User login
Four lifestyle changes might prevent 40% of heart failure
LAS VEGAS – Not smoking, maintaining a normal body weight, exercising regularly, and eating a healthy diet would avert roughly 40% of all cases of heart failure, Dr. Luc Djousse asserted at the annual meeting of the Heart Failure Society of America.
“Those four simple lifestyle changes offer a cost-effective opportunity for primary prevention of heart failure in the population,” observed Dr. Djousse, director of research in the division of aging at Brigham and Women’s Hospital, Boston.

The evidence to back his claim comes chiefly from well-conducted epidemiologic studies. For example, in the Physicians Health Study I, involving nearly 21,000 male physicians followed for a mean of 22 years, 40-year-olds who didn’t adhere to any of six key lifestyle factors – maintaining normal body weight, not smoking, regular exercise, moderate alcohol intake, consumption of fruits and vegetables, and eating breakfast cereals – had a lifetime heart failure risk of 21%.(JAMA 2009;302:394-400). “That’s right,” he asserted, “even if you’re a physician.”
In contrast, physicians who adhered to four or more of the six lifestyle factors cut their lifetime risk of heart failure by more than half, to 10.1%.
Similarly, a Finnish national population-based study of 18,346 men and 19,729 women who were ages 25-74, free of heart failure at baseline, and followed for a median of 14.1 years found that women who engaged in four healthy lifestyle behaviors -- not smoking, maintaining normal body weight, physical activity, and liberal intake of vegetables -- were an adjusted 81% less likely to develop heart failure than women who didn’t adhere to any of the four behaviors. Men who followed the four-fold path were 69% less likely to develop heart failure, again after adjusting for age, blood pressure, lipid levels, education, and history of heart disease (Circ. Heart Fail. 2011;4:607-12).
Dr. Djousse said that while Framingham Heart Study data show that hypertension accounts for 39% of the population-attributable risk for heart failure in men and 59% in women, analysis of Physicians Health Study data underscore the negative impact of unhealthy and modifiable lifestyle factors. In that analysis, smoking accounted for 20% of the population attributable risk for heart failure, being sedentary accounted for 12%, alcohol consumption of less than 1 drink per week 10%, and dietary shortcomings less than 10%.
In this analysis, individual dietary aspects made a relatively modest contribution to the incidence of heart failure compared to other modifiable lifestyle factors. Yet dietary issues are a neverending source of fascination both for the general public and physicians. So Dr. Djousse’s update on the evidence regarding a number of hot dietary topics received close attention:
Coffee: A meta-analysis of five prospective studies totalling more than 140,000 participants found a J-shaped dose-response relationship. Consumption of 4 cups per day was optimal, with an associated roughly 10% reduction in heart failure risk (Circ. Heart Fail. 2012;5:401-05). This information elicited a spontaneous cheer -- more of a roar, actually -- from Dr. Djousse’s large audience.
Red meat: In a population-based study of more than 37,000 Swedish men, consumption of at least 75 g/day of processed red meat, such as salami or prosciutto, was independently associated with a 28% increased risk of developing heart failure compared to that of men who ate less than 25 g/day. Intake of unprocessed red meat was unrelated to heart failure risk (Circ. Heart Fail. 2014;7:552-57).
Alcohol: A six-study meta-analysis by Dr. Djousse and coinvestigators concluded that light-to-moderate drinking was associated with a 23% reduction in the risk of heart failure compared to never drinkers. They defined moderate drinking as one to two drinks per day in men and one in women (Phys. Sportsmed. 2010; 38:84-89).
Fish: In a meta-analysis of seven prospective studies featuring more than 176,000 subjects and 5,480 incident cases of heart failure, regular fish consumption was associated with a 15% reduction in the risk of heart failure compared to the lowest category of fish intake (Clin. Nutr. 2012;31:846-53).
Chocolate: Among nearly 32,000 women participating in the prospective Swedish Mammography Cohort study, consumption of one or two servings of chocate per week was associated with a 32% reduction in the risk of incident heart failure in a multivariate analysis compared to no regular chocolate intake. However, no protective effect was seen with consumption or one or more daily servings (Circ. Heart Fail. 2010;3:612-16). Evidence from other studies suggests that dark chocolate, which is rich in cocoa flavinoids, is the type with the most cardioprotective effects, according to Dr. Djousse.
He reported receiving research support from Merck and GlaxoSmithKline and serving as a consultant to Bayer.
LAS VEGAS – Not smoking, maintaining a normal body weight, exercising regularly, and eating a healthy diet would avert roughly 40% of all cases of heart failure, Dr. Luc Djousse asserted at the annual meeting of the Heart Failure Society of America.
“Those four simple lifestyle changes offer a cost-effective opportunity for primary prevention of heart failure in the population,” observed Dr. Djousse, director of research in the division of aging at Brigham and Women’s Hospital, Boston.
The evidence to back his claim comes chiefly from well-conducted epidemiologic studies. For example, in the Physicians Health Study I, involving nearly 21,000 male physicians followed for a mean of 22 years, 40-year-olds who didn’t adhere to any of six key lifestyle factors – maintaining normal body weight, not smoking, regular exercise, moderate alcohol intake, consumption of fruits and vegetables, and eating breakfast cereals – had a lifetime heart failure risk of 21%.(JAMA 2009;302:394-400). “That’s right,” he asserted, “even if you’re a physician.”
In contrast, physicians who adhered to four or more of the six lifestyle factors cut their lifetime risk of heart failure by more than half, to 10.1%.
Similarly, a Finnish national population-based study of 18,346 men and 19,729 women who were ages 25-74, free of heart failure at baseline, and followed for a median of 14.1 years found that women who engaged in four healthy lifestyle behaviors -- not smoking, maintaining normal body weight, physical activity, and liberal intake of vegetables -- were an adjusted 81% less likely to develop heart failure than women who didn’t adhere to any of the four behaviors. Men who followed the four-fold path were 69% less likely to develop heart failure, again after adjusting for age, blood pressure, lipid levels, education, and history of heart disease (Circ. Heart Fail. 2011;4:607-12).
Dr. Djousse said that while Framingham Heart Study data show that hypertension accounts for 39% of the population-attributable risk for heart failure in men and 59% in women, analysis of Physicians Health Study data underscore the negative impact of unhealthy and modifiable lifestyle factors. In that analysis, smoking accounted for 20% of the population attributable risk for heart failure, being sedentary accounted for 12%, alcohol consumption of less than 1 drink per week 10%, and dietary shortcomings less than 10%.
In this analysis, individual dietary aspects made a relatively modest contribution to the incidence of heart failure compared to other modifiable lifestyle factors. Yet dietary issues are a neverending source of fascination both for the general public and physicians. So Dr. Djousse’s update on the evidence regarding a number of hot dietary topics received close attention:
Coffee: A meta-analysis of five prospective studies totalling more than 140,000 participants found a J-shaped dose-response relationship. Consumption of 4 cups per day was optimal, with an associated roughly 10% reduction in heart failure risk (Circ. Heart Fail. 2012;5:401-05). This information elicited a spontaneous cheer -- more of a roar, actually -- from Dr. Djousse’s large audience.
Red meat: In a population-based study of more than 37,000 Swedish men, consumption of at least 75 g/day of processed red meat, such as salami or prosciutto, was independently associated with a 28% increased risk of developing heart failure compared to that of men who ate less than 25 g/day. Intake of unprocessed red meat was unrelated to heart failure risk (Circ. Heart Fail. 2014;7:552-57).
Alcohol: A six-study meta-analysis by Dr. Djousse and coinvestigators concluded that light-to-moderate drinking was associated with a 23% reduction in the risk of heart failure compared to never drinkers. They defined moderate drinking as one to two drinks per day in men and one in women (Phys. Sportsmed. 2010; 38:84-89).
Fish: In a meta-analysis of seven prospective studies featuring more than 176,000 subjects and 5,480 incident cases of heart failure, regular fish consumption was associated with a 15% reduction in the risk of heart failure compared to the lowest category of fish intake (Clin. Nutr. 2012;31:846-53).
Chocolate: Among nearly 32,000 women participating in the prospective Swedish Mammography Cohort study, consumption of one or two servings of chocate per week was associated with a 32% reduction in the risk of incident heart failure in a multivariate analysis compared to no regular chocolate intake. However, no protective effect was seen with consumption or one or more daily servings (Circ. Heart Fail. 2010;3:612-16). Evidence from other studies suggests that dark chocolate, which is rich in cocoa flavinoids, is the type with the most cardioprotective effects, according to Dr. Djousse.
He reported receiving research support from Merck and GlaxoSmithKline and serving as a consultant to Bayer.
LAS VEGAS – Not smoking, maintaining a normal body weight, exercising regularly, and eating a healthy diet would avert roughly 40% of all cases of heart failure, Dr. Luc Djousse asserted at the annual meeting of the Heart Failure Society of America.
“Those four simple lifestyle changes offer a cost-effective opportunity for primary prevention of heart failure in the population,” observed Dr. Djousse, director of research in the division of aging at Brigham and Women’s Hospital, Boston.
The evidence to back his claim comes chiefly from well-conducted epidemiologic studies. For example, in the Physicians Health Study I, involving nearly 21,000 male physicians followed for a mean of 22 years, 40-year-olds who didn’t adhere to any of six key lifestyle factors – maintaining normal body weight, not smoking, regular exercise, moderate alcohol intake, consumption of fruits and vegetables, and eating breakfast cereals – had a lifetime heart failure risk of 21%.(JAMA 2009;302:394-400). “That’s right,” he asserted, “even if you’re a physician.”
In contrast, physicians who adhered to four or more of the six lifestyle factors cut their lifetime risk of heart failure by more than half, to 10.1%.
Similarly, a Finnish national population-based study of 18,346 men and 19,729 women who were ages 25-74, free of heart failure at baseline, and followed for a median of 14.1 years found that women who engaged in four healthy lifestyle behaviors -- not smoking, maintaining normal body weight, physical activity, and liberal intake of vegetables -- were an adjusted 81% less likely to develop heart failure than women who didn’t adhere to any of the four behaviors. Men who followed the four-fold path were 69% less likely to develop heart failure, again after adjusting for age, blood pressure, lipid levels, education, and history of heart disease (Circ. Heart Fail. 2011;4:607-12).
Dr. Djousse said that while Framingham Heart Study data show that hypertension accounts for 39% of the population-attributable risk for heart failure in men and 59% in women, analysis of Physicians Health Study data underscore the negative impact of unhealthy and modifiable lifestyle factors. In that analysis, smoking accounted for 20% of the population attributable risk for heart failure, being sedentary accounted for 12%, alcohol consumption of less than 1 drink per week 10%, and dietary shortcomings less than 10%.
In this analysis, individual dietary aspects made a relatively modest contribution to the incidence of heart failure compared to other modifiable lifestyle factors. Yet dietary issues are a neverending source of fascination both for the general public and physicians. So Dr. Djousse’s update on the evidence regarding a number of hot dietary topics received close attention:
Coffee: A meta-analysis of five prospective studies totalling more than 140,000 participants found a J-shaped dose-response relationship. Consumption of 4 cups per day was optimal, with an associated roughly 10% reduction in heart failure risk (Circ. Heart Fail. 2012;5:401-05). This information elicited a spontaneous cheer -- more of a roar, actually -- from Dr. Djousse’s large audience.
Red meat: In a population-based study of more than 37,000 Swedish men, consumption of at least 75 g/day of processed red meat, such as salami or prosciutto, was independently associated with a 28% increased risk of developing heart failure compared to that of men who ate less than 25 g/day. Intake of unprocessed red meat was unrelated to heart failure risk (Circ. Heart Fail. 2014;7:552-57).
Alcohol: A six-study meta-analysis by Dr. Djousse and coinvestigators concluded that light-to-moderate drinking was associated with a 23% reduction in the risk of heart failure compared to never drinkers. They defined moderate drinking as one to two drinks per day in men and one in women (Phys. Sportsmed. 2010; 38:84-89).
Fish: In a meta-analysis of seven prospective studies featuring more than 176,000 subjects and 5,480 incident cases of heart failure, regular fish consumption was associated with a 15% reduction in the risk of heart failure compared to the lowest category of fish intake (Clin. Nutr. 2012;31:846-53).
Chocolate: Among nearly 32,000 women participating in the prospective Swedish Mammography Cohort study, consumption of one or two servings of chocate per week was associated with a 32% reduction in the risk of incident heart failure in a multivariate analysis compared to no regular chocolate intake. However, no protective effect was seen with consumption or one or more daily servings (Circ. Heart Fail. 2010;3:612-16). Evidence from other studies suggests that dark chocolate, which is rich in cocoa flavinoids, is the type with the most cardioprotective effects, according to Dr. Djousse.
He reported receiving research support from Merck and GlaxoSmithKline and serving as a consultant to Bayer.
EXPERT ANALYSIS FROM THE HFSA ANNUAL SCIENTIFIC MEETING

