User login
Traditional or centralized models of diabetes care: The multidisciplinary diabetes team approach
Nontraditional or noncentralized models of diabetes care: Medication therapy management services
Nontraditional or noncentralized models of diabetes care: Boutique medicine
- Medication therapy management (MTM) services were introduced in the mid-2000s as part of Medicare Part D—the prescription drug benefit
- Key goals of MTM services are to:
- – Counsel patients to improve understanding of their medications
- – Improve medication adherence
- – Detect adverse drug reactions and patterns of improper drug use
- MTM services are becoming well established in pharmacy practice
- Pharmacists can help improve outcomes by:
- – Following patient progress between physician visits
- – Utilizing their clinical expertise to monitor and manage diabetes medication plans
- – Educating patients on disease, lifestyle, and adherence issues
- Although referral by a physician/health care professional (HCP) is not required for MTM provided by a pharmacist, the physician/ HCP needs to be contacted for anything that requires a change in management
Introduction
Patients with type 2 diabetes mellitus (T2DM) have a large unmet medical need for appropriate treatment and continuity of care. Treatment of T2DM requires a complex, stepped approach combining behavioral modifications and multiple medications, as well as close monitoring of the effects of these interventions. In addition, these patients often require treatment for diabetes-related complications and comorbid medical conditions. Problems may arise from the complex medication regimens that T2DM patients often require. The primary care physician (PCP) has been the traditional provider or coordinator of care for T2DM. However, recent trends have imposed limits on access to the full scope of primary care needed by the growing number of patients affected by this and other chronic illnesses. The pool of PCPs is shrinking, physicians lack the time needed for complex patient interactions, and planners are discussing the shifting of primary care responsibilities to other types of health care professionals (HCPs), such as nurse practitioners, physician assistants, and pharmacists.1-4
The pharmacist’s role in managing chronic diseases
Pharmacists are a professional group with sufficient education and skills to take a leading role in the primary care of patients with T2DM and other patients with complex needs. Pharmacists are the third-largest group of health professionals in the United States (US).2 The emphasis of professional pharmacy practice has been shifting from a product-oriented, medication-dispensing role, to a patient-centered role, in which the pharmacist provides cognitive services and patient management. Provision of time-consuming primary care for T2DM is made more feasible not only by this growing supply of practicing pharmacists—expected to reach 300,000 by 2020—but also by 2 trends that should increase the availability of their time: the automation of pharmacy practice and the growth of certified pharmacy technicians to a number about equal to that of pharmacists.4
The “pharmaceutical care” philosophy was first articulated 2 decades ago as a call for pharmacists to assume a wider scope of professional responsibility in improving the outcomes of drug therapy, preventing medication-related morbidity and mortality, and improving patients’ quality of life.5 Falling within this paradigm are diabetes self-management education or training (DSME/DSMT), disease management, and collaborative drug therapy management (CDTM), all of which are models that have been applied to pharmacy care in recent decades.6,7 DSME/DSMT programs aim to educate patients on all aspects of diabetes control, including nutrition and exercise, blood glucose control, medication management, and prevention of complications. DSME is taught in an individual or classroom format by certified diabetes educator (CDE) nurses, dietitians, pharmacists, or other professionals. The CDE credential, administered by the National Certification Board of Diabetes Educators, is the national credential for health professionals who provide diabetes patient education and counseling.8
Disease management programs, widely adopted in the 1990s, may be delivered by physicians, pharmacists, or other HCPs or teams. These programs are disease-specific and focus on conditions that require a considerable degree of patient self-management. They provide a wider range of services than just patient education, and may include drug and nondrug therapy. However, they do not usually encompass the needs of patients with multiple chronic illnesses. Some pharmacists are now specializing in management of specific diseases, such as diabetes, and the Board Certified-Advanced Diabetes Management (BC-ADM) credential has been introduced for pharmacists, nurses, and dietitians.9 This credential was originally introduced in 2000, but is currently being reviewed by the American Association of Diabetes Educators. The BC-ADM certifies expertise in patient evaluation and clinical management, as well as patient education. However, because the responsibilities for disease management are often shared among members of a team, pharmacists who provide disease management services may have difficulty obtaining compensation for their contribution.7
CDTM programs consist of partnerships between physicians and pharmacists in which the pharmacist can start, modify, or continue drug therapy for a specific patient according to a written protocol. Protocols may be specific to a single patient or may cover all patients treated by a physician for a specified condition. For example, in a low-risk patient with T2DM, a protocol might specify that the pharmacist can adjust a patient’s insulin dose as long as the glycated hemoglobin (A1C) or blood glucose remains below a certain threshold, but the physician should be contacted if a threshold is exceeded. CDTM programs also may allow pharmacists to take responsibility for ordering tests and providing patient education. Individual state laws have established CDTM legislation, and the activity of pharmacists within CDTM programs is regulated at the state level. The programs are currently available in all but 3 states: Alabama, Oklahoma, and Maine. In most jurisdictions, CTDM agreements are easily established between physicians and regular retail pharmacists, or pharmacists working in a clinic setting.6,10,11 In New York, CDTM was recently assessed for pharmacists practicing in teaching hospitals only.
Medication therapy management (MTM) programs are a further evolution in pharmaceutical patient care. MTM was introduced as part of Medicare legislation in the mid-2000s as a means for pharmacists and other qualified HCPs to improve the care of selected Medicare beneficiaries with multiple chronic illnesses who require multiple medications. MTM services may help address the need to prevent medication-related morbidity and mortality in patients with T2DM and comorbid conditions. Pharmacists can provide continuity of care by following patient progress between physician visits; by utilizing their clinical expertise to monitor and manage diabetes medication plans; and by educating patients on disease, lifestyle, and adherence issues. This level of service can be provided adequately by pharmacists, pharmacist CDEs, and pharmacists with the BC-ADM credential. In addition, many local, state, and national pharmacy organizations and pharmacy schools are providing targeted training for pharmacists wishing to deliver MTM services.12-14
Overview of MTM services
The US Medicare Modernization Act of 2003 established MTM services as part of Medicare Part D—the prescription drug benefit. The Act requires Medicare insurers to provide MTM services to a defined group of beneficiaries expected to benefit from enhanced medication management. Key goals of MTM services are to counsel patients to improve understanding of their medications, to improve medication adherence, and to detect adverse drug reactions and patterns of improper drug use.15 For the first time, the Act created a mechanism for insurers to compensate pharmacists directly for providing these services. To encourage competition and innovation, the exact nature of MTM services and the criteria for patients to qualify were initially left undefined. Basic program requirements and eligibility criteria have since evolved, although the programs are far from standardized. A consortium of 11 national pharmacy organizations developed a consensus definition of MTM programs that identified pharmacists as the key service providers.16 The eligibility criteria for beneficiaries of MTM programs are described in TABLE 1.17 Benefit plans can offer MTM services to patients with any chronic disease or may limit them to selected diseases. Diabetes is the most frequently targeted disease and is covered by virtually all MTM services (FIGURE).17
Pharmacy organizations next developed a guideline that specified 5 core activities of MTM services to be provided in pharmacies (TABLE 2).18 According to this guideline (hereafter referred to as the “Core Elements of MTM”), patients who qualify for MTM services must receive an annual comprehensive medication therapy review, with additional reviews and ongoing pharmacist monitoring as necessary.17,18 Over-the-counter medications, herbal therapies, and dietary supplements should be included in the medication review. Though face-to-face interaction is preferred, and should be required, services may be provided by telephone and may be either by appointment or on a walk-in basis.18 According to the guideline, patients should be provided with a printed or written document, such as a summary of recommendations or an action plan, to take with them. Services may be provided regardless of whether the pharmacist is dispensing medications to the patient. Physician referrals are also not required for pharmacists to offer MTM services to qualifying patients.18 However, although referral by a physician/ HCP is not required for MTM provided by a pharmacist, the physician/HCP does need to be contacted for anything that requires a change in management (eg, changes to treatment). In my practice, I typically write a summary letter to the patient’s physician/HCP; this includes my assessment of the session and any recommendations. Patients are also encouraged to share their personal medication record and action plan with their HCPs. MTM enrollment requirements were revised in 2010 and now require payers to identify target beneficiaries for automatic enrollment.17
TABLE 1
Patient eligibility criteria for MTM programs17
| Multiple chronic diseases |
Programs must offer MTM services to patients who have at least 2 or 3 chronic diseases (at the plan’s discretion) and must target at least 4 of the following:
|
| Multiple covered drugs |
| Plans vary in the number of drugs patients must be prescribed to qualify, with thresholds ranging from 2 to 8. |
| Cost threshold |
| Patients must be expected to incur at least $3000 in annual Part D drug costs. |
| COPD, chronic obstructive pulmonary disease; MTM, medication therapy management. |
FIGURE
The top 10 diseases targeted by MTM programs in 2010 and the percentage of MTM programs that targeted these diseases17
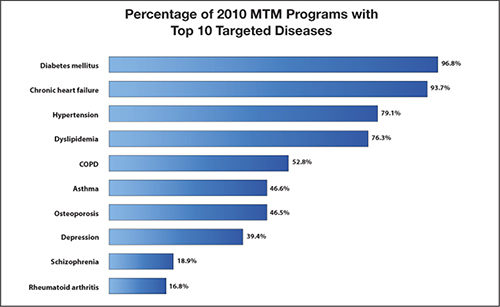
COPD, chronic obstructive pulmonary disease; MTM, medication therapy management.
