User login
Official Newspaper of the American College of Surgeons
VIDEO: Novel imaging technique helps hunt for pulmonary lesions
PHOENIX – Each year more than 250,000 patients present with ground-glass opacities and other solitary pulmonary nodules, and they are difficult to locate.
“There’s been a need for our field to develop new technologies to find these nodules in the OR,” Dr. Sunil Singhal said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “The fallback plan has always been that we can make a thoracotomy. Some studies have shown that in about one out of every two cases you end up opening a patient just to find a tiny little nodule.”
Dr. Singhal of the division of cardiothoracic surgery at the University of Pennsylvania School of Medicine, Philadelphia, discussed preoperative and intraoperative localization methods, including an investigational technology in which patients receive an intravascular dye that localizes the pulmonary tumor. “When we put our video-assisted thoracoscopic surgery camera in, the tumors are glowing,” he said. “We can then do a localized wedge excision and confirm margins of the staple line. We’ve done this [in] about 80 patients, and it’s been non-toxic, very safe, and very effective. Our biggest limitation has been our depth of penetration.”
Dr. Singhal reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – Each year more than 250,000 patients present with ground-glass opacities and other solitary pulmonary nodules, and they are difficult to locate.
“There’s been a need for our field to develop new technologies to find these nodules in the OR,” Dr. Sunil Singhal said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “The fallback plan has always been that we can make a thoracotomy. Some studies have shown that in about one out of every two cases you end up opening a patient just to find a tiny little nodule.”
Dr. Singhal of the division of cardiothoracic surgery at the University of Pennsylvania School of Medicine, Philadelphia, discussed preoperative and intraoperative localization methods, including an investigational technology in which patients receive an intravascular dye that localizes the pulmonary tumor. “When we put our video-assisted thoracoscopic surgery camera in, the tumors are glowing,” he said. “We can then do a localized wedge excision and confirm margins of the staple line. We’ve done this [in] about 80 patients, and it’s been non-toxic, very safe, and very effective. Our biggest limitation has been our depth of penetration.”
Dr. Singhal reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – Each year more than 250,000 patients present with ground-glass opacities and other solitary pulmonary nodules, and they are difficult to locate.
“There’s been a need for our field to develop new technologies to find these nodules in the OR,” Dr. Sunil Singhal said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “The fallback plan has always been that we can make a thoracotomy. Some studies have shown that in about one out of every two cases you end up opening a patient just to find a tiny little nodule.”
Dr. Singhal of the division of cardiothoracic surgery at the University of Pennsylvania School of Medicine, Philadelphia, discussed preoperative and intraoperative localization methods, including an investigational technology in which patients receive an intravascular dye that localizes the pulmonary tumor. “When we put our video-assisted thoracoscopic surgery camera in, the tumors are glowing,” he said. “We can then do a localized wedge excision and confirm margins of the staple line. We’ve done this [in] about 80 patients, and it’s been non-toxic, very safe, and very effective. Our biggest limitation has been our depth of penetration.”
Dr. Singhal reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE STS ANNUAL MEETING

VIDEO: One in five hospital patients get health care–acquired infection
PHOENIX – If you happen to believe that the impact of health care–acquired infections is insignificant, think again. According to Dr. Kevin W. Lobdell, health care–acquired infections (HAIs) cause more deaths each year in the United States than breast cancer, lung cancer, and AIDS combined.
“If you look at hospitalized patients, one in five will acquire a health care–acquired infection,” Dr. Lobdell of the Sanger Heart and Vascular Institute at Carolinas Health System, Charlotte, N.C., said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “With respect to length of stay, that goes from 5 days on average for a normal, uninfected patient, to 22 days if they’ve had an infection. The mortality rate can be as high as 6% in those people that have developed infections, so that in itself is an enormous burden.”
He went on to discuss the most common HAIs in the hospital setting and noted that combating them involves strategies that consider people, the environment, and technology. He predicted that in coming years clinicians will have a better “analytic capability to understand what we’ve done in the past and what correlates with success in the future, and then be able to implement and learn from that.”
Dr. Lobdell reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – If you happen to believe that the impact of health care–acquired infections is insignificant, think again. According to Dr. Kevin W. Lobdell, health care–acquired infections (HAIs) cause more deaths each year in the United States than breast cancer, lung cancer, and AIDS combined.
“If you look at hospitalized patients, one in five will acquire a health care–acquired infection,” Dr. Lobdell of the Sanger Heart and Vascular Institute at Carolinas Health System, Charlotte, N.C., said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “With respect to length of stay, that goes from 5 days on average for a normal, uninfected patient, to 22 days if they’ve had an infection. The mortality rate can be as high as 6% in those people that have developed infections, so that in itself is an enormous burden.”
He went on to discuss the most common HAIs in the hospital setting and noted that combating them involves strategies that consider people, the environment, and technology. He predicted that in coming years clinicians will have a better “analytic capability to understand what we’ve done in the past and what correlates with success in the future, and then be able to implement and learn from that.”
Dr. Lobdell reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – If you happen to believe that the impact of health care–acquired infections is insignificant, think again. According to Dr. Kevin W. Lobdell, health care–acquired infections (HAIs) cause more deaths each year in the United States than breast cancer, lung cancer, and AIDS combined.
“If you look at hospitalized patients, one in five will acquire a health care–acquired infection,” Dr. Lobdell of the Sanger Heart and Vascular Institute at Carolinas Health System, Charlotte, N.C., said in a video interview at the annual meeting of the Society of Thoracic Surgeons. “With respect to length of stay, that goes from 5 days on average for a normal, uninfected patient, to 22 days if they’ve had an infection. The mortality rate can be as high as 6% in those people that have developed infections, so that in itself is an enormous burden.”
He went on to discuss the most common HAIs in the hospital setting and noted that combating them involves strategies that consider people, the environment, and technology. He predicted that in coming years clinicians will have a better “analytic capability to understand what we’ve done in the past and what correlates with success in the future, and then be able to implement and learn from that.”
Dr. Lobdell reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE STS ANNUAL MEETING

STS: Score stratifies risks for isolated tricuspid valve surgery patients
PHOENIX – A team of cardiac surgeons has developed the first clinical risk score for predicting the risk that patients face for operative mortality and postsurgical major morbidity when undergoing isolated tricuspid valve repair or replacement.
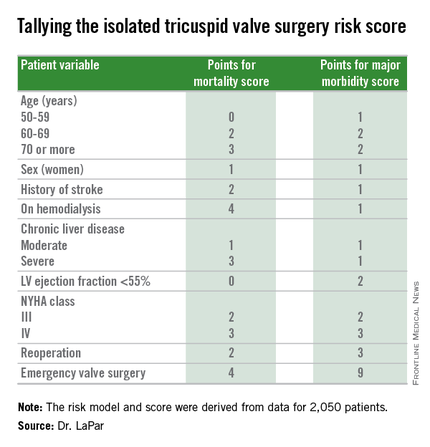
The risk score uses nine easily collected variables, and the derived model discriminates outcomes based on patients who score from 0-10 or more points on both a mortality and a morbidity risk scale, Dr. Damien J. LaPar said at the annual meeting of the Society of Thoracic Surgeons.

