User login
Melanoma incidence increased in older non-Hispanic whites
reported Dawn M. Holman, MPH, of the division of cancer prevention and control at the Centers for Disease Control and Prevention, and her coauthors.
In non-Hispanic white females aged 15 years and older, 131,976 melanomas were diagnosed between January 2010 and December 2014. In non-Hispanic white males, 192,979 melanomas were diagnosed during this time period. More than 70% of melanomas were diagnosed in patients aged 55 years or older, the authors reported. In females, melanoma incidence rates ranged from 4.5/100,000 population in those aged 15-24 years to 60.9/100,000 population in those aged 85 years and older. For males, melanoma incidence ranged from 2.0/100,000 population in those aged 15-24 years to 198.3/100,000 population in men aged 85 years and older.
Investigators analyzed data from the CDC National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Melanoma incidence rates and average annual counts by 10-year age groups were calculated from January 2010 to December 2014, as was average annual percent change (AAPC) by 10-year age groups from January 2005 to December 2014.
Overall, the increase in melanoma incidence was statistically significant for both males and females 15 years of age and older (AAPC, 1.4; P less than .05). However, melanoma incidence decreased significantly in younger patients aged 15-24 years, 25-34 years, and 35-44 years (AAPC, –5.1, –1.7, and –0.5 respectively; P less than .05), and increased significantly in those aged 55-64 years, 65-74 years, 75-84 years, and older than 85 years (AAPC, 1.3, 2.5, 3.6, and 4.6 respectively; P less than .05). The increase in melanoma incidence was statistically significant in men older than 54 years and in women older than 44 years, Ms. Holman and her associates reported in a research letter in JAMA Dermatology.
The findings suggest that recent decreases in indoor tanning and sunburn prevalence may account for the reduction in melanoma incidence over time, especially in adolescents and young adults, they said.
“Although primary skin cancer prevention efforts have often focused on children, adolescents, and young adults, the steady increase in melanoma incidence rates among older adults indicates a need for efforts that promote skin cancer preventive behaviors throughout adulthood. Such efforts could focus on groups at high risk, such as outdoor workers and intentional tanners,” Ms. Holman and her associates concluded.
The authors did not disclose any conflicts of interest. The study was partially supported by appointments to the CDC Research Participation Program through an interagency agreement with the U.S. Department of Energy.
SOURCE: Holman DM et al. JAMA Dermatol. 2018 Jan 31. doi: 10.1001/jamadermatol.2017.5541.
reported Dawn M. Holman, MPH, of the division of cancer prevention and control at the Centers for Disease Control and Prevention, and her coauthors.
In non-Hispanic white females aged 15 years and older, 131,976 melanomas were diagnosed between January 2010 and December 2014. In non-Hispanic white males, 192,979 melanomas were diagnosed during this time period. More than 70% of melanomas were diagnosed in patients aged 55 years or older, the authors reported. In females, melanoma incidence rates ranged from 4.5/100,000 population in those aged 15-24 years to 60.9/100,000 population in those aged 85 years and older. For males, melanoma incidence ranged from 2.0/100,000 population in those aged 15-24 years to 198.3/100,000 population in men aged 85 years and older.
Investigators analyzed data from the CDC National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Melanoma incidence rates and average annual counts by 10-year age groups were calculated from January 2010 to December 2014, as was average annual percent change (AAPC) by 10-year age groups from January 2005 to December 2014.
Overall, the increase in melanoma incidence was statistically significant for both males and females 15 years of age and older (AAPC, 1.4; P less than .05). However, melanoma incidence decreased significantly in younger patients aged 15-24 years, 25-34 years, and 35-44 years (AAPC, –5.1, –1.7, and –0.5 respectively; P less than .05), and increased significantly in those aged 55-64 years, 65-74 years, 75-84 years, and older than 85 years (AAPC, 1.3, 2.5, 3.6, and 4.6 respectively; P less than .05). The increase in melanoma incidence was statistically significant in men older than 54 years and in women older than 44 years, Ms. Holman and her associates reported in a research letter in JAMA Dermatology.
The findings suggest that recent decreases in indoor tanning and sunburn prevalence may account for the reduction in melanoma incidence over time, especially in adolescents and young adults, they said.
“Although primary skin cancer prevention efforts have often focused on children, adolescents, and young adults, the steady increase in melanoma incidence rates among older adults indicates a need for efforts that promote skin cancer preventive behaviors throughout adulthood. Such efforts could focus on groups at high risk, such as outdoor workers and intentional tanners,” Ms. Holman and her associates concluded.
The authors did not disclose any conflicts of interest. The study was partially supported by appointments to the CDC Research Participation Program through an interagency agreement with the U.S. Department of Energy.
SOURCE: Holman DM et al. JAMA Dermatol. 2018 Jan 31. doi: 10.1001/jamadermatol.2017.5541.
reported Dawn M. Holman, MPH, of the division of cancer prevention and control at the Centers for Disease Control and Prevention, and her coauthors.
In non-Hispanic white females aged 15 years and older, 131,976 melanomas were diagnosed between January 2010 and December 2014. In non-Hispanic white males, 192,979 melanomas were diagnosed during this time period. More than 70% of melanomas were diagnosed in patients aged 55 years or older, the authors reported. In females, melanoma incidence rates ranged from 4.5/100,000 population in those aged 15-24 years to 60.9/100,000 population in those aged 85 years and older. For males, melanoma incidence ranged from 2.0/100,000 population in those aged 15-24 years to 198.3/100,000 population in men aged 85 years and older.
Investigators analyzed data from the CDC National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Melanoma incidence rates and average annual counts by 10-year age groups were calculated from January 2010 to December 2014, as was average annual percent change (AAPC) by 10-year age groups from January 2005 to December 2014.
Overall, the increase in melanoma incidence was statistically significant for both males and females 15 years of age and older (AAPC, 1.4; P less than .05). However, melanoma incidence decreased significantly in younger patients aged 15-24 years, 25-34 years, and 35-44 years (AAPC, –5.1, –1.7, and –0.5 respectively; P less than .05), and increased significantly in those aged 55-64 years, 65-74 years, 75-84 years, and older than 85 years (AAPC, 1.3, 2.5, 3.6, and 4.6 respectively; P less than .05). The increase in melanoma incidence was statistically significant in men older than 54 years and in women older than 44 years, Ms. Holman and her associates reported in a research letter in JAMA Dermatology.
The findings suggest that recent decreases in indoor tanning and sunburn prevalence may account for the reduction in melanoma incidence over time, especially in adolescents and young adults, they said.
“Although primary skin cancer prevention efforts have often focused on children, adolescents, and young adults, the steady increase in melanoma incidence rates among older adults indicates a need for efforts that promote skin cancer preventive behaviors throughout adulthood. Such efforts could focus on groups at high risk, such as outdoor workers and intentional tanners,” Ms. Holman and her associates concluded.
The authors did not disclose any conflicts of interest. The study was partially supported by appointments to the CDC Research Participation Program through an interagency agreement with the U.S. Department of Energy.
SOURCE: Holman DM et al. JAMA Dermatol. 2018 Jan 31. doi: 10.1001/jamadermatol.2017.5541.
FROM JAMA DERMATOLOGY
Key clinical point: Melanoma incidence has increased in older non-Hispanic whites, but decreased in younger members of this population.
Major finding: Overall increase in melanoma incidence was statistically significant for both males and females 15 years of age and older (AAPC = 1.4; P less than .05).
Study details: An analysis of data from the CDC’s National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program from January 2010 to December 2014 (for incidence and rates) and from January 2005 to December 2014 (for trends over time).
Disclosures: The authors did not disclose any conflicts of interest. The study was partially supported by appointments to the CDC Research Participation Program through an interagency agreement with the U.S. Department of Energy.
Source: Holman DM et al. JAMA Dermatol. 2018 Jan 31. doi: 10.1001/jamadermatol.2017.5541.
Women with acne more likely to have hyperkeratinization, study finds
The finding was seen in women with both types of acne – diffuse and mandibular – and in patients with both inflammatory and hyperkeratinization features, wrote Louise M. Guenot, MD, of the dermatology department at CHU Nantes, France, and her coauthors. In the women with mandibular acne, there were significantly more follicle abnormalities on the mandibular area of the face, compared with the forehead area, with no acne lesions.
The investigators evaluated two groups of women: 15 women with diffuse acne lesions across the forehead, cheeks, and chin (mean age 38 years) and 15 women with mandibular acne only (mean age 31 years). Skin that appeared to be acne free among those in the diffuse acne group was compared with the skin of a control group of six women with no acne history. In the mandibular acne group, patients served as their own controls: Healthy forehead skin was compared with mandibular skin. In the diffuse acne group, 791 forehead follicles were evaluated, and in the mandibular group, 569 mandible follicles and 475 forehead follicles were evaluated.
The investigators studied several features, including diameter of the infundibulum, thickness of the border, onion-like appearance, keratin plugs, signs of inflammation, vascularization, and presence of Demodex mites.
In the diffuse acne group, infundibulum was larger, compared with controls (94.9 mcm vs. 74.9 mcm; P = .047). The follicle border was thicker, was more hyperkeratinized, and had more keratin plugs in the infundibulum compared with controls, all statistically significant differences. Signs of inflammation, vascularization, and the presence of Demodex mites did not differ significantly between those with acne and controls.
In the mandibular acne group, where each patient served as her own control, follicles in the mandibular area were larger than those on the forehead (99 mcm vs. 91 mcm, P = .03), and the follicle border in the mandibular area was significantly thicker, with an “onion-like hyperkeratinized appearance” that was significantly more common in the mandibular area. In addition, images showed a keratin plug in the infundibulum was present more often in the follicles in the mandibular area compared with the forehead (46.7% vs. 36.8%, P = .002). Inflammation and vascularization were also significantly more common in the mandibular area compared with the forehead.
