User login
CASE Bleeding, a large uterus, and no response to hormones
“M.G.,” a 42-year-old nullipara, complains of menstrual periods that last 10 days and occur on a 28-day cycle. She says the bleeding is extremely heavy, with frequent, copious clotting. She routinely avoids planning social activities around the time of her period and occasionally cancels nonessential engagements because of it. Over the past year, this professional woman has missed 6 days of work because of the problem with her menses.
When you ask about her history, she reports that another gynecologist first palpated an enlarged and irregular uterus 5 years earlier, and an ultrasound at that time revealed a multinodular fundus of approximately 12 weeks’ size. Oral contraceptives were prescribed, but the problem returned to pretreatment levels over the next 3 years. Oral medroxyprogesterone acetate was added to the regimen without success. Hysteroscopy and a dilation and curettage revealed no submucous fibroids, but by then the uterus had enlarged to 14 weeks’ size. M.G. was counseled about continued conservative management, uterine artery embolization, endometrial ablation, and vaginal hysterectomy. She now wants to go ahead with total vaginal hysterectomy and ovarian preservation.
Is the vaginal approach feasible?
Vaginal hysterectomy is not only feasible, it is preferred. Although laparoscopic surgeons are fond of using the phrase “minimally invasive surgery” to describe their procedures, when it comes to hysterectomy, only the vaginal route qualifies for this superlative description. And although uterine size does sometimes limit use of the vaginal route, it need do so in only a minority of cases.
This article describes surgical techniques for vaginal removal of the large uterus, using morcellation, coring, cervicectomy, and other strategies.
Is the vaginal approach always best?
Guidelines addressing this question were developed by the Society of Pelvic Reconstructive Surgeons and evaluated by Kovac et al (FIGURE 1).1 These guidelines, widely used around the world, recommend the vaginal approach for the small, mobile uterus in a pelvis that has no substantial, identifiable pathology. The guidelines recommend the abdominal route when an adnexal mass of unknown character is present or malignancy is suspected. They suggest the use of laparoscopy to identify or quantify pathology and to help convert cases from the abdominal route to laparoscopically assisted vaginal hysterectomy.
I view these guidelines as a minimum standard of care. As a surgeon’s confidence and skills increase, wider application of the vaginal route should be possible in progressively challenging cases. In the personal series of expert surgeons, use of the vaginal route often exceeds 90%. In contrast, the overall US average is 25%, including laparoscopically assisted procedures.2,3
The indications for salpingo-oophorectomy remain the same regardless of route. At present, the adnexa are removed in only 10% of vaginal hysterectomies and in 60% of abdominal procedures.2,3 However, successful routine removal of the adnexa through the vagina is well documented in the literature.4
Contraindications. There are few absolute contraindications to vaginal hysterectomy beyond known or suspected malignancy, but some conditions do increase the technical skill required (TABLE). Nor do complications increase, provided the surgeon has the proper skill and instrumentations.
FIGURE 1 How to choose a hysterectomy route
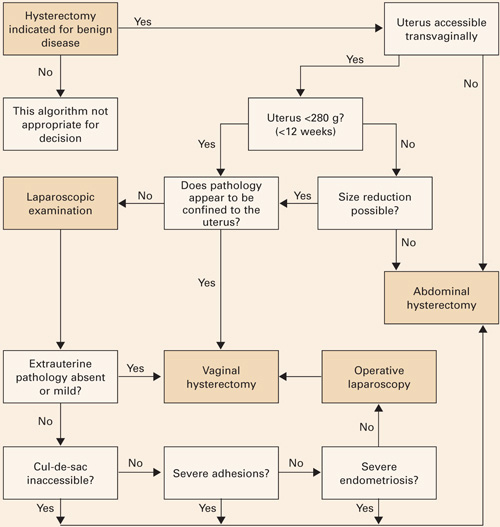
Source: Kovac SR et al1; used by permission of the American Journal of Obstetrics and Gynecology.TABLE
Contraindications to vaginal hysterectomy
| ABSOLUTE |
|
| RELATIVE |
|
Technique
Every procedure involves 3 basic tasks
Before the uterus can be removed vaginally, the surgeon must:
- enter the peritoneal cavity,
- divide the uterosacral, cardinal, and pubourethral ligamentous attachments of the paracolpium, and
- ligate the uterine artery.
Posterior entry is usually easier
Although peritoneal entry may be anterior or posterior, the latter is almost always easier. Apply an Allis clamp to the vaginal epithelium over the posterior cul-de-sac approximately 2 to 4 cm behind the cervix. Apply a small amount of traction to the clamp to create a vertical crease, which denotes the proper location for colpotomy. Palpate the crease manually to ensure no bowel is present. Then make a full-thickness incision with sharp scissors to enter the peritoneal cavity. Incomplete incisions and blunt dissection simply slow the process.
Once the peritoneum is entered, bluntly extend the incision laterally to the uterosacral ligaments, and place a weighted Steiner-Auvard retractor in the incision.
Dissect first, then divide the ligaments
When leiomyomata are present, anatomical distortion tends to be limited to the fundus; cervical anatomy remains relatively unaltered. After completing the circular cervical incision, dissect the vesicocervical and vesicouterine spaces. Some sharp dissection is usually required at the level of the pericervical ring—the supravaginal septum—which consists of dense fibroelastic connective tissue. Place a Heaney or Breisky-Navratil retractor within the anterior incision to obtain full cervical access.
Next, sequentially clamp, divide, and ligate the uterosacral, cardinal, and pubourethral ligaments. Once this task is done, the vascular bundle containing the uterine artery and veins becomes accessible; divide it as well.
If the anterior peritoneum has not been passively entered, it can now be easily incised.
Now that the suspensory apparatus and the major blood supply have been divided, uteroreductive techniques can be employed.
No absolute size limit
There is no objective limit to the size of a uterus that can be safely removed using reductive techniques. Generally, extra skill and experience are needed to remove an organ larger than 12 weeks’ size (approximately 280 g). Numerous reports document the safe removal of enlarged uteri, even those larger than 1,000 g.5-17
Uterine size is reduced in 3 ways: morcellation, coring, and/or cervicectomy.
The best method varies from case to case, depending on the specific uterine anatomy and the surgeon’s skill. Often, more than 1 debulking technique is used in a single case.
Do not begin debulking until peritoneal access is attained, the paracolpium is divided, and the uterine artery is ligated.
Morcellation is well suited to multiple fibroids
First, sharply divide the cervix, cutting vertically in the midline, and extend the incision into the uterine fundus using the endocervical canal and endometrial cavity as visual guides for the incision (FIGURE 2A). As leiomyomata are encountered, grasp each with a Myotome grasper (Marina Medical, Hollywood, Fla) and remove them with Myotomes (Marina Medical). Both the spoon-tipped and chisel-tipped Myotomes have dissecting tips that allow rapid and precise enucleation of tumors. The tip is sharp enough to dissect the capsule of the myomata, but not so sharp that it endangers adjacent structures.
Continue to remove the fibroids as they become accessible. If incisions into the serosa of the uterus are necessary to remove palpable subserosal tumors, make the incisions under direct vision. Access to the serosa usually is greater on the posterior surface of the uterus. With adequate retraction, the anterior surface can also be incised.
If a bulky uterus prevents immediate access to leiomyomata, one strategy is to remove elliptical wedges of myometrium adjacent to the uterine bisecting incision. The Martin myomectomy scissors (Marina Medical) have serrated edges originally designed by orthopedists to cut cartilage, as well as sharp tips that can be inserted into a tumor prior to cutting. They help debulk large myomata (FIGURE 2B) and can be used to quickly remove wedges of myometrium. After sufficient debulking, large myomata can be removed safely (FIGURE 2C).
This morcellation method minimizes the need to use a knife in the “invisible” upper reaches of the fundus. Continuous downward traction on the divided cervix prevents bleeding, and the gradual reduction in size of the debulked fundus allows for sufficient descent of the uterus; it also permits posterior rotation. Ultimately, it becomes possible to clamp the utero-ovarian pedicles and to completely remove the uterus.
In most cases, the uterine serosa can be left intact using morcellation. The size of the uterus that can be removed using this technique is limited only by the experience of the surgeon (FIGURE 3).
FIGURE 2 Expose, debulk, and remove the dominant myoma
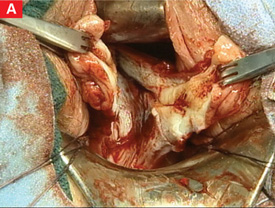
Incise the cervix along the midline to gain access to the fundus and expose the dominant myoma.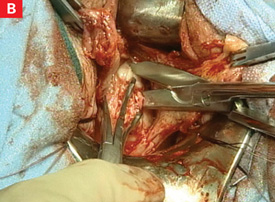
Insert the sharp tip of the scissors into the myoma prior to cutting.
When the myoma has been sufficiently debulked, remove it through the vagina.
FIGURE 3 Massive uteri can be removed vaginally

This uterus and multiple myomata were removed from a single patient using the vaginal route.
Use coring for moderately enlarged uteri
This is a useful technique when the uterus contains multiple small leiomyomata, a single dominant tumor, or cicatrized adenomyosis. Begin by making a circular incision into the fundus of the uterus just above the isthmus. The incision should be parallel to the central axis of the endometrial cavity.18
Apply firm downward traction on the cervix to allow the portion of the uterus central to the incision to evert. Continue to incise the uterus in a circular pattern to allow more of the bulk of the fundus to descend.
This technique converts the globular, anatomically distorted fundus into a cylinder. Be sure to make the encircling incision under direct vision to reduce the risk of injuring adjacent structures.
In most cases, coring has the advantage of leaving the endometrial cavity and serosa intact. With practice, this technique can quickly and reliably reduce a large uterus to a manageable size.
In some cases, you may have to remove the cervix before debulking
If the cervix is particularly bulky or prevents access to the fundus, perform cervicectomy prior to debulking. This type of debulking is not highly technical, and it may make the remainder of the procedure easier to accomplish. As debulking proceeds, use the endocervical canal or endometrial cavity for orientation.
