User login
The Official Newspaper of the American Association for Thoracic Surgery
Drug Resistance Triggers Lung Cancer Transformation
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
Nonsurgical Approaches to Perforation Are Rising
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
Endosonography Plus Surgical Staging for NSCLC?
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
Drug Resistance Triggers Lung Cancer Transformation
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
Nonsurgical Approaches to Perforation Are Rising
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
Endosonography Plus Surgical Staging for NSCLC?
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
The main question raised by this study is not whether endosonography improves the sensitivity of surgical staging but whether the combined approach can be translated into a larger patient population and yield equivalent outcomes there, according to Dr. Mark D. Iannettoni. The level of expertise in endoscopic techniques was likely much higher at the referral centers in this study than it is at community hospitals where most thoracic surgery takes place. "This fact is extremely important because these modalities are highly operator dependent," he noted. "Until this modality can be reproduced at all centers where thoracic surgery is commonly performed, or until all of these patients are cared for at specialized centers, surgical staging must remain the gold standard for adequate preoperative evaluation," he said.
Mark D. Iannettoni, M.D., is in cardiothoracic surgery at the University of Iowa Heart and Vascular Center, Iowa City. He reported that he had no financial disclosures. These comments were taken from his editorial accompanying Dr. Annema's report (JAMA 2010;304:2296-7).
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
For patients with suspected non-small cell lung cancer, adding endosonography before surgical staging improves detection of mediastinal nodal metastases, thus reducing unnecessary thoracotomies by more than half, a study has shown.
In addition, because endosonography is minimally invasive, adding this step doesn't raise the rate of complications for staging procedures, said Dr. Jouke T. Annema of Leiden (the Netherlands) University Medical Center and associates.
The researchers compared surgical staging alone to endosonography followed by surgical staging because "at present it is not known whether initial mediastinal tissue staging of lung cancer by endosonography improves the detection of nodal metastases." Failure to detect such metastases during staging results in patients undergoing thoracotomy for tumor resection, only to have the thoracotomy aborted when unresectable or metastatic lung disease is discovered (JAMA 2010;304:2245-52).
The investigators randomized 241 patients suspected of having resectable NSCLC, who were treated at four tertiary referral centers in Belgium, the Netherlands, and the United Kingdom. Patients were assigned to surgical staging alone, which is the current standard of care (118 subjects), or to endosonography followed by surgical staging (123 subjects).
The sensitivity of surgical staging alone was 79%. This improved to 94% when endosonography was combined with surgical staging, Dr. Annema and colleagues said.
Mediastinal nodal metastases were found in 41 of 118 patients (35%) by surgical staging alone, compared with 62 of 123 patients (50%) by the combined approach. This means that there were 21 unnecessary thoracotomies with surgical staging alone, for a rate of 18%, compared with 9 with the combined approach, for a rate of 7%.
The complication rate was 6% for surgical staging, compared with 1% for endosonography.
These findings show that endosonography improves the sensitivity of surgical staging, halves the rate of unnecessary thoracotomy, and has a low complication rate. Because it also does not require general anesthesia and has been shown in previous studies to be cost effective as well as preferred by patients, "endosonography should be the first step for mediastinal nodal staging," the investigators said.
They added that all of the staging procedures in this study were performed in specialty centers by highly trained and experienced interventionists, so the applicability of the study findings to other settings is limited.
This study was supported in part by Hitachi Medical Systems, COOK, Olympus, the Zorgprogramma Oncologie Gent, the U.K. National Health Service R & D Health Technology Assessment Program, and the National Institute for Health Research Cambridge Biomedical Research Centre.
Vanderbilt Uses Genotyping Prior To Catheterization
CHICAGO - Last fall, physicians at Vanderbilt University Medical Center began routinely testing all patients who were scheduled for coronary catheterization with a broad genotyping screen that - among other things - would identify whether they had a problem activating clopidogrel. By mid-November, the program had tested about 300 patients, including 10 found to have a poor-metabolizer genotype in the hepatic-enzyme gene CYP2C19 that would likely blunt the efficacy of a conventional clopidogrel dose. Many of the 10 patients received a doubled dose to compensate, whereas others who weren't aged 75 or older received the pricier, alternative agent prasugrel.