The risk scores allow surgeons to better describe and quantify to patients considering isolated tricuspid valve surgery the risks they face from the operation, and they have already been incorporated into practice at the University of Virginia, in Charlottesville, where Dr. LaPar practices.
“Patients love to better understand their risks. We can provide them with empirical data from a large, heterogeneous population that are better than a surgeon’s gut feeling” about the risks they face, said Dr. LaPar, a cardiothoracic surgeon at the University.
Another consequence of having the new risk model and score is that it identified certain key risk factors that are controllable, and thereby, “makes the case for early referrals” for isolated tricuspid valve surgery, Dr. LaPar said in an interview. For example, the risk score shows that patients who are older, on hemodialysis, have a reduced left ventricular ejection fraction, or require emergency intervention all contribute to worse outcomes, compared with patients who are younger, have better renal function, better cardiac output, or can be treated on a more routine basis.
Many physicians have viewed isolated tricuspid valve surgery as posing similar risks to all patients, with an overall average operative mortality rate of about 10%, he noted. The new risk score model shows that some patients who are younger and healthier have operative mortality rates below 5%, while older and sicker patients have rates that can surpass 20%.
“Our data show a spectrum of risk, and that it is better to operate sooner than later. That is the huge clinical message of these data,” Dr. LaPar said.
Designated discussant Dr. Michael A. Acker noted that the risk score for tricuspid-valve surgery “is a first of its kind and a major contribution.” Dr. Acker is professor of surgery and chief of cardiovascular surgery at the University of Pennsylvania in Philadelphia. He is a consultant to Thoratec and HeartWare.
Dr. LaPar and his associates derived the risk model and score from data collected on 2,050 patients who underwent isolated tricuspid valve repair or replacement at 49 hospitals in Virginia or Michigan during 2002-2014. The data came from databases maintained by the Virginia Cardiac Surgery Quality Initiative and by the Michigan Society of Thoracic & Cardiovascular Surgeons, and reported to the Adult Cardiac Surgery Database of the Society of Thoracic Surgeons. The model they developed showed operative mortality rates that ranged from 2%, for patients with a mortality score of zero, to 34% for patients with a score of 10 or more. It further showed major morbidity rates of 13%, for patients with a morbidity score of zero, to 71% for those with a score of 10 or more. Scoring for mortality uses a slightly different system than the scoring for morbidity, so the scores must be calculated individually, and the score totals for a patient can differ for each endpoint. The maximum score is 22 for mortality and 23 for morbidity.
Only 5%-15% of patients undergoing tricuspid valve surgery have an isolated procedure, so a relatively limited number of patients fall into this category, a fact that has in the past limited collection of data from large numbers of patients. The dataset used for this analysis, with 2,050 patients “is one of the largest series collected,” and made possible derivation of a robust risk model and scoring system. Future analysis of even more patients should further improve the model and scoring system.
“These data set the stage for looking at national-level data to further refine the model and make it even more generalizable,” Dr. LaPar said.
On Twitter @mitchelzoler
PHOENIX – A team of cardiac surgeons has developed the first clinical risk score for predicting the risk that patients face for operative mortality and postsurgical major morbidity when undergoing isolated tricuspid valve repair or replacement.
The risk score uses nine easily collected variables, and the derived model discriminates outcomes based on patients who score from 0-10 or more points on both a mortality and a morbidity risk scale, Dr. Damien J. LaPar said at the annual meeting of the Society of Thoracic Surgeons.
The risk scores allow surgeons to better describe and quantify to patients considering isolated tricuspid valve surgery the risks they face from the operation, and they have already been incorporated into practice at the University of Virginia, in Charlottesville, where Dr. LaPar practices.
“Patients love to better understand their risks. We can provide them with empirical data from a large, heterogeneous population that are better than a surgeon’s gut feeling” about the risks they face, said Dr. LaPar, a cardiothoracic surgeon at the University.
Another consequence of having the new risk model and score is that it identified certain key risk factors that are controllable, and thereby, “makes the case for early referrals” for isolated tricuspid valve surgery, Dr. LaPar said in an interview. For example, the risk score shows that patients who are older, on hemodialysis, have a reduced left ventricular ejection fraction, or require emergency intervention all contribute to worse outcomes, compared with patients who are younger, have better renal function, better cardiac output, or can be treated on a more routine basis.
Many physicians have viewed isolated tricuspid valve surgery as posing similar risks to all patients, with an overall average operative mortality rate of about 10%, he noted. The new risk score model shows that some patients who are younger and healthier have operative mortality rates below 5%, while older and sicker patients have rates that can surpass 20%.
“Our data show a spectrum of risk, and that it is better to operate sooner than later. That is the huge clinical message of these data,” Dr. LaPar said.
Designated discussant Dr. Michael A. Acker noted that the risk score for tricuspid-valve surgery “is a first of its kind and a major contribution.” Dr. Acker is professor of surgery and chief of cardiovascular surgery at the University of Pennsylvania in Philadelphia. He is a consultant to Thoratec and HeartWare.
Dr. LaPar and his associates derived the risk model and score from data collected on 2,050 patients who underwent isolated tricuspid valve repair or replacement at 49 hospitals in Virginia or Michigan during 2002-2014. The data came from databases maintained by the Virginia Cardiac Surgery Quality Initiative and by the Michigan Society of Thoracic & Cardiovascular Surgeons, and reported to the Adult Cardiac Surgery Database of the Society of Thoracic Surgeons. The model they developed showed operative mortality rates that ranged from 2%, for patients with a mortality score of zero, to 34% for patients with a score of 10 or more. It further showed major morbidity rates of 13%, for patients with a morbidity score of zero, to 71% for those with a score of 10 or more. Scoring for mortality uses a slightly different system than the scoring for morbidity, so the scores must be calculated individually, and the score totals for a patient can differ for each endpoint. The maximum score is 22 for mortality and 23 for morbidity.
Only 5%-15% of patients undergoing tricuspid valve surgery have an isolated procedure, so a relatively limited number of patients fall into this category, a fact that has in the past limited collection of data from large numbers of patients. The dataset used for this analysis, with 2,050 patients “is one of the largest series collected,” and made possible derivation of a robust risk model and scoring system. Future analysis of even more patients should further improve the model and scoring system.
“These data set the stage for looking at national-level data to further refine the model and make it even more generalizable,” Dr. LaPar said.
On Twitter @mitchelzoler
PHOENIX – A team of cardiac surgeons has developed the first clinical risk score for predicting the risk that patients face for operative mortality and postsurgical major morbidity when undergoing isolated tricuspid valve repair or replacement.
The risk score uses nine easily collected variables, and the derived model discriminates outcomes based on patients who score from 0-10 or more points on both a mortality and a morbidity risk scale, Dr. Damien J. LaPar said at the annual meeting of the Society of Thoracic Surgeons.
The risk scores allow surgeons to better describe and quantify to patients considering isolated tricuspid valve surgery the risks they face from the operation, and they have already been incorporated into practice at the University of Virginia, in Charlottesville, where Dr. LaPar practices.
“Patients love to better understand their risks. We can provide them with empirical data from a large, heterogeneous population that are better than a surgeon’s gut feeling” about the risks they face, said Dr. LaPar, a cardiothoracic surgeon at the University.
Another consequence of having the new risk model and score is that it identified certain key risk factors that are controllable, and thereby, “makes the case for early referrals” for isolated tricuspid valve surgery, Dr. LaPar said in an interview. For example, the risk score shows that patients who are older, on hemodialysis, have a reduced left ventricular ejection fraction, or require emergency intervention all contribute to worse outcomes, compared with patients who are younger, have better renal function, better cardiac output, or can be treated on a more routine basis.
Many physicians have viewed isolated tricuspid valve surgery as posing similar risks to all patients, with an overall average operative mortality rate of about 10%, he noted. The new risk score model shows that some patients who are younger and healthier have operative mortality rates below 5%, while older and sicker patients have rates that can surpass 20%.
“Our data show a spectrum of risk, and that it is better to operate sooner than later. That is the huge clinical message of these data,” Dr. LaPar said.
Designated discussant Dr. Michael A. Acker noted that the risk score for tricuspid-valve surgery “is a first of its kind and a major contribution.” Dr. Acker is professor of surgery and chief of cardiovascular surgery at the University of Pennsylvania in Philadelphia. He is a consultant to Thoratec and HeartWare.
Dr. LaPar and his associates derived the risk model and score from data collected on 2,050 patients who underwent isolated tricuspid valve repair or replacement at 49 hospitals in Virginia or Michigan during 2002-2014. The data came from databases maintained by the Virginia Cardiac Surgery Quality Initiative and by the Michigan Society of Thoracic & Cardiovascular Surgeons, and reported to the Adult Cardiac Surgery Database of the Society of Thoracic Surgeons. The model they developed showed operative mortality rates that ranged from 2%, for patients with a mortality score of zero, to 34% for patients with a score of 10 or more. It further showed major morbidity rates of 13%, for patients with a morbidity score of zero, to 71% for those with a score of 10 or more. Scoring for mortality uses a slightly different system than the scoring for morbidity, so the scores must be calculated individually, and the score totals for a patient can differ for each endpoint. The maximum score is 22 for mortality and 23 for morbidity.
Only 5%-15% of patients undergoing tricuspid valve surgery have an isolated procedure, so a relatively limited number of patients fall into this category, a fact that has in the past limited collection of data from large numbers of patients. The dataset used for this analysis, with 2,050 patients “is one of the largest series collected,” and made possible derivation of a robust risk model and scoring system. Future analysis of even more patients should further improve the model and scoring system.
“These data set the stage for looking at national-level data to further refine the model and make it even more generalizable,” Dr. LaPar said.
On Twitter @mitchelzoler
AT THE STS ANNUAL MEETING
Key clinical point: A risk-scoring system estimates a patient’s mortality and morbidity risk when undergoing isolated tricuspid valve surgery.
Major finding: The scoring system discriminated mortality risk from 2% to 34%, and major morbidity risk from 13% to 71%.
Data source: Analysis of 2,050 patients who underwent isolated tricuspid valve surgery in the STS Adult Cardiac Surgery Database.
Disclosures: Dr. LaPar had no disclosures.

