User login
Official Newspaper of the American College of Surgeons
Hybrid approach tackles critical limb ischemia
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.

The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
AT MIDWESTERN VASCULAR 2015
Key clinical point: Hybrid-based iliofemoral endarterectomy provides robust inflow restoration comparable to aortofemoral bypass, with minimal perioperative morbidity.
Major finding: Primary patency was 100% with a mean follow-up of 13 months.
Data source: Five-year retrospective study in 40 limbs in 33 patients with critical limb ischemia.
Disclosures: The authors reported having no financial disclosures.

Psychiatrists’ role in bariatric surgery important
Obesity has been officially declared a global epidemic by the World Health Organization. In virtually every region of the world, obesity’s adverse health effects are a well-documented public health crisis that affects people of all ages. In light of poor long-term weight management reported in most traditional diet strategies, attention has shifted to gastric bypass surgery as an effective treatment option for obesity.
Bariatric weight loss procedures are associated with numerous health benefits in patients: dramatic weight loss, rapid improvement in blood glucose levels, blood pressure stabilization, and resolution of obesity-related orthopedic problems. It’s not surprising, then, that gastric bypass surgery is a life-changing event for many patients.

Recently however, it has become clear that “life-changing” interventions do not always mean happy endings. Alongside these encouraging postsurgical outcomes are alarming counterintuitive reports of increased self-harm events. A recent study published in JAMA Surgery by Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto, and colleagues reported an increase in suicide attempts among postoperative gastric bypass patients (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414). The study conducted at Sunnybrook found that the rate of self-harm emergencies from attempted suicide was four times higher in these patients, compared with the general population.
Most gastric bypass surgery programs require a pre-op mental health evaluation. This is not enough, according to Dr. Peter F. Crookes, associate professor* of Bariatric Surgery at Keck Hospital of the University of Southern California, Los Angeles. Dr. Crookes’s clinical experiences and my (Dr. Baron’s) 20-plus years of conducting psychiatric evaluations on bypass patients have revealed more vexing issues regarding psychiatric illnesses occurring in morbidly obese patients. The requirement has been established for presurgical psychiatric assessment, but long-term post-surgical emotional and behavioral challenges need to be evaluated as well. In addition to primary mental illness, obese patients are at risk for stress-related exacerbations of preexisting psychopathology. After a body-altering surgical procedure like gastric bypass, maladaptive coping strategies are likely to complicate a patient’s physical AND emotional long-term recovery.
Many factors play into the development of these psychiatric symptoms, not the least of which are coping and emotional support systems. Literature on obesity and psychiatry has revealed connections between weight status and issues, such as childhood trauma, especially sexual abuse in childhood. While some patients claim that their weight loss surgery was the best thing they ever did for themselves, other patients have reported to me after significant weight loss: “I feel like a fat person trapped in a skinny body.” This surgery is not just body altering but can be identity altering. Patients also have reported relationship issues after significant weight loss. Relationship dynamics for both partners can become strained as a result of perceived changes in sexual attractiveness.
Given the short- and long-term consequences, it is essential for psychiatrists and other mental health care providers to work closely with the bypass surgical team at 1 month, 3 months, and 1-year postsurgical follow-up visits. These follow-ups are particularly important for patients who experience depression, relationship stress, or worsened psychiatric symptoms. In 2004, Dr. Crookes coauthored a then controversial study concerning bariatric surgery for obese patients with a formal diagnosis of schizophrenia or schizoaffective disorder (Obes Surg. 2004 Mar;14[3]:349-52). Historically, bariatric surgeons had avoided operating on these patients. However, his study showed that when psychotic symptoms were controlled postoperatively, these patients’ weight loss results were comparable to those of nonpsychotic patients.
Quality of life after gastric bypass depends on much more than a decrease in the number on the scale or clothing label. These reports demonstrate that psychiatrists play an important role in the overall biopsychosocial outcome of the patient.
Dr. Baron is professor of clinical psychiatry and interim chair of the department of psychiatry at the University of Southern California, Los Angeles. He also serves as director of the Global Center for Exercise, Psychiatry and Sports at USC. Ms. In addition, Dr. Baron is former chair of the department of psychiatry at Temple University, Philadelphia, where he directed the psychiatric component of the Bariatric Surgery program. Ms. Uno is a third-year medical student at USC.
*Correction, 10/29/2015: An earlier version of this story misstated the title of Dr. Crookes.
Obesity has been officially declared a global epidemic by the World Health Organization. In virtually every region of the world, obesity’s adverse health effects are a well-documented public health crisis that affects people of all ages. In light of poor long-term weight management reported in most traditional diet strategies, attention has shifted to gastric bypass surgery as an effective treatment option for obesity.
Bariatric weight loss procedures are associated with numerous health benefits in patients: dramatic weight loss, rapid improvement in blood glucose levels, blood pressure stabilization, and resolution of obesity-related orthopedic problems. It’s not surprising, then, that gastric bypass surgery is a life-changing event for many patients.
Recently however, it has become clear that “life-changing” interventions do not always mean happy endings. Alongside these encouraging postsurgical outcomes are alarming counterintuitive reports of increased self-harm events. A recent study published in JAMA Surgery by Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto, and colleagues reported an increase in suicide attempts among postoperative gastric bypass patients (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414). The study conducted at Sunnybrook found that the rate of self-harm emergencies from attempted suicide was four times higher in these patients, compared with the general population.
Most gastric bypass surgery programs require a pre-op mental health evaluation. This is not enough, according to Dr. Peter F. Crookes, associate professor* of Bariatric Surgery at Keck Hospital of the University of Southern California, Los Angeles. Dr. Crookes’s clinical experiences and my (Dr. Baron’s) 20-plus years of conducting psychiatric evaluations on bypass patients have revealed more vexing issues regarding psychiatric illnesses occurring in morbidly obese patients. The requirement has been established for presurgical psychiatric assessment, but long-term post-surgical emotional and behavioral challenges need to be evaluated as well. In addition to primary mental illness, obese patients are at risk for stress-related exacerbations of preexisting psychopathology. After a body-altering surgical procedure like gastric bypass, maladaptive coping strategies are likely to complicate a patient’s physical AND emotional long-term recovery.
Many factors play into the development of these psychiatric symptoms, not the least of which are coping and emotional support systems. Literature on obesity and psychiatry has revealed connections between weight status and issues, such as childhood trauma, especially sexual abuse in childhood. While some patients claim that their weight loss surgery was the best thing they ever did for themselves, other patients have reported to me after significant weight loss: “I feel like a fat person trapped in a skinny body.” This surgery is not just body altering but can be identity altering. Patients also have reported relationship issues after significant weight loss. Relationship dynamics for both partners can become strained as a result of perceived changes in sexual attractiveness.
Given the short- and long-term consequences, it is essential for psychiatrists and other mental health care providers to work closely with the bypass surgical team at 1 month, 3 months, and 1-year postsurgical follow-up visits. These follow-ups are particularly important for patients who experience depression, relationship stress, or worsened psychiatric symptoms. In 2004, Dr. Crookes coauthored a then controversial study concerning bariatric surgery for obese patients with a formal diagnosis of schizophrenia or schizoaffective disorder (Obes Surg. 2004 Mar;14[3]:349-52). Historically, bariatric surgeons had avoided operating on these patients. However, his study showed that when psychotic symptoms were controlled postoperatively, these patients’ weight loss results were comparable to those of nonpsychotic patients.
Quality of life after gastric bypass depends on much more than a decrease in the number on the scale or clothing label. These reports demonstrate that psychiatrists play an important role in the overall biopsychosocial outcome of the patient.
Dr. Baron is professor of clinical psychiatry and interim chair of the department of psychiatry at the University of Southern California, Los Angeles. He also serves as director of the Global Center for Exercise, Psychiatry and Sports at USC. Ms. In addition, Dr. Baron is former chair of the department of psychiatry at Temple University, Philadelphia, where he directed the psychiatric component of the Bariatric Surgery program. Ms. Uno is a third-year medical student at USC.
*Correction, 10/29/2015: An earlier version of this story misstated the title of Dr. Crookes.
Obesity has been officially declared a global epidemic by the World Health Organization. In virtually every region of the world, obesity’s adverse health effects are a well-documented public health crisis that affects people of all ages. In light of poor long-term weight management reported in most traditional diet strategies, attention has shifted to gastric bypass surgery as an effective treatment option for obesity.
Bariatric weight loss procedures are associated with numerous health benefits in patients: dramatic weight loss, rapid improvement in blood glucose levels, blood pressure stabilization, and resolution of obesity-related orthopedic problems. It’s not surprising, then, that gastric bypass surgery is a life-changing event for many patients.
Recently however, it has become clear that “life-changing” interventions do not always mean happy endings. Alongside these encouraging postsurgical outcomes are alarming counterintuitive reports of increased self-harm events. A recent study published in JAMA Surgery by Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto, and colleagues reported an increase in suicide attempts among postoperative gastric bypass patients (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414). The study conducted at Sunnybrook found that the rate of self-harm emergencies from attempted suicide was four times higher in these patients, compared with the general population.
Most gastric bypass surgery programs require a pre-op mental health evaluation. This is not enough, according to Dr. Peter F. Crookes, associate professor* of Bariatric Surgery at Keck Hospital of the University of Southern California, Los Angeles. Dr. Crookes’s clinical experiences and my (Dr. Baron’s) 20-plus years of conducting psychiatric evaluations on bypass patients have revealed more vexing issues regarding psychiatric illnesses occurring in morbidly obese patients. The requirement has been established for presurgical psychiatric assessment, but long-term post-surgical emotional and behavioral challenges need to be evaluated as well. In addition to primary mental illness, obese patients are at risk for stress-related exacerbations of preexisting psychopathology. After a body-altering surgical procedure like gastric bypass, maladaptive coping strategies are likely to complicate a patient’s physical AND emotional long-term recovery.
Many factors play into the development of these psychiatric symptoms, not the least of which are coping and emotional support systems. Literature on obesity and psychiatry has revealed connections between weight status and issues, such as childhood trauma, especially sexual abuse in childhood. While some patients claim that their weight loss surgery was the best thing they ever did for themselves, other patients have reported to me after significant weight loss: “I feel like a fat person trapped in a skinny body.” This surgery is not just body altering but can be identity altering. Patients also have reported relationship issues after significant weight loss. Relationship dynamics for both partners can become strained as a result of perceived changes in sexual attractiveness.
Given the short- and long-term consequences, it is essential for psychiatrists and other mental health care providers to work closely with the bypass surgical team at 1 month, 3 months, and 1-year postsurgical follow-up visits. These follow-ups are particularly important for patients who experience depression, relationship stress, or worsened psychiatric symptoms. In 2004, Dr. Crookes coauthored a then controversial study concerning bariatric surgery for obese patients with a formal diagnosis of schizophrenia or schizoaffective disorder (Obes Surg. 2004 Mar;14[3]:349-52). Historically, bariatric surgeons had avoided operating on these patients. However, his study showed that when psychotic symptoms were controlled postoperatively, these patients’ weight loss results were comparable to those of nonpsychotic patients.
Quality of life after gastric bypass depends on much more than a decrease in the number on the scale or clothing label. These reports demonstrate that psychiatrists play an important role in the overall biopsychosocial outcome of the patient.
Dr. Baron is professor of clinical psychiatry and interim chair of the department of psychiatry at the University of Southern California, Los Angeles. He also serves as director of the Global Center for Exercise, Psychiatry and Sports at USC. Ms. In addition, Dr. Baron is former chair of the department of psychiatry at Temple University, Philadelphia, where he directed the psychiatric component of the Bariatric Surgery program. Ms. Uno is a third-year medical student at USC.
*Correction, 10/29/2015: An earlier version of this story misstated the title of Dr. Crookes.
Blacks receive inferior care for localized prostate cancer
Black patients with localized prostate cancer who underwent radical prostatectomy received inferior surgical care, compared with whites, as evidenced by fewer lymph node dissections and longer delays from diagnosis to treatment, among other indicators, researchers reported.
The time from diagnosis to treatment was longer in blacks than whites (79 vs. 71 days, P = .001). Overall, 57.7% of blacks had surgery without adjuvant therapy, compared with 61.3% of whites (P = .001). Blacks were less likely to undergo lymph node dissection (52.8% vs. 61.5%, P less than .001). The difference persisted but was not significant when the lymph node dissection analysis was restricted to patients with intermediate- and high-risk disease. Blacks were more likely to visit the emergency department within 30 days (P = .04) and beyond 30 days (P = .006) (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384).
When the lymph node dissection analysis was adjusted for geographic location (health service area), there were no differences between groups, which suggests that geographic variation in quality of care is tightly linked to racial disparities and may account for a large proportion of the differences.
The retrospective analysis of Medicare billing records evaluated 26,482 patients (2,020 blacks [7.6%] and 24,462 non-Hispanic whites [92.4%]) who underwent radical prostatectomy from 1992 through 2009.
Prostate cancer–specific mortality was not significantly different between blacks and whites. Unadjusted overall mortality was increased in blacks, but after adjustment for geographic location, overall mortality was similar between groups.
“Despite important constellations of poor quality of care for blacks undergoing [radical prostatectomy], we did not detect significant differences in overall and cancer-specific survival,” wrote Dr. Marianne Schmid of Brigham and Women’s Hospital, Harvard Medical School, Boston, and her colleagues. Furthermore, the research revealed no regional variation in cancer-specific mortality among patients who underwent surgery.
“A possible interpretation of our findings is that the biological differences in tumor aggressiveness among blacks may have been exaggerated, and that the perceived gap in survival is a result of lack of access or cultural perceptions with regard to surgical care for [prostate cancer] or other factors that differentiate who makes it to the operating table,” the researchers noted.
Median total calculated costs were lower for blacks ($13,015 vs. $15,758), but surgical treatment was associated with higher incremental annual costs, with the top 50% spending $1,185 more. Increased costs are likely due to the higher prevalence of radiotherapy and androgen deprivation therapy, and increased rates of emergency department visits, rather than the use of newer, more expensive technologies.
The research indicates that unfavorable quality of care for black patients did not translate to worse overall survival and cancer-specific survival. Rather, lower survival among black patients with prostate cancer may result from barriers to definitive treatment, according to the investigators.
Dr. Schmid reported having no relevant financial disclosures. Several of her coauthors reported financial ties to several industry sources.
The findings of the study by Dr. Schmid and her colleagues point to racial health inequalities in the United States and are applicable to medical care of the American population in general, not just to men with prostate cancer.

