User login
New topical agents for acne rolling out
WAILEA, HAWAII – The Food and Drug Administration’s approval of adapalene gel 0.1% as an over-the-counter treatment for acne is a potential game changer that could lead to revision of guideline-recommended treatment algorithms, Lawrence F. Eichenfield, MD, predicted at the Hawaii Dermatology Seminar.
In addition to discussing the implications of the FDA’s unprecedented approval of a full prescription–strength topical retinoid for OTC use, he highlighted other developments in topical therapy for acne, including the 2016 approval of dapsone 7.5% gel, as well as several agents with novel mechanisms of action now wending their way through the developmental pipeline.

“This development could be very interesting from an access standpoint and in terms of how physicians write prescriptions for retinoids, in light of the copays for other agents,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego.
“We know that with other retinoids, access is an issue. In Southern California, for example, we have strong pharmacy benefits’ managers for the insurance companies, and they’re very restrictive. It seems like every 3 months, they change the tiering of the different retinoids. It’s something we have to work on to get our patients a fair price,” he explained.
Dapsone 7.5% gel, marketed as Aczone Gel, 7.5% by Allergan, is a once-daily reformulation of the older 5% product administered twice daily. It received FDA approval for use in patients aged 12 years and older based on two 12-week, double-blind, placebo-controlled, randomized trials totaling more than 4,300 acne patients. The studies showed the stronger once-daily product was extremely well tolerated, with application site dryness and itching rates similar to placebo. In terms of efficacy, a Global Acne Assessment Score of 0 or 1 with at least a 2-grade improvement was achieved in 30% of patients assigned to dapsone 7.5% gel, compared with 21% of vehicle-treated controls.
Dr. Eichenfield was lead investigator in a recently published positive phase IIb, randomized, vehicle-controlled study of a topical nitric oxide-releasing agent for acne known for now as SB204 (J Drugs Dermatol. 2016 Dec 1;15[12]:1496-502). The product has both antimicrobial and anti-inflammatory properties, bacteria don’t develop resistance to it, and there is no significant systemic absorption.

“I haven’t seen the data yet. We’ll have to wait and see whether this agent continues to go forward,” Dr. Eichenfield said at the meeting, sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
In its press release, Novan stated that the company believes “its cash on hand is sufficient to fund operations at least through the end of 2017, of which the allocation of capital will be dependent upon further assessment of the SB204 phase III trial results.”
DRM01 is a novel topical inhibitor of acetyl coenzyme-A carboxylase, an enzyme involved in synthesis of the fatty acids that are an essential component of sebum. A phase IIb randomized trial in 420 adult acne patients yielded positive results, according to Dermira, which is developing DRM01. The company plans to begin a pivotal phase III trial in the first half of 2017.
Another investigational topical acne therapy to keep an eye on is cortexolone. This peripherally selective antiandrogenic agent is under development by Cassiopea* Pharmaceuticals.
Dr. Eichenfield’s financial disclosures included serving as an investigator for Novan, Regeneron, Galderma, and Astellas Pharma US; and as a consultant for Galderma, Genentech, Janssen, Lilly, Otsuka, and TopMD.
SDEF and this news organization are owned by the same parent company.
bjancin@frontlinemedcom.com
*An earlier version of this article misstated the company that developed the peripherally selective antiandrogenic agent.
WAILEA, HAWAII – The Food and Drug Administration’s approval of adapalene gel 0.1% as an over-the-counter treatment for acne is a potential game changer that could lead to revision of guideline-recommended treatment algorithms, Lawrence F. Eichenfield, MD, predicted at the Hawaii Dermatology Seminar.
In addition to discussing the implications of the FDA’s unprecedented approval of a full prescription–strength topical retinoid for OTC use, he highlighted other developments in topical therapy for acne, including the 2016 approval of dapsone 7.5% gel, as well as several agents with novel mechanisms of action now wending their way through the developmental pipeline.
“This development could be very interesting from an access standpoint and in terms of how physicians write prescriptions for retinoids, in light of the copays for other agents,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego.
“We know that with other retinoids, access is an issue. In Southern California, for example, we have strong pharmacy benefits’ managers for the insurance companies, and they’re very restrictive. It seems like every 3 months, they change the tiering of the different retinoids. It’s something we have to work on to get our patients a fair price,” he explained.
Dapsone 7.5% gel, marketed as Aczone Gel, 7.5% by Allergan, is a once-daily reformulation of the older 5% product administered twice daily. It received FDA approval for use in patients aged 12 years and older based on two 12-week, double-blind, placebo-controlled, randomized trials totaling more than 4,300 acne patients. The studies showed the stronger once-daily product was extremely well tolerated, with application site dryness and itching rates similar to placebo. In terms of efficacy, a Global Acne Assessment Score of 0 or 1 with at least a 2-grade improvement was achieved in 30% of patients assigned to dapsone 7.5% gel, compared with 21% of vehicle-treated controls.
Dr. Eichenfield was lead investigator in a recently published positive phase IIb, randomized, vehicle-controlled study of a topical nitric oxide-releasing agent for acne known for now as SB204 (J Drugs Dermatol. 2016 Dec 1;15[12]:1496-502). The product has both antimicrobial and anti-inflammatory properties, bacteria don’t develop resistance to it, and there is no significant systemic absorption.
“I haven’t seen the data yet. We’ll have to wait and see whether this agent continues to go forward,” Dr. Eichenfield said at the meeting, sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
In its press release, Novan stated that the company believes “its cash on hand is sufficient to fund operations at least through the end of 2017, of which the allocation of capital will be dependent upon further assessment of the SB204 phase III trial results.”
DRM01 is a novel topical inhibitor of acetyl coenzyme-A carboxylase, an enzyme involved in synthesis of the fatty acids that are an essential component of sebum. A phase IIb randomized trial in 420 adult acne patients yielded positive results, according to Dermira, which is developing DRM01. The company plans to begin a pivotal phase III trial in the first half of 2017.
Another investigational topical acne therapy to keep an eye on is cortexolone. This peripherally selective antiandrogenic agent is under development by Cassiopea* Pharmaceuticals.
Dr. Eichenfield’s financial disclosures included serving as an investigator for Novan, Regeneron, Galderma, and Astellas Pharma US; and as a consultant for Galderma, Genentech, Janssen, Lilly, Otsuka, and TopMD.
SDEF and this news organization are owned by the same parent company.
bjancin@frontlinemedcom.com
*An earlier version of this article misstated the company that developed the peripherally selective antiandrogenic agent.
WAILEA, HAWAII – The Food and Drug Administration’s approval of adapalene gel 0.1% as an over-the-counter treatment for acne is a potential game changer that could lead to revision of guideline-recommended treatment algorithms, Lawrence F. Eichenfield, MD, predicted at the Hawaii Dermatology Seminar.
In addition to discussing the implications of the FDA’s unprecedented approval of a full prescription–strength topical retinoid for OTC use, he highlighted other developments in topical therapy for acne, including the 2016 approval of dapsone 7.5% gel, as well as several agents with novel mechanisms of action now wending their way through the developmental pipeline.
“This development could be very interesting from an access standpoint and in terms of how physicians write prescriptions for retinoids, in light of the copays for other agents,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego.
“We know that with other retinoids, access is an issue. In Southern California, for example, we have strong pharmacy benefits’ managers for the insurance companies, and they’re very restrictive. It seems like every 3 months, they change the tiering of the different retinoids. It’s something we have to work on to get our patients a fair price,” he explained.
Dapsone 7.5% gel, marketed as Aczone Gel, 7.5% by Allergan, is a once-daily reformulation of the older 5% product administered twice daily. It received FDA approval for use in patients aged 12 years and older based on two 12-week, double-blind, placebo-controlled, randomized trials totaling more than 4,300 acne patients. The studies showed the stronger once-daily product was extremely well tolerated, with application site dryness and itching rates similar to placebo. In terms of efficacy, a Global Acne Assessment Score of 0 or 1 with at least a 2-grade improvement was achieved in 30% of patients assigned to dapsone 7.5% gel, compared with 21% of vehicle-treated controls.
Dr. Eichenfield was lead investigator in a recently published positive phase IIb, randomized, vehicle-controlled study of a topical nitric oxide-releasing agent for acne known for now as SB204 (J Drugs Dermatol. 2016 Dec 1;15[12]:1496-502). The product has both antimicrobial and anti-inflammatory properties, bacteria don’t develop resistance to it, and there is no significant systemic absorption.
“I haven’t seen the data yet. We’ll have to wait and see whether this agent continues to go forward,” Dr. Eichenfield said at the meeting, sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
In its press release, Novan stated that the company believes “its cash on hand is sufficient to fund operations at least through the end of 2017, of which the allocation of capital will be dependent upon further assessment of the SB204 phase III trial results.”
DRM01 is a novel topical inhibitor of acetyl coenzyme-A carboxylase, an enzyme involved in synthesis of the fatty acids that are an essential component of sebum. A phase IIb randomized trial in 420 adult acne patients yielded positive results, according to Dermira, which is developing DRM01. The company plans to begin a pivotal phase III trial in the first half of 2017.
Another investigational topical acne therapy to keep an eye on is cortexolone. This peripherally selective antiandrogenic agent is under development by Cassiopea* Pharmaceuticals.
Dr. Eichenfield’s financial disclosures included serving as an investigator for Novan, Regeneron, Galderma, and Astellas Pharma US; and as a consultant for Galderma, Genentech, Janssen, Lilly, Otsuka, and TopMD.
SDEF and this news organization are owned by the same parent company.
bjancin@frontlinemedcom.com
*An earlier version of this article misstated the company that developed the peripherally selective antiandrogenic agent.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
Hypertension risk soars in offspring of early-HT parents
NEW ORLEANS – Young adults whose parents develop hypertension before age 55 years are themselves at sharply increased risk of developing the disease, according to a new report from the Framingham (Mass.) Heart Study.
“Our results demonstrate that early-onset but not late-onset hypertension in parents is a strong risk factor for incident hypertension. It may be important for physicians to distinguish between early- and late-onset hypertension as a familial trait when assessing an individual’s risk for hypertension,” Teemu J. Niiranen, MD, said at the American Heart Association scientific sessions.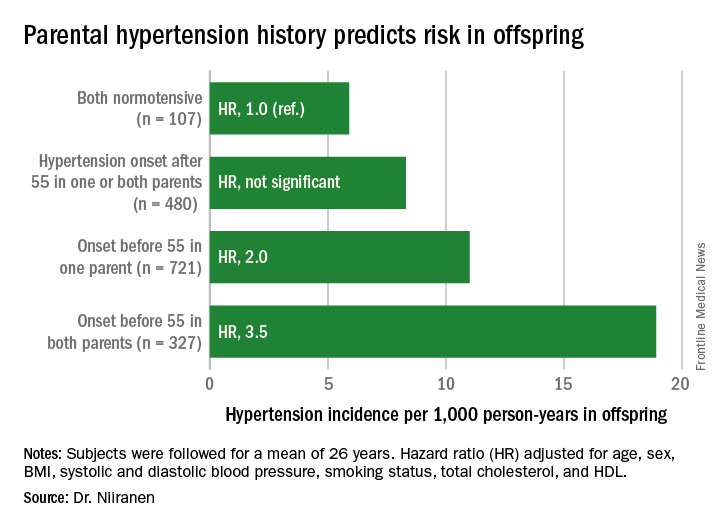
He reported on 1,635 participants in the Offspring cohort of the Framingham Heart Study who were normotensive when they enrolled in the prospective study beginning in 1972. At that time, they averaged 32 years of age. They were followed for a mean of 26 years. Like their parents who enrolled in the Original cohort of the landmark study beginning in 1948, they underwent meticulous blood pressure measurement roughly every 2 years.