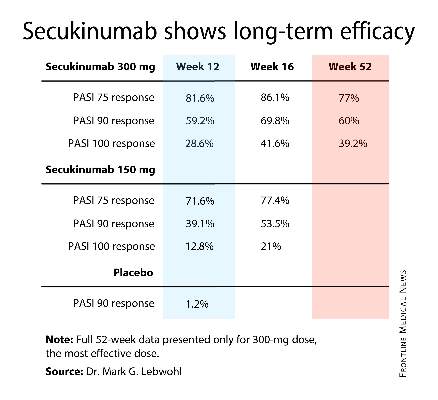
Novel psoriasis biologic wows with jaw-dropping results
AMSTERDAM– The spectacular long-term efficacy achieved with a novel biologic agent for psoriasis in a first-in-humans, proof-of-concept study has raised the prospect of clinical outcomes continuing to ratchet higher in the treatment of moderate-to-severe chronic plaque psoriasis.
How much higher? Six of nine treated patients followed long-term have maintained a PASI 100 response – that is, completely clear – for up to 66 months after a single subcutaneous injection of the agent known for now as BI 655066, Dr. James G. Krueger reported at the annual congress of the European Academy of Dermatology and Venereology.

“For me, this is one of the most interesting features of this proof-of-concept study,” he added. “If this kind of activity is confirmed in the ongoing phase IIb trial, I think this represents the potential for very long-term disease modification. This could become an important agent in the future to treat psoriasis.”
BI 655066 is a monoclonal antibody that specifically targets the p19 subunit of interleukin (IL)-23. Unlike ustekinumab (Stelara), which blocks both IL-23 and IL-12, BI 655066 selectively blocks only IL-23, which Dr. Krueger believes is the central driving force in activating and sustaining the T-cell subsets responsible for the hyperproliferative and inflammatory reactions that define psoriasis.
“This study is all about testing for the specific pathogenic contribution of IL-23 to psoriasis in a first-in-humans study. Our findings really emphasize the importance of IL-23 in driving the key pathways of psoriasis,” observed Dr. Krueger, professor of investigative dermatology and director of the Milstein Medical Research Program at Rockefeller University, New York.
The study included 39 patients with moderate to severe plaque psoriasis. Their baseline PASI was 18, and they averaged more than a 20-year history of psoriasis. Twenty-four patients were randomized 3:1 to a single intravenous injection of BI 655066 at various doses ranging from 0.01 mg/kg to 5 mg/kg or to placebo in order to get an initial sense of the agent’s safety and tolerability.
In the second part of the study, 15 other participants received a single subcutaneous injection: two got placebo and the rest were randomized to BI 655066 at either 0.25 mg/kg or 1.0 mg/kg. Safety and efficacy were assessed at weeks 0, 2, 4, 12, and 24. In addition, skin biopsies were obtained at weeks 0 and 8 for immunohistochemistry studies and RNA sequencing analysis.
By week 12, the PASI 75 response rate in subcutaneous BI 655066 recipients was 87% and the PASI 90 rate was 58%. At week 24, nine patients elected to continue structured prospective follow-up while remaining off treatment, including six PASI 100 responders. Those six PASI 100 responders remained PASI 100 at ongoing follow-up 48-66 weeks after receiving their single dose of the agent.
Biopsy specimens obtained at week 8 showed normalization of the epidermal psoriasiform hyperplasia which had been present at baseline. A normal-looking granular layer had been reestablished. “This looks essentially like the pattern of normal or nonlesional skin,” according to the dermatologist.
RNA sequencing analysis and gene profiling showed normalized production of the IL-23/IL-17-induced proteins that had been strongly overexpressed at baseline, including lipocalin, beta-defensin, and psoriasin.
“The immune axis is turned down. The number of immune cells is way down, although they’re not completely eliminated. With placebo, you still see a psoriasislike pattern of the disease. With blockade of IL-23, most cases have a gene profile like nonlesional skin. This represents a profound cellular and disease modulation,” Dr. Krueger said.
Among all 39 participants, the only serious adverse event deemed possibly treatment related was a 5-minute transient ischemic attack (TIA) episode in a patient on BI 655066. This caught Dr. Krueger’s attention as a possible red flag; however, he noted that more than 200 patients have since received the biologic agent in the ongoing phase IIb trial, with no reported major adverse cardiovascular events.
“I think that TIA may just be bad luck with small numbers,” he added.
Asked what he thinks might explain the remarkably lengthy disease remission seen following a single dose of the biologic, Dr. Krueger offered two possibilities.
“It may be that IL-23 is necessary to sustain pathogenic clones of memory cells in the skin, and as we get rid of it those clones most likely apoptose. And if you’ve sufficiently removed the clones, then you don’t get the expansion. That’s guess one. Guess two would be that we’ve renormalized tolerance mechanisms in some way. Both of these hypotheses can be tested,” according to Dr. Krueger.
The study was funded by Boehringer Ingelheim. Dr. Krueger reported receiving funding from that pharmaceutical company and nearly two dozen others.
AMSTERDAM– The spectacular long-term efficacy achieved with a novel biologic agent for psoriasis in a first-in-humans, proof-of-concept study has raised the prospect of clinical outcomes continuing to ratchet higher in the treatment of moderate-to-severe chronic plaque psoriasis.
How much higher? Six of nine treated patients followed long-term have maintained a PASI 100 response – that is, completely clear – for up to 66 months after a single subcutaneous injection of the agent known for now as BI 655066, Dr. James G. Krueger reported at the annual congress of the European Academy of Dermatology and Venereology.
“For me, this is one of the most interesting features of this proof-of-concept study,” he added. “If this kind of activity is confirmed in the ongoing phase IIb trial, I think this represents the potential for very long-term disease modification. This could become an important agent in the future to treat psoriasis.”
BI 655066 is a monoclonal antibody that specifically targets the p19 subunit of interleukin (IL)-23. Unlike ustekinumab (Stelara), which blocks both IL-23 and IL-12, BI 655066 selectively blocks only IL-23, which Dr. Krueger believes is the central driving force in activating and sustaining the T-cell subsets responsible for the hyperproliferative and inflammatory reactions that define psoriasis.
“This study is all about testing for the specific pathogenic contribution of IL-23 to psoriasis in a first-in-humans study. Our findings really emphasize the importance of IL-23 in driving the key pathways of psoriasis,” observed Dr. Krueger, professor of investigative dermatology and director of the Milstein Medical Research Program at Rockefeller University, New York.
The study included 39 patients with moderate to severe plaque psoriasis. Their baseline PASI was 18, and they averaged more than a 20-year history of psoriasis. Twenty-four patients were randomized 3:1 to a single intravenous injection of BI 655066 at various doses ranging from 0.01 mg/kg to 5 mg/kg or to placebo in order to get an initial sense of the agent’s safety and tolerability.
In the second part of the study, 15 other participants received a single subcutaneous injection: two got placebo and the rest were randomized to BI 655066 at either 0.25 mg/kg or 1.0 mg/kg. Safety and efficacy were assessed at weeks 0, 2, 4, 12, and 24. In addition, skin biopsies were obtained at weeks 0 and 8 for immunohistochemistry studies and RNA sequencing analysis.
By week 12, the PASI 75 response rate in subcutaneous BI 655066 recipients was 87% and the PASI 90 rate was 58%. At week 24, nine patients elected to continue structured prospective follow-up while remaining off treatment, including six PASI 100 responders. Those six PASI 100 responders remained PASI 100 at ongoing follow-up 48-66 weeks after receiving their single dose of the agent.
Biopsy specimens obtained at week 8 showed normalization of the epidermal psoriasiform hyperplasia which had been present at baseline. A normal-looking granular layer had been reestablished. “This looks essentially like the pattern of normal or nonlesional skin,” according to the dermatologist.
RNA sequencing analysis and gene profiling showed normalized production of the IL-23/IL-17-induced proteins that had been strongly overexpressed at baseline, including lipocalin, beta-defensin, and psoriasin.
“The immune axis is turned down. The number of immune cells is way down, although they’re not completely eliminated. With placebo, you still see a psoriasislike pattern of the disease. With blockade of IL-23, most cases have a gene profile like nonlesional skin. This represents a profound cellular and disease modulation,” Dr. Krueger said.
Among all 39 participants, the only serious adverse event deemed possibly treatment related was a 5-minute transient ischemic attack (TIA) episode in a patient on BI 655066. This caught Dr. Krueger’s attention as a possible red flag; however, he noted that more than 200 patients have since received the biologic agent in the ongoing phase IIb trial, with no reported major adverse cardiovascular events.
“I think that TIA may just be bad luck with small numbers,” he added.
Asked what he thinks might explain the remarkably lengthy disease remission seen following a single dose of the biologic, Dr. Krueger offered two possibilities.
“It may be that IL-23 is necessary to sustain pathogenic clones of memory cells in the skin, and as we get rid of it those clones most likely apoptose. And if you’ve sufficiently removed the clones, then you don’t get the expansion. That’s guess one. Guess two would be that we’ve renormalized tolerance mechanisms in some way. Both of these hypotheses can be tested,” according to Dr. Krueger.
The study was funded by Boehringer Ingelheim. Dr. Krueger reported receiving funding from that pharmaceutical company and nearly two dozen others.
AMSTERDAM– The spectacular long-term efficacy achieved with a novel biologic agent for psoriasis in a first-in-humans, proof-of-concept study has raised the prospect of clinical outcomes continuing to ratchet higher in the treatment of moderate-to-severe chronic plaque psoriasis.
How much higher? Six of nine treated patients followed long-term have maintained a PASI 100 response – that is, completely clear – for up to 66 months after a single subcutaneous injection of the agent known for now as BI 655066, Dr. James G. Krueger reported at the annual congress of the European Academy of Dermatology and Venereology.
“For me, this is one of the most interesting features of this proof-of-concept study,” he added. “If this kind of activity is confirmed in the ongoing phase IIb trial, I think this represents the potential for very long-term disease modification. This could become an important agent in the future to treat psoriasis.”
BI 655066 is a monoclonal antibody that specifically targets the p19 subunit of interleukin (IL)-23. Unlike ustekinumab (Stelara), which blocks both IL-23 and IL-12, BI 655066 selectively blocks only IL-23, which Dr. Krueger believes is the central driving force in activating and sustaining the T-cell subsets responsible for the hyperproliferative and inflammatory reactions that define psoriasis.
“This study is all about testing for the specific pathogenic contribution of IL-23 to psoriasis in a first-in-humans study. Our findings really emphasize the importance of IL-23 in driving the key pathways of psoriasis,” observed Dr. Krueger, professor of investigative dermatology and director of the Milstein Medical Research Program at Rockefeller University, New York.
The study included 39 patients with moderate to severe plaque psoriasis. Their baseline PASI was 18, and they averaged more than a 20-year history of psoriasis. Twenty-four patients were randomized 3:1 to a single intravenous injection of BI 655066 at various doses ranging from 0.01 mg/kg to 5 mg/kg or to placebo in order to get an initial sense of the agent’s safety and tolerability.
In the second part of the study, 15 other participants received a single subcutaneous injection: two got placebo and the rest were randomized to BI 655066 at either 0.25 mg/kg or 1.0 mg/kg. Safety and efficacy were assessed at weeks 0, 2, 4, 12, and 24. In addition, skin biopsies were obtained at weeks 0 and 8 for immunohistochemistry studies and RNA sequencing analysis.
By week 12, the PASI 75 response rate in subcutaneous BI 655066 recipients was 87% and the PASI 90 rate was 58%. At week 24, nine patients elected to continue structured prospective follow-up while remaining off treatment, including six PASI 100 responders. Those six PASI 100 responders remained PASI 100 at ongoing follow-up 48-66 weeks after receiving their single dose of the agent.
Biopsy specimens obtained at week 8 showed normalization of the epidermal psoriasiform hyperplasia which had been present at baseline. A normal-looking granular layer had been reestablished. “This looks essentially like the pattern of normal or nonlesional skin,” according to the dermatologist.
RNA sequencing analysis and gene profiling showed normalized production of the IL-23/IL-17-induced proteins that had been strongly overexpressed at baseline, including lipocalin, beta-defensin, and psoriasin.
“The immune axis is turned down. The number of immune cells is way down, although they’re not completely eliminated. With placebo, you still see a psoriasislike pattern of the disease. With blockade of IL-23, most cases have a gene profile like nonlesional skin. This represents a profound cellular and disease modulation,” Dr. Krueger said.
Among all 39 participants, the only serious adverse event deemed possibly treatment related was a 5-minute transient ischemic attack (TIA) episode in a patient on BI 655066. This caught Dr. Krueger’s attention as a possible red flag; however, he noted that more than 200 patients have since received the biologic agent in the ongoing phase IIb trial, with no reported major adverse cardiovascular events.
“I think that TIA may just be bad luck with small numbers,” he added.
Asked what he thinks might explain the remarkably lengthy disease remission seen following a single dose of the biologic, Dr. Krueger offered two possibilities.
“It may be that IL-23 is necessary to sustain pathogenic clones of memory cells in the skin, and as we get rid of it those clones most likely apoptose. And if you’ve sufficiently removed the clones, then you don’t get the expansion. That’s guess one. Guess two would be that we’ve renormalized tolerance mechanisms in some way. Both of these hypotheses can be tested,” according to Dr. Krueger.
The study was funded by Boehringer Ingelheim. Dr. Krueger reported receiving funding from that pharmaceutical company and nearly two dozen others.
AT THE EADV CONGRESS
Key clinical point: Up to 66 months after receiving a single subcutaneous injection of a biologic agent that selectively blocks interleukin-23, six patients with moderate to severe chronic plaque psoriasis at baseline remained PASI 100 responders with clear skin.
Major finding: The PASI 75 response rate 12 weeks after receiving a single dose of the investigational agent BI 655066 was 87%, and the PASI 90 rate was 58%.
Data source: This was a first-in-humans, proof-of-concept study involving 39 psoriasis patients.
Disclosures: The study was sponsored by Boehringer Ingelheim. The presenter reported receiving research funding from that pharmaceutical company and nearly two dozen others.

