User login
Teen survives double lung transplant after vaping injury
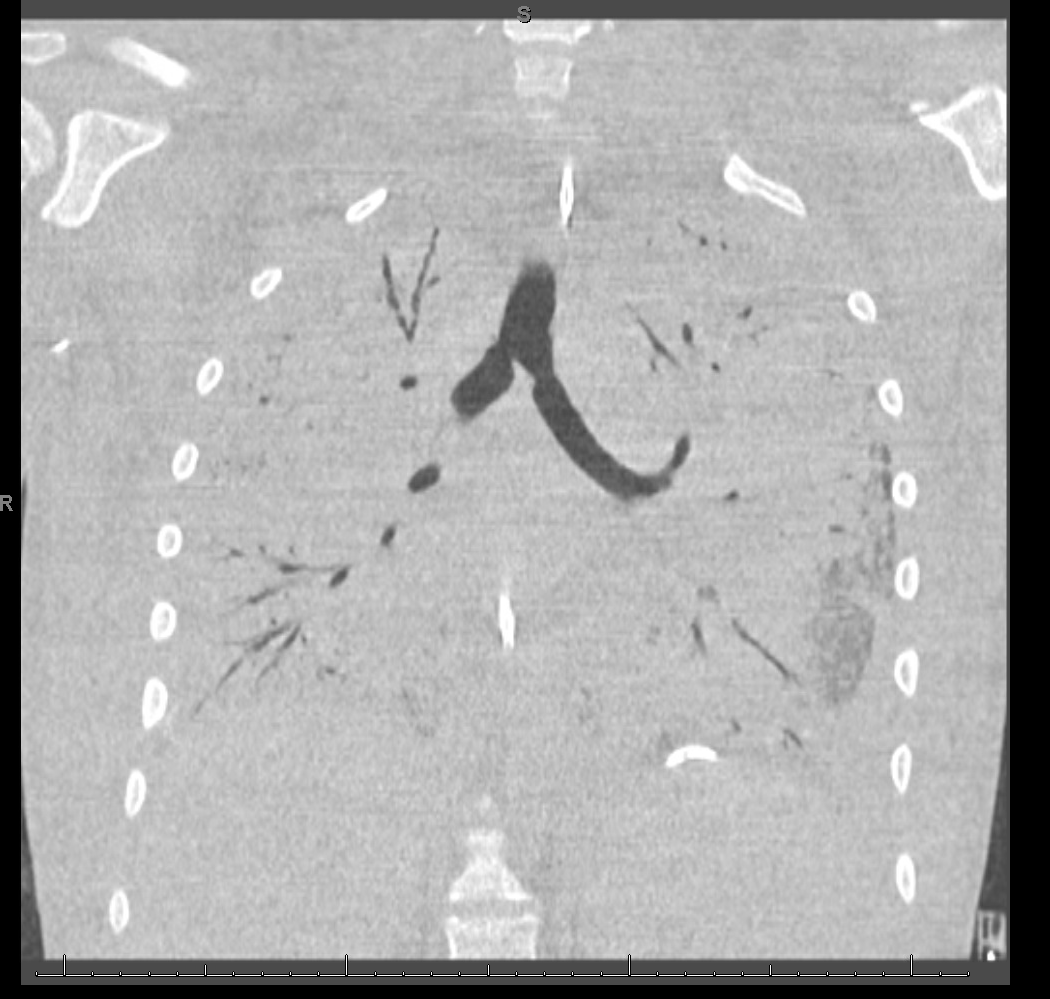
A Michigan teenager, described as an athlete and otherwise healthy, has survived a double lung transplant following lung damage attributed to vaping.

“On the 15th of October, the transplant team performed what we believe is the first double lung transplant done in the nation for a vaping-injury victim, who is a teenager,” Hassan Nemeh, MD, cardiothoracic surgeon with the Henry Ford Health System in Detroit, said during a Nov. 12, 2019, press conference to discuss the surgery.
“What I saw in his lungs is nothing that I have ever seen before and I have been doing lung transplants for 20 years,” Dr. Nemeh said. “There was an enormous amount of inflammation and scarring, in addition to multiple spots of dead tissue. The lung itself was so firm and scarred, we had to deliver it out of the chest. This is an evil that I haven’t faced before.”
He noted that the patient, now 17 years old but 16 when the surgical procedure occurred, is doing well in his recovery, and although the patient and the family are not yet ready to be identified, the health system made the decision to tell the story of the surgery as a cautionary tale.
“The reason we wanted to bring this case to public attention is because of the epidemic of e-cigarettes and vaping-induced lung injury that we are witnessing in the country,” including more than 2,000 cases of injury and 39 deaths that have been confirmed from lung failure related to e-cigarettes and vaping that have been reported to the Centers for Disease Control and Prevention, he said.
“Our teenage patient would have faced certain death if it weren’t for the lung transplant happening,” Dr. Nemeh said, adding that, while vaping and e-cigarettes are being presented as a benign habit, there are potentially very deadly consequences that Henry Ford Hospital System wanted to highlight. He described the patient’s lungs as essentially being nonfunctional with very little air being able to be passed into them, with the destruction to his native lung from pneumonia and dead tissue almost completely covering his lungs.
This story began with a morning call on Oct. 1 from the Children’s Hospital of Michigan alerting the Henry Ford Health System that they had a patient on life support because of complete lung failure who was not showing signs of healing and asking if the Henry Ford Health System could possibly handle a lung transplant for this patient.
Dr. Nemeh said that the patient was on a nontransportable extracorporeal membrane oxygenation (ECMO) machine at Children’s. Dr. Nemeh and the team at Henry Ford determined that the situation for the patient was so dire that they put a portable ECMO machine into the trunk of Dr. Nemeh’s car and delivered it to Children’s in order to facilitate the transfer of the patient for transplantation surgery.
Victor Coba, MD, a critical care specialist and medical director of the ECMO program at Henry Ford, said: “We evaluated the irreversible lung damage that had occurred associated with vaping. Working closely with the lung transplant team and noting that his lungs would not recover, we worked to get him on the lung transplant list.”
Lisa Allenspach, MD, pulmonologist and medical director of the lung transplant program at Henry Ford, reiterated the need for caution when it comes to vaping and e-cigarette use.
“Vaping-related injuries are all too common these days and, actually, our adolescents are faced with a crisis,” she said. “I believe we are just beginning to see the tip of the iceberg. Making sure that our teens understand the danger of vaping is of paramount importance.”
She did not disclose specific details about the teen’s use of vaping/e-cigarette products, so it is unknown whether the injury was caused by standard off-the-shelf products or if it was related to vaping cartridges containing tetrahydrocannabinol.
“We are here today to beg the public to pay special attention to the steps that were taken in this case,” said Nicholas Yeldo, MD, anesthesiology and critical care specialist with Henry Ford. “Without the heroic measures that were taken in this case, this young patient would have died. There is no doubt about it. ... This was not just an unlucky one. This is happening way, way too much.”
Dr. Allenspach was positive that the young patient could live a long life, noting that there are those who have received lung transplants have survived for 15-20 years and second transplants are possible.
A Michigan teenager, described as an athlete and otherwise healthy, has survived a double lung transplant following lung damage attributed to vaping.
“On the 15th of October, the transplant team performed what we believe is the first double lung transplant done in the nation for a vaping-injury victim, who is a teenager,” Hassan Nemeh, MD, cardiothoracic surgeon with the Henry Ford Health System in Detroit, said during a Nov. 12, 2019, press conference to discuss the surgery.
“What I saw in his lungs is nothing that I have ever seen before and I have been doing lung transplants for 20 years,” Dr. Nemeh said. “There was an enormous amount of inflammation and scarring, in addition to multiple spots of dead tissue. The lung itself was so firm and scarred, we had to deliver it out of the chest. This is an evil that I haven’t faced before.”
He noted that the patient, now 17 years old but 16 when the surgical procedure occurred, is doing well in his recovery, and although the patient and the family are not yet ready to be identified, the health system made the decision to tell the story of the surgery as a cautionary tale.
“The reason we wanted to bring this case to public attention is because of the epidemic of e-cigarettes and vaping-induced lung injury that we are witnessing in the country,” including more than 2,000 cases of injury and 39 deaths that have been confirmed from lung failure related to e-cigarettes and vaping that have been reported to the Centers for Disease Control and Prevention, he said.
“Our teenage patient would have faced certain death if it weren’t for the lung transplant happening,” Dr. Nemeh said, adding that, while vaping and e-cigarettes are being presented as a benign habit, there are potentially very deadly consequences that Henry Ford Hospital System wanted to highlight. He described the patient’s lungs as essentially being nonfunctional with very little air being able to be passed into them, with the destruction to his native lung from pneumonia and dead tissue almost completely covering his lungs.
This story began with a morning call on Oct. 1 from the Children’s Hospital of Michigan alerting the Henry Ford Health System that they had a patient on life support because of complete lung failure who was not showing signs of healing and asking if the Henry Ford Health System could possibly handle a lung transplant for this patient.
Dr. Nemeh said that the patient was on a nontransportable extracorporeal membrane oxygenation (ECMO) machine at Children’s. Dr. Nemeh and the team at Henry Ford determined that the situation for the patient was so dire that they put a portable ECMO machine into the trunk of Dr. Nemeh’s car and delivered it to Children’s in order to facilitate the transfer of the patient for transplantation surgery.
Victor Coba, MD, a critical care specialist and medical director of the ECMO program at Henry Ford, said: “We evaluated the irreversible lung damage that had occurred associated with vaping. Working closely with the lung transplant team and noting that his lungs would not recover, we worked to get him on the lung transplant list.”
Lisa Allenspach, MD, pulmonologist and medical director of the lung transplant program at Henry Ford, reiterated the need for caution when it comes to vaping and e-cigarette use.
“Vaping-related injuries are all too common these days and, actually, our adolescents are faced with a crisis,” she said. “I believe we are just beginning to see the tip of the iceberg. Making sure that our teens understand the danger of vaping is of paramount importance.”