Dr. Niiranen and his coinvestigators divided the Offspring cohort into four groups based upon parental hypertension status. There were 107 offspring with normotensive parents, 480 with one or both parents having developed late-onset hypertension after age 55 years, 721 offspring who had one parent with onset of hypertension before age 55 years, and 327 with both parents having early-onset hypertension.
The incidence rate of hypertension in the Offspring cohort climbed in concert with parental early hypertension status. So did the multivariate-adjusted relative risk of the disease, compared with children of normotensive parents.
Moreover, the earlier in life the parents developed hypertension, the earlier their offspring did, too.
Session moderator David J. Maron, MD, of Stanford (Calif.) University, commented, “Everybody’s thinking ‘genetics’ as we look at your findings. But do you have any way to tease out nature versus nurture in understanding the association?”
Dr. Niiranen replied that in a separate study of three generations of Framingham participants, the investigators incorporated two lifestyle factors in their analysis: level of exercise and sodium intake.
“Those didn’t have much effect on the results, so it seems like genetics is driving most of the outcome,” he said.
Dr. Niiranen reported having no financial conflicts of interest regarding his study, sponsored by the National Heart, Lung, and Blood Institute.
NEW ORLEANS – Young adults whose parents develop hypertension before age 55 years are themselves at sharply increased risk of developing the disease, according to a new report from the Framingham (Mass.) Heart Study.
“Our results demonstrate that early-onset but not late-onset hypertension in parents is a strong risk factor for incident hypertension. It may be important for physicians to distinguish between early- and late-onset hypertension as a familial trait when assessing an individual’s risk for hypertension,” Teemu J. Niiranen, MD, said at the American Heart Association scientific sessions.
He reported on 1,635 participants in the Offspring cohort of the Framingham Heart Study who were normotensive when they enrolled in the prospective study beginning in 1972. At that time, they averaged 32 years of age. They were followed for a mean of 26 years. Like their parents who enrolled in the Original cohort of the landmark study beginning in 1948, they underwent meticulous blood pressure measurement roughly every 2 years.
Dr. Niiranen and his coinvestigators divided the Offspring cohort into four groups based upon parental hypertension status. There were 107 offspring with normotensive parents, 480 with one or both parents having developed late-onset hypertension after age 55 years, 721 offspring who had one parent with onset of hypertension before age 55 years, and 327 with both parents having early-onset hypertension.
The incidence rate of hypertension in the Offspring cohort climbed in concert with parental early hypertension status. So did the multivariate-adjusted relative risk of the disease, compared with children of normotensive parents.
Moreover, the earlier in life the parents developed hypertension, the earlier their offspring did, too.
Session moderator David J. Maron, MD, of Stanford (Calif.) University, commented, “Everybody’s thinking ‘genetics’ as we look at your findings. But do you have any way to tease out nature versus nurture in understanding the association?”
Dr. Niiranen replied that in a separate study of three generations of Framingham participants, the investigators incorporated two lifestyle factors in their analysis: level of exercise and sodium intake.
“Those didn’t have much effect on the results, so it seems like genetics is driving most of the outcome,” he said.
Dr. Niiranen reported having no financial conflicts of interest regarding his study, sponsored by the National Heart, Lung, and Blood Institute.
NEW ORLEANS – Young adults whose parents develop hypertension before age 55 years are themselves at sharply increased risk of developing the disease, according to a new report from the Framingham (Mass.) Heart Study.
“Our results demonstrate that early-onset but not late-onset hypertension in parents is a strong risk factor for incident hypertension. It may be important for physicians to distinguish between early- and late-onset hypertension as a familial trait when assessing an individual’s risk for hypertension,” Teemu J. Niiranen, MD, said at the American Heart Association scientific sessions.
He reported on 1,635 participants in the Offspring cohort of the Framingham Heart Study who were normotensive when they enrolled in the prospective study beginning in 1972. At that time, they averaged 32 years of age. They were followed for a mean of 26 years. Like their parents who enrolled in the Original cohort of the landmark study beginning in 1948, they underwent meticulous blood pressure measurement roughly every 2 years.
Dr. Niiranen and his coinvestigators divided the Offspring cohort into four groups based upon parental hypertension status. There were 107 offspring with normotensive parents, 480 with one or both parents having developed late-onset hypertension after age 55 years, 721 offspring who had one parent with onset of hypertension before age 55 years, and 327 with both parents having early-onset hypertension.
The incidence rate of hypertension in the Offspring cohort climbed in concert with parental early hypertension status. So did the multivariate-adjusted relative risk of the disease, compared with children of normotensive parents.
Moreover, the earlier in life the parents developed hypertension, the earlier their offspring did, too.
Session moderator David J. Maron, MD, of Stanford (Calif.) University, commented, “Everybody’s thinking ‘genetics’ as we look at your findings. But do you have any way to tease out nature versus nurture in understanding the association?”
Dr. Niiranen replied that in a separate study of three generations of Framingham participants, the investigators incorporated two lifestyle factors in their analysis: level of exercise and sodium intake.
“Those didn’t have much effect on the results, so it seems like genetics is driving most of the outcome,” he said.
Dr. Niiranen reported having no financial conflicts of interest regarding his study, sponsored by the National Heart, Lung, and Blood Institute.
Key clinical point:
Major finding: Young adults with two parents who developed hypertension before age 55 years are at 3.5-fold greater risk of subsequently developing hypertension than if both parents were normotensive.
Data source: This was an analysis of the incidence of hypertension during a mean prospective follow-up of 26 years in 1,635 members of the Offspring cohort of the Framingham Heart Study who enrolled as young adults.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study sponsored by the National Heart, Lung, and Blood Institute.
STICHES boosts CABG role in severe LV dysfunction
SNOWMASS, COLO. – Coronary artery bypass graft surgery in patients with severe ischemic left ventricular dysfunction is overdue for an upgrade in status in the American College of Cardiology/American Heart Association guidelines on the strength of the landmark STICH trial and its extended follow-up stage known as STICHES, according to Vinod H. Thourani, MD.
Currently, the guidelines give CABG in this large and growing population a class IIb recommendation, meaning it “might be considered.” This undervalues the study’s core lesson: “STICHES showed a clear survival benefit with CABG, so this most likely should become a class IIa recommendation,” Dr. Thourani said at the Annual Cardiovascular Conference at Snowmass.
He went on to describe how he applies the key study findings to individual patients.

At 5 and 10 years of follow-up, the probability of all-cause mortality was reduced by 14% and 16%, respectively, in the CABG group. The surgery provided on average an 18-month extension of life. The price paid for the CABG benefit was a 3.6% mortality rate at 30 days; however, this was overcome by the 2-year mark, at which point survival in the CABG group surpassed that in controls. Thereafter, the all-cause mortality gap between the two groups continued to widen for the duration of follow-up.
For the composite endpoint of all-cause mortality or cardiovascular hospitalization, the CABG group enjoyed a 26% relative risk reduction, compared with optimal medical management alone at 5 years, and a 28% reduction in risk at 10 years. The two study groups diverged in terms of risk of cardiovascular hospitalization after only 3 months.
CABG provided a reduction in the risk of cardiovascular death that was consistent across all ages. In contrast, the reduction in all-cause mortality was not, since a higher proportion of deaths in older patients came from cancer and other noncardiovascular causes (Circulation. 2016 Nov 1;134[18]:1314-24).
There have been no randomized, controlled trials of percutaneous coronary intervention in patients with heart failure.
“An interesting finding in STICHES was that medical therapy had a much higher 10-year all-cause mortality the younger the patient was. So CABG particularly benefits those who are at a younger age – in this study, age 60 or less. As you get older, say, at 80 years of age, I’m not sure there’s a huge benefit in all-cause mortality at that point,” said Dr. Thourani, professor of surgery and medicine, and codirector of the structural heart and valve center at Emory University in Atlanta.
In a STICH substudy, roughly half of participants underwent presurgical myocardial viability testing via single-photon emission CT and/or dobutamine echocardiography. The investigators found that the results didn’t predict mortality benefit for CABG (N Engl J Med. 2011 Apr 28;364[17]:1617-25).
More recently, however, other investigators have reported MRI to have prognostic value. For example, Belgian investigators showed that medical therapy in patients with ischemic heart failure and dysfunctional but viable myocardium on delayed-enhanced MRI was associated with a 4.56-fold increased likelihood of mortality during 3 years of follow-up, compared with complete revascularization via CABG (J Am Coll Cardiol. 2012 Feb 28;59[9]:825-35).
“This observation has been useful for me,” Dr. Thourani said. “My own personal practice is if I have good targets, I don’t do viability testing, but if I have really bad targets where I know I’m going to have a tough time sewing grafts, I try to get an MRI for viability testing.”
One important lesson of STICH is that all patients with heart failure and a low left ventricular ejection fraction should have a coronary angiogram, even if they are free of ischemia on noninvasive testing and have no angina. That’s because the patients enrolled in STICH had little or no angina, the surgeon continued.
These STICH-type patients will benefit greatly from a heart team assessment factoring in an individual’s Society of Thoracic Surgeons’ predicted risk score, based on age, comorbidities, and other factors. For example, if a patient’s STS risk score with CABG is 0.7%, that’s a strong argument for opting for the surgery, since the 30-day operative mortality in STICH was 3.6%. If, on the other hand, the STS score is greater than 7%, that’s a tougher call.
“I think it’s really important that a heart team assessment includes a noninvasive cardiologist as well as an interventional cardiologist and cardiac surgeon because I think interventionalists and cardiac surgeons sometimes get a little goofy in their assessment of these patients,” Dr. Thourani said.
Patients with a low ejection fraction and coronary artery disease who are deemed poor candidates for CABG should be evaluated for a mechanical circulatory support device or a heart transplant.
“I think that’s something we don’t think about enough, quite honestly,” he said.
Dr. Thourani reported serving as a consultant to Abbott Vascular, Edwards Lifesciences, and Gore, and receiving research grants from numerous companies.
SNOWMASS, COLO. – Coronary artery bypass graft surgery in patients with severe ischemic left ventricular dysfunction is overdue for an upgrade in status in the American College of Cardiology/American Heart Association guidelines on the strength of the landmark STICH trial and its extended follow-up stage known as STICHES, according to Vinod H. Thourani, MD.
Currently, the guidelines give CABG in this large and growing population a class IIb recommendation, meaning it “might be considered.” This undervalues the study’s core lesson: “STICHES showed a clear survival benefit with CABG, so this most likely should become a class IIa recommendation,” Dr. Thourani said at the Annual Cardiovascular Conference at Snowmass.
He went on to describe how he applies the key study findings to individual patients.
At 5 and 10 years of follow-up, the probability of all-cause mortality was reduced by 14% and 16%, respectively, in the CABG group. The surgery provided on average an 18-month extension of life. The price paid for the CABG benefit was a 3.6% mortality rate at 30 days; however, this was overcome by the 2-year mark, at which point survival in the CABG group surpassed that in controls. Thereafter, the all-cause mortality gap between the two groups continued to widen for the duration of follow-up.