DEA’s rescheduling of hydrocodone tied to declines in prescribing
Prescriptions for hydrocodone analgesics abruptly and markedly declined after the U.S. Drug Enforcement Administration reclassified them from schedule III to the more restrictive schedule II of the Controlled Substances Act, according to a research letter to the editor published online in JAMA Internal Medicine Jan. 25.
Hydrocodone, usually formulated in combination with nonopioid analgesics, is one of the most frequently abused opioids, accounting for nearly 100,000 abuse-related emergency department visits during one recent year. In October 2014, the DEA rescheduled these agents to subject them to more rigorous control, said Christopher M. Jones, Pharm.D., MPH, of the Department of Health and Human Services, Washington, and his associates.

To assess any effect this rescheduling had on prescribing patterns, the investigators analyzed information in the IMS Health National Prescription Audit, a database that captures nearly 80% of all prescriptions dispensed from U.S. pharmacies, focusing on the 3 years before and the 1 year after rescheduling. They also analyzed information in an American Medical Association database to assess prescribing of hydrocodone combination agents across medical specialties during the year after rescheduling.
Prescriptions for hydrocodone combination agents decreased by 22% after rescheduling, and those for hydrocodone combination tablets decreased by 16%. There were 26.3 million fewer prescriptions for hydrocodone combination products, and 1.1 billion fewer hydrocodone combination tablets in the year after rescheduling.
Most of this decline (74%) was attributable to a profound reduction in refills, which is “consistent with the prohibition on prescription refills for schedule II medications,” Dr. Jones and his associates said (JAMA Intern Med. 2016 Jan 25. doi: 10.1001/jamainternmed.2015.7799).
In contrast, prescriptions for nonhydrocodone combination opioid analgesics increased by 5%, and those for nonhydrocodone tablets by 1%, during the year after rescheduling.
The reductions in prescribing occurred across most medical specialties. Surgeons and primary care physicians accounted for the largest decreases in both hydrocodone-containing prescriptions (-38.4% and -22.9%, respectively) and tablets (-30.8% and -17.1%, respectively). Oncologists, emergency medicine specialists, and nurse practitioners and physician assistants also contributed heavily to the declines. Dentists and physical/rehabilitation/occupational medicine specialists accounted for smaller reductions.
In contrast, pain medicine specialists showed modest increases in prescriptions for hydrocodone combination products and tablets.
“Future research should examine whether these changes are sustained, have had an effect on access for patients, and are associated with the desired goals of reduced abuse, addiction, and overdose,” Dr. Jones and his associates noted.
This study was funded by the U.S. Food and Drug Administration. Dr. Jones and his associates reported having no relevant financial disclosures.
Prescriptions for hydrocodone analgesics abruptly and markedly declined after the U.S. Drug Enforcement Administration reclassified them from schedule III to the more restrictive schedule II of the Controlled Substances Act, according to a research letter to the editor published online in JAMA Internal Medicine Jan. 25.
Hydrocodone, usually formulated in combination with nonopioid analgesics, is one of the most frequently abused opioids, accounting for nearly 100,000 abuse-related emergency department visits during one recent year. In October 2014, the DEA rescheduled these agents to subject them to more rigorous control, said Christopher M. Jones, Pharm.D., MPH, of the Department of Health and Human Services, Washington, and his associates.
To assess any effect this rescheduling had on prescribing patterns, the investigators analyzed information in the IMS Health National Prescription Audit, a database that captures nearly 80% of all prescriptions dispensed from U.S. pharmacies, focusing on the 3 years before and the 1 year after rescheduling. They also analyzed information in an American Medical Association database to assess prescribing of hydrocodone combination agents across medical specialties during the year after rescheduling.
Prescriptions for hydrocodone combination agents decreased by 22% after rescheduling, and those for hydrocodone combination tablets decreased by 16%. There were 26.3 million fewer prescriptions for hydrocodone combination products, and 1.1 billion fewer hydrocodone combination tablets in the year after rescheduling.
Most of this decline (74%) was attributable to a profound reduction in refills, which is “consistent with the prohibition on prescription refills for schedule II medications,” Dr. Jones and his associates said (JAMA Intern Med. 2016 Jan 25. doi: 10.1001/jamainternmed.2015.7799).
In contrast, prescriptions for nonhydrocodone combination opioid analgesics increased by 5%, and those for nonhydrocodone tablets by 1%, during the year after rescheduling.
The reductions in prescribing occurred across most medical specialties. Surgeons and primary care physicians accounted for the largest decreases in both hydrocodone-containing prescriptions (-38.4% and -22.9%, respectively) and tablets (-30.8% and -17.1%, respectively). Oncologists, emergency medicine specialists, and nurse practitioners and physician assistants also contributed heavily to the declines. Dentists and physical/rehabilitation/occupational medicine specialists accounted for smaller reductions.
In contrast, pain medicine specialists showed modest increases in prescriptions for hydrocodone combination products and tablets.
“Future research should examine whether these changes are sustained, have had an effect on access for patients, and are associated with the desired goals of reduced abuse, addiction, and overdose,” Dr. Jones and his associates noted.
This study was funded by the U.S. Food and Drug Administration. Dr. Jones and his associates reported having no relevant financial disclosures.
Prescriptions for hydrocodone analgesics abruptly and markedly declined after the U.S. Drug Enforcement Administration reclassified them from schedule III to the more restrictive schedule II of the Controlled Substances Act, according to a research letter to the editor published online in JAMA Internal Medicine Jan. 25.
Hydrocodone, usually formulated in combination with nonopioid analgesics, is one of the most frequently abused opioids, accounting for nearly 100,000 abuse-related emergency department visits during one recent year. In October 2014, the DEA rescheduled these agents to subject them to more rigorous control, said Christopher M. Jones, Pharm.D., MPH, of the Department of Health and Human Services, Washington, and his associates.
To assess any effect this rescheduling had on prescribing patterns, the investigators analyzed information in the IMS Health National Prescription Audit, a database that captures nearly 80% of all prescriptions dispensed from U.S. pharmacies, focusing on the 3 years before and the 1 year after rescheduling. They also analyzed information in an American Medical Association database to assess prescribing of hydrocodone combination agents across medical specialties during the year after rescheduling.
Prescriptions for hydrocodone combination agents decreased by 22% after rescheduling, and those for hydrocodone combination tablets decreased by 16%. There were 26.3 million fewer prescriptions for hydrocodone combination products, and 1.1 billion fewer hydrocodone combination tablets in the year after rescheduling.
Most of this decline (74%) was attributable to a profound reduction in refills, which is “consistent with the prohibition on prescription refills for schedule II medications,” Dr. Jones and his associates said (JAMA Intern Med. 2016 Jan 25. doi: 10.1001/jamainternmed.2015.7799).
In contrast, prescriptions for nonhydrocodone combination opioid analgesics increased by 5%, and those for nonhydrocodone tablets by 1%, during the year after rescheduling.
The reductions in prescribing occurred across most medical specialties. Surgeons and primary care physicians accounted for the largest decreases in both hydrocodone-containing prescriptions (-38.4% and -22.9%, respectively) and tablets (-30.8% and -17.1%, respectively). Oncologists, emergency medicine specialists, and nurse practitioners and physician assistants also contributed heavily to the declines. Dentists and physical/rehabilitation/occupational medicine specialists accounted for smaller reductions.
In contrast, pain medicine specialists showed modest increases in prescriptions for hydrocodone combination products and tablets.
“Future research should examine whether these changes are sustained, have had an effect on access for patients, and are associated with the desired goals of reduced abuse, addiction, and overdose,” Dr. Jones and his associates noted.
This study was funded by the U.S. Food and Drug Administration. Dr. Jones and his associates reported having no relevant financial disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: The DEA’s reclassifying of hydrocodone analgesics from schedule III to the more restrictive schedule II produced an abrupt and marked decline in prescriptions.
Major finding: There were 26.3 million fewer prescriptions for hydrocodone combination products and 1.1 billion fewer prescriptions for hydrocodone combination tablets in the year after rescheduling.
Data source: An analysis of a nationally representative prescription database during the 3 years before and the 1 year after the DEA rescheduled hydrocodone.
Disclosures: This study was funded by the U.S. Food and Drug Administration. Dr. Jones and his associates reported having no relevant financial disclosures.