Reproduced with permission from Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management (MTM) Programs. https://www.cms.gov/PrescriptionDrugCovContra/ Downloads/MTMFactSheet_2010_06-2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.TABLE 2
Core elements of an MTM service model18
| Medication therapy review |
| Systematic review of the patient’s medications to assess and prioritize problems and create a plan to resolve them. |
| Personal medical record |
| Comprehensive record of the patient’s prescription and nonprescription medications, herbal agents, and nutritional supplements. The record is kept and updated by the patient, brought to appointments in different settings, and used by the patient in medication self-management. |
| Medication-related action plan |
| List of actions for the patient to use in self-management. The plan is developed collaboratively by the patient and pharmacist and used to track progress toward achieving specific goals. |
| Intervention and/or referral |
| The pharmacist intervenes or refers the patient to another health professional to address medication-related problems. |
| Documentation and follow-up |
| The pharmacist documents all MTM services and interventions— ideally, electronically. Follow-up or a referral to a different care setting is scheduled based on the patient’s needs. |
| MTM, medication therapy management. |
MTM services in pharmacy practice
MTM services are becoming well established in pharmacy practice. According to an annual survey conducted by the American Pharmacists Association, 72% of pharmacist respondents were offering MTM services in 2009, and about one-third of the rest planned to offer the services soon.19 About 84% of payer respondents (mostly health maintenance organizations, managed care insurers, and prescription benefit management plans) were offering MTM services. Contracted pharmacists provided about two-thirds of MTM care, with in-house pharmacists and contracted MTM organizations providing substantial amounts of services, and nurses and physicians providing a small proportion.19-20 MTM services are not restricted to Medicare patients, but are increasingly being offered by managed care organizations and fee-for-service plans.12,21 Some payers support pharmacist-provided MTM services as part of a broader multidisciplinary disease management program.20
Community pharmacists wishing to offer MTM services have several potential business models. Although they can contract directly with Medicare Part D insurers, it can be difficult and time-consuming to develop these individual contracts. Many insurers are not yet equipped to deal efficiently with pharmacists wishing to initiate this type of arrangement, and insurers are only slowly making the shift toward regarding pharmacists as providers.
A second option is to contract with an MTM intermediary company that links payers with pharmacists. These companies can be approached via their Web sites.12 Their services make it unnecessary for pharmacists to contract with different payers, find patients, or establish new billing systems. The American Society of Consultant Pharmacists offers a program through its Web site (http://www.ascp.org). Known as the MTM Provider Partners Program, it is a pathway for its members to enter the MTM world.
A third option is for pharmacists to provide patients with MTM services and then bill payers—so-called blind billing. Bills for patients covered by Medicare can be submitted using the CMS-1500 form available from the Web site of the Centers for Medicare and Medicaid Services, http://www.cms.gov. Assistance with billing codes is available from the Pharmacist Services Technical Advisory Coalition, http://www.pstac.org. It should be noted that although submission of these claims to various payers is becoming more standardized, there is no guarantee of payment with blind billing. Pharmacists may be reluctant to provide complex, time-consuming MTM services in the absence of such a guarantee. Providing MTM directly to patients in a fee-for-service manner is another option being explored in a few pharmacies.
Inconsistent documentation requirements and reimbursement policies among payers are barriers to community pharmacists’ adoption of MTMs.20 Other barriers to adoption of MTMs, or to their most effective use, include a lack of pharmacists’ time, staffing issues, difficulty forming collaborative relationships with physicians, poor patient mobility and low health literacy, a lack of medical information, and difficulty motivating patients to engage in the programs.15,20-23 It can be challenging to persuade patients of the value of a commitment to time-consuming MTM care, but once they have tried it, many become enthusiastic participants. As the following case study illustrates, use of the various components of the MTM model can help give patients with diabetes and multiple other illnesses a sense of ownership and control.
CASE STUDY Patient with T2DM and multiple comorbidities
A 49-year-old African American woman, who qualifies for Medicare because of disability, first enrolled in our pharmacy’s advertised diabetes education classes 3 years ago, out of concern over her long history of uncontrolled diabetes. At that time, her body mass index (BMI) was 35 kg/m2 and her A1C was 10%. In addition to T2DM, she had asthma, gastroesophageal reflux disease (GERD), hypertension, hyperlipidemia, gout, seasonal allergies, and a prior myocardial infarction.
I have worked closely with this patient over the succeeding 3 years, providing weekly diabetes education and counseling. At first she was using NPH insulin twice a day and adjusting the doses on her own, without the close involvement of her endocrinologist. As long-acting insulin analogs (ie, insulin glargine and insulin detemir) have relatively flat and more predictable time–action profiles that last up to 24 hours,24 I persuaded her to switch to a basal–bolus regimen with insulin detemir and insulin aspart. Insulin detemir is also associated with less weight gain and fewer hypoglycemic episodes than NPH insulin,25-27 which was especially important given this patient’s obesity and fear of hypoglycemia. It is, however, important to note that changes in medication should also be reviewed with the patient’s treating physician. In addition, I spent a year working closely with the patient on carbohydrate counting.
Pharmacists can also explore different insulin delivery methods with patients. Many patients find insulin pens more convenient, more discreet, and easier to use than a vial and syringe.28,29 Insulin pumps can also be a useful option for certain patients.30 Recently, this patient began using an insulin pump, which was recommended to help her achieve better blood glucose control, despite her erratic meal patterns. The results are generally good, although she still has glucose spikes due to metabolic issues and inconsistent eating patterns, and her BMI has increased slightly (36.1 kg/m2). However, her current A1C is 7.1%.
This patient’s complicated medical history and large number of medications (TABLE 3) suggested the need for a comprehensive medication review, as described in the Core Elements of MTM.18 The result of the review was a letter to her physician, with a number of recommendations about her medications, lifestyle changes, and symptoms to investigate. Among the problems discovered were muscle pain and creatine kinase elevation as a possible side effect of her statin therapy; poorly controlled hypertension; poor compliance with some of her medications; the possibility of an interaction between her insulin and beta-blocker; symptoms of congestive heart failure; and signs of possible Cushing’s syndrome. Among the recommended actions were withdrawal of the statin until muscle symptoms could be investigated and modifications of some of her medications to a more easily tolerated form or dosage schedule. Diet, exercise, and weight loss were recommended to ameliorate many of her health problems. Her physician was also advised that she should avoid foods that would exacerbate her GERD and gout and that she should follow the low-salt DASH (Dietary Approaches to Stop Hypertension) diet to help manage her hypertension. It is important to note that, while the pharmacist may make recommendations for symptoms to be investigated, it is the physician who should be making the diagnosis, and pharmacists and physicians should be collaborating as part of a treatment team.
This patient’s fear of hypoglycemia has presented an ongoing challenge in her diabetes education. She often would load up on carbohydrates before leaving work to avoid becoming hypoglycemic on the train ride home. She is extremely insulin resistant, and it has required a major effort to help her feel comfortable with taking enough insulin. She has been very conscientious in documenting the results of her glucose self-monitoring, but has received little education from her physician about what to do with the information. Carbohydrate counting has been difficult for her and continues to be a major focus of our weekly sessions.
The close attention that this patient receives from her pharmacist contrasts with the usual care received by many patients with diabetes. It is not uncommon for patients to tell me that, when they were first diagnosed with T2DM, they were given a prescription and, at best, sent to a dietitian for nutritional counseling. Newly diagnosed patients are advised to monitor their blood glucose; because I see patients once a week, it is easy to help them understand the immediate interactions between diet, exercise, insulin sensitivity, specific medications and doses, and glucose levels.
The medication-related action plan (MAP), one of the Core Elements of MTM,18 is a useful tool to help patients take control of their progress in managing their diabetes. We use it as a medical action plan, involving far more than just medications. These plans are completed at every visit, collaboratively with the patient, and reviewed as follow-up at the next visit. The form contains a space for each planned activity and a space to document progress toward that activity or its completion. Activities might include changing the time of day a medication is taken, going for a lab test, asking the physician to explain cholesterol levels, or observing the emotional states that might lead to binge eating. Holding patients accountable for the activities in the MAP helps them to achieve their self-management goals.
TABLE 3
Case study: Health problems and medications at the time of medication therapy review
| Health problems | Medications | Recommendations |
|---|---|---|
| Type 2 diabetes |
|
|
| Hyperlipidemia |
|
|
| Hypertension (poorly controlled) |
|
|
| Cardiovascular disease |
|
|
| Gout | — |
|
| GERD |
|
|
| Obesity | — |
|
| Seasonal allergies |
|
|
| DASH, Dietary Approaches to Stop Hypertension; GERD, gastroesophageal reflux disease. | ||
Clinical and economic outcomes of MTM
As MTM programs are too diverse to be studied as a group, most outcome studies conducted to date provide data only on specific MTM programs and provide little information about MTMs overall.15 Furthermore, few, if any, studies have examined the effects of MTMs specifically in diabetes. However, numerous publications suggest that pharmacist-provided care can improve clinical outcomes. According to 2 systematic reviews of studies conducted in patients with diabetes, A1C was highly sensitive to a variety of interventions by pharmacists, such as diabetes education and medication management.31,32 In a Veterans Affairs Health Care System, pharmacists’ use of a preplanned insulin initiation and titration protocol resulted in the successful implementation of an insulin initiation clinic through CDTM and improved patients’ glycemic control compared with when the patients were receiving only oral antihyperglycemic agents.33 Two often-cited programs, the Asheville Project34 and the Diabetes Ten City Challenge,35 demonstrated that pharmacist-provided MTM-like care for T2DM resulted in health care cost savings, as well as improved clinical outcomes. However, these results are not directly applicable to MTM services because they were conducted in relatively healthy employee populations. Many studies have examined the overall effects of MTMs on health care costs, but results have been inconsistent, in part because of variation in which costs were included in the analyses.20 It seems inevitable that as the MTM model matures, data will demonstrate the clinical and economic value of pharmacists providing primary care for patients with T2DM and other complex medical conditions.