For the composite endpoint of all-cause mortality or cardiovascular hospitalization, the CABG group enjoyed a 26% relative risk reduction, compared with optimal medical management alone at 5 years, and a 28% reduction in risk at 10 years. The two study groups diverged in terms of risk of cardiovascular hospitalization after only 3 months.
CABG provided a reduction in the risk of cardiovascular death that was consistent across all ages. In contrast, the reduction in all-cause mortality was not, since a higher proportion of deaths in older patients came from cancer and other noncardiovascular causes (Circulation. 2016 Nov 1;134[18]:1314-24).
There have been no randomized, controlled trials of percutaneous coronary intervention in patients with heart failure.
“An interesting finding in STICHES was that medical therapy had a much higher 10-year all-cause mortality the younger the patient was. So CABG particularly benefits those who are at a younger age – in this study, age 60 or less. As you get older, say, at 80 years of age, I’m not sure there’s a huge benefit in all-cause mortality at that point,” said Dr. Thourani, professor of surgery and medicine, and codirector of the structural heart and valve center at Emory University in Atlanta.
In a STICH substudy, roughly half of participants underwent presurgical myocardial viability testing via single-photon emission CT and/or dobutamine echocardiography. The investigators found that the results didn’t predict mortality benefit for CABG (N Engl J Med. 2011 Apr 28;364[17]:1617-25).
More recently, however, other investigators have reported MRI to have prognostic value. For example, Belgian investigators showed that medical therapy in patients with ischemic heart failure and dysfunctional but viable myocardium on delayed-enhanced MRI was associated with a 4.56-fold increased likelihood of mortality during 3 years of follow-up, compared with complete revascularization via CABG (J Am Coll Cardiol. 2012 Feb 28;59[9]:825-35).
“This observation has been useful for me,” Dr. Thourani said. “My own personal practice is if I have good targets, I don’t do viability testing, but if I have really bad targets where I know I’m going to have a tough time sewing grafts, I try to get an MRI for viability testing.”
One important lesson of STICH is that all patients with heart failure and a low left ventricular ejection fraction should have a coronary angiogram, even if they are free of ischemia on noninvasive testing and have no angina. That’s because the patients enrolled in STICH had little or no angina, the surgeon continued.
These STICH-type patients will benefit greatly from a heart team assessment factoring in an individual’s Society of Thoracic Surgeons’ predicted risk score, based on age, comorbidities, and other factors. For example, if a patient’s STS risk score with CABG is 0.7%, that’s a strong argument for opting for the surgery, since the 30-day operative mortality in STICH was 3.6%. If, on the other hand, the STS score is greater than 7%, that’s a tougher call.
“I think it’s really important that a heart team assessment includes a noninvasive cardiologist as well as an interventional cardiologist and cardiac surgeon because I think interventionalists and cardiac surgeons sometimes get a little goofy in their assessment of these patients,” Dr. Thourani said.
Patients with a low ejection fraction and coronary artery disease who are deemed poor candidates for CABG should be evaluated for a mechanical circulatory support device or a heart transplant.
“I think that’s something we don’t think about enough, quite honestly,” he said.
Dr. Thourani reported serving as a consultant to Abbott Vascular, Edwards Lifesciences, and Gore, and receiving research grants from numerous companies.
SNOWMASS, COLO. – Coronary artery bypass graft surgery in patients with severe ischemic left ventricular dysfunction is overdue for an upgrade in status in the American College of Cardiology/American Heart Association guidelines on the strength of the landmark STICH trial and its extended follow-up stage known as STICHES, according to Vinod H. Thourani, MD.
Currently, the guidelines give CABG in this large and growing population a class IIb recommendation, meaning it “might be considered.” This undervalues the study’s core lesson: “STICHES showed a clear survival benefit with CABG, so this most likely should become a class IIa recommendation,” Dr. Thourani said at the Annual Cardiovascular Conference at Snowmass.
He went on to describe how he applies the key study findings to individual patients.
At 5 and 10 years of follow-up, the probability of all-cause mortality was reduced by 14% and 16%, respectively, in the CABG group. The surgery provided on average an 18-month extension of life. The price paid for the CABG benefit was a 3.6% mortality rate at 30 days; however, this was overcome by the 2-year mark, at which point survival in the CABG group surpassed that in controls. Thereafter, the all-cause mortality gap between the two groups continued to widen for the duration of follow-up.
For the composite endpoint of all-cause mortality or cardiovascular hospitalization, the CABG group enjoyed a 26% relative risk reduction, compared with optimal medical management alone at 5 years, and a 28% reduction in risk at 10 years. The two study groups diverged in terms of risk of cardiovascular hospitalization after only 3 months.
CABG provided a reduction in the risk of cardiovascular death that was consistent across all ages. In contrast, the reduction in all-cause mortality was not, since a higher proportion of deaths in older patients came from cancer and other noncardiovascular causes (Circulation. 2016 Nov 1;134[18]:1314-24).
There have been no randomized, controlled trials of percutaneous coronary intervention in patients with heart failure.
“An interesting finding in STICHES was that medical therapy had a much higher 10-year all-cause mortality the younger the patient was. So CABG particularly benefits those who are at a younger age – in this study, age 60 or less. As you get older, say, at 80 years of age, I’m not sure there’s a huge benefit in all-cause mortality at that point,” said Dr. Thourani, professor of surgery and medicine, and codirector of the structural heart and valve center at Emory University in Atlanta.
In a STICH substudy, roughly half of participants underwent presurgical myocardial viability testing via single-photon emission CT and/or dobutamine echocardiography. The investigators found that the results didn’t predict mortality benefit for CABG (N Engl J Med. 2011 Apr 28;364[17]:1617-25).
More recently, however, other investigators have reported MRI to have prognostic value. For example, Belgian investigators showed that medical therapy in patients with ischemic heart failure and dysfunctional but viable myocardium on delayed-enhanced MRI was associated with a 4.56-fold increased likelihood of mortality during 3 years of follow-up, compared with complete revascularization via CABG (J Am Coll Cardiol. 2012 Feb 28;59[9]:825-35).
“This observation has been useful for me,” Dr. Thourani said. “My own personal practice is if I have good targets, I don’t do viability testing, but if I have really bad targets where I know I’m going to have a tough time sewing grafts, I try to get an MRI for viability testing.”
One important lesson of STICH is that all patients with heart failure and a low left ventricular ejection fraction should have a coronary angiogram, even if they are free of ischemia on noninvasive testing and have no angina. That’s because the patients enrolled in STICH had little or no angina, the surgeon continued.
These STICH-type patients will benefit greatly from a heart team assessment factoring in an individual’s Society of Thoracic Surgeons’ predicted risk score, based on age, comorbidities, and other factors. For example, if a patient’s STS risk score with CABG is 0.7%, that’s a strong argument for opting for the surgery, since the 30-day operative mortality in STICH was 3.6%. If, on the other hand, the STS score is greater than 7%, that’s a tougher call.
“I think it’s really important that a heart team assessment includes a noninvasive cardiologist as well as an interventional cardiologist and cardiac surgeon because I think interventionalists and cardiac surgeons sometimes get a little goofy in their assessment of these patients,” Dr. Thourani said.
Patients with a low ejection fraction and coronary artery disease who are deemed poor candidates for CABG should be evaluated for a mechanical circulatory support device or a heart transplant.
“I think that’s something we don’t think about enough, quite honestly,” he said.
Dr. Thourani reported serving as a consultant to Abbott Vascular, Edwards Lifesciences, and Gore, and receiving research grants from numerous companies.
EXPERT ANALYSIS AT THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Experts say don’t SPRINT to adopt low blood pressure target
NEW ORLEANS – The key message of the SPRINT trial – that aggressive antihypertensive therapy to a target systolic blood pressure (SBP) of less than 120 mm Hg reduces all-cause mortality, compared with a target SBP under 140 mm Hg – is not broadly applicable as a routine strategy in managing hypertension, experts declared at the American Heart Association scientific sessions.
“My concern is that the patients in the SPRINT trial ended up being highly selected for having a strong ability to achieve and tolerate being at systolic blood pressure levels that we generally don’t see in a lot of treated hypertensives today in this country,” cautioned Peter M. Okin, MD, of Columbia University, New York.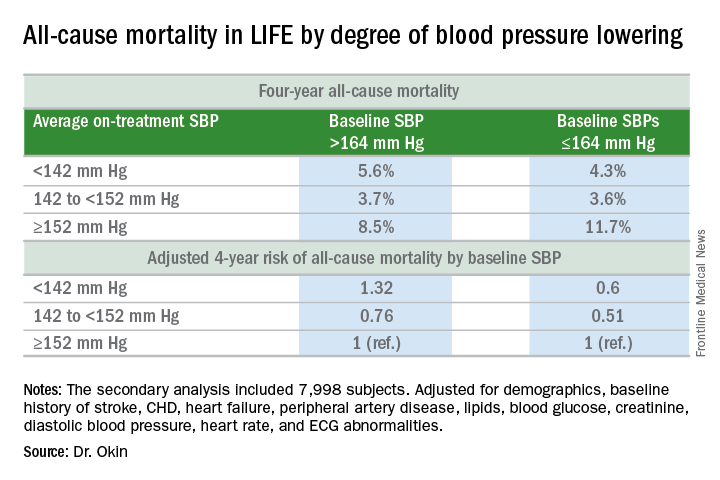
It will be interesting to see how Dr. Okin’s opinion, which is shared by many leading cardiologists, is addressed in new hypertension treatment guidelines from the American College of Cardiology and the American Heart Association. The guidelines are anticipated in March.
Dr. Okin presented a secondary analysis of the earlier landmark LIFE (Losartan Intervention for Endpoint Reduction in Hypertension) trial that’s diametrically at odds with the main finding in SPRINT (the Systolic Blood Pressure Intervention Trial): namely, in LIFE (Lancet. 2002 Mar 23;359[9311]:1004-10), all-cause mortality during follow-up was heavily dependent upon baseline blood pressure.
Among LIFE participants with a baseline SBP below 164 mm Hg, achievement of an average on-treatment SBP below 142 mm Hg was associated with a 40% reduction in all-cause mortality more than 4 years of follow-up, compared with those with an achieved SBP of 152 mm Hg or more. In contrast, LIFE subjects whose baseline SBP was greater than 164 mm Hg actually had a 32% increase in all-cause mortality if their achieved SBP was less than 142 mm Hg, compared with those whose average on-treatment SBP was 152 mm Hg or higher.
How to account for the disparate results of LIFE and SPRINT?
SPRINT (N Engl J Med. 2015 Nov 26; 373:2103-16) enrolled nondiabetic patients aged 50 years or older who had an SBP of 130 mm Hg or more and high cardiovascular risk, with a 10-year Framingham Risk Score greater than 15%. But because the SBP threshold for entry was set so low, at 130 mm Hg, roughly half of SPRINT participants had baseline SBP levels that were already at or below the standard treatment target of 140 mm Hg. For those patients, getting to roughly 120 mm Hg on treatment wasn’t all that big a stretch in terms of the magnitude of blood pressure reduction, Dr. Okin said.
“Our analysis doesn’t invalidate SPRINT in any way, shape, or fashion. It just gives us some pause for thought,” he added.
His post-hoc analysis of LIFE was restricted to the 7,998 participants without diabetes at baseline, since SPRINT excluded diabetics from enrollment.
