User login
Dendritic cells appear to promote T-ALL

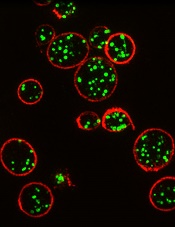
Dendritic cells may play a key role in T-cell acute lymphoblastic leukemia (T-ALL), according to research published in PNAS.
Investigators identified tumor-associated dendritic cells that appeared to promote T-ALL growth and survival at primary and metastatic tumor sites in mice.
Analyses of samples from patients with T-ALL suggested dendritic cells are positioned to support T-ALL growth in humans as well.
“It’s only more recently that people have really appreciated that tumors are complex organs in and of themselves, with all of the heterogenous cell types that can talk to each other and promote each other’s survival and proliferation,” said study author Lauren Ehrlich, PhD, of the University of Texas at Austin.
Dr Ehrlich and her colleagues first found that primary T-ALL cells required tumor stroma for survival ex vivo. When T-ALL cells were cultured alone or in wild-type thymic stroma, the cells died off. Only T-ALL cells cultured with tumor-associated stroma survived.
Subsequent experiments suggested it was tumor-associated dendritic cells that spurred T-ALL growth, both for newly developing T-ALL cells and tumors that had spread to distant organs in mouse models. Tissue samples from pediatric T-ALL patients had similar growth environments with abundant dendritic cells.
To determine the mechanism by which dendritic cells support T-ALL, the investigators performed gene expression profiling. They found upregulation of PDGFRB and IGF1R on T-ALL cells, with concomitant expression of their ligands by tumor-associated dendritic cells.
The team said PDGFRB and IGF1R were activated in T-ALL cells ex vivo. And when they cocultured T-ALL cells with tumor-associated dendritic cells, they observed sustained IGF1R activation. However, they did not see this activation when they cocultured T-ALL cells with normal thymic dendritic cells.
Finally, the investigators found that IGF1R signaling was necessary for dendritic cell-mediated T-ALL survival.
The team said this is the first evidence that endogenous tumor-associated dendritic cells supply signals driving T-ALL growth.
“We hope this study will be a catalyst to spur other research groups to further elucidate the roles of dendritic cells in supporting T-ALL,” said study author Todd Triplett, PhD, also of the University of Texas at Austin.
“[T]hat could ultimately lead to the discovery of novel therapeutic targets that are more effective and less toxic than current treatment regimens.” ![]()
Dendritic cells may play a key role in T-cell acute lymphoblastic leukemia (T-ALL), according to research published in PNAS.
Investigators identified tumor-associated dendritic cells that appeared to promote T-ALL growth and survival at primary and metastatic tumor sites in mice.
Analyses of samples from patients with T-ALL suggested dendritic cells are positioned to support T-ALL growth in humans as well.
“It’s only more recently that people have really appreciated that tumors are complex organs in and of themselves, with all of the heterogenous cell types that can talk to each other and promote each other’s survival and proliferation,” said study author Lauren Ehrlich, PhD, of the University of Texas at Austin.
Dr Ehrlich and her colleagues first found that primary T-ALL cells required tumor stroma for survival ex vivo. When T-ALL cells were cultured alone or in wild-type thymic stroma, the cells died off. Only T-ALL cells cultured with tumor-associated stroma survived.
Subsequent experiments suggested it was tumor-associated dendritic cells that spurred T-ALL growth, both for newly developing T-ALL cells and tumors that had spread to distant organs in mouse models. Tissue samples from pediatric T-ALL patients had similar growth environments with abundant dendritic cells.
To determine the mechanism by which dendritic cells support T-ALL, the investigators performed gene expression profiling. They found upregulation of PDGFRB and IGF1R on T-ALL cells, with concomitant expression of their ligands by tumor-associated dendritic cells.
The team said PDGFRB and IGF1R were activated in T-ALL cells ex vivo. And when they cocultured T-ALL cells with tumor-associated dendritic cells, they observed sustained IGF1R activation. However, they did not see this activation when they cocultured T-ALL cells with normal thymic dendritic cells.
Finally, the investigators found that IGF1R signaling was necessary for dendritic cell-mediated T-ALL survival.
The team said this is the first evidence that endogenous tumor-associated dendritic cells supply signals driving T-ALL growth.
“We hope this study will be a catalyst to spur other research groups to further elucidate the roles of dendritic cells in supporting T-ALL,” said study author Todd Triplett, PhD, also of the University of Texas at Austin.
“[T]hat could ultimately lead to the discovery of novel therapeutic targets that are more effective and less toxic than current treatment regimens.” ![]()
Dendritic cells may play a key role in T-cell acute lymphoblastic leukemia (T-ALL), according to research published in PNAS.
Investigators identified tumor-associated dendritic cells that appeared to promote T-ALL growth and survival at primary and metastatic tumor sites in mice.
Analyses of samples from patients with T-ALL suggested dendritic cells are positioned to support T-ALL growth in humans as well.
“It’s only more recently that people have really appreciated that tumors are complex organs in and of themselves, with all of the heterogenous cell types that can talk to each other and promote each other’s survival and proliferation,” said study author Lauren Ehrlich, PhD, of the University of Texas at Austin.
Dr Ehrlich and her colleagues first found that primary T-ALL cells required tumor stroma for survival ex vivo. When T-ALL cells were cultured alone or in wild-type thymic stroma, the cells died off. Only T-ALL cells cultured with tumor-associated stroma survived.
Subsequent experiments suggested it was tumor-associated dendritic cells that spurred T-ALL growth, both for newly developing T-ALL cells and tumors that had spread to distant organs in mouse models. Tissue samples from pediatric T-ALL patients had similar growth environments with abundant dendritic cells.
