User login
Patients want more info about medical imaging risks

Photo by Rhoda Baer
Patients want more information about medical imaging tests that use radiation, according to research published in Radiology.
Most of the 30 subjects involved in this study said their healthcare providers did not initiate a discussion about the risks and benefits of imaging tests.
So a majority of participants obtained information from the Internet. Researchers said these findings highlight a need for better communication between patients and providers.
“This may not be what we in the medical field want to hear, but I think it’s important that we hear it,” said study author Jennifer Hay, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“Patients want this information, and they prefer to receive it from doctors they know and trust.”
Dr Hay and her colleagues analyzed over 9 hours of transcribed conversations with 30 people who had undergone medical imaging exams or consented for their children to undergo such exams.
The goal was to determine the subjects’ understanding of the benefits and risks associated with various medical imaging procedures and their expectations regarding communication of those benefits and risks.
The study group was divided into 6 focus groups, including 5 groups of cancer patients (or parents of young cancer patients) and 1 group of participants in a lung cancer screening program.
Quantifying subjects’ knowledge
The researchers found that participants perceived clear benefits from imaging tests like X-rays, computed tomography (CT) scans, and nuclear medicine examinations.
And most subjects were highly aware of the risks associated with ionizing radiation exposure, including the potential risk of future cancer. But their knowledge regarding which imaging tests use ionizing radiation varied.
In general, participants were more likely to understand that X-rays, CTs, and positron emission tomography (PET) scans deliver ionizing radiation and less likely to know about mammography, bone scanning, or stress tests. Many subjects did not know if magnetic resonance imaging (MRI) involved ionizing radiation.
Some participants did not know how tests differed, and some believed there was a “best” imaging test. Occasionally, subjects confused ionizing radiation from diagnostic medical imaging with radiation therapy.
Desire for information
Participants considered the availability of basic benefit-risk information to be a fundamental component of care. And they expressed a desire for a wide range of information about medical imaging tests.
Most subjects wanted basic education about which imaging tests use ionizing radiation and how doses compare among them. Nearly all subjects wanted to understand how tests differ, what governs selection of one over another, and why multiple tests are sometimes ordered.
A majority of participants met their needs for more information through self-directed Internet searches.
Concern about risks
Most subjects agreed that learning about possible future risks was important, but having this information would probably not alter their decision to proceed with a recommended test.
The desire for information about risks was strongest among cancer patients who had made the transition from treatment to survivorship.
These patients wanted to know how risk accumulates from multiple exams over time, whether additional ionizing radiation exposure could be avoided by substituting MRI for CT, and if longer intervals between follow-up examinations could be negotiated.
“Interest in having more information and participating in decision-making about medical imaging clearly increased as patients transitioned from active cancer treatment to survivorship,” said study author Raymond H. Thornton, MD, of Memorial Sloan Kettering Cancer Center.
“Cancer survivors typically focus on healthful living and risk-factor reduction, so they were particularly eager to participate in discussions about potential long-term risks of radiation.”
The different levels of desire for information among the study subjects lend support to a tiered approach for patient-centered communication, according to Dr Hay.
“A tiered approach would provide all patients with information and offer additional options to those who want to dig deeper and find out more,” she said.
Presenting information
Subjects expressed interest in 2 different modes of information exchange. Many participants said the ideal situation would be a face-to-face discussion with their personal physician, a medical physicist, or radiologist.
Others expressed an interest in written resources, especially hospital-endorsed Internet sites and printed materials. ![]()
Photo by Rhoda Baer
Patients want more information about medical imaging tests that use radiation, according to research published in Radiology.
Most of the 30 subjects involved in this study said their healthcare providers did not initiate a discussion about the risks and benefits of imaging tests.
So a majority of participants obtained information from the Internet. Researchers said these findings highlight a need for better communication between patients and providers.
“This may not be what we in the medical field want to hear, but I think it’s important that we hear it,” said study author Jennifer Hay, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“Patients want this information, and they prefer to receive it from doctors they know and trust.”
Dr Hay and her colleagues analyzed over 9 hours of transcribed conversations with 30 people who had undergone medical imaging exams or consented for their children to undergo such exams.
The goal was to determine the subjects’ understanding of the benefits and risks associated with various medical imaging procedures and their expectations regarding communication of those benefits and risks.
The study group was divided into 6 focus groups, including 5 groups of cancer patients (or parents of young cancer patients) and 1 group of participants in a lung cancer screening program.
Quantifying subjects’ knowledge
The researchers found that participants perceived clear benefits from imaging tests like X-rays, computed tomography (CT) scans, and nuclear medicine examinations.
And most subjects were highly aware of the risks associated with ionizing radiation exposure, including the potential risk of future cancer. But their knowledge regarding which imaging tests use ionizing radiation varied.
In general, participants were more likely to understand that X-rays, CTs, and positron emission tomography (PET) scans deliver ionizing radiation and less likely to know about mammography, bone scanning, or stress tests. Many subjects did not know if magnetic resonance imaging (MRI) involved ionizing radiation.
Some participants did not know how tests differed, and some believed there was a “best” imaging test. Occasionally, subjects confused ionizing radiation from diagnostic medical imaging with radiation therapy.
Desire for information
Participants considered the availability of basic benefit-risk information to be a fundamental component of care. And they expressed a desire for a wide range of information about medical imaging tests.
Most subjects wanted basic education about which imaging tests use ionizing radiation and how doses compare among them. Nearly all subjects wanted to understand how tests differ, what governs selection of one over another, and why multiple tests are sometimes ordered.
A majority of participants met their needs for more information through self-directed Internet searches.
Concern about risks
Most subjects agreed that learning about possible future risks was important, but having this information would probably not alter their decision to proceed with a recommended test.
The desire for information about risks was strongest among cancer patients who had made the transition from treatment to survivorship.
These patients wanted to know how risk accumulates from multiple exams over time, whether additional ionizing radiation exposure could be avoided by substituting MRI for CT, and if longer intervals between follow-up examinations could be negotiated.
“Interest in having more information and participating in decision-making about medical imaging clearly increased as patients transitioned from active cancer treatment to survivorship,” said study author Raymond H. Thornton, MD, of Memorial Sloan Kettering Cancer Center.
“Cancer survivors typically focus on healthful living and risk-factor reduction, so they were particularly eager to participate in discussions about potential long-term risks of radiation.”
The different levels of desire for information among the study subjects lend support to a tiered approach for patient-centered communication, according to Dr Hay.
“A tiered approach would provide all patients with information and offer additional options to those who want to dig deeper and find out more,” she said.
Presenting information
Subjects expressed interest in 2 different modes of information exchange. Many participants said the ideal situation would be a face-to-face discussion with their personal physician, a medical physicist, or radiologist.
Others expressed an interest in written resources, especially hospital-endorsed Internet sites and printed materials. ![]()
Photo by Rhoda Baer
Patients want more information about medical imaging tests that use radiation, according to research published in Radiology.
Most of the 30 subjects involved in this study said their healthcare providers did not initiate a discussion about the risks and benefits of imaging tests.
So a majority of participants obtained information from the Internet. Researchers said these findings highlight a need for better communication between patients and providers.
“This may not be what we in the medical field want to hear, but I think it’s important that we hear it,” said study author Jennifer Hay, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“Patients want this information, and they prefer to receive it from doctors they know and trust.”
Dr Hay and her colleagues analyzed over 9 hours of transcribed conversations with 30 people who had undergone medical imaging exams or consented for their children to undergo such exams.
The goal was to determine the subjects’ understanding of the benefits and risks associated with various medical imaging procedures and their expectations regarding communication of those benefits and risks.
The study group was divided into 6 focus groups, including 5 groups of cancer patients (or parents of young cancer patients) and 1 group of participants in a lung cancer screening program.
Quantifying subjects’ knowledge
The researchers found that participants perceived clear benefits from imaging tests like X-rays, computed tomography (CT) scans, and nuclear medicine examinations.
And most subjects were highly aware of the risks associated with ionizing radiation exposure, including the potential risk of future cancer. But their knowledge regarding which imaging tests use ionizing radiation varied.
In general, participants were more likely to understand that X-rays, CTs, and positron emission tomography (PET) scans deliver ionizing radiation and less likely to know about mammography, bone scanning, or stress tests. Many subjects did not know if magnetic resonance imaging (MRI) involved ionizing radiation.
Some participants did not know how tests differed, and some believed there was a “best” imaging test. Occasionally, subjects confused ionizing radiation from diagnostic medical imaging with radiation therapy.
Desire for information
Participants considered the availability of basic benefit-risk information to be a fundamental component of care. And they expressed a desire for a wide range of information about medical imaging tests.
Most subjects wanted basic education about which imaging tests use ionizing radiation and how doses compare among them. Nearly all subjects wanted to understand how tests differ, what governs selection of one over another, and why multiple tests are sometimes ordered.
A majority of participants met their needs for more information through self-directed Internet searches.
Concern about risks
Most subjects agreed that learning about possible future risks was important, but having this information would probably not alter their decision to proceed with a recommended test.
The desire for information about risks was strongest among cancer patients who had made the transition from treatment to survivorship.
These patients wanted to know how risk accumulates from multiple exams over time, whether additional ionizing radiation exposure could be avoided by substituting MRI for CT, and if longer intervals between follow-up examinations could be negotiated.
“Interest in having more information and participating in decision-making about medical imaging clearly increased as patients transitioned from active cancer treatment to survivorship,” said study author Raymond H. Thornton, MD, of Memorial Sloan Kettering Cancer Center.
“Cancer survivors typically focus on healthful living and risk-factor reduction, so they were particularly eager to participate in discussions about potential long-term risks of radiation.”
The different levels of desire for information among the study subjects lend support to a tiered approach for patient-centered communication, according to Dr Hay.
“A tiered approach would provide all patients with information and offer additional options to those who want to dig deeper and find out more,” she said.
Presenting information
Subjects expressed interest in 2 different modes of information exchange. Many participants said the ideal situation would be a face-to-face discussion with their personal physician, a medical physicist, or radiologist.
Others expressed an interest in written resources, especially hospital-endorsed Internet sites and printed materials. ![]()
NICE OKs rivaroxaban, rejects pomalidomide

Photo courtesy of CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued final guidance documents for rivaroxaban (Xarelto) and pomalidomide (Imnovid).
The agency is recommending rivaroxaban (in combination) as an option for preventing atherothrombotic events in patients with acute coronary syndrome (ACS).
But NICE said it cannot recommend pomalidomide (in combination) for the treatment of relapsed/refractory multiple myeloma (MM).
Rivaroxaban
Rivaroxaban is licensed in the European Union to prevent atherothrombotic events in adults who have an ACS severe enough to result in the release of cardiac biomarkers into the blood. The drug is given with aspirin and clopidogrel or aspirin alone.