This experience marked the first phase of a new Vanderbilt program that will expand over time to include other patients in line to receive a drug with a pharmacogenetic dimension, Dr. Dan M. Roden said at the meeting. The genotyping program will soon expand to include patients who are scheduled for knee- or hip-replacement surgery, anticipating their need to start on warfarin. Genotype data can also help physicians select the best dosage for starting a warfarin regimen, said Dr. Roden, a cardiologist and assistant vice chancellor for personalized medicine at Vanderbilt in Nashville, Tenn.
Subsequent expansion plans are not yet set, but other candidates for genotyping include patients who are either already on or at an increased risk for soon starting tamoxifen, abacavir, azathioprine, 6-mercaptopurine, codeine, or "virtually any antidepressant or most antipsychotics,” Dr. Roden said in an interview.
"In the long perspective, every 50-year-old” is a good bet to eventually receive at least one drug for which a dosage adjustment based on genotype is warranted, but - stopping short of such global use right now - the Vanderbilt program will instead gradually phase in new groups of patients to the offer of genotyping.
"Implementation is a huge challenge. In my opinion, this will only work with preemptive implementation. Electronic records are not just repositories of information, but are nimble enough to provide support at the time of a prescription,” he said. "The way it ought to work is, a physician prescribes a drug and the electronic system recognizes [that] the drug has a genetic element and goes into the patient's record and finds the genotype information” to decide whether to flash a screen alert about the patient's genotype and the implications.
The program, known as PREDICT (Pharmacogenomic Resource for Enhanced Decisions in Care and Treatment) launched on Sept. 15. It uses a genotyping panel sold on the U.S. market by Illumina that screens for 184 different genetic polymorphisms in 34 genes that affect the absorption, distribution, metabolism, or excretion of various drugs.
Test results get posted into the record within a day of specimen collection.
So far, Vanderbilt itself has completely funded the program, which involved a year of planning and "a huge amount of money,” said Dr. Roden, adding that the program is the first of its kind worldwide. PREDICT is expected to improve patient outcomes and its developers hope to eventually convince payers to cover the cost.
Dr. Roden stated that he is or has been a consultant to several drug companies and has received royalties from Clinical Data Inc.
CHICAGO - Last fall, physicians at Vanderbilt University Medical Center began routinely testing all patients who were scheduled for coronary catheterization with a broad genotyping screen that - among other things - would identify whether they had a problem activating clopidogrel. By mid-November, the program had tested about 300 patients, including 10 found to have a poor-metabolizer genotype in the hepatic-enzyme gene CYP2C19 that would likely blunt the efficacy of a conventional clopidogrel dose. Many of the 10 patients received a doubled dose to compensate, whereas others who weren't aged 75 or older received the pricier, alternative agent prasugrel.
This experience marked the first phase of a new Vanderbilt program that will expand over time to include other patients in line to receive a drug with a pharmacogenetic dimension, Dr. Dan M. Roden said at the meeting. The genotyping program will soon expand to include patients who are scheduled for knee- or hip-replacement surgery, anticipating their need to start on warfarin. Genotype data can also help physicians select the best dosage for starting a warfarin regimen, said Dr. Roden, a cardiologist and assistant vice chancellor for personalized medicine at Vanderbilt in Nashville, Tenn.
Subsequent expansion plans are not yet set, but other candidates for genotyping include patients who are either already on or at an increased risk for soon starting tamoxifen, abacavir, azathioprine, 6-mercaptopurine, codeine, or "virtually any antidepressant or most antipsychotics,” Dr. Roden said in an interview.
"In the long perspective, every 50-year-old” is a good bet to eventually receive at least one drug for which a dosage adjustment based on genotype is warranted, but - stopping short of such global use right now - the Vanderbilt program will instead gradually phase in new groups of patients to the offer of genotyping.
"Implementation is a huge challenge. In my opinion, this will only work with preemptive implementation. Electronic records are not just repositories of information, but are nimble enough to provide support at the time of a prescription,” he said. "The way it ought to work is, a physician prescribes a drug and the electronic system recognizes [that] the drug has a genetic element and goes into the patient's record and finds the genotype information” to decide whether to flash a screen alert about the patient's genotype and the implications.
The program, known as PREDICT (Pharmacogenomic Resource for Enhanced Decisions in Care and Treatment) launched on Sept. 15. It uses a genotyping panel sold on the U.S. market by Illumina that screens for 184 different genetic polymorphisms in 34 genes that affect the absorption, distribution, metabolism, or excretion of various drugs.
Test results get posted into the record within a day of specimen collection.
