User login
Giving the Smallest GI Transplant Patients a New Lease On Life
The best part about working with kids is that “I get to laugh every day,” said Ke-You (Yoyo) Zhang, MD, clinical assistant professor for pediatrics–gastroenterology and hepatology at Stanford Medicine in California.
Everyday life for them is a challenge.

Dealing with sick children is difficult. “But I think the difference between pediatrics and adults is despite how hard things get, children are the single most resilient people you’re ever going to meet,” she said.
Kids don’t always know they’re sick and they don’t act sick, even when they are. “Every day, I literally get on the floor, I get to play, I get to run around. And truly, I have fun every single day. I get excited to go to work. And I think that’s what makes work not feel like work,” said Dr. Zhang.
In an interview, she discussed the satisfaction of following patients throughout their care continuum and her research to reduce the likelihood of transplant rejection.
She also shared an inspirational story of one young patient who spent his life tied to an IV, and how a transplant exposed him to the normal joys of life, like swimming, going to camp and getting on a plane for the first time.
Q: Why did you choose this subspecialty of pediatric GI?
I think it’s the best subspecialty because I think it combines a lot of the things that I enjoy, which is long-term continuity of care. It’s about growing up with your patients and seeing them through all the various stages of their life, often meeting patients when they’re babies. I get pictures of high school graduations and life milestones and even see some of my patients have families of their own. Becoming a part of their family is very meaningful to me. I also like complexity and acuity, and gastroenterology and hepatology provide those things.
And then lastly, it’s great to be able to exercise procedural skills and constantly learn new procedural skills.
Q: How did you become interested in the field of pediatric intestinal and liver transplantation?
I did all my training here at Stanford. We have one of the largest pediatric transplant centers and we also have a very large intestinal rehabilitation population.
Coming through residency and fellowship, I had a lot of exposure to transplant and intestinal failure, intestinal rehabilitation. I really liked the longitudinal relationship I got to form with my patients. Sometimes they’re in the neonatal ICU, where you’re meeting them in their very first days of life. You follow them through their chronic illness, through transplant and after transplant for many years. You become not just their GI, but the center of their care.
Q: What challenges are unique to this type of transplant work?
Pediatric intestinal failure and intestinal transplant represents an incredibly small subset of children. Oftentimes, they do not get the resources and recognition on a national policy level or even at the hospital level that other gastrointestinal diseases receive. What’s difficult is they are such a small subset but their complexity and their needs are probably in the highest percentile. So that’s a really challenging combination to start with. And there’s only a few centers that specialize in doing intestinal rehabilitation and intestinal transplantation for children in the country.
Developing expertise has been slow. But I think in the last decade or so, our understanding and success with intestinal rehabilitation and intestinal transplantation has really improved, especially at large centers like Stanford. We’ve had a lot of success stories and have not had any graft loss since 2014.
Q: Are these transplants hard to acquire?
Yes, especially when you’re transplanting not just the intestines but the liver as well. You’re waiting for two organs, not just one organ. And on top of that, you’re waiting for an appropriately sized donor; usually a child who’s around the same size or same age who’s passed away. Those organs would have to be a good match. Children can wait multiple years for a transplant.
Q: Is there a success story you’d like to share?
One patient I met in the neonatal ICU had congenital short bowel syndrome. He was born with hardly any intestines. He developed complications of being on long-term intravenous nutrition, which included recurrent central line infections and liver disease. He was never able to eat because he really didn’t have a digestive system that could adequately absorb anything. He had a central line in one of his large veins, so he couldn’t go swimming.
He had to have special adaptive wear to even shower or bathe and couldn’t travel. It’s these types of patients that benefit so much from transplant. Putting any kid through transplant is a massive undertaking and it certainly has risks. But he underwent a successful transplant at the age of 8—not just an intestinal transplant, but a multi-visceral transplant of the liver, intestine, and pancreas. He’s 9 years old now, and no longer needs intravenous nutrition. He ate by mouth for the very first time after transplant. He’s trying all sorts of new foods and he was able to go to a special transplant camp for children. Getting on a plane to Los Angeles, which is where our transplant camp is, was a huge deal.
He was able to swim in the lake. He’s never been able to do that. And he wants to start doing sports this fall. This was really a life-changing story for him.
Q: What advancements lie ahead for this field of work? Have you work on any notable research?
I think our understanding of transplant immunology has really progressed, especially recently. That’s what part of my research is about—using novel therapies to modulate the immune system of pediatric transplant recipients. The No. 1 complication that occurs after intestinal transplant is rejection because obviously you’re implanting somebody else’s organs into a patient.
I am involved in a clinical trial that’s looking at the use of extracellular vesicles that are isolated from hematopoietic stem cells. These vesicles contain various growth factors, anti-inflammatory proteins and tissue repair factors that we are infusing into intestinal transplant patients with the aim to repair the intestinal tissue patients are rejecting.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
My husband and I have an almost 2-year-old little girl. She keeps us busy and I spend my afternoons chasing after a crazy toddler.
Lightning Round
Texting or talking?
Huge texter
Favorite junk food?
French fries
Cat or dog person?
Dog
Favorite ice cream?
Strawberry
If you weren’t a gastroenterologist, what would you be?Florist
Best place you’ve traveled to?
Thailand
Number of cups of coffee you drink per day?
Too many
Favorite city in the US besides the one you live in?
New York City
Favorite sport?
Tennis
Optimist or pessimist?
Optimist
The best part about working with kids is that “I get to laugh every day,” said Ke-You (Yoyo) Zhang, MD, clinical assistant professor for pediatrics–gastroenterology and hepatology at Stanford Medicine in California.
Everyday life for them is a challenge.
Dealing with sick children is difficult. “But I think the difference between pediatrics and adults is despite how hard things get, children are the single most resilient people you’re ever going to meet,” she said.
Kids don’t always know they’re sick and they don’t act sick, even when they are. “Every day, I literally get on the floor, I get to play, I get to run around. And truly, I have fun every single day. I get excited to go to work. And I think that’s what makes work not feel like work,” said Dr. Zhang.
In an interview, she discussed the satisfaction of following patients throughout their care continuum and her research to reduce the likelihood of transplant rejection.
She also shared an inspirational story of one young patient who spent his life tied to an IV, and how a transplant exposed him to the normal joys of life, like swimming, going to camp and getting on a plane for the first time.
Q: Why did you choose this subspecialty of pediatric GI?
I think it’s the best subspecialty because I think it combines a lot of the things that I enjoy, which is long-term continuity of care. It’s about growing up with your patients and seeing them through all the various stages of their life, often meeting patients when they’re babies. I get pictures of high school graduations and life milestones and even see some of my patients have families of their own. Becoming a part of their family is very meaningful to me. I also like complexity and acuity, and gastroenterology and hepatology provide those things.
And then lastly, it’s great to be able to exercise procedural skills and constantly learn new procedural skills.
Q: How did you become interested in the field of pediatric intestinal and liver transplantation?
I did all my training here at Stanford. We have one of the largest pediatric transplant centers and we also have a very large intestinal rehabilitation population.
Coming through residency and fellowship, I had a lot of exposure to transplant and intestinal failure, intestinal rehabilitation. I really liked the longitudinal relationship I got to form with my patients. Sometimes they’re in the neonatal ICU, where you’re meeting them in their very first days of life. You follow them through their chronic illness, through transplant and after transplant for many years. You become not just their GI, but the center of their care.
Q: What challenges are unique to this type of transplant work?
Pediatric intestinal failure and intestinal transplant represents an incredibly small subset of children. Oftentimes, they do not get the resources and recognition on a national policy level or even at the hospital level that other gastrointestinal diseases receive. What’s difficult is they are such a small subset but their complexity and their needs are probably in the highest percentile. So that’s a really challenging combination to start with. And there’s only a few centers that specialize in doing intestinal rehabilitation and intestinal transplantation for children in the country.
Developing expertise has been slow. But I think in the last decade or so, our understanding and success with intestinal rehabilitation and intestinal transplantation has really improved, especially at large centers like Stanford. We’ve had a lot of success stories and have not had any graft loss since 2014.
Q: Are these transplants hard to acquire?
Yes, especially when you’re transplanting not just the intestines but the liver as well. You’re waiting for two organs, not just one organ. And on top of that, you’re waiting for an appropriately sized donor; usually a child who’s around the same size or same age who’s passed away. Those organs would have to be a good match. Children can wait multiple years for a transplant.
Q: Is there a success story you’d like to share?
One patient I met in the neonatal ICU had congenital short bowel syndrome. He was born with hardly any intestines. He developed complications of being on long-term intravenous nutrition, which included recurrent central line infections and liver disease. He was never able to eat because he really didn’t have a digestive system that could adequately absorb anything. He had a central line in one of his large veins, so he couldn’t go swimming.
He had to have special adaptive wear to even shower or bathe and couldn’t travel. It’s these types of patients that benefit so much from transplant. Putting any kid through transplant is a massive undertaking and it certainly has risks. But he underwent a successful transplant at the age of 8—not just an intestinal transplant, but a multi-visceral transplant of the liver, intestine, and pancreas. He’s 9 years old now, and no longer needs intravenous nutrition. He ate by mouth for the very first time after transplant. He’s trying all sorts of new foods and he was able to go to a special transplant camp for children. Getting on a plane to Los Angeles, which is where our transplant camp is, was a huge deal.
He was able to swim in the lake. He’s never been able to do that. And he wants to start doing sports this fall. This was really a life-changing story for him.
