User login
Commentary: The locum tenens ‘itch’ strikes again
Dec. 1 : Flying north from San Diego to Reno, Nev., along the spine of the Sierra Nevada Mountains, the plane crossed over Lake Tahoe, just before landing in Reno. The mountains surrounding the lake were white. The trees were grey-green; and the lake itself, black, in shadow from the mountains, just before sundown. I looked down upon a California-Nevada chiaroscuro. I was on my way to a locum tenens psychiatric outpatient assignment northwest of Reno, in the eastern foothills of the Sierras, in Timberton, Calif.
Locum tenens is Latin for “holding a place.” Because of staff departures from hospitals, clinics, or private practice, temporary replacement doctors (or nurses or dentists) are needed until permanent staff members can be hired. In essence, a locum tenens is a “rent-a-doc.”

|
Dr. Neal A. Kline |
Landing in Reno, I left the main terminal lobby with its silver sculpture of a downhill skier and picked up my rental car. (For a locum tenens, the plane, the car, lodging, malpractice insurance, and the contracted hourly fee-for-service are included in the locum tenens agency’s monetary province. Not food and not gas.)
Driving north on the interstate, the car skidded a bit on a patch of black ice. Even though the car skidded only “a bit,” still, that was enough to focus my attention. (Oh! That’s what black ice is all about. Slow down, Hopalong!)
My destination was close now, and I pulled off the highway onto Main Street, Timberton.
Two blocks off Main Street was my bed and breakfast: a pale green Victorian house decorated for Christmas with white mini-lights hung as icicles from the porch roof’s eaves. The home was storybook-immaculate; the innkeepers, extraordinarily gracious. Neatness and kindliness count.
Outside, 2 or 3 inches of snow accumulated, and a snow plow “chingled” up the street, pushing the snow aside. For the rest of the evening, no sounds disturbed the winter’s silent night.
The next morning, on route to my worksite, I passed the once-upon-a time Timberton railroad station. Nearby, California Bigleaf Maple trees – their autumn hues so strikingly similar to the color palette of Eastern sugar maples in the fall – were nearly bare. A few leaves – vivid reds and yellows – were hanging on for dear life, trying to maintain the glory of the Crayola-colored fall, just passed. Eventually, however, for the leaves – and all else – time and seasons move on, waiting for no one and no thing.
In days gone by, this railroad depot bustled with passenger traffic. And lines of timber-laden freight cars with both cut logs and milled boards rolled through, supplying lumber for a growing nation. History matters.
At the clinic, my first patient asked, “Will you be my new doctor?” “Will you be here for a short time or a long time?” “ I’ve already had four doctors since I’ve been coming here.”
My night times were filled with reading:
“Of Human Bondage,” by W. Somerset Maugham, the story of a crippled atheistic English lad, attending a London medical school, seeking the meaning of life … and a square meal. [Or is that redundant?]
“Main Street,” by Sinclair Lewis. [Forget about it! My Main Street is way better than Lewis’s! Women here have the right to vote!]
“Moby-Dick,” by Herman Melville, I read cover-to-cover, for drill, to show Melville I could outlast him, no matter how long he went on.
With spring’s arrival, green leaf-buds burst forth on skeletal oak trees, enveloping the branches in a yellow-green glow that became progressively brighter and brighter as the days grew longer and longer still. Lilacs flooded the scene. Little League tryouts were in progress. Baseballs in gloves snapped. Snow clung to the hilltops, while in the valley, short sleeves prevailed. The clinic hummed.
May 1: The end of my locum tenens contract loomed. I told my patients, “This will probably be our last visit before my time at the clinic comes to an end.” Thirty days and counting.
The patients reacted with shock or indifference: shock, with the fear of changing doctors; indifference, as many had been down this road before.
“Who will be my new doctor?” “Will the new doctor be nice?” “I hope the new doctor won’t change my medicines.”
Others accepted a “waiting list” but worriedly so.
Some had me transfer their medications to their primary care physician (PCP), if the PCP would temporarily “watch over” these medications until the new clinic doctor arrived.
And in a just-before-we-stop flourish, one patient and I explored issues of “standing out and fitting in,” emphasizing the “and.” Indeed, three sessions can be a ton of time.
One person summed it up, “Doctors come, and doctors go.”