So far, Vanderbilt itself has completely funded the program, which involved a year of planning and "a huge amount of money,” said Dr. Roden, adding that the program is the first of its kind worldwide. PREDICT is expected to improve patient outcomes and its developers hope to eventually convince payers to cover the cost.
Dr. Roden stated that he is or has been a consultant to several drug companies and has received royalties from Clinical Data Inc.
CHICAGO - Last fall, physicians at Vanderbilt University Medical Center began routinely testing all patients who were scheduled for coronary catheterization with a broad genotyping screen that - among other things - would identify whether they had a problem activating clopidogrel. By mid-November, the program had tested about 300 patients, including 10 found to have a poor-metabolizer genotype in the hepatic-enzyme gene CYP2C19 that would likely blunt the efficacy of a conventional clopidogrel dose. Many of the 10 patients received a doubled dose to compensate, whereas others who weren't aged 75 or older received the pricier, alternative agent prasugrel.
This experience marked the first phase of a new Vanderbilt program that will expand over time to include other patients in line to receive a drug with a pharmacogenetic dimension, Dr. Dan M. Roden said at the meeting. The genotyping program will soon expand to include patients who are scheduled for knee- or hip-replacement surgery, anticipating their need to start on warfarin. Genotype data can also help physicians select the best dosage for starting a warfarin regimen, said Dr. Roden, a cardiologist and assistant vice chancellor for personalized medicine at Vanderbilt in Nashville, Tenn.
Subsequent expansion plans are not yet set, but other candidates for genotyping include patients who are either already on or at an increased risk for soon starting tamoxifen, abacavir, azathioprine, 6-mercaptopurine, codeine, or "virtually any antidepressant or most antipsychotics,” Dr. Roden said in an interview.
"In the long perspective, every 50-year-old” is a good bet to eventually receive at least one drug for which a dosage adjustment based on genotype is warranted, but - stopping short of such global use right now - the Vanderbilt program will instead gradually phase in new groups of patients to the offer of genotyping.
"Implementation is a huge challenge. In my opinion, this will only work with preemptive implementation. Electronic records are not just repositories of information, but are nimble enough to provide support at the time of a prescription,” he said. "The way it ought to work is, a physician prescribes a drug and the electronic system recognizes [that] the drug has a genetic element and goes into the patient's record and finds the genotype information” to decide whether to flash a screen alert about the patient's genotype and the implications.
The program, known as PREDICT (Pharmacogenomic Resource for Enhanced Decisions in Care and Treatment) launched on Sept. 15. It uses a genotyping panel sold on the U.S. market by Illumina that screens for 184 different genetic polymorphisms in 34 genes that affect the absorption, distribution, metabolism, or excretion of various drugs.
Test results get posted into the record within a day of specimen collection.
So far, Vanderbilt itself has completely funded the program, which involved a year of planning and "a huge amount of money,” said Dr. Roden, adding that the program is the first of its kind worldwide. PREDICT is expected to improve patient outcomes and its developers hope to eventually convince payers to cover the cost.
Dr. Roden stated that he is or has been a consultant to several drug companies and has received royalties from Clinical Data Inc.
Gait Predicts Outcomes in Elderly Cardiac Surgery
Gait speed independently predicts both major morbidity and mortality in elderly patients who are about to undergo cardiac surgery, according to a prospective, blinded study reported in the Journal of the American College of Cardiology.
"This simple, rapid, and inexpensive test effectively stratifies patients beyond traditional estimates of risk, which tend to be inaccurate in the elderly," said Dr. Jonathan Afilalo of McGill University, Montreal, and his associates.
Half the cardiac surgeries done in North America involve elderly patients (aged at least 70 years), but scoring systems for estimating operative risk perform poorly in this age group, "overestimating mortality by as much as 250%," they noted.
Dr. Afilalo and his colleagues performed what they described as the first study to test the value of gait speed as a predictor of poor outcomes in elderly cardiac surgery patients. The prospective, blinded study involved 131 patients (mean age, 76 years) who were scheduled to undergo elective coronary artery bypass and/or valve replacement or repair via standard sternotomy at four university-affiliated medical centers across Canada and the United States.
Before surgery, the study subjects were timed as they walked a distance of 5 meters in a well-lit hallway; subjects were permitted to use an aid such as a cane or walker if needed. A time of 6 seconds or longer was classified as a slow gait speed, whereas any time under 6 seconds was classified as a normal gait speed.
The primary composite end point was in-hospital mortality or any of five major complications (stroke, renal failure, prolonged ventilation, deep sternal wound infection, and need for reoperation).
