User login
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
PRACTICE POINTS
- Horse flies (Tabanidae) are hematophagous insects that can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers or systemic illness.
- Mild reactions are managed symptomatically; anaphylaxis requires epinephrine, and tularemia requires systemic antibiotics such as gentamicin.
- Patients should be counseled on avoidance strategies, including wearing protective clothing and using topical repellents and environmental traps.

Dome-Shaped White Papules on the Earlobe
Dome-Shaped White Papules on the Earlobe
THE DIAGNOSIS: Trichodiscoma
Histologic evaluation revealed an unremarkable epidermal surface and a subjacent well-demarcated superficial dermal nodule showing a proliferation, sometimes fascicular, of wavy and spindled fibroblasts with some stellate forms within a variably loose fibrous stroma. Some angioplasia and vascular ectasia also were seen (Figure). A diagnosis of trichodiscoma was made based on these histologic findings.
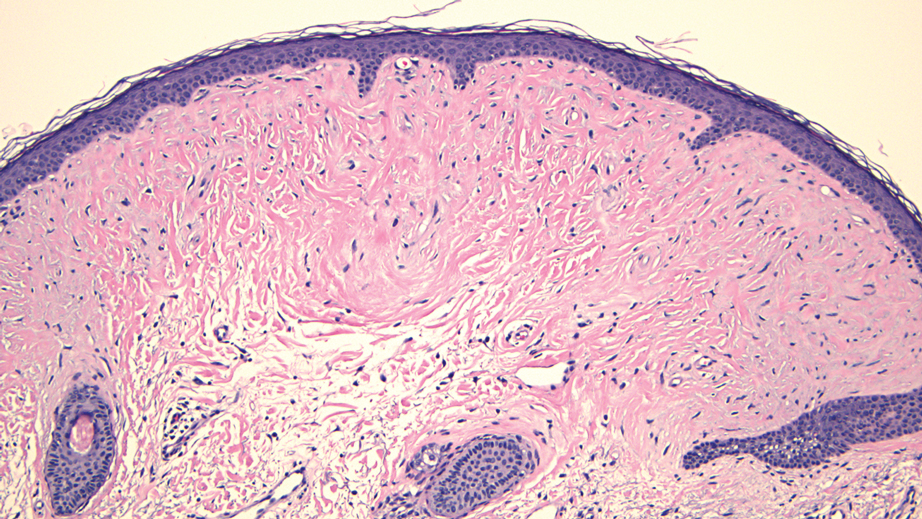
While the patient’s personal and family history of pneumothorax originally had been attributed to other causes, the diagnosis of trichodiscoma raised suspicion for Birt-Hogg-Dubé syndrome due to the classic association of skin lesions (often trichodiscomas), renal cell carcinoma, and spontaneous pneumothorax in this condition. The patient was sent for genetic testing for the associated folliculin (FLCN) gene, which was positive and thereby confirmed the diagnosis of Birt-Hogg-Dubé syndrome. At the most recent follow-up almost 2 years after initial presentation, the lesions on the earlobe were stable. The patient has since undergone screening for abdominal and renal neoplasia with negative results, and he has had no other occurrences of pneumothorax.
Our case highlights the association between trichodiscomas and Birt-Hogg-Dubé syndrome, which necessitates screening for renal cell carcinoma, pneumothorax, and lung cysts.1 Birt-Hogg-Dubé syndrome is an autosomal- dominant disorder of the skin and lungs that is characterized by a predisposition for renal carcinoma, pneumothorax, and colon polyps as well as cutaneous markers that include fibrofolliculomas, acrochordons, and trichodiscomas; the trichodiscomas tend to manifest as numerous smooth, flesh-colored or grayish-white papules on the face, ears, neck, and/or upper trunk.1
Trichodiscomas are benign lesions and do not require treatment2; however, if they are cosmetically bothersome to the patient, surgical excision is an option for single lesions. For more widespread cutaneous disease, combination therapy with a CO2 laser and erbium-doped yttrium aluminum garnet laser may be utilized.3 The differential diagnosis for trichodiscoma includes basal cell carcinoma, fibrous papule, dermal nevus, and trichofolliculoma.