She did not disclose specific details about the teen’s use of vaping/e-cigarette products, so it is unknown whether the injury was caused by standard off-the-shelf products or if it was related to vaping cartridges containing tetrahydrocannabinol.
“We are here today to beg the public to pay special attention to the steps that were taken in this case,” said Nicholas Yeldo, MD, anesthesiology and critical care specialist with Henry Ford. “Without the heroic measures that were taken in this case, this young patient would have died. There is no doubt about it. ... This was not just an unlucky one. This is happening way, way too much.”
Dr. Allenspach was positive that the young patient could live a long life, noting that there are those who have received lung transplants have survived for 15-20 years and second transplants are possible.
A Michigan teenager, described as an athlete and otherwise healthy, has survived a double lung transplant following lung damage attributed to vaping.
“On the 15th of October, the transplant team performed what we believe is the first double lung transplant done in the nation for a vaping-injury victim, who is a teenager,” Hassan Nemeh, MD, cardiothoracic surgeon with the Henry Ford Health System in Detroit, said during a Nov. 12, 2019, press conference to discuss the surgery.
“What I saw in his lungs is nothing that I have ever seen before and I have been doing lung transplants for 20 years,” Dr. Nemeh said. “There was an enormous amount of inflammation and scarring, in addition to multiple spots of dead tissue. The lung itself was so firm and scarred, we had to deliver it out of the chest. This is an evil that I haven’t faced before.”
He noted that the patient, now 17 years old but 16 when the surgical procedure occurred, is doing well in his recovery, and although the patient and the family are not yet ready to be identified, the health system made the decision to tell the story of the surgery as a cautionary tale.
“The reason we wanted to bring this case to public attention is because of the epidemic of e-cigarettes and vaping-induced lung injury that we are witnessing in the country,” including more than 2,000 cases of injury and 39 deaths that have been confirmed from lung failure related to e-cigarettes and vaping that have been reported to the Centers for Disease Control and Prevention, he said.
“Our teenage patient would have faced certain death if it weren’t for the lung transplant happening,” Dr. Nemeh said, adding that, while vaping and e-cigarettes are being presented as a benign habit, there are potentially very deadly consequences that Henry Ford Hospital System wanted to highlight. He described the patient’s lungs as essentially being nonfunctional with very little air being able to be passed into them, with the destruction to his native lung from pneumonia and dead tissue almost completely covering his lungs.
This story began with a morning call on Oct. 1 from the Children’s Hospital of Michigan alerting the Henry Ford Health System that they had a patient on life support because of complete lung failure who was not showing signs of healing and asking if the Henry Ford Health System could possibly handle a lung transplant for this patient.
Dr. Nemeh said that the patient was on a nontransportable extracorporeal membrane oxygenation (ECMO) machine at Children’s. Dr. Nemeh and the team at Henry Ford determined that the situation for the patient was so dire that they put a portable ECMO machine into the trunk of Dr. Nemeh’s car and delivered it to Children’s in order to facilitate the transfer of the patient for transplantation surgery.
Victor Coba, MD, a critical care specialist and medical director of the ECMO program at Henry Ford, said: “We evaluated the irreversible lung damage that had occurred associated with vaping. Working closely with the lung transplant team and noting that his lungs would not recover, we worked to get him on the lung transplant list.”
Lisa Allenspach, MD, pulmonologist and medical director of the lung transplant program at Henry Ford, reiterated the need for caution when it comes to vaping and e-cigarette use.
“Vaping-related injuries are all too common these days and, actually, our adolescents are faced with a crisis,” she said. “I believe we are just beginning to see the tip of the iceberg. Making sure that our teens understand the danger of vaping is of paramount importance.”
She did not disclose specific details about the teen’s use of vaping/e-cigarette products, so it is unknown whether the injury was caused by standard off-the-shelf products or if it was related to vaping cartridges containing tetrahydrocannabinol.
“We are here today to beg the public to pay special attention to the steps that were taken in this case,” said Nicholas Yeldo, MD, anesthesiology and critical care specialist with Henry Ford. “Without the heroic measures that were taken in this case, this young patient would have died. There is no doubt about it. ... This was not just an unlucky one. This is happening way, way too much.”
Dr. Allenspach was positive that the young patient could live a long life, noting that there are those who have received lung transplants have survived for 15-20 years and second transplants are possible.
Worse air quality linked to premature deaths
, according to a working paper issued by the National Bureau of Economic Research.

The increase in air pollution, defined as the amount of fine particulate matter (PM2.5) in the air, was associated with an additional 9,700 premature deaths from 2016 to 2018, representing damages totaling $89 billion, wrote Karen Clay and Nicholas C. Miller of Carnegie Mellon University, Pittsburgh. The increase may reflect in part the impact of the a major wildfire that occurred in the fall of 2018.
“These increases are worrisome, because previous studies have shown that PM2.5 increases premature mortality risk,” the researchers wrote. To assess the changes in air quality, they reviewed data from the Air Quality System (AQS) database including total PM2.5 and three PM2.5 species: ammonium nitrate, sulfate, and elemental carbon.
To examine the impact of pollution on public health, the researchers used data from the damage function approach used in the Environmental Protection Agency’s Benefit-Cost Analysis of the Clean Air Act, the Regulatory Impact Analysis for PM2.5, and multiple academic studies.
The number of premature deaths linked to PM2.5 increased by approximately 4,900 between 2016 and 2017 and by 9,700 from 2016 to 2018 in U.S. counties with monitors.
Elderly individuals are especially vulnerable to particulate matter exposure and experience approximately 80% of the burden of disease related to pollution, the researchers said.
“While some deaths among the elderly are shifted by days or weeks, recent research suggests that the burden is ‘concentrated among the elderly with 5-10 years of remaining life expectancy, followed by those with 2-5 years remaining, because these groups represent a large fraction of the Medicare population and are also vulnerable to acute particulate matter exposure,’” they said.
Overall, pollution levels across the United States stopped declining in 2016. When broken down by four Census regions, no change in PM2.5 levels occurred in the Northeast and South between 2016 and 2018; the Midwest and West showed increases in PM2.5 of 9.3% and 11.5%, respectively.
The researchers suggested three possible factors affecting the increase in pollution: economic activity, wildfires, and air quality enforcement. They noted that increases in PM2.5 were especially high in California, and that California accounted for 43% of the increase in pollution-related premature deaths nationwide between 2016 and 2018. When the researchers examined PM2.5 month by month, “November 2018 had an outsized effect on our mortality calculations,” largely because the devastating Camp Fire occurred in California at that time, they said.
With regard to the impact of economic activity on pollution, the researchers reviewed data from the National Highway Administration and Energy Information Administration that showed increased use of natural gas and increased vehicle travel as contributing to higher levels of nitrate and elemental carbon in the air.
Finally, the researchers reported that enforcement of the Clean Air Act appeared to have declined since 2013, and this decline, although it might reflect increased compliance in some areas “is concerning in light of the increases in air pollution in both attainment and nonattainment counties after 2016,” they said.
The researchers had no financial conflicts to disclose.
SOURCE: Clay K, Miller NZ. NBER 2019. Working Paper 26381. doi: 10.3386/w26381.
, according to a working paper issued by the National Bureau of Economic Research.
The increase in air pollution, defined as the amount of fine particulate matter (PM2.5) in the air, was associated with an additional 9,700 premature deaths from 2016 to 2018, representing damages totaling $89 billion, wrote Karen Clay and Nicholas C. Miller of Carnegie Mellon University, Pittsburgh. The increase may reflect in part the impact of the a major wildfire that occurred in the fall of 2018.
“These increases are worrisome, because previous studies have shown that PM2.5 increases premature mortality risk,” the researchers wrote. To assess the changes in air quality, they reviewed data from the Air Quality System (AQS) database including total PM2.5 and three PM2.5 species: ammonium nitrate, sulfate, and elemental carbon.
To examine the impact of pollution on public health, the researchers used data from the damage function approach used in the Environmental Protection Agency’s Benefit-Cost Analysis of the Clean Air Act, the Regulatory Impact Analysis for PM2.5, and multiple academic studies.
The number of premature deaths linked to PM2.5 increased by approximately 4,900 between 2016 and 2017 and by 9,700 from 2016 to 2018 in U.S. counties with monitors.
Elderly individuals are especially vulnerable to particulate matter exposure and experience approximately 80% of the burden of disease related to pollution, the researchers said.
“While some deaths among the elderly are shifted by days or weeks, recent research suggests that the burden is ‘concentrated among the elderly with 5-10 years of remaining life expectancy, followed by those with 2-5 years remaining, because these groups represent a large fraction of the Medicare population and are also vulnerable to acute particulate matter exposure,’” they said.
Overall, pollution levels across the United States stopped declining in 2016. When broken down by four Census regions, no change in PM2.5 levels occurred in the Northeast and South between 2016 and 2018; the Midwest and West showed increases in PM2.5 of 9.3% and 11.5%, respectively.
The researchers suggested three possible factors affecting the increase in pollution: economic activity, wildfires, and air quality enforcement. They noted that increases in PM2.5 were especially high in California, and that California accounted for 43% of the increase in pollution-related premature deaths nationwide between 2016 and 2018. When the researchers examined PM2.5 month by month, “November 2018 had an outsized effect on our mortality calculations,” largely because the devastating Camp Fire occurred in California at that time, they said.
With regard to the impact of economic activity on pollution, the researchers reviewed data from the National Highway Administration and Energy Information Administration that showed increased use of natural gas and increased vehicle travel as contributing to higher levels of nitrate and elemental carbon in the air.
Finally, the researchers reported that enforcement of the Clean Air Act appeared to have declined since 2013, and this decline, although it might reflect increased compliance in some areas “is concerning in light of the increases in air pollution in both attainment and nonattainment counties after 2016,” they said.
The researchers had no financial conflicts to disclose.
SOURCE: Clay K, Miller NZ. NBER 2019. Working Paper 26381. doi: 10.3386/w26381.
