User login
Official Newspaper of the American College of Surgeons
New Cushing’s guidelines emphasize team approach
New clinical practice guidelines for the treatment of Cushing’s syndrome stress coordinated care and patient involvement, and solidify an evidence-based treatment path for surgical and medical treatment options. The Endocrine Society released the guidelines, which were developed in conjunction with the European Society of Endocrinology (J Clin Endocrinol Metab. 2015 Aug;100[8]:2807-2831).
Dr. Lynette Nieman, chair of the task force that developed the guidelines, commented in an interview that the guidelines don’t really contain new or controversial elements, but they do help clarify existing best practices. “This is not a common diagnosis, but it is very important to understand how to handle this disorder,” said Dr. Nieman of the program in reproductive and adult endocrinology at the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md. “Cushing’s syndrome really needs to be treated with a team approach and by expert surgeons and expert endocrinologists,” she said.

In establishing treatment goals, the guidelines emphasize clinically based treatment, only recommending normalization of cortisol levels or action when overt Cushing’s syndrome (CS) and an established diagnosis exist (grade 1 recommendation). “Surgical resection of the causal lesion(s) is generally the first-line approach,” said Dr. Nieman and coauthors (grade 1 recommendation). Medical management of comorbidities and sequelae of hypercortisolism should always accompany any medical or surgical treatment. The guidelines also provide for emergent surgical or medical management of hypercortisolism if life-threatening complications are present (grade 1 recommendation).
Adjunctive management is directed at a patient-centered, multidisciplinary approach to address potential cortisol-dependent comorbidities. These may include hypertension and dyslipidemia, diabetes, electrolyte disturbances, increased infection risk, osteoporosis and deconditioning, and psychiatric illnesses (ungraded best practice recommendation). Additionally, the guidelines recommend perioperative prophylaxis for venous thromboembolism for CS patients (grade 2 recommendation).
For Cushing’s disease (CD), the guidelines recommend excision of ectopic and adrenal lesions, barring contraindications or low likelihood of successful surgery, with unilateral adrenal resection by an experienced adrenal surgeon recommended in benign unilateral disease. Ectopic adrenocorticotropic hormone (ACTH)–secreting tumors should be resected, with local node dissection as appropriate. Transsphenoidal selective adenomectomy is the recommended treatment for CD in adults and children, and should be performed by an experienced pituitary surgeon. Serum sodium should be measured several times during the first 2 weeks after surgery, and free T4 and prolactin by no more than 2 weeks after surgery (all grade 1 recommendations).
The task force recommends an MRI by 3 months after transsphenoidal surgery (ungraded best practice recommendation). When adrenal disorders are bilateral, the task force recommends surgical resection and medical therapy to block aberrant hormone receptors (grade 2 recommendation).
Carrying through the theme of an individualized, patient-centered approach, the task force recommends individualized postoperative management depending on postoperative cortisol levels. Persistent and overt postsurgical hypercortisolism should be treated, while patients with eucortisolism should have serum or salivary cortisol measured late at night. Patients with ACTH-dependent CS should be screened for recurrence of hypercortisolism (all grade 1 recommendations).
Glucocorticoid replacement, when required for hypocortisolemic patients, should be accompanied by appropriate patient education. When patients have an intact adrenal gland remaining, hypothalamic-pituitary-adrenal (HPA) axis recovery should be assessed at follow-up, so glucocorticoids can be stopped when recovery occurs. Other pituitary hormone deficiencies may occur, and care should include assessing the need to treat these deficiencies as well (all grade 1 recommendations).
In the difficult cases where surgery is not possible or does not cure ACTH-dependent CS, shared patient decision making is recommended to choose among the various second-line therapies that may be of benefit (grade 2 recommendation).
Therapy choices may include bilateral adrenalectomy, reserved for occult or metastatic ectopic ACTH secretion, or in an emergency situation where the procedure may be lifesaving (grade 2 recommendation); repeat transsphenoidal surgery when imaging or the clinical picture points to a new lesion or incomplete resection (grade 2 recommendation); radiation therapy or radiosurgery for those who fail transsphenoidal surgery or whose CD recurs, or where mass effect may be of concern (grade 1-2 recommendations; and medical treatment with steroidogenesis inhibitors in limited circumstances (grade 1 recommendation).
Specific medical treatment recommendations include the use of steroidogenesis inhibitors after transsphenoidal surgery for patients with CD or to treat occult or metastatic cases of ectopic ACTH secretion, and as an adjunct in adrenocortical carcinoma (grade 1 recommendation). The task force, in the discussion accompanying the guidelines, lists pros and cons of the various medical choices in order to present a balanced view of medical treatment options, said Dr. Nieman.
The long-term follow-up of individuals with CS should include screening and treating for the comorbidities that may persist even after successful surgery. Follow-up should be lifelong, with each comorbidity followed to resolution and ongoing vigilance for recurrence (except in patients with successfully resected low-attenuation adrenal adenomas – grade 1 recommendation).
In an interview, Dr. Rebecca S. Sippel of the University of Wisconsin–Madison brought an endocrine surgeon’s perspective to the guidelines, agreeing that the document generally reflects accepted practice. She also agreed that the interdisciplinary approach advocated by the task force is critical. “It’s important that discharge planning is done in a systematic way, so there’s systematic follow-up of patients after excision,” she said. She noted that CS patients on her service all receive an endocrine consult while they are inpatients to ensure adequate discharge planning.
Future research directions recommended by Dr. Nieman and the task force coauthors include identification of markers that will “explain the variable clinical effect of steroids among individuals,” with the goal of achieving better quantification of treatment effect and tracking response and remission. Health care–related quality of life is negatively affected by CS even after resolution to eucortisolism in many patients, so the guidelines recommend further research into quality of life and cognitive problems experienced by individuals with CS. Dr. Nieman specifically called for more multisite research, noting that diagnoses of Cushing’s disease and Cushing’s syndrome are rare, and etiologies are varied. “In order to get the numbers we need to do good research, we will need to cooperate,” she said.
All authors of the clinical practice guidelines had financial disclosures; a complete listing of disclosures and the task force’s methodology for resolving conflicts may be found in the downloadable guidelines.
On Twitter @karioakes
New clinical practice guidelines for the treatment of Cushing’s syndrome stress coordinated care and patient involvement, and solidify an evidence-based treatment path for surgical and medical treatment options. The Endocrine Society released the guidelines, which were developed in conjunction with the European Society of Endocrinology (J Clin Endocrinol Metab. 2015 Aug;100[8]:2807-2831).
Dr. Lynette Nieman, chair of the task force that developed the guidelines, commented in an interview that the guidelines don’t really contain new or controversial elements, but they do help clarify existing best practices. “This is not a common diagnosis, but it is very important to understand how to handle this disorder,” said Dr. Nieman of the program in reproductive and adult endocrinology at the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md. “Cushing’s syndrome really needs to be treated with a team approach and by expert surgeons and expert endocrinologists,” she said.
In establishing treatment goals, the guidelines emphasize clinically based treatment, only recommending normalization of cortisol levels or action when overt Cushing’s syndrome (CS) and an established diagnosis exist (grade 1 recommendation). “Surgical resection of the causal lesion(s) is generally the first-line approach,” said Dr. Nieman and coauthors (grade 1 recommendation). Medical management of comorbidities and sequelae of hypercortisolism should always accompany any medical or surgical treatment. The guidelines also provide for emergent surgical or medical management of hypercortisolism if life-threatening complications are present (grade 1 recommendation).
Adjunctive management is directed at a patient-centered, multidisciplinary approach to address potential cortisol-dependent comorbidities. These may include hypertension and dyslipidemia, diabetes, electrolyte disturbances, increased infection risk, osteoporosis and deconditioning, and psychiatric illnesses (ungraded best practice recommendation). Additionally, the guidelines recommend perioperative prophylaxis for venous thromboembolism for CS patients (grade 2 recommendation).
For Cushing’s disease (CD), the guidelines recommend excision of ectopic and adrenal lesions, barring contraindications or low likelihood of successful surgery, with unilateral adrenal resection by an experienced adrenal surgeon recommended in benign unilateral disease. Ectopic adrenocorticotropic hormone (ACTH)–secreting tumors should be resected, with local node dissection as appropriate. Transsphenoidal selective adenomectomy is the recommended treatment for CD in adults and children, and should be performed by an experienced pituitary surgeon. Serum sodium should be measured several times during the first 2 weeks after surgery, and free T4 and prolactin by no more than 2 weeks after surgery (all grade 1 recommendations).
The task force recommends an MRI by 3 months after transsphenoidal surgery (ungraded best practice recommendation). When adrenal disorders are bilateral, the task force recommends surgical resection and medical therapy to block aberrant hormone receptors (grade 2 recommendation).
Carrying through the theme of an individualized, patient-centered approach, the task force recommends individualized postoperative management depending on postoperative cortisol levels. Persistent and overt postsurgical hypercortisolism should be treated, while patients with eucortisolism should have serum or salivary cortisol measured late at night. Patients with ACTH-dependent CS should be screened for recurrence of hypercortisolism (all grade 1 recommendations).
Glucocorticoid replacement, when required for hypocortisolemic patients, should be accompanied by appropriate patient education. When patients have an intact adrenal gland remaining, hypothalamic-pituitary-adrenal (HPA) axis recovery should be assessed at follow-up, so glucocorticoids can be stopped when recovery occurs. Other pituitary hormone deficiencies may occur, and care should include assessing the need to treat these deficiencies as well (all grade 1 recommendations).
In the difficult cases where surgery is not possible or does not cure ACTH-dependent CS, shared patient decision making is recommended to choose among the various second-line therapies that may be of benefit (grade 2 recommendation).
Therapy choices may include bilateral adrenalectomy, reserved for occult or metastatic ectopic ACTH secretion, or in an emergency situation where the procedure may be lifesaving (grade 2 recommendation); repeat transsphenoidal surgery when imaging or the clinical picture points to a new lesion or incomplete resection (grade 2 recommendation); radiation therapy or radiosurgery for those who fail transsphenoidal surgery or whose CD recurs, or where mass effect may be of concern (grade 1-2 recommendations; and medical treatment with steroidogenesis inhibitors in limited circumstances (grade 1 recommendation).
Specific medical treatment recommendations include the use of steroidogenesis inhibitors after transsphenoidal surgery for patients with CD or to treat occult or metastatic cases of ectopic ACTH secretion, and as an adjunct in adrenocortical carcinoma (grade 1 recommendation). The task force, in the discussion accompanying the guidelines, lists pros and cons of the various medical choices in order to present a balanced view of medical treatment options, said Dr. Nieman.
The long-term follow-up of individuals with CS should include screening and treating for the comorbidities that may persist even after successful surgery. Follow-up should be lifelong, with each comorbidity followed to resolution and ongoing vigilance for recurrence (except in patients with successfully resected low-attenuation adrenal adenomas – grade 1 recommendation).
In an interview, Dr. Rebecca S. Sippel of the University of Wisconsin–Madison brought an endocrine surgeon’s perspective to the guidelines, agreeing that the document generally reflects accepted practice. She also agreed that the interdisciplinary approach advocated by the task force is critical. “It’s important that discharge planning is done in a systematic way, so there’s systematic follow-up of patients after excision,” she said. She noted that CS patients on her service all receive an endocrine consult while they are inpatients to ensure adequate discharge planning.