June 1: Departure day. Farewell, Main Street. Farewell, Timberton.
At the airport, the plane – No. 1 in line for departure, Reno to San Diego – began its take-off roll down the runway. The roll seemed to go on forever, and I apprehensively considered: “Might we run out of runway? Now Giddyup!”
In San Diego for 3 months, the “locum tenens itch” struck me again. A recruiter called at the right time. Four weeks later, I was in the air to Sacramento.
I drove north past fruit orchards, and nut trees, and rice paddies – wet, and filled to the brim. I wondered what the locum tenens fates might have in store for me this time around – the Lady or the Tiger?
Up ahead, train tracks crossed the road. A train horn howled. I braked to a stop ...
Dr. Kline worked for more than 30 years as a staff psychiatrist for San Diego County Mental Health. He also worked for several years as a locum tenens psychiatric physician.
Dec. 1 : Flying north from San Diego to Reno, Nev., along the spine of the Sierra Nevada Mountains, the plane crossed over Lake Tahoe, just before landing in Reno. The mountains surrounding the lake were white. The trees were grey-green; and the lake itself, black, in shadow from the mountains, just before sundown. I looked down upon a California-Nevada chiaroscuro. I was on my way to a locum tenens psychiatric outpatient assignment northwest of Reno, in the eastern foothills of the Sierras, in Timberton, Calif.
Locum tenens is Latin for “holding a place.” Because of staff departures from hospitals, clinics, or private practice, temporary replacement doctors (or nurses or dentists) are needed until permanent staff members can be hired. In essence, a locum tenens is a “rent-a-doc.”
|
|
Dr. Neal A. Kline |
Landing in Reno, I left the main terminal lobby with its silver sculpture of a downhill skier and picked up my rental car. (For a locum tenens, the plane, the car, lodging, malpractice insurance, and the contracted hourly fee-for-service are included in the locum tenens agency’s monetary province. Not food and not gas.)
Driving north on the interstate, the car skidded a bit on a patch of black ice. Even though the car skidded only “a bit,” still, that was enough to focus my attention. (Oh! That’s what black ice is all about. Slow down, Hopalong!)
My destination was close now, and I pulled off the highway onto Main Street, Timberton.
Two blocks off Main Street was my bed and breakfast: a pale green Victorian house decorated for Christmas with white mini-lights hung as icicles from the porch roof’s eaves. The home was storybook-immaculate; the innkeepers, extraordinarily gracious. Neatness and kindliness count.
Outside, 2 or 3 inches of snow accumulated, and a snow plow “chingled” up the street, pushing the snow aside. For the rest of the evening, no sounds disturbed the winter’s silent night.
The next morning, on route to my worksite, I passed the once-upon-a time Timberton railroad station. Nearby, California Bigleaf Maple trees – their autumn hues so strikingly similar to the color palette of Eastern sugar maples in the fall – were nearly bare. A few leaves – vivid reds and yellows – were hanging on for dear life, trying to maintain the glory of the Crayola-colored fall, just passed. Eventually, however, for the leaves – and all else – time and seasons move on, waiting for no one and no thing.
In days gone by, this railroad depot bustled with passenger traffic. And lines of timber-laden freight cars with both cut logs and milled boards rolled through, supplying lumber for a growing nation. History matters.
At the clinic, my first patient asked, “Will you be my new doctor?” “Will you be here for a short time or a long time?” “ I’ve already had four doctors since I’ve been coming here.”
My night times were filled with reading:
“Of Human Bondage,” by W. Somerset Maugham, the story of a crippled atheistic English lad, attending a London medical school, seeking the meaning of life … and a square meal. [Or is that redundant?]
“Main Street,” by Sinclair Lewis. [Forget about it! My Main Street is way better than Lewis’s! Women here have the right to vote!]
“Moby-Dick,” by Herman Melville, I read cover-to-cover, for drill, to show Melville I could outlast him, no matter how long he went on.
With spring’s arrival, green leaf-buds burst forth on skeletal oak trees, enveloping the branches in a yellow-green glow that became progressively brighter and brighter as the days grew longer and longer still. Lilacs flooded the scene. Little League tryouts were in progress. Baseballs in gloves snapped. Snow clung to the hilltops, while in the valley, short sleeves prevailed. The clinic hummed.
May 1: The end of my locum tenens contract loomed. I told my patients, “This will probably be our last visit before my time at the clinic comes to an end.” Thirty days and counting.
The patients reacted with shock or indifference: shock, with the fear of changing doctors; indifference, as many had been down this road before.
“Who will be my new doctor?” “Will the new doctor be nice?” “I hope the new doctor won’t change my medicines.”
Others accepted a “waiting list” but worriedly so.
Some had me transfer their medications to their primary care physician (PCP), if the PCP would temporarily “watch over” these medications until the new clinic doctor arrived.
And in a just-before-we-stop flourish, one patient and I explored issues of “standing out and fitting in,” emphasizing the “and.” Indeed, three sessions can be a ton of time.
One person summed it up, “Doctors come, and doctors go.”
June 1: Departure day. Farewell, Main Street. Farewell, Timberton.
At the airport, the plane – No. 1 in line for departure, Reno to San Diego – began its take-off roll down the runway. The roll seemed to go on forever, and I apprehensively considered: “Might we run out of runway? Now Giddyup!”
In San Diego for 3 months, the “locum tenens itch” struck me again. A recruiter called at the right time. Four weeks later, I was in the air to Sacramento.
I drove north past fruit orchards, and nut trees, and rice paddies – wet, and filled to the brim. I wondered what the locum tenens fates might have in store for me this time around – the Lady or the Tiger?
Up ahead, train tracks crossed the road. A train horn howled. I braked to a stop ...
Dr. Kline worked for more than 30 years as a staff psychiatrist for San Diego County Mental Health. He also worked for several years as a locum tenens psychiatric physician.
Dec. 1 : Flying north from San Diego to Reno, Nev., along the spine of the Sierra Nevada Mountains, the plane crossed over Lake Tahoe, just before landing in Reno. The mountains surrounding the lake were white. The trees were grey-green; and the lake itself, black, in shadow from the mountains, just before sundown. I looked down upon a California-Nevada chiaroscuro. I was on my way to a locum tenens psychiatric outpatient assignment northwest of Reno, in the eastern foothills of the Sierras, in Timberton, Calif.
Locum tenens is Latin for “holding a place.” Because of staff departures from hospitals, clinics, or private practice, temporary replacement doctors (or nurses or dentists) are needed until permanent staff members can be hired. In essence, a locum tenens is a “rent-a-doc.”
|
|
Dr. Neal A. Kline |
Landing in Reno, I left the main terminal lobby with its silver sculpture of a downhill skier and picked up my rental car. (For a locum tenens, the plane, the car, lodging, malpractice insurance, and the contracted hourly fee-for-service are included in the locum tenens agency’s monetary province. Not food and not gas.)
Driving north on the interstate, the car skidded a bit on a patch of black ice. Even though the car skidded only “a bit,” still, that was enough to focus my attention. (Oh! That’s what black ice is all about. Slow down, Hopalong!)
My destination was close now, and I pulled off the highway onto Main Street, Timberton.
Two blocks off Main Street was my bed and breakfast: a pale green Victorian house decorated for Christmas with white mini-lights hung as icicles from the porch roof’s eaves. The home was storybook-immaculate; the innkeepers, extraordinarily gracious. Neatness and kindliness count.
Outside, 2 or 3 inches of snow accumulated, and a snow plow “chingled” up the street, pushing the snow aside. For the rest of the evening, no sounds disturbed the winter’s silent night.
The next morning, on route to my worksite, I passed the once-upon-a time Timberton railroad station. Nearby, California Bigleaf Maple trees – their autumn hues so strikingly similar to the color palette of Eastern sugar maples in the fall – were nearly bare. A few leaves – vivid reds and yellows – were hanging on for dear life, trying to maintain the glory of the Crayola-colored fall, just passed. Eventually, however, for the leaves – and all else – time and seasons move on, waiting for no one and no thing.
In days gone by, this railroad depot bustled with passenger traffic. And lines of timber-laden freight cars with both cut logs and milled boards rolled through, supplying lumber for a growing nation. History matters.
At the clinic, my first patient asked, “Will you be my new doctor?” “Will you be here for a short time or a long time?” “ I’ve already had four doctors since I’ve been coming here.”
My night times were filled with reading:
“Of Human Bondage,” by W. Somerset Maugham, the story of a crippled atheistic English lad, attending a London medical school, seeking the meaning of life … and a square meal. [Or is that redundant?]
“Main Street,” by Sinclair Lewis. [Forget about it! My Main Street is way better than Lewis’s! Women here have the right to vote!]
“Moby-Dick,” by Herman Melville, I read cover-to-cover, for drill, to show Melville I could outlast him, no matter how long he went on.
With spring’s arrival, green leaf-buds burst forth on skeletal oak trees, enveloping the branches in a yellow-green glow that became progressively brighter and brighter as the days grew longer and longer still. Lilacs flooded the scene. Little League tryouts were in progress. Baseballs in gloves snapped. Snow clung to the hilltops, while in the valley, short sleeves prevailed. The clinic hummed.
May 1: The end of my locum tenens contract loomed. I told my patients, “This will probably be our last visit before my time at the clinic comes to an end.” Thirty days and counting.
The patients reacted with shock or indifference: shock, with the fear of changing doctors; indifference, as many had been down this road before.
“Who will be my new doctor?” “Will the new doctor be nice?” “I hope the new doctor won’t change my medicines.”
Others accepted a “waiting list” but worriedly so.
Some had me transfer their medications to their primary care physician (PCP), if the PCP would temporarily “watch over” these medications until the new clinic doctor arrived.
And in a just-before-we-stop flourish, one patient and I explored issues of “standing out and fitting in,” emphasizing the “and.” Indeed, three sessions can be a ton of time.
One person summed it up, “Doctors come, and doctors go.”
June 1: Departure day. Farewell, Main Street. Farewell, Timberton.
At the airport, the plane – No. 1 in line for departure, Reno to San Diego – began its take-off roll down the runway. The roll seemed to go on forever, and I apprehensively considered: “Might we run out of runway? Now Giddyup!”
In San Diego for 3 months, the “locum tenens itch” struck me again. A recruiter called at the right time. Four weeks later, I was in the air to Sacramento.
I drove north past fruit orchards, and nut trees, and rice paddies – wet, and filled to the brim. I wondered what the locum tenens fates might have in store for me this time around – the Lady or the Tiger?
Up ahead, train tracks crossed the road. A train horn howled. I braked to a stop ...
Dr. Kline worked for more than 30 years as a staff psychiatrist for San Diego County Mental Health. He also worked for several years as a locum tenens psychiatric physician.

Understanding the intractability of PTSD
"I am I plus my circumstances."
Flying from Boston to San Diego, next to me was a man in his 40s or 50s. A summer downdraft dropped the floor of the plane precipitously.
“Oh, my,” I said out loud.
“Roger that,” my row mate said.
With the social silence broken, he asked if I were leaving or returning, for business or pleasure, and what I did for a living.
“Physician, psychiatrist. And you?”
“Electrical engineer. I design heads-up displays for fighter-bomber aircraft cockpit simulators. What kind of psychiatry? Medication? Talk?”

“Posttraumatic stress disorder. Inner city. Talk and medication. However, many of the people I see would rather not participate in talking therapy and not take medication, wishing impossibly to return to the life they were living before the traumatic event occurred. Here’s an example: I recently saw a woman in her late 30s. She told me of sitting on her stoop at home with her 14-year-old son. In a drive-by hail of bullets, her son was hit in the head and died at her feet. She was referred to me by her general physician who told her she was depressed. ‘Depressed,’ she repeated. ‘I don’t eat or sleep. I don’t go outdoors if I can avoid it. And I put my hands over my ears if I hear a siren outside. But I don’t want therapy, and I don’t want medication. I want my son back. I want my life to be the way it used to be.’ ”
“Like hysteresis,” the engineer said. “Hysteresis is a scientific term, from the Greek root meaning ‘late’ or ‘lagging behind.’ Hysteresis is about being changed and not being able to reverse the change. It’s being permanently changed by the changing event.”
Tearing out a page from his magazine and folding it in half, he said, “Unfold it.”
I complied.
“But what about the fold line?” he asked. “Can you return the paper to its unfolded state with no evidence of its having been folded? The paper has acquired and retained memory of being folded. There’s a residual line you cannot get rid of.”
Then he drew for me a hysteresis-magnetization graph of an iron particle in a variable electromagnetic field. Starting at the origin (O), where the x-axis/horizontal and the y-axis/vertical intersect, he “pulled” the particle to the right using a hypothetical electromagnetic force, and graphed the rise of the iron particle’s magnetized state by its position on the vertical axis. But the graph was not linear. The iron’s magnetic induction lagged behind the force applied to it.
“It takes time and energy for magnetic molecular rearrangement, for magnetism to get started, so there’s a lag in the saturation curve.
“At the top of the curve, at magnetic saturation, if the magnetizing current is stopped, the curve does not trace itself back to the origin. Rather, it stays flat at the top, lagging, needing time and energy to disaggregate the magnetized molecular domains. Belatedly, the iron speck’s magnetization responds to the lack of current, with reduced magnetization, and follows an independent downward curve, crossing the y axis significantly above the origin, O (Figure 1).
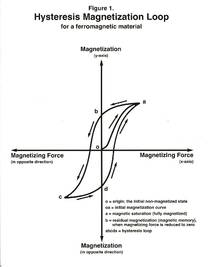
“This is the point of residual magnetization, the partial magnetization that remains from the full current from the past, now turned off – representing the iron’s ‘remembering’ its history.”
As the engineer drew his hysteresis magnetization curves, I looked over his shoulder and reframed, for sport, his terminologies from the upper right quadrant of his graph as follows: his “a,” “fully magnetized,” I changed to “fully traumatized”; “b,” his “residual magnetization” (magnetic memory), I changed to “residual traumatization” (memory of the trauma); and “o,” his “initial nonmagnetized state,” I changed to the “initial nontraumatized state,” to which the person never returns, that is, with no evidence of having been exposed to the traumatizing circumstance. However, his three other magnetization quadrants did not lend themselves to my “traumatic relabeling,” as conceptually there is no “traumatization in the opposite direction” or “traumatizing force in the opposite direction.” Indeed, rape has no antonym.
Our plane continued westward, crossing the Mississippi and the Grand Canyon while my new best friend and I examined one-way events, or entities, that could not be returned to their previous states once significant change had been made, no matter how diligent the efforts at remedy:
Humpty Dumpty…
Death…
Aging…
An insult, given or received…
First impression…
Surprise ending…
Snapped twig…
Popcorn…
Curdled milk…
Nuclear explosion…
Beginning our descent into San Diego, the engineer turned to me, “A hysteretically induced iron particle knows no anguish, just ferromagnetic indifference. An iron particle is mute. It has no objections, no regrets, no despair – no feelings.”
And I replied, “In PTSD from genocide or combat or rape or domestic violence or natural disasters, feelings – such as fear, sadness, and anger – are action-enhanced protections from the perils of life-threatening circumstances. PTSD feelings are survival tactics.”
Touching down and arriving at our gate, my friend and I grabbed our carry-ons and made our way into the terminal crush. He walked with a limp. We all walk with a limp.
Dr. Kline, a former lieutenant commander in the U.S. Navy’s Medical Corps, worked for more than 20 years as medical director of the PTSD Clinical Team at the VA Healthcare System, San Diego; and as a staff psychiatrist, San Diego County Mental Health. He also served as an associate professor of clinical psychiatry at the University of California, San Diego.
"I am I plus my circumstances."
Flying from Boston to San Diego, next to me was a man in his 40s or 50s. A summer downdraft dropped the floor of the plane precipitously.
“Oh, my,” I said out loud.
“Roger that,” my row mate said.
With the social silence broken, he asked if I were leaving or returning, for business or pleasure, and what I did for a living.
“Physician, psychiatrist. And you?”
“Electrical engineer. I design heads-up displays for fighter-bomber aircraft cockpit simulators. What kind of psychiatry? Medication? Talk?”
“Posttraumatic stress disorder. Inner city. Talk and medication. However, many of the people I see would rather not participate in talking therapy and not take medication, wishing impossibly to return to the life they were living before the traumatic event occurred. Here’s an example: I recently saw a woman in her late 30s. She told me of sitting on her stoop at home with her 14-year-old son. In a drive-by hail of bullets, her son was hit in the head and died at her feet. She was referred to me by her general physician who told her she was depressed. ‘Depressed,’ she repeated. ‘I don’t eat or sleep. I don’t go outdoors if I can avoid it. And I put my hands over my ears if I hear a siren outside. But I don’t want therapy, and I don’t want medication. I want my son back. I want my life to be the way it used to be.’ ”
“Like hysteresis,” the engineer said. “Hysteresis is a scientific term, from the Greek root meaning ‘late’ or ‘lagging behind.’ Hysteresis is about being changed and not being able to reverse the change. It’s being permanently changed by the changing event.”
Tearing out a page from his magazine and folding it in half, he said, “Unfold it.”
I complied.
“But what about the fold line?” he asked. “Can you return the paper to its unfolded state with no evidence of its having been folded? The paper has acquired and retained memory of being folded. There’s a residual line you cannot get rid of.”
Then he drew for me a hysteresis-magnetization graph of an iron particle in a variable electromagnetic field. Starting at the origin (O), where the x-axis/horizontal and the y-axis/vertical intersect, he “pulled” the particle to the right using a hypothetical electromagnetic force, and graphed the rise of the iron particle’s magnetized state by its position on the vertical axis. But the graph was not linear. The iron’s magnetic induction lagged behind the force applied to it.
“It takes time and energy for magnetic molecular rearrangement, for magnetism to get started, so there’s a lag in the saturation curve.
“At the top of the curve, at magnetic saturation, if the magnetizing current is stopped, the curve does not trace itself back to the origin. Rather, it stays flat at the top, lagging, needing time and energy to disaggregate the magnetized molecular domains. Belatedly, the iron speck’s magnetization responds to the lack of current, with reduced magnetization, and follows an independent downward curve, crossing the y axis significantly above the origin, O (Figure 1).
“This is the point of residual magnetization, the partial magnetization that remains from the full current from the past, now turned off – representing the iron’s ‘remembering’ its history.”
As the engineer drew his hysteresis magnetization curves, I looked over his shoulder and reframed, for sport, his terminologies from the upper right quadrant of his graph as follows: his “a,” “fully magnetized,” I changed to “fully traumatized”; “b,” his “residual magnetization” (magnetic memory), I changed to “residual traumatization” (memory of the trauma); and “o,” his “initial nonmagnetized state,” I changed to the “initial nontraumatized state,” to which the person never returns, that is, with no evidence of having been exposed to the traumatizing circumstance. However, his three other magnetization quadrants did not lend themselves to my “traumatic relabeling,” as conceptually there is no “traumatization in the opposite direction” or “traumatizing force in the opposite direction.” Indeed, rape has no antonym.
Our plane continued westward, crossing the Mississippi and the Grand Canyon while my new best friend and I examined one-way events, or entities, that could not be returned to their previous states once significant change had been made, no matter how diligent the efforts at remedy:
Humpty Dumpty…
Death…
Aging…
An insult, given or received…
First impression…
Surprise ending…
Snapped twig…
Popcorn…
Curdled milk…
Nuclear explosion…
Beginning our descent into San Diego, the engineer turned to me, “A hysteretically induced iron particle knows no anguish, just ferromagnetic indifference. An iron particle is mute. It has no objections, no regrets, no despair – no feelings.”
And I replied, “In PTSD from genocide or combat or rape or domestic violence or natural disasters, feelings – such as fear, sadness, and anger – are action-enhanced protections from the perils of life-threatening circumstances. PTSD feelings are survival tactics.”
Touching down and arriving at our gate, my friend and I grabbed our carry-ons and made our way into the terminal crush. He walked with a limp. We all walk with a limp.
Dr. Kline, a former lieutenant commander in the U.S. Navy’s Medical Corps, worked for more than 20 years as medical director of the PTSD Clinical Team at the VA Healthcare System, San Diego; and as a staff psychiatrist, San Diego County Mental Health. He also served as an associate professor of clinical psychiatry at the University of California, San Diego.
"I am I plus my circumstances."
Flying from Boston to San Diego, next to me was a man in his 40s or 50s. A summer downdraft dropped the floor of the plane precipitously.
“Oh, my,” I said out loud.
“Roger that,” my row mate said.
With the social silence broken, he asked if I were leaving or returning, for business or pleasure, and what I did for a living.
“Physician, psychiatrist. And you?”
“Electrical engineer. I design heads-up displays for fighter-bomber aircraft cockpit simulators. What kind of psychiatry? Medication? Talk?”
