Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
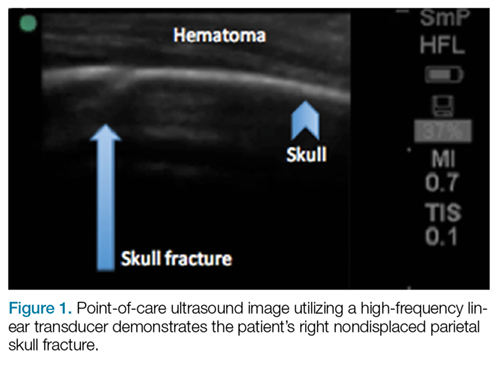
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Figure 1.A POC ultrasound scan performed over the hematoma demonstrated a right nondisplaced parietal skull fracture (Figure 1).
Imaging Technique
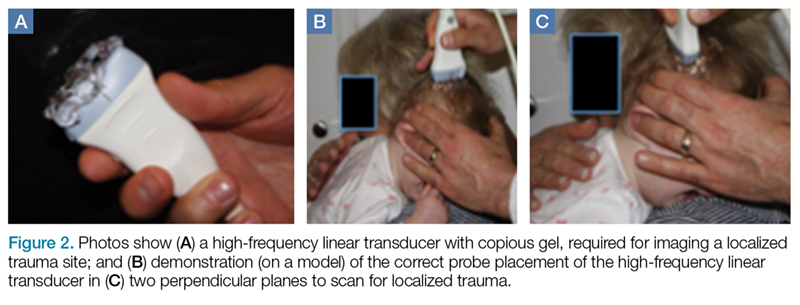
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Figure 2.Skull fracture on ultrasound will appear as a cortical irregularity that is distinguishable from normal skull suture lines. If a cortical disruption is identified, the contralateral side should be scanned to distinguish the fracture from skull suture lines.2 Suture lines can be distinguished from a nondisplaced fracture because suture lines can be followed back to the associated fontanelle.3
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
References
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Figure 1.A POC ultrasound scan performed over the hematoma demonstrated a right nondisplaced parietal skull fracture (Figure 1).
Imaging Technique
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Figure 2.Skull fracture on ultrasound will appear as a cortical irregularity that is distinguishable from normal skull suture lines. If a cortical disruption is identified, the contralateral side should be scanned to distinguish the fracture from skull suture lines.2 Suture lines can be distinguished from a nondisplaced fracture because suture lines can be followed back to the associated fontanelle.3
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Figure 1.A POC ultrasound scan performed over the hematoma demonstrated a right nondisplaced parietal skull fracture (Figure 1).
Imaging Technique
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Figure 2.Skull fracture on ultrasound will appear as a cortical irregularity that is distinguishable from normal skull suture lines. If a cortical disruption is identified, the contralateral side should be scanned to distinguish the fracture from skull suture lines.2 Suture lines can be distinguished from a nondisplaced fracture because suture lines can be followed back to the associated fontanelle.3
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
References
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
References
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
Emergency Ultrasound: Identification of Aortic Dissection Using Limited Bedside Ultrasound
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.