Among controls, though, no differences in infundibulum diameter, follicle thickness, or quantity of keratin plugs were seen on the forehead compared with the mandibular area. There was no more onion-like appearance or keratin plugs on the forehead than in the mandibular area, Dr. Guenot and her coauthors reported. Their findings show that “the follicle morphology on apparently healthy skin of adult women with acne was significantly different from that of follicles on the normal skin of healthy subjects.”
The results also “support the concept that the management of acne with mandibular involvement, even if the main clinical lesions are inflammatory, should take into account the hyperkeratinization process, and the treatment should thus be both comedolytic and anti-inflammatory,” they added.
The authors had no financial disclosures, and there was no funding source.
SOURCE: Guenot et al. Int J Dermatol. 2018 Jan 25. doi: 10.1111/ijd.13910.
The finding was seen in women with both types of acne – diffuse and mandibular – and in patients with both inflammatory and hyperkeratinization features, wrote Louise M. Guenot, MD, of the dermatology department at CHU Nantes, France, and her coauthors. In the women with mandibular acne, there were significantly more follicle abnormalities on the mandibular area of the face, compared with the forehead area, with no acne lesions.
The investigators evaluated two groups of women: 15 women with diffuse acne lesions across the forehead, cheeks, and chin (mean age 38 years) and 15 women with mandibular acne only (mean age 31 years). Skin that appeared to be acne free among those in the diffuse acne group was compared with the skin of a control group of six women with no acne history. In the mandibular acne group, patients served as their own controls: Healthy forehead skin was compared with mandibular skin. In the diffuse acne group, 791 forehead follicles were evaluated, and in the mandibular group, 569 mandible follicles and 475 forehead follicles were evaluated.
The investigators studied several features, including diameter of the infundibulum, thickness of the border, onion-like appearance, keratin plugs, signs of inflammation, vascularization, and presence of Demodex mites.
In the diffuse acne group, infundibulum was larger, compared with controls (94.9 mcm vs. 74.9 mcm; P = .047). The follicle border was thicker, was more hyperkeratinized, and had more keratin plugs in the infundibulum compared with controls, all statistically significant differences. Signs of inflammation, vascularization, and the presence of Demodex mites did not differ significantly between those with acne and controls.
In the mandibular acne group, where each patient served as her own control, follicles in the mandibular area were larger than those on the forehead (99 mcm vs. 91 mcm, P = .03), and the follicle border in the mandibular area was significantly thicker, with an “onion-like hyperkeratinized appearance” that was significantly more common in the mandibular area. In addition, images showed a keratin plug in the infundibulum was present more often in the follicles in the mandibular area compared with the forehead (46.7% vs. 36.8%, P = .002). Inflammation and vascularization were also significantly more common in the mandibular area compared with the forehead.
Among controls, though, no differences in infundibulum diameter, follicle thickness, or quantity of keratin plugs were seen on the forehead compared with the mandibular area. There was no more onion-like appearance or keratin plugs on the forehead than in the mandibular area, Dr. Guenot and her coauthors reported. Their findings show that “the follicle morphology on apparently healthy skin of adult women with acne was significantly different from that of follicles on the normal skin of healthy subjects.”
The results also “support the concept that the management of acne with mandibular involvement, even if the main clinical lesions are inflammatory, should take into account the hyperkeratinization process, and the treatment should thus be both comedolytic and anti-inflammatory,” they added.
The authors had no financial disclosures, and there was no funding source.
SOURCE: Guenot et al. Int J Dermatol. 2018 Jan 25. doi: 10.1111/ijd.13910.
The finding was seen in women with both types of acne – diffuse and mandibular – and in patients with both inflammatory and hyperkeratinization features, wrote Louise M. Guenot, MD, of the dermatology department at CHU Nantes, France, and her coauthors. In the women with mandibular acne, there were significantly more follicle abnormalities on the mandibular area of the face, compared with the forehead area, with no acne lesions.
The investigators evaluated two groups of women: 15 women with diffuse acne lesions across the forehead, cheeks, and chin (mean age 38 years) and 15 women with mandibular acne only (mean age 31 years). Skin that appeared to be acne free among those in the diffuse acne group was compared with the skin of a control group of six women with no acne history. In the mandibular acne group, patients served as their own controls: Healthy forehead skin was compared with mandibular skin. In the diffuse acne group, 791 forehead follicles were evaluated, and in the mandibular group, 569 mandible follicles and 475 forehead follicles were evaluated.
The investigators studied several features, including diameter of the infundibulum, thickness of the border, onion-like appearance, keratin plugs, signs of inflammation, vascularization, and presence of Demodex mites.
In the diffuse acne group, infundibulum was larger, compared with controls (94.9 mcm vs. 74.9 mcm; P = .047). The follicle border was thicker, was more hyperkeratinized, and had more keratin plugs in the infundibulum compared with controls, all statistically significant differences. Signs of inflammation, vascularization, and the presence of Demodex mites did not differ significantly between those with acne and controls.
In the mandibular acne group, where each patient served as her own control, follicles in the mandibular area were larger than those on the forehead (99 mcm vs. 91 mcm, P = .03), and the follicle border in the mandibular area was significantly thicker, with an “onion-like hyperkeratinized appearance” that was significantly more common in the mandibular area. In addition, images showed a keratin plug in the infundibulum was present more often in the follicles in the mandibular area compared with the forehead (46.7% vs. 36.8%, P = .002). Inflammation and vascularization were also significantly more common in the mandibular area compared with the forehead.
Among controls, though, no differences in infundibulum diameter, follicle thickness, or quantity of keratin plugs were seen on the forehead compared with the mandibular area. There was no more onion-like appearance or keratin plugs on the forehead than in the mandibular area, Dr. Guenot and her coauthors reported. Their findings show that “the follicle morphology on apparently healthy skin of adult women with acne was significantly different from that of follicles on the normal skin of healthy subjects.”
The results also “support the concept that the management of acne with mandibular involvement, even if the main clinical lesions are inflammatory, should take into account the hyperkeratinization process, and the treatment should thus be both comedolytic and anti-inflammatory,” they added.
The authors had no financial disclosures, and there was no funding source.
SOURCE: Guenot et al. Int J Dermatol. 2018 Jan 25. doi: 10.1111/ijd.13910.
FROM THE INTERNATIONAL JOURNAL OF DERMATOLOGY
Key clinical point: Imaging performed with confocal microscopy showed hyperkeratinization and other abnormalities in healthy-looking skin of acne patients.
Major finding: Follicle abnormalities were significantly more common in the healthy appearing skin of adult women with acne, compared with the skin of controls with no acne.
Data source: A study evaluated skin structures with confocal microscopy in 15 women with diffuse acne and 15 with mandibular acne.
Disclosures: The authors had no financial disclosures, and there was no funding source.
Source: Guenot LM et al. Int J Dermatol. 2018 Jan 25. doi: 10.1111/ijd.13910.
Literature review: Cryolipolysis safe, effective for reducing submental fat
Cryolipolysis is a safe and effective noninvasive treatment for reducing submental fat, according to a review of several published studies.
In a review of four clinical trials and one case series, which involved a total of 101 patients, , reported Shari R. Lipner, MD, of the department of dermatology at Cornell University, New York.
In 2015, the Food and Drug Administration cleared a cryolipolysis device for use in the submental area.
The literature review was performed in May 2017 using Pubmed, EMBASE, Web of Science, and CINAHL databases, searching for the terms cryolipolysis, submental, and paradoxical adipose hyperplasia. Non-English studies were excluded.
The studies included an open-label prospective multicenter trial of 60 patients who underwent cryolipolysis for submental fat reduction once or twice at –10°C for 60 minutes, which found that in 58 evaluable patients, blinded independent reviewers correctly identified baseline photos in 91.4% of cases (P less than .0001). Ultrasound, used to evaluate 57 patients, determined the mean fat layer reduction was 2.0 mm or 20% (ranging from an increase of 2.0 mm to a reduction of –5.9 mm; P less than .0001). Side effects included erythema, edema, bruising, and numbness, which resolved by week 12. Additionally, 83% of the 60 patients were satisfied with the results.
In another study, a prospective nonrandomized study that evaluated overlapping cryolipolysis applications on different visits in 14 patients, pretreatment and post-treatment photographs were correctly identified by blinded independent reviewers 81% of the time (95% confidence interval, 65.9%-91.4%; P = .02). In addition, the mean fat layer reduction, as measured with skin-fold calipers, was 2.3 mm (95% CI, 1.9-2.7 mm; P less than .001), and 93% of the patients were satisfied with the results.
A prospective nonrandomized single-center open-label study of 15 Hispanic patients evaluated cryolipolysis applied to the submental area at two different temperatures (–12°C for 45 minutes and –15°C for 30 minutes) with treatments given 10 weeks apart. The mean reduction in submental fat, as measured by calipers, was 33%, with no significant difference between the two. Blinded physicians correctly identified pre- and post- treatment photos in 60% of cases, and 80% of the patients said they “were satisfied or very satisfied” with the results, according to Dr. Lipner’s review, published online in the Journal of Cosmetic Dermatology.
All studies reported adverse side effects, most commonly erythema, which resolved within weeks of treatment, she wrote. To date, she noted, no cases of mandibular nerve injury or paradoxical adipose hyperplasia have been reported after cryolipolysis for submental fat.
Dr. Lipner referred to early trials in humans found that cryolipolysis was safe and effective for treatment of the back, arms, and chest. Additional trials found no significant changes in lipids or liver function at 1, 4, and 12 weeks’ follow-up when patients were treated for fat in the flanks and lower abdomen.