|
Dr. Otis Brawley |
Despite the fact that black patients in this study had insurance and access to care and were considered healthy enough for surgery, there was still a disparity in quality of care. Interestingly, there were no differences between the groups in all-cause or cancer-specific mortality. This is hard evidence that the biology of prostate cancer is similar for black and white men with localized disease.
Is the disparity in quality of care due to racism on the part of physicians? Probably not. More likely, a higher proportion of black men have physicians who do not routinely perform radical prostatectomies, and a higher proportion of blacks are treated at hospitals that have a low volume of prostate surgery.
Even though a significant proportion of blacks received inferior treatment, similar outcomes for the two groups suggests that some patients with localized prostate cancer are overtreated, and the medical community should be more discerning in who receives treatment.
Dr. Otis Brawley is the chief medical officer for the American Cancer Society and professor of hematology, oncology, medicine, and epidemiology at Emory University, Atlanta. These remarks were part of an editorial accompanying the report (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384). Dr. Brawley reported having no relevant financial disclosures.
The findings of the study by Dr. Schmid and her colleagues point to racial health inequalities in the United States and are applicable to medical care of the American population in general, not just to men with prostate cancer.
|
|
Dr. Otis Brawley |
Despite the fact that black patients in this study had insurance and access to care and were considered healthy enough for surgery, there was still a disparity in quality of care. Interestingly, there were no differences between the groups in all-cause or cancer-specific mortality. This is hard evidence that the biology of prostate cancer is similar for black and white men with localized disease.
Is the disparity in quality of care due to racism on the part of physicians? Probably not. More likely, a higher proportion of black men have physicians who do not routinely perform radical prostatectomies, and a higher proportion of blacks are treated at hospitals that have a low volume of prostate surgery.
Even though a significant proportion of blacks received inferior treatment, similar outcomes for the two groups suggests that some patients with localized prostate cancer are overtreated, and the medical community should be more discerning in who receives treatment.
Dr. Otis Brawley is the chief medical officer for the American Cancer Society and professor of hematology, oncology, medicine, and epidemiology at Emory University, Atlanta. These remarks were part of an editorial accompanying the report (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384). Dr. Brawley reported having no relevant financial disclosures.
The findings of the study by Dr. Schmid and her colleagues point to racial health inequalities in the United States and are applicable to medical care of the American population in general, not just to men with prostate cancer.
|
|
Dr. Otis Brawley |
Despite the fact that black patients in this study had insurance and access to care and were considered healthy enough for surgery, there was still a disparity in quality of care. Interestingly, there were no differences between the groups in all-cause or cancer-specific mortality. This is hard evidence that the biology of prostate cancer is similar for black and white men with localized disease.
Is the disparity in quality of care due to racism on the part of physicians? Probably not. More likely, a higher proportion of black men have physicians who do not routinely perform radical prostatectomies, and a higher proportion of blacks are treated at hospitals that have a low volume of prostate surgery.
Even though a significant proportion of blacks received inferior treatment, similar outcomes for the two groups suggests that some patients with localized prostate cancer are overtreated, and the medical community should be more discerning in who receives treatment.
Dr. Otis Brawley is the chief medical officer for the American Cancer Society and professor of hematology, oncology, medicine, and epidemiology at Emory University, Atlanta. These remarks were part of an editorial accompanying the report (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384). Dr. Brawley reported having no relevant financial disclosures.
Black patients with localized prostate cancer who underwent radical prostatectomy received inferior surgical care, compared with whites, as evidenced by fewer lymph node dissections and longer delays from diagnosis to treatment, among other indicators, researchers reported.
The time from diagnosis to treatment was longer in blacks than whites (79 vs. 71 days, P = .001). Overall, 57.7% of blacks had surgery without adjuvant therapy, compared with 61.3% of whites (P = .001). Blacks were less likely to undergo lymph node dissection (52.8% vs. 61.5%, P less than .001). The difference persisted but was not significant when the lymph node dissection analysis was restricted to patients with intermediate- and high-risk disease. Blacks were more likely to visit the emergency department within 30 days (P = .04) and beyond 30 days (P = .006) (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384).
When the lymph node dissection analysis was adjusted for geographic location (health service area), there were no differences between groups, which suggests that geographic variation in quality of care is tightly linked to racial disparities and may account for a large proportion of the differences.
The retrospective analysis of Medicare billing records evaluated 26,482 patients (2,020 blacks [7.6%] and 24,462 non-Hispanic whites [92.4%]) who underwent radical prostatectomy from 1992 through 2009.
Prostate cancer–specific mortality was not significantly different between blacks and whites. Unadjusted overall mortality was increased in blacks, but after adjustment for geographic location, overall mortality was similar between groups.
“Despite important constellations of poor quality of care for blacks undergoing [radical prostatectomy], we did not detect significant differences in overall and cancer-specific survival,” wrote Dr. Marianne Schmid of Brigham and Women’s Hospital, Harvard Medical School, Boston, and her colleagues. Furthermore, the research revealed no regional variation in cancer-specific mortality among patients who underwent surgery.
“A possible interpretation of our findings is that the biological differences in tumor aggressiveness among blacks may have been exaggerated, and that the perceived gap in survival is a result of lack of access or cultural perceptions with regard to surgical care for [prostate cancer] or other factors that differentiate who makes it to the operating table,” the researchers noted.
Median total calculated costs were lower for blacks ($13,015 vs. $15,758), but surgical treatment was associated with higher incremental annual costs, with the top 50% spending $1,185 more. Increased costs are likely due to the higher prevalence of radiotherapy and androgen deprivation therapy, and increased rates of emergency department visits, rather than the use of newer, more expensive technologies.
The research indicates that unfavorable quality of care for black patients did not translate to worse overall survival and cancer-specific survival. Rather, lower survival among black patients with prostate cancer may result from barriers to definitive treatment, according to the investigators.
Dr. Schmid reported having no relevant financial disclosures. Several of her coauthors reported financial ties to several industry sources.
Black patients with localized prostate cancer who underwent radical prostatectomy received inferior surgical care, compared with whites, as evidenced by fewer lymph node dissections and longer delays from diagnosis to treatment, among other indicators, researchers reported.
The time from diagnosis to treatment was longer in blacks than whites (79 vs. 71 days, P = .001). Overall, 57.7% of blacks had surgery without adjuvant therapy, compared with 61.3% of whites (P = .001). Blacks were less likely to undergo lymph node dissection (52.8% vs. 61.5%, P less than .001). The difference persisted but was not significant when the lymph node dissection analysis was restricted to patients with intermediate- and high-risk disease. Blacks were more likely to visit the emergency department within 30 days (P = .04) and beyond 30 days (P = .006) (JAMA Oncol. 2015 Oct 22. doi: 10.1001/jamaoncol/2015.3384).
When the lymph node dissection analysis was adjusted for geographic location (health service area), there were no differences between groups, which suggests that geographic variation in quality of care is tightly linked to racial disparities and may account for a large proportion of the differences.
The retrospective analysis of Medicare billing records evaluated 26,482 patients (2,020 blacks [7.6%] and 24,462 non-Hispanic whites [92.4%]) who underwent radical prostatectomy from 1992 through 2009.
Prostate cancer–specific mortality was not significantly different between blacks and whites. Unadjusted overall mortality was increased in blacks, but after adjustment for geographic location, overall mortality was similar between groups.
“Despite important constellations of poor quality of care for blacks undergoing [radical prostatectomy], we did not detect significant differences in overall and cancer-specific survival,” wrote Dr. Marianne Schmid of Brigham and Women’s Hospital, Harvard Medical School, Boston, and her colleagues. Furthermore, the research revealed no regional variation in cancer-specific mortality among patients who underwent surgery.
“A possible interpretation of our findings is that the biological differences in tumor aggressiveness among blacks may have been exaggerated, and that the perceived gap in survival is a result of lack of access or cultural perceptions with regard to surgical care for [prostate cancer] or other factors that differentiate who makes it to the operating table,” the researchers noted.
Median total calculated costs were lower for blacks ($13,015 vs. $15,758), but surgical treatment was associated with higher incremental annual costs, with the top 50% spending $1,185 more. Increased costs are likely due to the higher prevalence of radiotherapy and androgen deprivation therapy, and increased rates of emergency department visits, rather than the use of newer, more expensive technologies.
The research indicates that unfavorable quality of care for black patients did not translate to worse overall survival and cancer-specific survival. Rather, lower survival among black patients with prostate cancer may result from barriers to definitive treatment, according to the investigators.
Dr. Schmid reported having no relevant financial disclosures. Several of her coauthors reported financial ties to several industry sources.
FROM JAMA ONCOLOGY
Key clinical point: Compared with whites, black patients with localized prostate cancer received lower quality of care.
Major finding: Blacks were less likely to undergo lymph node dissection than whites (52.8% vs. 61.5%; OR, 0.76; P less than .001), and had more postoperative complications, emergency department visits, and readmissions (P less than .05 for all comparisons).
Data source: A retrospective analysis of Medicare billing records of 26,482 patients (7.6% blacks and 92.4% non-Hispanic whites) who underwent radical prostatectomy from 1992 through 2009.
Disclosures: Dr. Schmid reported having no relevant financial disclosures. Several of her coauthors reported financial ties to several industry sources.