To determine the mechanism by which dendritic cells support T-ALL, the investigators performed gene expression profiling. They found upregulation of PDGFRB and IGF1R on T-ALL cells, with concomitant expression of their ligands by tumor-associated dendritic cells.
The team said PDGFRB and IGF1R were activated in T-ALL cells ex vivo. And when they cocultured T-ALL cells with tumor-associated dendritic cells, they observed sustained IGF1R activation. However, they did not see this activation when they cocultured T-ALL cells with normal thymic dendritic cells.
Finally, the investigators found that IGF1R signaling was necessary for dendritic cell-mediated T-ALL survival.
The team said this is the first evidence that endogenous tumor-associated dendritic cells supply signals driving T-ALL growth.
“We hope this study will be a catalyst to spur other research groups to further elucidate the roles of dendritic cells in supporting T-ALL,” said study author Todd Triplett, PhD, also of the University of Texas at Austin.
“[T]hat could ultimately lead to the discovery of novel therapeutic targets that are more effective and less toxic than current treatment regimens.” ![]()
Development of myelofibrosis drug on hold

The US Food and Drug Administration (FDA) has placed a full clinical hold on trials conducted under the investigational new drug application for pacritinib, a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The hold means all patients currently on pacritinib must stop taking the drug immediately, and no patients can be enrolled on a pacritinib trial or start pacritinib as initial or crossover treatment.
In addition, CTI BioPharma has withdrawn the new drug application for pacritinib while the company reviews data from the phase 3 PERSIST-2 trial.
The FDA’s decision to place a full clinical hold on pacritinib trials was due to interim results from PERSIST-2. The aim of this trial was to compare pacritinib to best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
The overall survival results from PERSIST-2 indicate that pacritinib had a detrimental effect on survival, which is consistent with results from the PERSIST-1 trial. The deaths in pacritinib-treated patients on PERSIST-2 include intracranial hemorrhage, cardiac failure, and cardiac arrest.
Based on these results, the FDA has made recommendations for CTI BioPharma that supersede the agency’s previous recommendations.
On February 4, 2016, the FDA placed a partial clinical hold on pacritinib trials and made related recommendations for CTI BioPharma, advising that the company modify trial protocols and take other actions in compliance with the partial clinical hold.
Now that pacritinib trials are on full clinical hold, the FDA is recommending that CTI BioPharma conduct dose exploration studies for pacritinib in patients with MF and submit final study reports and datasets for PERSIST-1 and PERSIST-2.
The FDA is also recommending that CTI BioPharma provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, make certain modifications to protocols, and request a meeting with the FDA prior to submitting a response to the full clinical hold.
CTI BioPharma said all clinical investigators worldwide have been notified of the hold. ![]()
The US Food and Drug Administration (FDA) has placed a full clinical hold on trials conducted under the investigational new drug application for pacritinib, a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The hold means all patients currently on pacritinib must stop taking the drug immediately, and no patients can be enrolled on a pacritinib trial or start pacritinib as initial or crossover treatment.
In addition, CTI BioPharma has withdrawn the new drug application for pacritinib while the company reviews data from the phase 3 PERSIST-2 trial.
The FDA’s decision to place a full clinical hold on pacritinib trials was due to interim results from PERSIST-2. The aim of this trial was to compare pacritinib to best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
The overall survival results from PERSIST-2 indicate that pacritinib had a detrimental effect on survival, which is consistent with results from the PERSIST-1 trial. The deaths in pacritinib-treated patients on PERSIST-2 include intracranial hemorrhage, cardiac failure, and cardiac arrest.
Based on these results, the FDA has made recommendations for CTI BioPharma that supersede the agency’s previous recommendations.
On February 4, 2016, the FDA placed a partial clinical hold on pacritinib trials and made related recommendations for CTI BioPharma, advising that the company modify trial protocols and take other actions in compliance with the partial clinical hold.
Now that pacritinib trials are on full clinical hold, the FDA is recommending that CTI BioPharma conduct dose exploration studies for pacritinib in patients with MF and submit final study reports and datasets for PERSIST-1 and PERSIST-2.
The FDA is also recommending that CTI BioPharma provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, make certain modifications to protocols, and request a meeting with the FDA prior to submitting a response to the full clinical hold.
CTI BioPharma said all clinical investigators worldwide have been notified of the hold. ![]()
The US Food and Drug Administration (FDA) has placed a full clinical hold on trials conducted under the investigational new drug application for pacritinib, a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The hold means all patients currently on pacritinib must stop taking the drug immediately, and no patients can be enrolled on a pacritinib trial or start pacritinib as initial or crossover treatment.
In addition, CTI BioPharma has withdrawn the new drug application for pacritinib while the company reviews data from the phase 3 PERSIST-2 trial.
The FDA’s decision to place a full clinical hold on pacritinib trials was due to interim results from PERSIST-2. The aim of this trial was to compare pacritinib to best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
The overall survival results from PERSIST-2 indicate that pacritinib had a detrimental effect on survival, which is consistent with results from the PERSIST-1 trial. The deaths in pacritinib-treated patients on PERSIST-2 include intracranial hemorrhage, cardiac failure, and cardiac arrest.
Based on these results, the FDA has made recommendations for CTI BioPharma that supersede the agency’s previous recommendations.
On February 4, 2016, the FDA placed a partial clinical hold on pacritinib trials and made related recommendations for CTI BioPharma, advising that the company modify trial protocols and take other actions in compliance with the partial clinical hold.
Now that pacritinib trials are on full clinical hold, the FDA is recommending that CTI BioPharma conduct dose exploration studies for pacritinib in patients with MF and submit final study reports and datasets for PERSIST-1 and PERSIST-2.