Q: What advancements lie ahead for this field of work? Have you work on any notable research?
I think our understanding of transplant immunology has really progressed, especially recently. That’s what part of my research is about—using novel therapies to modulate the immune system of pediatric transplant recipients. The No. 1 complication that occurs after intestinal transplant is rejection because obviously you’re implanting somebody else’s organs into a patient.
I am involved in a clinical trial that’s looking at the use of extracellular vesicles that are isolated from hematopoietic stem cells. These vesicles contain various growth factors, anti-inflammatory proteins and tissue repair factors that we are infusing into intestinal transplant patients with the aim to repair the intestinal tissue patients are rejecting.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
My husband and I have an almost 2-year-old little girl. She keeps us busy and I spend my afternoons chasing after a crazy toddler.
Lightning Round
Texting or talking?
Huge texter
Favorite junk food?
French fries
Cat or dog person?
Dog
Favorite ice cream?
Strawberry
If you weren’t a gastroenterologist, what would you be?Florist
Best place you’ve traveled to?
Thailand
Number of cups of coffee you drink per day?
Too many
Favorite city in the US besides the one you live in?
New York City
Favorite sport?
Tennis
Optimist or pessimist?
Optimist
The best part about working with kids is that “I get to laugh every day,” said Ke-You (Yoyo) Zhang, MD, clinical assistant professor for pediatrics–gastroenterology and hepatology at Stanford Medicine in California.
Everyday life for them is a challenge.
Dealing with sick children is difficult. “But I think the difference between pediatrics and adults is despite how hard things get, children are the single most resilient people you’re ever going to meet,” she said.
Kids don’t always know they’re sick and they don’t act sick, even when they are. “Every day, I literally get on the floor, I get to play, I get to run around. And truly, I have fun every single day. I get excited to go to work. And I think that’s what makes work not feel like work,” said Dr. Zhang.
In an interview, she discussed the satisfaction of following patients throughout their care continuum and her research to reduce the likelihood of transplant rejection.
She also shared an inspirational story of one young patient who spent his life tied to an IV, and how a transplant exposed him to the normal joys of life, like swimming, going to camp and getting on a plane for the first time.
Q: Why did you choose this subspecialty of pediatric GI?
I think it’s the best subspecialty because I think it combines a lot of the things that I enjoy, which is long-term continuity of care. It’s about growing up with your patients and seeing them through all the various stages of their life, often meeting patients when they’re babies. I get pictures of high school graduations and life milestones and even see some of my patients have families of their own. Becoming a part of their family is very meaningful to me. I also like complexity and acuity, and gastroenterology and hepatology provide those things.
And then lastly, it’s great to be able to exercise procedural skills and constantly learn new procedural skills.
Q: How did you become interested in the field of pediatric intestinal and liver transplantation?
I did all my training here at Stanford. We have one of the largest pediatric transplant centers and we also have a very large intestinal rehabilitation population.
Coming through residency and fellowship, I had a lot of exposure to transplant and intestinal failure, intestinal rehabilitation. I really liked the longitudinal relationship I got to form with my patients. Sometimes they’re in the neonatal ICU, where you’re meeting them in their very first days of life. You follow them through their chronic illness, through transplant and after transplant for many years. You become not just their GI, but the center of their care.
Q: What challenges are unique to this type of transplant work?
Pediatric intestinal failure and intestinal transplant represents an incredibly small subset of children. Oftentimes, they do not get the resources and recognition on a national policy level or even at the hospital level that other gastrointestinal diseases receive. What’s difficult is they are such a small subset but their complexity and their needs are probably in the highest percentile. So that’s a really challenging combination to start with. And there’s only a few centers that specialize in doing intestinal rehabilitation and intestinal transplantation for children in the country.
Developing expertise has been slow. But I think in the last decade or so, our understanding and success with intestinal rehabilitation and intestinal transplantation has really improved, especially at large centers like Stanford. We’ve had a lot of success stories and have not had any graft loss since 2014.
Q: Are these transplants hard to acquire?
Yes, especially when you’re transplanting not just the intestines but the liver as well. You’re waiting for two organs, not just one organ. And on top of that, you’re waiting for an appropriately sized donor; usually a child who’s around the same size or same age who’s passed away. Those organs would have to be a good match. Children can wait multiple years for a transplant.
Q: Is there a success story you’d like to share?
One patient I met in the neonatal ICU had congenital short bowel syndrome. He was born with hardly any intestines. He developed complications of being on long-term intravenous nutrition, which included recurrent central line infections and liver disease. He was never able to eat because he really didn’t have a digestive system that could adequately absorb anything. He had a central line in one of his large veins, so he couldn’t go swimming.
He had to have special adaptive wear to even shower or bathe and couldn’t travel. It’s these types of patients that benefit so much from transplant. Putting any kid through transplant is a massive undertaking and it certainly has risks. But he underwent a successful transplant at the age of 8—not just an intestinal transplant, but a multi-visceral transplant of the liver, intestine, and pancreas. He’s 9 years old now, and no longer needs intravenous nutrition. He ate by mouth for the very first time after transplant. He’s trying all sorts of new foods and he was able to go to a special transplant camp for children. Getting on a plane to Los Angeles, which is where our transplant camp is, was a huge deal.
He was able to swim in the lake. He’s never been able to do that. And he wants to start doing sports this fall. This was really a life-changing story for him.
Q: What advancements lie ahead for this field of work? Have you work on any notable research?
I think our understanding of transplant immunology has really progressed, especially recently. That’s what part of my research is about—using novel therapies to modulate the immune system of pediatric transplant recipients. The No. 1 complication that occurs after intestinal transplant is rejection because obviously you’re implanting somebody else’s organs into a patient.
I am involved in a clinical trial that’s looking at the use of extracellular vesicles that are isolated from hematopoietic stem cells. These vesicles contain various growth factors, anti-inflammatory proteins and tissue repair factors that we are infusing into intestinal transplant patients with the aim to repair the intestinal tissue patients are rejecting.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
My husband and I have an almost 2-year-old little girl. She keeps us busy and I spend my afternoons chasing after a crazy toddler.
Lightning Round
Texting or talking?
Huge texter
Favorite junk food?
French fries
Cat or dog person?
Dog
Favorite ice cream?
Strawberry
If you weren’t a gastroenterologist, what would you be?Florist
Best place you’ve traveled to?
Thailand
Number of cups of coffee you drink per day?
Too many
Favorite city in the US besides the one you live in?
New York City
Favorite sport?
Tennis
Optimist or pessimist?
Optimist
In a Parallel Universe, “I’d Be a Concert Pianist” Says Tennessee GI
She also relishes opportunities to think, to analyze, and solve problems for her patients.
One of her chief interests is inflammatory bowel disease (IBD). It’s reassuring to focus on a field of work “where I know exactly what’s causing the issue, and I can select a therapeutic approach (medication and lifestyle changes) that help a patient achieve remission,” said Dr. Pointer, co-owner and managing partner of Digestive and Liver Health Specialists in Hendersonville, Tenn. She’s also the medical director and a principal investigator of Quality Medical Research in Nashville, and currently serves as chair of the AGA Trainee and Early Career Committee.

Starting her own practice has been just as challenging and rewarding as going through medical school. Medical training does not prepare you for starting your own practice, Dr. Pointer said, so she and her business partner have had to learn as they go. “But I think we’ve done very well. We’ve taken the ups and downs in stride.”
In an interview, Dr. Pointer spoke more about her work in IBD and the ways in which she’s given back to the community through music and mentoring.
Q: Why did you choose GI?
I knew from a very young age that I was going to be a physician. I had always been interested in science. When I got into medical school and became exposed to the different areas, I really liked the cognitive skills where you had to think through a problem or an issue. But I also liked the procedural things as well.
During my internal medicine residency training, I felt that I had a knack for it. As I was looking at different options, I decided on gastroenterology because it combined both cognitive thinking through issues, but also taking it to the next step and intervening through procedures.
Q: During fellowship, your focus was inflammatory bowel disease. What drew your interest to this condition?
There are a lot of different areas within gastroenterology that one can subspecialize in, as we see the full gamut of gastrointestinal and hepatic disorders. But treating some conditions, like functional disorders, means taking more of a ‘trial and error’ approach, and you may not always get the patient a hundred percent better. That’s not to say that we can’t improve a patient’s quality of life, but it’s not always a guarantee.
But inflammatory bowel disease is a little bit different. Because I can point to an exact spot in the intestines that’s causing the problem, it’s very fulfilling for me as a physician to take a patient who is having 10-12 bloody bowel movements a day, to normal form stools and no abdominal pain. They’re able to gain weight and go on about their lives and about their day. So that was why I picked inflammatory bowel disease as my subspecialty.
Q: Tell me about the gastroenterology elective you developed for family medicine residents and undergraduate students. What’s the status of the program now?
I’ve always been interested in teaching and giving back to the next generations. I feel like I had great mentor opportunities and people who helped me along the way. In my previous hospital position, I was able to work with the family medicine department and create an elective through which residents and even undergraduate students could come and shadow and work with me in the clinic and see me performing procedures.
That elective ended once I left that position, at least as far as I’m aware. But in the private practice that I co-own now, we have numerous shadowing opportunities. I was able to give a lecture at Middle Tennessee State University for some students. And through that lecture, many students have reached out to me to shadow. I have allowed them to come shadow and do clinic work as a medical assistant and watch me perform procedures. I have multiple students working with me weekly.
Q: Years ago, you founded the non-profit Enchanted Fingers Piano Lessons, which gave free piano lessons to underserved youth. What was that experience like?