Benefits, risks of total knee replacement for OA illuminated in trial
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.

|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
|
|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
|
|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Total knee replacement is superior to nonsurgical treatment in decreasing pain and improving function and quality of life.
Major finding: The surgical group showed a significantly greater improvement 1 year from baseline (32.5 out of a possible 100 points) than did the nonsurgical group (16.0 points) in mean Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life.
Data source: A randomized, controlled trial comparing 1-year outcomes after total knee replacement (50 patients) vs. nonsurgical treatment (50 patients) for osteoarthritis.
Disclosures: This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.

Malpractice premiums flat in 2015, but changes could be ahead
Physicians paid about the same in liability insurance premiums in 2015 as in 2014, and analysts don’t see costs changing anytime soon. A nationwide survey of insurers by the Medical Liability Monitor shows that 71% of insurance premiums did not change this year, while 17% of rates rose and 12% fell.
Internists experienced an average premium increase of 0.6% in 2015, while general surgeons saw a 0.2% average rate decrease, and ob.gyns experienced an average 0.5% rate increase.

The static premium market is being largely driven by the low number of lawsuits filed by patients and family members in recent years, said survey coauthor Paul Greve Jr., executive vice president/senior consultant for the Willis Health Care Practice, a global risk management consultant firm.
“It’s amazing to see the continuing stability in claim frequency,” Mr. Greve said in an interview. “The claims counts are just not rising. Its great for the industry, and it’s great for physicians, but it is puzzling because you wonder what has caused what amounts to a sea change in the attitudes of the general public toward malpractice litigation such that the claim counts were drop off.”
Premiums continue to vary geographically. Southern Florida internists for example, will pay $47,707 for malpractice insurance this year, while their counterparts in Minnesota will pay $3,375. For ob.gyns., premiums range from $214,999 in southern New York to $16,240 in central California. General surgeons in Southern Florida will pay $190,829 this year, while Wisconsin surgeons will pay $10,868.