Based on results of the ATLAS-ACS 2-TIMI 51 trial, an appraisal committee advising NICE concluded that rivaroxaban given at 2.5 mg twice daily in combination with aspirin plus clopidogrel or with aspirin alone was more effective than aspirin plus clopidogrel or aspirin alone for preventing further cardiovascular deaths and myocardial infarction in patients with ACS and raised cardiac biomarkers.
The committee also found rivaroxaban to be a cost-effective use of National Health Service (NHS) resources. They noted, however, that the drug can increase the risk of bleeding.
“Because rivaroxaban is associated with a higher risk of causing bleeding than clopidogrel in combination with aspirin or aspirin alone, the guidance recommends that, before starting treatment, doctors should carry out a careful assessment of a person’s bleeding risk,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“The decision to start treatment should be made after an informed discussion between the doctor and patient about the benefits and risks of rivaroxaban. Also, because there is limited experience of treatment with rivaroxaban up to 24 months, the guidance recommends careful consideration should be given to whether treatment is continued beyond 12 months.”
Pomalidomide
NICE’s final guidance on pomalidomide said the agency cannot recommend the drug as a treatment option for MM.
Pomalidomide is approved in the European Union for use in combination with dexamethasone to treat adults with relapsed and refractory MM who have had at least 2 prior treatments, including lenalidomide and bortezomib, and whose disease has progressed on the last therapy.
“Unfortunately, we cannot recommend pomalidomide, as the analyses from Celgene, the company that markets the drug, showed that it does not offer enough benefit to justify its high price,” said Sir Andrew Dillon, NICE chief executive.
NICE said the appraisal committee could not judge with any confidence how effective pomalidomide is compared to current treatment options based on the available evidence provided before and after consultation.
Bearing in mind the magnitude of the differences in the overall survival estimates between pomalidomide and high-dose dexamethasone in the phase 3 MM-003 trial and all data presented to the committee for comparators, the committee was persuaded that pomalidomide extends life for at least 3 months on average when compared with standard NHS care.
However, considering the incremental cost-effectiveness ratios, the committee concluded that, even with the end-of-life criteria met, the weighting that would have to be placed on the quality-adjusted life-years gained would be too high to consider pomalidomide a cost-effective use of NHS resources.
The committee also said the uncertainty in the relative effectiveness of pomalidomide compared with established NHS practice would affect any weighting that could be placed on quality-adjusted life-years gained. ![]()
Photo courtesy of CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued final guidance documents for rivaroxaban (Xarelto) and pomalidomide (Imnovid).
The agency is recommending rivaroxaban (in combination) as an option for preventing atherothrombotic events in patients with acute coronary syndrome (ACS).
But NICE said it cannot recommend pomalidomide (in combination) for the treatment of relapsed/refractory multiple myeloma (MM).
Rivaroxaban
Rivaroxaban is licensed in the European Union to prevent atherothrombotic events in adults who have an ACS severe enough to result in the release of cardiac biomarkers into the blood. The drug is given with aspirin and clopidogrel or aspirin alone.
Based on results of the ATLAS-ACS 2-TIMI 51 trial, an appraisal committee advising NICE concluded that rivaroxaban given at 2.5 mg twice daily in combination with aspirin plus clopidogrel or with aspirin alone was more effective than aspirin plus clopidogrel or aspirin alone for preventing further cardiovascular deaths and myocardial infarction in patients with ACS and raised cardiac biomarkers.
The committee also found rivaroxaban to be a cost-effective use of National Health Service (NHS) resources. They noted, however, that the drug can increase the risk of bleeding.
“Because rivaroxaban is associated with a higher risk of causing bleeding than clopidogrel in combination with aspirin or aspirin alone, the guidance recommends that, before starting treatment, doctors should carry out a careful assessment of a person’s bleeding risk,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“The decision to start treatment should be made after an informed discussion between the doctor and patient about the benefits and risks of rivaroxaban. Also, because there is limited experience of treatment with rivaroxaban up to 24 months, the guidance recommends careful consideration should be given to whether treatment is continued beyond 12 months.”
Pomalidomide
NICE’s final guidance on pomalidomide said the agency cannot recommend the drug as a treatment option for MM.
Pomalidomide is approved in the European Union for use in combination with dexamethasone to treat adults with relapsed and refractory MM who have had at least 2 prior treatments, including lenalidomide and bortezomib, and whose disease has progressed on the last therapy.
“Unfortunately, we cannot recommend pomalidomide, as the analyses from Celgene, the company that markets the drug, showed that it does not offer enough benefit to justify its high price,” said Sir Andrew Dillon, NICE chief executive.
NICE said the appraisal committee could not judge with any confidence how effective pomalidomide is compared to current treatment options based on the available evidence provided before and after consultation.
Bearing in mind the magnitude of the differences in the overall survival estimates between pomalidomide and high-dose dexamethasone in the phase 3 MM-003 trial and all data presented to the committee for comparators, the committee was persuaded that pomalidomide extends life for at least 3 months on average when compared with standard NHS care.
However, considering the incremental cost-effectiveness ratios, the committee concluded that, even with the end-of-life criteria met, the weighting that would have to be placed on the quality-adjusted life-years gained would be too high to consider pomalidomide a cost-effective use of NHS resources.
The committee also said the uncertainty in the relative effectiveness of pomalidomide compared with established NHS practice would affect any weighting that could be placed on quality-adjusted life-years gained. ![]()
Photo courtesy of CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued final guidance documents for rivaroxaban (Xarelto) and pomalidomide (Imnovid).
The agency is recommending rivaroxaban (in combination) as an option for preventing atherothrombotic events in patients with acute coronary syndrome (ACS).
But NICE said it cannot recommend pomalidomide (in combination) for the treatment of relapsed/refractory multiple myeloma (MM).
Rivaroxaban
Rivaroxaban is licensed in the European Union to prevent atherothrombotic events in adults who have an ACS severe enough to result in the release of cardiac biomarkers into the blood. The drug is given with aspirin and clopidogrel or aspirin alone.
Based on results of the ATLAS-ACS 2-TIMI 51 trial, an appraisal committee advising NICE concluded that rivaroxaban given at 2.5 mg twice daily in combination with aspirin plus clopidogrel or with aspirin alone was more effective than aspirin plus clopidogrel or aspirin alone for preventing further cardiovascular deaths and myocardial infarction in patients with ACS and raised cardiac biomarkers.
The committee also found rivaroxaban to be a cost-effective use of National Health Service (NHS) resources. They noted, however, that the drug can increase the risk of bleeding.
“Because rivaroxaban is associated with a higher risk of causing bleeding than clopidogrel in combination with aspirin or aspirin alone, the guidance recommends that, before starting treatment, doctors should carry out a careful assessment of a person’s bleeding risk,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“The decision to start treatment should be made after an informed discussion between the doctor and patient about the benefits and risks of rivaroxaban. Also, because there is limited experience of treatment with rivaroxaban up to 24 months, the guidance recommends careful consideration should be given to whether treatment is continued beyond 12 months.”
Pomalidomide
NICE’s final guidance on pomalidomide said the agency cannot recommend the drug as a treatment option for MM.
Pomalidomide is approved in the European Union for use in combination with dexamethasone to treat adults with relapsed and refractory MM who have had at least 2 prior treatments, including lenalidomide and bortezomib, and whose disease has progressed on the last therapy.
“Unfortunately, we cannot recommend pomalidomide, as the analyses from Celgene, the company that markets the drug, showed that it does not offer enough benefit to justify its high price,” said Sir Andrew Dillon, NICE chief executive.
NICE said the appraisal committee could not judge with any confidence how effective pomalidomide is compared to current treatment options based on the available evidence provided before and after consultation.
Bearing in mind the magnitude of the differences in the overall survival estimates between pomalidomide and high-dose dexamethasone in the phase 3 MM-003 trial and all data presented to the committee for comparators, the committee was persuaded that pomalidomide extends life for at least 3 months on average when compared with standard NHS care.
However, considering the incremental cost-effectiveness ratios, the committee concluded that, even with the end-of-life criteria met, the weighting that would have to be placed on the quality-adjusted life-years gained would be too high to consider pomalidomide a cost-effective use of NHS resources.
The committee also said the uncertainty in the relative effectiveness of pomalidomide compared with established NHS practice would affect any weighting that could be placed on quality-adjusted life-years gained. ![]()
Enzyme keeps HSCs functional to prevent anemia
Preclinical research suggests an enzyme found in hematopoietic stem cells (HSCs) is key to maintaining periods of inactivity, thereby decreasing the odds that HSCs will divide too often and acquire mutations or cell damage.
Experiments showed that animals lacking this enzyme, inositol trisphosphate 3-kinase B (Itpkb), experience dangerous HSC activation and ultimately succumb to lethal anemia.
“These HSCs remain active too long and then disappear,” said Karsten Sauer, PhD, of The Scripps Research Institute in La Jolla, California.
“As a consequence, the mice lose their red blood cells and die.”
With this new understanding of Itpkb, Dr Sauer and his colleagues believe they are closer to improving therapies for diseases such as bone marrow failure syndrome, anemia, leukemia, and lymphoma.
The team described their research in Blood.
The group set out to investigate the mechanisms that activate and deactivate HSCs. They focused on Itpkb because it is produced in HSCs, and the enzyme is known to dampen activating signaling in other cells.
“We hypothesized that Itpkb might do the same in HSCs to keep them at rest,” Dr Sauer said. “Moreover, Itpkb is an enzyme whose function can be controlled by small molecules. This might facilitate drug development if our hypothesis were true.”
The researchers started with a strain of mice that lacked the gene to produce Itpkb. As expected, these mice developed hyperactive HSCs. Eventually, the mutant HSCs exhausted themselves and stopped producing progenitor cells, so the mice developed severe anemia and died.
Dr Sauer and his colleagues linked the abnormal behavior of the mutant HSCs to a chain of events at the molecular level.
Itpkb’s job is to attach phosphates to molecules called inositols, which then send messages to other parts of the cell. The researchers found that Itpkb can turn one inositol, IP3, into another inositol known as IP4.
This is significant because IP4 controls cell proliferation, cellular metabolism, and aspects of the immune system. The study showed that IP4 also protects HSCs by dampening PI3K/Akt/mTOR signaling.
To confirm this finding, the researchers treated the animals with the mTOR inhibitor rapamycin. The drug halted the abnormal signaling process and prevented the excessive division of HSCs lacking Itpkb. This supported the notion that Itpkb maintains HSCs’ quiescence by dampening PI3K/Akt/mTOR signaling.
Dr Sauer said future research in his lab will focus on studying whether Itpkb has a similar function in human HSCs.
“A major question is whether we can translate our findings into innovative therapies,” he said. “If we can show that Itpkb also keeps human HSCs healthy, this could open avenues to target Itpkb to improve HSC function in bone marrow failure syndromes and immunodeficiencies or to increase the success rates of HSC transplantation therapies for leukemias and lymphomas.” ![]()
Preclinical research suggests an enzyme found in hematopoietic stem cells (HSCs) is key to maintaining periods of inactivity, thereby decreasing the odds that HSCs will divide too often and acquire mutations or cell damage.
