User login
Official Newspaper of the American College of Surgeons
Apply by June 1 for Claude Organ, Jr., MD, FACS, Traveling Fellowship
As a lasting memorial to the extraordinary life and work of the late Claude H. Organ, Jr., MD, FACS, former ACS President, his family and friends established an endowment through the American College of Surgeons (ACS) Foundation in 2008 to provide funding for an annual fellowship to be awarded to an outstanding surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association. The fellowship is available to a U.S. or Canadian ACS Fellow who is 45 years old or younger. The award of $5,000 will support the travel, per diem, and course costs for the recipient to attend a meeting or make a research-related visit.
The full requirements for the 2015 traveling fellowship are posted on the ACS website at https://www.facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, and decisions will be made by July 31. Questions and applications should be submitted to the attention of the ACS Scholarships Administrator at kearly@facs.org.
As a lasting memorial to the extraordinary life and work of the late Claude H. Organ, Jr., MD, FACS, former ACS President, his family and friends established an endowment through the American College of Surgeons (ACS) Foundation in 2008 to provide funding for an annual fellowship to be awarded to an outstanding surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association. The fellowship is available to a U.S. or Canadian ACS Fellow who is 45 years old or younger. The award of $5,000 will support the travel, per diem, and course costs for the recipient to attend a meeting or make a research-related visit.
The full requirements for the 2015 traveling fellowship are posted on the ACS website at https://www.facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, and decisions will be made by July 31. Questions and applications should be submitted to the attention of the ACS Scholarships Administrator at kearly@facs.org.
As a lasting memorial to the extraordinary life and work of the late Claude H. Organ, Jr., MD, FACS, former ACS President, his family and friends established an endowment through the American College of Surgeons (ACS) Foundation in 2008 to provide funding for an annual fellowship to be awarded to an outstanding surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association. The fellowship is available to a U.S. or Canadian ACS Fellow who is 45 years old or younger. The award of $5,000 will support the travel, per diem, and course costs for the recipient to attend a meeting or make a research-related visit.
The full requirements for the 2015 traveling fellowship are posted on the ACS website at https://www.facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, and decisions will be made by July 31. Questions and applications should be submitted to the attention of the ACS Scholarships Administrator at kearly@facs.org.
Wall Street Journal features ‘enhanced recovery’ protocols
Enhanced recovery” protocols are changing surgical patients’ perioperative care and improving outcomes, according to an article in the March 30 issue of The Wall Street Journal (WSJ).
WSJ journalist Laura Landro, who writes “The Informed Patient” column, interviews Traci Hedrick, MD, FACS, co-author of a study published online at https://www.facs.org/media/press%20releases/jacs/colorectal0205 in February in the Journal of the American College of Surgeons. Dr. Hedrick’s team at the University of Virginia Health System, Charlottesville, found that when used in colorectal-surgery patients, enhanced recovery contributed to reducing length of hospital stay by 2.2 days compared with a control group. Furthermore, complications were reduced by 17 percent, patient satisfaction with pain control increased by 55 percent, and overall estimated cost savings was $7,129 per patient. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) is pursuing an initiative for increased acceptance of enhanced recovery protocols throughout surgery. Profiled in the article is a positive patient care enhanced recovery experience at Duke University Medical Center, Durham, NC. In addition, “Kaiser Permanente Northern California is currently rolling out the enhanced recovery protocol in its 21 medical centers, focusing first on colorectal surgery and hip fracture patients. It plans to expand the program soon to total joint replacement,” Ms. Landro reports.
Ms. Landro writes of this “national initiative led by experts including Julie Thacker, [MD] assistant professor of surgery at Duke University School of Medicine and medical director of the enhanced recovery program at Duke University Hospital, which has been able to reduce hospital stays and readmissions with the approach.”
For details on ACS NSQIP’s role in enhanced recovery, contact: acsnsqip@facs.org.
Read the full text of the article and view the news video online at http://tinyurl.com/l3pmrvd.
Enhanced recovery” protocols are changing surgical patients’ perioperative care and improving outcomes, according to an article in the March 30 issue of The Wall Street Journal (WSJ).
WSJ journalist Laura Landro, who writes “The Informed Patient” column, interviews Traci Hedrick, MD, FACS, co-author of a study published online at https://www.facs.org/media/press%20releases/jacs/colorectal0205 in February in the Journal of the American College of Surgeons. Dr. Hedrick’s team at the University of Virginia Health System, Charlottesville, found that when used in colorectal-surgery patients, enhanced recovery contributed to reducing length of hospital stay by 2.2 days compared with a control group. Furthermore, complications were reduced by 17 percent, patient satisfaction with pain control increased by 55 percent, and overall estimated cost savings was $7,129 per patient. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) is pursuing an initiative for increased acceptance of enhanced recovery protocols throughout surgery. Profiled in the article is a positive patient care enhanced recovery experience at Duke University Medical Center, Durham, NC. In addition, “Kaiser Permanente Northern California is currently rolling out the enhanced recovery protocol in its 21 medical centers, focusing first on colorectal surgery and hip fracture patients. It plans to expand the program soon to total joint replacement,” Ms. Landro reports.
Ms. Landro writes of this “national initiative led by experts including Julie Thacker, [MD] assistant professor of surgery at Duke University School of Medicine and medical director of the enhanced recovery program at Duke University Hospital, which has been able to reduce hospital stays and readmissions with the approach.”
For details on ACS NSQIP’s role in enhanced recovery, contact: acsnsqip@facs.org.
Read the full text of the article and view the news video online at http://tinyurl.com/l3pmrvd.
Enhanced recovery” protocols are changing surgical patients’ perioperative care and improving outcomes, according to an article in the March 30 issue of The Wall Street Journal (WSJ).
WSJ journalist Laura Landro, who writes “The Informed Patient” column, interviews Traci Hedrick, MD, FACS, co-author of a study published online at https://www.facs.org/media/press%20releases/jacs/colorectal0205 in February in the Journal of the American College of Surgeons. Dr. Hedrick’s team at the University of Virginia Health System, Charlottesville, found that when used in colorectal-surgery patients, enhanced recovery contributed to reducing length of hospital stay by 2.2 days compared with a control group. Furthermore, complications were reduced by 17 percent, patient satisfaction with pain control increased by 55 percent, and overall estimated cost savings was $7,129 per patient. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) is pursuing an initiative for increased acceptance of enhanced recovery protocols throughout surgery. Profiled in the article is a positive patient care enhanced recovery experience at Duke University Medical Center, Durham, NC. In addition, “Kaiser Permanente Northern California is currently rolling out the enhanced recovery protocol in its 21 medical centers, focusing first on colorectal surgery and hip fracture patients. It plans to expand the program soon to total joint replacement,” Ms. Landro reports.
Ms. Landro writes of this “national initiative led by experts including Julie Thacker, [MD] assistant professor of surgery at Duke University School of Medicine and medical director of the enhanced recovery program at Duke University Hospital, which has been able to reduce hospital stays and readmissions with the approach.”
For details on ACS NSQIP’s role in enhanced recovery, contact: acsnsqip@facs.org.
Read the full text of the article and view the news video online at http://tinyurl.com/l3pmrvd.
Lancet Commission on Global Surgery to host forum May 6 in Boston, MA
The Lancet Commission on Global Surgery will host its North American launch of Global Surgery 2030 May 6, at the Joseph B. Martin Conference Center, Harvard University Medical School, Boston, MA.
Global Surgery 2030 will examine the Commission’s key findings on surgical care and universal public health measures and the role of stakeholders in building a movement for equitable, sustainable health systems.
Paul Farmer, MD, co-founder of Partners In Health, will deliver the keynote address at the day-long session. Jim Yong Kim, MD, PhD, the current president of the World Bank Group, will address the gathering via a video presentation, and panel discussions of surgical issues and public health matters will follow. ACS Executive Director David B. Hoyt, MD, FACS, will be among the participants in the discussions.
View the agenda online at http://www.globalsurgery.info/global-surgery-2030/. Register online at http://goo.gl/j1olRS. Registration is free and open to the public. An update on the Lancet Commission’s activities and its executive summary appear in the April and June 2015 issues, respectively, of the Bulletin of the American College of Surgeons, available at http://bulletin.facs.org/.
The Lancet Commission on Global Surgery will host its North American launch of Global Surgery 2030 May 6, at the Joseph B. Martin Conference Center, Harvard University Medical School, Boston, MA.
Global Surgery 2030 will examine the Commission’s key findings on surgical care and universal public health measures and the role of stakeholders in building a movement for equitable, sustainable health systems.