Various factors influence premium amounts, including the overall legal climate and the rate of insurer competition in each state, said Susan J. Forray, principal and consulting actuary with the Milwaukee office of Milliman, a global provider of actuarial services.
“The dollar amounts themselves are a function of the litigation environment [and] the cost level of medicine or living within the state,” Ms. Forray said in an interview. “In terms of rate changes, we are seeing certain environments where there is more competition. Obviously, those more competitive markets are more likely to have rate decreases or perhaps, stable rates, where perhaps markets with less competition are more likely to see increased rates.”
On a regional basis, Southern physicians experienced the largest rate increases, while doctors in the Northeast, West, and Midwest continued to see decreases. The Midwest’s 0.8% rate decrease was the largest decline, while Western states experienced a 0.2% average rate decrease. On average, the South showed a rate increase of 0.9% and the Northeast experienced a 0.1% average decrease. Doctors in Georgia, North Carolina, and Texas saw rate increases in excess of 5%, while Iowa physicians experienced an 11% rate decrease. Only three western states experienced rate increases: New Mexico at 2.5%, Oregon at 2%, and Idaho at 1%. Premium changes for Northeastern doctors fluctuated from Rhode Island’s 7% increase to Pennsylvania’s 8% decrease. Additionally, for the first time in 8 years, the premium market experienced an average overall increase of 0.3% in 2015, compared with an average overall decrease of 1.5% last year.
The jury is still out on how the Affordable Care Act and other health reforms will impact the malpractice premium market, according to Mr. Greve. He said that he believes the majority of upcoming health reforms will improve patient safety, thus reducing liability for doctors. However, as more physicians become part of larger networks to deliver new models of care, their contractual liability spreads, he said. However, as value-based care becomes the law of the land, new claims could arise.
“We’re just beginning to see the tip of the iceberg here,” Mr. Greve said. “In the past, it was overutilization, [the claim] that you did something in order to put money in your pocket. With putting providers at financial risk with capitated or bundled payments or global payments, then the argument is going to be, ‘You didn’t deliver enough care,’ or ‘You [used that device] because it was less expensive.’ ”
The MLM survey, published yearly in October, gathered July 1 premium data from the major malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med
Physicians paid about the same in liability insurance premiums in 2015 as in 2014, and analysts don’t see costs changing anytime soon. A nationwide survey of insurers by the Medical Liability Monitor shows that 71% of insurance premiums did not change this year, while 17% of rates rose and 12% fell.
Internists experienced an average premium increase of 0.6% in 2015, while general surgeons saw a 0.2% average rate decrease, and ob.gyns experienced an average 0.5% rate increase.
The static premium market is being largely driven by the low number of lawsuits filed by patients and family members in recent years, said survey coauthor Paul Greve Jr., executive vice president/senior consultant for the Willis Health Care Practice, a global risk management consultant firm.
“It’s amazing to see the continuing stability in claim frequency,” Mr. Greve said in an interview. “The claims counts are just not rising. Its great for the industry, and it’s great for physicians, but it is puzzling because you wonder what has caused what amounts to a sea change in the attitudes of the general public toward malpractice litigation such that the claim counts were drop off.”
Premiums continue to vary geographically. Southern Florida internists for example, will pay $47,707 for malpractice insurance this year, while their counterparts in Minnesota will pay $3,375. For ob.gyns., premiums range from $214,999 in southern New York to $16,240 in central California. General surgeons in Southern Florida will pay $190,829 this year, while Wisconsin surgeons will pay $10,868.
Various factors influence premium amounts, including the overall legal climate and the rate of insurer competition in each state, said Susan J. Forray, principal and consulting actuary with the Milwaukee office of Milliman, a global provider of actuarial services.
“The dollar amounts themselves are a function of the litigation environment [and] the cost level of medicine or living within the state,” Ms. Forray said in an interview. “In terms of rate changes, we are seeing certain environments where there is more competition. Obviously, those more competitive markets are more likely to have rate decreases or perhaps, stable rates, where perhaps markets with less competition are more likely to see increased rates.”
On a regional basis, Southern physicians experienced the largest rate increases, while doctors in the Northeast, West, and Midwest continued to see decreases. The Midwest’s 0.8% rate decrease was the largest decline, while Western states experienced a 0.2% average rate decrease. On average, the South showed a rate increase of 0.9% and the Northeast experienced a 0.1% average decrease. Doctors in Georgia, North Carolina, and Texas saw rate increases in excess of 5%, while Iowa physicians experienced an 11% rate decrease. Only three western states experienced rate increases: New Mexico at 2.5%, Oregon at 2%, and Idaho at 1%. Premium changes for Northeastern doctors fluctuated from Rhode Island’s 7% increase to Pennsylvania’s 8% decrease. Additionally, for the first time in 8 years, the premium market experienced an average overall increase of 0.3% in 2015, compared with an average overall decrease of 1.5% last year.
The jury is still out on how the Affordable Care Act and other health reforms will impact the malpractice premium market, according to Mr. Greve. He said that he believes the majority of upcoming health reforms will improve patient safety, thus reducing liability for doctors. However, as more physicians become part of larger networks to deliver new models of care, their contractual liability spreads, he said. However, as value-based care becomes the law of the land, new claims could arise.
“We’re just beginning to see the tip of the iceberg here,” Mr. Greve said. “In the past, it was overutilization, [the claim] that you did something in order to put money in your pocket. With putting providers at financial risk with capitated or bundled payments or global payments, then the argument is going to be, ‘You didn’t deliver enough care,’ or ‘You [used that device] because it was less expensive.’ ”
The MLM survey, published yearly in October, gathered July 1 premium data from the major malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med
Physicians paid about the same in liability insurance premiums in 2015 as in 2014, and analysts don’t see costs changing anytime soon. A nationwide survey of insurers by the Medical Liability Monitor shows that 71% of insurance premiums did not change this year, while 17% of rates rose and 12% fell.
Internists experienced an average premium increase of 0.6% in 2015, while general surgeons saw a 0.2% average rate decrease, and ob.gyns experienced an average 0.5% rate increase.
The static premium market is being largely driven by the low number of lawsuits filed by patients and family members in recent years, said survey coauthor Paul Greve Jr., executive vice president/senior consultant for the Willis Health Care Practice, a global risk management consultant firm.
“It’s amazing to see the continuing stability in claim frequency,” Mr. Greve said in an interview. “The claims counts are just not rising. Its great for the industry, and it’s great for physicians, but it is puzzling because you wonder what has caused what amounts to a sea change in the attitudes of the general public toward malpractice litigation such that the claim counts were drop off.”
Premiums continue to vary geographically. Southern Florida internists for example, will pay $47,707 for malpractice insurance this year, while their counterparts in Minnesota will pay $3,375. For ob.gyns., premiums range from $214,999 in southern New York to $16,240 in central California. General surgeons in Southern Florida will pay $190,829 this year, while Wisconsin surgeons will pay $10,868.
Various factors influence premium amounts, including the overall legal climate and the rate of insurer competition in each state, said Susan J. Forray, principal and consulting actuary with the Milwaukee office of Milliman, a global provider of actuarial services.
“The dollar amounts themselves are a function of the litigation environment [and] the cost level of medicine or living within the state,” Ms. Forray said in an interview. “In terms of rate changes, we are seeing certain environments where there is more competition. Obviously, those more competitive markets are more likely to have rate decreases or perhaps, stable rates, where perhaps markets with less competition are more likely to see increased rates.”
On a regional basis, Southern physicians experienced the largest rate increases, while doctors in the Northeast, West, and Midwest continued to see decreases. The Midwest’s 0.8% rate decrease was the largest decline, while Western states experienced a 0.2% average rate decrease. On average, the South showed a rate increase of 0.9% and the Northeast experienced a 0.1% average decrease. Doctors in Georgia, North Carolina, and Texas saw rate increases in excess of 5%, while Iowa physicians experienced an 11% rate decrease. Only three western states experienced rate increases: New Mexico at 2.5%, Oregon at 2%, and Idaho at 1%. Premium changes for Northeastern doctors fluctuated from Rhode Island’s 7% increase to Pennsylvania’s 8% decrease. Additionally, for the first time in 8 years, the premium market experienced an average overall increase of 0.3% in 2015, compared with an average overall decrease of 1.5% last year.
The jury is still out on how the Affordable Care Act and other health reforms will impact the malpractice premium market, according to Mr. Greve. He said that he believes the majority of upcoming health reforms will improve patient safety, thus reducing liability for doctors. However, as more physicians become part of larger networks to deliver new models of care, their contractual liability spreads, he said. However, as value-based care becomes the law of the land, new claims could arise.
“We’re just beginning to see the tip of the iceberg here,” Mr. Greve said. “In the past, it was overutilization, [the claim] that you did something in order to put money in your pocket. With putting providers at financial risk with capitated or bundled payments or global payments, then the argument is going to be, ‘You didn’t deliver enough care,’ or ‘You [used that device] because it was less expensive.’ ”
The MLM survey, published yearly in October, gathered July 1 premium data from the major malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med

Botox suppresses atrial fibrillation after CABG
Injections of botulinum toxin into epicardial fat pads during cardiac surgery may provide long-term suppression of atrial fibrillation, according to results from a randomized, placebo-controlled trial published Oct. 20.
Sixty patients with a history of atrial fibrillation, who were undergoing coronary artery bypass graft surgery, were randomized to an injection of botulinum toxin or saline into each epicardial fat pad during surgery.

Data from 12 months of monitoring via an implantable loop recorder showed patients who received the botulinum toxin injections had a significantly reduced incidence of atrial fibrillation, compared with the placebo group in the 30 days after surgery (7% vs. 30%, P = .024) and at 12 months (0% vs. 27%, P = .002).
Both groups showed significant decreases in heart rate variability after surgery, but at 3 months, these had largely recovered in the placebo group and remained depressed in the botulinum toxin group until 6 months (Circ Arrhythm Electrophysiol. 2015 Oct 20. doi: 10.1161/CIRCEP.115.003199).
No patients in the botulinum group developed persistent atrial fibrillation or required antiarrhythmic therapy or interventions, and there were no significant differences between the two groups in other outcomes such as hospital length of stay or postoperative complications.
“The blocking effects are temporary and recover in 1 to 6 months, depending on the injection site [but] for patients with a high short-term risk of postoperative AF after cardiac surgery, temporary suppression of AF without any destruction of the anatomic structures is clinically desirable,” wrote Dr. Evgeny Pokushalov of State Research Institute of Circulation Pathology, Novosibirsk, Russia, and coauthors.
No conflicts of interest were declared.
Injections of botulinum toxin into epicardial fat pads during cardiac surgery may provide long-term suppression of atrial fibrillation, according to results from a randomized, placebo-controlled trial published Oct. 20.
Sixty patients with a history of atrial fibrillation, who were undergoing coronary artery bypass graft surgery, were randomized to an injection of botulinum toxin or saline into each epicardial fat pad during surgery.
Data from 12 months of monitoring via an implantable loop recorder showed patients who received the botulinum toxin injections had a significantly reduced incidence of atrial fibrillation, compared with the placebo group in the 30 days after surgery (7% vs. 30%, P = .024) and at 12 months (0% vs. 27%, P = .002).
Both groups showed significant decreases in heart rate variability after surgery, but at 3 months, these had largely recovered in the placebo group and remained depressed in the botulinum toxin group until 6 months (Circ Arrhythm Electrophysiol. 2015 Oct 20. doi: 10.1161/CIRCEP.115.003199).
No patients in the botulinum group developed persistent atrial fibrillation or required antiarrhythmic therapy or interventions, and there were no significant differences between the two groups in other outcomes such as hospital length of stay or postoperative complications.
“The blocking effects are temporary and recover in 1 to 6 months, depending on the injection site [but] for patients with a high short-term risk of postoperative AF after cardiac surgery, temporary suppression of AF without any destruction of the anatomic structures is clinically desirable,” wrote Dr. Evgeny Pokushalov of State Research Institute of Circulation Pathology, Novosibirsk, Russia, and coauthors.
No conflicts of interest were declared.
Injections of botulinum toxin into epicardial fat pads during cardiac surgery may provide long-term suppression of atrial fibrillation, according to results from a randomized, placebo-controlled trial published Oct. 20.
Sixty patients with a history of atrial fibrillation, who were undergoing coronary artery bypass graft surgery, were randomized to an injection of botulinum toxin or saline into each epicardial fat pad during surgery.
Data from 12 months of monitoring via an implantable loop recorder showed patients who received the botulinum toxin injections had a significantly reduced incidence of atrial fibrillation, compared with the placebo group in the 30 days after surgery (7% vs. 30%, P = .024) and at 12 months (0% vs. 27%, P = .002).
Both groups showed significant decreases in heart rate variability after surgery, but at 3 months, these had largely recovered in the placebo group and remained depressed in the botulinum toxin group until 6 months (Circ Arrhythm Electrophysiol. 2015 Oct 20. doi: 10.1161/CIRCEP.115.003199).
No patients in the botulinum group developed persistent atrial fibrillation or required antiarrhythmic therapy or interventions, and there were no significant differences between the two groups in other outcomes such as hospital length of stay or postoperative complications.
“The blocking effects are temporary and recover in 1 to 6 months, depending on the injection site [but] for patients with a high short-term risk of postoperative AF after cardiac surgery, temporary suppression of AF without any destruction of the anatomic structures is clinically desirable,” wrote Dr. Evgeny Pokushalov of State Research Institute of Circulation Pathology, Novosibirsk, Russia, and coauthors.
No conflicts of interest were declared.
FROM CIRCULATION: ARRHYTHMIA AND ELECTROPHYSIOLOGY
Key clinical point:Injections of botulinum toxin into epicardial fat pads during cardiac surgery may provide long-term suppression of atrial fibrillation.
Major finding: Patients who received the botulinum injections into epicardial fat pads had a significantly reduced incidence of atrial fibrillation (7%), compared with placebo (30%).
Data source: Randomized placebo-controlled trial of 60 patients with a history of atrial fibrillation who were undergoing coronary artery bypass graft surgery.
Disclosures: No conflicts of interest were declared.

VIDEO: A better option for C. difficile toxic megacolon
CHICAGO – Last-minute colectomy isn’t the way to go for Clostridium difficile–induced toxic megacolon; outcomes are better with a timely loop ileostomy and colonic lavage.
University of Pittsburgh surgery professor Dr. Brian Zuckerbraun, a pioneer of the technique, explained the procedure and its benefits in an interview at the annual Clinical Congress of the American College of Surgeons.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Last-minute colectomy isn’t the way to go for Clostridium difficile–induced toxic megacolon; outcomes are better with a timely loop ileostomy and colonic lavage.
University of Pittsburgh surgery professor Dr. Brian Zuckerbraun, a pioneer of the technique, explained the procedure and its benefits in an interview at the annual Clinical Congress of the American College of Surgeons.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Last-minute colectomy isn’t the way to go for Clostridium difficile–induced toxic megacolon; outcomes are better with a timely loop ileostomy and colonic lavage.
University of Pittsburgh surgery professor Dr. Brian Zuckerbraun, a pioneer of the technique, explained the procedure and its benefits in an interview at the annual Clinical Congress of the American College of Surgeons.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE ACS CLINICAL CONGRESS

What is your practice worth?
Over the last couple of years, I’ve written quite a lot about the trend toward consolidation. That trend shows no sign of abating; more and more soloists and small groups are selling or merging their practices with hospitals, multispecialty groups, or other large entities.
I have seen evidence, though, that many sellers are not receiving a fair price for the equity that they have worked so hard to build over several decades. If you are contemplating selling or merging, it is important that you not simply take the buyer’s word for how much your practice is worth. You need an impartial appraisal.
Of course, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in 750 words; but three basic yardsticks are essential for a practice appraisal:
• Tangible assets. Equipment, cash, accounts receivable and other property owned by the practice.
• Liabilities. Accounts payable, outstanding loans, and anything else owed to others.
• Intangible assets. Sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the equity, or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons why patients come back (if in fact they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferable. For example, unique skills with a laser, neurotoxins, or filler substances, or extraordinary personal charisma, may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash Flow Analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of Earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline Comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings (and thus its overall value) are.
Asset-based valuation is the most popular, but by no means the only method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not its income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll cover some sale and merger options that you may not have thought of next month.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
Over the last couple of years, I’ve written quite a lot about the trend toward consolidation. That trend shows no sign of abating; more and more soloists and small groups are selling or merging their practices with hospitals, multispecialty groups, or other large entities.
I have seen evidence, though, that many sellers are not receiving a fair price for the equity that they have worked so hard to build over several decades. If you are contemplating selling or merging, it is important that you not simply take the buyer’s word for how much your practice is worth. You need an impartial appraisal.
Of course, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in 750 words; but three basic yardsticks are essential for a practice appraisal:
• Tangible assets. Equipment, cash, accounts receivable and other property owned by the practice.
• Liabilities. Accounts payable, outstanding loans, and anything else owed to others.
• Intangible assets. Sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the equity, or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons why patients come back (if in fact they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferable. For example, unique skills with a laser, neurotoxins, or filler substances, or extraordinary personal charisma, may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash Flow Analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of Earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline Comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings (and thus its overall value) are.
Asset-based valuation is the most popular, but by no means the only method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not its income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll cover some sale and merger options that you may not have thought of next month.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
Over the last couple of years, I’ve written quite a lot about the trend toward consolidation. That trend shows no sign of abating; more and more soloists and small groups are selling or merging their practices with hospitals, multispecialty groups, or other large entities.
I have seen evidence, though, that many sellers are not receiving a fair price for the equity that they have worked so hard to build over several decades. If you are contemplating selling or merging, it is important that you not simply take the buyer’s word for how much your practice is worth. You need an impartial appraisal.
Of course, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in 750 words; but three basic yardsticks are essential for a practice appraisal:
• Tangible assets. Equipment, cash, accounts receivable and other property owned by the practice.
• Liabilities. Accounts payable, outstanding loans, and anything else owed to others.
• Intangible assets. Sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the equity, or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons why patients come back (if in fact they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferable. For example, unique skills with a laser, neurotoxins, or filler substances, or extraordinary personal charisma, may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash Flow Analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of Earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline Comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings (and thus its overall value) are.
Asset-based valuation is the most popular, but by no means the only method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not its income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll cover some sale and merger options that you may not have thought of next month.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.