Experiments showed that animals lacking this enzyme, inositol trisphosphate 3-kinase B (Itpkb), experience dangerous HSC activation and ultimately succumb to lethal anemia.
“These HSCs remain active too long and then disappear,” said Karsten Sauer, PhD, of The Scripps Research Institute in La Jolla, California.
“As a consequence, the mice lose their red blood cells and die.”
With this new understanding of Itpkb, Dr Sauer and his colleagues believe they are closer to improving therapies for diseases such as bone marrow failure syndrome, anemia, leukemia, and lymphoma.
The team described their research in Blood.
The group set out to investigate the mechanisms that activate and deactivate HSCs. They focused on Itpkb because it is produced in HSCs, and the enzyme is known to dampen activating signaling in other cells.
“We hypothesized that Itpkb might do the same in HSCs to keep them at rest,” Dr Sauer said. “Moreover, Itpkb is an enzyme whose function can be controlled by small molecules. This might facilitate drug development if our hypothesis were true.”
The researchers started with a strain of mice that lacked the gene to produce Itpkb. As expected, these mice developed hyperactive HSCs. Eventually, the mutant HSCs exhausted themselves and stopped producing progenitor cells, so the mice developed severe anemia and died.
Dr Sauer and his colleagues linked the abnormal behavior of the mutant HSCs to a chain of events at the molecular level.
Itpkb’s job is to attach phosphates to molecules called inositols, which then send messages to other parts of the cell. The researchers found that Itpkb can turn one inositol, IP3, into another inositol known as IP4.
This is significant because IP4 controls cell proliferation, cellular metabolism, and aspects of the immune system. The study showed that IP4 also protects HSCs by dampening PI3K/Akt/mTOR signaling.
To confirm this finding, the researchers treated the animals with the mTOR inhibitor rapamycin. The drug halted the abnormal signaling process and prevented the excessive division of HSCs lacking Itpkb. This supported the notion that Itpkb maintains HSCs’ quiescence by dampening PI3K/Akt/mTOR signaling.
Dr Sauer said future research in his lab will focus on studying whether Itpkb has a similar function in human HSCs.
“A major question is whether we can translate our findings into innovative therapies,” he said. “If we can show that Itpkb also keeps human HSCs healthy, this could open avenues to target Itpkb to improve HSC function in bone marrow failure syndromes and immunodeficiencies or to increase the success rates of HSC transplantation therapies for leukemias and lymphomas.” ![]()
Preclinical research suggests an enzyme found in hematopoietic stem cells (HSCs) is key to maintaining periods of inactivity, thereby decreasing the odds that HSCs will divide too often and acquire mutations or cell damage.
Experiments showed that animals lacking this enzyme, inositol trisphosphate 3-kinase B (Itpkb), experience dangerous HSC activation and ultimately succumb to lethal anemia.
“These HSCs remain active too long and then disappear,” said Karsten Sauer, PhD, of The Scripps Research Institute in La Jolla, California.
“As a consequence, the mice lose their red blood cells and die.”
With this new understanding of Itpkb, Dr Sauer and his colleagues believe they are closer to improving therapies for diseases such as bone marrow failure syndrome, anemia, leukemia, and lymphoma.
The team described their research in Blood.
The group set out to investigate the mechanisms that activate and deactivate HSCs. They focused on Itpkb because it is produced in HSCs, and the enzyme is known to dampen activating signaling in other cells.
“We hypothesized that Itpkb might do the same in HSCs to keep them at rest,” Dr Sauer said. “Moreover, Itpkb is an enzyme whose function can be controlled by small molecules. This might facilitate drug development if our hypothesis were true.”
The researchers started with a strain of mice that lacked the gene to produce Itpkb. As expected, these mice developed hyperactive HSCs. Eventually, the mutant HSCs exhausted themselves and stopped producing progenitor cells, so the mice developed severe anemia and died.
Dr Sauer and his colleagues linked the abnormal behavior of the mutant HSCs to a chain of events at the molecular level.
Itpkb’s job is to attach phosphates to molecules called inositols, which then send messages to other parts of the cell. The researchers found that Itpkb can turn one inositol, IP3, into another inositol known as IP4.
This is significant because IP4 controls cell proliferation, cellular metabolism, and aspects of the immune system. The study showed that IP4 also protects HSCs by dampening PI3K/Akt/mTOR signaling.
To confirm this finding, the researchers treated the animals with the mTOR inhibitor rapamycin. The drug halted the abnormal signaling process and prevented the excessive division of HSCs lacking Itpkb. This supported the notion that Itpkb maintains HSCs’ quiescence by dampening PI3K/Akt/mTOR signaling.
Dr Sauer said future research in his lab will focus on studying whether Itpkb has a similar function in human HSCs.
“A major question is whether we can translate our findings into innovative therapies,” he said. “If we can show that Itpkb also keeps human HSCs healthy, this could open avenues to target Itpkb to improve HSC function in bone marrow failure syndromes and immunodeficiencies or to increase the success rates of HSC transplantation therapies for leukemias and lymphomas.” ![]()
Pesticides may cause NHL, other cancers

Photo by John Messina
The International Agency for Research on Cancer (IARC), the specialized cancer agency of the World Health Organization, has found evidence suggesting that 5 organophosphate pesticides may be carcinogenic.
The IARC classified the herbicide glyphosate and the insecticides malathion and diazinon as “probably carcinogenic” to humans and the insecticides tetrachlorvinphos and parathion as “possibly carcinogenic” to humans.
A summary of these findings has been published in The Lancet Oncology.
Glyphosate
For the herbicide glyphosate, the IARC found limited evidence of carcinogenicity in humans. Case-control studies of occupational exposure to glyphosate in the US, Canada, and Sweden showed increased risks for non-Hodgkin lymphoma (NHL).
However, the Agricultural Health Study (AHS) showed no significantly increased risk of NHL in subjects exposed to glyphosate.
A study of community residents showed increases in blood markers of chromosomal damage after glyphosate formulations were sprayed nearby. And glyphosate was shown to cause DNA and chromosomal damage in human cells, although bacterial mutagenesis tests were negative.
In studies of male mice, glyphosate increased the incidence of renal tubule carcinoma and hemangiosarcoma. Glyphosate also increased the incidence of pancreatic islet-cell adenoma in male rats, and a glyphosate formulation promoted skin tumors in mice.
The IARC said glyphosate has the highest global production volume of all herbicides. It is used in agriculture, forestry, urban, and home applications.
Glyphosate has been detected in the air during spraying, in water, and in food. The general population is exposed to the chemical primarily by living near sprayed areas, home use, and diet. But the IARC said the level of exposure observed is generally low.
Malathion
The IARC classified malathion as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL and prostate cancer. Occupational use of malathion was associated with an increased risk of prostate cancer in a Canadian case-control study and in the AHS.
Studies of occupational exposures in the US, Canada, and Sweden revealed positive associations between malathion and NHL. However, results of the AHS did not show an association between the insecticide and NHL.
Studies showed that malathion induced DNA and chromosomal damage in humans and animals, although bacterial mutagenesis tests were negative. Results also suggested malathion disrupts hormone pathways.
Experiments in mice showed malathion increased the incidence of hepatocellular adenoma or carcinoma (combined). In rats, the insecticide increased the incidence of thyroid carcinoma in males, hepatocellular adenoma or carcinoma (combined) in females, and mammary gland adenocarcinoma after subcutaneous injection in females.
The IARC said malathion is used in “substantial volumes throughout the world” to control insects in agricultural and residential areas.
Workers may be exposed to malathion during the use and production of the product. The general population may be exposed if they live near sprayed areas, use the product at home, or consume food exposed to the chemical.
Diazinon
The IARC classified diazinon as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL, leukemia, and lung cancer.
Two multicenter, case-control studies of agricultural exposures suggested a positive association between diazinon and NHL. The AHS showed positive associations with specific subtypes of NHL but no overall increased risk of NHL. The AHS also suggested an increased risk of leukemia and lung cancer in subjects exposed to diazinon.
Evidence suggested that diazinon induced DNA or chromosomal damage in human and mammalian cells in vitro. In vivo, diazinon increased the incidence of hepatocellular carcinoma in mice and leukemia or lymphoma (combined) in rats, but only in males receiving the low dose in each study.
Diazinon has been used to control insects in agricultural and residential areas. The IARC said production volumes have been relatively low and decreased further after 2006 due to restrictions in the US and the European Union (EU). There was limited information on the use of this pesticide in other countries.
Tetrachlorvinphos
The insecticide tetrachlorvinphos was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals. The IARC said the evidence in humans was inadequate.
However, tetrachlorvinphos was shown to induce hepatocellular tumors (benign or malignant) in mice, renal tubule tumors (benign or malignant) in male mice, and spleen hemangioma in male rats.
Tetrachlorvinphos is banned in the EU. In the US, the insecticide is still used on livestock and pets (in flea collars). The IARC said there was no information available on tetrachlorvinphos use in other countries.
Parathion
The insecticide parathion was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals.
Researchers have observed associations between the insecticide and cancers in several tissues in occupational studies. But the IARC said the evidence that parathion is carcinogenic in humans remains sparse.
Experiments in mice showed that parathion increased the incidence of bronchioloalveolar adenoma and/or carcinoma in males and lymphoma in females. In rats, parathion induced adrenal cortical adenoma or carcinoma (combined), malignant pancreatic tumors, and thyroid follicular cell adenoma in males, and mammary gland adenocarcinoma (after subcutaneous injection in females).
Parathion use has been severely restricted since the 1980s, and all authorized uses of this chemical were cancelled in the EU and the US by 2003. ![]()
Photo by John Messina
The International Agency for Research on Cancer (IARC), the specialized cancer agency of the World Health Organization, has found evidence suggesting that 5 organophosphate pesticides may be carcinogenic.
The IARC classified the herbicide glyphosate and the insecticides malathion and diazinon as “probably carcinogenic” to humans and the insecticides tetrachlorvinphos and parathion as “possibly carcinogenic” to humans.
A summary of these findings has been published in The Lancet Oncology.
Glyphosate
For the herbicide glyphosate, the IARC found limited evidence of carcinogenicity in humans. Case-control studies of occupational exposure to glyphosate in the US, Canada, and Sweden showed increased risks for non-Hodgkin lymphoma (NHL).
However, the Agricultural Health Study (AHS) showed no significantly increased risk of NHL in subjects exposed to glyphosate.
A study of community residents showed increases in blood markers of chromosomal damage after glyphosate formulations were sprayed nearby. And glyphosate was shown to cause DNA and chromosomal damage in human cells, although bacterial mutagenesis tests were negative.
