User login
BMI linked to need for blood transfusion
![]()
Photo courtesy of UAB Hospital
VIENNA—New research suggests that having a higher body mass index (BMI) is associated with a decreased need for blood transfusion among patients undergoing hip or knee replacement surgery.
In this retrospective, single-center study, overweight and obese patients were less likely than patients with a normal BMI to require blood transfusions.
The investigators said these results add to the conflicting body of research examining the association between BMI and blood transfusions in this patient population.
The results were presented at the International Society for Technology in Arthroplasty Annual Congress.
“The results were surprising to us,” said investigator Craig Silverton, DO, of Henry Ford Health System in Detroit, Michigan.
“It goes against the normal thought process. It’s hard to explain, but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
For this study, Dr Silverton and his colleagues evaluated 2399 patients, 1503 of whom underwent knee replacement and 896 of whom underwent hip surgery.
The investigators divided patients into 3 groups according to BMI: normal (BMI less than 25), overweight (BMI of 25 to 29.9), and obese (BMI more than 30).
As BMI increased, there was a significant increase in the estimated blood loss for both types of surgery.
Among hip surgery patients, the estimated blood loss was 268.2± 313.9 mL in patients with a normal BMI, 282.0 ± 208.7 mL in overweight patients, and 330.5 ± 302.4 mL in obese patients.
Among knee surgery patients, the estimated blood loss was 85.7 ± 153.8 mL in patients with a normal BMI, 90.5 ± 164.6 mL in overweight patients, and 89.4 ± 72.4 mL in obese patients.
However, with increasing BMI, there was a significant decrease in the estimated blood volume lost.
Among hip surgery patients, the estimated blood volume lost was 6.12% ± 8.12 in patients with a normal BMI, 4.92% ± 3.05 in overweight patients, and 4.50% ± 3.25 in obese patients.
Among knee surgery patients, the estimated blood volume lost was 2.05% ± 4.00 in patients with a normal BMI, 1.55% ± 2.73 in overweight patients, and 1.26% ± 1.01 in obese patients.
Likewise, there was a significant reduction in transfusion rates as BMI increased.
Among hip surgery patients, the transfusion rate was 34.8% for those with a normal BMI, 27.6% for those who were overweight, and 21.9% for obese patients.
Among knee surgery patients, the transfusion rate was 17.3% for those with a normal BMI, 11.4% for those who were overweight, and 8.3% for obese patients.
The investigators noted that there was no identifiable relationship between BMI and deep vein thrombosis, pulmonary embolism, myocardial infarction, length of hospital stay, 30-day readmission rate, or preoperative hemoglobin level.
There was a trend toward increased deep surgical site infections with increased BMI, but only among patients who underwent hip surgery. ![]()
![]()
Photo courtesy of UAB Hospital
VIENNA—New research suggests that having a higher body mass index (BMI) is associated with a decreased need for blood transfusion among patients undergoing hip or knee replacement surgery.
In this retrospective, single-center study, overweight and obese patients were less likely than patients with a normal BMI to require blood transfusions.
The investigators said these results add to the conflicting body of research examining the association between BMI and blood transfusions in this patient population.
The results were presented at the International Society for Technology in Arthroplasty Annual Congress.
“The results were surprising to us,” said investigator Craig Silverton, DO, of Henry Ford Health System in Detroit, Michigan.
“It goes against the normal thought process. It’s hard to explain, but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
For this study, Dr Silverton and his colleagues evaluated 2399 patients, 1503 of whom underwent knee replacement and 896 of whom underwent hip surgery.
The investigators divided patients into 3 groups according to BMI: normal (BMI less than 25), overweight (BMI of 25 to 29.9), and obese (BMI more than 30).
As BMI increased, there was a significant increase in the estimated blood loss for both types of surgery.
Among hip surgery patients, the estimated blood loss was 268.2± 313.9 mL in patients with a normal BMI, 282.0 ± 208.7 mL in overweight patients, and 330.5 ± 302.4 mL in obese patients.
Among knee surgery patients, the estimated blood loss was 85.7 ± 153.8 mL in patients with a normal BMI, 90.5 ± 164.6 mL in overweight patients, and 89.4 ± 72.4 mL in obese patients.
However, with increasing BMI, there was a significant decrease in the estimated blood volume lost.
Among hip surgery patients, the estimated blood volume lost was 6.12% ± 8.12 in patients with a normal BMI, 4.92% ± 3.05 in overweight patients, and 4.50% ± 3.25 in obese patients.
Among knee surgery patients, the estimated blood volume lost was 2.05% ± 4.00 in patients with a normal BMI, 1.55% ± 2.73 in overweight patients, and 1.26% ± 1.01 in obese patients.
Likewise, there was a significant reduction in transfusion rates as BMI increased.
Among hip surgery patients, the transfusion rate was 34.8% for those with a normal BMI, 27.6% for those who were overweight, and 21.9% for obese patients.
Among knee surgery patients, the transfusion rate was 17.3% for those with a normal BMI, 11.4% for those who were overweight, and 8.3% for obese patients.
The investigators noted that there was no identifiable relationship between BMI and deep vein thrombosis, pulmonary embolism, myocardial infarction, length of hospital stay, 30-day readmission rate, or preoperative hemoglobin level.
There was a trend toward increased deep surgical site infections with increased BMI, but only among patients who underwent hip surgery. ![]()
![]()
Photo courtesy of UAB Hospital
VIENNA—New research suggests that having a higher body mass index (BMI) is associated with a decreased need for blood transfusion among patients undergoing hip or knee replacement surgery.
In this retrospective, single-center study, overweight and obese patients were less likely than patients with a normal BMI to require blood transfusions.
The investigators said these results add to the conflicting body of research examining the association between BMI and blood transfusions in this patient population.
The results were presented at the International Society for Technology in Arthroplasty Annual Congress.
“The results were surprising to us,” said investigator Craig Silverton, DO, of Henry Ford Health System in Detroit, Michigan.
“It goes against the normal thought process. It’s hard to explain, but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
For this study, Dr Silverton and his colleagues evaluated 2399 patients, 1503 of whom underwent knee replacement and 896 of whom underwent hip surgery.
The investigators divided patients into 3 groups according to BMI: normal (BMI less than 25), overweight (BMI of 25 to 29.9), and obese (BMI more than 30).
As BMI increased, there was a significant increase in the estimated blood loss for both types of surgery.
Among hip surgery patients, the estimated blood loss was 268.2± 313.9 mL in patients with a normal BMI, 282.0 ± 208.7 mL in overweight patients, and 330.5 ± 302.4 mL in obese patients.
Among knee surgery patients, the estimated blood loss was 85.7 ± 153.8 mL in patients with a normal BMI, 90.5 ± 164.6 mL in overweight patients, and 89.4 ± 72.4 mL in obese patients.
However, with increasing BMI, there was a significant decrease in the estimated blood volume lost.
Among hip surgery patients, the estimated blood volume lost was 6.12% ± 8.12 in patients with a normal BMI, 4.92% ± 3.05 in overweight patients, and 4.50% ± 3.25 in obese patients.
Among knee surgery patients, the estimated blood volume lost was 2.05% ± 4.00 in patients with a normal BMI, 1.55% ± 2.73 in overweight patients, and 1.26% ± 1.01 in obese patients.
Likewise, there was a significant reduction in transfusion rates as BMI increased.
Among hip surgery patients, the transfusion rate was 34.8% for those with a normal BMI, 27.6% for those who were overweight, and 21.9% for obese patients.
Among knee surgery patients, the transfusion rate was 17.3% for those with a normal BMI, 11.4% for those who were overweight, and 8.3% for obese patients.
The investigators noted that there was no identifiable relationship between BMI and deep vein thrombosis, pulmonary embolism, myocardial infarction, length of hospital stay, 30-day readmission rate, or preoperative hemoglobin level.
There was a trend toward increased deep surgical site infections with increased BMI, but only among patients who underwent hip surgery. ![]()
Trio wins Nobel Prize for DNA repair discoveries

Image by Tom Ellenberger
Three researchers have won this year’s Nobel Prize in Chemistry for mechanistic studies of DNA repair.
Tomas Lindahl, MD, PhD, Paul Modrich, PhD, and Aziz Sancar, MD, PhD, each mapped how DNA repair systems function at a detailed molecular level.
Their work has provided insight into how cells function, knowledge that can be used in the development of new cancer treatments, among other applications.
In the early 1970s, scientists believed that DNA was an extremely stable molecule, but Dr Lindahl demonstrated that DNA decays at a rate that ought to have made life on Earth impossible.
This insight led to the discovery of molecular machinery known as base excision repair, which constantly counteracts the collapse of our DNA.
For his part, Dr Sancar mapped nucleotide excision repair, the mechanism that cells use to repair UV damage to DNA.
People born with defects in this repair system will develop skin cancer if they are exposed to sunlight. The cell also utilizes nucleotide excision repair to correct defects caused by mutagenic substances, among other things.
Dr Modrich demonstrated how the cell corrects errors that occur when DNA is replicated during cell division.
This mechanism, mismatch repair, reduces the error frequency during DNA replication by about a thousand-fold. Congenital defects in mismatch repair are known, for example, to cause a hereditary variant of colon cancer.
About the winners
Tomas Lindahl was born in 1938 in Stockholm, Sweden. He earned his PhD in 1967 and his MD in 1970, both from Karolinska Institutet in Sweden. He is currently emeritus group leader at the Francis Crick Institute in London, UK.
Paul Modrich was born in 1946. In 1973, he earned his PhD from Stanford University in California. He is currently an investigator at Howard Hughes Medical Institute in Chevy Chase, Maryland, and a professor at Duke University School of Medicine in Durham, North Carolina.
Aziz Sancar was born in 1946 in Savur, Turkey. He earned his MD in 1969 from Istanbul University in Turkey and his PhD in 1977 from the University of Texas in Dallas. He is currently a professor at the University of North Carolina School of Medicine in Chapel Hill. ![]()
Image by Tom Ellenberger
Three researchers have won this year’s Nobel Prize in Chemistry for mechanistic studies of DNA repair.
Tomas Lindahl, MD, PhD, Paul Modrich, PhD, and Aziz Sancar, MD, PhD, each mapped how DNA repair systems function at a detailed molecular level.
Their work has provided insight into how cells function, knowledge that can be used in the development of new cancer treatments, among other applications.
In the early 1970s, scientists believed that DNA was an extremely stable molecule, but Dr Lindahl demonstrated that DNA decays at a rate that ought to have made life on Earth impossible.
This insight led to the discovery of molecular machinery known as base excision repair, which constantly counteracts the collapse of our DNA.
For his part, Dr Sancar mapped nucleotide excision repair, the mechanism that cells use to repair UV damage to DNA.
People born with defects in this repair system will develop skin cancer if they are exposed to sunlight. The cell also utilizes nucleotide excision repair to correct defects caused by mutagenic substances, among other things.
Dr Modrich demonstrated how the cell corrects errors that occur when DNA is replicated during cell division.
This mechanism, mismatch repair, reduces the error frequency during DNA replication by about a thousand-fold. Congenital defects in mismatch repair are known, for example, to cause a hereditary variant of colon cancer.
About the winners
Tomas Lindahl was born in 1938 in Stockholm, Sweden. He earned his PhD in 1967 and his MD in 1970, both from Karolinska Institutet in Sweden. He is currently emeritus group leader at the Francis Crick Institute in London, UK.
Paul Modrich was born in 1946. In 1973, he earned his PhD from Stanford University in California. He is currently an investigator at Howard Hughes Medical Institute in Chevy Chase, Maryland, and a professor at Duke University School of Medicine in Durham, North Carolina.
Aziz Sancar was born in 1946 in Savur, Turkey. He earned his MD in 1969 from Istanbul University in Turkey and his PhD in 1977 from the University of Texas in Dallas. He is currently a professor at the University of North Carolina School of Medicine in Chapel Hill. ![]()
Image by Tom Ellenberger
Three researchers have won this year’s Nobel Prize in Chemistry for mechanistic studies of DNA repair.
Tomas Lindahl, MD, PhD, Paul Modrich, PhD, and Aziz Sancar, MD, PhD, each mapped how DNA repair systems function at a detailed molecular level.
Their work has provided insight into how cells function, knowledge that can be used in the development of new cancer treatments, among other applications.