Future research directions recommended by Dr. Nieman and the task force coauthors include identification of markers that will “explain the variable clinical effect of steroids among individuals,” with the goal of achieving better quantification of treatment effect and tracking response and remission. Health care–related quality of life is negatively affected by CS even after resolution to eucortisolism in many patients, so the guidelines recommend further research into quality of life and cognitive problems experienced by individuals with CS. Dr. Nieman specifically called for more multisite research, noting that diagnoses of Cushing’s disease and Cushing’s syndrome are rare, and etiologies are varied. “In order to get the numbers we need to do good research, we will need to cooperate,” she said.
All authors of the clinical practice guidelines had financial disclosures; a complete listing of disclosures and the task force’s methodology for resolving conflicts may be found in the downloadable guidelines.
On Twitter @karioakes
New clinical practice guidelines for the treatment of Cushing’s syndrome stress coordinated care and patient involvement, and solidify an evidence-based treatment path for surgical and medical treatment options. The Endocrine Society released the guidelines, which were developed in conjunction with the European Society of Endocrinology (J Clin Endocrinol Metab. 2015 Aug;100[8]:2807-2831).
Dr. Lynette Nieman, chair of the task force that developed the guidelines, commented in an interview that the guidelines don’t really contain new or controversial elements, but they do help clarify existing best practices. “This is not a common diagnosis, but it is very important to understand how to handle this disorder,” said Dr. Nieman of the program in reproductive and adult endocrinology at the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md. “Cushing’s syndrome really needs to be treated with a team approach and by expert surgeons and expert endocrinologists,” she said.
In establishing treatment goals, the guidelines emphasize clinically based treatment, only recommending normalization of cortisol levels or action when overt Cushing’s syndrome (CS) and an established diagnosis exist (grade 1 recommendation). “Surgical resection of the causal lesion(s) is generally the first-line approach,” said Dr. Nieman and coauthors (grade 1 recommendation). Medical management of comorbidities and sequelae of hypercortisolism should always accompany any medical or surgical treatment. The guidelines also provide for emergent surgical or medical management of hypercortisolism if life-threatening complications are present (grade 1 recommendation).
Adjunctive management is directed at a patient-centered, multidisciplinary approach to address potential cortisol-dependent comorbidities. These may include hypertension and dyslipidemia, diabetes, electrolyte disturbances, increased infection risk, osteoporosis and deconditioning, and psychiatric illnesses (ungraded best practice recommendation). Additionally, the guidelines recommend perioperative prophylaxis for venous thromboembolism for CS patients (grade 2 recommendation).
For Cushing’s disease (CD), the guidelines recommend excision of ectopic and adrenal lesions, barring contraindications or low likelihood of successful surgery, with unilateral adrenal resection by an experienced adrenal surgeon recommended in benign unilateral disease. Ectopic adrenocorticotropic hormone (ACTH)–secreting tumors should be resected, with local node dissection as appropriate. Transsphenoidal selective adenomectomy is the recommended treatment for CD in adults and children, and should be performed by an experienced pituitary surgeon. Serum sodium should be measured several times during the first 2 weeks after surgery, and free T4 and prolactin by no more than 2 weeks after surgery (all grade 1 recommendations).
The task force recommends an MRI by 3 months after transsphenoidal surgery (ungraded best practice recommendation). When adrenal disorders are bilateral, the task force recommends surgical resection and medical therapy to block aberrant hormone receptors (grade 2 recommendation).
Carrying through the theme of an individualized, patient-centered approach, the task force recommends individualized postoperative management depending on postoperative cortisol levels. Persistent and overt postsurgical hypercortisolism should be treated, while patients with eucortisolism should have serum or salivary cortisol measured late at night. Patients with ACTH-dependent CS should be screened for recurrence of hypercortisolism (all grade 1 recommendations).
Glucocorticoid replacement, when required for hypocortisolemic patients, should be accompanied by appropriate patient education. When patients have an intact adrenal gland remaining, hypothalamic-pituitary-adrenal (HPA) axis recovery should be assessed at follow-up, so glucocorticoids can be stopped when recovery occurs. Other pituitary hormone deficiencies may occur, and care should include assessing the need to treat these deficiencies as well (all grade 1 recommendations).
In the difficult cases where surgery is not possible or does not cure ACTH-dependent CS, shared patient decision making is recommended to choose among the various second-line therapies that may be of benefit (grade 2 recommendation).
Therapy choices may include bilateral adrenalectomy, reserved for occult or metastatic ectopic ACTH secretion, or in an emergency situation where the procedure may be lifesaving (grade 2 recommendation); repeat transsphenoidal surgery when imaging or the clinical picture points to a new lesion or incomplete resection (grade 2 recommendation); radiation therapy or radiosurgery for those who fail transsphenoidal surgery or whose CD recurs, or where mass effect may be of concern (grade 1-2 recommendations; and medical treatment with steroidogenesis inhibitors in limited circumstances (grade 1 recommendation).
Specific medical treatment recommendations include the use of steroidogenesis inhibitors after transsphenoidal surgery for patients with CD or to treat occult or metastatic cases of ectopic ACTH secretion, and as an adjunct in adrenocortical carcinoma (grade 1 recommendation). The task force, in the discussion accompanying the guidelines, lists pros and cons of the various medical choices in order to present a balanced view of medical treatment options, said Dr. Nieman.
The long-term follow-up of individuals with CS should include screening and treating for the comorbidities that may persist even after successful surgery. Follow-up should be lifelong, with each comorbidity followed to resolution and ongoing vigilance for recurrence (except in patients with successfully resected low-attenuation adrenal adenomas – grade 1 recommendation).
In an interview, Dr. Rebecca S. Sippel of the University of Wisconsin–Madison brought an endocrine surgeon’s perspective to the guidelines, agreeing that the document generally reflects accepted practice. She also agreed that the interdisciplinary approach advocated by the task force is critical. “It’s important that discharge planning is done in a systematic way, so there’s systematic follow-up of patients after excision,” she said. She noted that CS patients on her service all receive an endocrine consult while they are inpatients to ensure adequate discharge planning.
Future research directions recommended by Dr. Nieman and the task force coauthors include identification of markers that will “explain the variable clinical effect of steroids among individuals,” with the goal of achieving better quantification of treatment effect and tracking response and remission. Health care–related quality of life is negatively affected by CS even after resolution to eucortisolism in many patients, so the guidelines recommend further research into quality of life and cognitive problems experienced by individuals with CS. Dr. Nieman specifically called for more multisite research, noting that diagnoses of Cushing’s disease and Cushing’s syndrome are rare, and etiologies are varied. “In order to get the numbers we need to do good research, we will need to cooperate,” she said.
All authors of the clinical practice guidelines had financial disclosures; a complete listing of disclosures and the task force’s methodology for resolving conflicts may be found in the downloadable guidelines.
On Twitter @karioakes
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM

Percutaneous thrombectomy reduces risk of postthrombotic syndrome
Adding a mechanical suction technique to local thrombolysis to break up and remove blood clots reduced postthrombotic syndrome (PTS) after deep vein thrombosis (DVT) without causing increased complications, according to a small retrospective study.
Dr. Chun-Yang Huang of the National Yang Ming University (Taipei, Taiwan) and colleagues examined patients diagnosed with acute proximal lower limb DVT. Patients received either thrombolysis alone via a catheter-directed thrombolysis (CDT), or percutaneous mechanical thrombectomy (PMT) by a combination of pharmacologic thrombolysis and suction; both techniques were accompanied by systemic anticoagulation. Though both treatment groups fared well during treatment and for the 12-month follow-up period, the PMT group had a significantly lower incidence of PTS 1 year after treatment (Ann. Vascular Surg. 2015. doi: 10.1016/j.avsg.2015.01.014).
For those with DVT, parenteral anticoagulation prevents propagation of the clot and minimizes risk of pulmonary embolism (PE); however, anticoagulation does not accelerate dissolution of the existing clot. According to study authors, 30%-40% of those with proximal leg DVTs will go on to develop PTS, with the prolonged distal venous stasis from an undisturbed clot causing loss of valvular competence and resultant chronic venous insufficiency. PTS can involve leg swelling, discomfort, skin changes, and ulceration, with significant impact on quality of life and health care costs.
Techniques such as CDT and PMT can increase the rate of clot dissolution, thus restoring patency sooner and minimizing risk for PTS. However, these methods also can carry increased risk of bleeding and infection, considerations that must be balanced against potential benefit.
Investigators reviewed records for 39 patients who were diagnosed with ultrasound- or CT-confirmed acute proximal lower limb DVT and received either CDT or PMT during the period from November 2010 to November 2013. Patients were not randomized to treatment arms but were assigned using clinical judgment and patient preference. During the 12-month follow-up, three participants died of malignancy and two were lost to follow-up. Analysis was completed for the remaining 34 patients.
Overall, patient characteristics did not differ significantly between groups, with mean ages of 62.75 for the PMT group (n = 16) and 64.17 for the CDT group (n = 18). In all, 13/34 participants were female. Patients in both treatment groups fared well, with no 30-day mortality, and no episodes of major bleeding, PE, or renal failure. Ten patients in the PMT group and six in the CDT group required stenting of the common iliac vein to maintain patency, a nonsignificant difference. Just one participant in the CDE group experienced a minor bleeding event.
Turning to outcomes, study authors assessed postprocedure patency, finding improved patency for both procedures (P less than .001 for both, compared with preoperation patency scores), with no significant difference between the two groups post procedure. Thrombus scores were also significantly better for both treatment arms post procedure (P less than .001). Clot burden tended to improve more rapidly over the 12-month follow-up period for the PMT group, though the difference between groups was just short of statistically significant.
At 12 months, though the amount of venous reflux did not differ significantly between groups, those who had received PMT had significantly fewer signs and symptoms of PTS. This assessment used the Villalta scale, a standardized assessment and scoring system for PTS, where higher numbers indicate worse PTS. The PMT group’s Villalta score was 2.06 +/–2.95, compared with 5.06 +/–4.07 for the CDT group (P = .030).
Study limitations included the small study size, retrospective study design, and lack of randomization. Acknowledging these limitations, Dr. Huang and coauthors called for larger, multicenter, randomized controlled studies of PMT. The personal and economic costs of PTS, they argue, warrant exploring whether PMT may help minimize total thrombolysis dose, reduce hospital stays, and decrease costs while minimizing the risks of chronic venous insufficiency post DVT.
Dr. Huang and coauthors reported no conflicts of interest.
Adding a mechanical suction technique to local thrombolysis to break up and remove blood clots reduced postthrombotic syndrome (PTS) after deep vein thrombosis (DVT) without causing increased complications, according to a small retrospective study.
Dr. Chun-Yang Huang of the National Yang Ming University (Taipei, Taiwan) and colleagues examined patients diagnosed with acute proximal lower limb DVT. Patients received either thrombolysis alone via a catheter-directed thrombolysis (CDT), or percutaneous mechanical thrombectomy (PMT) by a combination of pharmacologic thrombolysis and suction; both techniques were accompanied by systemic anticoagulation. Though both treatment groups fared well during treatment and for the 12-month follow-up period, the PMT group had a significantly lower incidence of PTS 1 year after treatment (Ann. Vascular Surg. 2015. doi: 10.1016/j.avsg.2015.01.014).
