User login
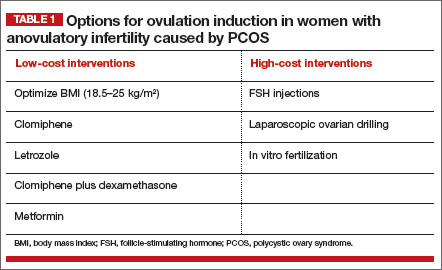
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
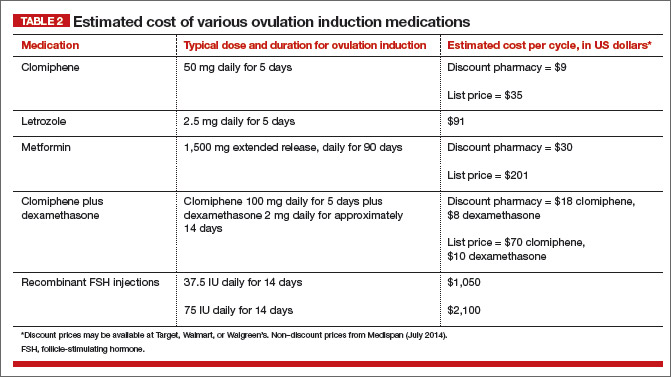
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018