When complete removal is impossible
Occasionally, it is not possible to complete vaginal removal of the large uterus. While this scenario is not ideal, no evidence exists that conversion to the abdominal or laparoscopic route endangers the patient, especially if the decision is made in a timely and judicious manner. Perform cervicectomy before converting to the abdominal or laparoscopic route. The cervical cuff may also be closed prior to conversion.
Be sure to weigh the specimen
Inform the pathologist of the reason for the morcellated specimen so that an accurate total weight can be determined. This is important because CPT codes for uteri larger than 250 g carry more relative value units than the codes for smaller uteri, based on the extra time in the OR as well as the greater technical skill required.
CASE 610-g uterus safely removed
M.G. undergoes vaginal hysterectomy with uteroreductive morcellation. Estimated blood loss is 200 cc.
The morning after her surgery, M.G. voids after removal of the urinary catheter, and is able to tolerate a regular diet. She walks without difficulty and is discharged home. Seven days after her surgery, she returns to work. Her job allows her the freedom to define her own responsibilities, and she has no manual duties.
The pathology report reveals that her uterus weighed 610 g, with multiple leiomyomata. The largest myoma was 8.0×5.5×4.0 cm. No other abnormalities were present.
One year later, M.G. reports a substantially improved lifestyle and expresses satisfaction with her decision to undergo vaginal hysterectomy.
1. Kovac SR, Barhan S, Lister M, Tucker L, Bishop M, Das A. Guidelines for the selection of the route of hysterectomy: application in a resident clinic population. Am J Obstet Gynecol. 2002;187:1521-1527.
2. Kovac SR. Guidelines to determine the route of hysterectomy. Obstet Gynecol. 1995;85:18-23.
3. Kovac SR. Clinical opinion: guidelines for hysterectomy. Am J Obstet Gynecol. 2004;191:635-640.
4. Sheth S, Malpani A. Routine prophylactic oophorectomy at the time of vaginal hysterectomy in postmenopausal women. Arch Gynecol Obstet. 1992;251:87-91.
5. El-Lamie IK. Vaginal hysterectomy for uteri weighing 250 grams or more. J Pelvic Surg. 2001;7:140-146.
6. Grody MH. Vaginal hysterectomy: the large uterus. J Gynecol Surg. 1989;5:301-312.
7. Grody MH. Vaginal hysterectomy: the enlarged uterus. Operative Tech Gynecol Surg. 1999;4:53-61.
8. Grody MH, Pruzbylko K, Pagano AM. A practical method for removal of the huge benign fibromyomatous uterus through the vaginal route. J Pelvic Surg. 2000;6:39-44.
9. Kammerer-Doak D, Mao J. Vaginal hysterectomy with and without morcellation: the University of New Mexico’s experience. Obstet Gynecol. 1996;88:560-563.
10. Larson SL. Uterine morcellation-review of 443 cases. Obstet Gynecol. 1999;4:61S.-
11. Lash AF. A method for reducing the size of the uterus in vaginal hysterectomy. Am J Obstet Gynecol. 1941;42:452-459.
12. Lash AF. Technique for removal of abnormally large uteri without entering cavities. Clin Obstet Gynecol. 1961;4:210-216.
13. Magos A, Bournas N, Sinha R, et al. Vaginal hysterectomy for the large uterus. Br J Obstet Gynecol. 1996;103:246-251.
14. Moen MD, Webb MJ, Wilson TO. Vaginal hysterectomy in patients with benign uterine enlargement. J Pelvic Surg. 1995;4:197-203.
15. Peham H, Amreich I, Ferguson L. Operative Gynecology. Philadelphia: JB Lippincott; 1934.
16. Pelosi MA, II, Pelosi MA, III. Should uterine size alone require laparoscopic assistance? Vaginal hysterectomy for a 2,003-g uterus. J Lapendo Adv Surg Tech. 1998;8:99-103.
17. Pratt JH, Gunnlaugsson GH. Vaginal hysterectomy by morcellation. Mayo Clin Proc. 1970;45:374-387.
18. Kovac SR. Intramyometrial coring as an adjunct to vaginal hysterectomy. Obstet Gynecol. 1986;67:131-134.
Dr. Zimmerman reports that he is a consultant and instrument designer for Marina Medical, Inc.
CASE Bleeding, a large uterus, and no response to hormones
“M.G.,” a 42-year-old nullipara, complains of menstrual periods that last 10 days and occur on a 28-day cycle. She says the bleeding is extremely heavy, with frequent, copious clotting. She routinely avoids planning social activities around the time of her period and occasionally cancels nonessential engagements because of it. Over the past year, this professional woman has missed 6 days of work because of the problem with her menses.
When you ask about her history, she reports that another gynecologist first palpated an enlarged and irregular uterus 5 years earlier, and an ultrasound at that time revealed a multinodular fundus of approximately 12 weeks’ size. Oral contraceptives were prescribed, but the problem returned to pretreatment levels over the next 3 years. Oral medroxyprogesterone acetate was added to the regimen without success. Hysteroscopy and a dilation and curettage revealed no submucous fibroids, but by then the uterus had enlarged to 14 weeks’ size. M.G. was counseled about continued conservative management, uterine artery embolization, endometrial ablation, and vaginal hysterectomy. She now wants to go ahead with total vaginal hysterectomy and ovarian preservation.