Piano was one of my first loves. In some parallel universe, there’s a Dr. Pointer who is a classical, concert pianist. I started taking piano lessons when I was in early middle school, and I took to it very quickly. I was able to excel. I just loved it. I enjoyed practicing and I still play.
The impetus for starting Enchanted Fingers Piano lessons was because I wanted to give back again to the community. I came from an underserved community. Oftentimes children and young adults in those communities don’t get exposed to extracurricular activities and they don’t even know what they could potentially have a passion for. And I definitely had a passion for piano. I partnered with a church organization and they allowed me to use their church to host these piano lessons, and it was a phenomenal and rewarding experience. I would definitely like to start it up again one day in the future. It was an amazing experience.
It’s actually how I met my husband. He was one of the young adult students who signed up to take lessons. We both still enjoy playing the piano together.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
I’m a creative at heart. I really enjoy sewing and I’m working on a few sewing projects. I just got a serger. It is a machine that helps you finish a seam. It can also be used to sew entire garments. That has been fun, learning how to thread that machine. When I’m not doing that or just relaxing with my family, I do enjoy curling up with a good book. Stephen King is one of my favorite authors.
Lightning Round
Texting or talking?
Talking
Favorite junk food?
Chocolate chip cookies
Cat or dog person?
Cat
Favorite vacation?
Hawaii
How many cups of coffee do you drink per day?
I don’t drink coffee
Favorite ice cream?
Butter pecan
Favorite sport?
I don’t watch sports
Optimist or pessimist?
Optimist
She also relishes opportunities to think, to analyze, and solve problems for her patients.
One of her chief interests is inflammatory bowel disease (IBD). It’s reassuring to focus on a field of work “where I know exactly what’s causing the issue, and I can select a therapeutic approach (medication and lifestyle changes) that help a patient achieve remission,” said Dr. Pointer, co-owner and managing partner of Digestive and Liver Health Specialists in Hendersonville, Tenn. She’s also the medical director and a principal investigator of Quality Medical Research in Nashville, and currently serves as chair of the AGA Trainee and Early Career Committee.
Starting her own practice has been just as challenging and rewarding as going through medical school. Medical training does not prepare you for starting your own practice, Dr. Pointer said, so she and her business partner have had to learn as they go. “But I think we’ve done very well. We’ve taken the ups and downs in stride.”
In an interview, Dr. Pointer spoke more about her work in IBD and the ways in which she’s given back to the community through music and mentoring.
Q: Why did you choose GI?
I knew from a very young age that I was going to be a physician. I had always been interested in science. When I got into medical school and became exposed to the different areas, I really liked the cognitive skills where you had to think through a problem or an issue. But I also liked the procedural things as well.
During my internal medicine residency training, I felt that I had a knack for it. As I was looking at different options, I decided on gastroenterology because it combined both cognitive thinking through issues, but also taking it to the next step and intervening through procedures.
Q: During fellowship, your focus was inflammatory bowel disease. What drew your interest to this condition?
There are a lot of different areas within gastroenterology that one can subspecialize in, as we see the full gamut of gastrointestinal and hepatic disorders. But treating some conditions, like functional disorders, means taking more of a ‘trial and error’ approach, and you may not always get the patient a hundred percent better. That’s not to say that we can’t improve a patient’s quality of life, but it’s not always a guarantee.
But inflammatory bowel disease is a little bit different. Because I can point to an exact spot in the intestines that’s causing the problem, it’s very fulfilling for me as a physician to take a patient who is having 10-12 bloody bowel movements a day, to normal form stools and no abdominal pain. They’re able to gain weight and go on about their lives and about their day. So that was why I picked inflammatory bowel disease as my subspecialty.
Q: Tell me about the gastroenterology elective you developed for family medicine residents and undergraduate students. What’s the status of the program now?
I’ve always been interested in teaching and giving back to the next generations. I feel like I had great mentor opportunities and people who helped me along the way. In my previous hospital position, I was able to work with the family medicine department and create an elective through which residents and even undergraduate students could come and shadow and work with me in the clinic and see me performing procedures.
That elective ended once I left that position, at least as far as I’m aware. But in the private practice that I co-own now, we have numerous shadowing opportunities. I was able to give a lecture at Middle Tennessee State University for some students. And through that lecture, many students have reached out to me to shadow. I have allowed them to come shadow and do clinic work as a medical assistant and watch me perform procedures. I have multiple students working with me weekly.
Q: Years ago, you founded the non-profit Enchanted Fingers Piano Lessons, which gave free piano lessons to underserved youth. What was that experience like?
Piano was one of my first loves. In some parallel universe, there’s a Dr. Pointer who is a classical, concert pianist. I started taking piano lessons when I was in early middle school, and I took to it very quickly. I was able to excel. I just loved it. I enjoyed practicing and I still play.
The impetus for starting Enchanted Fingers Piano lessons was because I wanted to give back again to the community. I came from an underserved community. Oftentimes children and young adults in those communities don’t get exposed to extracurricular activities and they don’t even know what they could potentially have a passion for. And I definitely had a passion for piano. I partnered with a church organization and they allowed me to use their church to host these piano lessons, and it was a phenomenal and rewarding experience. I would definitely like to start it up again one day in the future. It was an amazing experience.
It’s actually how I met my husband. He was one of the young adult students who signed up to take lessons. We both still enjoy playing the piano together.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
I’m a creative at heart. I really enjoy sewing and I’m working on a few sewing projects. I just got a serger. It is a machine that helps you finish a seam. It can also be used to sew entire garments. That has been fun, learning how to thread that machine. When I’m not doing that or just relaxing with my family, I do enjoy curling up with a good book. Stephen King is one of my favorite authors.
Lightning Round
Texting or talking?
Talking
Favorite junk food?
Chocolate chip cookies
Cat or dog person?
Cat
Favorite vacation?
Hawaii
How many cups of coffee do you drink per day?
I don’t drink coffee
Favorite ice cream?
Butter pecan
Favorite sport?
I don’t watch sports
Optimist or pessimist?
Optimist
She also relishes opportunities to think, to analyze, and solve problems for her patients.
One of her chief interests is inflammatory bowel disease (IBD). It’s reassuring to focus on a field of work “where I know exactly what’s causing the issue, and I can select a therapeutic approach (medication and lifestyle changes) that help a patient achieve remission,” said Dr. Pointer, co-owner and managing partner of Digestive and Liver Health Specialists in Hendersonville, Tenn. She’s also the medical director and a principal investigator of Quality Medical Research in Nashville, and currently serves as chair of the AGA Trainee and Early Career Committee.
Starting her own practice has been just as challenging and rewarding as going through medical school. Medical training does not prepare you for starting your own practice, Dr. Pointer said, so she and her business partner have had to learn as they go. “But I think we’ve done very well. We’ve taken the ups and downs in stride.”
In an interview, Dr. Pointer spoke more about her work in IBD and the ways in which she’s given back to the community through music and mentoring.
Q: Why did you choose GI?
I knew from a very young age that I was going to be a physician. I had always been interested in science. When I got into medical school and became exposed to the different areas, I really liked the cognitive skills where you had to think through a problem or an issue. But I also liked the procedural things as well.
During my internal medicine residency training, I felt that I had a knack for it. As I was looking at different options, I decided on gastroenterology because it combined both cognitive thinking through issues, but also taking it to the next step and intervening through procedures.
Q: During fellowship, your focus was inflammatory bowel disease. What drew your interest to this condition?
There are a lot of different areas within gastroenterology that one can subspecialize in, as we see the full gamut of gastrointestinal and hepatic disorders. But treating some conditions, like functional disorders, means taking more of a ‘trial and error’ approach, and you may not always get the patient a hundred percent better. That’s not to say that we can’t improve a patient’s quality of life, but it’s not always a guarantee.
But inflammatory bowel disease is a little bit different. Because I can point to an exact spot in the intestines that’s causing the problem, it’s very fulfilling for me as a physician to take a patient who is having 10-12 bloody bowel movements a day, to normal form stools and no abdominal pain. They’re able to gain weight and go on about their lives and about their day. So that was why I picked inflammatory bowel disease as my subspecialty.
Q: Tell me about the gastroenterology elective you developed for family medicine residents and undergraduate students. What’s the status of the program now?
I’ve always been interested in teaching and giving back to the next generations. I feel like I had great mentor opportunities and people who helped me along the way. In my previous hospital position, I was able to work with the family medicine department and create an elective through which residents and even undergraduate students could come and shadow and work with me in the clinic and see me performing procedures.
That elective ended once I left that position, at least as far as I’m aware. But in the private practice that I co-own now, we have numerous shadowing opportunities. I was able to give a lecture at Middle Tennessee State University for some students. And through that lecture, many students have reached out to me to shadow. I have allowed them to come shadow and do clinic work as a medical assistant and watch me perform procedures. I have multiple students working with me weekly.
Q: Years ago, you founded the non-profit Enchanted Fingers Piano Lessons, which gave free piano lessons to underserved youth. What was that experience like?
Piano was one of my first loves. In some parallel universe, there’s a Dr. Pointer who is a classical, concert pianist. I started taking piano lessons when I was in early middle school, and I took to it very quickly. I was able to excel. I just loved it. I enjoyed practicing and I still play.
The impetus for starting Enchanted Fingers Piano lessons was because I wanted to give back again to the community. I came from an underserved community. Oftentimes children and young adults in those communities don’t get exposed to extracurricular activities and they don’t even know what they could potentially have a passion for. And I definitely had a passion for piano. I partnered with a church organization and they allowed me to use their church to host these piano lessons, and it was a phenomenal and rewarding experience. I would definitely like to start it up again one day in the future. It was an amazing experience.
It’s actually how I met my husband. He was one of the young adult students who signed up to take lessons. We both still enjoy playing the piano together.
Q: When you’re not being a GI, how do you spend your free weekend afternoons?
I’m a creative at heart. I really enjoy sewing and I’m working on a few sewing projects. I just got a serger. It is a machine that helps you finish a seam. It can also be used to sew entire garments. That has been fun, learning how to thread that machine. When I’m not doing that or just relaxing with my family, I do enjoy curling up with a good book. Stephen King is one of my favorite authors.
Lightning Round
Texting or talking?
Talking
Favorite junk food?
Chocolate chip cookies
Cat or dog person?
Cat
Favorite vacation?
Hawaii
How many cups of coffee do you drink per day?
I don’t drink coffee
Favorite ice cream?
Butter pecan
Favorite sport?
I don’t watch sports
Optimist or pessimist?
Optimist

New SVS Task Force Explores Vascular Certification Program
The Society for Vascular Surgery (SVS) executive board has established a task force to explore developing a vascular certification program for inpatient and outpatient care settings.
Noting the shift in professional reimbursement from payment for volume to payment for quality, along with a surge in outpatient endovascular care, “The SVS executive board believes that it is a critical time for vascular surgery to set standards based on quality improvement, efficiency and appropriateness,” said Dr. R. Clement Darling III, SVS president.
Task force chair Dr. Tony Sidawy will oversee two subcommittees, one for inpatient and one for office-based endovascular care (OBEC). Dr. Krishna Jain has been appointed chair of the OBEC subcommittee. A chair for the inpatient subcommittee has yet to be named.
“Vascular surgeons represented by the SVS should take the lead in defining quality and value standards for vascular care before they are defined for us,” said Dr. Sidawy.
“Offering an SVS-led certification process will inspire the most appropriate, high-quality vascular care and optimal outcomes for all patients,” Dr. Jain added.
Many SVS members are pioneers in the design and delivery of care in office-based practice settings, and they have been fierce advocates for this effort, said Dr. Darling. “We have heard our members loud and clear. They want SVS to play a major role in shaping the future of the office-based endovascular center, setting the bar for appropriateness and quality and helping all practitioners achieve it.
“We feel that to provide the best vascular care in a data-driven, quality-based system, the SVS needs to be actively involved in this process," he added. "Vascular surgeons have a long history of making data-driven decisions about which patients need an intervention, and since we treat patients medically as well as by endovascular or open techniques, we have a unique perspective."
A data registry is a critical component and will be provided by the SVS Patient Safety Organization and Vascular Quality Initiative (SVS VQI). VQI registries are already used in more than 430 vascular care settings, ranging from academic to community practice. VQI data can be used to benchmark performance and improve the quality of vascular care.
“Given that the SVS VQI has already been adopted by all types of facilities, including OBECs and vein centers, the SVS VQI is well positioned to help assess and improve quality of care,” said Dr. Jens Eldrup-Jorgensen, SVS PSO medical director.
The process will include discussions and potential collaboration with partners such as the American College of Surgeons, the Outpatient Endovascular and Interventional Society and the Intersociety Accreditation Council, Dr. Darling said, as well as societies such as the American Venous Forum, the Society for Vascular Ultrasound, and the Society for Vascular Nursing.
If established, a pilot program would be launched in 2018 with a full launch planned in 2019.
The Society for Vascular Surgery (SVS) executive board has established a task force to explore developing a vascular certification program for inpatient and outpatient care settings.
Noting the shift in professional reimbursement from payment for volume to payment for quality, along with a surge in outpatient endovascular care, “The SVS executive board believes that it is a critical time for vascular surgery to set standards based on quality improvement, efficiency and appropriateness,” said Dr. R. Clement Darling III, SVS president.
Task force chair Dr. Tony Sidawy will oversee two subcommittees, one for inpatient and one for office-based endovascular care (OBEC). Dr. Krishna Jain has been appointed chair of the OBEC subcommittee. A chair for the inpatient subcommittee has yet to be named.
“Vascular surgeons represented by the SVS should take the lead in defining quality and value standards for vascular care before they are defined for us,” said Dr. Sidawy.
“Offering an SVS-led certification process will inspire the most appropriate, high-quality vascular care and optimal outcomes for all patients,” Dr. Jain added.
Many SVS members are pioneers in the design and delivery of care in office-based practice settings, and they have been fierce advocates for this effort, said Dr. Darling. “We have heard our members loud and clear. They want SVS to play a major role in shaping the future of the office-based endovascular center, setting the bar for appropriateness and quality and helping all practitioners achieve it.
“We feel that to provide the best vascular care in a data-driven, quality-based system, the SVS needs to be actively involved in this process," he added. "Vascular surgeons have a long history of making data-driven decisions about which patients need an intervention, and since we treat patients medically as well as by endovascular or open techniques, we have a unique perspective."
A data registry is a critical component and will be provided by the SVS Patient Safety Organization and Vascular Quality Initiative (SVS VQI). VQI registries are already used in more than 430 vascular care settings, ranging from academic to community practice. VQI data can be used to benchmark performance and improve the quality of vascular care.
“Given that the SVS VQI has already been adopted by all types of facilities, including OBECs and vein centers, the SVS VQI is well positioned to help assess and improve quality of care,” said Dr. Jens Eldrup-Jorgensen, SVS PSO medical director.
The process will include discussions and potential collaboration with partners such as the American College of Surgeons, the Outpatient Endovascular and Interventional Society and the Intersociety Accreditation Council, Dr. Darling said, as well as societies such as the American Venous Forum, the Society for Vascular Ultrasound, and the Society for Vascular Nursing.
If established, a pilot program would be launched in 2018 with a full launch planned in 2019.
The Society for Vascular Surgery (SVS) executive board has established a task force to explore developing a vascular certification program for inpatient and outpatient care settings.
Noting the shift in professional reimbursement from payment for volume to payment for quality, along with a surge in outpatient endovascular care, “The SVS executive board believes that it is a critical time for vascular surgery to set standards based on quality improvement, efficiency and appropriateness,” said Dr. R. Clement Darling III, SVS president.
Task force chair Dr. Tony Sidawy will oversee two subcommittees, one for inpatient and one for office-based endovascular care (OBEC). Dr. Krishna Jain has been appointed chair of the OBEC subcommittee. A chair for the inpatient subcommittee has yet to be named.
“Vascular surgeons represented by the SVS should take the lead in defining quality and value standards for vascular care before they are defined for us,” said Dr. Sidawy.
“Offering an SVS-led certification process will inspire the most appropriate, high-quality vascular care and optimal outcomes for all patients,” Dr. Jain added.
Many SVS members are pioneers in the design and delivery of care in office-based practice settings, and they have been fierce advocates for this effort, said Dr. Darling. “We have heard our members loud and clear. They want SVS to play a major role in shaping the future of the office-based endovascular center, setting the bar for appropriateness and quality and helping all practitioners achieve it.
“We feel that to provide the best vascular care in a data-driven, quality-based system, the SVS needs to be actively involved in this process," he added. "Vascular surgeons have a long history of making data-driven decisions about which patients need an intervention, and since we treat patients medically as well as by endovascular or open techniques, we have a unique perspective."
A data registry is a critical component and will be provided by the SVS Patient Safety Organization and Vascular Quality Initiative (SVS VQI). VQI registries are already used in more than 430 vascular care settings, ranging from academic to community practice. VQI data can be used to benchmark performance and improve the quality of vascular care.
“Given that the SVS VQI has already been adopted by all types of facilities, including OBECs and vein centers, the SVS VQI is well positioned to help assess and improve quality of care,” said Dr. Jens Eldrup-Jorgensen, SVS PSO medical director.
The process will include discussions and potential collaboration with partners such as the American College of Surgeons, the Outpatient Endovascular and Interventional Society and the Intersociety Accreditation Council, Dr. Darling said, as well as societies such as the American Venous Forum, the Society for Vascular Ultrasound, and the Society for Vascular Nursing.
If established, a pilot program would be launched in 2018 with a full launch planned in 2019.
VAM ’17 Will Be a ‘Spectacular Meeting’
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Dr. David Lieberman: A Groundbreaking Career in Gastroenterology
David Lieberman, MD, AGAF, spent much of his long career asking questions about everyday clinical practice in GI medicine and then researching ways to answer those questions.
“The answer to one question often leads to further questions. And I think that’s what makes this research so exciting and dynamic,” said Lieberman, professor emeritus with Oregon Health and Science University, where he served as chief of the Division of Gastroenterology and Hepatology for 24 years.
He was also instrumental in creating a blood and tissue repository for colorectal cancer (CRC) research, and a national endoscopic database.
His groundbreaking GI research in colorectal cancer screening earned him AGA’s Julius Friedenwald Medal, a top career honor. “We started off with some questions about the role of specific screening tests like colonoscopy and stool-based tests for screening,” he said. This led to the first large study about the value of screening with colonoscopy, which set the stage for current screening guidelines. Assessing more than 3,000 asymptomatic adults, Lieberman and colleagues determined that colonoscopy was more effective than sigmoidoscopy in detecting advanced colonic neoplasms.

The next phase of research focused on how well GI doctors were performing colonoscopy, asking questions about the quality of the colonoscopies being performed, and what course of action to take in polyp discovery. “We did some work related to polyp surveillance, what happens after we take out polyps and some recommendations for the appropriate length of follow up afterwards,” he summarized.