“Posttraumatic stress disorder. Inner city. Talk and medication. However, many of the people I see would rather not participate in talking therapy and not take medication, wishing impossibly to return to the life they were living before the traumatic event occurred. Here’s an example: I recently saw a woman in her late 30s. She told me of sitting on her stoop at home with her 14-year-old son. In a drive-by hail of bullets, her son was hit in the head and died at her feet. She was referred to me by her general physician who told her she was depressed. ‘Depressed,’ she repeated. ‘I don’t eat or sleep. I don’t go outdoors if I can avoid it. And I put my hands over my ears if I hear a siren outside. But I don’t want therapy, and I don’t want medication. I want my son back. I want my life to be the way it used to be.’ ”
“Like hysteresis,” the engineer said. “Hysteresis is a scientific term, from the Greek root meaning ‘late’ or ‘lagging behind.’ Hysteresis is about being changed and not being able to reverse the change. It’s being permanently changed by the changing event.”
Tearing out a page from his magazine and folding it in half, he said, “Unfold it.”
I complied.
“But what about the fold line?” he asked. “Can you return the paper to its unfolded state with no evidence of its having been folded? The paper has acquired and retained memory of being folded. There’s a residual line you cannot get rid of.”
Then he drew for me a hysteresis-magnetization graph of an iron particle in a variable electromagnetic field. Starting at the origin (O), where the x-axis/horizontal and the y-axis/vertical intersect, he “pulled” the particle to the right using a hypothetical electromagnetic force, and graphed the rise of the iron particle’s magnetized state by its position on the vertical axis. But the graph was not linear. The iron’s magnetic induction lagged behind the force applied to it.
“It takes time and energy for magnetic molecular rearrangement, for magnetism to get started, so there’s a lag in the saturation curve.
“At the top of the curve, at magnetic saturation, if the magnetizing current is stopped, the curve does not trace itself back to the origin. Rather, it stays flat at the top, lagging, needing time and energy to disaggregate the magnetized molecular domains. Belatedly, the iron speck’s magnetization responds to the lack of current, with reduced magnetization, and follows an independent downward curve, crossing the y axis significantly above the origin, O (Figure 1).
“This is the point of residual magnetization, the partial magnetization that remains from the full current from the past, now turned off – representing the iron’s ‘remembering’ its history.”
As the engineer drew his hysteresis magnetization curves, I looked over his shoulder and reframed, for sport, his terminologies from the upper right quadrant of his graph as follows: his “a,” “fully magnetized,” I changed to “fully traumatized”; “b,” his “residual magnetization” (magnetic memory), I changed to “residual traumatization” (memory of the trauma); and “o,” his “initial nonmagnetized state,” I changed to the “initial nontraumatized state,” to which the person never returns, that is, with no evidence of having been exposed to the traumatizing circumstance. However, his three other magnetization quadrants did not lend themselves to my “traumatic relabeling,” as conceptually there is no “traumatization in the opposite direction” or “traumatizing force in the opposite direction.” Indeed, rape has no antonym.
Our plane continued westward, crossing the Mississippi and the Grand Canyon while my new best friend and I examined one-way events, or entities, that could not be returned to their previous states once significant change had been made, no matter how diligent the efforts at remedy:
Humpty Dumpty…
Death…
Aging…
An insult, given or received…
First impression…
Surprise ending…
Snapped twig…
Popcorn…
Curdled milk…
Nuclear explosion…
Beginning our descent into San Diego, the engineer turned to me, “A hysteretically induced iron particle knows no anguish, just ferromagnetic indifference. An iron particle is mute. It has no objections, no regrets, no despair – no feelings.”
And I replied, “In PTSD from genocide or combat or rape or domestic violence or natural disasters, feelings – such as fear, sadness, and anger – are action-enhanced protections from the perils of life-threatening circumstances. PTSD feelings are survival tactics.”
Touching down and arriving at our gate, my friend and I grabbed our carry-ons and made our way into the terminal crush. He walked with a limp. We all walk with a limp.
Dr. Kline, a former lieutenant commander in the U.S. Navy’s Medical Corps, worked for more than 20 years as medical director of the PTSD Clinical Team at the VA Healthcare System, San Diego; and as a staff psychiatrist, San Diego County Mental Health. He also served as an associate professor of clinical psychiatry at the University of California, San Diego.