For those with DVT, parenteral anticoagulation prevents propagation of the clot and minimizes risk of pulmonary embolism (PE); however, anticoagulation does not accelerate dissolution of the existing clot. According to study authors, 30%-40% of those with proximal leg DVTs will go on to develop PTS, with the prolonged distal venous stasis from an undisturbed clot causing loss of valvular competence and resultant chronic venous insufficiency. PTS can involve leg swelling, discomfort, skin changes, and ulceration, with significant impact on quality of life and health care costs.
Techniques such as CDT and PMT can increase the rate of clot dissolution, thus restoring patency sooner and minimizing risk for PTS. However, these methods also can carry increased risk of bleeding and infection, considerations that must be balanced against potential benefit.
Investigators reviewed records for 39 patients who were diagnosed with ultrasound- or CT-confirmed acute proximal lower limb DVT and received either CDT or PMT during the period from November 2010 to November 2013. Patients were not randomized to treatment arms but were assigned using clinical judgment and patient preference. During the 12-month follow-up, three participants died of malignancy and two were lost to follow-up. Analysis was completed for the remaining 34 patients.
Overall, patient characteristics did not differ significantly between groups, with mean ages of 62.75 for the PMT group (n = 16) and 64.17 for the CDT group (n = 18). In all, 13/34 participants were female. Patients in both treatment groups fared well, with no 30-day mortality, and no episodes of major bleeding, PE, or renal failure. Ten patients in the PMT group and six in the CDT group required stenting of the common iliac vein to maintain patency, a nonsignificant difference. Just one participant in the CDE group experienced a minor bleeding event.
Turning to outcomes, study authors assessed postprocedure patency, finding improved patency for both procedures (P less than .001 for both, compared with preoperation patency scores), with no significant difference between the two groups post procedure. Thrombus scores were also significantly better for both treatment arms post procedure (P less than .001). Clot burden tended to improve more rapidly over the 12-month follow-up period for the PMT group, though the difference between groups was just short of statistically significant.
At 12 months, though the amount of venous reflux did not differ significantly between groups, those who had received PMT had significantly fewer signs and symptoms of PTS. This assessment used the Villalta scale, a standardized assessment and scoring system for PTS, where higher numbers indicate worse PTS. The PMT group’s Villalta score was 2.06 +/–2.95, compared with 5.06 +/–4.07 for the CDT group (P = .030).
Study limitations included the small study size, retrospective study design, and lack of randomization. Acknowledging these limitations, Dr. Huang and coauthors called for larger, multicenter, randomized controlled studies of PMT. The personal and economic costs of PTS, they argue, warrant exploring whether PMT may help minimize total thrombolysis dose, reduce hospital stays, and decrease costs while minimizing the risks of chronic venous insufficiency post DVT.
Dr. Huang and coauthors reported no conflicts of interest.
Adding a mechanical suction technique to local thrombolysis to break up and remove blood clots reduced postthrombotic syndrome (PTS) after deep vein thrombosis (DVT) without causing increased complications, according to a small retrospective study.
Dr. Chun-Yang Huang of the National Yang Ming University (Taipei, Taiwan) and colleagues examined patients diagnosed with acute proximal lower limb DVT. Patients received either thrombolysis alone via a catheter-directed thrombolysis (CDT), or percutaneous mechanical thrombectomy (PMT) by a combination of pharmacologic thrombolysis and suction; both techniques were accompanied by systemic anticoagulation. Though both treatment groups fared well during treatment and for the 12-month follow-up period, the PMT group had a significantly lower incidence of PTS 1 year after treatment (Ann. Vascular Surg. 2015. doi: 10.1016/j.avsg.2015.01.014).
For those with DVT, parenteral anticoagulation prevents propagation of the clot and minimizes risk of pulmonary embolism (PE); however, anticoagulation does not accelerate dissolution of the existing clot. According to study authors, 30%-40% of those with proximal leg DVTs will go on to develop PTS, with the prolonged distal venous stasis from an undisturbed clot causing loss of valvular competence and resultant chronic venous insufficiency. PTS can involve leg swelling, discomfort, skin changes, and ulceration, with significant impact on quality of life and health care costs.
Techniques such as CDT and PMT can increase the rate of clot dissolution, thus restoring patency sooner and minimizing risk for PTS. However, these methods also can carry increased risk of bleeding and infection, considerations that must be balanced against potential benefit.
Investigators reviewed records for 39 patients who were diagnosed with ultrasound- or CT-confirmed acute proximal lower limb DVT and received either CDT or PMT during the period from November 2010 to November 2013. Patients were not randomized to treatment arms but were assigned using clinical judgment and patient preference. During the 12-month follow-up, three participants died of malignancy and two were lost to follow-up. Analysis was completed for the remaining 34 patients.
Overall, patient characteristics did not differ significantly between groups, with mean ages of 62.75 for the PMT group (n = 16) and 64.17 for the CDT group (n = 18). In all, 13/34 participants were female. Patients in both treatment groups fared well, with no 30-day mortality, and no episodes of major bleeding, PE, or renal failure. Ten patients in the PMT group and six in the CDT group required stenting of the common iliac vein to maintain patency, a nonsignificant difference. Just one participant in the CDE group experienced a minor bleeding event.
Turning to outcomes, study authors assessed postprocedure patency, finding improved patency for both procedures (P less than .001 for both, compared with preoperation patency scores), with no significant difference between the two groups post procedure. Thrombus scores were also significantly better for both treatment arms post procedure (P less than .001). Clot burden tended to improve more rapidly over the 12-month follow-up period for the PMT group, though the difference between groups was just short of statistically significant.
At 12 months, though the amount of venous reflux did not differ significantly between groups, those who had received PMT had significantly fewer signs and symptoms of PTS. This assessment used the Villalta scale, a standardized assessment and scoring system for PTS, where higher numbers indicate worse PTS. The PMT group’s Villalta score was 2.06 +/–2.95, compared with 5.06 +/–4.07 for the CDT group (P = .030).
Study limitations included the small study size, retrospective study design, and lack of randomization. Acknowledging these limitations, Dr. Huang and coauthors called for larger, multicenter, randomized controlled studies of PMT. The personal and economic costs of PTS, they argue, warrant exploring whether PMT may help minimize total thrombolysis dose, reduce hospital stays, and decrease costs while minimizing the risks of chronic venous insufficiency post DVT.
Dr. Huang and coauthors reported no conflicts of interest.
Key clinical point: Both percutaneous PMT and catheter-directed thrombolysis (CDT) were safe and effective, but PMT reduced risk of postthrombotic syndrome.
Major finding: In a small retrospective analysis of patients with deep vein thrombosis (DVT), both PMT and CDT were safe and effective when used in combination with systemic anticoagulation; however, postthrombotic syndrome (PTS) scoring was significantly better for those receiving PMT (Villalta score 2.1 +/- 3.0 vs. 5.1 +/- 4.1, P = .030).
Data source: Retrospective study of 39 patients who were diagnosed with acute proximal DVT of the lower limb between November 2010 and November 2013 at a Taiwanese hospital.
Disclosures: The authors reported that they had no conflicts of interest; funding source was not provided.
Endovascular stents effective for iliofemoral obstructions in patients with PTS
Endovascular stenting is a safe and effective way to treat iliofemoral obstructions in patients with postthrombotic syndrome, according to Dr. M. Yin of Shanghai (China) JiaoTong University, and associates.
The stenting process was achieved without major complications in 95% of cases. Cumulative primary, assisted primary, and secondary patency rates after 3 years were 69%, 79%, and 92%, respectively. Patients with severe postthrombotic syndrome (PTS) saw a significant drop in their Villalta score, compared with patients treated with elastic compression stockings (ECS) therapy, though scores were similar in patients with moderate PTS in both groups. The 24-month recurrence-free ulcer healing rate was significantly higher in the stenting group (87% vs. 71%).
“ECS therapy shows equal clinical effects with stent placement in patients with moderate PTS,” but the stented patients did not have to wear stockings after the procedure, the researchers wrote.
Find the full study in the European Journal of Vascular & Endovascular Surgery (doi: 10.1016/j.ejvs.2015.03.029).
Endovascular stenting is a safe and effective way to treat iliofemoral obstructions in patients with postthrombotic syndrome, according to Dr. M. Yin of Shanghai (China) JiaoTong University, and associates.
The stenting process was achieved without major complications in 95% of cases. Cumulative primary, assisted primary, and secondary patency rates after 3 years were 69%, 79%, and 92%, respectively. Patients with severe postthrombotic syndrome (PTS) saw a significant drop in their Villalta score, compared with patients treated with elastic compression stockings (ECS) therapy, though scores were similar in patients with moderate PTS in both groups. The 24-month recurrence-free ulcer healing rate was significantly higher in the stenting group (87% vs. 71%).
“ECS therapy shows equal clinical effects with stent placement in patients with moderate PTS,” but the stented patients did not have to wear stockings after the procedure, the researchers wrote.
Find the full study in the European Journal of Vascular & Endovascular Surgery (doi: 10.1016/j.ejvs.2015.03.029).
Endovascular stenting is a safe and effective way to treat iliofemoral obstructions in patients with postthrombotic syndrome, according to Dr. M. Yin of Shanghai (China) JiaoTong University, and associates.
The stenting process was achieved without major complications in 95% of cases. Cumulative primary, assisted primary, and secondary patency rates after 3 years were 69%, 79%, and 92%, respectively. Patients with severe postthrombotic syndrome (PTS) saw a significant drop in their Villalta score, compared with patients treated with elastic compression stockings (ECS) therapy, though scores were similar in patients with moderate PTS in both groups. The 24-month recurrence-free ulcer healing rate was significantly higher in the stenting group (87% vs. 71%).
“ECS therapy shows equal clinical effects with stent placement in patients with moderate PTS,” but the stented patients did not have to wear stockings after the procedure, the researchers wrote.
Find the full study in the European Journal of Vascular & Endovascular Surgery (doi: 10.1016/j.ejvs.2015.03.029).
Are oral antibiotics enough to reduce colorectal surgery infections?
CHICAGO – Oral antibiotics alone or in combination with mechanical bowel preparation were independently associated with reduced surgical site infections after elective colorectal resection in a large national patient sample.
Oral antibiotics (OA) alone significantly reduced the rate of any surgical site infection (SSI) by 44% (odds ratio, 0.56; 95% confidence interval, 0.36-0.87) and wound SSI by 59% (OR, 0.41; 95% CI, 0.23-0.72), compared with no bowel preparation in propensity-adjusted multivariate analysis.

OA combined with mechanical bowel preparation (MBP) was independently associated with significant reductions of 54%, 58%, and 41%, respectively, for any SSI (OR, 0.46; 95% CI, 0.38-0.55), wound SSI (OR, 0.42; 95% CI, 0.33-0.53), and organ space SSI (OR, 0.59; 95% CI, 0.44-0.78).
In contrast, MBP, which was used in 40.8% of cases, was not independently associated with reduced rates of any SSI (OR, 0.95; 95% CI, 0.82-1.10), wound SSI (OR, 0.91; 95% CI, 0.76-1.09), or organ space SSI (OR, 1.0; 95% CI, 0.79-1.27), according to Dr. Sarah Koller of Temple University Hospital in Philadelphia and her associates.
