User login
Obstetrics Moonshots: 50 years of discoveries
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
VIDEO: A case study in diagnosing depression or demoralization after retirement
Why is your geriatric patient whose life seemed fulfilling before retirement now talking about not feeling “right”? “Am I depressed, or is this normal,” your patient wants to know. What should be your reply, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this video, part of the Mental Health Consult series of roundtable discussions, our panel members discuss their recommendations for work-up and next steps for managing a 65-year-old recently retired man with a history of prostate cancer but no psychiatric disorders. He has some mild depressive symptoms, and he brings up suicide during the office visit.
Join our panel of experts from George Washington University, Washington, including Katalin Roth, MD, director of geriatrics and palliative medicine; April Barbour, MD, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to differentiate between the distress often inherent in life passages and mental illness, and how practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight
Why is your geriatric patient whose life seemed fulfilling before retirement now talking about not feeling “right”? “Am I depressed, or is this normal,” your patient wants to know. What should be your reply, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this video, part of the Mental Health Consult series of roundtable discussions, our panel members discuss their recommendations for work-up and next steps for managing a 65-year-old recently retired man with a history of prostate cancer but no psychiatric disorders. He has some mild depressive symptoms, and he brings up suicide during the office visit.
Join our panel of experts from George Washington University, Washington, including Katalin Roth, MD, director of geriatrics and palliative medicine; April Barbour, MD, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to differentiate between the distress often inherent in life passages and mental illness, and how practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight
Why is your geriatric patient whose life seemed fulfilling before retirement now talking about not feeling “right”? “Am I depressed, or is this normal,” your patient wants to know. What should be your reply, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this video, part of the Mental Health Consult series of roundtable discussions, our panel members discuss their recommendations for work-up and next steps for managing a 65-year-old recently retired man with a history of prostate cancer but no psychiatric disorders. He has some mild depressive symptoms, and he brings up suicide during the office visit.
Join our panel of experts from George Washington University, Washington, including Katalin Roth, MD, director of geriatrics and palliative medicine; April Barbour, MD, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to differentiate between the distress often inherent in life passages and mental illness, and how practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight

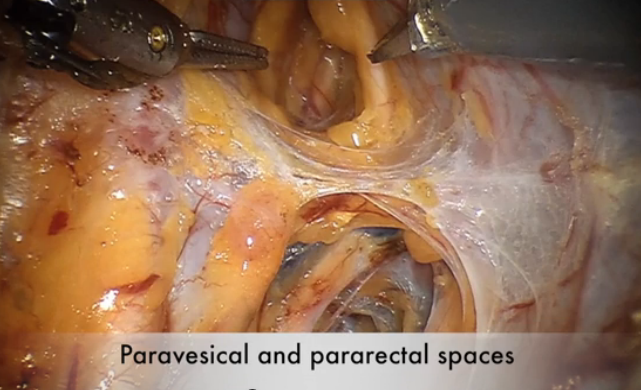
Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer

For more videos from the Society of Gynecologic Surgeons, click here
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
For more videos from the Society of Gynecologic Surgeons, click here
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
For more videos from the Society of Gynecologic Surgeons, click here
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
This video is brought to you by ![]()
VIDEO: Telecardiology improves chronic care management, reduces cost
MINNEAPOLIS – The use of telecardiology can vastly improve outcomes, reduce hospitalizations, and lower health care costs, explained Michael Shen, MD, a cardiologist and chief medical officer at Duxlink Health in Sunrise, Fla.
Dr. Shen recently spoke at the American Telemedicine Association annual meeting about the impact of telecardiology on the practice of cardiology.
“This is at the very beginning of the technology, and it will be very good for cardiologists to be early adopters – to be the early users – so they can engage the technology as leaders, rather than followers,” explained Dr. Shen.
In a video interview at the meeting, he discussed how telecardiology has advanced over the years and how the technology can improve chronic care management. Dr. Shen also shared details about a telecardiology program implemented in his practice, and he discussed how the program has affected patient care and hospital readmissions.
Dr. Shen had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
MINNEAPOLIS – The use of telecardiology can vastly improve outcomes, reduce hospitalizations, and lower health care costs, explained Michael Shen, MD, a cardiologist and chief medical officer at Duxlink Health in Sunrise, Fla.
Dr. Shen recently spoke at the American Telemedicine Association annual meeting about the impact of telecardiology on the practice of cardiology.
“This is at the very beginning of the technology, and it will be very good for cardiologists to be early adopters – to be the early users – so they can engage the technology as leaders, rather than followers,” explained Dr. Shen.
In a video interview at the meeting, he discussed how telecardiology has advanced over the years and how the technology can improve chronic care management. Dr. Shen also shared details about a telecardiology program implemented in his practice, and he discussed how the program has affected patient care and hospital readmissions.
Dr. Shen had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
MINNEAPOLIS – The use of telecardiology can vastly improve outcomes, reduce hospitalizations, and lower health care costs, explained Michael Shen, MD, a cardiologist and chief medical officer at Duxlink Health in Sunrise, Fla.
Dr. Shen recently spoke at the American Telemedicine Association annual meeting about the impact of telecardiology on the practice of cardiology.
“This is at the very beginning of the technology, and it will be very good for cardiologists to be early adopters – to be the early users – so they can engage the technology as leaders, rather than followers,” explained Dr. Shen.
In a video interview at the meeting, he discussed how telecardiology has advanced over the years and how the technology can improve chronic care management. Dr. Shen also shared details about a telecardiology program implemented in his practice, and he discussed how the program has affected patient care and hospital readmissions.
Dr. Shen had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med