In all, 60 patients (46%) were judged to have slow gait speed before surgery. Interestingly, gait speed did not correlate with the Society of Thoracic Surgeons' risk score, "suggesting that these were representing distinct domains," the investigators said.
After surgery, 30 patients (23%) experienced the primary composite end point.
Slow gait speed was a strong and independent predictor, associated with a 3.17-fold increase in risk of the primary end point. Moreover, adding gait speed to existing risk prediction models improved their performance in predicting which patients would experience an adverse event and which patients would need "to be discharged to a health care facility for ongoing medical care or rehabilitation."
Women with slow gait speed appeared to be at particularly high risk for adverse outcomes.
The study findings have three clinical implications. "First, by refining risk predictions in this challenging group, clinicians can have a more comprehensive assessment of their patient and provide a more accurate estimate of risk to the patient," Dr. Afilalo and his associates said (J. Am. Coll. Cardiol. 2010;56:1668-76).
Second, clinicians can better assess which elderly patients might have better success with less-invasive techniques such as trans-catheter valve implantation.
And third, patients who were found to have slow gait speed might benefit from extra interventions in the perioperative period, such as more intensive monitoring, early mobilization, low-intensity exercise training, or planned discharge to a specialized rehabilitation facility, they said.
The investigators reported no financial conflicts of interest.
Existing risk-assessment tools for elderly cardiac patients are inadequate, according to Dr. Joseph C. Cleveland Jr. "We must prepare ourselves to face decisions regarding treatment options for this exponentially growing segment of our population with scant data to appropriately guide our decisions."
In this context, Dr. Afilalo and his associates have given clinicians an important, simple, and "extraordinarily cost-effective" tool, he wrote in an editorial accompanying the study (J. Am. Coll. Cardiol. 2010; 56:1677-8). Assessing gait speed requires only an observer, a stopwatch, and a well-lit hallway.
He added that the investigators also should be commended for expanding the list of adverse outcomes beyond simple mortality, "because many elderly people fear loss of independence as a fate worse than death." Slow gait speed doubled the chances that a patient would be discharged to a health care facility or would have a prolonged hospital stay. "These data are sorely needed when facing elderly patients and counseling them," Dr. Cleveland said.
The researchers' finding of an interaction between slow gait speed and female sex also is particularly important. "Elderly women with slow gait speed had an eightfold increase in morbidity and mortality" and clearly represent a high-risk subgroup, he noted.
Existing risk-assessment tools for elderly cardiac patients are inadequate, according to Dr. Joseph C. Cleveland Jr. "We must prepare ourselves to face decisions regarding treatment options for this exponentially growing segment of our population with scant data to appropriately guide our decisions."
In this context, Dr. Afilalo and his associates have given clinicians an important, simple, and "extraordinarily cost-effective" tool, he wrote in an editorial accompanying the study (J. Am. Coll. Cardiol. 2010; 56:1677-8). Assessing gait speed requires only an observer, a stopwatch, and a well-lit hallway.
He added that the investigators also should be commended for expanding the list of adverse outcomes beyond simple mortality, "because many elderly people fear loss of independence as a fate worse than death." Slow gait speed doubled the chances that a patient would be discharged to a health care facility or would have a prolonged hospital stay. "These data are sorely needed when facing elderly patients and counseling them," Dr. Cleveland said.
The researchers' finding of an interaction between slow gait speed and female sex also is particularly important. "Elderly women with slow gait speed had an eightfold increase in morbidity and mortality" and clearly represent a high-risk subgroup, he noted.
Existing risk-assessment tools for elderly cardiac patients are inadequate, according to Dr. Joseph C. Cleveland Jr. "We must prepare ourselves to face decisions regarding treatment options for this exponentially growing segment of our population with scant data to appropriately guide our decisions."
In this context, Dr. Afilalo and his associates have given clinicians an important, simple, and "extraordinarily cost-effective" tool, he wrote in an editorial accompanying the study (J. Am. Coll. Cardiol. 2010; 56:1677-8). Assessing gait speed requires only an observer, a stopwatch, and a well-lit hallway.
He added that the investigators also should be commended for expanding the list of adverse outcomes beyond simple mortality, "because many elderly people fear loss of independence as a fate worse than death." Slow gait speed doubled the chances that a patient would be discharged to a health care facility or would have a prolonged hospital stay. "These data are sorely needed when facing elderly patients and counseling them," Dr. Cleveland said.