The results of the literature review suggest that cryolipolysis is safe and effective for submental fat, Dr. Lipner wrote. Appropriate patient selection is important and “patients should be counseled on clinical improvement in the submental contour, number of sessions necessary, side effects, downtime, and cost,” she noted. Liposuction is still the gold standard for removal of large fat deposits, and although cryolipolysis can reduce submental fat, “it may also worsen the appearance on the neck by making platysmal banding or skin imperfections more obvious,” she added.
Dr. Lipner did not report any relevant disclosures. No funding source was provided.
SOURCE: J Cosmet Dermatol. 2018 Jan 17. doi: 10.1111/jocd.12495.
Cryolipolysis is a safe and effective noninvasive treatment for reducing submental fat, according to a review of several published studies.
In a review of four clinical trials and one case series, which involved a total of 101 patients, , reported Shari R. Lipner, MD, of the department of dermatology at Cornell University, New York.
In 2015, the Food and Drug Administration cleared a cryolipolysis device for use in the submental area.
The literature review was performed in May 2017 using Pubmed, EMBASE, Web of Science, and CINAHL databases, searching for the terms cryolipolysis, submental, and paradoxical adipose hyperplasia. Non-English studies were excluded.
The studies included an open-label prospective multicenter trial of 60 patients who underwent cryolipolysis for submental fat reduction once or twice at –10°C for 60 minutes, which found that in 58 evaluable patients, blinded independent reviewers correctly identified baseline photos in 91.4% of cases (P less than .0001). Ultrasound, used to evaluate 57 patients, determined the mean fat layer reduction was 2.0 mm or 20% (ranging from an increase of 2.0 mm to a reduction of –5.9 mm; P less than .0001). Side effects included erythema, edema, bruising, and numbness, which resolved by week 12. Additionally, 83% of the 60 patients were satisfied with the results.
In another study, a prospective nonrandomized study that evaluated overlapping cryolipolysis applications on different visits in 14 patients, pretreatment and post-treatment photographs were correctly identified by blinded independent reviewers 81% of the time (95% confidence interval, 65.9%-91.4%; P = .02). In addition, the mean fat layer reduction, as measured with skin-fold calipers, was 2.3 mm (95% CI, 1.9-2.7 mm; P less than .001), and 93% of the patients were satisfied with the results.
A prospective nonrandomized single-center open-label study of 15 Hispanic patients evaluated cryolipolysis applied to the submental area at two different temperatures (–12°C for 45 minutes and –15°C for 30 minutes) with treatments given 10 weeks apart. The mean reduction in submental fat, as measured by calipers, was 33%, with no significant difference between the two. Blinded physicians correctly identified pre- and post- treatment photos in 60% of cases, and 80% of the patients said they “were satisfied or very satisfied” with the results, according to Dr. Lipner’s review, published online in the Journal of Cosmetic Dermatology.
All studies reported adverse side effects, most commonly erythema, which resolved within weeks of treatment, she wrote. To date, she noted, no cases of mandibular nerve injury or paradoxical adipose hyperplasia have been reported after cryolipolysis for submental fat.
Dr. Lipner referred to early trials in humans found that cryolipolysis was safe and effective for treatment of the back, arms, and chest. Additional trials found no significant changes in lipids or liver function at 1, 4, and 12 weeks’ follow-up when patients were treated for fat in the flanks and lower abdomen.
The results of the literature review suggest that cryolipolysis is safe and effective for submental fat, Dr. Lipner wrote. Appropriate patient selection is important and “patients should be counseled on clinical improvement in the submental contour, number of sessions necessary, side effects, downtime, and cost,” she noted. Liposuction is still the gold standard for removal of large fat deposits, and although cryolipolysis can reduce submental fat, “it may also worsen the appearance on the neck by making platysmal banding or skin imperfections more obvious,” she added.
Dr. Lipner did not report any relevant disclosures. No funding source was provided.
SOURCE: J Cosmet Dermatol. 2018 Jan 17. doi: 10.1111/jocd.12495.
Cryolipolysis is a safe and effective noninvasive treatment for reducing submental fat, according to a review of several published studies.
In a review of four clinical trials and one case series, which involved a total of 101 patients, , reported Shari R. Lipner, MD, of the department of dermatology at Cornell University, New York.
In 2015, the Food and Drug Administration cleared a cryolipolysis device for use in the submental area.
The literature review was performed in May 2017 using Pubmed, EMBASE, Web of Science, and CINAHL databases, searching for the terms cryolipolysis, submental, and paradoxical adipose hyperplasia. Non-English studies were excluded.
The studies included an open-label prospective multicenter trial of 60 patients who underwent cryolipolysis for submental fat reduction once or twice at –10°C for 60 minutes, which found that in 58 evaluable patients, blinded independent reviewers correctly identified baseline photos in 91.4% of cases (P less than .0001). Ultrasound, used to evaluate 57 patients, determined the mean fat layer reduction was 2.0 mm or 20% (ranging from an increase of 2.0 mm to a reduction of –5.9 mm; P less than .0001). Side effects included erythema, edema, bruising, and numbness, which resolved by week 12. Additionally, 83% of the 60 patients were satisfied with the results.
In another study, a prospective nonrandomized study that evaluated overlapping cryolipolysis applications on different visits in 14 patients, pretreatment and post-treatment photographs were correctly identified by blinded independent reviewers 81% of the time (95% confidence interval, 65.9%-91.4%; P = .02). In addition, the mean fat layer reduction, as measured with skin-fold calipers, was 2.3 mm (95% CI, 1.9-2.7 mm; P less than .001), and 93% of the patients were satisfied with the results.
A prospective nonrandomized single-center open-label study of 15 Hispanic patients evaluated cryolipolysis applied to the submental area at two different temperatures (–12°C for 45 minutes and –15°C for 30 minutes) with treatments given 10 weeks apart. The mean reduction in submental fat, as measured by calipers, was 33%, with no significant difference between the two. Blinded physicians correctly identified pre- and post- treatment photos in 60% of cases, and 80% of the patients said they “were satisfied or very satisfied” with the results, according to Dr. Lipner’s review, published online in the Journal of Cosmetic Dermatology.
All studies reported adverse side effects, most commonly erythema, which resolved within weeks of treatment, she wrote. To date, she noted, no cases of mandibular nerve injury or paradoxical adipose hyperplasia have been reported after cryolipolysis for submental fat.
Dr. Lipner referred to early trials in humans found that cryolipolysis was safe and effective for treatment of the back, arms, and chest. Additional trials found no significant changes in lipids or liver function at 1, 4, and 12 weeks’ follow-up when patients were treated for fat in the flanks and lower abdomen.
The results of the literature review suggest that cryolipolysis is safe and effective for submental fat, Dr. Lipner wrote. Appropriate patient selection is important and “patients should be counseled on clinical improvement in the submental contour, number of sessions necessary, side effects, downtime, and cost,” she noted. Liposuction is still the gold standard for removal of large fat deposits, and although cryolipolysis can reduce submental fat, “it may also worsen the appearance on the neck by making platysmal banding or skin imperfections more obvious,” she added.
Dr. Lipner did not report any relevant disclosures. No funding source was provided.
SOURCE: J Cosmet Dermatol. 2018 Jan 17. doi: 10.1111/jocd.12495.
FROM THE JOURNAL OF COSMETIC DERMATOLOGY
Key clinical point: Cryolipolysis appears to be a safe, effective noninvasive treatment for submental fat.
Major finding: Endpoints evaluating the effects of the cooling technique on submental fat included evaluations of blinded patient photos by blinded reviewers, who, in one study, correctly identified baseline photos in 91.4% of cases (P less than .0001).
Data source: A literature review of four clinical trials and one case series of a total of 101 patients who underwent cryolipolysis for reducing submental fat.
Disclosures: The author did not report any relevant disclosures. No funding source was provided.
Source: Cosmet Dermatol. 2018 Jan 17. doi: 10.1111/jocd.12495.
AAD guidelines favor surgery for nonmelanoma skin cancers
, according to new practice guidelines issued by the American Academy of Dermatology.
Nonsurgical approaches such as cryotherapy, photodynamic therapy, and radiation may be considered for low-risk cancers if surgery is contraindicated, but these methods have lower cure rates, according to the guidelines. Christopher K. Bichakjian, MD, professor of dermatology, University of Michigan, Ann Arbor, and Murad Alam, MD, professor of dermatology, Northwestern University, Chicago, cochaired the work groups that developed the guidelines.

The guidelines for BCC and cSCC, published online in two separate papers (J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.006; J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.007), also discuss biopsy techniques, tumor staging, and prevention of recurrence of nonmelanoma skin cancers.
The most suitable stratification for localized BCC and cSCC is the framework provided by the National Comprehensive Cancer Network, the authors said in the guidelines.
For suspected BCC and cSCC, recommended biopsy techniques are punch biopsy, shave biopsy, and excisional biopsy. Biopsy technique is “contingent on the clinical characteristics of the suspected tumor, including morphology, expected histologic subtype and depth, natural history, and anatomic location; patient-specific factors, such as bleeding and wound healing diatheses; and patient preference and physician judgment,” the guidelines state. If the initial biopsy proves insufficient for diagnosis, a repeat biopsy may be considered.
For surgical treatment of BCC, curettage and electrodessication may be considered for low-risk tumors in nonterminal hair-bearing locations. Surgical excision with 4-mm clinical margins and histologic margin assessment is recommended for low-risk primary BCC. For high-risk BCC, Mohs micrographic surgery is recommended, the authors said.
Surgical options for cSCC also include curettage and electrodessication and standard excision for low-risk disease, and Mohs micrographic surgery for high-risk cSCC. In both BCC and cSCC, standard excision may be considered for high-risk tumors in some cases, but “strong caution is advised when selecting a treatment modality” for high-risk tumors “without complete margin assessment,” the guidelines state.