Most recently, Lieberman has centered his research on program effectiveness. “If you’re doing high quality colonoscopy and you’re doing appropriate surveillance, how effective is that? And what are the potential problems that might impair effectiveness?”
Adherence and participation remain significant challenges, he said. “If people don’t get the tests done, then they’re not going to be effective. Or if they get part of it done, there can be issues.”
In an interview, Lieberman discussed the reasons why people resist CRC screening, and the new technologies and research underway to make screening options more palatable for reluctant patients.
What do you think are the biggest deterrents to getting screened for CRC?
Dr. Lieberman: The whole idea of dealing with a stool sample is not appealing to patients. The second issue, and this has been shown in many studies, is patients who are referred for colonoscopy may resist because they have heard stories about bowel preps and about colonoscopy itself. But there are many other reasons. I mean, there are issues with access to care that are important. What if you have a positive stool test and you need to get a colonoscopy? How do you get a colonoscopy? There are barriers in moving from one test to the other in a different setting. There are issues with having to take a day off work that’s potentially a financial hardship for some patients. If you’re taking care of elderly relatives or children or if you need transportation, that’s an issue for people.
So, there are many potential barriers, and we’ve been trying to work at a national level to try to understand these barriers and then develop tools to mitigate these problems and improve the overall participation in screening.
How has the field of GI changed since you started practicing medicine?
Dr. Lieberman: I think there have been many exciting changes in technology. The endoscopes we used when I started my career were called fiberoptic scopes. These were scopes that contained tiny glass fibers that ran the length of the scope, and they were good, but not great in terms of imaging, and sometimes they would break down. We now have digital imaging that far surpasses the quality there. We’ve come a long way in terms of things like CT scans, for example, and MRI imaging. The other big technology change has been the development of minimally invasive treatments. For example, if you have a gallstone that’s in your bile duct, we now have ways to remove that without sending the patient to surgery.
The second big change has been the assessment of quality. When I started my career in gastroenterology, we were doing a lot of things, but we didn’t necessarily know if we were doing them well. Most of us thought we were doing them well, of course, but nobody was really measuring quality. There were no quality benchmarks. And so if you don’t measure it, you don’t know. Where we are today in gastroenterology is we’re intensively concerned about quality and measuring quality in various aspects of what we do. And I think that’s a positive development.
What key achievements came out of the U.S. Multi-Society Task Force on Colorectal Cancer?
Dr. Lieberman: This panel evolved because back in the early 2000s, each of the GI organizations were producing guidelines related to colon cancer screening and follow-up. And they were slightly different. This was an attempt to bring all the relevant groups together and try to align the guidelines and recommendations among the GI organizations so that there wouldn’t be a confusing message.
Over the history of this task force, which started around 2002, it’s been remarkably productive. The task force has really examined all aspects of colorectal cancer, including things like the bowel prep, quality of exams, high risk management, hereditary syndromes that can lead to the higher likelihood of developing colon cancer, polypectomy and polypectomy techniques, and screening and surveillance recommendations, which have evolved over time. It’s been, in my opinion, a remarkably productive task force and continues to this day. I’m so very proud of that group.
Could you give a status update on the blood and tissue repository you created for CRC research?
Dr. Lieberman: Our initial studies were part of a Veterans Affairs cooperative study, which is a mechanism of funding within the VA that allows us to work with multiple VA centers to collect data and information. At the very outset of this study, we were performing screening colonoscopies in individuals, and we decided to create a bio-repository that included blood samples, polyp tissue, and normal rectal tissue. The thinking was at some point we might be able to do some genomic studies that might help us predict which patients are most likely to develop colon polyps and colon cancer. All that happened in the 1990s. It was supported by the National Cancer Institute. We created this repository, which sat for a long period of time while we were waiting for the technology to develop and so that we could perform genomic studies in a cost-effective way.
We’re now at that point, which is really exciting. We’re beginning to look at this tissue and perform some genomic studies. Some of this data has been presented at national meetings. This was a precursor to creating a similar type of bio-repository in a larger VA cooperative study. CSP #577 Colonoscopy vs. Fecal Immunochemical Test in Reducing Mortality from Colorectal Cancer (CONFIRM) is a randomized study comparing two forms of screening, a fecal immunochemical test versus a colonoscopy. We’re in the process of enrolling 50,000 patients in that study. We have also created a blood and tissue repository, which we hope will be useful for future studies.
You lead the AGA CRC Task Force, which advances research and policy initiatives to improve screening rates and patient outcomes. What would you like to see in future GI research, particularly in colorectal cancer?
Dr. Lieberman: We have new blood tests coming along that are going to be very attractive to both patients and physicians. You can obtain a blood sample at a point of service and patients won’t have to deal with stool samples. We need to understand how those tests perform in clinical practice. If the test is abnormal, indicating a patient has a higher risk of colon cancer and should get a colonoscopy, are they getting that colonoscopy or not? And what are the barriers? And if it’s normal, then that patient should have a repeat test at an appropriate interval.
We know that the effectiveness of screening really depends on the participation of individuals in terms of completing the steps. We’ve published some work already on trying to understand the role of these blood tests. We expect that these tests will continue to improve over time.
We’re also working on trying to develop these risk stratification tools that could be used in clinical practice to help figure out the most appropriate test for a particular individual.
Let’s say you go to your doctor for colon cancer screening, and if we could determine that you are a low-risk individual, you may benefit best from having a non-invasive test, like a blood test or a stool test. Whereas if you’re a higher risk individual, you may need to have a more invasive screening test like colonoscopy.
This falls into a concept of personalized medicine where we’re trying to use all the information we have from the medical history, and maybe genomic information that I mentioned earlier, to try to determine who needs the most intensive screening and who might benefit from less intensive screening.
I think the most recent work is really focused on these gaps in screening. And the biggest gap are patients that get a non-invasive test, like a stool test, but do not get a colonoscopy that renders the program ineffective if they don’t get the colonoscopy. We’re trying to highlight that for primary care providers and make sure that everyone understands the importance of this follow-up. And then, trying to develop tools to help the primary care provider navigate that patient to a colonoscopy.
What do you think is the biggest misconception about your specialty?
Dr. Lieberman: If there’s a misconception, it’s that GI physicians are focused on procedures. I think a good GI provider should be holistic, and I think many are. What I mean by holistic is that many GI symptoms could be due to stress, medications, diet, or other aspects of behavior, and the remedy is not necessarily a procedure. I think that many GI physicians are really skilled at obtaining this information and trying to help guide the patient through some uncomfortable symptoms.
It means being more like an internist, spending time with the patient to take a detailed history and delve into many different possibilities that might be going on.
David Lieberman, MD, AGAF, spent much of his long career asking questions about everyday clinical practice in GI medicine and then researching ways to answer those questions.
“The answer to one question often leads to further questions. And I think that’s what makes this research so exciting and dynamic,” said Lieberman, professor emeritus with Oregon Health and Science University, where he served as chief of the Division of Gastroenterology and Hepatology for 24 years.
He was also instrumental in creating a blood and tissue repository for colorectal cancer (CRC) research, and a national endoscopic database.
His groundbreaking GI research in colorectal cancer screening earned him AGA’s Julius Friedenwald Medal, a top career honor. “We started off with some questions about the role of specific screening tests like colonoscopy and stool-based tests for screening,” he said. This led to the first large study about the value of screening with colonoscopy, which set the stage for current screening guidelines. Assessing more than 3,000 asymptomatic adults, Lieberman and colleagues determined that colonoscopy was more effective than sigmoidoscopy in detecting advanced colonic neoplasms.
The next phase of research focused on how well GI doctors were performing colonoscopy, asking questions about the quality of the colonoscopies being performed, and what course of action to take in polyp discovery. “We did some work related to polyp surveillance, what happens after we take out polyps and some recommendations for the appropriate length of follow up afterwards,” he summarized.
Most recently, Lieberman has centered his research on program effectiveness. “If you’re doing high quality colonoscopy and you’re doing appropriate surveillance, how effective is that? And what are the potential problems that might impair effectiveness?”
Adherence and participation remain significant challenges, he said. “If people don’t get the tests done, then they’re not going to be effective. Or if they get part of it done, there can be issues.”
In an interview, Lieberman discussed the reasons why people resist CRC screening, and the new technologies and research underway to make screening options more palatable for reluctant patients.
What do you think are the biggest deterrents to getting screened for CRC?
Dr. Lieberman: The whole idea of dealing with a stool sample is not appealing to patients. The second issue, and this has been shown in many studies, is patients who are referred for colonoscopy may resist because they have heard stories about bowel preps and about colonoscopy itself. But there are many other reasons. I mean, there are issues with access to care that are important. What if you have a positive stool test and you need to get a colonoscopy? How do you get a colonoscopy? There are barriers in moving from one test to the other in a different setting. There are issues with having to take a day off work that’s potentially a financial hardship for some patients. If you’re taking care of elderly relatives or children or if you need transportation, that’s an issue for people.
So, there are many potential barriers, and we’ve been trying to work at a national level to try to understand these barriers and then develop tools to mitigate these problems and improve the overall participation in screening.
How has the field of GI changed since you started practicing medicine?
Dr. Lieberman: I think there have been many exciting changes in technology. The endoscopes we used when I started my career were called fiberoptic scopes. These were scopes that contained tiny glass fibers that ran the length of the scope, and they were good, but not great in terms of imaging, and sometimes they would break down. We now have digital imaging that far surpasses the quality there. We’ve come a long way in terms of things like CT scans, for example, and MRI imaging. The other big technology change has been the development of minimally invasive treatments. For example, if you have a gallstone that’s in your bile duct, we now have ways to remove that without sending the patient to surgery.