The researchers' finding of an interaction between slow gait speed and female sex also is particularly important. "Elderly women with slow gait speed had an eightfold increase in morbidity and mortality" and clearly represent a high-risk subgroup, he noted.
Gait speed independently predicts both major morbidity and mortality in elderly patients who are about to undergo cardiac surgery, according to a prospective, blinded study reported in the Journal of the American College of Cardiology.
"This simple, rapid, and inexpensive test effectively stratifies patients beyond traditional estimates of risk, which tend to be inaccurate in the elderly," said Dr. Jonathan Afilalo of McGill University, Montreal, and his associates.
Half the cardiac surgeries done in North America involve elderly patients (aged at least 70 years), but scoring systems for estimating operative risk perform poorly in this age group, "overestimating mortality by as much as 250%," they noted.
Dr. Afilalo and his colleagues performed what they described as the first study to test the value of gait speed as a predictor of poor outcomes in elderly cardiac surgery patients. The prospective, blinded study involved 131 patients (mean age, 76 years) who were scheduled to undergo elective coronary artery bypass and/or valve replacement or repair via standard sternotomy at four university-affiliated medical centers across Canada and the United States.
Before surgery, the study subjects were timed as they walked a distance of 5 meters in a well-lit hallway; subjects were permitted to use an aid such as a cane or walker if needed. A time of 6 seconds or longer was classified as a slow gait speed, whereas any time under 6 seconds was classified as a normal gait speed.
The primary composite end point was in-hospital mortality or any of five major complications (stroke, renal failure, prolonged ventilation, deep sternal wound infection, and need for reoperation).
In all, 60 patients (46%) were judged to have slow gait speed before surgery. Interestingly, gait speed did not correlate with the Society of Thoracic Surgeons' risk score, "suggesting that these were representing distinct domains," the investigators said.
After surgery, 30 patients (23%) experienced the primary composite end point.
Slow gait speed was a strong and independent predictor, associated with a 3.17-fold increase in risk of the primary end point. Moreover, adding gait speed to existing risk prediction models improved their performance in predicting which patients would experience an adverse event and which patients would need "to be discharged to a health care facility for ongoing medical care or rehabilitation."
Women with slow gait speed appeared to be at particularly high risk for adverse outcomes.
The study findings have three clinical implications. "First, by refining risk predictions in this challenging group, clinicians can have a more comprehensive assessment of their patient and provide a more accurate estimate of risk to the patient," Dr. Afilalo and his associates said (J. Am. Coll. Cardiol. 2010;56:1668-76).
Second, clinicians can better assess which elderly patients might have better success with less-invasive techniques such as trans-catheter valve implantation.
And third, patients who were found to have slow gait speed might benefit from extra interventions in the perioperative period, such as more intensive monitoring, early mobilization, low-intensity exercise training, or planned discharge to a specialized rehabilitation facility, they said.
The investigators reported no financial conflicts of interest.
Gait speed independently predicts both major morbidity and mortality in elderly patients who are about to undergo cardiac surgery, according to a prospective, blinded study reported in the Journal of the American College of Cardiology.
"This simple, rapid, and inexpensive test effectively stratifies patients beyond traditional estimates of risk, which tend to be inaccurate in the elderly," said Dr. Jonathan Afilalo of McGill University, Montreal, and his associates.
Half the cardiac surgeries done in North America involve elderly patients (aged at least 70 years), but scoring systems for estimating operative risk perform poorly in this age group, "overestimating mortality by as much as 250%," they noted.
Dr. Afilalo and his colleagues performed what they described as the first study to test the value of gait speed as a predictor of poor outcomes in elderly cardiac surgery patients. The prospective, blinded study involved 131 patients (mean age, 76 years) who were scheduled to undergo elective coronary artery bypass and/or valve replacement or repair via standard sternotomy at four university-affiliated medical centers across Canada and the United States.
Before surgery, the study subjects were timed as they walked a distance of 5 meters in a well-lit hallway; subjects were permitted to use an aid such as a cane or walker if needed. A time of 6 seconds or longer was classified as a slow gait speed, whereas any time under 6 seconds was classified as a normal gait speed.
The primary composite end point was in-hospital mortality or any of five major complications (stroke, renal failure, prolonged ventilation, deep sternal wound infection, and need for reoperation).
In all, 60 patients (46%) were judged to have slow gait speed before surgery. Interestingly, gait speed did not correlate with the Society of Thoracic Surgeons' risk score, "suggesting that these were representing distinct domains," the investigators said.