In studies of male mice, glyphosate increased the incidence of renal tubule carcinoma and hemangiosarcoma. Glyphosate also increased the incidence of pancreatic islet-cell adenoma in male rats, and a glyphosate formulation promoted skin tumors in mice.
The IARC said glyphosate has the highest global production volume of all herbicides. It is used in agriculture, forestry, urban, and home applications.
Glyphosate has been detected in the air during spraying, in water, and in food. The general population is exposed to the chemical primarily by living near sprayed areas, home use, and diet. But the IARC said the level of exposure observed is generally low.
Malathion
The IARC classified malathion as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL and prostate cancer. Occupational use of malathion was associated with an increased risk of prostate cancer in a Canadian case-control study and in the AHS.
Studies of occupational exposures in the US, Canada, and Sweden revealed positive associations between malathion and NHL. However, results of the AHS did not show an association between the insecticide and NHL.
Studies showed that malathion induced DNA and chromosomal damage in humans and animals, although bacterial mutagenesis tests were negative. Results also suggested malathion disrupts hormone pathways.
Experiments in mice showed malathion increased the incidence of hepatocellular adenoma or carcinoma (combined). In rats, the insecticide increased the incidence of thyroid carcinoma in males, hepatocellular adenoma or carcinoma (combined) in females, and mammary gland adenocarcinoma after subcutaneous injection in females.
The IARC said malathion is used in “substantial volumes throughout the world” to control insects in agricultural and residential areas.
Workers may be exposed to malathion during the use and production of the product. The general population may be exposed if they live near sprayed areas, use the product at home, or consume food exposed to the chemical.
Diazinon
The IARC classified diazinon as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL, leukemia, and lung cancer.
Two multicenter, case-control studies of agricultural exposures suggested a positive association between diazinon and NHL. The AHS showed positive associations with specific subtypes of NHL but no overall increased risk of NHL. The AHS also suggested an increased risk of leukemia and lung cancer in subjects exposed to diazinon.
Evidence suggested that diazinon induced DNA or chromosomal damage in human and mammalian cells in vitro. In vivo, diazinon increased the incidence of hepatocellular carcinoma in mice and leukemia or lymphoma (combined) in rats, but only in males receiving the low dose in each study.
Diazinon has been used to control insects in agricultural and residential areas. The IARC said production volumes have been relatively low and decreased further after 2006 due to restrictions in the US and the European Union (EU). There was limited information on the use of this pesticide in other countries.
Tetrachlorvinphos
The insecticide tetrachlorvinphos was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals. The IARC said the evidence in humans was inadequate.
However, tetrachlorvinphos was shown to induce hepatocellular tumors (benign or malignant) in mice, renal tubule tumors (benign or malignant) in male mice, and spleen hemangioma in male rats.
Tetrachlorvinphos is banned in the EU. In the US, the insecticide is still used on livestock and pets (in flea collars). The IARC said there was no information available on tetrachlorvinphos use in other countries.
Parathion
The insecticide parathion was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals.
Researchers have observed associations between the insecticide and cancers in several tissues in occupational studies. But the IARC said the evidence that parathion is carcinogenic in humans remains sparse.
Experiments in mice showed that parathion increased the incidence of bronchioloalveolar adenoma and/or carcinoma in males and lymphoma in females. In rats, parathion induced adrenal cortical adenoma or carcinoma (combined), malignant pancreatic tumors, and thyroid follicular cell adenoma in males, and mammary gland adenocarcinoma (after subcutaneous injection in females).
Parathion use has been severely restricted since the 1980s, and all authorized uses of this chemical were cancelled in the EU and the US by 2003. ![]()
Photo by John Messina
The International Agency for Research on Cancer (IARC), the specialized cancer agency of the World Health Organization, has found evidence suggesting that 5 organophosphate pesticides may be carcinogenic.
The IARC classified the herbicide glyphosate and the insecticides malathion and diazinon as “probably carcinogenic” to humans and the insecticides tetrachlorvinphos and parathion as “possibly carcinogenic” to humans.
A summary of these findings has been published in The Lancet Oncology.
Glyphosate
For the herbicide glyphosate, the IARC found limited evidence of carcinogenicity in humans. Case-control studies of occupational exposure to glyphosate in the US, Canada, and Sweden showed increased risks for non-Hodgkin lymphoma (NHL).
However, the Agricultural Health Study (AHS) showed no significantly increased risk of NHL in subjects exposed to glyphosate.
A study of community residents showed increases in blood markers of chromosomal damage after glyphosate formulations were sprayed nearby. And glyphosate was shown to cause DNA and chromosomal damage in human cells, although bacterial mutagenesis tests were negative.
In studies of male mice, glyphosate increased the incidence of renal tubule carcinoma and hemangiosarcoma. Glyphosate also increased the incidence of pancreatic islet-cell adenoma in male rats, and a glyphosate formulation promoted skin tumors in mice.
The IARC said glyphosate has the highest global production volume of all herbicides. It is used in agriculture, forestry, urban, and home applications.
Glyphosate has been detected in the air during spraying, in water, and in food. The general population is exposed to the chemical primarily by living near sprayed areas, home use, and diet. But the IARC said the level of exposure observed is generally low.
Malathion
The IARC classified malathion as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL and prostate cancer. Occupational use of malathion was associated with an increased risk of prostate cancer in a Canadian case-control study and in the AHS.
Studies of occupational exposures in the US, Canada, and Sweden revealed positive associations between malathion and NHL. However, results of the AHS did not show an association between the insecticide and NHL.
Studies showed that malathion induced DNA and chromosomal damage in humans and animals, although bacterial mutagenesis tests were negative. Results also suggested malathion disrupts hormone pathways.
Experiments in mice showed malathion increased the incidence of hepatocellular adenoma or carcinoma (combined). In rats, the insecticide increased the incidence of thyroid carcinoma in males, hepatocellular adenoma or carcinoma (combined) in females, and mammary gland adenocarcinoma after subcutaneous injection in females.
The IARC said malathion is used in “substantial volumes throughout the world” to control insects in agricultural and residential areas.
Workers may be exposed to malathion during the use and production of the product. The general population may be exposed if they live near sprayed areas, use the product at home, or consume food exposed to the chemical.
Diazinon
The IARC classified diazinon as “probably carcinogenic” for humans based on limited evidence linking the insecticide to NHL, leukemia, and lung cancer.
Two multicenter, case-control studies of agricultural exposures suggested a positive association between diazinon and NHL. The AHS showed positive associations with specific subtypes of NHL but no overall increased risk of NHL. The AHS also suggested an increased risk of leukemia and lung cancer in subjects exposed to diazinon.
Evidence suggested that diazinon induced DNA or chromosomal damage in human and mammalian cells in vitro. In vivo, diazinon increased the incidence of hepatocellular carcinoma in mice and leukemia or lymphoma (combined) in rats, but only in males receiving the low dose in each study.
Diazinon has been used to control insects in agricultural and residential areas. The IARC said production volumes have been relatively low and decreased further after 2006 due to restrictions in the US and the European Union (EU). There was limited information on the use of this pesticide in other countries.
Tetrachlorvinphos
The insecticide tetrachlorvinphos was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals. The IARC said the evidence in humans was inadequate.
However, tetrachlorvinphos was shown to induce hepatocellular tumors (benign or malignant) in mice, renal tubule tumors (benign or malignant) in male mice, and spleen hemangioma in male rats.
Tetrachlorvinphos is banned in the EU. In the US, the insecticide is still used on livestock and pets (in flea collars). The IARC said there was no information available on tetrachlorvinphos use in other countries.
Parathion
The insecticide parathion was classified as “possibly carcinogenic” to humans based on convincing evidence that the agent causes cancer in lab animals.
Researchers have observed associations between the insecticide and cancers in several tissues in occupational studies. But the IARC said the evidence that parathion is carcinogenic in humans remains sparse.
Experiments in mice showed that parathion increased the incidence of bronchioloalveolar adenoma and/or carcinoma in males and lymphoma in females. In rats, parathion induced adrenal cortical adenoma or carcinoma (combined), malignant pancreatic tumors, and thyroid follicular cell adenoma in males, and mammary gland adenocarcinoma (after subcutaneous injection in females).
Parathion use has been severely restricted since the 1980s, and all authorized uses of this chemical were cancelled in the EU and the US by 2003. ![]()
Studies investigate risk of DVT, infection with PICCs
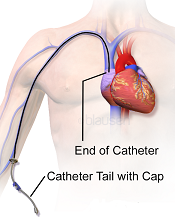
Image courtesy of Blausen
Medical Communications, Inc.
Three recently published papers may help ensure the appropriate use of peripherally inserted central catheters (PICCs).
A case-control study uncovered several factors that appear to affect the risk of deep vein thrombosis (DVT) associated with PICCs.
A retrospective study revealed the “prevalence, patterns, and predictors” of PICC-associated bloodstream infections.
And a literature review informed the creation of a guide to help hospitalists choose the right intravenous device.
“[PICCs] are very popular, but in an under-the-radar way, because they make care more convenient and can be placed relatively easily,” said Vineet Chopra, MD, an author on all 3 articles and a hospitalist at the University of Michigan Health System in Ann Arbor.
“But our new results, and review of research on the topic, show it’s important for physicians to think hard about both the risks and the benefits.”
Case-control study
In the study of PICC-DVT, published in Thrombosis Research, the investigators looked at records from 909 patients who received PICCs at the University of Michigan Health System in 2012 and 2013.
Patients had PICCs placed so they could receive long-term intravenous antibiotic therapy (n=447; 49.1%) or total parenteral nutrition (n=120; 6.7%). They also required PICCs for in-hospital venous access for blood draws or infusion of medications (n=342; 44.2%).
In all, 268 patients developed a DVT associated with their PICC. The median time to DVT development was 12.4 days from PICC placement.
Patients who were already taking aspirin and statins before their PICC was placed had a significantly lower risk of DVT-PICC (odds ratio [OR]=0.31). Patients who received pharmacological DVT prophylaxis had a lower risk of DVT-PICC than patients who were not on prophylaxis, although the difference was not statistically significant (OR=0.72).
Patients had a significantly greater risk of PICC-DVT if they underwent surgery during their hospital stay (OR=2.17) or had a prior history of venous thromboembolism (OR=1.70). And, compared to patients who received 4-Fr PICCs, those who had 5-Fr or 6-Fr PICCs had a significantly greater risk of DVT (ORs=2.74 and 7.40, respectively).
Retrospective study
In The American Journal of Medicine, Dr Chopra and his colleagues described a retrospective study of bloodstream infections associated with PICCs.
The investigators analyzed data from 747 patients who received 966 PICCs for a total of 26,887 catheter days. Patients had PICCs for long-term antibiotic administration (n=503; 52%), venous access (n=201; 21%), total parenteral nutrition (n=155; 16%), and chemotherapy (n=107; 11%).
There were 58 cases (6%) of PICC-bloodstream infection over 1156 catheter days, for an infection rate of 2.16 per 1000 catheter days. The median time to infection was 10 days.