The second big change has been the assessment of quality. When I started my career in gastroenterology, we were doing a lot of things, but we didn’t necessarily know if we were doing them well. Most of us thought we were doing them well, of course, but nobody was really measuring quality. There were no quality benchmarks. And so if you don’t measure it, you don’t know. Where we are today in gastroenterology is we’re intensively concerned about quality and measuring quality in various aspects of what we do. And I think that’s a positive development.
What key achievements came out of the U.S. Multi-Society Task Force on Colorectal Cancer?
Dr. Lieberman: This panel evolved because back in the early 2000s, each of the GI organizations were producing guidelines related to colon cancer screening and follow-up. And they were slightly different. This was an attempt to bring all the relevant groups together and try to align the guidelines and recommendations among the GI organizations so that there wouldn’t be a confusing message.
Over the history of this task force, which started around 2002, it’s been remarkably productive. The task force has really examined all aspects of colorectal cancer, including things like the bowel prep, quality of exams, high risk management, hereditary syndromes that can lead to the higher likelihood of developing colon cancer, polypectomy and polypectomy techniques, and screening and surveillance recommendations, which have evolved over time. It’s been, in my opinion, a remarkably productive task force and continues to this day. I’m so very proud of that group.
Could you give a status update on the blood and tissue repository you created for CRC research?
Dr. Lieberman: Our initial studies were part of a Veterans Affairs cooperative study, which is a mechanism of funding within the VA that allows us to work with multiple VA centers to collect data and information. At the very outset of this study, we were performing screening colonoscopies in individuals, and we decided to create a bio-repository that included blood samples, polyp tissue, and normal rectal tissue. The thinking was at some point we might be able to do some genomic studies that might help us predict which patients are most likely to develop colon polyps and colon cancer. All that happened in the 1990s. It was supported by the National Cancer Institute. We created this repository, which sat for a long period of time while we were waiting for the technology to develop and so that we could perform genomic studies in a cost-effective way.
We’re now at that point, which is really exciting. We’re beginning to look at this tissue and perform some genomic studies. Some of this data has been presented at national meetings. This was a precursor to creating a similar type of bio-repository in a larger VA cooperative study. CSP #577 Colonoscopy vs. Fecal Immunochemical Test in Reducing Mortality from Colorectal Cancer (CONFIRM) is a randomized study comparing two forms of screening, a fecal immunochemical test versus a colonoscopy. We’re in the process of enrolling 50,000 patients in that study. We have also created a blood and tissue repository, which we hope will be useful for future studies.
You lead the AGA CRC Task Force, which advances research and policy initiatives to improve screening rates and patient outcomes. What would you like to see in future GI research, particularly in colorectal cancer?
Dr. Lieberman: We have new blood tests coming along that are going to be very attractive to both patients and physicians. You can obtain a blood sample at a point of service and patients won’t have to deal with stool samples. We need to understand how those tests perform in clinical practice. If the test is abnormal, indicating a patient has a higher risk of colon cancer and should get a colonoscopy, are they getting that colonoscopy or not? And what are the barriers? And if it’s normal, then that patient should have a repeat test at an appropriate interval.
We know that the effectiveness of screening really depends on the participation of individuals in terms of completing the steps. We’ve published some work already on trying to understand the role of these blood tests. We expect that these tests will continue to improve over time.
We’re also working on trying to develop these risk stratification tools that could be used in clinical practice to help figure out the most appropriate test for a particular individual.
Let’s say you go to your doctor for colon cancer screening, and if we could determine that you are a low-risk individual, you may benefit best from having a non-invasive test, like a blood test or a stool test. Whereas if you’re a higher risk individual, you may need to have a more invasive screening test like colonoscopy.
This falls into a concept of personalized medicine where we’re trying to use all the information we have from the medical history, and maybe genomic information that I mentioned earlier, to try to determine who needs the most intensive screening and who might benefit from less intensive screening.
I think the most recent work is really focused on these gaps in screening. And the biggest gap are patients that get a non-invasive test, like a stool test, but do not get a colonoscopy that renders the program ineffective if they don’t get the colonoscopy. We’re trying to highlight that for primary care providers and make sure that everyone understands the importance of this follow-up. And then, trying to develop tools to help the primary care provider navigate that patient to a colonoscopy.
What do you think is the biggest misconception about your specialty?
Dr. Lieberman: If there’s a misconception, it’s that GI physicians are focused on procedures. I think a good GI provider should be holistic, and I think many are. What I mean by holistic is that many GI symptoms could be due to stress, medications, diet, or other aspects of behavior, and the remedy is not necessarily a procedure. I think that many GI physicians are really skilled at obtaining this information and trying to help guide the patient through some uncomfortable symptoms.
It means being more like an internist, spending time with the patient to take a detailed history and delve into many different possibilities that might be going on.
David Lieberman, MD, AGAF, spent much of his long career asking questions about everyday clinical practice in GI medicine and then researching ways to answer those questions.
“The answer to one question often leads to further questions. And I think that’s what makes this research so exciting and dynamic,” said Lieberman, professor emeritus with Oregon Health and Science University, where he served as chief of the Division of Gastroenterology and Hepatology for 24 years.
He was also instrumental in creating a blood and tissue repository for colorectal cancer (CRC) research, and a national endoscopic database.
His groundbreaking GI research in colorectal cancer screening earned him AGA’s Julius Friedenwald Medal, a top career honor. “We started off with some questions about the role of specific screening tests like colonoscopy and stool-based tests for screening,” he said. This led to the first large study about the value of screening with colonoscopy, which set the stage for current screening guidelines. Assessing more than 3,000 asymptomatic adults, Lieberman and colleagues determined that colonoscopy was more effective than sigmoidoscopy in detecting advanced colonic neoplasms.
The next phase of research focused on how well GI doctors were performing colonoscopy, asking questions about the quality of the colonoscopies being performed, and what course of action to take in polyp discovery. “We did some work related to polyp surveillance, what happens after we take out polyps and some recommendations for the appropriate length of follow up afterwards,” he summarized.
Most recently, Lieberman has centered his research on program effectiveness. “If you’re doing high quality colonoscopy and you’re doing appropriate surveillance, how effective is that? And what are the potential problems that might impair effectiveness?”
Adherence and participation remain significant challenges, he said. “If people don’t get the tests done, then they’re not going to be effective. Or if they get part of it done, there can be issues.”
In an interview, Lieberman discussed the reasons why people resist CRC screening, and the new technologies and research underway to make screening options more palatable for reluctant patients.
What do you think are the biggest deterrents to getting screened for CRC?
Dr. Lieberman: The whole idea of dealing with a stool sample is not appealing to patients. The second issue, and this has been shown in many studies, is patients who are referred for colonoscopy may resist because they have heard stories about bowel preps and about colonoscopy itself. But there are many other reasons. I mean, there are issues with access to care that are important. What if you have a positive stool test and you need to get a colonoscopy? How do you get a colonoscopy? There are barriers in moving from one test to the other in a different setting. There are issues with having to take a day off work that’s potentially a financial hardship for some patients. If you’re taking care of elderly relatives or children or if you need transportation, that’s an issue for people.
So, there are many potential barriers, and we’ve been trying to work at a national level to try to understand these barriers and then develop tools to mitigate these problems and improve the overall participation in screening.
How has the field of GI changed since you started practicing medicine?
Dr. Lieberman: I think there have been many exciting changes in technology. The endoscopes we used when I started my career were called fiberoptic scopes. These were scopes that contained tiny glass fibers that ran the length of the scope, and they were good, but not great in terms of imaging, and sometimes they would break down. We now have digital imaging that far surpasses the quality there. We’ve come a long way in terms of things like CT scans, for example, and MRI imaging. The other big technology change has been the development of minimally invasive treatments. For example, if you have a gallstone that’s in your bile duct, we now have ways to remove that without sending the patient to surgery.
The second big change has been the assessment of quality. When I started my career in gastroenterology, we were doing a lot of things, but we didn’t necessarily know if we were doing them well. Most of us thought we were doing them well, of course, but nobody was really measuring quality. There were no quality benchmarks. And so if you don’t measure it, you don’t know. Where we are today in gastroenterology is we’re intensively concerned about quality and measuring quality in various aspects of what we do. And I think that’s a positive development.
What key achievements came out of the U.S. Multi-Society Task Force on Colorectal Cancer?
Dr. Lieberman: This panel evolved because back in the early 2000s, each of the GI organizations were producing guidelines related to colon cancer screening and follow-up. And they were slightly different. This was an attempt to bring all the relevant groups together and try to align the guidelines and recommendations among the GI organizations so that there wouldn’t be a confusing message.
Over the history of this task force, which started around 2002, it’s been remarkably productive. The task force has really examined all aspects of colorectal cancer, including things like the bowel prep, quality of exams, high risk management, hereditary syndromes that can lead to the higher likelihood of developing colon cancer, polypectomy and polypectomy techniques, and screening and surveillance recommendations, which have evolved over time. It’s been, in my opinion, a remarkably productive task force and continues to this day. I’m so very proud of that group.
Could you give a status update on the blood and tissue repository you created for CRC research?