Basal cell carcinoma is the most common type of skin cancer.4 Clinically, it typically manifests as pink or flesh-colored papules on the head or neck, often with overlying ulceration or telangiectasia. Due to its association with chronic sun exposure, the median age of diagnosis for basal cell carcinoma is 68 years. Histopathologically, basal cell carcinoma is characterized by islands or nests of atypical basaloid cells with palisading cells at the periphery.4 Treatment depends on the location and size of the lesion, but Mohs micrographic surgery is the most common intervention on the face and ears.5
In contrast, fibrous papules are benign lesions that manifest clinically as small, firm, flesh-colored papules that most commonly are found on the nose.6,7 On dermatopathology, classic findings include fibrovascular proliferation and scattered multinucleated triangular or stellate cells in the upper dermis.7 Due to the benign nature of the lesion, treatment is not required6; however, shave excision, electrodessication, and laser therapies can be attempted if the patient chooses to pursue treatment.8
Dermal nevus is a type of benign acquired melanocytic nevus that manifests clinically as a light-brown to flesh-colored, dome-shaped or papillomatous papule.9 It typically develops in areas that are exposed to the sun, including the face.10 There also have been cases of dermal nevi on the ear.11 Histopathology shows melanocytic nevus cells that have completely detached from the epidermis and are located entirely in the dermis.12 While dermal nevi are benign and treatment is not necessary, surgical excision is an option for patients who request removal.13
Trichofolliculoma is a benign tumor of the adnexa that shows follicular differentiation on histopathology.14 On physical examination, it manifests as an isolated flesh-colored papule or nodule with a central pore from which tufted hairs protrude. These lesions usually appear on the face or scalp and occur more commonly in women than in men. While these may be clinically indistinguishable from trichodiscomas, the absence of protruding hair in our patient’s case makes trichofolliculoma less likely. When biopsied, histopathology classically shows a cystically dilated hair follicle with keratinous material and several mature and immature branched follicular structures. Preferred treatment for trichofolliculomas is surgical excision, and recurrence is rare.14
- Toro JR, Glenn G, Duray P, et al. Birt-Hogg-Dubé syndrome: a novel marker of kidney neoplasia. Arch Dermatol. 1999;135:1195-202. doi:10.1001/archderm.135.10.1195
- Tong Y, Coda AB, Schneider JA, et al. Familial multiple trichodiscomas: case report and concise review. Cureus. 2017;9:E1596. doi:10.7759/cureus.1596
- Riley J, Athalye L, Tran D, et al. Concomitant fibrofolliculoma and trichodiscoma on the abdomen. Cutis. 2018;102:E30-E32.
- McDaniel B, Badri T, Steele RB. Basal cell carcinoma. StatPearls [Internet]. Updated March 13, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482439/
- Bittner GC, Kubo EM, Fantini BC, et al. Auricular reconstruction after Mohs micrographic surgery: analysis of 101 cases. An Bras Dermatol. 2021;96:408-415. doi:10.1016/j.abd.2020.12.008
- Damman J, Biswas A. Fibrous papule: a histopathologic review. Am J Dermatopathol. 2018;40:551-560. doi:10.1097/DAD.0000000000001083
- Jacyk WK, Rütten A, Requena L. Fibrous papule of the face with granular cells. Dermatology. 2008;216:56-59. doi:10.1159/000109359
- Macri A, Kwan E, Tanner LS. Cutaneous angiofibroma. StatPearls [Internet]. Updated July 19, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482470/
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Conforti C, Giuffrida R, Agozzino M, et al. Basal cell carcinoma and dermal nevi of the face: comparison of localization and dermatoscopic features. Int J Dermatol. 2021;60:996-1002. doi:10.1111/ijd.15554
- Alves RV, Brandão FH, Aquino JE, et al. Intradermal melanocytic nevus of the external auditory canal. Braz J Otorhinolaryngol. 2005;71:104-106. doi: 10.1016/s1808-8694(15)31295-7
- Muradia I, Khunger N, Yadav AK. A clinical, dermoscopic, and histopathological analysis of common acquired melanocytic nevi in skin of color. J Clin Aesthet Dermatol. 2022;15:41-51.
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Massara B, Sellami K, Graja S, et al. Trichofolliculoma: a case series. J Clin Aesthet Dermatol. 2023;16:41-43.
THE DIAGNOSIS: Trichodiscoma
Histologic evaluation revealed an unremarkable epidermal surface and a subjacent well-demarcated superficial dermal nodule showing a proliferation, sometimes fascicular, of wavy and spindled fibroblasts with some stellate forms within a variably loose fibrous stroma. Some angioplasia and vascular ectasia also were seen (Figure). A diagnosis of trichodiscoma was made based on these histologic findings.
While the patient’s personal and family history of pneumothorax originally had been attributed to other causes, the diagnosis of trichodiscoma raised suspicion for Birt-Hogg-Dubé syndrome due to the classic association of skin lesions (often trichodiscomas), renal cell carcinoma, and spontaneous pneumothorax in this condition. The patient was sent for genetic testing for the associated folliculin (FLCN) gene, which was positive and thereby confirmed the diagnosis of Birt-Hogg-Dubé syndrome. At the most recent follow-up almost 2 years after initial presentation, the lesions on the earlobe were stable. The patient has since undergone screening for abdominal and renal neoplasia with negative results, and he has had no other occurrences of pneumothorax.
Our case highlights the association between trichodiscomas and Birt-Hogg-Dubé syndrome, which necessitates screening for renal cell carcinoma, pneumothorax, and lung cysts.1 Birt-Hogg-Dubé syndrome is an autosomal- dominant disorder of the skin and lungs that is characterized by a predisposition for renal carcinoma, pneumothorax, and colon polyps as well as cutaneous markers that include fibrofolliculomas, acrochordons, and trichodiscomas; the trichodiscomas tend to manifest as numerous smooth, flesh-colored or grayish-white papules on the face, ears, neck, and/or upper trunk.1
Trichodiscomas are benign lesions and do not require treatment2; however, if they are cosmetically bothersome to the patient, surgical excision is an option for single lesions. For more widespread cutaneous disease, combination therapy with a CO2 laser and erbium-doped yttrium aluminum garnet laser may be utilized.3 The differential diagnosis for trichodiscoma includes basal cell carcinoma, fibrous papule, dermal nevus, and trichofolliculoma.
