User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Combination approach to melasma treatment yields best results
When establishing a treatment plan for patients with melasma, counseling them about realistic expectations is key.

“It’s important that they understand that this is a chronic condition, so it does require long-term maintenance therapy,” Arisa E. Ortiz, MD, said at the virtual annual Masters of Aesthetics Symposium. “We can improve melasma, but it’s difficult to cure melasma.”
While hydroquinone and other bleaching agents are typical treatment mainstays, chemical peels with glycolic acid, trichloroacetic acid, and salicylic acid can benefit some individuals. “For chemical peels, I really like glycolic acid peels because there is no downtime; it peels at the microscopic level,” said Dr. Ortiz, who is director of laser and cosmetic dermatology at the University of California, San Diego. “This is something they may need to repeat monthly, and having a week of peeling may be difficult to go through every month.”
Other common melasma treatments include lasers, intense pulsed light (IPL), and oral medications. “I personally am not impressed with microdermabrasion for melasma, so I don’t use that very much,” she said. “With laser treatment, you want to make sure you’re using low-energy lasers so that it doesn’t exacerbate or make them relapse or rebound.”
While hydroquinone is a mainstay of therapy, “you can’t use it chronically because of the risk of ochronosis (permanent darkening), so you do need to take drug holidays,” Dr. Ortiz said. “During those drug holidays, you want to make sure patients have a nonhydroquinone bleaching agent so that they don’t flare.” Options include lignin peroxidase, oligopeptide, Lytera, Melaplex, 4-n-butylresorcinol, Cysteamine cream, tranexamic acid, and oral antioxidants.
In a study sponsored by SkinMedica, investigators conducted a randomized, double-blind, half-face study in females with moderate to severe facial hyperpigmentation to assess the efficacy and tolerability of three new skin brightener formulations containing SMA-432, a prostaglandin E2 inhibitor, compared with topical 4% hydroquinone (J Drugs Dermatol 2012 Dec;11[12]:1478-82). They found that the nonhydroquinone skin formulations were better tolerated and were just as effective as 4% hydroquinone.
In a separate unpublished study of 22 females, investigators assessed the efficacy of the U.SK Advanced Defense Booster, which contains ferulic acid, maslinic acid, peptides, and olive leaf extract. They observed that 98% of patients saw improvement after 28 days of treatment.
When it comes to using lasers for melasma treatment, low-energy devices provide the best outcomes. “I prefer using something like the 1927-nm fractional diode lasers at 3.75% density, really low densities because there’s less risk for rebound,” Dr. Ortiz said. “They also enhance skin permeability for the use of topicals.”
In an observational study of 27 female patients with refractory melasma, Arielle Kauvar, MD, director of New York Laser & Skin Care, combined microdermabrasion with the Q-switched Nd:YAG (Lasers in Surgery and Medicine 2012; 44:117-24). “The settings she used were very low fluence, so there was no clinical endpoint or no whitening,” Dr. Ortiz said. Specifically, she used a laser at 1.6-2 J/cm2 with a 5- or 6-mm spot size immediately following microdermabrasion for 4 weeks. “She got a good improvement using a skin care regimen of sunscreen, hydroquinone, and tretinoin or vitamin C,” she said. “Remission lasted at least 6 months.”
In a study presented at the 2019 annual meeting of the America Society for Laser Medicine and Surgery, Dr. Ortiz and Tanya Greywal, MD, of the University of California, San Diego, used three passes of the 10764-nm Nd:YAG laser to treat 10 subjects with melasma skin types 2-5. The device has a 650-microsecond pulse duration, a 6-mm spot size, and an energy mode of 11-14 J/cm3. “There was no downtime with these patients, and they saw a mean improvement of 26%-50% as early as 3 weeks,” she said. “Patients did require multiple treatments to see adequate resolution, but no anesthesia or numbing cream was required. This is a good option for patients who need chronic maintenance treatment.”
Topicals also play a key role following the laser treatment of melasma. Dr. Ortiz characterized clobetasol as “kind of like the magic ointment.” She uses one application immediately post procedure “whenever I’m worried about a patient having postinflammatory hyperpigmentation or if I don’t want melasma patients to rebound. It can help reduce swelling and inflammation to decrease the risk of postinflammatory hyperpigmentation.”
Researchers have discovered that there is a vascular component to melasma. Paul M. Friedman, MD, of the Dermatology and Laser Surgery Center, Houston, and his colleagues used spectrocolorimetry to detect an underlying prominent vascular component in 11 patients with melasma (Lasers Surg Med 2017 Jan;49[1]:20-6). They determined that melasma lesions exhibiting subtle or subclinical telangiectatic erythema may be improved by combined vascular-targeted laser therapy together with fractional low-powered diode laser therapy. “A parallel improvement in telangiectatic erythema suggests a relationship between the underlying vasculature and hyperpigmentation,” said Dr. Ortiz, who was not affiliated with the study. “So, patients who have a vascular component to their melasma actually can get improved efficacy.”
Another strategy for melasma patients involves oral treatment with Polypodium leucotomos extract (PLE), a fern from the Polypodiaceae family with antioxidant properties that has been shown to be photoprotective against UVA and UVB radiation. “I like to think of it as an internal sunscreen,” Dr. Ortiz said. “It does not replace your external sunscreen, but it adds extra protection. It has been shown to significantly reduce the severity of sunburn and decrease the risk of UV radiation–induced skin cancer, as well as prevent skin aging.” The purported mechanism of action includes decreasing UV-mediated oxidative damage to DNA, enhancing the activity of endogenous antioxidant systems, increasing the minimal erythema dose, blocking UV radiation–induced cyclooxygenase-2 expression, reducing UV-induced immune suppression, and promoting p53 suppressor gene expression.
In a pilot placebo-controlled study of melasma patients on their normal regimen of hydroquinone and sunscreen, 40 Asian patients with melasma were randomized to receive either oral PLE supplementation or placebo for 12 weeks (J Clin Aesthet Dermatol 2018 Mar;11[3]:14-9). They found that PLE significantly improved and accelerated the outcome reached with hydroquinone and sunscreen from the first month of treatment, compared with placebo.
Dr. Ortiz next discussed the role of oral tranexamic acid, an antifibrinolytic, procoagulant agent that is approved by the Food and Drug Administration for the treatment of menorrhagia and for prevention of hemorrhage in patients with hemophilia undergoing tooth extractions. “It is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule, and it’s a game changer for melasma treatment,” she said. “One of the side effects is that it inhibits melanogenesis and neovascularization. It’s been effective for melasma, but its use is limited by the risk for thromboembolism. It’s a slight increased risk, something patients should be aware of, but not something that should scare us away from prescribing it.”
In a study of 561 patients with melasma, 90% improved after a median treatment duration of 4 months, and only 7% had side effects (J Am Acad Dermatol 2016;75:385-92). The most common side effects were abdominal bloating and pain. One patient developed a DVT during treatment, but that person was found to have a protein S deficiency.
The daily dosing of tranexamic acid for menorrhagia is 3,900 mg daily, while the dose for melasma has ranged from 500 mg-1,500 mg per day, Dr. Ortiz said. It’s available as a 650-mg pill in the United States. “I prescribe 325 mg twice a day, but studies have shown that 650 mg once a day is just as effective,” she said.
Prior to prescribing tranexamic acid, Dr. Ortiz does not order labs, but she performs an extensive history of present illness. She does not prescribe it in patients with an increased risk of clotting, including people who smoke and those who take oral contraceptives or are on hormone supplementation. Use is also contraindicated in people with a current malignancy, those with a history of stroke or DVT, and those who have any clotting disorder.
She concluded her presentation by noting that she favors a combination approach to treating melasma patients that starts with a broad spectrum sunscreen and PLE. “For bleaching, I like to use 12% hydroquinone with 6% kojic acid in VersaBase,” she said. “Once I get them in better control, then I switch them to 4% hydroquinone for maintenance. I use glycolic peels, low-energy lasers, and tranexamic acid if the melasma is severe, and they have no contraindications. A combination approach really achieves the best results, and counseling is key.”
Dr. Ortiz disclosed having financial relationships with numerous pharmaceutical and device companies. She is also cochair of MOA.
When establishing a treatment plan for patients with melasma, counseling them about realistic expectations is key.
“It’s important that they understand that this is a chronic condition, so it does require long-term maintenance therapy,” Arisa E. Ortiz, MD, said at the virtual annual Masters of Aesthetics Symposium. “We can improve melasma, but it’s difficult to cure melasma.”
While hydroquinone and other bleaching agents are typical treatment mainstays, chemical peels with glycolic acid, trichloroacetic acid, and salicylic acid can benefit some individuals. “For chemical peels, I really like glycolic acid peels because there is no downtime; it peels at the microscopic level,” said Dr. Ortiz, who is director of laser and cosmetic dermatology at the University of California, San Diego. “This is something they may need to repeat monthly, and having a week of peeling may be difficult to go through every month.”
Other common melasma treatments include lasers, intense pulsed light (IPL), and oral medications. “I personally am not impressed with microdermabrasion for melasma, so I don’t use that very much,” she said. “With laser treatment, you want to make sure you’re using low-energy lasers so that it doesn’t exacerbate or make them relapse or rebound.”
While hydroquinone is a mainstay of therapy, “you can’t use it chronically because of the risk of ochronosis (permanent darkening), so you do need to take drug holidays,” Dr. Ortiz said. “During those drug holidays, you want to make sure patients have a nonhydroquinone bleaching agent so that they don’t flare.” Options include lignin peroxidase, oligopeptide, Lytera, Melaplex, 4-n-butylresorcinol, Cysteamine cream, tranexamic acid, and oral antioxidants.
In a study sponsored by SkinMedica, investigators conducted a randomized, double-blind, half-face study in females with moderate to severe facial hyperpigmentation to assess the efficacy and tolerability of three new skin brightener formulations containing SMA-432, a prostaglandin E2 inhibitor, compared with topical 4% hydroquinone (J Drugs Dermatol 2012 Dec;11[12]:1478-82). They found that the nonhydroquinone skin formulations were better tolerated and were just as effective as 4% hydroquinone.
In a separate unpublished study of 22 females, investigators assessed the efficacy of the U.SK Advanced Defense Booster, which contains ferulic acid, maslinic acid, peptides, and olive leaf extract. They observed that 98% of patients saw improvement after 28 days of treatment.
When it comes to using lasers for melasma treatment, low-energy devices provide the best outcomes. “I prefer using something like the 1927-nm fractional diode lasers at 3.75% density, really low densities because there’s less risk for rebound,” Dr. Ortiz said. “They also enhance skin permeability for the use of topicals.”