Bivariate analysis revealed several factors associated with PICC-bloodstream infections. These included intensive care unit status (ICU; OR=3.23), mechanical ventilation (OR=4.39), length of stay (hospital, OR=1.04; ICU, OR=1.03), PowerPICCs (OR=2.58), devices placed by interventional radiology (OR=2.57), double lumens (OR=5.21), and triple lumens (OR=10.84).
In multivariable analysis, only some of these factors remained significantly associated with PICC-bloodstream infection. These included hospital length of stay (OR=1.04), ICU status (OR=1.02), double lumens (OR=3.99), and triple lumens (OR=6.34).
Dr Chopra said the results of these 2 studies suggest hospitalists should tread carefully when considering PICCs.
“These are not innocuous devices,” he said. “The time has come to stop thinking of them as a device of convenience and rather one with clear risks and benefits.”
Review and guide
In the Journal of Hospital Medicine, Dr Chopra and his colleagues offered advice on choosing vascular access devices. After reviewing the literature, the investigators designed a flow chart that can help hospitalists decide which device is appropriate for each patient.
For instance, different devices will work best depending on whether access to the bloodstream is needed urgently or less urgently, whether the patient will likely need the device for more or less than a week, what kind of drug or nutrition the doctor will order, and whether the patient’s kidneys are functioning normally. ![]()
Image courtesy of Blausen
Medical Communications, Inc.
Three recently published papers may help ensure the appropriate use of peripherally inserted central catheters (PICCs).
A case-control study uncovered several factors that appear to affect the risk of deep vein thrombosis (DVT) associated with PICCs.
A retrospective study revealed the “prevalence, patterns, and predictors” of PICC-associated bloodstream infections.
And a literature review informed the creation of a guide to help hospitalists choose the right intravenous device.
“[PICCs] are very popular, but in an under-the-radar way, because they make care more convenient and can be placed relatively easily,” said Vineet Chopra, MD, an author on all 3 articles and a hospitalist at the University of Michigan Health System in Ann Arbor.
“But our new results, and review of research on the topic, show it’s important for physicians to think hard about both the risks and the benefits.”
Case-control study
In the study of PICC-DVT, published in Thrombosis Research, the investigators looked at records from 909 patients who received PICCs at the University of Michigan Health System in 2012 and 2013.
Patients had PICCs placed so they could receive long-term intravenous antibiotic therapy (n=447; 49.1%) or total parenteral nutrition (n=120; 6.7%). They also required PICCs for in-hospital venous access for blood draws or infusion of medications (n=342; 44.2%).
In all, 268 patients developed a DVT associated with their PICC. The median time to DVT development was 12.4 days from PICC placement.
Patients who were already taking aspirin and statins before their PICC was placed had a significantly lower risk of DVT-PICC (odds ratio [OR]=0.31). Patients who received pharmacological DVT prophylaxis had a lower risk of DVT-PICC than patients who were not on prophylaxis, although the difference was not statistically significant (OR=0.72).
Patients had a significantly greater risk of PICC-DVT if they underwent surgery during their hospital stay (OR=2.17) or had a prior history of venous thromboembolism (OR=1.70). And, compared to patients who received 4-Fr PICCs, those who had 5-Fr or 6-Fr PICCs had a significantly greater risk of DVT (ORs=2.74 and 7.40, respectively).
Retrospective study
In The American Journal of Medicine, Dr Chopra and his colleagues described a retrospective study of bloodstream infections associated with PICCs.
The investigators analyzed data from 747 patients who received 966 PICCs for a total of 26,887 catheter days. Patients had PICCs for long-term antibiotic administration (n=503; 52%), venous access (n=201; 21%), total parenteral nutrition (n=155; 16%), and chemotherapy (n=107; 11%).
There were 58 cases (6%) of PICC-bloodstream infection over 1156 catheter days, for an infection rate of 2.16 per 1000 catheter days. The median time to infection was 10 days.
Bivariate analysis revealed several factors associated with PICC-bloodstream infections. These included intensive care unit status (ICU; OR=3.23), mechanical ventilation (OR=4.39), length of stay (hospital, OR=1.04; ICU, OR=1.03), PowerPICCs (OR=2.58), devices placed by interventional radiology (OR=2.57), double lumens (OR=5.21), and triple lumens (OR=10.84).
In multivariable analysis, only some of these factors remained significantly associated with PICC-bloodstream infection. These included hospital length of stay (OR=1.04), ICU status (OR=1.02), double lumens (OR=3.99), and triple lumens (OR=6.34).
Dr Chopra said the results of these 2 studies suggest hospitalists should tread carefully when considering PICCs.
“These are not innocuous devices,” he said. “The time has come to stop thinking of them as a device of convenience and rather one with clear risks and benefits.”
Review and guide
In the Journal of Hospital Medicine, Dr Chopra and his colleagues offered advice on choosing vascular access devices. After reviewing the literature, the investigators designed a flow chart that can help hospitalists decide which device is appropriate for each patient.
For instance, different devices will work best depending on whether access to the bloodstream is needed urgently or less urgently, whether the patient will likely need the device for more or less than a week, what kind of drug or nutrition the doctor will order, and whether the patient’s kidneys are functioning normally. ![]()
Image courtesy of Blausen
Medical Communications, Inc.
Three recently published papers may help ensure the appropriate use of peripherally inserted central catheters (PICCs).
A case-control study uncovered several factors that appear to affect the risk of deep vein thrombosis (DVT) associated with PICCs.
A retrospective study revealed the “prevalence, patterns, and predictors” of PICC-associated bloodstream infections.
And a literature review informed the creation of a guide to help hospitalists choose the right intravenous device.
“[PICCs] are very popular, but in an under-the-radar way, because they make care more convenient and can be placed relatively easily,” said Vineet Chopra, MD, an author on all 3 articles and a hospitalist at the University of Michigan Health System in Ann Arbor.
“But our new results, and review of research on the topic, show it’s important for physicians to think hard about both the risks and the benefits.”
Case-control study
In the study of PICC-DVT, published in Thrombosis Research, the investigators looked at records from 909 patients who received PICCs at the University of Michigan Health System in 2012 and 2013.
Patients had PICCs placed so they could receive long-term intravenous antibiotic therapy (n=447; 49.1%) or total parenteral nutrition (n=120; 6.7%). They also required PICCs for in-hospital venous access for blood draws or infusion of medications (n=342; 44.2%).
In all, 268 patients developed a DVT associated with their PICC. The median time to DVT development was 12.4 days from PICC placement.
Patients who were already taking aspirin and statins before their PICC was placed had a significantly lower risk of DVT-PICC (odds ratio [OR]=0.31). Patients who received pharmacological DVT prophylaxis had a lower risk of DVT-PICC than patients who were not on prophylaxis, although the difference was not statistically significant (OR=0.72).
Patients had a significantly greater risk of PICC-DVT if they underwent surgery during their hospital stay (OR=2.17) or had a prior history of venous thromboembolism (OR=1.70). And, compared to patients who received 4-Fr PICCs, those who had 5-Fr or 6-Fr PICCs had a significantly greater risk of DVT (ORs=2.74 and 7.40, respectively).
Retrospective study
In The American Journal of Medicine, Dr Chopra and his colleagues described a retrospective study of bloodstream infections associated with PICCs.
The investigators analyzed data from 747 patients who received 966 PICCs for a total of 26,887 catheter days. Patients had PICCs for long-term antibiotic administration (n=503; 52%), venous access (n=201; 21%), total parenteral nutrition (n=155; 16%), and chemotherapy (n=107; 11%).
There were 58 cases (6%) of PICC-bloodstream infection over 1156 catheter days, for an infection rate of 2.16 per 1000 catheter days. The median time to infection was 10 days.
Bivariate analysis revealed several factors associated with PICC-bloodstream infections. These included intensive care unit status (ICU; OR=3.23), mechanical ventilation (OR=4.39), length of stay (hospital, OR=1.04; ICU, OR=1.03), PowerPICCs (OR=2.58), devices placed by interventional radiology (OR=2.57), double lumens (OR=5.21), and triple lumens (OR=10.84).
In multivariable analysis, only some of these factors remained significantly associated with PICC-bloodstream infection. These included hospital length of stay (OR=1.04), ICU status (OR=1.02), double lumens (OR=3.99), and triple lumens (OR=6.34).
Dr Chopra said the results of these 2 studies suggest hospitalists should tread carefully when considering PICCs.
“These are not innocuous devices,” he said. “The time has come to stop thinking of them as a device of convenience and rather one with clear risks and benefits.”
Review and guide
In the Journal of Hospital Medicine, Dr Chopra and his colleagues offered advice on choosing vascular access devices. After reviewing the literature, the investigators designed a flow chart that can help hospitalists decide which device is appropriate for each patient.
For instance, different devices will work best depending on whether access to the bloodstream is needed urgently or less urgently, whether the patient will likely need the device for more or less than a week, what kind of drug or nutrition the doctor will order, and whether the patient’s kidneys are functioning normally. ![]()
Team describes new method to target MM cells

Researchers say they have discovered a new way to target multiple myeloma (MM) and other cancer cells.
The investigators developed human T-cell receptors (TCRs) that have no tolerance toward human cancer antigens and specifically recognize the antigen MAGE-A1, which is present on MM and other cancer cells.
Matthias Obenaus, MD, of the Max-Delbrück-Center for Molecular Medicine in Berlin, Germany, and his colleagues described this work in Nature Biotechnology.
Instead of directly using human-derived TCRs, which do not mediate substantial anti-tumor effects, the researchers took a “detour” by employing a mouse model.
First, they transferred the genetic information for human TCRs into the mice, thereby creating an arsenal of human TCRs.
Then, the investigators isolated the TCRs from the mice and transferred them into human T cells. This “trained” the cells to recognize MM and other cancer cells (eg, melanoma and fibrosarcoma cells) as foreign.
The researchers noted that some people possess T cells that naturally recognize MAGE-A1 on tumor cells, but only in vitro.
In vivo experiments revealed that only the human TCRs derived from mice were effective against tumors. The TCRs derived directly from humans were too weak to recognize the tumor antigens sufficiently.
The investigators said the fact that their mouse-derived human TCRs were more effective is a strong indication that human T cells are tolerant toward MAGE-A1.
Using the TCRs they developed, the researchers are now planning a clinical trial of patients with MAGE-A1 positive MM. ![]()
Researchers say they have discovered a new way to target multiple myeloma (MM) and other cancer cells.
The investigators developed human T-cell receptors (TCRs) that have no tolerance toward human cancer antigens and specifically recognize the antigen MAGE-A1, which is present on MM and other cancer cells.
Matthias Obenaus, MD, of the Max-Delbrück-Center for Molecular Medicine in Berlin, Germany, and his colleagues described this work in Nature Biotechnology.