VIDEO: Preventing healthcare acquired infections after CT surgery
PHOENIX – More and more attention is being paid to preventing healthcare acquired infections (HAIs) in the hospital setting, and the role of HAIs in cardiothoracic surgery is a particlularly important area of focus.
“The good news is that cardiothoracic surgeons are really good at preventing infections. There’s been a lot of pressure over the past many years to report infections after cardiothoracic surgery, and so they’ve gotten a lot of things right,” Dr. Emily Landon said in a video interview at the annual meeting of the Society of Thoracic Surgeons.
“However, patients that undergo cardiothoracic surgery are still at risk of the infections that plague everyone in hospitals ... all of these are a problem based on whatever the hospital’s current situation is.”
Dr. Landon, who is the medical director of antimicrobial stewardship and infection control at University of Chicago Medicine, Chicago, discussed how cardiothroacic surgeons can maintain their own good outcomes and how they can have a postive impact outside the OR on protecting their patients after surgery.
Dr. Landon reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – More and more attention is being paid to preventing healthcare acquired infections (HAIs) in the hospital setting, and the role of HAIs in cardiothoracic surgery is a particlularly important area of focus.
“The good news is that cardiothoracic surgeons are really good at preventing infections. There’s been a lot of pressure over the past many years to report infections after cardiothoracic surgery, and so they’ve gotten a lot of things right,” Dr. Emily Landon said in a video interview at the annual meeting of the Society of Thoracic Surgeons.
“However, patients that undergo cardiothoracic surgery are still at risk of the infections that plague everyone in hospitals ... all of these are a problem based on whatever the hospital’s current situation is.”
Dr. Landon, who is the medical director of antimicrobial stewardship and infection control at University of Chicago Medicine, Chicago, discussed how cardiothroacic surgeons can maintain their own good outcomes and how they can have a postive impact outside the OR on protecting their patients after surgery.
Dr. Landon reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – More and more attention is being paid to preventing healthcare acquired infections (HAIs) in the hospital setting, and the role of HAIs in cardiothoracic surgery is a particlularly important area of focus.
“The good news is that cardiothoracic surgeons are really good at preventing infections. There’s been a lot of pressure over the past many years to report infections after cardiothoracic surgery, and so they’ve gotten a lot of things right,” Dr. Emily Landon said in a video interview at the annual meeting of the Society of Thoracic Surgeons.
“However, patients that undergo cardiothoracic surgery are still at risk of the infections that plague everyone in hospitals ... all of these are a problem based on whatever the hospital’s current situation is.”
Dr. Landon, who is the medical director of antimicrobial stewardship and infection control at University of Chicago Medicine, Chicago, discussed how cardiothroacic surgeons can maintain their own good outcomes and how they can have a postive impact outside the OR on protecting their patients after surgery.
Dr. Landon reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE STS ANNUAL MEETING

STS: Hybrid thoracic suite leverages CT’s imaging sensitivity
PHOENIX – Using CT imaging to detect lung cancers in people at high risk for developing it has made it possible to find small tumors with substantially increased sensitivity than is possible with radiography, However, this approach has posed a new challenge to thoracic surgeons: How to visualize these nodules – subcentimeter and nonpalpable – for biopsy or for resection?
The answer may be the hybrid thoracic operating room developed by Dr. Kazuhiro Yasufuku and his associates at Toronto General Hospital, a novel surgical suite that he described at the annual meeting of the Society of Thoracic Surgeons.

Dr. Yasufuku and his team began using the hybrid operating room on an investigational basis in 2013 and have now done about 50 cases as part of several research protocols. The trials address the feasibility of resection, biopsy, and nodule localization, as well as whether the hybrid approach reduces the amount of radiation exposure to both patients and to the surgical team, he said. They plan to report some of their initial results later this year.
The Toronto group assembled the hybrid array of equipment into a single operating room that includes both a dual-source, dual-energy CT scanner and a robotic cone-beam CT scanner, equipment for minimally invasive procedures including video-assisted thoracoscopic and robotic surgery, and advanced endoscopic technology including endobronchial ultrasound and navigational bronchoscopy. “We use innovative methods that we already know about, but bring them all together” within a single space, Dr. Yasufuku explained. “Rather than having patients go to several locations, we can do everything at the same time in one room.”