, according to a working paper issued by the National Bureau of Economic Research.
The increase in air pollution, defined as the amount of fine particulate matter (PM2.5) in the air, was associated with an additional 9,700 premature deaths from 2016 to 2018, representing damages totaling $89 billion, wrote Karen Clay and Nicholas C. Miller of Carnegie Mellon University, Pittsburgh. The increase may reflect in part the impact of the a major wildfire that occurred in the fall of 2018.
“These increases are worrisome, because previous studies have shown that PM2.5 increases premature mortality risk,” the researchers wrote. To assess the changes in air quality, they reviewed data from the Air Quality System (AQS) database including total PM2.5 and three PM2.5 species: ammonium nitrate, sulfate, and elemental carbon.
To examine the impact of pollution on public health, the researchers used data from the damage function approach used in the Environmental Protection Agency’s Benefit-Cost Analysis of the Clean Air Act, the Regulatory Impact Analysis for PM2.5, and multiple academic studies.
The number of premature deaths linked to PM2.5 increased by approximately 4,900 between 2016 and 2017 and by 9,700 from 2016 to 2018 in U.S. counties with monitors.
Elderly individuals are especially vulnerable to particulate matter exposure and experience approximately 80% of the burden of disease related to pollution, the researchers said.
“While some deaths among the elderly are shifted by days or weeks, recent research suggests that the burden is ‘concentrated among the elderly with 5-10 years of remaining life expectancy, followed by those with 2-5 years remaining, because these groups represent a large fraction of the Medicare population and are also vulnerable to acute particulate matter exposure,’” they said.
Overall, pollution levels across the United States stopped declining in 2016. When broken down by four Census regions, no change in PM2.5 levels occurred in the Northeast and South between 2016 and 2018; the Midwest and West showed increases in PM2.5 of 9.3% and 11.5%, respectively.
The researchers suggested three possible factors affecting the increase in pollution: economic activity, wildfires, and air quality enforcement. They noted that increases in PM2.5 were especially high in California, and that California accounted for 43% of the increase in pollution-related premature deaths nationwide between 2016 and 2018. When the researchers examined PM2.5 month by month, “November 2018 had an outsized effect on our mortality calculations,” largely because the devastating Camp Fire occurred in California at that time, they said.
With regard to the impact of economic activity on pollution, the researchers reviewed data from the National Highway Administration and Energy Information Administration that showed increased use of natural gas and increased vehicle travel as contributing to higher levels of nitrate and elemental carbon in the air.
Finally, the researchers reported that enforcement of the Clean Air Act appeared to have declined since 2013, and this decline, although it might reflect increased compliance in some areas “is concerning in light of the increases in air pollution in both attainment and nonattainment counties after 2016,” they said.
The researchers had no financial conflicts to disclose.
SOURCE: Clay K, Miller NZ. NBER 2019. Working Paper 26381. doi: 10.3386/w26381.
FROM AN NBER AIR QUALITY STUDY
Benefits of BGF triple fixed-dose therapy consistent in COPD patients without exacerbation history
NEW ORLEANS – When looking specifically at the subgroup patients with no recent exacerbations, in patients with moderate to very severe chronic obstructive pulmonary disorder (COPD), an analysis of the phase 3 KRONOS study shows.

For that subgroup of patients with no moderate to severe exacerbations in the past year, BGF MDI was associated with a nominally significant reduction in the rate of subsequent COPD exacerbations, compared with glycopyrrolate/formoterol fumarate (GFF) MDI, according to investigator Fernando J. Martinez MD, of Weill Cornell Medical College, New York.
Results for the COPD patients with no recent history of exacerbation were consistent with the overall results of KRONOS, suggesting that the benefits of BGF MDI shown in that study were not driven by patients with a recent exacerbation history, Dr. Martinez said at the annual meeting of the American College of Chest Physicians.
“It was clear that the effect of this particular triple did not really appear to be dramatically different by the prior history or not in the comparison of the triple versus dual bronchodilator,” he said in a late-breaking clinical trial session.
About three-quarters of the patients in KRONOS (1,411 out of 1,896) lacked a recent exacerbation history. These patients had a mean age of 65.5 years, 72.8% were male, and 69.9% used inhaled corticosteroids at screening, which are demographics were similar to the overall KRONOS patient population, Dr. Martinez said.
In this subset of patients with no recent exacerbation history, treatment with BGF MDI significantly reduced the rate of moderate or severe exacerbations, compared with GFF MDI, with a treatment incidence rate ratio of 0.52 (95% confidence interval, 0.37-0.72; P = .0001).
“The results were remarkably similar,” Dr. Martinez said. “I was surprised, to be honest with you, when I saw these results. I did not anticipate that would be the case.”
By contrast, BGF MDI did not significantly reduce the rate of moderate or severe exacerbations, compared with budesonide/formoterol fumarate (BFF) MDI or open-label budesonide/formoterol fumarate dihydrate dry-powder inhaler (BUD/FORM DPI) as studied in KRONOS, Dr. Martinez said.
The change from baseline in morning predose trough forced expiratory volume in 1 second (FEV1) at week 24 was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI, according to the investigator. Similarly, the FEV1 area under the curve from 0 to 4 hours was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI.
Dr. Martinez reported disclosures related to AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Chiesi, Sunovion, and Teva.
SOURCE: Martinez FJ et al. CHEST 2019, Abstract.
NEW ORLEANS – When looking specifically at the subgroup patients with no recent exacerbations, in patients with moderate to very severe chronic obstructive pulmonary disorder (COPD), an analysis of the phase 3 KRONOS study shows.
For that subgroup of patients with no moderate to severe exacerbations in the past year, BGF MDI was associated with a nominally significant reduction in the rate of subsequent COPD exacerbations, compared with glycopyrrolate/formoterol fumarate (GFF) MDI, according to investigator Fernando J. Martinez MD, of Weill Cornell Medical College, New York.
Results for the COPD patients with no recent history of exacerbation were consistent with the overall results of KRONOS, suggesting that the benefits of BGF MDI shown in that study were not driven by patients with a recent exacerbation history, Dr. Martinez said at the annual meeting of the American College of Chest Physicians.
“It was clear that the effect of this particular triple did not really appear to be dramatically different by the prior history or not in the comparison of the triple versus dual bronchodilator,” he said in a late-breaking clinical trial session.
About three-quarters of the patients in KRONOS (1,411 out of 1,896) lacked a recent exacerbation history. These patients had a mean age of 65.5 years, 72.8% were male, and 69.9% used inhaled corticosteroids at screening, which are demographics were similar to the overall KRONOS patient population, Dr. Martinez said.
In this subset of patients with no recent exacerbation history, treatment with BGF MDI significantly reduced the rate of moderate or severe exacerbations, compared with GFF MDI, with a treatment incidence rate ratio of 0.52 (95% confidence interval, 0.37-0.72; P = .0001).
“The results were remarkably similar,” Dr. Martinez said. “I was surprised, to be honest with you, when I saw these results. I did not anticipate that would be the case.”
By contrast, BGF MDI did not significantly reduce the rate of moderate or severe exacerbations, compared with budesonide/formoterol fumarate (BFF) MDI or open-label budesonide/formoterol fumarate dihydrate dry-powder inhaler (BUD/FORM DPI) as studied in KRONOS, Dr. Martinez said.
The change from baseline in morning predose trough forced expiratory volume in 1 second (FEV1) at week 24 was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI, according to the investigator. Similarly, the FEV1 area under the curve from 0 to 4 hours was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI.
Dr. Martinez reported disclosures related to AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Chiesi, Sunovion, and Teva.
SOURCE: Martinez FJ et al. CHEST 2019, Abstract.
NEW ORLEANS – When looking specifically at the subgroup patients with no recent exacerbations, in patients with moderate to very severe chronic obstructive pulmonary disorder (COPD), an analysis of the phase 3 KRONOS study shows.
For that subgroup of patients with no moderate to severe exacerbations in the past year, BGF MDI was associated with a nominally significant reduction in the rate of subsequent COPD exacerbations, compared with glycopyrrolate/formoterol fumarate (GFF) MDI, according to investigator Fernando J. Martinez MD, of Weill Cornell Medical College, New York.
Results for the COPD patients with no recent history of exacerbation were consistent with the overall results of KRONOS, suggesting that the benefits of BGF MDI shown in that study were not driven by patients with a recent exacerbation history, Dr. Martinez said at the annual meeting of the American College of Chest Physicians.
“It was clear that the effect of this particular triple did not really appear to be dramatically different by the prior history or not in the comparison of the triple versus dual bronchodilator,” he said in a late-breaking clinical trial session.
About three-quarters of the patients in KRONOS (1,411 out of 1,896) lacked a recent exacerbation history. These patients had a mean age of 65.5 years, 72.8% were male, and 69.9% used inhaled corticosteroids at screening, which are demographics were similar to the overall KRONOS patient population, Dr. Martinez said.
In this subset of patients with no recent exacerbation history, treatment with BGF MDI significantly reduced the rate of moderate or severe exacerbations, compared with GFF MDI, with a treatment incidence rate ratio of 0.52 (95% confidence interval, 0.37-0.72; P = .0001).
“The results were remarkably similar,” Dr. Martinez said. “I was surprised, to be honest with you, when I saw these results. I did not anticipate that would be the case.”
By contrast, BGF MDI did not significantly reduce the rate of moderate or severe exacerbations, compared with budesonide/formoterol fumarate (BFF) MDI or open-label budesonide/formoterol fumarate dihydrate dry-powder inhaler (BUD/FORM DPI) as studied in KRONOS, Dr. Martinez said.
The change from baseline in morning predose trough forced expiratory volume in 1 second (FEV1) at week 24 was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI, according to the investigator. Similarly, the FEV1 area under the curve from 0 to 4 hours was significantly improved for BGF MDI, compared with BFF MDI and BUD/FORM DPI, but not compared with GFF MDI.
Dr. Martinez reported disclosures related to AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Chiesi, Sunovion, and Teva.