After surgery, 30 patients (23%) experienced the primary composite end point.
Slow gait speed was a strong and independent predictor, associated with a 3.17-fold increase in risk of the primary end point. Moreover, adding gait speed to existing risk prediction models improved their performance in predicting which patients would experience an adverse event and which patients would need "to be discharged to a health care facility for ongoing medical care or rehabilitation."
Women with slow gait speed appeared to be at particularly high risk for adverse outcomes.
The study findings have three clinical implications. "First, by refining risk predictions in this challenging group, clinicians can have a more comprehensive assessment of their patient and provide a more accurate estimate of risk to the patient," Dr. Afilalo and his associates said (J. Am. Coll. Cardiol. 2010;56:1668-76).
Second, clinicians can better assess which elderly patients might have better success with less-invasive techniques such as trans-catheter valve implantation.
And third, patients who were found to have slow gait speed might benefit from extra interventions in the perioperative period, such as more intensive monitoring, early mobilization, low-intensity exercise training, or planned discharge to a specialized rehabilitation facility, they said.
The investigators reported no financial conflicts of interest.
REV, Metras Beat Rastelli for TGA, VSD, and LVOTO
Optimal surgical management of patients with transposition of the great arteries, ventricular septal defect, and left ventricular outflow obstruction is still considered controversial. Although the Rastelli operation is the most commonly performed procedure, the Réparation à l'Etage Ventriculaire procedure and Metras modification yielded the best long-term results for both survival and event-free survival, according to a retrospective study of 146 patients who underwent surgery from 1980 to 2008 in eight European hospitals.
The multicenter study compared use and outcomes of several different surgical operations for transposition of the great arteries (TGA), ventricular septal defect (VSD), and left ventricular outflow obstruction (LVOTO), according to a report published in the European Journal of Cardio-thoracic Surgery.
A total of 141 patients had TGA, VSD, and LVOTO; 5 patients had the TGA type of double-outlet right ventricle (DORV) with LVOTO. Only those patients for whom the surgical method chosen was equivalent to those for TGA, VSD, and LVOTO were included in the study; all other DORV types were excluded, according to Dr. Mark Gerard Hazekamp of Leids Universitair Medisch Centrum, Leiden, the Netherlands, and his colleagues from various European universities on behalf of the European Congenital Heart Surgeons Association.
The procedures investigated were the Rastelli (82 patients), arterial (24) and atrial (5) switch operation with relief of LVOTO, Reparation l'Etage Ventriculaire (REV) procedure (7), and Metras modification (24), as well as the Nikaidoh (4). The type of surgery used has traditionally been different in different countries, they said, with the REV procedure and Metras modification mainly in France and the Rastelli procedure being the norm in most other countries.
Patients had a median age at operation of 21.5 months (range 0.2-165.1 months) and a median weight of 10 kg (range 2.0-41.0 kg). Pulmonary stenosis was found in 119 patients, while 27 had pulmonary atresia. LVOTO was solely valvar in 24% of the patients, only subvalvar in 37% of patients, and multilevel in 39%.
The location of the most important VSD was known in 143 patients, with outlet septum in 102, inlet septum in 14, trabecular septum in 3, and a combination of the three in 24 patients. The great majority of the 140 patients for whom data were available had great artery commitment of the biggest VSD: to the aorta in 60, the pulmonary artery in 32, and doubly committed to both in 19. Only 29 patients had noncommitment of one of the great arteries to the VSD.
Overall postoperative survival was 92% at 1 month, 88% at 1 year, 88% at 10 years, and 58% at 20 years. Events were followed as an outcome and were defined as death, reoperation, transcatheter intervention, or cardiac transplantation. The frequent necessity of reintervention (40.7% over follow-up) caused the overall event-free survival to be lower: 85% at 1 month, 80% at 1 year, 45% at 10 years, and 26% at 20 years (Euro. J. Cardiothorac. Surg. 2010;38:699-706).
There were 41 surgical reinterventions and 20 percutaneous procedures, with the most frequent cause of reoperation being RVOT obstruction, including conduit failure (25.0%), followed by LVOT obstruction (7.9%), residual VSD closure (7.1%), and pulmonary artery plasty (4.3%).
In multivariate analysis, age at the corrective surgery, year of the operation, and type of operation were significant predictors for reoperation and trans-catheter intervention, in general, as well as for RVOT reoperation/intervention. The younger the patient at the time of operation, the higher the risk of later reoperation, leading the researchers to speculate that the more recent the surgery, the less the probability that a patient would undergo reoperation.