Basal cell carcinoma is the most common type of skin cancer.4 Clinically, it typically manifests as pink or flesh-colored papules on the head or neck, often with overlying ulceration or telangiectasia. Due to its association with chronic sun exposure, the median age of diagnosis for basal cell carcinoma is 68 years. Histopathologically, basal cell carcinoma is characterized by islands or nests of atypical basaloid cells with palisading cells at the periphery.4 Treatment depends on the location and size of the lesion, but Mohs micrographic surgery is the most common intervention on the face and ears.5
In contrast, fibrous papules are benign lesions that manifest clinically as small, firm, flesh-colored papules that most commonly are found on the nose.6,7 On dermatopathology, classic findings include fibrovascular proliferation and scattered multinucleated triangular or stellate cells in the upper dermis.7 Due to the benign nature of the lesion, treatment is not required6; however, shave excision, electrodessication, and laser therapies can be attempted if the patient chooses to pursue treatment.8
Dermal nevus is a type of benign acquired melanocytic nevus that manifests clinically as a light-brown to flesh-colored, dome-shaped or papillomatous papule.9 It typically develops in areas that are exposed to the sun, including the face.10 There also have been cases of dermal nevi on the ear.11 Histopathology shows melanocytic nevus cells that have completely detached from the epidermis and are located entirely in the dermis.12 While dermal nevi are benign and treatment is not necessary, surgical excision is an option for patients who request removal.13
Trichofolliculoma is a benign tumor of the adnexa that shows follicular differentiation on histopathology.14 On physical examination, it manifests as an isolated flesh-colored papule or nodule with a central pore from which tufted hairs protrude. These lesions usually appear on the face or scalp and occur more commonly in women than in men. While these may be clinically indistinguishable from trichodiscomas, the absence of protruding hair in our patient’s case makes trichofolliculoma less likely. When biopsied, histopathology classically shows a cystically dilated hair follicle with keratinous material and several mature and immature branched follicular structures. Preferred treatment for trichofolliculomas is surgical excision, and recurrence is rare.14
THE DIAGNOSIS: Trichodiscoma
Histologic evaluation revealed an unremarkable epidermal surface and a subjacent well-demarcated superficial dermal nodule showing a proliferation, sometimes fascicular, of wavy and spindled fibroblasts with some stellate forms within a variably loose fibrous stroma. Some angioplasia and vascular ectasia also were seen (Figure). A diagnosis of trichodiscoma was made based on these histologic findings.
While the patient’s personal and family history of pneumothorax originally had been attributed to other causes, the diagnosis of trichodiscoma raised suspicion for Birt-Hogg-Dubé syndrome due to the classic association of skin lesions (often trichodiscomas), renal cell carcinoma, and spontaneous pneumothorax in this condition. The patient was sent for genetic testing for the associated folliculin (FLCN) gene, which was positive and thereby confirmed the diagnosis of Birt-Hogg-Dubé syndrome. At the most recent follow-up almost 2 years after initial presentation, the lesions on the earlobe were stable. The patient has since undergone screening for abdominal and renal neoplasia with negative results, and he has had no other occurrences of pneumothorax.
Our case highlights the association between trichodiscomas and Birt-Hogg-Dubé syndrome, which necessitates screening for renal cell carcinoma, pneumothorax, and lung cysts.1 Birt-Hogg-Dubé syndrome is an autosomal- dominant disorder of the skin and lungs that is characterized by a predisposition for renal carcinoma, pneumothorax, and colon polyps as well as cutaneous markers that include fibrofolliculomas, acrochordons, and trichodiscomas; the trichodiscomas tend to manifest as numerous smooth, flesh-colored or grayish-white papules on the face, ears, neck, and/or upper trunk.1
Trichodiscomas are benign lesions and do not require treatment2; however, if they are cosmetically bothersome to the patient, surgical excision is an option for single lesions. For more widespread cutaneous disease, combination therapy with a CO2 laser and erbium-doped yttrium aluminum garnet laser may be utilized.3 The differential diagnosis for trichodiscoma includes basal cell carcinoma, fibrous papule, dermal nevus, and trichofolliculoma.
Basal cell carcinoma is the most common type of skin cancer.4 Clinically, it typically manifests as pink or flesh-colored papules on the head or neck, often with overlying ulceration or telangiectasia. Due to its association with chronic sun exposure, the median age of diagnosis for basal cell carcinoma is 68 years. Histopathologically, basal cell carcinoma is characterized by islands or nests of atypical basaloid cells with palisading cells at the periphery.4 Treatment depends on the location and size of the lesion, but Mohs micrographic surgery is the most common intervention on the face and ears.5
In contrast, fibrous papules are benign lesions that manifest clinically as small, firm, flesh-colored papules that most commonly are found on the nose.6,7 On dermatopathology, classic findings include fibrovascular proliferation and scattered multinucleated triangular or stellate cells in the upper dermis.7 Due to the benign nature of the lesion, treatment is not required6; however, shave excision, electrodessication, and laser therapies can be attempted if the patient chooses to pursue treatment.8
Dermal nevus is a type of benign acquired melanocytic nevus that manifests clinically as a light-brown to flesh-colored, dome-shaped or papillomatous papule.9 It typically develops in areas that are exposed to the sun, including the face.10 There also have been cases of dermal nevi on the ear.11 Histopathology shows melanocytic nevus cells that have completely detached from the epidermis and are located entirely in the dermis.12 While dermal nevi are benign and treatment is not necessary, surgical excision is an option for patients who request removal.13
Trichofolliculoma is a benign tumor of the adnexa that shows follicular differentiation on histopathology.14 On physical examination, it manifests as an isolated flesh-colored papule or nodule with a central pore from which tufted hairs protrude. These lesions usually appear on the face or scalp and occur more commonly in women than in men. While these may be clinically indistinguishable from trichodiscomas, the absence of protruding hair in our patient’s case makes trichofolliculoma less likely. When biopsied, histopathology classically shows a cystically dilated hair follicle with keratinous material and several mature and immature branched follicular structures. Preferred treatment for trichofolliculomas is surgical excision, and recurrence is rare.14
- Toro JR, Glenn G, Duray P, et al. Birt-Hogg-Dubé syndrome: a novel marker of kidney neoplasia. Arch Dermatol. 1999;135:1195-202. doi:10.1001/archderm.135.10.1195
- Tong Y, Coda AB, Schneider JA, et al. Familial multiple trichodiscomas: case report and concise review. Cureus. 2017;9:E1596. doi:10.7759/cureus.1596
- Riley J, Athalye L, Tran D, et al. Concomitant fibrofolliculoma and trichodiscoma on the abdomen. Cutis. 2018;102:E30-E32.
- McDaniel B, Badri T, Steele RB. Basal cell carcinoma. StatPearls [Internet]. Updated March 13, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482439/
- Bittner GC, Kubo EM, Fantini BC, et al. Auricular reconstruction after Mohs micrographic surgery: analysis of 101 cases. An Bras Dermatol. 2021;96:408-415. doi:10.1016/j.abd.2020.12.008
- Damman J, Biswas A. Fibrous papule: a histopathologic review. Am J Dermatopathol. 2018;40:551-560. doi:10.1097/DAD.0000000000001083
- Jacyk WK, Rütten A, Requena L. Fibrous papule of the face with granular cells. Dermatology. 2008;216:56-59. doi:10.1159/000109359
- Macri A, Kwan E, Tanner LS. Cutaneous angiofibroma. StatPearls [Internet]. Updated July 19, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482470/
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Conforti C, Giuffrida R, Agozzino M, et al. Basal cell carcinoma and dermal nevi of the face: comparison of localization and dermatoscopic features. Int J Dermatol. 2021;60:996-1002. doi:10.1111/ijd.15554
- Alves RV, Brandão FH, Aquino JE, et al. Intradermal melanocytic nevus of the external auditory canal. Braz J Otorhinolaryngol. 2005;71:104-106. doi: 10.1016/s1808-8694(15)31295-7
- Muradia I, Khunger N, Yadav AK. A clinical, dermoscopic, and histopathological analysis of common acquired melanocytic nevi in skin of color. J Clin Aesthet Dermatol. 2022;15:41-51.
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Massara B, Sellami K, Graja S, et al. Trichofolliculoma: a case series. J Clin Aesthet Dermatol. 2023;16:41-43.
- Toro JR, Glenn G, Duray P, et al. Birt-Hogg-Dubé syndrome: a novel marker of kidney neoplasia. Arch Dermatol. 1999;135:1195-202. doi:10.1001/archderm.135.10.1195
- Tong Y, Coda AB, Schneider JA, et al. Familial multiple trichodiscomas: case report and concise review. Cureus. 2017;9:E1596. doi:10.7759/cureus.1596
- Riley J, Athalye L, Tran D, et al. Concomitant fibrofolliculoma and trichodiscoma on the abdomen. Cutis. 2018;102:E30-E32.
- McDaniel B, Badri T, Steele RB. Basal cell carcinoma. StatPearls [Internet]. Updated March 13, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482439/
- Bittner GC, Kubo EM, Fantini BC, et al. Auricular reconstruction after Mohs micrographic surgery: analysis of 101 cases. An Bras Dermatol. 2021;96:408-415. doi:10.1016/j.abd.2020.12.008
- Damman J, Biswas A. Fibrous papule: a histopathologic review. Am J Dermatopathol. 2018;40:551-560. doi:10.1097/DAD.0000000000001083
- Jacyk WK, Rütten A, Requena L. Fibrous papule of the face with granular cells. Dermatology. 2008;216:56-59. doi:10.1159/000109359
- Macri A, Kwan E, Tanner LS. Cutaneous angiofibroma. StatPearls [Internet]. Updated July 19, 2024. Accessed December 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK482470/
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Conforti C, Giuffrida R, Agozzino M, et al. Basal cell carcinoma and dermal nevi of the face: comparison of localization and dermatoscopic features. Int J Dermatol. 2021;60:996-1002. doi:10.1111/ijd.15554
- Alves RV, Brandão FH, Aquino JE, et al. Intradermal melanocytic nevus of the external auditory canal. Braz J Otorhinolaryngol. 2005;71:104-106. doi: 10.1016/s1808-8694(15)31295-7
- Muradia I, Khunger N, Yadav AK. A clinical, dermoscopic, and histopathological analysis of common acquired melanocytic nevi in skin of color. J Clin Aesthet Dermatol. 2022;15:41-51.
