User login
Appendicitis Review
Appendicitis is a transmural inflammatory process and a common cause of an acute abdomen. Inflammation that leads to perforation of the appendix, which is associated with increased morbidity and mortality, warrants prompt diagnosis. Etiology, clinical presentation, diagnostic studies, and the management of confirmed appendicitis will be addressed here.
Frequently, the etiology of appendicitis is luminal obstruction by a fecalith (the result of inspissated fecal material and inorganic salts1), but the condition may also result from parasites, a malignancy, a foreign body, or fibrosis.1-3 In some instances, lymphoid hyperplasia, resulting from a viral or bacterial infection, has been targeted as the cause of luminal obstruction.1,4 Nevertheless, in one-third to one-half of patients, obstruction is not evident as a precipitating factor in the development of appendicitis. In such cases, the basis for the inflammation is unknown.5
As the obstructed appendix becomes congested, the intraluminal pressure and venous pressure increase, leading to stasis and ischemia.1,5-8 The appendix becomes engorged with secretions. At this stage, the condition is considered uncomplicated, but if an inflamed appendix becomes gangrenous or perforates, the condition is then referred to as complicated appendicitis. Complicated appendicitis allows for invasion by intestinal bacteria of the abdominal cavity, potentially leading to peritonitis, septicemia, abscess, or fistula formation.5,9
Conventional teaching supports the concept that uncomplicated appendicitis, unless treated surgically, eventually evolves into complicated appendicitis.10 Recent research refutes this assumption, however, as different etiologies may be associated with differences in progression10-12; whether uncomplicated and complicated appendicitis are attributable to different etiologies is a question requiring further research. Irrespective of the natural progression of the disease, the current standard of care for appendicitis is still an appendectomy.13 In US hospitals in 2007 (the most recent year for which data are available), appendectomy was performed on 326,000 patients, or 10.9 patients per 10,000 population.14
EPIDEMIOLOGY
Appendicitis is most frequently seen in the second decade of life and occurs slightly more often in males than in females.2,15 Furthermore, according to data reported to the National Hospital Discharge Survey (1970 to 2004), the rate of nonperforated appendicitis is much higher in men than in women.12 In appendicitis, the risk for rupture is small within the first 36 hours of symptom onset. Beyond that point, there is a 5% increased risk for rupture with each ensuing 12-hour period.16
In neonates and infants, appendicitis is rare.3 In children younger than 3 years, however, the rate of perforation is 80% to 100%.3,17,18 This high rate may be explained by the very young child’s limited ability to articulate his or her symptoms, or by caregiver reports that are typically limited to irritability or change in diet.3,17,19 According to Marudanayagam et al,2 who performed a retrospective study of 2,660 appendectomies during a six-year period, the perforation rate declined from 23.4% in patients age 10 or younger to 6.9% in those in their 20s, then rose steadily to more than 50% in patients 70 or older.
PATIENT EVALUATION
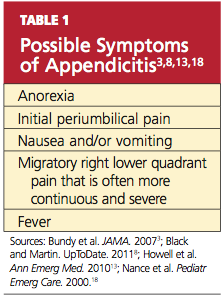
In most cases, a diagnosis of appendicitis can be made with a careful history, systematic physical exam, and a limited number of laboratory tests without special diagnostic modalities.13 The presence of symptoms and signs may help to rule in a diagnosis of appendicitis, but the absence of clinical findings often does not exclude its possibility.16 While adult and pediatric patients with appendicitis share many clinical findings (see Table 13,8,13,18), the occurrence rate of the various findings may differ among patient populations.3,15
The median time from onset of symptoms until the patient presents for a medical evaluation averages 24 hours or less.16 Diagnosis in patients at extremes of age often proves more difficult than in other patients.20 Thus, a high level of suspicion must be maintained in these patient populations.
The Symptom History
The appendix is located in the posteromedial wall of the cecum, approximately 3 cm below the ileocecal valve.1 Initial pain perceived around the umbilicus represents a referred pain resulting from the visceral innervation of the midgut.20 As the inflammatory process within the appendix advances, the pain localizes to the anatomical position of the right lower quadrant (RLQ), with involvement of the surrounding parietal peritoneum.20(McBurney’s point, at the junction of the lateral and middle thirds of a line extending from the anterior superior iliac spine to the umbilicus, was noted as the point of maximal tenderness to palpation in acute appendicitis by Charles McBurney in the late 1800s.21)
This progression of symptoms, first recognized by John Benjamin Murphy in 1904, is considered a more reliable indicator of appendicitis than RLQ pain alone3,22; in one large retrospective study, this migratory pain had the highest positive predictive value for pediatric and adult patients (94.2% and 89.6%, respectively).15 However, migration of pain occurs in only 50% to 60% of patients, and therefore may not be helpful.1,23
According to results from other studies, unfortunately, this progression of symptoms is not often present in pediatric patients.17 The somatic RLQ pain is continuous and more severe than is the early visceral periumbilical pain.1 Since the anatomic position of the appendix can vary, a number of patients do not necessarily present with pain in the RLQ but elsewhere.24
Certain clinical findings appear to be relatively age-dependent (see Table 225,26).
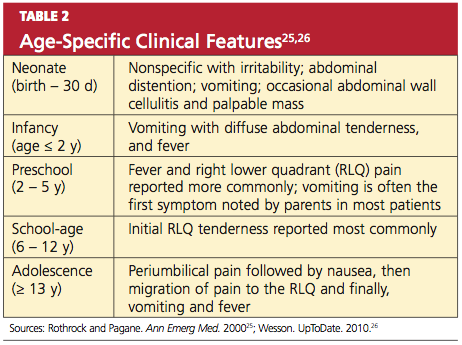
Classic findings in the adult diagnosed with appendicitis, as described by Becker et al,27 begin with periumbilical pain, then nausea, followed by migration of the pain to the RLQ, then vomiting and fever. Abdominal pain and anorexia are the most common presenting symptoms.20 Nausea and vomiting that begin after the onset of abdominal pain are typical; in isolation, however, these manifestations have weak diagnostic predictability for appendicitis.28 In adults, if nausea and vomiting precede abdominal pain, consideration should be given to a diagnosis of gastroenteritis rather than appendicitis.29
Among patients who are pregnant or elderly, RLQ pain remains a significant historical finding.30 In the pregnant woman, a diagnosis of appendicitis is often overlooked because of the discomforts common to pregnancy and the expanding gravid uterus.31 Elderly patients often present with vague or atypical symptoms, such as mild pain.20 In these patient populations, the diagnosis of appendicitis is often delayed.
In addition to obtaining a thorough history of the presentation of pain, it is important to conduct a complete review of the gastrointestinal, genitourinary, pulmonary, musculoskeletal, neurologic, and reproductive systems for possible alternate etiologies.
Physical Examination
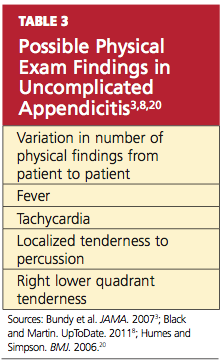
The number of physical findings varies among patients who present with appendicitis3,8,20 (see Table 33,8,20). A thorough physical examination is thus required to help the clinician exclude other diseases and establish the diagnosis of appendicitis. It is important to tailor the exam according to the patient’s age and developmental stage.19
The cooperation of children undergoing the physical examination for appendicitis may vary. It may be helpful to instruct a young child to “show me with your finger where it hurts the most.”3 However, Bundy et al3 report that the presence of RLQ tenderness on palpation is of minimal value in children; rather, fever is the single most useful sign among pediatric patients and conversely, its absence reduces the risk.
Tachycardia is associated with risk for rupture.16,20 In the elderly patient, fever (> 38°C) is also strongly correlated with an increased risk for rupture.30
To alleviate pain, a patient with appendicitis may maintain the hips and knees in a slightly flexed position. While asking distracting questions, the examiner should observe the patient’s facial expressions to detect involuntary guarding.3 RLQ tenderness to percussion is often positive.
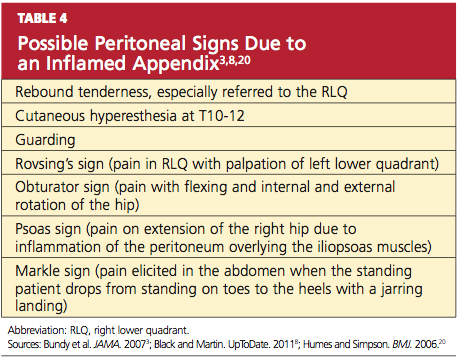
The patient may experience tenderness on palpation of the posterior abdominal wall (K sign) or right-side flank tenderness.24 Increased pain with coughing (Dunphy’s sign) or firm percussion of the heel (the heel jar test) may be elicited.8,25 A number of additional peritoneal signs, resulting from an inflamed appendix, may occur (see Table 43,8,20), but examination techniques that elicit these signs should be minimized so as to not cause the patient any unnecessary pain.
Depending on the location of the appendix, rectal and vaginal exams may yield normal findings or may elicit tenderness.32 The rectal examination should be performed with considerable care, using the smallest digit possible for an adequate assessment, especially in the younger patient.33
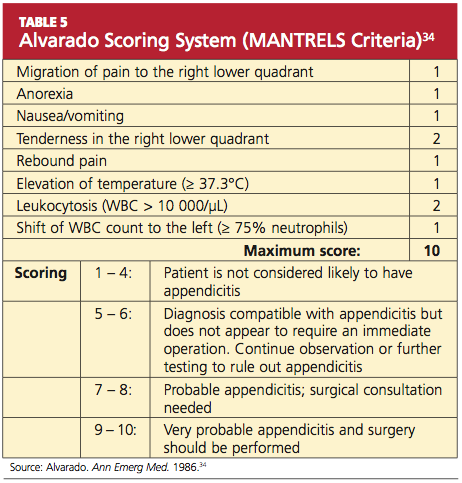
Several scoring systems have been designed for adults and children with suspected appendicitis, using findings from the history, the physical exam, and laboratory testing (see Table 5,34 for example). Despite their protocol-based approach, the scoring systems have yielded mixed results in clinical practice,34-36 and there is no scoring system for evaluation of the pregnant patient.37 Neither has there been any recommendation for or endorsement of a diagnostic guideline from any medical or professional organization.38 Thus, clinical gestalt is usually relied upon instead.
Conditions to Rule Out
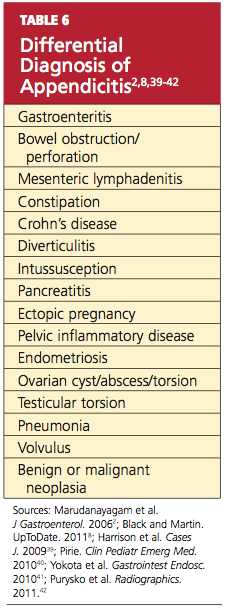
The patient with abdominal pain and suspected appendicitis should be evaluated for other causes during the physical examination (see Table 62,8,39-42). In addition to investigation for other abdominal etiologies, auscultation to the heart and lungs and an assessment of the peripheral vasculature are imperative. Auscultation of the lungs is important to rule out a right lower lobe pneumonia that may generate referred pain to the RLQ due to a shared T9 dermatome distribution.20,25
In males, the patient with abdominal pain should be assessed for a testicular etiology, and a pelvic examination is indicated in any female with abdominal pain, to rule out a gynecologic origin.1,3 In the infant with suspected appendicitis, a diagnosis of Hirschsprung’s disease (a congenital obstruction of the colon) should also be considered.17
LABORATORY WORK-UP
Based on the patient’s history and physical exam findings, certain laboratory and imaging studies can be useful in confirming the diagnosis of appendicitis. A white blood cell (WBC) count with differential is helpful in both diagnosis and exclusion of appendicitis: Appendicitis often leads to moderate leukocytosis (WBC, 10,000 to 20,000/μL) with neutrophilia.13 Similarly, the finding of a normal or low WBC and absent left shift helps to rule out appendicitis.43
A C-reactive protein (CRP) value greater than 3.0 mg/dL, when combined with moderate leukocytosis, may increase the likelihood of appendicitis and rule out other conditions (eg, gastroenteritis, mesenteric adenitis, pelvic inflammatory disease).15,44 Additionally, an elevated CRP may be sensitive (83% to > 90%) for detecting appendiceal perforation and abscess formation.44 The role of cytokine levels, such as interleukin-6 (IL-6) and IL-10, may be helpful but remain under investigation and are not typically used in the diagnosis of appendicitis.45
Because negative findings in the β-hCG rule out intrauterine or ectopic pregnancy, this test should be ordered for all women capable of pregnancy who present with acute abdominal pain.20 Urinalysis may be indicated to exclude abdominal pain of urinary tract etiology.3,46
Imaging Studies
Not all patients with a presumptive diagnosis of appendicitis require imaging. Such studies can be foregone in patients with low clinical suspicion for appendicitis, although they should be instructed to return if the pain worsens, changes, or does not resolve. Likewise, patients with a high clinical suspicion for appendicitis may be referred to a surgeon as early as possible (without imaging).13
In children, however, the classic clinical and laboratory findings are often less reliable in diagnosing appendicitis. Positive results on CT or ultrasound—that is, inflammation and distention of the appendix or free fluid in the abdomen—are associated with confirmed appendicitis more than 90% of the time.15
CT and ultrasound are currently considered the imaging studies of choice.13 Of the two, multidetector CT is more accurate for detecting inflammation of the appendix (sensitivity, 98.5%; specificity, 98%; 99.5% negative predictive value),47 especially in the obese patient.48 While CT use has increased, the overall negative appendectomy rate was similar in some clinical trials with or without CT use.49,50 Additionally, the cost, availability, length of test, and radiation exposure associated with CT have raised concern about this imaging choice.
Ultrasound is useful to confirm appendicitis, particularly in patients with limited abdominal fat, but it has limitations in ruling out the condition.51 These include its operator-dependent nature, limited ability to allow visualization of the appendix in obese patients, and lack of sensitivity in cases in which the appendix is perforated or only the distal tip is involved.7
Plain radiographs are not used to diagnose appendicitis, although they may be helpful to evaluate patients with atypical symptoms1 or to rule out other causes of abdominal pain. For example, a chest x-ray may be used to rule out pneumonia or to look for free air under the diaphragm, suggesting a different etiology.20,25
Imaging studies can be helpful when differentiating between complicated versus uncomplicated appendicitis and ruling out other causes of the acute abdomen (eg, gastroenteritis, diverticulitis, pelvic inflammatory disease). Alternatively, watchful observation is essential until the diagnosis becomes clearer or exploratory laparoscopic surgeries have been used to evaluate the acute abdomen.52
MANAGEMENT OF APPENDICITIS
Appendectomy remains the standard of care for appendicitis.13,53,54 While the clinical presentation often dictates what surgical approach should be taken, up to 76% of appendectomies are performed using a laparoscopic procedure rather than open surgery.55
Patients with uncomplicated appendicitis should be given nothing by mouth, but adequate hydration should be provided with IV fluids. IV analgesia should be considered if pain is causing distress to the patient. Current evidence suggests that administration of opioids does not alter the clinician’s diagnostic accuracy.56
The treatment of a patient with complicated appendicitis who is hemodynamically stable is less clear. The conventional treatment is antibiotics and drainage, followed by appendectomy at a later date6; this procedure is referred to as interval appendectomy. Some authorities suggest that in cases of appendicitis resolved with antibiotics, interval appendectomy should no longer be recommended.57,58 In 2011, Blakely et al59 reported that in children with perforated appendicitis, early surgery results in reduced recovery time and fewer adverse events, compared with delayed appendectomy.
Preoperative antibiotics have demonstrated efficacy in decreasing postoperative wound infections; the timing of antibiotic administration is critical to its efficacy.60,61 The first dose should be given within 60 minutes before the incision is made to achieve adequate antibiotic serum and tissue levels. The antibiotic should be discontinued 24 hours after the surgery has been completed.60,62
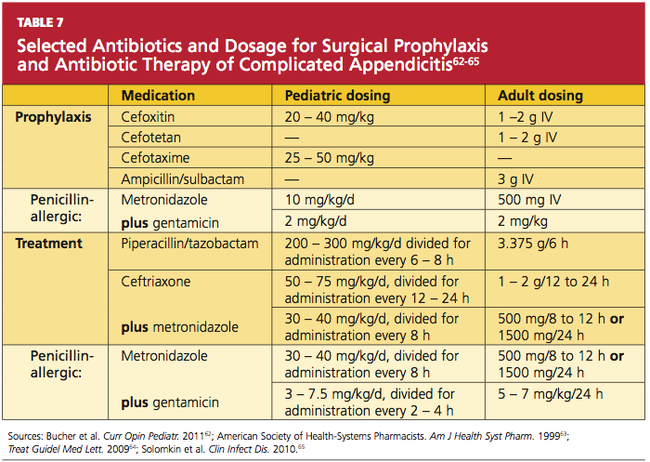
The agent selected for antibiotic prophylaxis should be effective against the most likely infecting organism.17,61,62 In a patient with uncomplicated appendicitis, the antibiotic of choice should be effective against gram-negative bacilli, such as Escherichia coli and Bacteroides fragilis.46,61,62 A single dose of cefoxitin, cefotetan, cefotaxime, or ampicillin/sulbactam is typically prescribed to prevent postsurgical site infections in patients with uncomplicated appendicitis (Table 762-65). For β-lactam–allergic patients, an alternative antibiotic regimen is metronidazole with an aminoglycoside.61,62
In Lieu of Surgery
As an alternative to surgery, several randomized studies have suggested that antibiotics alone can be used to treat uncomplicated appendicitis.66-68 Recent evidence suggests that a nonsurgical antibiotic approach may result in significant cost savings,69 attributable to eliminating surgery and a reduced risk for complications. Of additional benefit is eliminating surgery-associated morbidity and mortality.
Because design limitations lessen the reliability of the studies cited, however, appendectomy is still preferred, based on the current evidence.53,54 More studies are needed to determine the efficacy of antibiotic therapy alone, with consideration of the surgical risks associated with appendectomy.
POSTOPERATIVE CARE
Adequate pain control, advancement of diet, and monitoring for development of complications constitute typical postoperative care. Complications of appendectomy include both short- and long-term risks (eg, infection, adhesions, obstruction) associated with any surgical intervention.
CONCLUSION
Primary care providers should be well versed in identifying the symptoms and signs of appendicitis. In cases with equivocal findings, imaging studies and/or laboratory tests should be ordered to help confirm the diagnosis. The standard of care is appendectomy; therefore, a surgical consult is needed. Recent evidence suggests that a nonsurgical, antibiotic approach in the treatment of uncomplicated appendicitis may be beneficial. However, large, randomized trials with children enrolled, clear inclusion criteria, and outcome reporting with an intention-to-treat basis will help validate this approach as an alternative to current practice.
1. Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000;215(2):337-348.
2. Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2660 appendicectomy specimens. J Gastroenterol. 2006;41(8):745-749.
3. Bundy DG, Byerley JS, Liles EA, et al. Does this child have appendicitis? JAMA. 2007;298(4):438-451.
4. Alder AC, Fomby TB, Woodward WA, et al. Association of viral infection and appendicitis. Arch Surg. 2010;145(1):63-71.
5. Rubin R. The gastrointestinal tract. In: Rubin R, Strayer DS, eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine. 6th ed. Lippincott, Williams and Wilkins; 2012: 671.
6. McQuaid KR. Gastrointestinal disorders. In: McPhee SJ, Papadakis MA, eds. 2011 Current Medical Diagnosis and Treatment. 50th ed. McGraw Hill; 2011: 606-608.
7. Brennan GD. Pediatric appendicitis: pathophysiology and appropriate use of diagnostic imaging. CJEM. 2006;8(6):425-432.
8. Black C, Martin R. Acute appendicitis in adults: clinical manifestations and diagnosis (2011). www .uptodate.com/contents/acute-appendicitis-in-adults-clinical-manifestations-and-diagnosis. Accessed December 14, 2011.
9. Pittman-Waller VA, Myers JG, Stewart RM, et al. Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies. Am Surg. 2000; 6(66):548-554.