Delayed diagnosis tops breast cancer malpractice claims
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.

“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
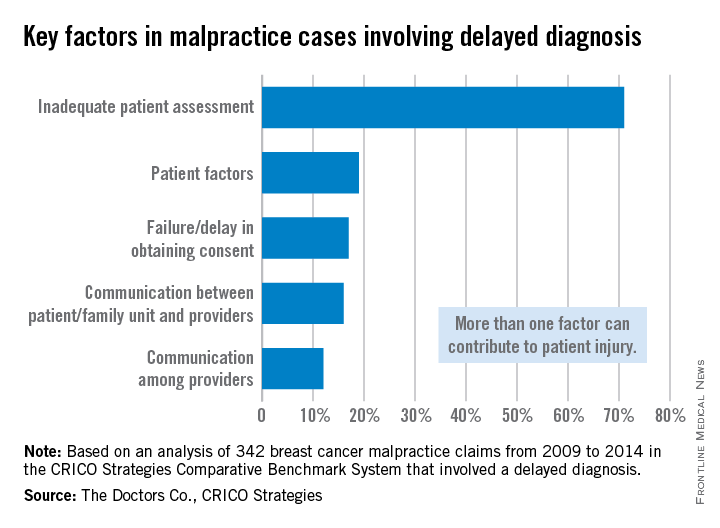
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med

Responding to online physician review sites
Recently, Niam Yaraghi of the Brookings Institution caused quite a kerfuffle regarding the validity of online doctor reviews in a U.S. News and World Report op-ed piece titled, “Don’t Yelp Your Doctor.”
In it, he argues that customers are “generally qualified and capable” of reviewing a restaurant – anyone can tell if a steak is chewy or a server is rude, he says. (Of course, chefs may disagree.) Yet, when it comes to online physician reviews, Mr. Yaraghi argues that “patients are neither qualified nor capable of evaluating the quality of the medical services that they receive.” I can see many of you nodding in vigorous agreement with that last sentence.
Who among us hasn’t felt indignant after reading a negative online review? Particularly one that criticizes our office decor or billing, yet makes no mention of our expert clinical abilities? But here’s my advice. Have your moment of indignation, then start working on improving your online reputation, which may improve your actual practice as well.
Here are a few tips for optimizing online physician review sites:
• Google yourself and your practice to see which sites your patients are commonly using.
• Set up a Google Alert at https://www.google.com/alerts. Google Alerts are email updates that you receive based on your queries. Include your name and the name of your practice. This way, you’ll receive notice when you’re mentioned online.
• According to SoftwareAdvice.com, the most trusted review sites in descending order are: Yelp and Healthgrades (tied), RateMDs, Vitals, ZocDoc, and others. So familiarize yourself with these sites.
• Claim your page on review sites. Be sure all of the information listed is updated and correct.
• Upload a professional photo of yourself. It’s much more effective to see a picture of you than an empty avatar.
• Be sure someone in your office is responsible for responding to comments online, particularly negative ones. It’s best to respond promptly rather than have it linger without a response for weeks. If you don’t write it, then at least approve it before it is posted.
• Respond to both positive and negative comments. Yelp, for instance, rewards business owners who maintain their site and actively respond to comments.
• For specific tips on how to respond to negative online reviews, see my column from July 2013 titled “How to handle negative reviews.”
When it comes to online physician reviews, I want you to remember a few things:
• Physician reviews are usually favorable.
• Negative reviews are sometimes opportunities to improve your service.
• In the long run, we should want more, not fewer, reviews. Which would you rather have, two negative reviews, or two negative reviews and eight positive ones?
• The more reviews you have, the more credible you appear to prospective patients. This is particularly true for cosmetic practices.
• Patients are more likely to leave a positive review when they see other positive reviews posted about you.
Let’s delve more deeply into the second point, “Negative reviews are opportunities for you and your staff to improve your service.”
According to the 2014 “IndustryView report” from Software Advice, when it came to administrative issues such as wait times, billing, and staff friendliness, 25% of respondents cited wait times as the most important factor in their experience. Moreover, their 2013 report found that 41% of patients said they would consider switching doctors if it reduced their wait times
We live in a consumer-centric society and service matters. For most patients, service equals quality. If you’ve got multiple negative reviews regarding your front desk staff, for instance, then address it directly with them. If you’ve got complaints about long wait times, then consider ways to improve it or improve the patient’s experience of waiting. You might hire a consultant to help with reducing wait times or you might provide Wi-Fi or light refreshments in your waiting room to make the wait more pleasant.
Let’s return to Mr. Yaraghi’s contention that patients are unqualified to accurately assess our abilities. It is a moot discussion. Patients have, and will continue, evaluating us regardless of how qualified they are to do so. A restaurant patron may not be an expert of sous-vide cooking but can judge his or her experience of the meal and restaurant staff. Similarly, a patient may not be an expert in psoriasis, but he or she can accurately assess an experience in our office and with our staff.
The good news is that there are sites that are trying to incorporate more objective data in the reviews. For instance, Healthgrades lists doctors’ board certifications, hospital affiliations, conditions treated, and procedures performed. The hope is that more objective criteria will improve the quality of the reviews and make the occasional angry and unwarranted rant less important.
One thing is for sure, there is much more discussion to come.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Recently, Niam Yaraghi of the Brookings Institution caused quite a kerfuffle regarding the validity of online doctor reviews in a U.S. News and World Report op-ed piece titled, “Don’t Yelp Your Doctor.”
In it, he argues that customers are “generally qualified and capable” of reviewing a restaurant – anyone can tell if a steak is chewy or a server is rude, he says. (Of course, chefs may disagree.) Yet, when it comes to online physician reviews, Mr. Yaraghi argues that “patients are neither qualified nor capable of evaluating the quality of the medical services that they receive.” I can see many of you nodding in vigorous agreement with that last sentence.
Who among us hasn’t felt indignant after reading a negative online review? Particularly one that criticizes our office decor or billing, yet makes no mention of our expert clinical abilities? But here’s my advice. Have your moment of indignation, then start working on improving your online reputation, which may improve your actual practice as well.
Here are a few tips for optimizing online physician review sites:
• Google yourself and your practice to see which sites your patients are commonly using.
• Set up a Google Alert at https://www.google.com/alerts. Google Alerts are email updates that you receive based on your queries. Include your name and the name of your practice. This way, you’ll receive notice when you’re mentioned online.
• According to SoftwareAdvice.com, the most trusted review sites in descending order are: Yelp and Healthgrades (tied), RateMDs, Vitals, ZocDoc, and others. So familiarize yourself with these sites.
• Claim your page on review sites. Be sure all of the information listed is updated and correct.
• Upload a professional photo of yourself. It’s much more effective to see a picture of you than an empty avatar.
• Be sure someone in your office is responsible for responding to comments online, particularly negative ones. It’s best to respond promptly rather than have it linger without a response for weeks. If you don’t write it, then at least approve it before it is posted.
• Respond to both positive and negative comments. Yelp, for instance, rewards business owners who maintain their site and actively respond to comments.
• For specific tips on how to respond to negative online reviews, see my column from July 2013 titled “How to handle negative reviews.”
When it comes to online physician reviews, I want you to remember a few things:
• Physician reviews are usually favorable.
• Negative reviews are sometimes opportunities to improve your service.
• In the long run, we should want more, not fewer, reviews. Which would you rather have, two negative reviews, or two negative reviews and eight positive ones?
• The more reviews you have, the more credible you appear to prospective patients. This is particularly true for cosmetic practices.
• Patients are more likely to leave a positive review when they see other positive reviews posted about you.
Let’s delve more deeply into the second point, “Negative reviews are opportunities for you and your staff to improve your service.”
According to the 2014 “IndustryView report” from Software Advice, when it came to administrative issues such as wait times, billing, and staff friendliness, 25% of respondents cited wait times as the most important factor in their experience. Moreover, their 2013 report found that 41% of patients said they would consider switching doctors if it reduced their wait times
We live in a consumer-centric society and service matters. For most patients, service equals quality. If you’ve got multiple negative reviews regarding your front desk staff, for instance, then address it directly with them. If you’ve got complaints about long wait times, then consider ways to improve it or improve the patient’s experience of waiting. You might hire a consultant to help with reducing wait times or you might provide Wi-Fi or light refreshments in your waiting room to make the wait more pleasant.
Let’s return to Mr. Yaraghi’s contention that patients are unqualified to accurately assess our abilities. It is a moot discussion. Patients have, and will continue, evaluating us regardless of how qualified they are to do so. A restaurant patron may not be an expert of sous-vide cooking but can judge his or her experience of the meal and restaurant staff. Similarly, a patient may not be an expert in psoriasis, but he or she can accurately assess an experience in our office and with our staff.
The good news is that there are sites that are trying to incorporate more objective data in the reviews. For instance, Healthgrades lists doctors’ board certifications, hospital affiliations, conditions treated, and procedures performed. The hope is that more objective criteria will improve the quality of the reviews and make the occasional angry and unwarranted rant less important.
One thing is for sure, there is much more discussion to come.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Recently, Niam Yaraghi of the Brookings Institution caused quite a kerfuffle regarding the validity of online doctor reviews in a U.S. News and World Report op-ed piece titled, “Don’t Yelp Your Doctor.”
In it, he argues that customers are “generally qualified and capable” of reviewing a restaurant – anyone can tell if a steak is chewy or a server is rude, he says. (Of course, chefs may disagree.) Yet, when it comes to online physician reviews, Mr. Yaraghi argues that “patients are neither qualified nor capable of evaluating the quality of the medical services that they receive.” I can see many of you nodding in vigorous agreement with that last sentence.
Who among us hasn’t felt indignant after reading a negative online review? Particularly one that criticizes our office decor or billing, yet makes no mention of our expert clinical abilities? But here’s my advice. Have your moment of indignation, then start working on improving your online reputation, which may improve your actual practice as well.
Here are a few tips for optimizing online physician review sites:
• Google yourself and your practice to see which sites your patients are commonly using.
• Set up a Google Alert at https://www.google.com/alerts. Google Alerts are email updates that you receive based on your queries. Include your name and the name of your practice. This way, you’ll receive notice when you’re mentioned online.
• According to SoftwareAdvice.com, the most trusted review sites in descending order are: Yelp and Healthgrades (tied), RateMDs, Vitals, ZocDoc, and others. So familiarize yourself with these sites.
• Claim your page on review sites. Be sure all of the information listed is updated and correct.
• Upload a professional photo of yourself. It’s much more effective to see a picture of you than an empty avatar.
• Be sure someone in your office is responsible for responding to comments online, particularly negative ones. It’s best to respond promptly rather than have it linger without a response for weeks. If you don’t write it, then at least approve it before it is posted.
• Respond to both positive and negative comments. Yelp, for instance, rewards business owners who maintain their site and actively respond to comments.
• For specific tips on how to respond to negative online reviews, see my column from July 2013 titled “How to handle negative reviews.”
When it comes to online physician reviews, I want you to remember a few things:
• Physician reviews are usually favorable.
• Negative reviews are sometimes opportunities to improve your service.
• In the long run, we should want more, not fewer, reviews. Which would you rather have, two negative reviews, or two negative reviews and eight positive ones?
• The more reviews you have, the more credible you appear to prospective patients. This is particularly true for cosmetic practices.
• Patients are more likely to leave a positive review when they see other positive reviews posted about you.
Let’s delve more deeply into the second point, “Negative reviews are opportunities for you and your staff to improve your service.”
According to the 2014 “IndustryView report” from Software Advice, when it came to administrative issues such as wait times, billing, and staff friendliness, 25% of respondents cited wait times as the most important factor in their experience. Moreover, their 2013 report found that 41% of patients said they would consider switching doctors if it reduced their wait times
We live in a consumer-centric society and service matters. For most patients, service equals quality. If you’ve got multiple negative reviews regarding your front desk staff, for instance, then address it directly with them. If you’ve got complaints about long wait times, then consider ways to improve it or improve the patient’s experience of waiting. You might hire a consultant to help with reducing wait times or you might provide Wi-Fi or light refreshments in your waiting room to make the wait more pleasant.
Let’s return to Mr. Yaraghi’s contention that patients are unqualified to accurately assess our abilities. It is a moot discussion. Patients have, and will continue, evaluating us regardless of how qualified they are to do so. A restaurant patron may not be an expert of sous-vide cooking but can judge his or her experience of the meal and restaurant staff. Similarly, a patient may not be an expert in psoriasis, but he or she can accurately assess an experience in our office and with our staff.
The good news is that there are sites that are trying to incorporate more objective data in the reviews. For instance, Healthgrades lists doctors’ board certifications, hospital affiliations, conditions treated, and procedures performed. The hope is that more objective criteria will improve the quality of the reviews and make the occasional angry and unwarranted rant less important.
One thing is for sure, there is much more discussion to come.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
