option is to refrain from use when definitive answers are absent,” Dr. Stogner and Dr. Miller noted.
Find the full perspective in Pediatrics (doi:10.1542/peds.2015-0454).
Chronic anemia associated with high PAP in SLE patients
Chronic anemic hypoxia is associated with increased pulmonary artery pressure (PAP) in patients with systemic lupus erythematosus (SLE), according to Dr. Ki-Jo Kim and associates.
In this study of 132 SLE patients, those with increased PAP had significantly lower oxygen delivery levels than those with normal PAP. Oxygen delivery also was directly correlated with hemoglobin levels. Increased PAP was more likely when patients had a longer duration of anemia during the preceding 6-24 months, and patients who had anemia for more than half of the preceding 6 months also had increased risk.
Higher levels of interleukin-6 likely plays a role in raising PAP levels, as IL-6 levels increased with higher PAP but decreased across tertiles of hemoglobin, the investigators noted. Pulmonary arterial hypertension is a rare but serious complication of SLE.
Find the full study in Arthritis Care & Research (doi:10.1002/acr.22630).
Chronic anemic hypoxia is associated with increased pulmonary artery pressure (PAP) in patients with systemic lupus erythematosus (SLE), according to Dr. Ki-Jo Kim and associates.
In this study of 132 SLE patients, those with increased PAP had significantly lower oxygen delivery levels than those with normal PAP. Oxygen delivery also was directly correlated with hemoglobin levels. Increased PAP was more likely when patients had a longer duration of anemia during the preceding 6-24 months, and patients who had anemia for more than half of the preceding 6 months also had increased risk.
Higher levels of interleukin-6 likely plays a role in raising PAP levels, as IL-6 levels increased with higher PAP but decreased across tertiles of hemoglobin, the investigators noted. Pulmonary arterial hypertension is a rare but serious complication of SLE.
Find the full study in Arthritis Care & Research (doi:10.1002/acr.22630).
Chronic anemic hypoxia is associated with increased pulmonary artery pressure (PAP) in patients with systemic lupus erythematosus (SLE), according to Dr. Ki-Jo Kim and associates.
In this study of 132 SLE patients, those with increased PAP had significantly lower oxygen delivery levels than those with normal PAP. Oxygen delivery also was directly correlated with hemoglobin levels. Increased PAP was more likely when patients had a longer duration of anemia during the preceding 6-24 months, and patients who had anemia for more than half of the preceding 6 months also had increased risk.
Higher levels of interleukin-6 likely plays a role in raising PAP levels, as IL-6 levels increased with higher PAP but decreased across tertiles of hemoglobin, the investigators noted. Pulmonary arterial hypertension is a rare but serious complication of SLE.
Find the full study in Arthritis Care & Research (doi:10.1002/acr.22630).
Rontalizumab effective in interferon signature matrix–low SLE patients
Rontalizumab was an effective treatment for systemic lupus erythematosus patients with low interferon signature matrix scores, according to Dr. Kenneth Kalunian of the University of California, San Diego, and his associates.
The exploratory subgroup of ISM-low patients on rontalizumab had higher SLE response index rates and lower steroid use than those on the placebo. These patients also had a reduced SLE Disease Activity Index flare rates, with a hazard ratio of 0.61. Adverse side effects were similar in the placebo and rontalizumab groups.
In the main portion of the 238-patient study, no difference in response rates between the rontalizumab and placebo groups in ISM-high patients was found, the investigators reported. Rontalizumab is a humanized IgG1 anti-interferon alpha (anti-IFN-alpha) monoclonal antibody.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206090).
Rontalizumab was an effective treatment for systemic lupus erythematosus patients with low interferon signature matrix scores, according to Dr. Kenneth Kalunian of the University of California, San Diego, and his associates.
The exploratory subgroup of ISM-low patients on rontalizumab had higher SLE response index rates and lower steroid use than those on the placebo. These patients also had a reduced SLE Disease Activity Index flare rates, with a hazard ratio of 0.61. Adverse side effects were similar in the placebo and rontalizumab groups.
In the main portion of the 238-patient study, no difference in response rates between the rontalizumab and placebo groups in ISM-high patients was found, the investigators reported. Rontalizumab is a humanized IgG1 anti-interferon alpha (anti-IFN-alpha) monoclonal antibody.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206090).