Conclusions
Pharmacists can help optimize diabetes drug therapy by improving tolerability, reducing risks, and increasing patients’ likelihood of attaining treatment goals. Pharmacist-led diabetes education can go beyond medication and glycemic control to promote overall wellness and a healthy lifestyle. With their involvement in MTM, pharmacists can apply their expertise in drug therapy to a patient population with complex and challenging needs.
1. Biola H, Green LA, Phillips RL, et al. The U.S. primary care physician workforce: minimal growth 1980–1999. Am Fam Physician. 2003;68(8):1483.-
2. Council on Credentialing in Pharmacy. Scope of contemporary pharmacy practice: roles, responsibilities, and functions of pharmacists and pharmacy technicians. J Am Pharm Assoc (2003). 2010;50(2):e35-e69.
3. Drab S. Translating clinical guidelines into clinical practice. Role of the pharmacist in type 2 diabetes management. J Am Pharm Assoc (2003). 2009;49(6):e152-e162.
4. Posey LM, Tanzi MG. Diabetes care: Model for the future of primary care. J Am Pharm Assoc (2003). 2010;50(5):623-626.
5. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533-543.
6. Malloy MJ, DeBellis R. Collaborative drug therapy management, medication treatment management, and Medicare Part D: What do they have in common? Harvard Health Policy Review. 2006;7(1):186-188.
7. McGivney MS, Meyer SM, Duncan-Hewitt W, Hall DL, Goode JV, Smith RB. Medication therapy management: its relationship to patient counseling, disease management, and pharmaceutical care. J Am Pharm Assoc (2003). 2007;47(5):620-628.
8. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2011;34(suppl 1):S89-S96.
9. Daly A, Kulkarni K, Boucher J. The new credential: advanced diabetes management. J Am Diet Assoc. 2001;101(8):940-943.
10. Alliance for Pharmaceutical Care. Collaborative Drug Therapy Management: A Coordinated Approach to Patient Care. http://www.ashp.org/s_ashp/docs/files/about/CDTM.doc. Accessed February 3, 2011.
11. Roberts S, Gainsbrugh R. Medication therapy management and collaborative drug therapy management [letter]. J Managed Care Pharm. 2010;16(1):67-68.
12. Martin CM, McSpadden CS. Dispelling the myths about medication therapy management services. Consult Pharm. 2008;23(11):866-872, 875.
13. American Pharmacists Association. Delivering Medication Therapy Management Services in the Community. http://www.pharmacist.com/ctp/mtm. Published March 1, 2009. Accessed February 1, 2011.
14. American Society of Consultant Pharmacists. Delivering Medication Therapy Management Services in The Community—Updated for 2010. https://www.ascp.com/articles/professional-development/delivering-medication-therapy-management-services-community-update. Accessed February 1, 2011.
15. Pellegrino AN, Martin MT, Tilton JJ, Touchette DR. Medication therapy management services: definitions and outcomes. Drugs. 2009;69(4):393-406.
16. Bluml BM. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc (2003). 2005;45(5):566-572.
17. Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management Programs. https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet_2010_06_2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.
18. American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0). J Am Pharm Assoc (2003). 2008;48(3):341-353.
19. American Pharmacists Association. Medication Therapy Management Digest. Perspectives on 2009: A Year of Changing Opportunities. http://www.pharmacist.com/AM/Template.cfm?Section=Home2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=22674. Published March 2010. Accessed February 1, 2011.
20. Abt Associates. Exploratory Research on Medication Therapy Management. Final report. http://www.cms.hhs.gov/Reports/downloads/blackwell.pdf. Published July 8, 2008. Accessed February 1, 2011.
21. Buffington DE. Future of medication therapy management services in delivering patient-centered care. Am J Health Syst Pharm. 2007;64(15 suppl 10):S10-S12; quiz S21–S23.
22. Law AV, Okamoto MP, Brock K. Ready, willing, and able to provide MTM services?: A survey of community pharmacists in the USA. Res Social Adm Pharm. 2009;5(4):376-381.
23. Lounsbery JL, Green CG, Bennett MS, Pedersen CA. Evaluation of pharmacists’ barriers to the implementation of medication therapy management services. J Am Pharm Assoc (2003). 2009;49(1):51-58.
24. Freeman JS. Insulin analog therapy: improving the match with physiologic insulin secretion. J Am Osteopath Assoc. 2009;109(1):26-36.
25. Davies MJ, Derezinski T, Pedersen CB, Clauson P. Reduced weight gain with insulin detemir compared to NPH insulin is not explained by a reduction in hypoglycemia. Diabetes Technol Ther. 2008;10(4):273-277.
26. Fajardo Montanana C, Hernandez Herrero C, Rivas Fernandez M. Less weight gain and hypoglycaemia with once-daily insulin detemir than NPH insulin in intensification of insulin therapy in overweight Type 2 diabetes patients: the PREDICTIVE BMI clinical trial. Diabet Med. 2008;25(8):916-923.
27. Mandosi E, Fallarino M, Rossetti M, Gatti A, Morano S. Waist circumference reduction after insulin detemir therapy in type 2 diabetes patients previously treated with NPH. Diabetes Res Clin Pract. 2009;84(2):e18-e20.
28. Korytkowski M, Bell D, Jacobsen C, Suwannasari R. A multicenter, randomized, open-label, comparative, two-period crossover trial of preference, efficacy, and safety profiles of a prefilled, disposable pen and conventional vial/syringe for insulin injection in patients with type 1 or 2 diabetes mellitus. Clin Ther. 2003;25(11):2836-2848.
29. Molife C, Lee LJ, Shi L, Sawhney M, Lenox SM. Assessment of patient-reported outcomes of insulin pen devices versus conventional vial and syringe. Diabetes Technol Ther. 2009;11(8):529-538.
30. Jankovec Z, Cechurova D, Krcma M, Lacigova S, Zourek M, Rusavy Z. The influence of insulin pump treatment on metabolic syndrome parameters in type 2 diabetes mellitus. Wien Klin Wochenschr. 2009;121(13-14):459-463.
31. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part I: systematic review and meta analysis in diabetes management. Ann Pharmacother. 2007;41(10):1569-1582.
32. Wubben DP, Vivian EM. Effects of pharmacist outpatient interventions on adults with diabetes mellitus: a systematic review. Pharmacotherapy. 2008;28(4):421-436.
33. Rochester CD, Leon N, Dombrowski R, Haines ST. Collaborative drug therapy management for initiating and adjusting insulin therapy in patients with type 2 diabetes mellitus. Am J Health Syst Pharm. 2010;67(1):42-48.
34. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc (Wash). 2003;43(2):173-184.
35. Fera T, Bluml BM, Ellis WM. Diabetes Ten City Challenge: Final economic and clinical results. J Am Pharm Assoc (2003). 2009;49(3):383-391.
Traditional or centralized models of diabetes care: The multidisciplinary diabetes team approach
Nontraditional or noncentralized models of diabetes care: Medication therapy management services
Nontraditional or noncentralized models of diabetes care: Boutique medicine
- Medication therapy management (MTM) services were introduced in the mid-2000s as part of Medicare Part D—the prescription drug benefit
- Key goals of MTM services are to:
- – Counsel patients to improve understanding of their medications
- – Improve medication adherence
- – Detect adverse drug reactions and patterns of improper drug use
- MTM services are becoming well established in pharmacy practice
- Pharmacists can help improve outcomes by:
- – Following patient progress between physician visits
- – Utilizing their clinical expertise to monitor and manage diabetes medication plans
- – Educating patients on disease, lifestyle, and adherence issues
- Although referral by a physician/health care professional (HCP) is not required for MTM provided by a pharmacist, the physician/ HCP needs to be contacted for anything that requires a change in management
Introduction
Patients with type 2 diabetes mellitus (T2DM) have a large unmet medical need for appropriate treatment and continuity of care. Treatment of T2DM requires a complex, stepped approach combining behavioral modifications and multiple medications, as well as close monitoring of the effects of these interventions. In addition, these patients often require treatment for diabetes-related complications and comorbid medical conditions. Problems may arise from the complex medication regimens that T2DM patients often require. The primary care physician (PCP) has been the traditional provider or coordinator of care for T2DM. However, recent trends have imposed limits on access to the full scope of primary care needed by the growing number of patients affected by this and other chronic illnesses. The pool of PCPs is shrinking, physicians lack the time needed for complex patient interactions, and planners are discussing the shifting of primary care responsibilities to other types of health care professionals (HCPs), such as nurse practitioners, physician assistants, and pharmacists.1-4
The pharmacist’s role in managing chronic diseases
Pharmacists are a professional group with sufficient education and skills to take a leading role in the primary care of patients with T2DM and other patients with complex needs. Pharmacists are the third-largest group of health professionals in the United States (US).2 The emphasis of professional pharmacy practice has been shifting from a product-oriented, medication-dispensing role, to a patient-centered role, in which the pharmacist provides cognitive services and patient management. Provision of time-consuming primary care for T2DM is made more feasible not only by this growing supply of practicing pharmacists—expected to reach 300,000 by 2020—but also by 2 trends that should increase the availability of their time: the automation of pharmacy practice and the growth of certified pharmacy technicians to a number about equal to that of pharmacists.4
The “pharmaceutical care” philosophy was first articulated 2 decades ago as a call for pharmacists to assume a wider scope of professional responsibility in improving the outcomes of drug therapy, preventing medication-related morbidity and mortality, and improving patients’ quality of life.5 Falling within this paradigm are diabetes self-management education or training (DSME/DSMT), disease management, and collaborative drug therapy management (CDTM), all of which are models that have been applied to pharmacy care in recent decades.6,7 DSME/DSMT programs aim to educate patients on all aspects of diabetes control, including nutrition and exercise, blood glucose control, medication management, and prevention of complications. DSME is taught in an individual or classroom format by certified diabetes educator (CDE) nurses, dietitians, pharmacists, or other professionals. The CDE credential, administered by the National Certification Board of Diabetes Educators, is the national credential for health professionals who provide diabetes patient education and counseling.8
Disease management programs, widely adopted in the 1990s, may be delivered by physicians, pharmacists, or other HCPs or teams. These programs are disease-specific and focus on conditions that require a considerable degree of patient self-management. They provide a wider range of services than just patient education, and may include drug and nondrug therapy. However, they do not usually encompass the needs of patients with multiple chronic illnesses. Some pharmacists are now specializing in management of specific diseases, such as diabetes, and the Board Certified-Advanced Diabetes Management (BC-ADM) credential has been introduced for pharmacists, nurses, and dietitians.9 This credential was originally introduced in 2000, but is currently being reviewed by the American Association of Diabetes Educators. The BC-ADM certifies expertise in patient evaluation and clinical management, as well as patient education. However, because the responsibilities for disease management are often shared among members of a team, pharmacists who provide disease management services may have difficulty obtaining compensation for their contribution.7
CDTM programs consist of partnerships between physicians and pharmacists in which the pharmacist can start, modify, or continue drug therapy for a specific patient according to a written protocol. Protocols may be specific to a single patient or may cover all patients treated by a physician for a specified condition. For example, in a low-risk patient with T2DM, a protocol might specify that the pharmacist can adjust a patient’s insulin dose as long as the glycated hemoglobin (A1C) or blood glucose remains below a certain threshold, but the physician should be contacted if a threshold is exceeded. CDTM programs also may allow pharmacists to take responsibility for ordering tests and providing patient education. Individual state laws have established CDTM legislation, and the activity of pharmacists within CDTM programs is regulated at the state level. The programs are currently available in all but 3 states: Alabama, Oklahoma, and Maine. In most jurisdictions, CTDM agreements are easily established between physicians and regular retail pharmacists, or pharmacists working in a clinic setting.6,10,11 In New York, CDTM was recently assessed for pharmacists practicing in teaching hospitals only.