Nonsurgical therapies are generally not recommended as first-line treatment, especially in cSCC because of possible recurrence and metastasis. In cases where nonsurgical therapies are preferred, options may include cryosurgery, topical therapy, photodynamic therapy, radiation, or laser therapy, “with the understanding that the cure rate may be lower,” the authors wrote.
Patients with diagnosed nonmelanoma skin cancer should continue to undergo screening for new primary skin cancers (including BCC, cSCC, and melanoma) at least once per year, the guideline states. They should also be counseled on sun protection, tanning bed avoidance, and regular use of broad-spectrum sunscreen.
Although the new guidelines mainly “reaffirm common knowledge and current practice,” they offer a reminder of “alternative therapeutic or preventive options when insufficient evidence is available to support new therapies or previously dogmatic practice patterns,” the authors said.
These are the first guidelines of care for BCC and cSCC published by the AAD. Commonly used guidelines for the management of BCC and cSCC are published by the National Comprehensive Cancer Network, which are frequently referenced throughout the new AAD guidelines, Dr. Bichakjian said in an interview. While the aim of the cancer network is to develop multidisciplinary guidelines, reflected by the composition of the panel members, “AAD guidelines of care are established primarily by dermatologists for dermatologists,” he pointed out. “However, the work group recognizes that a variety of health care providers outside of dermatology take care of patients with BCC and cSCC, and acknowledges the importance of multidisciplinary care,” he added. “With these considerations in mind, reviewers from specialties outside of dermatology, including plastic surgery, otolaryngology/head and neck surgery, medical oncology, radiation oncology, and family medicine, were invited to critically review the current guidelines.”

The guidelines do not cover the management of actinic keratosis and cSCC in situ, he said. “The work group acknowledges the importance of appropriate management of premalignant and in situ lesions in the prevention of their potential progression to cSCC. However, additional data to provide comprehensive evidence-based recommendations were deemed too extensive to include in the current guidelines and will need to addressed separately.”
In an interview, David J. Leffell, MD, who was not an author of the guidelines, said that the new guidelines do an effective job of “highlighting where valid outcomes data exist and areas where they do not” for a wide range of therapies. They also “attempt to standardize approaches to diagnosis and care of nonmelanoma skin cancer and in general are consistent with established practice patterns,” he added. “Those contemporary approaches have developed in largely empirical fashion over many decades, but bear clarification and reinforcement,” said Dr. Leffell, professor of dermatology and surgery and chief of the section of dermatologic surgery and cutaneous oncology at Yale University, New Haven, Conn.
The guidelines “thoroughly summarize evidence-based recommendations for the entire spectrum of disease management,” Daniel D. Bennett, MD, of the department of dermatology at the University of Wisconsin – Madison, said in an interview. “While surgery remains the mainstay of treatment for BCC and cutaneous SCC, these guidelines include excellent reviews of nonsurgical management options,” he said.
Dr. Bichakjian, who is also chief of the division of cutaneous surgery and oncology at the University of Michigan, had no relevant financial disclosures to report. Dr. Alam, who is also chief of cutaneous and aesthetic surgery in the department of dermatology at Northwestern, disclosed relationships with Amway, OptMed, and 3M. Dr. Bennett and Dr. Leffell had no relevant disclosures.
, according to new practice guidelines issued by the American Academy of Dermatology.
Nonsurgical approaches such as cryotherapy, photodynamic therapy, and radiation may be considered for low-risk cancers if surgery is contraindicated, but these methods have lower cure rates, according to the guidelines. Christopher K. Bichakjian, MD, professor of dermatology, University of Michigan, Ann Arbor, and Murad Alam, MD, professor of dermatology, Northwestern University, Chicago, cochaired the work groups that developed the guidelines.
The guidelines for BCC and cSCC, published online in two separate papers (J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.006; J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.007), also discuss biopsy techniques, tumor staging, and prevention of recurrence of nonmelanoma skin cancers.
The most suitable stratification for localized BCC and cSCC is the framework provided by the National Comprehensive Cancer Network, the authors said in the guidelines.
For suspected BCC and cSCC, recommended biopsy techniques are punch biopsy, shave biopsy, and excisional biopsy. Biopsy technique is “contingent on the clinical characteristics of the suspected tumor, including morphology, expected histologic subtype and depth, natural history, and anatomic location; patient-specific factors, such as bleeding and wound healing diatheses; and patient preference and physician judgment,” the guidelines state. If the initial biopsy proves insufficient for diagnosis, a repeat biopsy may be considered.
For surgical treatment of BCC, curettage and electrodessication may be considered for low-risk tumors in nonterminal hair-bearing locations. Surgical excision with 4-mm clinical margins and histologic margin assessment is recommended for low-risk primary BCC. For high-risk BCC, Mohs micrographic surgery is recommended, the authors said.
Surgical options for cSCC also include curettage and electrodessication and standard excision for low-risk disease, and Mohs micrographic surgery for high-risk cSCC. In both BCC and cSCC, standard excision may be considered for high-risk tumors in some cases, but “strong caution is advised when selecting a treatment modality” for high-risk tumors “without complete margin assessment,” the guidelines state.
Nonsurgical therapies are generally not recommended as first-line treatment, especially in cSCC because of possible recurrence and metastasis. In cases where nonsurgical therapies are preferred, options may include cryosurgery, topical therapy, photodynamic therapy, radiation, or laser therapy, “with the understanding that the cure rate may be lower,” the authors wrote.
Patients with diagnosed nonmelanoma skin cancer should continue to undergo screening for new primary skin cancers (including BCC, cSCC, and melanoma) at least once per year, the guideline states. They should also be counseled on sun protection, tanning bed avoidance, and regular use of broad-spectrum sunscreen.
Although the new guidelines mainly “reaffirm common knowledge and current practice,” they offer a reminder of “alternative therapeutic or preventive options when insufficient evidence is available to support new therapies or previously dogmatic practice patterns,” the authors said.
These are the first guidelines of care for BCC and cSCC published by the AAD. Commonly used guidelines for the management of BCC and cSCC are published by the National Comprehensive Cancer Network, which are frequently referenced throughout the new AAD guidelines, Dr. Bichakjian said in an interview. While the aim of the cancer network is to develop multidisciplinary guidelines, reflected by the composition of the panel members, “AAD guidelines of care are established primarily by dermatologists for dermatologists,” he pointed out. “However, the work group recognizes that a variety of health care providers outside of dermatology take care of patients with BCC and cSCC, and acknowledges the importance of multidisciplinary care,” he added. “With these considerations in mind, reviewers from specialties outside of dermatology, including plastic surgery, otolaryngology/head and neck surgery, medical oncology, radiation oncology, and family medicine, were invited to critically review the current guidelines.”
The guidelines do not cover the management of actinic keratosis and cSCC in situ, he said. “The work group acknowledges the importance of appropriate management of premalignant and in situ lesions in the prevention of their potential progression to cSCC. However, additional data to provide comprehensive evidence-based recommendations were deemed too extensive to include in the current guidelines and will need to addressed separately.”
In an interview, David J. Leffell, MD, who was not an author of the guidelines, said that the new guidelines do an effective job of “highlighting where valid outcomes data exist and areas where they do not” for a wide range of therapies. They also “attempt to standardize approaches to diagnosis and care of nonmelanoma skin cancer and in general are consistent with established practice patterns,” he added. “Those contemporary approaches have developed in largely empirical fashion over many decades, but bear clarification and reinforcement,” said Dr. Leffell, professor of dermatology and surgery and chief of the section of dermatologic surgery and cutaneous oncology at Yale University, New Haven, Conn.
The guidelines “thoroughly summarize evidence-based recommendations for the entire spectrum of disease management,” Daniel D. Bennett, MD, of the department of dermatology at the University of Wisconsin – Madison, said in an interview. “While surgery remains the mainstay of treatment for BCC and cutaneous SCC, these guidelines include excellent reviews of nonsurgical management options,” he said.
Dr. Bichakjian, who is also chief of the division of cutaneous surgery and oncology at the University of Michigan, had no relevant financial disclosures to report. Dr. Alam, who is also chief of cutaneous and aesthetic surgery in the department of dermatology at Northwestern, disclosed relationships with Amway, OptMed, and 3M. Dr. Bennett and Dr. Leffell had no relevant disclosures.
, according to new practice guidelines issued by the American Academy of Dermatology.
Nonsurgical approaches such as cryotherapy, photodynamic therapy, and radiation may be considered for low-risk cancers if surgery is contraindicated, but these methods have lower cure rates, according to the guidelines. Christopher K. Bichakjian, MD, professor of dermatology, University of Michigan, Ann Arbor, and Murad Alam, MD, professor of dermatology, Northwestern University, Chicago, cochaired the work groups that developed the guidelines.
The guidelines for BCC and cSCC, published online in two separate papers (J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.006; J Am Acad Dermatol. 2018 Jan. 10. doi: 10.1016/j.jaad.2017.10.007), also discuss biopsy techniques, tumor staging, and prevention of recurrence of nonmelanoma skin cancers.
The most suitable stratification for localized BCC and cSCC is the framework provided by the National Comprehensive Cancer Network, the authors said in the guidelines.
For suspected BCC and cSCC, recommended biopsy techniques are punch biopsy, shave biopsy, and excisional biopsy. Biopsy technique is “contingent on the clinical characteristics of the suspected tumor, including morphology, expected histologic subtype and depth, natural history, and anatomic location; patient-specific factors, such as bleeding and wound healing diatheses; and patient preference and physician judgment,” the guidelines state. If the initial biopsy proves insufficient for diagnosis, a repeat biopsy may be considered.
For surgical treatment of BCC, curettage and electrodessication may be considered for low-risk tumors in nonterminal hair-bearing locations. Surgical excision with 4-mm clinical margins and histologic margin assessment is recommended for low-risk primary BCC. For high-risk BCC, Mohs micrographic surgery is recommended, the authors said.
Surgical options for cSCC also include curettage and electrodessication and standard excision for low-risk disease, and Mohs micrographic surgery for high-risk cSCC. In both BCC and cSCC, standard excision may be considered for high-risk tumors in some cases, but “strong caution is advised when selecting a treatment modality” for high-risk tumors “without complete margin assessment,” the guidelines state.
Nonsurgical therapies are generally not recommended as first-line treatment, especially in cSCC because of possible recurrence and metastasis. In cases where nonsurgical therapies are preferred, options may include cryosurgery, topical therapy, photodynamic therapy, radiation, or laser therapy, “with the understanding that the cure rate may be lower,” the authors wrote.
Patients with diagnosed nonmelanoma skin cancer should continue to undergo screening for new primary skin cancers (including BCC, cSCC, and melanoma) at least once per year, the guideline states. They should also be counseled on sun protection, tanning bed avoidance, and regular use of broad-spectrum sunscreen.
Although the new guidelines mainly “reaffirm common knowledge and current practice,” they offer a reminder of “alternative therapeutic or preventive options when insufficient evidence is available to support new therapies or previously dogmatic practice patterns,” the authors said.
These are the first guidelines of care for BCC and cSCC published by the AAD. Commonly used guidelines for the management of BCC and cSCC are published by the National Comprehensive Cancer Network, which are frequently referenced throughout the new AAD guidelines, Dr. Bichakjian said in an interview. While the aim of the cancer network is to develop multidisciplinary guidelines, reflected by the composition of the panel members, “AAD guidelines of care are established primarily by dermatologists for dermatologists,” he pointed out. “However, the work group recognizes that a variety of health care providers outside of dermatology take care of patients with BCC and cSCC, and acknowledges the importance of multidisciplinary care,” he added. “With these considerations in mind, reviewers from specialties outside of dermatology, including plastic surgery, otolaryngology/head and neck surgery, medical oncology, radiation oncology, and family medicine, were invited to critically review the current guidelines.”
The guidelines do not cover the management of actinic keratosis and cSCC in situ, he said. “The work group acknowledges the importance of appropriate management of premalignant and in situ lesions in the prevention of their potential progression to cSCC. However, additional data to provide comprehensive evidence-based recommendations were deemed too extensive to include in the current guidelines and will need to addressed separately.”
In an interview, David J. Leffell, MD, who was not an author of the guidelines, said that the new guidelines do an effective job of “highlighting where valid outcomes data exist and areas where they do not” for a wide range of therapies. They also “attempt to standardize approaches to diagnosis and care of nonmelanoma skin cancer and in general are consistent with established practice patterns,” he added. “Those contemporary approaches have developed in largely empirical fashion over many decades, but bear clarification and reinforcement,” said Dr. Leffell, professor of dermatology and surgery and chief of the section of dermatologic surgery and cutaneous oncology at Yale University, New Haven, Conn.
The guidelines “thoroughly summarize evidence-based recommendations for the entire spectrum of disease management,” Daniel D. Bennett, MD, of the department of dermatology at the University of Wisconsin – Madison, said in an interview. “While surgery remains the mainstay of treatment for BCC and cutaneous SCC, these guidelines include excellent reviews of nonsurgical management options,” he said.
Dr. Bichakjian, who is also chief of the division of cutaneous surgery and oncology at the University of Michigan, had no relevant financial disclosures to report. Dr. Alam, who is also chief of cutaneous and aesthetic surgery in the department of dermatology at Northwestern, disclosed relationships with Amway, OptMed, and 3M. Dr. Bennett and Dr. Leffell had no relevant disclosures.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Gastric bypass T2D benefit can fade over time
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
FROM JAMA
Key clinical point: Adding gastric bypass surgery to lifestyle and medical management improves diabetes outcomes – but with diminished effect over time.
Major finding: Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group.
Data source: A randomized study of 113 patients at four sites in the United States and Taiwan with a HbA1c level of 8% or higher and a BMI of 30-39.9 kg/m2.
Disclosures: Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics
SOURCE: Ikramuddin S et al. JAMA. 2018;319(3):266-278.
APA guideline backs naltrexone, acamprosate for alcohol use disorder
Naltrexone or acamprosate should be offered as first-line pharmacologic therapy to patients with moderate to severe alcohol use disorder (AUD) who do not respond to nonpharmacologic therapy alone, according to a practice guideline published by the American Psychiatric Association.
if naltrexone and acamprosate are not effective or well tolerated, the report said.
The APA guideline recommends against the use of antidepressants and benzodiazepines for patients with alcohol use disorder, except for situations where a co-occurring disorder requires treatment. In addition, the guideline recommends against the use of acamprosate in patients with renal impairment, and specifies that naltrexone should not be used by patients with acute hepatitis, hepatic failure, or opioid dependence.
“Naltrexone and acamprosate have the best available evidence as pharmacotherapy for patients with AUD,” wrote Victor I. Reus, MD, and his coauthors in the APA Guideline Writing Group, which formed the guideline using a systematic review of current literature in accordance with Institute of Medicine (now called the National Academy of Medicine) and Agency for Healthcare Research and Quality standards.
Naltrexone, an opioid receptor antagonist, is effective in treating both AUD and opioid use disorder. Studies have shown that it may decrease cravings, and is associated with fewer drinking days and a reduced likelihood of return to drinking, the authors reported. In patients with a history of renal impairment, serum creatinine should be measured, and results should be reviewed before initiating treatment with acamprosate – a synthetic amino acid.
Disulfiram breaks down acetaldehyde, an ethanol byproduct, and should be used only to treat patients with a goal of abstinence. It is not recommended as a first-line therapy because of the side effects of concurrent alcohol use, including tachycardia, flushing, headache, nausea, and vomiting, reported Dr. Reus of the psychiatry department at the University of California, San Francisco, and his coauthors.
“Patients should be fully informed of the physiological consequences of consuming alcohol while taking disulfiram and should agree to taking the medication,” the authors wrote. “They should be instructed to abstain from drinking alcohol for at least 12 hours before taking a dose of the medication and be advised that reactions with alcohol can occur up to 14 days after taking disulfiram.”
Lastly, topiramate and gabapentin may be used in patients for whom naltrexone and acamprosate are ineffective, though topiramate may have side effects of concern to the patient, including cognitive dysfunction and numbness, tingling, paresthesias, dizziness, taste abnormalities, and decreased appetite or weight loss, the report said.
Although the APA guideline acknowledges the importance of psychiatric evaluation and nonpharmacologic treatments such as cognitive-behavioral therapy and 12-step programs, it does not provide recommendations on those treatment options.
Further research on alcohol use disorder should include study of quantitative measures for longitudinal monitoring, co-occurring medical and psychiatric conditions, and the effectiveness of naltrexone versus combination therapy for patients with both AUD and opioid use disorder, the authors said.
“The overall goal of this guideline is to enhance the treatment of AUD for millions of affected individuals, thereby reducing the significant psychosocial and public health consequences of this important psychiatric condition,” the report concluded. An executive summary of the guideline was published in the American Journal of Psychiatry.
The guideline authors disclosed no conflicts of interest with their work on the guideline.
SOURCE: Reus VI et al. Am J Psychiatry. 2018;175:86-90.
Naltrexone or acamprosate should be offered as first-line pharmacologic therapy to patients with moderate to severe alcohol use disorder (AUD) who do not respond to nonpharmacologic therapy alone, according to a practice guideline published by the American Psychiatric Association.
if naltrexone and acamprosate are not effective or well tolerated, the report said.
The APA guideline recommends against the use of antidepressants and benzodiazepines for patients with alcohol use disorder, except for situations where a co-occurring disorder requires treatment. In addition, the guideline recommends against the use of acamprosate in patients with renal impairment, and specifies that naltrexone should not be used by patients with acute hepatitis, hepatic failure, or opioid dependence.
“Naltrexone and acamprosate have the best available evidence as pharmacotherapy for patients with AUD,” wrote Victor I. Reus, MD, and his coauthors in the APA Guideline Writing Group, which formed the guideline using a systematic review of current literature in accordance with Institute of Medicine (now called the National Academy of Medicine) and Agency for Healthcare Research and Quality standards.
Naltrexone, an opioid receptor antagonist, is effective in treating both AUD and opioid use disorder. Studies have shown that it may decrease cravings, and is associated with fewer drinking days and a reduced likelihood of return to drinking, the authors reported. In patients with a history of renal impairment, serum creatinine should be measured, and results should be reviewed before initiating treatment with acamprosate – a synthetic amino acid.
Disulfiram breaks down acetaldehyde, an ethanol byproduct, and should be used only to treat patients with a goal of abstinence. It is not recommended as a first-line therapy because of the side effects of concurrent alcohol use, including tachycardia, flushing, headache, nausea, and vomiting, reported Dr. Reus of the psychiatry department at the University of California, San Francisco, and his coauthors.
“Patients should be fully informed of the physiological consequences of consuming alcohol while taking disulfiram and should agree to taking the medication,” the authors wrote. “They should be instructed to abstain from drinking alcohol for at least 12 hours before taking a dose of the medication and be advised that reactions with alcohol can occur up to 14 days after taking disulfiram.”
Lastly, topiramate and gabapentin may be used in patients for whom naltrexone and acamprosate are ineffective, though topiramate may have side effects of concern to the patient, including cognitive dysfunction and numbness, tingling, paresthesias, dizziness, taste abnormalities, and decreased appetite or weight loss, the report said.