In the early 1970s, scientists believed that DNA was an extremely stable molecule, but Dr Lindahl demonstrated that DNA decays at a rate that ought to have made life on Earth impossible.
This insight led to the discovery of molecular machinery known as base excision repair, which constantly counteracts the collapse of our DNA.
For his part, Dr Sancar mapped nucleotide excision repair, the mechanism that cells use to repair UV damage to DNA.
People born with defects in this repair system will develop skin cancer if they are exposed to sunlight. The cell also utilizes nucleotide excision repair to correct defects caused by mutagenic substances, among other things.
Dr Modrich demonstrated how the cell corrects errors that occur when DNA is replicated during cell division.
This mechanism, mismatch repair, reduces the error frequency during DNA replication by about a thousand-fold. Congenital defects in mismatch repair are known, for example, to cause a hereditary variant of colon cancer.
About the winners
Tomas Lindahl was born in 1938 in Stockholm, Sweden. He earned his PhD in 1967 and his MD in 1970, both from Karolinska Institutet in Sweden. He is currently emeritus group leader at the Francis Crick Institute in London, UK.
Paul Modrich was born in 1946. In 1973, he earned his PhD from Stanford University in California. He is currently an investigator at Howard Hughes Medical Institute in Chevy Chase, Maryland, and a professor at Duke University School of Medicine in Durham, North Carolina.
Aziz Sancar was born in 1946 in Savur, Turkey. He earned his MD in 1969 from Istanbul University in Turkey and his PhD in 1977 from the University of Texas in Dallas. He is currently a professor at the University of North Carolina School of Medicine in Chapel Hill. ![]()
Case suggests GSIs could treat Notch-mutated ALL
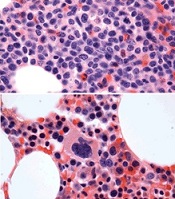
before (top) and after 7 weeks
of treatment (bottom)
© Knoechel et al.
Results of a case study suggest a gamma-secretase inhibitor (GSI) can be effective against Notch-mutated acute lymphoblastic leukemia (ALL).
The patient, who had early T-cell precursor ALL (ETP-ALL), achieved a complete hematologic response to treatment with BMS-906024, a GSI with anti-Notch
activity.
The patient was then able to proceed to hematopoietic stem cell transplant and was leukemia-free at last follow-up.
The researchers said this suggests that GSIs might hold promise for treating ALL and other cancers characterized by Notch mutations.
Birgit Knoechel, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues described this case study in Cold Spring Harbor Molecular Case Studies.
The patient was a 53-year-old male with ETP-ALL who had failed previous rounds of chemotherapy and was then enrolled in a clinical trial of BMS-906024.
The patient began to show immediate improvement after starting treatment with the GSI. After 3 cycles, he went on to transplant and has since been leukemia-free—for 19 months so far.
To determine the genetic basis for the patient’s response to BMS-906024, researchers performed targeted and whole-exome sequencing on his leukemic cells.
They identified 4 potential mutations driving disease progression, including a novel mutation in the NOTCH1 gene that resulted in hyperactive signaling. This mutated gene copy was also duplicated in the cancer genome, resulting in elevated expression.
However, the NOTCH1 mutation, along with 2 of the other mutations, were absent in the remission bone marrow.
The researchers also cultured the patient’s leukemic cells to determine the molecular response to treatment.
Cells treated with BMS-906024 had greatly reduced levels of mutated NOTCH1 protein. RNA sequencing demonstrated that Notch target genes were sensitive to the treatment.
The MYC oncogene, on the other hand, was not sensitive to BMS-906024.
Epigenetic analysis revealed that the enhancer driving MYC expression in the leukemic cells was not Notch-dependent, but rather BRD4-dependent, suggesting another possible therapeutic option for MYC-expressing tumors. ![]()
before (top) and after 7 weeks
of treatment (bottom)
© Knoechel et al.
Results of a case study suggest a gamma-secretase inhibitor (GSI) can be effective against Notch-mutated acute lymphoblastic leukemia (ALL).
The patient, who had early T-cell precursor ALL (ETP-ALL), achieved a complete hematologic response to treatment with BMS-906024, a GSI with anti-Notch
activity.
The patient was then able to proceed to hematopoietic stem cell transplant and was leukemia-free at last follow-up.
The researchers said this suggests that GSIs might hold promise for treating ALL and other cancers characterized by Notch mutations.
Birgit Knoechel, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues described this case study in Cold Spring Harbor Molecular Case Studies.
The patient was a 53-year-old male with ETP-ALL who had failed previous rounds of chemotherapy and was then enrolled in a clinical trial of BMS-906024.
The patient began to show immediate improvement after starting treatment with the GSI. After 3 cycles, he went on to transplant and has since been leukemia-free—for 19 months so far.
To determine the genetic basis for the patient’s response to BMS-906024, researchers performed targeted and whole-exome sequencing on his leukemic cells.
They identified 4 potential mutations driving disease progression, including a novel mutation in the NOTCH1 gene that resulted in hyperactive signaling. This mutated gene copy was also duplicated in the cancer genome, resulting in elevated expression.
However, the NOTCH1 mutation, along with 2 of the other mutations, were absent in the remission bone marrow.
The researchers also cultured the patient’s leukemic cells to determine the molecular response to treatment.
Cells treated with BMS-906024 had greatly reduced levels of mutated NOTCH1 protein. RNA sequencing demonstrated that Notch target genes were sensitive to the treatment.
The MYC oncogene, on the other hand, was not sensitive to BMS-906024.
Epigenetic analysis revealed that the enhancer driving MYC expression in the leukemic cells was not Notch-dependent, but rather BRD4-dependent, suggesting another possible therapeutic option for MYC-expressing tumors. ![]()
before (top) and after 7 weeks
of treatment (bottom)
© Knoechel et al.
Results of a case study suggest a gamma-secretase inhibitor (GSI) can be effective against Notch-mutated acute lymphoblastic leukemia (ALL).
The patient, who had early T-cell precursor ALL (ETP-ALL), achieved a complete hematologic response to treatment with BMS-906024, a GSI with anti-Notch
activity.
The patient was then able to proceed to hematopoietic stem cell transplant and was leukemia-free at last follow-up.