In an observational study of 27 female patients with refractory melasma, Arielle Kauvar, MD, director of New York Laser & Skin Care, combined microdermabrasion with the Q-switched Nd:YAG (Lasers in Surgery and Medicine 2012; 44:117-24). “The settings she used were very low fluence, so there was no clinical endpoint or no whitening,” Dr. Ortiz said. Specifically, she used a laser at 1.6-2 J/cm2 with a 5- or 6-mm spot size immediately following microdermabrasion for 4 weeks. “She got a good improvement using a skin care regimen of sunscreen, hydroquinone, and tretinoin or vitamin C,” she said. “Remission lasted at least 6 months.”
In a study presented at the 2019 annual meeting of the America Society for Laser Medicine and Surgery, Dr. Ortiz and Tanya Greywal, MD, of the University of California, San Diego, used three passes of the 10764-nm Nd:YAG laser to treat 10 subjects with melasma skin types 2-5. The device has a 650-microsecond pulse duration, a 6-mm spot size, and an energy mode of 11-14 J/cm3. “There was no downtime with these patients, and they saw a mean improvement of 26%-50% as early as 3 weeks,” she said. “Patients did require multiple treatments to see adequate resolution, but no anesthesia or numbing cream was required. This is a good option for patients who need chronic maintenance treatment.”
Topicals also play a key role following the laser treatment of melasma. Dr. Ortiz characterized clobetasol as “kind of like the magic ointment.” She uses one application immediately post procedure “whenever I’m worried about a patient having postinflammatory hyperpigmentation or if I don’t want melasma patients to rebound. It can help reduce swelling and inflammation to decrease the risk of postinflammatory hyperpigmentation.”
Researchers have discovered that there is a vascular component to melasma. Paul M. Friedman, MD, of the Dermatology and Laser Surgery Center, Houston, and his colleagues used spectrocolorimetry to detect an underlying prominent vascular component in 11 patients with melasma (Lasers Surg Med 2017 Jan;49[1]:20-6). They determined that melasma lesions exhibiting subtle or subclinical telangiectatic erythema may be improved by combined vascular-targeted laser therapy together with fractional low-powered diode laser therapy. “A parallel improvement in telangiectatic erythema suggests a relationship between the underlying vasculature and hyperpigmentation,” said Dr. Ortiz, who was not affiliated with the study. “So, patients who have a vascular component to their melasma actually can get improved efficacy.”
Another strategy for melasma patients involves oral treatment with Polypodium leucotomos extract (PLE), a fern from the Polypodiaceae family with antioxidant properties that has been shown to be photoprotective against UVA and UVB radiation. “I like to think of it as an internal sunscreen,” Dr. Ortiz said. “It does not replace your external sunscreen, but it adds extra protection. It has been shown to significantly reduce the severity of sunburn and decrease the risk of UV radiation–induced skin cancer, as well as prevent skin aging.” The purported mechanism of action includes decreasing UV-mediated oxidative damage to DNA, enhancing the activity of endogenous antioxidant systems, increasing the minimal erythema dose, blocking UV radiation–induced cyclooxygenase-2 expression, reducing UV-induced immune suppression, and promoting p53 suppressor gene expression.
In a pilot placebo-controlled study of melasma patients on their normal regimen of hydroquinone and sunscreen, 40 Asian patients with melasma were randomized to receive either oral PLE supplementation or placebo for 12 weeks (J Clin Aesthet Dermatol 2018 Mar;11[3]:14-9). They found that PLE significantly improved and accelerated the outcome reached with hydroquinone and sunscreen from the first month of treatment, compared with placebo.
Dr. Ortiz next discussed the role of oral tranexamic acid, an antifibrinolytic, procoagulant agent that is approved by the Food and Drug Administration for the treatment of menorrhagia and for prevention of hemorrhage in patients with hemophilia undergoing tooth extractions. “It is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule, and it’s a game changer for melasma treatment,” she said. “One of the side effects is that it inhibits melanogenesis and neovascularization. It’s been effective for melasma, but its use is limited by the risk for thromboembolism. It’s a slight increased risk, something patients should be aware of, but not something that should scare us away from prescribing it.”
In a study of 561 patients with melasma, 90% improved after a median treatment duration of 4 months, and only 7% had side effects (J Am Acad Dermatol 2016;75:385-92). The most common side effects were abdominal bloating and pain. One patient developed a DVT during treatment, but that person was found to have a protein S deficiency.
The daily dosing of tranexamic acid for menorrhagia is 3,900 mg daily, while the dose for melasma has ranged from 500 mg-1,500 mg per day, Dr. Ortiz said. It’s available as a 650-mg pill in the United States. “I prescribe 325 mg twice a day, but studies have shown that 650 mg once a day is just as effective,” she said.
Prior to prescribing tranexamic acid, Dr. Ortiz does not order labs, but she performs an extensive history of present illness. She does not prescribe it in patients with an increased risk of clotting, including people who smoke and those who take oral contraceptives or are on hormone supplementation. Use is also contraindicated in people with a current malignancy, those with a history of stroke or DVT, and those who have any clotting disorder.
She concluded her presentation by noting that she favors a combination approach to treating melasma patients that starts with a broad spectrum sunscreen and PLE. “For bleaching, I like to use 12% hydroquinone with 6% kojic acid in VersaBase,” she said. “Once I get them in better control, then I switch them to 4% hydroquinone for maintenance. I use glycolic peels, low-energy lasers, and tranexamic acid if the melasma is severe, and they have no contraindications. A combination approach really achieves the best results, and counseling is key.”
Dr. Ortiz disclosed having financial relationships with numerous pharmaceutical and device companies. She is also cochair of MOA.
When establishing a treatment plan for patients with melasma, counseling them about realistic expectations is key.
“It’s important that they understand that this is a chronic condition, so it does require long-term maintenance therapy,” Arisa E. Ortiz, MD, said at the virtual annual Masters of Aesthetics Symposium. “We can improve melasma, but it’s difficult to cure melasma.”
While hydroquinone and other bleaching agents are typical treatment mainstays, chemical peels with glycolic acid, trichloroacetic acid, and salicylic acid can benefit some individuals. “For chemical peels, I really like glycolic acid peels because there is no downtime; it peels at the microscopic level,” said Dr. Ortiz, who is director of laser and cosmetic dermatology at the University of California, San Diego. “This is something they may need to repeat monthly, and having a week of peeling may be difficult to go through every month.”
Other common melasma treatments include lasers, intense pulsed light (IPL), and oral medications. “I personally am not impressed with microdermabrasion for melasma, so I don’t use that very much,” she said. “With laser treatment, you want to make sure you’re using low-energy lasers so that it doesn’t exacerbate or make them relapse or rebound.”
While hydroquinone is a mainstay of therapy, “you can’t use it chronically because of the risk of ochronosis (permanent darkening), so you do need to take drug holidays,” Dr. Ortiz said. “During those drug holidays, you want to make sure patients have a nonhydroquinone bleaching agent so that they don’t flare.” Options include lignin peroxidase, oligopeptide, Lytera, Melaplex, 4-n-butylresorcinol, Cysteamine cream, tranexamic acid, and oral antioxidants.
In a study sponsored by SkinMedica, investigators conducted a randomized, double-blind, half-face study in females with moderate to severe facial hyperpigmentation to assess the efficacy and tolerability of three new skin brightener formulations containing SMA-432, a prostaglandin E2 inhibitor, compared with topical 4% hydroquinone (J Drugs Dermatol 2012 Dec;11[12]:1478-82). They found that the nonhydroquinone skin formulations were better tolerated and were just as effective as 4% hydroquinone.
In a separate unpublished study of 22 females, investigators assessed the efficacy of the U.SK Advanced Defense Booster, which contains ferulic acid, maslinic acid, peptides, and olive leaf extract. They observed that 98% of patients saw improvement after 28 days of treatment.
When it comes to using lasers for melasma treatment, low-energy devices provide the best outcomes. “I prefer using something like the 1927-nm fractional diode lasers at 3.75% density, really low densities because there’s less risk for rebound,” Dr. Ortiz said. “They also enhance skin permeability for the use of topicals.”
In an observational study of 27 female patients with refractory melasma, Arielle Kauvar, MD, director of New York Laser & Skin Care, combined microdermabrasion with the Q-switched Nd:YAG (Lasers in Surgery and Medicine 2012; 44:117-24). “The settings she used were very low fluence, so there was no clinical endpoint or no whitening,” Dr. Ortiz said. Specifically, she used a laser at 1.6-2 J/cm2 with a 5- or 6-mm spot size immediately following microdermabrasion for 4 weeks. “She got a good improvement using a skin care regimen of sunscreen, hydroquinone, and tretinoin or vitamin C,” she said. “Remission lasted at least 6 months.”
In a study presented at the 2019 annual meeting of the America Society for Laser Medicine and Surgery, Dr. Ortiz and Tanya Greywal, MD, of the University of California, San Diego, used three passes of the 10764-nm Nd:YAG laser to treat 10 subjects with melasma skin types 2-5. The device has a 650-microsecond pulse duration, a 6-mm spot size, and an energy mode of 11-14 J/cm3. “There was no downtime with these patients, and they saw a mean improvement of 26%-50% as early as 3 weeks,” she said. “Patients did require multiple treatments to see adequate resolution, but no anesthesia or numbing cream was required. This is a good option for patients who need chronic maintenance treatment.”
Topicals also play a key role following the laser treatment of melasma. Dr. Ortiz characterized clobetasol as “kind of like the magic ointment.” She uses one application immediately post procedure “whenever I’m worried about a patient having postinflammatory hyperpigmentation or if I don’t want melasma patients to rebound. It can help reduce swelling and inflammation to decrease the risk of postinflammatory hyperpigmentation.”
Researchers have discovered that there is a vascular component to melasma. Paul M. Friedman, MD, of the Dermatology and Laser Surgery Center, Houston, and his colleagues used spectrocolorimetry to detect an underlying prominent vascular component in 11 patients with melasma (Lasers Surg Med 2017 Jan;49[1]:20-6). They determined that melasma lesions exhibiting subtle or subclinical telangiectatic erythema may be improved by combined vascular-targeted laser therapy together with fractional low-powered diode laser therapy. “A parallel improvement in telangiectatic erythema suggests a relationship between the underlying vasculature and hyperpigmentation,” said Dr. Ortiz, who was not affiliated with the study. “So, patients who have a vascular component to their melasma actually can get improved efficacy.”
Another strategy for melasma patients involves oral treatment with Polypodium leucotomos extract (PLE), a fern from the Polypodiaceae family with antioxidant properties that has been shown to be photoprotective against UVA and UVB radiation. “I like to think of it as an internal sunscreen,” Dr. Ortiz said. “It does not replace your external sunscreen, but it adds extra protection. It has been shown to significantly reduce the severity of sunburn and decrease the risk of UV radiation–induced skin cancer, as well as prevent skin aging.” The purported mechanism of action includes decreasing UV-mediated oxidative damage to DNA, enhancing the activity of endogenous antioxidant systems, increasing the minimal erythema dose, blocking UV radiation–induced cyclooxygenase-2 expression, reducing UV-induced immune suppression, and promoting p53 suppressor gene expression.