Perhaps the most novel aspect of this operating room is inclusion of a robotic cone-beam CT scanner, which uses mobile, flat CT-imaging panels that overcome the limitations of a conventional, fixed CT scanner. “They scan the patient and then we can retract them and get them out of the way” to better facilitate surgery, he said in an interview.
“We do not have a culture in thoracic surgery of using imaging during surgery,” said Dr. Yasufuku, director of the interventional thoracic surgery program at the University of Toronto. Hybrid operating rooms using noninvasive or minimally invasive equipment and procedures have become commonplace for cardiovascular surgeons and cardiac interventionalists, but this approach has generally not yet been applied to thoracic surgery for cancer, in large part because of the imaging limitations, he said. “It is difficult to perform video-assisted thorascopic surgery using fixed CT.”
Bronchoscopic technologies provide additional, important tools for minimally invasive thoracic surgery. “We use the hybrid operating room to mark small [nonpalpable] lesions.” One approach to marking is to place a microcoil within the nodule with a percutaneous needle. Another approach is to tag the nodule with a fluorescent dye using navigational bronchoscopy.
Dr. Yasufuku also emphasized that the hybrid operating room will also be valuable when new, minimally invasive, nonsurgical therapeutic options for treatment of lung cancer become available in the near future.
Dr. Yasufuku said that he had no relevant disclosures.
On Twitter @mitchelzoler
PHOENIX – Using CT imaging to detect lung cancers in people at high risk for developing it has made it possible to find small tumors with substantially increased sensitivity than is possible with radiography, However, this approach has posed a new challenge to thoracic surgeons: How to visualize these nodules – subcentimeter and nonpalpable – for biopsy or for resection?
The answer may be the hybrid thoracic operating room developed by Dr. Kazuhiro Yasufuku and his associates at Toronto General Hospital, a novel surgical suite that he described at the annual meeting of the Society of Thoracic Surgeons.
Dr. Yasufuku and his team began using the hybrid operating room on an investigational basis in 2013 and have now done about 50 cases as part of several research protocols. The trials address the feasibility of resection, biopsy, and nodule localization, as well as whether the hybrid approach reduces the amount of radiation exposure to both patients and to the surgical team, he said. They plan to report some of their initial results later this year.
The Toronto group assembled the hybrid array of equipment into a single operating room that includes both a dual-source, dual-energy CT scanner and a robotic cone-beam CT scanner, equipment for minimally invasive procedures including video-assisted thoracoscopic and robotic surgery, and advanced endoscopic technology including endobronchial ultrasound and navigational bronchoscopy. “We use innovative methods that we already know about, but bring them all together” within a single space, Dr. Yasufuku explained. “Rather than having patients go to several locations, we can do everything at the same time in one room.”
Perhaps the most novel aspect of this operating room is inclusion of a robotic cone-beam CT scanner, which uses mobile, flat CT-imaging panels that overcome the limitations of a conventional, fixed CT scanner. “They scan the patient and then we can retract them and get them out of the way” to better facilitate surgery, he said in an interview.
“We do not have a culture in thoracic surgery of using imaging during surgery,” said Dr. Yasufuku, director of the interventional thoracic surgery program at the University of Toronto. Hybrid operating rooms using noninvasive or minimally invasive equipment and procedures have become commonplace for cardiovascular surgeons and cardiac interventionalists, but this approach has generally not yet been applied to thoracic surgery for cancer, in large part because of the imaging limitations, he said. “It is difficult to perform video-assisted thorascopic surgery using fixed CT.”
Bronchoscopic technologies provide additional, important tools for minimally invasive thoracic surgery. “We use the hybrid operating room to mark small [nonpalpable] lesions.” One approach to marking is to place a microcoil within the nodule with a percutaneous needle. Another approach is to tag the nodule with a fluorescent dye using navigational bronchoscopy.
Dr. Yasufuku also emphasized that the hybrid operating room will also be valuable when new, minimally invasive, nonsurgical therapeutic options for treatment of lung cancer become available in the near future.
Dr. Yasufuku said that he had no relevant disclosures.
On Twitter @mitchelzoler
PHOENIX – Using CT imaging to detect lung cancers in people at high risk for developing it has made it possible to find small tumors with substantially increased sensitivity than is possible with radiography, However, this approach has posed a new challenge to thoracic surgeons: How to visualize these nodules – subcentimeter and nonpalpable – for biopsy or for resection?
The answer may be the hybrid thoracic operating room developed by Dr. Kazuhiro Yasufuku and his associates at Toronto General Hospital, a novel surgical suite that he described at the annual meeting of the Society of Thoracic Surgeons.
Dr. Yasufuku and his team began using the hybrid operating room on an investigational basis in 2013 and have now done about 50 cases as part of several research protocols. The trials address the feasibility of resection, biopsy, and nodule localization, as well as whether the hybrid approach reduces the amount of radiation exposure to both patients and to the surgical team, he said. They plan to report some of their initial results later this year.
The Toronto group assembled the hybrid array of equipment into a single operating room that includes both a dual-source, dual-energy CT scanner and a robotic cone-beam CT scanner, equipment for minimally invasive procedures including video-assisted thoracoscopic and robotic surgery, and advanced endoscopic technology including endobronchial ultrasound and navigational bronchoscopy. “We use innovative methods that we already know about, but bring them all together” within a single space, Dr. Yasufuku explained. “Rather than having patients go to several locations, we can do everything at the same time in one room.”
Perhaps the most novel aspect of this operating room is inclusion of a robotic cone-beam CT scanner, which uses mobile, flat CT-imaging panels that overcome the limitations of a conventional, fixed CT scanner. “They scan the patient and then we can retract them and get them out of the way” to better facilitate surgery, he said in an interview.
“We do not have a culture in thoracic surgery of using imaging during surgery,” said Dr. Yasufuku, director of the interventional thoracic surgery program at the University of Toronto. Hybrid operating rooms using noninvasive or minimally invasive equipment and procedures have become commonplace for cardiovascular surgeons and cardiac interventionalists, but this approach has generally not yet been applied to thoracic surgery for cancer, in large part because of the imaging limitations, he said. “It is difficult to perform video-assisted thorascopic surgery using fixed CT.”
Bronchoscopic technologies provide additional, important tools for minimally invasive thoracic surgery. “We use the hybrid operating room to mark small [nonpalpable] lesions.” One approach to marking is to place a microcoil within the nodule with a percutaneous needle. Another approach is to tag the nodule with a fluorescent dye using navigational bronchoscopy.
Dr. Yasufuku also emphasized that the hybrid operating room will also be valuable when new, minimally invasive, nonsurgical therapeutic options for treatment of lung cancer become available in the near future.
Dr. Yasufuku said that he had no relevant disclosures.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE STS ANNUAL MEETING