- Sardana K, Chakravarty P, Goel K. Optimal management of common acquired melanocytic nevi (moles): current perspectives. Clin Cosmet Investig Dermatol. 2014;7:89-103. doi:10.2147/CCID.S57782
- Massara B, Sellami K, Graja S, et al. Trichofolliculoma: a case series. J Clin Aesthet Dermatol. 2023;16:41-43.
Dome-Shaped White Papules on the Earlobe
Dome-Shaped White Papules on the Earlobe
A 70-year-old man presented to the dermatology clinic for a routine full-body skin examination that revealed multiple asymptomatic, dome-shaped, white papules on the left posterior earlobe. The patient had a personal and family history of spontaneous pneumothorax and no history of cancer. A shave biopsy of one of the papules was performed.


Oval Brown Plaque on the Palm
The Diagnosis: Poroma
Histopathology showed an endophytic expansion of the epidermis by bland, uniform, basaloid epithelial cells with focal ductal differentiation and an abrupt transition with surrounding epidermal keratinocytes (Figure), consistent with a diagnosis of poroma. The patient elected to monitor the lesion rather than to have it excised.

Eccrine poroma, used interchangeably with the term poroma, is a rare benign adnexal tumor of the eccrine sweat glands resulting from proliferation of the acrosyringium.1,2 It often occurs on the palms or soles, though it also can arise anywhere sweat glands are present.1 Eccrine poromas often appear in middle-aged individuals as singular, well-circumscribed, red-brown papules or nodules.3 A characteristic feature is a shallow, cup-shaped depression within the larger papule or nodule.1
Because the condition is benign and often asymptomatic, it can be safely monitored for progression.1 However, if the lesion is symptomatic or located in a sensitive area, complete excision is curative.4 Eccrine poromas can recur, making close monitoring following excision important.5 The development of bleeding, itching, or pain in a previously asymptomatic lesion may indicate possible malignant transformation, which occurs in only 18% of cases.6
The differential diagnosis includes basal cell carcinoma, circumscribed acral hypokeratosis, Kaposi sarcoma, and pyogenic granuloma. Basal cell carcinoma is the most common type of skin cancer.7 In rare cases it has been shown to present on the palms or soles as a slowgrowing, reddish-pink papule or plaque with central ulceration. It typically is asymptomatic. Histopathology shows dermal nests of basaloid cells with peripheral palisading, stromal mucin, and peritumoral clefts. Treatment is surgical excision.7
Circumscribed acral hypokeratosis presents on the palms or soles as a solitary, shallow, well-defined lesion with a flat base and raised border.8 It often is red-pink in color and most frequently occurs in middle-aged women. Although the cause of the condition is unknown, it is thought to be the result of trauma or human papillomavirus infection.8 Biopsy results characteristically show hypokeratosis demarcated by a sharp and frayed cutoff from uninvolved acral skin with discrete hypogranulosis, dilated blood vessels in the papillary dermis, and slightly thickened collagen fibers in the reticular dermis.9 Surgical excision is a potential treatment option, as topical corticosteroids, retinoids, and calcipotriene have not been shown to be effective; spontaneous resolution has been reported.8
Kaposi sarcoma is a vascular neoplasm that is associated with human herpesvirus 8 infection.10 It typically presents on mucocutaneous sites and the lower extremities. Palmar involvement has been reported in rare cases, occurring as a solitary, well-demarcated, violaceous macule or patch that may be painful.10-12 Characteristic histopathologic features include a proliferation in the dermis of slitlike vascular spaces and spindle cell proliferation.13 Treatment options include cryosurgery; pulsed dye laser; and topical, intralesional, or systemic chemotherapy agents, depending on the stage of the patient’s disease. Antiretroviral therapy is indicated for patients with Kaposi sarcoma secondary to AIDS.14
Pyogenic granuloma presents as a solitary red-brown or bluish-black papule or nodule that bleeds easily when manipulated.15 It commonly occurs following trauma, typically on the fingers, feet, and lips.6 Although benign, potential complications include ulceration and blood loss. Pyogenic granulomas can be treated via curettage and cautery, excision, cryosurgery, or pulsed dye laser.15
- Wankhade V, Singh R, Sadhwani V, et al. Eccrine poroma. Indian Dermatol Online J. 2015;6:304-305.