The FDA is also recommending that CTI BioPharma provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, make certain modifications to protocols, and request a meeting with the FDA prior to submitting a response to the full clinical hold.
CTI BioPharma said all clinical investigators worldwide have been notified of the hold. ![]()
Chemo regimen can be ‘highly effective’ against ENKTL

Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
Method could improve diagnosis of platelet disorders
Courtesy of Dan Cutler
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
Courtesy of Dan Cutler
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
Courtesy of Dan Cutler
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
EBV-CTLs get orphan designation for EBV-PTLD

among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
Gut microbiota linked to severity of malaria

Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Dual inhibitor could treat ATLL

Photo by Larry Young
SAN FRANCISCO—Preclinical research suggests a compound that inhibits both EZH1 and EZH2 could be effective against adult T-cell leukemia/lymphoma (ATLL).
The compound, known as OR-S1, has demonstrated activity against ATLL in vitro and in vivo.
Researchers said OR-S1 reversed epigenetic disruption in ATLL cells, selectively eliminated both ATLL cells and cells infected with human T-cell leukemia virus type I (HTLV-1), and inhibited tumor growth in mouse models of ATLL.
Based on these results, the researchers are planning a phase 1 study of the compound.
Makoto Yamagishi, PhD, of The University of Tokyo in Japan, described the preclinical research with OR-S1 and discussed the rationale for developing the compound at the 8th Annual T-cell Lymphoma Forum. The work was carried out in collaboration with Daiichi Sankyo Co., Ltd.
“We do not precisely understand the molecular mechanism of ATLL development, including genetic and epigenetic abnormalities,” Dr Yamagishi noted.
To gain some insight, he and his colleagues performed microRNA profiling, gene expression profiling, and histone methylation/epigenetic factor profiling on cells from ATLL patients and CD4+ T cells from healthy donors.
The team found that PRC2 factors were significantly upregulated in ATLL. EZH2 was the most upregulated histone methyltransferase, but ATLL cells did not have active mutations in the EZH2 gene. Dr Yamagishi said this suggests EZH2 upregulation is critical for the ATLL-specific epigenome.
“At long last, we determined the epigenetic pattern of ATLL,” he said. “ATLL cells showed specific and significant reprogramming of the epigenome, especially H3K27me3 gain. We found abnormal H3K27me3 change in half of genes, and gain was dominant.”
“But, interestingly, the methylated genes are specific in ATLL and do not overlap with other EZH2-dependent cell types, such as embryonic stem cells and diffuse large B-cell lymphoma cells. So ATLL has a very unique epigenome.”
Further investigation revealed that both EZH1 and EZH2 contribute to ATLL-specific epigenetic deregulation. More than 80% of H3K27me3 accumulated genes are occupied by EZH1 and/or EZH2.
So the researchers decided to examine the effects of knocking down EZH1 and EZH2 in ATLL cells.
Compared with knockdown of either gene alone, double knockdown synergistically influenced target gene expression. It led to complete dysfunction of the Polycomb family and had a significant impact on ATLL cell survival.
The researchers also found that EZH1 depletion enhanced ATLL cells’ sensitivity to the EZH2 inhibitor GSK126.
So the team decided to develop a dual EZH1/EZH2 inhibitor. They created OR-S1, which showed “strong activity” against EZH1 and EZH2 but none of the other histone methyltransferases tested.
In in vitro experiments, OR-S1 completely removed H3K27me3 and significantly reduced cell growth in the ATLL-derived cell line TL-Om1.
The drug also reduced cell viability in primary ATLL cells. All 15 samples tested proved sensitive to OR-S1. In addition, OR-S1 treatment selectively removed HTLV-1-infected cells from samples taken from 16 asymptomatic carriers.
Finally, OR-S1 proved active in mice. The drug prevented engraftment of ATLL cells in immunocompromised mice. All 6 OR-S1-treated mice were alive and tumor-free at 49 days, whereas 5 of 6 control mice had died (P=0.0041).
In mice treated after ATLL cell engraftment, OR-S1 reduced tumor growth without causing notable weight loss.
“Synthetic lethality by targeting EZH1 and EZH2 is promising [for ATLL],” Dr Yamagishi said. “Toxicity tests suggest the EZH1/2 dual inhibitor may be sufficient for clinical use, so we are now planning a phase 1 study.” ![]()
Photo by Larry Young
SAN FRANCISCO—Preclinical research suggests a compound that inhibits both EZH1 and EZH2 could be effective against adult T-cell leukemia/lymphoma (ATLL).
The compound, known as OR-S1, has demonstrated activity against ATLL in vitro and in vivo.
Researchers said OR-S1 reversed epigenetic disruption in ATLL cells, selectively eliminated both ATLL cells and cells infected with human T-cell leukemia virus type I (HTLV-1), and inhibited tumor growth in mouse models of ATLL.
Based on these results, the researchers are planning a phase 1 study of the compound.
Makoto Yamagishi, PhD, of The University of Tokyo in Japan, described the preclinical research with OR-S1 and discussed the rationale for developing the compound at the 8th Annual T-cell Lymphoma Forum. The work was carried out in collaboration with Daiichi Sankyo Co., Ltd.
“We do not precisely understand the molecular mechanism of ATLL development, including genetic and epigenetic abnormalities,” Dr Yamagishi noted.
To gain some insight, he and his colleagues performed microRNA profiling, gene expression profiling, and histone methylation/epigenetic factor profiling on cells from ATLL patients and CD4+ T cells from healthy donors.
The team found that PRC2 factors were significantly upregulated in ATLL. EZH2 was the most upregulated histone methyltransferase, but ATLL cells did not have active mutations in the EZH2 gene. Dr Yamagishi said this suggests EZH2 upregulation is critical for the ATLL-specific epigenome.
“At long last, we determined the epigenetic pattern of ATLL,” he said. “ATLL cells showed specific and significant reprogramming of the epigenome, especially H3K27me3 gain. We found abnormal H3K27me3 change in half of genes, and gain was dominant.”
“But, interestingly, the methylated genes are specific in ATLL and do not overlap with other EZH2-dependent cell types, such as embryonic stem cells and diffuse large B-cell lymphoma cells. So ATLL has a very unique epigenome.”
Further investigation revealed that both EZH1 and EZH2 contribute to ATLL-specific epigenetic deregulation. More than 80% of H3K27me3 accumulated genes are occupied by EZH1 and/or EZH2.
So the researchers decided to examine the effects of knocking down EZH1 and EZH2 in ATLL cells.
Compared with knockdown of either gene alone, double knockdown synergistically influenced target gene expression. It led to complete dysfunction of the Polycomb family and had a significant impact on ATLL cell survival.
The researchers also found that EZH1 depletion enhanced ATLL cells’ sensitivity to the EZH2 inhibitor GSK126.
So the team decided to develop a dual EZH1/EZH2 inhibitor. They created OR-S1, which showed “strong activity” against EZH1 and EZH2 but none of the other histone methyltransferases tested.
In in vitro experiments, OR-S1 completely removed H3K27me3 and significantly reduced cell growth in the ATLL-derived cell line TL-Om1.
The drug also reduced cell viability in primary ATLL cells. All 15 samples tested proved sensitive to OR-S1. In addition, OR-S1 treatment selectively removed HTLV-1-infected cells from samples taken from 16 asymptomatic carriers.
Finally, OR-S1 proved active in mice. The drug prevented engraftment of ATLL cells in immunocompromised mice. All 6 OR-S1-treated mice were alive and tumor-free at 49 days, whereas 5 of 6 control mice had died (P=0.0041).
In mice treated after ATLL cell engraftment, OR-S1 reduced tumor growth without causing notable weight loss.
“Synthetic lethality by targeting EZH1 and EZH2 is promising [for ATLL],” Dr Yamagishi said. “Toxicity tests suggest the EZH1/2 dual inhibitor may be sufficient for clinical use, so we are now planning a phase 1 study.” ![]()
Photo by Larry Young
SAN FRANCISCO—Preclinical research suggests a compound that inhibits both EZH1 and EZH2 could be effective against adult T-cell leukemia/lymphoma (ATLL).
The compound, known as OR-S1, has demonstrated activity against ATLL in vitro and in vivo.
Researchers said OR-S1 reversed epigenetic disruption in ATLL cells, selectively eliminated both ATLL cells and cells infected with human T-cell leukemia virus type I (HTLV-1), and inhibited tumor growth in mouse models of ATLL.
Based on these results, the researchers are planning a phase 1 study of the compound.
Makoto Yamagishi, PhD, of The University of Tokyo in Japan, described the preclinical research with OR-S1 and discussed the rationale for developing the compound at the 8th Annual T-cell Lymphoma Forum. The work was carried out in collaboration with Daiichi Sankyo Co., Ltd.
“We do not precisely understand the molecular mechanism of ATLL development, including genetic and epigenetic abnormalities,” Dr Yamagishi noted.
To gain some insight, he and his colleagues performed microRNA profiling, gene expression profiling, and histone methylation/epigenetic factor profiling on cells from ATLL patients and CD4+ T cells from healthy donors.
The team found that PRC2 factors were significantly upregulated in ATLL. EZH2 was the most upregulated histone methyltransferase, but ATLL cells did not have active mutations in the EZH2 gene. Dr Yamagishi said this suggests EZH2 upregulation is critical for the ATLL-specific epigenome.
“At long last, we determined the epigenetic pattern of ATLL,” he said. “ATLL cells showed specific and significant reprogramming of the epigenome, especially H3K27me3 gain. We found abnormal H3K27me3 change in half of genes, and gain was dominant.”
“But, interestingly, the methylated genes are specific in ATLL and do not overlap with other EZH2-dependent cell types, such as embryonic stem cells and diffuse large B-cell lymphoma cells. So ATLL has a very unique epigenome.”
Further investigation revealed that both EZH1 and EZH2 contribute to ATLL-specific epigenetic deregulation. More than 80% of H3K27me3 accumulated genes are occupied by EZH1 and/or EZH2.
So the researchers decided to examine the effects of knocking down EZH1 and EZH2 in ATLL cells.
Compared with knockdown of either gene alone, double knockdown synergistically influenced target gene expression. It led to complete dysfunction of the Polycomb family and had a significant impact on ATLL cell survival.
The researchers also found that EZH1 depletion enhanced ATLL cells’ sensitivity to the EZH2 inhibitor GSK126.
So the team decided to develop a dual EZH1/EZH2 inhibitor. They created OR-S1, which showed “strong activity” against EZH1 and EZH2 but none of the other histone methyltransferases tested.
In in vitro experiments, OR-S1 completely removed H3K27me3 and significantly reduced cell growth in the ATLL-derived cell line TL-Om1.
The drug also reduced cell viability in primary ATLL cells. All 15 samples tested proved sensitive to OR-S1. In addition, OR-S1 treatment selectively removed HTLV-1-infected cells from samples taken from 16 asymptomatic carriers.
Finally, OR-S1 proved active in mice. The drug prevented engraftment of ATLL cells in immunocompromised mice. All 6 OR-S1-treated mice were alive and tumor-free at 49 days, whereas 5 of 6 control mice had died (P=0.0041).
In mice treated after ATLL cell engraftment, OR-S1 reduced tumor growth without causing notable weight loss.