10. Mazuski JE, Solomkin JS. Intra-abdominal infections. Surg Clin North Am. 2009;89(2):421-437.
11. Andersson RE. The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg. 2007;31(1):86-92.
12. Livingston EH, Woodward WA, Sarosi GA, Haley RW. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg. 2007;245(6):886-892.
13. Howell JM, Eddy OL, Lukens TW, et al; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of emergency department patients with suspected appendicitis. Ann Emerg Med. 2010; 55(1):71-116.
14. CDC. Number, rate, and standard error of all-listed surgical and nonsurgical procedures for discharges from short-stay hospitals, by selected procedure categories: United States, 2007. www.cdc
.gov/nchs/data/nhds/4procedures/2009 pro4_num berrate.pdf. Accessed December 14, 2011.
15. Lee SL, Ho HS. Acute appendicitis: is there a difference between children and adults? Am Surg. 2006;5(72):409-413.
16. Bickell NA, Aufses AH Jr, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg. 2006;202(3):401-406.
17. Morrow SE, Newman KD. Current management of appendicitis. Semin Pediatr Surg. 2007; 16(1):34-40.
18. Nance ML, Adamson WT, Hedrick HL. Appendicitis in the young child: a continuing diagnostic challenge. Pediatr Emerg Care. 2000; 16(3):160-162.
19. Feinberg AN, Feinberg LA. The gastrointestinal tract, liver, gallbladder, and pancreas. In: Greydanus D, Feinberg A, Patel D, Homnick D, eds. The Pediatic Diagnostic Examination. McGraw-Hill Professional; 2008:267.
20. Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006;333(7567):530-534.
21. Yale SH, Musana KA. Charles Heber McBurney (1845-1913). Clin Med Res. 2005;3(3):187-189.
22. Murphy JB. Two thousand operations for appendicitis with deductions from his personal experience. Am J Med Sci. 1904;128:187-211.
23. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg. 2004;91(1):28-37.
24. Wani I. K-sign in retrocaecal appendicitis: a case series. Cases J. 2009;2:157.
25. Rothrock SG, Pagane J. Acute appendicitis in children: emergency department diagnosis and management. Ann Emerg Med. 2000;36(1):39-51.
26. Wesson DE. Acute appendicitis in children: clinical manifestations and diagnosis (2010). www .uptodate.com/contents/acute-appendicitis-in-chil dren-clinical-manifestations-and-diagnosis? source=related_link. Accessed December 14, 2011.
27. Becker T, Kharbanda A, Bachur R. Atypical clinical features of pediatric appendicitis. Acad Emerg Med. 2007;14(2):124-129.
28. Laméris W, van Randen A, Go P, et al. Single and combined diagnostic value of clinical features and laboratory tests in acute appendicitis. Acad Emerg Med. 2009;16(9):835-842.
29. McCollough M, Sharieff G. Abdominal pain in children. Pediatr Clin N Am. 2006;53:107-137.
30. Sheu BF, Chiu TF, Chen JC, et al. Risk factors associated with perforated appendicitis in elderly patients presenting with signs and symptoms of acute appendicitis. ANZ J Surg. 2007;77(8):662-666.
31. Borst AR. Acute appendicitis: pregnancy complicates this diagnosis. JAAPA. 2007; 20(12):36-38.
32. Sedlak M, Wagner OJ, Wild B, et al. Is there still a role for rectal examination in suspected appendicitis in adults? Am J Emerg Med. 2008;26 (3):359-377.
33. Ylitalo AW. Digital rectal examination. http://emedicine.medscape.com/article/1948001-overview#a1. Accessed December 14, 2011.
34. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15(5):557-564.
35. Schneider C, Kharbanda A, Bachur R. Evaluating appendicitis scoring systems using a prospective pediatric cohort. Ann Emerg Med. 2007; 49(6):778-784.
36. Kharbanda AB, Taylor GA, Fishman SJ, Bachur RG. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005; 116(3):709–16.
37. Brown JJ, Wilson C, Coleman S, Joypaul BV. Appendicitis in pregnancy. Colorectal Dis. 2009; 11(2):116-122.
38. Richardson E, Paulson C, Hitchcock K. Clinical inquiries. History, exam, and labs: is one enough to diagnose acute adult appendicitis? J Fam Practice. 2007;56(6):474-476.
39. Harrison S, Mahawar K, Brown D, et al. Acute appendicitis presenting as small bowel obstruction: two case reports. Cases J. 2009;2:9106.
40. Pirie J. Management of constipation in the emergency department. Clin Pediatr Emerg Med. 2010;11(3):182-188.
41. Yokota S, Togashi K, Kasahara N, et al. Crohn’s disease confined to the appendix. Gastrointest Endosc. 2010;72(5):1063-1064.
42. Purysko AS, Remer EM, Filho HM, et al. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics. 2011;31(4):927-947.
43. Wang LT, Prentiss KA, Simon JZ, et al. The use of white blood cell count and left shift in the diagnosis of appendicitis in children. Pediatr Emerg Care. 2007;23(2):69-76.
44. Kwan KY, Nager AL. Diagnosing pediatric appendicitis: usefulness of laboratory markers. Am J Emerg Med. 2010;28(9):1009-1015.
45. Yildirim O, Solak C, Koçer B, et al. The role of serum inflammatory markers in acute appendicitis and their success in preventing negative laparotomy. J Invest Surg. 2006;19(6):345-352.
46. Spirt MJ. Complicated intra-abdominal infections: a focus on appendicitis and diverticulitis. Postgrad Med. 2010;122(1):39-51.
47. Pickhardt PJ, Lawrence EM, Pooler D, Bruce RJ. Diagnostic performance of multidetector computed tomography for suspected acute appendicitis. Ann Intern Med. 2011:154(12):789-796.
48. Coursey CA, Nelson RC, Moreno RD, et al. Appendicitis, body mass index, and CT: is CT more valuable for obese patients than thin patients? Am Surg. 2011;77(4):471-475.
49. Petrosyan M, Estrada J, Chan S, et al. CT scan in patients with suspected appendicitis: clinical implications for the acute care surgeon. Eur Surg Res. 2008;40(2):211-219.
50. Huynh V, Lalezarzadeh F, Lawandy S, et al. Abdominal computed tomography in the evaluation of acute and perforated appendicitis in the community setting. Am Surg. 2007;73(10):1002-1005.
51. Fox JC, Solley M, Anderson CL, et al. Prospective evaluation of emergency physician performed bedside ultrasound to detect acute appendicitis. Eur J Emerg Med. 2008;15(2):80-85.
52. Al-Mulhim AS, Nasser MA, Abdullah MM, et al. Emergency laparoscopy for acute abdominal conditions: a prospective study. J Laparoendosc Adv Surg Tech A. 2008;18(4):599-602.
53. Varadhan KK, Humes DJ, Neal KR, Lobo DN. Antibiotic therapy versus appendectomy for acute appendicitis: a meta-analysis. World J Surg. 2010;34(2):199-209.
54. Fitzmaurice GJ, McWilliams B, Hurreiz H, Epanomeritakis E. Antibiotics versus appendectomy in the management of acute appendicitis: a review of the current evidence. Can J Surg. 2011; 54(5):307-314.
55. Ingraham AM, Cohen ME, Bilimoria KY, et al. Comparison of outcomes after laparoscopic versus open appendectomy for acute appendicitis at 222 ACS NSQIP hospitals. Surgery. 2010;148(4): 625-635.
56. Manterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011;(1):CD005660.
57. Puapong D, Lee SL, Haigh PI, et al. Routine interval appendectomy in children is not indicated. J Pediatr Surg. 2007;42(9):1500-1503.
58. Deakin DE, Ahmed I. Interval appendectomy after resolution of adult inflammatory appendix mass: is it necessary? Surgeon. 2007;5(1):45-50.
59. Blakely ML, Williams R, Dassinger MS, et al. Early vs interval appendectomy for children with perforated appendicitis. Arch Surg. 2011;146 (6):660-665.
60. Salkind AR, Rao KC. Antibiotic prophylaxis to prevent surgical site infections. Am Fam Physician. 2011;83(5):585-590.
61. James M. Antibiotics and perioperative infections. Best Pract Res Clin Anaesthesiol. 2008; 22(3):571-584.
62. Bucher BT, Warner BW, Dillon PA. Antibiotic prophylaxis and the prevention of surgical site infection. Curr Opin Pediatr. 2011;23(3):334-338.
63. American Society of Health-Systems Pharmacists. ASHP therapeutic guidelines on antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 1999;56(18):1839-1888.
64. Antimicrobial prophylaxis for surgery. Treat Guidel Med Lett. 2009;7(82):47-52.
65. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133-164.
66. Vons C, Barry C, Maitre S, et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomized controlled trial. Lancet. 2011;377(9777):1573-1579.
67. Hansson J, Körner U, Khorram-Manesh A, et al. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br J Surg. 2009;96(5):473-481.
68. Styrud J, Eriksson S, Nilsson I, et al. Appendectomy versus antibiotic treatment in acute appendicitis: a prospective multicenter randomized control trial. World J Surg. 2006;30(6):1033-1037.
69. Sakorafas GH, Mastoraki A, Lappas C, et al. Conservative treatment of acute appendicitis: heresy or an effective and acceptable alternative to surgery? Eur J Gastroenterol Hepatol. 2011;23 (2):121-127.
Appendicitis is a transmural inflammatory process and a common cause of an acute abdomen. Inflammation that leads to perforation of the appendix, which is associated with increased morbidity and mortality, warrants prompt diagnosis. Etiology, clinical presentation, diagnostic studies, and the management of confirmed appendicitis will be addressed here.