Audience comments were split between cardiologists who consider SPRINT a game-changer in the treatment of hypertension and those who, like Dr. Okin, have reservations. Among those reservations was the unexpected and difficult-to-explain finding that aggressive SBP lowering didn’t reduce the risk of stroke, compared with less-intensive SBP lowering, unlike the case in other clinical trials and epidemiologic studies in hypertension. Also, audience members took issue with the fact that blood pressure measurements in SPRINT weren’t done in the standard office measurement way employed in other major trials. Instead, SPRINT relied upon automated blood pressure monitoring of a patient alone in a room, which several cardiologists in the audience thought might have skewed the study results, since automated measurements tend to run lower.
Elsewhere at the AHA meeting, former AHA president Clyde W. Yancy, MD, offered a cautionary note regarding SPRINT.
“I think it’s important that we emphasize to this audience that SPRINT is looking at a very select patient population that probably describes only 15% of those with hypertension, specifically those with very high cardiovascular disease risk profiles. So we have to be very careful when we take the blood pressure targets that were identified in SPRINT and try to extrapolate those to other populations,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University, Chicago.
Dr. Okin reported having no financial conflicts of interest.
NEW ORLEANS – The key message of the SPRINT trial – that aggressive antihypertensive therapy to a target systolic blood pressure (SBP) of less than 120 mm Hg reduces all-cause mortality, compared with a target SBP under 140 mm Hg – is not broadly applicable as a routine strategy in managing hypertension, experts declared at the American Heart Association scientific sessions.
“My concern is that the patients in the SPRINT trial ended up being highly selected for having a strong ability to achieve and tolerate being at systolic blood pressure levels that we generally don’t see in a lot of treated hypertensives today in this country,” cautioned Peter M. Okin, MD, of Columbia University, New York.
It will be interesting to see how Dr. Okin’s opinion, which is shared by many leading cardiologists, is addressed in new hypertension treatment guidelines from the American College of Cardiology and the American Heart Association. The guidelines are anticipated in March.
Dr. Okin presented a secondary analysis of the earlier landmark LIFE (Losartan Intervention for Endpoint Reduction in Hypertension) trial that’s diametrically at odds with the main finding in SPRINT (the Systolic Blood Pressure Intervention Trial): namely, in LIFE (Lancet. 2002 Mar 23;359[9311]:1004-10), all-cause mortality during follow-up was heavily dependent upon baseline blood pressure.
Among LIFE participants with a baseline SBP below 164 mm Hg, achievement of an average on-treatment SBP below 142 mm Hg was associated with a 40% reduction in all-cause mortality more than 4 years of follow-up, compared with those with an achieved SBP of 152 mm Hg or more. In contrast, LIFE subjects whose baseline SBP was greater than 164 mm Hg actually had a 32% increase in all-cause mortality if their achieved SBP was less than 142 mm Hg, compared with those whose average on-treatment SBP was 152 mm Hg or higher.
How to account for the disparate results of LIFE and SPRINT?
SPRINT (N Engl J Med. 2015 Nov 26; 373:2103-16) enrolled nondiabetic patients aged 50 years or older who had an SBP of 130 mm Hg or more and high cardiovascular risk, with a 10-year Framingham Risk Score greater than 15%. But because the SBP threshold for entry was set so low, at 130 mm Hg, roughly half of SPRINT participants had baseline SBP levels that were already at or below the standard treatment target of 140 mm Hg. For those patients, getting to roughly 120 mm Hg on treatment wasn’t all that big a stretch in terms of the magnitude of blood pressure reduction, Dr. Okin said.
“Our analysis doesn’t invalidate SPRINT in any way, shape, or fashion. It just gives us some pause for thought,” he added.
His post-hoc analysis of LIFE was restricted to the 7,998 participants without diabetes at baseline, since SPRINT excluded diabetics from enrollment.
Audience comments were split between cardiologists who consider SPRINT a game-changer in the treatment of hypertension and those who, like Dr. Okin, have reservations. Among those reservations was the unexpected and difficult-to-explain finding that aggressive SBP lowering didn’t reduce the risk of stroke, compared with less-intensive SBP lowering, unlike the case in other clinical trials and epidemiologic studies in hypertension. Also, audience members took issue with the fact that blood pressure measurements in SPRINT weren’t done in the standard office measurement way employed in other major trials. Instead, SPRINT relied upon automated blood pressure monitoring of a patient alone in a room, which several cardiologists in the audience thought might have skewed the study results, since automated measurements tend to run lower.
Elsewhere at the AHA meeting, former AHA president Clyde W. Yancy, MD, offered a cautionary note regarding SPRINT.
“I think it’s important that we emphasize to this audience that SPRINT is looking at a very select patient population that probably describes only 15% of those with hypertension, specifically those with very high cardiovascular disease risk profiles. So we have to be very careful when we take the blood pressure targets that were identified in SPRINT and try to extrapolate those to other populations,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University, Chicago.
Dr. Okin reported having no financial conflicts of interest.
NEW ORLEANS – The key message of the SPRINT trial – that aggressive antihypertensive therapy to a target systolic blood pressure (SBP) of less than 120 mm Hg reduces all-cause mortality, compared with a target SBP under 140 mm Hg – is not broadly applicable as a routine strategy in managing hypertension, experts declared at the American Heart Association scientific sessions.
“My concern is that the patients in the SPRINT trial ended up being highly selected for having a strong ability to achieve and tolerate being at systolic blood pressure levels that we generally don’t see in a lot of treated hypertensives today in this country,” cautioned Peter M. Okin, MD, of Columbia University, New York.
It will be interesting to see how Dr. Okin’s opinion, which is shared by many leading cardiologists, is addressed in new hypertension treatment guidelines from the American College of Cardiology and the American Heart Association. The guidelines are anticipated in March.
Dr. Okin presented a secondary analysis of the earlier landmark LIFE (Losartan Intervention for Endpoint Reduction in Hypertension) trial that’s diametrically at odds with the main finding in SPRINT (the Systolic Blood Pressure Intervention Trial): namely, in LIFE (Lancet. 2002 Mar 23;359[9311]:1004-10), all-cause mortality during follow-up was heavily dependent upon baseline blood pressure.
Among LIFE participants with a baseline SBP below 164 mm Hg, achievement of an average on-treatment SBP below 142 mm Hg was associated with a 40% reduction in all-cause mortality more than 4 years of follow-up, compared with those with an achieved SBP of 152 mm Hg or more. In contrast, LIFE subjects whose baseline SBP was greater than 164 mm Hg actually had a 32% increase in all-cause mortality if their achieved SBP was less than 142 mm Hg, compared with those whose average on-treatment SBP was 152 mm Hg or higher.
How to account for the disparate results of LIFE and SPRINT?
SPRINT (N Engl J Med. 2015 Nov 26; 373:2103-16) enrolled nondiabetic patients aged 50 years or older who had an SBP of 130 mm Hg or more and high cardiovascular risk, with a 10-year Framingham Risk Score greater than 15%. But because the SBP threshold for entry was set so low, at 130 mm Hg, roughly half of SPRINT participants had baseline SBP levels that were already at or below the standard treatment target of 140 mm Hg. For those patients, getting to roughly 120 mm Hg on treatment wasn’t all that big a stretch in terms of the magnitude of blood pressure reduction, Dr. Okin said.
“Our analysis doesn’t invalidate SPRINT in any way, shape, or fashion. It just gives us some pause for thought,” he added.
His post-hoc analysis of LIFE was restricted to the 7,998 participants without diabetes at baseline, since SPRINT excluded diabetics from enrollment.
Audience comments were split between cardiologists who consider SPRINT a game-changer in the treatment of hypertension and those who, like Dr. Okin, have reservations. Among those reservations was the unexpected and difficult-to-explain finding that aggressive SBP lowering didn’t reduce the risk of stroke, compared with less-intensive SBP lowering, unlike the case in other clinical trials and epidemiologic studies in hypertension. Also, audience members took issue with the fact that blood pressure measurements in SPRINT weren’t done in the standard office measurement way employed in other major trials. Instead, SPRINT relied upon automated blood pressure monitoring of a patient alone in a room, which several cardiologists in the audience thought might have skewed the study results, since automated measurements tend to run lower.
Elsewhere at the AHA meeting, former AHA president Clyde W. Yancy, MD, offered a cautionary note regarding SPRINT.
“I think it’s important that we emphasize to this audience that SPRINT is looking at a very select patient population that probably describes only 15% of those with hypertension, specifically those with very high cardiovascular disease risk profiles. So we have to be very careful when we take the blood pressure targets that were identified in SPRINT and try to extrapolate those to other populations,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University, Chicago.
Dr. Okin reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
Multivessel PCI in STEMI gains traction
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.

Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.
Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
SNOWMASS, COLO. – The tide appears to have turned regarding the merits of percutaneous coronary intervention in non-infarct-related arteries in conjunction with primary PCI for ST-elevation MI in patients with multivessel disease, Douglas E. Drachman, MD, said at the Annual Cardiovascular Conference at Snowmass.
Previously, multivessel PCI in STEMI patients who are hemodynamically stable was believed harmful and was given a Class IIIb recommendation – meaning don’t do it – in the 2013 American College of Cardiology/American Heart Association STEMI guidelines. Just 2 years later, however, new evidence in the form of three randomized trials prompted a focused update of the joint guidelines in which the practice was upgraded to Class IIb status, meaning it could be considered and may be beneficial.
Roughly 50% of STEMI patients have significant lesions in non-infarct-related arteries (non-IRA). The question of how best to treat such patients is an important one because multivessel coronary disease in STEMI is associated with increased risks of both reinfarction and mortality, noted Dr. Drachman, an interventional cardiologist at Massachusetts General Hospital in Boston.
He offered several reasons why the findings of the three influential randomized trials differed from earlier negative retrospective observational studies: “I would argue there’s been significant improvement in our technique in doing PCI. We’re primarily doing transradial interventions now for our patients, so the risk associated with multiple accesses is reduced. Our ability to use more potent antithrombotic strategies is enhanced by our concern about bleeding risk. And the stent platforms that we use in our interventional strategies have improved to the point that we are tackling ever more challenging lesions with greater aplomb and less concern that we may cause harm. I think all these factors have enhanced the ability of the interventionalist to select and treat non-IRAs in a staged fashion and be less parsimonious at the point of care.”
The remaining questions are which non-IRA lesions should be treated, in whom, when relative to primary PCI, and what are the cost implications? These issues are being tackled in at least eight active randomized controlled trials. Depending upon the answers to come, multivessel PCI in STEMI patients could receive a further upgrade in the guidelines.
Since release of the 2015 focused guideline update, several large studies have provided further backing for multivessel PCI in STEMI patients with significant multivessel disease, although these weren’t randomized prospective studies and hence must be considered hypothesis-generating.
One of these major pieces of evidence was a meta-analysis of observational studies led by Eric R. Bates, MD, professor of internal medicine at the University of Michigan in Ann Arbor. He and his coinvestigators analyzed studies comparing culprit vessel-only primary PCI for STEMI patients with multivessel disease versus staged PCI in which primary PCI was done first, followed by PCI of a non-infarct-related vessel later during the same hospitalization or soon after. Staged PCI was the clear winner, with a 2.2-fold greater likelihood of freedom from mortality (J Am Coll Cardiol. 2016 Sep 6;68(10):1066-81).
When the investigators compared studies of staged PCI versus multivessel PCI in the same session as primary PCI, staged PCI was again the clear winner, with a 4-fold greater freedom from mortality.