British study downplays cognitive impact of adolescent cannabis use
BERLIN – Occasional to moderate cannabis use at a young age is not associated with detrimental effects on cognition or educational performance, according to the findings of a large U.K. study.
Adolescents with heavier use – defined in the study as self-reported lifetime use of cannabis 50 times or more by age 15 – had a modest 2.9% decrease in educational performance on a compulsory school exam given at age 15 or 16, compared with never-users. However, heavier use had no impact at all on IQ scores measured at age 15 after adjustment for potential confounding factors, Claire Mokrysz reported at the annual congress of the European College of Neuropsychopharmacology.

These results from the Avon Longitudinal Study of Parents and Children (ALSPAC), also known as “the Children of the 90’s Study,” stand in sharp contrast to those from an earlier Duke University study, which concluded that cannabis use likely has a neurotoxic effect on the adolescent brain that is apparent in midlife (Proc. Natl. Acad. Sci. USA 2012;109: E2657-64).
“Previous research findings showing poorer cognitive performance in cannabis users may have resulted from the lifestyle, behavior, and personal history typically associated with cannabis use rather than cannabis use itself,” said Ms. Mokrysz, of University College London.
She reported on 2,612 children in ALSPAC who had their IQ tested at ages 8 and 15.
Adolescents with heavier cannabis use by age 15 had a nearly a 3-point lower IQ at that age than did never users, after adjustment for IQ at age 8. However, upon further adjustment for maternal education, pregnancy, and early-life factors, and use of tobacco, alcohol, and other recreational drugs, the difference in IQ between heavier and never-users vanished.
Heavier users of cannabis scored an initially impressive 11% lower than never-users on the standardized educational performance exam in an unadjusted analysis. After adjustment for the potential confounders, however, the difference shrank to a modest 2.9%.
“People often believe that using cannabis can be very damaging to intellectual ability in the long term, but it is extremely difficult to separate the direct effects of cannabis from other potential explanations,” she said. “This is a potentially important public health message: The belief that cannabis is particularly harmful may detract focus from and awareness of other potentially harmful behaviors.”
ECNP President Guy Goodwin called the ALSPAC analysis potentially important.
“It suggests that the current focus on the alleged harms of cannabis may be obscuring the fact that its use is often correlated with that of other even more freely available drugs and possibly lifestyle factors. These may be as or more important than cannabis itself,” said Dr. Goodwin, professor of psychiatry at the University of Oxford (England).
The ALSPAC study is funded by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. Ms. Mokrysz reported having no financial conflicts.
BERLIN – Occasional to moderate cannabis use at a young age is not associated with detrimental effects on cognition or educational performance, according to the findings of a large U.K. study.
Adolescents with heavier use – defined in the study as self-reported lifetime use of cannabis 50 times or more by age 15 – had a modest 2.9% decrease in educational performance on a compulsory school exam given at age 15 or 16, compared with never-users. However, heavier use had no impact at all on IQ scores measured at age 15 after adjustment for potential confounding factors, Claire Mokrysz reported at the annual congress of the European College of Neuropsychopharmacology.
These results from the Avon Longitudinal Study of Parents and Children (ALSPAC), also known as “the Children of the 90’s Study,” stand in sharp contrast to those from an earlier Duke University study, which concluded that cannabis use likely has a neurotoxic effect on the adolescent brain that is apparent in midlife (Proc. Natl. Acad. Sci. USA 2012;109: E2657-64).
“Previous research findings showing poorer cognitive performance in cannabis users may have resulted from the lifestyle, behavior, and personal history typically associated with cannabis use rather than cannabis use itself,” said Ms. Mokrysz, of University College London.
She reported on 2,612 children in ALSPAC who had their IQ tested at ages 8 and 15.
Adolescents with heavier cannabis use by age 15 had a nearly a 3-point lower IQ at that age than did never users, after adjustment for IQ at age 8. However, upon further adjustment for maternal education, pregnancy, and early-life factors, and use of tobacco, alcohol, and other recreational drugs, the difference in IQ between heavier and never-users vanished.
Heavier users of cannabis scored an initially impressive 11% lower than never-users on the standardized educational performance exam in an unadjusted analysis. After adjustment for the potential confounders, however, the difference shrank to a modest 2.9%.
“People often believe that using cannabis can be very damaging to intellectual ability in the long term, but it is extremely difficult to separate the direct effects of cannabis from other potential explanations,” she said. “This is a potentially important public health message: The belief that cannabis is particularly harmful may detract focus from and awareness of other potentially harmful behaviors.”
ECNP President Guy Goodwin called the ALSPAC analysis potentially important.
“It suggests that the current focus on the alleged harms of cannabis may be obscuring the fact that its use is often correlated with that of other even more freely available drugs and possibly lifestyle factors. These may be as or more important than cannabis itself,” said Dr. Goodwin, professor of psychiatry at the University of Oxford (England).
The ALSPAC study is funded by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. Ms. Mokrysz reported having no financial conflicts.
BERLIN – Occasional to moderate cannabis use at a young age is not associated with detrimental effects on cognition or educational performance, according to the findings of a large U.K. study.
Adolescents with heavier use – defined in the study as self-reported lifetime use of cannabis 50 times or more by age 15 – had a modest 2.9% decrease in educational performance on a compulsory school exam given at age 15 or 16, compared with never-users. However, heavier use had no impact at all on IQ scores measured at age 15 after adjustment for potential confounding factors, Claire Mokrysz reported at the annual congress of the European College of Neuropsychopharmacology.
These results from the Avon Longitudinal Study of Parents and Children (ALSPAC), also known as “the Children of the 90’s Study,” stand in sharp contrast to those from an earlier Duke University study, which concluded that cannabis use likely has a neurotoxic effect on the adolescent brain that is apparent in midlife (Proc. Natl. Acad. Sci. USA 2012;109: E2657-64).
“Previous research findings showing poorer cognitive performance in cannabis users may have resulted from the lifestyle, behavior, and personal history typically associated with cannabis use rather than cannabis use itself,” said Ms. Mokrysz, of University College London.
She reported on 2,612 children in ALSPAC who had their IQ tested at ages 8 and 15.
Adolescents with heavier cannabis use by age 15 had a nearly a 3-point lower IQ at that age than did never users, after adjustment for IQ at age 8. However, upon further adjustment for maternal education, pregnancy, and early-life factors, and use of tobacco, alcohol, and other recreational drugs, the difference in IQ between heavier and never-users vanished.
Heavier users of cannabis scored an initially impressive 11% lower than never-users on the standardized educational performance exam in an unadjusted analysis. After adjustment for the potential confounders, however, the difference shrank to a modest 2.9%.
“People often believe that using cannabis can be very damaging to intellectual ability in the long term, but it is extremely difficult to separate the direct effects of cannabis from other potential explanations,” she said. “This is a potentially important public health message: The belief that cannabis is particularly harmful may detract focus from and awareness of other potentially harmful behaviors.”
ECNP President Guy Goodwin called the ALSPAC analysis potentially important.
“It suggests that the current focus on the alleged harms of cannabis may be obscuring the fact that its use is often correlated with that of other even more freely available drugs and possibly lifestyle factors. These may be as or more important than cannabis itself,” said Dr. Goodwin, professor of psychiatry at the University of Oxford (England).
The ALSPAC study is funded by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. Ms. Mokrysz reported having no financial conflicts.
AT THE ECNP CONGRESS
Key clinical point: “Previous research findings showing poorer cognitive performance in cannabis users may have resulted from the lifestyle, behavior, and personal history typically associated with cannabis use rather than cannabis use itself.”
Major finding: Teens who reported using cannabis 50 times or more by age 15 did not have a lower IQ than never-users, although they did score marginally lower on a standardized educational performance exam.
Data source: This analysis from the Avon Longitudinal Study of Parents and Children included 2,612 youths who underwent IQ testing at ages 8 and 15.
Disclosures: The ongoing study is funded by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. The presenter reported having no financial conflicts.

DSM-5 hasn’t opened adult ADHD floodgates
BERLIN – Concerns that the liberalized criteria for adult attention-deficit/hyperactivity disorder adopted in the DSM-5 would greatly inflate the disorder’s prevalence appear to have been misplaced.
“The adult ADHD prevalence under DSM-5 is in the same range as ADHD not otherwise specified in DSM-IV. There’s no dramatic increase,” Dr. Josep Antoni Ramos-Quiroga said at the annual congress of the European College of Neuropsychopharmacology.