In a pilot placebo-controlled study of melasma patients on their normal regimen of hydroquinone and sunscreen, 40 Asian patients with melasma were randomized to receive either oral PLE supplementation or placebo for 12 weeks (J Clin Aesthet Dermatol 2018 Mar;11[3]:14-9). They found that PLE significantly improved and accelerated the outcome reached with hydroquinone and sunscreen from the first month of treatment, compared with placebo.
Dr. Ortiz next discussed the role of oral tranexamic acid, an antifibrinolytic, procoagulant agent that is approved by the Food and Drug Administration for the treatment of menorrhagia and for prevention of hemorrhage in patients with hemophilia undergoing tooth extractions. “It is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule, and it’s a game changer for melasma treatment,” she said. “One of the side effects is that it inhibits melanogenesis and neovascularization. It’s been effective for melasma, but its use is limited by the risk for thromboembolism. It’s a slight increased risk, something patients should be aware of, but not something that should scare us away from prescribing it.”
In a study of 561 patients with melasma, 90% improved after a median treatment duration of 4 months, and only 7% had side effects (J Am Acad Dermatol 2016;75:385-92). The most common side effects were abdominal bloating and pain. One patient developed a DVT during treatment, but that person was found to have a protein S deficiency.
The daily dosing of tranexamic acid for menorrhagia is 3,900 mg daily, while the dose for melasma has ranged from 500 mg-1,500 mg per day, Dr. Ortiz said. It’s available as a 650-mg pill in the United States. “I prescribe 325 mg twice a day, but studies have shown that 650 mg once a day is just as effective,” she said.
Prior to prescribing tranexamic acid, Dr. Ortiz does not order labs, but she performs an extensive history of present illness. She does not prescribe it in patients with an increased risk of clotting, including people who smoke and those who take oral contraceptives or are on hormone supplementation. Use is also contraindicated in people with a current malignancy, those with a history of stroke or DVT, and those who have any clotting disorder.
She concluded her presentation by noting that she favors a combination approach to treating melasma patients that starts with a broad spectrum sunscreen and PLE. “For bleaching, I like to use 12% hydroquinone with 6% kojic acid in VersaBase,” she said. “Once I get them in better control, then I switch them to 4% hydroquinone for maintenance. I use glycolic peels, low-energy lasers, and tranexamic acid if the melasma is severe, and they have no contraindications. A combination approach really achieves the best results, and counseling is key.”
Dr. Ortiz disclosed having financial relationships with numerous pharmaceutical and device companies. She is also cochair of MOA.
EXPERT ANALYSIS FROM MOA 2020
Tools emerging to predict liver failure in cirrhosis
Systemic inflammation and portal hypertension are key predictors of acute-on-chronic liver failure (ACLF) in the 3 months after a hospital stay for acute decompensated cirrhosis and also of death after 12 months, a preliminary analysis of data from the PREDICT study shows.
“Before this, we never had any patient signatures to identify ACLF,” said Jonel Trebicka, MD, PhD, from the JW Goethe University Hospital in Frankfurt, Germany.
Now, Dr. Trebicka’s team has “characterized the phenotypes in pre-ACLF that will progress within 3 months,” he said in an interview. “Those with high levels of inflammatory proteins, white blood cell count, are more likely to develop ACLF.”
ACLF is a highly complex disorder that can lead liver, cardiovascular, renal, cerebral, pulmonary, intestinal, adrenal, and immune systems to fail, Dr. Trebicka explained when he discussed the analysis – published online in the Journal of Hepatology – during the virtual International Liver Congress (ILC) 2020.
The chance of survival after the onset of ACLF is low – the 28-day survival rate is 30% – and “the only treatment we have is liver transplant,” he said.
For their prospective observational study, Dr. Trebicka and his colleagues assessed 1071 participants from 48 European hospitals in 14 countries who were admitted for an episode of acute decompensation, defined as the development of ascites, hepatic encephalopathy, gastrointestinal hemorrhage, infection, or a combination thereof.
The researchers identified three distinct clinical courses for a patient hospitalized with acute decompensated cirrhosis that will help clinicians predict the development of ACLF.
At study enrollment, more than half of the patients at highest risk for ACLF had pre-ACLF and high-grade systemic inflammation. The patients at intermediate risk had unstable decompensated cirrhosis with low-grade systemic inflammation and complications related to severe portal hypertension. And those at lowest risk for ACLF had stable decompensated cirrhosis and no severe systemic inflammation or portal hypertension complications, and did not develop ACLF or another episode of acute decompensation in the subsequent 3 months.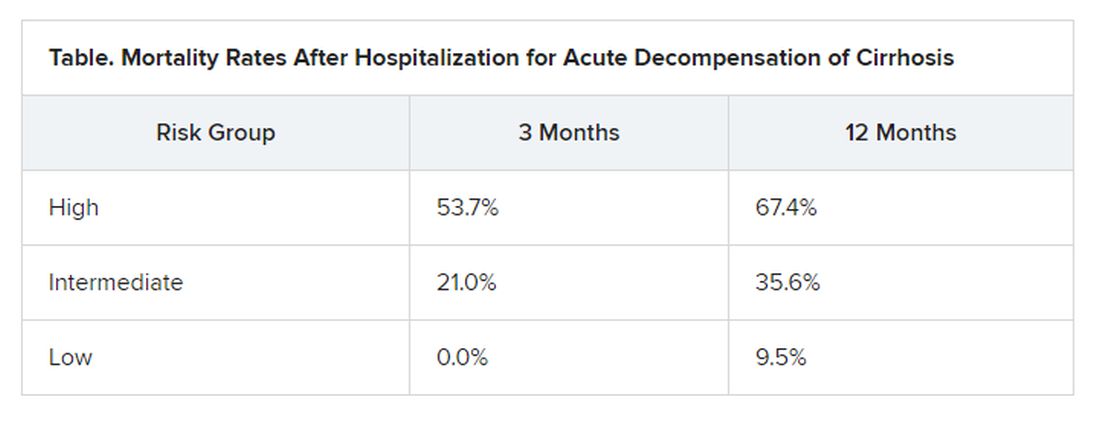
“There have been hints of possible phenotypes before – for stable and unstable ACLF – but we never had anything specific to diagnose,” Trebicka reported.
“We found that there are two main mechanisms in the development of ACLF that are most important,” he said. The first is systemic inflammation with high levels of proteins, which “leads to organ failure. This is the most striking acute mechanism.”
The second is the development of portal hypertension. “This is slower, but also very important, causing increased pressure in the portal vein, and leading to bleeding if the pressure is too great,” he said.
More tools emerging to help predict ACLF
The Albumin-functionality-test (AFT), which uses serum albumin levels to evaluate liver and kidney function, might also be useful in the prediction of ACLF and 12-month survival, according to a separate study an Italian group presented at the virtual ILC.
“Our main results are that parameters from albumin predict the development of ACLF in acute decompensated patients with the same diagnostic performance as the CLIF-AD score,” said Katja Waterstradt, PhD, from the University of Bologna in Italy.
And when the two tests are combined, diagnostic performance is increased, she added.
Dr. Trebicka has disclosed no relevant financial relationships. Dr. Waterstrand is a researcher for MedInnovation GmbH.
This article first appeared on Medscape.com.
Systemic inflammation and portal hypertension are key predictors of acute-on-chronic liver failure (ACLF) in the 3 months after a hospital stay for acute decompensated cirrhosis and also of death after 12 months, a preliminary analysis of data from the PREDICT study shows.
“Before this, we never had any patient signatures to identify ACLF,” said Jonel Trebicka, MD, PhD, from the JW Goethe University Hospital in Frankfurt, Germany.
Now, Dr. Trebicka’s team has “characterized the phenotypes in pre-ACLF that will progress within 3 months,” he said in an interview. “Those with high levels of inflammatory proteins, white blood cell count, are more likely to develop ACLF.”
ACLF is a highly complex disorder that can lead liver, cardiovascular, renal, cerebral, pulmonary, intestinal, adrenal, and immune systems to fail, Dr. Trebicka explained when he discussed the analysis – published online in the Journal of Hepatology – during the virtual International Liver Congress (ILC) 2020.
The chance of survival after the onset of ACLF is low – the 28-day survival rate is 30% – and “the only treatment we have is liver transplant,” he said.
For their prospective observational study, Dr. Trebicka and his colleagues assessed 1071 participants from 48 European hospitals in 14 countries who were admitted for an episode of acute decompensation, defined as the development of ascites, hepatic encephalopathy, gastrointestinal hemorrhage, infection, or a combination thereof.
The researchers identified three distinct clinical courses for a patient hospitalized with acute decompensated cirrhosis that will help clinicians predict the development of ACLF.
At study enrollment, more than half of the patients at highest risk for ACLF had pre-ACLF and high-grade systemic inflammation. The patients at intermediate risk had unstable decompensated cirrhosis with low-grade systemic inflammation and complications related to severe portal hypertension. And those at lowest risk for ACLF had stable decompensated cirrhosis and no severe systemic inflammation or portal hypertension complications, and did not develop ACLF or another episode of acute decompensation in the subsequent 3 months.
“There have been hints of possible phenotypes before – for stable and unstable ACLF – but we never had anything specific to diagnose,” Trebicka reported.
“We found that there are two main mechanisms in the development of ACLF that are most important,” he said. The first is systemic inflammation with high levels of proteins, which “leads to organ failure. This is the most striking acute mechanism.”
The second is the development of portal hypertension. “This is slower, but also very important, causing increased pressure in the portal vein, and leading to bleeding if the pressure is too great,” he said.
More tools emerging to help predict ACLF
The Albumin-functionality-test (AFT), which uses serum albumin levels to evaluate liver and kidney function, might also be useful in the prediction of ACLF and 12-month survival, according to a separate study an Italian group presented at the virtual ILC.
“Our main results are that parameters from albumin predict the development of ACLF in acute decompensated patients with the same diagnostic performance as the CLIF-AD score,” said Katja Waterstradt, PhD, from the University of Bologna in Italy.
And when the two tests are combined, diagnostic performance is increased, she added.
Dr. Trebicka has disclosed no relevant financial relationships. Dr. Waterstrand is a researcher for MedInnovation GmbH.
This article first appeared on Medscape.com.
Systemic inflammation and portal hypertension are key predictors of acute-on-chronic liver failure (ACLF) in the 3 months after a hospital stay for acute decompensated cirrhosis and also of death after 12 months, a preliminary analysis of data from the PREDICT study shows.
“Before this, we never had any patient signatures to identify ACLF,” said Jonel Trebicka, MD, PhD, from the JW Goethe University Hospital in Frankfurt, Germany.