Paul Farmer, MD, co-founder of Partners In Health, will deliver the keynote address at the day-long session. Jim Yong Kim, MD, PhD, the current president of the World Bank Group, will address the gathering via a video presentation, and panel discussions of surgical issues and public health matters will follow. ACS Executive Director David B. Hoyt, MD, FACS, will be among the participants in the discussions.
View the agenda online at http://www.globalsurgery.info/global-surgery-2030/. Register online at http://goo.gl/j1olRS. Registration is free and open to the public. An update on the Lancet Commission’s activities and its executive summary appear in the April and June 2015 issues, respectively, of the Bulletin of the American College of Surgeons, available at http://bulletin.facs.org/.
The Lancet Commission on Global Surgery will host its North American launch of Global Surgery 2030 May 6, at the Joseph B. Martin Conference Center, Harvard University Medical School, Boston, MA.
Global Surgery 2030 will examine the Commission’s key findings on surgical care and universal public health measures and the role of stakeholders in building a movement for equitable, sustainable health systems.
Paul Farmer, MD, co-founder of Partners In Health, will deliver the keynote address at the day-long session. Jim Yong Kim, MD, PhD, the current president of the World Bank Group, will address the gathering via a video presentation, and panel discussions of surgical issues and public health matters will follow. ACS Executive Director David B. Hoyt, MD, FACS, will be among the participants in the discussions.
View the agenda online at http://www.globalsurgery.info/global-surgery-2030/. Register online at http://goo.gl/j1olRS. Registration is free and open to the public. An update on the Lancet Commission’s activities and its executive summary appear in the April and June 2015 issues, respectively, of the Bulletin of the American College of Surgeons, available at http://bulletin.facs.org/.
Clinical Congress 2015 Panel Sessions
The American College of Surgeons (ACS) Clinical Congress 2015, October 4-8 in Chicago, IL, will offer more than 100 Panel Sessions from leading experts. With the goal of fostering high-quality surgical care, these innovative sessions will cover a range of multispecialty topics of interest to surgeons, including the following:
• The Lancet Commission on Global Surgery: Evidence and Solutions for Achieving Health, Welfare, and Economic Development
• Women’s Health Day Panel Sessions:
–Gynecology for the Non-Gynecologic Surgeon
–The Surgeon’s Role in Treating Endocrine and Metabolic Disorders
–Cardiovascular Disease: It’s Not Just About Men
–What’s New in Body Contouring and Reconstructive Surgery
–Managing Pelvic Floor Disorders
• 10 Hot Topics in Clinical Care
• Challenging Paradigms in the Management of Breast Cancer: Is Less Surgery Really Better?
• Thoracic Aortic Disease Management: From the Aortic Valve to the Bifurcation
• Managing the Unexpected Adnexal Mass
• Challenging Trauma Lessons from the Experts
• New Horizons in Skull-Based Surgery
• Enhanced Recovery Protocols for Gastrointestinal Surgery: The SMART Approach
• Modern Management of the Mangled Extremity
Watch for the ACS Clinical Congress 2015 Program Planner and the online registration site, which will become available in June.
Visit the ACS website at https://www.facs.org/education/clinical-congress or contact PanelSessions@facs.org to get more information.
The American College of Surgeons (ACS) Clinical Congress 2015, October 4-8 in Chicago, IL, will offer more than 100 Panel Sessions from leading experts. With the goal of fostering high-quality surgical care, these innovative sessions will cover a range of multispecialty topics of interest to surgeons, including the following:
• The Lancet Commission on Global Surgery: Evidence and Solutions for Achieving Health, Welfare, and Economic Development
• Women’s Health Day Panel Sessions:
–Gynecology for the Non-Gynecologic Surgeon
–The Surgeon’s Role in Treating Endocrine and Metabolic Disorders
–Cardiovascular Disease: It’s Not Just About Men
–What’s New in Body Contouring and Reconstructive Surgery
–Managing Pelvic Floor Disorders
• 10 Hot Topics in Clinical Care
• Challenging Paradigms in the Management of Breast Cancer: Is Less Surgery Really Better?
• Thoracic Aortic Disease Management: From the Aortic Valve to the Bifurcation
• Managing the Unexpected Adnexal Mass
• Challenging Trauma Lessons from the Experts
• New Horizons in Skull-Based Surgery
• Enhanced Recovery Protocols for Gastrointestinal Surgery: The SMART Approach
• Modern Management of the Mangled Extremity
Watch for the ACS Clinical Congress 2015 Program Planner and the online registration site, which will become available in June.