Medication therapy management (MTM) programs are a further evolution in pharmaceutical patient care. MTM was introduced as part of Medicare legislation in the mid-2000s as a means for pharmacists and other qualified HCPs to improve the care of selected Medicare beneficiaries with multiple chronic illnesses who require multiple medications. MTM services may help address the need to prevent medication-related morbidity and mortality in patients with T2DM and comorbid conditions. Pharmacists can provide continuity of care by following patient progress between physician visits; by utilizing their clinical expertise to monitor and manage diabetes medication plans; and by educating patients on disease, lifestyle, and adherence issues. This level of service can be provided adequately by pharmacists, pharmacist CDEs, and pharmacists with the BC-ADM credential. In addition, many local, state, and national pharmacy organizations and pharmacy schools are providing targeted training for pharmacists wishing to deliver MTM services.12-14
Overview of MTM services
The US Medicare Modernization Act of 2003 established MTM services as part of Medicare Part D—the prescription drug benefit. The Act requires Medicare insurers to provide MTM services to a defined group of beneficiaries expected to benefit from enhanced medication management. Key goals of MTM services are to counsel patients to improve understanding of their medications, to improve medication adherence, and to detect adverse drug reactions and patterns of improper drug use.15 For the first time, the Act created a mechanism for insurers to compensate pharmacists directly for providing these services. To encourage competition and innovation, the exact nature of MTM services and the criteria for patients to qualify were initially left undefined. Basic program requirements and eligibility criteria have since evolved, although the programs are far from standardized. A consortium of 11 national pharmacy organizations developed a consensus definition of MTM programs that identified pharmacists as the key service providers.16 The eligibility criteria for beneficiaries of MTM programs are described in TABLE 1.17 Benefit plans can offer MTM services to patients with any chronic disease or may limit them to selected diseases. Diabetes is the most frequently targeted disease and is covered by virtually all MTM services (FIGURE).17
Pharmacy organizations next developed a guideline that specified 5 core activities of MTM services to be provided in pharmacies (TABLE 2).18 According to this guideline (hereafter referred to as the “Core Elements of MTM”), patients who qualify for MTM services must receive an annual comprehensive medication therapy review, with additional reviews and ongoing pharmacist monitoring as necessary.17,18 Over-the-counter medications, herbal therapies, and dietary supplements should be included in the medication review. Though face-to-face interaction is preferred, and should be required, services may be provided by telephone and may be either by appointment or on a walk-in basis.18 According to the guideline, patients should be provided with a printed or written document, such as a summary of recommendations or an action plan, to take with them. Services may be provided regardless of whether the pharmacist is dispensing medications to the patient. Physician referrals are also not required for pharmacists to offer MTM services to qualifying patients.18 However, although referral by a physician/ HCP is not required for MTM provided by a pharmacist, the physician/HCP does need to be contacted for anything that requires a change in management (eg, changes to treatment). In my practice, I typically write a summary letter to the patient’s physician/HCP; this includes my assessment of the session and any recommendations. Patients are also encouraged to share their personal medication record and action plan with their HCPs. MTM enrollment requirements were revised in 2010 and now require payers to identify target beneficiaries for automatic enrollment.17
TABLE 1
Patient eligibility criteria for MTM programs17
| Multiple chronic diseases |
Programs must offer MTM services to patients who have at least 2 or 3 chronic diseases (at the plan’s discretion) and must target at least 4 of the following:
|
| Multiple covered drugs |
| Plans vary in the number of drugs patients must be prescribed to qualify, with thresholds ranging from 2 to 8. |
| Cost threshold |
| Patients must be expected to incur at least $3000 in annual Part D drug costs. |
| COPD, chronic obstructive pulmonary disease; MTM, medication therapy management. |
FIGURE
The top 10 diseases targeted by MTM programs in 2010 and the percentage of MTM programs that targeted these diseases17
COPD, chronic obstructive pulmonary disease; MTM, medication therapy management.
Reproduced with permission from Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management (MTM) Programs. https://www.cms.gov/PrescriptionDrugCovContra/ Downloads/MTMFactSheet_2010_06-2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.TABLE 2
Core elements of an MTM service model18
| Medication therapy review |
| Systematic review of the patient’s medications to assess and prioritize problems and create a plan to resolve them. |
| Personal medical record |
| Comprehensive record of the patient’s prescription and nonprescription medications, herbal agents, and nutritional supplements. The record is kept and updated by the patient, brought to appointments in different settings, and used by the patient in medication self-management. |
| Medication-related action plan |
| List of actions for the patient to use in self-management. The plan is developed collaboratively by the patient and pharmacist and used to track progress toward achieving specific goals. |
| Intervention and/or referral |
| The pharmacist intervenes or refers the patient to another health professional to address medication-related problems. |
| Documentation and follow-up |
| The pharmacist documents all MTM services and interventions— ideally, electronically. Follow-up or a referral to a different care setting is scheduled based on the patient’s needs. |
| MTM, medication therapy management. |
MTM services in pharmacy practice
MTM services are becoming well established in pharmacy practice. According to an annual survey conducted by the American Pharmacists Association, 72% of pharmacist respondents were offering MTM services in 2009, and about one-third of the rest planned to offer the services soon.19 About 84% of payer respondents (mostly health maintenance organizations, managed care insurers, and prescription benefit management plans) were offering MTM services. Contracted pharmacists provided about two-thirds of MTM care, with in-house pharmacists and contracted MTM organizations providing substantial amounts of services, and nurses and physicians providing a small proportion.19-20 MTM services are not restricted to Medicare patients, but are increasingly being offered by managed care organizations and fee-for-service plans.12,21 Some payers support pharmacist-provided MTM services as part of a broader multidisciplinary disease management program.20
Community pharmacists wishing to offer MTM services have several potential business models. Although they can contract directly with Medicare Part D insurers, it can be difficult and time-consuming to develop these individual contracts. Many insurers are not yet equipped to deal efficiently with pharmacists wishing to initiate this type of arrangement, and insurers are only slowly making the shift toward regarding pharmacists as providers.
A second option is to contract with an MTM intermediary company that links payers with pharmacists. These companies can be approached via their Web sites.12 Their services make it unnecessary for pharmacists to contract with different payers, find patients, or establish new billing systems. The American Society of Consultant Pharmacists offers a program through its Web site (http://www.ascp.org). Known as the MTM Provider Partners Program, it is a pathway for its members to enter the MTM world.
A third option is for pharmacists to provide patients with MTM services and then bill payers—so-called blind billing. Bills for patients covered by Medicare can be submitted using the CMS-1500 form available from the Web site of the Centers for Medicare and Medicaid Services, http://www.cms.gov. Assistance with billing codes is available from the Pharmacist Services Technical Advisory Coalition, http://www.pstac.org. It should be noted that although submission of these claims to various payers is becoming more standardized, there is no guarantee of payment with blind billing. Pharmacists may be reluctant to provide complex, time-consuming MTM services in the absence of such a guarantee. Providing MTM directly to patients in a fee-for-service manner is another option being explored in a few pharmacies.
Inconsistent documentation requirements and reimbursement policies among payers are barriers to community pharmacists’ adoption of MTMs.20 Other barriers to adoption of MTMs, or to their most effective use, include a lack of pharmacists’ time, staffing issues, difficulty forming collaborative relationships with physicians, poor patient mobility and low health literacy, a lack of medical information, and difficulty motivating patients to engage in the programs.15,20-23 It can be challenging to persuade patients of the value of a commitment to time-consuming MTM care, but once they have tried it, many become enthusiastic participants. As the following case study illustrates, use of the various components of the MTM model can help give patients with diabetes and multiple other illnesses a sense of ownership and control.