Dr. Lieberman: Our initial studies were part of a Veterans Affairs cooperative study, which is a mechanism of funding within the VA that allows us to work with multiple VA centers to collect data and information. At the very outset of this study, we were performing screening colonoscopies in individuals, and we decided to create a bio-repository that included blood samples, polyp tissue, and normal rectal tissue. The thinking was at some point we might be able to do some genomic studies that might help us predict which patients are most likely to develop colon polyps and colon cancer. All that happened in the 1990s. It was supported by the National Cancer Institute. We created this repository, which sat for a long period of time while we were waiting for the technology to develop and so that we could perform genomic studies in a cost-effective way.
We’re now at that point, which is really exciting. We’re beginning to look at this tissue and perform some genomic studies. Some of this data has been presented at national meetings. This was a precursor to creating a similar type of bio-repository in a larger VA cooperative study. CSP #577 Colonoscopy vs. Fecal Immunochemical Test in Reducing Mortality from Colorectal Cancer (CONFIRM) is a randomized study comparing two forms of screening, a fecal immunochemical test versus a colonoscopy. We’re in the process of enrolling 50,000 patients in that study. We have also created a blood and tissue repository, which we hope will be useful for future studies.
You lead the AGA CRC Task Force, which advances research and policy initiatives to improve screening rates and patient outcomes. What would you like to see in future GI research, particularly in colorectal cancer?
Dr. Lieberman: We have new blood tests coming along that are going to be very attractive to both patients and physicians. You can obtain a blood sample at a point of service and patients won’t have to deal with stool samples. We need to understand how those tests perform in clinical practice. If the test is abnormal, indicating a patient has a higher risk of colon cancer and should get a colonoscopy, are they getting that colonoscopy or not? And what are the barriers? And if it’s normal, then that patient should have a repeat test at an appropriate interval.
We know that the effectiveness of screening really depends on the participation of individuals in terms of completing the steps. We’ve published some work already on trying to understand the role of these blood tests. We expect that these tests will continue to improve over time.
We’re also working on trying to develop these risk stratification tools that could be used in clinical practice to help figure out the most appropriate test for a particular individual.
Let’s say you go to your doctor for colon cancer screening, and if we could determine that you are a low-risk individual, you may benefit best from having a non-invasive test, like a blood test or a stool test. Whereas if you’re a higher risk individual, you may need to have a more invasive screening test like colonoscopy.
This falls into a concept of personalized medicine where we’re trying to use all the information we have from the medical history, and maybe genomic information that I mentioned earlier, to try to determine who needs the most intensive screening and who might benefit from less intensive screening.
I think the most recent work is really focused on these gaps in screening. And the biggest gap are patients that get a non-invasive test, like a stool test, but do not get a colonoscopy that renders the program ineffective if they don’t get the colonoscopy. We’re trying to highlight that for primary care providers and make sure that everyone understands the importance of this follow-up. And then, trying to develop tools to help the primary care provider navigate that patient to a colonoscopy.
What do you think is the biggest misconception about your specialty?
Dr. Lieberman: If there’s a misconception, it’s that GI physicians are focused on procedures. I think a good GI provider should be holistic, and I think many are. What I mean by holistic is that many GI symptoms could be due to stress, medications, diet, or other aspects of behavior, and the remedy is not necessarily a procedure. I think that many GI physicians are really skilled at obtaining this information and trying to help guide the patient through some uncomfortable symptoms.
It means being more like an internist, spending time with the patient to take a detailed history and delve into many different possibilities that might be going on.
Why Your Support Matters Now
Federal research funding is uncertain, but discovery can’t wait.
As an AGA member, you can help the AGA Research Foundation ensure that critical digestive health research continues, regardless of the circumstances. With your donation, you will help fuel the next breakthroughs in digestive health by backing bold ideas and early-career investigators when federal dollars fall short.
By donating today, you become a vital part of the solution, helping to provide the necessary funding to foster scientific discovery and enhance patient care for those affected by digestive diseases.
Your support will transform lives and accelerate medical breakthroughs.
Donate by December 31 to receive a tax-credit in 2025. Make your gift by visiting www.foundation.gastro.org.
Federal research funding is uncertain, but discovery can’t wait.
As an AGA member, you can help the AGA Research Foundation ensure that critical digestive health research continues, regardless of the circumstances. With your donation, you will help fuel the next breakthroughs in digestive health by backing bold ideas and early-career investigators when federal dollars fall short.
By donating today, you become a vital part of the solution, helping to provide the necessary funding to foster scientific discovery and enhance patient care for those affected by digestive diseases.
Your support will transform lives and accelerate medical breakthroughs.
Donate by December 31 to receive a tax-credit in 2025. Make your gift by visiting www.foundation.gastro.org.
Federal research funding is uncertain, but discovery can’t wait.
As an AGA member, you can help the AGA Research Foundation ensure that critical digestive health research continues, regardless of the circumstances. With your donation, you will help fuel the next breakthroughs in digestive health by backing bold ideas and early-career investigators when federal dollars fall short.
By donating today, you become a vital part of the solution, helping to provide the necessary funding to foster scientific discovery and enhance patient care for those affected by digestive diseases.
Your support will transform lives and accelerate medical breakthroughs.
Donate by December 31 to receive a tax-credit in 2025. Make your gift by visiting www.foundation.gastro.org.
More Than 100 GIs Strong for Advocacy Day 2025!
For our leaders, showing up on behalf of their patients is a privilege and an opportunity to represent the specialty with individuals who have a role in dictating health care policy.

In total, 124 members, patient advocates, and AGA staffers met with lawmakers and attended 130 meetings – 70 unique House districts and 60 unique Senate districts – with Republican and Democratic staff.
Our advocacy contingent represented the diversity of the country with 30 states represented from coast-to-coast. No matter the home state, everyone was united in the calls to Congress: to reform prior authorization, increase digestive disease funding, and secure a permanent solution for Medicare physician reimbursement.
As in past years, patient advocates participated alongside GI clinicians and researchers.
Their participation underscored the importance of including diverse voices. As patients with chronic health conditions, they were able to convey how their experiences navigating insurance barriers or managing delays to care as prescribed by their health care provider impacted their well-being and quality of life.
Throughout the day, patient advocates and GIs alike were encouraged by their meetings with congressional staffers. Conversations were constructive, engaging, and meaningful as everyone collaborated on common ground: seeking solutions to ensure GI patients have timely access to care that they need.
Many AGA leaders appreciated the value of being able to unite with colleagues to advocate and share their firsthand experiences in the lab or clinic in meetings with House and Senate staffers.
While Advocacy Day lasts a single day, its value hasn’t diminished. Thanks to the engagement and participation of the more than 100 AGA leaders and patient advocates, we can continue to build positive relationships with influential policymakers and make strides to improve and protect access to GI patient care.
For our leaders, showing up on behalf of their patients is a privilege and an opportunity to represent the specialty with individuals who have a role in dictating health care policy.
In total, 124 members, patient advocates, and AGA staffers met with lawmakers and attended 130 meetings – 70 unique House districts and 60 unique Senate districts – with Republican and Democratic staff.
Our advocacy contingent represented the diversity of the country with 30 states represented from coast-to-coast. No matter the home state, everyone was united in the calls to Congress: to reform prior authorization, increase digestive disease funding, and secure a permanent solution for Medicare physician reimbursement.
As in past years, patient advocates participated alongside GI clinicians and researchers.
Their participation underscored the importance of including diverse voices. As patients with chronic health conditions, they were able to convey how their experiences navigating insurance barriers or managing delays to care as prescribed by their health care provider impacted their well-being and quality of life.
Throughout the day, patient advocates and GIs alike were encouraged by their meetings with congressional staffers. Conversations were constructive, engaging, and meaningful as everyone collaborated on common ground: seeking solutions to ensure GI patients have timely access to care that they need.
Many AGA leaders appreciated the value of being able to unite with colleagues to advocate and share their firsthand experiences in the lab or clinic in meetings with House and Senate staffers.
While Advocacy Day lasts a single day, its value hasn’t diminished. Thanks to the engagement and participation of the more than 100 AGA leaders and patient advocates, we can continue to build positive relationships with influential policymakers and make strides to improve and protect access to GI patient care.
For our leaders, showing up on behalf of their patients is a privilege and an opportunity to represent the specialty with individuals who have a role in dictating health care policy.
In total, 124 members, patient advocates, and AGA staffers met with lawmakers and attended 130 meetings – 70 unique House districts and 60 unique Senate districts – with Republican and Democratic staff.
Our advocacy contingent represented the diversity of the country with 30 states represented from coast-to-coast. No matter the home state, everyone was united in the calls to Congress: to reform prior authorization, increase digestive disease funding, and secure a permanent solution for Medicare physician reimbursement.
As in past years, patient advocates participated alongside GI clinicians and researchers.
Their participation underscored the importance of including diverse voices. As patients with chronic health conditions, they were able to convey how their experiences navigating insurance barriers or managing delays to care as prescribed by their health care provider impacted their well-being and quality of life.
Throughout the day, patient advocates and GIs alike were encouraged by their meetings with congressional staffers. Conversations were constructive, engaging, and meaningful as everyone collaborated on common ground: seeking solutions to ensure GI patients have timely access to care that they need.
Many AGA leaders appreciated the value of being able to unite with colleagues to advocate and share their firsthand experiences in the lab or clinic in meetings with House and Senate staffers.
While Advocacy Day lasts a single day, its value hasn’t diminished. Thanks to the engagement and participation of the more than 100 AGA leaders and patient advocates, we can continue to build positive relationships with influential policymakers and make strides to improve and protect access to GI patient care.