Is the vaginal approach feasible?
Vaginal hysterectomy is not only feasible, it is preferred. Although laparoscopic surgeons are fond of using the phrase “minimally invasive surgery” to describe their procedures, when it comes to hysterectomy, only the vaginal route qualifies for this superlative description. And although uterine size does sometimes limit use of the vaginal route, it need do so in only a minority of cases.
This article describes surgical techniques for vaginal removal of the large uterus, using morcellation, coring, cervicectomy, and other strategies.
Is the vaginal approach always best?
Guidelines addressing this question were developed by the Society of Pelvic Reconstructive Surgeons and evaluated by Kovac et al (FIGURE 1).1 These guidelines, widely used around the world, recommend the vaginal approach for the small, mobile uterus in a pelvis that has no substantial, identifiable pathology. The guidelines recommend the abdominal route when an adnexal mass of unknown character is present or malignancy is suspected. They suggest the use of laparoscopy to identify or quantify pathology and to help convert cases from the abdominal route to laparoscopically assisted vaginal hysterectomy.
I view these guidelines as a minimum standard of care. As a surgeon’s confidence and skills increase, wider application of the vaginal route should be possible in progressively challenging cases. In the personal series of expert surgeons, use of the vaginal route often exceeds 90%. In contrast, the overall US average is 25%, including laparoscopically assisted procedures.2,3
The indications for salpingo-oophorectomy remain the same regardless of route. At present, the adnexa are removed in only 10% of vaginal hysterectomies and in 60% of abdominal procedures.2,3 However, successful routine removal of the adnexa through the vagina is well documented in the literature.4
Contraindications. There are few absolute contraindications to vaginal hysterectomy beyond known or suspected malignancy, but some conditions do increase the technical skill required (TABLE). Nor do complications increase, provided the surgeon has the proper skill and instrumentations.
FIGURE 1 How to choose a hysterectomy route
Source: Kovac SR et al1; used by permission of the American Journal of Obstetrics and Gynecology.TABLE
Contraindications to vaginal hysterectomy
| ABSOLUTE |
|
| RELATIVE |
|
Technique
Every procedure involves 3 basic tasks
Before the uterus can be removed vaginally, the surgeon must:
- enter the peritoneal cavity,
- divide the uterosacral, cardinal, and pubourethral ligamentous attachments of the paracolpium, and
- ligate the uterine artery.
Posterior entry is usually easier
Although peritoneal entry may be anterior or posterior, the latter is almost always easier. Apply an Allis clamp to the vaginal epithelium over the posterior cul-de-sac approximately 2 to 4 cm behind the cervix. Apply a small amount of traction to the clamp to create a vertical crease, which denotes the proper location for colpotomy. Palpate the crease manually to ensure no bowel is present. Then make a full-thickness incision with sharp scissors to enter the peritoneal cavity. Incomplete incisions and blunt dissection simply slow the process.
Once the peritoneum is entered, bluntly extend the incision laterally to the uterosacral ligaments, and place a weighted Steiner-Auvard retractor in the incision.
Dissect first, then divide the ligaments
When leiomyomata are present, anatomical distortion tends to be limited to the fundus; cervical anatomy remains relatively unaltered. After completing the circular cervical incision, dissect the vesicocervical and vesicouterine spaces. Some sharp dissection is usually required at the level of the pericervical ring—the supravaginal septum—which consists of dense fibroelastic connective tissue. Place a Heaney or Breisky-Navratil retractor within the anterior incision to obtain full cervical access.
Next, sequentially clamp, divide, and ligate the uterosacral, cardinal, and pubourethral ligaments. Once this task is done, the vascular bundle containing the uterine artery and veins becomes accessible; divide it as well.
If the anterior peritoneum has not been passively entered, it can now be easily incised.
Now that the suspensory apparatus and the major blood supply have been divided, uteroreductive techniques can be employed.
No absolute size limit
There is no objective limit to the size of a uterus that can be safely removed using reductive techniques. Generally, extra skill and experience are needed to remove an organ larger than 12 weeks’ size (approximately 280 g). Numerous reports document the safe removal of enlarged uteri, even those larger than 1,000 g.5-17
Uterine size is reduced in 3 ways: morcellation, coring, and/or cervicectomy.
The best method varies from case to case, depending on the specific uterine anatomy and the surgeon’s skill. Often, more than 1 debulking technique is used in a single case.
Do not begin debulking until peritoneal access is attained, the paracolpium is divided, and the uterine artery is ligated.
Morcellation is well suited to multiple fibroids
First, sharply divide the cervix, cutting vertically in the midline, and extend the incision into the uterine fundus using the endocervical canal and endometrial cavity as visual guides for the incision (FIGURE 2A). As leiomyomata are encountered, grasp each with a Myotome grasper (Marina Medical, Hollywood, Fla) and remove them with Myotomes (Marina Medical). Both the spoon-tipped and chisel-tipped Myotomes have dissecting tips that allow rapid and precise enucleation of tumors. The tip is sharp enough to dissect the capsule of the myomata, but not so sharp that it endangers adjacent structures.