SOURCE: Martinez FJ et al. CHEST 2019, Abstract.
REPORTING FROM CHEST 2019
Smokers with PE have higher rate of hospital readmission
NEW ORLEANS – , according to a retrospective study.
The rate of readmission was significantly higher among patients with tobacco dependence, and tobacco dependence was independently associated with an increased risk of readmission.
“This is the first study to quantify the increased rate of hospital readmission due to smoking,” said study investigator Kam Sing Ho, MD, of Mount Sinai St. Luke’s and Mount Sinai West, New York.
Dr. Ho and colleagues described this study and its results in a poster presented at the annual meeting of the American College of Chest Physicians.
The researchers analyzed data on 168,891 hospital admissions of adults with PE, 34.2% of whom had tobacco dependence. Patients with and without tobacco dependence were propensity matched for baseline characteristics (n = 24,262 in each group).
The 30-day readmission rate was significantly higher in patients with tobacco dependence than in those without it – 11.0% and 8.9%, respectively (P less than .001). The most common reason for readmission in both groups was PE.
Dr. Ho said the higher readmission rate among patients with tobacco dependence might be explained by the fact that smokers have a higher level of fibrinogen, which may affect blood viscosity and contribute to thrombus formation (Proc Am Thorac Soc. 2005;2[1]:71-7).
The investigators also found that tobacco dependence was an independent predictor of readmission (hazard ratio, 1.43; P less than .001). And the mortality rate was significantly higher after readmission than after index admission – 6.27% and 3.15%, respectively (P less than .001).
The increased risk of readmission and death among smokers highlights the importance of smoking cessation services. Dr. Ho cited previous research suggesting these services are underused in the hospital setting (BMJ Qual Improv Rep. 2014;3[1]:u204964.w2110).
“Given that smoking is a common phenomenon among patients admitted with pulmonary embolism, we suggest that more rigorous smoking cessation services are implemented prior to discharge for all active smokers,” Dr. Ho said. “[P]atients have the right to be informed on the benefits of smoking cessation and the autonomy to choose. Future research will focus on implementing inpatient smoking cessation at our hospital and its effect on local readmission rate, health resources utilization, and mortality.”
Dr. Ho has no relevant relationships to disclose.
SOURCE: Ho KS et al. CHEST 2019 October. doi: 10.1016/j.chest.2019.08.1551.
NEW ORLEANS – , according to a retrospective study.
The rate of readmission was significantly higher among patients with tobacco dependence, and tobacco dependence was independently associated with an increased risk of readmission.
“This is the first study to quantify the increased rate of hospital readmission due to smoking,” said study investigator Kam Sing Ho, MD, of Mount Sinai St. Luke’s and Mount Sinai West, New York.
Dr. Ho and colleagues described this study and its results in a poster presented at the annual meeting of the American College of Chest Physicians.
The researchers analyzed data on 168,891 hospital admissions of adults with PE, 34.2% of whom had tobacco dependence. Patients with and without tobacco dependence were propensity matched for baseline characteristics (n = 24,262 in each group).
The 30-day readmission rate was significantly higher in patients with tobacco dependence than in those without it – 11.0% and 8.9%, respectively (P less than .001). The most common reason for readmission in both groups was PE.
Dr. Ho said the higher readmission rate among patients with tobacco dependence might be explained by the fact that smokers have a higher level of fibrinogen, which may affect blood viscosity and contribute to thrombus formation (Proc Am Thorac Soc. 2005;2[1]:71-7).
The investigators also found that tobacco dependence was an independent predictor of readmission (hazard ratio, 1.43; P less than .001). And the mortality rate was significantly higher after readmission than after index admission – 6.27% and 3.15%, respectively (P less than .001).
The increased risk of readmission and death among smokers highlights the importance of smoking cessation services. Dr. Ho cited previous research suggesting these services are underused in the hospital setting (BMJ Qual Improv Rep. 2014;3[1]:u204964.w2110).
“Given that smoking is a common phenomenon among patients admitted with pulmonary embolism, we suggest that more rigorous smoking cessation services are implemented prior to discharge for all active smokers,” Dr. Ho said. “[P]atients have the right to be informed on the benefits of smoking cessation and the autonomy to choose. Future research will focus on implementing inpatient smoking cessation at our hospital and its effect on local readmission rate, health resources utilization, and mortality.”
Dr. Ho has no relevant relationships to disclose.
SOURCE: Ho KS et al. CHEST 2019 October. doi: 10.1016/j.chest.2019.08.1551.
NEW ORLEANS – , according to a retrospective study.
The rate of readmission was significantly higher among patients with tobacco dependence, and tobacco dependence was independently associated with an increased risk of readmission.
“This is the first study to quantify the increased rate of hospital readmission due to smoking,” said study investigator Kam Sing Ho, MD, of Mount Sinai St. Luke’s and Mount Sinai West, New York.
Dr. Ho and colleagues described this study and its results in a poster presented at the annual meeting of the American College of Chest Physicians.
The researchers analyzed data on 168,891 hospital admissions of adults with PE, 34.2% of whom had tobacco dependence. Patients with and without tobacco dependence were propensity matched for baseline characteristics (n = 24,262 in each group).
The 30-day readmission rate was significantly higher in patients with tobacco dependence than in those without it – 11.0% and 8.9%, respectively (P less than .001). The most common reason for readmission in both groups was PE.
Dr. Ho said the higher readmission rate among patients with tobacco dependence might be explained by the fact that smokers have a higher level of fibrinogen, which may affect blood viscosity and contribute to thrombus formation (Proc Am Thorac Soc. 2005;2[1]:71-7).
The investigators also found that tobacco dependence was an independent predictor of readmission (hazard ratio, 1.43; P less than .001). And the mortality rate was significantly higher after readmission than after index admission – 6.27% and 3.15%, respectively (P less than .001).
The increased risk of readmission and death among smokers highlights the importance of smoking cessation services. Dr. Ho cited previous research suggesting these services are underused in the hospital setting (BMJ Qual Improv Rep. 2014;3[1]:u204964.w2110).
“Given that smoking is a common phenomenon among patients admitted with pulmonary embolism, we suggest that more rigorous smoking cessation services are implemented prior to discharge for all active smokers,” Dr. Ho said. “[P]atients have the right to be informed on the benefits of smoking cessation and the autonomy to choose. Future research will focus on implementing inpatient smoking cessation at our hospital and its effect on local readmission rate, health resources utilization, and mortality.”
Dr. Ho has no relevant relationships to disclose.
SOURCE: Ho KS et al. CHEST 2019 October. doi: 10.1016/j.chest.2019.08.1551.
REPORTING FROM CHEST 2019
One in five chest tube placements/removals goes awry
SAN FRANCISCO – , according to a prospective observational study conducted at 14 adult trauma centers.
“The sad part is, I don’t know if it was surprisingly high, but I’m glad somebody has taken the time to document it,” said Robert Sawyer, MD, professor of surgery at Western Michigan University, Kalamazoo, Mich., who comoderated the session at the annual clinical congress of the American College of Surgeons, where the study was presented.
The researchers examined error rates in both insertions and removals, and compared some of the practices and characteristics of trauma centers with unusually good or poor records. The work could begin to inform quality improvement initiatives. “That’s very parallel to where we were 20 or 25 years ago with central venous catheters. We used to put them in and thought it was never a problem, and then we started taking a close look at it and found out, yeah, there was a problem. We systematically made our procedures more consistent and had better outcomes. I think chest tubes is going to be ripe for that,” Dr. Sawyer said in an interview.
“In some ways we have been lying to ourselves. We acknowledge that trainees have a high rate of complications in chest tube insertion and removal, but we haven’t fixed it as a systematic problem. We’re behind in our work to reduce complications for this bedside procedure,” echoed the session’s other comoderator, Tam Pham, MD, professor of surgery at the University of Washington, Seattle, in an interview.
The researchers defined chest tube errors as anything that resulted in a need to manipulate, replace, or revise an existing tube; a worsening of the condition that the tube was intended to address; or complications that resulted in additional length of stay or interventions. A total of 381 chest tubes were placed in 273 patients over a 3-month period, about 55% by residents and about 28% by trauma attending physicians. Around 80% were traditional chest tubes, and most of the rest were Pigtail, with a very small fraction of Trocar chest tubes, according to a pie chart displayed by Michaela West, MD, a trauma surgeon at North Memorial Health, Robbinsdale, Minn., who presented the research.
Dr. West reported a wide range of complication rates among the 14 institutions, ranging from under 10% to nearly 60%, and some centers reported far more complications with removal or insertion, while some had closer to an even split. The overall average rate of insertion complications was 18.7%, and the average for removal was 17.7%.
When the researchers looked at some of the best and worst performing centers, they identified some trends. A total of 98.6% of chest tubes were tunneled in the best-performing centers, while 14.3% were tunneled in the worst. An initial air leak was more common in the best performing centers (52.5% versus 21.7%). Higher performing centers had a greater percentage of patients with gunshot wounds (24.3% versus 13%), and had a longer duration of stay (5.3 days versus 3.4 days; P less than .05 for all).
In the single highest performing center, all chest tubes were removed by midlevel individuals, and the other two best performing centers relied on an attending physician or resident. The worst performing centers often had postgraduate year 1 and 2 residents removing the chest tubes.
Dr. West, Dr. Pham, and Dr. Sawyer have no relevant financial disclosures.
SOURCE: West M et al. Clinical Congress 2019 Abstract.
SAN FRANCISCO – , according to a prospective observational study conducted at 14 adult trauma centers.
“The sad part is, I don’t know if it was surprisingly high, but I’m glad somebody has taken the time to document it,” said Robert Sawyer, MD, professor of surgery at Western Michigan University, Kalamazoo, Mich., who comoderated the session at the annual clinical congress of the American College of Surgeons, where the study was presented.