Now, Dr. Trebicka’s team has “characterized the phenotypes in pre-ACLF that will progress within 3 months,” he said in an interview. “Those with high levels of inflammatory proteins, white blood cell count, are more likely to develop ACLF.”
ACLF is a highly complex disorder that can lead liver, cardiovascular, renal, cerebral, pulmonary, intestinal, adrenal, and immune systems to fail, Dr. Trebicka explained when he discussed the analysis – published online in the Journal of Hepatology – during the virtual International Liver Congress (ILC) 2020.
The chance of survival after the onset of ACLF is low – the 28-day survival rate is 30% – and “the only treatment we have is liver transplant,” he said.
For their prospective observational study, Dr. Trebicka and his colleagues assessed 1071 participants from 48 European hospitals in 14 countries who were admitted for an episode of acute decompensation, defined as the development of ascites, hepatic encephalopathy, gastrointestinal hemorrhage, infection, or a combination thereof.
The researchers identified three distinct clinical courses for a patient hospitalized with acute decompensated cirrhosis that will help clinicians predict the development of ACLF.
At study enrollment, more than half of the patients at highest risk for ACLF had pre-ACLF and high-grade systemic inflammation. The patients at intermediate risk had unstable decompensated cirrhosis with low-grade systemic inflammation and complications related to severe portal hypertension. And those at lowest risk for ACLF had stable decompensated cirrhosis and no severe systemic inflammation or portal hypertension complications, and did not develop ACLF or another episode of acute decompensation in the subsequent 3 months.
“There have been hints of possible phenotypes before – for stable and unstable ACLF – but we never had anything specific to diagnose,” Trebicka reported.
“We found that there are two main mechanisms in the development of ACLF that are most important,” he said. The first is systemic inflammation with high levels of proteins, which “leads to organ failure. This is the most striking acute mechanism.”
The second is the development of portal hypertension. “This is slower, but also very important, causing increased pressure in the portal vein, and leading to bleeding if the pressure is too great,” he said.
More tools emerging to help predict ACLF
The Albumin-functionality-test (AFT), which uses serum albumin levels to evaluate liver and kidney function, might also be useful in the prediction of ACLF and 12-month survival, according to a separate study an Italian group presented at the virtual ILC.
“Our main results are that parameters from albumin predict the development of ACLF in acute decompensated patients with the same diagnostic performance as the CLIF-AD score,” said Katja Waterstradt, PhD, from the University of Bologna in Italy.
And when the two tests are combined, diagnostic performance is increased, she added.
Dr. Trebicka has disclosed no relevant financial relationships. Dr. Waterstrand is a researcher for MedInnovation GmbH.
This article first appeared on Medscape.com.
Novel smart needle system designed to reduce risk of filler complications
In the very near future, clinicians injecting

That is the goal of an experienced team composed of leading clinicians, academics, and researchers developing S3 Inject, a first-in-class safety innovation that has entered human trials.
“When physicians inject the fillers, they hope experience and technique will enable them to avoid adverse events,” Irina Erenburg, PhD, said during the virtual annual Masters of Aesthetics Symposium. “If they inadvertently hit a blood vessel, the filler can actually occlude that vessel and cause either an infarct of the skin or, in certain serious cases, blindness. This is a challenging adverse event that every injector is focused on avoiding. While hyaluronidase is used as a rescue [medication] in certain cases, the risk is real,” she added.
Vision abnormalities, including blindness, and necrosis are among the adverse events associated with dermal fillers that have been reported to the Food and Drug Administration.
S3 Inject is a sensing needle that can differentiate tissues such as fat, blood vessels, and muscle. Its proprietary algorithms provide immediate feedback via a micro LED light embedded in the needle hub. Results from recent human trials demonstrate that, as the needle tip passes through different biological tissues and fluids, “it senses changes in specific electrical properties and with that information sends a very precise signal to the needle hub,” said Dr. Erenburg, CEO and President of Waltham, Mass.–based Blossom Innovations, a company focused on developing early stage medical devices in dermatology. “With that information, the physician can make real-time treatment decisions.”
Currently, in order to determine if the needle is in a blood vessel, physicians pull back on the syringe and look for a flash of blood. “In speaking with physicians, the pull back technique has limitations, in part, because filler in the syringe can limit easy pull back to check the presence of a blood vessel,” she said. “Our needles provide an immediate response for a safer injection.”
Blossom Innovations has developed a proprietary manufacturing process that will initially target 27 gauge needles, but over time it plans to introduce multiple sizes, as well as cannulas.
“The physicians in our industry are committed to patient safety and they’re looking for better outcomes with a solution that does not impact their technique,” said Dr. Erenburg, who founded Blossom Innovations along with R. Rox Anderson, MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston; Dieter Manstein, MD, PhD, also at Massachusetts General Hospital; and Henry H.L. Chan, MD, PhD, of the Hong Kong Dermatology and Laser Center. During market research for S3 Inject, which was conducted with 15 leading injectors, thought leaders, and trend makers, the country’s leading injectors expressed strong interest in “solutions that allow them to provide additional safety for their patients and provide personal reassurance to the physician,” she said. “They definitely would want to train all their physicians and injectors on its use.”
As clinical testing continues, the company is preparing to submit data to the FDA’s Premarket Notification program, known as the 510(k) process. “Our intent is to create a scale-up manufacturing over the course of the coming year in time for our clearance, with a planned launch at the end of 2021,” Dr. Erenburg said. “Based on our clinical research and physician discussions, we are confident that S3 Inject is a breakthrough safety technology which will drive a better outcome for patients.”
Dr. Erenburg is an employee of Blossom Innovations.
dbrunk@mdedge.com
In the very near future, clinicians injecting
That is the goal of an experienced team composed of leading clinicians, academics, and researchers developing S3 Inject, a first-in-class safety innovation that has entered human trials.
“When physicians inject the fillers, they hope experience and technique will enable them to avoid adverse events,” Irina Erenburg, PhD, said during the virtual annual Masters of Aesthetics Symposium. “If they inadvertently hit a blood vessel, the filler can actually occlude that vessel and cause either an infarct of the skin or, in certain serious cases, blindness. This is a challenging adverse event that every injector is focused on avoiding. While hyaluronidase is used as a rescue [medication] in certain cases, the risk is real,” she added.
Vision abnormalities, including blindness, and necrosis are among the adverse events associated with dermal fillers that have been reported to the Food and Drug Administration.
S3 Inject is a sensing needle that can differentiate tissues such as fat, blood vessels, and muscle. Its proprietary algorithms provide immediate feedback via a micro LED light embedded in the needle hub. Results from recent human trials demonstrate that, as the needle tip passes through different biological tissues and fluids, “it senses changes in specific electrical properties and with that information sends a very precise signal to the needle hub,” said Dr. Erenburg, CEO and President of Waltham, Mass.–based Blossom Innovations, a company focused on developing early stage medical devices in dermatology. “With that information, the physician can make real-time treatment decisions.”
Currently, in order to determine if the needle is in a blood vessel, physicians pull back on the syringe and look for a flash of blood. “In speaking with physicians, the pull back technique has limitations, in part, because filler in the syringe can limit easy pull back to check the presence of a blood vessel,” she said. “Our needles provide an immediate response for a safer injection.”
Blossom Innovations has developed a proprietary manufacturing process that will initially target 27 gauge needles, but over time it plans to introduce multiple sizes, as well as cannulas.
“The physicians in our industry are committed to patient safety and they’re looking for better outcomes with a solution that does not impact their technique,” said Dr. Erenburg, who founded Blossom Innovations along with R. Rox Anderson, MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston; Dieter Manstein, MD, PhD, also at Massachusetts General Hospital; and Henry H.L. Chan, MD, PhD, of the Hong Kong Dermatology and Laser Center. During market research for S3 Inject, which was conducted with 15 leading injectors, thought leaders, and trend makers, the country’s leading injectors expressed strong interest in “solutions that allow them to provide additional safety for their patients and provide personal reassurance to the physician,” she said. “They definitely would want to train all their physicians and injectors on its use.”
As clinical testing continues, the company is preparing to submit data to the FDA’s Premarket Notification program, known as the 510(k) process. “Our intent is to create a scale-up manufacturing over the course of the coming year in time for our clearance, with a planned launch at the end of 2021,” Dr. Erenburg said. “Based on our clinical research and physician discussions, we are confident that S3 Inject is a breakthrough safety technology which will drive a better outcome for patients.”
Dr. Erenburg is an employee of Blossom Innovations.
dbrunk@mdedge.com
In the very near future, clinicians injecting
That is the goal of an experienced team composed of leading clinicians, academics, and researchers developing S3 Inject, a first-in-class safety innovation that has entered human trials.
“When physicians inject the fillers, they hope experience and technique will enable them to avoid adverse events,” Irina Erenburg, PhD, said during the virtual annual Masters of Aesthetics Symposium. “If they inadvertently hit a blood vessel, the filler can actually occlude that vessel and cause either an infarct of the skin or, in certain serious cases, blindness. This is a challenging adverse event that every injector is focused on avoiding. While hyaluronidase is used as a rescue [medication] in certain cases, the risk is real,” she added.
Vision abnormalities, including blindness, and necrosis are among the adverse events associated with dermal fillers that have been reported to the Food and Drug Administration.
S3 Inject is a sensing needle that can differentiate tissues such as fat, blood vessels, and muscle. Its proprietary algorithms provide immediate feedback via a micro LED light embedded in the needle hub. Results from recent human trials demonstrate that, as the needle tip passes through different biological tissues and fluids, “it senses changes in specific electrical properties and with that information sends a very precise signal to the needle hub,” said Dr. Erenburg, CEO and President of Waltham, Mass.–based Blossom Innovations, a company focused on developing early stage medical devices in dermatology. “With that information, the physician can make real-time treatment decisions.”
Currently, in order to determine if the needle is in a blood vessel, physicians pull back on the syringe and look for a flash of blood. “In speaking with physicians, the pull back technique has limitations, in part, because filler in the syringe can limit easy pull back to check the presence of a blood vessel,” she said. “Our needles provide an immediate response for a safer injection.”
Blossom Innovations has developed a proprietary manufacturing process that will initially target 27 gauge needles, but over time it plans to introduce multiple sizes, as well as cannulas.
“The physicians in our industry are committed to patient safety and they’re looking for better outcomes with a solution that does not impact their technique,” said Dr. Erenburg, who founded Blossom Innovations along with R. Rox Anderson, MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston; Dieter Manstein, MD, PhD, also at Massachusetts General Hospital; and Henry H.L. Chan, MD, PhD, of the Hong Kong Dermatology and Laser Center. During market research for S3 Inject, which was conducted with 15 leading injectors, thought leaders, and trend makers, the country’s leading injectors expressed strong interest in “solutions that allow them to provide additional safety for their patients and provide personal reassurance to the physician,” she said. “They definitely would want to train all their physicians and injectors on its use.”