Although the APA guideline acknowledges the importance of psychiatric evaluation and nonpharmacologic treatments such as cognitive-behavioral therapy and 12-step programs, it does not provide recommendations on those treatment options.
Further research on alcohol use disorder should include study of quantitative measures for longitudinal monitoring, co-occurring medical and psychiatric conditions, and the effectiveness of naltrexone versus combination therapy for patients with both AUD and opioid use disorder, the authors said.
“The overall goal of this guideline is to enhance the treatment of AUD for millions of affected individuals, thereby reducing the significant psychosocial and public health consequences of this important psychiatric condition,” the report concluded. An executive summary of the guideline was published in the American Journal of Psychiatry.
The guideline authors disclosed no conflicts of interest with their work on the guideline.
SOURCE: Reus VI et al. Am J Psychiatry. 2018;175:86-90.
Naltrexone or acamprosate should be offered as first-line pharmacologic therapy to patients with moderate to severe alcohol use disorder (AUD) who do not respond to nonpharmacologic therapy alone, according to a practice guideline published by the American Psychiatric Association.
if naltrexone and acamprosate are not effective or well tolerated, the report said.
The APA guideline recommends against the use of antidepressants and benzodiazepines for patients with alcohol use disorder, except for situations where a co-occurring disorder requires treatment. In addition, the guideline recommends against the use of acamprosate in patients with renal impairment, and specifies that naltrexone should not be used by patients with acute hepatitis, hepatic failure, or opioid dependence.
“Naltrexone and acamprosate have the best available evidence as pharmacotherapy for patients with AUD,” wrote Victor I. Reus, MD, and his coauthors in the APA Guideline Writing Group, which formed the guideline using a systematic review of current literature in accordance with Institute of Medicine (now called the National Academy of Medicine) and Agency for Healthcare Research and Quality standards.
Naltrexone, an opioid receptor antagonist, is effective in treating both AUD and opioid use disorder. Studies have shown that it may decrease cravings, and is associated with fewer drinking days and a reduced likelihood of return to drinking, the authors reported. In patients with a history of renal impairment, serum creatinine should be measured, and results should be reviewed before initiating treatment with acamprosate – a synthetic amino acid.
Disulfiram breaks down acetaldehyde, an ethanol byproduct, and should be used only to treat patients with a goal of abstinence. It is not recommended as a first-line therapy because of the side effects of concurrent alcohol use, including tachycardia, flushing, headache, nausea, and vomiting, reported Dr. Reus of the psychiatry department at the University of California, San Francisco, and his coauthors.
“Patients should be fully informed of the physiological consequences of consuming alcohol while taking disulfiram and should agree to taking the medication,” the authors wrote. “They should be instructed to abstain from drinking alcohol for at least 12 hours before taking a dose of the medication and be advised that reactions with alcohol can occur up to 14 days after taking disulfiram.”
Lastly, topiramate and gabapentin may be used in patients for whom naltrexone and acamprosate are ineffective, though topiramate may have side effects of concern to the patient, including cognitive dysfunction and numbness, tingling, paresthesias, dizziness, taste abnormalities, and decreased appetite or weight loss, the report said.
Although the APA guideline acknowledges the importance of psychiatric evaluation and nonpharmacologic treatments such as cognitive-behavioral therapy and 12-step programs, it does not provide recommendations on those treatment options.
Further research on alcohol use disorder should include study of quantitative measures for longitudinal monitoring, co-occurring medical and psychiatric conditions, and the effectiveness of naltrexone versus combination therapy for patients with both AUD and opioid use disorder, the authors said.
“The overall goal of this guideline is to enhance the treatment of AUD for millions of affected individuals, thereby reducing the significant psychosocial and public health consequences of this important psychiatric condition,” the report concluded. An executive summary of the guideline was published in the American Journal of Psychiatry.
The guideline authors disclosed no conflicts of interest with their work on the guideline.
SOURCE: Reus VI et al. Am J Psychiatry. 2018;175:86-90.
FROM THE AMERICAN JOURNAL OF PSYCHIATRY
Palliative care underutilized in dementia patients with acute abdomen
Despite high rates of in-hospital mortality and nonroutine discharge, palliative care is underutilized in patients with dementia and acute abdominal emergency, according to findings published in Surgery.
“Currently little is known about palliative care utilization among patients with dementia in possible need of surgical intervention. This raises the question of whether the acute surgical emergency represents an appropriate episode during which to introduce palliative care for patients with dementia,” wrote Ana Berlin, MD, FACS, of the department of surgery at New Jersey Medical School, Newark, N.J., and her coauthors (Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048).
Of 15,209 patients aged 50 years and older with dementia and acute abdomen, 7.5% received palliative care. Patients discharged nonroutinely and patients treated operatively were less likely to receive palliative care, the researchers reported.
Dr. Berlin and her colleagues used the National Inpatient Sample database to identify patients with dementia and acute abdomen who were admitted nonelectively between 2009 and 2013. They used ICD-9 primary and secondary codes to limit surgical diagnoses to gastrointestinal obstruction, ischemia, and perforation.
Overall, 50.9% of patients were admitted for gastrointestinal obstruction, 39.8% for perforation, 5.1% for bowel ischemia, and 4.3% for mixed pathology; 17.8% of patients were managed operatively.
Patients with intestinal ischemia had the highest rate of both operation and mortality, at 22.8% and 27.6%, respectively. These patients also had the lowest rate of routine discharge, at 15.9%, the authors said. In comparison, patients with obstruction had surgical intervention and in-hospital mortality rates of 17% and 10.1%, respectively, and a routine discharge rate of 20.9%. Patients with perforation had an operation rate of 13.8%, in-hospital mortality rate of 6.8%, and routine discharge rate of 26.9%.
The palliative care utilization rate overall was 7.5%. Patients with mixed pathology who did not have surgery were most likely to receive palliative care, at 21.1%, noted Dr. Berlin and her coauthors.
Patients who died postoperatively were less likely than were those who died without surgical intervention to have received palliative care (20.9% vs. 31.4%; odds ratio = 0.63, 95% confidence interval, 0.46-0.86; P = .0039), and those who were discharged nonroutinely after an operation were less likely than were patients who were discharged nonroutinely without an operation to receive palliative care (3.7% vs. 7.0%; OR = 0.44, 95% CI, 0.34-0.57; P less than .0001).
Lastly, patients who received palliative care had shorter median hospital stays than did those who did not receive palliative care (5 days vs. 6 days; P less than .0001). These patients also had lower median hospital charges ($29,500 vs. $31,600; P = .0403).
The results identify two subsets of patients with unmet palliative care needs: patients requiring operative intervention, and patients with a diagnosis of intestinal ischemia, the authors said. In addition, the findings suggest that “surgeons should consider initiating palliative care … early in the hospital course for patients with dementia presenting with acute surgical abdomen,” they wrote.
“Both hip fracture and intensive care unit admission in patients with dementia have been described as appropriate triggers for palliative care assessment. ... Acute abdominal emergency [may also represent] an appropriate episode during which to introduce palliative care for patients with dementia,” they concluded.
The study was funded by the Rutgers New Jersey Medical School department of surgery and the New Jersey Medical School Hispanic Center of Excellence, Health Resources, and Services Administration. No other disclosures were reported.
SOURCE: Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048.
Few surgeons would argue that a patient with dementia and an acute abdomen would be less appropriate for a palliative care consultation than demented patients with a hip fracture or ICU admission who have been shown to benefit from triggered palliative care consults. However, the dynamic interaction between patient, family, and surgeon, described by Thomas Miner as the “palliative triangle,” will likely prevent universal acceptance of triggered consults (Ann Surg Oncol. 2002;9[7]:696-709). Despite the current trend of increasingly algorithmic care, there is still a need for surgeon autonomy for treatment decisions even when the recommended triggered intervention is highly appropriate. A mentor of mine put it, “I never do things routinely, but there are some things I do all the time.” As the benefits of palliative care become more evident, the referrals for palliative care for this latest indication will become “some things I do all the time” just as pharmacokinetics referrals have become for antibiotics, anticoagulation, and total parenteral nutrition.

Few surgeons would argue that a patient with dementia and an acute abdomen would be less appropriate for a palliative care consultation than demented patients with a hip fracture or ICU admission who have been shown to benefit from triggered palliative care consults. However, the dynamic interaction between patient, family, and surgeon, described by Thomas Miner as the “palliative triangle,” will likely prevent universal acceptance of triggered consults (Ann Surg Oncol. 2002;9[7]:696-709). Despite the current trend of increasingly algorithmic care, there is still a need for surgeon autonomy for treatment decisions even when the recommended triggered intervention is highly appropriate. A mentor of mine put it, “I never do things routinely, but there are some things I do all the time.” As the benefits of palliative care become more evident, the referrals for palliative care for this latest indication will become “some things I do all the time” just as pharmacokinetics referrals have become for antibiotics, anticoagulation, and total parenteral nutrition.
Few surgeons would argue that a patient with dementia and an acute abdomen would be less appropriate for a palliative care consultation than demented patients with a hip fracture or ICU admission who have been shown to benefit from triggered palliative care consults. However, the dynamic interaction between patient, family, and surgeon, described by Thomas Miner as the “palliative triangle,” will likely prevent universal acceptance of triggered consults (Ann Surg Oncol. 2002;9[7]:696-709). Despite the current trend of increasingly algorithmic care, there is still a need for surgeon autonomy for treatment decisions even when the recommended triggered intervention is highly appropriate. A mentor of mine put it, “I never do things routinely, but there are some things I do all the time.” As the benefits of palliative care become more evident, the referrals for palliative care for this latest indication will become “some things I do all the time” just as pharmacokinetics referrals have become for antibiotics, anticoagulation, and total parenteral nutrition.