The researchers examined error rates in both insertions and removals, and compared some of the practices and characteristics of trauma centers with unusually good or poor records. The work could begin to inform quality improvement initiatives. “That’s very parallel to where we were 20 or 25 years ago with central venous catheters. We used to put them in and thought it was never a problem, and then we started taking a close look at it and found out, yeah, there was a problem. We systematically made our procedures more consistent and had better outcomes. I think chest tubes is going to be ripe for that,” Dr. Sawyer said in an interview.
“In some ways we have been lying to ourselves. We acknowledge that trainees have a high rate of complications in chest tube insertion and removal, but we haven’t fixed it as a systematic problem. We’re behind in our work to reduce complications for this bedside procedure,” echoed the session’s other comoderator, Tam Pham, MD, professor of surgery at the University of Washington, Seattle, in an interview.
The researchers defined chest tube errors as anything that resulted in a need to manipulate, replace, or revise an existing tube; a worsening of the condition that the tube was intended to address; or complications that resulted in additional length of stay or interventions. A total of 381 chest tubes were placed in 273 patients over a 3-month period, about 55% by residents and about 28% by trauma attending physicians. Around 80% were traditional chest tubes, and most of the rest were Pigtail, with a very small fraction of Trocar chest tubes, according to a pie chart displayed by Michaela West, MD, a trauma surgeon at North Memorial Health, Robbinsdale, Minn., who presented the research.
Dr. West reported a wide range of complication rates among the 14 institutions, ranging from under 10% to nearly 60%, and some centers reported far more complications with removal or insertion, while some had closer to an even split. The overall average rate of insertion complications was 18.7%, and the average for removal was 17.7%.
When the researchers looked at some of the best and worst performing centers, they identified some trends. A total of 98.6% of chest tubes were tunneled in the best-performing centers, while 14.3% were tunneled in the worst. An initial air leak was more common in the best performing centers (52.5% versus 21.7%). Higher performing centers had a greater percentage of patients with gunshot wounds (24.3% versus 13%), and had a longer duration of stay (5.3 days versus 3.4 days; P less than .05 for all).
In the single highest performing center, all chest tubes were removed by midlevel individuals, and the other two best performing centers relied on an attending physician or resident. The worst performing centers often had postgraduate year 1 and 2 residents removing the chest tubes.
Dr. West, Dr. Pham, and Dr. Sawyer have no relevant financial disclosures.
SOURCE: West M et al. Clinical Congress 2019 Abstract.
SAN FRANCISCO – , according to a prospective observational study conducted at 14 adult trauma centers.
“The sad part is, I don’t know if it was surprisingly high, but I’m glad somebody has taken the time to document it,” said Robert Sawyer, MD, professor of surgery at Western Michigan University, Kalamazoo, Mich., who comoderated the session at the annual clinical congress of the American College of Surgeons, where the study was presented.
The researchers examined error rates in both insertions and removals, and compared some of the practices and characteristics of trauma centers with unusually good or poor records. The work could begin to inform quality improvement initiatives. “That’s very parallel to where we were 20 or 25 years ago with central venous catheters. We used to put them in and thought it was never a problem, and then we started taking a close look at it and found out, yeah, there was a problem. We systematically made our procedures more consistent and had better outcomes. I think chest tubes is going to be ripe for that,” Dr. Sawyer said in an interview.
“In some ways we have been lying to ourselves. We acknowledge that trainees have a high rate of complications in chest tube insertion and removal, but we haven’t fixed it as a systematic problem. We’re behind in our work to reduce complications for this bedside procedure,” echoed the session’s other comoderator, Tam Pham, MD, professor of surgery at the University of Washington, Seattle, in an interview.
The researchers defined chest tube errors as anything that resulted in a need to manipulate, replace, or revise an existing tube; a worsening of the condition that the tube was intended to address; or complications that resulted in additional length of stay or interventions. A total of 381 chest tubes were placed in 273 patients over a 3-month period, about 55% by residents and about 28% by trauma attending physicians. Around 80% were traditional chest tubes, and most of the rest were Pigtail, with a very small fraction of Trocar chest tubes, according to a pie chart displayed by Michaela West, MD, a trauma surgeon at North Memorial Health, Robbinsdale, Minn., who presented the research.
Dr. West reported a wide range of complication rates among the 14 institutions, ranging from under 10% to nearly 60%, and some centers reported far more complications with removal or insertion, while some had closer to an even split. The overall average rate of insertion complications was 18.7%, and the average for removal was 17.7%.
When the researchers looked at some of the best and worst performing centers, they identified some trends. A total of 98.6% of chest tubes were tunneled in the best-performing centers, while 14.3% were tunneled in the worst. An initial air leak was more common in the best performing centers (52.5% versus 21.7%). Higher performing centers had a greater percentage of patients with gunshot wounds (24.3% versus 13%), and had a longer duration of stay (5.3 days versus 3.4 days; P less than .05 for all).
In the single highest performing center, all chest tubes were removed by midlevel individuals, and the other two best performing centers relied on an attending physician or resident. The worst performing centers often had postgraduate year 1 and 2 residents removing the chest tubes.
Dr. West, Dr. Pham, and Dr. Sawyer have no relevant financial disclosures.
SOURCE: West M et al. Clinical Congress 2019 Abstract.
REPORTING FROM CLINICAL CONGRESS 2019
Getting high heightens stroke, arrhythmia risks
Stoners, beware: , and people with cannabis use disorder are at a 50% greater risk of being hospitalized for arrhythmias, according to new research presented at the American Heart Association Scientific Sessions 2019.

An analysis of pooled data on nearly 44,000 participants in a cross-sectional survey showed that, among the 13.6% who reported using marijuana within the last 30 days, the adjusted odds ratio for young-onset stroke (aged 18-44 years), compared with non-users, was 2.75, reported Tarang Parekh, MBBS, a health policy researcher of George Mason University in Fairfax, Va., and colleagues.
In a separate study, a retrospective analysis of national inpatient data showed that people diagnosed with cannabis use disorder – a pathological pattern of impaired control, social impairment, risky behavior or physiological adaptation similar in nature to alcoholism – had a 47%-52% increased likelihood of hospitalization for an arrhythmia, reported Rikinkumar S. Patel, MD, a psychiatry resident at Griffin Memorial Hospital in Norman, Okla.
“As these [cannabis] products become increasingly used across the country, getting clearer, scientifically rigorous data is going to be important as we try to understand the overall health effects of cannabis,” said AHA President Robert Harrington, MD, of Stanford (Calif.) University in a statement.
Currently, use of both medical and recreational marijuana is fully legal in 11 U.S. states and the District of Columbia. Medical marijuana is legal with recreational use decriminalized (or penalties reduced) in 28 other states, and totally illegal in 11 other states, according to employee screening firm DISA Global Solutions.
Stroke study
In an oral presentation with simultaneous publication in the AHA journal Stroke, Dr. Parekh and colleagues presented an analysis of pooled data from the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative cross-sectional survey collected by the Centers for Disease Control and Prevention in 2016 and 2017.
They looked at baseline sociodemographic data and created multivariable logistic regression models with state fixed effects to determine whether marijuana use within the last 30 days was associated with young-onset stroke.
They identified 43,860 participants representing a weighted sample of 35.5 million Americans. Of the sample, 63.3% were male, and 13.6 % of all participants reported using marijuana in the last 30 days.
They found in an unadjusted model that marijuana users had an odds ratio for stroke, compared with nonusers, of 1.59 (P less than.1), and in a model adjusted for demographic factors (gender, race, ethnicity, and education) the OR increased to 1.76 (P less than .05).
When they threw risk behavior into the model (physical activity, body mass index, heavy drinking, and cigarette smoking), they saw that the OR for stroke shot up to 2.75 (P less than .01).
“Physicians should ask patients if they use cannabis and counsel them about its potential stroke risk as part of regular doctor visits,” Dr. Parekh said in a statement.
Arrhythmias study

Based on recent studies suggesting that cannabis use may trigger cardiovascular events, Dr. Patel and colleagues studied whether cannabis use disorder may be related to arrhythmias, approaching the question through hospital records.
“The effects of using cannabis are seen within 15 minutes and last for around 3 hours. At lower doses, it is linked to a rapid heartbeat. At higher doses, it is linked to a too-slow heartbeat,” he said in a statement.
Dr. Patel and colleagues conducted a retrospective analysis of the Nationwide Inpatient Sample from 2010-2014, a period during which medical marijuana became legal in several states and recreational marijuana became legal in Colorado and Washington. The sample is a database maintained by the Healthcare Cost and Utilization Project of the U.S. Office of Disease Prevention and Health Promotion.
They identified 570,557 patients aged 15-54 years with a primary diagnosis of arrhythmia, and compared them with a sample of 67,662,082 patients hospitalized with no arrhythmia diagnosed during the same period.
They found a 2.6% incidence of cannabis use disorder among patients hospitalized for arrhythmias. Patients with cannabis use disorder tended to be younger (15- to 24-years-old; OR, 4.23), male (OR, 1.70) and African American (OR, 2.70).
In regression analysis adjusted for demographics and comorbidities, cannabis use disorder was associated with higher odds of arrhythmia hospitalization in young patients, at 1.28 times among 15- to 24-year-olds (95% confidence interval, 1.229-1.346) and 1.52 times for 25- to 34-year-olds (95% CI, 1.469-1.578).
“As medical and recreational cannabis is legalized in many states, it is important to know the difference between therapeutic cannabis dosing for medical purposes and the consequences of cannabis abuse. We urgently need additional research to understand these issues,” Dr. Patel said.
“It’s not proving that there’s a direct link, but it’s raising a suggestion in an observational analysis that [this] indeed might be the case. What that means for clinicians is that, if you’re seeing a patient who is presenting with a symptomatic arrhythmia, adding cannabis usage to your list of questions as you begin to try to understand possible precipitating factors for this arrhythmia seems to be a reasonable thing to do,” Dr. Harrington commented.
Stoners, beware: , and people with cannabis use disorder are at a 50% greater risk of being hospitalized for arrhythmias, according to new research presented at the American Heart Association Scientific Sessions 2019.