“Synthetic lethality by targeting EZH1 and EZH2 is promising [for ATLL],” Dr Yamagishi said. “Toxicity tests suggest the EZH1/2 dual inhibitor may be sufficient for clinical use, so we are now planning a phase 1 study.”
New insight into Ph-like ALL could lead to new treatment
Photo courtesy of St. Jude
Children’s Research Hospital
Research published in Cancer Cell appears to explain how the abnormal breakage and rearrangement of chromosomes in white blood cells triggers Philadelphia chromosome-like (Ph-like) acute lymphoblastic leukemia (ALL).
Genomic analysis revealed 4 chromosomal rearrangements that all resulted in a truncated version of the erythropoietin receptor (EPOR) gene and drove white blood cells to proliferate out of control.
“To our knowledge, this is a previously unknown mechanism for leukemia,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Our search of cancer genomic data has shown that there are many other examples of chromosomal rearrangements that alter genes’ structure, but this type—where a truncating rearrangement leads to activation—is new.”
Although Dr Mullighan and his colleagues had previously identified an abnormal chromosome rearrangement in Ph-like ALL, little was known about the biological effects of that rearrangement. So they set out to pinpoint those effects by studying human leukemic cells and mouse cells engineered to mimic Ph-like ALL.
The investigators discovered the 4 rearrangements of EPOR, all of which resulted in truncation of the cytoplasmic tail of EPOR at residues similar to those mutated in primary familial congenital polycythemia. The proximal tyrosine essential for receptor activation was preserved, but distal regulatory residues were lost.
The team said these rearrangements resulted in deregulated EPOR expression, hypersensitivity to erythropoietin stimulation, and heightened JAK-STAT activation.
The investigators noted that the rearrangements were present in all of the leukemic cells from patients, which suggests these changes were fundamental to Ph-like ALL development. The team also showed that introducing truncated EPOR in mouse B-cell progenitors gave rise to ALL in mice.
Further investigation revealed that EPOR rearrangements arise early in the development of Ph-like ALL and persist as the disease progresses.
“That finding was important because it suggests that treatments for this leukemia targeting this receptor won’t just impact a subset of the leukemia cells, allowing others to keep proliferating,” said study author Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital.
The investigators then found that human leukemic cells with EPOR rearrangements were sensitive to JAK-STAT inhibition via treatment with ruxolitinib.
The team also cited the case of an adult patient treated at MD Anderson Cancer Research Center in Houston, Texas, whose genetic analysis revealed EPOR-rearranged ALL. That patient had not responded significantly to other chemotherapy drugs. But, when given ruxolitinib, the patient showed a major drop in leukemia cells.
In experiments with leukemic cells, the investigators found that ruxolitinib worked synergistically with 3 chemotherapeutic agents—dexamethasone, vincristine, and daunorubicin.
“We think these findings provide a useful road map for planning more accurate testing of combination chemotherapies,” Dr Mullighan said.
“These findings expand the number of ALL patients who should be amenable to precision medicine therapies that add targeted inhibitors to chemotherapy for ALL patents with specific genetic changes in the leukemia cells,” added study author Stephen Hunger, MD, of Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hunger said the Children’s Oncology Group has developed a clinical trial testing this strategy with ruxolitinib, which will begin treating patients in mid-2016. Based on the results of the Cancer Cell research, the trial will include children with ALL and EPOR rearrangements.
Photo courtesy of St. Jude
Children’s Research Hospital
Research published in Cancer Cell appears to explain how the abnormal breakage and rearrangement of chromosomes in white blood cells triggers Philadelphia chromosome-like (Ph-like) acute lymphoblastic leukemia (ALL).
Genomic analysis revealed 4 chromosomal rearrangements that all resulted in a truncated version of the erythropoietin receptor (EPOR) gene and drove white blood cells to proliferate out of control.
“To our knowledge, this is a previously unknown mechanism for leukemia,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Our search of cancer genomic data has shown that there are many other examples of chromosomal rearrangements that alter genes’ structure, but this type—where a truncating rearrangement leads to activation—is new.”
Although Dr Mullighan and his colleagues had previously identified an abnormal chromosome rearrangement in Ph-like ALL, little was known about the biological effects of that rearrangement. So they set out to pinpoint those effects by studying human leukemic cells and mouse cells engineered to mimic Ph-like ALL.
The investigators discovered the 4 rearrangements of EPOR, all of which resulted in truncation of the cytoplasmic tail of EPOR at residues similar to those mutated in primary familial congenital polycythemia. The proximal tyrosine essential for receptor activation was preserved, but distal regulatory residues were lost.
The team said these rearrangements resulted in deregulated EPOR expression, hypersensitivity to erythropoietin stimulation, and heightened JAK-STAT activation.
The investigators noted that the rearrangements were present in all of the leukemic cells from patients, which suggests these changes were fundamental to Ph-like ALL development. The team also showed that introducing truncated EPOR in mouse B-cell progenitors gave rise to ALL in mice.
Further investigation revealed that EPOR rearrangements arise early in the development of Ph-like ALL and persist as the disease progresses.
“That finding was important because it suggests that treatments for this leukemia targeting this receptor won’t just impact a subset of the leukemia cells, allowing others to keep proliferating,” said study author Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital.
The investigators then found that human leukemic cells with EPOR rearrangements were sensitive to JAK-STAT inhibition via treatment with ruxolitinib.
The team also cited the case of an adult patient treated at MD Anderson Cancer Research Center in Houston, Texas, whose genetic analysis revealed EPOR-rearranged ALL. That patient had not responded significantly to other chemotherapy drugs. But, when given ruxolitinib, the patient showed a major drop in leukemia cells.