Frequently, the etiology of appendicitis is luminal obstruction by a fecalith (the result of inspissated fecal material and inorganic salts1), but the condition may also result from parasites, a malignancy, a foreign body, or fibrosis.1-3 In some instances, lymphoid hyperplasia, resulting from a viral or bacterial infection, has been targeted as the cause of luminal obstruction.1,4 Nevertheless, in one-third to one-half of patients, obstruction is not evident as a precipitating factor in the development of appendicitis. In such cases, the basis for the inflammation is unknown.5
As the obstructed appendix becomes congested, the intraluminal pressure and venous pressure increase, leading to stasis and ischemia.1,5-8 The appendix becomes engorged with secretions. At this stage, the condition is considered uncomplicated, but if an inflamed appendix becomes gangrenous or perforates, the condition is then referred to as complicated appendicitis. Complicated appendicitis allows for invasion by intestinal bacteria of the abdominal cavity, potentially leading to peritonitis, septicemia, abscess, or fistula formation.5,9
Conventional teaching supports the concept that uncomplicated appendicitis, unless treated surgically, eventually evolves into complicated appendicitis.10 Recent research refutes this assumption, however, as different etiologies may be associated with differences in progression10-12; whether uncomplicated and complicated appendicitis are attributable to different etiologies is a question requiring further research. Irrespective of the natural progression of the disease, the current standard of care for appendicitis is still an appendectomy.13 In US hospitals in 2007 (the most recent year for which data are available), appendectomy was performed on 326,000 patients, or 10.9 patients per 10,000 population.14
EPIDEMIOLOGY
Appendicitis is most frequently seen in the second decade of life and occurs slightly more often in males than in females.2,15 Furthermore, according to data reported to the National Hospital Discharge Survey (1970 to 2004), the rate of nonperforated appendicitis is much higher in men than in women.12 In appendicitis, the risk for rupture is small within the first 36 hours of symptom onset. Beyond that point, there is a 5% increased risk for rupture with each ensuing 12-hour period.16
In neonates and infants, appendicitis is rare.3 In children younger than 3 years, however, the rate of perforation is 80% to 100%.3,17,18 This high rate may be explained by the very young child’s limited ability to articulate his or her symptoms, or by caregiver reports that are typically limited to irritability or change in diet.3,17,19 According to Marudanayagam et al,2 who performed a retrospective study of 2,660 appendectomies during a six-year period, the perforation rate declined from 23.4% in patients age 10 or younger to 6.9% in those in their 20s, then rose steadily to more than 50% in patients 70 or older.
PATIENT EVALUATION
In most cases, a diagnosis of appendicitis can be made with a careful history, systematic physical exam, and a limited number of laboratory tests without special diagnostic modalities.13 The presence of symptoms and signs may help to rule in a diagnosis of appendicitis, but the absence of clinical findings often does not exclude its possibility.16 While adult and pediatric patients with appendicitis share many clinical findings (see Table 13,8,13,18), the occurrence rate of the various findings may differ among patient populations.3,15
The median time from onset of symptoms until the patient presents for a medical evaluation averages 24 hours or less.16 Diagnosis in patients at extremes of age often proves more difficult than in other patients.20 Thus, a high level of suspicion must be maintained in these patient populations.
The Symptom History
The appendix is located in the posteromedial wall of the cecum, approximately 3 cm below the ileocecal valve.1 Initial pain perceived around the umbilicus represents a referred pain resulting from the visceral innervation of the midgut.20 As the inflammatory process within the appendix advances, the pain localizes to the anatomical position of the right lower quadrant (RLQ), with involvement of the surrounding parietal peritoneum.20(McBurney’s point, at the junction of the lateral and middle thirds of a line extending from the anterior superior iliac spine to the umbilicus, was noted as the point of maximal tenderness to palpation in acute appendicitis by Charles McBurney in the late 1800s.21)
This progression of symptoms, first recognized by John Benjamin Murphy in 1904, is considered a more reliable indicator of appendicitis than RLQ pain alone3,22; in one large retrospective study, this migratory pain had the highest positive predictive value for pediatric and adult patients (94.2% and 89.6%, respectively).15 However, migration of pain occurs in only 50% to 60% of patients, and therefore may not be helpful.1,23
According to results from other studies, unfortunately, this progression of symptoms is not often present in pediatric patients.17 The somatic RLQ pain is continuous and more severe than is the early visceral periumbilical pain.1 Since the anatomic position of the appendix can vary, a number of patients do not necessarily present with pain in the RLQ but elsewhere.24
Certain clinical findings appear to be relatively age-dependent (see Table 225,26).
Classic findings in the adult diagnosed with appendicitis, as described by Becker et al,27 begin with periumbilical pain, then nausea, followed by migration of the pain to the RLQ, then vomiting and fever. Abdominal pain and anorexia are the most common presenting symptoms.20 Nausea and vomiting that begin after the onset of abdominal pain are typical; in isolation, however, these manifestations have weak diagnostic predictability for appendicitis.28 In adults, if nausea and vomiting precede abdominal pain, consideration should be given to a diagnosis of gastroenteritis rather than appendicitis.29
Among patients who are pregnant or elderly, RLQ pain remains a significant historical finding.30 In the pregnant woman, a diagnosis of appendicitis is often overlooked because of the discomforts common to pregnancy and the expanding gravid uterus.31 Elderly patients often present with vague or atypical symptoms, such as mild pain.20 In these patient populations, the diagnosis of appendicitis is often delayed.
In addition to obtaining a thorough history of the presentation of pain, it is important to conduct a complete review of the gastrointestinal, genitourinary, pulmonary, musculoskeletal, neurologic, and reproductive systems for possible alternate etiologies.
Physical Examination
The number of physical findings varies among patients who present with appendicitis3,8,20 (see Table 33,8,20). A thorough physical examination is thus required to help the clinician exclude other diseases and establish the diagnosis of appendicitis. It is important to tailor the exam according to the patient’s age and developmental stage.19
The cooperation of children undergoing the physical examination for appendicitis may vary. It may be helpful to instruct a young child to “show me with your finger where it hurts the most.”3 However, Bundy et al3 report that the presence of RLQ tenderness on palpation is of minimal value in children; rather, fever is the single most useful sign among pediatric patients and conversely, its absence reduces the risk.
Tachycardia is associated with risk for rupture.16,20 In the elderly patient, fever (> 38°C) is also strongly correlated with an increased risk for rupture.30
To alleviate pain, a patient with appendicitis may maintain the hips and knees in a slightly flexed position. While asking distracting questions, the examiner should observe the patient’s facial expressions to detect involuntary guarding.3 RLQ tenderness to percussion is often positive.
The patient may experience tenderness on palpation of the posterior abdominal wall (K sign) or right-side flank tenderness.24 Increased pain with coughing (Dunphy’s sign) or firm percussion of the heel (the heel jar test) may be elicited.8,25 A number of additional peritoneal signs, resulting from an inflamed appendix, may occur (see Table 43,8,20), but examination techniques that elicit these signs should be minimized so as to not cause the patient any unnecessary pain.
Depending on the location of the appendix, rectal and vaginal exams may yield normal findings or may elicit tenderness.32 The rectal examination should be performed with considerable care, using the smallest digit possible for an adequate assessment, especially in the younger patient.33
Several scoring systems have been designed for adults and children with suspected appendicitis, using findings from the history, the physical exam, and laboratory testing (see Table 5,34 for example). Despite their protocol-based approach, the scoring systems have yielded mixed results in clinical practice,34-36 and there is no scoring system for evaluation of the pregnant patient.37 Neither has there been any recommendation for or endorsement of a diagnostic guideline from any medical or professional organization.38 Thus, clinical gestalt is usually relied upon instead.
Conditions to Rule Out
The patient with abdominal pain and suspected appendicitis should be evaluated for other causes during the physical examination (see Table 62,8,39-42). In addition to investigation for other abdominal etiologies, auscultation to the heart and lungs and an assessment of the peripheral vasculature are imperative. Auscultation of the lungs is important to rule out a right lower lobe pneumonia that may generate referred pain to the RLQ due to a shared T9 dermatome distribution.20,25
In males, the patient with abdominal pain should be assessed for a testicular etiology, and a pelvic examination is indicated in any female with abdominal pain, to rule out a gynecologic origin.1,3 In the infant with suspected appendicitis, a diagnosis of Hirschsprung’s disease (a congenital obstruction of the colon) should also be considered.17
LABORATORY WORK-UP
Based on the patient’s history and physical exam findings, certain laboratory and imaging studies can be useful in confirming the diagnosis of appendicitis. A white blood cell (WBC) count with differential is helpful in both diagnosis and exclusion of appendicitis: Appendicitis often leads to moderate leukocytosis (WBC, 10,000 to 20,000/μL) with neutrophilia.13 Similarly, the finding of a normal or low WBC and absent left shift helps to rule out appendicitis.43
A C-reactive protein (CRP) value greater than 3.0 mg/dL, when combined with moderate leukocytosis, may increase the likelihood of appendicitis and rule out other conditions (eg, gastroenteritis, mesenteric adenitis, pelvic inflammatory disease).15,44 Additionally, an elevated CRP may be sensitive (83% to > 90%) for detecting appendiceal perforation and abscess formation.44 The role of cytokine levels, such as interleukin-6 (IL-6) and IL-10, may be helpful but remain under investigation and are not typically used in the diagnosis of appendicitis.45
Because negative findings in the β-hCG rule out intrauterine or ectopic pregnancy, this test should be ordered for all women capable of pregnancy who present with acute abdominal pain.20 Urinalysis may be indicated to exclude abdominal pain of urinary tract etiology.3,46
Imaging Studies
Not all patients with a presumptive diagnosis of appendicitis require imaging. Such studies can be foregone in patients with low clinical suspicion for appendicitis, although they should be instructed to return if the pain worsens, changes, or does not resolve. Likewise, patients with a high clinical suspicion for appendicitis may be referred to a surgeon as early as possible (without imaging).13
In children, however, the classic clinical and laboratory findings are often less reliable in diagnosing appendicitis. Positive results on CT or ultrasound—that is, inflammation and distention of the appendix or free fluid in the abdomen—are associated with confirmed appendicitis more than 90% of the time.15
CT and ultrasound are currently considered the imaging studies of choice.13 Of the two, multidetector CT is more accurate for detecting inflammation of the appendix (sensitivity, 98.5%; specificity, 98%; 99.5% negative predictive value),47 especially in the obese patient.48 While CT use has increased, the overall negative appendectomy rate was similar in some clinical trials with or without CT use.49,50 Additionally, the cost, availability, length of test, and radiation exposure associated with CT have raised concern about this imaging choice.