The DSM-IV and DSM-5 criteria differ in two ways. One difference is that the required age of onset for ADHD symptoms has changed from prior to age 7 years to prior to age 12 years. The other change is that the minimum number of symptoms of attention and/or hyperactivity/impulsivity required for the diagnosis has decreased from 6 to 5 out of a possible 9.
These changes came under fire from some quarters during the lengthy DSM-5 development process, but two recent large studies suggest that the clinical impact of the revised criteria is minimal, according to Dr. Ramos-Quiroga, coordinator of the ADHD program at Vall d’Hebron University Hospital in Barcelona.
He was a coinvestigator in the ADPSYC study, an observational study in which 1,986 nonpsychotic psychiatric outpatients in eight European countries were evaluated for adult ADHD. As he and his colleagues predicted, the prevalence of the disorder proved much higher than the consensus estimate of 2.5% in the general adult population. Indeed, using the Diagnostic Interview for ADHD in Adults (DIVA) based upon the DSM-IV criteria, 15.8% of the psychiatric patients in a variety of outpatient settings had adult ADHD. When the investigators applied the DSM-5 criteria, the prevalence rose to 17.4%.
Dr. Ramos-Quiroga also was a coinvestigator in the International ADHD in Substance Use Disorders Prevalence study (IASP), a cross-sectional study involving 3,558 treatment-seeking substance-use disorder (SUD) patients in the United States, Australia, and eight European countries. The prevalence of adult ADHD by DSM-IV criteria varied substantially from country to country but averaged 13.9% overall. By DSM-5 criteria, the prevalence was only slightly higher (Drug Alcohol Depend. 2014;134:158-66).
It has been known for at least 2 decades that adults with SUD have an increased prevalence of comorbid ADHD, compared with the general population and that these dual-diagnosis patients have a more severe course of substance use, the psychiatrist noted.
In another report from the IASP study, Dr. Ramos-Quiroga and his colleagues found that SUD patients with adult ADHD had a 7-fold greater rate of borderline personality disorder, a 2.8-fold increase in antisocial personality disorder, and a 4.3-fold greater prevalence of hypomanic episodes, compared with SUD patients without ADHD. Also, among the subset of patients with alcohol as their primary substance of abuse, those with adult ADHD had a 4.3-fold greater prevalence of major depression than those without ADHD (Addiction 2014;109:262-72).
The ADPSYC study was supported by Eli Lilly. Dr. Ramos-Quiroga reported acting as a consultant to and serving on the speakers bureau for that pharmaceutical company and a handful of others. The IASP study was supported by the International Collaboration on ADHD and Substance Abuse.
BERLIN – Concerns that the liberalized criteria for adult attention-deficit/hyperactivity disorder adopted in the DSM-5 would greatly inflate the disorder’s prevalence appear to have been misplaced.
“The adult ADHD prevalence under DSM-5 is in the same range as ADHD not otherwise specified in DSM-IV. There’s no dramatic increase,” Dr. Josep Antoni Ramos-Quiroga said at the annual congress of the European College of Neuropsychopharmacology.
The DSM-IV and DSM-5 criteria differ in two ways. One difference is that the required age of onset for ADHD symptoms has changed from prior to age 7 years to prior to age 12 years. The other change is that the minimum number of symptoms of attention and/or hyperactivity/impulsivity required for the diagnosis has decreased from 6 to 5 out of a possible 9.
These changes came under fire from some quarters during the lengthy DSM-5 development process, but two recent large studies suggest that the clinical impact of the revised criteria is minimal, according to Dr. Ramos-Quiroga, coordinator of the ADHD program at Vall d’Hebron University Hospital in Barcelona.
He was a coinvestigator in the ADPSYC study, an observational study in which 1,986 nonpsychotic psychiatric outpatients in eight European countries were evaluated for adult ADHD. As he and his colleagues predicted, the prevalence of the disorder proved much higher than the consensus estimate of 2.5% in the general adult population. Indeed, using the Diagnostic Interview for ADHD in Adults (DIVA) based upon the DSM-IV criteria, 15.8% of the psychiatric patients in a variety of outpatient settings had adult ADHD. When the investigators applied the DSM-5 criteria, the prevalence rose to 17.4%.
Dr. Ramos-Quiroga also was a coinvestigator in the International ADHD in Substance Use Disorders Prevalence study (IASP), a cross-sectional study involving 3,558 treatment-seeking substance-use disorder (SUD) patients in the United States, Australia, and eight European countries. The prevalence of adult ADHD by DSM-IV criteria varied substantially from country to country but averaged 13.9% overall. By DSM-5 criteria, the prevalence was only slightly higher (Drug Alcohol Depend. 2014;134:158-66).
It has been known for at least 2 decades that adults with SUD have an increased prevalence of comorbid ADHD, compared with the general population and that these dual-diagnosis patients have a more severe course of substance use, the psychiatrist noted.
In another report from the IASP study, Dr. Ramos-Quiroga and his colleagues found that SUD patients with adult ADHD had a 7-fold greater rate of borderline personality disorder, a 2.8-fold increase in antisocial personality disorder, and a 4.3-fold greater prevalence of hypomanic episodes, compared with SUD patients without ADHD. Also, among the subset of patients with alcohol as their primary substance of abuse, those with adult ADHD had a 4.3-fold greater prevalence of major depression than those without ADHD (Addiction 2014;109:262-72).
The ADPSYC study was supported by Eli Lilly. Dr. Ramos-Quiroga reported acting as a consultant to and serving on the speakers bureau for that pharmaceutical company and a handful of others. The IASP study was supported by the International Collaboration on ADHD and Substance Abuse.
BERLIN – Concerns that the liberalized criteria for adult attention-deficit/hyperactivity disorder adopted in the DSM-5 would greatly inflate the disorder’s prevalence appear to have been misplaced.
“The adult ADHD prevalence under DSM-5 is in the same range as ADHD not otherwise specified in DSM-IV. There’s no dramatic increase,” Dr. Josep Antoni Ramos-Quiroga said at the annual congress of the European College of Neuropsychopharmacology.
The DSM-IV and DSM-5 criteria differ in two ways. One difference is that the required age of onset for ADHD symptoms has changed from prior to age 7 years to prior to age 12 years. The other change is that the minimum number of symptoms of attention and/or hyperactivity/impulsivity required for the diagnosis has decreased from 6 to 5 out of a possible 9.
These changes came under fire from some quarters during the lengthy DSM-5 development process, but two recent large studies suggest that the clinical impact of the revised criteria is minimal, according to Dr. Ramos-Quiroga, coordinator of the ADHD program at Vall d’Hebron University Hospital in Barcelona.
He was a coinvestigator in the ADPSYC study, an observational study in which 1,986 nonpsychotic psychiatric outpatients in eight European countries were evaluated for adult ADHD. As he and his colleagues predicted, the prevalence of the disorder proved much higher than the consensus estimate of 2.5% in the general adult population. Indeed, using the Diagnostic Interview for ADHD in Adults (DIVA) based upon the DSM-IV criteria, 15.8% of the psychiatric patients in a variety of outpatient settings had adult ADHD. When the investigators applied the DSM-5 criteria, the prevalence rose to 17.4%.
Dr. Ramos-Quiroga also was a coinvestigator in the International ADHD in Substance Use Disorders Prevalence study (IASP), a cross-sectional study involving 3,558 treatment-seeking substance-use disorder (SUD) patients in the United States, Australia, and eight European countries. The prevalence of adult ADHD by DSM-IV criteria varied substantially from country to country but averaged 13.9% overall. By DSM-5 criteria, the prevalence was only slightly higher (Drug Alcohol Depend. 2014;134:158-66).
It has been known for at least 2 decades that adults with SUD have an increased prevalence of comorbid ADHD, compared with the general population and that these dual-diagnosis patients have a more severe course of substance use, the psychiatrist noted.
In another report from the IASP study, Dr. Ramos-Quiroga and his colleagues found that SUD patients with adult ADHD had a 7-fold greater rate of borderline personality disorder, a 2.8-fold increase in antisocial personality disorder, and a 4.3-fold greater prevalence of hypomanic episodes, compared with SUD patients without ADHD. Also, among the subset of patients with alcohol as their primary substance of abuse, those with adult ADHD had a 4.3-fold greater prevalence of major depression than those without ADHD (Addiction 2014;109:262-72).
The ADPSYC study was supported by Eli Lilly. Dr. Ramos-Quiroga reported acting as a consultant to and serving on the speakers bureau for that pharmaceutical company and a handful of others. The IASP study was supported by the International Collaboration on ADHD and Substance Abuse.
EXPERT ANALYSIS FROM THE ECNP CONGRESS

MS Overrepresented in Depression, Bipolar; Schizophrenia Possibly Protective
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.
The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.
The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.
The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
AT THE ECNP CONGRESS
MS overrepresented in depression, bipolar; schizophrenia possibly protective
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.