Continue to remove the fibroids as they become accessible. If incisions into the serosa of the uterus are necessary to remove palpable subserosal tumors, make the incisions under direct vision. Access to the serosa usually is greater on the posterior surface of the uterus. With adequate retraction, the anterior surface can also be incised.
If a bulky uterus prevents immediate access to leiomyomata, one strategy is to remove elliptical wedges of myometrium adjacent to the uterine bisecting incision. The Martin myomectomy scissors (Marina Medical) have serrated edges originally designed by orthopedists to cut cartilage, as well as sharp tips that can be inserted into a tumor prior to cutting. They help debulk large myomata (FIGURE 2B) and can be used to quickly remove wedges of myometrium. After sufficient debulking, large myomata can be removed safely (FIGURE 2C).
This morcellation method minimizes the need to use a knife in the “invisible” upper reaches of the fundus. Continuous downward traction on the divided cervix prevents bleeding, and the gradual reduction in size of the debulked fundus allows for sufficient descent of the uterus; it also permits posterior rotation. Ultimately, it becomes possible to clamp the utero-ovarian pedicles and to completely remove the uterus.
In most cases, the uterine serosa can be left intact using morcellation. The size of the uterus that can be removed using this technique is limited only by the experience of the surgeon (FIGURE 3).
FIGURE 2 Expose, debulk, and remove the dominant myoma
Incise the cervix along the midline to gain access to the fundus and expose the dominant myoma.
Insert the sharp tip of the scissors into the myoma prior to cutting.
When the myoma has been sufficiently debulked, remove it through the vagina.
FIGURE 3 Massive uteri can be removed vaginally
This uterus and multiple myomata were removed from a single patient using the vaginal route.
Use coring for moderately enlarged uteri
This is a useful technique when the uterus contains multiple small leiomyomata, a single dominant tumor, or cicatrized adenomyosis. Begin by making a circular incision into the fundus of the uterus just above the isthmus. The incision should be parallel to the central axis of the endometrial cavity.18
Apply firm downward traction on the cervix to allow the portion of the uterus central to the incision to evert. Continue to incise the uterus in a circular pattern to allow more of the bulk of the fundus to descend.
This technique converts the globular, anatomically distorted fundus into a cylinder. Be sure to make the encircling incision under direct vision to reduce the risk of injuring adjacent structures.
In most cases, coring has the advantage of leaving the endometrial cavity and serosa intact. With practice, this technique can quickly and reliably reduce a large uterus to a manageable size.
In some cases, you may have to remove the cervix before debulking
If the cervix is particularly bulky or prevents access to the fundus, perform cervicectomy prior to debulking. This type of debulking is not highly technical, and it may make the remainder of the procedure easier to accomplish. As debulking proceeds, use the endocervical canal or endometrial cavity for orientation.
When complete removal is impossible
Occasionally, it is not possible to complete vaginal removal of the large uterus. While this scenario is not ideal, no evidence exists that conversion to the abdominal or laparoscopic route endangers the patient, especially if the decision is made in a timely and judicious manner. Perform cervicectomy before converting to the abdominal or laparoscopic route. The cervical cuff may also be closed prior to conversion.
Be sure to weigh the specimen
Inform the pathologist of the reason for the morcellated specimen so that an accurate total weight can be determined. This is important because CPT codes for uteri larger than 250 g carry more relative value units than the codes for smaller uteri, based on the extra time in the OR as well as the greater technical skill required.
CASE 610-g uterus safely removed
M.G. undergoes vaginal hysterectomy with uteroreductive morcellation. Estimated blood loss is 200 cc.
The morning after her surgery, M.G. voids after removal of the urinary catheter, and is able to tolerate a regular diet. She walks without difficulty and is discharged home. Seven days after her surgery, she returns to work. Her job allows her the freedom to define her own responsibilities, and she has no manual duties.
The pathology report reveals that her uterus weighed 610 g, with multiple leiomyomata. The largest myoma was 8.0×5.5×4.0 cm. No other abnormalities were present.
One year later, M.G. reports a substantially improved lifestyle and expresses satisfaction with her decision to undergo vaginal hysterectomy.
CASE Bleeding, a large uterus, and no response to hormones
“M.G.,” a 42-year-old nullipara, complains of menstrual periods that last 10 days and occur on a 28-day cycle. She says the bleeding is extremely heavy, with frequent, copious clotting. She routinely avoids planning social activities around the time of her period and occasionally cancels nonessential engagements because of it. Over the past year, this professional woman has missed 6 days of work because of the problem with her menses.
When you ask about her history, she reports that another gynecologist first palpated an enlarged and irregular uterus 5 years earlier, and an ultrasound at that time revealed a multinodular fundus of approximately 12 weeks’ size. Oral contraceptives were prescribed, but the problem returned to pretreatment levels over the next 3 years. Oral medroxyprogesterone acetate was added to the regimen without success. Hysteroscopy and a dilation and curettage revealed no submucous fibroids, but by then the uterus had enlarged to 14 weeks’ size. M.G. was counseled about continued conservative management, uterine artery embolization, endometrial ablation, and vaginal hysterectomy. She now wants to go ahead with total vaginal hysterectomy and ovarian preservation.
Is the vaginal approach feasible?
Vaginal hysterectomy is not only feasible, it is preferred. Although laparoscopic surgeons are fond of using the phrase “minimally invasive surgery” to describe their procedures, when it comes to hysterectomy, only the vaginal route qualifies for this superlative description. And although uterine size does sometimes limit use of the vaginal route, it need do so in only a minority of cases.
This article describes surgical techniques for vaginal removal of the large uterus, using morcellation, coring, cervicectomy, and other strategies.
Is the vaginal approach always best?
Guidelines addressing this question were developed by the Society of Pelvic Reconstructive Surgeons and evaluated by Kovac et al (FIGURE 1).1 These guidelines, widely used around the world, recommend the vaginal approach for the small, mobile uterus in a pelvis that has no substantial, identifiable pathology. The guidelines recommend the abdominal route when an adnexal mass of unknown character is present or malignancy is suspected. They suggest the use of laparoscopy to identify or quantify pathology and to help convert cases from the abdominal route to laparoscopically assisted vaginal hysterectomy.
I view these guidelines as a minimum standard of care. As a surgeon’s confidence and skills increase, wider application of the vaginal route should be possible in progressively challenging cases. In the personal series of expert surgeons, use of the vaginal route often exceeds 90%. In contrast, the overall US average is 25%, including laparoscopically assisted procedures.2,3
The indications for salpingo-oophorectomy remain the same regardless of route. At present, the adnexa are removed in only 10% of vaginal hysterectomies and in 60% of abdominal procedures.2,3 However, successful routine removal of the adnexa through the vagina is well documented in the literature.4
Contraindications. There are few absolute contraindications to vaginal hysterectomy beyond known or suspected malignancy, but some conditions do increase the technical skill required (TABLE). Nor do complications increase, provided the surgeon has the proper skill and instrumentations.
FIGURE 1 How to choose a hysterectomy route
Source: Kovac SR et al1; used by permission of the American Journal of Obstetrics and Gynecology.TABLE
Contraindications to vaginal hysterectomy
| ABSOLUTE |
|
| RELATIVE |
|
Technique
Every procedure involves 3 basic tasks
Before the uterus can be removed vaginally, the surgeon must:
- enter the peritoneal cavity,
- divide the uterosacral, cardinal, and pubourethral ligamentous attachments of the paracolpium, and
- ligate the uterine artery.
Posterior entry is usually easier
Although peritoneal entry may be anterior or posterior, the latter is almost always easier. Apply an Allis clamp to the vaginal epithelium over the posterior cul-de-sac approximately 2 to 4 cm behind the cervix. Apply a small amount of traction to the clamp to create a vertical crease, which denotes the proper location for colpotomy. Palpate the crease manually to ensure no bowel is present. Then make a full-thickness incision with sharp scissors to enter the peritoneal cavity. Incomplete incisions and blunt dissection simply slow the process.
Once the peritoneum is entered, bluntly extend the incision laterally to the uterosacral ligaments, and place a weighted Steiner-Auvard retractor in the incision.
Dissect first, then divide the ligaments
When leiomyomata are present, anatomical distortion tends to be limited to the fundus; cervical anatomy remains relatively unaltered. After completing the circular cervical incision, dissect the vesicocervical and vesicouterine spaces. Some sharp dissection is usually required at the level of the pericervical ring—the supravaginal septum—which consists of dense fibroelastic connective tissue. Place a Heaney or Breisky-Navratil retractor within the anterior incision to obtain full cervical access.
Next, sequentially clamp, divide, and ligate the uterosacral, cardinal, and pubourethral ligaments. Once this task is done, the vascular bundle containing the uterine artery and veins becomes accessible; divide it as well.
If the anterior peritoneum has not been passively entered, it can now be easily incised.
Now that the suspensory apparatus and the major blood supply have been divided, uteroreductive techniques can be employed.
No absolute size limit
There is no objective limit to the size of a uterus that can be safely removed using reductive techniques. Generally, extra skill and experience are needed to remove an organ larger than 12 weeks’ size (approximately 280 g). Numerous reports document the safe removal of enlarged uteri, even those larger than 1,000 g.5-17
Uterine size is reduced in 3 ways: morcellation, coring, and/or cervicectomy.
The best method varies from case to case, depending on the specific uterine anatomy and the surgeon’s skill. Often, more than 1 debulking technique is used in a single case.
Do not begin debulking until peritoneal access is attained, the paracolpium is divided, and the uterine artery is ligated.
Morcellation is well suited to multiple fibroids
First, sharply divide the cervix, cutting vertically in the midline, and extend the incision into the uterine fundus using the endocervical canal and endometrial cavity as visual guides for the incision (FIGURE 2A). As leiomyomata are encountered, grasp each with a Myotome grasper (Marina Medical, Hollywood, Fla) and remove them with Myotomes (Marina Medical). Both the spoon-tipped and chisel-tipped Myotomes have dissecting tips that allow rapid and precise enucleation of tumors. The tip is sharp enough to dissect the capsule of the myomata, but not so sharp that it endangers adjacent structures.
Continue to remove the fibroids as they become accessible. If incisions into the serosa of the uterus are necessary to remove palpable subserosal tumors, make the incisions under direct vision. Access to the serosa usually is greater on the posterior surface of the uterus. With adequate retraction, the anterior surface can also be incised.
If a bulky uterus prevents immediate access to leiomyomata, one strategy is to remove elliptical wedges of myometrium adjacent to the uterine bisecting incision. The Martin myomectomy scissors (Marina Medical) have serrated edges originally designed by orthopedists to cut cartilage, as well as sharp tips that can be inserted into a tumor prior to cutting. They help debulk large myomata (FIGURE 2B) and can be used to quickly remove wedges of myometrium. After sufficient debulking, large myomata can be removed safely (FIGURE 2C).
This morcellation method minimizes the need to use a knife in the “invisible” upper reaches of the fundus. Continuous downward traction on the divided cervix prevents bleeding, and the gradual reduction in size of the debulked fundus allows for sufficient descent of the uterus; it also permits posterior rotation. Ultimately, it becomes possible to clamp the utero-ovarian pedicles and to completely remove the uterus.
In most cases, the uterine serosa can be left intact using morcellation. The size of the uterus that can be removed using this technique is limited only by the experience of the surgeon (FIGURE 3).
FIGURE 2 Expose, debulk, and remove the dominant myoma
Incise the cervix along the midline to gain access to the fundus and expose the dominant myoma.
Insert the sharp tip of the scissors into the myoma prior to cutting.
When the myoma has been sufficiently debulked, remove it through the vagina.
FIGURE 3 Massive uteri can be removed vaginally
This uterus and multiple myomata were removed from a single patient using the vaginal route.
Use coring for moderately enlarged uteri
This is a useful technique when the uterus contains multiple small leiomyomata, a single dominant tumor, or cicatrized adenomyosis. Begin by making a circular incision into the fundus of the uterus just above the isthmus. The incision should be parallel to the central axis of the endometrial cavity.18
Apply firm downward traction on the cervix to allow the portion of the uterus central to the incision to evert. Continue to incise the uterus in a circular pattern to allow more of the bulk of the fundus to descend.
This technique converts the globular, anatomically distorted fundus into a cylinder. Be sure to make the encircling incision under direct vision to reduce the risk of injuring adjacent structures.
In most cases, coring has the advantage of leaving the endometrial cavity and serosa intact. With practice, this technique can quickly and reliably reduce a large uterus to a manageable size.
In some cases, you may have to remove the cervix before debulking
If the cervix is particularly bulky or prevents access to the fundus, perform cervicectomy prior to debulking. This type of debulking is not highly technical, and it may make the remainder of the procedure easier to accomplish. As debulking proceeds, use the endocervical canal or endometrial cavity for orientation.
When complete removal is impossible
Occasionally, it is not possible to complete vaginal removal of the large uterus. While this scenario is not ideal, no evidence exists that conversion to the abdominal or laparoscopic route endangers the patient, especially if the decision is made in a timely and judicious manner. Perform cervicectomy before converting to the abdominal or laparoscopic route. The cervical cuff may also be closed prior to conversion.
Be sure to weigh the specimen
Inform the pathologist of the reason for the morcellated specimen so that an accurate total weight can be determined. This is important because CPT codes for uteri larger than 250 g carry more relative value units than the codes for smaller uteri, based on the extra time in the OR as well as the greater technical skill required.
CASE 610-g uterus safely removed
M.G. undergoes vaginal hysterectomy with uteroreductive morcellation. Estimated blood loss is 200 cc.
The morning after her surgery, M.G. voids after removal of the urinary catheter, and is able to tolerate a regular diet. She walks without difficulty and is discharged home. Seven days after her surgery, she returns to work. Her job allows her the freedom to define her own responsibilities, and she has no manual duties.
The pathology report reveals that her uterus weighed 610 g, with multiple leiomyomata. The largest myoma was 8.0×5.5×4.0 cm. No other abnormalities were present.
One year later, M.G. reports a substantially improved lifestyle and expresses satisfaction with her decision to undergo vaginal hysterectomy.
1. Kovac SR, Barhan S, Lister M, Tucker L, Bishop M, Das A. Guidelines for the selection of the route of hysterectomy: application in a resident clinic population. Am J Obstet Gynecol. 2002;187:1521-1527.
2. Kovac SR. Guidelines to determine the route of hysterectomy. Obstet Gynecol. 1995;85:18-23.
3. Kovac SR. Clinical opinion: guidelines for hysterectomy. Am J Obstet Gynecol. 2004;191:635-640.
4. Sheth S, Malpani A. Routine prophylactic oophorectomy at the time of vaginal hysterectomy in postmenopausal women. Arch Gynecol Obstet. 1992;251:87-91.
5. El-Lamie IK. Vaginal hysterectomy for uteri weighing 250 grams or more. J Pelvic Surg. 2001;7:140-146.
6. Grody MH. Vaginal hysterectomy: the large uterus. J Gynecol Surg. 1989;5:301-312.
7. Grody MH. Vaginal hysterectomy: the enlarged uterus. Operative Tech Gynecol Surg. 1999;4:53-61.
8. Grody MH, Pruzbylko K, Pagano AM. A practical method for removal of the huge benign fibromyomatous uterus through the vaginal route. J Pelvic Surg. 2000;6:39-44.
9. Kammerer-Doak D, Mao J. Vaginal hysterectomy with and without morcellation: the University of New Mexico’s experience. Obstet Gynecol. 1996;88:560-563.
10. Larson SL. Uterine morcellation-review of 443 cases. Obstet Gynecol. 1999;4:61S.-
11. Lash AF. A method for reducing the size of the uterus in vaginal hysterectomy. Am J Obstet Gynecol. 1941;42:452-459.
12. Lash AF. Technique for removal of abnormally large uteri without entering cavities. Clin Obstet Gynecol. 1961;4:210-216.
13. Magos A, Bournas N, Sinha R, et al. Vaginal hysterectomy for the large uterus. Br J Obstet Gynecol. 1996;103:246-251.
14. Moen MD, Webb MJ, Wilson TO. Vaginal hysterectomy in patients with benign uterine enlargement. J Pelvic Surg. 1995;4:197-203.
15. Peham H, Amreich I, Ferguson L. Operative Gynecology. Philadelphia: JB Lippincott; 1934.
16. Pelosi MA, II, Pelosi MA, III. Should uterine size alone require laparoscopic assistance? Vaginal hysterectomy for a 2,003-g uterus. J Lapendo Adv Surg Tech. 1998;8:99-103.
17. Pratt JH, Gunnlaugsson GH. Vaginal hysterectomy by morcellation. Mayo Clin Proc. 1970;45:374-387.
18. Kovac SR. Intramyometrial coring as an adjunct to vaginal hysterectomy. Obstet Gynecol. 1986;67:131-134.
Dr. Zimmerman reports that he is a consultant and instrument designer for Marina Medical, Inc.
1. Kovac SR, Barhan S, Lister M, Tucker L, Bishop M, Das A. Guidelines for the selection of the route of hysterectomy: application in a resident clinic population. Am J Obstet Gynecol. 2002;187:1521-1527.
2. Kovac SR. Guidelines to determine the route of hysterectomy. Obstet Gynecol. 1995;85:18-23.
3. Kovac SR. Clinical opinion: guidelines for hysterectomy. Am J Obstet Gynecol. 2004;191:635-640.
4. Sheth S, Malpani A. Routine prophylactic oophorectomy at the time of vaginal hysterectomy in postmenopausal women. Arch Gynecol Obstet. 1992;251:87-91.
5. El-Lamie IK. Vaginal hysterectomy for uteri weighing 250 grams or more. J Pelvic Surg. 2001;7:140-146.
6. Grody MH. Vaginal hysterectomy: the large uterus. J Gynecol Surg. 1989;5:301-312.
7. Grody MH. Vaginal hysterectomy: the enlarged uterus. Operative Tech Gynecol Surg. 1999;4:53-61.
8. Grody MH, Pruzbylko K, Pagano AM. A practical method for removal of the huge benign fibromyomatous uterus through the vaginal route. J Pelvic Surg. 2000;6:39-44.
9. Kammerer-Doak D, Mao J. Vaginal hysterectomy with and without morcellation: the University of New Mexico’s experience. Obstet Gynecol. 1996;88:560-563.
10. Larson SL. Uterine morcellation-review of 443 cases. Obstet Gynecol. 1999;4:61S.-
11. Lash AF. A method for reducing the size of the uterus in vaginal hysterectomy. Am J Obstet Gynecol. 1941;42:452-459.
12. Lash AF. Technique for removal of abnormally large uteri without entering cavities. Clin Obstet Gynecol. 1961;4:210-216.
13. Magos A, Bournas N, Sinha R, et al. Vaginal hysterectomy for the large uterus. Br J Obstet Gynecol. 1996;103:246-251.
14. Moen MD, Webb MJ, Wilson TO. Vaginal hysterectomy in patients with benign uterine enlargement. J Pelvic Surg. 1995;4:197-203.
15. Peham H, Amreich I, Ferguson L. Operative Gynecology. Philadelphia: JB Lippincott; 1934.
16. Pelosi MA, II, Pelosi MA, III. Should uterine size alone require laparoscopic assistance? Vaginal hysterectomy for a 2,003-g uterus. J Lapendo Adv Surg Tech. 1998;8:99-103.
17. Pratt JH, Gunnlaugsson GH. Vaginal hysterectomy by morcellation. Mayo Clin Proc. 1970;45:374-387.
18. Kovac SR. Intramyometrial coring as an adjunct to vaginal hysterectomy. Obstet Gynecol. 1986;67:131-134.
Dr. Zimmerman reports that he is a consultant and instrument designer for Marina Medical, Inc.