Reoperation for RVOTO was most common in patients with a Rastelli operation, according to the authors.
"Although there are some differences between Rastelli outcomes among different groups, the all-over rates of freedom from reoperation and, especially, event-free survival, are not satisfactory with event-free survival rates at 10 years that vary from 24% to 49%," they said.
"The Rastelli procedure was a significant independent risk factor for re-operation, with the REV/Metras and the Nikaidoh having the lowest re-intervention rates," they wrote.
They indicated more patients need to be studied with longer follow-up, especially for the Nikaidoh technique.
The authors had no disclosures.
Optimal surgical management of patients with transposition of the great arteries, ventricular septal defect, and left ventricular outflow obstruction is still considered controversial. Although the Rastelli operation is the most commonly performed procedure, the Réparation à l'Etage Ventriculaire procedure and Metras modification yielded the best long-term results for both survival and event-free survival, according to a retrospective study of 146 patients who underwent surgery from 1980 to 2008 in eight European hospitals.
The multicenter study compared use and outcomes of several different surgical operations for transposition of the great arteries (TGA), ventricular septal defect (VSD), and left ventricular outflow obstruction (LVOTO), according to a report published in the European Journal of Cardio-thoracic Surgery.
A total of 141 patients had TGA, VSD, and LVOTO; 5 patients had the TGA type of double-outlet right ventricle (DORV) with LVOTO. Only those patients for whom the surgical method chosen was equivalent to those for TGA, VSD, and LVOTO were included in the study; all other DORV types were excluded, according to Dr. Mark Gerard Hazekamp of Leids Universitair Medisch Centrum, Leiden, the Netherlands, and his colleagues from various European universities on behalf of the European Congenital Heart Surgeons Association.
The procedures investigated were the Rastelli (82 patients), arterial (24) and atrial (5) switch operation with relief of LVOTO, Reparation l'Etage Ventriculaire (REV) procedure (7), and Metras modification (24), as well as the Nikaidoh (4). The type of surgery used has traditionally been different in different countries, they said, with the REV procedure and Metras modification mainly in France and the Rastelli procedure being the norm in most other countries.
Patients had a median age at operation of 21.5 months (range 0.2-165.1 months) and a median weight of 10 kg (range 2.0-41.0 kg). Pulmonary stenosis was found in 119 patients, while 27 had pulmonary atresia. LVOTO was solely valvar in 24% of the patients, only subvalvar in 37% of patients, and multilevel in 39%.
The location of the most important VSD was known in 143 patients, with outlet septum in 102, inlet septum in 14, trabecular septum in 3, and a combination of the three in 24 patients. The great majority of the 140 patients for whom data were available had great artery commitment of the biggest VSD: to the aorta in 60, the pulmonary artery in 32, and doubly committed to both in 19. Only 29 patients had noncommitment of one of the great arteries to the VSD.
Overall postoperative survival was 92% at 1 month, 88% at 1 year, 88% at 10 years, and 58% at 20 years. Events were followed as an outcome and were defined as death, reoperation, transcatheter intervention, or cardiac transplantation. The frequent necessity of reintervention (40.7% over follow-up) caused the overall event-free survival to be lower: 85% at 1 month, 80% at 1 year, 45% at 10 years, and 26% at 20 years (Euro. J. Cardiothorac. Surg. 2010;38:699-706).
There were 41 surgical reinterventions and 20 percutaneous procedures, with the most frequent cause of reoperation being RVOT obstruction, including conduit failure (25.0%), followed by LVOT obstruction (7.9%), residual VSD closure (7.1%), and pulmonary artery plasty (4.3%).
In multivariate analysis, age at the corrective surgery, year of the operation, and type of operation were significant predictors for reoperation and trans-catheter intervention, in general, as well as for RVOT reoperation/intervention. The younger the patient at the time of operation, the higher the risk of later reoperation, leading the researchers to speculate that the more recent the surgery, the less the probability that a patient would undergo reoperation.
Reoperation for RVOTO was most common in patients with a Rastelli operation, according to the authors.
"Although there are some differences between Rastelli outcomes among different groups, the all-over rates of freedom from reoperation and, especially, event-free survival, are not satisfactory with event-free survival rates at 10 years that vary from 24% to 49%," they said.