An analysis of pooled data on nearly 44,000 participants in a cross-sectional survey showed that, among the 13.6% who reported using marijuana within the last 30 days, the adjusted odds ratio for young-onset stroke (aged 18-44 years), compared with non-users, was 2.75, reported Tarang Parekh, MBBS, a health policy researcher of George Mason University in Fairfax, Va., and colleagues.
In a separate study, a retrospective analysis of national inpatient data showed that people diagnosed with cannabis use disorder – a pathological pattern of impaired control, social impairment, risky behavior or physiological adaptation similar in nature to alcoholism – had a 47%-52% increased likelihood of hospitalization for an arrhythmia, reported Rikinkumar S. Patel, MD, a psychiatry resident at Griffin Memorial Hospital in Norman, Okla.
“As these [cannabis] products become increasingly used across the country, getting clearer, scientifically rigorous data is going to be important as we try to understand the overall health effects of cannabis,” said AHA President Robert Harrington, MD, of Stanford (Calif.) University in a statement.
Currently, use of both medical and recreational marijuana is fully legal in 11 U.S. states and the District of Columbia. Medical marijuana is legal with recreational use decriminalized (or penalties reduced) in 28 other states, and totally illegal in 11 other states, according to employee screening firm DISA Global Solutions.
Stroke study
In an oral presentation with simultaneous publication in the AHA journal Stroke, Dr. Parekh and colleagues presented an analysis of pooled data from the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative cross-sectional survey collected by the Centers for Disease Control and Prevention in 2016 and 2017.
They looked at baseline sociodemographic data and created multivariable logistic regression models with state fixed effects to determine whether marijuana use within the last 30 days was associated with young-onset stroke.
They identified 43,860 participants representing a weighted sample of 35.5 million Americans. Of the sample, 63.3% were male, and 13.6 % of all participants reported using marijuana in the last 30 days.
They found in an unadjusted model that marijuana users had an odds ratio for stroke, compared with nonusers, of 1.59 (P less than.1), and in a model adjusted for demographic factors (gender, race, ethnicity, and education) the OR increased to 1.76 (P less than .05).
When they threw risk behavior into the model (physical activity, body mass index, heavy drinking, and cigarette smoking), they saw that the OR for stroke shot up to 2.75 (P less than .01).
“Physicians should ask patients if they use cannabis and counsel them about its potential stroke risk as part of regular doctor visits,” Dr. Parekh said in a statement.
Arrhythmias study
Based on recent studies suggesting that cannabis use may trigger cardiovascular events, Dr. Patel and colleagues studied whether cannabis use disorder may be related to arrhythmias, approaching the question through hospital records.
“The effects of using cannabis are seen within 15 minutes and last for around 3 hours. At lower doses, it is linked to a rapid heartbeat. At higher doses, it is linked to a too-slow heartbeat,” he said in a statement.
Dr. Patel and colleagues conducted a retrospective analysis of the Nationwide Inpatient Sample from 2010-2014, a period during which medical marijuana became legal in several states and recreational marijuana became legal in Colorado and Washington. The sample is a database maintained by the Healthcare Cost and Utilization Project of the U.S. Office of Disease Prevention and Health Promotion.
They identified 570,557 patients aged 15-54 years with a primary diagnosis of arrhythmia, and compared them with a sample of 67,662,082 patients hospitalized with no arrhythmia diagnosed during the same period.
They found a 2.6% incidence of cannabis use disorder among patients hospitalized for arrhythmias. Patients with cannabis use disorder tended to be younger (15- to 24-years-old; OR, 4.23), male (OR, 1.70) and African American (OR, 2.70).
In regression analysis adjusted for demographics and comorbidities, cannabis use disorder was associated with higher odds of arrhythmia hospitalization in young patients, at 1.28 times among 15- to 24-year-olds (95% confidence interval, 1.229-1.346) and 1.52 times for 25- to 34-year-olds (95% CI, 1.469-1.578).
“As medical and recreational cannabis is legalized in many states, it is important to know the difference between therapeutic cannabis dosing for medical purposes and the consequences of cannabis abuse. We urgently need additional research to understand these issues,” Dr. Patel said.
“It’s not proving that there’s a direct link, but it’s raising a suggestion in an observational analysis that [this] indeed might be the case. What that means for clinicians is that, if you’re seeing a patient who is presenting with a symptomatic arrhythmia, adding cannabis usage to your list of questions as you begin to try to understand possible precipitating factors for this arrhythmia seems to be a reasonable thing to do,” Dr. Harrington commented.
Stoners, beware: , and people with cannabis use disorder are at a 50% greater risk of being hospitalized for arrhythmias, according to new research presented at the American Heart Association Scientific Sessions 2019.
An analysis of pooled data on nearly 44,000 participants in a cross-sectional survey showed that, among the 13.6% who reported using marijuana within the last 30 days, the adjusted odds ratio for young-onset stroke (aged 18-44 years), compared with non-users, was 2.75, reported Tarang Parekh, MBBS, a health policy researcher of George Mason University in Fairfax, Va., and colleagues.
In a separate study, a retrospective analysis of national inpatient data showed that people diagnosed with cannabis use disorder – a pathological pattern of impaired control, social impairment, risky behavior or physiological adaptation similar in nature to alcoholism – had a 47%-52% increased likelihood of hospitalization for an arrhythmia, reported Rikinkumar S. Patel, MD, a psychiatry resident at Griffin Memorial Hospital in Norman, Okla.
“As these [cannabis] products become increasingly used across the country, getting clearer, scientifically rigorous data is going to be important as we try to understand the overall health effects of cannabis,” said AHA President Robert Harrington, MD, of Stanford (Calif.) University in a statement.
Currently, use of both medical and recreational marijuana is fully legal in 11 U.S. states and the District of Columbia. Medical marijuana is legal with recreational use decriminalized (or penalties reduced) in 28 other states, and totally illegal in 11 other states, according to employee screening firm DISA Global Solutions.
Stroke study
In an oral presentation with simultaneous publication in the AHA journal Stroke, Dr. Parekh and colleagues presented an analysis of pooled data from the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative cross-sectional survey collected by the Centers for Disease Control and Prevention in 2016 and 2017.
They looked at baseline sociodemographic data and created multivariable logistic regression models with state fixed effects to determine whether marijuana use within the last 30 days was associated with young-onset stroke.
They identified 43,860 participants representing a weighted sample of 35.5 million Americans. Of the sample, 63.3% were male, and 13.6 % of all participants reported using marijuana in the last 30 days.
They found in an unadjusted model that marijuana users had an odds ratio for stroke, compared with nonusers, of 1.59 (P less than.1), and in a model adjusted for demographic factors (gender, race, ethnicity, and education) the OR increased to 1.76 (P less than .05).
When they threw risk behavior into the model (physical activity, body mass index, heavy drinking, and cigarette smoking), they saw that the OR for stroke shot up to 2.75 (P less than .01).
“Physicians should ask patients if they use cannabis and counsel them about its potential stroke risk as part of regular doctor visits,” Dr. Parekh said in a statement.
Arrhythmias study
Based on recent studies suggesting that cannabis use may trigger cardiovascular events, Dr. Patel and colleagues studied whether cannabis use disorder may be related to arrhythmias, approaching the question through hospital records.
“The effects of using cannabis are seen within 15 minutes and last for around 3 hours. At lower doses, it is linked to a rapid heartbeat. At higher doses, it is linked to a too-slow heartbeat,” he said in a statement.
Dr. Patel and colleagues conducted a retrospective analysis of the Nationwide Inpatient Sample from 2010-2014, a period during which medical marijuana became legal in several states and recreational marijuana became legal in Colorado and Washington. The sample is a database maintained by the Healthcare Cost and Utilization Project of the U.S. Office of Disease Prevention and Health Promotion.
They identified 570,557 patients aged 15-54 years with a primary diagnosis of arrhythmia, and compared them with a sample of 67,662,082 patients hospitalized with no arrhythmia diagnosed during the same period.
They found a 2.6% incidence of cannabis use disorder among patients hospitalized for arrhythmias. Patients with cannabis use disorder tended to be younger (15- to 24-years-old; OR, 4.23), male (OR, 1.70) and African American (OR, 2.70).
In regression analysis adjusted for demographics and comorbidities, cannabis use disorder was associated with higher odds of arrhythmia hospitalization in young patients, at 1.28 times among 15- to 24-year-olds (95% confidence interval, 1.229-1.346) and 1.52 times for 25- to 34-year-olds (95% CI, 1.469-1.578).
“As medical and recreational cannabis is legalized in many states, it is important to know the difference between therapeutic cannabis dosing for medical purposes and the consequences of cannabis abuse. We urgently need additional research to understand these issues,” Dr. Patel said.
“It’s not proving that there’s a direct link, but it’s raising a suggestion in an observational analysis that [this] indeed might be the case. What that means for clinicians is that, if you’re seeing a patient who is presenting with a symptomatic arrhythmia, adding cannabis usage to your list of questions as you begin to try to understand possible precipitating factors for this arrhythmia seems to be a reasonable thing to do,” Dr. Harrington commented.
REPORTING FROM AHA 2019
Tiotropium/olodaterol improved lung function in steroid-free patients with COPD
New Orleans – compared with tiotropium alone, according to results of a pooled analysis of phase 3 trial data.
Lung function, symptoms, and quality of life were all improved irrespective of disease severity and baseline symptoms, and these benefits were apparent across multiple subgroups of non-ICS patients, investigator Peter M. Calverley, MBChB, of the University of Liverpool (England) reported at the annual meeting of the American College of Chest Physicians.
“Perhaps frustratingly, we can’t personalize [treatment] – everybody seemed to get benefit across the board, and the magnitude of that benefit was rather similar,” Dr. Calverley said in a podium presentation of the results.
The subgroup analysis was undertaken to fill a knowledge gap, according to Dr. Calverley, regarding the efficacy of combined long-acting muscarinic antagonist/long-acting beta2-agonist (LAMA/LABA) treatment in the sizable proportion of COPD patients who are not receiving ICS.