Among the possible risks of performing PCI of a non-IRA in the same session as primary PCI are increased risks of thrombosis, contrast-induced nephropathy, stent undersizing due to vasospasm, and unintended jeopardy of distant viable myocardium due to microembolization or side branch occlusion, Dr. Drachman said.
“Maybe in certain circumstances it’s best to let the dust settle after the urgent vessel intervention. Wait a couple of days and then make your plan,” the cardiologist advised.
Another informative recent piece of evidence was provided by a Canadian retrospective observational study which compared revascularization strategies in 6,503 consecutive STEMI patients with multivessel disease. Staged multivessel PCI during the index hospitalization was performed in 658 patients, multivessel PCI during the primary PCI session in 1,325, and PCI limited to the infarct-related artery in 4,520. The study endpoints were 2-year all-cause mortality and repeat revascularization.
Staged multivessel PCI had the lowest mortality and repeat revascularization rates. The 2-year mortality rate associated with this strategy was 45% less than with multivessel intervention at the time of primary PCI and 35% lower than for culprit vessel-only PCI, which unsurprisingly had the highest repeat revascularization rate (JACC Cardiovasc Interv. 2017 Jan 9;10(1):11-23).
The first of the three randomized trials that led to a change in the guidelines was the UK PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction). It showed at a mean 23-months followup that STEMI patients with multivessel disease had a 65% reduction in the relative risk of a composite endoint of cardiovascular death, MI, or refractory angina if they received non-IRA PCI at the same time as primary PCI compared with PCI limited to the IRA (N Engl J Med. 2013 Sep 19;369(12):1115-23).
Next came another UK trial: CvLPRIT (Complete vs. Culprit-Lesion Only Primary PCI) demonstrated a 65% reduction in the composite 12-month outcome of all-cause mortality, MI, heart failure, or ischemia-driven PCI with staged PCI during the index hospitalization compared with culprit vessel-only PCI (J Am Coll Cardiol. 2015 Mar 17;65(10):963-72).
Finally, DANAMI-3-PRIMULTI (the Third Danish Study of Optimal Acute Treatment of Patients with STEMI: Primary PCI in Multivessel Disease) showed a dramatic reduction in the risk of ischemia-driven PCI during a median 27 months of followup in patients who underwent staged multivessel PCI guided by the findings of fractional flow reserve measurement compared with primary PCI limited to the IRA (Lancet. 2015 Aug 15;386(9994):665-71). However, fractional flow reserve-guided multivessel PCI didn’t decrease the risk of death or nonfatal recurrent MI, leaving its role unsettled pending the results of ongoing clinical trials.
Dr. Drachman said it’s clear certain STEMI patients should not undergo non-IRA PCI. These include anyone in whom the procedure would be lengthy due to vessel tortuosity or chronic total occlusion, as well as patients with stable saphenous vein graft disease or heavily calcified lesions requiring atherectomy, since multivessel PCI in those settings would pose a high risk for additional left ventricular dysfunction.
“Be thoughtful about patients who have renal dysfunction,” he added.
Dr. Drachman reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
New thinking on septal myectomy vs. alcohol ablation for obstructive cardiomyopathy
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
SNOWMASS, COLO. – The first-ever national study of the impact of hospital volume on outcomes of septal myectomy versus alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy deserves to be practice-changing, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
Prior to release of these eye-opening data, conventional thinking held that referral for percutaneous septal ablation was the preferred option for elderly, sedentary patients with lots of comorbid conditions and a limited remaining lifespan, while surgical septal myectomy was the best fix for young, active, relatively healthy patients because of its impressive durability of benefit.
Similarly, 80% of alcohol ablations took place at centers doing less than 20 cases over 9 years. But the success of the percutaneous procedure was less dependent upon large institutional volumes. Only at the lowest-volume centers, where a total of fewer than 10 of the procedures were done over 9 years, was procedural mortality significantly higher – indeed, three- to fourfold higher – than at mid- or high-volume institutions or centers of excellence, all of which had similar mortality rates. The same was true for rates of postoperative complete heart block requiring a permanent pacemaker: significantly higher only at the lowest-volume institutions, according to the investigators from Weill Cornell Medical College in New York (JAMA Cardiol. 2016 Jun 1;1[3]:324-32).
“I think the bottom line is this: for the patient who is severely symptomatic with obstruction on optimal medical therapy, septal myectomy probably offers the best chance of excellent long-term symptomatic improvement, but the mortality depends on the center and the surgical expertise there, and complications do, too. This is something good to know that we never had data on before, that if you can’t get to a center with an experienced surgeon doing myectomies, it’s reasonable to go to a center doing ablations as long as there is some experience with the procedure there,” said Dr. Nishimura, professor of cardiovascular diseases and hypertension at the Mayo Clinic in Rochester, Minn.
Of the 11,248 patients treated for obstructive hypertrophic cardiomyopathy identified by the Cornell investigators using the Agency for Healthcare Research and Quality National Inpatient Sample database, 57% got myectomy and 43% underwent ablation. During the study years ablation increased in popularity by about 50%, rising from an annual rate of 1.6 to 2.5 procedures per million per year, while myectomy declined from 2.0 to 1.5 cases per million population per year. But that’s not what’s happened at the Mayo Clinic and other hypertrophic cardiomyopathy centers of excellence.
At the Mayo Clinic, for example, the volume of septal myectomies climbed from roughly 50 procedures per year in 2000 to close to 250 in 2015. Meanwhile the rate of alcohol septal ablation procedures remained steady at fewer than 20 per year.
“With shared decision making at Mayo, surgery has gone way up,” said Dr. Nishimura. “In an experienced surgeon’s hands, operative mortality is 0.8%, the gradient improves to 3%, and 94% of patients are postoperative New York Heart Association class I or II. This lasts for decades. We have 20-, 30-, and 40-year follow-up data now showing that over 90% of patients will have an excellent symptomatic benefit and be able to return to a normal lifestyle. The septum doesn’t come back. They’re good for life. So it’s a wonderful operation.”
In contrast, catheter-based septal ablation has a 4-year rate of survival free of death, NYHA class III or IV, or myectomy of 76%.
“One in four treated patients will not benefit,” the cardiologist emphasized.
The percutaneous procedure entails instilling alcohol into the septal perforator artery supplying the area of obstruction in order to cause a localized MI. Over a period of several weeks this causes the septum to shrink, thereby relieving the outflow tract obstruction.
When the procedure fails to bring about improvement, it’s often because the patient had a very long septal perforator artery and instilling the alcohol caused a large MI, making things worse. Or the patient didn’t have a septal perforator artery, or had one with so many branches that the cardiologist couldn’t identify the right one to treat to target the septum.
Dr. Nishimura reported having no financial conflicts.
Laser vaginal rejuvenation procedures
VIENNA – Vaginal rejuvenation is a major practice growth opportunity for dermatologists who have expertise with lasers, Peter Bjerring, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
The rejuvenation procedures involve heating the connective tissue of the vaginal wall to 40-42 C in order to stimulate tissue remodeling with formation of new collagen and elastic fibers. The evidence base for vaginal rejuvenation using a variety of noninvasive energy-based devices developed for vaginal use isn’t nearly as extensive as it is for skin rejuvenation using lasers. Research is beginning to increase for this indication, but current results are primarily limited to small single-arm studies based on self-reported improvements. Further, studies don’t compare outcomes vs another treatment, such as estrogen cream.
Despite the minimal evidence base for laser procedures, “feminine rejuvenation is becoming very popular. These are (women) who might present to a dermatologist or to a gynecologist,” observed Dr. Bjerring, medical director and head of the Skin and Laser Center at Malholm (Denmark) Hospital.
Minimally ablative or nonablative fractional laser therapy for vaginal rejuvenation requires no anesthesia and no downtime. The lasers being used for this purpose are similar to those already used most often for skin resurfacing and rejuvenation of the face and neck: fractional CO2 lasers at the 10,600-nm wavelength, such as the MonaLisa Touch or FemTouch, and 2,940-nm nonablative erbium:yttrium-aluminum-garnet (Er:YAG) lasers such as the IntimaLase. A course of treatment with these devices typically consists of three, 15-minute sessions at 4- to 6-week intervals.
Dr. Bjerring noted that this mechanism of benefit has been demonstrated by Italian investigators who conducted a histologic study of the effects of microablative fractional CO2 laser therapy on ex vivo specimens of atrophic vaginal tissue obtained from women with vulvovaginal atrophy who underwent major surgery for pelvic organ prolapse.
The investigators treated one side of the atrophic vaginal wall specimen with the microablative fractional CO2 laser and left the contralateral area untreated as a control. They documented that laser therapy restored the vaginal squamous stratified epithelium, with enhanced storage of glycogen in the epithelial cells and shedding of glycogen-rich cells at the epithelial surface. In the connective tissue, activated fibroblasts synthesized new collagen-laden extracellular matrix. All this was accomplished without damage to adjacent untreated tissue (Menopause 2015 Aug;22(8):845-9).
In a single-arm study performed by many of the same Italian investigators, 77 postmenopausal women underwent a course of fractional microablative CO2 laser therapy because they experienced painful sexual intercourse due to vulvovaginal atrophy. At 12 weeks of followup, the group reported significant improvement in sexual function and satisfaction with their sexual life as measured by the Short Form-12 and the Female Sexual Function Index. Self-rated scores of vaginal burning, dryness, and itching improved significantly, as did complaints of pain during intercourse or urination. At baseline, 20 of the 77 women were not sexually active due to the severity of their vulvovaginal atrophy; at followup, 17 of the 20 had reestablished sexual activity (Climacteric. 2015 Apr;18(2):219-25).
Dr. Bjerring also highlighted an American study, again single-arm, in which 27 women with genitourinary syndrome of menopause were examined at baseline and again 3 months after their third and final treatment with a fractional CO2 laser. At follow up, 26 of the 27 pronounced themselves satisfied or extremely satisfied with the results, with significant improvement in the same outcome measures used in the Italian study. At follow up, 25 of the women had an increase in comfortable dilator size (Menopause 2016 Oct;23(10):1102-7).
Dr. Bjerring reported having no financial conflicts of interest regarding his presentation.
VIENNA – Vaginal rejuvenation is a major practice growth opportunity for dermatologists who have expertise with lasers, Peter Bjerring, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
The rejuvenation procedures involve heating the connective tissue of the vaginal wall to 40-42 C in order to stimulate tissue remodeling with formation of new collagen and elastic fibers. The evidence base for vaginal rejuvenation using a variety of noninvasive energy-based devices developed for vaginal use isn’t nearly as extensive as it is for skin rejuvenation using lasers. Research is beginning to increase for this indication, but current results are primarily limited to small single-arm studies based on self-reported improvements. Further, studies don’t compare outcomes vs another treatment, such as estrogen cream.
Despite the minimal evidence base for laser procedures, “feminine rejuvenation is becoming very popular. These are (women) who might present to a dermatologist or to a gynecologist,” observed Dr. Bjerring, medical director and head of the Skin and Laser Center at Malholm (Denmark) Hospital.
Minimally ablative or nonablative fractional laser therapy for vaginal rejuvenation requires no anesthesia and no downtime. The lasers being used for this purpose are similar to those already used most often for skin resurfacing and rejuvenation of the face and neck: fractional CO2 lasers at the 10,600-nm wavelength, such as the MonaLisa Touch or FemTouch, and 2,940-nm nonablative erbium:yttrium-aluminum-garnet (Er:YAG) lasers such as the IntimaLase. A course of treatment with these devices typically consists of three, 15-minute sessions at 4- to 6-week intervals.