Visit the ACS website at https://www.facs.org/education/clinical-congress or contact PanelSessions@facs.org to get more information.
The American College of Surgeons (ACS) Clinical Congress 2015, October 4-8 in Chicago, IL, will offer more than 100 Panel Sessions from leading experts. With the goal of fostering high-quality surgical care, these innovative sessions will cover a range of multispecialty topics of interest to surgeons, including the following:
• The Lancet Commission on Global Surgery: Evidence and Solutions for Achieving Health, Welfare, and Economic Development
• Women’s Health Day Panel Sessions:
–Gynecology for the Non-Gynecologic Surgeon
–The Surgeon’s Role in Treating Endocrine and Metabolic Disorders
–Cardiovascular Disease: It’s Not Just About Men
–What’s New in Body Contouring and Reconstructive Surgery
–Managing Pelvic Floor Disorders
• 10 Hot Topics in Clinical Care
• Challenging Paradigms in the Management of Breast Cancer: Is Less Surgery Really Better?
• Thoracic Aortic Disease Management: From the Aortic Valve to the Bifurcation
• Managing the Unexpected Adnexal Mass
• Challenging Trauma Lessons from the Experts
• New Horizons in Skull-Based Surgery
• Enhanced Recovery Protocols for Gastrointestinal Surgery: The SMART Approach
• Modern Management of the Mangled Extremity
Watch for the ACS Clinical Congress 2015 Program Planner and the online registration site, which will become available in June.
Visit the ACS website at https://www.facs.org/education/clinical-congress or contact PanelSessions@facs.org to get more information.
ACS Surgical History Group accepting poster abstracts
The Surgical History Group (SHG) of the American College of Surgeons (ACS) has issued a call for abstracts for the inaugural ACS SHG Poster Presentation at Clinical Congress 2015, October 4−8 at McCormick Place, Chicago, IL. The College encourages submissions from ACS Fellows, Retired and Senior Members, International Fellows, Resident and Associate Society Members, and Medical Student Members with an ACS sponsor. The deadline for abstract submissions is 5:00 pm CDT, Friday, May 29.
The posters should examine the historical impact on the development of today’s ACS surgeon. The authors of posters chosen for display will receive continuing medical education credit and will be notified by July 15. View the ACS website at https://www.facs.org/about-acs/archives for set-up and presentation guidelines as well as answers to frequently asked questions. Submit abstracts and additional questions to Adam Carey, MA, MLIS, ACS Archivist and SHG Coordinator, at acarey@facs.org. Abstracts must be limited to 250 words. Late submissions will not be accepted.
The Surgical History Group (SHG) of the American College of Surgeons (ACS) has issued a call for abstracts for the inaugural ACS SHG Poster Presentation at Clinical Congress 2015, October 4−8 at McCormick Place, Chicago, IL. The College encourages submissions from ACS Fellows, Retired and Senior Members, International Fellows, Resident and Associate Society Members, and Medical Student Members with an ACS sponsor. The deadline for abstract submissions is 5:00 pm CDT, Friday, May 29.
The posters should examine the historical impact on the development of today’s ACS surgeon. The authors of posters chosen for display will receive continuing medical education credit and will be notified by July 15. View the ACS website at https://www.facs.org/about-acs/archives for set-up and presentation guidelines as well as answers to frequently asked questions. Submit abstracts and additional questions to Adam Carey, MA, MLIS, ACS Archivist and SHG Coordinator, at acarey@facs.org. Abstracts must be limited to 250 words. Late submissions will not be accepted.
The Surgical History Group (SHG) of the American College of Surgeons (ACS) has issued a call for abstracts for the inaugural ACS SHG Poster Presentation at Clinical Congress 2015, October 4−8 at McCormick Place, Chicago, IL. The College encourages submissions from ACS Fellows, Retired and Senior Members, International Fellows, Resident and Associate Society Members, and Medical Student Members with an ACS sponsor. The deadline for abstract submissions is 5:00 pm CDT, Friday, May 29.
The posters should examine the historical impact on the development of today’s ACS surgeon. The authors of posters chosen for display will receive continuing medical education credit and will be notified by July 15. View the ACS website at https://www.facs.org/about-acs/archives for set-up and presentation guidelines as well as answers to frequently asked questions. Submit abstracts and additional questions to Adam Carey, MA, MLIS, ACS Archivist and SHG Coordinator, at acarey@facs.org. Abstracts must be limited to 250 words. Late submissions will not be accepted.
VIDEO: Hybrid thoracoscopic and transcatheter ablation of persistent AF
SEATTLE – The presentation of the late-breaking HISTORIC-AF Trial by Dr. Claudio Muneretto and his colleagues “is a very interesting one, which brings to the table a very different approach of hybrid procedures to treat stand-alone atrial fibrillation,” said Dr. Niv Ad of Inova Heart and Vascular Institute, Falls Church, Va.
Dr. Ad gave his comments in a video interview at the annual meeting of the American Association for Thoracic Surgery.
In his assessment, Dr. Ad noted that such studies are useful and can stimulate discussion, even if he would prefer a prospective, comparative study of all procedures. “I hope someday we can create an algorithm where everything has a place: catheter ablation, hybrid procedures where you do catheter ablation and surgical procedure together or in stage, and the stand-alone Maze procedure on pump,” Dr. Ad said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – The presentation of the late-breaking HISTORIC-AF Trial by Dr. Claudio Muneretto and his colleagues “is a very interesting one, which brings to the table a very different approach of hybrid procedures to treat stand-alone atrial fibrillation,” said Dr. Niv Ad of Inova Heart and Vascular Institute, Falls Church, Va.
Dr. Ad gave his comments in a video interview at the annual meeting of the American Association for Thoracic Surgery.
In his assessment, Dr. Ad noted that such studies are useful and can stimulate discussion, even if he would prefer a prospective, comparative study of all procedures. “I hope someday we can create an algorithm where everything has a place: catheter ablation, hybrid procedures where you do catheter ablation and surgical procedure together or in stage, and the stand-alone Maze procedure on pump,” Dr. Ad said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – The presentation of the late-breaking HISTORIC-AF Trial by Dr. Claudio Muneretto and his colleagues “is a very interesting one, which brings to the table a very different approach of hybrid procedures to treat stand-alone atrial fibrillation,” said Dr. Niv Ad of Inova Heart and Vascular Institute, Falls Church, Va.
Dr. Ad gave his comments in a video interview at the annual meeting of the American Association for Thoracic Surgery.
In his assessment, Dr. Ad noted that such studies are useful and can stimulate discussion, even if he would prefer a prospective, comparative study of all procedures. “I hope someday we can create an algorithm where everything has a place: catheter ablation, hybrid procedures where you do catheter ablation and surgical procedure together or in stage, and the stand-alone Maze procedure on pump,” Dr. Ad said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AATS ANNUAL MEETING

VIDEO: Esophagectomy outcomes better in hospitals that handle complex cases
SEATTLE – Hospitals that perform at least one nongastric conduit esophageal reconstruction per year have half the esophagectomy mortality of hospitals that do not, according to a review by the Mayo Clinic in Rochester, Minn., of 11,211 esophagectomies in the Nationwide Inpatient Sample database from 2000 to 2011.
“There is tremendous variation in outcome after esophagectomy, and some advocate for regionalization to high-volume hospitals,” the investigators said. The findings suggest that case complexity could be one of the things that help define which hospitals do it best, they added.
The study seems to confirm that hospital case volume makes a difference in surgical outcomes, said Dr. Nabil Rizk, a thoracic surgeon at Memorial Sloan-Kettering Cancer Center in New York.
Dr. Rizk, a discussant on the paper at the American Association for Thoracic Surgery annual meeting, explained how the study fits into regionalization trends, but also shared his concerns about the work in an interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Hospitals that perform at least one nongastric conduit esophageal reconstruction per year have half the esophagectomy mortality of hospitals that do not, according to a review by the Mayo Clinic in Rochester, Minn., of 11,211 esophagectomies in the Nationwide Inpatient Sample database from 2000 to 2011.
“There is tremendous variation in outcome after esophagectomy, and some advocate for regionalization to high-volume hospitals,” the investigators said. The findings suggest that case complexity could be one of the things that help define which hospitals do it best, they added.
The study seems to confirm that hospital case volume makes a difference in surgical outcomes, said Dr. Nabil Rizk, a thoracic surgeon at Memorial Sloan-Kettering Cancer Center in New York.
Dr. Rizk, a discussant on the paper at the American Association for Thoracic Surgery annual meeting, explained how the study fits into regionalization trends, but also shared his concerns about the work in an interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Hospitals that perform at least one nongastric conduit esophageal reconstruction per year have half the esophagectomy mortality of hospitals that do not, according to a review by the Mayo Clinic in Rochester, Minn., of 11,211 esophagectomies in the Nationwide Inpatient Sample database from 2000 to 2011.