The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.
The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
BERLIN– The risk of multiple sclerosis in patients with depression or bipolar disorder is roughly double that of controls free of those psychiatric diagnoses, according to a Swedish national study.
In contrast, having schizophrenia actually appeared to protect against developing MS, a finding that cries out for further study, Dr. Viktoria Johansson observed at the annual congress of the European College of Neuropsychopharmacology.
The observed association between MS and mood disorders cannot be explained by shared genetic predisposition. In this Swedish study, having a sibling with depression or bipolar disorder did not increase an individual’s risk of MS, noted Dr. Johansson, a psychiatrist at the Karolinska Institute, Stockholm.
She and her coinvestigators searched the Sweden’s National Patient Register, which incorporates the nation’s entire 8.2 million population and identified all individuals born during 1932-1991 who carried an ICD diagnosis of depression (172,479 patients), bipolar disorder (30,761), bipolar type 1 (8,695), schizophrenia (22,781), or MS (16,467 patients). Ten unaffected controls matched for birth year and sex were randomly selected for each subject. The prevalence of MS was 83% greater in patients with bipolar disorder than in controls. The prevalence of the neurologic disease was 2.29-fold greater in those with bipolar type 1. Patients diagnosed with depression had an 86% increase in MS.
In contrast, individuals with schizophrenia were 38% less likely to have MS than did controls. This finding came as a surprise to the investigators. MS is an autoimmune inflammatory disease, and mounting evidence points to neuroinflammation as playing a key role in depression, bipolar disease, and schizophrenia. However, while some smaller prior studies have reported an association between MS and schizophrenia and others have not, the very large Swedish registry study is the first to point to the psychotic disorder having a possible protective effect.
One hypothesis Dr. Johansson hopes to explore further is that contemporary antipsychotic medications exert a protective effect against MS. That would be ironic, given that the first-generation antipsychotics were famous for causing movement disorders, particularly tardive dyskinesia, as a prominent side effect.
Dr. Johansson’s study was funded by the Swedish Society of Medicine and the Karolinska Institute. She reported having no financial conflicts.
AT THE ECNP CONGRESS
Key clinical point: Be on the lookout for the development of neurologic symptoms in patients with major depression or bipolar disorder.
Major finding: The risk of multiple sclerosis is increased by 83% in patients with bipolar disorder, while those with bipolar type I had a 2.29-fold increased risk, and patients with depression are at 86% increased risk for MS, compared with the general population.
Data source: This was a Swedish national study that compared the MS rates in more than 30,000 Swedes diagnosed with bipolar disorder, 172,000 with depression, and nearly 23,000 with schizophrenia to a 10-fold larger population of matched controls.
Disclosures: The study was funded by the Swedish Society of Medicine and the Karolinska Institute. The presenter reported having no financial conflicts.
Consider ADHD in adult nonpsychotic psychiatric outpatients
BERLIN – The prevalence of attention-deficit/hyperactivity disorder among nonpsychotic adults in outpatient settings is markedly higher than in the general adult population, according to a major eight-nation observational study.
“I think this is a wake-up call for clinicians to include adult ADHD in their differential diagnostic considerations in a broad range of psychiatric patients,” Dr. Johannes Thome said in presenting the ADPSYC study results at the annual congress of the European College of Neuropsychopharmacology.
The study included 2,284 unselected participants in eight European countries. Nonpsychotic patients in outpatient care for any psychiatric disorder were eligible. A variety of outpatient settings were deliberately included: private psychiatric practices, community mental health centers, outpatient psychiatric clinics associated with medical centers, and outpatient clinics linked with psychiatric hospitals.
Participants were asked whether they’d ever been diagnosed with ADHD and also were screened using the Adult ADHD Self-Report Scale. If ADHD was suspected on either basis, they were further assessed using the Diagnostic Interview for ADHD in Adults, upon which the diagnosis hinged.
A total of 15.8% of the psychiatric outpatients were diagnosed with adult ADHD based on the criteria of the DSM-IV, 4th edition, as were 17.4% using DSM-5 criteria. In contrast, the consensus estimate of the prevalence of ADHD in the general adult population is 2.5%.
By DSM-IV criteria, 4.7% of the total ADPSYC population had the inattentive subtype of ADHD, 1.1% had the hyperactive/impulsive subtype, and 10% had the combined form, reported Dr. Thome, professor and chair of the department of psychiatry at the University of Rostock in Germany.
As is seen in the general population, the prevalence of ADHD in psychiatric outpatients was lower in women: 14.4%, compared with 21.6% among men. Illustrating the dictum that ADHD runs in families, 14.9% of patients with ADHD had a first-degree relative who’d been diagnosed with the disorder, as did just 3.7% of psychiatric outpatients without ADHD.
Twenty percent of patients with ADHD met criteria for substance abuse or dependence, compared with 12.6% of non-ADHD patients.
Quality of life and disability burden were assessed in all ADPSYC participants via the Clinical Global Impressions-Severity scale, (CGI-S); the Sheehan Disability Scale; and the EuroQol-5 Dimension questionnaire. These metrics showed that adult psychiatric outpatients with ADHD had significantly worse quality of life and more overall disability than outpatients without ADHD. For example, the mean CGI-S score in outpatients with ADHD was 3.8, compared with 3.3 in outpatients without ADHD. Sixty-four percent of outpatients with ADHD had scores placing them in the moderately, markedly, or severely ill range, compared with 47% of psychiatric patients without ADHD.
Moreover, the mean total score on the Sheehan Disability Scale averaged 18.9 in outpatients with ADHD, compared with 11.6 in psychiatric patients without ADHD. Those with ADHD scored markedly worse in multiple domains, including social life, family life, work/school, and underproductive days in the past week.
On the EuroQol-5 Dimension questionnaire, 25% of patients with ADHD reported being extremely anxious or depressed, compared with 16% without ADHD, Dr. Thome continued.
He emphasized that these quality of life impairment and disability scores highlight a key point about adult ADHD, one that applies to affected patients regardless of whether or not they have a comorbid psychiatric disorder: The impact of adult ADHD extends well beyond the core symptoms.
While ADHD by definition in the DSM-5 must start before age 12, “You have to expect that the older an affected patient gets, the more social problems will occur and the more comorbidity you’ll see,” he observed.
“If you are a clinician, you will probably never, ever find a patient who comes to you and says, ‘Doctor, I’m suffering from inattention, and I’m so impulsive, and my mood regulation doesn’t work well.’ Rather, they’ll come to you and say, ‘I have a problem at my workplace; I’m always having arguments with my boss and with my wife,’ ” according to the psychiatrist. “From the patient’s perspective, usually it’s much more important how their quality of life changes with treatment, rather than how much certain ADHD scales change.”
Along those lines, it’s important to note that numerous studies have demonstrated that individuals with adult ADHD have three times more emergency department visits, a 10-fold greater rate of outpatient medical visits, and three times more inpatient hospitalizations than the general adult population. They also have an increased risk of serious motor vehicle accidents, which appears to be reduced with the use of ADHD medications (JAMA Psychiatry 2014;71:319-25). A study by Dr. Thome and his colleagues showed that adult ADHD is also accompanied by significant alterations in circadian rhythms at the endocrine, genetic, and behavioral levels (Mol. Psychiatry 2012;17:988-95), which may in part explain the patients’ propensity for mishaps.
Moreover, a major Swedish national registry study involving more than 25,000 patients with adult ADHD established that the disorder is associated with increased rates of criminality, and that during periods when patients were on ADHD medications, their risk of arrests and convictions was significantly reduced (N. Engl. J. Med. 2012;367:2006-14). But while this study drew extensive media attention, heralding a “treatment for criminality,” Dr. Thome cautioned that association in an observational study does not prove causality.
“Some people argue that because they can’t focus and are so impatient, people with adult ADHD are simply worse at hiding the crime and are much more easily caught by the police, and that during periods when they’re on medication they are more likely to be seeing a social worker or have other social support. That might be a partial explanation,” Dr. Thome said. “But my main point here is I want you to understand that you don’t need to be afraid of adult ADHD patients. They’re not more dangerous than others.”
With regard to treatment, he emphasized that a comprehensive plan for adult ADHD needs to address psychological, behavioral, and educational or occupational needs with a range of interventions.
“I want to make the point that psychologic therapy is at least as important as medication,” Dr. Thome said. “Pills don’t give you skills.”
The ADPSYC study was funded by Eli Lilly. Dr. Thome reported having received research grants and/or serving on advisory boards for Lilly and more than a dozen other companies.
BERLIN – The prevalence of attention-deficit/hyperactivity disorder among nonpsychotic adults in outpatient settings is markedly higher than in the general adult population, according to a major eight-nation observational study.
“I think this is a wake-up call for clinicians to include adult ADHD in their differential diagnostic considerations in a broad range of psychiatric patients,” Dr. Johannes Thome said in presenting the ADPSYC study results at the annual congress of the European College of Neuropsychopharmacology.
The study included 2,284 unselected participants in eight European countries. Nonpsychotic patients in outpatient care for any psychiatric disorder were eligible. A variety of outpatient settings were deliberately included: private psychiatric practices, community mental health centers, outpatient psychiatric clinics associated with medical centers, and outpatient clinics linked with psychiatric hospitals.
Participants were asked whether they’d ever been diagnosed with ADHD and also were screened using the Adult ADHD Self-Report Scale. If ADHD was suspected on either basis, they were further assessed using the Diagnostic Interview for ADHD in Adults, upon which the diagnosis hinged.
A total of 15.8% of the psychiatric outpatients were diagnosed with adult ADHD based on the criteria of the DSM-IV, 4th edition, as were 17.4% using DSM-5 criteria. In contrast, the consensus estimate of the prevalence of ADHD in the general adult population is 2.5%.
By DSM-IV criteria, 4.7% of the total ADPSYC population had the inattentive subtype of ADHD, 1.1% had the hyperactive/impulsive subtype, and 10% had the combined form, reported Dr. Thome, professor and chair of the department of psychiatry at the University of Rostock in Germany.
As is seen in the general population, the prevalence of ADHD in psychiatric outpatients was lower in women: 14.4%, compared with 21.6% among men. Illustrating the dictum that ADHD runs in families, 14.9% of patients with ADHD had a first-degree relative who’d been diagnosed with the disorder, as did just 3.7% of psychiatric outpatients without ADHD.
Twenty percent of patients with ADHD met criteria for substance abuse or dependence, compared with 12.6% of non-ADHD patients.
Quality of life and disability burden were assessed in all ADPSYC participants via the Clinical Global Impressions-Severity scale, (CGI-S); the Sheehan Disability Scale; and the EuroQol-5 Dimension questionnaire. These metrics showed that adult psychiatric outpatients with ADHD had significantly worse quality of life and more overall disability than outpatients without ADHD. For example, the mean CGI-S score in outpatients with ADHD was 3.8, compared with 3.3 in outpatients without ADHD. Sixty-four percent of outpatients with ADHD had scores placing them in the moderately, markedly, or severely ill range, compared with 47% of psychiatric patients without ADHD.
Moreover, the mean total score on the Sheehan Disability Scale averaged 18.9 in outpatients with ADHD, compared with 11.6 in psychiatric patients without ADHD. Those with ADHD scored markedly worse in multiple domains, including social life, family life, work/school, and underproductive days in the past week.
On the EuroQol-5 Dimension questionnaire, 25% of patients with ADHD reported being extremely anxious or depressed, compared with 16% without ADHD, Dr. Thome continued.
He emphasized that these quality of life impairment and disability scores highlight a key point about adult ADHD, one that applies to affected patients regardless of whether or not they have a comorbid psychiatric disorder: The impact of adult ADHD extends well beyond the core symptoms.
While ADHD by definition in the DSM-5 must start before age 12, “You have to expect that the older an affected patient gets, the more social problems will occur and the more comorbidity you’ll see,” he observed.
“If you are a clinician, you will probably never, ever find a patient who comes to you and says, ‘Doctor, I’m suffering from inattention, and I’m so impulsive, and my mood regulation doesn’t work well.’ Rather, they’ll come to you and say, ‘I have a problem at my workplace; I’m always having arguments with my boss and with my wife,’ ” according to the psychiatrist. “From the patient’s perspective, usually it’s much more important how their quality of life changes with treatment, rather than how much certain ADHD scales change.”
Along those lines, it’s important to note that numerous studies have demonstrated that individuals with adult ADHD have three times more emergency department visits, a 10-fold greater rate of outpatient medical visits, and three times more inpatient hospitalizations than the general adult population. They also have an increased risk of serious motor vehicle accidents, which appears to be reduced with the use of ADHD medications (JAMA Psychiatry 2014;71:319-25). A study by Dr. Thome and his colleagues showed that adult ADHD is also accompanied by significant alterations in circadian rhythms at the endocrine, genetic, and behavioral levels (Mol. Psychiatry 2012;17:988-95), which may in part explain the patients’ propensity for mishaps.
Moreover, a major Swedish national registry study involving more than 25,000 patients with adult ADHD established that the disorder is associated with increased rates of criminality, and that during periods when patients were on ADHD medications, their risk of arrests and convictions was significantly reduced (N. Engl. J. Med. 2012;367:2006-14). But while this study drew extensive media attention, heralding a “treatment for criminality,” Dr. Thome cautioned that association in an observational study does not prove causality.
“Some people argue that because they can’t focus and are so impatient, people with adult ADHD are simply worse at hiding the crime and are much more easily caught by the police, and that during periods when they’re on medication they are more likely to be seeing a social worker or have other social support. That might be a partial explanation,” Dr. Thome said. “But my main point here is I want you to understand that you don’t need to be afraid of adult ADHD patients. They’re not more dangerous than others.”
With regard to treatment, he emphasized that a comprehensive plan for adult ADHD needs to address psychological, behavioral, and educational or occupational needs with a range of interventions.
“I want to make the point that psychologic therapy is at least as important as medication,” Dr. Thome said. “Pills don’t give you skills.”
The ADPSYC study was funded by Eli Lilly. Dr. Thome reported having received research grants and/or serving on advisory boards for Lilly and more than a dozen other companies.
BERLIN – The prevalence of attention-deficit/hyperactivity disorder among nonpsychotic adults in outpatient settings is markedly higher than in the general adult population, according to a major eight-nation observational study.
“I think this is a wake-up call for clinicians to include adult ADHD in their differential diagnostic considerations in a broad range of psychiatric patients,” Dr. Johannes Thome said in presenting the ADPSYC study results at the annual congress of the European College of Neuropsychopharmacology.
The study included 2,284 unselected participants in eight European countries. Nonpsychotic patients in outpatient care for any psychiatric disorder were eligible. A variety of outpatient settings were deliberately included: private psychiatric practices, community mental health centers, outpatient psychiatric clinics associated with medical centers, and outpatient clinics linked with psychiatric hospitals.
Participants were asked whether they’d ever been diagnosed with ADHD and also were screened using the Adult ADHD Self-Report Scale. If ADHD was suspected on either basis, they were further assessed using the Diagnostic Interview for ADHD in Adults, upon which the diagnosis hinged.
A total of 15.8% of the psychiatric outpatients were diagnosed with adult ADHD based on the criteria of the DSM-IV, 4th edition, as were 17.4% using DSM-5 criteria. In contrast, the consensus estimate of the prevalence of ADHD in the general adult population is 2.5%.
By DSM-IV criteria, 4.7% of the total ADPSYC population had the inattentive subtype of ADHD, 1.1% had the hyperactive/impulsive subtype, and 10% had the combined form, reported Dr. Thome, professor and chair of the department of psychiatry at the University of Rostock in Germany.
As is seen in the general population, the prevalence of ADHD in psychiatric outpatients was lower in women: 14.4%, compared with 21.6% among men. Illustrating the dictum that ADHD runs in families, 14.9% of patients with ADHD had a first-degree relative who’d been diagnosed with the disorder, as did just 3.7% of psychiatric outpatients without ADHD.
Twenty percent of patients with ADHD met criteria for substance abuse or dependence, compared with 12.6% of non-ADHD patients.
Quality of life and disability burden were assessed in all ADPSYC participants via the Clinical Global Impressions-Severity scale, (CGI-S); the Sheehan Disability Scale; and the EuroQol-5 Dimension questionnaire. These metrics showed that adult psychiatric outpatients with ADHD had significantly worse quality of life and more overall disability than outpatients without ADHD. For example, the mean CGI-S score in outpatients with ADHD was 3.8, compared with 3.3 in outpatients without ADHD. Sixty-four percent of outpatients with ADHD had scores placing them in the moderately, markedly, or severely ill range, compared with 47% of psychiatric patients without ADHD.
Moreover, the mean total score on the Sheehan Disability Scale averaged 18.9 in outpatients with ADHD, compared with 11.6 in psychiatric patients without ADHD. Those with ADHD scored markedly worse in multiple domains, including social life, family life, work/school, and underproductive days in the past week.
On the EuroQol-5 Dimension questionnaire, 25% of patients with ADHD reported being extremely anxious or depressed, compared with 16% without ADHD, Dr. Thome continued.
He emphasized that these quality of life impairment and disability scores highlight a key point about adult ADHD, one that applies to affected patients regardless of whether or not they have a comorbid psychiatric disorder: The impact of adult ADHD extends well beyond the core symptoms.
While ADHD by definition in the DSM-5 must start before age 12, “You have to expect that the older an affected patient gets, the more social problems will occur and the more comorbidity you’ll see,” he observed.
“If you are a clinician, you will probably never, ever find a patient who comes to you and says, ‘Doctor, I’m suffering from inattention, and I’m so impulsive, and my mood regulation doesn’t work well.’ Rather, they’ll come to you and say, ‘I have a problem at my workplace; I’m always having arguments with my boss and with my wife,’ ” according to the psychiatrist. “From the patient’s perspective, usually it’s much more important how their quality of life changes with treatment, rather than how much certain ADHD scales change.”
Along those lines, it’s important to note that numerous studies have demonstrated that individuals with adult ADHD have three times more emergency department visits, a 10-fold greater rate of outpatient medical visits, and three times more inpatient hospitalizations than the general adult population. They also have an increased risk of serious motor vehicle accidents, which appears to be reduced with the use of ADHD medications (JAMA Psychiatry 2014;71:319-25). A study by Dr. Thome and his colleagues showed that adult ADHD is also accompanied by significant alterations in circadian rhythms at the endocrine, genetic, and behavioral levels (Mol. Psychiatry 2012;17:988-95), which may in part explain the patients’ propensity for mishaps.
Moreover, a major Swedish national registry study involving more than 25,000 patients with adult ADHD established that the disorder is associated with increased rates of criminality, and that during periods when patients were on ADHD medications, their risk of arrests and convictions was significantly reduced (N. Engl. J. Med. 2012;367:2006-14). But while this study drew extensive media attention, heralding a “treatment for criminality,” Dr. Thome cautioned that association in an observational study does not prove causality.
“Some people argue that because they can’t focus and are so impatient, people with adult ADHD are simply worse at hiding the crime and are much more easily caught by the police, and that during periods when they’re on medication they are more likely to be seeing a social worker or have other social support. That might be a partial explanation,” Dr. Thome said. “But my main point here is I want you to understand that you don’t need to be afraid of adult ADHD patients. They’re not more dangerous than others.”
With regard to treatment, he emphasized that a comprehensive plan for adult ADHD needs to address psychological, behavioral, and educational or occupational needs with a range of interventions.
“I want to make the point that psychologic therapy is at least as important as medication,” Dr. Thome said. “Pills don’t give you skills.”
The ADPSYC study was funded by Eli Lilly. Dr. Thome reported having received research grants and/or serving on advisory boards for Lilly and more than a dozen other companies.
AT THE ECNP CONGRESS
Key clinical point: Adult ADHD should be included in differential diagnosic considerations “in a broad range of psychiatric patients.”
Major finding: By DSM-IV criteria, 15.8% of an unselected population of adult nonpsychotic psychiatric outpatients were found to have ADHD.
Data source: The ADPSYC study included 2,284 nonpsychotic adult psychiatric outpatients in a variety of treatment settings in eight European countries.
Disclosures: The study was funded by Eli Lilly. The presenter reported having received research grants from and/or serving on advisory boards for Lilly and more than a dozen other companies.
Internet addiction surprisingly rare among former opiate addicts
BERLIN – Internet addiction and drug addiction do not, as it turns out, go together like ham and eggs. It’s more like oil and water.
Indeed, Internet addiction proved rare among former opiate addicts in methadone maintenance treatment clinics, both in Las Vegas and Tel Aviv, Einat Peles, Ph.D., reported at the annual congress of the European College of Neuropsychopharmacology.