A limitation of the study was the lack of information on type of OA or MBP used, patient compliance, and use of parenteral antibiotic prophylaxis.
“Randomized clinical trials are needed to determine the true benefits of oral antibiotics alone versus combined oral antibiotics and mechanical bowel prep prior to elective colorectal resection,” Dr. Koller said at the American College of Surgeons/National Surgery Quality Improvement Program National Conference.
Session comoderator Dr. E. Patchen Dellinger, of the University of Washington in Seattle, commented, “Logically, it’s hard for me to believe that oral antibiotics would affect a couple of kilograms of stool in the colon and yet here are these tantalizing data. So we do need the prospective trial you mention.

“But, the other thing that blows my mind every time I see these data is 49% of people getting a mechanical bowel prep without oral antibiotics, which has conclusively been shown to be useless for anything but torture of the patient.”
Significant variability in the use of bowel preparation exists within the surgical community, with a recent survey of colorectal surgeons revealing that 76% routinely used MBP and only 36% routinely used oral antibiotics, Dr. Koller observed.
In the current analysis, just 3.3% of patients received OA, 30.4% OA plus MBP, 40.8% MBP, and 25.5% no bowel preparation.
Physicians have been slow to abandon MBP, despite multiple studies showing that MBP alone does not reduce SSIs in elective colon and rectal surgery. There also have been reports of higher rates of anastomotic leak, increased cardiac or metabolic complications, and a slower return of bowel function with MBP.
Several studies, including a recent Cochrane Database Review, have shown that oral or intravenous antibiotic prophylaxis reduces surgical wound infection after colorectal surgery. The comparison groups are not uniform across the studies, however, and the controversy persists as to which type of bowel prep best reduces SSI after colorectal surgery, she said.
To explore this issue, the investigators identified all patients who underwent elective, nonemergent colorectal resections in both the ACS NSQIP Participant Use Data File (PUF) and the Procedure Targeted PUF for colectomy from 2012 to 2013. The cohort included 19,372 patients with complete preoperative bowel preparation data. Patients who were ventilator dependent or had infections or open wounds at the time of surgery were excluded.
The overall rates of any SSI, wound SSI (superficial and/or deep), and organ space SSI were 9.5%, 6.4%, and 3.5%, respectively.
With regard to adverse outcomes cited in previous studies, only OA plus MBP was shown to independently reduce anastomotic leak (OR, 0.57; 95% CI, 0.42-0.78) and postoperative ileus (OR, 0.79; 95% CI, 0.68-0.92), compared with no bowel prep, Dr. Koller reported.
Both OA and OA plus MBP, however, decreased length of stay by 0.83 days.
None of the bowel preparations were independently associated with increased rates of cardiac or renal complications, she said.
The investigators were not able to track rates of Clostridium difficile colitis after administration of the oral antibiotics. Dr. Koller acknowledged this is a concern when using oral antibiotics and may contribute to why they aren’t used frequently.
Dr. Koller reported having no conflicts of interest. A coauthor disclosed consulting for Intuitive Surgical.
CHICAGO – Oral antibiotics alone or in combination with mechanical bowel preparation were independently associated with reduced surgical site infections after elective colorectal resection in a large national patient sample.
Oral antibiotics (OA) alone significantly reduced the rate of any surgical site infection (SSI) by 44% (odds ratio, 0.56; 95% confidence interval, 0.36-0.87) and wound SSI by 59% (OR, 0.41; 95% CI, 0.23-0.72), compared with no bowel preparation in propensity-adjusted multivariate analysis.
OA combined with mechanical bowel preparation (MBP) was independently associated with significant reductions of 54%, 58%, and 41%, respectively, for any SSI (OR, 0.46; 95% CI, 0.38-0.55), wound SSI (OR, 0.42; 95% CI, 0.33-0.53), and organ space SSI (OR, 0.59; 95% CI, 0.44-0.78).
In contrast, MBP, which was used in 40.8% of cases, was not independently associated with reduced rates of any SSI (OR, 0.95; 95% CI, 0.82-1.10), wound SSI (OR, 0.91; 95% CI, 0.76-1.09), or organ space SSI (OR, 1.0; 95% CI, 0.79-1.27), according to Dr. Sarah Koller of Temple University Hospital in Philadelphia and her associates.
A limitation of the study was the lack of information on type of OA or MBP used, patient compliance, and use of parenteral antibiotic prophylaxis.
“Randomized clinical trials are needed to determine the true benefits of oral antibiotics alone versus combined oral antibiotics and mechanical bowel prep prior to elective colorectal resection,” Dr. Koller said at the American College of Surgeons/National Surgery Quality Improvement Program National Conference.
Session comoderator Dr. E. Patchen Dellinger, of the University of Washington in Seattle, commented, “Logically, it’s hard for me to believe that oral antibiotics would affect a couple of kilograms of stool in the colon and yet here are these tantalizing data. So we do need the prospective trial you mention.
“But, the other thing that blows my mind every time I see these data is 49% of people getting a mechanical bowel prep without oral antibiotics, which has conclusively been shown to be useless for anything but torture of the patient.”
Significant variability in the use of bowel preparation exists within the surgical community, with a recent survey of colorectal surgeons revealing that 76% routinely used MBP and only 36% routinely used oral antibiotics, Dr. Koller observed.
In the current analysis, just 3.3% of patients received OA, 30.4% OA plus MBP, 40.8% MBP, and 25.5% no bowel preparation.
Physicians have been slow to abandon MBP, despite multiple studies showing that MBP alone does not reduce SSIs in elective colon and rectal surgery. There also have been reports of higher rates of anastomotic leak, increased cardiac or metabolic complications, and a slower return of bowel function with MBP.
Several studies, including a recent Cochrane Database Review, have shown that oral or intravenous antibiotic prophylaxis reduces surgical wound infection after colorectal surgery. The comparison groups are not uniform across the studies, however, and the controversy persists as to which type of bowel prep best reduces SSI after colorectal surgery, she said.
To explore this issue, the investigators identified all patients who underwent elective, nonemergent colorectal resections in both the ACS NSQIP Participant Use Data File (PUF) and the Procedure Targeted PUF for colectomy from 2012 to 2013. The cohort included 19,372 patients with complete preoperative bowel preparation data. Patients who were ventilator dependent or had infections or open wounds at the time of surgery were excluded.
The overall rates of any SSI, wound SSI (superficial and/or deep), and organ space SSI were 9.5%, 6.4%, and 3.5%, respectively.
With regard to adverse outcomes cited in previous studies, only OA plus MBP was shown to independently reduce anastomotic leak (OR, 0.57; 95% CI, 0.42-0.78) and postoperative ileus (OR, 0.79; 95% CI, 0.68-0.92), compared with no bowel prep, Dr. Koller reported.
Both OA and OA plus MBP, however, decreased length of stay by 0.83 days.
None of the bowel preparations were independently associated with increased rates of cardiac or renal complications, she said.
The investigators were not able to track rates of Clostridium difficile colitis after administration of the oral antibiotics. Dr. Koller acknowledged this is a concern when using oral antibiotics and may contribute to why they aren’t used frequently.
Dr. Koller reported having no conflicts of interest. A coauthor disclosed consulting for Intuitive Surgical.
CHICAGO – Oral antibiotics alone or in combination with mechanical bowel preparation were independently associated with reduced surgical site infections after elective colorectal resection in a large national patient sample.
Oral antibiotics (OA) alone significantly reduced the rate of any surgical site infection (SSI) by 44% (odds ratio, 0.56; 95% confidence interval, 0.36-0.87) and wound SSI by 59% (OR, 0.41; 95% CI, 0.23-0.72), compared with no bowel preparation in propensity-adjusted multivariate analysis.
OA combined with mechanical bowel preparation (MBP) was independently associated with significant reductions of 54%, 58%, and 41%, respectively, for any SSI (OR, 0.46; 95% CI, 0.38-0.55), wound SSI (OR, 0.42; 95% CI, 0.33-0.53), and organ space SSI (OR, 0.59; 95% CI, 0.44-0.78).
In contrast, MBP, which was used in 40.8% of cases, was not independently associated with reduced rates of any SSI (OR, 0.95; 95% CI, 0.82-1.10), wound SSI (OR, 0.91; 95% CI, 0.76-1.09), or organ space SSI (OR, 1.0; 95% CI, 0.79-1.27), according to Dr. Sarah Koller of Temple University Hospital in Philadelphia and her associates.
A limitation of the study was the lack of information on type of OA or MBP used, patient compliance, and use of parenteral antibiotic prophylaxis.
“Randomized clinical trials are needed to determine the true benefits of oral antibiotics alone versus combined oral antibiotics and mechanical bowel prep prior to elective colorectal resection,” Dr. Koller said at the American College of Surgeons/National Surgery Quality Improvement Program National Conference.
Session comoderator Dr. E. Patchen Dellinger, of the University of Washington in Seattle, commented, “Logically, it’s hard for me to believe that oral antibiotics would affect a couple of kilograms of stool in the colon and yet here are these tantalizing data. So we do need the prospective trial you mention.
“But, the other thing that blows my mind every time I see these data is 49% of people getting a mechanical bowel prep without oral antibiotics, which has conclusively been shown to be useless for anything but torture of the patient.”
Significant variability in the use of bowel preparation exists within the surgical community, with a recent survey of colorectal surgeons revealing that 76% routinely used MBP and only 36% routinely used oral antibiotics, Dr. Koller observed.
In the current analysis, just 3.3% of patients received OA, 30.4% OA plus MBP, 40.8% MBP, and 25.5% no bowel preparation.
Physicians have been slow to abandon MBP, despite multiple studies showing that MBP alone does not reduce SSIs in elective colon and rectal surgery. There also have been reports of higher rates of anastomotic leak, increased cardiac or metabolic complications, and a slower return of bowel function with MBP.
Several studies, including a recent Cochrane Database Review, have shown that oral or intravenous antibiotic prophylaxis reduces surgical wound infection after colorectal surgery. The comparison groups are not uniform across the studies, however, and the controversy persists as to which type of bowel prep best reduces SSI after colorectal surgery, she said.
To explore this issue, the investigators identified all patients who underwent elective, nonemergent colorectal resections in both the ACS NSQIP Participant Use Data File (PUF) and the Procedure Targeted PUF for colectomy from 2012 to 2013. The cohort included 19,372 patients with complete preoperative bowel preparation data. Patients who were ventilator dependent or had infections or open wounds at the time of surgery were excluded.
The overall rates of any SSI, wound SSI (superficial and/or deep), and organ space SSI were 9.5%, 6.4%, and 3.5%, respectively.
With regard to adverse outcomes cited in previous studies, only OA plus MBP was shown to independently reduce anastomotic leak (OR, 0.57; 95% CI, 0.42-0.78) and postoperative ileus (OR, 0.79; 95% CI, 0.68-0.92), compared with no bowel prep, Dr. Koller reported.
Both OA and OA plus MBP, however, decreased length of stay by 0.83 days.
None of the bowel preparations were independently associated with increased rates of cardiac or renal complications, she said.
The investigators were not able to track rates of Clostridium difficile colitis after administration of the oral antibiotics. Dr. Koller acknowledged this is a concern when using oral antibiotics and may contribute to why they aren’t used frequently.
Dr. Koller reported having no conflicts of interest. A coauthor disclosed consulting for Intuitive Surgical.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: Oral antibiotics alone or in combination with mechanical bowel preparation were independently associated with reduced surgical site infections after elective colorectal resection.