“There is tremendous variation in outcome after esophagectomy, and some advocate for regionalization to high-volume hospitals,” the investigators said. The findings suggest that case complexity could be one of the things that help define which hospitals do it best, they added.
The study seems to confirm that hospital case volume makes a difference in surgical outcomes, said Dr. Nabil Rizk, a thoracic surgeon at Memorial Sloan-Kettering Cancer Center in New York.
Dr. Rizk, a discussant on the paper at the American Association for Thoracic Surgery annual meeting, explained how the study fits into regionalization trends, but also shared his concerns about the work in an interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AATS ANNUAL MEETING

VIDEO: Cardiosphere-derived cells improve outcomes in hypoplastic left heart syndrome
SEATTLE – Autologous stem cell therapy improves surgery outcomes in children with hypoplastic left heart syndrome, according to the results of a small prospective trial from Okayama University in Japan.
The investigators cultured cardiosphere-derived cells (CDCs) – cardiac progenitor cells – from right atrium samples taken during stage 2 or 3 surgical palliations in seven HLHS children. A month later, they injected 300,000 CDCs/kg into the children’s coronary arteries by catheter, with each child getting cells cultured from their own tissue.
The cells seemed to jump-start the intrinsic regenerative properties of very young hearts. At 30 months follow-up, right ventricular mass and ejection fractions were about 10% greater in CDC treated patients compared to seven controls. Treated children also had better growth.
It’s possible the technique could help older children, too, and even adults, said lead investigator Dr. Shunji Sano, professor and chairman of the department of cardiovascular surgery at Okayama. He explained the work, its implications, and the next phase of research in an interview at the annual meeting of the American Association for Thoracic Surgery.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Autologous stem cell therapy improves surgery outcomes in children with hypoplastic left heart syndrome, according to the results of a small prospective trial from Okayama University in Japan.
The investigators cultured cardiosphere-derived cells (CDCs) – cardiac progenitor cells – from right atrium samples taken during stage 2 or 3 surgical palliations in seven HLHS children. A month later, they injected 300,000 CDCs/kg into the children’s coronary arteries by catheter, with each child getting cells cultured from their own tissue.
The cells seemed to jump-start the intrinsic regenerative properties of very young hearts. At 30 months follow-up, right ventricular mass and ejection fractions were about 10% greater in CDC treated patients compared to seven controls. Treated children also had better growth.
It’s possible the technique could help older children, too, and even adults, said lead investigator Dr. Shunji Sano, professor and chairman of the department of cardiovascular surgery at Okayama. He explained the work, its implications, and the next phase of research in an interview at the annual meeting of the American Association for Thoracic Surgery.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Autologous stem cell therapy improves surgery outcomes in children with hypoplastic left heart syndrome, according to the results of a small prospective trial from Okayama University in Japan.
The investigators cultured cardiosphere-derived cells (CDCs) – cardiac progenitor cells – from right atrium samples taken during stage 2 or 3 surgical palliations in seven HLHS children. A month later, they injected 300,000 CDCs/kg into the children’s coronary arteries by catheter, with each child getting cells cultured from their own tissue.
The cells seemed to jump-start the intrinsic regenerative properties of very young hearts. At 30 months follow-up, right ventricular mass and ejection fractions were about 10% greater in CDC treated patients compared to seven controls. Treated children also had better growth.
It’s possible the technique could help older children, too, and even adults, said lead investigator Dr. Shunji Sano, professor and chairman of the department of cardiovascular surgery at Okayama. He explained the work, its implications, and the next phase of research in an interview at the annual meeting of the American Association for Thoracic Surgery.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AATS ANNUAL MEETING

VIDEO: Less tricuspid regurgitation seen with Sano shunt in Norwood procedures
SEATTLE – Sano shunts outperform Blalock-Taussig shunts for Norwood procedures in neonates with hypoplastic left heart syndrome, according to a research registry study of 322 patients at the Cleveland Clinic and elsewhere.
The 166 newborns who had Sano shunts were matched to 166 who had Blalock-Taussig (BT) shunts.
“For comparable neonates with HLHS [hypoplastic left heart syndrome] undergoing Norwood operations, Sano offers better late survival [more than 3 years], less late tricuspid regurgitation, and perhaps less late right ventricular dysfunction than BT,” the investigators concluded.
