User login
In the Literature: February 2010
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura

Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura
Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura
Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
A Case of Shortness of Breath, Abdominal Pain, and Hematuria
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
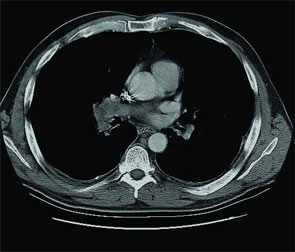
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5

Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.