- Yorulmaz A, Aksoy GG, Ozhamam EU. A growing mass under the nail: subungual eccrine poroma. Skin Appendage Disord. 2020;6:254-257.
- Wang Y, Liu M, Zheng Y, et al. Eccrine poroma presented as spindleshaped plaque: a case report. Medicine (Baltimore). 2021;100:E25971. doi:10.1097/MD.0000000000025971
- Sharma M, Singh M, Gupta K, et al. Eccrine poroma of the eyelid. Indian J Ophthalmol. 2020;68:2522.
- Rasool MN, Hawary MB. Benign eccrine poroma in the palm of the hand. Ann Saudi Med. 2004;24:46-47.
- Sawaya JL, Khachemoune A. Poroma: a review of eccrine, apocrine, and malignant forms [published online April 2, 2014]. Int J Dermatol. 2014;53:1053-1061. doi:10.1111/ijd.12448
- López-Sánchez C, Ferguson P, Collgros H. Basal cell carcinoma of the palm: an unusual presentation of a common tumour [published online August 6, 2019]. Australas J Dermatol. 2020;61:69-70. doi:10.1111/ajd.13129
- Berk DR, Böer A, Bauschard FD, et al. Circumscribed acral hypokeratosis [published online April 6, 2007]. J Am Acad Dermatol. 2007;57:292-296. doi:10.1016/j.jaad.2007.02.022
- Majluf-Cáceres P, Vera-Kellet C, González-Bombardiere S. New dermoscopic keys for circumscribed acral hypokeratosis: report of four cases. Dermatol Pract Concept. 2021;11:E2021010. doi:10.5826/dpc.1102a10
- Simonart T, De Dobbeleer G, Stallenberg B. Classic Kaposi’s sarcoma of the palm in a metallurgist: role of iron filings in its development? Br J Dermatol. 2003;148:1061-1063. doi:10.1046/j.1365-2133.2003.05331.x
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Al Zolibani AA, Al Robaee AA. Primary palmoplantar Kaposi’s sarcoma: an unusual presentation. Skinmed. 2006;5:248-249. doi:10.1111/j.1540-9740.2006.04662.x
- Cesarman E, Damania B, Krown SE, et al. Kaposi sarcoma. Nat Rev Dis Primers. 2019;5:9. doi:10.1038/s41572-019-0060-9
- Etemad SA, Dewan AK. Kaposi sarcoma updates [published online July 10, 2019]. Dermatol Clin. 2019;37:505-517. doi:10.1016/j. det.2019.05.008
- Murthy SC, Nagaraj A. Pyogenic granuloma. Indian Pediatr. 2012;49:855. doi:10.1007/s13312-012-0184-4
The Diagnosis: Poroma
Histopathology showed an endophytic expansion of the epidermis by bland, uniform, basaloid epithelial cells with focal ductal differentiation and an abrupt transition with surrounding epidermal keratinocytes (Figure), consistent with a diagnosis of poroma. The patient elected to monitor the lesion rather than to have it excised.
Eccrine poroma, used interchangeably with the term poroma, is a rare benign adnexal tumor of the eccrine sweat glands resulting from proliferation of the acrosyringium.1,2 It often occurs on the palms or soles, though it also can arise anywhere sweat glands are present.1 Eccrine poromas often appear in middle-aged individuals as singular, well-circumscribed, red-brown papules or nodules.3 A characteristic feature is a shallow, cup-shaped depression within the larger papule or nodule.1
Because the condition is benign and often asymptomatic, it can be safely monitored for progression.1 However, if the lesion is symptomatic or located in a sensitive area, complete excision is curative.4 Eccrine poromas can recur, making close monitoring following excision important.5 The development of bleeding, itching, or pain in a previously asymptomatic lesion may indicate possible malignant transformation, which occurs in only 18% of cases.6
The differential diagnosis includes basal cell carcinoma, circumscribed acral hypokeratosis, Kaposi sarcoma, and pyogenic granuloma. Basal cell carcinoma is the most common type of skin cancer.7 In rare cases it has been shown to present on the palms or soles as a slowgrowing, reddish-pink papule or plaque with central ulceration. It typically is asymptomatic. Histopathology shows dermal nests of basaloid cells with peripheral palisading, stromal mucin, and peritumoral clefts. Treatment is surgical excision.7
Circumscribed acral hypokeratosis presents on the palms or soles as a solitary, shallow, well-defined lesion with a flat base and raised border.8 It often is red-pink in color and most frequently occurs in middle-aged women. Although the cause of the condition is unknown, it is thought to be the result of trauma or human papillomavirus infection.8 Biopsy results characteristically show hypokeratosis demarcated by a sharp and frayed cutoff from uninvolved acral skin with discrete hypogranulosis, dilated blood vessels in the papillary dermis, and slightly thickened collagen fibers in the reticular dermis.9 Surgical excision is a potential treatment option, as topical corticosteroids, retinoids, and calcipotriene have not been shown to be effective; spontaneous resolution has been reported.8
Kaposi sarcoma is a vascular neoplasm that is associated with human herpesvirus 8 infection.10 It typically presents on mucocutaneous sites and the lower extremities. Palmar involvement has been reported in rare cases, occurring as a solitary, well-demarcated, violaceous macule or patch that may be painful.10-12 Characteristic histopathologic features include a proliferation in the dermis of slitlike vascular spaces and spindle cell proliferation.13 Treatment options include cryosurgery; pulsed dye laser; and topical, intralesional, or systemic chemotherapy agents, depending on the stage of the patient’s disease. Antiretroviral therapy is indicated for patients with Kaposi sarcoma secondary to AIDS.14
Pyogenic granuloma presents as a solitary red-brown or bluish-black papule or nodule that bleeds easily when manipulated.15 It commonly occurs following trauma, typically on the fingers, feet, and lips.6 Although benign, potential complications include ulceration and blood loss. Pyogenic granulomas can be treated via curettage and cautery, excision, cryosurgery, or pulsed dye laser.15
The Diagnosis: Poroma
Histopathology showed an endophytic expansion of the epidermis by bland, uniform, basaloid epithelial cells with focal ductal differentiation and an abrupt transition with surrounding epidermal keratinocytes (Figure), consistent with a diagnosis of poroma. The patient elected to monitor the lesion rather than to have it excised.