Ultrasound is useful to confirm appendicitis, particularly in patients with limited abdominal fat, but it has limitations in ruling out the condition.51 These include its operator-dependent nature, limited ability to allow visualization of the appendix in obese patients, and lack of sensitivity in cases in which the appendix is perforated or only the distal tip is involved.7
Plain radiographs are not used to diagnose appendicitis, although they may be helpful to evaluate patients with atypical symptoms1 or to rule out other causes of abdominal pain. For example, a chest x-ray may be used to rule out pneumonia or to look for free air under the diaphragm, suggesting a different etiology.20,25
Imaging studies can be helpful when differentiating between complicated versus uncomplicated appendicitis and ruling out other causes of the acute abdomen (eg, gastroenteritis, diverticulitis, pelvic inflammatory disease). Alternatively, watchful observation is essential until the diagnosis becomes clearer or exploratory laparoscopic surgeries have been used to evaluate the acute abdomen.52
MANAGEMENT OF APPENDICITIS
Appendectomy remains the standard of care for appendicitis.13,53,54 While the clinical presentation often dictates what surgical approach should be taken, up to 76% of appendectomies are performed using a laparoscopic procedure rather than open surgery.55
Patients with uncomplicated appendicitis should be given nothing by mouth, but adequate hydration should be provided with IV fluids. IV analgesia should be considered if pain is causing distress to the patient. Current evidence suggests that administration of opioids does not alter the clinician’s diagnostic accuracy.56
The treatment of a patient with complicated appendicitis who is hemodynamically stable is less clear. The conventional treatment is antibiotics and drainage, followed by appendectomy at a later date6; this procedure is referred to as interval appendectomy. Some authorities suggest that in cases of appendicitis resolved with antibiotics, interval appendectomy should no longer be recommended.57,58 In 2011, Blakely et al59 reported that in children with perforated appendicitis, early surgery results in reduced recovery time and fewer adverse events, compared with delayed appendectomy.
Preoperative antibiotics have demonstrated efficacy in decreasing postoperative wound infections; the timing of antibiotic administration is critical to its efficacy.60,61 The first dose should be given within 60 minutes before the incision is made to achieve adequate antibiotic serum and tissue levels. The antibiotic should be discontinued 24 hours after the surgery has been completed.60,62
The agent selected for antibiotic prophylaxis should be effective against the most likely infecting organism.17,61,62 In a patient with uncomplicated appendicitis, the antibiotic of choice should be effective against gram-negative bacilli, such as Escherichia coli and Bacteroides fragilis.46,61,62 A single dose of cefoxitin, cefotetan, cefotaxime, or ampicillin/sulbactam is typically prescribed to prevent postsurgical site infections in patients with uncomplicated appendicitis (Table 762-65). For β-lactam–allergic patients, an alternative antibiotic regimen is metronidazole with an aminoglycoside.61,62
In Lieu of Surgery
As an alternative to surgery, several randomized studies have suggested that antibiotics alone can be used to treat uncomplicated appendicitis.66-68 Recent evidence suggests that a nonsurgical antibiotic approach may result in significant cost savings,69 attributable to eliminating surgery and a reduced risk for complications. Of additional benefit is eliminating surgery-associated morbidity and mortality.
Because design limitations lessen the reliability of the studies cited, however, appendectomy is still preferred, based on the current evidence.53,54 More studies are needed to determine the efficacy of antibiotic therapy alone, with consideration of the surgical risks associated with appendectomy.
POSTOPERATIVE CARE
Adequate pain control, advancement of diet, and monitoring for development of complications constitute typical postoperative care. Complications of appendectomy include both short- and long-term risks (eg, infection, adhesions, obstruction) associated with any surgical intervention.
CONCLUSION
Primary care providers should be well versed in identifying the symptoms and signs of appendicitis. In cases with equivocal findings, imaging studies and/or laboratory tests should be ordered to help confirm the diagnosis. The standard of care is appendectomy; therefore, a surgical consult is needed. Recent evidence suggests that a nonsurgical, antibiotic approach in the treatment of uncomplicated appendicitis may be beneficial. However, large, randomized trials with children enrolled, clear inclusion criteria, and outcome reporting with an intention-to-treat basis will help validate this approach as an alternative to current practice.
Appendicitis is a transmural inflammatory process and a common cause of an acute abdomen. Inflammation that leads to perforation of the appendix, which is associated with increased morbidity and mortality, warrants prompt diagnosis. Etiology, clinical presentation, diagnostic studies, and the management of confirmed appendicitis will be addressed here.
Frequently, the etiology of appendicitis is luminal obstruction by a fecalith (the result of inspissated fecal material and inorganic salts1), but the condition may also result from parasites, a malignancy, a foreign body, or fibrosis.1-3 In some instances, lymphoid hyperplasia, resulting from a viral or bacterial infection, has been targeted as the cause of luminal obstruction.1,4 Nevertheless, in one-third to one-half of patients, obstruction is not evident as a precipitating factor in the development of appendicitis. In such cases, the basis for the inflammation is unknown.5
As the obstructed appendix becomes congested, the intraluminal pressure and venous pressure increase, leading to stasis and ischemia.1,5-8 The appendix becomes engorged with secretions. At this stage, the condition is considered uncomplicated, but if an inflamed appendix becomes gangrenous or perforates, the condition is then referred to as complicated appendicitis. Complicated appendicitis allows for invasion by intestinal bacteria of the abdominal cavity, potentially leading to peritonitis, septicemia, abscess, or fistula formation.5,9
Conventional teaching supports the concept that uncomplicated appendicitis, unless treated surgically, eventually evolves into complicated appendicitis.10 Recent research refutes this assumption, however, as different etiologies may be associated with differences in progression10-12; whether uncomplicated and complicated appendicitis are attributable to different etiologies is a question requiring further research. Irrespective of the natural progression of the disease, the current standard of care for appendicitis is still an appendectomy.13 In US hospitals in 2007 (the most recent year for which data are available), appendectomy was performed on 326,000 patients, or 10.9 patients per 10,000 population.14
EPIDEMIOLOGY
Appendicitis is most frequently seen in the second decade of life and occurs slightly more often in males than in females.2,15 Furthermore, according to data reported to the National Hospital Discharge Survey (1970 to 2004), the rate of nonperforated appendicitis is much higher in men than in women.12 In appendicitis, the risk for rupture is small within the first 36 hours of symptom onset. Beyond that point, there is a 5% increased risk for rupture with each ensuing 12-hour period.16
In neonates and infants, appendicitis is rare.3 In children younger than 3 years, however, the rate of perforation is 80% to 100%.3,17,18 This high rate may be explained by the very young child’s limited ability to articulate his or her symptoms, or by caregiver reports that are typically limited to irritability or change in diet.3,17,19 According to Marudanayagam et al,2 who performed a retrospective study of 2,660 appendectomies during a six-year period, the perforation rate declined from 23.4% in patients age 10 or younger to 6.9% in those in their 20s, then rose steadily to more than 50% in patients 70 or older.
PATIENT EVALUATION
In most cases, a diagnosis of appendicitis can be made with a careful history, systematic physical exam, and a limited number of laboratory tests without special diagnostic modalities.13 The presence of symptoms and signs may help to rule in a diagnosis of appendicitis, but the absence of clinical findings often does not exclude its possibility.16 While adult and pediatric patients with appendicitis share many clinical findings (see Table 13,8,13,18), the occurrence rate of the various findings may differ among patient populations.3,15
The median time from onset of symptoms until the patient presents for a medical evaluation averages 24 hours or less.16 Diagnosis in patients at extremes of age often proves more difficult than in other patients.20 Thus, a high level of suspicion must be maintained in these patient populations.
The Symptom History
The appendix is located in the posteromedial wall of the cecum, approximately 3 cm below the ileocecal valve.1 Initial pain perceived around the umbilicus represents a referred pain resulting from the visceral innervation of the midgut.20 As the inflammatory process within the appendix advances, the pain localizes to the anatomical position of the right lower quadrant (RLQ), with involvement of the surrounding parietal peritoneum.20(McBurney’s point, at the junction of the lateral and middle thirds of a line extending from the anterior superior iliac spine to the umbilicus, was noted as the point of maximal tenderness to palpation in acute appendicitis by Charles McBurney in the late 1800s.21)
This progression of symptoms, first recognized by John Benjamin Murphy in 1904, is considered a more reliable indicator of appendicitis than RLQ pain alone3,22; in one large retrospective study, this migratory pain had the highest positive predictive value for pediatric and adult patients (94.2% and 89.6%, respectively).15 However, migration of pain occurs in only 50% to 60% of patients, and therefore may not be helpful.1,23
According to results from other studies, unfortunately, this progression of symptoms is not often present in pediatric patients.17 The somatic RLQ pain is continuous and more severe than is the early visceral periumbilical pain.1 Since the anatomic position of the appendix can vary, a number of patients do not necessarily present with pain in the RLQ but elsewhere.24
Certain clinical findings appear to be relatively age-dependent (see Table 225,26).
Classic findings in the adult diagnosed with appendicitis, as described by Becker et al,27 begin with periumbilical pain, then nausea, followed by migration of the pain to the RLQ, then vomiting and fever. Abdominal pain and anorexia are the most common presenting symptoms.20 Nausea and vomiting that begin after the onset of abdominal pain are typical; in isolation, however, these manifestations have weak diagnostic predictability for appendicitis.28 In adults, if nausea and vomiting precede abdominal pain, consideration should be given to a diagnosis of gastroenteritis rather than appendicitis.29
Among patients who are pregnant or elderly, RLQ pain remains a significant historical finding.30 In the pregnant woman, a diagnosis of appendicitis is often overlooked because of the discomforts common to pregnancy and the expanding gravid uterus.31 Elderly patients often present with vague or atypical symptoms, such as mild pain.20 In these patient populations, the diagnosis of appendicitis is often delayed.
In addition to obtaining a thorough history of the presentation of pain, it is important to conduct a complete review of the gastrointestinal, genitourinary, pulmonary, musculoskeletal, neurologic, and reproductive systems for possible alternate etiologies.