Instead of directly using human-derived TCRs, which do not mediate substantial anti-tumor effects, the researchers took a “detour” by employing a mouse model.
First, they transferred the genetic information for human TCRs into the mice, thereby creating an arsenal of human TCRs.
Then, the investigators isolated the TCRs from the mice and transferred them into human T cells. This “trained” the cells to recognize MM and other cancer cells (eg, melanoma and fibrosarcoma cells) as foreign.
The researchers noted that some people possess T cells that naturally recognize MAGE-A1 on tumor cells, but only in vitro.
In vivo experiments revealed that only the human TCRs derived from mice were effective against tumors. The TCRs derived directly from humans were too weak to recognize the tumor antigens sufficiently.
The investigators said the fact that their mouse-derived human TCRs were more effective is a strong indication that human T cells are tolerant toward MAGE-A1.
Using the TCRs they developed, the researchers are now planning a clinical trial of patients with MAGE-A1 positive MM. ![]()
Researchers say they have discovered a new way to target multiple myeloma (MM) and other cancer cells.
The investigators developed human T-cell receptors (TCRs) that have no tolerance toward human cancer antigens and specifically recognize the antigen MAGE-A1, which is present on MM and other cancer cells.
Matthias Obenaus, MD, of the Max-Delbrück-Center for Molecular Medicine in Berlin, Germany, and his colleagues described this work in Nature Biotechnology.
Instead of directly using human-derived TCRs, which do not mediate substantial anti-tumor effects, the researchers took a “detour” by employing a mouse model.
First, they transferred the genetic information for human TCRs into the mice, thereby creating an arsenal of human TCRs.
Then, the investigators isolated the TCRs from the mice and transferred them into human T cells. This “trained” the cells to recognize MM and other cancer cells (eg, melanoma and fibrosarcoma cells) as foreign.
The researchers noted that some people possess T cells that naturally recognize MAGE-A1 on tumor cells, but only in vitro.
In vivo experiments revealed that only the human TCRs derived from mice were effective against tumors. The TCRs derived directly from humans were too weak to recognize the tumor antigens sufficiently.
The investigators said the fact that their mouse-derived human TCRs were more effective is a strong indication that human T cells are tolerant toward MAGE-A1.
Using the TCRs they developed, the researchers are now planning a clinical trial of patients with MAGE-A1 positive MM. ![]()
Pathway appears critical to HSC aging

in the bone marrow
Scientists say they’ve identified a molecular pathway that is critical to hematopoietic stem cell (HSC) aging and can be manipulated to rejuvenate blood.
The researchers found that HSCs’ ability to repair damage caused by inappropriate protein folding in the mitochondria is essential for the cells’ survival and regenerative capacity.
The discovery has implications for research on reversing the signs of aging, a process thought to be caused by increased cellular stress and damage.
“Ultimately, a cell dies when it can’t deal well with stress,” said study author Danica Chen, PhD, of the University of California, Berkeley.
“We found that by slowing down the activity of mitochondria in the blood stem cells of mice, we were able to enhance their capacity to handle stress and rejuvenate old blood. This confirms the significance of this pathway in the aging process.”
Mitochondria host a multitude of proteins that must be folded properly to function correctly. When the folding goes awry, the mitochondrial unfolded-protein response (UPRmt) kicks in to boost the production of specific proteins to fix or remove the misfolded protein.
There has been little research on the UPRmt pathway, but studies in roundworms suggest its activity increases when there is a burst of mitochondrial growth.
Dr Chen and her colleagues noted that adult stem cells are normally in a quiescent state with little mitochondrial activity. They are activated only when needed to replenish tissue.
At that time, the mitochondrial activity increases, and stem cells proliferate and differentiate. When protein-folding problems occur, this fast growth could lead to more harm.
Dr Chen’s lab stumbled upon the importance of UPRmt in HSC aging while studying sirtuins, a class of proteins recognized as stress-resistance regulators.
The researchers noticed that levels of one particular sirtuin, SIRT7, increase as a way to help cells cope with stress from misfolded proteins in the mitochondria. But SIRT7 levels decline with age.
“We isolated blood stem cells from aged mice and found that when we increased the levels of SIRT7, we were able to reduce mitochondrial protein-folding stress,” Dr Chen said. “We then transplanted the blood stem cells back into mice, and SIRT7 improved the blood stem cells’ regenerative capacity.”
The researchers also found that HSCs deficient in SIRT7 proliferate more. This faster growth is due to increased protein production and increased activity of the mitochondria, and slowing things down appears to be a critical step in giving cells time to recover from stress.
Dr Chen likened this to an auto accident or stalled car stopping traffic on a freeway.
“When there’s a mitochondrial protein-folding problem, there is a traffic jam in the mitochondria,” she said. “If you prevent more proteins from being created and added to the mitochondria, you are helping to reduce the jam.”
Until this study, it was unclear which stress signals regulate HSCs’ transition to and from the quiescent state and how that related to tissue regeneration during aging.
“Identifying the role of this mitochondrial pathway in blood stem cells gives us a new target for controlling the aging process,” Dr Chen said.
She and her colleagues described this work in Science. ![]()
in the bone marrow
Scientists say they’ve identified a molecular pathway that is critical to hematopoietic stem cell (HSC) aging and can be manipulated to rejuvenate blood.
The researchers found that HSCs’ ability to repair damage caused by inappropriate protein folding in the mitochondria is essential for the cells’ survival and regenerative capacity.
The discovery has implications for research on reversing the signs of aging, a process thought to be caused by increased cellular stress and damage.
“Ultimately, a cell dies when it can’t deal well with stress,” said study author Danica Chen, PhD, of the University of California, Berkeley.
“We found that by slowing down the activity of mitochondria in the blood stem cells of mice, we were able to enhance their capacity to handle stress and rejuvenate old blood. This confirms the significance of this pathway in the aging process.”
Mitochondria host a multitude of proteins that must be folded properly to function correctly. When the folding goes awry, the mitochondrial unfolded-protein response (UPRmt) kicks in to boost the production of specific proteins to fix or remove the misfolded protein.
There has been little research on the UPRmt pathway, but studies in roundworms suggest its activity increases when there is a burst of mitochondrial growth.
Dr Chen and her colleagues noted that adult stem cells are normally in a quiescent state with little mitochondrial activity. They are activated only when needed to replenish tissue.
At that time, the mitochondrial activity increases, and stem cells proliferate and differentiate. When protein-folding problems occur, this fast growth could lead to more harm.
Dr Chen’s lab stumbled upon the importance of UPRmt in HSC aging while studying sirtuins, a class of proteins recognized as stress-resistance regulators.
The researchers noticed that levels of one particular sirtuin, SIRT7, increase as a way to help cells cope with stress from misfolded proteins in the mitochondria. But SIRT7 levels decline with age.
“We isolated blood stem cells from aged mice and found that when we increased the levels of SIRT7, we were able to reduce mitochondrial protein-folding stress,” Dr Chen said. “We then transplanted the blood stem cells back into mice, and SIRT7 improved the blood stem cells’ regenerative capacity.”
The researchers also found that HSCs deficient in SIRT7 proliferate more. This faster growth is due to increased protein production and increased activity of the mitochondria, and slowing things down appears to be a critical step in giving cells time to recover from stress.
Dr Chen likened this to an auto accident or stalled car stopping traffic on a freeway.
“When there’s a mitochondrial protein-folding problem, there is a traffic jam in the mitochondria,” she said. “If you prevent more proteins from being created and added to the mitochondria, you are helping to reduce the jam.”
Until this study, it was unclear which stress signals regulate HSCs’ transition to and from the quiescent state and how that related to tissue regeneration during aging.
“Identifying the role of this mitochondrial pathway in blood stem cells gives us a new target for controlling the aging process,” Dr Chen said.
She and her colleagues described this work in Science. ![]()
in the bone marrow
Scientists say they’ve identified a molecular pathway that is critical to hematopoietic stem cell (HSC) aging and can be manipulated to rejuvenate blood.
The researchers found that HSCs’ ability to repair damage caused by inappropriate protein folding in the mitochondria is essential for the cells’ survival and regenerative capacity.
The discovery has implications for research on reversing the signs of aging, a process thought to be caused by increased cellular stress and damage.
“Ultimately, a cell dies when it can’t deal well with stress,” said study author Danica Chen, PhD, of the University of California, Berkeley.
“We found that by slowing down the activity of mitochondria in the blood stem cells of mice, we were able to enhance their capacity to handle stress and rejuvenate old blood. This confirms the significance of this pathway in the aging process.”
Mitochondria host a multitude of proteins that must be folded properly to function correctly. When the folding goes awry, the mitochondrial unfolded-protein response (UPRmt) kicks in to boost the production of specific proteins to fix or remove the misfolded protein.
There has been little research on the UPRmt pathway, but studies in roundworms suggest its activity increases when there is a burst of mitochondrial growth.
Dr Chen and her colleagues noted that adult stem cells are normally in a quiescent state with little mitochondrial activity. They are activated only when needed to replenish tissue.
At that time, the mitochondrial activity increases, and stem cells proliferate and differentiate. When protein-folding problems occur, this fast growth could lead to more harm.
Dr Chen’s lab stumbled upon the importance of UPRmt in HSC aging while studying sirtuins, a class of proteins recognized as stress-resistance regulators.
The researchers noticed that levels of one particular sirtuin, SIRT7, increase as a way to help cells cope with stress from misfolded proteins in the mitochondria. But SIRT7 levels decline with age.
“We isolated blood stem cells from aged mice and found that when we increased the levels of SIRT7, we were able to reduce mitochondrial protein-folding stress,” Dr Chen said. “We then transplanted the blood stem cells back into mice, and SIRT7 improved the blood stem cells’ regenerative capacity.”
The researchers also found that HSCs deficient in SIRT7 proliferate more. This faster growth is due to increased protein production and increased activity of the mitochondria, and slowing things down appears to be a critical step in giving cells time to recover from stress.
Dr Chen likened this to an auto accident or stalled car stopping traffic on a freeway.
“When there’s a mitochondrial protein-folding problem, there is a traffic jam in the mitochondria,” she said. “If you prevent more proteins from being created and added to the mitochondria, you are helping to reduce the jam.”
Until this study, it was unclear which stress signals regulate HSCs’ transition to and from the quiescent state and how that related to tissue regeneration during aging.
“Identifying the role of this mitochondrial pathway in blood stem cells gives us a new target for controlling the aging process,” Dr Chen said.
She and her colleagues described this work in Science.
Predicting pregnancy complications in SCD patients

Photo by Nina Matthews
Results of a new analysis may help physicians predict the likelihood of complications in pregnant women with sickle cell disease (SCD).
The research showed that pregnant women with SCD had an increased risk of stillbirth, pre-eclampsia, preterm delivery, having infants who were born small for their gestational age, and other adverse outcomes.
Women with severe SCD, but not those with milder SCD, had a substantially higher risk of mortality than their healthy peers.