The researchers said this suggests that GSIs might hold promise for treating ALL and other cancers characterized by Notch mutations.
Birgit Knoechel, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues described this case study in Cold Spring Harbor Molecular Case Studies.
The patient was a 53-year-old male with ETP-ALL who had failed previous rounds of chemotherapy and was then enrolled in a clinical trial of BMS-906024.
The patient began to show immediate improvement after starting treatment with the GSI. After 3 cycles, he went on to transplant and has since been leukemia-free—for 19 months so far.
To determine the genetic basis for the patient’s response to BMS-906024, researchers performed targeted and whole-exome sequencing on his leukemic cells.
They identified 4 potential mutations driving disease progression, including a novel mutation in the NOTCH1 gene that resulted in hyperactive signaling. This mutated gene copy was also duplicated in the cancer genome, resulting in elevated expression.
However, the NOTCH1 mutation, along with 2 of the other mutations, were absent in the remission bone marrow.
The researchers also cultured the patient’s leukemic cells to determine the molecular response to treatment.
Cells treated with BMS-906024 had greatly reduced levels of mutated NOTCH1 protein. RNA sequencing demonstrated that Notch target genes were sensitive to the treatment.
The MYC oncogene, on the other hand, was not sensitive to BMS-906024.
Epigenetic analysis revealed that the enhancer driving MYC expression in the leukemic cells was not Notch-dependent, but rather BRD4-dependent, suggesting another possible therapeutic option for MYC-expressing tumors. ![]()
Word choice affects public perception of drugs

Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Team identifies therapeutic target for HIT

Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Hematocrit level may predict need for transfusion

Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Study reveals tumor suppressor in AML

The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said. ![]()
The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said. ![]()
The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said.
Treating EBV-associated lymphomas with VSTs

among uninfected cells (blue)
Image by Benjamin
Chaigne-Delalande
NEW YORK—Type 2 Epstein-Barr virus (EBV) tumors, such as Hodgkin and non-Hodgkin lymphomas, are challenging to treat with virus-specific T (VST) cells, according to researchers.
These lymphomas express a more restricted array of EBV antigens that are not particularly immunogenic.
Nevertheless, researchers are devising an approach using peptide mixtures to activate EBV VSTs for use in these patients.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described this work at the inaugural CRI-CIMT-EATI-AACR International Immunotherapy of Cancer Conference. She also described the researchers’ efforts to create off-the-shelf VSTs.
Dr Heslop explained that, in addition to the more restricted array of EBV antigens, EBV-associated tumors often produce inhibitory cytokines that can impede the activity of T cells.
So the researchers devised a strategy to expand these low-frequency clones by stimulating responding T cells with dendritic cells genetically modified with an ADV viral vector to overexpress LMP1 and LMP2. After multiple stimulations, they obtained an autologous product from the patient.
The team then tested the cytotoxic T cells in 21 patients with relapsed disease and in 29 patients as adjuvant therapy after stem cell transplant (n=14) or chemotherapy (n=15).
In the adjuvant arm, all patients but 1 remain in remission up to 5 years later.
In the relapsed arm, 11 had a complete response (CR), 2 had a partial response (PR), and 8 had progressive disease within 2 to 8 weeks.
“Importantly, there was no toxicity,” Dr Heslop said. “[A]ll were heavily pretreated with multiple lines of therapy for lymphoma, so I think the response rate is encouraging.”
An alternative approach: Pepmix-activated EBV VSTs
Although the antitumor effects of the above approach were encouraging, “we had a very complex manufacturing methodology that we didn’t think was sufficiently scaleable and robust for clinical studies,” Dr Heslop said.
“We also thought there would be potential regulatory issues with live EBV virus and the adenoviral vector,” she added.
And the researchers were concerned about the competition from the EBV/Ad-LMP dominant antigens.
So they devised an alternative approach using peptide mixture (pepmix)-activated EBVSTs.
This approach used autologous monocyte-derived dendritic cells as the antigen-presenting cells for the first stimulation.
The researchers pulsed them with overlapping peptides derived from 4 EBV antigens expressed in the tumors (EBV-LMP1, LMP2, EBNA1, and BARF1). They then expanded and opsonized the cells with IL-7 and IL-15.
For the second stimulation, the team used the T cells pulsed with the peptides and a K562 line pulsed with co-stimulatory molecules. And this process took 23 days, as opposed to the 2-3 months with the previous product.
The researchers have treated 9 patients with these EBVSTs as adjuvant therapy after autologous stem cell transplant. All patients remain in remission.
They also treated 6 patients with active disease. Two are in CR, 2 are in PR, and 2 have progressed.
This trial is ongoing, but the researchers believe that targeting the more challenging type 2 latency tumors with autologous cells can overcome T-cell anergy by using IL-7 and IL-15.
“Obviously, we need more numbers to know what the range of response is,” Dr Heslop said, although, at this early stage, it appears pepmix-activated T cells can produce antitumor responses. .
among uninfected cells (blue)
Image by Benjamin
Chaigne-Delalande
NEW YORK—Type 2 Epstein-Barr virus (EBV) tumors, such as Hodgkin and non-Hodgkin lymphomas, are challenging to treat with virus-specific T (VST) cells, according to researchers.
These lymphomas express a more restricted array of EBV antigens that are not particularly immunogenic.
Nevertheless, researchers are devising an approach using peptide mixtures to activate EBV VSTs for use in these patients.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described this work at the inaugural CRI-CIMT-EATI-AACR International Immunotherapy of Cancer Conference. She also described the researchers’ efforts to create off-the-shelf VSTs.
Dr Heslop explained that, in addition to the more restricted array of EBV antigens, EBV-associated tumors often produce inhibitory cytokines that can impede the activity of T cells.
So the researchers devised a strategy to expand these low-frequency clones by stimulating responding T cells with dendritic cells genetically modified with an ADV viral vector to overexpress LMP1 and LMP2. After multiple stimulations, they obtained an autologous product from the patient.
The team then tested the cytotoxic T cells in 21 patients with relapsed disease and in 29 patients as adjuvant therapy after stem cell transplant (n=14) or chemotherapy (n=15).
In the adjuvant arm, all patients but 1 remain in remission up to 5 years later.