Major finding: Oral antibiotics alone significantly reduced the rate of any surgical site infection by 44% and wound SSI by 59%.
Data source: Data from 19,372 patients who underwent elective, nonemergent colorectal resections in both the ACS NSQIP Participant Use Data File (PUF) and the Procedure Targeted PUF for colectomy from 2012 to 2013.
Disclosures: Dr. Koller reported having no conflicts of interest. A coauthor disclosed consulting for Intuitive Surgical.

Orbera intragastric balloon approved for weight loss in obese adults
Another endoscopically delivered intragastric balloon indicated as a weight loss aid in obese adults has been approved by the Food and Drug Administration.
The Orbera intragastric balloon has been approved as a treatment for weight loss, in obese adults, with a body mass index between 30 and 40 kg/m2, the manufacturer, Apollo Endosurgery, announced on Aug. 6. It is intended for obese adults who are considering invasive surgery or for whom invasive surgery is not appropriate, when diet and exercise or pharmaceutical interventions have not worked, the statement said.

During a 20- to 30-minute procedure, the deflated Orbera silicone balloon is placed in the stomach via an endoscopic procedure under a mild sedative, where it is then filled with saline until it is about the size of a grapefruit, according to the company. The patient usually can go home on the same day; the balloon is deflated and removed 6 months later. The company will provide patients with an individualized weight-loss program for patients for 1 year, starting from the time of balloon placement.
The approval of this device follows the approval of the ReShape intragastric balloon for obese adults, for up to 6 months, announced by the FDA on July 28. ReShape was the first such device to be approved in the United States.
The results of the pivotal U.S. 12-month multicenter trial of the Orbera balloon in more than 250 obese adults with a BMI of 30-40 kg/m2 were reported at the Digestive Disease Week meeting in May, by Dr. Barham K. Abu Dayyeh of the Mayo Clinic in Rochester, Minn. For more than 2 years, patients were randomized to a 12-month behavioral modification program, with or without endoscopic placement of the balloon, which was removed at 6 months. Eighteen patients withdrew before treatment; 215 patients were evaluable at 6 months, 206 at 9 months, and 191 at 12 months.
At 6 months, the mean percent total body weight loss was about 10% in the balloon group, vs. 4% in the control group, a significant difference (P less than .001). In addition, the total body weight loss was significantly higher in the balloon group at 3, 6, 9, and 12 months, and the mean percent of excess weight loss at 6 months was better in the balloon group than in the control group (about 40% vs. 13%; P less than .001), he said at the meeting. The majority of excess weight loss achieved at 6 months was also maintained at 12 months.
Serious adverse events were reported in 7% of controls and almost 10% of the balloon group, which included eight early removals for intolerance, one gastric outlet obstruction, one laryngospasm during placement, one case of severe abdominal cramping, and one case of severe dehydration. Early device removals occurred in 22% of patients, 15 for symptoms and 13 at subject request, Dr. Abu Dayyeh said. There were no deaths during the study.
The Orbera balloon has been available in more than 80 countries, according to the manufacturer.
More information is available on the FDA website.
Another endoscopically delivered intragastric balloon indicated as a weight loss aid in obese adults has been approved by the Food and Drug Administration.
The Orbera intragastric balloon has been approved as a treatment for weight loss, in obese adults, with a body mass index between 30 and 40 kg/m2, the manufacturer, Apollo Endosurgery, announced on Aug. 6. It is intended for obese adults who are considering invasive surgery or for whom invasive surgery is not appropriate, when diet and exercise or pharmaceutical interventions have not worked, the statement said.
During a 20- to 30-minute procedure, the deflated Orbera silicone balloon is placed in the stomach via an endoscopic procedure under a mild sedative, where it is then filled with saline until it is about the size of a grapefruit, according to the company. The patient usually can go home on the same day; the balloon is deflated and removed 6 months later. The company will provide patients with an individualized weight-loss program for patients for 1 year, starting from the time of balloon placement.
The approval of this device follows the approval of the ReShape intragastric balloon for obese adults, for up to 6 months, announced by the FDA on July 28. ReShape was the first such device to be approved in the United States.
The results of the pivotal U.S. 12-month multicenter trial of the Orbera balloon in more than 250 obese adults with a BMI of 30-40 kg/m2 were reported at the Digestive Disease Week meeting in May, by Dr. Barham K. Abu Dayyeh of the Mayo Clinic in Rochester, Minn. For more than 2 years, patients were randomized to a 12-month behavioral modification program, with or without endoscopic placement of the balloon, which was removed at 6 months. Eighteen patients withdrew before treatment; 215 patients were evaluable at 6 months, 206 at 9 months, and 191 at 12 months.
At 6 months, the mean percent total body weight loss was about 10% in the balloon group, vs. 4% in the control group, a significant difference (P less than .001). In addition, the total body weight loss was significantly higher in the balloon group at 3, 6, 9, and 12 months, and the mean percent of excess weight loss at 6 months was better in the balloon group than in the control group (about 40% vs. 13%; P less than .001), he said at the meeting. The majority of excess weight loss achieved at 6 months was also maintained at 12 months.
Serious adverse events were reported in 7% of controls and almost 10% of the balloon group, which included eight early removals for intolerance, one gastric outlet obstruction, one laryngospasm during placement, one case of severe abdominal cramping, and one case of severe dehydration. Early device removals occurred in 22% of patients, 15 for symptoms and 13 at subject request, Dr. Abu Dayyeh said. There were no deaths during the study.
The Orbera balloon has been available in more than 80 countries, according to the manufacturer.
More information is available on the FDA website.
Another endoscopically delivered intragastric balloon indicated as a weight loss aid in obese adults has been approved by the Food and Drug Administration.
The Orbera intragastric balloon has been approved as a treatment for weight loss, in obese adults, with a body mass index between 30 and 40 kg/m2, the manufacturer, Apollo Endosurgery, announced on Aug. 6. It is intended for obese adults who are considering invasive surgery or for whom invasive surgery is not appropriate, when diet and exercise or pharmaceutical interventions have not worked, the statement said.
During a 20- to 30-minute procedure, the deflated Orbera silicone balloon is placed in the stomach via an endoscopic procedure under a mild sedative, where it is then filled with saline until it is about the size of a grapefruit, according to the company. The patient usually can go home on the same day; the balloon is deflated and removed 6 months later. The company will provide patients with an individualized weight-loss program for patients for 1 year, starting from the time of balloon placement.
The approval of this device follows the approval of the ReShape intragastric balloon for obese adults, for up to 6 months, announced by the FDA on July 28. ReShape was the first such device to be approved in the United States.
The results of the pivotal U.S. 12-month multicenter trial of the Orbera balloon in more than 250 obese adults with a BMI of 30-40 kg/m2 were reported at the Digestive Disease Week meeting in May, by Dr. Barham K. Abu Dayyeh of the Mayo Clinic in Rochester, Minn. For more than 2 years, patients were randomized to a 12-month behavioral modification program, with or without endoscopic placement of the balloon, which was removed at 6 months. Eighteen patients withdrew before treatment; 215 patients were evaluable at 6 months, 206 at 9 months, and 191 at 12 months.
At 6 months, the mean percent total body weight loss was about 10% in the balloon group, vs. 4% in the control group, a significant difference (P less than .001). In addition, the total body weight loss was significantly higher in the balloon group at 3, 6, 9, and 12 months, and the mean percent of excess weight loss at 6 months was better in the balloon group than in the control group (about 40% vs. 13%; P less than .001), he said at the meeting. The majority of excess weight loss achieved at 6 months was also maintained at 12 months.
Serious adverse events were reported in 7% of controls and almost 10% of the balloon group, which included eight early removals for intolerance, one gastric outlet obstruction, one laryngospasm during placement, one case of severe abdominal cramping, and one case of severe dehydration. Early device removals occurred in 22% of patients, 15 for symptoms and 13 at subject request, Dr. Abu Dayyeh said. There were no deaths during the study.
The Orbera balloon has been available in more than 80 countries, according to the manufacturer.
More information is available on the FDA website.

Elderly LARC patients had similar nCRT outcomes to younger patients
Clinical outcomes of elderly patients treated with neoadjuvant chemoradiation (nCRT) for locally advanced rectal cancer (LARC) were similar enough to outcomes of younger patients that doctors may want to reconsider using age alone for determining eligibility for nCRT and surgery, investigators reported online in the Annals of Oncology.
Dr. D. M. Jiang of the University of Ottawa (Ont.) and associates collected data from 1,172 patients with LARC who received nCRT and curative intent surgery, 25% (n = 295) of whom were 70 years old or older, from five major Canadian cancer centers between 2005 and 2012. When compared with younger patients, elderly patients were less likely to receive adjuvant chemotherapy (ACT) (60% vs. 79%; P less than .0001), oxaliplatin-based ACT (12% vs. 31%; P less than .0001), less likely to complete nCT (76% vs. 86%; P less than .001), and more likely to be anemic at initiation of nCRT (42% vs. 30%; P = .0004).
The investigators found that increasing age was not predictive of disease-free survival (hazard ratio, 1.00; 95% confidence interval, 0.99-1.02; P = .49) or cancer-specific survival (HR, 1.002; 95% CI, 0.98-1.02; P = .88) among LARC patients; however, advanced age correlated with an inferior overall survival (HR, 1.02; 95% CI, 1.00-1.03; P = .04).
Read the full article here.
Clinical outcomes of elderly patients treated with neoadjuvant chemoradiation (nCRT) for locally advanced rectal cancer (LARC) were similar enough to outcomes of younger patients that doctors may want to reconsider using age alone for determining eligibility for nCRT and surgery, investigators reported online in the Annals of Oncology.
Dr. D. M. Jiang of the University of Ottawa (Ont.) and associates collected data from 1,172 patients with LARC who received nCRT and curative intent surgery, 25% (n = 295) of whom were 70 years old or older, from five major Canadian cancer centers between 2005 and 2012. When compared with younger patients, elderly patients were less likely to receive adjuvant chemotherapy (ACT) (60% vs. 79%; P less than .0001), oxaliplatin-based ACT (12% vs. 31%; P less than .0001), less likely to complete nCT (76% vs. 86%; P less than .001), and more likely to be anemic at initiation of nCRT (42% vs. 30%; P = .0004).
The investigators found that increasing age was not predictive of disease-free survival (hazard ratio, 1.00; 95% confidence interval, 0.99-1.02; P = .49) or cancer-specific survival (HR, 1.002; 95% CI, 0.98-1.02; P = .88) among LARC patients; however, advanced age correlated with an inferior overall survival (HR, 1.02; 95% CI, 1.00-1.03; P = .04).
Read the full article here.
Clinical outcomes of elderly patients treated with neoadjuvant chemoradiation (nCRT) for locally advanced rectal cancer (LARC) were similar enough to outcomes of younger patients that doctors may want to reconsider using age alone for determining eligibility for nCRT and surgery, investigators reported online in the Annals of Oncology.