Eccrine poroma, used interchangeably with the term poroma, is a rare benign adnexal tumor of the eccrine sweat glands resulting from proliferation of the acrosyringium.1,2 It often occurs on the palms or soles, though it also can arise anywhere sweat glands are present.1 Eccrine poromas often appear in middle-aged individuals as singular, well-circumscribed, red-brown papules or nodules.3 A characteristic feature is a shallow, cup-shaped depression within the larger papule or nodule.1
Because the condition is benign and often asymptomatic, it can be safely monitored for progression.1 However, if the lesion is symptomatic or located in a sensitive area, complete excision is curative.4 Eccrine poromas can recur, making close monitoring following excision important.5 The development of bleeding, itching, or pain in a previously asymptomatic lesion may indicate possible malignant transformation, which occurs in only 18% of cases.6
The differential diagnosis includes basal cell carcinoma, circumscribed acral hypokeratosis, Kaposi sarcoma, and pyogenic granuloma. Basal cell carcinoma is the most common type of skin cancer.7 In rare cases it has been shown to present on the palms or soles as a slowgrowing, reddish-pink papule or plaque with central ulceration. It typically is asymptomatic. Histopathology shows dermal nests of basaloid cells with peripheral palisading, stromal mucin, and peritumoral clefts. Treatment is surgical excision.7
Circumscribed acral hypokeratosis presents on the palms or soles as a solitary, shallow, well-defined lesion with a flat base and raised border.8 It often is red-pink in color and most frequently occurs in middle-aged women. Although the cause of the condition is unknown, it is thought to be the result of trauma or human papillomavirus infection.8 Biopsy results characteristically show hypokeratosis demarcated by a sharp and frayed cutoff from uninvolved acral skin with discrete hypogranulosis, dilated blood vessels in the papillary dermis, and slightly thickened collagen fibers in the reticular dermis.9 Surgical excision is a potential treatment option, as topical corticosteroids, retinoids, and calcipotriene have not been shown to be effective; spontaneous resolution has been reported.8
Kaposi sarcoma is a vascular neoplasm that is associated with human herpesvirus 8 infection.10 It typically presents on mucocutaneous sites and the lower extremities. Palmar involvement has been reported in rare cases, occurring as a solitary, well-demarcated, violaceous macule or patch that may be painful.10-12 Characteristic histopathologic features include a proliferation in the dermis of slitlike vascular spaces and spindle cell proliferation.13 Treatment options include cryosurgery; pulsed dye laser; and topical, intralesional, or systemic chemotherapy agents, depending on the stage of the patient’s disease. Antiretroviral therapy is indicated for patients with Kaposi sarcoma secondary to AIDS.14
Pyogenic granuloma presents as a solitary red-brown or bluish-black papule or nodule that bleeds easily when manipulated.15 It commonly occurs following trauma, typically on the fingers, feet, and lips.6 Although benign, potential complications include ulceration and blood loss. Pyogenic granulomas can be treated via curettage and cautery, excision, cryosurgery, or pulsed dye laser.15
- Wankhade V, Singh R, Sadhwani V, et al. Eccrine poroma. Indian Dermatol Online J. 2015;6:304-305.
- Yorulmaz A, Aksoy GG, Ozhamam EU. A growing mass under the nail: subungual eccrine poroma. Skin Appendage Disord. 2020;6:254-257.
- Wang Y, Liu M, Zheng Y, et al. Eccrine poroma presented as spindleshaped plaque: a case report. Medicine (Baltimore). 2021;100:E25971. doi:10.1097/MD.0000000000025971
- Sharma M, Singh M, Gupta K, et al. Eccrine poroma of the eyelid. Indian J Ophthalmol. 2020;68:2522.
- Rasool MN, Hawary MB. Benign eccrine poroma in the palm of the hand. Ann Saudi Med. 2004;24:46-47.