As clinical testing continues, the company is preparing to submit data to the FDA’s Premarket Notification program, known as the 510(k) process. “Our intent is to create a scale-up manufacturing over the course of the coming year in time for our clearance, with a planned launch at the end of 2021,” Dr. Erenburg said. “Based on our clinical research and physician discussions, we are confident that S3 Inject is a breakthrough safety technology which will drive a better outcome for patients.”
Dr. Erenburg is an employee of Blossom Innovations.
dbrunk@mdedge.com
REPORTING FROM MOA 2020
‘No mobile phone’ phobia tied to sleep problems in college students
In a study of more than 300 college students, nearly 9 in 10 (89%) were classified as having moderate to severe nomophobia. Greater levels of nomophobia were significantly linked to daytime sleepiness and more behaviors associated with poor sleep hygiene.
“My undergraduate research team came up with the idea for this study,” said study investigator Jennifer Peszka, PhD, professor of psychology at Hendrix College, Conway, Ark. She explained that her students had been looking at the impact of technology use in the 2 hours before bed, and hypothesized that ‘cell phone addiction’ might play a role in sleep problems.
Incidentally, “that group of students were all pretty high on nomophobia themselves so they were really interested in the outcome,” Dr. Peszka said.
The study findings were presented at the virtual annual meeting of the Associated Professional Sleep Societies.
A likely suspect
The study involved 327 undergraduates (mean age, 19.7 years) recruited from introductory psychology courses and campus newsletters. They completed several questionnaires, including the Nomophobia Questionnaire, the Epworth Sleepiness Scale, and the Sleep Hygiene Index.
Nomophobia was prevalent, with mild, moderate, and severe nomophobia reported by 10%, 83%, and 7% of students, respectively. Only one student reported no nomophobia at all. Dr. Peszka said the fact that 89% of students had moderate or severe nomophobia is “concerning,” given a 2012 study suggesting that 77% of 18- to 24-year-olds had nomophobia. This phobia “very well may be on a rapid rise,” she lamented.
Greater severity of nomophobia was significantly correlated with greater sleepiness measured by both the Epworth Sleepiness Scale (P < .05) and the Associated Features of Poor Sleep Hygiene daytime sleepiness item (P < .05). More severe nomophobia was also related to decreased motivation (a commonly reported symptom of insufficient sleep) and with more maladaptive sleep hygiene behaviors (including using technology during sleep time, long daytime naps, inconsistent wake and bed times, using bed for nonsleep purposes, uncomfortable bed, and bedtime cognitive rumination).
Prior research has shown that smartphones may lead to compulsive “checking” habits, compulsive usage, increased distress, and potentially addictive behaviors. Active phone use at bedtime has also been implicated in disrupted sleep. Nomophobia is likely to be an important consideration when treating sleep disorders and/or making any sleep hygiene recommendations, Dr. Peszka said.
Proliferation of ‘night owls’
Reached for comment, Rajkumar (Raj) Dasgupta, MD, University of Southern California, Los Angeles, said this is a “very timely study with COVID-19. Right now, more than ever, technology is a double-edged sword. I’m a father of three kids and, for now, technology is the only way some kids are going to be socializing and learning.”
Yet a foundation of good sleep hygiene is keeping a nightly sleep routine, said Dr. Dasgupta, who was not involved in the study. “Right now, it seems like all my sleep patients are becoming night owls and sleep time is becoming more and more delayed because there is so much news to keep up with. Also, you may be stressed at night and you may not have the motivation to wake up early in the morning.”
He said it is important to counsel patients to “put technology away at night. That goes for kids and adults.”
Support for the study was provided by Hendrix College Charles Brewer Fund for Psychology. Dr. Peszka and Dr. Dasgupta disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In a study of more than 300 college students, nearly 9 in 10 (89%) were classified as having moderate to severe nomophobia. Greater levels of nomophobia were significantly linked to daytime sleepiness and more behaviors associated with poor sleep hygiene.
“My undergraduate research team came up with the idea for this study,” said study investigator Jennifer Peszka, PhD, professor of psychology at Hendrix College, Conway, Ark. She explained that her students had been looking at the impact of technology use in the 2 hours before bed, and hypothesized that ‘cell phone addiction’ might play a role in sleep problems.
Incidentally, “that group of students were all pretty high on nomophobia themselves so they were really interested in the outcome,” Dr. Peszka said.
The study findings were presented at the virtual annual meeting of the Associated Professional Sleep Societies.
A likely suspect
The study involved 327 undergraduates (mean age, 19.7 years) recruited from introductory psychology courses and campus newsletters. They completed several questionnaires, including the Nomophobia Questionnaire, the Epworth Sleepiness Scale, and the Sleep Hygiene Index.
Nomophobia was prevalent, with mild, moderate, and severe nomophobia reported by 10%, 83%, and 7% of students, respectively. Only one student reported no nomophobia at all. Dr. Peszka said the fact that 89% of students had moderate or severe nomophobia is “concerning,” given a 2012 study suggesting that 77% of 18- to 24-year-olds had nomophobia. This phobia “very well may be on a rapid rise,” she lamented.
Greater severity of nomophobia was significantly correlated with greater sleepiness measured by both the Epworth Sleepiness Scale (P < .05) and the Associated Features of Poor Sleep Hygiene daytime sleepiness item (P < .05). More severe nomophobia was also related to decreased motivation (a commonly reported symptom of insufficient sleep) and with more maladaptive sleep hygiene behaviors (including using technology during sleep time, long daytime naps, inconsistent wake and bed times, using bed for nonsleep purposes, uncomfortable bed, and bedtime cognitive rumination).
Prior research has shown that smartphones may lead to compulsive “checking” habits, compulsive usage, increased distress, and potentially addictive behaviors. Active phone use at bedtime has also been implicated in disrupted sleep. Nomophobia is likely to be an important consideration when treating sleep disorders and/or making any sleep hygiene recommendations, Dr. Peszka said.
Proliferation of ‘night owls’
Reached for comment, Rajkumar (Raj) Dasgupta, MD, University of Southern California, Los Angeles, said this is a “very timely study with COVID-19. Right now, more than ever, technology is a double-edged sword. I’m a father of three kids and, for now, technology is the only way some kids are going to be socializing and learning.”
Yet a foundation of good sleep hygiene is keeping a nightly sleep routine, said Dr. Dasgupta, who was not involved in the study. “Right now, it seems like all my sleep patients are becoming night owls and sleep time is becoming more and more delayed because there is so much news to keep up with. Also, you may be stressed at night and you may not have the motivation to wake up early in the morning.”
He said it is important to counsel patients to “put technology away at night. That goes for kids and adults.”
Support for the study was provided by Hendrix College Charles Brewer Fund for Psychology. Dr. Peszka and Dr. Dasgupta disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In a study of more than 300 college students, nearly 9 in 10 (89%) were classified as having moderate to severe nomophobia. Greater levels of nomophobia were significantly linked to daytime sleepiness and more behaviors associated with poor sleep hygiene.
“My undergraduate research team came up with the idea for this study,” said study investigator Jennifer Peszka, PhD, professor of psychology at Hendrix College, Conway, Ark. She explained that her students had been looking at the impact of technology use in the 2 hours before bed, and hypothesized that ‘cell phone addiction’ might play a role in sleep problems.
Incidentally, “that group of students were all pretty high on nomophobia themselves so they were really interested in the outcome,” Dr. Peszka said.
The study findings were presented at the virtual annual meeting of the Associated Professional Sleep Societies.
A likely suspect
The study involved 327 undergraduates (mean age, 19.7 years) recruited from introductory psychology courses and campus newsletters. They completed several questionnaires, including the Nomophobia Questionnaire, the Epworth Sleepiness Scale, and the Sleep Hygiene Index.
Nomophobia was prevalent, with mild, moderate, and severe nomophobia reported by 10%, 83%, and 7% of students, respectively. Only one student reported no nomophobia at all. Dr. Peszka said the fact that 89% of students had moderate or severe nomophobia is “concerning,” given a 2012 study suggesting that 77% of 18- to 24-year-olds had nomophobia. This phobia “very well may be on a rapid rise,” she lamented.
Greater severity of nomophobia was significantly correlated with greater sleepiness measured by both the Epworth Sleepiness Scale (P < .05) and the Associated Features of Poor Sleep Hygiene daytime sleepiness item (P < .05). More severe nomophobia was also related to decreased motivation (a commonly reported symptom of insufficient sleep) and with more maladaptive sleep hygiene behaviors (including using technology during sleep time, long daytime naps, inconsistent wake and bed times, using bed for nonsleep purposes, uncomfortable bed, and bedtime cognitive rumination).
Prior research has shown that smartphones may lead to compulsive “checking” habits, compulsive usage, increased distress, and potentially addictive behaviors. Active phone use at bedtime has also been implicated in disrupted sleep. Nomophobia is likely to be an important consideration when treating sleep disorders and/or making any sleep hygiene recommendations, Dr. Peszka said.
Proliferation of ‘night owls’
Reached for comment, Rajkumar (Raj) Dasgupta, MD, University of Southern California, Los Angeles, said this is a “very timely study with COVID-19. Right now, more than ever, technology is a double-edged sword. I’m a father of three kids and, for now, technology is the only way some kids are going to be socializing and learning.”
Yet a foundation of good sleep hygiene is keeping a nightly sleep routine, said Dr. Dasgupta, who was not involved in the study. “Right now, it seems like all my sleep patients are becoming night owls and sleep time is becoming more and more delayed because there is so much news to keep up with. Also, you may be stressed at night and you may not have the motivation to wake up early in the morning.”
He said it is important to counsel patients to “put technology away at night. That goes for kids and adults.”
Support for the study was provided by Hendrix College Charles Brewer Fund for Psychology. Dr. Peszka and Dr. Dasgupta disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SLEEP 2020
Experts advocate for the elimination of daylight savings time
In the interest of public health and safety, – a recommendation that has garnered strong support from multiple medical and other high-profile organizations.
“Permanent, year-round standard time is the best choice to most closely match our circadian sleep-wake cycle,” M. Adeel Rishi, MD, lead author of the AASM position statement, said in a news release. “Daylight saving time results in more darkness in the morning and more light in the evening, disrupting the body’s natural rhythm,” said Dr. Rishi, of the department of pulmonology, critical care, and sleep medicine, Mayo Clinic, Eau Claire, Wis., and vice chair of the AASM Public Safety Committee.
The position statement was published Aug. 26 in the Journal of Clinical Sleep Medicine to coincide with the virtual annual meeting of the Associated Professional Sleep Societies .
Significant health risks
In the United States, the annual “spring forward” to daylight saving time and “fall back” to standard time is required by law, although under the statute some exceptions are permitted.