Physical Examination
The number of physical findings varies among patients who present with appendicitis3,8,20 (see Table 33,8,20). A thorough physical examination is thus required to help the clinician exclude other diseases and establish the diagnosis of appendicitis. It is important to tailor the exam according to the patient’s age and developmental stage.19
The cooperation of children undergoing the physical examination for appendicitis may vary. It may be helpful to instruct a young child to “show me with your finger where it hurts the most.”3 However, Bundy et al3 report that the presence of RLQ tenderness on palpation is of minimal value in children; rather, fever is the single most useful sign among pediatric patients and conversely, its absence reduces the risk.
Tachycardia is associated with risk for rupture.16,20 In the elderly patient, fever (> 38°C) is also strongly correlated with an increased risk for rupture.30
To alleviate pain, a patient with appendicitis may maintain the hips and knees in a slightly flexed position. While asking distracting questions, the examiner should observe the patient’s facial expressions to detect involuntary guarding.3 RLQ tenderness to percussion is often positive.
The patient may experience tenderness on palpation of the posterior abdominal wall (K sign) or right-side flank tenderness.24 Increased pain with coughing (Dunphy’s sign) or firm percussion of the heel (the heel jar test) may be elicited.8,25 A number of additional peritoneal signs, resulting from an inflamed appendix, may occur (see Table 43,8,20), but examination techniques that elicit these signs should be minimized so as to not cause the patient any unnecessary pain.
Depending on the location of the appendix, rectal and vaginal exams may yield normal findings or may elicit tenderness.32 The rectal examination should be performed with considerable care, using the smallest digit possible for an adequate assessment, especially in the younger patient.33
Several scoring systems have been designed for adults and children with suspected appendicitis, using findings from the history, the physical exam, and laboratory testing (see Table 5,34 for example). Despite their protocol-based approach, the scoring systems have yielded mixed results in clinical practice,34-36 and there is no scoring system for evaluation of the pregnant patient.37 Neither has there been any recommendation for or endorsement of a diagnostic guideline from any medical or professional organization.38 Thus, clinical gestalt is usually relied upon instead.
Conditions to Rule Out
The patient with abdominal pain and suspected appendicitis should be evaluated for other causes during the physical examination (see Table 62,8,39-42). In addition to investigation for other abdominal etiologies, auscultation to the heart and lungs and an assessment of the peripheral vasculature are imperative. Auscultation of the lungs is important to rule out a right lower lobe pneumonia that may generate referred pain to the RLQ due to a shared T9 dermatome distribution.20,25
In males, the patient with abdominal pain should be assessed for a testicular etiology, and a pelvic examination is indicated in any female with abdominal pain, to rule out a gynecologic origin.1,3 In the infant with suspected appendicitis, a diagnosis of Hirschsprung’s disease (a congenital obstruction of the colon) should also be considered.17
LABORATORY WORK-UP
Based on the patient’s history and physical exam findings, certain laboratory and imaging studies can be useful in confirming the diagnosis of appendicitis. A white blood cell (WBC) count with differential is helpful in both diagnosis and exclusion of appendicitis: Appendicitis often leads to moderate leukocytosis (WBC, 10,000 to 20,000/μL) with neutrophilia.13 Similarly, the finding of a normal or low WBC and absent left shift helps to rule out appendicitis.43
A C-reactive protein (CRP) value greater than 3.0 mg/dL, when combined with moderate leukocytosis, may increase the likelihood of appendicitis and rule out other conditions (eg, gastroenteritis, mesenteric adenitis, pelvic inflammatory disease).15,44 Additionally, an elevated CRP may be sensitive (83% to > 90%) for detecting appendiceal perforation and abscess formation.44 The role of cytokine levels, such as interleukin-6 (IL-6) and IL-10, may be helpful but remain under investigation and are not typically used in the diagnosis of appendicitis.45
Because negative findings in the β-hCG rule out intrauterine or ectopic pregnancy, this test should be ordered for all women capable of pregnancy who present with acute abdominal pain.20 Urinalysis may be indicated to exclude abdominal pain of urinary tract etiology.3,46
Imaging Studies
Not all patients with a presumptive diagnosis of appendicitis require imaging. Such studies can be foregone in patients with low clinical suspicion for appendicitis, although they should be instructed to return if the pain worsens, changes, or does not resolve. Likewise, patients with a high clinical suspicion for appendicitis may be referred to a surgeon as early as possible (without imaging).13
In children, however, the classic clinical and laboratory findings are often less reliable in diagnosing appendicitis. Positive results on CT or ultrasound—that is, inflammation and distention of the appendix or free fluid in the abdomen—are associated with confirmed appendicitis more than 90% of the time.15
CT and ultrasound are currently considered the imaging studies of choice.13 Of the two, multidetector CT is more accurate for detecting inflammation of the appendix (sensitivity, 98.5%; specificity, 98%; 99.5% negative predictive value),47 especially in the obese patient.48 While CT use has increased, the overall negative appendectomy rate was similar in some clinical trials with or without CT use.49,50 Additionally, the cost, availability, length of test, and radiation exposure associated with CT have raised concern about this imaging choice.
Ultrasound is useful to confirm appendicitis, particularly in patients with limited abdominal fat, but it has limitations in ruling out the condition.51 These include its operator-dependent nature, limited ability to allow visualization of the appendix in obese patients, and lack of sensitivity in cases in which the appendix is perforated or only the distal tip is involved.7
Plain radiographs are not used to diagnose appendicitis, although they may be helpful to evaluate patients with atypical symptoms1 or to rule out other causes of abdominal pain. For example, a chest x-ray may be used to rule out pneumonia or to look for free air under the diaphragm, suggesting a different etiology.20,25
Imaging studies can be helpful when differentiating between complicated versus uncomplicated appendicitis and ruling out other causes of the acute abdomen (eg, gastroenteritis, diverticulitis, pelvic inflammatory disease). Alternatively, watchful observation is essential until the diagnosis becomes clearer or exploratory laparoscopic surgeries have been used to evaluate the acute abdomen.52
MANAGEMENT OF APPENDICITIS
Appendectomy remains the standard of care for appendicitis.13,53,54 While the clinical presentation often dictates what surgical approach should be taken, up to 76% of appendectomies are performed using a laparoscopic procedure rather than open surgery.55
Patients with uncomplicated appendicitis should be given nothing by mouth, but adequate hydration should be provided with IV fluids. IV analgesia should be considered if pain is causing distress to the patient. Current evidence suggests that administration of opioids does not alter the clinician’s diagnostic accuracy.56
The treatment of a patient with complicated appendicitis who is hemodynamically stable is less clear. The conventional treatment is antibiotics and drainage, followed by appendectomy at a later date6; this procedure is referred to as interval appendectomy. Some authorities suggest that in cases of appendicitis resolved with antibiotics, interval appendectomy should no longer be recommended.57,58 In 2011, Blakely et al59 reported that in children with perforated appendicitis, early surgery results in reduced recovery time and fewer adverse events, compared with delayed appendectomy.
Preoperative antibiotics have demonstrated efficacy in decreasing postoperative wound infections; the timing of antibiotic administration is critical to its efficacy.60,61 The first dose should be given within 60 minutes before the incision is made to achieve adequate antibiotic serum and tissue levels. The antibiotic should be discontinued 24 hours after the surgery has been completed.60,62
The agent selected for antibiotic prophylaxis should be effective against the most likely infecting organism.17,61,62 In a patient with uncomplicated appendicitis, the antibiotic of choice should be effective against gram-negative bacilli, such as Escherichia coli and Bacteroides fragilis.46,61,62 A single dose of cefoxitin, cefotetan, cefotaxime, or ampicillin/sulbactam is typically prescribed to prevent postsurgical site infections in patients with uncomplicated appendicitis (Table 762-65). For β-lactam–allergic patients, an alternative antibiotic regimen is metronidazole with an aminoglycoside.61,62
In Lieu of Surgery
As an alternative to surgery, several randomized studies have suggested that antibiotics alone can be used to treat uncomplicated appendicitis.66-68 Recent evidence suggests that a nonsurgical antibiotic approach may result in significant cost savings,69 attributable to eliminating surgery and a reduced risk for complications. Of additional benefit is eliminating surgery-associated morbidity and mortality.
Because design limitations lessen the reliability of the studies cited, however, appendectomy is still preferred, based on the current evidence.53,54 More studies are needed to determine the efficacy of antibiotic therapy alone, with consideration of the surgical risks associated with appendectomy.
POSTOPERATIVE CARE
Adequate pain control, advancement of diet, and monitoring for development of complications constitute typical postoperative care. Complications of appendectomy include both short- and long-term risks (eg, infection, adhesions, obstruction) associated with any surgical intervention.
CONCLUSION
Primary care providers should be well versed in identifying the symptoms and signs of appendicitis. In cases with equivocal findings, imaging studies and/or laboratory tests should be ordered to help confirm the diagnosis. The standard of care is appendectomy; therefore, a surgical consult is needed. Recent evidence suggests that a nonsurgical, antibiotic approach in the treatment of uncomplicated appendicitis may be beneficial. However, large, randomized trials with children enrolled, clear inclusion criteria, and outcome reporting with an intention-to-treat basis will help validate this approach as an alternative to current practice.
1. Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000;215(2):337-348.
2. Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2660 appendicectomy specimens. J Gastroenterol. 2006;41(8):745-749.
3. Bundy DG, Byerley JS, Liles EA, et al. Does this child have appendicitis? JAMA. 2007;298(4):438-451.
4. Alder AC, Fomby TB, Woodward WA, et al. Association of viral infection and appendicitis. Arch Surg. 2010;145(1):63-71.
5. Rubin R. The gastrointestinal tract. In: Rubin R, Strayer DS, eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine. 6th ed. Lippincott, Williams and Wilkins; 2012: 671.
6. McQuaid KR. Gastrointestinal disorders. In: McPhee SJ, Papadakis MA, eds. 2011 Current Medical Diagnosis and Treatment. 50th ed. McGraw Hill; 2011: 606-608.
7. Brennan GD. Pediatric appendicitis: pathophysiology and appropriate use of diagnostic imaging. CJEM. 2006;8(6):425-432.