Rontalizumab was an effective treatment for systemic lupus erythematosus patients with low interferon signature matrix scores, according to Dr. Kenneth Kalunian of the University of California, San Diego, and his associates.
The exploratory subgroup of ISM-low patients on rontalizumab had higher SLE response index rates and lower steroid use than those on the placebo. These patients also had a reduced SLE Disease Activity Index flare rates, with a hazard ratio of 0.61. Adverse side effects were similar in the placebo and rontalizumab groups.
In the main portion of the 238-patient study, no difference in response rates between the rontalizumab and placebo groups in ISM-high patients was found, the investigators reported. Rontalizumab is a humanized IgG1 anti-interferon alpha (anti-IFN-alpha) monoclonal antibody.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206090).
Testosterone tied to face recognition in men with schizophrenia
Testosterone is related to activation of the inferior frontal gyrus during emotion face processing in men with schizophrenia but not in healthy patients, according to Ellen Ji and her associates.
The investigators assessed 16 males with schizophrenia and 16 healthy male controls by presenting them with 60 color pictures of human faces. Participants were told to pick the emotion shown using a button box, reported Ms. Ji of the University of New South Wales in Randwick, Australia, and her associates.
The men with schizophrenia showed much less inferior frontal gyrus activation than did those in the control group. Men with low-normal testosterone levels in the schizophrenia group had significantly worse face recognition results than did those with high-normal testosterone, but no correlation was found between low- and high-normal testosterone levels and face recognition in the control group.
“This preliminary finding provides the first evidence for a link between circulating testosterone levels and brain activity in a region characterized by hypoactivity during negative emotion face processing in men with schizophrenia, suggesting that an increase in normal levels of testosterone may have beneficial effects for emotion processing in men with schizophrenia,” the investigators concluded.
Find the full study in Behavioural Brain Research (2015;286:338-46 [doi:10.1016/j.bbr.2015.03.020]).
Testosterone is related to activation of the inferior frontal gyrus during emotion face processing in men with schizophrenia but not in healthy patients, according to Ellen Ji and her associates.
The investigators assessed 16 males with schizophrenia and 16 healthy male controls by presenting them with 60 color pictures of human faces. Participants were told to pick the emotion shown using a button box, reported Ms. Ji of the University of New South Wales in Randwick, Australia, and her associates.
The men with schizophrenia showed much less inferior frontal gyrus activation than did those in the control group. Men with low-normal testosterone levels in the schizophrenia group had significantly worse face recognition results than did those with high-normal testosterone, but no correlation was found between low- and high-normal testosterone levels and face recognition in the control group.
“This preliminary finding provides the first evidence for a link between circulating testosterone levels and brain activity in a region characterized by hypoactivity during negative emotion face processing in men with schizophrenia, suggesting that an increase in normal levels of testosterone may have beneficial effects for emotion processing in men with schizophrenia,” the investigators concluded.
Find the full study in Behavioural Brain Research (2015;286:338-46 [doi:10.1016/j.bbr.2015.03.020]).
Testosterone is related to activation of the inferior frontal gyrus during emotion face processing in men with schizophrenia but not in healthy patients, according to Ellen Ji and her associates.
The investigators assessed 16 males with schizophrenia and 16 healthy male controls by presenting them with 60 color pictures of human faces. Participants were told to pick the emotion shown using a button box, reported Ms. Ji of the University of New South Wales in Randwick, Australia, and her associates.
The men with schizophrenia showed much less inferior frontal gyrus activation than did those in the control group. Men with low-normal testosterone levels in the schizophrenia group had significantly worse face recognition results than did those with high-normal testosterone, but no correlation was found between low- and high-normal testosterone levels and face recognition in the control group.
“This preliminary finding provides the first evidence for a link between circulating testosterone levels and brain activity in a region characterized by hypoactivity during negative emotion face processing in men with schizophrenia, suggesting that an increase in normal levels of testosterone may have beneficial effects for emotion processing in men with schizophrenia,” the investigators concluded.
Find the full study in Behavioural Brain Research (2015;286:338-46 [doi:10.1016/j.bbr.2015.03.020]).