CASE STUDY Patient with T2DM and multiple comorbidities
A 49-year-old African American woman, who qualifies for Medicare because of disability, first enrolled in our pharmacy’s advertised diabetes education classes 3 years ago, out of concern over her long history of uncontrolled diabetes. At that time, her body mass index (BMI) was 35 kg/m2 and her A1C was 10%. In addition to T2DM, she had asthma, gastroesophageal reflux disease (GERD), hypertension, hyperlipidemia, gout, seasonal allergies, and a prior myocardial infarction.
I have worked closely with this patient over the succeeding 3 years, providing weekly diabetes education and counseling. At first she was using NPH insulin twice a day and adjusting the doses on her own, without the close involvement of her endocrinologist. As long-acting insulin analogs (ie, insulin glargine and insulin detemir) have relatively flat and more predictable time–action profiles that last up to 24 hours,24 I persuaded her to switch to a basal–bolus regimen with insulin detemir and insulin aspart. Insulin detemir is also associated with less weight gain and fewer hypoglycemic episodes than NPH insulin,25-27 which was especially important given this patient’s obesity and fear of hypoglycemia. It is, however, important to note that changes in medication should also be reviewed with the patient’s treating physician. In addition, I spent a year working closely with the patient on carbohydrate counting.
Pharmacists can also explore different insulin delivery methods with patients. Many patients find insulin pens more convenient, more discreet, and easier to use than a vial and syringe.28,29 Insulin pumps can also be a useful option for certain patients.30 Recently, this patient began using an insulin pump, which was recommended to help her achieve better blood glucose control, despite her erratic meal patterns. The results are generally good, although she still has glucose spikes due to metabolic issues and inconsistent eating patterns, and her BMI has increased slightly (36.1 kg/m2). However, her current A1C is 7.1%.
This patient’s complicated medical history and large number of medications (TABLE 3) suggested the need for a comprehensive medication review, as described in the Core Elements of MTM.18 The result of the review was a letter to her physician, with a number of recommendations about her medications, lifestyle changes, and symptoms to investigate. Among the problems discovered were muscle pain and creatine kinase elevation as a possible side effect of her statin therapy; poorly controlled hypertension; poor compliance with some of her medications; the possibility of an interaction between her insulin and beta-blocker; symptoms of congestive heart failure; and signs of possible Cushing’s syndrome. Among the recommended actions were withdrawal of the statin until muscle symptoms could be investigated and modifications of some of her medications to a more easily tolerated form or dosage schedule. Diet, exercise, and weight loss were recommended to ameliorate many of her health problems. Her physician was also advised that she should avoid foods that would exacerbate her GERD and gout and that she should follow the low-salt DASH (Dietary Approaches to Stop Hypertension) diet to help manage her hypertension. It is important to note that, while the pharmacist may make recommendations for symptoms to be investigated, it is the physician who should be making the diagnosis, and pharmacists and physicians should be collaborating as part of a treatment team.
This patient’s fear of hypoglycemia has presented an ongoing challenge in her diabetes education. She often would load up on carbohydrates before leaving work to avoid becoming hypoglycemic on the train ride home. She is extremely insulin resistant, and it has required a major effort to help her feel comfortable with taking enough insulin. She has been very conscientious in documenting the results of her glucose self-monitoring, but has received little education from her physician about what to do with the information. Carbohydrate counting has been difficult for her and continues to be a major focus of our weekly sessions.
The close attention that this patient receives from her pharmacist contrasts with the usual care received by many patients with diabetes. It is not uncommon for patients to tell me that, when they were first diagnosed with T2DM, they were given a prescription and, at best, sent to a dietitian for nutritional counseling. Newly diagnosed patients are advised to monitor their blood glucose; because I see patients once a week, it is easy to help them understand the immediate interactions between diet, exercise, insulin sensitivity, specific medications and doses, and glucose levels.
The medication-related action plan (MAP), one of the Core Elements of MTM,18 is a useful tool to help patients take control of their progress in managing their diabetes. We use it as a medical action plan, involving far more than just medications. These plans are completed at every visit, collaboratively with the patient, and reviewed as follow-up at the next visit. The form contains a space for each planned activity and a space to document progress toward that activity or its completion. Activities might include changing the time of day a medication is taken, going for a lab test, asking the physician to explain cholesterol levels, or observing the emotional states that might lead to binge eating. Holding patients accountable for the activities in the MAP helps them to achieve their self-management goals.
TABLE 3
Case study: Health problems and medications at the time of medication therapy review
| Health problems | Medications | Recommendations |
|---|---|---|
| Type 2 diabetes |
|
|
| Hyperlipidemia |
|
|
| Hypertension (poorly controlled) |
|
|
| Cardiovascular disease |
|
|
| Gout | — |
|
| GERD |
|
|
| Obesity | — |
|
| Seasonal allergies |
|
|
| DASH, Dietary Approaches to Stop Hypertension; GERD, gastroesophageal reflux disease. | ||
Clinical and economic outcomes of MTM
As MTM programs are too diverse to be studied as a group, most outcome studies conducted to date provide data only on specific MTM programs and provide little information about MTMs overall.15 Furthermore, few, if any, studies have examined the effects of MTMs specifically in diabetes. However, numerous publications suggest that pharmacist-provided care can improve clinical outcomes. According to 2 systematic reviews of studies conducted in patients with diabetes, A1C was highly sensitive to a variety of interventions by pharmacists, such as diabetes education and medication management.31,32 In a Veterans Affairs Health Care System, pharmacists’ use of a preplanned insulin initiation and titration protocol resulted in the successful implementation of an insulin initiation clinic through CDTM and improved patients’ glycemic control compared with when the patients were receiving only oral antihyperglycemic agents.33 Two often-cited programs, the Asheville Project34 and the Diabetes Ten City Challenge,35 demonstrated that pharmacist-provided MTM-like care for T2DM resulted in health care cost savings, as well as improved clinical outcomes. However, these results are not directly applicable to MTM services because they were conducted in relatively healthy employee populations. Many studies have examined the overall effects of MTMs on health care costs, but results have been inconsistent, in part because of variation in which costs were included in the analyses.20 It seems inevitable that as the MTM model matures, data will demonstrate the clinical and economic value of pharmacists providing primary care for patients with T2DM and other complex medical conditions.
Conclusions
Pharmacists can help optimize diabetes drug therapy by improving tolerability, reducing risks, and increasing patients’ likelihood of attaining treatment goals. Pharmacist-led diabetes education can go beyond medication and glycemic control to promote overall wellness and a healthy lifestyle. With their involvement in MTM, pharmacists can apply their expertise in drug therapy to a patient population with complex and challenging needs.
Traditional or centralized models of diabetes care: The multidisciplinary diabetes team approach
Nontraditional or noncentralized models of diabetes care: Medication therapy management services
Nontraditional or noncentralized models of diabetes care: Boutique medicine
- Medication therapy management (MTM) services were introduced in the mid-2000s as part of Medicare Part D—the prescription drug benefit
- Key goals of MTM services are to:
- – Counsel patients to improve understanding of their medications
- – Improve medication adherence
- – Detect adverse drug reactions and patterns of improper drug use
- MTM services are becoming well established in pharmacy practice
- Pharmacists can help improve outcomes by:
- – Following patient progress between physician visits
- – Utilizing their clinical expertise to monitor and manage diabetes medication plans
- – Educating patients on disease, lifestyle, and adherence issues
- Although referral by a physician/health care professional (HCP) is not required for MTM provided by a pharmacist, the physician/ HCP needs to be contacted for anything that requires a change in management
Introduction
Patients with type 2 diabetes mellitus (T2DM) have a large unmet medical need for appropriate treatment and continuity of care. Treatment of T2DM requires a complex, stepped approach combining behavioral modifications and multiple medications, as well as close monitoring of the effects of these interventions. In addition, these patients often require treatment for diabetes-related complications and comorbid medical conditions. Problems may arise from the complex medication regimens that T2DM patients often require. The primary care physician (PCP) has been the traditional provider or coordinator of care for T2DM. However, recent trends have imposed limits on access to the full scope of primary care needed by the growing number of patients affected by this and other chronic illnesses. The pool of PCPs is shrinking, physicians lack the time needed for complex patient interactions, and planners are discussing the shifting of primary care responsibilities to other types of health care professionals (HCPs), such as nurse practitioners, physician assistants, and pharmacists.1-4
The pharmacist’s role in managing chronic diseases
Pharmacists are a professional group with sufficient education and skills to take a leading role in the primary care of patients with T2DM and other patients with complex needs. Pharmacists are the third-largest group of health professionals in the United States (US).2 The emphasis of professional pharmacy practice has been shifting from a product-oriented, medication-dispensing role, to a patient-centered role, in which the pharmacist provides cognitive services and patient management. Provision of time-consuming primary care for T2DM is made more feasible not only by this growing supply of practicing pharmacists—expected to reach 300,000 by 2020—but also by 2 trends that should increase the availability of their time: the automation of pharmacy practice and the growth of certified pharmacy technicians to a number about equal to that of pharmacists.4
The “pharmaceutical care” philosophy was first articulated 2 decades ago as a call for pharmacists to assume a wider scope of professional responsibility in improving the outcomes of drug therapy, preventing medication-related morbidity and mortality, and improving patients’ quality of life.5 Falling within this paradigm are diabetes self-management education or training (DSME/DSMT), disease management, and collaborative drug therapy management (CDTM), all of which are models that have been applied to pharmacy care in recent decades.6,7 DSME/DSMT programs aim to educate patients on all aspects of diabetes control, including nutrition and exercise, blood glucose control, medication management, and prevention of complications. DSME is taught in an individual or classroom format by certified diabetes educator (CDE) nurses, dietitians, pharmacists, or other professionals. The CDE credential, administered by the National Certification Board of Diabetes Educators, is the national credential for health professionals who provide diabetes patient education and counseling.8
Disease management programs, widely adopted in the 1990s, may be delivered by physicians, pharmacists, or other HCPs or teams. These programs are disease-specific and focus on conditions that require a considerable degree of patient self-management. They provide a wider range of services than just patient education, and may include drug and nondrug therapy. However, they do not usually encompass the needs of patients with multiple chronic illnesses. Some pharmacists are now specializing in management of specific diseases, such as diabetes, and the Board Certified-Advanced Diabetes Management (BC-ADM) credential has been introduced for pharmacists, nurses, and dietitians.9 This credential was originally introduced in 2000, but is currently being reviewed by the American Association of Diabetes Educators. The BC-ADM certifies expertise in patient evaluation and clinical management, as well as patient education. However, because the responsibilities for disease management are often shared among members of a team, pharmacists who provide disease management services may have difficulty obtaining compensation for their contribution.7
CDTM programs consist of partnerships between physicians and pharmacists in which the pharmacist can start, modify, or continue drug therapy for a specific patient according to a written protocol. Protocols may be specific to a single patient or may cover all patients treated by a physician for a specified condition. For example, in a low-risk patient with T2DM, a protocol might specify that the pharmacist can adjust a patient’s insulin dose as long as the glycated hemoglobin (A1C) or blood glucose remains below a certain threshold, but the physician should be contacted if a threshold is exceeded. CDTM programs also may allow pharmacists to take responsibility for ordering tests and providing patient education. Individual state laws have established CDTM legislation, and the activity of pharmacists within CDTM programs is regulated at the state level. The programs are currently available in all but 3 states: Alabama, Oklahoma, and Maine. In most jurisdictions, CTDM agreements are easily established between physicians and regular retail pharmacists, or pharmacists working in a clinic setting.6,10,11 In New York, CDTM was recently assessed for pharmacists practicing in teaching hospitals only.
Medication therapy management (MTM) programs are a further evolution in pharmaceutical patient care. MTM was introduced as part of Medicare legislation in the mid-2000s as a means for pharmacists and other qualified HCPs to improve the care of selected Medicare beneficiaries with multiple chronic illnesses who require multiple medications. MTM services may help address the need to prevent medication-related morbidity and mortality in patients with T2DM and comorbid conditions. Pharmacists can provide continuity of care by following patient progress between physician visits; by utilizing their clinical expertise to monitor and manage diabetes medication plans; and by educating patients on disease, lifestyle, and adherence issues. This level of service can be provided adequately by pharmacists, pharmacist CDEs, and pharmacists with the BC-ADM credential. In addition, many local, state, and national pharmacy organizations and pharmacy schools are providing targeted training for pharmacists wishing to deliver MTM services.12-14
Overview of MTM services
The US Medicare Modernization Act of 2003 established MTM services as part of Medicare Part D—the prescription drug benefit. The Act requires Medicare insurers to provide MTM services to a defined group of beneficiaries expected to benefit from enhanced medication management. Key goals of MTM services are to counsel patients to improve understanding of their medications, to improve medication adherence, and to detect adverse drug reactions and patterns of improper drug use.15 For the first time, the Act created a mechanism for insurers to compensate pharmacists directly for providing these services. To encourage competition and innovation, the exact nature of MTM services and the criteria for patients to qualify were initially left undefined. Basic program requirements and eligibility criteria have since evolved, although the programs are far from standardized. A consortium of 11 national pharmacy organizations developed a consensus definition of MTM programs that identified pharmacists as the key service providers.16 The eligibility criteria for beneficiaries of MTM programs are described in TABLE 1.17 Benefit plans can offer MTM services to patients with any chronic disease or may limit them to selected diseases. Diabetes is the most frequently targeted disease and is covered by virtually all MTM services (FIGURE).17
Pharmacy organizations next developed a guideline that specified 5 core activities of MTM services to be provided in pharmacies (TABLE 2).18 According to this guideline (hereafter referred to as the “Core Elements of MTM”), patients who qualify for MTM services must receive an annual comprehensive medication therapy review, with additional reviews and ongoing pharmacist monitoring as necessary.17,18 Over-the-counter medications, herbal therapies, and dietary supplements should be included in the medication review. Though face-to-face interaction is preferred, and should be required, services may be provided by telephone and may be either by appointment or on a walk-in basis.18 According to the guideline, patients should be provided with a printed or written document, such as a summary of recommendations or an action plan, to take with them. Services may be provided regardless of whether the pharmacist is dispensing medications to the patient. Physician referrals are also not required for pharmacists to offer MTM services to qualifying patients.18 However, although referral by a physician/ HCP is not required for MTM provided by a pharmacist, the physician/HCP does need to be contacted for anything that requires a change in management (eg, changes to treatment). In my practice, I typically write a summary letter to the patient’s physician/HCP; this includes my assessment of the session and any recommendations. Patients are also encouraged to share their personal medication record and action plan with their HCPs. MTM enrollment requirements were revised in 2010 and now require payers to identify target beneficiaries for automatic enrollment.17
TABLE 1
Patient eligibility criteria for MTM programs17
| Multiple chronic diseases |
Programs must offer MTM services to patients who have at least 2 or 3 chronic diseases (at the plan’s discretion) and must target at least 4 of the following:
|
| Multiple covered drugs |
| Plans vary in the number of drugs patients must be prescribed to qualify, with thresholds ranging from 2 to 8. |
| Cost threshold |
| Patients must be expected to incur at least $3000 in annual Part D drug costs. |
| COPD, chronic obstructive pulmonary disease; MTM, medication therapy management. |
FIGURE
The top 10 diseases targeted by MTM programs in 2010 and the percentage of MTM programs that targeted these diseases17
COPD, chronic obstructive pulmonary disease; MTM, medication therapy management.
Reproduced with permission from Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management (MTM) Programs. https://www.cms.gov/PrescriptionDrugCovContra/ Downloads/MTMFactSheet_2010_06-2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.TABLE 2
Core elements of an MTM service model18
| Medication therapy review |
| Systematic review of the patient’s medications to assess and prioritize problems and create a plan to resolve them. |
| Personal medical record |
| Comprehensive record of the patient’s prescription and nonprescription medications, herbal agents, and nutritional supplements. The record is kept and updated by the patient, brought to appointments in different settings, and used by the patient in medication self-management. |
| Medication-related action plan |
| List of actions for the patient to use in self-management. The plan is developed collaboratively by the patient and pharmacist and used to track progress toward achieving specific goals. |
| Intervention and/or referral |
| The pharmacist intervenes or refers the patient to another health professional to address medication-related problems. |
| Documentation and follow-up |
| The pharmacist documents all MTM services and interventions— ideally, electronically. Follow-up or a referral to a different care setting is scheduled based on the patient’s needs. |
| MTM, medication therapy management. |
MTM services in pharmacy practice
MTM services are becoming well established in pharmacy practice. According to an annual survey conducted by the American Pharmacists Association, 72% of pharmacist respondents were offering MTM services in 2009, and about one-third of the rest planned to offer the services soon.19 About 84% of payer respondents (mostly health maintenance organizations, managed care insurers, and prescription benefit management plans) were offering MTM services. Contracted pharmacists provided about two-thirds of MTM care, with in-house pharmacists and contracted MTM organizations providing substantial amounts of services, and nurses and physicians providing a small proportion.19-20 MTM services are not restricted to Medicare patients, but are increasingly being offered by managed care organizations and fee-for-service plans.12,21 Some payers support pharmacist-provided MTM services as part of a broader multidisciplinary disease management program.20
Community pharmacists wishing to offer MTM services have several potential business models. Although they can contract directly with Medicare Part D insurers, it can be difficult and time-consuming to develop these individual contracts. Many insurers are not yet equipped to deal efficiently with pharmacists wishing to initiate this type of arrangement, and insurers are only slowly making the shift toward regarding pharmacists as providers.
A second option is to contract with an MTM intermediary company that links payers with pharmacists. These companies can be approached via their Web sites.12 Their services make it unnecessary for pharmacists to contract with different payers, find patients, or establish new billing systems. The American Society of Consultant Pharmacists offers a program through its Web site (http://www.ascp.org). Known as the MTM Provider Partners Program, it is a pathway for its members to enter the MTM world.
A third option is for pharmacists to provide patients with MTM services and then bill payers—so-called blind billing. Bills for patients covered by Medicare can be submitted using the CMS-1500 form available from the Web site of the Centers for Medicare and Medicaid Services, http://www.cms.gov. Assistance with billing codes is available from the Pharmacist Services Technical Advisory Coalition, http://www.pstac.org. It should be noted that although submission of these claims to various payers is becoming more standardized, there is no guarantee of payment with blind billing. Pharmacists may be reluctant to provide complex, time-consuming MTM services in the absence of such a guarantee. Providing MTM directly to patients in a fee-for-service manner is another option being explored in a few pharmacies.
Inconsistent documentation requirements and reimbursement policies among payers are barriers to community pharmacists’ adoption of MTMs.20 Other barriers to adoption of MTMs, or to their most effective use, include a lack of pharmacists’ time, staffing issues, difficulty forming collaborative relationships with physicians, poor patient mobility and low health literacy, a lack of medical information, and difficulty motivating patients to engage in the programs.15,20-23 It can be challenging to persuade patients of the value of a commitment to time-consuming MTM care, but once they have tried it, many become enthusiastic participants. As the following case study illustrates, use of the various components of the MTM model can help give patients with diabetes and multiple other illnesses a sense of ownership and control.
CASE STUDY Patient with T2DM and multiple comorbidities
A 49-year-old African American woman, who qualifies for Medicare because of disability, first enrolled in our pharmacy’s advertised diabetes education classes 3 years ago, out of concern over her long history of uncontrolled diabetes. At that time, her body mass index (BMI) was 35 kg/m2 and her A1C was 10%. In addition to T2DM, she had asthma, gastroesophageal reflux disease (GERD), hypertension, hyperlipidemia, gout, seasonal allergies, and a prior myocardial infarction.
I have worked closely with this patient over the succeeding 3 years, providing weekly diabetes education and counseling. At first she was using NPH insulin twice a day and adjusting the doses on her own, without the close involvement of her endocrinologist. As long-acting insulin analogs (ie, insulin glargine and insulin detemir) have relatively flat and more predictable time–action profiles that last up to 24 hours,24 I persuaded her to switch to a basal–bolus regimen with insulin detemir and insulin aspart. Insulin detemir is also associated with less weight gain and fewer hypoglycemic episodes than NPH insulin,25-27 which was especially important given this patient’s obesity and fear of hypoglycemia. It is, however, important to note that changes in medication should also be reviewed with the patient’s treating physician. In addition, I spent a year working closely with the patient on carbohydrate counting.
Pharmacists can also explore different insulin delivery methods with patients. Many patients find insulin pens more convenient, more discreet, and easier to use than a vial and syringe.28,29 Insulin pumps can also be a useful option for certain patients.30 Recently, this patient began using an insulin pump, which was recommended to help her achieve better blood glucose control, despite her erratic meal patterns. The results are generally good, although she still has glucose spikes due to metabolic issues and inconsistent eating patterns, and her BMI has increased slightly (36.1 kg/m2). However, her current A1C is 7.1%.
This patient’s complicated medical history and large number of medications (TABLE 3) suggested the need for a comprehensive medication review, as described in the Core Elements of MTM.18 The result of the review was a letter to her physician, with a number of recommendations about her medications, lifestyle changes, and symptoms to investigate. Among the problems discovered were muscle pain and creatine kinase elevation as a possible side effect of her statin therapy; poorly controlled hypertension; poor compliance with some of her medications; the possibility of an interaction between her insulin and beta-blocker; symptoms of congestive heart failure; and signs of possible Cushing’s syndrome. Among the recommended actions were withdrawal of the statin until muscle symptoms could be investigated and modifications of some of her medications to a more easily tolerated form or dosage schedule. Diet, exercise, and weight loss were recommended to ameliorate many of her health problems. Her physician was also advised that she should avoid foods that would exacerbate her GERD and gout and that she should follow the low-salt DASH (Dietary Approaches to Stop Hypertension) diet to help manage her hypertension. It is important to note that, while the pharmacist may make recommendations for symptoms to be investigated, it is the physician who should be making the diagnosis, and pharmacists and physicians should be collaborating as part of a treatment team.
This patient’s fear of hypoglycemia has presented an ongoing challenge in her diabetes education. She often would load up on carbohydrates before leaving work to avoid becoming hypoglycemic on the train ride home. She is extremely insulin resistant, and it has required a major effort to help her feel comfortable with taking enough insulin. She has been very conscientious in documenting the results of her glucose self-monitoring, but has received little education from her physician about what to do with the information. Carbohydrate counting has been difficult for her and continues to be a major focus of our weekly sessions.
The close attention that this patient receives from her pharmacist contrasts with the usual care received by many patients with diabetes. It is not uncommon for patients to tell me that, when they were first diagnosed with T2DM, they were given a prescription and, at best, sent to a dietitian for nutritional counseling. Newly diagnosed patients are advised to monitor their blood glucose; because I see patients once a week, it is easy to help them understand the immediate interactions between diet, exercise, insulin sensitivity, specific medications and doses, and glucose levels.
The medication-related action plan (MAP), one of the Core Elements of MTM,18 is a useful tool to help patients take control of their progress in managing their diabetes. We use it as a medical action plan, involving far more than just medications. These plans are completed at every visit, collaboratively with the patient, and reviewed as follow-up at the next visit. The form contains a space for each planned activity and a space to document progress toward that activity or its completion. Activities might include changing the time of day a medication is taken, going for a lab test, asking the physician to explain cholesterol levels, or observing the emotional states that might lead to binge eating. Holding patients accountable for the activities in the MAP helps them to achieve their self-management goals.
TABLE 3
Case study: Health problems and medications at the time of medication therapy review
| Health problems | Medications | Recommendations |
|---|---|---|
| Type 2 diabetes |
|
|
| Hyperlipidemia |
|
|
| Hypertension (poorly controlled) |
|
|
| Cardiovascular disease |
|
|
| Gout | — |
|
| GERD |
|
|
| Obesity | — |
|
| Seasonal allergies |
|
|
| DASH, Dietary Approaches to Stop Hypertension; GERD, gastroesophageal reflux disease. | ||
Clinical and economic outcomes of MTM
As MTM programs are too diverse to be studied as a group, most outcome studies conducted to date provide data only on specific MTM programs and provide little information about MTMs overall.15 Furthermore, few, if any, studies have examined the effects of MTMs specifically in diabetes. However, numerous publications suggest that pharmacist-provided care can improve clinical outcomes. According to 2 systematic reviews of studies conducted in patients with diabetes, A1C was highly sensitive to a variety of interventions by pharmacists, such as diabetes education and medication management.31,32 In a Veterans Affairs Health Care System, pharmacists’ use of a preplanned insulin initiation and titration protocol resulted in the successful implementation of an insulin initiation clinic through CDTM and improved patients’ glycemic control compared with when the patients were receiving only oral antihyperglycemic agents.33 Two often-cited programs, the Asheville Project34 and the Diabetes Ten City Challenge,35 demonstrated that pharmacist-provided MTM-like care for T2DM resulted in health care cost savings, as well as improved clinical outcomes. However, these results are not directly applicable to MTM services because they were conducted in relatively healthy employee populations. Many studies have examined the overall effects of MTMs on health care costs, but results have been inconsistent, in part because of variation in which costs were included in the analyses.20 It seems inevitable that as the MTM model matures, data will demonstrate the clinical and economic value of pharmacists providing primary care for patients with T2DM and other complex medical conditions.
Conclusions
Pharmacists can help optimize diabetes drug therapy by improving tolerability, reducing risks, and increasing patients’ likelihood of attaining treatment goals. Pharmacist-led diabetes education can go beyond medication and glycemic control to promote overall wellness and a healthy lifestyle. With their involvement in MTM, pharmacists can apply their expertise in drug therapy to a patient population with complex and challenging needs.
1. Biola H, Green LA, Phillips RL, et al. The U.S. primary care physician workforce: minimal growth 1980–1999. Am Fam Physician. 2003;68(8):1483.-
2. Council on Credentialing in Pharmacy. Scope of contemporary pharmacy practice: roles, responsibilities, and functions of pharmacists and pharmacy technicians. J Am Pharm Assoc (2003). 2010;50(2):e35-e69.
3. Drab S. Translating clinical guidelines into clinical practice. Role of the pharmacist in type 2 diabetes management. J Am Pharm Assoc (2003). 2009;49(6):e152-e162.
4. Posey LM, Tanzi MG. Diabetes care: Model for the future of primary care. J Am Pharm Assoc (2003). 2010;50(5):623-626.
5. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533-543.
6. Malloy MJ, DeBellis R. Collaborative drug therapy management, medication treatment management, and Medicare Part D: What do they have in common? Harvard Health Policy Review. 2006;7(1):186-188.
7. McGivney MS, Meyer SM, Duncan-Hewitt W, Hall DL, Goode JV, Smith RB. Medication therapy management: its relationship to patient counseling, disease management, and pharmaceutical care. J Am Pharm Assoc (2003). 2007;47(5):620-628.
8. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2011;34(suppl 1):S89-S96.
9. Daly A, Kulkarni K, Boucher J. The new credential: advanced diabetes management. J Am Diet Assoc. 2001;101(8):940-943.
10. Alliance for Pharmaceutical Care. Collaborative Drug Therapy Management: A Coordinated Approach to Patient Care. http://www.ashp.org/s_ashp/docs/files/about/CDTM.doc. Accessed February 3, 2011.
11. Roberts S, Gainsbrugh R. Medication therapy management and collaborative drug therapy management [letter]. J Managed Care Pharm. 2010;16(1):67-68.
12. Martin CM, McSpadden CS. Dispelling the myths about medication therapy management services. Consult Pharm. 2008;23(11):866-872, 875.
13. American Pharmacists Association. Delivering Medication Therapy Management Services in the Community. http://www.pharmacist.com/ctp/mtm. Published March 1, 2009. Accessed February 1, 2011.
14. American Society of Consultant Pharmacists. Delivering Medication Therapy Management Services in The Community—Updated for 2010. https://www.ascp.com/articles/professional-development/delivering-medication-therapy-management-services-community-update. Accessed February 1, 2011.
15. Pellegrino AN, Martin MT, Tilton JJ, Touchette DR. Medication therapy management services: definitions and outcomes. Drugs. 2009;69(4):393-406.
16. Bluml BM. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc (2003). 2005;45(5):566-572.
17. Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management Programs. https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet_2010_06_2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.
18. American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0). J Am Pharm Assoc (2003). 2008;48(3):341-353.
19. American Pharmacists Association. Medication Therapy Management Digest. Perspectives on 2009: A Year of Changing Opportunities. http://www.pharmacist.com/AM/Template.cfm?Section=Home2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=22674. Published March 2010. Accessed February 1, 2011.
20. Abt Associates. Exploratory Research on Medication Therapy Management. Final report. http://www.cms.hhs.gov/Reports/downloads/blackwell.pdf. Published July 8, 2008. Accessed February 1, 2011.
21. Buffington DE. Future of medication therapy management services in delivering patient-centered care. Am J Health Syst Pharm. 2007;64(15 suppl 10):S10-S12; quiz S21–S23.
22. Law AV, Okamoto MP, Brock K. Ready, willing, and able to provide MTM services?: A survey of community pharmacists in the USA. Res Social Adm Pharm. 2009;5(4):376-381.
23. Lounsbery JL, Green CG, Bennett MS, Pedersen CA. Evaluation of pharmacists’ barriers to the implementation of medication therapy management services. J Am Pharm Assoc (2003). 2009;49(1):51-58.
24. Freeman JS. Insulin analog therapy: improving the match with physiologic insulin secretion. J Am Osteopath Assoc. 2009;109(1):26-36.
25. Davies MJ, Derezinski T, Pedersen CB, Clauson P. Reduced weight gain with insulin detemir compared to NPH insulin is not explained by a reduction in hypoglycemia. Diabetes Technol Ther. 2008;10(4):273-277.
26. Fajardo Montanana C, Hernandez Herrero C, Rivas Fernandez M. Less weight gain and hypoglycaemia with once-daily insulin detemir than NPH insulin in intensification of insulin therapy in overweight Type 2 diabetes patients: the PREDICTIVE BMI clinical trial. Diabet Med. 2008;25(8):916-923.
27. Mandosi E, Fallarino M, Rossetti M, Gatti A, Morano S. Waist circumference reduction after insulin detemir therapy in type 2 diabetes patients previously treated with NPH. Diabetes Res Clin Pract. 2009;84(2):e18-e20.
28. Korytkowski M, Bell D, Jacobsen C, Suwannasari R. A multicenter, randomized, open-label, comparative, two-period crossover trial of preference, efficacy, and safety profiles of a prefilled, disposable pen and conventional vial/syringe for insulin injection in patients with type 1 or 2 diabetes mellitus. Clin Ther. 2003;25(11):2836-2848.
29. Molife C, Lee LJ, Shi L, Sawhney M, Lenox SM. Assessment of patient-reported outcomes of insulin pen devices versus conventional vial and syringe. Diabetes Technol Ther. 2009;11(8):529-538.
30. Jankovec Z, Cechurova D, Krcma M, Lacigova S, Zourek M, Rusavy Z. The influence of insulin pump treatment on metabolic syndrome parameters in type 2 diabetes mellitus. Wien Klin Wochenschr. 2009;121(13-14):459-463.
31. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part I: systematic review and meta analysis in diabetes management. Ann Pharmacother. 2007;41(10):1569-1582.
32. Wubben DP, Vivian EM. Effects of pharmacist outpatient interventions on adults with diabetes mellitus: a systematic review. Pharmacotherapy. 2008;28(4):421-436.
33. Rochester CD, Leon N, Dombrowski R, Haines ST. Collaborative drug therapy management for initiating and adjusting insulin therapy in patients with type 2 diabetes mellitus. Am J Health Syst Pharm. 2010;67(1):42-48.
34. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc (Wash). 2003;43(2):173-184.
35. Fera T, Bluml BM, Ellis WM. Diabetes Ten City Challenge: Final economic and clinical results. J Am Pharm Assoc (2003). 2009;49(3):383-391.
1. Biola H, Green LA, Phillips RL, et al. The U.S. primary care physician workforce: minimal growth 1980–1999. Am Fam Physician. 2003;68(8):1483.-
2. Council on Credentialing in Pharmacy. Scope of contemporary pharmacy practice: roles, responsibilities, and functions of pharmacists and pharmacy technicians. J Am Pharm Assoc (2003). 2010;50(2):e35-e69.
3. Drab S. Translating clinical guidelines into clinical practice. Role of the pharmacist in type 2 diabetes management. J Am Pharm Assoc (2003). 2009;49(6):e152-e162.
4. Posey LM, Tanzi MG. Diabetes care: Model for the future of primary care. J Am Pharm Assoc (2003). 2010;50(5):623-626.
5. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533-543.
6. Malloy MJ, DeBellis R. Collaborative drug therapy management, medication treatment management, and Medicare Part D: What do they have in common? Harvard Health Policy Review. 2006;7(1):186-188.
7. McGivney MS, Meyer SM, Duncan-Hewitt W, Hall DL, Goode JV, Smith RB. Medication therapy management: its relationship to patient counseling, disease management, and pharmaceutical care. J Am Pharm Assoc (2003). 2007;47(5):620-628.
8. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2011;34(suppl 1):S89-S96.
9. Daly A, Kulkarni K, Boucher J. The new credential: advanced diabetes management. J Am Diet Assoc. 2001;101(8):940-943.
10. Alliance for Pharmaceutical Care. Collaborative Drug Therapy Management: A Coordinated Approach to Patient Care. http://www.ashp.org/s_ashp/docs/files/about/CDTM.doc. Accessed February 3, 2011.
11. Roberts S, Gainsbrugh R. Medication therapy management and collaborative drug therapy management [letter]. J Managed Care Pharm. 2010;16(1):67-68.
12. Martin CM, McSpadden CS. Dispelling the myths about medication therapy management services. Consult Pharm. 2008;23(11):866-872, 875.
13. American Pharmacists Association. Delivering Medication Therapy Management Services in the Community. http://www.pharmacist.com/ctp/mtm. Published March 1, 2009. Accessed February 1, 2011.
14. American Society of Consultant Pharmacists. Delivering Medication Therapy Management Services in The Community—Updated for 2010. https://www.ascp.com/articles/professional-development/delivering-medication-therapy-management-services-community-update. Accessed February 1, 2011.
15. Pellegrino AN, Martin MT, Tilton JJ, Touchette DR. Medication therapy management services: definitions and outcomes. Drugs. 2009;69(4):393-406.
16. Bluml BM. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc (2003). 2005;45(5):566-572.
17. Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management Programs. https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet_2010_06_2010_final.pdf. Published June 8, 2010. Accessed February 1, 2011.
18. American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0). J Am Pharm Assoc (2003). 2008;48(3):341-353.
19. American Pharmacists Association. Medication Therapy Management Digest. Perspectives on 2009: A Year of Changing Opportunities. http://www.pharmacist.com/AM/Template.cfm?Section=Home2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=22674. Published March 2010. Accessed February 1, 2011.
20. Abt Associates. Exploratory Research on Medication Therapy Management. Final report. http://www.cms.hhs.gov/Reports/downloads/blackwell.pdf. Published July 8, 2008. Accessed February 1, 2011.
21. Buffington DE. Future of medication therapy management services in delivering patient-centered care. Am J Health Syst Pharm. 2007;64(15 suppl 10):S10-S12; quiz S21–S23.
22. Law AV, Okamoto MP, Brock K. Ready, willing, and able to provide MTM services?: A survey of community pharmacists in the USA. Res Social Adm Pharm. 2009;5(4):376-381.
23. Lounsbery JL, Green CG, Bennett MS, Pedersen CA. Evaluation of pharmacists’ barriers to the implementation of medication therapy management services. J Am Pharm Assoc (2003). 2009;49(1):51-58.
24. Freeman JS. Insulin analog therapy: improving the match with physiologic insulin secretion. J Am Osteopath Assoc. 2009;109(1):26-36.
25. Davies MJ, Derezinski T, Pedersen CB, Clauson P. Reduced weight gain with insulin detemir compared to NPH insulin is not explained by a reduction in hypoglycemia. Diabetes Technol Ther. 2008;10(4):273-277.
26. Fajardo Montanana C, Hernandez Herrero C, Rivas Fernandez M. Less weight gain and hypoglycaemia with once-daily insulin detemir than NPH insulin in intensification of insulin therapy in overweight Type 2 diabetes patients: the PREDICTIVE BMI clinical trial. Diabet Med. 2008;25(8):916-923.
27. Mandosi E, Fallarino M, Rossetti M, Gatti A, Morano S. Waist circumference reduction after insulin detemir therapy in type 2 diabetes patients previously treated with NPH. Diabetes Res Clin Pract. 2009;84(2):e18-e20.
28. Korytkowski M, Bell D, Jacobsen C, Suwannasari R. A multicenter, randomized, open-label, comparative, two-period crossover trial of preference, efficacy, and safety profiles of a prefilled, disposable pen and conventional vial/syringe for insulin injection in patients with type 1 or 2 diabetes mellitus. Clin Ther. 2003;25(11):2836-2848.
29. Molife C, Lee LJ, Shi L, Sawhney M, Lenox SM. Assessment of patient-reported outcomes of insulin pen devices versus conventional vial and syringe. Diabetes Technol Ther. 2009;11(8):529-538.
30. Jankovec Z, Cechurova D, Krcma M, Lacigova S, Zourek M, Rusavy Z. The influence of insulin pump treatment on metabolic syndrome parameters in type 2 diabetes mellitus. Wien Klin Wochenschr. 2009;121(13-14):459-463.
31. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part I: systematic review and meta analysis in diabetes management. Ann Pharmacother. 2007;41(10):1569-1582.
32. Wubben DP, Vivian EM. Effects of pharmacist outpatient interventions on adults with diabetes mellitus: a systematic review. Pharmacotherapy. 2008;28(4):421-436.
33. Rochester CD, Leon N, Dombrowski R, Haines ST. Collaborative drug therapy management for initiating and adjusting insulin therapy in patients with type 2 diabetes mellitus. Am J Health Syst Pharm. 2010;67(1):42-48.
34. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc (Wash). 2003;43(2):173-184.
35. Fera T, Bluml BM, Ellis WM. Diabetes Ten City Challenge: Final economic and clinical results. J Am Pharm Assoc (2003). 2009;49(3):383-391.