This finding was unexpected, because it’s known that drug addicts are predisposed to other addictive behaviors. For example, in a previous study, Dr. Peles and her coinvestigators documented a strong association between participation in methadone maintenance treatment and pathological gambling (Am. J. Orthopsychiatry 2010;80:311-6).
In the new Internet addiction study, she reported on 177 unselected patients from a Las Vegas methadone maintenance clinic and 71 others from a similar clinic in Tel Aviv. All were assessed using the Internet Addiction Test questionnaire. They also were evaluated for depression using the Center for Epidemiologic Studies Depression Scale (CES-D), since Internet addiction has been shown in a meta-analysis to be related to depression (Psychopathology 2013;46:1-13), noted Dr. Peles of the Tel Aviv Sourasky Medical Center.
None of the 248 study participants met the criteria for Internet addiction as defined by an Internet Addiction Test score of 80 or higher. Six patients – three from each clinic – were defined on the basis of a score of 50-79 on the 20-item questionnaire as having an occasional or frequent problems attributable to Internet use. And 23% of the Las Vegas cohort and 48% from Tel Aviv weren’t exposed to the Internet at all.
The unexpected rarity of Internet addiction among former opiate addicts in methadone treatment was consistent across the two clinics, even though the patient populations in the two cities were quite dissimilar. The Las Vegas patients were 36-fold more likely to be cannabis abusers and five times more likely to be women. They also were older, better educated, and more likely to be depressed than the Tel Aviv group.
After considerable debate, Internet addiction was not included as a recognized disorder in DSM-5.
The study was conducted free of commercial support. Dr. Peles reported having no financial conflicts regarding her study.
BERLIN – Internet addiction and drug addiction do not, as it turns out, go together like ham and eggs. It’s more like oil and water.
Indeed, Internet addiction proved rare among former opiate addicts in methadone maintenance treatment clinics, both in Las Vegas and Tel Aviv, Einat Peles, Ph.D., reported at the annual congress of the European College of Neuropsychopharmacology.
This finding was unexpected, because it’s known that drug addicts are predisposed to other addictive behaviors. For example, in a previous study, Dr. Peles and her coinvestigators documented a strong association between participation in methadone maintenance treatment and pathological gambling (Am. J. Orthopsychiatry 2010;80:311-6).
In the new Internet addiction study, she reported on 177 unselected patients from a Las Vegas methadone maintenance clinic and 71 others from a similar clinic in Tel Aviv. All were assessed using the Internet Addiction Test questionnaire. They also were evaluated for depression using the Center for Epidemiologic Studies Depression Scale (CES-D), since Internet addiction has been shown in a meta-analysis to be related to depression (Psychopathology 2013;46:1-13), noted Dr. Peles of the Tel Aviv Sourasky Medical Center.
None of the 248 study participants met the criteria for Internet addiction as defined by an Internet Addiction Test score of 80 or higher. Six patients – three from each clinic – were defined on the basis of a score of 50-79 on the 20-item questionnaire as having an occasional or frequent problems attributable to Internet use. And 23% of the Las Vegas cohort and 48% from Tel Aviv weren’t exposed to the Internet at all.
The unexpected rarity of Internet addiction among former opiate addicts in methadone treatment was consistent across the two clinics, even though the patient populations in the two cities were quite dissimilar. The Las Vegas patients were 36-fold more likely to be cannabis abusers and five times more likely to be women. They also were older, better educated, and more likely to be depressed than the Tel Aviv group.
After considerable debate, Internet addiction was not included as a recognized disorder in DSM-5.
The study was conducted free of commercial support. Dr. Peles reported having no financial conflicts regarding her study.
BERLIN – Internet addiction and drug addiction do not, as it turns out, go together like ham and eggs. It’s more like oil and water.
Indeed, Internet addiction proved rare among former opiate addicts in methadone maintenance treatment clinics, both in Las Vegas and Tel Aviv, Einat Peles, Ph.D., reported at the annual congress of the European College of Neuropsychopharmacology.
This finding was unexpected, because it’s known that drug addicts are predisposed to other addictive behaviors. For example, in a previous study, Dr. Peles and her coinvestigators documented a strong association between participation in methadone maintenance treatment and pathological gambling (Am. J. Orthopsychiatry 2010;80:311-6).
In the new Internet addiction study, she reported on 177 unselected patients from a Las Vegas methadone maintenance clinic and 71 others from a similar clinic in Tel Aviv. All were assessed using the Internet Addiction Test questionnaire. They also were evaluated for depression using the Center for Epidemiologic Studies Depression Scale (CES-D), since Internet addiction has been shown in a meta-analysis to be related to depression (Psychopathology 2013;46:1-13), noted Dr. Peles of the Tel Aviv Sourasky Medical Center.
None of the 248 study participants met the criteria for Internet addiction as defined by an Internet Addiction Test score of 80 or higher. Six patients – three from each clinic – were defined on the basis of a score of 50-79 on the 20-item questionnaire as having an occasional or frequent problems attributable to Internet use. And 23% of the Las Vegas cohort and 48% from Tel Aviv weren’t exposed to the Internet at all.
The unexpected rarity of Internet addiction among former opiate addicts in methadone treatment was consistent across the two clinics, even though the patient populations in the two cities were quite dissimilar. The Las Vegas patients were 36-fold more likely to be cannabis abusers and five times more likely to be women. They also were older, better educated, and more likely to be depressed than the Tel Aviv group.
After considerable debate, Internet addiction was not included as a recognized disorder in DSM-5.
The study was conducted free of commercial support. Dr. Peles reported having no financial conflicts regarding her study.
AT THE ECNP CONGRESS
Key clinical point: Patients in methadone maintenance therapy for opiate addiction are not predisposed to Internet addiction.
Major finding: Not one patient among an unselected group of 248 in methadone maintenance treatment clinics in Las Vegas and Tel Aviv met criteria for Internet addiction.
Data source: In this cross-sectional study, patients in methadone maintenance treatment clinics were evaluated using the Internet Addiction Test. None met criteria for Internet addiction.
Disclosures: The study was conducted free of commercial support. Dr. Peles reported having no financial conflicts regarding her study.

Major overhaul of psychotropic drug terminology launched
BERLIN – Official representatives of the world’s major neuropsychopharmacology organizations have grabbed their shovels in order to bury the time-honored and familiar terminology for the psychotropic medication categories, including “antipsychotics,” “anxiolytics,” “antidepressants,” and “hypnotics.”
These descriptors have long outlived their usefulness and are headed for the scrap heap, according to members of an international task force that unveiled a new neuroscience-based drug terminology at the annual congress of the European College of Neuropsychopharmacology.

“Our psychiatric medication nomenclature is hopelessly outdated. It is 50 years old. We are stuck in the 1960s,” explained Dr. Joseph Zohar, chair of the Joint Task Force on Nomenclature.
The old nomenclature neither reflects current scientific knowledge nor provides clinicians with pharmacologic information useful in making informed treatment decisions. And it certainly doesn’t help patients understand their physician’s rationale in choosing a particular medication.
“We talk about antidepressants, but many times, we give them for anxiety. We talk about antipsychotics, but often prescribe them for depression or anxiety. So the situation we face on almost a daily basis is the anxious patient asking us, ‘Why are you giving me an antidepressant for my anxiety?’ And which is even worse: the depressed patient asking, ‘Is my condition so bad that you’re giving me an antipsychotic?’ This has negative implications for compliance,” observed Dr. Zohar, director of the Anxiety and Obsessive Compulsive Clinic at Sheba Medical Center in Tel Hashomer, Israel.
Likewise, the widely used term “second-generation antipsychotic” is problematic. It encompasses compounds with fundamentally different pharmacologies, and clinicians unaware of that can unwittingly use these agents inappropriately.

“The term ‘second-generation antipsychotic’ is a marketing term. It’s not science,” he asserted.
The task force has created a new nomenclature along the lines of what’s used for antihypertensive medications, where a drug’s class – be it angiotensin-converting enzyme inhibitor, calcium channel blocker, diuretic, or beta-blocker – describes its mechanism of action. That way, when it becomes necessary to add a second or third antihypertensive agent in order to adequately control a patient’s blood pressure, a physician can pick agents having different mechanisms of action to maximize effectiveness and minimize side effects. That’s how it should work in biologic psychiatry, too, Dr. Zohar continued.
The new neuroscience-based nomenclature template has four components. Axis 1 describes the drug’s pharmacologic target and mode of action; to date, there are 11 possible pharmacologic targets and 10 modes of action. Axis 2 describes the drug’s approved indications. Axis 3 summarizes the panel’s collective opinion on the drug’s efficacy, which may extend beyond the approved indications, as for example, with the tricyclic antidepressants, as well as the drug’s major side effects. And Axis 4, which will mainly be of interest to neuroscientists rather than clinicians and patients, details the drug’s neurobiology. Take, for example, flurazepam (Dalmane). It’s often called an anxiolytic. That’s going to change, said task force member Dr. David J. Nutt, professor and head of the center for neuropsychopharmacology at Hammersmith Hospital, London.