There has been intense debate over the last several years about transitioning between standard and daylight saving time. The AASM says there is “an abundance of evidence” to indicate that quick transition from standard time to daylight saving time incurs significant public health and safety risks, including increased risk of heart attack, stroke, mood disorders, and car crashes.
“Although chronic effects of remaining in daylight saving time year-round have not been well-studied, daylight saving time is less aligned with human circadian biology – which, because of the impacts of the delayed natural light/dark cycle on human activity, could result in circadian misalignment, which has been associated in some studies with increased cardiovascular disease risk, metabolic syndrome and other health risks,” the authors wrote.
A recent study also showed an increase in medical errors in the week after switching to daylight saving time.
“Because the adoption of permanent standard time would be beneficial for public health and safety, the AASM will be advocating at the federal level for this legislative change,” said AASM President Kannan Ramar, MBBS, MD, with the Mayo Clinic in Rochester, Minn.
It seems that many Americans are in favor of the change. In July, an AASM survey of roughly 2,000 U.S. adults showed that two-thirds support doing away with the seasonal time change. Only 11% opposed it. In addition, the academy’s 2019 survey showed more than half of adults feel extremely, or somewhat, tired after the springing ahead to daylight saving time.
Strong support
The position statement has been endorsed by 19 organizations, including the American Academy of Cardiovascular Sleep Medicine, American College of Chest Physicians (CHEST), American College of Occupational and Environmental Medicine, National PTA, National Safety Council, Society of Anesthesia and Sleep Medicine, and the Society of Behavioral Sleep Medicine.
Weighing in on the issue, Saul Rothenberg, PhD, from the Sleep Center at Greenwich Hospital, Conn., said the literature on daylight saving time has grown over the past 20 years. He said he was ”humbled” by the research that shows that a “relatively small” misalignment of biological and social clocks has a measurable impact on human health and behavior.
“Because misalignment is associated with negative health and performance outcomes, keeping one set of hours year-round is promoted to minimize misalignment and associated consequences,” he added.
In light of this research, the recommendation to dispense with daylight saving time seems “quite reasonable” from a public health perspective. “I am left with a strengthened view on the importance of regular adequate sleep as a way to enhance health, performance, and quality of life,” he added.
This research had no commercial funding. Dr. Rishi and Dr. Rothenberg have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the interest of public health and safety, – a recommendation that has garnered strong support from multiple medical and other high-profile organizations.
“Permanent, year-round standard time is the best choice to most closely match our circadian sleep-wake cycle,” M. Adeel Rishi, MD, lead author of the AASM position statement, said in a news release. “Daylight saving time results in more darkness in the morning and more light in the evening, disrupting the body’s natural rhythm,” said Dr. Rishi, of the department of pulmonology, critical care, and sleep medicine, Mayo Clinic, Eau Claire, Wis., and vice chair of the AASM Public Safety Committee.
The position statement was published Aug. 26 in the Journal of Clinical Sleep Medicine to coincide with the virtual annual meeting of the Associated Professional Sleep Societies .
Significant health risks
In the United States, the annual “spring forward” to daylight saving time and “fall back” to standard time is required by law, although under the statute some exceptions are permitted.
There has been intense debate over the last several years about transitioning between standard and daylight saving time. The AASM says there is “an abundance of evidence” to indicate that quick transition from standard time to daylight saving time incurs significant public health and safety risks, including increased risk of heart attack, stroke, mood disorders, and car crashes.
“Although chronic effects of remaining in daylight saving time year-round have not been well-studied, daylight saving time is less aligned with human circadian biology – which, because of the impacts of the delayed natural light/dark cycle on human activity, could result in circadian misalignment, which has been associated in some studies with increased cardiovascular disease risk, metabolic syndrome and other health risks,” the authors wrote.
A recent study also showed an increase in medical errors in the week after switching to daylight saving time.
“Because the adoption of permanent standard time would be beneficial for public health and safety, the AASM will be advocating at the federal level for this legislative change,” said AASM President Kannan Ramar, MBBS, MD, with the Mayo Clinic in Rochester, Minn.
It seems that many Americans are in favor of the change. In July, an AASM survey of roughly 2,000 U.S. adults showed that two-thirds support doing away with the seasonal time change. Only 11% opposed it. In addition, the academy’s 2019 survey showed more than half of adults feel extremely, or somewhat, tired after the springing ahead to daylight saving time.
Strong support
The position statement has been endorsed by 19 organizations, including the American Academy of Cardiovascular Sleep Medicine, American College of Chest Physicians (CHEST), American College of Occupational and Environmental Medicine, National PTA, National Safety Council, Society of Anesthesia and Sleep Medicine, and the Society of Behavioral Sleep Medicine.
Weighing in on the issue, Saul Rothenberg, PhD, from the Sleep Center at Greenwich Hospital, Conn., said the literature on daylight saving time has grown over the past 20 years. He said he was ”humbled” by the research that shows that a “relatively small” misalignment of biological and social clocks has a measurable impact on human health and behavior.
“Because misalignment is associated with negative health and performance outcomes, keeping one set of hours year-round is promoted to minimize misalignment and associated consequences,” he added.
In light of this research, the recommendation to dispense with daylight saving time seems “quite reasonable” from a public health perspective. “I am left with a strengthened view on the importance of regular adequate sleep as a way to enhance health, performance, and quality of life,” he added.
This research had no commercial funding. Dr. Rishi and Dr. Rothenberg have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the interest of public health and safety, – a recommendation that has garnered strong support from multiple medical and other high-profile organizations.
“Permanent, year-round standard time is the best choice to most closely match our circadian sleep-wake cycle,” M. Adeel Rishi, MD, lead author of the AASM position statement, said in a news release. “Daylight saving time results in more darkness in the morning and more light in the evening, disrupting the body’s natural rhythm,” said Dr. Rishi, of the department of pulmonology, critical care, and sleep medicine, Mayo Clinic, Eau Claire, Wis., and vice chair of the AASM Public Safety Committee.
The position statement was published Aug. 26 in the Journal of Clinical Sleep Medicine to coincide with the virtual annual meeting of the Associated Professional Sleep Societies .
Significant health risks
In the United States, the annual “spring forward” to daylight saving time and “fall back” to standard time is required by law, although under the statute some exceptions are permitted.
There has been intense debate over the last several years about transitioning between standard and daylight saving time. The AASM says there is “an abundance of evidence” to indicate that quick transition from standard time to daylight saving time incurs significant public health and safety risks, including increased risk of heart attack, stroke, mood disorders, and car crashes.
“Although chronic effects of remaining in daylight saving time year-round have not been well-studied, daylight saving time is less aligned with human circadian biology – which, because of the impacts of the delayed natural light/dark cycle on human activity, could result in circadian misalignment, which has been associated in some studies with increased cardiovascular disease risk, metabolic syndrome and other health risks,” the authors wrote.
A recent study also showed an increase in medical errors in the week after switching to daylight saving time.
“Because the adoption of permanent standard time would be beneficial for public health and safety, the AASM will be advocating at the federal level for this legislative change,” said AASM President Kannan Ramar, MBBS, MD, with the Mayo Clinic in Rochester, Minn.
It seems that many Americans are in favor of the change. In July, an AASM survey of roughly 2,000 U.S. adults showed that two-thirds support doing away with the seasonal time change. Only 11% opposed it. In addition, the academy’s 2019 survey showed more than half of adults feel extremely, or somewhat, tired after the springing ahead to daylight saving time.
Strong support
The position statement has been endorsed by 19 organizations, including the American Academy of Cardiovascular Sleep Medicine, American College of Chest Physicians (CHEST), American College of Occupational and Environmental Medicine, National PTA, National Safety Council, Society of Anesthesia and Sleep Medicine, and the Society of Behavioral Sleep Medicine.
Weighing in on the issue, Saul Rothenberg, PhD, from the Sleep Center at Greenwich Hospital, Conn., said the literature on daylight saving time has grown over the past 20 years. He said he was ”humbled” by the research that shows that a “relatively small” misalignment of biological and social clocks has a measurable impact on human health and behavior.
“Because misalignment is associated with negative health and performance outcomes, keeping one set of hours year-round is promoted to minimize misalignment and associated consequences,” he added.
In light of this research, the recommendation to dispense with daylight saving time seems “quite reasonable” from a public health perspective. “I am left with a strengthened view on the importance of regular adequate sleep as a way to enhance health, performance, and quality of life,” he added.
This research had no commercial funding. Dr. Rishi and Dr. Rothenberg have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SLEEP 2020
Many advanced countries missing targets for HCV elimination
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
Help your patients better understand the risks and treatment for hepatitis C by sharing AGA GI Patient Center education at http://ow.ly/xV2S30r8L29.
A version of this article originally appeared on Medscape.com.
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
Help your patients better understand the risks and treatment for hepatitis C by sharing AGA GI Patient Center education at http://ow.ly/xV2S30r8L29.
A version of this article originally appeared on Medscape.com.
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
Help your patients better understand the risks and treatment for hepatitis C by sharing AGA GI Patient Center education at http://ow.ly/xV2S30r8L29.
A version of this article originally appeared on Medscape.com.
Final EVAPORATE results for Vascepa raise eyebrows
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Many advanced countries missing targets for HCV elimination
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Eleven high-income countries are on track to meet World Health Organization targets to eliminate hepatitis C infection by 2030, compared with 9 countries 2 years ago, researchers reported. But 28 countries, including the United States, are not expected to eliminate HCV until 2050.
“In the countries making progress, the common elements are political will, a clear national plan, and easing of restrictions on the cascade of care and testing,” Yuri Sanchez Gonzalez, PhD, director of health economics and outcomes research for biopharmaceutical company AbbVie said in an interview. That would include offering hepatitis C treatment to individuals who have liver fibrosis and those struggling with sobriety, he said. “We can’t overstate how much this is a massive driver of the hepatitis C epidemic.”
His research, presented at the digital edition of the International Liver Congress this week, showed more countries on target than in a study published 2 years ago in Liver International . “But it’s not enough,” Dr. Sanchez Gonzalez said. “We know that more than 80% of infections are in people who inject drugs. Stigmatization of drug use is still a very major issue.” Despite data clearly showing that countries who have harm-reduction programs make progress, “in many countries these programs are still illegal.”
To evaluate which countries are on target to eliminate hepatitis C by 2030, researchers performed Markov disease progression models of HCV infection in 45 high-income countries. The results showed that Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom are “in the green” (on target for 2030).
Austria, Malta, the Netherlands, New Zealand, and South Korea are “in the yellow” (on target for 2040), and 28 remaining countries, including the United States, are “in the red,” with targets estimated to be met by 2050.
Compared with an analysis performed 2 years ago, South Korea moved from green to yellow, while Canada, Germany, and Sweden moved from red to green.