Dr. Bjerring noted that this mechanism of benefit has been demonstrated by Italian investigators who conducted a histologic study of the effects of microablative fractional CO2 laser therapy on ex vivo specimens of atrophic vaginal tissue obtained from women with vulvovaginal atrophy who underwent major surgery for pelvic organ prolapse.
The investigators treated one side of the atrophic vaginal wall specimen with the microablative fractional CO2 laser and left the contralateral area untreated as a control. They documented that laser therapy restored the vaginal squamous stratified epithelium, with enhanced storage of glycogen in the epithelial cells and shedding of glycogen-rich cells at the epithelial surface. In the connective tissue, activated fibroblasts synthesized new collagen-laden extracellular matrix. All this was accomplished without damage to adjacent untreated tissue (Menopause 2015 Aug;22(8):845-9).
In a single-arm study performed by many of the same Italian investigators, 77 postmenopausal women underwent a course of fractional microablative CO2 laser therapy because they experienced painful sexual intercourse due to vulvovaginal atrophy. At 12 weeks of followup, the group reported significant improvement in sexual function and satisfaction with their sexual life as measured by the Short Form-12 and the Female Sexual Function Index. Self-rated scores of vaginal burning, dryness, and itching improved significantly, as did complaints of pain during intercourse or urination. At baseline, 20 of the 77 women were not sexually active due to the severity of their vulvovaginal atrophy; at followup, 17 of the 20 had reestablished sexual activity (Climacteric. 2015 Apr;18(2):219-25).
Dr. Bjerring also highlighted an American study, again single-arm, in which 27 women with genitourinary syndrome of menopause were examined at baseline and again 3 months after their third and final treatment with a fractional CO2 laser. At follow up, 26 of the 27 pronounced themselves satisfied or extremely satisfied with the results, with significant improvement in the same outcome measures used in the Italian study. At follow up, 25 of the women had an increase in comfortable dilator size (Menopause 2016 Oct;23(10):1102-7).
Dr. Bjerring reported having no financial conflicts of interest regarding his presentation.
VIENNA – Vaginal rejuvenation is a major practice growth opportunity for dermatologists who have expertise with lasers, Peter Bjerring, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
The rejuvenation procedures involve heating the connective tissue of the vaginal wall to 40-42 C in order to stimulate tissue remodeling with formation of new collagen and elastic fibers. The evidence base for vaginal rejuvenation using a variety of noninvasive energy-based devices developed for vaginal use isn’t nearly as extensive as it is for skin rejuvenation using lasers. Research is beginning to increase for this indication, but current results are primarily limited to small single-arm studies based on self-reported improvements. Further, studies don’t compare outcomes vs another treatment, such as estrogen cream.
Despite the minimal evidence base for laser procedures, “feminine rejuvenation is becoming very popular. These are (women) who might present to a dermatologist or to a gynecologist,” observed Dr. Bjerring, medical director and head of the Skin and Laser Center at Malholm (Denmark) Hospital.
Minimally ablative or nonablative fractional laser therapy for vaginal rejuvenation requires no anesthesia and no downtime. The lasers being used for this purpose are similar to those already used most often for skin resurfacing and rejuvenation of the face and neck: fractional CO2 lasers at the 10,600-nm wavelength, such as the MonaLisa Touch or FemTouch, and 2,940-nm nonablative erbium:yttrium-aluminum-garnet (Er:YAG) lasers such as the IntimaLase. A course of treatment with these devices typically consists of three, 15-minute sessions at 4- to 6-week intervals.
Dr. Bjerring noted that this mechanism of benefit has been demonstrated by Italian investigators who conducted a histologic study of the effects of microablative fractional CO2 laser therapy on ex vivo specimens of atrophic vaginal tissue obtained from women with vulvovaginal atrophy who underwent major surgery for pelvic organ prolapse.
The investigators treated one side of the atrophic vaginal wall specimen with the microablative fractional CO2 laser and left the contralateral area untreated as a control. They documented that laser therapy restored the vaginal squamous stratified epithelium, with enhanced storage of glycogen in the epithelial cells and shedding of glycogen-rich cells at the epithelial surface. In the connective tissue, activated fibroblasts synthesized new collagen-laden extracellular matrix. All this was accomplished without damage to adjacent untreated tissue (Menopause 2015 Aug;22(8):845-9).
In a single-arm study performed by many of the same Italian investigators, 77 postmenopausal women underwent a course of fractional microablative CO2 laser therapy because they experienced painful sexual intercourse due to vulvovaginal atrophy. At 12 weeks of followup, the group reported significant improvement in sexual function and satisfaction with their sexual life as measured by the Short Form-12 and the Female Sexual Function Index. Self-rated scores of vaginal burning, dryness, and itching improved significantly, as did complaints of pain during intercourse or urination. At baseline, 20 of the 77 women were not sexually active due to the severity of their vulvovaginal atrophy; at followup, 17 of the 20 had reestablished sexual activity (Climacteric. 2015 Apr;18(2):219-25).
Dr. Bjerring also highlighted an American study, again single-arm, in which 27 women with genitourinary syndrome of menopause were examined at baseline and again 3 months after their third and final treatment with a fractional CO2 laser. At follow up, 26 of the 27 pronounced themselves satisfied or extremely satisfied with the results, with significant improvement in the same outcome measures used in the Italian study. At follow up, 25 of the women had an increase in comfortable dilator size (Menopause 2016 Oct;23(10):1102-7).
Dr. Bjerring reported having no financial conflicts of interest regarding his presentation.
EXPERT ANALYSIS FROM THE EADV CONGRESS
Curb AF recurrences through risk factor modification
SNOWMASS, COLO. – Overlooking the common modifiable risk factors in patients with atrial fibrillation is missing out on an excellent opportunity to help curb the growing global pandemic of the arrhythmia, Patrick T. O’Gara, MD, said at the Annual Cardiovascular Conference at Snowmass.
“My purpose here is a wake up call to improve screening for and treatment of modifiable risk factors in patients with atrial fibrillation,” declared Dr. O’Gara, professor of medicine at Harvard Medical School, Boston.
Overweight/obesity: Investigators at the University of Adelaide (Australia) demonstrated in the LEGACY trial that patients with atrial fibrillation (AF) and a BMI of 27 kg/m2 or more reduced their AF symptom burden in a dose-response fashion as they shed excess pounds as part of an intensive weight management program. Those who shed at least 10% of their baseline body weight had a 46% rate of 5-year freedom from AF without resort to rhythm control medications or ablation procedures of 46%. With 3%-9% weight loss, the rate was 22%. And with 3% weight loss, it was 13%.
The best results came from sustained linear weight loss. Weight fluctuations of greater than 5% – the classic yoyo dieting pattern – partially offset the overall benefit of weight loss with respect to recurrent AF (J Am Coll Cardiol. 2015 May 26;65(20):2159-69).
In a separate study, the same team of Australian investigators offered an opportunity to participate in a risk factor management program to patients with AF and a BMI of 27 kg/m2 or more who were undergoing radiofrequency ablation for their arrhythmia. Participants had significantly fewer repeat ablation procedures during followup and were also less likely to be on antiarrhythmic drugs than the patients who opted for usual care (J Am Coll Cardiol. 2014 Dec 2;64(21):2222-31).
Alcohol: The ‘holiday heart’ syndrome is well known, but alcohol consumption beyond binging can increase risk for AF. Dr. O’Gara noted that in a recent review article entitled “Alcohol and Atrial Fibrillation: A Sobering Review,” investigators at the University of Melbourne showed that while the relationship between the number of standard drinks per week and risk of cardiovascular mortality is J-shaped, with a nadir at 14-21 drinks per week in men and fewer in women, the risk of developing AF is linear over time and appears to increase incrementally with every additional drink per week (J Am Coll Cardiol. 2016 Dec 13;68(23):2567-76).
Also, a prospective study of nearly 80,000 Swedes free from AF at baseline, coupled with a meta-analysis of seven prospective studies found that for each additional drink per day consumed the risk of developing AF rose over time by roughly a further 10% compared to that of teetotalers (J Am Coll Cardiol. 2014; Jul 22;64(3):281-9).
Physical inactivity: In the prospective Tromso Study, in which more than 20,000 Norwegian adults were followed for 20 years, leisure time physical activity displayed a J-shaped relationship with the risk of developing AF. Moderately active subjects were an adjusted 19% less likely to develop AF than those with low physical activity, while the risk in subjects who regularly engaged in vigorous physical activity was 37% higher than in the low-activity group (Eur Heart J. 2016 Aug 1;37(29):2307-13).
“This effect of moderate exercise might be due to the associated weight loss, improved endothelial function, better sleep, perhaps a better balance between the sympathetic and parasympathetic nervous systems,” Dr. O’Gara observed.
How much physical activity is right for patients with AF? Dr. O’Gara said one of the best reviews he’s seen came from the University of Adelaide group (Circulation. 2016 Feb 2;133(5):457-9). They recommended a total of 120-200 minutes of exercise per week spread over three to five sessions. While the research base is strongest for moderate-intensity exercise, the Australians also noted the effectiveness and safety of a novel program of repeated 4-minute intervals of high-intensity exercise at 85%-95% of peak heart rate as demonstrated in a randomized controlled trial by investigators at the Norwegian University of Science and Technology in Trondheim. They showed this approach resulted in reduced time in AF and decreased AF symptoms coupled with improved quality of life and left atrial and ventricular function (Circulation. 2016 Feb 2;133(5):466-73).
“I think you could look at this review and feel very confident that there is some evidence base to substantiate your strong recommendation that patients actively engage in exercise as treatment for their atrial fibrillation,” the cardiologist said.
Sleep apnea: Investigators at Brigham and Women’s Hospital in Boston have demonstrated that effective treatment of sleep apnea with continuous positive airway pressure in patients with atrial fibrillation is associated with smaller atrial size and ventricular mass, lower blood pressure, and a significantly reduced risk of recurrent AF following an AF ablation procedure (J Am Heart Assoc. 2013 Nov 25;2(6):e000421).
“Sleep hygiene is one of the least attended aspects of cardiovascular health,” according to Dr. O’Gara. “We need to ask the partner or spouse, ‘How well does your partner sleep? Do you hear thrashing about, snoring, gagging, or notice restless legs?’ Heart failure folks are really tuned into this, but in the practice of seeing patients come into the emergency room with new-onset atrial fibrillation, it’s tenth on the list of five questions one would ask.”
Dr. O’Gara reported having no financial conflicts.
SNOWMASS, COLO. – Overlooking the common modifiable risk factors in patients with atrial fibrillation is missing out on an excellent opportunity to help curb the growing global pandemic of the arrhythmia, Patrick T. O’Gara, MD, said at the Annual Cardiovascular Conference at Snowmass.
“My purpose here is a wake up call to improve screening for and treatment of modifiable risk factors in patients with atrial fibrillation,” declared Dr. O’Gara, professor of medicine at Harvard Medical School, Boston.