“We wouldn’t any longer say ‘flurazepam is an anxiolytic.’ What we’d say is ‘flurazepam is one treatment for anxiety, and it works through being a positive allosteric modulator at the GABA-A receptor,’ ” he explained.
The task force comprises representatives from the ECNP, the American College of Neuropsychopharmacology (ACNP), the Asian College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, and the International Union of Basic and Clinical Pharmacology.
The launch of the new nomenclature at the ACNP meeting was accompanied by release of the NbNomenclature app, which details the new terminology for 108 psychotropic drugs and is downloadable free at the App Store and Google Play. A paperback book covering the same material is also available.

Brandishing the book, Dr. Zohar declared, “We want this to be the DSM-5 of psychopharmacology.” That drew a wince from Dr. David J. Kupfer, the ACNP representative on the task force. As chair of the American Psychiatric Association’s task force for DSM-5, he had requested feedback as that controversial update took shape and wound up getting 14,000 responses, many quite critical. He’s not expecting anything of the sort in response to the proposed neuroscience-based drug nomenclature.
“It’s very clear that clinicians want this,” the psychiatrist said. “I think the scientific response will be very positive.”
The task force does, however, want the new nomenclature to be user friendly. Feedback is welcomed. The panel plans to meet at least once every 6 months to review outside comments and make thoughtful changes to the app, he added.
“Five years ago, when we started out, the idea of bringing international organizations together to work on a project like this seemed like Mission Impossible,” recalled Dr. Kupfer, professor of psychiatry at the University of Pittsburgh. “But now we’ve got a book and an app. We’ve accomplished phase 1 and have begun phase 2 of the implementation strategy.”
This next phase involves task force members holding meetings with editors of the major North American and European psychiatry and neuroscience journals in order to get their buy-in.
“We’re asking them to write an editorial commentary about the need for this new nomenclature. And we’ll ask them to develop a fairly uniform instruction for authors. Our target date is that by May 15, 2015 – while the APA is meeting in Toronto – the nomenclature will be adopted in manuscripts submitted to the journals, although maybe for a while the currently used terms will be in parentheses,” he said.
In the spring, the task force plans to reach out to the major psychiatric organizations with educational efforts. Also next spring, discussions will be held with the Food and Drug Administration, World Health Organization, and other regulatory bodies.
Further down the line, with a 3- to 5-year time horizon, the panel and its supporting organizations hope to get the new nomenclature introduced in textbooks and in the educational protocols used for medical students and psychiatry residents. They’ll also be meeting with the editors of the major nonpsychiatric medical journals as well as reaching out to leaders in primary care medicine.
“This is going to be an ongoing process,” Dr. Kupfer said. We’ll be educating a variety of different stakeholders, and that’s going to take time.”
Panelists said the new nomenclature won’t be used to rank medications or create clinical guidelines. However, the app can display all of the medications having a given efficacy and/or pharmacologic target.
Dr. Nutt said feedback from the pharmaceutical industry has been positive so far.
“We now meet with companies having compounds in phase 2 or 3 testing to discuss what their drug should be called. We think this is going to cut through a lot of the silliness and stupidity we’ve had over the last few decades,” he explained.
For example, companies developing new medications that target a specific aspect of schizophrenia, be it positive symptoms, negative symptoms, or cognitive symptoms, are well aware that under the traditional regulatory standards, their new agent would be classified as an antipsychotic. That means their drug would automatically get a black box warning label, even if its pharmacology is completely different from schizophrenia drugs that have been associated with serious side effects. The companies want to avoid that black box when it’s not warranted, and they’re starting to recognize that the new neuroscience-based nomenclature can be helpful in this regard, according to Dr. Nutt.

Dr. Eduard Vieta, chair of the ECNP communication committee, noted that pushing for the new nomenclature program represents a major commitment by the organization. The new terminology will ultimately change the way clinicians and their patients think about the drugs they use.
“There is a lot of important science being presented at this conference, but this nomenclature project is clearly the biggest news at the meeting,” observed Dr. Vieta, professor of psychiatry at the University of Barcelona.
The presenters reported having no financial relationships relevant to the nomenclature project.
BERLIN – Official representatives of the world’s major neuropsychopharmacology organizations have grabbed their shovels in order to bury the time-honored and familiar terminology for the psychotropic medication categories, including “antipsychotics,” “anxiolytics,” “antidepressants,” and “hypnotics.”
These descriptors have long outlived their usefulness and are headed for the scrap heap, according to members of an international task force that unveiled a new neuroscience-based drug terminology at the annual congress of the European College of Neuropsychopharmacology.
“Our psychiatric medication nomenclature is hopelessly outdated. It is 50 years old. We are stuck in the 1960s,” explained Dr. Joseph Zohar, chair of the Joint Task Force on Nomenclature.
The old nomenclature neither reflects current scientific knowledge nor provides clinicians with pharmacologic information useful in making informed treatment decisions. And it certainly doesn’t help patients understand their physician’s rationale in choosing a particular medication.
“We talk about antidepressants, but many times, we give them for anxiety. We talk about antipsychotics, but often prescribe them for depression or anxiety. So the situation we face on almost a daily basis is the anxious patient asking us, ‘Why are you giving me an antidepressant for my anxiety?’ And which is even worse: the depressed patient asking, ‘Is my condition so bad that you’re giving me an antipsychotic?’ This has negative implications for compliance,” observed Dr. Zohar, director of the Anxiety and Obsessive Compulsive Clinic at Sheba Medical Center in Tel Hashomer, Israel.
Likewise, the widely used term “second-generation antipsychotic” is problematic. It encompasses compounds with fundamentally different pharmacologies, and clinicians unaware of that can unwittingly use these agents inappropriately.
“The term ‘second-generation antipsychotic’ is a marketing term. It’s not science,” he asserted.
The task force has created a new nomenclature along the lines of what’s used for antihypertensive medications, where a drug’s class – be it angiotensin-converting enzyme inhibitor, calcium channel blocker, diuretic, or beta-blocker – describes its mechanism of action. That way, when it becomes necessary to add a second or third antihypertensive agent in order to adequately control a patient’s blood pressure, a physician can pick agents having different mechanisms of action to maximize effectiveness and minimize side effects. That’s how it should work in biologic psychiatry, too, Dr. Zohar continued.
The new neuroscience-based nomenclature template has four components. Axis 1 describes the drug’s pharmacologic target and mode of action; to date, there are 11 possible pharmacologic targets and 10 modes of action. Axis 2 describes the drug’s approved indications. Axis 3 summarizes the panel’s collective opinion on the drug’s efficacy, which may extend beyond the approved indications, as for example, with the tricyclic antidepressants, as well as the drug’s major side effects. And Axis 4, which will mainly be of interest to neuroscientists rather than clinicians and patients, details the drug’s neurobiology. Take, for example, flurazepam (Dalmane). It’s often called an anxiolytic. That’s going to change, said task force member Dr. David J. Nutt, professor and head of the center for neuropsychopharmacology at Hammersmith Hospital, London.
“We wouldn’t any longer say ‘flurazepam is an anxiolytic.’ What we’d say is ‘flurazepam is one treatment for anxiety, and it works through being a positive allosteric modulator at the GABA-A receptor,’ ” he explained.
The task force comprises representatives from the ECNP, the American College of Neuropsychopharmacology (ACNP), the Asian College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, and the International Union of Basic and Clinical Pharmacology.
The launch of the new nomenclature at the ACNP meeting was accompanied by release of the NbNomenclature app, which details the new terminology for 108 psychotropic drugs and is downloadable free at the App Store and Google Play. A paperback book covering the same material is also available.
Brandishing the book, Dr. Zohar declared, “We want this to be the DSM-5 of psychopharmacology.” That drew a wince from Dr. David J. Kupfer, the ACNP representative on the task force. As chair of the American Psychiatric Association’s task force for DSM-5, he had requested feedback as that controversial update took shape and wound up getting 14,000 responses, many quite critical. He’s not expecting anything of the sort in response to the proposed neuroscience-based drug nomenclature.
“It’s very clear that clinicians want this,” the psychiatrist said. “I think the scientific response will be very positive.”
The task force does, however, want the new nomenclature to be user friendly. Feedback is welcomed. The panel plans to meet at least once every 6 months to review outside comments and make thoughtful changes to the app, he added.
“Five years ago, when we started out, the idea of bringing international organizations together to work on a project like this seemed like Mission Impossible,” recalled Dr. Kupfer, professor of psychiatry at the University of Pittsburgh. “But now we’ve got a book and an app. We’ve accomplished phase 1 and have begun phase 2 of the implementation strategy.”
This next phase involves task force members holding meetings with editors of the major North American and European psychiatry and neuroscience journals in order to get their buy-in.
“We’re asking them to write an editorial commentary about the need for this new nomenclature. And we’ll ask them to develop a fairly uniform instruction for authors. Our target date is that by May 15, 2015 – while the APA is meeting in Toronto – the nomenclature will be adopted in manuscripts submitted to the journals, although maybe for a while the currently used terms will be in parentheses,” he said.
In the spring, the task force plans to reach out to the major psychiatric organizations with educational efforts. Also next spring, discussions will be held with the Food and Drug Administration, World Health Organization, and other regulatory bodies.
Further down the line, with a 3- to 5-year time horizon, the panel and its supporting organizations hope to get the new nomenclature introduced in textbooks and in the educational protocols used for medical students and psychiatry residents. They’ll also be meeting with the editors of the major nonpsychiatric medical journals as well as reaching out to leaders in primary care medicine.
“This is going to be an ongoing process,” Dr. Kupfer said. We’ll be educating a variety of different stakeholders, and that’s going to take time.”
Panelists said the new nomenclature won’t be used to rank medications or create clinical guidelines. However, the app can display all of the medications having a given efficacy and/or pharmacologic target.
Dr. Nutt said feedback from the pharmaceutical industry has been positive so far.
“We now meet with companies having compounds in phase 2 or 3 testing to discuss what their drug should be called. We think this is going to cut through a lot of the silliness and stupidity we’ve had over the last few decades,” he explained.
For example, companies developing new medications that target a specific aspect of schizophrenia, be it positive symptoms, negative symptoms, or cognitive symptoms, are well aware that under the traditional regulatory standards, their new agent would be classified as an antipsychotic. That means their drug would automatically get a black box warning label, even if its pharmacology is completely different from schizophrenia drugs that have been associated with serious side effects. The companies want to avoid that black box when it’s not warranted, and they’re starting to recognize that the new neuroscience-based nomenclature can be helpful in this regard, according to Dr. Nutt.
Dr. Eduard Vieta, chair of the ECNP communication committee, noted that pushing for the new nomenclature program represents a major commitment by the organization. The new terminology will ultimately change the way clinicians and their patients think about the drugs they use.
“There is a lot of important science being presented at this conference, but this nomenclature project is clearly the biggest news at the meeting,” observed Dr. Vieta, professor of psychiatry at the University of Barcelona.
The presenters reported having no financial relationships relevant to the nomenclature project.
BERLIN – Official representatives of the world’s major neuropsychopharmacology organizations have grabbed their shovels in order to bury the time-honored and familiar terminology for the psychotropic medication categories, including “antipsychotics,” “anxiolytics,” “antidepressants,” and “hypnotics.”
These descriptors have long outlived their usefulness and are headed for the scrap heap, according to members of an international task force that unveiled a new neuroscience-based drug terminology at the annual congress of the European College of Neuropsychopharmacology.
“Our psychiatric medication nomenclature is hopelessly outdated. It is 50 years old. We are stuck in the 1960s,” explained Dr. Joseph Zohar, chair of the Joint Task Force on Nomenclature.
The old nomenclature neither reflects current scientific knowledge nor provides clinicians with pharmacologic information useful in making informed treatment decisions. And it certainly doesn’t help patients understand their physician’s rationale in choosing a particular medication.
“We talk about antidepressants, but many times, we give them for anxiety. We talk about antipsychotics, but often prescribe them for depression or anxiety. So the situation we face on almost a daily basis is the anxious patient asking us, ‘Why are you giving me an antidepressant for my anxiety?’ And which is even worse: the depressed patient asking, ‘Is my condition so bad that you’re giving me an antipsychotic?’ This has negative implications for compliance,” observed Dr. Zohar, director of the Anxiety and Obsessive Compulsive Clinic at Sheba Medical Center in Tel Hashomer, Israel.
Likewise, the widely used term “second-generation antipsychotic” is problematic. It encompasses compounds with fundamentally different pharmacologies, and clinicians unaware of that can unwittingly use these agents inappropriately.
“The term ‘second-generation antipsychotic’ is a marketing term. It’s not science,” he asserted.
The task force has created a new nomenclature along the lines of what’s used for antihypertensive medications, where a drug’s class – be it angiotensin-converting enzyme inhibitor, calcium channel blocker, diuretic, or beta-blocker – describes its mechanism of action. That way, when it becomes necessary to add a second or third antihypertensive agent in order to adequately control a patient’s blood pressure, a physician can pick agents having different mechanisms of action to maximize effectiveness and minimize side effects. That’s how it should work in biologic psychiatry, too, Dr. Zohar continued.
The new neuroscience-based nomenclature template has four components. Axis 1 describes the drug’s pharmacologic target and mode of action; to date, there are 11 possible pharmacologic targets and 10 modes of action. Axis 2 describes the drug’s approved indications. Axis 3 summarizes the panel’s collective opinion on the drug’s efficacy, which may extend beyond the approved indications, as for example, with the tricyclic antidepressants, as well as the drug’s major side effects. And Axis 4, which will mainly be of interest to neuroscientists rather than clinicians and patients, details the drug’s neurobiology. Take, for example, flurazepam (Dalmane). It’s often called an anxiolytic. That’s going to change, said task force member Dr. David J. Nutt, professor and head of the center for neuropsychopharmacology at Hammersmith Hospital, London.
“We wouldn’t any longer say ‘flurazepam is an anxiolytic.’ What we’d say is ‘flurazepam is one treatment for anxiety, and it works through being a positive allosteric modulator at the GABA-A receptor,’ ” he explained.
The task force comprises representatives from the ECNP, the American College of Neuropsychopharmacology (ACNP), the Asian College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, and the International Union of Basic and Clinical Pharmacology.
The launch of the new nomenclature at the ACNP meeting was accompanied by release of the NbNomenclature app, which details the new terminology for 108 psychotropic drugs and is downloadable free at the App Store and Google Play. A paperback book covering the same material is also available.
Brandishing the book, Dr. Zohar declared, “We want this to be the DSM-5 of psychopharmacology.” That drew a wince from Dr. David J. Kupfer, the ACNP representative on the task force. As chair of the American Psychiatric Association’s task force for DSM-5, he had requested feedback as that controversial update took shape and wound up getting 14,000 responses, many quite critical. He’s not expecting anything of the sort in response to the proposed neuroscience-based drug nomenclature.
“It’s very clear that clinicians want this,” the psychiatrist said. “I think the scientific response will be very positive.”
The task force does, however, want the new nomenclature to be user friendly. Feedback is welcomed. The panel plans to meet at least once every 6 months to review outside comments and make thoughtful changes to the app, he added.
“Five years ago, when we started out, the idea of bringing international organizations together to work on a project like this seemed like Mission Impossible,” recalled Dr. Kupfer, professor of psychiatry at the University of Pittsburgh. “But now we’ve got a book and an app. We’ve accomplished phase 1 and have begun phase 2 of the implementation strategy.”
This next phase involves task force members holding meetings with editors of the major North American and European psychiatry and neuroscience journals in order to get their buy-in.
“We’re asking them to write an editorial commentary about the need for this new nomenclature. And we’ll ask them to develop a fairly uniform instruction for authors. Our target date is that by May 15, 2015 – while the APA is meeting in Toronto – the nomenclature will be adopted in manuscripts submitted to the journals, although maybe for a while the currently used terms will be in parentheses,” he said.
In the spring, the task force plans to reach out to the major psychiatric organizations with educational efforts. Also next spring, discussions will be held with the Food and Drug Administration, World Health Organization, and other regulatory bodies.
Further down the line, with a 3- to 5-year time horizon, the panel and its supporting organizations hope to get the new nomenclature introduced in textbooks and in the educational protocols used for medical students and psychiatry residents. They’ll also be meeting with the editors of the major nonpsychiatric medical journals as well as reaching out to leaders in primary care medicine.
“This is going to be an ongoing process,” Dr. Kupfer said. We’ll be educating a variety of different stakeholders, and that’s going to take time.”
Panelists said the new nomenclature won’t be used to rank medications or create clinical guidelines. However, the app can display all of the medications having a given efficacy and/or pharmacologic target.
Dr. Nutt said feedback from the pharmaceutical industry has been positive so far.
“We now meet with companies having compounds in phase 2 or 3 testing to discuss what their drug should be called. We think this is going to cut through a lot of the silliness and stupidity we’ve had over the last few decades,” he explained.
For example, companies developing new medications that target a specific aspect of schizophrenia, be it positive symptoms, negative symptoms, or cognitive symptoms, are well aware that under the traditional regulatory standards, their new agent would be classified as an antipsychotic. That means their drug would automatically get a black box warning label, even if its pharmacology is completely different from schizophrenia drugs that have been associated with serious side effects. The companies want to avoid that black box when it’s not warranted, and they’re starting to recognize that the new neuroscience-based nomenclature can be helpful in this regard, according to Dr. Nutt.
Dr. Eduard Vieta, chair of the ECNP communication committee, noted that pushing for the new nomenclature program represents a major commitment by the organization. The new terminology will ultimately change the way clinicians and their patients think about the drugs they use.
“There is a lot of important science being presented at this conference, but this nomenclature project is clearly the biggest news at the meeting,” observed Dr. Vieta, professor of psychiatry at the University of Barcelona.
The presenters reported having no financial relationships relevant to the nomenclature project.
EXPERT ANALYSIS FROM THE ECNP CONGRESS