"The Rastelli procedure was a significant independent risk factor for re-operation, with the REV/Metras and the Nikaidoh having the lowest re-intervention rates," they wrote.
They indicated more patients need to be studied with longer follow-up, especially for the Nikaidoh technique.
The authors had no disclosures.
Optimal surgical management of patients with transposition of the great arteries, ventricular septal defect, and left ventricular outflow obstruction is still considered controversial. Although the Rastelli operation is the most commonly performed procedure, the Réparation à l'Etage Ventriculaire procedure and Metras modification yielded the best long-term results for both survival and event-free survival, according to a retrospective study of 146 patients who underwent surgery from 1980 to 2008 in eight European hospitals.
The multicenter study compared use and outcomes of several different surgical operations for transposition of the great arteries (TGA), ventricular septal defect (VSD), and left ventricular outflow obstruction (LVOTO), according to a report published in the European Journal of Cardio-thoracic Surgery.
A total of 141 patients had TGA, VSD, and LVOTO; 5 patients had the TGA type of double-outlet right ventricle (DORV) with LVOTO. Only those patients for whom the surgical method chosen was equivalent to those for TGA, VSD, and LVOTO were included in the study; all other DORV types were excluded, according to Dr. Mark Gerard Hazekamp of Leids Universitair Medisch Centrum, Leiden, the Netherlands, and his colleagues from various European universities on behalf of the European Congenital Heart Surgeons Association.
The procedures investigated were the Rastelli (82 patients), arterial (24) and atrial (5) switch operation with relief of LVOTO, Reparation l'Etage Ventriculaire (REV) procedure (7), and Metras modification (24), as well as the Nikaidoh (4). The type of surgery used has traditionally been different in different countries, they said, with the REV procedure and Metras modification mainly in France and the Rastelli procedure being the norm in most other countries.
Patients had a median age at operation of 21.5 months (range 0.2-165.1 months) and a median weight of 10 kg (range 2.0-41.0 kg). Pulmonary stenosis was found in 119 patients, while 27 had pulmonary atresia. LVOTO was solely valvar in 24% of the patients, only subvalvar in 37% of patients, and multilevel in 39%.
The location of the most important VSD was known in 143 patients, with outlet septum in 102, inlet septum in 14, trabecular septum in 3, and a combination of the three in 24 patients. The great majority of the 140 patients for whom data were available had great artery commitment of the biggest VSD: to the aorta in 60, the pulmonary artery in 32, and doubly committed to both in 19. Only 29 patients had noncommitment of one of the great arteries to the VSD.
Overall postoperative survival was 92% at 1 month, 88% at 1 year, 88% at 10 years, and 58% at 20 years. Events were followed as an outcome and were defined as death, reoperation, transcatheter intervention, or cardiac transplantation. The frequent necessity of reintervention (40.7% over follow-up) caused the overall event-free survival to be lower: 85% at 1 month, 80% at 1 year, 45% at 10 years, and 26% at 20 years (Euro. J. Cardiothorac. Surg. 2010;38:699-706).
There were 41 surgical reinterventions and 20 percutaneous procedures, with the most frequent cause of reoperation being RVOT obstruction, including conduit failure (25.0%), followed by LVOT obstruction (7.9%), residual VSD closure (7.1%), and pulmonary artery plasty (4.3%).
In multivariate analysis, age at the corrective surgery, year of the operation, and type of operation were significant predictors for reoperation and trans-catheter intervention, in general, as well as for RVOT reoperation/intervention. The younger the patient at the time of operation, the higher the risk of later reoperation, leading the researchers to speculate that the more recent the surgery, the less the probability that a patient would undergo reoperation.
Reoperation for RVOTO was most common in patients with a Rastelli operation, according to the authors.
"Although there are some differences between Rastelli outcomes among different groups, the all-over rates of freedom from reoperation and, especially, event-free survival, are not satisfactory with event-free survival rates at 10 years that vary from 24% to 49%," they said.
"The Rastelli procedure was a significant independent risk factor for re-operation, with the REV/Metras and the Nikaidoh having the lowest re-intervention rates," they wrote.
They indicated more patients need to be studied with longer follow-up, especially for the Nikaidoh technique.
The authors had no disclosures.
Clinical Challenge
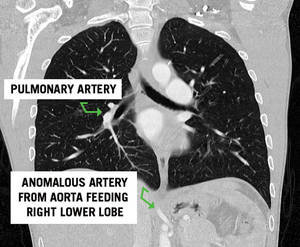
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.