In experiments with leukemic cells, the investigators found that ruxolitinib worked synergistically with 3 chemotherapeutic agents—dexamethasone, vincristine, and daunorubicin.
“We think these findings provide a useful road map for planning more accurate testing of combination chemotherapies,” Dr Mullighan said.
“These findings expand the number of ALL patients who should be amenable to precision medicine therapies that add targeted inhibitors to chemotherapy for ALL patents with specific genetic changes in the leukemia cells,” added study author Stephen Hunger, MD, of Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hunger said the Children’s Oncology Group has developed a clinical trial testing this strategy with ruxolitinib, which will begin treating patients in mid-2016. Based on the results of the Cancer Cell research, the trial will include children with ALL and EPOR rearrangements.
Photo courtesy of St. Jude
Children’s Research Hospital
Research published in Cancer Cell appears to explain how the abnormal breakage and rearrangement of chromosomes in white blood cells triggers Philadelphia chromosome-like (Ph-like) acute lymphoblastic leukemia (ALL).
Genomic analysis revealed 4 chromosomal rearrangements that all resulted in a truncated version of the erythropoietin receptor (EPOR) gene and drove white blood cells to proliferate out of control.
“To our knowledge, this is a previously unknown mechanism for leukemia,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Our search of cancer genomic data has shown that there are many other examples of chromosomal rearrangements that alter genes’ structure, but this type—where a truncating rearrangement leads to activation—is new.”
Although Dr Mullighan and his colleagues had previously identified an abnormal chromosome rearrangement in Ph-like ALL, little was known about the biological effects of that rearrangement. So they set out to pinpoint those effects by studying human leukemic cells and mouse cells engineered to mimic Ph-like ALL.
The investigators discovered the 4 rearrangements of EPOR, all of which resulted in truncation of the cytoplasmic tail of EPOR at residues similar to those mutated in primary familial congenital polycythemia. The proximal tyrosine essential for receptor activation was preserved, but distal regulatory residues were lost.
The team said these rearrangements resulted in deregulated EPOR expression, hypersensitivity to erythropoietin stimulation, and heightened JAK-STAT activation.
The investigators noted that the rearrangements were present in all of the leukemic cells from patients, which suggests these changes were fundamental to Ph-like ALL development. The team also showed that introducing truncated EPOR in mouse B-cell progenitors gave rise to ALL in mice.
Further investigation revealed that EPOR rearrangements arise early in the development of Ph-like ALL and persist as the disease progresses.
“That finding was important because it suggests that treatments for this leukemia targeting this receptor won’t just impact a subset of the leukemia cells, allowing others to keep proliferating,” said study author Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital.
The investigators then found that human leukemic cells with EPOR rearrangements were sensitive to JAK-STAT inhibition via treatment with ruxolitinib.
The team also cited the case of an adult patient treated at MD Anderson Cancer Research Center in Houston, Texas, whose genetic analysis revealed EPOR-rearranged ALL. That patient had not responded significantly to other chemotherapy drugs. But, when given ruxolitinib, the patient showed a major drop in leukemia cells.
In experiments with leukemic cells, the investigators found that ruxolitinib worked synergistically with 3 chemotherapeutic agents—dexamethasone, vincristine, and daunorubicin.
“We think these findings provide a useful road map for planning more accurate testing of combination chemotherapies,” Dr Mullighan said.
“These findings expand the number of ALL patients who should be amenable to precision medicine therapies that add targeted inhibitors to chemotherapy for ALL patents with specific genetic changes in the leukemia cells,” added study author Stephen Hunger, MD, of Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hunger said the Children’s Oncology Group has developed a clinical trial testing this strategy with ruxolitinib, which will begin treating patients in mid-2016. Based on the results of the Cancer Cell research, the trial will include children with ALL and EPOR rearrangements.
Study reveals delays in emergency blood transfusions
![]()
Photo courtesy of UAB Hospital
A new study suggests that as few as 2% of patients with life-threatening bleeding after serious injury receive optimal blood transfusion therapy in England and Wales.
Researchers estimate that nearly 5000 trauma patients sustain a major hemorrhage in England and Wales each year, and one-third of those patients die.
The current study, published in the British Journal of Surgery, highlights how delays in transfusions may contribute to this death rate.
“The rapid and consistent delivery of blood, plasma, platelets, and other clotting products to trauma patients is essential to maintain clotting during hemorrhage and has been shown to halve mortality,” said study author Karim Brohi, MBBS, of Queen Mary University of London in the UK.
“However, we found that only 2% of patients with massive hemorrhage received the optimal type of blood transfusion for their resuscitation. There is a clear opportunity for clinicians to improve the delivery of blood and clotting products during resuscitation for major hemorrhage.”
Dr Brohi and his colleagues analyzed 442 patients treated at 22 hospitals in England and Wales. The patients had experienced major hemorrhage as a result of injuries and received at least 4 units of packed red blood cells (PRBCs) in the first 24 hours of admission.
The patients’ median age was 38 (range, 24-54), and 74% were men. Thirty-three percent of patients (n=146) had massive hemorrhage.
Mortality from bleeding tended to occur early in these patients. Twenty-seven percent of patients (n=117) died in hospital—18% (n=79) within the first 24 hours. The 30-day mortality rate was about 27% (n=119), and 33% of evaluable patients had died at 1 year (127/383).
All 442 patients received PRBCs. The median number of PRBC units transfused within 24 hours was 7 (range, 5-11), and the median number of PRBC units given in 30 days was 9 (range, 6-15).
The average time to transfusion of PRBCs was longer than expected, at 41 minutes (range, 1-122).
Similarly, the researchers found the administration of blood components such as plasma and platelets to be significantly delayed, occurring, on average, 2 to 3 hours after admission.
Three-quarters of patients (n=330) received fresh-frozen plasma (FFP). The median number of FFP units given within 24 hours was 4 (range, 0-7), and the time to first FFP transfusion was 87 minutes (range, 42.5-229).
About 45% of patients (n=197) received platelets. The median dose was 0 (range, 0-1), and the time to first platelet transfusion was 146 minutes (range, 72.5-364).
About 28% of patients (n=122) received cryoprecipitate. The median dose was 0 (range, 0-1), and the time to first cryoprecipitate infusion was 179.5 minutes (range, 84.5-333.5).
“The rapid delivery of the right mix of blood components in an emergency environment is extremely challenging,” Dr Brohi said.
“Some transfusion components have to be thawed and, at present, aren’t always available for the patient quickly enough. More research is also needed into techniques and devices to control bleeding earlier, even at the scene of injury.”
The researchers noted that this study had its limitations, such as incomplete data for some patients.
![]()
Photo courtesy of UAB Hospital
A new study suggests that as few as 2% of patients with life-threatening bleeding after serious injury receive optimal blood transfusion therapy in England and Wales.
Researchers estimate that nearly 5000 trauma patients sustain a major hemorrhage in England and Wales each year, and one-third of those patients die.
The current study, published in the British Journal of Surgery, highlights how delays in transfusions may contribute to this death rate.
“The rapid and consistent delivery of blood, plasma, platelets, and other clotting products to trauma patients is essential to maintain clotting during hemorrhage and has been shown to halve mortality,” said study author Karim Brohi, MBBS, of Queen Mary University of London in the UK.
“However, we found that only 2% of patients with massive hemorrhage received the optimal type of blood transfusion for their resuscitation. There is a clear opportunity for clinicians to improve the delivery of blood and clotting products during resuscitation for major hemorrhage.”
Dr Brohi and his colleagues analyzed 442 patients treated at 22 hospitals in England and Wales. The patients had experienced major hemorrhage as a result of injuries and received at least 4 units of packed red blood cells (PRBCs) in the first 24 hours of admission.
The patients’ median age was 38 (range, 24-54), and 74% were men. Thirty-three percent of patients (n=146) had massive hemorrhage.
Mortality from bleeding tended to occur early in these patients. Twenty-seven percent of patients (n=117) died in hospital—18% (n=79) within the first 24 hours. The 30-day mortality rate was about 27% (n=119), and 33% of evaluable patients had died at 1 year (127/383).
All 442 patients received PRBCs. The median number of PRBC units transfused within 24 hours was 7 (range, 5-11), and the median number of PRBC units given in 30 days was 9 (range, 6-15).
The average time to transfusion of PRBCs was longer than expected, at 41 minutes (range, 1-122).
Similarly, the researchers found the administration of blood components such as plasma and platelets to be significantly delayed, occurring, on average, 2 to 3 hours after admission.
Three-quarters of patients (n=330) received fresh-frozen plasma (FFP). The median number of FFP units given within 24 hours was 4 (range, 0-7), and the time to first FFP transfusion was 87 minutes (range, 42.5-229).
About 45% of patients (n=197) received platelets. The median dose was 0 (range, 0-1), and the time to first platelet transfusion was 146 minutes (range, 72.5-364).
About 28% of patients (n=122) received cryoprecipitate. The median dose was 0 (range, 0-1), and the time to first cryoprecipitate infusion was 179.5 minutes (range, 84.5-333.5).
“The rapid delivery of the right mix of blood components in an emergency environment is extremely challenging,” Dr Brohi said.
“Some transfusion components have to be thawed and, at present, aren’t always available for the patient quickly enough. More research is also needed into techniques and devices to control bleeding earlier, even at the scene of injury.”
The researchers noted that this study had its limitations, such as incomplete data for some patients.
![]()
Photo courtesy of UAB Hospital
A new study suggests that as few as 2% of patients with life-threatening bleeding after serious injury receive optimal blood transfusion therapy in England and Wales.
Researchers estimate that nearly 5000 trauma patients sustain a major hemorrhage in England and Wales each year, and one-third of those patients die.
The current study, published in the British Journal of Surgery, highlights how delays in transfusions may contribute to this death rate.
“The rapid and consistent delivery of blood, plasma, platelets, and other clotting products to trauma patients is essential to maintain clotting during hemorrhage and has been shown to halve mortality,” said study author Karim Brohi, MBBS, of Queen Mary University of London in the UK.
“However, we found that only 2% of patients with massive hemorrhage received the optimal type of blood transfusion for their resuscitation. There is a clear opportunity for clinicians to improve the delivery of blood and clotting products during resuscitation for major hemorrhage.”
Dr Brohi and his colleagues analyzed 442 patients treated at 22 hospitals in England and Wales. The patients had experienced major hemorrhage as a result of injuries and received at least 4 units of packed red blood cells (PRBCs) in the first 24 hours of admission.
The patients’ median age was 38 (range, 24-54), and 74% were men. Thirty-three percent of patients (n=146) had massive hemorrhage.
Mortality from bleeding tended to occur early in these patients. Twenty-seven percent of patients (n=117) died in hospital—18% (n=79) within the first 24 hours. The 30-day mortality rate was about 27% (n=119), and 33% of evaluable patients had died at 1 year (127/383).
All 442 patients received PRBCs. The median number of PRBC units transfused within 24 hours was 7 (range, 5-11), and the median number of PRBC units given in 30 days was 9 (range, 6-15).
The average time to transfusion of PRBCs was longer than expected, at 41 minutes (range, 1-122).
Similarly, the researchers found the administration of blood components such as plasma and platelets to be significantly delayed, occurring, on average, 2 to 3 hours after admission.