Dr. D. M. Jiang of the University of Ottawa (Ont.) and associates collected data from 1,172 patients with LARC who received nCRT and curative intent surgery, 25% (n = 295) of whom were 70 years old or older, from five major Canadian cancer centers between 2005 and 2012. When compared with younger patients, elderly patients were less likely to receive adjuvant chemotherapy (ACT) (60% vs. 79%; P less than .0001), oxaliplatin-based ACT (12% vs. 31%; P less than .0001), less likely to complete nCT (76% vs. 86%; P less than .001), and more likely to be anemic at initiation of nCRT (42% vs. 30%; P = .0004).
The investigators found that increasing age was not predictive of disease-free survival (hazard ratio, 1.00; 95% confidence interval, 0.99-1.02; P = .49) or cancer-specific survival (HR, 1.002; 95% CI, 0.98-1.02; P = .88) among LARC patients; however, advanced age correlated with an inferior overall survival (HR, 1.02; 95% CI, 1.00-1.03; P = .04).
Read the full article here.
One-third of organ donations after circulatory death are unsuccessful
Despite the increase in donation of organs for transplant after circulatory death, many of these donations fail, according to a new study.
Dr. Joseph Scalea of the division of transplantation at the University of Wisconsin in Madison and his colleagues sought to explicate the process resulting in unsuccessful donation after circulatory death (DCD) and to explore the factors contributing to time to death in donors with successful organ donation. They conducted a retrospective study of data obtained from all organ donors at a single transplant center during January 2011-September 2014 (Ann Surg. 2015 Jul 15. doi: 10.1097/SLA.0000000000001298). A total of 506 organ donation procedures were studied, 169 of which were DCD. Time of death and outcomes data was obtained in 99.4% of the cases
The reasons for DCD failure appear to be rooted in the timing of support removal and the progression to death of these potential organ donors. A study of transplantation in the United Kingdom has shown that organs are less likely to be viable for transplantation if the donor does not progress to death within the first hour of withdrawal of support (Curr Opin Organ Transplant. 2013;18:133-9).

“People need to be aware that when folks have agreed to donate organs of a loved one and it is going to be a [circulatory death donation], that there is roughly a one in three chance, at least, that organ donation won’t come to fruition,” Dr. Jeffrey D. Punch, a transplant specialist at the University of Michigan in Ann Arbor, said in an interview.
Protocols vary by organization, but DCD typically involves the surgical team withdrawing life support in the absence of the organ recovery team. If circulatory death occurs within the time determined by the protocol, the organs are recovered for transplantation. Studies have indicated since the general acceptance of DCD since the 1990s, these donations account for as much as a 30% increase in donation rates in the United States and abroad (Am J Transplant. 2006 Feb;6(2):281-91; N Engl J Med. 2007;357:209-13).
The University of Wisconsin’s DCD protocol involved waiting up to 30 minutes after withdrawal of support (WOS) to recover pancreas and liver and up to 2 hours to recover kidneys.
During the study period, 33.4% (n = 169/506) of the organ donations were DCD. At least one organ was successfully donated in 72.8% of cases (n = 123), whereas in 27.2% (n = 46), the patient did not progress to death in the protocol time frame to be considered for donation. Head trauma (21.9%), cerebrovascular accident (23.7%), and anoxia (47.3%) were the most common diagnosis leading to DCD; however, success of DCD donation was not associated with the diagnosis. But if withdrawal of support was initiated in the OR, successful donation was more likely (P = .006).
“Those patients who underwent WOS in the ICU successfully donated organs less frequently. This difference is hard to interpret, as there may be different techniques of withdrawal in the ICU, or a selection bias (i.e., deemed less likely to die quickly) with which patients are considered for an ICU withdrawal,” the researchers wrote.
Dr. Punch, the Jeremiah and Claire Turcotte Professor of Surgery at the University of Michigan added, “It certainly makes more sense for withdrawal of support to happen in the operating room. It is more effective and they are more likely to be able to donate organs.”
The mean time from WOS to death was 28 minutes and 35 seconds for successful donations and 33 hours, 37 minutes, and 15 seconds for unsuccessful donations. In patients that successfully donated, 90.2% died less than an hour after WOS.
The investigators point out, “the ability to donate organs from a family member or loved one is often the only positive memory of an otherwise devastating experience. Unfortunately, not all donors successfully donate after attempted DCD.”
The authors reported no conflicts of interests.
Despite the increase in donation of organs for transplant after circulatory death, many of these donations fail, according to a new study.
Dr. Joseph Scalea of the division of transplantation at the University of Wisconsin in Madison and his colleagues sought to explicate the process resulting in unsuccessful donation after circulatory death (DCD) and to explore the factors contributing to time to death in donors with successful organ donation. They conducted a retrospective study of data obtained from all organ donors at a single transplant center during January 2011-September 2014 (Ann Surg. 2015 Jul 15. doi: 10.1097/SLA.0000000000001298). A total of 506 organ donation procedures were studied, 169 of which were DCD. Time of death and outcomes data was obtained in 99.4% of the cases
The reasons for DCD failure appear to be rooted in the timing of support removal and the progression to death of these potential organ donors. A study of transplantation in the United Kingdom has shown that organs are less likely to be viable for transplantation if the donor does not progress to death within the first hour of withdrawal of support (Curr Opin Organ Transplant. 2013;18:133-9).
“People need to be aware that when folks have agreed to donate organs of a loved one and it is going to be a [circulatory death donation], that there is roughly a one in three chance, at least, that organ donation won’t come to fruition,” Dr. Jeffrey D. Punch, a transplant specialist at the University of Michigan in Ann Arbor, said in an interview.
Protocols vary by organization, but DCD typically involves the surgical team withdrawing life support in the absence of the organ recovery team. If circulatory death occurs within the time determined by the protocol, the organs are recovered for transplantation. Studies have indicated since the general acceptance of DCD since the 1990s, these donations account for as much as a 30% increase in donation rates in the United States and abroad (Am J Transplant. 2006 Feb;6(2):281-91; N Engl J Med. 2007;357:209-13).
The University of Wisconsin’s DCD protocol involved waiting up to 30 minutes after withdrawal of support (WOS) to recover pancreas and liver and up to 2 hours to recover kidneys.
During the study period, 33.4% (n = 169/506) of the organ donations were DCD. At least one organ was successfully donated in 72.8% of cases (n = 123), whereas in 27.2% (n = 46), the patient did not progress to death in the protocol time frame to be considered for donation. Head trauma (21.9%), cerebrovascular accident (23.7%), and anoxia (47.3%) were the most common diagnosis leading to DCD; however, success of DCD donation was not associated with the diagnosis. But if withdrawal of support was initiated in the OR, successful donation was more likely (P = .006).
“Those patients who underwent WOS in the ICU successfully donated organs less frequently. This difference is hard to interpret, as there may be different techniques of withdrawal in the ICU, or a selection bias (i.e., deemed less likely to die quickly) with which patients are considered for an ICU withdrawal,” the researchers wrote.
Dr. Punch, the Jeremiah and Claire Turcotte Professor of Surgery at the University of Michigan added, “It certainly makes more sense for withdrawal of support to happen in the operating room. It is more effective and they are more likely to be able to donate organs.”
The mean time from WOS to death was 28 minutes and 35 seconds for successful donations and 33 hours, 37 minutes, and 15 seconds for unsuccessful donations. In patients that successfully donated, 90.2% died less than an hour after WOS.
The investigators point out, “the ability to donate organs from a family member or loved one is often the only positive memory of an otherwise devastating experience. Unfortunately, not all donors successfully donate after attempted DCD.”
The authors reported no conflicts of interests.
Despite the increase in donation of organs for transplant after circulatory death, many of these donations fail, according to a new study.
Dr. Joseph Scalea of the division of transplantation at the University of Wisconsin in Madison and his colleagues sought to explicate the process resulting in unsuccessful donation after circulatory death (DCD) and to explore the factors contributing to time to death in donors with successful organ donation. They conducted a retrospective study of data obtained from all organ donors at a single transplant center during January 2011-September 2014 (Ann Surg. 2015 Jul 15. doi: 10.1097/SLA.0000000000001298). A total of 506 organ donation procedures were studied, 169 of which were DCD. Time of death and outcomes data was obtained in 99.4% of the cases
The reasons for DCD failure appear to be rooted in the timing of support removal and the progression to death of these potential organ donors. A study of transplantation in the United Kingdom has shown that organs are less likely to be viable for transplantation if the donor does not progress to death within the first hour of withdrawal of support (Curr Opin Organ Transplant. 2013;18:133-9).
“People need to be aware that when folks have agreed to donate organs of a loved one and it is going to be a [circulatory death donation], that there is roughly a one in three chance, at least, that organ donation won’t come to fruition,” Dr. Jeffrey D. Punch, a transplant specialist at the University of Michigan in Ann Arbor, said in an interview.
Protocols vary by organization, but DCD typically involves the surgical team withdrawing life support in the absence of the organ recovery team. If circulatory death occurs within the time determined by the protocol, the organs are recovered for transplantation. Studies have indicated since the general acceptance of DCD since the 1990s, these donations account for as much as a 30% increase in donation rates in the United States and abroad (Am J Transplant. 2006 Feb;6(2):281-91; N Engl J Med. 2007;357:209-13).
The University of Wisconsin’s DCD protocol involved waiting up to 30 minutes after withdrawal of support (WOS) to recover pancreas and liver and up to 2 hours to recover kidneys.
During the study period, 33.4% (n = 169/506) of the organ donations were DCD. At least one organ was successfully donated in 72.8% of cases (n = 123), whereas in 27.2% (n = 46), the patient did not progress to death in the protocol time frame to be considered for donation. Head trauma (21.9%), cerebrovascular accident (23.7%), and anoxia (47.3%) were the most common diagnosis leading to DCD; however, success of DCD donation was not associated with the diagnosis. But if withdrawal of support was initiated in the OR, successful donation was more likely (P = .006).
“Those patients who underwent WOS in the ICU successfully donated organs less frequently. This difference is hard to interpret, as there may be different techniques of withdrawal in the ICU, or a selection bias (i.e., deemed less likely to die quickly) with which patients are considered for an ICU withdrawal,” the researchers wrote.
Dr. Punch, the Jeremiah and Claire Turcotte Professor of Surgery at the University of Michigan added, “It certainly makes more sense for withdrawal of support to happen in the operating room. It is more effective and they are more likely to be able to donate organs.”
The mean time from WOS to death was 28 minutes and 35 seconds for successful donations and 33 hours, 37 minutes, and 15 seconds for unsuccessful donations. In patients that successfully donated, 90.2% died less than an hour after WOS.
The investigators point out, “the ability to donate organs from a family member or loved one is often the only positive memory of an otherwise devastating experience. Unfortunately, not all donors successfully donate after attempted DCD.”
The authors reported no conflicts of interests.
FROM ANNALS OF SURGERY
Key clinical point: Some abdominal transplants are not possible because of failed DCD donation.
Major finding: At least one organ was successfully donated in 72.8% (n = 123), whereas 27.2% (n = 46) did not progress to death in the protocol time frame to be considered for donation.
Data source: Retrospective study of data obtained from all organ donors from a single transplant center during January 2011-September 2014.
Disclosures: The authors reported no conflicts of interests.

ERAS protocol cuts colorectal surgery morbidity, SSIs
CHICAGO – Implementing an enhanced recovery after surgery (ERAS) protocol at Canada’s second largest hospital significantly reduced morbidity and surgical site infections after elective colorectal surgery.