Supporting Exceptional Researchers
Did you know that the AGA Research Foundation helped support 74 researchers this past May?

But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: www.foundation@gastro.org or contact us at foundation@gastro.org.
Did you know that the AGA Research Foundation helped support 74 researchers this past May?
But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: www.foundation@gastro.org or contact us at foundation@gastro.org.
Did you know that the AGA Research Foundation helped support 74 researchers this past May?
But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: www.foundation@gastro.org or contact us at foundation@gastro.org.
Support GI Research Through a Named Research Award
Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Named award. An AGA pilot award can be renamed after you or a loved one, and targeted for a specific gastrointestinal research area. A new pilot research award can be established with a pledge of $40,000+ or through an estate gift. Gifts of cash or appreciated securities may be used to establish a named award.
Your next step. A named award gift is a wonderful way to acknowledge a loved one’s vision for the future. To learn more about ways to recognize your honoree, contact us at foundation@gastro.org.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Named award. An AGA pilot award can be renamed after you or a loved one, and targeted for a specific gastrointestinal research area. A new pilot research award can be established with a pledge of $40,000+ or through an estate gift. Gifts of cash or appreciated securities may be used to establish a named award.
Your next step. A named award gift is a wonderful way to acknowledge a loved one’s vision for the future. To learn more about ways to recognize your honoree, contact us at foundation@gastro.org.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Named award. An AGA pilot award can be renamed after you or a loved one, and targeted for a specific gastrointestinal research area. A new pilot research award can be established with a pledge of $40,000+ or through an estate gift. Gifts of cash or appreciated securities may be used to establish a named award.
Your next step. A named award gift is a wonderful way to acknowledge a loved one’s vision for the future. To learn more about ways to recognize your honoree, contact us at foundation@gastro.org.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
AGA Women’s Committee Outlines Roadmap Towards Gender Equity
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
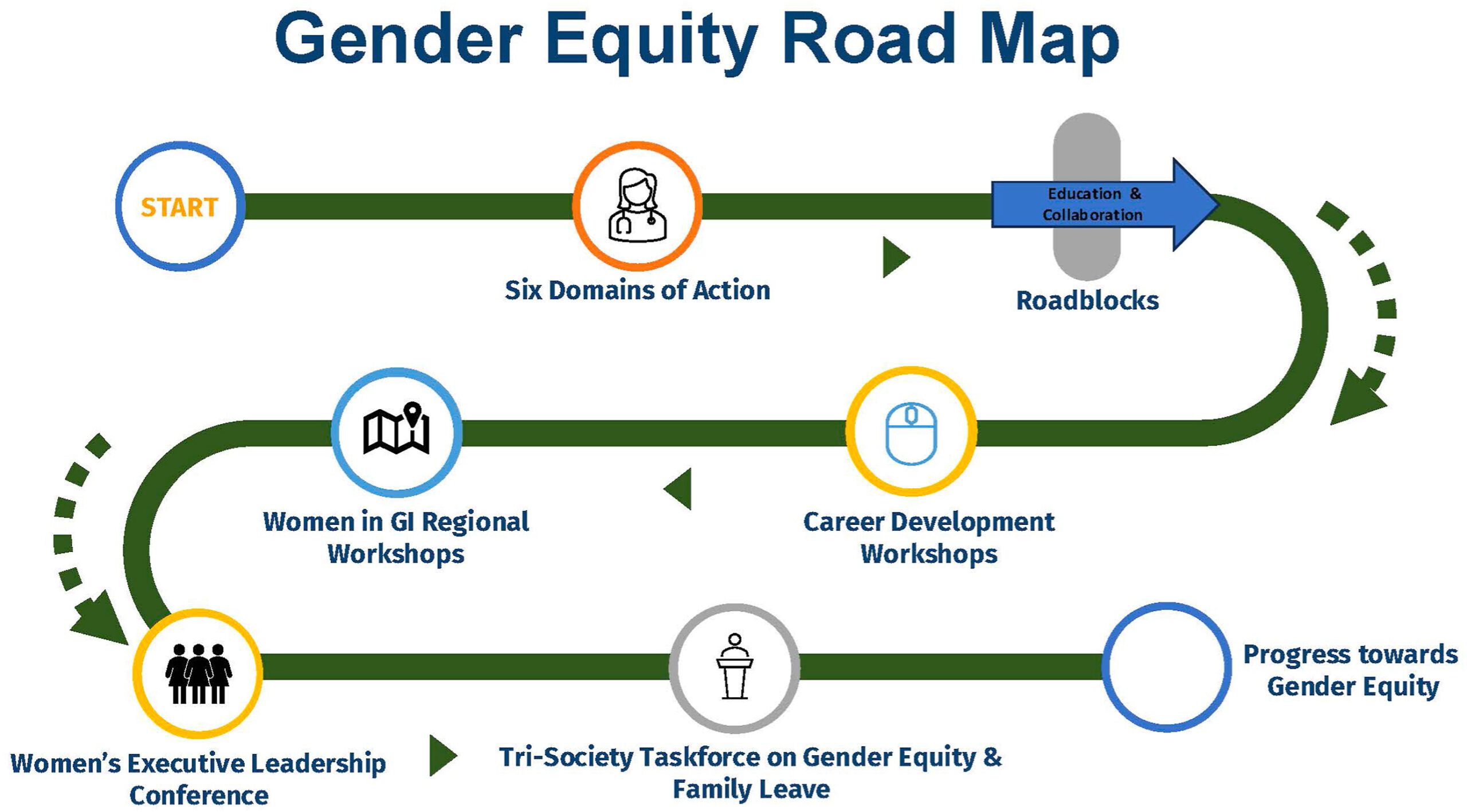
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
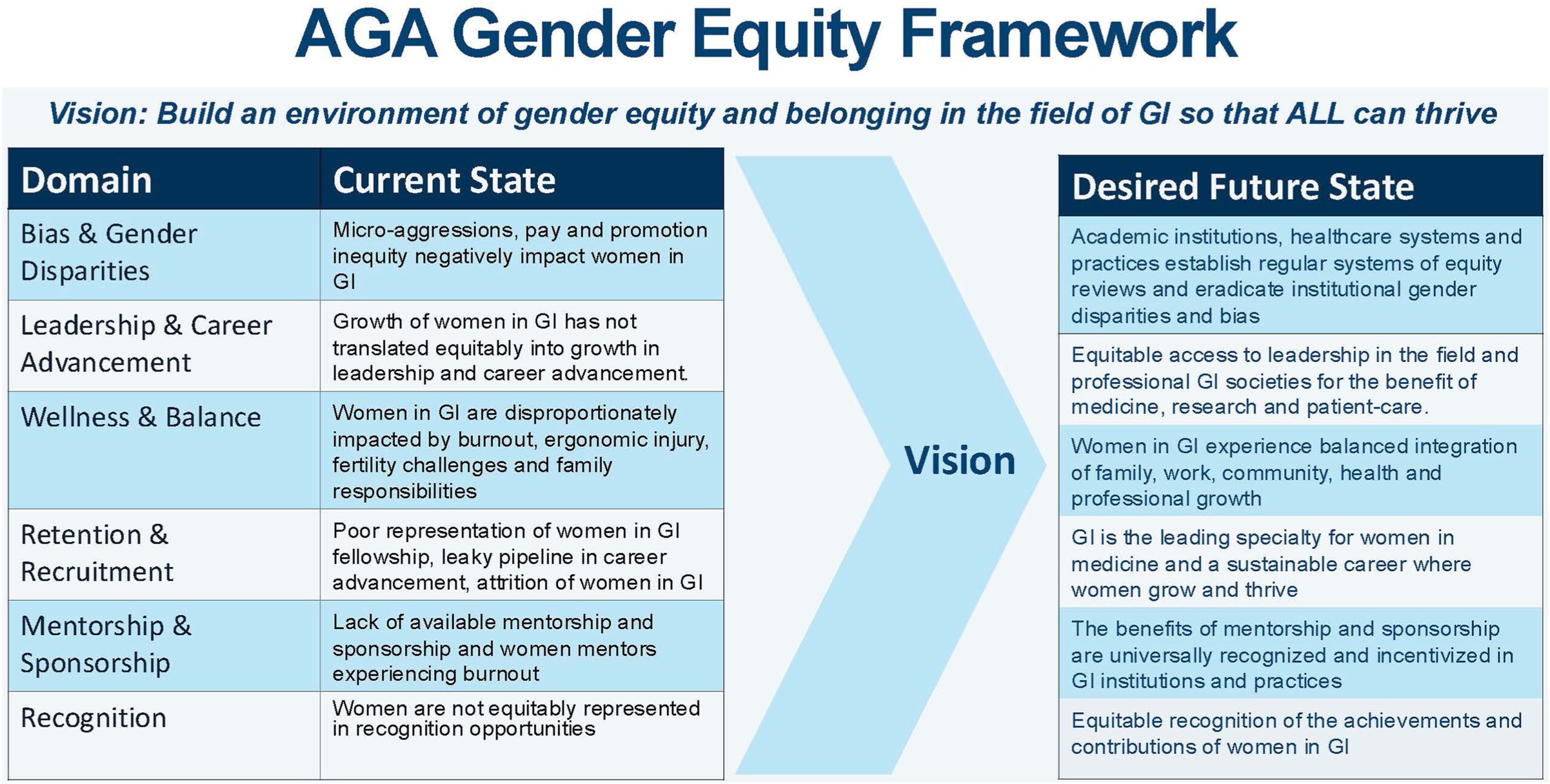
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.