Patients in LAMA/LABA clinical trials are frequently taking multiple therapies, including ICS, he explained.
The post hoc analysis of pooled data from the TONADO 1 and 2 and OTEMTO 1 and 2 trials included a total of 1,596 patients with COPD who were not receiving ICS at trial enrollment.
The no-ICS patients receiving tiotropium/olodaterol had a significantly greater improvement in trough forced expiratory volume in 1 second (FEV1) response by week 12 of treatment, compared with patients receiving tiotropium alone (0.054 L; P less than .0001), the researcher reported.
The trough FEV1 improvement accruing to the tiotropium/olodaterol–treated patients was consistent across subgroups stratified according to GOLD stage and symptoms at baseline (such as Baseline Dyspnea Index), he added.
Transition Dyspnea Index (TDI) score at 12 weeks in these patients not receiving ICS was likewise superior in the tiotropium/olodaterol treated patients, compared with the tiotropium monotherapy group (.575; P less than .0001), while changes in St. George’s Respiratory Questionnaire (SGRQ) total scores also favored the combination treatment, according to the analyses presented.
Taken together, results of this post hoc analysis support the use of dual bronchodilator therapy to improve key COPD outcomes, compared with single bronchodilator therapy. In addition, this strategy should be considered as an earlier treatment option, according to Dr. Calverley.
“Clearly dual bronchodilator therapy improves the key outcomes, compared with an effective single bronchodilator, and this perhaps is why it’s being picked up as an earlier treatment option, and certainly in some guidelines like the current [National Institute for Health Care and Excellence] guidelines where I live in the U.K., it’s becoming standard of care for most people with COPD,” he said in his presentation.
Dr. Calverley reported grants and personal fees from GlaxoSmithKline; personal fees from AstraZeneca, Recipharm, and Zambon; and personal and other fees from Boehringer Ingelheim outside the submitted work.
SOURCE: Calverley PM et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.310.
New Orleans – compared with tiotropium alone, according to results of a pooled analysis of phase 3 trial data.
Lung function, symptoms, and quality of life were all improved irrespective of disease severity and baseline symptoms, and these benefits were apparent across multiple subgroups of non-ICS patients, investigator Peter M. Calverley, MBChB, of the University of Liverpool (England) reported at the annual meeting of the American College of Chest Physicians.
“Perhaps frustratingly, we can’t personalize [treatment] – everybody seemed to get benefit across the board, and the magnitude of that benefit was rather similar,” Dr. Calverley said in a podium presentation of the results.
The subgroup analysis was undertaken to fill a knowledge gap, according to Dr. Calverley, regarding the efficacy of combined long-acting muscarinic antagonist/long-acting beta2-agonist (LAMA/LABA) treatment in the sizable proportion of COPD patients who are not receiving ICS.
Patients in LAMA/LABA clinical trials are frequently taking multiple therapies, including ICS, he explained.
The post hoc analysis of pooled data from the TONADO 1 and 2 and OTEMTO 1 and 2 trials included a total of 1,596 patients with COPD who were not receiving ICS at trial enrollment.
The no-ICS patients receiving tiotropium/olodaterol had a significantly greater improvement in trough forced expiratory volume in 1 second (FEV1) response by week 12 of treatment, compared with patients receiving tiotropium alone (0.054 L; P less than .0001), the researcher reported.
The trough FEV1 improvement accruing to the tiotropium/olodaterol–treated patients was consistent across subgroups stratified according to GOLD stage and symptoms at baseline (such as Baseline Dyspnea Index), he added.
Transition Dyspnea Index (TDI) score at 12 weeks in these patients not receiving ICS was likewise superior in the tiotropium/olodaterol treated patients, compared with the tiotropium monotherapy group (.575; P less than .0001), while changes in St. George’s Respiratory Questionnaire (SGRQ) total scores also favored the combination treatment, according to the analyses presented.
Taken together, results of this post hoc analysis support the use of dual bronchodilator therapy to improve key COPD outcomes, compared with single bronchodilator therapy. In addition, this strategy should be considered as an earlier treatment option, according to Dr. Calverley.
“Clearly dual bronchodilator therapy improves the key outcomes, compared with an effective single bronchodilator, and this perhaps is why it’s being picked up as an earlier treatment option, and certainly in some guidelines like the current [National Institute for Health Care and Excellence] guidelines where I live in the U.K., it’s becoming standard of care for most people with COPD,” he said in his presentation.
Dr. Calverley reported grants and personal fees from GlaxoSmithKline; personal fees from AstraZeneca, Recipharm, and Zambon; and personal and other fees from Boehringer Ingelheim outside the submitted work.
SOURCE: Calverley PM et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.310.
New Orleans – compared with tiotropium alone, according to results of a pooled analysis of phase 3 trial data.
Lung function, symptoms, and quality of life were all improved irrespective of disease severity and baseline symptoms, and these benefits were apparent across multiple subgroups of non-ICS patients, investigator Peter M. Calverley, MBChB, of the University of Liverpool (England) reported at the annual meeting of the American College of Chest Physicians.
“Perhaps frustratingly, we can’t personalize [treatment] – everybody seemed to get benefit across the board, and the magnitude of that benefit was rather similar,” Dr. Calverley said in a podium presentation of the results.
The subgroup analysis was undertaken to fill a knowledge gap, according to Dr. Calverley, regarding the efficacy of combined long-acting muscarinic antagonist/long-acting beta2-agonist (LAMA/LABA) treatment in the sizable proportion of COPD patients who are not receiving ICS.
Patients in LAMA/LABA clinical trials are frequently taking multiple therapies, including ICS, he explained.
The post hoc analysis of pooled data from the TONADO 1 and 2 and OTEMTO 1 and 2 trials included a total of 1,596 patients with COPD who were not receiving ICS at trial enrollment.
The no-ICS patients receiving tiotropium/olodaterol had a significantly greater improvement in trough forced expiratory volume in 1 second (FEV1) response by week 12 of treatment, compared with patients receiving tiotropium alone (0.054 L; P less than .0001), the researcher reported.
The trough FEV1 improvement accruing to the tiotropium/olodaterol–treated patients was consistent across subgroups stratified according to GOLD stage and symptoms at baseline (such as Baseline Dyspnea Index), he added.
Transition Dyspnea Index (TDI) score at 12 weeks in these patients not receiving ICS was likewise superior in the tiotropium/olodaterol treated patients, compared with the tiotropium monotherapy group (.575; P less than .0001), while changes in St. George’s Respiratory Questionnaire (SGRQ) total scores also favored the combination treatment, according to the analyses presented.
Taken together, results of this post hoc analysis support the use of dual bronchodilator therapy to improve key COPD outcomes, compared with single bronchodilator therapy. In addition, this strategy should be considered as an earlier treatment option, according to Dr. Calverley.
“Clearly dual bronchodilator therapy improves the key outcomes, compared with an effective single bronchodilator, and this perhaps is why it’s being picked up as an earlier treatment option, and certainly in some guidelines like the current [National Institute for Health Care and Excellence] guidelines where I live in the U.K., it’s becoming standard of care for most people with COPD,” he said in his presentation.
Dr. Calverley reported grants and personal fees from GlaxoSmithKline; personal fees from AstraZeneca, Recipharm, and Zambon; and personal and other fees from Boehringer Ingelheim outside the submitted work.
SOURCE: Calverley PM et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.310.
REPORTING FROM CHEST 2019

Lung cancer screening, early diagnosis still lower among blacks, Hispanics
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
REPORTING FROM CLINICAL CONGRESS 2019
CDC identifies probable culprit in vaping lung injuries
found in lung fluid of victims.

In a telebriefing on Friday, Anne Schuchat, MD, the CDC’s principal deputy director, provided an update on recent lab findings and on case and death numbers reported so far to the CDC. The findings and more case information were published in the Mortality and Morbidity Weekly Report.
At the telebriefing, Dr. Schuchat stated that CDC has received 29 samples of bronchoalveolar lavage (BAL) fluid from EVALI patients from 10 states and that vitamin E acetate was identified in all samples. Vitamin E acetate has already been found in some vaping devices and the discovery of the chemical in the lungs of patients increases the likelihood that this toxin is at least one source of EVALI. These findings are the first to link substances found in vaping products with biological samples from patients hospitalized with EVALI.
Tetrahydrocannabinol (THC) was found in 23 of 28 samples tested and nicotine was found in 16 of 26 samples tested. Other diluents and additives of concern (such as plant oils, medium chain triglyceride oil, petroleum distillates, and diluent terpenes) were not detected in BAL fluid specimens from EVALI patients.
BAL fluid specimens were collected from hospitalized EVALI patients in the course of their treatment, although not for the specific purpose of the CDC investigation, and sent to the CDC by public health laboratories and health departments in California, Connecticut, Hawaii, Illinois, Maryland, Michigan, Minnesota, Texas, Utah, and Wisconsin for analysis.
Dr. Schuchat stated that, as of Nov. 5, there have been 2,051 cases of EVALI reported to the CDC and 39 EVALI patients have died, with other deaths still under investigation as possibly related to EVALI. She said that the trend in new EVALI cases reported appears to be decreasing, but some states continue to see new cases. She cautioned that the lab findings of vitamin E acetate in BAL fluid do not rule out other possible compounds or ingredients that may contribute to EVALI and said the investigation will continue.
E-cigarette user survey
During the telebriefing, Jennifer Layden, MD, PhD, chief medical officer and state epidemiologist with the Illinois Department of Public Health (IDPH), gave an update on her department’s efforts to investigate vaping behaviors that might have led to EVALI in e-cigarette users and also to obtain more information on sources of vaping devices that could be linked to EVALI. The data were also reported in a MMWR.
The IDPH conducted an online public survey during September 2019 to October 2019 targeting e-cigarette, or vaping, product users in Illinois. The survey was promoted via social media on the IDPH website, local health departments, and other outlets. The survey yielded 4,631 respondents who answered questions about the frequency of vaping, sources of supply, and types of substances used. The investigators were then able to compare vaping-use habits and behaviors with similar information gleaned from EVALI patients.
