User login
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
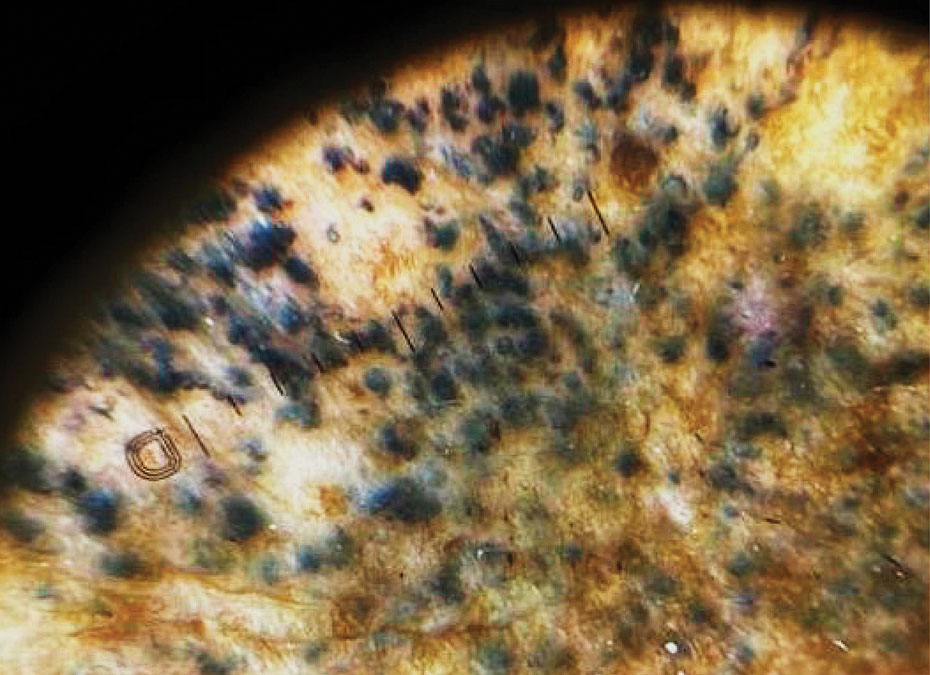
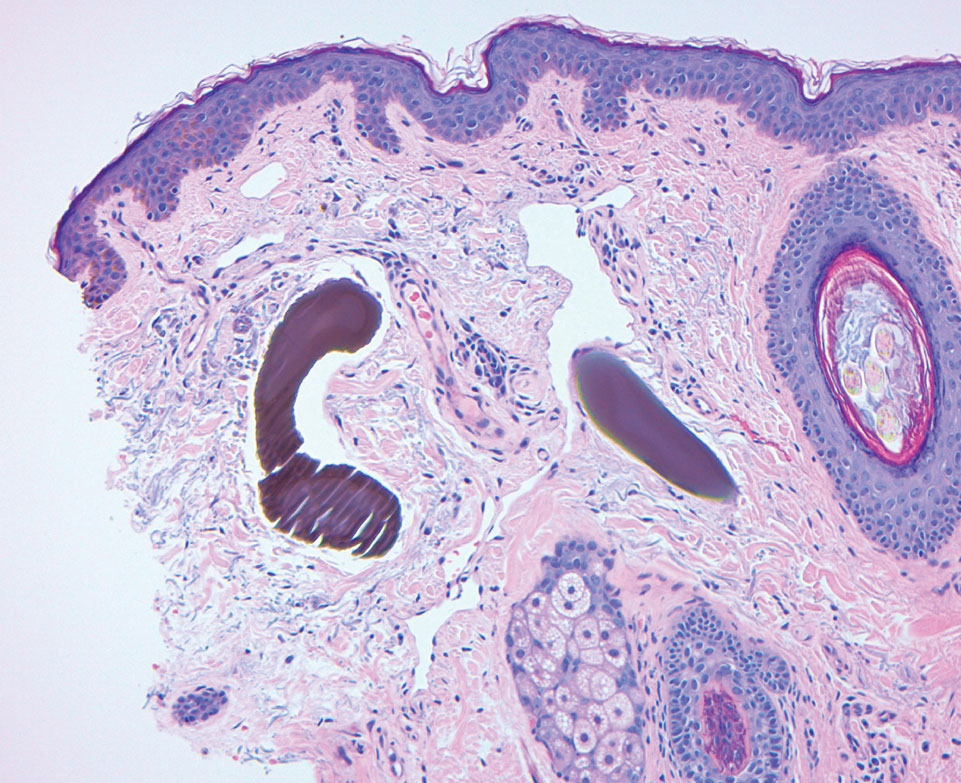
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.

Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Practice Points
- Exogenous ochronosis (EO) is a rare adverse effect of topical hydroquinone characterized by blue-black or gray-blue pigmentation, caviarlike papules, and distinctive banana-shaped dermal deposits on histopathology.
- Most reported cases of hydroquinone-induced EO occur after prolonged use of concentrations exceeding 4%; this case developed after only 6 months of exposure to hydroquinone cream 2% purchased online.
- Available evidence suggests that laser-based therapies may offer greater improvement than topical treatments in affected patients.