VIDEO: Which lesions are best for bronchoscopic endoluminal treatment?
PHOENIX – According to Dr. Moishe Liberman, promising lesions for bronchoscopic endoluminal treatment include endobronchial lesions and intraluminal exophytic tumors within the trachea or main bronchus, provided that the distal airway lumen is visible and you can get past the tumor with a flexible endoscope.
“We always teach the fellows that if you get pus back when you’re trying to get around the tumor or play with the tumor, you’re usually going to have a very good result,” said Dr. Liberman, a thoracic surgeon who directs the endoscopic tracheo-bronchial and oesophageal center at the Centre hospitalier de l’Université de Montréal, Quebec, Canada. “If you play with the tumor and you get the tumor out and you get nothing back, usually the CT scan or the X-ray postoperatively is going to look just like it did preoperatively, even though endoscopically you might have a good result.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Central lesions are also excellent candidates for endoluminal therapy, he said in a video interview at the meeting. Distal lesions in the small bronchi “are candidates but are much more difficult and require more specialized tools. The shorter the lesion, the more likely you are to have good success.”
Available options for delivering energy endoscopically include electrocautery, argon plasma coagulation, laser, and cryotherapy. A disadvantage of all of the thermal modalities except for cryotherapy “include the potential for airway fire and you have to work with low FiO2s [fraction of inspired oxygen],” Dr. Liberman noted. “A lot of these patients need high FiO2s to saturate, so I think that’s always an issue. We never go on cardiopulmonary bypass to do these cases and we never cannulate patients to do these cases. You also have to worry about gas emboli, especially when you open up big vessels. These modalities can also cause inadvertent airway injury, delayed effects, and bronchoscope damage.”
In general, he continued, laser-tissue interactions depend on the power and the wavelength of the laser as well as the color and the water content of the target tissue. “The power density of the wavelength you choose determines its ability to cut, coagulate, or vaporize the tissue,” he said.
“As the power density increases, the laser fiber approaches the target tissue. Power density is more important than the energy delivered.”
The Nd:YAG (neodymium-doped yttrium aluminium garnet) laser, which causes more destruction in the deep tissue than on the surface, is the most common laser used in interventional airway procedures, he said. Two other commonly used lasers include the KTP (potassium titanyl phosphate) and the CO2. “I like CO2s a lot for upper airway and subglottic problems as well as vocal cord problems,” Dr. Liberman said. “It’s very precise and has low penetration. The Nd:YAG is very good for deep penetration. You need familiarity with these. I don’t think you can just take one of these off the shelf if you’ve never used it before. Sometimes your ENT [ear nose and throat] or urology colleagues can help you, because they’re using a lot more of these lasers than we are.”
Contraindications for laser bronchoscopy include operable lesions. Dr. Liberman said that while he and his associates use lasers in a preoperative setting, “we’re very careful not to damage proximal or distal airway when we know we’re going to do a sleeve resection or pneumonectomy.”
Other contraindications for laser bronchoscopy include patients with a poor short-term prognosis, severe coagulation disorder, extrinsic airway obstruction, tracheoesophageal fistula or T-Med fistula, those with extensive submucosal disease causing obstruction, and those with lesion adjacent to the esophagus or to a major vessel.
Dr. Liberman reported having received research grants from Ethicon, Boston Scientific, Olympus, Covidien, and Baxter.
PHOENIX – According to Dr. Moishe Liberman, promising lesions for bronchoscopic endoluminal treatment include endobronchial lesions and intraluminal exophytic tumors within the trachea or main bronchus, provided that the distal airway lumen is visible and you can get past the tumor with a flexible endoscope.
“We always teach the fellows that if you get pus back when you’re trying to get around the tumor or play with the tumor, you’re usually going to have a very good result,” said Dr. Liberman, a thoracic surgeon who directs the endoscopic tracheo-bronchial and oesophageal center at the Centre hospitalier de l’Université de Montréal, Quebec, Canada. “If you play with the tumor and you get the tumor out and you get nothing back, usually the CT scan or the X-ray postoperatively is going to look just like it did preoperatively, even though endoscopically you might have a good result.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Central lesions are also excellent candidates for endoluminal therapy, he said in a video interview at the meeting. Distal lesions in the small bronchi “are candidates but are much more difficult and require more specialized tools. The shorter the lesion, the more likely you are to have good success.”
Available options for delivering energy endoscopically include electrocautery, argon plasma coagulation, laser, and cryotherapy. A disadvantage of all of the thermal modalities except for cryotherapy “include the potential for airway fire and you have to work with low FiO2s [fraction of inspired oxygen],” Dr. Liberman noted. “A lot of these patients need high FiO2s to saturate, so I think that’s always an issue. We never go on cardiopulmonary bypass to do these cases and we never cannulate patients to do these cases. You also have to worry about gas emboli, especially when you open up big vessels. These modalities can also cause inadvertent airway injury, delayed effects, and bronchoscope damage.”
In general, he continued, laser-tissue interactions depend on the power and the wavelength of the laser as well as the color and the water content of the target tissue. “The power density of the wavelength you choose determines its ability to cut, coagulate, or vaporize the tissue,” he said.
“As the power density increases, the laser fiber approaches the target tissue. Power density is more important than the energy delivered.”
The Nd:YAG (neodymium-doped yttrium aluminium garnet) laser, which causes more destruction in the deep tissue than on the surface, is the most common laser used in interventional airway procedures, he said. Two other commonly used lasers include the KTP (potassium titanyl phosphate) and the CO2. “I like CO2s a lot for upper airway and subglottic problems as well as vocal cord problems,” Dr. Liberman said. “It’s very precise and has low penetration. The Nd:YAG is very good for deep penetration. You need familiarity with these. I don’t think you can just take one of these off the shelf if you’ve never used it before. Sometimes your ENT [ear nose and throat] or urology colleagues can help you, because they’re using a lot more of these lasers than we are.”
Contraindications for laser bronchoscopy include operable lesions. Dr. Liberman said that while he and his associates use lasers in a preoperative setting, “we’re very careful not to damage proximal or distal airway when we know we’re going to do a sleeve resection or pneumonectomy.”
Other contraindications for laser bronchoscopy include patients with a poor short-term prognosis, severe coagulation disorder, extrinsic airway obstruction, tracheoesophageal fistula or T-Med fistula, those with extensive submucosal disease causing obstruction, and those with lesion adjacent to the esophagus or to a major vessel.
Dr. Liberman reported having received research grants from Ethicon, Boston Scientific, Olympus, Covidien, and Baxter.
PHOENIX – According to Dr. Moishe Liberman, promising lesions for bronchoscopic endoluminal treatment include endobronchial lesions and intraluminal exophytic tumors within the trachea or main bronchus, provided that the distal airway lumen is visible and you can get past the tumor with a flexible endoscope.
“We always teach the fellows that if you get pus back when you’re trying to get around the tumor or play with the tumor, you’re usually going to have a very good result,” said Dr. Liberman, a thoracic surgeon who directs the endoscopic tracheo-bronchial and oesophageal center at the Centre hospitalier de l’Université de Montréal, Quebec, Canada. “If you play with the tumor and you get the tumor out and you get nothing back, usually the CT scan or the X-ray postoperatively is going to look just like it did preoperatively, even though endoscopically you might have a good result.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Central lesions are also excellent candidates for endoluminal therapy, he said in a video interview at the meeting. Distal lesions in the small bronchi “are candidates but are much more difficult and require more specialized tools. The shorter the lesion, the more likely you are to have good success.”
Available options for delivering energy endoscopically include electrocautery, argon plasma coagulation, laser, and cryotherapy. A disadvantage of all of the thermal modalities except for cryotherapy “include the potential for airway fire and you have to work with low FiO2s [fraction of inspired oxygen],” Dr. Liberman noted. “A lot of these patients need high FiO2s to saturate, so I think that’s always an issue. We never go on cardiopulmonary bypass to do these cases and we never cannulate patients to do these cases. You also have to worry about gas emboli, especially when you open up big vessels. These modalities can also cause inadvertent airway injury, delayed effects, and bronchoscope damage.”
In general, he continued, laser-tissue interactions depend on the power and the wavelength of the laser as well as the color and the water content of the target tissue. “The power density of the wavelength you choose determines its ability to cut, coagulate, or vaporize the tissue,” he said.
“As the power density increases, the laser fiber approaches the target tissue. Power density is more important than the energy delivered.”
The Nd:YAG (neodymium-doped yttrium aluminium garnet) laser, which causes more destruction in the deep tissue than on the surface, is the most common laser used in interventional airway procedures, he said. Two other commonly used lasers include the KTP (potassium titanyl phosphate) and the CO2. “I like CO2s a lot for upper airway and subglottic problems as well as vocal cord problems,” Dr. Liberman said. “It’s very precise and has low penetration. The Nd:YAG is very good for deep penetration. You need familiarity with these. I don’t think you can just take one of these off the shelf if you’ve never used it before. Sometimes your ENT [ear nose and throat] or urology colleagues can help you, because they’re using a lot more of these lasers than we are.”
Contraindications for laser bronchoscopy include operable lesions. Dr. Liberman said that while he and his associates use lasers in a preoperative setting, “we’re very careful not to damage proximal or distal airway when we know we’re going to do a sleeve resection or pneumonectomy.”
Other contraindications for laser bronchoscopy include patients with a poor short-term prognosis, severe coagulation disorder, extrinsic airway obstruction, tracheoesophageal fistula or T-Med fistula, those with extensive submucosal disease causing obstruction, and those with lesion adjacent to the esophagus or to a major vessel.
Dr. Liberman reported having received research grants from Ethicon, Boston Scientific, Olympus, Covidien, and Baxter.
EXPERT ANALYSIS FROM THE STS ANNUAL MEETING

Simple change increases forced-air warming use in trauma
SAN ANTONIO – A month-long quality improvement project to increase the use of forced-air warming blankets reduced mean hypothermia times in trauma patients at Parkland Memorial Hospital, Dallas, from 229 to 154 minutes.
All it took to get doctors, nurses, and staff to use the forced-air warming blankets more often was a reminder that hypothermia is an independent predictor of death in trauma, and data showing that Parkland, a Level 1 trauma center, used forced-air warming in just 11% of its hypothermic trauma patients. Meetings to get those points across were held in December 2014.

Forced-air warming jumped to 70% of hypothermic patients over the next 4 months in 2015 (P equal to or less than .0001), leading to the 33% drop in rewarming times (P = .009). The improvement came without any shift in the use of the rewarming methods trauma teams were in the habit of using: warm blankets, room air, and IV fluids.
Investigator Dr. Frank Zhao thinks it’s something all trauma centers can and should do. “There’s no reason that we shouldn’t recommend this be part of the rewarming protocol in every trauma center. It took about a month to roll this out so everyone was on the same page and was easily achieved,” said Dr. Zhao, formerly a Parkland surgery resident but now a trauma and surgical critical care fellow at the Oregon Health and Sciences University in Portland.
The blankets are an almost universal presence in operating rooms to keep core temperatures at least 36 degrees Celsius, but “from what I’ve seen at multiple institutions, the Bair Hugger is probably one of the least used warming methods” in trauma. “They’re recommended for trauma rewarming, but we [didn’t] use them very often.” Staff were not in the habit, he said at the Eastern Association for the Surgery of Trauma scientific assembly.
From July to November 2014, before the intervention, 15.2% (114) of Levels 1 and 2 trauma patients arrived at Parkland hypothermic, versus 20.9% (82) during the colder period of January-April 2015. Almost 80% of the trauma patients over that time were male, and the average patient age was about 40 years.
The investigators have no disclosures, and there was no outside funding for the project.
SAN ANTONIO – A month-long quality improvement project to increase the use of forced-air warming blankets reduced mean hypothermia times in trauma patients at Parkland Memorial Hospital, Dallas, from 229 to 154 minutes.
All it took to get doctors, nurses, and staff to use the forced-air warming blankets more often was a reminder that hypothermia is an independent predictor of death in trauma, and data showing that Parkland, a Level 1 trauma center, used forced-air warming in just 11% of its hypothermic trauma patients. Meetings to get those points across were held in December 2014.
Forced-air warming jumped to 70% of hypothermic patients over the next 4 months in 2015 (P equal to or less than .0001), leading to the 33% drop in rewarming times (P = .009). The improvement came without any shift in the use of the rewarming methods trauma teams were in the habit of using: warm blankets, room air, and IV fluids.
Investigator Dr. Frank Zhao thinks it’s something all trauma centers can and should do. “There’s no reason that we shouldn’t recommend this be part of the rewarming protocol in every trauma center. It took about a month to roll this out so everyone was on the same page and was easily achieved,” said Dr. Zhao, formerly a Parkland surgery resident but now a trauma and surgical critical care fellow at the Oregon Health and Sciences University in Portland.
The blankets are an almost universal presence in operating rooms to keep core temperatures at least 36 degrees Celsius, but “from what I’ve seen at multiple institutions, the Bair Hugger is probably one of the least used warming methods” in trauma. “They’re recommended for trauma rewarming, but we [didn’t] use them very often.” Staff were not in the habit, he said at the Eastern Association for the Surgery of Trauma scientific assembly.
From July to November 2014, before the intervention, 15.2% (114) of Levels 1 and 2 trauma patients arrived at Parkland hypothermic, versus 20.9% (82) during the colder period of January-April 2015. Almost 80% of the trauma patients over that time were male, and the average patient age was about 40 years.
The investigators have no disclosures, and there was no outside funding for the project.
SAN ANTONIO – A month-long quality improvement project to increase the use of forced-air warming blankets reduced mean hypothermia times in trauma patients at Parkland Memorial Hospital, Dallas, from 229 to 154 minutes.
All it took to get doctors, nurses, and staff to use the forced-air warming blankets more often was a reminder that hypothermia is an independent predictor of death in trauma, and data showing that Parkland, a Level 1 trauma center, used forced-air warming in just 11% of its hypothermic trauma patients. Meetings to get those points across were held in December 2014.
Forced-air warming jumped to 70% of hypothermic patients over the next 4 months in 2015 (P equal to or less than .0001), leading to the 33% drop in rewarming times (P = .009). The improvement came without any shift in the use of the rewarming methods trauma teams were in the habit of using: warm blankets, room air, and IV fluids.
Investigator Dr. Frank Zhao thinks it’s something all trauma centers can and should do. “There’s no reason that we shouldn’t recommend this be part of the rewarming protocol in every trauma center. It took about a month to roll this out so everyone was on the same page and was easily achieved,” said Dr. Zhao, formerly a Parkland surgery resident but now a trauma and surgical critical care fellow at the Oregon Health and Sciences University in Portland.
The blankets are an almost universal presence in operating rooms to keep core temperatures at least 36 degrees Celsius, but “from what I’ve seen at multiple institutions, the Bair Hugger is probably one of the least used warming methods” in trauma. “They’re recommended for trauma rewarming, but we [didn’t] use them very often.” Staff were not in the habit, he said at the Eastern Association for the Surgery of Trauma scientific assembly.
From July to November 2014, before the intervention, 15.2% (114) of Levels 1 and 2 trauma patients arrived at Parkland hypothermic, versus 20.9% (82) during the colder period of January-April 2015. Almost 80% of the trauma patients over that time were male, and the average patient age was about 40 years.
The investigators have no disclosures, and there was no outside funding for the project.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: It can take as little as a month to make forced-air warming blankets a routine part of hypothermia care in trauma.
Major finding: A month-long quality improvement project to increase the use of forced-air warming blankets reduced mean hypothermia times at a Level 1 trauma center from 229 to 154 minutes.
Data source: The project involved 196 hypothermic trauma patients
Disclosures: The investigators have no disclosures, and there was no outside funding for the project.

Baux cut-points predict geriatric burn outcomes
SAN ANTONIO – Geriatric burn patients have less than a 50% chance of returning home with a Baux score of about 85, and the risk of death begins to climb steadily after a score 93, approaching 50% at 110 points and almost 100% at 130 points, according to a review of 8,001 elderly patients in the National Burn Repository.
The investigators are developing the findings into a decision-making tool to help counsel families and caregivers about their options when elderly loved ones are seriously burned.

“There’s just not a lot of data out there on prognosis after burn injury in the geriatric population. We thought a simple decision aid for discussion with key stakeholders would provide significant assistance,” said investigator Dr. Erica Hodgman, a surgery research resident at the University of Texas Southwestern Medical Center, Dallas.
The hope is that families and caregivers will be able to better judge if the patient would want to press on with treatment given the odds of returning home, being discharged to a skilled nursing or rehab facility, or dying. “I think it will help people” feel less guilty if they decide to withdraw care or not send patients far away to a burn center, she said at the Eastern Association for the Surgery of Trauma scientific assembly.
The Baux score, a well-known metric in the burn community, adds the patient’s age to the percentage of surface area burned, so a 70 year old patient burned over 23% of their body, for instance, would have a score of 93. A modified Baux score adds points for inhalation injuries, but because the data didn’t include inhalation injury severity, the investigators found it more useful to stick with the original formula.
They queried the repository for patients 65 years or older with second- or third-degree burns from 2002-2011. They excluded patients with a length of stay of a day or less, along with elective admissions, non-burn injuries, and transfers to other burn centers. Next, they calculated Baux scores for each of their 8,001 subjects and noted if the patients were discharged home or to an alternate facility, or if he or she died.
Most patients had moderate scores of 70-100, and almost half were sent home. Of the 1,509 that died in hospital, 264 (17.5%) had care withdraw at a median of 3 days, but a range of 0-231 days. Flames were the most common cause of injury, followed by scalding.
A receiver operating curve analysis found that a Baux score at or below 86.15 predicted discharge home (AUC 0.698, 75.28% sensitivity, 54.64% specificity); a score above 77.12 predicted discharge to an alternate setting (AUC 0.539, 74.91% sensitivity, 34.38% specificity); and a score above 93.3 predicted mortality (AUC 0.779, 57.46% sensitivity, 87.08% specificity).
Dr. Hodgman said she thinks the cut-points will remain useful even as burn care improves with new grafting techniques that require smaller donor sites. Such innovation will apply mostly to moderately injured patients; for the more severely injured, the predictive power of the findings should still hold.
The investigators have no disclosures.
SAN ANTONIO – Geriatric burn patients have less than a 50% chance of returning home with a Baux score of about 85, and the risk of death begins to climb steadily after a score 93, approaching 50% at 110 points and almost 100% at 130 points, according to a review of 8,001 elderly patients in the National Burn Repository.
The investigators are developing the findings into a decision-making tool to help counsel families and caregivers about their options when elderly loved ones are seriously burned.
“There’s just not a lot of data out there on prognosis after burn injury in the geriatric population. We thought a simple decision aid for discussion with key stakeholders would provide significant assistance,” said investigator Dr. Erica Hodgman, a surgery research resident at the University of Texas Southwestern Medical Center, Dallas.
The hope is that families and caregivers will be able to better judge if the patient would want to press on with treatment given the odds of returning home, being discharged to a skilled nursing or rehab facility, or dying. “I think it will help people” feel less guilty if they decide to withdraw care or not send patients far away to a burn center, she said at the Eastern Association for the Surgery of Trauma scientific assembly.
The Baux score, a well-known metric in the burn community, adds the patient’s age to the percentage of surface area burned, so a 70 year old patient burned over 23% of their body, for instance, would have a score of 93. A modified Baux score adds points for inhalation injuries, but because the data didn’t include inhalation injury severity, the investigators found it more useful to stick with the original formula.
They queried the repository for patients 65 years or older with second- or third-degree burns from 2002-2011. They excluded patients with a length of stay of a day or less, along with elective admissions, non-burn injuries, and transfers to other burn centers. Next, they calculated Baux scores for each of their 8,001 subjects and noted if the patients were discharged home or to an alternate facility, or if he or she died.
Most patients had moderate scores of 70-100, and almost half were sent home. Of the 1,509 that died in hospital, 264 (17.5%) had care withdraw at a median of 3 days, but a range of 0-231 days. Flames were the most common cause of injury, followed by scalding.
A receiver operating curve analysis found that a Baux score at or below 86.15 predicted discharge home (AUC 0.698, 75.28% sensitivity, 54.64% specificity); a score above 77.12 predicted discharge to an alternate setting (AUC 0.539, 74.91% sensitivity, 34.38% specificity); and a score above 93.3 predicted mortality (AUC 0.779, 57.46% sensitivity, 87.08% specificity).
Dr. Hodgman said she thinks the cut-points will remain useful even as burn care improves with new grafting techniques that require smaller donor sites. Such innovation will apply mostly to moderately injured patients; for the more severely injured, the predictive power of the findings should still hold.
The investigators have no disclosures.
SAN ANTONIO – Geriatric burn patients have less than a 50% chance of returning home with a Baux score of about 85, and the risk of death begins to climb steadily after a score 93, approaching 50% at 110 points and almost 100% at 130 points, according to a review of 8,001 elderly patients in the National Burn Repository.
The investigators are developing the findings into a decision-making tool to help counsel families and caregivers about their options when elderly loved ones are seriously burned.
“There’s just not a lot of data out there on prognosis after burn injury in the geriatric population. We thought a simple decision aid for discussion with key stakeholders would provide significant assistance,” said investigator Dr. Erica Hodgman, a surgery research resident at the University of Texas Southwestern Medical Center, Dallas.
The hope is that families and caregivers will be able to better judge if the patient would want to press on with treatment given the odds of returning home, being discharged to a skilled nursing or rehab facility, or dying. “I think it will help people” feel less guilty if they decide to withdraw care or not send patients far away to a burn center, she said at the Eastern Association for the Surgery of Trauma scientific assembly.
The Baux score, a well-known metric in the burn community, adds the patient’s age to the percentage of surface area burned, so a 70 year old patient burned over 23% of their body, for instance, would have a score of 93. A modified Baux score adds points for inhalation injuries, but because the data didn’t include inhalation injury severity, the investigators found it more useful to stick with the original formula.
They queried the repository for patients 65 years or older with second- or third-degree burns from 2002-2011. They excluded patients with a length of stay of a day or less, along with elective admissions, non-burn injuries, and transfers to other burn centers. Next, they calculated Baux scores for each of their 8,001 subjects and noted if the patients were discharged home or to an alternate facility, or if he or she died.
Most patients had moderate scores of 70-100, and almost half were sent home. Of the 1,509 that died in hospital, 264 (17.5%) had care withdraw at a median of 3 days, but a range of 0-231 days. Flames were the most common cause of injury, followed by scalding.
A receiver operating curve analysis found that a Baux score at or below 86.15 predicted discharge home (AUC 0.698, 75.28% sensitivity, 54.64% specificity); a score above 77.12 predicted discharge to an alternate setting (AUC 0.539, 74.91% sensitivity, 34.38% specificity); and a score above 93.3 predicted mortality (AUC 0.779, 57.46% sensitivity, 87.08% specificity).
Dr. Hodgman said she thinks the cut-points will remain useful even as burn care improves with new grafting techniques that require smaller donor sites. Such innovation will apply mostly to moderately injured patients; for the more severely injured, the predictive power of the findings should still hold.
The investigators have no disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Baux score cut-points help counsel families about their options when an elderly family member is seriously burned.
Major finding: Geriatric burn patients have less than a 50% chance of returning home with a Baux score of about 85, and the risk of death begins to climb steadily after a score 93.
Data source: Review of 8,001 patients over 65 years old in the National Burn Repository
Disclosures: The investigators have no disclosures.

Acupressure improves persistent fatigue in breast cancer survivors
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.

She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.
She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.
She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
AT SABCS 2015
Key clinical point: Acupressure is an easily learned, effective method for self-treatment of persistent fatigue in breast cancer survivors.
Major finding: Two-thirds of breast cancer survivors with persistent fatigue experienced significant improvement in response to 6 weeks of self-administered relaxation acupressure, compared with 31% of usual-care controls.
Data source: This was a 10-week, single-blind study involving 288 breast cancer survivors with persistent fatigue who were randomized to relaxation acupressure, stimulation acupressure, or usual care.
Disclosures: The study was sponsored by the National Cancer Institute. Dr. Zick reported having no financial conflicts.