Overweight/obesity: Investigators at the University of Adelaide (Australia) demonstrated in the LEGACY trial that patients with atrial fibrillation (AF) and a BMI of 27 kg/m2 or more reduced their AF symptom burden in a dose-response fashion as they shed excess pounds as part of an intensive weight management program. Those who shed at least 10% of their baseline body weight had a 46% rate of 5-year freedom from AF without resort to rhythm control medications or ablation procedures of 46%. With 3%-9% weight loss, the rate was 22%. And with 3% weight loss, it was 13%.
The best results came from sustained linear weight loss. Weight fluctuations of greater than 5% – the classic yoyo dieting pattern – partially offset the overall benefit of weight loss with respect to recurrent AF (J Am Coll Cardiol. 2015 May 26;65(20):2159-69).
In a separate study, the same team of Australian investigators offered an opportunity to participate in a risk factor management program to patients with AF and a BMI of 27 kg/m2 or more who were undergoing radiofrequency ablation for their arrhythmia. Participants had significantly fewer repeat ablation procedures during followup and were also less likely to be on antiarrhythmic drugs than the patients who opted for usual care (J Am Coll Cardiol. 2014 Dec 2;64(21):2222-31).
Alcohol: The ‘holiday heart’ syndrome is well known, but alcohol consumption beyond binging can increase risk for AF. Dr. O’Gara noted that in a recent review article entitled “Alcohol and Atrial Fibrillation: A Sobering Review,” investigators at the University of Melbourne showed that while the relationship between the number of standard drinks per week and risk of cardiovascular mortality is J-shaped, with a nadir at 14-21 drinks per week in men and fewer in women, the risk of developing AF is linear over time and appears to increase incrementally with every additional drink per week (J Am Coll Cardiol. 2016 Dec 13;68(23):2567-76).
Also, a prospective study of nearly 80,000 Swedes free from AF at baseline, coupled with a meta-analysis of seven prospective studies found that for each additional drink per day consumed the risk of developing AF rose over time by roughly a further 10% compared to that of teetotalers (J Am Coll Cardiol. 2014; Jul 22;64(3):281-9).
Physical inactivity: In the prospective Tromso Study, in which more than 20,000 Norwegian adults were followed for 20 years, leisure time physical activity displayed a J-shaped relationship with the risk of developing AF. Moderately active subjects were an adjusted 19% less likely to develop AF than those with low physical activity, while the risk in subjects who regularly engaged in vigorous physical activity was 37% higher than in the low-activity group (Eur Heart J. 2016 Aug 1;37(29):2307-13).
“This effect of moderate exercise might be due to the associated weight loss, improved endothelial function, better sleep, perhaps a better balance between the sympathetic and parasympathetic nervous systems,” Dr. O’Gara observed.
How much physical activity is right for patients with AF? Dr. O’Gara said one of the best reviews he’s seen came from the University of Adelaide group (Circulation. 2016 Feb 2;133(5):457-9). They recommended a total of 120-200 minutes of exercise per week spread over three to five sessions. While the research base is strongest for moderate-intensity exercise, the Australians also noted the effectiveness and safety of a novel program of repeated 4-minute intervals of high-intensity exercise at 85%-95% of peak heart rate as demonstrated in a randomized controlled trial by investigators at the Norwegian University of Science and Technology in Trondheim. They showed this approach resulted in reduced time in AF and decreased AF symptoms coupled with improved quality of life and left atrial and ventricular function (Circulation. 2016 Feb 2;133(5):466-73).
“I think you could look at this review and feel very confident that there is some evidence base to substantiate your strong recommendation that patients actively engage in exercise as treatment for their atrial fibrillation,” the cardiologist said.
Sleep apnea: Investigators at Brigham and Women’s Hospital in Boston have demonstrated that effective treatment of sleep apnea with continuous positive airway pressure in patients with atrial fibrillation is associated with smaller atrial size and ventricular mass, lower blood pressure, and a significantly reduced risk of recurrent AF following an AF ablation procedure (J Am Heart Assoc. 2013 Nov 25;2(6):e000421).
“Sleep hygiene is one of the least attended aspects of cardiovascular health,” according to Dr. O’Gara. “We need to ask the partner or spouse, ‘How well does your partner sleep? Do you hear thrashing about, snoring, gagging, or notice restless legs?’ Heart failure folks are really tuned into this, but in the practice of seeing patients come into the emergency room with new-onset atrial fibrillation, it’s tenth on the list of five questions one would ask.”
Dr. O’Gara reported having no financial conflicts.
SNOWMASS, COLO. – Overlooking the common modifiable risk factors in patients with atrial fibrillation is missing out on an excellent opportunity to help curb the growing global pandemic of the arrhythmia, Patrick T. O’Gara, MD, said at the Annual Cardiovascular Conference at Snowmass.
“My purpose here is a wake up call to improve screening for and treatment of modifiable risk factors in patients with atrial fibrillation,” declared Dr. O’Gara, professor of medicine at Harvard Medical School, Boston.
Overweight/obesity: Investigators at the University of Adelaide (Australia) demonstrated in the LEGACY trial that patients with atrial fibrillation (AF) and a BMI of 27 kg/m2 or more reduced their AF symptom burden in a dose-response fashion as they shed excess pounds as part of an intensive weight management program. Those who shed at least 10% of their baseline body weight had a 46% rate of 5-year freedom from AF without resort to rhythm control medications or ablation procedures of 46%. With 3%-9% weight loss, the rate was 22%. And with 3% weight loss, it was 13%.
The best results came from sustained linear weight loss. Weight fluctuations of greater than 5% – the classic yoyo dieting pattern – partially offset the overall benefit of weight loss with respect to recurrent AF (J Am Coll Cardiol. 2015 May 26;65(20):2159-69).
In a separate study, the same team of Australian investigators offered an opportunity to participate in a risk factor management program to patients with AF and a BMI of 27 kg/m2 or more who were undergoing radiofrequency ablation for their arrhythmia. Participants had significantly fewer repeat ablation procedures during followup and were also less likely to be on antiarrhythmic drugs than the patients who opted for usual care (J Am Coll Cardiol. 2014 Dec 2;64(21):2222-31).
Alcohol: The ‘holiday heart’ syndrome is well known, but alcohol consumption beyond binging can increase risk for AF. Dr. O’Gara noted that in a recent review article entitled “Alcohol and Atrial Fibrillation: A Sobering Review,” investigators at the University of Melbourne showed that while the relationship between the number of standard drinks per week and risk of cardiovascular mortality is J-shaped, with a nadir at 14-21 drinks per week in men and fewer in women, the risk of developing AF is linear over time and appears to increase incrementally with every additional drink per week (J Am Coll Cardiol. 2016 Dec 13;68(23):2567-76).
Also, a prospective study of nearly 80,000 Swedes free from AF at baseline, coupled with a meta-analysis of seven prospective studies found that for each additional drink per day consumed the risk of developing AF rose over time by roughly a further 10% compared to that of teetotalers (J Am Coll Cardiol. 2014; Jul 22;64(3):281-9).
Physical inactivity: In the prospective Tromso Study, in which more than 20,000 Norwegian adults were followed for 20 years, leisure time physical activity displayed a J-shaped relationship with the risk of developing AF. Moderately active subjects were an adjusted 19% less likely to develop AF than those with low physical activity, while the risk in subjects who regularly engaged in vigorous physical activity was 37% higher than in the low-activity group (Eur Heart J. 2016 Aug 1;37(29):2307-13).
“This effect of moderate exercise might be due to the associated weight loss, improved endothelial function, better sleep, perhaps a better balance between the sympathetic and parasympathetic nervous systems,” Dr. O’Gara observed.
How much physical activity is right for patients with AF? Dr. O’Gara said one of the best reviews he’s seen came from the University of Adelaide group (Circulation. 2016 Feb 2;133(5):457-9). They recommended a total of 120-200 minutes of exercise per week spread over three to five sessions. While the research base is strongest for moderate-intensity exercise, the Australians also noted the effectiveness and safety of a novel program of repeated 4-minute intervals of high-intensity exercise at 85%-95% of peak heart rate as demonstrated in a randomized controlled trial by investigators at the Norwegian University of Science and Technology in Trondheim. They showed this approach resulted in reduced time in AF and decreased AF symptoms coupled with improved quality of life and left atrial and ventricular function (Circulation. 2016 Feb 2;133(5):466-73).
“I think you could look at this review and feel very confident that there is some evidence base to substantiate your strong recommendation that patients actively engage in exercise as treatment for their atrial fibrillation,” the cardiologist said.
Sleep apnea: Investigators at Brigham and Women’s Hospital in Boston have demonstrated that effective treatment of sleep apnea with continuous positive airway pressure in patients with atrial fibrillation is associated with smaller atrial size and ventricular mass, lower blood pressure, and a significantly reduced risk of recurrent AF following an AF ablation procedure (J Am Heart Assoc. 2013 Nov 25;2(6):e000421).
“Sleep hygiene is one of the least attended aspects of cardiovascular health,” according to Dr. O’Gara. “We need to ask the partner or spouse, ‘How well does your partner sleep? Do you hear thrashing about, snoring, gagging, or notice restless legs?’ Heart failure folks are really tuned into this, but in the practice of seeing patients come into the emergency room with new-onset atrial fibrillation, it’s tenth on the list of five questions one would ask.”
Dr. O’Gara reported having no financial conflicts.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Cardiac procedures tied to higher cancer risk in adult congenital heart disease
NEW ORLEANS – The greater the lifetime number of cardiac procedures entailing exposure to low-dose ionizing radiation, the higher the associated cancer risk in adults with congenital heart disease, Sarah Cohen, MD, reported at the American Heart Association scientific sessions.
This finding takes on added clinical import because the use of such procedures has increased markedly in patients with adult congenital heart disease, added Dr. Cohen of McGill University in Montreal.
She presented analyses of nearly 25,000 patients in the Quebec congenital heart disease database who were ages 18-64 with no history of cancer in January 1995; 602 of them were diagnosed with cancer during follow-up through 2009. Each was matched to four cancer-free controls in the database on the basis of age, sex, congenital heart disease severity, and calendar year.
Patients with a lifetime total of four or five cardiac procedures involving exposure to low-dose ionizing radiation were 1.7-fold more likely to be diagnosed with cancer during follow-up than were those with a history of no such procedures or just one. With a lifetime history of six or more of the procedures, the relative risk climbed to 2.2-fold.
Nearly 90% of the malignancies were genitourinary, respiratory, digestive, breast, or hematologic cancers.
Dr. Cohen and her coinvestigators also conducted a cohort study comparing the relative risk of developing cancer in 1,781 high-exposure Quebec adults in the database who had a lifetime history of four or more cardiac procedures involving radiation exposure to more than 20,000 others with a history of not more than one such procedure. The high-exposure group had a 3.3-fold greater rate of malignancy during follow-up.
In a separate study, Dr. Cohen’s McGill colleagues analyzed the Quebec database and documented the sharp rise over time in low-dose ionizing radiation cardiac procedures, including catheter-based diagnostic procedures, structural heart interventions, nuclear procedures, coronary interventions, computed tomography scans of the chest, coronary interventions, and insertion or repair of pacemakers and implantable cardioverter-defibrillators. In 1990, the rate was 18.5 such procedures per 1,000 patients per year. By 2005, it had nearly tripled to 51.9 per 1,000 per year. The age at first procedure dropped from 5 years to 9 months (Circulation 2016 Jan 5;133[1]:12-20).
Dr. Cohen reported having no financial disclosures.