Researchers reported these findings in Blood.
“While we know that women with sickle cell disease will have high-risk pregnancies, we have lacked the evidence that would allow us to confidently tell these patients how likely they are to experience one complication over another,” said study author Eugene Oteng-Ntim, MD, of the Guy’s and St. Thomas’ NHS Foundation Trust in London, England.
“This reality makes it difficult for us as care providers to properly counsel our sickle cell patients considering pregnancy.”
To better estimate pregnancy-related complications in women with SCD, Dr Oteng-Ntim and his colleagues examined 21 published observational studies.
The team analyzed data on 26,349 pregnant women with SCD and 26,151,746 pregnant women who shared attributes with the SCD population, such as ethnicity or location, but were otherwise healthy.
The researchers classified the SCD population based on genotype, including 1276 women with the classic form (HbSS genotype), 279 with a milder form (HbSC genotype), and 24,794 whose disease genotype was unreported (non-specified SCD).
Thirteen of the studies originated from high-income countries ($30,000 income per capita or greater), and the remaining were from low- to median-income countries.
Compared to women without SCD, patients with HbSS genotype had an increased risk of death, with a risk ratio (RR) of 5.98. Women with non-specified SCD had an increased risk of death as well, with an RR of 18.51. There was only 1 death among women who were known to have HbSC SCD.
There was an increased risk of stillbirth among women with SCD, compared to those without the disease. The RRs were 3.94 for HbSS disease, 1.78 for HbSC disease, and 3.49 for non-specified SCD.
The researchers found a significantly lower risk of maternal mortality (odds ratio [OR]=0.15) and stillbirth (OR=0.28) in SCD patients from countries with a gross national income of $30,000 or greater. But income had no significant impact on pre-eclampsia, preterm delivery, or infants being small for their gestational age.
Women with all types of SCD had an increase in the risk of pre-eclampsia, compared to healthy women. The RRs were 2.43 for HbSS disease, 2.03 for HbSC disease, and 2.06 for non-specified SCD.
Women with SCD also had an increased risk of preterm delivery. The RRs were 2.21 for HbSS disease, 1.45 for HbSC disease, and 1.59 for non-specified SCD.
And women with SCD were more likely to have infants who were born small for their gestational age. The RRs were 3.72 for HbSS disease, 1.98 for HbSC disease, and 2.23 for non-specified SCD.
Analyses revealed that genotype (HbSS vs HbSC) had a significant impact on stillbirth, preterm delivery, and small infants, but it did not appear to impact the risk of pre-eclampsia.
The researchers said this study provides useful estimates of the morbidity and mortality associated with SCD in pregnancy.
“By improving care providers’ ability to more accurately predict adverse outcomes, this analysis is a first step toward improving universal care for all who suffer from this disease,” Dr Oteng-Ntim concluded.
Photo by Nina Matthews
Results of a new analysis may help physicians predict the likelihood of complications in pregnant women with sickle cell disease (SCD).
The research showed that pregnant women with SCD had an increased risk of stillbirth, pre-eclampsia, preterm delivery, having infants who were born small for their gestational age, and other adverse outcomes.
Women with severe SCD, but not those with milder SCD, had a substantially higher risk of mortality than their healthy peers.
Researchers reported these findings in Blood.
“While we know that women with sickle cell disease will have high-risk pregnancies, we have lacked the evidence that would allow us to confidently tell these patients how likely they are to experience one complication over another,” said study author Eugene Oteng-Ntim, MD, of the Guy’s and St. Thomas’ NHS Foundation Trust in London, England.
“This reality makes it difficult for us as care providers to properly counsel our sickle cell patients considering pregnancy.”
To better estimate pregnancy-related complications in women with SCD, Dr Oteng-Ntim and his colleagues examined 21 published observational studies.
The team analyzed data on 26,349 pregnant women with SCD and 26,151,746 pregnant women who shared attributes with the SCD population, such as ethnicity or location, but were otherwise healthy.
The researchers classified the SCD population based on genotype, including 1276 women with the classic form (HbSS genotype), 279 with a milder form (HbSC genotype), and 24,794 whose disease genotype was unreported (non-specified SCD).
Thirteen of the studies originated from high-income countries ($30,000 income per capita or greater), and the remaining were from low- to median-income countries.
Compared to women without SCD, patients with HbSS genotype had an increased risk of death, with a risk ratio (RR) of 5.98. Women with non-specified SCD had an increased risk of death as well, with an RR of 18.51. There was only 1 death among women who were known to have HbSC SCD.
There was an increased risk of stillbirth among women with SCD, compared to those without the disease. The RRs were 3.94 for HbSS disease, 1.78 for HbSC disease, and 3.49 for non-specified SCD.
The researchers found a significantly lower risk of maternal mortality (odds ratio [OR]=0.15) and stillbirth (OR=0.28) in SCD patients from countries with a gross national income of $30,000 or greater. But income had no significant impact on pre-eclampsia, preterm delivery, or infants being small for their gestational age.
Women with all types of SCD had an increase in the risk of pre-eclampsia, compared to healthy women. The RRs were 2.43 for HbSS disease, 2.03 for HbSC disease, and 2.06 for non-specified SCD.
Women with SCD also had an increased risk of preterm delivery. The RRs were 2.21 for HbSS disease, 1.45 for HbSC disease, and 1.59 for non-specified SCD.
And women with SCD were more likely to have infants who were born small for their gestational age. The RRs were 3.72 for HbSS disease, 1.98 for HbSC disease, and 2.23 for non-specified SCD.
Analyses revealed that genotype (HbSS vs HbSC) had a significant impact on stillbirth, preterm delivery, and small infants, but it did not appear to impact the risk of pre-eclampsia.
The researchers said this study provides useful estimates of the morbidity and mortality associated with SCD in pregnancy.
“By improving care providers’ ability to more accurately predict adverse outcomes, this analysis is a first step toward improving universal care for all who suffer from this disease,” Dr Oteng-Ntim concluded.
Photo by Nina Matthews
Results of a new analysis may help physicians predict the likelihood of complications in pregnant women with sickle cell disease (SCD).
The research showed that pregnant women with SCD had an increased risk of stillbirth, pre-eclampsia, preterm delivery, having infants who were born small for their gestational age, and other adverse outcomes.
Women with severe SCD, but not those with milder SCD, had a substantially higher risk of mortality than their healthy peers.
Researchers reported these findings in Blood.
“While we know that women with sickle cell disease will have high-risk pregnancies, we have lacked the evidence that would allow us to confidently tell these patients how likely they are to experience one complication over another,” said study author Eugene Oteng-Ntim, MD, of the Guy’s and St. Thomas’ NHS Foundation Trust in London, England.
“This reality makes it difficult for us as care providers to properly counsel our sickle cell patients considering pregnancy.”
To better estimate pregnancy-related complications in women with SCD, Dr Oteng-Ntim and his colleagues examined 21 published observational studies.
The team analyzed data on 26,349 pregnant women with SCD and 26,151,746 pregnant women who shared attributes with the SCD population, such as ethnicity or location, but were otherwise healthy.
The researchers classified the SCD population based on genotype, including 1276 women with the classic form (HbSS genotype), 279 with a milder form (HbSC genotype), and 24,794 whose disease genotype was unreported (non-specified SCD).
Thirteen of the studies originated from high-income countries ($30,000 income per capita or greater), and the remaining were from low- to median-income countries.
Compared to women without SCD, patients with HbSS genotype had an increased risk of death, with a risk ratio (RR) of 5.98. Women with non-specified SCD had an increased risk of death as well, with an RR of 18.51. There was only 1 death among women who were known to have HbSC SCD.
There was an increased risk of stillbirth among women with SCD, compared to those without the disease. The RRs were 3.94 for HbSS disease, 1.78 for HbSC disease, and 3.49 for non-specified SCD.
The researchers found a significantly lower risk of maternal mortality (odds ratio [OR]=0.15) and stillbirth (OR=0.28) in SCD patients from countries with a gross national income of $30,000 or greater. But income had no significant impact on pre-eclampsia, preterm delivery, or infants being small for their gestational age.
Women with all types of SCD had an increase in the risk of pre-eclampsia, compared to healthy women. The RRs were 2.43 for HbSS disease, 2.03 for HbSC disease, and 2.06 for non-specified SCD.
Women with SCD also had an increased risk of preterm delivery. The RRs were 2.21 for HbSS disease, 1.45 for HbSC disease, and 1.59 for non-specified SCD.
And women with SCD were more likely to have infants who were born small for their gestational age. The RRs were 3.72 for HbSS disease, 1.98 for HbSC disease, and 2.23 for non-specified SCD.
Analyses revealed that genotype (HbSS vs HbSC) had a significant impact on stillbirth, preterm delivery, and small infants, but it did not appear to impact the risk of pre-eclampsia.
The researchers said this study provides useful estimates of the morbidity and mortality associated with SCD in pregnancy.
“By improving care providers’ ability to more accurately predict adverse outcomes, this analysis is a first step toward improving universal care for all who suffer from this disease,” Dr Oteng-Ntim concluded.
Drug granted orphan designation for GVHD

The European Commission has granted orphan drug designation for intravenous (IV) alpha-1 antitrypsin (AAT) to treat graft-versus-host disease (GVHD).
AAT is a protein derived from human plasma that has demonstrated immunomodulatory, anti-inflammatory, tissue-protective, antimicrobial, and anti-apoptotic properties.
AAT may attenuate inflammation by lowering levels of pro-inflammatory mediators such as cytokines, chemokines, and proteases associated with GVHD.
The European Commission granted IV AAT orphan designation based on preliminary clinical and preclinical research.
Orphan designation is granted to a medicine intended to treat a rare condition occurring in not more than 5 in 10,000 people in the European Union. The designation allows the drug’s maker to benefit from incentives such as a 10-year period of market exclusivity, reduced regulatory fees, and protocol assistance from the European Medicines Agency.
IV AAT also has orphan designation to treat GVHD in the US.
Studies of AAT
AAT is being investigated in a phase 1/2 study involving 24 patients with GVHD who had an inadequate response to steroid treatment. The patients are enrolled in 4 dose cohorts, in which they receive up to 8 doses of AAT.
Interim results from this study were presented at the 2014 ASH Annual Meeting (abstract 3927). Preliminary results indicated that continuous administration of AAT as therapy for steroid-resistant gut GVHD is feasible in the subject population.
Following AAT administration, the researchers observed a decrease in diarrhea, a decrease in intestinal AAT loss, and improvement in endoscopic evaluation. In addition, AAT administration suppressed serum levels of pro-inflammatory cytokines and interfered with GVHD biomarkers.
Investigators have also published research on AAT in Blood. This study suggested that AAT has a protective effect against GVHD and enhances graft-vs-leukemia effects.
Kamada Ltd., the company developing IV AAT, plans to begin a phase 3 trial of the treatment in 2016 and get the product to market in 2019 or later.