8. Black C, Martin R. Acute appendicitis in adults: clinical manifestations and diagnosis (2011). www .uptodate.com/contents/acute-appendicitis-in-adults-clinical-manifestations-and-diagnosis. Accessed December 14, 2011.
9. Pittman-Waller VA, Myers JG, Stewart RM, et al. Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies. Am Surg. 2000; 6(66):548-554.
10. Mazuski JE, Solomkin JS. Intra-abdominal infections. Surg Clin North Am. 2009;89(2):421-437.
11. Andersson RE. The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg. 2007;31(1):86-92.
12. Livingston EH, Woodward WA, Sarosi GA, Haley RW. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg. 2007;245(6):886-892.
13. Howell JM, Eddy OL, Lukens TW, et al; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of emergency department patients with suspected appendicitis. Ann Emerg Med. 2010; 55(1):71-116.
14. CDC. Number, rate, and standard error of all-listed surgical and nonsurgical procedures for discharges from short-stay hospitals, by selected procedure categories: United States, 2007. www.cdc
.gov/nchs/data/nhds/4procedures/2009 pro4_num berrate.pdf. Accessed December 14, 2011.
15. Lee SL, Ho HS. Acute appendicitis: is there a difference between children and adults? Am Surg. 2006;5(72):409-413.
16. Bickell NA, Aufses AH Jr, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg. 2006;202(3):401-406.
17. Morrow SE, Newman KD. Current management of appendicitis. Semin Pediatr Surg. 2007; 16(1):34-40.
18. Nance ML, Adamson WT, Hedrick HL. Appendicitis in the young child: a continuing diagnostic challenge. Pediatr Emerg Care. 2000; 16(3):160-162.
19. Feinberg AN, Feinberg LA. The gastrointestinal tract, liver, gallbladder, and pancreas. In: Greydanus D, Feinberg A, Patel D, Homnick D, eds. The Pediatic Diagnostic Examination. McGraw-Hill Professional; 2008:267.
20. Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006;333(7567):530-534.
21. Yale SH, Musana KA. Charles Heber McBurney (1845-1913). Clin Med Res. 2005;3(3):187-189.
22. Murphy JB. Two thousand operations for appendicitis with deductions from his personal experience. Am J Med Sci. 1904;128:187-211.
23. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg. 2004;91(1):28-37.
24. Wani I. K-sign in retrocaecal appendicitis: a case series. Cases J. 2009;2:157.
25. Rothrock SG, Pagane J. Acute appendicitis in children: emergency department diagnosis and management. Ann Emerg Med. 2000;36(1):39-51.
26. Wesson DE. Acute appendicitis in children: clinical manifestations and diagnosis (2010). www .uptodate.com/contents/acute-appendicitis-in-chil dren-clinical-manifestations-and-diagnosis? source=related_link. Accessed December 14, 2011.
27. Becker T, Kharbanda A, Bachur R. Atypical clinical features of pediatric appendicitis. Acad Emerg Med. 2007;14(2):124-129.
28. Laméris W, van Randen A, Go P, et al. Single and combined diagnostic value of clinical features and laboratory tests in acute appendicitis. Acad Emerg Med. 2009;16(9):835-842.
29. McCollough M, Sharieff G. Abdominal pain in children. Pediatr Clin N Am. 2006;53:107-137.
30. Sheu BF, Chiu TF, Chen JC, et al. Risk factors associated with perforated appendicitis in elderly patients presenting with signs and symptoms of acute appendicitis. ANZ J Surg. 2007;77(8):662-666.
31. Borst AR. Acute appendicitis: pregnancy complicates this diagnosis. JAAPA. 2007; 20(12):36-38.
32. Sedlak M, Wagner OJ, Wild B, et al. Is there still a role for rectal examination in suspected appendicitis in adults? Am J Emerg Med. 2008;26 (3):359-377.
33. Ylitalo AW. Digital rectal examination. http://emedicine.medscape.com/article/1948001-overview#a1. Accessed December 14, 2011.
34. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15(5):557-564.
35. Schneider C, Kharbanda A, Bachur R. Evaluating appendicitis scoring systems using a prospective pediatric cohort. Ann Emerg Med. 2007; 49(6):778-784.
36. Kharbanda AB, Taylor GA, Fishman SJ, Bachur RG. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005; 116(3):709–16.
37. Brown JJ, Wilson C, Coleman S, Joypaul BV. Appendicitis in pregnancy. Colorectal Dis. 2009; 11(2):116-122.
38. Richardson E, Paulson C, Hitchcock K. Clinical inquiries. History, exam, and labs: is one enough to diagnose acute adult appendicitis? J Fam Practice. 2007;56(6):474-476.
39. Harrison S, Mahawar K, Brown D, et al. Acute appendicitis presenting as small bowel obstruction: two case reports. Cases J. 2009;2:9106.
40. Pirie J. Management of constipation in the emergency department. Clin Pediatr Emerg Med. 2010;11(3):182-188.
41. Yokota S, Togashi K, Kasahara N, et al. Crohn’s disease confined to the appendix. Gastrointest Endosc. 2010;72(5):1063-1064.
42. Purysko AS, Remer EM, Filho HM, et al. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics. 2011;31(4):927-947.
43. Wang LT, Prentiss KA, Simon JZ, et al. The use of white blood cell count and left shift in the diagnosis of appendicitis in children. Pediatr Emerg Care. 2007;23(2):69-76.
44. Kwan KY, Nager AL. Diagnosing pediatric appendicitis: usefulness of laboratory markers. Am J Emerg Med. 2010;28(9):1009-1015.
45. Yildirim O, Solak C, Koçer B, et al. The role of serum inflammatory markers in acute appendicitis and their success in preventing negative laparotomy. J Invest Surg. 2006;19(6):345-352.
46. Spirt MJ. Complicated intra-abdominal infections: a focus on appendicitis and diverticulitis. Postgrad Med. 2010;122(1):39-51.
47. Pickhardt PJ, Lawrence EM, Pooler D, Bruce RJ. Diagnostic performance of multidetector computed tomography for suspected acute appendicitis. Ann Intern Med. 2011:154(12):789-796.
48. Coursey CA, Nelson RC, Moreno RD, et al. Appendicitis, body mass index, and CT: is CT more valuable for obese patients than thin patients? Am Surg. 2011;77(4):471-475.
49. Petrosyan M, Estrada J, Chan S, et al. CT scan in patients with suspected appendicitis: clinical implications for the acute care surgeon. Eur Surg Res. 2008;40(2):211-219.
50. Huynh V, Lalezarzadeh F, Lawandy S, et al. Abdominal computed tomography in the evaluation of acute and perforated appendicitis in the community setting. Am Surg. 2007;73(10):1002-1005.
51. Fox JC, Solley M, Anderson CL, et al. Prospective evaluation of emergency physician performed bedside ultrasound to detect acute appendicitis. Eur J Emerg Med. 2008;15(2):80-85.
52. Al-Mulhim AS, Nasser MA, Abdullah MM, et al. Emergency laparoscopy for acute abdominal conditions: a prospective study. J Laparoendosc Adv Surg Tech A. 2008;18(4):599-602.
53. Varadhan KK, Humes DJ, Neal KR, Lobo DN. Antibiotic therapy versus appendectomy for acute appendicitis: a meta-analysis. World J Surg. 2010;34(2):199-209.
54. Fitzmaurice GJ, McWilliams B, Hurreiz H, Epanomeritakis E. Antibiotics versus appendectomy in the management of acute appendicitis: a review of the current evidence. Can J Surg. 2011; 54(5):307-314.
55. Ingraham AM, Cohen ME, Bilimoria KY, et al. Comparison of outcomes after laparoscopic versus open appendectomy for acute appendicitis at 222 ACS NSQIP hospitals. Surgery. 2010;148(4): 625-635.
56. Manterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011;(1):CD005660.
57. Puapong D, Lee SL, Haigh PI, et al. Routine interval appendectomy in children is not indicated. J Pediatr Surg. 2007;42(9):1500-1503.
58. Deakin DE, Ahmed I. Interval appendectomy after resolution of adult inflammatory appendix mass: is it necessary? Surgeon. 2007;5(1):45-50.
59. Blakely ML, Williams R, Dassinger MS, et al. Early vs interval appendectomy for children with perforated appendicitis. Arch Surg. 2011;146 (6):660-665.
60. Salkind AR, Rao KC. Antibiotic prophylaxis to prevent surgical site infections. Am Fam Physician. 2011;83(5):585-590.
61. James M. Antibiotics and perioperative infections. Best Pract Res Clin Anaesthesiol. 2008; 22(3):571-584.
62. Bucher BT, Warner BW, Dillon PA. Antibiotic prophylaxis and the prevention of surgical site infection. Curr Opin Pediatr. 2011;23(3):334-338.
63. American Society of Health-Systems Pharmacists. ASHP therapeutic guidelines on antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 1999;56(18):1839-1888.
64. Antimicrobial prophylaxis for surgery. Treat Guidel Med Lett. 2009;7(82):47-52.
65. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133-164.
66. Vons C, Barry C, Maitre S, et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomized controlled trial. Lancet. 2011;377(9777):1573-1579.
67. Hansson J, Körner U, Khorram-Manesh A, et al. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br J Surg. 2009;96(5):473-481.
68. Styrud J, Eriksson S, Nilsson I, et al. Appendectomy versus antibiotic treatment in acute appendicitis: a prospective multicenter randomized control trial. World J Surg. 2006;30(6):1033-1037.
69. Sakorafas GH, Mastoraki A, Lappas C, et al. Conservative treatment of acute appendicitis: heresy or an effective and acceptable alternative to surgery? Eur J Gastroenterol Hepatol. 2011;23 (2):121-127.
1. Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000;215(2):337-348.
2. Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2660 appendicectomy specimens. J Gastroenterol. 2006;41(8):745-749.
3. Bundy DG, Byerley JS, Liles EA, et al. Does this child have appendicitis? JAMA. 2007;298(4):438-451.
4. Alder AC, Fomby TB, Woodward WA, et al. Association of viral infection and appendicitis. Arch Surg. 2010;145(1):63-71.
5. Rubin R. The gastrointestinal tract. In: Rubin R, Strayer DS, eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine. 6th ed. Lippincott, Williams and Wilkins; 2012: 671.