In the relapsed arm, 11 had a complete response (CR), 2 had a partial response (PR), and 8 had progressive disease within 2 to 8 weeks.
“Importantly, there was no toxicity,” Dr Heslop said. “[A]ll were heavily pretreated with multiple lines of therapy for lymphoma, so I think the response rate is encouraging.”
An alternative approach: Pepmix-activated EBV VSTs
Although the antitumor effects of the above approach were encouraging, “we had a very complex manufacturing methodology that we didn’t think was sufficiently scaleable and robust for clinical studies,” Dr Heslop said.
“We also thought there would be potential regulatory issues with live EBV virus and the adenoviral vector,” she added.
And the researchers were concerned about the competition from the EBV/Ad-LMP dominant antigens.
So they devised an alternative approach using peptide mixture (pepmix)-activated EBVSTs.
This approach used autologous monocyte-derived dendritic cells as the antigen-presenting cells for the first stimulation.
The researchers pulsed them with overlapping peptides derived from 4 EBV antigens expressed in the tumors (EBV-LMP1, LMP2, EBNA1, and BARF1). They then expanded and opsonized the cells with IL-7 and IL-15.
For the second stimulation, the team used the T cells pulsed with the peptides and a K562 line pulsed with co-stimulatory molecules. And this process took 23 days, as opposed to the 2-3 months with the previous product.
The researchers have treated 9 patients with these EBVSTs as adjuvant therapy after autologous stem cell transplant. All patients remain in remission.
They also treated 6 patients with active disease. Two are in CR, 2 are in PR, and 2 have progressed.
This trial is ongoing, but the researchers believe that targeting the more challenging type 2 latency tumors with autologous cells can overcome T-cell anergy by using IL-7 and IL-15.
“Obviously, we need more numbers to know what the range of response is,” Dr Heslop said, although, at this early stage, it appears pepmix-activated T cells can produce antitumor responses. .
among uninfected cells (blue)
Image by Benjamin
Chaigne-Delalande
NEW YORK—Type 2 Epstein-Barr virus (EBV) tumors, such as Hodgkin and non-Hodgkin lymphomas, are challenging to treat with virus-specific T (VST) cells, according to researchers.
These lymphomas express a more restricted array of EBV antigens that are not particularly immunogenic.
Nevertheless, researchers are devising an approach using peptide mixtures to activate EBV VSTs for use in these patients.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described this work at the inaugural CRI-CIMT-EATI-AACR International Immunotherapy of Cancer Conference. She also described the researchers’ efforts to create off-the-shelf VSTs.
Dr Heslop explained that, in addition to the more restricted array of EBV antigens, EBV-associated tumors often produce inhibitory cytokines that can impede the activity of T cells.
So the researchers devised a strategy to expand these low-frequency clones by stimulating responding T cells with dendritic cells genetically modified with an ADV viral vector to overexpress LMP1 and LMP2. After multiple stimulations, they obtained an autologous product from the patient.
The team then tested the cytotoxic T cells in 21 patients with relapsed disease and in 29 patients as adjuvant therapy after stem cell transplant (n=14) or chemotherapy (n=15).
In the adjuvant arm, all patients but 1 remain in remission up to 5 years later.
In the relapsed arm, 11 had a complete response (CR), 2 had a partial response (PR), and 8 had progressive disease within 2 to 8 weeks.
“Importantly, there was no toxicity,” Dr Heslop said. “[A]ll were heavily pretreated with multiple lines of therapy for lymphoma, so I think the response rate is encouraging.”
An alternative approach: Pepmix-activated EBV VSTs
Although the antitumor effects of the above approach were encouraging, “we had a very complex manufacturing methodology that we didn’t think was sufficiently scaleable and robust for clinical studies,” Dr Heslop said.
“We also thought there would be potential regulatory issues with live EBV virus and the adenoviral vector,” she added.
And the researchers were concerned about the competition from the EBV/Ad-LMP dominant antigens.
So they devised an alternative approach using peptide mixture (pepmix)-activated EBVSTs.
This approach used autologous monocyte-derived dendritic cells as the antigen-presenting cells for the first stimulation.
The researchers pulsed them with overlapping peptides derived from 4 EBV antigens expressed in the tumors (EBV-LMP1, LMP2, EBNA1, and BARF1). They then expanded and opsonized the cells with IL-7 and IL-15.
For the second stimulation, the team used the T cells pulsed with the peptides and a K562 line pulsed with co-stimulatory molecules. And this process took 23 days, as opposed to the 2-3 months with the previous product.
The researchers have treated 9 patients with these EBVSTs as adjuvant therapy after autologous stem cell transplant. All patients remain in remission.
They also treated 6 patients with active disease. Two are in CR, 2 are in PR, and 2 have progressed.
This trial is ongoing, but the researchers believe that targeting the more challenging type 2 latency tumors with autologous cells can overcome T-cell anergy by using IL-7 and IL-15.
“Obviously, we need more numbers to know what the range of response is,” Dr Heslop said, although, at this early stage, it appears pepmix-activated T cells can produce antitumor responses. .
Creating off-the-shelf VSTs

Photo courtesy of Baylor
College of Medicine
NEW YORK—Researchers are creating virus-specific T cells (VST) to treat and prevent viral infections in patients who undergo hematopoietic stem cell transplant.
Thus far, the group has modified T cells with 5 viral vectors—Epstein-Barr virus (EBV), cytomegalovirus (CMV), adenovirus (ADV), BK virus (BKV), and human herpesvirus 6 (HHV6)—and are devising methods whereby these VSTs can be made readily available, off-the-shelf products.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described the efforts of the Baylor research team at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
The team’s tri-virus and 5-virus VST approaches have been described previously. Here, we focus on the team’s efforts to create an off-the-shelf product.
A companion story describes the team’s VST approach to treating type 2 EBV-associated lymphomas.
Despite promising results with these earlier methodologies both as prophylaxis and treatment after stem cell transplant, problems existed with the approaches that would impede broader implementation of VSTs.
“Most of these initial methodologies were complex,” Dr Heslop said.
And even though the production time of the 5-virus VSTs is only 10 days, it does not allow for urgent use.
To solve this problem, the researchers are developing VSTs as off-the-shelf, third-party banked cells for patients who don’t have the time to wait for donor-specific cells to be made.
“The strategy here is that we make lines that are well-characterized but are HLA-restricted and tied to specific viruses,” Dr Heslop said.
The cells are then cryopreserved so that they’re available, and patients receive VSTs according to their HLA type and the line that has suitable activity for their infections.
“We initially evaluated this approach through a multicenter study sponsored by the NHLBI [National Heart, Lung, and Blood Institute],” Dr Heslop said.
Tri-virus approach
The researchers used the original tri-virus methodology, which was lengthy, “but, in this case, because the cells were already available, the time was not a major issue,” Dr Heslop said.
The team also made some new lines for donors with common alleles. In all, they had 32 lines available while the study was running.
They treated 50 patients: 23 received VSTs for CMV, 18 for ADV, and 9 for EBV.
One patient who had CMV colitis received the VSTs and had a complete response (CR), as evidenced by a normal endoscopy with no viral inclusions.
Another patient had EBV persistent after 6 doses of rituximab. One month after receiving the VST infusion, the patient had a CR, even though the cell line had only 1 class 2 allele. And the patient has sustained the CR for several years.
The overall response rate for the study is 74.0% at day 42 after infusion.
The response rate was not significantly different for each virus, Dr Heslop pointed out. Patients with CMV had a 73.9% response rate, those with EBV had a 66.7% response rate, and those with ADV had a 77.8% response rate.
“This is a little bit lower than with the donor-specific T cells, but I think it’s still a promising approach,” she added.
5-virus peptide mix
The researchers are now evaluating the more rapid, 5-virus peptide mix method for creating off-the-shelf VSTs.
This method replaced live viruses with overlapping peptide pools and added immunogenic antigens for 5 viruses, including BKV and HHV6. The process takes only 10 days to produce VSTs.
The team has identified a line for over 90% of the patients screened.
“That’s because we will accept a line that’s only matched at 1 HLA allele, as long as we have activity against the infecting virus through the shared allele,” Dr Heslop explained.
So they’re conducting a clinical trial using this method, and thus far, they have enrolled 22 patients. Sixteen patients have had 1 infusion, and 6 patients have had multiple infusions.
The 22 patients had 25 infections: 10 CMV, 10 BKV, 2 EBV, 2 ADV, and 1 HHV6.
The overall response rate is 88%. Nine of 10 responses in patients with BKV were partial because BK is difficult to clear from urine. However, the BK patients who had hemorrhagic cystitis all had symptomatic improvement.
Dr Heslop pointed out that these results are similar to those at other centers using EBV third-party T cells.
The initial third-party studies were done in Scotland and had a response rate of about 60%, which increased to around 80% in follow-up studies, where they characterized the T cells more extensively.
Both donor-specific and third-party VSTs have low toxicity, sustained response rates, and activity confirmed by studies in multiple centers.
Dr Heslop believes the rapid manufacturing methodologies will facilitate definitive clinical trials.
She said Cell Medica provided support for some of the trials with EBV tumors.
Photo courtesy of Baylor
College of Medicine
NEW YORK—Researchers are creating virus-specific T cells (VST) to treat and prevent viral infections in patients who undergo hematopoietic stem cell transplant.
Thus far, the group has modified T cells with 5 viral vectors—Epstein-Barr virus (EBV), cytomegalovirus (CMV), adenovirus (ADV), BK virus (BKV), and human herpesvirus 6 (HHV6)—and are devising methods whereby these VSTs can be made readily available, off-the-shelf products.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described the efforts of the Baylor research team at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
The team’s tri-virus and 5-virus VST approaches have been described previously. Here, we focus on the team’s efforts to create an off-the-shelf product.
A companion story describes the team’s VST approach to treating type 2 EBV-associated lymphomas.
Despite promising results with these earlier methodologies both as prophylaxis and treatment after stem cell transplant, problems existed with the approaches that would impede broader implementation of VSTs.
“Most of these initial methodologies were complex,” Dr Heslop said.
And even though the production time of the 5-virus VSTs is only 10 days, it does not allow for urgent use.
To solve this problem, the researchers are developing VSTs as off-the-shelf, third-party banked cells for patients who don’t have the time to wait for donor-specific cells to be made.
“The strategy here is that we make lines that are well-characterized but are HLA-restricted and tied to specific viruses,” Dr Heslop said.
The cells are then cryopreserved so that they’re available, and patients receive VSTs according to their HLA type and the line that has suitable activity for their infections.
“We initially evaluated this approach through a multicenter study sponsored by the NHLBI [National Heart, Lung, and Blood Institute],” Dr Heslop said.
Tri-virus approach
The researchers used the original tri-virus methodology, which was lengthy, “but, in this case, because the cells were already available, the time was not a major issue,” Dr Heslop said.
The team also made some new lines for donors with common alleles. In all, they had 32 lines available while the study was running.
They treated 50 patients: 23 received VSTs for CMV, 18 for ADV, and 9 for EBV.
One patient who had CMV colitis received the VSTs and had a complete response (CR), as evidenced by a normal endoscopy with no viral inclusions.
Another patient had EBV persistent after 6 doses of rituximab. One month after receiving the VST infusion, the patient had a CR, even though the cell line had only 1 class 2 allele. And the patient has sustained the CR for several years.
The overall response rate for the study is 74.0% at day 42 after infusion.
The response rate was not significantly different for each virus, Dr Heslop pointed out. Patients with CMV had a 73.9% response rate, those with EBV had a 66.7% response rate, and those with ADV had a 77.8% response rate.
“This is a little bit lower than with the donor-specific T cells, but I think it’s still a promising approach,” she added.
5-virus peptide mix
The researchers are now evaluating the more rapid, 5-virus peptide mix method for creating off-the-shelf VSTs.
This method replaced live viruses with overlapping peptide pools and added immunogenic antigens for 5 viruses, including BKV and HHV6. The process takes only 10 days to produce VSTs.
The team has identified a line for over 90% of the patients screened.
“That’s because we will accept a line that’s only matched at 1 HLA allele, as long as we have activity against the infecting virus through the shared allele,” Dr Heslop explained.
So they’re conducting a clinical trial using this method, and thus far, they have enrolled 22 patients. Sixteen patients have had 1 infusion, and 6 patients have had multiple infusions.