Rates of postoperative morbidity declined 48.7% from 27.3% before implementation to 14% after full ERAS implementation (P less than .05), while total surgical site infections fell 45% (20.2% vs. 11%; P less than .05).
Nonsignificant reductions were also seen in superficial surgical site infections (11.1% vs. 7.3%), deep SSIs (2% vs. 0.6%), and organ space SSIs (7.1% vs. 3.4%).
“Our results illustrate that using a multidisciplinary team, with attention to details and small multiple changes, aggregation of marginal gains can result in dramatic improvements in patient outcomes,” primary author Tracey Hong, R.N., said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
The ERAS protocol was implemented at Vancouver General Hospital, after ACS NSQIP risk-adjusted reports showed the 743-bed hospital had a high odds ratio of 1.50 for colorectal operative mortality.

“We had a problem,” Ms. Hong, the hospital’s quality and patient safety coordinator, said.
ERAS documents were developed, staff were educated on the protocol, intraoperative components were implemented and audited, and the full protocol was initiated in November 2013.
To explore the effects of ERAS implementation, chart reviews were conducted on 278 general surgery patients undergoing elective colorectal surgery: 99 patients before ERAS implementation (July 2011 through June 2013) and 179 patients in the first 10 months after full implementation (November 2013 through August 2014).
Laparoscopic colon resections were performed in 53% of the pre-ERAS group and 62% of the post-ERAS group, laparoscopic anterior and abdominoperineal resections in 10% and 23%, and open anterior and abdominoperineal resections in 23% and 18%, respectively. The median American Society of Anesthesiologists classification in both groups was 2.
After ERAS implementation, there was a trend for less postoperative pneumonia, unplanned intubation, ventilator use greater than 48 hours, and urinary tract infections (data not presented).
The median length of stay was reduced from 7 to 5 days, while readmissions increased from 7.1% to 11.7% (both changes were nonsignificant), according to Ms. Hong, who won the conference’s 2015 Surgical Clinical Reviewers Abstract Competition.
The reason for the increased readmissions is unclear, but opportunities to avoid preventable readmissions have been identified and are currently being worked on, she said.
Process measures showed that the goal of achieving a minimum 80% compliance from August 2014 to March 2015 was met within 4 months and sustained for the preoperative and intraoperative ERAS components, in aggregate. The aggregate postoperative components, which include early oral nutrition, early ambulation, early catheter removal, use of chewing gum, and defined discharge criteria, were the slowest to change, but are trending in the right direction, Ms. Hong said.
The key to achieving better outcomes with ERAS lies in involving a multidisciplinary team in all stages of planning and implementation, ongoing communication and sharing of results with stakeholders to foster commitment and ownership, and real-time auditing and use of plan-do-study-act cycles to enhance the rate of improvement, she said.
“It takes time to change culture; tenacity is important,” Ms. Hong added.
In a separate poster presentation, Ms. Hong and her colleagues reported compliance of ERAS components under the control of the anesthesiologist. The highest rate of compliance was seen in practices with few barriers to implementation such as active pre- and intraoperative warming (96%) and appropriate admission of antibiotics (92%) and antiemetics (86%). Conversely, rates were lower for multimodal analgesia (72%) and goal-directed fluid therapy (50%), which can be more labor intensive. Also, there is controversy around goal-directed fluid therapy’s benefit in low-risk patients, which may contribute to the lower compliance rates, the study authors noted. Overall, just under three-quarters of patients received at least four out of five components in their care.
On the basis of the success of the protocol, ERAS is now used for patients undergoing radical cystectomy, with plans to expand its use to all emergent and urgent cases within general surgery at Vancouver General as well as bariatric surgery at Richmond Hospital, also a member of Vancouver Coastal Health, Andrea Bisaillon, operations director of surgical services at Vancouver General Hospital, said in an interview.
“We’re rolling out ERAS to all the surgical patients because it’s best practice for all of surgery, not just colorectal surgery anymore,” she said.
CHICAGO – Implementing an enhanced recovery after surgery (ERAS) protocol at Canada’s second largest hospital significantly reduced morbidity and surgical site infections after elective colorectal surgery.
Rates of postoperative morbidity declined 48.7% from 27.3% before implementation to 14% after full ERAS implementation (P less than .05), while total surgical site infections fell 45% (20.2% vs. 11%; P less than .05).
Nonsignificant reductions were also seen in superficial surgical site infections (11.1% vs. 7.3%), deep SSIs (2% vs. 0.6%), and organ space SSIs (7.1% vs. 3.4%).
“Our results illustrate that using a multidisciplinary team, with attention to details and small multiple changes, aggregation of marginal gains can result in dramatic improvements in patient outcomes,” primary author Tracey Hong, R.N., said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
The ERAS protocol was implemented at Vancouver General Hospital, after ACS NSQIP risk-adjusted reports showed the 743-bed hospital had a high odds ratio of 1.50 for colorectal operative mortality.
“We had a problem,” Ms. Hong, the hospital’s quality and patient safety coordinator, said.
ERAS documents were developed, staff were educated on the protocol, intraoperative components were implemented and audited, and the full protocol was initiated in November 2013.
To explore the effects of ERAS implementation, chart reviews were conducted on 278 general surgery patients undergoing elective colorectal surgery: 99 patients before ERAS implementation (July 2011 through June 2013) and 179 patients in the first 10 months after full implementation (November 2013 through August 2014).
Laparoscopic colon resections were performed in 53% of the pre-ERAS group and 62% of the post-ERAS group, laparoscopic anterior and abdominoperineal resections in 10% and 23%, and open anterior and abdominoperineal resections in 23% and 18%, respectively. The median American Society of Anesthesiologists classification in both groups was 2.
After ERAS implementation, there was a trend for less postoperative pneumonia, unplanned intubation, ventilator use greater than 48 hours, and urinary tract infections (data not presented).
The median length of stay was reduced from 7 to 5 days, while readmissions increased from 7.1% to 11.7% (both changes were nonsignificant), according to Ms. Hong, who won the conference’s 2015 Surgical Clinical Reviewers Abstract Competition.
The reason for the increased readmissions is unclear, but opportunities to avoid preventable readmissions have been identified and are currently being worked on, she said.
Process measures showed that the goal of achieving a minimum 80% compliance from August 2014 to March 2015 was met within 4 months and sustained for the preoperative and intraoperative ERAS components, in aggregate. The aggregate postoperative components, which include early oral nutrition, early ambulation, early catheter removal, use of chewing gum, and defined discharge criteria, were the slowest to change, but are trending in the right direction, Ms. Hong said.
The key to achieving better outcomes with ERAS lies in involving a multidisciplinary team in all stages of planning and implementation, ongoing communication and sharing of results with stakeholders to foster commitment and ownership, and real-time auditing and use of plan-do-study-act cycles to enhance the rate of improvement, she said.
“It takes time to change culture; tenacity is important,” Ms. Hong added.
In a separate poster presentation, Ms. Hong and her colleagues reported compliance of ERAS components under the control of the anesthesiologist. The highest rate of compliance was seen in practices with few barriers to implementation such as active pre- and intraoperative warming (96%) and appropriate admission of antibiotics (92%) and antiemetics (86%). Conversely, rates were lower for multimodal analgesia (72%) and goal-directed fluid therapy (50%), which can be more labor intensive. Also, there is controversy around goal-directed fluid therapy’s benefit in low-risk patients, which may contribute to the lower compliance rates, the study authors noted. Overall, just under three-quarters of patients received at least four out of five components in their care.
On the basis of the success of the protocol, ERAS is now used for patients undergoing radical cystectomy, with plans to expand its use to all emergent and urgent cases within general surgery at Vancouver General as well as bariatric surgery at Richmond Hospital, also a member of Vancouver Coastal Health, Andrea Bisaillon, operations director of surgical services at Vancouver General Hospital, said in an interview.
“We’re rolling out ERAS to all the surgical patients because it’s best practice for all of surgery, not just colorectal surgery anymore,” she said.
CHICAGO – Implementing an enhanced recovery after surgery (ERAS) protocol at Canada’s second largest hospital significantly reduced morbidity and surgical site infections after elective colorectal surgery.
Rates of postoperative morbidity declined 48.7% from 27.3% before implementation to 14% after full ERAS implementation (P less than .05), while total surgical site infections fell 45% (20.2% vs. 11%; P less than .05).
Nonsignificant reductions were also seen in superficial surgical site infections (11.1% vs. 7.3%), deep SSIs (2% vs. 0.6%), and organ space SSIs (7.1% vs. 3.4%).
“Our results illustrate that using a multidisciplinary team, with attention to details and small multiple changes, aggregation of marginal gains can result in dramatic improvements in patient outcomes,” primary author Tracey Hong, R.N., said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
The ERAS protocol was implemented at Vancouver General Hospital, after ACS NSQIP risk-adjusted reports showed the 743-bed hospital had a high odds ratio of 1.50 for colorectal operative mortality.
“We had a problem,” Ms. Hong, the hospital’s quality and patient safety coordinator, said.
ERAS documents were developed, staff were educated on the protocol, intraoperative components were implemented and audited, and the full protocol was initiated in November 2013.
To explore the effects of ERAS implementation, chart reviews were conducted on 278 general surgery patients undergoing elective colorectal surgery: 99 patients before ERAS implementation (July 2011 through June 2013) and 179 patients in the first 10 months after full implementation (November 2013 through August 2014).
Laparoscopic colon resections were performed in 53% of the pre-ERAS group and 62% of the post-ERAS group, laparoscopic anterior and abdominoperineal resections in 10% and 23%, and open anterior and abdominoperineal resections in 23% and 18%, respectively. The median American Society of Anesthesiologists classification in both groups was 2.
After ERAS implementation, there was a trend for less postoperative pneumonia, unplanned intubation, ventilator use greater than 48 hours, and urinary tract infections (data not presented).
The median length of stay was reduced from 7 to 5 days, while readmissions increased from 7.1% to 11.7% (both changes were nonsignificant), according to Ms. Hong, who won the conference’s 2015 Surgical Clinical Reviewers Abstract Competition.
The reason for the increased readmissions is unclear, but opportunities to avoid preventable readmissions have been identified and are currently being worked on, she said.
Process measures showed that the goal of achieving a minimum 80% compliance from August 2014 to March 2015 was met within 4 months and sustained for the preoperative and intraoperative ERAS components, in aggregate. The aggregate postoperative components, which include early oral nutrition, early ambulation, early catheter removal, use of chewing gum, and defined discharge criteria, were the slowest to change, but are trending in the right direction, Ms. Hong said.
The key to achieving better outcomes with ERAS lies in involving a multidisciplinary team in all stages of planning and implementation, ongoing communication and sharing of results with stakeholders to foster commitment and ownership, and real-time auditing and use of plan-do-study-act cycles to enhance the rate of improvement, she said.
“It takes time to change culture; tenacity is important,” Ms. Hong added.
In a separate poster presentation, Ms. Hong and her colleagues reported compliance of ERAS components under the control of the anesthesiologist. The highest rate of compliance was seen in practices with few barriers to implementation such as active pre- and intraoperative warming (96%) and appropriate admission of antibiotics (92%) and antiemetics (86%). Conversely, rates were lower for multimodal analgesia (72%) and goal-directed fluid therapy (50%), which can be more labor intensive. Also, there is controversy around goal-directed fluid therapy’s benefit in low-risk patients, which may contribute to the lower compliance rates, the study authors noted. Overall, just under three-quarters of patients received at least four out of five components in their care.
On the basis of the success of the protocol, ERAS is now used for patients undergoing radical cystectomy, with plans to expand its use to all emergent and urgent cases within general surgery at Vancouver General as well as bariatric surgery at Richmond Hospital, also a member of Vancouver Coastal Health, Andrea Bisaillon, operations director of surgical services at Vancouver General Hospital, said in an interview.
“We’re rolling out ERAS to all the surgical patients because it’s best practice for all of surgery, not just colorectal surgery anymore,” she said.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: Through an ERAS protocol, attention to details and small multiple changes can result in dramatic improvements in patient outcomes.
Major finding: After full ERAS implementation, rates of postoperative morbidity and total surgical site infection were reduced 48.7% and 45%, respectively.
Data source: A retrospective analysis of 278 patients undergoing elective colorectal surgery.
Disclosures: The study authors reported having no relevant financial conflicts.

Limited resection inferior for elderly with early NSCLC
Limited resection is inferior to lobectomy for older patients with early-stage invasive NSCLC, yielding lower overall survival and cancer-specific survival, according to a study published online Aug. 3 in Journal of Clinical Oncology.
Limited resection – wedge resection or segmentectomy – is increasingly chosen over lobectomy for patients older than 65 because it is thought to yield equivalent survival among patients who are already near the end of their lives and to cut down on perioperative and postoperative complications. Moreover, the number of these surgeries is expected to increase substantially when the recently released U.S. Preventive Services Task Force recommendations for lung cancer screening are fully implemented, said Dr. Rajwanth R. Veluswamy of the division of hematology and medical oncology, Mount Sinai University, New York, and his associates.

However, the evidence supporting the equivalency of limited resection to lobectomy is scant and not of high quality. To examine the issue more closely, the investigators analyzed survival outcomes for 3,147 patients aged 65 and older who were included in the nationally representative population-based Surveillance, Epidemiology, and End Results (SEER) database. These patients had stage 1A NSCLC of 2 cm or less in diameter and were treated surgically in 1998 through 2009.
Limited resection was found to be inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.66) among patients with invasive adenocarcinoma. Limited resection also was inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.41) among patients with squamous cell carcinoma, Dr. Veluswamy and his associates said (J Clin Oncol. 2015 Aug. 3. doi:10.1200/JCO.2014.60.6624).
“Our findings should help decide the best treatment for older patients by balancing the potential short- and long-term risks of limited resection versus lobectomy,” they said.
The investigators added that they focused on patients older than age 65 because that is the age group most frequently affected by invasive NSCLC and most likely to be considered for limited resection. These results cannot be extrapolated to younger patients because they have longer life expectancies and thus higher risk of recurrence after “limited” treatment.
The U.S. Agency for Healthcare Research and Quality supported the study. Dr. Veluswamy had no disclosures; his associates reported ties to Pfizer, Otsuka, Teva Neuroscience, EHE International, United BioSource, Ethicon, Covidien, Genentech, IMS Health, Merck, Bristol-Myers Squibb, Quintiles, and Sanofi.
Limited resection is inferior to lobectomy for older patients with early-stage invasive NSCLC, yielding lower overall survival and cancer-specific survival, according to a study published online Aug. 3 in Journal of Clinical Oncology.
Limited resection – wedge resection or segmentectomy – is increasingly chosen over lobectomy for patients older than 65 because it is thought to yield equivalent survival among patients who are already near the end of their lives and to cut down on perioperative and postoperative complications. Moreover, the number of these surgeries is expected to increase substantially when the recently released U.S. Preventive Services Task Force recommendations for lung cancer screening are fully implemented, said Dr. Rajwanth R. Veluswamy of the division of hematology and medical oncology, Mount Sinai University, New York, and his associates.
However, the evidence supporting the equivalency of limited resection to lobectomy is scant and not of high quality. To examine the issue more closely, the investigators analyzed survival outcomes for 3,147 patients aged 65 and older who were included in the nationally representative population-based Surveillance, Epidemiology, and End Results (SEER) database. These patients had stage 1A NSCLC of 2 cm or less in diameter and were treated surgically in 1998 through 2009.
Limited resection was found to be inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.66) among patients with invasive adenocarcinoma. Limited resection also was inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.41) among patients with squamous cell carcinoma, Dr. Veluswamy and his associates said (J Clin Oncol. 2015 Aug. 3. doi:10.1200/JCO.2014.60.6624).
“Our findings should help decide the best treatment for older patients by balancing the potential short- and long-term risks of limited resection versus lobectomy,” they said.
The investigators added that they focused on patients older than age 65 because that is the age group most frequently affected by invasive NSCLC and most likely to be considered for limited resection. These results cannot be extrapolated to younger patients because they have longer life expectancies and thus higher risk of recurrence after “limited” treatment.
The U.S. Agency for Healthcare Research and Quality supported the study. Dr. Veluswamy had no disclosures; his associates reported ties to Pfizer, Otsuka, Teva Neuroscience, EHE International, United BioSource, Ethicon, Covidien, Genentech, IMS Health, Merck, Bristol-Myers Squibb, Quintiles, and Sanofi.
Limited resection is inferior to lobectomy for older patients with early-stage invasive NSCLC, yielding lower overall survival and cancer-specific survival, according to a study published online Aug. 3 in Journal of Clinical Oncology.
Limited resection – wedge resection or segmentectomy – is increasingly chosen over lobectomy for patients older than 65 because it is thought to yield equivalent survival among patients who are already near the end of their lives and to cut down on perioperative and postoperative complications. Moreover, the number of these surgeries is expected to increase substantially when the recently released U.S. Preventive Services Task Force recommendations for lung cancer screening are fully implemented, said Dr. Rajwanth R. Veluswamy of the division of hematology and medical oncology, Mount Sinai University, New York, and his associates.
However, the evidence supporting the equivalency of limited resection to lobectomy is scant and not of high quality. To examine the issue more closely, the investigators analyzed survival outcomes for 3,147 patients aged 65 and older who were included in the nationally representative population-based Surveillance, Epidemiology, and End Results (SEER) database. These patients had stage 1A NSCLC of 2 cm or less in diameter and were treated surgically in 1998 through 2009.
Limited resection was found to be inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.66) among patients with invasive adenocarcinoma. Limited resection also was inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.41) among patients with squamous cell carcinoma, Dr. Veluswamy and his associates said (J Clin Oncol. 2015 Aug. 3. doi:10.1200/JCO.2014.60.6624).
“Our findings should help decide the best treatment for older patients by balancing the potential short- and long-term risks of limited resection versus lobectomy,” they said.
The investigators added that they focused on patients older than age 65 because that is the age group most frequently affected by invasive NSCLC and most likely to be considered for limited resection. These results cannot be extrapolated to younger patients because they have longer life expectancies and thus higher risk of recurrence after “limited” treatment.
The U.S. Agency for Healthcare Research and Quality supported the study. Dr. Veluswamy had no disclosures; his associates reported ties to Pfizer, Otsuka, Teva Neuroscience, EHE International, United BioSource, Ethicon, Covidien, Genentech, IMS Health, Merck, Bristol-Myers Squibb, Quintiles, and Sanofi.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Limited resection is inferior to lobectomy for older patients with early-stage invasive NSCLC.
Major finding: Limited resection was found to be inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.66) among patients with invasive adenocarcinoma. Limited resection also was inferior to lobectomy regarding overall survival (HR, 1.21) and lung cancer–specific survival (HR, 1.41) among patients with squamous cell carcinoma, .
Data source: An analysis of population-based data of survival outcomes in 3,147 older patients with early-stage invasive NSCLC treated surgically in 1998-2009.
Disclosures: The U.S. Agency for Healthcare Research and Quality supported the study. Dr. Veluswamy had no disclosures; his associates reported ties to Pfizer, Otsuka, Teva Neuroscience, EHE International, United BioSource, Ethicon, Covidien, Genentech, IMS Health, Merck, Bristol-Myers Squibb, Quintiles, and Sanofi.

Medicare hospital costs down over last 6 months of life
Inpatient costs for Medicare patients over the last 6 months of life dropped 23% per death from 2009 to 2013, a study showed.
After adjustment for inflation, the average inpatient cost for patients aged 65 years and older who died was over $17,400 in 2009. By 2013, Medicare spending in the last 6 months of life had dropped to just under $13,400. The trend in spending was similar over the last 3 months of life and over the last month, but the declines – 18% for the last 3 months and 14.5% for the last month – were not as great, reported Dr. Harlan M. Krumholz of Yale University in New Haven, Conn., and his associates (JAMA. 2015;314(4):355-365).
The investigators noted that “approximately 60% of spending in the last 6 months of beneficiaries’ lives occurred during their final month.”
The analysis included 60,056,069 individuals aged 65 years or older who were enrolled in a Medicare fee-for-service plan for at least 1 month between 1999 and 2013.
Dr. Krumholz is supported by a grant from the National Heart, Lung, and Blood Institute.
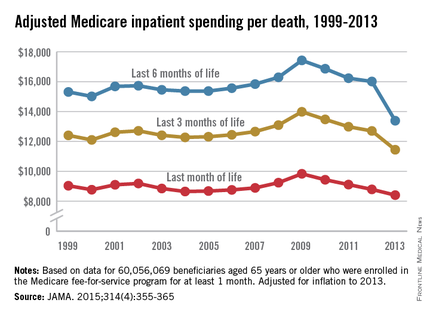
Inpatient costs for Medicare patients over the last 6 months of life dropped 23% per death from 2009 to 2013, a study showed.
After adjustment for inflation, the average inpatient cost for patients aged 65 years and older who died was over $17,400 in 2009. By 2013, Medicare spending in the last 6 months of life had dropped to just under $13,400. The trend in spending was similar over the last 3 months of life and over the last month, but the declines – 18% for the last 3 months and 14.5% for the last month – were not as great, reported Dr. Harlan M. Krumholz of Yale University in New Haven, Conn., and his associates (JAMA. 2015;314(4):355-365).
The investigators noted that “approximately 60% of spending in the last 6 months of beneficiaries’ lives occurred during their final month.”
The analysis included 60,056,069 individuals aged 65 years or older who were enrolled in a Medicare fee-for-service plan for at least 1 month between 1999 and 2013.
Dr. Krumholz is supported by a grant from the National Heart, Lung, and Blood Institute.
Inpatient costs for Medicare patients over the last 6 months of life dropped 23% per death from 2009 to 2013, a study showed.
After adjustment for inflation, the average inpatient cost for patients aged 65 years and older who died was over $17,400 in 2009. By 2013, Medicare spending in the last 6 months of life had dropped to just under $13,400. The trend in spending was similar over the last 3 months of life and over the last month, but the declines – 18% for the last 3 months and 14.5% for the last month – were not as great, reported Dr. Harlan M. Krumholz of Yale University in New Haven, Conn., and his associates (JAMA. 2015;314(4):355-365).
The investigators noted that “approximately 60% of spending in the last 6 months of beneficiaries’ lives occurred during their final month.”
The analysis included 60,056,069 individuals aged 65 years or older who were enrolled in a Medicare fee-for-service plan for at least 1 month between 1999 and 2013.
Dr. Krumholz is supported by a grant from the National Heart, Lung, and Blood Institute.
FROM JAMA