6. McQuaid KR. Gastrointestinal disorders. In: McPhee SJ, Papadakis MA, eds. 2011 Current Medical Diagnosis and Treatment. 50th ed. McGraw Hill; 2011: 606-608.
7. Brennan GD. Pediatric appendicitis: pathophysiology and appropriate use of diagnostic imaging. CJEM. 2006;8(6):425-432.
8. Black C, Martin R. Acute appendicitis in adults: clinical manifestations and diagnosis (2011). www .uptodate.com/contents/acute-appendicitis-in-adults-clinical-manifestations-and-diagnosis. Accessed December 14, 2011.
9. Pittman-Waller VA, Myers JG, Stewart RM, et al. Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies. Am Surg. 2000; 6(66):548-554.
10. Mazuski JE, Solomkin JS. Intra-abdominal infections. Surg Clin North Am. 2009;89(2):421-437.
11. Andersson RE. The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg. 2007;31(1):86-92.
12. Livingston EH, Woodward WA, Sarosi GA, Haley RW. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg. 2007;245(6):886-892.
13. Howell JM, Eddy OL, Lukens TW, et al; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of emergency department patients with suspected appendicitis. Ann Emerg Med. 2010; 55(1):71-116.
14. CDC. Number, rate, and standard error of all-listed surgical and nonsurgical procedures for discharges from short-stay hospitals, by selected procedure categories: United States, 2007. www.cdc
.gov/nchs/data/nhds/4procedures/2009 pro4_num berrate.pdf. Accessed December 14, 2011.
15. Lee SL, Ho HS. Acute appendicitis: is there a difference between children and adults? Am Surg. 2006;5(72):409-413.
16. Bickell NA, Aufses AH Jr, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg. 2006;202(3):401-406.
17. Morrow SE, Newman KD. Current management of appendicitis. Semin Pediatr Surg. 2007; 16(1):34-40.
18. Nance ML, Adamson WT, Hedrick HL. Appendicitis in the young child: a continuing diagnostic challenge. Pediatr Emerg Care. 2000; 16(3):160-162.
19. Feinberg AN, Feinberg LA. The gastrointestinal tract, liver, gallbladder, and pancreas. In: Greydanus D, Feinberg A, Patel D, Homnick D, eds. The Pediatic Diagnostic Examination. McGraw-Hill Professional; 2008:267.
20. Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006;333(7567):530-534.
21. Yale SH, Musana KA. Charles Heber McBurney (1845-1913). Clin Med Res. 2005;3(3):187-189.
22. Murphy JB. Two thousand operations for appendicitis with deductions from his personal experience. Am J Med Sci. 1904;128:187-211.
23. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg. 2004;91(1):28-37.
24. Wani I. K-sign in retrocaecal appendicitis: a case series. Cases J. 2009;2:157.
25. Rothrock SG, Pagane J. Acute appendicitis in children: emergency department diagnosis and management. Ann Emerg Med. 2000;36(1):39-51.
26. Wesson DE. Acute appendicitis in children: clinical manifestations and diagnosis (2010). www .uptodate.com/contents/acute-appendicitis-in-chil dren-clinical-manifestations-and-diagnosis? source=related_link. Accessed December 14, 2011.
27. Becker T, Kharbanda A, Bachur R. Atypical clinical features of pediatric appendicitis. Acad Emerg Med. 2007;14(2):124-129.
28. Laméris W, van Randen A, Go P, et al. Single and combined diagnostic value of clinical features and laboratory tests in acute appendicitis. Acad Emerg Med. 2009;16(9):835-842.
29. McCollough M, Sharieff G. Abdominal pain in children. Pediatr Clin N Am. 2006;53:107-137.
30. Sheu BF, Chiu TF, Chen JC, et al. Risk factors associated with perforated appendicitis in elderly patients presenting with signs and symptoms of acute appendicitis. ANZ J Surg. 2007;77(8):662-666.
31. Borst AR. Acute appendicitis: pregnancy complicates this diagnosis. JAAPA. 2007; 20(12):36-38.
32. Sedlak M, Wagner OJ, Wild B, et al. Is there still a role for rectal examination in suspected appendicitis in adults? Am J Emerg Med. 2008;26 (3):359-377.
33. Ylitalo AW. Digital rectal examination. http://emedicine.medscape.com/article/1948001-overview#a1. Accessed December 14, 2011.
34. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15(5):557-564.
35. Schneider C, Kharbanda A, Bachur R. Evaluating appendicitis scoring systems using a prospective pediatric cohort. Ann Emerg Med. 2007; 49(6):778-784.
36. Kharbanda AB, Taylor GA, Fishman SJ, Bachur RG. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005; 116(3):709–16.
37. Brown JJ, Wilson C, Coleman S, Joypaul BV. Appendicitis in pregnancy. Colorectal Dis. 2009; 11(2):116-122.
38. Richardson E, Paulson C, Hitchcock K. Clinical inquiries. History, exam, and labs: is one enough to diagnose acute adult appendicitis? J Fam Practice. 2007;56(6):474-476.
39. Harrison S, Mahawar K, Brown D, et al. Acute appendicitis presenting as small bowel obstruction: two case reports. Cases J. 2009;2:9106.
40. Pirie J. Management of constipation in the emergency department. Clin Pediatr Emerg Med. 2010;11(3):182-188.
41. Yokota S, Togashi K, Kasahara N, et al. Crohn’s disease confined to the appendix. Gastrointest Endosc. 2010;72(5):1063-1064.
42. Purysko AS, Remer EM, Filho HM, et al. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics. 2011;31(4):927-947.
43. Wang LT, Prentiss KA, Simon JZ, et al. The use of white blood cell count and left shift in the diagnosis of appendicitis in children. Pediatr Emerg Care. 2007;23(2):69-76.
44. Kwan KY, Nager AL. Diagnosing pediatric appendicitis: usefulness of laboratory markers. Am J Emerg Med. 2010;28(9):1009-1015.
45. Yildirim O, Solak C, Koçer B, et al. The role of serum inflammatory markers in acute appendicitis and their success in preventing negative laparotomy. J Invest Surg. 2006;19(6):345-352.
46. Spirt MJ. Complicated intra-abdominal infections: a focus on appendicitis and diverticulitis. Postgrad Med. 2010;122(1):39-51.
47. Pickhardt PJ, Lawrence EM, Pooler D, Bruce RJ. Diagnostic performance of multidetector computed tomography for suspected acute appendicitis. Ann Intern Med. 2011:154(12):789-796.
48. Coursey CA, Nelson RC, Moreno RD, et al. Appendicitis, body mass index, and CT: is CT more valuable for obese patients than thin patients? Am Surg. 2011;77(4):471-475.
49. Petrosyan M, Estrada J, Chan S, et al. CT scan in patients with suspected appendicitis: clinical implications for the acute care surgeon. Eur Surg Res. 2008;40(2):211-219.
50. Huynh V, Lalezarzadeh F, Lawandy S, et al. Abdominal computed tomography in the evaluation of acute and perforated appendicitis in the community setting. Am Surg. 2007;73(10):1002-1005.
51. Fox JC, Solley M, Anderson CL, et al. Prospective evaluation of emergency physician performed bedside ultrasound to detect acute appendicitis. Eur J Emerg Med. 2008;15(2):80-85.
52. Al-Mulhim AS, Nasser MA, Abdullah MM, et al. Emergency laparoscopy for acute abdominal conditions: a prospective study. J Laparoendosc Adv Surg Tech A. 2008;18(4):599-602.
53. Varadhan KK, Humes DJ, Neal KR, Lobo DN. Antibiotic therapy versus appendectomy for acute appendicitis: a meta-analysis. World J Surg. 2010;34(2):199-209.
54. Fitzmaurice GJ, McWilliams B, Hurreiz H, Epanomeritakis E. Antibiotics versus appendectomy in the management of acute appendicitis: a review of the current evidence. Can J Surg. 2011; 54(5):307-314.
55. Ingraham AM, Cohen ME, Bilimoria KY, et al. Comparison of outcomes after laparoscopic versus open appendectomy for acute appendicitis at 222 ACS NSQIP hospitals. Surgery. 2010;148(4): 625-635.
56. Manterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011;(1):CD005660.
57. Puapong D, Lee SL, Haigh PI, et al. Routine interval appendectomy in children is not indicated. J Pediatr Surg. 2007;42(9):1500-1503.
58. Deakin DE, Ahmed I. Interval appendectomy after resolution of adult inflammatory appendix mass: is it necessary? Surgeon. 2007;5(1):45-50.
59. Blakely ML, Williams R, Dassinger MS, et al. Early vs interval appendectomy for children with perforated appendicitis. Arch Surg. 2011;146 (6):660-665.
60. Salkind AR, Rao KC. Antibiotic prophylaxis to prevent surgical site infections. Am Fam Physician. 2011;83(5):585-590.
61. James M. Antibiotics and perioperative infections. Best Pract Res Clin Anaesthesiol. 2008; 22(3):571-584.
62. Bucher BT, Warner BW, Dillon PA. Antibiotic prophylaxis and the prevention of surgical site infection. Curr Opin Pediatr. 2011;23(3):334-338.
63. American Society of Health-Systems Pharmacists. ASHP therapeutic guidelines on antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 1999;56(18):1839-1888.
64. Antimicrobial prophylaxis for surgery. Treat Guidel Med Lett. 2009;7(82):47-52.
65. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133-164.
66. Vons C, Barry C, Maitre S, et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomized controlled trial. Lancet. 2011;377(9777):1573-1579.
67. Hansson J, Körner U, Khorram-Manesh A, et al. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br J Surg. 2009;96(5):473-481.
68. Styrud J, Eriksson S, Nilsson I, et al. Appendectomy versus antibiotic treatment in acute appendicitis: a prospective multicenter randomized control trial. World J Surg. 2006;30(6):1033-1037.
69. Sakorafas GH, Mastoraki A, Lappas C, et al. Conservative treatment of acute appendicitis: heresy or an effective and acceptable alternative to surgery? Eur J Gastroenterol Hepatol. 2011;23 (2):121-127.