The 22 patients had 25 infections: 10 CMV, 10 BKV, 2 EBV, 2 ADV, and 1 HHV6.
The overall response rate is 88%. Nine of 10 responses in patients with BKV were partial because BK is difficult to clear from urine. However, the BK patients who had hemorrhagic cystitis all had symptomatic improvement.
Dr Heslop pointed out that these results are similar to those at other centers using EBV third-party T cells.
The initial third-party studies were done in Scotland and had a response rate of about 60%, which increased to around 80% in follow-up studies, where they characterized the T cells more extensively.
Both donor-specific and third-party VSTs have low toxicity, sustained response rates, and activity confirmed by studies in multiple centers.
Dr Heslop believes the rapid manufacturing methodologies will facilitate definitive clinical trials.
She said Cell Medica provided support for some of the trials with EBV tumors.
Photo courtesy of Baylor
College of Medicine
NEW YORK—Researchers are creating virus-specific T cells (VST) to treat and prevent viral infections in patients who undergo hematopoietic stem cell transplant.
Thus far, the group has modified T cells with 5 viral vectors—Epstein-Barr virus (EBV), cytomegalovirus (CMV), adenovirus (ADV), BK virus (BKV), and human herpesvirus 6 (HHV6)—and are devising methods whereby these VSTs can be made readily available, off-the-shelf products.
Helen Heslop, MD, of Baylor College of Medicine in Houston, Texas, described the efforts of the Baylor research team at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
The team’s tri-virus and 5-virus VST approaches have been described previously. Here, we focus on the team’s efforts to create an off-the-shelf product.
A companion story describes the team’s VST approach to treating type 2 EBV-associated lymphomas.
Despite promising results with these earlier methodologies both as prophylaxis and treatment after stem cell transplant, problems existed with the approaches that would impede broader implementation of VSTs.
“Most of these initial methodologies were complex,” Dr Heslop said.
And even though the production time of the 5-virus VSTs is only 10 days, it does not allow for urgent use.
To solve this problem, the researchers are developing VSTs as off-the-shelf, third-party banked cells for patients who don’t have the time to wait for donor-specific cells to be made.
“The strategy here is that we make lines that are well-characterized but are HLA-restricted and tied to specific viruses,” Dr Heslop said.
The cells are then cryopreserved so that they’re available, and patients receive VSTs according to their HLA type and the line that has suitable activity for their infections.
“We initially evaluated this approach through a multicenter study sponsored by the NHLBI [National Heart, Lung, and Blood Institute],” Dr Heslop said.
Tri-virus approach
The researchers used the original tri-virus methodology, which was lengthy, “but, in this case, because the cells were already available, the time was not a major issue,” Dr Heslop said.
The team also made some new lines for donors with common alleles. In all, they had 32 lines available while the study was running.
They treated 50 patients: 23 received VSTs for CMV, 18 for ADV, and 9 for EBV.
One patient who had CMV colitis received the VSTs and had a complete response (CR), as evidenced by a normal endoscopy with no viral inclusions.
Another patient had EBV persistent after 6 doses of rituximab. One month after receiving the VST infusion, the patient had a CR, even though the cell line had only 1 class 2 allele. And the patient has sustained the CR for several years.
The overall response rate for the study is 74.0% at day 42 after infusion.
The response rate was not significantly different for each virus, Dr Heslop pointed out. Patients with CMV had a 73.9% response rate, those with EBV had a 66.7% response rate, and those with ADV had a 77.8% response rate.
“This is a little bit lower than with the donor-specific T cells, but I think it’s still a promising approach,” she added.
5-virus peptide mix
The researchers are now evaluating the more rapid, 5-virus peptide mix method for creating off-the-shelf VSTs.
This method replaced live viruses with overlapping peptide pools and added immunogenic antigens for 5 viruses, including BKV and HHV6. The process takes only 10 days to produce VSTs.
The team has identified a line for over 90% of the patients screened.
“That’s because we will accept a line that’s only matched at 1 HLA allele, as long as we have activity against the infecting virus through the shared allele,” Dr Heslop explained.
So they’re conducting a clinical trial using this method, and thus far, they have enrolled 22 patients. Sixteen patients have had 1 infusion, and 6 patients have had multiple infusions.
The 22 patients had 25 infections: 10 CMV, 10 BKV, 2 EBV, 2 ADV, and 1 HHV6.
The overall response rate is 88%. Nine of 10 responses in patients with BKV were partial because BK is difficult to clear from urine. However, the BK patients who had hemorrhagic cystitis all had symptomatic improvement.
Dr Heslop pointed out that these results are similar to those at other centers using EBV third-party T cells.
The initial third-party studies were done in Scotland and had a response rate of about 60%, which increased to around 80% in follow-up studies, where they characterized the T cells more extensively.
Both donor-specific and third-party VSTs have low toxicity, sustained response rates, and activity confirmed by studies in multiple centers.
Dr Heslop believes the rapid manufacturing methodologies will facilitate definitive clinical trials.
She said Cell Medica provided support for some of the trials with EBV tumors.
Patients may need anticoagulation

A new study suggests that certain patients with bioprosthetic aortic heart valves may require anticoagulant therapy.
In some patients, researchers observed reduced motion of the leaflets affecting the valve opening.
The team believes this may be a sign of subclinical leaflet thrombosis, particularly since anticoagulant therapy was able to restore leaflet motion.
The researchers described this study in NEJM.
“Transcatheter and surgically implantable tissue valves are life-saving devices in patients with aortic valve stenosis,” said study author Raj Makkar, MD, of the Cedars-Sinai Heart Institute in Los Angeles, California.
“These findings allow us a potentially valuable opportunity to further optimize the outcomes of these procedures. We are not recommending that all patients with these devices be on blood thinners, but, clearly, further studies need to be done to define best medication regimens.”
Dr Makkar and his colleagues began this research when a clinical trial participant with a bioprosthetic aortic heart valve had a stroke. High-resolution imaging revealed reduced motion of the leaflets that open and close to regulate the flow of blood.
“We wanted to find out if patients undergoing a tissue valve procedure are susceptible to blood clots on the leaflets and study the clinical consequences of the same,” Dr Makkar said.
“We also wanted to understand whether our aortic valve patients were more susceptible to having blood clots and whether those clots could indicate that the patient might experience a neurological complication—a mini-stroke.”