Despite high rates of in-hospital mortality and nonroutine discharge, palliative care is underutilized in patients with dementia and acute abdominal emergency, according to findings published in Surgery.
“Currently little is known about palliative care utilization among patients with dementia in possible need of surgical intervention. This raises the question of whether the acute surgical emergency represents an appropriate episode during which to introduce palliative care for patients with dementia,” wrote Ana Berlin, MD, FACS, of the department of surgery at New Jersey Medical School, Newark, N.J., and her coauthors (Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048).
Of 15,209 patients aged 50 years and older with dementia and acute abdomen, 7.5% received palliative care. Patients discharged nonroutinely and patients treated operatively were less likely to receive palliative care, the researchers reported.
Dr. Berlin and her colleagues used the National Inpatient Sample database to identify patients with dementia and acute abdomen who were admitted nonelectively between 2009 and 2013. They used ICD-9 primary and secondary codes to limit surgical diagnoses to gastrointestinal obstruction, ischemia, and perforation.
Overall, 50.9% of patients were admitted for gastrointestinal obstruction, 39.8% for perforation, 5.1% for bowel ischemia, and 4.3% for mixed pathology; 17.8% of patients were managed operatively.
Patients with intestinal ischemia had the highest rate of both operation and mortality, at 22.8% and 27.6%, respectively. These patients also had the lowest rate of routine discharge, at 15.9%, the authors said. In comparison, patients with obstruction had surgical intervention and in-hospital mortality rates of 17% and 10.1%, respectively, and a routine discharge rate of 20.9%. Patients with perforation had an operation rate of 13.8%, in-hospital mortality rate of 6.8%, and routine discharge rate of 26.9%.
The palliative care utilization rate overall was 7.5%. Patients with mixed pathology who did not have surgery were most likely to receive palliative care, at 21.1%, noted Dr. Berlin and her coauthors.
Patients who died postoperatively were less likely than were those who died without surgical intervention to have received palliative care (20.9% vs. 31.4%; odds ratio = 0.63, 95% confidence interval, 0.46-0.86; P = .0039), and those who were discharged nonroutinely after an operation were less likely than were patients who were discharged nonroutinely without an operation to receive palliative care (3.7% vs. 7.0%; OR = 0.44, 95% CI, 0.34-0.57; P less than .0001).
Lastly, patients who received palliative care had shorter median hospital stays than did those who did not receive palliative care (5 days vs. 6 days; P less than .0001). These patients also had lower median hospital charges ($29,500 vs. $31,600; P = .0403).
The results identify two subsets of patients with unmet palliative care needs: patients requiring operative intervention, and patients with a diagnosis of intestinal ischemia, the authors said. In addition, the findings suggest that “surgeons should consider initiating palliative care … early in the hospital course for patients with dementia presenting with acute surgical abdomen,” they wrote.
“Both hip fracture and intensive care unit admission in patients with dementia have been described as appropriate triggers for palliative care assessment. ... Acute abdominal emergency [may also represent] an appropriate episode during which to introduce palliative care for patients with dementia,” they concluded.
The study was funded by the Rutgers New Jersey Medical School department of surgery and the New Jersey Medical School Hispanic Center of Excellence, Health Resources, and Services Administration. No other disclosures were reported.
SOURCE: Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048.
Despite high rates of in-hospital mortality and nonroutine discharge, palliative care is underutilized in patients with dementia and acute abdominal emergency, according to findings published in Surgery.
“Currently little is known about palliative care utilization among patients with dementia in possible need of surgical intervention. This raises the question of whether the acute surgical emergency represents an appropriate episode during which to introduce palliative care for patients with dementia,” wrote Ana Berlin, MD, FACS, of the department of surgery at New Jersey Medical School, Newark, N.J., and her coauthors (Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048).
Of 15,209 patients aged 50 years and older with dementia and acute abdomen, 7.5% received palliative care. Patients discharged nonroutinely and patients treated operatively were less likely to receive palliative care, the researchers reported.
Dr. Berlin and her colleagues used the National Inpatient Sample database to identify patients with dementia and acute abdomen who were admitted nonelectively between 2009 and 2013. They used ICD-9 primary and secondary codes to limit surgical diagnoses to gastrointestinal obstruction, ischemia, and perforation.
Overall, 50.9% of patients were admitted for gastrointestinal obstruction, 39.8% for perforation, 5.1% for bowel ischemia, and 4.3% for mixed pathology; 17.8% of patients were managed operatively.
Patients with intestinal ischemia had the highest rate of both operation and mortality, at 22.8% and 27.6%, respectively. These patients also had the lowest rate of routine discharge, at 15.9%, the authors said. In comparison, patients with obstruction had surgical intervention and in-hospital mortality rates of 17% and 10.1%, respectively, and a routine discharge rate of 20.9%. Patients with perforation had an operation rate of 13.8%, in-hospital mortality rate of 6.8%, and routine discharge rate of 26.9%.
The palliative care utilization rate overall was 7.5%. Patients with mixed pathology who did not have surgery were most likely to receive palliative care, at 21.1%, noted Dr. Berlin and her coauthors.
Patients who died postoperatively were less likely than were those who died without surgical intervention to have received palliative care (20.9% vs. 31.4%; odds ratio = 0.63, 95% confidence interval, 0.46-0.86; P = .0039), and those who were discharged nonroutinely after an operation were less likely than were patients who were discharged nonroutinely without an operation to receive palliative care (3.7% vs. 7.0%; OR = 0.44, 95% CI, 0.34-0.57; P less than .0001).
Lastly, patients who received palliative care had shorter median hospital stays than did those who did not receive palliative care (5 days vs. 6 days; P less than .0001). These patients also had lower median hospital charges ($29,500 vs. $31,600; P = .0403).
The results identify two subsets of patients with unmet palliative care needs: patients requiring operative intervention, and patients with a diagnosis of intestinal ischemia, the authors said. In addition, the findings suggest that “surgeons should consider initiating palliative care … early in the hospital course for patients with dementia presenting with acute surgical abdomen,” they wrote.
“Both hip fracture and intensive care unit admission in patients with dementia have been described as appropriate triggers for palliative care assessment. ... Acute abdominal emergency [may also represent] an appropriate episode during which to introduce palliative care for patients with dementia,” they concluded.
The study was funded by the Rutgers New Jersey Medical School department of surgery and the New Jersey Medical School Hispanic Center of Excellence, Health Resources, and Services Administration. No other disclosures were reported.
SOURCE: Surgery. 2017 Dec 4. doi: 10.1016/j.surg.2017.09.048.
FROM SURGERY
Key clinical point: Despite high mortality and frequent nonroutine discharges, palliative care is underutilized in dementia patients with acute abdominal emergency.
Major finding: Among dementia patients with acute abdominal emergency, 7.5% received palliative care.
Data source: A retrospective analysis of 15,209 patients aged 50 years and older from the National Inpatient Sample, for the period of 2009-2013.
Disclosures: The study was funded by the Rutgers New Jersey Medical School Department of Surgery and the New Jersey Medical School Hispanic Center of Excellence, Health Resources, and Services Administration.
SOURCE: Surgery. 2017 Dec 4. doi: http://dx.doi.org/10.1016/j.surg.2017.09.048.
Varenicline may reduce heavy drinking in male smokers
The smoking cessation aid varenicline tartrate is effective for reducing heavy drinking in men with alcohol use disorder and comorbid cigarette smoking, according to findings published Dec. 20, 2017. The drug also increased smoking abstinence in participants overall, reported Stephanie S. O’Malley, PhD, of the department of psychiatry at Yale University, New Haven, Conn., and her coauthors.

Women had a smaller decrease in PHDD (P = .15), and 5% had NHDD, compared with 25% of the women on placebo.
The trial was conducted between September 2012 and August 2015 at research facilities affiliated with Columbia University in New York and with Yale. The study group was made up of 92 men and 39 women aged 18-70 years who met DSM-IV-TR criteria for alcohol dependence. Most of the respondents (52.7%) identified themselves as black. They reported heavy drinking at least twice per week for the preceding 90 days, having seven or fewer consecutive days of alcohol abstinence, and smoking at least twice per week, the investigators reported.
the authors reported, whereas none of the participants on placebo quit smoking (P = .003).
The sex differences in the trial may be attributed to differences in baseline characteristics, such as greater alcohol dependence and lower nicotine dependence, Dr. O’Malley and her colleagues said.
Additionally, women were more likely to reduce or discontinue varenicline dose. “From a methodological perspective, we permitted dose reductions to minimize adherence problems because lower varenicline doses are effective for smoking cessation,” they said.
The clinical implications of the findings are important, Dr. O’Malley and her colleagues said. “Individuals treated for alcoholism are more likely to die of smoking than from alcohol-related causes,” they wrote, and “most smokers do not receive smoking-cessation assistance, yet heavy-drinking smokers see these behaviors as highly associated.”
Lastly, the trial was limited by the small sample size of women.
“Future studies should evaluate the effectiveness and safety of varenicline in women and men separately in larger samples to establish whether the observed effects are of clinical significance,” the authors concluded.
The study was funded by grants from the National Institutes of Health and from Connecticut’s Department of Mental Health and Addiction Services. Pfizer, the manufacturer of varenicline under the name Chantix, provided varenicline and placebo pills.
The authors disclosed relationships with several companies, including Pfizer.
SOURCE: O’Malley SS et al. JAMA Psychiatry. 2017 Dec 20. doi: 10.1001/jamapsychiatry.2017.3544.
Despite its limitations, this study provides an important contribution to the body of addiction research, wrote A. Eden Evins, MD, MPH, in an accompanying editorial.
“Outcome measures that take into account multiple addictions are largely unexplored,” Dr. Evins said.
In addition to demonstrating its tolerability in patients with substance use disorders, the study makes “a creative contribution toward improved treatment trials for those who use multiple addictive substances by including an exploratory mixed outcome of no heavy drinking days and no tobacco use,” she wrote.
Future research should further explore sex differences, as well as proactive treatment strategies for smokers who are not ready to quit but are willing to try medications to improve their chances of quitting, Dr. Evins concluded.
Dr. A. Eden Evins is affiliated with the Center for Addiction Medicine at the department of psychiatry at Massachusetts General Hospital and with Harvard Medical School, both in Boston. She disclosed financial relationships with Forum Pharmaceuticals, Pfizer, and Brain Solutions.
Despite its limitations, this study provides an important contribution to the body of addiction research, wrote A. Eden Evins, MD, MPH, in an accompanying editorial.
“Outcome measures that take into account multiple addictions are largely unexplored,” Dr. Evins said.
In addition to demonstrating its tolerability in patients with substance use disorders, the study makes “a creative contribution toward improved treatment trials for those who use multiple addictive substances by including an exploratory mixed outcome of no heavy drinking days and no tobacco use,” she wrote.
Future research should further explore sex differences, as well as proactive treatment strategies for smokers who are not ready to quit but are willing to try medications to improve their chances of quitting, Dr. Evins concluded.
Dr. A. Eden Evins is affiliated with the Center for Addiction Medicine at the department of psychiatry at Massachusetts General Hospital and with Harvard Medical School, both in Boston. She disclosed financial relationships with Forum Pharmaceuticals, Pfizer, and Brain Solutions.
Despite its limitations, this study provides an important contribution to the body of addiction research, wrote A. Eden Evins, MD, MPH, in an accompanying editorial.
“Outcome measures that take into account multiple addictions are largely unexplored,” Dr. Evins said.
In addition to demonstrating its tolerability in patients with substance use disorders, the study makes “a creative contribution toward improved treatment trials for those who use multiple addictive substances by including an exploratory mixed outcome of no heavy drinking days and no tobacco use,” she wrote.
Future research should further explore sex differences, as well as proactive treatment strategies for smokers who are not ready to quit but are willing to try medications to improve their chances of quitting, Dr. Evins concluded.
Dr. A. Eden Evins is affiliated with the Center for Addiction Medicine at the department of psychiatry at Massachusetts General Hospital and with Harvard Medical School, both in Boston. She disclosed financial relationships with Forum Pharmaceuticals, Pfizer, and Brain Solutions.
The smoking cessation aid varenicline tartrate is effective for reducing heavy drinking in men with alcohol use disorder and comorbid cigarette smoking, according to findings published Dec. 20, 2017. The drug also increased smoking abstinence in participants overall, reported Stephanie S. O’Malley, PhD, of the department of psychiatry at Yale University, New Haven, Conn., and her coauthors.
Women had a smaller decrease in PHDD (P = .15), and 5% had NHDD, compared with 25% of the women on placebo.
The trial was conducted between September 2012 and August 2015 at research facilities affiliated with Columbia University in New York and with Yale. The study group was made up of 92 men and 39 women aged 18-70 years who met DSM-IV-TR criteria for alcohol dependence. Most of the respondents (52.7%) identified themselves as black. They reported heavy drinking at least twice per week for the preceding 90 days, having seven or fewer consecutive days of alcohol abstinence, and smoking at least twice per week, the investigators reported.
the authors reported, whereas none of the participants on placebo quit smoking (P = .003).
The sex differences in the trial may be attributed to differences in baseline characteristics, such as greater alcohol dependence and lower nicotine dependence, Dr. O’Malley and her colleagues said.
Additionally, women were more likely to reduce or discontinue varenicline dose. “From a methodological perspective, we permitted dose reductions to minimize adherence problems because lower varenicline doses are effective for smoking cessation,” they said.
The clinical implications of the findings are important, Dr. O’Malley and her colleagues said. “Individuals treated for alcoholism are more likely to die of smoking than from alcohol-related causes,” they wrote, and “most smokers do not receive smoking-cessation assistance, yet heavy-drinking smokers see these behaviors as highly associated.”
Lastly, the trial was limited by the small sample size of women.
“Future studies should evaluate the effectiveness and safety of varenicline in women and men separately in larger samples to establish whether the observed effects are of clinical significance,” the authors concluded.
The study was funded by grants from the National Institutes of Health and from Connecticut’s Department of Mental Health and Addiction Services. Pfizer, the manufacturer of varenicline under the name Chantix, provided varenicline and placebo pills.
The authors disclosed relationships with several companies, including Pfizer.
SOURCE: O’Malley SS et al. JAMA Psychiatry. 2017 Dec 20. doi: 10.1001/jamapsychiatry.2017.3544.
The smoking cessation aid varenicline tartrate is effective for reducing heavy drinking in men with alcohol use disorder and comorbid cigarette smoking, according to findings published Dec. 20, 2017. The drug also increased smoking abstinence in participants overall, reported Stephanie S. O’Malley, PhD, of the department of psychiatry at Yale University, New Haven, Conn., and her coauthors.
Women had a smaller decrease in PHDD (P = .15), and 5% had NHDD, compared with 25% of the women on placebo.
The trial was conducted between September 2012 and August 2015 at research facilities affiliated with Columbia University in New York and with Yale. The study group was made up of 92 men and 39 women aged 18-70 years who met DSM-IV-TR criteria for alcohol dependence. Most of the respondents (52.7%) identified themselves as black. They reported heavy drinking at least twice per week for the preceding 90 days, having seven or fewer consecutive days of alcohol abstinence, and smoking at least twice per week, the investigators reported.
the authors reported, whereas none of the participants on placebo quit smoking (P = .003).
The sex differences in the trial may be attributed to differences in baseline characteristics, such as greater alcohol dependence and lower nicotine dependence, Dr. O’Malley and her colleagues said.
Additionally, women were more likely to reduce or discontinue varenicline dose. “From a methodological perspective, we permitted dose reductions to minimize adherence problems because lower varenicline doses are effective for smoking cessation,” they said.
The clinical implications of the findings are important, Dr. O’Malley and her colleagues said. “Individuals treated for alcoholism are more likely to die of smoking than from alcohol-related causes,” they wrote, and “most smokers do not receive smoking-cessation assistance, yet heavy-drinking smokers see these behaviors as highly associated.”
Lastly, the trial was limited by the small sample size of women.
“Future studies should evaluate the effectiveness and safety of varenicline in women and men separately in larger samples to establish whether the observed effects are of clinical significance,” the authors concluded.
The study was funded by grants from the National Institutes of Health and from Connecticut’s Department of Mental Health and Addiction Services. Pfizer, the manufacturer of varenicline under the name Chantix, provided varenicline and placebo pills.
The authors disclosed relationships with several companies, including Pfizer.
SOURCE: O’Malley SS et al. JAMA Psychiatry. 2017 Dec 20. doi: 10.1001/jamapsychiatry.2017.3544.
FROM JAMA PSYCHIATRY
Key clinical point: The smoking cessation aid varenicline tartrate reduced heavy drinking in men and increased smoking abstinence in men and women.
Major finding: Varenicline resulted in a decrease in heavy drinking in men (95% confidence interval, –0.09 to 1.18; P = .09) and prolonged smoking abstinence in 13% of participants overall.
Study details: A phase 2, randomized, double-blind study of 131 participants with alcohol use disorder and comorbid smoking.
Disclosures: The study was funded by grants from the National Institutes of Health and from Connecticut’s Department of Mental Health and Addiction Services. Varenicline and placebo pills were provided by Pfizer, manufacturer of varenicline under the name Chantix. The authors disclosed relationships with several companies and organizations, including Pfizer.
Source: O’Malley SS et al. JAMA Psychiatry. 2017 Dec 20. doi: 10.1001/jamapsychiatry.2017.3544.
Tc-325 effective for immediate GI tumor bleeding
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
FROM GASTROINTESTINAL ENDOSCOPY
Key clinical point: Tc-325 is promising for initial hemostasis in patients with gastrointestinal tumor bleeding.
Major finding: Tc-325 achieved immediate hemostasis in 97.7% of patients with bleeding from GI tumors.
Data source: A multicenter retrospective study of 88 eligible patients with GI tumor-related hemorrhage from 2011 to 2016.
Disclosures: The authors did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
Source: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
Arthritis prevalence higher than previously thought, especially in adults under 65
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).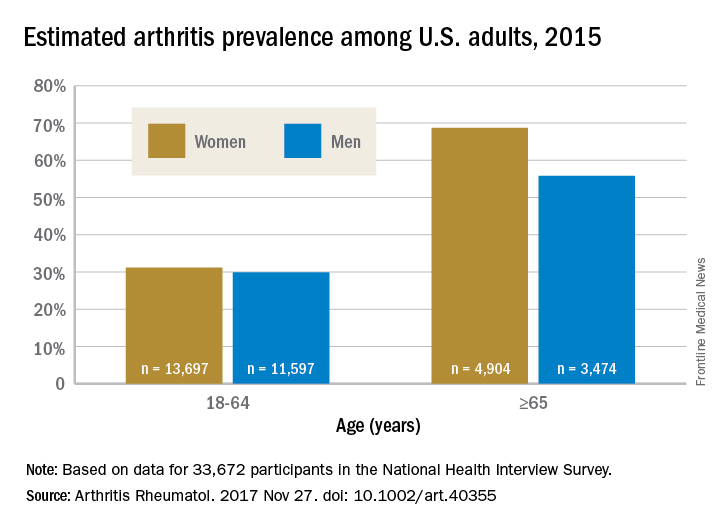
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: An estimated 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%).
Data source: Data from 33,672 respondents to the 2015 National Health Interview Survey.
Disclosures: The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.