The European Commission has granted orphan drug designation for intravenous (IV) alpha-1 antitrypsin (AAT) to treat graft-versus-host disease (GVHD).
AAT is a protein derived from human plasma that has demonstrated immunomodulatory, anti-inflammatory, tissue-protective, antimicrobial, and anti-apoptotic properties.
AAT may attenuate inflammation by lowering levels of pro-inflammatory mediators such as cytokines, chemokines, and proteases associated with GVHD.
The European Commission granted IV AAT orphan designation based on preliminary clinical and preclinical research.
Orphan designation is granted to a medicine intended to treat a rare condition occurring in not more than 5 in 10,000 people in the European Union. The designation allows the drug’s maker to benefit from incentives such as a 10-year period of market exclusivity, reduced regulatory fees, and protocol assistance from the European Medicines Agency.
IV AAT also has orphan designation to treat GVHD in the US.
Studies of AAT
AAT is being investigated in a phase 1/2 study involving 24 patients with GVHD who had an inadequate response to steroid treatment. The patients are enrolled in 4 dose cohorts, in which they receive up to 8 doses of AAT.
Interim results from this study were presented at the 2014 ASH Annual Meeting (abstract 3927). Preliminary results indicated that continuous administration of AAT as therapy for steroid-resistant gut GVHD is feasible in the subject population.
Following AAT administration, the researchers observed a decrease in diarrhea, a decrease in intestinal AAT loss, and improvement in endoscopic evaluation. In addition, AAT administration suppressed serum levels of pro-inflammatory cytokines and interfered with GVHD biomarkers.
Investigators have also published research on AAT in Blood. This study suggested that AAT has a protective effect against GVHD and enhances graft-vs-leukemia effects.
Kamada Ltd., the company developing IV AAT, plans to begin a phase 3 trial of the treatment in 2016 and get the product to market in 2019 or later.
The European Commission has granted orphan drug designation for intravenous (IV) alpha-1 antitrypsin (AAT) to treat graft-versus-host disease (GVHD).
AAT is a protein derived from human plasma that has demonstrated immunomodulatory, anti-inflammatory, tissue-protective, antimicrobial, and anti-apoptotic properties.
AAT may attenuate inflammation by lowering levels of pro-inflammatory mediators such as cytokines, chemokines, and proteases associated with GVHD.
The European Commission granted IV AAT orphan designation based on preliminary clinical and preclinical research.
Orphan designation is granted to a medicine intended to treat a rare condition occurring in not more than 5 in 10,000 people in the European Union. The designation allows the drug’s maker to benefit from incentives such as a 10-year period of market exclusivity, reduced regulatory fees, and protocol assistance from the European Medicines Agency.
IV AAT also has orphan designation to treat GVHD in the US.
Studies of AAT
AAT is being investigated in a phase 1/2 study involving 24 patients with GVHD who had an inadequate response to steroid treatment. The patients are enrolled in 4 dose cohorts, in which they receive up to 8 doses of AAT.
Interim results from this study were presented at the 2014 ASH Annual Meeting (abstract 3927). Preliminary results indicated that continuous administration of AAT as therapy for steroid-resistant gut GVHD is feasible in the subject population.
Following AAT administration, the researchers observed a decrease in diarrhea, a decrease in intestinal AAT loss, and improvement in endoscopic evaluation. In addition, AAT administration suppressed serum levels of pro-inflammatory cytokines and interfered with GVHD biomarkers.
Investigators have also published research on AAT in Blood. This study suggested that AAT has a protective effect against GVHD and enhances graft-vs-leukemia effects.
Kamada Ltd., the company developing IV AAT, plans to begin a phase 3 trial of the treatment in 2016 and get the product to market in 2019 or later.
Team advocates liver MRI to measure iron

Magnetic resonance imaging (MRI) should be the gold standard for measuring liver iron concentration (LIC) in patients receiving ongoing transfusion therapy, according to a group of researchers.
The team found evidence suggesting that liver MRI is more accurate than liver biopsy in determining total body iron balance in patients with sickle cell disease and other disorders requiring regular blood transfusions.
The findings have been published in Magnetic Resonance Imaging.
“Measuring total body iron using MRI is safer and less painful than biopsy,” said study author John Wood, MD, PhD, of Children’s Hospital Los Angeles in California.
“In this study, we’ve demonstrated that it is also more accurate. MRI should be recognized as the new gold standard for determining iron accumulation in the body.”
Dr Wood and his colleagues came to this conclusion after analyzing data from 49 patients who were undergoing treatment with deferitazole, an experimental chelating agent.
The team looked at the amount of iron the patients were receiving by transfusion and the amount of chelating agent they consumed, providing insights into the expected changes in iron levels at 12, 24, and 48 weeks after the start of deferitazole.
To compare MRI and liver biopsy, the researchers used serial estimates of iron chelation efficiency (ICE) calculated by R2 and R2* MRI LIC estimates as well as by simulated liver biopsy (over all physically reasonable sampling variability).
The estimates suggested that MRI liver iron measurements (R2 and R2*) are more accurate than a physically realizable liver biopsy (which has a sampling error of 10% or higher).
For R2, the standard deviation of ICE was 44.8% at 12 weeks, 14.8% at 24 weeks, and 7.4% at 48 weeks. For R2*, the standard deviation was 22.9% at 12 weeks, 9.3% at 24 weeks, and 5.7% at 48 weeks.
For a biopsy with a sampling error of 0%, the standard deviation of ICE was 25.9% at 12 weeks, 12.8% at 24 weeks, and 6.7% at 48 weeks. For a biopsy with a sampling error of 10%, it was 32.8%, 16.5%, and 8.7%, respectively.
For a biopsy with a sampling error of 20%, the standard deviation of ICE was 49.1% at 12 weeks, 24.9% at 24 weeks, and 13% at 48 weeks. For a biopsy with a sampling error of 30%, it was 68.1%, 34.5%, and 18%, respectively. And for a biopsy with a sampling error of 40%, it was 88.1%, 44.6%, and 23.2%, respectively.
In practice, the accuracy of MRI compared to liver biopsy is likely even greater than these estimates suggest, Dr Wood said.
Magnetic resonance imaging (MRI) should be the gold standard for measuring liver iron concentration (LIC) in patients receiving ongoing transfusion therapy, according to a group of researchers.
The team found evidence suggesting that liver MRI is more accurate than liver biopsy in determining total body iron balance in patients with sickle cell disease and other disorders requiring regular blood transfusions.
The findings have been published in Magnetic Resonance Imaging.
“Measuring total body iron using MRI is safer and less painful than biopsy,” said study author John Wood, MD, PhD, of Children’s Hospital Los Angeles in California.
“In this study, we’ve demonstrated that it is also more accurate. MRI should be recognized as the new gold standard for determining iron accumulation in the body.”
Dr Wood and his colleagues came to this conclusion after analyzing data from 49 patients who were undergoing treatment with deferitazole, an experimental chelating agent.
The team looked at the amount of iron the patients were receiving by transfusion and the amount of chelating agent they consumed, providing insights into the expected changes in iron levels at 12, 24, and 48 weeks after the start of deferitazole.
To compare MRI and liver biopsy, the researchers used serial estimates of iron chelation efficiency (ICE) calculated by R2 and R2* MRI LIC estimates as well as by simulated liver biopsy (over all physically reasonable sampling variability).
The estimates suggested that MRI liver iron measurements (R2 and R2*) are more accurate than a physically realizable liver biopsy (which has a sampling error of 10% or higher).
For R2, the standard deviation of ICE was 44.8% at 12 weeks, 14.8% at 24 weeks, and 7.4% at 48 weeks. For R2*, the standard deviation was 22.9% at 12 weeks, 9.3% at 24 weeks, and 5.7% at 48 weeks.
For a biopsy with a sampling error of 0%, the standard deviation of ICE was 25.9% at 12 weeks, 12.8% at 24 weeks, and 6.7% at 48 weeks. For a biopsy with a sampling error of 10%, it was 32.8%, 16.5%, and 8.7%, respectively.
For a biopsy with a sampling error of 20%, the standard deviation of ICE was 49.1% at 12 weeks, 24.9% at 24 weeks, and 13% at 48 weeks. For a biopsy with a sampling error of 30%, it was 68.1%, 34.5%, and 18%, respectively. And for a biopsy with a sampling error of 40%, it was 88.1%, 44.6%, and 23.2%, respectively.
In practice, the accuracy of MRI compared to liver biopsy is likely even greater than these estimates suggest, Dr Wood said.
Magnetic resonance imaging (MRI) should be the gold standard for measuring liver iron concentration (LIC) in patients receiving ongoing transfusion therapy, according to a group of researchers.
The team found evidence suggesting that liver MRI is more accurate than liver biopsy in determining total body iron balance in patients with sickle cell disease and other disorders requiring regular blood transfusions.
The findings have been published in Magnetic Resonance Imaging.
“Measuring total body iron using MRI is safer and less painful than biopsy,” said study author John Wood, MD, PhD, of Children’s Hospital Los Angeles in California.
“In this study, we’ve demonstrated that it is also more accurate. MRI should be recognized as the new gold standard for determining iron accumulation in the body.”
Dr Wood and his colleagues came to this conclusion after analyzing data from 49 patients who were undergoing treatment with deferitazole, an experimental chelating agent.
The team looked at the amount of iron the patients were receiving by transfusion and the amount of chelating agent they consumed, providing insights into the expected changes in iron levels at 12, 24, and 48 weeks after the start of deferitazole.
To compare MRI and liver biopsy, the researchers used serial estimates of iron chelation efficiency (ICE) calculated by R2 and R2* MRI LIC estimates as well as by simulated liver biopsy (over all physically reasonable sampling variability).
The estimates suggested that MRI liver iron measurements (R2 and R2*) are more accurate than a physically realizable liver biopsy (which has a sampling error of 10% or higher).
For R2, the standard deviation of ICE was 44.8% at 12 weeks, 14.8% at 24 weeks, and 7.4% at 48 weeks. For R2*, the standard deviation was 22.9% at 12 weeks, 9.3% at 24 weeks, and 5.7% at 48 weeks.
For a biopsy with a sampling error of 0%, the standard deviation of ICE was 25.9% at 12 weeks, 12.8% at 24 weeks, and 6.7% at 48 weeks. For a biopsy with a sampling error of 10%, it was 32.8%, 16.5%, and 8.7%, respectively.
For a biopsy with a sampling error of 20%, the standard deviation of ICE was 49.1% at 12 weeks, 24.9% at 24 weeks, and 13% at 48 weeks. For a biopsy with a sampling error of 30%, it was 68.1%, 34.5%, and 18%, respectively. And for a biopsy with a sampling error of 40%, it was 88.1%, 44.6%, and 23.2%, respectively.
In practice, the accuracy of MRI compared to liver biopsy is likely even greater than these estimates suggest, Dr Wood said.