So Dr Makkar and his colleagues analyzed 187 patients who received a new valve via a transcatheter procedure or open-heart surgery—55 patients in a trial and 132 patients enrolled in registries.
All patients underwent high-resolution imaging—4-dimensional CT angiography—so the researchers could detect reduced leaflet motion.
Overall, 20% of patients (39/187) had reduced leaflet motion—40% in the trial (22/55) and 13% (17/132) in the registries. This included patients with multiple bioprosthesis types.
The researchers observed a lower incidence of reduced leaflet motion in patients receiving anticoagulant therapy.
The incidence was significantly lower in patients on warfarin than in those receiving dual antiplatelet therapy. It was 0% and 55%, respectively, in the clinical trial (P=0.01) and 0% and 29%, respectively, in the registry patients (P=0.04).
Dr Makkar and his colleagues also re-evaluated a handful of patients who underwent a follow-up CT—11 who were receiving anticoagulation and 10 who were not. Leaflet motion was restored in all 11 treated patients and 1 of the untreated patients (P<0.001).
Lastly, there was some suggestion that the incidence of stroke or transient ischemic attacks might be higher among patients with reduced valve motion. But the researchers said this finding was inconclusive and requires further study.
A new study suggests that certain patients with bioprosthetic aortic heart valves may require anticoagulant therapy.
In some patients, researchers observed reduced motion of the leaflets affecting the valve opening.
The team believes this may be a sign of subclinical leaflet thrombosis, particularly since anticoagulant therapy was able to restore leaflet motion.
The researchers described this study in NEJM.
“Transcatheter and surgically implantable tissue valves are life-saving devices in patients with aortic valve stenosis,” said study author Raj Makkar, MD, of the Cedars-Sinai Heart Institute in Los Angeles, California.
“These findings allow us a potentially valuable opportunity to further optimize the outcomes of these procedures. We are not recommending that all patients with these devices be on blood thinners, but, clearly, further studies need to be done to define best medication regimens.”
Dr Makkar and his colleagues began this research when a clinical trial participant with a bioprosthetic aortic heart valve had a stroke. High-resolution imaging revealed reduced motion of the leaflets that open and close to regulate the flow of blood.
“We wanted to find out if patients undergoing a tissue valve procedure are susceptible to blood clots on the leaflets and study the clinical consequences of the same,” Dr Makkar said.
“We also wanted to understand whether our aortic valve patients were more susceptible to having blood clots and whether those clots could indicate that the patient might experience a neurological complication—a mini-stroke.”
So Dr Makkar and his colleagues analyzed 187 patients who received a new valve via a transcatheter procedure or open-heart surgery—55 patients in a trial and 132 patients enrolled in registries.
All patients underwent high-resolution imaging—4-dimensional CT angiography—so the researchers could detect reduced leaflet motion.
Overall, 20% of patients (39/187) had reduced leaflet motion—40% in the trial (22/55) and 13% (17/132) in the registries. This included patients with multiple bioprosthesis types.
The researchers observed a lower incidence of reduced leaflet motion in patients receiving anticoagulant therapy.
The incidence was significantly lower in patients on warfarin than in those receiving dual antiplatelet therapy. It was 0% and 55%, respectively, in the clinical trial (P=0.01) and 0% and 29%, respectively, in the registry patients (P=0.04).
Dr Makkar and his colleagues also re-evaluated a handful of patients who underwent a follow-up CT—11 who were receiving anticoagulation and 10 who were not. Leaflet motion was restored in all 11 treated patients and 1 of the untreated patients (P<0.001).
Lastly, there was some suggestion that the incidence of stroke or transient ischemic attacks might be higher among patients with reduced valve motion. But the researchers said this finding was inconclusive and requires further study.
A new study suggests that certain patients with bioprosthetic aortic heart valves may require anticoagulant therapy.
In some patients, researchers observed reduced motion of the leaflets affecting the valve opening.
The team believes this may be a sign of subclinical leaflet thrombosis, particularly since anticoagulant therapy was able to restore leaflet motion.
The researchers described this study in NEJM.
“Transcatheter and surgically implantable tissue valves are life-saving devices in patients with aortic valve stenosis,” said study author Raj Makkar, MD, of the Cedars-Sinai Heart Institute in Los Angeles, California.
“These findings allow us a potentially valuable opportunity to further optimize the outcomes of these procedures. We are not recommending that all patients with these devices be on blood thinners, but, clearly, further studies need to be done to define best medication regimens.”
Dr Makkar and his colleagues began this research when a clinical trial participant with a bioprosthetic aortic heart valve had a stroke. High-resolution imaging revealed reduced motion of the leaflets that open and close to regulate the flow of blood.
“We wanted to find out if patients undergoing a tissue valve procedure are susceptible to blood clots on the leaflets and study the clinical consequences of the same,” Dr Makkar said.
“We also wanted to understand whether our aortic valve patients were more susceptible to having blood clots and whether those clots could indicate that the patient might experience a neurological complication—a mini-stroke.”
So Dr Makkar and his colleagues analyzed 187 patients who received a new valve via a transcatheter procedure or open-heart surgery—55 patients in a trial and 132 patients enrolled in registries.
All patients underwent high-resolution imaging—4-dimensional CT angiography—so the researchers could detect reduced leaflet motion.
Overall, 20% of patients (39/187) had reduced leaflet motion—40% in the trial (22/55) and 13% (17/132) in the registries. This included patients with multiple bioprosthesis types.
The researchers observed a lower incidence of reduced leaflet motion in patients receiving anticoagulant therapy.
The incidence was significantly lower in patients on warfarin than in those receiving dual antiplatelet therapy. It was 0% and 55%, respectively, in the clinical trial (P=0.01) and 0% and 29%, respectively, in the registry patients (P=0.04).
Dr Makkar and his colleagues also re-evaluated a handful of patients who underwent a follow-up CT—11 who were receiving anticoagulation and 10 who were not. Leaflet motion was restored in all 11 treated patients and 1 of the untreated patients (P<0.001).
Lastly, there was some suggestion that the incidence of stroke or transient ischemic attacks might be higher among patients with reduced valve motion. But the researchers said this finding was inconclusive and requires further study.