Secukinumab showed sustained efficacy in psoriasis
AMSTERDAM – The investigational biologic agent secukinumab continued to show strong efficacy through 52 weeks of treatment in a new secondary analysis of the pivotal phase III ERASURE trial.
For example, 60% of patients treated for moderate-to-severe chronic plaque psoriasis at the 300-mg dose of secukinumab continued to maintain a PASI 90 response through 52 weeks of therapy, Dr. Mark G. Lebwohl reported at the annual congress of the European Academy of Dermatology and Venereology.
Secukinumab is a fully human monoclonal antibody directed against interleukin-17A. While the Food and Drug Administration requested that the primary outcome in ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) should be the degree of skin clearing at week 12, the efficacy actually peaked at 16 weeks and was then sustained with only modest tailoff through the remainder of the 52-week study (see graphic).
This is important new information, Dr. Lebwohl noted, because 12-week outcomes don’t provide a full picture regarding potent therapies. Psoriasis is a chronic disease requiring long-term therapy, and some biologic agents now marketed for psoriasis tend to show a loss of effect over time. Reassuringly, the long-term ERASURE data show that’s not the case for secukinumab, explained Dr. Lebwohl, professor and chairman of the department of dermatology at Mt. Sinai Medical Center in New York.
ERASURE involved 738 patients randomized double-blind to secukinumab at either 150 mg or 300 mg, or to placebo. Following an initial loading-dose phase when the biologic was given subcutaneously once weekly for 5 weeks, it was then administered every 4 weeks for the remainder of the year-long trial.
The safety profile of secukinumab was similar to placebo with one exception: Upper respiratory tract infections were three- to fourfold more common in patients on the IL-17A inhibitor.
Novartis funded the ERASURE trial, whose primary results were recently published (N. Engl. J. Med. 2014;371:326-38). Dr. Lebwohl reported serving as a consultant to Novartis and more than a dozen other pharmaceutical companies.
AMSTERDAM – The investigational biologic agent secukinumab continued to show strong efficacy through 52 weeks of treatment in a new secondary analysis of the pivotal phase III ERASURE trial.
For example, 60% of patients treated for moderate-to-severe chronic plaque psoriasis at the 300-mg dose of secukinumab continued to maintain a PASI 90 response through 52 weeks of therapy, Dr. Mark G. Lebwohl reported at the annual congress of the European Academy of Dermatology and Venereology.
Secukinumab is a fully human monoclonal antibody directed against interleukin-17A. While the Food and Drug Administration requested that the primary outcome in ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) should be the degree of skin clearing at week 12, the efficacy actually peaked at 16 weeks and was then sustained with only modest tailoff through the remainder of the 52-week study (see graphic).
This is important new information, Dr. Lebwohl noted, because 12-week outcomes don’t provide a full picture regarding potent therapies. Psoriasis is a chronic disease requiring long-term therapy, and some biologic agents now marketed for psoriasis tend to show a loss of effect over time. Reassuringly, the long-term ERASURE data show that’s not the case for secukinumab, explained Dr. Lebwohl, professor and chairman of the department of dermatology at Mt. Sinai Medical Center in New York.
ERASURE involved 738 patients randomized double-blind to secukinumab at either 150 mg or 300 mg, or to placebo. Following an initial loading-dose phase when the biologic was given subcutaneously once weekly for 5 weeks, it was then administered every 4 weeks for the remainder of the year-long trial.
The safety profile of secukinumab was similar to placebo with one exception: Upper respiratory tract infections were three- to fourfold more common in patients on the IL-17A inhibitor.
Novartis funded the ERASURE trial, whose primary results were recently published (N. Engl. J. Med. 2014;371:326-38). Dr. Lebwohl reported serving as a consultant to Novartis and more than a dozen other pharmaceutical companies.
AMSTERDAM – The investigational biologic agent secukinumab continued to show strong efficacy through 52 weeks of treatment in a new secondary analysis of the pivotal phase III ERASURE trial.
For example, 60% of patients treated for moderate-to-severe chronic plaque psoriasis at the 300-mg dose of secukinumab continued to maintain a PASI 90 response through 52 weeks of therapy, Dr. Mark G. Lebwohl reported at the annual congress of the European Academy of Dermatology and Venereology.
Secukinumab is a fully human monoclonal antibody directed against interleukin-17A. While the Food and Drug Administration requested that the primary outcome in ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) should be the degree of skin clearing at week 12, the efficacy actually peaked at 16 weeks and was then sustained with only modest tailoff through the remainder of the 52-week study (see graphic).
This is important new information, Dr. Lebwohl noted, because 12-week outcomes don’t provide a full picture regarding potent therapies. Psoriasis is a chronic disease requiring long-term therapy, and some biologic agents now marketed for psoriasis tend to show a loss of effect over time. Reassuringly, the long-term ERASURE data show that’s not the case for secukinumab, explained Dr. Lebwohl, professor and chairman of the department of dermatology at Mt. Sinai Medical Center in New York.
ERASURE involved 738 patients randomized double-blind to secukinumab at either 150 mg or 300 mg, or to placebo. Following an initial loading-dose phase when the biologic was given subcutaneously once weekly for 5 weeks, it was then administered every 4 weeks for the remainder of the year-long trial.
The safety profile of secukinumab was similar to placebo with one exception: Upper respiratory tract infections were three- to fourfold more common in patients on the IL-17A inhibitor.
Novartis funded the ERASURE trial, whose primary results were recently published (N. Engl. J. Med. 2014;371:326-38). Dr. Lebwohl reported serving as a consultant to Novartis and more than a dozen other pharmaceutical companies.
AT THE EADV CONGRESS
Key clinical point: Psoriasis patients’ initial strong clinical response to the interleukin-17A inhibitor secukinumab is sustained through 52 weeks of therapy.
Major finding: Sixty percent of patients with moderate-to-severe chronic plaque psoriasis had a PASI 90 response sustained through a full year of treatment.
Data source: The 52-week long, double-blind, multicenter ERASURE trial randomized 738 patients with moderate-to-severe chronic plaque psoriasis to secukinumab at 150 mg or 300 mg, or to placebo.
Disclosures: Novartis funded the study. Dr. Lebwohl reported serving as a consultant to the company.