Three-quarters of patients (n=330) received fresh-frozen plasma (FFP). The median number of FFP units given within 24 hours was 4 (range, 0-7), and the time to first FFP transfusion was 87 minutes (range, 42.5-229).
About 45% of patients (n=197) received platelets. The median dose was 0 (range, 0-1), and the time to first platelet transfusion was 146 minutes (range, 72.5-364).
About 28% of patients (n=122) received cryoprecipitate. The median dose was 0 (range, 0-1), and the time to first cryoprecipitate infusion was 179.5 minutes (range, 84.5-333.5).
“The rapid delivery of the right mix of blood components in an emergency environment is extremely challenging,” Dr Brohi said.
“Some transfusion components have to be thawed and, at present, aren’t always available for the patient quickly enough. More research is also needed into techniques and devices to control bleeding earlier, even at the scene of injury.”
The researchers noted that this study had its limitations, such as incomplete data for some patients.
MF drug trials placed on partial clinical hold

The US Food and Drug Administration (FDA) has placed a partial clinical hold on trials conducted under the investigational new drug
(IND) application for pacritinib.
Pacritinib is a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The partial clinical hold impacts part of the clinical work currently being conducted under the pacritinib IND and will also affect planned clinical trials.
The FDA said the reasons for the partial clinical hold are excess mortality and other adverse events in pacritinib-treated patients (compared to the control arm) in the PERSIST-1 trial.
The excess mortality was most evident during the non-randomized crossover period following the initial 24 weeks of randomized treatment, during which patients in the control arm could switch to pacritinib treatment.
Under the partial clinical hold, investigators may not enroll new patients or start pacritinib as initial or crossover treatment, and patients not deriving benefit after 30 weeks of pacritinib treatment must stop using pacritinib.
In addition, the FDA has recommended that CTI BioPharma make certain modifications to protocols, provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, and take certain other actions.
CTI BioPharma said it intends to implement the FDA’s recommendations, and all clinical investigators worldwide have been notified of the partial clinical hold.
Just before the FDA notified CTI BioPharma of the partial clinical hold, the company completed enrollment in the phase 3 PERSIST-2 trial.
In PERSIST-2, researchers are comparing the efficacy and safety of pacritinib and best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
Under the partial clinical hold, patients on this trial who are currently receiving pacritinib may continue to do so unless they are not deriving benefit after 30 weeks of pacritinib treatment, and crossover of patients from the control arm to the pacritinib arm will not be allowed.
The US Food and Drug Administration (FDA) has placed a partial clinical hold on trials conducted under the investigational new drug
(IND) application for pacritinib.
Pacritinib is a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The partial clinical hold impacts part of the clinical work currently being conducted under the pacritinib IND and will also affect planned clinical trials.
The FDA said the reasons for the partial clinical hold are excess mortality and other adverse events in pacritinib-treated patients (compared to the control arm) in the PERSIST-1 trial.
The excess mortality was most evident during the non-randomized crossover period following the initial 24 weeks of randomized treatment, during which patients in the control arm could switch to pacritinib treatment.
Under the partial clinical hold, investigators may not enroll new patients or start pacritinib as initial or crossover treatment, and patients not deriving benefit after 30 weeks of pacritinib treatment must stop using pacritinib.
In addition, the FDA has recommended that CTI BioPharma make certain modifications to protocols, provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, and take certain other actions.
CTI BioPharma said it intends to implement the FDA’s recommendations, and all clinical investigators worldwide have been notified of the partial clinical hold.
Just before the FDA notified CTI BioPharma of the partial clinical hold, the company completed enrollment in the phase 3 PERSIST-2 trial.
In PERSIST-2, researchers are comparing the efficacy and safety of pacritinib and best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
Under the partial clinical hold, patients on this trial who are currently receiving pacritinib may continue to do so unless they are not deriving benefit after 30 weeks of pacritinib treatment, and crossover of patients from the control arm to the pacritinib arm will not be allowed.
The US Food and Drug Administration (FDA) has placed a partial clinical hold on trials conducted under the investigational new drug
(IND) application for pacritinib.
Pacritinib is a JAK2/FLT3 inhibitor being developed by CTI BioPharma for the treatment of myelofibrosis (MF).
The partial clinical hold impacts part of the clinical work currently being conducted under the pacritinib IND and will also affect planned clinical trials.
The FDA said the reasons for the partial clinical hold are excess mortality and other adverse events in pacritinib-treated patients (compared to the control arm) in the PERSIST-1 trial.
The excess mortality was most evident during the non-randomized crossover period following the initial 24 weeks of randomized treatment, during which patients in the control arm could switch to pacritinib treatment.
Under the partial clinical hold, investigators may not enroll new patients or start pacritinib as initial or crossover treatment, and patients not deriving benefit after 30 weeks of pacritinib treatment must stop using pacritinib.
In addition, the FDA has recommended that CTI BioPharma make certain modifications to protocols, provide certain notifications, revise relevant statements in the related investigator’s brochure and informed consent documents, and take certain other actions.
CTI BioPharma said it intends to implement the FDA’s recommendations, and all clinical investigators worldwide have been notified of the partial clinical hold.
Just before the FDA notified CTI BioPharma of the partial clinical hold, the company completed enrollment in the phase 3 PERSIST-2 trial.
In PERSIST-2, researchers are comparing the efficacy and safety of pacritinib and best available therapy in patients with thrombocytopenia and primary MF, post-polycythemia vera MF, or post-essential thrombocythemia MF.
Under the partial clinical hold, patients on this trial who are currently receiving pacritinib may continue to do so unless they are not deriving benefit after 30 weeks of pacritinib treatment, and crossover of patients from the control arm to the pacritinib arm will not be allowed.