Researchers say that the countries moving the needle are the ones addressing barriers to care.
EASL: Eliminate barriers to treatment
During this week’s Congress, the European Association for the Study of the Liver (EASL) launched a policy statement recommending breaking down all barriers that prevent people who inject drugs from getting access to hepatitis C treatment, including encouragement of laws and policies that “decriminalize drug use, drug possession and drug users themselves,” said statement coauthor Mojca Maticic, MD, PhD, University of Ljubljana, Slovenia.
“To reach the desired WHO goal, combining decriminalization of personal drug consumption and integrated interventions that include hepatitis C testing and treatment should be implemented,” she added. We need to adopt “an approach based on public health promotion, respect for human rights, and evidence.”
Although harm reduction is the top strategy for making 2030 targets, having precision data also helps a lot.
“High-quality data and harm-reduction innovation to curb the overdose crisis has moved us out of the red and into the green,” Canadian researcher Jordan Feld, MD, MPH, University of Toronto, said in an interview. He points to British Columbia, Canada’s third-most populous province, putting harm reduction programs in place as key to Canadian progress.
“Given the increasing opioid epidemic, you’re creating yourself a bigger problem if you don’t treat this population,” Dr. Feld said. When a person needs 6 months to get sober in order to be treated for HCV, that’s more potential time to pass the infection to others. His study, also presented at ILC this week, outlines anticipated timing of hepatitis C in Canada’s four most populous provinces (Ontario, Quebec, British Columbia, and Alberta), and shows British Columbia will reach targets by 2028.
Lifting all restrictions clearly helps, Dr. Sanchez Gonzalez reported. He pointed to Sweden as a good example, a country that recently lifted HCV treatment restrictions for individuals living with fibrosis. Sweden moved from a red to a green spot in this analysis and is now on target for 2030.
“As long as everyone who needs treatment gets treatment, you can make tremendous progress,” he said.
Keeping track is also essential to moving the needle. Since the WHO has no enforcement power, “these studies, which offer a report card of progress, really matter,” Dr. Sanchez Gonzalez explained. When a country knows where they stand, they are more likely to take action to change. “Nobody likes to be shown in the red.”
Still, “it’s not a shaming exercise,” he said. It’s about starting a conversation, showing who’s on track, and sharing how to get on track. “Knowing that there is something in your power to move the needle toward elimination by learning from your neighbors is powerful – often, it just takes political will.”
Dr. Feld has received consulting fees from AbbVie. Dr. Sanchez Gonzalez is on staff as the Director of Economics at AbbVie. Dr. Maticic has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Early evolocumab quickly lowers LDL cholesterol after primary PCI
Early administration of evolocumab significantly reduced levels of LDL cholesterol in patients with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention, according to data from an open-label randomized trial of 102 adults in Japan.

Data from previous studies have shown that proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors can reduce LDL cholesterol in acute coronary syndrome patients, wrote Tomoaki Okada, MD, of Kagawa (Japan) Prefectural Central Hospital and colleagues.
In particular, “The EVOPACS trial [J Am Coll Cardiol 2019; 74:2452-62] reported that evolocumab therapy initiated at an early phase of ACS showed [LDL cholesterol] level reduction by 4-8 weeks,” they said.
“However, the 4-week efficacy of PCSK9 inhibitor therapy combined with a statin remains unknown,” they said.
In a study presented at the virtual annual congress of the European Society of Cardiology and published simultaneously in JACC: Cardiovascular Interventions, the researchers randomized 52 patients to receive 140 mg of evolocumab subcutaneously within 24 hours of indexed percutaneous coronary intervention and again after 2 weeks. A group of 50 controls received evolocumab after PCI only, but no additional dose after 2 weeks.
The average age of the patients was 65 years, 88% were men, and 26% had a history of statin treatment.
A total of 49 patients in each group were included in the final analysis, with a primary outcome of change in LDL cholesterol levels from baseline to 4 weeks.
Baseline LCL cholesterol levels were 120.8 mg/dL and 124.7 mg/dL in the evolocumab and control groups, respectively. Changes from baseline were significantly greater in the evolocumab group, compared with controls, at –76% and –33%, respectively.
All patients in the evolocumab group and 27% of patients in the control groups achieved LDL cholesterol levels of less than 70 mg/dL at 4 weeks. In addition, 92% and 96% of evolocumab patients achieved LDL cholesterol levels less than 55 mg/dL at 2 weeks and 4 weeks, respectively.
Overall changes in non-HDL cholesterol, HDL cholesterol, and small dense LDL in the evolocumab and control groups were –66.2% and –26.0%; 2.8% and –0.7%; and –67% and –13.8%, respectively. Of these, changes in non-HDL cholesterol and small dense LDL were significantly different between the groups.
In addition, patients in the evolocumab group showed a 3% decrease in lipoprotein, compared with an 82% increase in the control group. This finding suggests the additional benefit of including evolocumab for managing residual risk in patients with high lipoprotein(a) levels” after acute MI, the researchers noted.
Adverse events and serious adverse events were similar between the groups.
‘Early and strong’ LDL cholesterol lowering best for preventing repeat events
“By using the PCSK9 inhibitors, we have the opportunity to lower LDL cholesterol [LDL-C]” both quickly and dramatically, said Heinz Drexel, MD, in an interview.
“This Japanese study shows that very low LDL-C levels can be obtained as fast as within 4 weeks,” he said. “This fits into the concept that risk for future infarctions and strokes is best reduced by early and strong LDL-C lowering,” he explained.
Dr. Drexel said that he was not surprised by the magnitude of the decrease in LDL cholesterol in study findings in light of the EVOPACS study and other research, as well as his own clinical experience.
“The primary message for doctors is that it is now possible to achieve these low levels of LDL-C in a short time,” he said.
“Additional research must prove that this low LDL-C translates to reduction of MIs and strokes, and there is increasing evidence that this will happen,” Dr. Drexel noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Drexel had no financial conflicts to disclose.
SOURCE: Okada T et al. ESC 2020. JACC Cardiovascular Interventions. 2020 Aug 28. doi: 10.1016/j.jcin.2020.08.026.
Early administration of evolocumab significantly reduced levels of LDL cholesterol in patients with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention, according to data from an open-label randomized trial of 102 adults in Japan.
Data from previous studies have shown that proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors can reduce LDL cholesterol in acute coronary syndrome patients, wrote Tomoaki Okada, MD, of Kagawa (Japan) Prefectural Central Hospital and colleagues.
In particular, “The EVOPACS trial [J Am Coll Cardiol 2019; 74:2452-62] reported that evolocumab therapy initiated at an early phase of ACS showed [LDL cholesterol] level reduction by 4-8 weeks,” they said.
“However, the 4-week efficacy of PCSK9 inhibitor therapy combined with a statin remains unknown,” they said.
In a study presented at the virtual annual congress of the European Society of Cardiology and published simultaneously in JACC: Cardiovascular Interventions, the researchers randomized 52 patients to receive 140 mg of evolocumab subcutaneously within 24 hours of indexed percutaneous coronary intervention and again after 2 weeks. A group of 50 controls received evolocumab after PCI only, but no additional dose after 2 weeks.
The average age of the patients was 65 years, 88% were men, and 26% had a history of statin treatment.
A total of 49 patients in each group were included in the final analysis, with a primary outcome of change in LDL cholesterol levels from baseline to 4 weeks.
Baseline LCL cholesterol levels were 120.8 mg/dL and 124.7 mg/dL in the evolocumab and control groups, respectively. Changes from baseline were significantly greater in the evolocumab group, compared with controls, at –76% and –33%, respectively.
All patients in the evolocumab group and 27% of patients in the control groups achieved LDL cholesterol levels of less than 70 mg/dL at 4 weeks. In addition, 92% and 96% of evolocumab patients achieved LDL cholesterol levels less than 55 mg/dL at 2 weeks and 4 weeks, respectively.
Overall changes in non-HDL cholesterol, HDL cholesterol, and small dense LDL in the evolocumab and control groups were –66.2% and –26.0%; 2.8% and –0.7%; and –67% and –13.8%, respectively. Of these, changes in non-HDL cholesterol and small dense LDL were significantly different between the groups.
In addition, patients in the evolocumab group showed a 3% decrease in lipoprotein, compared with an 82% increase in the control group. This finding suggests the additional benefit of including evolocumab for managing residual risk in patients with high lipoprotein(a) levels” after acute MI, the researchers noted.
Adverse events and serious adverse events were similar between the groups.
‘Early and strong’ LDL cholesterol lowering best for preventing repeat events
“By using the PCSK9 inhibitors, we have the opportunity to lower LDL cholesterol [LDL-C]” both quickly and dramatically, said Heinz Drexel, MD, in an interview.
“This Japanese study shows that very low LDL-C levels can be obtained as fast as within 4 weeks,” he said. “This fits into the concept that risk for future infarctions and strokes is best reduced by early and strong LDL-C lowering,” he explained.
Dr. Drexel said that he was not surprised by the magnitude of the decrease in LDL cholesterol in study findings in light of the EVOPACS study and other research, as well as his own clinical experience.
“The primary message for doctors is that it is now possible to achieve these low levels of LDL-C in a short time,” he said.
“Additional research must prove that this low LDL-C translates to reduction of MIs and strokes, and there is increasing evidence that this will happen,” Dr. Drexel noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Drexel had no financial conflicts to disclose.
SOURCE: Okada T et al. ESC 2020. JACC Cardiovascular Interventions. 2020 Aug 28. doi: 10.1016/j.jcin.2020.08.026.
Early administration of evolocumab significantly reduced levels of LDL cholesterol in patients with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention, according to data from an open-label randomized trial of 102 adults in Japan.
Data from previous studies have shown that proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors can reduce LDL cholesterol in acute coronary syndrome patients, wrote Tomoaki Okada, MD, of Kagawa (Japan) Prefectural Central Hospital and colleagues.
In particular, “The EVOPACS trial [J Am Coll Cardiol 2019; 74:2452-62] reported that evolocumab therapy initiated at an early phase of ACS showed [LDL cholesterol] level reduction by 4-8 weeks,” they said.
“However, the 4-week efficacy of PCSK9 inhibitor therapy combined with a statin remains unknown,” they said.
In a study presented at the virtual annual congress of the European Society of Cardiology and published simultaneously in JACC: Cardiovascular Interventions, the researchers randomized 52 patients to receive 140 mg of evolocumab subcutaneously within 24 hours of indexed percutaneous coronary intervention and again after 2 weeks. A group of 50 controls received evolocumab after PCI only, but no additional dose after 2 weeks.
The average age of the patients was 65 years, 88% were men, and 26% had a history of statin treatment.
A total of 49 patients in each group were included in the final analysis, with a primary outcome of change in LDL cholesterol levels from baseline to 4 weeks.