- Sawaya JL, Khachemoune A. Poroma: a review of eccrine, apocrine, and malignant forms [published online April 2, 2014]. Int J Dermatol. 2014;53:1053-1061. doi:10.1111/ijd.12448
- López-Sánchez C, Ferguson P, Collgros H. Basal cell carcinoma of the palm: an unusual presentation of a common tumour [published online August 6, 2019]. Australas J Dermatol. 2020;61:69-70. doi:10.1111/ajd.13129
- Berk DR, Böer A, Bauschard FD, et al. Circumscribed acral hypokeratosis [published online April 6, 2007]. J Am Acad Dermatol. 2007;57:292-296. doi:10.1016/j.jaad.2007.02.022
- Majluf-Cáceres P, Vera-Kellet C, González-Bombardiere S. New dermoscopic keys for circumscribed acral hypokeratosis: report of four cases. Dermatol Pract Concept. 2021;11:E2021010. doi:10.5826/dpc.1102a10
- Simonart T, De Dobbeleer G, Stallenberg B. Classic Kaposi’s sarcoma of the palm in a metallurgist: role of iron filings in its development? Br J Dermatol. 2003;148:1061-1063. doi:10.1046/j.1365-2133.2003.05331.x
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Al Zolibani AA, Al Robaee AA. Primary palmoplantar Kaposi’s sarcoma: an unusual presentation. Skinmed. 2006;5:248-249. doi:10.1111/j.1540-9740.2006.04662.x
- Cesarman E, Damania B, Krown SE, et al. Kaposi sarcoma. Nat Rev Dis Primers. 2019;5:9. doi:10.1038/s41572-019-0060-9
- Etemad SA, Dewan AK. Kaposi sarcoma updates [published online July 10, 2019]. Dermatol Clin. 2019;37:505-517. doi:10.1016/j. det.2019.05.008
- Murthy SC, Nagaraj A. Pyogenic granuloma. Indian Pediatr. 2012;49:855. doi:10.1007/s13312-012-0184-4
- Wankhade V, Singh R, Sadhwani V, et al. Eccrine poroma. Indian Dermatol Online J. 2015;6:304-305.
- Yorulmaz A, Aksoy GG, Ozhamam EU. A growing mass under the nail: subungual eccrine poroma. Skin Appendage Disord. 2020;6:254-257.
- Wang Y, Liu M, Zheng Y, et al. Eccrine poroma presented as spindleshaped plaque: a case report. Medicine (Baltimore). 2021;100:E25971. doi:10.1097/MD.0000000000025971
- Sharma M, Singh M, Gupta K, et al. Eccrine poroma of the eyelid. Indian J Ophthalmol. 2020;68:2522.
- Rasool MN, Hawary MB. Benign eccrine poroma in the palm of the hand. Ann Saudi Med. 2004;24:46-47.
- Sawaya JL, Khachemoune A. Poroma: a review of eccrine, apocrine, and malignant forms [published online April 2, 2014]. Int J Dermatol. 2014;53:1053-1061. doi:10.1111/ijd.12448
- López-Sánchez C, Ferguson P, Collgros H. Basal cell carcinoma of the palm: an unusual presentation of a common tumour [published online August 6, 2019]. Australas J Dermatol. 2020;61:69-70. doi:10.1111/ajd.13129
- Berk DR, Böer A, Bauschard FD, et al. Circumscribed acral hypokeratosis [published online April 6, 2007]. J Am Acad Dermatol. 2007;57:292-296. doi:10.1016/j.jaad.2007.02.022
- Majluf-Cáceres P, Vera-Kellet C, González-Bombardiere S. New dermoscopic keys for circumscribed acral hypokeratosis: report of four cases. Dermatol Pract Concept. 2021;11:E2021010. doi:10.5826/dpc.1102a10
- Simonart T, De Dobbeleer G, Stallenberg B. Classic Kaposi’s sarcoma of the palm in a metallurgist: role of iron filings in its development? Br J Dermatol. 2003;148:1061-1063. doi:10.1046/j.1365-2133.2003.05331.x
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Al Zolibani AA, Al Robaee AA. Primary palmoplantar Kaposi’s sarcoma: an unusual presentation. Skinmed. 2006;5:248-249. doi:10.1111/j.1540-9740.2006.04662.x
- Cesarman E, Damania B, Krown SE, et al. Kaposi sarcoma. Nat Rev Dis Primers. 2019;5:9. doi:10.1038/s41572-019-0060-9
- Etemad SA, Dewan AK. Kaposi sarcoma updates [published online July 10, 2019]. Dermatol Clin. 2019;37:505-517. doi:10.1016/j. det.2019.05.008
- Murthy SC, Nagaraj A. Pyogenic granuloma. Indian Pediatr. 2012;49:855. doi:10.1007/s13312-012-0184-4
A 43-year-old woman presented with a painful lesion on the palm of 30 years’ duration that had grown in size. Physical examination revealed an oval, brown, lobulated plaque with a hyperkeratotic rim on the left palm. She reported bleeding and pain. A shallow cup-shaped depression was noted within the plaque. A 4-mm punch biopsy was performed.