Even so, Dr. Richard Ohye, professor of cardiac surgery at the University of Michigan, Ann Arbor, said the jury is still out on which shunt is best. He explained why in an interview at the American Association for Thoracic Surgery annual meeting. He also shared tips on shunt selection and explained a novel technique he has developed for doing a Sano shunt with a smaller hole in the right ventricle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Sano shunts outperform Blalock-Taussig shunts for Norwood procedures in neonates with hypoplastic left heart syndrome, according to a research registry study of 322 patients at the Cleveland Clinic and elsewhere.
The 166 newborns who had Sano shunts were matched to 166 who had Blalock-Taussig (BT) shunts.
“For comparable neonates with HLHS [hypoplastic left heart syndrome] undergoing Norwood operations, Sano offers better late survival [more than 3 years], less late tricuspid regurgitation, and perhaps less late right ventricular dysfunction than BT,” the investigators concluded.
Even so, Dr. Richard Ohye, professor of cardiac surgery at the University of Michigan, Ann Arbor, said the jury is still out on which shunt is best. He explained why in an interview at the American Association for Thoracic Surgery annual meeting. He also shared tips on shunt selection and explained a novel technique he has developed for doing a Sano shunt with a smaller hole in the right ventricle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SEATTLE – Sano shunts outperform Blalock-Taussig shunts for Norwood procedures in neonates with hypoplastic left heart syndrome, according to a research registry study of 322 patients at the Cleveland Clinic and elsewhere.
The 166 newborns who had Sano shunts were matched to 166 who had Blalock-Taussig (BT) shunts.
“For comparable neonates with HLHS [hypoplastic left heart syndrome] undergoing Norwood operations, Sano offers better late survival [more than 3 years], less late tricuspid regurgitation, and perhaps less late right ventricular dysfunction than BT,” the investigators concluded.
Even so, Dr. Richard Ohye, professor of cardiac surgery at the University of Michigan, Ann Arbor, said the jury is still out on which shunt is best. He explained why in an interview at the American Association for Thoracic Surgery annual meeting. He also shared tips on shunt selection and explained a novel technique he has developed for doing a Sano shunt with a smaller hole in the right ventricle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AATS ANNUAL MEETING

AAN: Facial nerve stimulator relieves cluster headaches
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
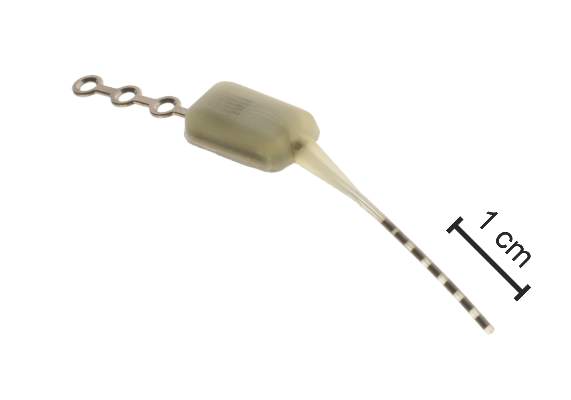
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
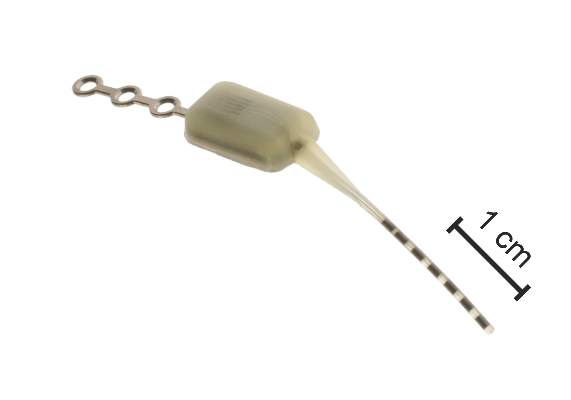
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING
Key clinical point: An implantable device that stimulates the sphenopalatine ganglion nerve provided pain relief in cluster headaches.
Major finding: The device reduced or eliminated pain in 68% of more than 5,000 cluster headaches.
Data source: A 3-year follow-up study that examined response in more than 5,000 cluster headaches.
Disclosures: The trial was sponsored by Autonomic Technologies Inc., which makes the Pulsante System. Dr. Lainez had no financial disclosures.