Baseline LCL cholesterol levels were 120.8 mg/dL and 124.7 mg/dL in the evolocumab and control groups, respectively. Changes from baseline were significantly greater in the evolocumab group, compared with controls, at –76% and –33%, respectively.
All patients in the evolocumab group and 27% of patients in the control groups achieved LDL cholesterol levels of less than 70 mg/dL at 4 weeks. In addition, 92% and 96% of evolocumab patients achieved LDL cholesterol levels less than 55 mg/dL at 2 weeks and 4 weeks, respectively.
Overall changes in non-HDL cholesterol, HDL cholesterol, and small dense LDL in the evolocumab and control groups were –66.2% and –26.0%; 2.8% and –0.7%; and –67% and –13.8%, respectively. Of these, changes in non-HDL cholesterol and small dense LDL were significantly different between the groups.
In addition, patients in the evolocumab group showed a 3% decrease in lipoprotein, compared with an 82% increase in the control group. This finding suggests the additional benefit of including evolocumab for managing residual risk in patients with high lipoprotein(a) levels” after acute MI, the researchers noted.
Adverse events and serious adverse events were similar between the groups.
‘Early and strong’ LDL cholesterol lowering best for preventing repeat events
“By using the PCSK9 inhibitors, we have the opportunity to lower LDL cholesterol [LDL-C]” both quickly and dramatically, said Heinz Drexel, MD, in an interview.
“This Japanese study shows that very low LDL-C levels can be obtained as fast as within 4 weeks,” he said. “This fits into the concept that risk for future infarctions and strokes is best reduced by early and strong LDL-C lowering,” he explained.
Dr. Drexel said that he was not surprised by the magnitude of the decrease in LDL cholesterol in study findings in light of the EVOPACS study and other research, as well as his own clinical experience.
“The primary message for doctors is that it is now possible to achieve these low levels of LDL-C in a short time,” he said.
“Additional research must prove that this low LDL-C translates to reduction of MIs and strokes, and there is increasing evidence that this will happen,” Dr. Drexel noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Drexel had no financial conflicts to disclose.
SOURCE: Okada T et al. ESC 2020. JACC Cardiovascular Interventions. 2020 Aug 28. doi: 10.1016/j.jcin.2020.08.026.
FROM ESC CONGRESS 2020
Repeat FIB-4 blood tests help predict cirrhosis
Repeat Fibrosis-4 (FIB-4) scores can be used to identify people at greatest risk for cirrhosis of the liver, new research shows.
“Done repeatedly, this test can improve prediction capacity to identify who will develop cirrhosis of the liver later in life,” said lead researcher Hannes Hagström, MD, from the Karolinska University Hospital in Stockholm.
A FIB-4 score that rises from one test to the next indicates that a person is at increased risk for severe liver disease, whereas a score that drops indicates a decreased risk, he told Medscape Medical News. The study results — published online July 1 in the Journal of Hepatology, was presented at the Digital International Liver Congress 2020.
The noninvasive, widely available, cheap FIB-4 test — which is calculated on the basis of age, transaminase level, and platelet count — is commonly used to identify the risk for advanced fibrosis in liver disease, but it has not been used to predict future risk.
To evaluate risk for cirrhosis, Hagström and his colleagues looked at 812,073 blood tests performed from 1985 to 1996 on people enrolled in the Swedish Apolipoprotein Mortality Risk (AMORIS) study.
They excluded people younger than 35 years and older than 79 years and anyone with a diagnosis of any liver disease at baseline.
The 40,729 people who had two FIB-4 measurements taken less than 5 years apart were included in the analysis. Test results were categorized into three risk groups: low (<1.30), intermediate (1.30 - 2.67), and high (>2.67).
After a median of 16.2 years, 11,929 people in the study cohort had died and 581 had a severe liver disease event.
Severe liver disease events were more common in people who had both tests categorized as high risk than in people who had both tests categorized as low risk (13.2% vs 1.0%; aHR, 17.04; 95% CI, 11.67 - 24.88).
The researchers found that a one-unit increase between the two test results was continuously predictive of a severe liver disease event (aHR, 1.81; 95% CI, 1.67 - 1.96).
One test not enough
The absolute risk for severe liver disease in the general population is 2%, but the FIB-4 score is elevated in about one-third of people in the general population.
“A lot of people who have increased levels of this biomarker will never develop cirrhosis,” Hagström told Medscape Medical News.
Although two FIB-4 scores might not identify everyone who will get cirrhosis, comparing scores provides insight into who is at greatest risk, he explained.
This information can be useful, particularly for primary care doctors. If you know that someone is at higher risk, “you can send that patient for a FibroScan, which is a much more sensitive measurement,” but also much more expensive. “Now we can better know who to send,” he said.
However, “the main problem is that these tests are not widely known” or used enough by primary care doctors, Hagström said.
A lack of knowledge about the utility of this test is a problem, agreed Jérôme Boursier, MD, PhD, from Angers University in France.
“The younger doctors are using these tests more often,” he told Medscape Medical News, but “the older doctors are not aware they exist.”
This study supports repeating the tests. “One test offers quite poor prediction,” Boursier said. But “when you have a higher score on a second one, this can help the conversation with the patient.”
Hagström and Boursier have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Repeat Fibrosis-4 (FIB-4) scores can be used to identify people at greatest risk for cirrhosis of the liver, new research shows.
“Done repeatedly, this test can improve prediction capacity to identify who will develop cirrhosis of the liver later in life,” said lead researcher Hannes Hagström, MD, from the Karolinska University Hospital in Stockholm.
A FIB-4 score that rises from one test to the next indicates that a person is at increased risk for severe liver disease, whereas a score that drops indicates a decreased risk, he told Medscape Medical News. The study results — published online July 1 in the Journal of Hepatology, was presented at the Digital International Liver Congress 2020.
The noninvasive, widely available, cheap FIB-4 test — which is calculated on the basis of age, transaminase level, and platelet count — is commonly used to identify the risk for advanced fibrosis in liver disease, but it has not been used to predict future risk.
To evaluate risk for cirrhosis, Hagström and his colleagues looked at 812,073 blood tests performed from 1985 to 1996 on people enrolled in the Swedish Apolipoprotein Mortality Risk (AMORIS) study.
They excluded people younger than 35 years and older than 79 years and anyone with a diagnosis of any liver disease at baseline.
The 40,729 people who had two FIB-4 measurements taken less than 5 years apart were included in the analysis. Test results were categorized into three risk groups: low (<1.30), intermediate (1.30 - 2.67), and high (>2.67).
After a median of 16.2 years, 11,929 people in the study cohort had died and 581 had a severe liver disease event.
Severe liver disease events were more common in people who had both tests categorized as high risk than in people who had both tests categorized as low risk (13.2% vs 1.0%; aHR, 17.04; 95% CI, 11.67 - 24.88).
The researchers found that a one-unit increase between the two test results was continuously predictive of a severe liver disease event (aHR, 1.81; 95% CI, 1.67 - 1.96).
One test not enough
The absolute risk for severe liver disease in the general population is 2%, but the FIB-4 score is elevated in about one-third of people in the general population.
“A lot of people who have increased levels of this biomarker will never develop cirrhosis,” Hagström told Medscape Medical News.
Although two FIB-4 scores might not identify everyone who will get cirrhosis, comparing scores provides insight into who is at greatest risk, he explained.
This information can be useful, particularly for primary care doctors. If you know that someone is at higher risk, “you can send that patient for a FibroScan, which is a much more sensitive measurement,” but also much more expensive. “Now we can better know who to send,” he said.
However, “the main problem is that these tests are not widely known” or used enough by primary care doctors, Hagström said.
A lack of knowledge about the utility of this test is a problem, agreed Jérôme Boursier, MD, PhD, from Angers University in France.
“The younger doctors are using these tests more often,” he told Medscape Medical News, but “the older doctors are not aware they exist.”
This study supports repeating the tests. “One test offers quite poor prediction,” Boursier said. But “when you have a higher score on a second one, this can help the conversation with the patient.”
Hagström and Boursier have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Repeat Fibrosis-4 (FIB-4) scores can be used to identify people at greatest risk for cirrhosis of the liver, new research shows.
“Done repeatedly, this test can improve prediction capacity to identify who will develop cirrhosis of the liver later in life,” said lead researcher Hannes Hagström, MD, from the Karolinska University Hospital in Stockholm.
A FIB-4 score that rises from one test to the next indicates that a person is at increased risk for severe liver disease, whereas a score that drops indicates a decreased risk, he told Medscape Medical News. The study results — published online July 1 in the Journal of Hepatology, was presented at the Digital International Liver Congress 2020.
The noninvasive, widely available, cheap FIB-4 test — which is calculated on the basis of age, transaminase level, and platelet count — is commonly used to identify the risk for advanced fibrosis in liver disease, but it has not been used to predict future risk.
To evaluate risk for cirrhosis, Hagström and his colleagues looked at 812,073 blood tests performed from 1985 to 1996 on people enrolled in the Swedish Apolipoprotein Mortality Risk (AMORIS) study.
They excluded people younger than 35 years and older than 79 years and anyone with a diagnosis of any liver disease at baseline.
The 40,729 people who had two FIB-4 measurements taken less than 5 years apart were included in the analysis. Test results were categorized into three risk groups: low (<1.30), intermediate (1.30 - 2.67), and high (>2.67).
After a median of 16.2 years, 11,929 people in the study cohort had died and 581 had a severe liver disease event.
Severe liver disease events were more common in people who had both tests categorized as high risk than in people who had both tests categorized as low risk (13.2% vs 1.0%; aHR, 17.04; 95% CI, 11.67 - 24.88).
The researchers found that a one-unit increase between the two test results was continuously predictive of a severe liver disease event (aHR, 1.81; 95% CI, 1.67 - 1.96).
One test not enough
The absolute risk for severe liver disease in the general population is 2%, but the FIB-4 score is elevated in about one-third of people in the general population.
“A lot of people who have increased levels of this biomarker will never develop cirrhosis,” Hagström told Medscape Medical News.
Although two FIB-4 scores might not identify everyone who will get cirrhosis, comparing scores provides insight into who is at greatest risk, he explained.
This information can be useful, particularly for primary care doctors. If you know that someone is at higher risk, “you can send that patient for a FibroScan, which is a much more sensitive measurement,” but also much more expensive. “Now we can better know who to send,” he said.
However, “the main problem is that these tests are not widely known” or used enough by primary care doctors, Hagström said.
A lack of knowledge about the utility of this test is a problem, agreed Jérôme Boursier, MD, PhD, from Angers University in France.
“The younger doctors are using these tests more often,” he told Medscape Medical News, but “the older doctors are not aware they exist.”
This study supports repeating the tests. “One test offers quite poor prediction,” Boursier said. But “when you have a higher score on a second one, this can help the conversation with the patient.”
Hagström and Boursier have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.