NEW ORLEANS – The greater the lifetime number of cardiac procedures entailing exposure to low-dose ionizing radiation, the higher the associated cancer risk in adults with congenital heart disease, Sarah Cohen, MD, reported at the American Heart Association scientific sessions.
This finding takes on added clinical import because the use of such procedures has increased markedly in patients with adult congenital heart disease, added Dr. Cohen of McGill University in Montreal.
She presented analyses of nearly 25,000 patients in the Quebec congenital heart disease database who were ages 18-64 with no history of cancer in January 1995; 602 of them were diagnosed with cancer during follow-up through 2009. Each was matched to four cancer-free controls in the database on the basis of age, sex, congenital heart disease severity, and calendar year.
Patients with a lifetime total of four or five cardiac procedures involving exposure to low-dose ionizing radiation were 1.7-fold more likely to be diagnosed with cancer during follow-up than were those with a history of no such procedures or just one. With a lifetime history of six or more of the procedures, the relative risk climbed to 2.2-fold.
Nearly 90% of the malignancies were genitourinary, respiratory, digestive, breast, or hematologic cancers.
Dr. Cohen and her coinvestigators also conducted a cohort study comparing the relative risk of developing cancer in 1,781 high-exposure Quebec adults in the database who had a lifetime history of four or more cardiac procedures involving radiation exposure to more than 20,000 others with a history of not more than one such procedure. The high-exposure group had a 3.3-fold greater rate of malignancy during follow-up.
In a separate study, Dr. Cohen’s McGill colleagues analyzed the Quebec database and documented the sharp rise over time in low-dose ionizing radiation cardiac procedures, including catheter-based diagnostic procedures, structural heart interventions, nuclear procedures, coronary interventions, computed tomography scans of the chest, coronary interventions, and insertion or repair of pacemakers and implantable cardioverter-defibrillators. In 1990, the rate was 18.5 such procedures per 1,000 patients per year. By 2005, it had nearly tripled to 51.9 per 1,000 per year. The age at first procedure dropped from 5 years to 9 months (Circulation 2016 Jan 5;133[1]:12-20).
Dr. Cohen reported having no financial disclosures.
NEW ORLEANS – The greater the lifetime number of cardiac procedures entailing exposure to low-dose ionizing radiation, the higher the associated cancer risk in adults with congenital heart disease, Sarah Cohen, MD, reported at the American Heart Association scientific sessions.
This finding takes on added clinical import because the use of such procedures has increased markedly in patients with adult congenital heart disease, added Dr. Cohen of McGill University in Montreal.
She presented analyses of nearly 25,000 patients in the Quebec congenital heart disease database who were ages 18-64 with no history of cancer in January 1995; 602 of them were diagnosed with cancer during follow-up through 2009. Each was matched to four cancer-free controls in the database on the basis of age, sex, congenital heart disease severity, and calendar year.
Patients with a lifetime total of four or five cardiac procedures involving exposure to low-dose ionizing radiation were 1.7-fold more likely to be diagnosed with cancer during follow-up than were those with a history of no such procedures or just one. With a lifetime history of six or more of the procedures, the relative risk climbed to 2.2-fold.
Nearly 90% of the malignancies were genitourinary, respiratory, digestive, breast, or hematologic cancers.
Dr. Cohen and her coinvestigators also conducted a cohort study comparing the relative risk of developing cancer in 1,781 high-exposure Quebec adults in the database who had a lifetime history of four or more cardiac procedures involving radiation exposure to more than 20,000 others with a history of not more than one such procedure. The high-exposure group had a 3.3-fold greater rate of malignancy during follow-up.
In a separate study, Dr. Cohen’s McGill colleagues analyzed the Quebec database and documented the sharp rise over time in low-dose ionizing radiation cardiac procedures, including catheter-based diagnostic procedures, structural heart interventions, nuclear procedures, coronary interventions, computed tomography scans of the chest, coronary interventions, and insertion or repair of pacemakers and implantable cardioverter-defibrillators. In 1990, the rate was 18.5 such procedures per 1,000 patients per year. By 2005, it had nearly tripled to 51.9 per 1,000 per year. The age at first procedure dropped from 5 years to 9 months (Circulation 2016 Jan 5;133[1]:12-20).
Dr. Cohen reported having no financial disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Adults with congenital heart disease who had a lifetime history of six or more cardiac procedures involving exposure to low-dose ionizing radiation were 2.2-fold more likely to develop cancer during follow-up than were those with not more than one such procedure.
Data source: This nested, case-control study included 602 adults with congenital heart disease who developed cancer, each matched to four controls who did not.
Disclosures: The study presenter reported having no financial disclosures.
A sweet new solution for rosacea
VIENNA – A medical-grade topical honey product proved safe and effective for the treatment of rosacea in a randomized, placebo-controlled clinical trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The product, known as Honevo, is a cream consisting of 90% New Zealand kanuka honey and 10% glycerine. It is applied twice daily as a face mask. Honevo is designed to wash off easily and is less sticky than honey.
The primary outcome in the trial was at least a 2-point improvement from baseline on the 7-point Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) as assessed by blinded investigators. This outcome, which reflects a clinical improvement from severe to moderate or from moderate to mild, was achieved in 34% of the Honevo group, compared with 17% of controls. Significant improvement in the honey group was seen after 2 weeks.
Rosacea resolved in 13% of the Honevo group and in 3% of controls, based on a week 8 IGA-RSS of zero, noted Dr. Dreno, professor and chair of the department of dermatology at the University of Nantes (France).
The investigators, from the Medical Research Institute of New Zealand and the University of Otago in Wellington, observed that the study outcomes look at least as good as the results of placebo-controlled studies of topical metronidazole or azelaic cream. They plan to conduct randomized, head-to-head comparative trials of those prescription drugs versus Honevo, which is an OTC product.
The mechanism of action of kanuka honey in treating rosacea is believed to involve its previously reported antibacterial and anti-inflammatory effects, according to the investigators (BMJ Open. 2015 Jun 24;5[6]:e007651. doi: 10.1136/bmjopen-2015-007651).
The researchers noted that many rosacea patients aren’t interested in long-term antibiotic therapy. They want a natural product that doesn’t contribute to the global antibiotic resistance problem and is available OTC. And Honevo is one of the few natural or complementary medicine therapies backed by data from a rigorous clinical trial, in this case one registered in the Australian New Zealand Clinical Trials Registry (ACTRN12614000004662).
Dr. Dreno wasn’t involved in the study but included it in a talk in which she examined the strengths and weaknesses of current rosacea therapies. She is waiting for a confirmatory study before she incorporates Honevo in her own treatment algorithm. She said that she also would like to see studies examining whether combining the topical honey product with prescription drugs for rosacea provides synergistic efficacy.
HoneyLab, which funded the clinical trial and markets Honevo, ships the product to customers worldwide from its New Zealand headquarters.
VIENNA – A medical-grade topical honey product proved safe and effective for the treatment of rosacea in a randomized, placebo-controlled clinical trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The product, known as Honevo, is a cream consisting of 90% New Zealand kanuka honey and 10% glycerine. It is applied twice daily as a face mask. Honevo is designed to wash off easily and is less sticky than honey.
The primary outcome in the trial was at least a 2-point improvement from baseline on the 7-point Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) as assessed by blinded investigators. This outcome, which reflects a clinical improvement from severe to moderate or from moderate to mild, was achieved in 34% of the Honevo group, compared with 17% of controls. Significant improvement in the honey group was seen after 2 weeks.
Rosacea resolved in 13% of the Honevo group and in 3% of controls, based on a week 8 IGA-RSS of zero, noted Dr. Dreno, professor and chair of the department of dermatology at the University of Nantes (France).
The investigators, from the Medical Research Institute of New Zealand and the University of Otago in Wellington, observed that the study outcomes look at least as good as the results of placebo-controlled studies of topical metronidazole or azelaic cream. They plan to conduct randomized, head-to-head comparative trials of those prescription drugs versus Honevo, which is an OTC product.
The mechanism of action of kanuka honey in treating rosacea is believed to involve its previously reported antibacterial and anti-inflammatory effects, according to the investigators (BMJ Open. 2015 Jun 24;5[6]:e007651. doi: 10.1136/bmjopen-2015-007651).
The researchers noted that many rosacea patients aren’t interested in long-term antibiotic therapy. They want a natural product that doesn’t contribute to the global antibiotic resistance problem and is available OTC. And Honevo is one of the few natural or complementary medicine therapies backed by data from a rigorous clinical trial, in this case one registered in the Australian New Zealand Clinical Trials Registry (ACTRN12614000004662).
Dr. Dreno wasn’t involved in the study but included it in a talk in which she examined the strengths and weaknesses of current rosacea therapies. She is waiting for a confirmatory study before she incorporates Honevo in her own treatment algorithm. She said that she also would like to see studies examining whether combining the topical honey product with prescription drugs for rosacea provides synergistic efficacy.
HoneyLab, which funded the clinical trial and markets Honevo, ships the product to customers worldwide from its New Zealand headquarters.
VIENNA – A medical-grade topical honey product proved safe and effective for the treatment of rosacea in a randomized, placebo-controlled clinical trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The product, known as Honevo, is a cream consisting of 90% New Zealand kanuka honey and 10% glycerine. It is applied twice daily as a face mask. Honevo is designed to wash off easily and is less sticky than honey.
The primary outcome in the trial was at least a 2-point improvement from baseline on the 7-point Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) as assessed by blinded investigators. This outcome, which reflects a clinical improvement from severe to moderate or from moderate to mild, was achieved in 34% of the Honevo group, compared with 17% of controls. Significant improvement in the honey group was seen after 2 weeks.
Rosacea resolved in 13% of the Honevo group and in 3% of controls, based on a week 8 IGA-RSS of zero, noted Dr. Dreno, professor and chair of the department of dermatology at the University of Nantes (France).
The investigators, from the Medical Research Institute of New Zealand and the University of Otago in Wellington, observed that the study outcomes look at least as good as the results of placebo-controlled studies of topical metronidazole or azelaic cream. They plan to conduct randomized, head-to-head comparative trials of those prescription drugs versus Honevo, which is an OTC product.
The mechanism of action of kanuka honey in treating rosacea is believed to involve its previously reported antibacterial and anti-inflammatory effects, according to the investigators (BMJ Open. 2015 Jun 24;5[6]:e007651. doi: 10.1136/bmjopen-2015-007651).
The researchers noted that many rosacea patients aren’t interested in long-term antibiotic therapy. They want a natural product that doesn’t contribute to the global antibiotic resistance problem and is available OTC. And Honevo is one of the few natural or complementary medicine therapies backed by data from a rigorous clinical trial, in this case one registered in the Australian New Zealand Clinical Trials Registry (ACTRN12614000004662).
Dr. Dreno wasn’t involved in the study but included it in a talk in which she examined the strengths and weaknesses of current rosacea therapies. She is waiting for a confirmatory study before she incorporates Honevo in her own treatment algorithm. She said that she also would like to see studies examining whether combining the topical honey product with prescription drugs for rosacea provides synergistic efficacy.
HoneyLab, which funded the clinical trial and markets Honevo, ships the product to customers worldwide from its New Zealand headquarters.
AT THE EADV CONGRESS
Key clinical point:
Major finding: 34% of rosacea patients experienced clinically meaningful improvement in response to twice-daily kanuka honey face masks, a rate twice that in controls.
Data source: This was a randomized, placebo-controlled, single-blind, 8-week clinical trial involving 138 adults with rosacea.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study.