Among survey respondents, 94% reported using any nicotine-containing e-cigarette, or vaping, products in the past 3 months; 21% used any THC-containing products; and 11% used both THC-containing products and nicotine-containing products. THC-containing product use was highest among survey respondents aged 18-24 years (36%) and decreased with increasing age. Compared with these survey respondents, EVALI patients were more likely to report exclusive use of THC-containing products (adjusted odds ratio, 2.0; 95% confidence interval, 1.1-3.6), frequent use (more than five times per day) of these products (aOR, 3.1; 95% CI, 1.6-6.0), and obtaining these products from informal sources, such as from a dealer, off the street, or from a friend (aOR, 9.2; 95% CI, 2.2-39.4). In addition, “the odds of using Dank Vapes, a class of largely counterfeit THC-containing products, was also higher among EVALI patients” (aOR, 8.5; 95% CI, 3.8-19.0), according to the MMWR.
Recommendations
CDC recommends that people should not buy any type of e-cigarette, or vaping, products, particularly those containing THC, off the street. They should also refrain from modifying or adding any substances to e-cigarette, or vaping, products that are not intended by the manufacturer, including products purchased through retail establishments.
Dr. Layden concluded, “we are in a better place today than we were a few weeks ago in terms of having one very strong culprit of concern based on the lung fluid testing,” but since the specific substances causing lung injury are not yet known, the only way to assure that individuals are not at risk while the investigation continues is to consider refraining from use of all vaping products.
For more information and resources visit For the Public, For Healthcare Providers, and For Health Departments pages, as well as the CDC’s Publications and Resources page.
found in lung fluid of victims.
In a telebriefing on Friday, Anne Schuchat, MD, the CDC’s principal deputy director, provided an update on recent lab findings and on case and death numbers reported so far to the CDC. The findings and more case information were published in the Mortality and Morbidity Weekly Report.
At the telebriefing, Dr. Schuchat stated that CDC has received 29 samples of bronchoalveolar lavage (BAL) fluid from EVALI patients from 10 states and that vitamin E acetate was identified in all samples. Vitamin E acetate has already been found in some vaping devices and the discovery of the chemical in the lungs of patients increases the likelihood that this toxin is at least one source of EVALI. These findings are the first to link substances found in vaping products with biological samples from patients hospitalized with EVALI.
Tetrahydrocannabinol (THC) was found in 23 of 28 samples tested and nicotine was found in 16 of 26 samples tested. Other diluents and additives of concern (such as plant oils, medium chain triglyceride oil, petroleum distillates, and diluent terpenes) were not detected in BAL fluid specimens from EVALI patients.
BAL fluid specimens were collected from hospitalized EVALI patients in the course of their treatment, although not for the specific purpose of the CDC investigation, and sent to the CDC by public health laboratories and health departments in California, Connecticut, Hawaii, Illinois, Maryland, Michigan, Minnesota, Texas, Utah, and Wisconsin for analysis.
Dr. Schuchat stated that, as of Nov. 5, there have been 2,051 cases of EVALI reported to the CDC and 39 EVALI patients have died, with other deaths still under investigation as possibly related to EVALI. She said that the trend in new EVALI cases reported appears to be decreasing, but some states continue to see new cases. She cautioned that the lab findings of vitamin E acetate in BAL fluid do not rule out other possible compounds or ingredients that may contribute to EVALI and said the investigation will continue.
E-cigarette user survey
During the telebriefing, Jennifer Layden, MD, PhD, chief medical officer and state epidemiologist with the Illinois Department of Public Health (IDPH), gave an update on her department’s efforts to investigate vaping behaviors that might have led to EVALI in e-cigarette users and also to obtain more information on sources of vaping devices that could be linked to EVALI. The data were also reported in a MMWR.
The IDPH conducted an online public survey during September 2019 to October 2019 targeting e-cigarette, or vaping, product users in Illinois. The survey was promoted via social media on the IDPH website, local health departments, and other outlets. The survey yielded 4,631 respondents who answered questions about the frequency of vaping, sources of supply, and types of substances used. The investigators were then able to compare vaping-use habits and behaviors with similar information gleaned from EVALI patients.
Among survey respondents, 94% reported using any nicotine-containing e-cigarette, or vaping, products in the past 3 months; 21% used any THC-containing products; and 11% used both THC-containing products and nicotine-containing products. THC-containing product use was highest among survey respondents aged 18-24 years (36%) and decreased with increasing age. Compared with these survey respondents, EVALI patients were more likely to report exclusive use of THC-containing products (adjusted odds ratio, 2.0; 95% confidence interval, 1.1-3.6), frequent use (more than five times per day) of these products (aOR, 3.1; 95% CI, 1.6-6.0), and obtaining these products from informal sources, such as from a dealer, off the street, or from a friend (aOR, 9.2; 95% CI, 2.2-39.4). In addition, “the odds of using Dank Vapes, a class of largely counterfeit THC-containing products, was also higher among EVALI patients” (aOR, 8.5; 95% CI, 3.8-19.0), according to the MMWR.
Recommendations
CDC recommends that people should not buy any type of e-cigarette, or vaping, products, particularly those containing THC, off the street. They should also refrain from modifying or adding any substances to e-cigarette, or vaping, products that are not intended by the manufacturer, including products purchased through retail establishments.
Dr. Layden concluded, “we are in a better place today than we were a few weeks ago in terms of having one very strong culprit of concern based on the lung fluid testing,” but since the specific substances causing lung injury are not yet known, the only way to assure that individuals are not at risk while the investigation continues is to consider refraining from use of all vaping products.
For more information and resources visit For the Public, For Healthcare Providers, and For Health Departments pages, as well as the CDC’s Publications and Resources page.
found in lung fluid of victims.
In a telebriefing on Friday, Anne Schuchat, MD, the CDC’s principal deputy director, provided an update on recent lab findings and on case and death numbers reported so far to the CDC. The findings and more case information were published in the Mortality and Morbidity Weekly Report.
At the telebriefing, Dr. Schuchat stated that CDC has received 29 samples of bronchoalveolar lavage (BAL) fluid from EVALI patients from 10 states and that vitamin E acetate was identified in all samples. Vitamin E acetate has already been found in some vaping devices and the discovery of the chemical in the lungs of patients increases the likelihood that this toxin is at least one source of EVALI. These findings are the first to link substances found in vaping products with biological samples from patients hospitalized with EVALI.
Tetrahydrocannabinol (THC) was found in 23 of 28 samples tested and nicotine was found in 16 of 26 samples tested. Other diluents and additives of concern (such as plant oils, medium chain triglyceride oil, petroleum distillates, and diluent terpenes) were not detected in BAL fluid specimens from EVALI patients.
BAL fluid specimens were collected from hospitalized EVALI patients in the course of their treatment, although not for the specific purpose of the CDC investigation, and sent to the CDC by public health laboratories and health departments in California, Connecticut, Hawaii, Illinois, Maryland, Michigan, Minnesota, Texas, Utah, and Wisconsin for analysis.
Dr. Schuchat stated that, as of Nov. 5, there have been 2,051 cases of EVALI reported to the CDC and 39 EVALI patients have died, with other deaths still under investigation as possibly related to EVALI. She said that the trend in new EVALI cases reported appears to be decreasing, but some states continue to see new cases. She cautioned that the lab findings of vitamin E acetate in BAL fluid do not rule out other possible compounds or ingredients that may contribute to EVALI and said the investigation will continue.
E-cigarette user survey
During the telebriefing, Jennifer Layden, MD, PhD, chief medical officer and state epidemiologist with the Illinois Department of Public Health (IDPH), gave an update on her department’s efforts to investigate vaping behaviors that might have led to EVALI in e-cigarette users and also to obtain more information on sources of vaping devices that could be linked to EVALI. The data were also reported in a MMWR.
The IDPH conducted an online public survey during September 2019 to October 2019 targeting e-cigarette, or vaping, product users in Illinois. The survey was promoted via social media on the IDPH website, local health departments, and other outlets. The survey yielded 4,631 respondents who answered questions about the frequency of vaping, sources of supply, and types of substances used. The investigators were then able to compare vaping-use habits and behaviors with similar information gleaned from EVALI patients.
Among survey respondents, 94% reported using any nicotine-containing e-cigarette, or vaping, products in the past 3 months; 21% used any THC-containing products; and 11% used both THC-containing products and nicotine-containing products. THC-containing product use was highest among survey respondents aged 18-24 years (36%) and decreased with increasing age. Compared with these survey respondents, EVALI patients were more likely to report exclusive use of THC-containing products (adjusted odds ratio, 2.0; 95% confidence interval, 1.1-3.6), frequent use (more than five times per day) of these products (aOR, 3.1; 95% CI, 1.6-6.0), and obtaining these products from informal sources, such as from a dealer, off the street, or from a friend (aOR, 9.2; 95% CI, 2.2-39.4). In addition, “the odds of using Dank Vapes, a class of largely counterfeit THC-containing products, was also higher among EVALI patients” (aOR, 8.5; 95% CI, 3.8-19.0), according to the MMWR.
Recommendations
CDC recommends that people should not buy any type of e-cigarette, or vaping, products, particularly those containing THC, off the street. They should also refrain from modifying or adding any substances to e-cigarette, or vaping, products that are not intended by the manufacturer, including products purchased through retail establishments.
Dr. Layden concluded, “we are in a better place today than we were a few weeks ago in terms of having one very strong culprit of concern based on the lung fluid testing,” but since the specific substances causing lung injury are not yet known, the only way to assure that individuals are not at risk while the investigation continues is to consider refraining from use of all vaping products.
For more information and resources visit For the Public, For Healthcare Providers, and For Health Departments pages, as well as the CDC’s Publications and Resources page.
Tide beginning to turn on vaccine hesitancy
NEW ORLEANS –

The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
NEW ORLEANS –
The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
NEW ORLEANS –
The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM AAP 2019