VIDEO: Minimal disease activity criteria sought for axial spondyloarthritis
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.

“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.
“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.
“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE 2016 SPARTAN ANNUAL MEETING

Promoting your older patient’s healthy ‘brain aging’

VIDEO: Alzheimer’s anti-tau drug fails, but shows hint of effect when taken alone
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT AAIC 2016
Key clinical point: Negative primary outcomes from a phase III trial of the anti-tau drug LMTX for Alzheimer’s disease were tempered by intriguing positive subanalysis data.
Major finding: ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those for patients taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls.
Data source: A phase III trial of the anti-tau drug LMTX in 891 patients with mild-moderate Alzheimer’s disease.
Disclosures: The trial was sponsored by TauRx. Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.

VIDEO: Proposed Alzheimer’s funding boost could mean wider research scope
TORONTO – In 2011, President Barack Obama signed into law the National Alzheimer’s Project Act, with the lofty goal of preventing or effectively treating Alzheimer’s disease by 2025. A year later, a panel of leading researchers translated that goal into harsh reality: Reaching it would cost at least $2 billion each year. That level of funding would put Alzheimer’s research on the same footing as research on cancer, heart disease, and HIV – areas that have experienced rapid and sustained clinical progress.
But securing federal funding support has been a slow go. At the end of 2016, even with historic funding increases, the total allocation still fell short of $1 billion. That’s about to change for the better. The proposed 2017 budget, if approved, will boost the allocation to $1.4 billion.
What will that new money mean to researchers who’ve struggled for years to get grants? And what could it mean to doctors, patients, and families who still face a devastating disease with no cure, no prevention, and no effective treatments? Robert J. Egge, chief public policy officer for the Alzheimer’s Association, breaks it down in this video interview at the Alzheimer’s Association International Conference 2016.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – In 2011, President Barack Obama signed into law the National Alzheimer’s Project Act, with the lofty goal of preventing or effectively treating Alzheimer’s disease by 2025. A year later, a panel of leading researchers translated that goal into harsh reality: Reaching it would cost at least $2 billion each year. That level of funding would put Alzheimer’s research on the same footing as research on cancer, heart disease, and HIV – areas that have experienced rapid and sustained clinical progress.
But securing federal funding support has been a slow go. At the end of 2016, even with historic funding increases, the total allocation still fell short of $1 billion. That’s about to change for the better. The proposed 2017 budget, if approved, will boost the allocation to $1.4 billion.
What will that new money mean to researchers who’ve struggled for years to get grants? And what could it mean to doctors, patients, and families who still face a devastating disease with no cure, no prevention, and no effective treatments? Robert J. Egge, chief public policy officer for the Alzheimer’s Association, breaks it down in this video interview at the Alzheimer’s Association International Conference 2016.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – In 2011, President Barack Obama signed into law the National Alzheimer’s Project Act, with the lofty goal of preventing or effectively treating Alzheimer’s disease by 2025. A year later, a panel of leading researchers translated that goal into harsh reality: Reaching it would cost at least $2 billion each year. That level of funding would put Alzheimer’s research on the same footing as research on cancer, heart disease, and HIV – areas that have experienced rapid and sustained clinical progress.
But securing federal funding support has been a slow go. At the end of 2016, even with historic funding increases, the total allocation still fell short of $1 billion. That’s about to change for the better. The proposed 2017 budget, if approved, will boost the allocation to $1.4 billion.
What will that new money mean to researchers who’ve struggled for years to get grants? And what could it mean to doctors, patients, and families who still face a devastating disease with no cure, no prevention, and no effective treatments? Robert J. Egge, chief public policy officer for the Alzheimer’s Association, breaks it down in this video interview at the Alzheimer’s Association International Conference 2016.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT AAIC 2016

VIDEO: Loss of function in Rab10 gene cuts Alzheimer’s risk by up to 40%
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT AAIC 2016

Webcast: Hormonal contraception and risk of venous thromboembolism

Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:
Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:
Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:
