User login
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list

The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions

A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
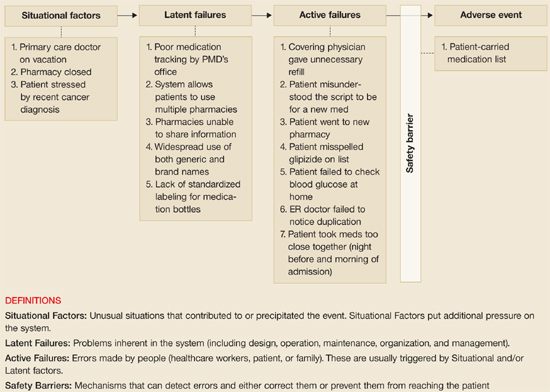
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list
The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions
A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list
The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions
A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu